Embed Size (px)
Citation preview

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 1
Narrative Quarterly Report Quarter 2: January 1, 2020 – March 31, 2020
BETTER OUTCOMES FOR CHILDREN AND YOUTH IN EASTERN AND NORTHERN UGANDA
Through the delivery of the No Means No (NMN) program, BOCY is building a generation of young men champions committed to GBV prevention, including these four young men who completed NMN training for BOCY in Q2.
Submission Date: May 20, 2020 Number: AID-617-A-15-00003 Activity Start Date and End Date: April 2015 to April 2021 AOR: Catherine Muwanga Submitted by: Alexander Mugume, Chief of Party
The Bantwana Initiative of World Education, Inc. Email: [email protected] This document was produced for review by the United States Agency for International Development Uganda Mission (USAID/Uganda).

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 1
ACTIVITY OVERVIEW/SUMMARY
Activity Name: Narrative Quarterly Report
Project: Better Outcomes for Children and Youth in Eastern and Northern Uganda
Activity Start Date and End Date:
April 21, 2015 to April 20, 2021
Name of Prime Implementing Partner:
The Bantwana Initiative of World Education, Inc.
[Contract/Agreement] Number:
AID-617-A-15-00003
Name of Sub-contractors/Sub-awardees and Dollar Amounts for FY 2020
Association of Volunteers in International Service Foundation (AVSI-Uganda) - UGX 5,094,104,843 ($1,407,211) Multi Community Based Development Initiative (MUCOBADI) - UGX 2,041,100,888 ($563,840) mothers2mothers (m2m) – UGX 2,208,031,502 ($609,953) SOS Children’s Villages (SOS) – UGX 1,322,091,660 ($365,219) AIDS Information Centre (AIC) – UGX 1,849,104,012 ($510,802)
Geographic Coverage Changes (Districts):
North: Arua, Gulu, Omoro, Oyam, Agago, Kitgum, Lira, Apac, Kwania, Kole, Kotido, and Dokolo (12) East: Mbale, Tororo, Busia, Namayingo, Bugiri, Iganga, Bugweeri, Mayuge, Jinja, and Kamuli (10)
Reporting Period: January 1, 2020 – March 31, 2020

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 2
ACRONYMS AND ABBREVIATIONS AIC AIDS Information Centre ART Antiretroviral Therapy BOCY Better Outcomes for Children and Youth CDO Community Development Officer COMVIS Community Vision Uganda CSO Civil Society Organization CUG Closed-User Group CRP Community Resource Persons DBT District-Based Trainer DOVCC District OVC Committee ECD Early Childhood Development EID Early Infant Diagnosis ES Economic Strengthening ESTO Economic Strengthening Technical Officer GBV Gender-Based Violence HEI HIV-Exposed Infant HHs Households HTS HIV Testing Services IAC Intensive Adherence Counselling IGA Income-Generating Activity LG Local Government LTFU Lost to Follow Up M&E Monitoring and Evaluation MELP Monitoring, Evaluation, and Learning Plan MGSLD Ministry of Gender, Labour and Social Development MIS Management Information System MoH Ministry of Health MUCOBADI Multi Community Based Development Initiative NFE Non-Formal Education NMN No Means No OVC Orphans and Vulnerable Children PEC Peer Educator Club PMTCT Prevention of Mother-to-Child Transmission PSS Psychosocial Support PSW Para-Social Worker SOVCC Sub-County OVC Committee SPM Selection, Planning, and Management VAC Violence Against Children VHT Village Health Team VL Viral Load VMMC Voluntary Medical Male Circumcision VSLA Village Savings and Loan Association WEI/Bantwana The Bantwana Initiative of World Education, Inc.
Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 3
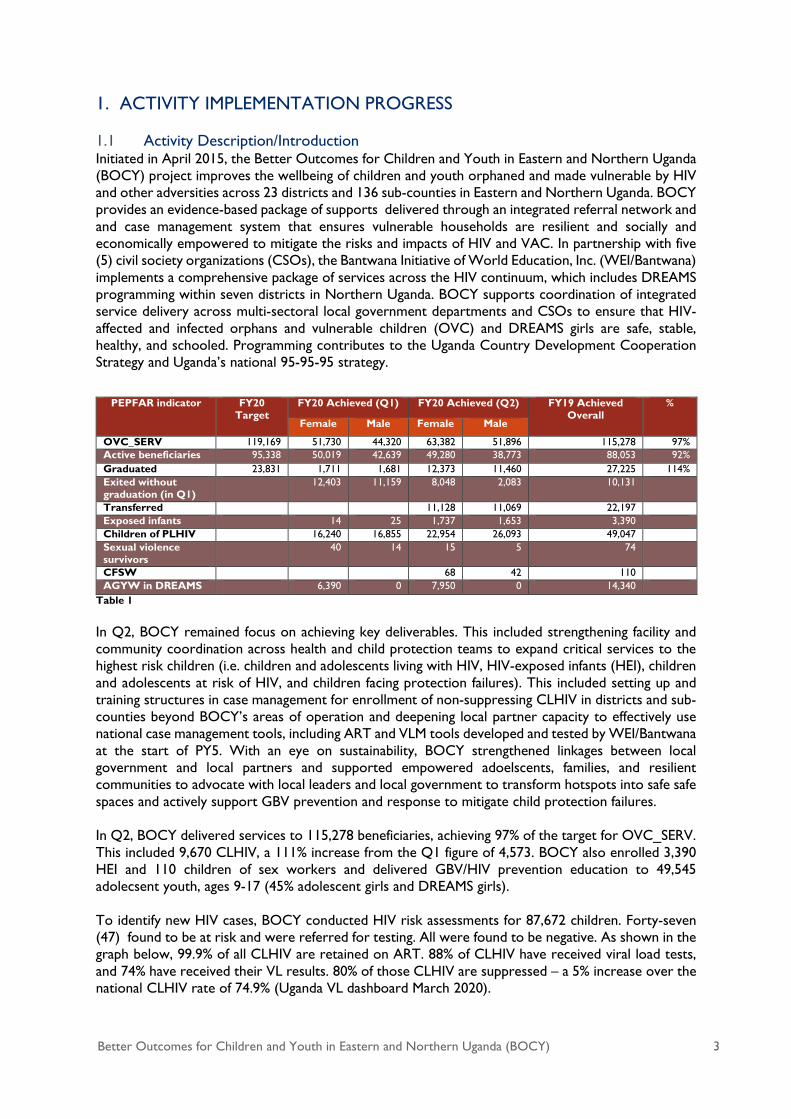
1. ACTIVITY IMPLEMENTATION PROGRESS 1.1 Activity Description/Introduction Initiated in April 2015, the Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) project improves the wellbeing of children and youth orphaned and made vulnerable by HIV and other adversities across 23 districts and 136 sub-counties in Eastern and Northern Uganda. BOCY provides an evidence-based package of supports delivered through an integrated referral network and and case management system that ensures vulnerable households are resilient and socially and economically empowered to mitigate the risks and impacts of HIV and VAC. In partnership with five (5) civil society organizations (CSOs), the Bantwana Initiative of World Education, Inc. (WEI/Bantwana) implements a comprehensive package of services across the HIV continuum, which includes DREAMS programming within seven districts in Northern Uganda. BOCY supports coordination of integrated service delivery across multi-sectoral local government departments and CSOs to ensure that HIV-affected and infected orphans and vulnerable children (OVC) and DREAMS girls are safe, stable, healthy, and schooled. Programming contributes to the Uganda Country Development Cooperation Strategy and Uganda’s national 95-95-95 strategy.
Table 1 In Q2, BOCY remained focus on achieving key deliverables. This included strengthening facility and community coordination across health and child protection teams to expand critical services to the highest risk children (i.e. children and adolescents living with HIV, HIV-exposed infants (HEI), children and adolescents at risk of HIV, and children facing protection failures). This included setting up and training structures in case management for enrollment of non-suppressing CLHIV in districts and sub-counties beyond BOCY’s areas of operation and deepening local partner capacity to effectively use national case management tools, including ART and VLM tools developed and tested by WEI/Bantwana at the start of PY5. With an eye on sustainability, BOCY strengthened linkages between local government and local partners and supported empowered adoelscents, families, and resilient communities to advocate with local leaders and local government to transform hotspots into safe safe spaces and actively support GBV prevention and response to mitigate child protection failures. In Q2, BOCY delivered services to 115,278 beneficiaries, achieving 97% of the target for OVC_SERV. This included 9,670 CLHIV, a 111% increase from the Q1 figure of 4,573. BOCY also enrolled 3,390 HEI and 110 children of sex workers and delivered GBV/HIV prevention education to 49,545 adolecsent youth, ages 9-17 (45% adolescent girls and DREAMS girls). To identify new HIV cases, BOCY conducted HIV risk assessments for 87,672 children. Forty-seven (47) found to be at risk and were referred for testing. All were found to be negative. As shown in the graph below, 99.9% of all CLHIV are retained on ART. 88% of CLHIV have received viral load tests, and 74% have received their VL results. 80% of those CLHIV are suppressed – a 5% increase over the national CLHIV rate of 74.9% (Uganda VL dashboard March 2020).
PEPFAR indicator FY20 Target
FY20 Achieved (Q1) FY20 Achieved (Q2) FY19 Achieved Overall
%
Female Male Female Male
OVC_SERV 119,169 51,730 44,320 63,382 51,896 115,278 97% Active beneficiaries 95,338 50,019 42,639 49,280 38,773 88,053 92% Graduated 23,831 1,711 1,681 12,373 11,460 27,225 114% Exited without graduation (in Q1)
12,403 11,159 8,048 2,083 10,131
Transferred 11,128 11,069 22,197 Exposed infants 14 25 1,737 1,653 3,390 Children of PLHIV 16,240 16,855 22,954 26,093 49,047 Sexual violence survivors
40 14 15 5 74
CFSW 68 42 110 AGYW in DREAMS 6,390 0 7,950 0 14,340

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 4
Graph 1: HIV Cascade, Q2 Other notable achievements included the graduation of 5,678 HHs, achieving 8,078 (74%) layering of the primary package for DREAMS girls; support for 136 destitute HHs through the VSLA OVC Fund; provision of education support to 3,735 girls, economic empowerment for 8,862 youth, and positive parenting education for 16,507 caregivers and children. Despite these achievements, implementation gradually halted from the 18th of March with the announcement of MOH guidelines for social distancing, stoppage of group meetings, a ban on public gatherings and transport and school closures which all took effect on the 20th of March in response to the COVID-19 pandemic. The announcement of lockdown on the 26th of March brought all group based activities to a halt as partners sent staff back from duty stations to their respective homes. This created challenges to complete activities planned for the last two weeks of Q2.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 5
1.2 Results to Date Table 2(a): PMP/Project Indicator Progress - USAID Standard Indicators and Project Custom Indicators PERIOD: Oct - Dec 2019 [Strategic Objective]
Indicator
Data Source
Baseline Data
FY 2020
Quarterly Status – FY 2020
Performance to Date (%)
Comment(s) Year Value Annual Planned Target
Annual Cumulative
Actual
Q1 Q2 Q3 Q4 Q2
Purpose: To ensure more orphaned and vulnerable children and youth and their caregivers access and utilize core services that improve health, nutrition, education, and psychosocial well-being and reduce abuse, exploitation, and neglect in the northern and eastern regions of Uganda % of OVC with improved wellbeing
This is a five-year indicator on which BOCY shall report at the end of the project.
% of households that graduate from vulnerability
45%
58% 3% 26%
58% Through continuous household assessments to identify red flags and to support households to address them, BOCY was able to achieve 58% of the COP 19 target and is on track to meet the annual target.
OVC_SERV: # of active beneficiaries served by PEPFAR OVC programs for children and families affected by HIV/AIDS
Service registers, referral forms, client records, organization records, monitoring tools
2015 Not available
119,169 97% (11,5278)
96,050 115,278
97% Targeting enrolment and service delivery of new TX_CURR households with CLHIV in Q2 accelerated target achievement. BOCY is on track to meet the annual target.
OVC_HIVSTAT: % of orphans and vulnerable children (<18 years old) with HIV status reported to implementing partner (including status not reported), disaggregated by status type
Tools for HIV risk assessment referrals; VLS, ART registers
100% 98.8%
99.5%
98.8%
98.8% Intensive enrollment of CLHIV, and HEI with unknown status nominally affected Q2 results,
Intermediate Result 1: Economically empowered OVC and youth and their caregivers access core services IR 1.1: Increased temporary consumption support % of destitute households successfully linked to social protection assistance
BOCY linkages tracking form (HAT)
2015
50% 82%
14% 41% (136/332)
82% BOCY’s strong networks with local government and other community actors facilitated quick linkages between destitute households and social protection support. Efforts to link and document destitute households enrolled in the last month of Q2 will be reported in Q3.
IR 1.2: Increased savings and credit opportunities

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 6
% of beneficiary households accessing formal and informal financial services
VSLA MIS, VSLA records, linkages forms
2015
60% 48% 29.4%
29.4% (5,711/ 19,429)
48% Mature VSLAs now operate independently with BOCY monitoring bi annually. These HHs are accessing formal services but were not tracked in Q2 as enrollment of non suppressing CLHIV (TX CURR) were prioritized which increased the HH denominator. Time did not allow for the delivery of financial services to newly enrolled HHs in Q2. Achievement of annual targets may be impacted by the COVID 19 pandemic.
IR 1.3: Increased opportunities for growing income and assets Number of households accessing agribusiness services through voucher and private sector engagement
VSLA MIS
2015 1,000 389 (44%)
46 389
44% BOCY delivered services to 44% of targeted HHs to access agribusiness services, 6% below the semi-annual target. Due to budget constraints in PY 5, BOCY has delivered agribusiness services primarily through private sector linkages. Achievement of annual results may be impacted by the COVID 19 pandemic.
IR 1.4: Increased group-based education and support programming % of caregivers who access group-based education
Group activity forms
2015 0 60% 40% 41% 24% (4,754/ 19,429)
40% Enrollment of an additional 7550 TX CURR caregivers expanded the caregiver denominator impacting the overall result. BOCY will continue to prioritize relevant group based support in Q3 to CLHIV within the COVID pandemic context.
Intermediate Result 2: Improved core services for OVC, youth, and their caregivers by local governments, CSOs, and informal community structures
% of individual OVC and caregivers served with core services
BOCY database, referral form, home visit tool
2015
60%
105%
59% (56,050/ 96,050)
63.2% (72,828/ 115,278)
105% BOCY continued to layer multiple services across all BOCY service platforms to ensure the delivery of targeted, comprehensive support.
IR 2.3: Increased local government staffing levels and higher performing workforce Number of service providers trained who serve vulnerable persons
2015 Not available
2,500 49 (2%)
- 49 2% BOCY has delivered all relevant trainings to implementing partners and continues to coach and mentor local partners for continuous quality improvement in programming and data collection.
IR 2.5: Improved service models and delivery mechanisms for VYC Number of USG-assisted organizations and/or service delivery systems that serve vulnerable persons strengthened
2015 Not available
819 1,619 (198%)
- 1,619 198% As part of a sustainability strategy, BOCY supported VSLAs to register as CBOs, which are now able to support more OVC HHs through the VSLA OVC Fund. The achievement is mostly attributed to the increased number of registered VSLAs supporting OVC.
Number of OVC supported to access education
Linkages forms 2015 6,057 3,795 (63%)
1,798 3,795
63% The process of payment for school subsidies was still
ongoing when schools closed in late March due to the COVID-19 pandemic. BOCY is in close discussion

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 7
with USAID to adapt school-related supports provided during the ongoing school closure.
Intermediate Result 3: Improved coordination of community-based clinical and socio-economic services for efficiency and effectiveness along the continuum of care IR: 3.1: Improved referral systems and linkages between community-based clinical and socio-economic services Number of OVC supported to access HIV-related services
Referral forms, linkages forms
2015 - 70,000 49,802 (71%)
32,878 49,802
71% Due to demographic targeting shifts, OVC and DREAMS girls (CLHIV, and in school and 9-14,) HIV risk is lower among BOCY beneficiaries which reduces the need for HIV testing services. BOCY will continue to prioritize HIV services for the most at risk OVC while continuing intensified response services to CLHIV.
IR 3.2: Improved models for integrating clinical and socio-economic services for very young OVC Number of children <5 who receive integrated community-based clinical and socio-economic services
Group activity forms, indirect beneficiaries tool, HAT
2015 5,000 6,262 (125%)
3,258 6,262
125% In line with USAID guidance, BOCY’s rigorous focus on delivering services to HIV-positive and -exposed infants in Q2 drove target overachievement.
IR 3.3: Improved models for integrating clinical and socio-economic services for vulnerable youth and caregivers Number of adolescents reached with integrated clinical and socio-economic services
Group activity forms, linkages form
2015 40,000 41,830 (105%)
25,804 41,830
105% Overachievement is attributed to the scaling up of the Stepping Stones and Journeys curricula under DREAMS.
2. ACTIVITY IMPLEMENTATION PROGRESS 2.1 Summary of Implementation Status
Summary Of Planned Activities In Quarter Actual Achieved In Quarter Activities Shifted To Next Quarter Result 1: Economically empowered OVC and youth and their caregivers access core services IR 1.1: Increased temporary consumption support (TCS)
Link 4,141 beneficiaries to the VSLA+ OVC Fund BOCY delivered education, food, and health support to 2,002 destitute children, including 341 children living with HIV (CLHIV). Increased linkages with external social protection programs reduced the need for OVC Fund support in Q2. With significant enrollment of new TX_CURRENT CLHIV at the end of Q2, BOCY expects to expand OVC Fund support to additional CLHIV in Q3.
In Q3, BOCY will intensify prioritization of OVC Fund support for CLHIV in close collaboration with district COVID response teams.
Link 107 households to other external programs for social protection services
Leveraging BOCY’s strong community partner relationships, 213 HHs (including 38 HHs with CLHIV) were linked to and supported by urgent social protection services.
Train Village Agents to replace program staff in implementing VSLAs for continuity and sustainability
Identified, trained, and mentored 23 VAs, who formed 16 groups in Q2, split between eastern and northern sub-counties.
Link 63 VSLAs to financial institutions and assist the groups to open accounts
Linked 23 VLSAs to financial institutions, reaching 81% of the annual target
Deliver GBV prevention and response information to 1,925 VSLA caregivers
Delivered GBV prevention and response information to 1,434 caregivers, including 417 PLHIV VSLA members
In Q3, BOCY will focus on GBV in Q3 in concert with COVID district response teams.
Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 8
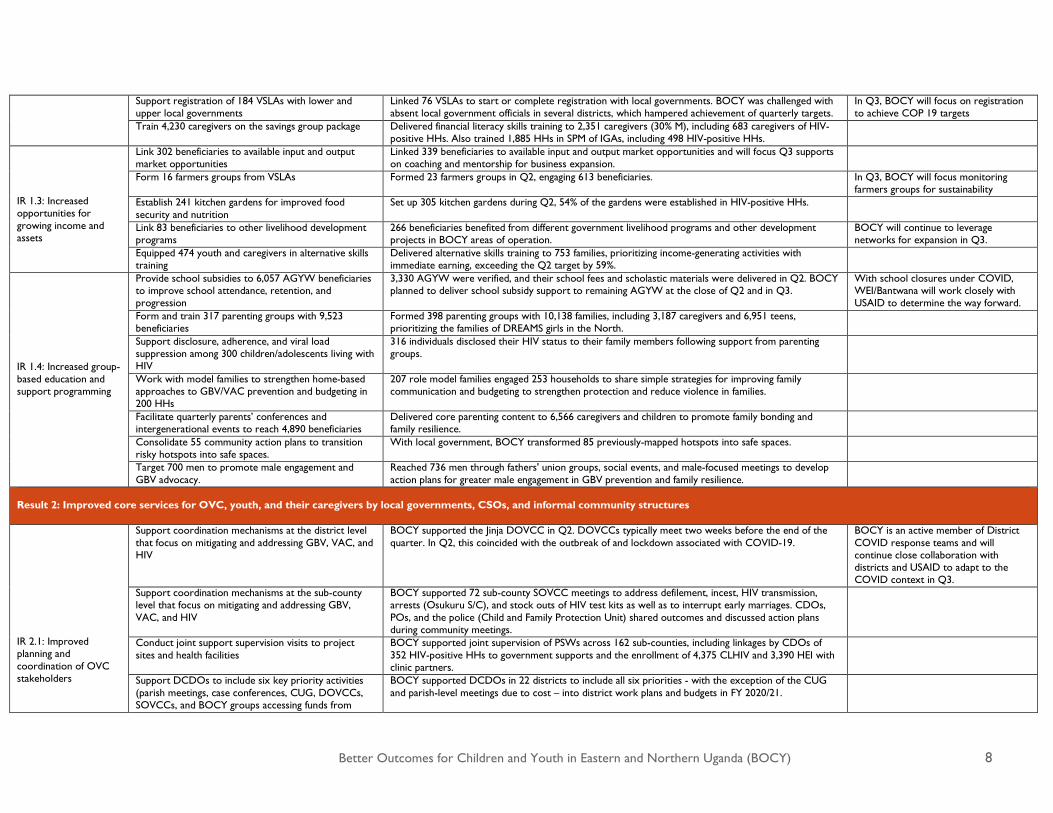
Support registration of 184 VSLAs with lower and upper local governments
Linked 76 VSLAs to start or complete registration with local governments. BOCY was challenged with absent local government officials in several districts, which hampered achievement of quarterly targets.
In Q3, BOCY will focus on registration to achieve COP 19 targets
Train 4,230 caregivers on the savings group package Delivered financial literacy skills training to 2,351 caregivers (30% M), including 683 caregivers of HIV-positive HHs. Also trained 1,885 HHs in SPM of IGAs, including 498 HIV-positive HHs.
IR 1.3: Increased opportunities for growing income and assets
Link 302 beneficiaries to available input and output market opportunities
Linked 339 beneficiaries to available input and output market opportunities and will focus Q3 supports on coaching and mentorship for business expansion.
Form 16 farmers groups from VSLAs Formed 23 farmers groups in Q2, engaging 613 beneficiaries. In Q3, BOCY will focus monitoring farmers groups for sustainability
Establish 241 kitchen gardens for improved food security and nutrition
Set up 305 kitchen gardens during Q2, 54% of the gardens were established in HIV-positive HHs.
Link 83 beneficiaries to other livelihood development programs
266 beneficiaries benefited from different government livelihood programs and other development projects in BOCY areas of operation.
BOCY will continue to leverage networks for expansion in Q3.
Equipped 474 youth and caregivers in alternative skills training
Delivered alternative skills training to 753 families, prioritizing income-generating activities with immediate earning, exceeding the Q2 target by 59%.
IR 1.4: Increased group-based education and support programming
Provide school subsidies to 6,057 AGYW beneficiaries to improve school attendance, retention, and progression
3,330 AGYW were verified, and their school fees and scholastic materials were delivered in Q2. BOCY planned to deliver school subsidy support to remaining AGYW at the close of Q2 and in Q3.
With school closures under COVID, WEI/Bantwana will work closely with USAID to determine the way forward.
Form and train 317 parenting groups with 9,523 beneficiaries
Formed 398 parenting groups with 10,138 families, including 3,187 caregivers and 6,951 teens, prioritizing the families of DREAMS girls in the North.
Support disclosure, adherence, and viral load suppression among 300 children/adolescents living with HIV
316 individuals disclosed their HIV status to their family members following support from parenting groups.
Work with model families to strengthen home-based approaches to GBV/VAC prevention and budgeting in 200 HHs
207 role model families engaged 253 households to share simple strategies for improving family communication and budgeting to strengthen protection and reduce violence in families.
Facilitate quarterly parents’ conferences and intergenerational events to reach 4,890 beneficiaries
Delivered core parenting content to 6,566 caregivers and children to promote family bonding and family resilience.
Consolidate 55 community action plans to transition risky hotspots into safe spaces.
With local government, BOCY transformed 85 previously-mapped hotspots into safe spaces.
Target 700 men to promote male engagement and GBV advocacy.
Reached 736 men through fathers' union groups, social events, and male-focused meetings to develop action plans for greater male engagement in GBV prevention and family resilience.
Result 2: Improved core services for OVC, youth, and their caregivers by local governments, CSOs, and informal community structures IR 2.1: Improved planning and coordination of OVC stakeholders
Support coordination mechanisms at the district level that focus on mitigating and addressing GBV, VAC, and HIV
BOCY supported the Jinja DOVCC in Q2. DOVCCs typically meet two weeks before the end of the quarter. In Q2, this coincided with the outbreak of and lockdown associated with COVID-19.
BOCY is an active member of District COVID response teams and will continue close collaboration with districts and USAID to adapt to the COVID context in Q3.
Support coordination mechanisms at the sub-county level that focus on mitigating and addressing GBV, VAC, and HIV
BOCY supported 72 sub-county SOVCC meetings to address defilement, incest, HIV transmission, arrests (Osukuru S/C), and stock outs of HIV test kits as well as to interrupt early marriages. CDOs, POs, and the police (Child and Family Protection Unit) shared outcomes and discussed action plans during community meetings.
Conduct joint support supervision visits to project sites and health facilities
BOCY supported joint supervision of PSWs across 162 sub-counties, including linkages by CDOs of 352 HIV-positive HHs to government supports and the enrollment of 4,375 CLHIV and 3,390 HEI with clinic partners.
Support DCDOs to include six key priority activities (parish meetings, case conferences, CUG, DOVCCs, SOVCCs, and BOCY groups accessing funds from
BOCY supported DCDOs in 22 districts to include all six priorities - with the exception of the CUG and parish-level meetings due to cost – into district work plans and budgets in FY 2020/21.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 9
government programs) in district work plans and budgets Attend RHITES-supported district health management committee meetings and meetings organized by RHITES operating in BOCY districts
BOCY’s deliberate participation and advocacy in RHITES-supported health management meetings across 11 districts has alleviated community-clinic case management and coordination bottlenecks (i.e. addressing HIV test kit stockouts, CLHIV clinic transport issues for ART refills) and has strengthened coordination between DHOs and CDOs for improve health and protection.
Support districts to popularize ordinances and by-laws that mitigate and respond to GBV and VAC
BOCY supported all the districts to popularize/disseminate ordinances at the community level. In Kamuli, BOCY partner, MUCOBADI, supported the dissemination of the teenage and early marriage ordinances coupled with the child labor ordinances in Kisozi and Wankole Sub-Counties.
IR 2.2: Increased financing for OVC youth and caregivers
Support rollout of OVC indicators in BOCY operation districts
BOCY is still pursuing a waiver from USAID, which was anticipated to be released in March 2020. However, the COVID-19 crisis and country lockdown has delayed progress.
IR 2.3: Increased staffing levels and a higher performance workforce
Orient CSO staff on SOPs for improving performance in enrolling CLHIV and HEI
BOCY developed and oriented CSO staff on the SOPs for profiling and enrolling CLHIV and HEI, leading to the enrollment of 4,375 CLHIV beneficiaries in Q2.
Hold monthly district cluster QI team planning and performance review meetings among BOCY CSO partners
Data-driven support to district cluster QI teams accelerated progress on HH graduation, profiling and enrolment of CLHIV (TX_CURR) onto BOCY, and service layering and completion. The support also strengthened linkages of eligible HHs to government social protection supports. With WEI/Bantwana support, BOCY partners developed and jointly tracked milestone progress.
Support CSOs to strengthen functionality of their QI systems (QI plans, minutes, and journals)
BOCY supported cluster QI teams to develop QI plans focused on graduation, enrolment of TX_CURR, tracking viral load suppression, club formation, and service layering. These program aspects were QI projects for implementing partners for which BOCY registered milestones.
Support MUCOBADI NUPAS preparation BOCY continued supporting MUCOBADI to review their policies and to build their financial, HR, and operations systems in preparation for the USAID NUPAS review, which was delayed due to the COVID-19 outbreak.
Orient IP staff on the GBV data collection tool to facilitate reporting in the GBVMIS at the district level
WEI/Bantwana and BOCY CSO M&E staff oriented technical teams on the GBV data collection tool and data reporting to the GBVMIS through the district GBV focal person.
Support districts to analyze and generate statistical reports from national databases focused on GBV, VAC, and HIV to be shared through coordination, planning, and decision-making platforms.
BOCY supported OVCMIS and GBV focal persons in 22 districts to generate OVC and GBV data. WEI/Bantwana supported districts to use school dropouts, defilement, early marriage, teenage pregnancy, child neglect and child labor data to develop community surveillance plans.
IR 2.5: Improved service models and delivery mechanisms for VYC
Support districts to establish and operationalize District Action Centres
WEI/Bantwana delayed this activity until Q3 following a resolution of a requested waiver from USAID
Facilitate CDOs to follow up critical cases of GBV, VAC and HIV
The activity was postponed to this quarter when USAID can issue BOCY a waiver to facilitate government staff that will be involved in implementing the activity.
Liaise with the DCDO to prioritize HHs with HIV-positive children or caregivers for livelihoods support
BOCY linked 352 HIV-affected households to social protection supports, including agricultural inputs, hoes and seeds, herbicides, and training in farming best practices through the Production Department in Oyam, Arua, Kamuli, Mayuge, Bugiri, Tororo, Busia and Namayingo Districts.
Advocate with local government to secure access to government programs for BOCY youth and VSLA groups.
Three VSLA groups in Dokolo, Mbale, and Lira Districts secured animals and seed funds to start IGAs.
Result 3: Improved coordination of community-based clinical and socioeconomic services for efficiency and effectiveness along the continuum of care
Coach and mentor 1,200 PSWs and Expert Clients to continue delivering critical HIV services
BOCY delivered coaching, mentoring, and support supervision to 1,178 PSWs, including 234 Expert Clients, through case conferences, field visits, and parish-level meetings. New Expert Clients recruited to profile and enroll TX_CURR CLHIV onto BOCY and to support ART retention and viral load tracking (prioritizing non-suppressing CLHIV) were trained in the case management package.
Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 10
1 Oyam, Gulu, Lira, Jinja, Mbale & Tororo
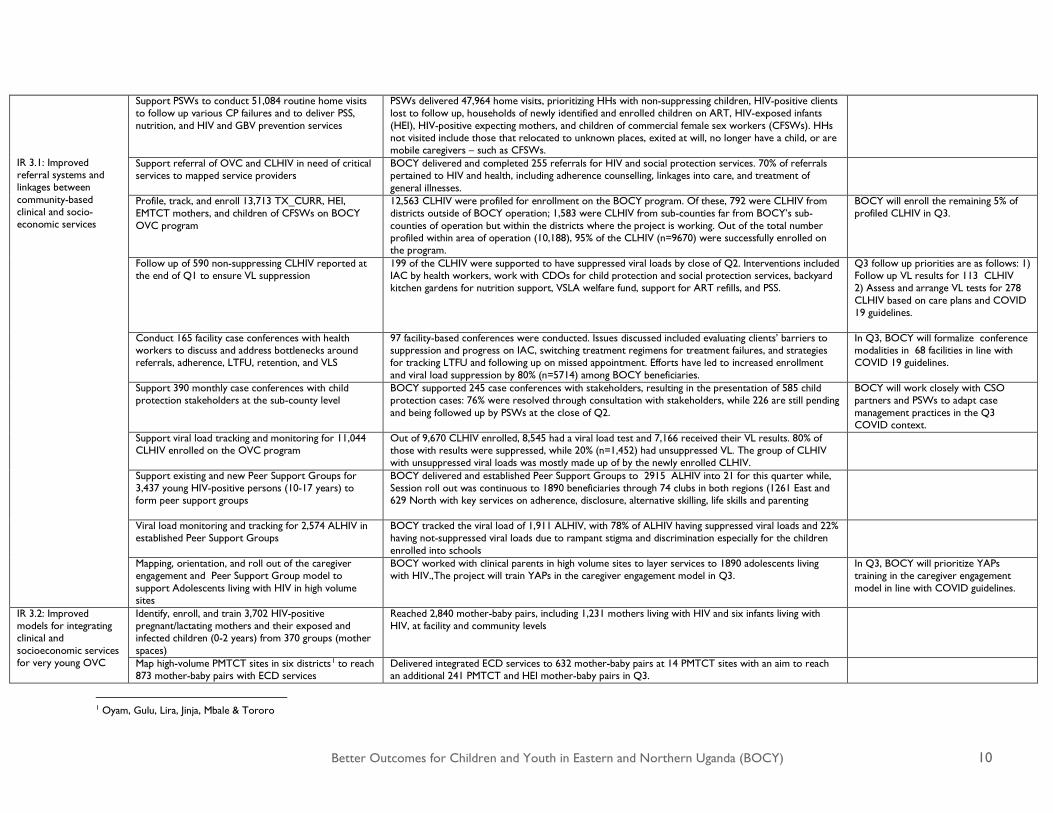
IR 3.1: Improved referral systems and linkages between community-based clinical and socio-economic services
Support PSWs to conduct 51,084 routine home visits to follow up various CP failures and to deliver PSS, nutrition, and HIV and GBV prevention services
PSWs delivered 47,964 home visits, prioritizing HHs with non-suppressing children, HIV-positive clients lost to follow up, households of newly identified and enrolled children on ART, HIV-exposed infants (HEI), HIV-positive expecting mothers, and children of commercial female sex workers (CFSWs). HHs not visited include those that relocated to unknown places, exited at will, no longer have a child, or are mobile caregivers – such as CFSWs.
Support referral of OVC and CLHIV in need of critical services to mapped service providers
BOCY delivered and completed 255 referrals for HIV and social protection services. 70% of referrals pertained to HIV and health, including adherence counselling, linkages into care, and treatment of general illnesses.
Profile, track, and enroll 13,713 TX_CURR, HEI, EMTCT mothers, and children of CFSWs on BOCY OVC program
12,563 CLHIV were profiled for enrollment on the BOCY program. Of these, 792 were CLHIV from districts outside of BOCY operation; 1,583 were CLHIV from sub-counties far from BOCY’s sub-counties of operation but within the districts where the project is working. Out of the total number profiled within area of operation (10,188), 95% of the CLHIV (n=9670) were successfully enrolled on the program.
BOCY will enroll the remaining 5% of profiled CLHIV in Q3.
Follow up of 590 non-suppressing CLHIV reported at the end of Q1 to ensure VL suppression
199 of the CLHIV were supported to have suppressed viral loads by close of Q2. Interventions included IAC by health workers, work with CDOs for child protection and social protection services, backyard kitchen gardens for nutrition support, VSLA welfare fund, support for ART refills, and PSS.
Q3 follow up priorities are as follows: 1) Follow up VL results for 113 CLHIV 2) Assess and arrange VL tests for 278 CLHIV based on care plans and COVID 19 guidelines.
Conduct 165 facility case conferences with health workers to discuss and address bottlenecks around referrals, adherence, LTFU, retention, and VLS
97 facility-based conferences were conducted. Issues discussed included evaluating clients’ barriers to suppression and progress on IAC, switching treatment regimens for treatment failures, and strategies for tracking LTFU and following up on missed appointment. Efforts have led to increased enrollment and viral load suppression by 80% (n=5714) among BOCY beneficiaries.
In Q3, BOCY will formalize conference modalities in 68 facilities in line with COVID 19 guidelines.
Support 390 monthly case conferences with child protection stakeholders at the sub-county level
BOCY supported 245 case conferences with stakeholders, resulting in the presentation of 585 child protection cases: 76% were resolved through consultation with stakeholders, while 226 are still pending and being followed up by PSWs at the close of Q2.
BOCY will work closely with CSO partners and PSWs to adapt case management practices in the Q3 COVID context.
Support viral load tracking and monitoring for 11,044 CLHIV enrolled on the OVC program
Out of 9,670 CLHIV enrolled, 8,545 had a viral load test and 7,166 received their VL results. 80% of those with results were suppressed, while 20% (n=1,452) had unsuppressed VL. The group of CLHIV with unsuppressed viral loads was mostly made up of by the newly enrolled CLHIV.
Support existing and new Peer Support Groups for 3,437 young HIV-positive persons (10-17 years) to form peer support groups
BOCY delivered and established Peer Support Groups to 2915 ALHIV into 21 for this quarter while, Session roll out was continuous to 1890 beneficiaries through 74 clubs in both regions (1261 East and 629 North with key services on adherence, disclosure, alternative skilling, life skills and parenting
Viral load monitoring and tracking for 2,574 ALHIV in established Peer Support Groups
BOCY tracked the viral load of 1,911 ALHIV, with 78% of ALHIV having suppressed viral loads and 22% having not-suppressed viral loads due to rampant stigma and discrimination especially for the children enrolled into schools
Mapping, orientation, and roll out of the caregiver engagement and Peer Support Group model to support Adolescents living with HIV in high volume sites
BOCY worked with clinical parents in high volume sites to layer services to 1890 adolescents living with HIV.,The project will train YAPs in the caregiver engagement model in Q3.
In Q3, BOCY will prioritize YAPs training in the caregiver engagement model in line with COVID guidelines.
IR 3.2: Improved models for integrating clinical and socioeconomic services for very young OVC
Identify, enroll, and train 3,702 HIV-positive pregnant/lactating mothers and their exposed and infected children (0-2 years) from 370 groups (mother spaces)
Reached 2,840 mother-baby pairs, including 1,231 mothers living with HIV and six infants living with HIV, at facility and community levels
Map high-volume PMTCT sites in six districts1 to reach 873 mother-baby pairs with ECD services
Delivered integrated ECD services to 632 mother-baby pairs at 14 PMTCT sites with an aim to reach an additional 241 PMTCT and HEI mother-baby pairs in Q3.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 11
Conduct ECD outreaches with 1,334 mother-baby pairs
Delivered 1,106 cooking demonstrations, immunization, backyard gardening, nutrition, and growth-monitoring activities to mother-baby pairs. Remaining activities will be delivered in Q3.
IR 3.3: Improved models for clinical SES for youth and caregivers
Layer integrated services to 64,000 adolescent youth and DREAMS girls (parenting; Stepping Stones; Journeys; and HIV, ARSH, and GBV prevention services)
Delivered integrated service to 64,451 adolescent youth DREAMS AGYW including parenting package, sessions on Journeys and Stepping Stones, and HIV and GBV primary prevention core services.
No Means No (NMN) roll out
NMN activities for boys (2,300) and girls (2,025) in Mbale and Tororo
BOCY delivered No Means No programming to 1,873 girls in both Mbale and Tororo. BOCY delivered pre-test surveys to 177 boys in Tororo and trained 18 male instructors and two BOCY CSO social workers (instructor supervisors).

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 12
Progress Narrative Result 1: Economically empowered OVC, youth, and their caregivers access core services In Q2, BOCY targeted economic strengthening (ES) support to move families along the economic resilience pathway, including expansion aimed to help struggling families meet financial security benchmarks and expanding ES, health, education, and GBV and HIV prevention supports to families with C/PLHIV, DREAMS girls, and other children most at risk of HIV. With an eye to sustainability and planning for the transfer of project-supported efforts to local government and other social protection providers, BOCY facilitated the linkages of 213 HHs (including 29 HIV-positive HHs) to the government-supported SAGE program, the Uganda Women’s Empowerment Program (UWEP), and the District Discretionary Equalization Grant (DDG). BOCY intensified efforts to link mature savings groups to formal financial institutions and expanded the registration of mature groups with local government for onward livelihoods support. The project also expanded the community-supported Village Agent Model for continuous replication of savings groups beyond the life of the project. Specific Q2 outcomes are outlined below. IR 1.1 Increased temporary consumption support (TCS) Institutionalizing the OVC Fund for sustained support: In Q2, BOCY supported 9,874 children, including 341 CLHIV, from destitute HHs with education, health, and food/nutrition supports with a total value of UGX 39,147,600 ($10,814). These funds were raised through the OVC Fund, which is institutionalized in the standard operating procedures (SOPs) for all BOCY savings groups, including groups replicated through the Village Agent model. Cumulatively, the total payout of OVC Fund benefits equals UGX 577,354,350 ($159,490), and the cumulative OVC Fund contribution stands at UGX 810,349,950 ($223,853). Groups have also used the OVC Fund to buy seeds for setting up demonstration gardens at their respective meeting venues. Graph 2: Q2 OVC Fund Distribution
Source: VSLA MIS (March 2020 report) IR 1.2 Increased savings and credit opportunities In Q2, BOCY trained an additional 23 Village Agents who formed 20 new saving groups, including four facility-based savings groups for caregivers of CLHIV. All VSLA groups increased their savings by UGX 180,421,600 ($49,840) this quarter, increasing the culmulative total from $1,666,117 (UGX 6,081,328,400) in Q1 to $1,729,765 (UGX 6,261,750,050) in Q2. Through BOCY community resource persons and local government protection officers (i.e. parenting facilitators, PSWs, CDOs, Expert Clients), BOCY delivered GBV prevention education to 1,434 savings group members and financial literacy and SPM supports to
Education, 386,961,100,
67%
Health, 115,702,600,
20%
Food and Nutrition,
61,792,700, 11%
Others, 12,897,950,
2%
Education Health Food and Nutrition OthersVSLA group in Arua distributing food to vulnerable
households bought with OVC Fund proceeds.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 13
1,885 members as well as registered 42 groups with local government and assessed the readiness of 139 savings groups to self-manage — 88.4% of which were ready to operate independently. Table 2: Cumulative Financial Performance of Youth Savings Groups
Youth learn the culture of saving: With a focus on DREAMS girls and CLHIV, BOCY delivered ES supports to 8,832 adolescent youth through 174 youth savings groups (60% DREAMS girls) with an emphasis on savings, budgeting, and financial planning to prepare youth well for their transition into adulthood.
IR 1.3 Increased opportunities for growing income and asset To accelerate income and asset growth, BOCY linked 339 (65% F) financially stable caregivers to locally available and reliable agro-input dealers and agro-product buyers, delivered alternative skills training for 753 adolescents and caregivers (55% F), and linked 266 adolescents (58% F) and caregivers to other livelihood development programs.
Expansion of Junior Farmer Field School (JFFS) model for in- and out-of-school adolescents: In Q2, BOCY established 32 new JFFSs and community demonstration gardens (75% N) with in- and out-of-school clubs and delivered ongoing support to 38 clubs. JFFSs formed in PY4 continue to maintain their demonstration gardens and have replicated the same in their homes. Adolescents report that they use produce from gardens for their own use and also sell some produce, using profits to buy scholastic materials. For example, at Abela Primary School in Aleka Sub-County, Oyam District, the school provided a ready market for the cabbages grown by the youth, and the proceeds were used to purchase scholastic materials for vulnerable children in the club.
Financial Performance of Youth Saving Groups (March 2020) Region No. of Youth Groups Saving-UGX Average Saving-UGX EDF-UGX Average EDF-UGX EDF
Utilization ROS
East 26 38,187,000 61,373 16,949,250 111,622 43.3% 8.9%
North 148 106,329,150 49,580 46,510,900 58,720 48.2% 8.0%
Total 174 144,516,150 55,477 63,460,150 85,171 45.7% 8.5%
Source: VSLA MIS (End of March 2020 reports), ROS=Return on Savings, EDF = Enterprise Development Fund
“My time in the club has paid off. I planted tomatoes during my vacation, sold them, and got UGX 100,000. I used the money to buy personal belongings when joining secondary school. I left some in the nursery bed. I will harvest at the
right time.” -Ruth Akello, BOCY in-school club member, Oyam District
“I earn at least UGX 25,000 in a week, and this has enabled me to pay school fees for my child and my little sister. I can also take care of myself and provide the basics for my dependents. All of this is possible because I joined the youth VSLA group. I therefore encourage my fellow youth to join VSLA groups and start saving so as to ease their lives.” -Scovia Aceng, DREAMS girl from Oyam, who joined a youth VSLA in 2017. After she turned 18, she borrowed UGX 50,000 to start a small business selling groceries, which continues to operate today.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 14
Alternative skilling for DREAMS girls and other high-risk adolescents: BOCY continued to prioritize program delivery on adolescents most at risk of HIV and GBV through accelerated delivery of the low-cost alternative skills training to 502 in school DREAMS girls, CLHIV (through facility-based Peer Support Clubs) and other out of school adolescents. BOCY targeted alternative skills training for making reusable menstrual pads (RUMPS) to in-school DREAMS girls as well as training to make sponges, liquid soap, chapatis, pancakes and knitting, basket weaving, and simple crafts making. For example, in Unyama Sub-County and Layibi Division in Gulu District, adolescents of Shalom Christian School and New Generation DREAMS Girls First Clubs are selling liquid soap at the school and to the neighboring community members. In Bugiri, BOCY leveraged the ‘‘Keep the Girl Child in School’’ campaign to train additional girls in RUMPS-making to support their retention in school during their periods. Supporting households to establish kitchen gardens: With an intensified focus on bolstering adherence support for CLHIV, BOCY established 305 kitchen gardens (78% E) with BOCY HHs in Q2, 54% of which were CLHIV households, expanding the PY5 total to 1,085 gardens. BOCY established 28 demonstration gardens with VSLA members who purchased seeds using collective social welfare funds. Following collective training through demonstration gardens, members then replicated kitchen gardens at home while continuing to consult with one another during savings group meetings and with local production agents and BOCY community resource persons. IR 1.4 Increased group-based education and support programming Positive parenting has continued to play a pivotal role in strengthening family relationships, mobilizing family efforts for planning and generating income for resource utilization, unity, and child protection. Expanded child-to-child campaigns, male engagement, intergenerational events, and model family activities in Q2 deepened family and community capacity to advocate with government, schools, and clinics on their own behalf and champion child protection, girls’ education, adherence and resilience for CLHIV, GBV prevention, and positive social norms change. Strengthened and empowered children, youth, caregivers, families, and community members able to advocate for themselves and their children will be one of BOCY’s greatest legacies. Expanded delivery of positive parenting for family resilience and disclosure for PLHIV families: In Q2, BOCY delivered parenting to an additional 10,138 adolescents and caregivers (80% N), targeting DREAMS girls, HIV-positive households, and other vulnerable households with protection failures. With support from parenting facilitators who double at Village Health Teams (VHTs) and Expert Clients, BOCY delivered integrated health education, including safe HIV status disclosure, nutrition, ART adherence, and viral load suppression. As a result, 316 (80% N) individuals disclosed their HIV status to
Twesimbe Club of St. Mary’s P/S, Kamuli district preparing their eggplant nursery beds with their teachers support.
Obanga Ber VSLA+ Group, Ngetta Sub-County, Lira District receive agricultural inputs from S/C officials following successful
advocacy from BOCY support.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 15
family members and peers2 during family “special time,” home/group sessions, and community outreaches. HIV-positive caregivers reported that safe disclosure created room for more care, support, trust, and open interactions among families and peers that helped with positive living, the development of sustainability plans, and good ART adherence and viral load suppression. This is evidenced in the 233 caregivers and 12 children who disclosed that they were suppressing following their last viral load test. Parenting facilitators work closely with PSWs and the HIV community to ensure that HIV-positive caregivers disclosing during group sessions are supported. Intensive support for home practices helped families to consolidate positive practices for improved anger and emotional management. Role model families expand positive parenting and social norms change impact: In Q2, 207 role model families engaged 253 households experiencing social and emotional issues, including poor ART adherence, GBV/VAC and child neglect. Working in pairs, model families shared their own stories of change and offered emotional support guided by their own experiences and learning from the positive parenting program. These empowered families will become part of BOCY’s sustainable community resource network, carrying on their exemplary GBV and HIV prevention work long after the project closes. In Q2, male engagement efforts engaged 736 men (80% N). Topics of discussion during meetings included joint planning and decision making, the involvement of men in family planning, and positive parenting practices that promote child upbringing. SINOVUYO Facilitators also facilitated sessions on how to communicate and resolve conflicts without violence, how to facilitate family budgeting and saving, and solicited input from men on how they can contribute to protection of children from HIV and SGBV and combat excessive drinking strongly linked to GBV, violence, and poverty in families. To strengthen attendance of their routine meetings and to practically develop capacity to provide for their families, some groups started savings groups alongside their weekly group discussions. For example, in Q2, the Basadha Group in Bulidha Sub-County, Bugiri District shared out their accumulated total savings of UGX 5,045,040 ($1,393) from their weekly savings. Members testified how much they appreciated their newfound thinking about their parenting roles that they gained through the positive parenting sessions and through the VSLAs, which enabled them to better meet their family’s basic needs. Thirty-six child-to-child groups, consisting of girls in DREAMS districts and other vulnerable in and out of school adolescents engaged 1,831 adoelscents (87% N) with VAC messages in their schools and communities. This includes encouraging learners to report incidents of violence in schools to matron and patrons and intensified sensitization around challenges facing CLHIV to reduce stigma and encourage safe disclosure by CLHIV to teachers and peers as part of BOCY’s larger retention and adherence strategy. Intensified collaboration between communities and local government health and child protection officials to prevent GBV: Leveraging strong, effect relationships with local government, local government officials, health facilities and child protection units, BOCY strengthened the GBV response. For example, in Mbale and Kamuli districts, community dialogues facilitated by Probation and Social Welfare Officers engaged 442 caregivers and community members to address GBV, including an emphasis on the early reporting of suspected perpetrators to relevant authorities to take timely action, reinforcing the importance of keeping girls in school, sharing success stories from caregivers, and urging local leaders to continue using village meeting platforms to raise awareness and promote action on GBV.
2 Ten disclosures were made by CLHIV to their peers and caregivers, while the remaining 306 disclosures were made by caregivers to their children and family members as well as to their parenting groups.
“I was so demoralized when my father-in-law denied me the right to cultivate land, yet I am an HIV-positive widow with three children to look after. A role model family and my Sinovuyo facilitator, Ogolla Eriah, intervened, and I am now cultivating the land. My maize has matured, and I have enough food to eat.”
-Florence Okiror, Kagora Village, Kamuli Parish, Mukujo Sub-County, Tororo District

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 16
Empowered communities successfully advocate with local government to transform mapped hotspots into safe spaces: In Q2, with support from Sinovuyo facilitators, communities engaged local leaders to prioritize the safety of children by transforming 33 local bars; 18 video halls; 16 trading centers, markets, sugarcane and rice plantations, stone quarries, and landing sites – 85 (70% N) hotspots total – through community by-laws and the involvement of the police. Caregivers also committed to positive parenting, including setting family rules and routines to ensure children are protected. Result 2: Improved core services for OVC, youth and their caregivers by local governments, CSOs, and informal community structures IR 2.1 Improved planning and coordination of OVC stakeholders In Q2, intensified advocacy with district and sub-county stakeholders to plan and hold district and sub-county coordination meetings resulted in the occurrence 72 of the 98 sub-county meetings, while all districts (but Jinja) canceled meetings scheduled during the last two weeks of Q2 due to the COVID-19 pandemic. At the sub-county level, stakeholders addressed child sexual abuse (defilement), stock-outs of HIV test kits, early marriages, and teenage pregnancies, and CDOs, Probation Officers, and a police representative from the CPFU rolled out GBV and VAC awareness activities in the community. Iganga District responded quickly to the COVID-19 pandemic and managed to hold its DOVCC meeting, which it expanded to tackle both child protection issues and COVID-19 responses. In the meeting, the district resolved to improve children homes assessments by probation officers, de-institutionalize children in orphanages, and strengthen referrals and support to children living with disabilities. For the COVID response, the district shared hotlines for reporting suspected COVID-19 cases and shared measures on how to prevent its spread transmission IR 2.3 Increased staffing levels and a higher performance workforce In anticipation of project close and handover, BOCY continued to target effective planning, reviews, and providing activity implementation technical support to its implementing partners and technical staff at district and sub-county levels. With BOCY support, CSOs addressed performance gaps emerging from program performance data and programming gap analyses. As performance gaps varied by district, BOCY also supported CSO partners to develop district-specific strategies that led to improved performance in lagging activities, such as household graduation and CLHIV enrolment. Quality improvement teams consisting of CSO partner staff and WEI/Bantwana technical staff rolled out and tracked the revised strategies undergirding of the SAPR achievements highlighted in Section 1.2 (Results to Date (PMP)). WEI/Bantwana advances local transition efforts with MUCOBADI and USAID Following MUCOBADI’s completion of its capacity building benchmarks, WEI/Bantwana invited USAID to conduct a NUPAS assessment and begin the process of transitioning MUCOBADI to be a direct USAID grant recipient. To achieve this milestone in a short timeframe, BOCY intensified its capacity building support by providing multiple supports to MUCOBADI to complete the revisions of their policies, orient staff on the new policies, and roll them out across the organization. The BOCY team received technical support from the WEI/Bantwana Capacity Building team and Andrew Kigozi, an independent consultant who worked with MUCOBADI to finalize their policies and prepare for a NUPAS assessment.
Children of Adilang Lalal P/S in Adilang S/C, Agago District identify risky places in their community. This exercise has created more awareness
and empowered children to take actions that improve on their individual and collective safety.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 17
MUCOBADI successfully rolled out its revised policies and procedures and financial and operational systems and was ready to undergo the NUPAS assessment in February. However, USAID postponed the assessment and has rescheduled to conduct it in Q3. IR 2.4 Improved MIS accountability and evidence building systems for VYC and their caregivers For improving planning, accountability, and evidence in service delivery, BOCY lobbied probation officers across the 22 districts to hold quarterly OVCMIS data validation meetings. However, the meetings that were scheduled at the end of the quarter were cancelled because of the COVID-19 pandemic restrictions/response. After orienting M&E and technical officers on the GBV data collection tool, BOCY improved on reporting GBV data to district focal persons. This data, which is used for the generation of reports for the SOVCC, informs data-driven program activity to address school dropouts, defilement, early marriage, teenage pregnancy, child neglect, child labor attributed to poverty, and the weak enforcement of child protection laws. Uniform resolutions focused on intensifying awareness creation, community surveillance, and reporting. Result 3: Improved coordination of community-based clinical and socioeconomic services for efficiency and effectiveness along the continuum of care IR 3.1 Improved referral systems and linkages between community-based clinical and socio-economic services In Q2, BOCY accelerated focus on enrollment of new TX_CURR and non-suppressing CLHIV, strengthening clinic and community coordination among HIV and social protection staff and structures to eliminate loss to follow up and to support CLHIV adherence, viral load testing and delivery, and linkages to critical child and social protection supports to further enhance resilience of BOCY’s HIV-positive and most vulnerable families. Further collaboration with clinic partners in Q2 included expanded support for existing and new Peer Support Clubs and the enrollment and layering of early childhood development services on clinic and community outreaches targeting PMTCT mothers and HEI babies. BOCY has also provided targeted coaching and mentoring of PSWs to coordinate case management with clinic partners and community structures as well as recruiting and training new Expert Clients to support newly enrolled non-suppressing CLHIV in districts and sub-counties outside of the BOCY area of operations in response to USAID’s request. HIV risk assessment for BOCY beneficiaries: In Q2, BOCY HIV risk screened 1,447 OVC with unknown status, resulting in onward referral of 72 children, 100% of whom tested HIV negative. Clinic providers delivered nutritious and therapeutic foods for those that had malnutrition signs, nutrition and reinforce HIV prevention through good hygiene and nutrition. BOCY will closely follow these children in Q3. Home visits conducted and documented: BOCY prioritized 47,964 home visits to non-suppressing children, clients lost to follow up (LTFU), those who had missed appointments, households of newly identified and enrolled children on ART, HIV exposed infants (HEI), eMTCT expecting mothers, and children of commercial sex workers. During the home visits, PSWs delivered wide-ranging services, including nutrition education, psychosocial support, and GBV/VAC prevention. With Expert Clients and trained parenting facilitators, PSWs also supported family disclosure and monitored ART adherence and retention in ART care and treatment.
Waiwe George, a lab technician, conducts an HIV test with a BOCY caregiver and her children during an integrated outreach with BOCY
and the Lulyambuze HC III in Kumuli District in March 2020.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 18
Upskilled PSWs and Expert Clients to accelerate CLHIV enrollment, adherence and VLM support: BOCY continued to mentor 1,178 PSWs to strengthen clinic coordination, documentation, and case planning through case conference meetings, support supervision field visits and parish level meetings as well as to support BOCY’s semiannual household (HH) graduation assessment exercise, viral load tracking, and case documentation and reporting. In addition, BOCY identified and trained 234 Expert Clients to enroll and deliver adherence and viral load monitoring support to CLHIV outside of BOCY’s operational areas. Between Q4 PY 4 and and Q2 PY 5, CLHIV enrollment more than doubled and viral load suppression increased to 80% (see Graph 3).
Targeted HIV and social protection referrals completed: Leveraging strong community and clinic relationships and mapped service points, BOCY PSWs and other community structures successfully made 255 referrals – 70% of which were for health and HIV-related services, including adherence counseling and ART linkages, as well as other general health issues and food, nutrition, savings groups, and education supports. In Arua, 66 non-suppressing ALHIV, indentified during home visits and BOCY-supported Peers Support Group sessions, were referred, linked, and physically escorted to a health service provider for Intensive Adherence Counseling (IAC) by PSWs. BOCY later supported these families to establish kitchen gardens to boost their nutrition status as the clinic, and community teams worked with
caregivers and children to improve communication, emotional bonding, and address child neglect and HIV-related stigma to enhance adherence and resilience. Profiling and BOCY enrollment of priority CLHIV (i.e. HEI and children of female sex workers) and other most vulnerable children: In Q2, BOCY profiled 12,563 CLHIV and enrolled 9,172 (90%) of the CLHIV onto the program, including 2,375 CLHIV from outside BOCY areas of operation. In Q3, BOCY will enroll the remaining 10% of CLHIV who are based in distant rural areas, requiring more time for relationship building and coordination with clinics and introduce children to the program during ART refill days, provide intensive training of Expert Clients in case management, and follow up with caregivers for consent. Table 3: Regional Enrollment Results
Region Status TX_CURR HEI eMTCT CFSWs
North
Target - verified 8,572 3,157 508 110
Achieved as at 23/3/2020 6,987 1,877 877 104
% Achieved 81% 59% 173% 95%
East
Target verified 3,198 2,133 583 00
Achieved as at 23/3/2020 2,185 1,435 323 00
% Achieved 68% 67% 55% 00
Total Enrolled 9,172 3,321 1,200 104
4426 4573
967078%
80% 80%
77%
78%
78%
79%
79%
80%
80%
81%
0
2000
4000
6000
8000
10000
12000
Q4 Q1 Q2
COP 18 COP 19
CLHIV Suppressed
An integrated health and child protection team conducts a joint home visit to address child protection and HIV adherence issues with a caregiver and her child (Bala S/C, Kole District).
Graph 3: Trend of CLHIV Enrollment and Suppression

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 19
Table 4: Challenges and Mitigation Strategies
Lessons Learned Strong relationships with influential stakeholders was key to enrollment and ongoing programming successes: DHO introductory letters for strategic district stakeholder engagement was paramount for rapid identification, cooperation, enrollment, and service delivery for new CLHIV, while involvement of Health Center In-Charges in debrief meetings increased support for enrolment and ownership of the activity by all those involved. Most caregivers and CLHIV have trust in health workers and easily disclosed information and referrals to the BOCY program. To avoid stigma, many CLHIV receive ART refills from clinics in BOCY sub-counties where they do not live, and caregivers use different names at facilities and in the community, which made the tracking and tracing of their homes difficult. Utilization of facility-based enrollment, targeting caregivers and CLHIV during ART clinic days was very helpful in achievement of results. Profiling, VLM, and addressing non-suppression requires a team approach: By close of Q1, BOCY reported 590 non-suppressed CLHIV (50% N). As underlying causes of non-suppression in children typically include a complex mix of clinical and/or social/child protection issues that can be easily overlooked at the clinic level, BOCY intensified the team approach, drawing on trusted and strong relationships between PSWs, BOCY social worker, RHITES Expert Clients, and clinic staff to deliver and coordinate case management services to CLHIV and to other highly complex cases through the engagement of BOCY CSO partner social workers, in collaboration with a strategic configuration of health workers, Expert Client/PSWs, or the Community Development Officer, depending on the nature of the
No. Challenges Encountered How the Challenges were Mitigated 1. Managing financial renumeration expectations of
health workers and Linkage Facilitators/Expert Clients who expected pay at level similar to what USAID/RHITES clinical partners offer.
Further engagement meetings were held for harmonization and they accepted to take the smaller facilitation offered by BOCY.
2. Difficulty in accessing TX_CURR data from private and high-volume hospitals without DHO letters and MoUs.
BOCY successfully advocated with DHOs to write introductory letters to clinic heads and MoUs were established, as needed.
3. Incorrect client information on facility records hampered tracing (names, telephone numbers, and villages).
Use of ART clinic days of such clients to access proper and updated information for location and enrolment.
4. Locating HHs of CLHIV based in rural areas Local leaders, especially LCs and cultural leaders, supported identification.
5. High relocation rates of HHs of TX_CURR in urban settings make it difficult to locate and enroll beneficiaries.
Facility records and ART days were used to meet such clients, identify new locations, and enroll.
6. Fear of stigma by female sex workers demanding tough conditions, such as paying their children’s school fees and not visiting their homes. During consent seeking at facility, some clients did not want to be followed up to the HH because of social relationships (i.e non-disclosure to partners).
Offered services based on preference/needs of clients (i.e. only at facility and not at HH level).
7. Trusted facilty–based Expert Clients recommended by ART clinic in-charges to support BOCY enrollment were too busy with their daily facility duties.
Other community structures such as PSWs and Village Health Teams were trained and supported to enrol TX_CURR CLHIV
8. Long distances between HHs and scattered HHs increased need for transport facilitation for affected Expert Clients and linkage facilitors
This was treated on case by case basis with enrolment fee adjustments and or social workers used project motorcycles to transport Expert Clients. Expert Clients and Village Heath Teams from based in distant clients villages were recruited for convenience.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 20
issue. These teams may make multiple visits – using different configurations – throughout the case management process to address a range of issues, including caregiver neglect, lack of functional knowledge about ART, and stigma as well as adherence issues around food/nutrition insecurity, limited care for CLHIV in boarding schools, long distances to health facilities, pill fatigue, or GBV. Individual care plans are then developed together with the caregivers and adolescents (when appropriate) to address identified barriers to suppression on a case-by-case basis. Involvement of health workers enabled CLHIV to receive onsite intensive adherence counseling (IAC), while CDOs provided child protection and social protection services and project social workers provided psychosocial support during home visits and supported families to access other services, including backyard kitchen gardens for nutrition support and linkages to VSLA groups for access to a welfare fund and the OVC Fund to subsidize transport to facilities for. Through these coordinated efforts, 199 non-suppressing CLHIV (75% E) were suppressing by the close of Q2. Linkage Officers supported by BOCY at high-volume facilities were also crucial members of the team, supporting filling; updating clients’ records; and facilitating linkages with community structures for reminders on ART appointment days and follow ups for missed appointments and lost clients. Further efforts were put in identifying, profiling, and viral load monitoring among the newly enrolled CLHIV and their caregivers. Overall, 862 new cases of non-suppressing CLHIV were identified during this quarter, the majority of which were those CLHIV who were newly enrolled. BOCY is using similar coordinated approaches with community and clinic teams to assess and develop targeted care plans to address complex non-adherence issues. Case conferences assist in resolving complex issues: During Q2, the project supported community case conferences (with child protection stakeholders) and clinic case conferences (with health workers) for targeted support to address specialized needs. Multisectoral3 community case conferences prioritize complex abuse cases of abuse and evaluate the actions taken on referred or pending cases – especially those too complex in nature to be handled by PSWs. Out of 1,999 child protection related cases presented and of these, 59% (1,179) were resolved through consultation with stakeholders, six were lost due to relocated HHs, and 814 were still pending and being followed up by the end of reporting quarter. The majority of cases resolved focused on child maintenance (neglect), emotional abuse, and irregular school attendance. Cases that remained pending by close of the quarter included cases around non-suppression, poor adherence, and GBV (including defilement), which are complex and often require sustained follow up for resolution.
3 Multisector stakeholders include para-social workers, CDOs, health workers, head teachers, the police, religious leaders, representatives of mapped child protection service providers, and BOCY-supported social workers (Linkage Officers, GBV Assistants, Economic Strengthening Assistants, Parenting and ECD facilitators).
BOCY CSO Social Worker in Tororo developing care plan after PSS session with caregiver of malnourished and non-suppressed CLHIV at Kirewa H/C III in Tororo.
“There are many cases of young children going to the facilities for ART refills unaccompanied by their caregivers, which makes it hard for the health workers to deliver intensive adherence counseling. Such caregivers may end up giving wrong dosages to the children, worsening the viral load copies. We encourage caregivers to come to the clinic with their children, but it is also critical to follow up with them at home to address issues that relate to home and family life.” –Clinic staff following a facility-based case conference, Mbale District

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 21
In Q2, BOCY supported 97 facility-based cases conferences in collaboration with high-volume sites. Participants included the clinic In-Charges, heads of departments, Case Management Assistants, Community Facility Linkage Assistants, Linkage Facilitators, Adherence Counsellors, and Expert Clients. Conferences focused on barriers to non-suppression and progress on IAC, plans for switching treatment regimens from first regimen to second for clients that have failed to respond to their current regimen, strategies for tracking those lost to follow up or those who had missed appointments, creating plans for follow up on viral load testing through physical follow up at the community level, updating client files, and reviewing Health Management Information System (HMIS) tools. Meetings also provide platforms for health facility teams and community structures to appreciate their roles and to improve coordination and support for clients by strengthening linkages and referrals. Targeted linkages, referrals, and tracking of SGBV survivors across the service cascade: The majority of the 288 GBV cases addressed in Q2 included emotional and physical violence at home which are typically handled between the PSW, Local Council leaders and CDO through mediation, dialogue and counselling of HH members. BOCY responded to and referred 23 statutory cases involving SGBV (defilement) and physical abuse reported these to the police. BOCY delivered psychosocial support and routine follow up home visits to all survivors, supported two survivors to access PEP, treatment of minor injuries and emergency pills. Through collaboration with Uganda Child Helpline (UCHL) team, 16 SVA cases were referred to BOCY and 9 were outside BOCY area of operation. Of the remaining seven cases, five were followed up (two relocated, two were closed, and one child was enrolled on the OVC program). In advance of International Women’s Day Celebration and to address and respond to issues of GBV and VAC at community level, BOCY supported 62 integrated community dialogues4 across 10 districts with high numbers of GBV cases in collaboration with health workers, local council leaders, police, CDO and clan leaders engaging and sensitizing 7955 community members to underlying causes of GBV and ways to improve positive parenting. Dialogues also enabled caregivers to understand different roles of police, CDO and teachers in prevention violence agains children. Case conference reports presented by PSWs informed most of the issues discussed at community level and facilitated service delivery and stronger trust between community members, police, CDOs and other authorities. The BOCY transport emergency fund supported 23 child SBGV suvivors to access health services with support from District Action Centre Officers and the Probation Office. Services received included PSS, medical examinations, and treatment of minor injuries as well as referrals to police for legal redress. BOCY CSO social workers continued to support the survivors through the healing process. Other cases handled included the assistance of HIV-positive and non-suppressing children that were sick and had challenges accessing health facilities due to transport and nutrition challenges. With BOCY support, CLHIV received ART refills, therapeutic foods and treatment for other illnesses. IR 3.2 Improved models for integrating clinical and socio-economic services for very young OVC BOCY Intensified integrated service delivery to EMTCT mothers and their HEI, delivering health and ECS services to 2,195 mother-baby pairs at the facility level, including 907 HIV-positive mother-baby pairs that were profiled with facilities during the BOCY enrollment surge. Health facility staff continue to applaud the contribution of ECD sessions for bringing mothers from the EID clinic together to share their experiences on how they protect their children from HIV transmission. Of the mother-baby pairs reached
4 These were mainly conducted in 10 BOCY districts of Lira, Dokolo, Kole, Agago, Kitgum, Oyam, Arua, Kamuli, Mayuge and Namayingo.
A facility-based case conference made up of RHITES and BOCY health and child protection actors in Namokora Health Center IV-Kitgum

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 22
at facilities, 632 were engagements at 14 PMTCT sites where mother-baby pairs already attended their ART clinic days. These included HIV-positive expectant or lactating mothers and their exposed infants who were identified with support of the EID/EMTCT In-Charges and who were enrolled at the facilities. ECD sessions conducted at PMTCT sites have helped in educating the mothers on nutritional issues, caring for exposed infants, and ensuring completion of immunization schedules. Experiences shared by the lactating mothers during facility-based sessions and follow-up visits indicate that some HIV-positive mothers had enrolled on ART without disclosing to their partners for fear of their reaction. The ECD sessions included strategies to support safe disclosure with their partners. BOCY trained ECD Facilitators have worked hand-in-hand with lead mothers to follow-up on issues in the community, viral load monitoring and follow-up on scheduled hospital visits, supporting the “Bringing back mother baby pairs in care” campaign with 11 mother-baby pairs returned to care while 2 non-suppressing mothers had their ART regiments changed for viral suppression and coordinate support for follow up visits with PSWs through case management. ECD home sessions strengthen good practices for promoting infant development: BOCY delivered 144 home sessions (68% N), targeting mother-baby pairs struggling with nutrition, growth, and adherence challenges ad supported the demonstration of key skills learned from the group in a family set-up. The home sessions also allowed the project to check on how mothers were utilizing the skills and knowledge acquired from the group learnings. Through these activities, mothers and caregivers were reminded to attend antenatal visits, immunize their children, improve hygiene in their homes by establishing simple hand-washing facilities at latrine sites. Integrated ECD outreaches, cooking demonstrations, and nutrition education: To enhance the health of mothers living with HIV and their infants, to bring services closer to family homes to eliminate long travel times, and to expand critical ECD services to the full community of vulnerable mothers with young children, BOCY delivered a range of cooking demonstrations, nutrition education, financial literacy sessions, backyard/kitchen gardening education, HIV prevention education, HIV screening, and family planning sessions for adults for 1,106 mother-baby pairs. Services for the infants included growth monitoring and nutrition screening, immunization, and general medical examinations. IR 3.3 Improved models for integrating clinical and socio-economic services for vulnerable youth and caregivers Peer support groups for adolescents living with HIV/AIDS – a team approach: To bolster support and address gaps in adherence and VLS for ALHIV, BOCY established Peer Support Groups in 44 high-volume clinical facilities, reaching 1,387 ALHIV. Drawing on lessons from the caregiver engagement model tested by BOCY last year, BOCY delivered HIV and treatment literacy, alternative skilling, life skills, and positive parenting services in collaboration with health workers and community structures. BOCY also delivered sessions to 2,110 youth in existing groups. At St. Joseph’s Health Facility in Kitgum, in Kuluva, and at Oli Health Centre in Arua, adolescents report that they feel better about their lives (improved resilience), more confident with peers and caregivers, and excited by the chance to earn small income from alternative skills and to improve food security and nutrition from baking bread and other enriched foods.
“I have always been worried that my child is HIV-positive since I delivered from home. However, during home sessions, I was encouraged to take her for all the PCR tests for confirmation. I’m glad my child was confirmed negative after the third PCR test, and now I can sleep with no stress,” -Nambozo, mother living with HIV, Mbale District

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 23
In Oyam, Minakulu, and Kitgum, caregivers were excited about their backyard gardens where they harvest vegetables to improve their diet. At Bufumbo Health Centre in Mbale, caregivers sold vegetables from their gardens to other community members during the HIV clinic day. This enables them to save money for transport to the facility during clinic days and to buy essential medicines that may be inaccessible at the facility. Caregivers at this facility also established a group that includes positive adolescents and are involved in peer support activities, positive parenting groups, and savings groups. In Q2, the group accumulated savings of UGX 782,000, including UGX 88,500 for the social fund and UGX 90,000 for the OVC Fund. The health workers at this facility have reported 95% caregiver attendance during clinic days due to the introduced savings component, while the caregivers expressed gratitude to the project as now they have reduced challenges of transport to the facility through their savings.
Due to the peer support group interventions and caregiver engagement, there has been a significant improvement in viral load suppression among adolescents enrolled into the peer support groups. Viral load tracking conducted this quarter indicated that in the East, out of 2,574 ALHIV, most adolescents (1,506) are now suppressing, compared to the 680 last quarter. In the North, out of 1,946 monitored, 1,208 were suppressing. Most adolescents had adherence challenges
emanating from issues such as domestic violence, caregiver neglect, poor feeding habits, and lack of a conducive environment for those children at school. Strategies to address these issues were established, including intensive adherence counselling by health workers, trained Expert Clients, and Linkage Facilitators as well as intensified home visits by PSWs and discussion with head teachers and senior men and women during facility stakeholder meetings to address school-relaetd stigma and disclosure challenges. One specific challenge faced in programming for ALHIV is the lack of harmonized days for ART refills for adolescents in some facilities, making it difficult to deliver sessions to all adolescents at once. To address this challenge, the project is engaging facility In-Charges to harmonize ART days for adolescents. Integrated GBV/HIV prevention service delivery targeting DREAMS girls and most at risk adolescents: in Q2, BOCY intensified efforts to deliver HIV and GBV prevention services to 9-14 year olds through 372 school-based Clubs reaching 11,160 children using the SINOVUYO curriculum enhanced with three PEPFAR-developed modules aimed to help young girls learn about their bodies, understand their vulnerability to and protect themselves from sexual abuse. BOCY also delivered integrated GBV and HIV prevention, ARSH, financial literacy and alternatively skill trainings to 10,160 out- of-school adolescent youth and DREAM girls. This included intensified delivery of JFFS and alternative skills training to DREAMS girls - from 13% in Q1 to 55% in Q2 - to mitigate HIV risk links to dependence on men for basic needs. Expanding NO MEANS NO SGBV prevention for girls and boys: To deepen the impact of the No Means No sexual violence prevention activities for adolescent girls in Tororo and Mbale, BOCY began the delivery of the boys’ version of the No Means No program with district and sub-county entry
“I have lived with HIV all my life. I had no happiness and hope in life. My stepmother made me believe that I am useless and cannot amount to anything important in life because of my status. However, ever since I joined this group, my life has changed. I have learnt that life does not not lose meaning and value because of HIV. I have made five beautiful friends who care about me. I am happier and I love my life. My friends support me to take my drugs and my viral load has been suppressed.” – Aidah, 16-year-old adoelscnet living with HIV, Mbale District
“I am so grateful because I joined this SIRA group. I used to be in pain and hated men because my aunt’s husband whom I trusted so much raped me. He made my aunt hate me. She sent me away from her home and that was the end of my education. This group has helped me a lot to heal my pain. I have learnt to accept what happened to me and I believed that it was not my fault, and my life is better.” -16-year-old girl from Northern Division, Mbale District
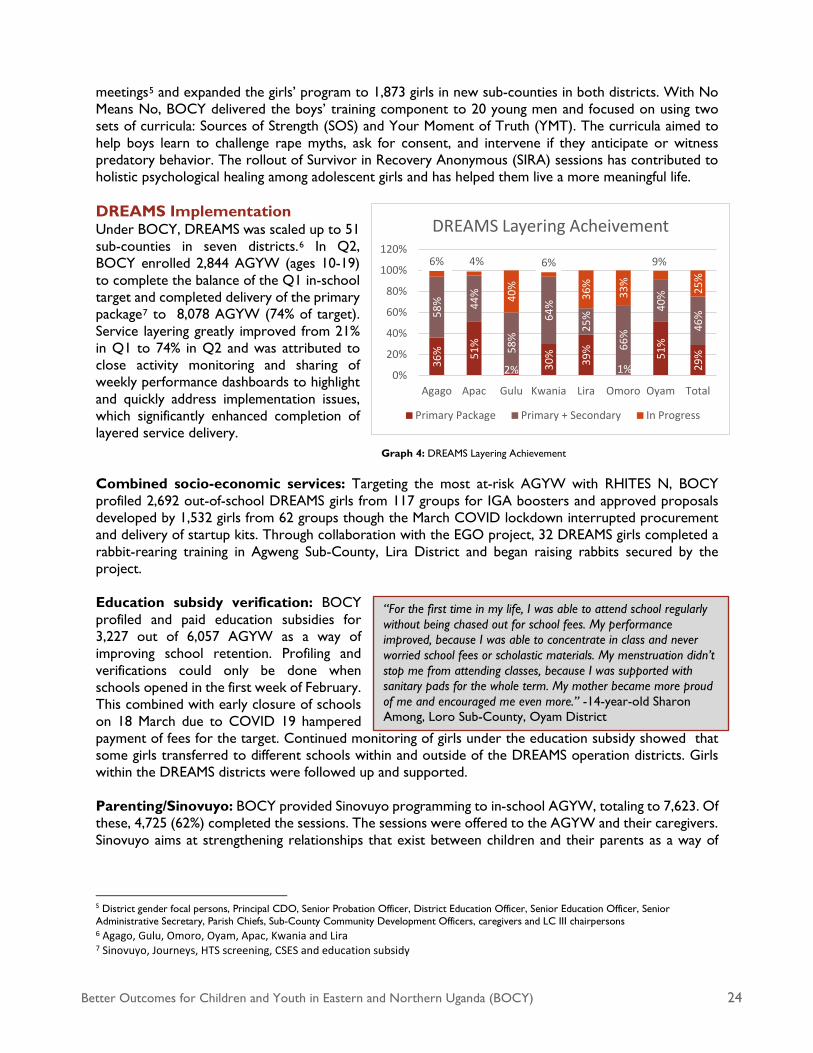
Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 24
meetings5 and expanded the girls’ program to 1,873 girls in new sub-counties in both districts. With No Means No, BOCY delivered the boys’ training component to 20 young men and focused on using two sets of curricula: Sources of Strength (SOS) and Your Moment of Truth (YMT). The curricula aimed to help boys learn to challenge rape myths, ask for consent, and intervene if they anticipate or witness predatory behavior. The rollout of Survivor in Recovery Anonymous (SIRA) sessions has contributed to holistic psychological healing among adolescent girls and has helped them live a more meaningful life. DREAMS Implementation Under BOCY, DREAMS was scaled up to 51 sub-counties in seven districts.6 In Q2, BOCY enrolled 2,844 AGYW (ages 10-19) to complete the balance of the Q1 in-school target and completed delivery of the primary package7 to 8,078 AGYW (74% of target). Service layering greatly improved from 21% in Q1 to 74% in Q2 and was attributed to close activity monitoring and sharing of weekly performance dashboards to highlight and quickly address implementation issues, which significantly enhanced completion of layered service delivery. Combined socio-economic services: Targeting the most at-risk AGYW with RHITES N, BOCY profiled 2,692 out-of-school DREAMS girls from 117 groups for IGA boosters and approved proposals developed by 1,532 girls from 62 groups though the March COVID lockdown interrupted procurement and delivery of startup kits. Through collaboration with the EGO project, 32 DREAMS girls completed a rabbit-rearing training in Agweng Sub-County, Lira District and began raising rabbits secured by the project. Education subsidy verification: BOCY profiled and paid education subsidies for 3,227 out of 6,057 AGYW as a way of improving school retention. Profiling and verifications could only be done when schools opened in the first week of February. This combined with early closure of schools on 18 March due to COVID 19 hampered payment of fees for the target. Continued monitoring of girls under the education subsidy showed that some girls transferred to different schools within and outside of the DREAMS operation districts. Girls within the DREAMS districts were followed up and supported. Parenting/Sinovuyo: BOCY provided Sinovuyo programming to in-school AGYW, totaling to 7,623. Of these, 4,725 (62%) completed the sessions. The sessions were offered to the AGYW and their caregivers. Sinovuyo aims at strengthening relationships that exist between children and their parents as a way of
5 District gender focal persons, Principal CDO, Senior Probation Officer, District Education Officer, Senior Education Officer, Senior Administrative Secretary, Parish Chiefs, Sub-County Community Development Officers, caregivers and LC III chairpersons 6 Agago, Gulu, Omoro, Oyam, Apac, Kwania and Lira 7 Sinovuyo, Journeys, HTS screening, CSES and education subsidy
“For the first time in my life, I was able to attend school regularly without being chased out for school fees. My performance improved, because I was able to concentrate in class and never worried school fees or scholastic materials. My menstruation didn’t stop me from attending classes, because I was supported with sanitary pads for the whole term. My mother became more proud of me and encouraged me even more.” -14-year-old Sharon Among, Loro Sub-County, Oyam District
36% 51
%
2% 30% 39%
1%
51%
29%
58% 44
%
58%
64%
25%
66%
40%
46%
6% 4%
40%
6%
36%
33%
9%
25%
0%
20%
40%
60%
80%
100%
120%
Agago Apac Gulu Kwania Lira Omoro Oyam Total
DREAMS Layering Acheivement
Primary Package Primary + Secondary In Progress
Graph 4: DREAMS Layering Achievement

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 25
curbing violence against children within families. In Q3 BOCY will explore very small group based8 engagement to continue service provision and complete service layering. Other activities: Together with RHITES North Lango, BOCY conducted an internal DREAMS DQA9 in sub-counties10 in the Lango region, which showed improved usage of the registers by all partners. BOCY also participated in bi-weekly coordination meetings in the Lango region and monthly meetings in the Acholi region to address implementation changes, data entry gaps, and service layering. DREAMS enrolment tools, service trackers, passports, and service registers were distributed to the CSOs in the field to improve documentation, and 12511 safe spaces (i.e. schools, churches) were identified for club meetings. BOCY also attended the interagency DREAMS IP meeting held in Kampala and continued to work with Community Development Officers, health officials, and the police in responding to GBV through community dialogues. Result 4: Monitoring, Evaluation, and Learning BOCY continued to monitor project progress against all indicator targets. Within Q2, 115,278 (77% children) project-supported OVC and caregivers were tracked and monitored through the various monitoring platforms (home visits, outreaches, group-based trainings/education). IR 4.1.1 Household graduation results In Q2, BOCY administered graduation assessments to 16,056 households. As a result, 5,678 households, constituting 27,225 OVC and caregivers (52% F), were graduated. BOCY retained 547 qualifying CLHIV HHs to ensure ongoing support for adherence and viral load suppression through the program close.12 Financial security (FS) constrained 50% of HH missing only one benchmark and 83% of HHs missing two benchmarks (FS and any other benchmark). IR 4.1.2 Review of MEL tools and upgrading of project database Following PEPFAR MER Version 2.4 tool upgrades13 in Q1, BOCY upgraded and operationalized the project e-database to enable OVC_MIS, DREAMS (from UDOTS) data uploads via API, avoiding manual entry and easing reporting and minimizing data transcription errors. An API was successfully developed that enabled the upload of individual beneficiary data from the BOCY database to the OVC_MIS, thus minimizing transcription errors that could arise from manual data entry of OVC_MIS forms by CSOs.
8 2 Caregivers and their children 9 Data Quality Assessment 10 Loro, Minakulu, Otwal, Iceme, Abok, Barr, Amach, Aromo, Cawente, Akokoro, Apac, and Ibuje 11 Oyam (50), Lira (34), Agago (14), Gulu/Omoro (24) 12 WEI/Bantwana is working closely with USAID on the process of transitioning to new programming partners, as appropriate. 13 Viral load monitoring tool; HIV risk assessment tool to include TB screening questions; home visit tool to include beneficiary risk categories; and updated linkages tool to enable effective collection of data on group-based activities and outreaches for HIV cascade, including ART linkages, adherence support, and viral suppression.
Graph 5: BOCY FY20 SAPR Graduation Cascade

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 26
IR 4.1.3 MEL mentorship and support supervision The BOCY MEL team continued to provide mentorship and support supervision to its IPs, thereby promoting the appreciation of data quality and use of data to inform programming. Following the orientation of CSO staff on the revised PEPFAR MER guidelines (version 2.4) and the training in advanced analysis using Excel in Q1, dashboards were used at the CSO level to inform performance across IPs. BOCY further collaborated with SITES through onsite reviews of Q1 performance and jointly identified strengths for replication as well as areas of concern. A key recommendation from SITES was transferring HIV-negative households to local government, which BOCY will do in Q3 and Q4. 3. ADAPTIVE MANAGEMENT APPROACH AND GUIDING PRINCIPLES 3.1 Collaboration and Stakeholder Engagement The BOCY project continued to leverage support for its beneficiaries through collaborative efforts with different partners, including CSOs working under the BOCY project. BOCY engaged AVSI’s Skilling Youth for Employment in Agribusiness (SKY) project to train 45 BOCY beneficiaries in Lira District in rabbit rearing and the management and provision of seed rabbits. AVSI14 also facilitated transport and SDA for 20 health workers attending BOCY’s integrated health outreaches in six Kitgum sub-counties. Health workers played a key role in profiling the CLHIV/HEI; supporting ECD group formation; participating in nutrition education, adherence, viral load sessions, and cooking demonstrations with PMTCT mother-baby pairs at health facilities; and supporting infants to access PCR/DNA, immunization, and other growth monitoring services at different health facilities. In West Nile, BOCY collaborated with IDI in viral load tracking, HTS provision, tracking of LTFU, and the mainstreaming of the YAPS rollout. Engagement with RHITES-EC and RHITES-E improved the quality of service for Peer Support Groups meeting at facilities. Through work with Mbale District in collaboration with Uganda Adolescent Health Forum (UAHF), RHITES-E, TASO, and the Red Cross, the project served over 5,000 adolescents during the SHE DECIDES festival with sexual and reproductive health education, cancer screening, family planning information, and SACCO seeds for eggplant. Collaboration with the police and local government leaders in sub-counties led to physical policing of video halls, stone quarry sites, and sugar cane plantations to monitor issues of child rights violations as well as to enforce community by-laws. The project also collaborated with the Probation Officers, the DHO, and LCs to raise awareness on GBV and violence against children in the districts of Kamuli and Mbale, reaching 442 youth. In Gulu, collaboration with a private company called Re-Fruit and Gulu Agricultural Development supported a youth group, Green Palace, in the production of vegetables through irrigation. The group is now involved in the production of okra, pumpkins, green paper, and other vegetables for home consumption and sale. 3.2 Learning and Adaptation BOCY adapted its strategy of performance tracking through weekly DREAMS dashboards and district-specific strategies to address low performance through subsequent follow up on action plans. To assess activity progress and budget tracking, BOCY adopted intervention trackers for curriculum-based services to identify challenges or gaps in service provision. Use of the dashboard and strategies resulted in DREAMS layering improving to a rate of 74%. 3.3 Inclusive Development Adolescents living with HIV are particularly disadvantaged and excluded from within their communities as well as at their schools. BOCY uses positive youth development approach across all of its adolescent platforms include in and out of school Clubs for OVC and DREAMS girls, parenting, No Means No and 14 Using funds from the Italian Agency for Cooperation and Development (AICS) Project.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 27
Peer Support Group platforms that aim build agency and competence in adolescents to develop goals, protect themselves from and report violence, and become positive role models and change agents at school, at home and in their communities. 4. MANAGEMENT AND ADMINISTRATIVE ISSUES 4.1 Key Management Issues In response to the COVID-19 pandemic, BOCY put in place measures aligned with MoH and PEPFAR guidance to promote social distancing, handwashing, and the dissemination of COVID-19 prevention protocols to ensure the safety of staff. In early March, BOCY made changes to its work procedures, encouraging staff to take time off or work from home and to only have staff working on critical and essential activities at the office. BOCY procured supplies for use in protecting staff, including sanitizers and hand-washing utensils, and oriented staff on COVID-19 signs, symptoms, prevention methods, and government directives. Aligned with President Museveni’s statement on March 26, 2020 announcing the national lockdown, BOCY management took the following measures: (a) closed all offices and established mechanisms to monitor the safety of the office and assets; (b) allowed staff working at the regional offices to move to their families before lockdown; (c) established virtual platforms for coordination, collaboration, meeting, and reporting; and (d) coordinated with CSO partners and have been supporting them in their response to the pandemic. The management team further decided and provided guidance to CSO partners to continue to implement critical case management activities, focusing on the distribution of ARVs to CLHIV and caregivers; facilitating transport for EMTCT mothers and non-suppressing children who had overdue clinical appointments but could not afford access to services; and providing child protection and gender-based violence activities. BOCY ceased all other activities, including group-based activities (VSLAs, parenting, ECD, No Means No, YAPS, JFFS, and DREAMS clubs), in compliance with government directives to stop meetings of more than four persons. These groups will resume when the restrictions are lifted and the situation improves. To respond to the COVID-19 emergency, BOCY submitted a $90,000 emergency plan and budget request to USAID. The plan will reach 15,000 at-risk beneficiaries in the areas of case management, child protection, emergency food distribution, and economic strengthening.15 5. HOW IMPLEMENTING PARTNER HAS ADDRESSED A/COR COMMENTS
FROM THE LAST QUARTERLY OR SEMI-ANNUAL REPORT While it was not formally documented in the annual report feedback, the AOR emphasized in various meetings the importance of BOCY enrolling 100% CLHIV on ART, HEI, and EMTCT mothers on the OVC program. As a response, the project launched an enrollment surge on February 3, 2020 to March 15, 2020, profiling a total of 12,563 CLHIV across BOCY-supported districts for enrollment. 6. PLANNED ACTIVITIES FOR NEXT QUARTER INCLUDING UPCOMING
EVENTS
1. Graduation of HHs that have met graduation benchmarks 2. IP localization activities with MUCOBADI 3. Support to YAPS
15 Non-suppressing children, non-suppressing lactating mothers, CLHIV children, EMTCT mothers, and GBV cases.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 28
4. Payment of education subsidies 5. ART adherence counselling and support
a. Psychological support for clients integrated with messages on COVID-19 b. Health education talks through groups with an emphasis on adherence c. Supported Expert Clients for peer support d. Intensive adherence counselling for the non-suppressed
6. DREAMS - Completion of service packages, including the backlog of AGYW 7. Implementation of COVID-19 contingency plan
7. FINANCIAL MANAGEMENT
Activity Financial Analysis Award Details: a. Total Estimated Cost $41,716,912 b. Start/End Date 4/21/2015 4/20/2021 c. Total Obligated Amount $38,706,496 d. Total Expenditure billed to USAID/Uganda $34,934,368 e. Expenditure incurred but not yet billed $1,003,948 f. Total Accrued Expenditure (both billed and not yet billed); sum of lines d and e $35,938,316
Actual Expenditures Projections for the
Next Two Quarters Q1 Q2 Q3 Q4 Average Quarterly Expenditure Rate $1,860,312 $1,608,934 $1,989,129 $1,627,564 Percentage Expenditure Against COP19 Budget 26% 23% 28% 23% Expenditures during the quarter were uneven compared to budgets. Monthly expenditures were as follows:
The overall expenditure for Q2 represents 69% of the Q2 budget. This was mainly due to outstanding education subsidy payments that were not completed in the quarter and need to be done in Q3.
Month Amount January 2020 $414,832 February 2020 $540,186 March 2020 $653,916 Total $1,608,934

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 29
ANNEX A: SUCCESS STORY
Improving adherence, viral load suppression, and resilience through
integrated case management and coordinated clinic-community service delivery
Forty-five-year-old Byobona Margaret Nafuula is a bubbly mother of five children—16, 14, 13, nine, and six years old. But nearly 11 years ago, her life was falling apart. She was ill frequently. On one occasion, when the sickness persisted, she went to Nawandala Health Centre III in Iganga District to seek medical treatment. She was tested and found to be HIV-positive. As a breastfeeding mother, she immediately became worried about her infant child. The health workers advised her to bring the baby and her other children for testing. Two of the children, now 13-year-old Nabirye Christine and nine-year-old Walugyo Moses, were found to be HIV-positive.
Both children were enrolled onto ART. Margaret was frank and disclosed her status to her husband. He was tested at the health facility and found to be HIV-negative. However, a year ago, their daughter, Nabirye Christine, was discovered to be non-suppressing following the results she received from a viral load test (1,699 copies) at Nawandala Health Centre III. Under the USAID/Uganda Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) activity, the project’s case management team has worked diligently to enhance coordination between community cadres and clinic stakeholders, like those at Nawandala Health Centre III, to improve follow-up care for children living with HIV (CLHIV). Improved community-clinic coordination has allowed clinic-based staff (i.e. nurses, Expert Clients, BOCY-supported Linkage Officers) to work with community cadres like Para-Social Workers (PSWs) and, when necessary, supervising social workers to more regularly track adherence and address non-suppression among CLHIV. Upon the discovery of Christine’s viral load results, the community team called on her to conduct further assessment and consultation. Upon their outreach, they learned that Christine’s caregivers were largely absent from home, working to earn money from fishing and farming in Busia District. The children were left under the care of their eldest sister, who was just 15 years old at the time. It was quickly discovered that the challenges the family faced were numerous. They lived in a rented house, and with both parents away, the landlord often harassed the children for any rent defaulted. They only ate once in a while, when a community member was benevolent. The extreme stress and harassment from the landlord, poor nutrition, and neglect that the children faced compounded the non-suppression issues faced by Christine and her brother, Moses. Additionally, the long distance from home to the health facility impeded the eldest sibling from taking her two HIV-positive siblings for ART refills. In response, with the health workers at the clinic, the BOCY team worked to develop a care plan to support Christine. The first step was to work with Margaret and her husband to encourage them to move back home. The PSW shared his concerns with the children’s father about the stress that the children were facing and how their circumstances were endangering with their health. The PSW encouraged him and Margaret to permanently move back home, suggesting that the couple could enroll in a savings group and, with BOCY
“The news that my children tested HIV-positive hit me hard. It was a struggle to feed the children. We did not have a stable place to live. It was hard dealing with my own diagnosis and having two of the children test positive was heartbreaking. But as a mother, I had to be strong for them,” Margaret shared.

Better Outcomes for Children and Youth in Eastern and Northern Uganda (BOCY) 30
support, start up a backyard garden. Margaret and her husband were also advised to get the children food in a timely manner and to monitor whether the two children on ART were taking their drugs. Upon returning home, Margaret was enrolled into a Village Savings and Loans Association (VLSA) by a BOCY PSW as an economic strengthening measure to improve the family’s savings and access to finances. The couple also trained in backyard gardening. They planted Sukuma wiki, ntuula, tomatoes, and okra. The silver fish and vegetables grown in the backyard greatly improved on the family’s nutrition. The PSW and Expert Client continued to check in with the family regularly by cell phone and through targeted home visits to address any adherence challenges faced by Christine and Moses, including travel to the clinic for regular ART appointments and regular access to nutritious foods. When clinic travel was not possible, the PSW or Expert Client delivered their medication to their home during home visits. The household also received other core services, including psychosocial support, intensive adherence counselling, nutritional education, economic strengthening packages, HIV and other health-related services, and emergency/temporary consumption support. Christine’s condition soon improved with consistent follow up from the PSW, better nutrition, and the benefit of having both parents present to monitor her adherence. Within two months, she had suppressed (less than 839 copies). She now feels better and stronger. She is making new friends at school and has even been elected Class Monitor. Margaret happily reflects on what life is like now for the family: “We have built our own home. Our children do not have to deal with the stress of terrorizing landlords anymore. We have also expanded our farming ventures to include the rearing of chickens, ducks, cattle, and goats. I am grateful that Christine is suppressing and that the other children are in good health. I can finally envision a future where the children complete school uninhibited by health issues or financial woes.”
Margaret and her children share a lighthearted moment in their garden.