Embed Size (px)
Citation preview

Better Collaboration,
Better Care: improving
the value of CME in the
health care setting
Dave Davis, MD, FCFPSenior Director, Continuing Education & Performance Improvement
Forest Plourde-ColeResearch and Development Specialist, Continuing Education and Improvement

© 2015 AAMC. May not be reproduced without permission.
• Introduction/overview (Dave)
• Force for change in the clinical environment
• Aligning & Educating for Quality (ae4Q)
• Outputs and outcomes
• Size, scope and impact of the ae4Q community (Forest)
• Drilling Down: some case examples of change (Dave/Forest)
• Looking ahead: marrying staff & faculty development and ae4Q – Educating for Quality in the academic medical center and hospital setting
Agenda

© 2015 AAMC. May not be reproduced without permission.
Our Task: Provide Care That Is…
Safe
Effective
Efficient
Timely
Personalized
Equitable
IOM, 2002
• Better care for
patients
• Better health for
communities
• Lower cost for
both

© 2015 AAMC. May not be reproduced without permission.
..in this sort of environment
• Increasing uncertainty in the system
• Accelerating rate of change
• Shifting professional roles
• Decreasing resources; increasing expectations
• Expectations of transparency; increased workload
• Diminished joy
4
Spiegelman and Berrett, Patients Come Second, 2014.

© 2015 AAMC. May not be reproduced without permission.
Quality improvement: the patient’s perspective
The clinical care gap

© 2015 AAMC. May not be reproduced without permission.
Forces for change in the system
Aligned CE/GME/
QI/PS
Research about effective CME,
QI, implementation
Regionalization; population
health management
QI/PS initiatives
Cost transparency and sensitivity
HIT, EHR, quality dataPractice model
evolution
ACA
Alignment of clinical and academic
enterprises
ACGME/CLERACCME
Outcomes-based
education, recertification,
MOC

© 2015 AAMC. May not be reproduced without permission.
Two worldsThe “magic” happens here
ae4Q (and
Te4Q)

© 2015 AAMC. May not be reproduced without permission.
ae4q: aligning and educating for qualitythe consultative process
Alignment: Organizational Alignment of CME and GME, QI/PI initiatives, practice plans, electronic health records, faculty/staff development, credentials…
Education: Tools
• Use of quality metrics in planning and assessment
• Use of evidence based CME/CPD interventions (including HIT, team training, interactivity, other methods)
Support: On-line Resources, Community of Practice

© 2015 AAMC. May not be reproduced without permission.
• Introduction/overview (Dave)
• Force for change in the clinical environment
• What does ae4Q do?
• Outputs and outcomes (Forest)
• Size, scope and impact of the ae4Q community
• Drilling Down: some case examples of change (Dave)
• Looking ahead: marrying faculty development and ae4Q – Educating for Quality in the academic medical center and hospital setting (Forest and Dave)
Agenda

© 2015 AAMC. May not be reproduced without permission.
Outputs – Current State
In 2012, 11 pilot sites
launched
34 ae4Q sites, as of
August 2015
Across all four regions
of the USA, with four
sites in Canada
Active community that
engages through
webinars, newsletters,
and networking

© 2015 AAMC. May not be reproduced without permission.
Outputs – Our Goal
All health systems,
AMCs specifically,
have adopted the ae4Q
approach, either
through direct AAMC
engagement or
through self-direction
How do we share and
proliferate the
learnings from ae4Q
across the country?

© 2015 AAMC. May not be reproduced without permission.
Outcomes – Current State
Two surveys over the last two years have served as proxies for ae4Q outcomes
Two publications have explored ae4Q outputs and outcomes in more detail
Davis NL, Davis DA, Johnson NM, et al. Aligning Academic Continuing
Medical Education With Quality Improvement: A Model for the 21st Century.
Academic Medicine. 2013;88(10):1437-1441.

© 2015 AAMC. May not be reproduced without permission.
Outcomes – Current State
2015 survey solicited perceptions of outcomes attributable
to ae4Q intervention (n=23)
Organizational improvements cited included:
New champions or stakeholders for CME/QI alignment
and integration (60.8%)
New roles for the CME/CPD office, staff, and leadership
(78.2%)
Organizational/administrative changes or re-alignment
(34.7%)
Improvement in QI/PS culture (47.8 %)

© 2015 AAMC. May not be reproduced without permission.
Outcomes – Current State
What quality improvement activities has your institution
undertaken as a result of ae4Q?

© 2015 AAMC. May not be reproduced without permission.
Outcomes – Our Goal
How do you validate this?
Clinician behavior or practice improvement was reported in 13%
of sites and improvement in clinical outcomes was reported in
17.3% of sites.

© 2015 AAMC. May not be reproduced without permission.
• Introduction/overview (Dave)
• Force for change in the clinical environment
• What does ae4Q do?
• Outputs and outcomes
• Size, scope and impact of the ae4Q community (Forest)
• Drilling Down: some case examples of change (Dave/Forest)
• Looking ahead: marrying faculty development and ae4Q – Educating for Quality in the academic medical center and hospital setting
Agenda

© 2015 AAMC. May not be reproduced without permission.
M&M/Improvement Conferences

© 2015 AAMC. May not be reproduced without permission.
M&M/Improvement Conferences: Key Considerations
Current
• Based on a single case
• Little attention to pre-determined objectives
• Interested in finding ‘fault’
• Setting often confrontational, blaming
• No framework for discussion
• No follow-up
The M&M/Improvement Conference
• Often based on multiple similar cases
• Objectives clear: systems-based
• Open setting, avoiding blame and shame
• Provide framework for analyzing systems, e.g. Fishbone diagram
• Require follow-up

© 2015 AAMC. May not be reproduced without permission.19
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned, what will we improve)
Improvement
SYSTEM-BASED PRACTICE
(What is the Process?On whom do we depend and
who depends on us)
PROFESSIONALISM(How must we act)
INTERPERSONAL AND COMMUNICATION SKILLS
(What must we say)
MEDICAL KNOWLEDGE(What must we know)
PATIENT CARE(Overall Assessment)
Yes/No
Assessment
PATIENT-CENTERED
EQUITABLEEFFICIENTEFFECTIVETIMELYSAFEAims
Competencies
Healthcare Matrix: Care of Patient(s) with….
© 2004 Bingham, Quinn Vanderbilt University

© 2015 AAMC. May not be reproduced without permission.
Fishbone (Cause & Effect) Diagram
Why has room
turnover
time increased?
People Place
Policies Processes
Cause
WhyEFFECT
CAUSES
• Structured team brainstorming
• Represents relationship between some effect and all of the possible causes influencing it

© 2015 AAMC. May not be reproduced without permission.
Quality Grand Rounds

© 2015 AAMC. May not be reproduced without permission.
Quality Rounds
Current approach
Case presentation –resident’s case of the week, say
Review and critically appraise the evidence
Leave <25% time for Q&A
Quality Round approach
Start with a system problem
Use & present local data
Introduce QI methodology
Engage participants in discussion about how to address QI problem, >25% of the time

© 2015 AAMC. May not be reproduced without permission.
Planning:change rounds planning from this…
Isn’t ID always
the third
Tuesday?
I heard Jane XXX at a
recent meeting; she
was GREAT!
Don’t you have a friend at
Pfizer who could support
this?
Isn’t it Joe’s
turn to speak
this month?
What are we doing
here? I thought the
AA planned rounds..

© 2015 AAMC. May not be reproduced without permission.
….to thisWhat are the
clinical
problems
we’re trying to
solve here?
How do we know it’s
a problem? What do
the data show?
What are the barriers to
solving them? What about
a systems-based
approach? We’ve had
enough of the one-offs
How can we
use education
to solve it?
What types of education? How
could we deploy them? What
else could we do?

© 2015 AAMC. May not be reproduced without permission.
Embedding the Promotion of QI in Educational Activities
1. Highlight clinical areas with quality problems in a traditional educational activity
2. Explicitly add QI content to education on specific clinical topics
3. Embed educational activities in larger QI initiatives; use quality metrics to plan and assess learning activities
4. Supplement education with post-event deliverables
Ann Intern Med 2012;156:305

© 2015 AAMC. May not be reproduced without permission.
System-wide changes

© 2015 AAMC. May not be reproduced without permission.
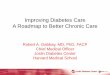
Outcomes – Our Goal
The 2013 publication, Reduction of
Venous Thromboembolism (VTE) in
Hospitalized Patients: Aligning
Continuing Education With
Interprofessional Team-Based
Quality Improvement in an Academic
Medical Center, concluded that
aligning continuing education
with quality improvement through
an interprofessional,
multidisciplinary team approach
was associated with a decrease in
VTE.

© 2015 AAMC. May not be reproduced without permission.
Outcomes – Our Goal
Committee constructed of
quality experts, clinicians and
CME office
Investigated charts to determine
where to focus intervention
(80/20 rule applied)
Used Pathman/PRECEDE model
to deliver educational
intervention
VTE rates dropped from 12.68
per 1,000 patients in December
2010 to 6.10 per 1,000 patients

© 2015 AAMC. May not be reproduced without permission.
• Introduction/overview (Dave)
• Force for change in the clinical environment
• What does ae4Q do?
• Outputs and outcomes
• Size, scope and impact of the ae4Q community (Forest)
• Drilling Down: some case examples of change
• Looking ahead: marrying staff & faculty development and ae4Q in the academic medical center and hospital setting (Forest and Dave)
Agenda

© 2015 AAMC. May not be reproduced without permission.
Aligning Education with Quality
Ann Intern Med 2012;156:305

© 2015 AAMC. May not be reproduced without permission.
Consultative
engagement to
align education
enterprise
(UME, GME,
CME) with
health system
and patient care
needs
Development of
customized
initiatives and
organizational
changes to
leverage
education to
support QI work
OPTION 2:
Delivery of
Te4Q Faculty
Development
Program Part 1
to train clinical
faculty in QI
basics
Continued
support to
implement
recommendation
s from initial
consultation
Delivery of
TE4Q
workshop,
training faulty
how to teach
QI across the
educational
continuum
Aligning Educational and
Clinical Elements
OPTION 1:
Basic
quality/safety
training for
faculty, site-
driven
Delivery of Quality and Safety Training Across the System
The Educating for Quality suite of services

©Website: www.aamc.org/ae4qEmails:
[email protected]@[email protected]@aamc.org
Karyn Baum, MD, MEd, senior consultant, Quality Educational Initiatives, AAMC
Professor of Medicine, University of Minnesota