Embed Size (px)
Citation preview

CCR TranslationsCommentary on Kayani et al., p. 6021
Better Late than Early: FDG-PET Imaging in MetastaticRenal Cell Carcinoma
Michael R. Harrison1,3 and Daniel J. George1,2,3
Sunitinib treatment benefits patients with metastatic renal cell carcinoma (mRCC), but response
duration can vary widely and resistance is not predicted by standard measures. [18F]fluoro-2-deoxy-2-
D-glucose positron emission tomography (FDG-PET) uptake is variable in mRCC, but changes in FDG-PET
uptake may be useful in monitoring disease progression. Further work is needed to personalize treatment
for patients with mRCC. Clin Cancer Res; 17(18); 5841–3. �2011 AACR.
In this issue of Clinical Cancer Research, Kayani andcolleagues report in a cohort of 44 metastatic renal cellcarcinoma (mRCC) patients treated with sunitinib that ametabolic response by sequential [18F]fluoro-2-deoxy-2-D-glucose (FDG) positron emission tomography (PET) at4 weeks did not correlate with outcomes, whereas meta-bolic progression at 16 weeks was predictive of inferiorsurvival (1). Historically, FDG-PET imaging was notthought to be particularly useful in kidney cancer. Mostradiotracers, including FDG, are eliminated by the kidneysand primary renal cell carcinoma tumors seemed to haverelatively low glucose uptake (2). FDG-PET did not seem toadd anything to conventional imaging for the characteri-zation of renal masses. Previously, data were scant on therole of FDG-PET for treatment monitoring of mRCC (3, 4).Kidney cancer is a heterogeneous disease. Consequently,
prognostic models have been developed in the era of VEGF-targeted therapy based on clinical variables to classifypatients into risk groups (5). Such classifications are espe-cially important for patient counseling and risk-directedtherapy, as well as for clinical trial design. The finding byKayani and colleagues that the maximum standardizeduptake value (SUVmax) correlated with decreased survival(1) is important, and SUVmax should be considered as acriterion for incorporation in future prognostic models.Despite the success of newer targeted therapies such assunitinib in improving outcomes, essentially all patientsexperience progression, although the duration can varywidely (6). With an increasing number of treatment
options for patients with mRCC, it is essential to developpredictive biomarkers for clinical benefit to sunitinib treat-ment, so that patients benefiting will stay on therapy,whereas those who are not may be considered for alterna-tive approaches.
Standard anatomic radiographic imaging does not seemto do well in predicting mRCC patients who may benefitfromsunitinib treatment (7). Functionalmolecular imaging,like PET, may provide additional information about tumorbiology when used sequentially as a kind of "noninvasivebiopsy." As such, Kayani and colleagues prospectivelyexplored the prognostic and predictive significance ofsequential FDG-PET. Clinically, at least 3 distinct patternsof resistance to sunitinib therapy are recognized, as observ-able by standard radiographic imaging. Some patients willnot have anymeasurable tumor regression and will progressrapidly (intrinsic nonresponsiveness). Others will have aminor measurable tumor regression followed by diseaseprogression. Still others will have remarkable, sustainedtumor responses, with slow, perhaps mixed, progressionto a lower tumor burden than that observed prior totherapy. Ideally, we would like a tool that discriminatesamong these phenotypes early in the treatment courseand more accurately than standard imaging, to optimizetreatment decisions in individual patients and better de-fine patient populations for subsequent clinical studies.
FDG-PET imaging in cancer takes advantage of 2 generalprinciples: (i) cancer cells tend to have elevated rates ofglucose uptake and glycolysis compared with normal cells,and (ii) once the FDG radiotracer is taken up by cells andphosphorylated, it becomes trapped intracellularly. Thereprogramming of energy metabolism is now considereda hallmark of cancer (8), in addition to the original para-digms of aberrant growth signaling, tissue invasion andmetastasis, limitless replicative potential, sustained angio-genesis, and evasion of apoptosis. The capability of cancercells to undergo "aerobic glycolysis" by limiting theirenergy metabolism largely to glycolysis, avoiding oxidativephosphorylation even under aerobic conditions (Fig. 1A),was first described by Otto Warburg (9). The glucose
Authors' Affiliations: Divisions of 1Medical Oncology, Department ofMedicine, and 2Urology, Department of Surgery, Duke University MedicalCenter; 3Duke Cancer Institute, Durham, North Carolina
Note: This manuscript is original work and has neither been published norsubmitted elsewhere, in whole or in part.
Corresponding Author: Daniel J. George, DUMC 102002, 10 BryanSearle Drive, 471 Seeley Mudd Bldg., Durham, NC 27710. Phone: 919-668-4615; Fax: 919-668-7117; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-11-1768
�2011 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 5841
Cancer Research. by guest on September 4, 2020. Copyright 2011 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

analogue FDG is moved into cancer cells by glucose trans-porters and phosphorylated by hexokinase to FDG-6-phos-phate (Fig. 1B). Tissue FDG accumulation can be expressedsemiquantitatively by the SUV, which normalizes the con-centration of tissue radioactivity to the dose of the injectedradiotracer and the patient’s body weight. Although theSUVmax is most often used in the clinic, several differentSUV parameters have been defined (Fig. 1C).
Kayani and colleagues report that although 57% ofpatients had a metabolic response in the SUVmax metastaticlesion at week 4 (a 20% or greater decrease in SUVmax), thiswas not associated with improved progression-free survival(PFS) or overall survival (OS). This contrasts with thefinding that PFS correlated with week 4 metabolic responsein sunitinib-treated gastrointestinal stromal tumors (GIST;ref. 10). One key difference in the 2 studies is that the lattermeasured SUV in a 2-cm3 volume (i.e., SUVpeak) for each of
the 3 most metabolically active lesions at baseline, whichwere then averaged and reevaluated at week 4. This dis-crepancy may reflect the inherent biological differencesbetween mRCC and GIST or the dynamic nature of mRCCtumors, as the authors suggest (1). One alternative expla-nation is that the single most FDG-avid voxel (Fig. 1C),chosen from the median 6.5 FDG-avid sites per patient,may not by itself be reflective of treatment changes. To putit another way, the response to therapy by a patient’sdisease might not be able to be boiled down to 1 number,calculated from just 1 point reflecting relative SUVmax,within 1 of a patient’s many tumors. Finally, it is possiblethat other aspects of tumor biology in addition to increasedglucose metabolism become dominant in response totreatment and, thus, drive outcomes.
So, how do wemake sense of the findings that metabolicresponse at 4 weeks was not predictive, but metabolic
© 2011 American Association for Cancer Research
Glucose
A B C
Glucose
Glucose-6-PO4
Glucose-
6-PhosphataseGlycolysis
NADH NAD+
LDH-ALactate
Mitochondrion
[18F]Fluoro-2-deoxy-2-D-glucose (FDG)
uptake by cancer cells
Cancer cell metabolism
of glucose: Warburg effect
Acetyl-CoA
Anaerobic
Pyruvate
Glycolysis
Pyruvate
Aerobic
Cell
membrane
Lactate
Cytoplasm
Hexokinase
High
glucose
Rib
SUVMax
SUVPeak
1cm
Tumor
Intercostal
space
Boiling a tumor down to one number:
Comparison of imaging parameters
Unidimensionalä(RECIST)
Hexokinase
FDG-6-PO4
Intracellular
Trapping
FDG
FDG
Low
glucose
TCA
Cycle
Citrate
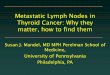
Figure 1. A, cancer cell metabolism of glucose. Glucose enters the cell through a transporter and is converted to pyruvate by glycolysis. Under hypoxicconditions, pyruvate is converted to lactate. Cancer cells convert pyruvate to lactate even in normoxic conditions, whereas in normal cells pyruvateenters the tricarboxylic acid cycle (TCA) in mitochondria. By favoring glycolysis over oxidative phosphorylation (the Warburg Effect), cancer cells mustcompensate for the many-fold lower efficiency of energy production by upregulating glucose transporters and glycolysis enzymes, resulting inincreased glucose uptake and use compared with normal cells. B, FDG uptake by cancer cells. FDG enters cells by glucose transporters and is phosphorylatedby hexokinase to FDG-6-phosphate. Because it cannot be metabolized further along the glycolytic pathway and tumor cells do not contain enoughof the enzyme necessary to reverse the phosphorylation, FDG-6-phosphate is trapped intracellularly. C, selected PET imaging parameters (SUV) incomparison with a standard radiographic imaging parameter. Voxel, a 3-dimensional pixel; SUVmax, maximum SUV of a tumor (voxel); SUVpeak, the mean SUVwithin a sphere centered on SUVmax (different diameter spheres have been used in the literature); Response Evaluation Criteria in Solid Tumors (RECIST), theunidimensional largest diameter of a tumor lesion.
Harrison and George
Clin Cancer Res; 17(18) September 15, 2011 Clinical Cancer Research5842
Cancer Research. by guest on September 4, 2020. Copyright 2011 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

progression (i.e., increase in SUVmax) at week 16 didcorrelate with inferior outcomes (1)? The authors’ expla-nation is that timing FDG-PET in week 4may have been tooearly in mRCC to predict resistance, especially given that82% of metabolic progressors at week 16 (n ¼ 12) had aresponse at week 4. An alternative might be that whenone evaluates at a point of maximal activity, attenuation isnecessary, but not sufficient, to portend outcome. In otherwords, the SUVmax is just the tip of the iceberg: When itdisappears below the surface of the water, it does not giveus any information about what may be going on beneaththe surface, but when it continues to rise higher above thesurface of the water, it may be more reflective of changesgoing on below the surface. In some respects, it is remark-able that an increase in SUVmax on FDG-PET from a singleselected lesion provides any insight into patient outcome,because it is not a direct measure of other biologicalchanges simultaneously going on within the tumor involv-ing growth signaling and/or proliferation, hypoxia andblood vessel formation, or programmed cell death.Kayani and colleagues should be commended for
incorporating an elegantly designed secondary analysisinto a prospective treatment trial, shedding light on therole of treatment monitoring with FDG-PET in mRCCpatients treated with sunitinib. However, more work
remains to be done. Liu and colleagues have evaluatedearly changes in proliferation after sunitinib treatmentin mRCC using a thymidine analogue (11). AdditionalPET radiotracers, perhaps in combination, and SUVparameters, should continue to be evaluated to obtainthe best biological readout. Other functional imagingmodalities should also be evaluated. For example, arecent study compared microbubble ultrasound, dyna-mic contrast-enhanced MRI, and dynamic contrast-enhanced computed tomography for assessment of vas-cular responses (12). Although more research is neededto translate these findings to clinical treatment monitor-ing for the benefit of patients, the work by Kayani andcolleagues provides seminal insights into the biologyand timing for biomarkers of sunitinib treatmentresponse in mRCC patients.
Disclosure of Potential Conflicts of Interest
D.George: commercial research support, Novartis, Pfizer, Bristol-MyersSquibb, GlaxoSmithKline; honoraria, Novartis, Pfizer, and Genentech;consultant, Novartis, Pfizer, and Genentech. M. Harrison: honorarium,Novartis.
Received July 27, 2011; accepted August 1, 2011; published OnlineFirstSeptember 13, 2011.
References1. Kayani I, Avril N, Bomani J, Chowdhury S, Rockall A, Sahdev A, et al.
Sequential FDG-PET/CT as a biomarker of response to sunitinib inmetastatic clear cell renal cancer. Clin Cancer Res 2011;17:6021–8.
2. Miyakita H, Tokunaga M, Onda H, Usui Y, Kinoshita H, Kawamura N,et al. Significance of 18F-fluorodeoxyglucose positron emissiontomography (FDG-PET) for detection of renal cell carcinoma andimmunohistochemical glucose transporter 1 (GLUT-1) expression inthe cancer. Int J Urol 2002;9:15–8.
3. Vercellino L, Bousquet G, Baillet G, Barr�e E, Mathieu O, Just PA, et al.18F-FDG PET/CT imaging for an early assessment of response tosunitinib in metastatic renal carcinoma: preliminary study. CancerBiother Radiopharm 2009;24:137–44.
4. Revheim ME, Winge-Main AK, Hagen G, Fjeld JG, Fossa�SD, Lilleby
W. Combined positron emission tomography/computed tomographyin sunitinib therapy assessment of patients with metastatic renal cellcarcinoma. Clin Oncol (R Coll Radiol) 2011;23:339–43.
5. Heng DY, Xie W, Regan MM, Warren MA, Golshayan AR, Sahi C,et al. Prognostic factors for overall survival in patients with meta-static renal cell carcinoma treated with vascular endothelial growthfactor-targeted agents: results from a large, multicenter study. JClin Oncol 2009;27:5794–9.
6. Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM,Oudard S, et al. Overall survival and updated results for sunitinib
compared with interferon alfa in patients with metastatic renal cellcarcinoma. J Clin Oncol 2009;27:3584–90.
7. Kontovinis LF, Papazisis KT, Touplikioti P, Andreadis C, MouratidouD, Kortsaris AH. Sunitinib treatment for patients with clear-cell met-astatic renal cell carcinoma: clinical outcomes and plasma angiogen-esis markers. BMC Cancer 2009;9:82.
8. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation.Cell 2011;144:646–74.
9. Warburg O. On respiratory impairment in cancer cells. Science1956;124:269–70.
10. Prior JO, Montemurro M, Orcurto MV, Michielin O, Luthi F, Ben-hattar J, et al. Early prediction of response to sunitinib after imatinibfailure by 18F-fluorodeoxyglucose positron emission tomography inpatients with gastrointestinal stromal tumor. J Clin Oncol 2009;27:439–45.
11. Liu G, Jeraj R, Perlman S, Vanderhoek M, Kolesar J, Eickhoff J, et al.Pharmacodynamic study of FLT-PET imaging in patients treated withsunitinib. J Clin Oncol 2008;26:3515.
12. Bjarnason GA, Williams R, Hudson JM, Bailey C, Lee CR, Lloyd BA,et al. Microbubble ultrasound (DCE-US) compared to DCE-MRIand DCE-CT for the assessment of vascular response tosunitinib in renal cell carcinoma (RCC). J Clin Oncol 2011;29:4627.
FDG-PET Imaging in mRCC
www.aacrjournals.org Clin Cancer Res; 17(18) September 15, 2011 5843
Cancer Research. by guest on September 4, 2020. Copyright 2011 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from