Embed Size (px)
DESCRIPTION
An Enhanced Video for Adults With Low Vision: Impact on Knowledge, Attitudes and the Use of Assistive Devices. Beth Dugan, Ph.D. The Institute for Studies on Aging New England Research Institutes 9 Galen Street Watertown, MA 02472 USA (617) 923-7747 ext 210 [email protected]. - PowerPoint PPT Presentation
Citation preview

An Enhanced Video for Adults With Low An Enhanced Video for Adults With Low Vision: Impact on Knowledge, Attitudes andVision: Impact on Knowledge, Attitudes and
the Use of Assistive Devicesthe Use of Assistive Devices
Beth Dugan, Ph.D.The Institute for Studies on AgingNew England Research Institutes
9 Galen StreetWatertown, MA 02472 USA(617) 923-7747 ext 210

AcknowledgementAcknowledgement
Research supported by the National Eye Institute (EY012443).

Project TeamProject Team
Sharon Tennstedt, PhD, InvestigatorEli Peli, OD, Co-InvestigatorRobert Goldstein, PhD, Co-InvestigatorFelicia Trachtenberg, PhD, BiostatisticianSteve Braun, BA, ProducerNancy Gee, BA, Data ManagerKristina Richards, BA, Field Supervisor

OutlineOutline
• Low Vision• Patient education• Content of the video• Evaluation study• Implications

Low Vision DefinitionLow Vision Definition
A visual impairment, not correctable by standard glasses, contact lenses, medicine, or surgery, that interferes with a person's ability to perform everyday activities.
Age-related macular degeneration (AMD) accounts for approximately one-half of all cases of low vision. There are two types of AMD, wet and dry type accounting for 10% and 90% of cases respectively.

Low VisionLow Vision
In the US approximately 3-5 million adults have low vision.
Annual total costs exceed $22 billion on care and services for people who are blind or have visual impairments. (National Alliance for Eye and Vision Research, 1995.)

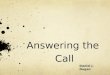
Living With Central Vision Living With Central Vision LossLoss
Normal W/ Low Vision

Why Patient Education?Why Patient Education?
During the often rushed clinical encounter when a person first gets the diagnosis – they may be so overwhelmed that they only hear
“legally blind” or “no known cure”…
….which may lead the person to stop visiting an eye care professional altogether.

Why Patient Education?Why Patient Education?
• believe it is a natural part of aging• not aware of treatment options or how
to access help• believe services are only for the blind,
not those with central vision loss• cost

????
A video for the A video for the visually impairedvisually impaired
????

• Low vision is a loss of central vision, not total blindness.
• Most Americans have access to a television and many have access to a VCR.
• The video is informative for family members as well.
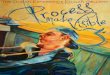
• Peli and colleagues have pioneered the use of computerized image enhancement to improve the visibility of the video images for low vision patients.

This figure shows the difference between the enhanced (on the right) and original unenhanced version (on the left). The actual video only presented the enhanced images.

The anatomy and basic pathology of AMD were illustrated – and showed the location and nature of changes that occur with macular degeneration.


The virtual home animation included environmental adaptations and use of visual aids. Changes were depicted for the kitchen, bathroom, bedroom, and living room.

Hope in SightHope in Sight Video Video
• Winner, 24th Annual Telly Award; 2003
• Finalist, International Health & Medical Media Awards, Health Education; 2003. (Freddie Award)

Research QuestionsResearch Questions
1. Will the video intervention increase patient knowledge and improve attitudes?
2. Will the video intervention have a positive impact on adaptive behavior?

Evaluation PlanEvaluation Plan
Proximal Outcomes:• Knowledge (eye anatomy and physiology;
types of rehab devices; resources).• Self-efficacy, emotional responses.• Willingness to use low vision aids.
Distal Outcomes• Behavior change (use assistive devices;
environmental changes; rehab svc).

Eligibility:Eligibility:
Speak and understand English. Be diagnosed with low vision in both eyes. Not limited by hearing impairment (able to hear
a video). Access to a VCR and telephone.

Sample description (N=151)Sample description (N=151)Gender Male Female
5497
36%64%
Race White All others
1465
97%3%
Years ARMD diagnosed (median) 4.0 8.23 (sd)
Live Alone2 person household3 or more person household
28117
6
19%78%3%

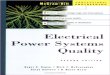
Subject Pool
Informed consent and enrollment
T0 Interview (N=156)
T1 Interview at 2 weeks (n=75)
T1 Interview at 2 weeks (n=79)
T2 Interview at 3 mo. (n=74)
T2 Interview at 3 months (n=77)
Randomization
Watch the Video
Intervention Group
Control Group
Video

MeasurementMeasurement
A. Demographics.B. Knowledge (eye anatomy, physiology,
pathology of macular degeneration).C. Assistive devices (knowledge of,
access to, attitude toward).D. Adaptive changes (home, lifestyle)E. Self-efficacyF. Social aspects of low visionG. Emotions re: low vision

HypothesesHypotheses
Compared to the control group, the intervention group will show greater improvement in:
• Knowledge
• Attitudes (emotions; self-efficacy)
• Behavioral changes (use of assistive devices, adaptive changes in the home).

Statistical AnalysesStatistical Analyses
Analysis of covariance (ANCOVA) was used to determine differences by treatment group.

CovariatesCovariates
We controlled for baseline values and covariates: age gender marital status education length of vision impairment # people in household employment health

ResultsResults
Descriptive statistics showed that the intervention and control group were equivalent with respect to all key baseline characteristics.

KnowledgeKnowledge
The intervention group improved more in knowledge than the control group;
p <.001, Adj R2 = 0.39
Magnitude of Change? Control group 0.4 pts vs Video group 1.4
pts. (approx one question difference)

KnowledgeKnowledge
• People who lived alone learned more (~never married, older age);
• those who had worse health learned less);

AttitudesAttitudes
The intervention group improved more than the control group in their willingness to use assistive devices
Books-on-tape (those who lived alone were especially willing to use books on tape);
p<.001, Adj R2 = 0.53; Talking appliances (no significant covariates) p<.001, Adj R2 = 0.38;

EmotionsEmotionsThe intervention group had a decline in
reported fear and sadness than the control group.
Less afraid (people in better health became less afraid, people in poor health showed no improvement in fear)
p<.001, Adj R2 = 0.34;
Less sad (age and gender trends) p<.001, Adj R2 = 0.28;

Self-efficacySelf-efficacy
No difference between groups.

BehaviorBehavior
No difference between groups in adaptive changes in the home, or actual use of assistive devices.

ConclusionsConclusions
The video had an impact on our proximal but not the distal outcome measures.

ConclusionsConclusions
The video was effective in:
• improving knowledge
• Improving a few attitudes (willingness to use books on tape, and talking appliances)
• Improving the emotional aspects of low vision (reducing fear, reducing sadness).

ConclusionsConclusions
The video was not effective in:• Improving self-efficacy• Changing the actual use of assistive
devices or rehabilitation services.

LimitationsLimitations
1. Relied on self-report data.
2. Three-month timeframe. It may take as long as 3 months to make an appointment with a low vision specialist and even longer to obtain devices.
3. The recruitment strategy and inclusion criteria limited the diversity of the sample, which limits the generalizability of the results.

Future ResearchFuture Research
1. Will the distal outcomes (e.g., increase the use of assistive devices; increase the use of rehabilitation services) change if allowed more time?
2. If not, what intervention is needed to increase the use of assistive devices and rehabilitative services?