Embed Size (px)
Citation preview

COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
Cost & Quality Academy
Best Practices in Patient Care ExperienceCOMMUNITY INSIGHTS FOR DRIVING PATIENT EDUCATION, ENGAGEMENT, AND SATISFACTION

3COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
Note to Members of The AcademyThis report is based on publicly available information as well as financial and other information provided to or represented to the Cost & Quality Academy (“The Academy”) from numerous sources which are generally deemed reliable. While The Academy believes the information is both accurate and complete, The Academy does not represent this information as such.
The Academy does not provide organizations with legal, clinical, or other professional advice, and this report should not be regarded as such under any circumstances. The Academy has not been requested to opine as to, and does not guarantee, warrant or opine upon: (i) any organization’s underlying business decision to proceed (or not to proceed) with any business transaction; or (ii) the failure of any business transaction to perform in any particular manner. Any opinion expressed in this report shall not amount to any form of guarantee that The Academy has determined or predicted future events or circumstances, and no such reliance may be inferred or implied.
This report has been developed by The Academy for exclusive use by its Members and contains proprietary information belonging to The Academy. Therefore, without the express consent of The Academy, Members are expected to maintain the information provided in strictest confidence; not disclose this report, or any part of it, to third parties; and not use The Academy’s name in any promotion, prospectus or other document available to third parties. Notwithstanding the foregoing, The Academy shall not be liable to, nor shall there be any reliance on the report by, any Member, organization, or third party.
If you do not agree with this obligation, please immediately return this report to The Academy.
Additional copies of the report are available for members. Please contact The Academy at 888.700.5223 to obtain as many as you need.
With the significant percentage of the Hospital Value-Based Purchasing Program that is and will be devoted to the patient and caregiver experience of care, many organizations are striving to identify the best opportunities to improve this measure. Beyond regulatory compliance, the benefits of bolstering patient experience are wide ranging and can include better patient outcomes, more engaged patients, and happier, more engaged healthcare staff. Nonetheless, even with these reasons, the patient care experience is often not as robust and superlative as it could be. Patients may not understand the education being provided to them, may not feel that the hospital or health system cares for their opinion or involvement in their care, and may not find the experience satisfying.
In response, the Cost & Quality Academy has identified, reviewed, and analyzed the practices of hundreds of organizations over the last year, gathering within this report case studies, implementation tools, and data that highlight the practices of better performing organizations within the membership community to help you and your organization maximize the patient and caregiver-centered experience of care.
Table of Contents
Case Studies .......................................................................................................................................................................................... 5
1. Creating Improved Patient Education Practices and Opportunities ............................................... 9
2. Promoting a Highly Engaged Atmosphere for Patients ......................................................................... 19
3. Reducing Stressors and Miscommunication to Bolster Patient Satisfaction ........................ 29
Academy Communities ............................................................................................................................................................. 39
About This ReportBest Practices in Patient Care Experience

5
Best Practices in Patient Care ExperienceCASE STUDIES

6 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
Understanding Statements of Work PagesCase Studies
Following conversations with HBI members and a desire to present the most impactful information in the most efficient way, The Academy has adapted the introduction of each practice within this report to reflect the type of statements of work that are often utilized to build consensus and the case for changing processes as a means to improve cost, operational efficiency, and quality. Below is a visual guide for interpreting these pages in the report.
11COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ADisease-Specific Education
BReducing Stigma of Mental Illness
CStandardizing Curriculum
Scope Statement
Newly diagnosed cancer patients without adequate support can feel overwhelmed and underprepared for treatment
The stigma surrounding mental illness often discourages individuals from seeking necessary treatment
Inconsistent messages from providers can leave oncology patients feeling confused about next steps
Peer Best Practice
Utilize nurse navigators at the front end of the diagnosis to ensure health literacy and engagement
Apply structured programs to improve communication and educate patients, staff, and community on mental health
Standardize the oncology education curriculum to provide a consistent message to patients from all staff
Typical Approach
Nurse navigators often provide generalized support intermittently throughout care but do not offer disease-specific education
Many organizations implement mental health programs, but do not address challenges to delivering better care experience to such patients
Departments typically have their own processes and procedures that are not necessarily communicated to other departments, leaving education fragmented
Business Case
Educating patients immediately following diagnosis with disease-specific resources can promote patient appointment compliance and care engagement
Patients treated respectfully will enjoy a better experience, which can drive related score improvement and reduce compassion fatigue among staff
Offering collaborative approaches to oncology education can increase patient satisfaction and ultimately bolster patient outcomes
Stakeholder Alignment
Physicians, Nurse Leaders, Nurse Navigators
Nurses, Nurse Practitioners, Physicians, Counselors, Therapists
Educators, Oncology Physicians, Clinical Leaders, Nurses
Intended Outcomes
Tailoring education based on diagnosis increases program usage and satisfaction
Increased communication through TLC4 model reduces stigmatizing language and attitudes among patients and providers
Standardizing educational materials ensures oncology patients have the best opportunities to participate in their care
Statements of WorkPractice 1: Creating Improved Patient Education Practices and Opportunities
% of Medical Information Not Retained During an Office Visit
Source: Agency for Healthcare Research and Quality (2015)
Perceived General Public Attitudes Among Americans Toward People with Mental Illness
Source: CDC (2010)
of the medical information patients are told during an office visit is forgotten
Industry Trends Supporting the Need for Improvement
With the rising importance of the patient experience, a wide majority of individuals perceiving indifference to their mental illness in general provides an opportunity for care providers to rise above the norm and consistently show empathy
Perceived Sympathy
24.6%
Perceived Indifference
75.4%
At least 40% of information conveyed to patients during an office visit is not retained—and nearly half of the information patients do retain is incorrect—underscoring a need for effective teach-back strategies
40–80%
Data that emphasizes existing trends, and in some cases, challenges the “Peer Best Practices” aim to overcome
Each row corresponds to one of the case studies that can be found in more detail on the following pages
Describes a featured organization’s best practice
Defines, in most cases, a historically common practice
Summarizes the high-level improvements that may be seen as a result of the “Peer Best Practice”
Identifies roles that are integral to the best practice’s success
Provides a brief overview of the situation in the healthcare industry that drives need for improvement
Summarizes positive results experienced by the featured organization using the “Peer Best Practice”

7COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
Below is a visual guide for interpreting the following pages.
Understanding Case Study PagesCase Studies
The left-hand side of each case study explores either a common challenge currently facing healthcare organizations or an emerging trend, along with related data regarding nationwide performance of a certain metric or prevalence of a specific practice
At the top of each case study page, three highlights are listed to emphasize the key considerations or strategies realized by the organization as integral to success
Each two-page spread that follows features a case study example of an organization that succeeded in employing a best practice or garnering significant improvements in overall performance, patient experience, etc.
Illustrations quantify the organization’s improvement, show an analysis conducted by the organization, or provide further insight with respect to the practice employed
Each two-page spread closes by noting where additional information on the topic can be obtained via The Academy’s members-only web portal
16 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Children’s Hospital & Medical Center, a 145-bed non-profit organization in Omaha, Nebraska, includes an oncology continuum of care that consists of an ambulatory clinic, infusion center, inpatient unit, and home healthcare—viewed by staff as separate areas with their own processes, but seen by patients and families as one collective oncology service line
• To address inconsistencies across the continuum of care, nursing leadership implemented a performance improvement project, beginning with Lean principles, PDSA methodologies, and an oncology staff survey; results of this survey signified that only 39% of staff were confident in their role in the oncology educational process, while only 37% were aware of the available educational resources
• Given this evidence, an interdisciplinary team was formed to assess current educational resources and processes, and perform a comprehensive analysis to identify gaps and inconsistencies; patient and family feedback was additionally instrumental in developing the new diagnosis educational materials and processes
• In order to ensure that patients and families receive a consistent message, that could be provided at the patient’s own pace and customized to their learning style, the organization hired a dedicated oncology educator who was trained in the teach-back method and given responsibility for maintaining each educational document’s ongoing relevance
• Education materials were made available through the organization’s intranet site as well as to patients, families, and primary care providers via their online health portal
Standardizing Curriculum for Newly Diagnosed PatientsPractice 1: Creating Improved Patient Education Practices and Opportunities
Business ChallengeOncology-Specific Education Remains Relative to Individual Staff ExperienceAs newly diagnosed oncology patients begin treatment, they expect to receive a consistent message and a standardized approach to education from oncology staff. This consistency is especially crucial for pediatric patients, as the care required can be particularly complex. Strong communication and collaboration between clinicians is required to provide a standardized approach but may pose a challenge. Additionally, variances between the teaching style of clinicians can also lead to patient confusion and a further lack of compliance for the prescribed treatment.
Without a standardized educational curriculum to ensure patient needs are being met and that the organizational message remains consistent among all departments, patient safety and outcomes can be compromised. In an effort to improve the quality of care for oncology patients and to provide a consistent message across the care continuum, bridging this gap will be necessary.
% of Oncology Staff Who Understood Their Organization’s Educational Process at Children’s
Hospital & Medical Center
Less than half of the oncology staff surveyed felt they fully understood Children’s Hospital’s educational curriculum in addition to knowing their role in teaching newly diagnosed patients
Developing a curriculum across the continuum boosts consistency
Standardizing the delivery of education enhances patient understanding
Appointing a dedicated oncology educator ensures resource relevancy High
light
s
39%
Improvement to Staff Familiarity with Oncology Resources and Educational Process at Children’s Hospital & Medical Center
Pre-Implementation Post-Implementation
37%
67%
39%
74%
Resources Process
17COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: “Following Chemotherapy” Caregiver Educational Handout Chemotherapy can cause a variety of side effects among children, such as nausea, vomiting, and fatigue—symptoms that usually reflect illness and can drive considerable concern. To ensure that patients and their caregivers leave a chemotherapy treatment with understanding of their care at Children’s Hospital & Medical Center, caregivers are given an educational handout. This document describes how to carefully dispose of clothing or bedding that comes into contact with the child’s bodily fluids, food preparation, sun protection, and nail care, among other suggestions.
For additional insight on how other organizations have improved the care experience of oncology patients, download The Academy’s white paper, “Expanding Survivorship Care with Persistent Follow-Up and Individualized Treatment,” from the Analyst Advisory page of the members-only web portal
Excerpt from Children’s Hospital & Medical Center’s Caregiver Educational Handout
Disclaimer: This document is not intended to be a substitute for, nor does it constitute, professional medical advice. Always seek the advice of a physician or other qualified health provider with any questions you may have regarding a medical condition. Do not delay seeking professional medical advice due to something you have read in this document.
Copyright © 2016 by Children’s Hospital & Medical Center
Returning to School Going to school is an important part of helping your child feel “normal.” We can help to ease the transition for children returning to school. Timing for when your child can return to school will be based on their diagnosis and type of treatment. In general, your child should have an ANC >500 to return to school. There may be times throughout therapy in which we anticipate your child’s counts to be dropping. During those times we may decide it would be best to keep your child home from school. This can be discussed with your provider. Fertility
The radiation and chemotherapy that are used to treat cancer can sometimes cause problems with your child’s ability to get pregnant or make someone pregnant, also known as fertility. You can talk with your health care team about how likely it is for their treatment to affect fertility. They may be able to offer some options for fertility preservation or ways to make it more likely for your child to have a baby in the future.
Caring for Your Child
Disclaimer: This document is not intended to be a substitute for, nor does it constitute, professional medical advice. Always seek the advice of a physician or other qualified health provider with any questions you may have regarding a medical condition. Do not delay seeking professional medical advice due to something you have read in this document.
Copyright © 2016 by Children’s Hospital & Medical Center
Bodily Fluids
Chemotherapy drugs can come out of your child’s body fluids (urine, stool, vomit and semen). Family members should always wear gloves before coming into contact with your child’s body fluids for at least 48 hours after the chemotherapy has been given. If your child accidentally soils clothing or bedding with any body fluids within 48 hours of receiving chemotherapy, wash the soiled laundry twice in hot water separately from other laundry. When you are at home, flush the toilet twice with the lid down after your child uses the restroom during the 48 hours after receiving chemotherapy. If your child wears diapers, double-bag the soiled diapers and dispose of them immediately. Nail Care
Your child’s fingernails and toe nails should be kept trimmed by using nail clippers, an emery board or cuticle scissors. Discourage nail biting and thumb sucking as they both can be a source of infection. Never let your child tear nails or hang nails.
Sun Protection Chemotherapy will make your child’s skin extremely sensitive to sun. To avoid sunburn, your child should wear sunscreen and a hat year-round and limit the amount of time s/he spends in direct sunlight. Food Preparation
You usually will not need to make any major changes in your child’s diet during therapy. It is recommended to avoid unnecessary exposure to bacteria in foods while your child’s immune system is suppressed. This includes avoiding raw or undercooked meat, unpasteurized dairy products, raw honey and uncooked Brewer’s yeast. In addition, wash all fruits and vegetables thoroughly and avoid any expired food or any food with visible mold. Most milk and yogurt, as well as some cheeses, are pasteurized and are safe to eat.
Caring for Your Child This introductory paragraph explains each process aid in more detail as well as how it was leveraged by the featured organization—or capacities in which it could be utilized effectively by other providers
The second page of each two-page spread displays a process aid that, in most cases, was utilized by the organization featured—or a related tool developed by The Academy may also be included

9
Best Practices in Patient Care ExperienceCREATING IMPROVED PATIENT EDUCATION PRACTICES AND OPPORTUNITIES

10 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
Around the nation, many hospitals and health systems are experiencing shifting patient volumes, whether in terms of a net increase of census or flux across types of services most heavily utilized. In each of these cases—and any other care situation—the knowledge of the patient has a distinct, often significant impact on the eventual outcomes of any health services offered. Studies have shown limited health literacy to be associated with an increase in preventable hospital admissions and 30-day readmissions. Lack of patient education in healthcare can also have a negative psychological effect on patients, particularly in patient populations with an associated cultural and social stigma, such as those managing mental illness.
Providing such patients with resources, such as peer-to-peer storytelling, can promote increased communication and education, while destigmatizing mental health conditions among patients and staff. Additionally, employing these tactics among staff members can promote effective communication between patients and providers by prioritizing welcoming language and reducing the occurrence of compassion fatigue.
The challenges of effective patient education are further exacerbated for patients with a chronic disease. For example, patients who receive a cancer diagnosis often feel confused about their next steps and available choices. Depending on diagnosis and treatment options, they could be choosing between radiation, chemotherapy, surgery, or another avenue—each of which comes with its own emotional, mental, physical, and financial costs. When combined with the preexisting responsibilities of each patient’s life outside of their new diagnosis, comprehending and balancing such choices and treatments can be more than many can handle without help.
Offering a standardized education curriculum from specially trained staff can ensure that these patients are receiving consistent information regarding their condition and what to expect during treatment. Furthermore, appointing a designated oncology educator who utilizes teach-back methods can promote a consistent point of contact and ensure effective communication and understanding for patients and families. Ultimately, appropriate education provides patients with the tools to understand the care they have received, the requirements expected of them going forward, and their experience of care as a whole.
IntroductionPractice 1: Creating Improved Patient Education Practices and Opportunities
Average % of Patient Visits in Hospital Outpatient Department in Which Health Education Was
Provided to Patient, by Provider TypeSource: Ritsema TS et al. (2014)
% of Total Population Projected to Be Diagnosed with Cancer at
Some Point During Their LifetimeSource: National Cancer Institute (2012)
With nearly four of every 10 Americans projected to be diagnosed with cancer in their lifetime, the value of effective education in helping these individuals manage their care cannot be understated
With distinct differences dependent on the type of provider involved when it comes to patient education, standardizing roles for education and specially training the staff involved could have considerable positive impact and improve overall efficiency
20.2%
Physician Physician Assistant
Nurse Practitioner
31.0%28.6%
39.6%

11COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ADisease-Specific Education
BReducing Stigma of Mental Illness
CStandardizing Curriculum
Scope Statement
Newly diagnosed cancer patients without adequate support can feel overwhelmed and underprepared for treatment
The stigma surrounding mental illness often discourages individuals from seeking necessary treatment
Inconsistent messages from providers can leave oncology patients feeling confused about next steps
Peer Best Practice
Utilize nurse navigators at the front end of the diagnosis to ensure health literacy and engagement
Apply structured programs to improve communication and educate patients, staff, and community on mental health
Standardize the oncology education curriculum to provide a consistent message to patients from all staff
Typical Approach
Nurse navigators often provide generalized support intermittently throughout care but do not offer disease-specific education
Many organizations implement mental health programs, but do not address challenges to delivering better care experience to such patients
Departments typically have their own processes and procedures that are not necessarily communicated to other departments, leaving education fragmented
Business Case
Educating patients immediately following diagnosis with disease-specific resources can promote patient appointment compliance and care engagement
Patients treated respectfully will enjoy a better experience, which can drive related score improvement and reduce compassion fatigue among staff
Offering collaborative approaches to oncology education can increase patient satisfaction and ultimately bolster patient outcomes
Stakeholder Alignment
Physicians, Nurse Leaders, Nurse Navigators
Nurses, Nurse Practitioners, Physicians, Counselors, Therapists
Educators, Oncology Physicians, Clinical Leaders, Nurses
Intended Outcomes
Tailoring education based on diagnosis increases program usage and satisfaction
Increased communication through TLC4 model reduces stigmatizing language and attitudes among patients and providers
Standardizing educational materials ensures oncology patients have the best opportunities to participate in their care
Statements of WorkPractice 1: Creating Improved Patient Education Practices and Opportunities
% of Medical Information Not Retained During an Office Visit
Source: Agency for Healthcare Research and Quality (2015)
Perceived General Public Attitudes Among Americans Toward People with Mental Illness
Source: CDC (2010)
of the medical information patients are told during an office visit is forgotten
Industry Trends Supporting the Need for Improvement
With the rising importance of the patient experience, a wide majority of individuals perceiving indifference to their mental illness in general provides an opportunity for care providers to rise above the norm and consistently show empathy
Perceived Sympathy
24.6%
Perceived Indifference
75.4%
At least 40% of information conveyed to patients during an office visit is not retained—and nearly half of the information patients do retain is incorrect—underscoring a need for effective teach-back strategies
40–80%

12 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• At Poudre Valley Hospital (PVH), a 270-bed regional medical center that is part of the University of Colorado Health System, navigation support is emphasized at the front end of cancer care, following patients from diagnosis through treatment to ensure that their patients are able to make informed health decisions regarding the future treatment plan
• After initially offering navigation for patients who might need additional financial and community resources, PVH streamlined these services to a disease-specific level for enhanced education assistance
• As part of this process, nurse navigators frontload each patient with education and support resources specific to the diagnosis; patients therefore feel confident and have a clearer understanding of the treatment while providers convey positive feedback regarding the nurse navigator’s educational responsibilities
• Each week, a nurse navigator may see between five and eight new patients, but will have closer to 30 to 40 patients who are waiting—potentially up to a few months—for treatment for whom the navigator will progress and monitor medication therapies, as well as potential future treatment options
• Apart from one-on-one therapy services, nurse navigators may additionally provide resources in a group setting for further support opportunities; as a result of the wide range of services the nurse navigators provide, Poudre Valley experienced over double patient participation between 2012 and 2015; with fewer than 900 in 2012 increasing to over 2,000 patients by 2015, highlighting the organization’s efforts in providing quality care across the oncology spectrum
Utilizing Disease-Specific Education and SupportPractice 1: Creating Improved Patient Education Practices and Opportunities
Business ChallengeLack of Support Resources at Diagnosis Breeds Undereducation As more individuals are newly diagnosed with cancer, patient education resources to address the anxiety associated with that diagnosis often remain inconsistent across many hospitals and health systems. Often, a lack of designated staff to address these concerns contributes to greater patient misunderstanding. Treatment appointments between patients and physicians are therefore utilized as a venue to answer questions, connect to community resources, and address financial concerns, rather than focus on treatment itself.
Nurse navigators frequently used at some organizations to facilitate the care of these patients are able to provide general educational support but may lack disease-specific education. Without adequate support systems in place, oncology patients are less informed about their care plan, commonly overwhelmed with balancing traditional activities and new needs related to their condition, and often unable to fully engage in their treatment.
Estimated Number of Individuals with New Cancer
Diagnoses in the U.S. AnnuallySource: American Cancer Society (2016)
With more cancer diagnoses projected each year, education to support this growing population remains critical
Offer education at a disease-specific level to increase understanding
Meeting patients early can free time to discuss treatment options
Monitoring progress between visits ensures patient needs are metHigh
light
s
2012 2016
1,638,910 1,685,210
Number of Oncology Patients Treated Utilizing Disease-Specific Education at Poudre Valley Hospital
By offering nurse navigation support for oncology patients with built-in disease-focused education, Poudre Valley has experienced considerable program growth and commensurate positive patient feedback
2,000
<900
20152012

13COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Oncology Nurse Navigator Job DescriptionPoudre Valley Hospital’s emphasis on navigation support at the front end of cancer care is successful through the role of a nurse navigator. Nurse navigators provide disease-specific education while guiding patients from diagnosis through treatment, offering community resources, assessing financial stability and at-home support, and ensuring transportation needs are met. To encourage the recruitment and use of this position, The Academy has reviewed several job descriptions for the role and created this sample description based on common needs and requirements between those descriptions.
For further details on Poudre Valley Hospital’s disease-specific oncology education efforts, download The Academy’s white paper, “Improving Front-End Care Processes with Nurse Navigators Through Disease-Specific Education and Support,” from the Analyst Advisory page of the members-only web portal
Excerpt from The Academy’s Oncology Nurse Navigator Job Description
Cost & Quality Academy
Copyright © Decision Resources, Inc. All Rights Reserved.
Oncology Nurse Navigator Job Description
Position Summary As the primary point of contact for oncology patients, the oncology nurse navigator is responsible for guiding the patient through each facet of the care continuum, while integrating community resources to address the needs of the patient. The oncology nurse navigator monitors patients throughout their treatment and assists in facilitating their care, additionally providing thorough educational materials and services based on a particular condition and overall patient needs.
Roles and Responsibilities • Identify patient financial, transportation, educational, and at-home care needs and provide support as
necessary
• Build awareness surrounding a disease-specific diagnosis through educational resources, both written and verbal
• Coordinate a defined care plan which outlines goals for managing the patient’s condition
• Collaborate with the patient’s multidisciplinary care team to ensure all needs are met
The above statements reflect the general duties considered necessary to describe the principal functions of the job as identified and should not be considered a detailed description of all the work requirements that may be inherent to the position.
Position Qualifications Education - Bachelor of Science degree in Nursing
Licenses - Current RN license to practice in the State of [State] required
Experience - Previous case management experience preferred - At least two years of clinical experience required
Knowledge, Skills, and Abilities - Strong communication skills, both written and verbal - Understanding of available oncology community resources - Proficient computer and telephone skills

14 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Rogers Behavioral Health System, comprised of 10 locations throughout the nation, created the Rogers InHealth program, which works to decrease the stigma surrounding individuals working through mental illness, as a means of enhancing care quality
• Rogers InHealth implemented the TLC4 model, an acronym for targeted, local, credible, continuous, and change-focused contact; the model evolved under the collaboration of other behavioral health community partners via a coalition as well as an academic researcher at the Illinois Institute of Technology
• Specifically, this evidence-based model works to decrease stereotypes, prejudices, and discrimination surrounding mental health by engaging providers and patients with individuals living in recovery with a mental health challenge; through the relationships that develop via these engagements, assumptions and suppositions can be broken down, with considerable benefit to empathy and compassion as a result
Storytelling to Reduce the Stigma of Mental IllnessPractice 1: Creating Improved Patient Education Practices and Opportunities
• With compassion fatigue acting as an all-too-prevalent threat in the industry, the TLC4 model additionally supports staff in fatigue relief by providing a safe space to share personal recovery stories; via practitioners willing to relate a personal experience of mental illness recovery to their peers, illusions of difference or barriers of understanding can be broken down, building personal experience and relieving tension, discomfort, or fear
• Through these efforts, Rogers Behavioral Health System has reduced the stigma surrounding mental illness through improved communication and education and created an inclusive environment for patients overcoming mental illness by incorporating the principles of the TLC4 model and offering resources for storytelling
“We so often talk about the signs and symptoms of mental illness, and we don’t often talk about the hope of recovery. We raise up those stories to demonstrate that people with mental health challenges are good, are able.”
– Suzette Urbashich, Co-Director of Rogers InHealth,
Rogers Behavioral Health System
Business ChallengeInconsistent Communication Results in Stigma Surrounding Mental IllnessAccording to the National Institute of Mental Health, depression, bipolar disorder, and dysthymic disorder together represent the third most common cause of hospitalization in the U.S., demanding the need for approachable, accessible, and respectful treatment options. Unfortunately, stigma toward these individuals and others with mental health challenges all too often interferes with creating a positive patient experience. Stigma can take many forms both overt and accidental, but the impact on patients cannot be understated. In response, a few organizations have structured programs that initiate a positive conversation with patients and the community about mental health to build shared understanding and empathy.
Efforts to improve the care of these patients can sometimes, unintentionally, play into the same misconceptions that drive stigma, and providers who mean well may find long-standing words and phrases to have a negative connotation, risking the well-being of patients in the process.
% of American Adults Experiencing Mental IllnessSource: National Institute of Mental
Health (2014)
Approximately 1 in 5 adults, or 43.8 million, experience mental illness in any given year; underscoring a need for decreased stigma and improved patient and provider education
Emphasizing peer-to-peer contact ensures patients feel understood
Educating staff on mental illness can minimize stigma
Collaboration among staff builds awareness of compassion fatigueHigh
light
s
18.5%
Through peer-to-peer storytelling, Rogers Behavioral Health System is able to destigmatize mental illness and instill hope for recovery among patients

15COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Tip Sheet to Reduce Stigmatizing LanguageOften, corrective efforts for staff—even when out of a preventive or positive spirit—can be accompanied by feelings, intended or otherwise, of blame or shame. To bolster efforts to destigmatize mental illness in the care setting through education and awareness, Rogers Behavioral Health System additionally provides a list of suggested techniques to reduce stigma while avoiding judgement. Utilizing the techniques listed within this document can be used to hold other individuals accountable to their own words and actions while also encouraging those with a mental illness to share their own stories of recovery.
For more information on Rogers Behavioral Health System’s efforts to destigmatize mental illness in the healthcare setting, download The Academy’s white paper, “Using Peer-to-Peer Storytelling and a Targeted Model to Reduce the Stigma of Mental Illness in the Hospital Setting,” from the Analyst Advisory page of the members-only web portal
Excerpt from Rogers Behavioral Health System’s Tip Sheet on “Culturally Sensitive Responses to Challenge Stigmatizing Language”
Culturally Sensitive Responses to Challenge Stigmatizing Language
General Tips:
1. Avoid value judgments (i.e. “that’s a terrible thing to say”; “you don’t know what you are talking about”)
2. The response depends on the relationship and level of trust you’ve built with a person. 3. The goal is to start a meaningful dialogue and conversation. We don’t want to be thought of
as “language police”. 4. Use creative language. 5. Use humor. 6. Share recovery stories to counter myths. 7. Assume positive intent. 8. Tone makes a difference. Approach with compassion and curiosity. 9. Ask for what you need.
Teach and Learn:
1. Re-frame what is said; offer language options. “I’m learning that people usually prefer person-first language, such as ‘a person living with bipolar disorder’.”
2. Gently suggest person-first language. “I dealt with challenges from anorexia, I’m not ‘an anorexic’. I don’t like to define myself by my past with an eating disorder.”
3. Normalize it. Say, “Everyone has a certain level of dysfunction.” 4. Ask others to help hold you accountable for your own language use to model openness to
growth. “You’ve told me it bothers you when people say ___________. If I slip up, will you hold me accountable? I want to respect your wishes.”
5. Be curious. “What about your experience makes you say that?” or, “Can you help me understand what you mean by that?” Or genuinely inquire about a person’s familiarity with mental health issues. “How much do you know about mental health?”
6. Talk about your own feelings and perspective in response to the comment. “I’m feeling uncomfortable as a result of you saying __________.” Or start with, “Well, in my experience…”
7. Name it, claim it, tame it. For example, someone says, “Crazy people should be locked up and not left to wander the streets.” Response: “You may not know this, but you’re talking about me. I have schizophrenia.”
8. Deflect their words. For example, if someone calls you crazy, say, “I’m good with that.” 9. When someone makes a stigmatizing generalization like: “Borderlines sure are crazy”,
respond with compassion to elicit empathy, for example. “I wonder how traumatic her background was” or “I wonder what it’s like to face that challenge.”
10. Let people know how their words and actions make you feel. For example, “That felt a little harsh.” Then ask for what you need. “Can I ask you to be a little more sensitive?”
11. Share your preference for using or not using labels. “You know, I don’t like to use labels to talk about my experience with mental health challenges.”

16 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Children’s Hospital & Medical Center, a 145-bed non-profit organization in Omaha, Nebraska, includes an oncology continuum of care that consists of an ambulatory clinic, infusion center, inpatient unit, and home healthcare—viewed by staff as separate areas with their own processes, but seen by patients and families as one collective oncology service line
• To address inconsistencies across the continuum of care, nursing leadership implemented a performance improvement project, beginning with Lean principles, PDSA methodologies, and an oncology staff survey; results of this survey signified that only 39% of staff were confident in their role in the oncology educational process, while only 37% were aware of the available educational resources
• Given this evidence, an interdisciplinary team was formed to assess current educational resources and processes, and perform a comprehensive analysis to identify gaps and inconsistencies; patient and family feedback was additionally instrumental in developing the new diagnosis educational materials and processes
• In order to ensure that patients and families receive a consistent message, that could be provided at the patient’s own pace and customized to their learning style, the organization hired a dedicated oncology educator who was trained in the teach-back method and given responsibility for maintaining each educational document’s ongoing relevance
• Education materials were made available through the organization’s intranet site as well as to patients, families, and primary care providers via their online health portal
Standardizing Curriculum for Newly Diagnosed PatientsPractice 1: Creating Improved Patient Education Practices and Opportunities
Business ChallengeOncology-Specific Education Remains Relative to Individual Staff ExperienceAs newly diagnosed oncology patients begin treatment, they expect to receive a consistent message and a standardized approach to education from oncology staff. This consistency is especially crucial for pediatric patients, as the care required can be particularly complex. Strong communication and collaboration between clinicians is required to provide a standardized approach but may pose a challenge. Additionally, variances between the teaching style of clinicians can also lead to patient confusion and a further lack of compliance for the prescribed treatment.
Without a standardized educational curriculum to ensure patient needs are being met and that the organizational message remains consistent among all departments, patient safety and outcomes can be compromised. In an effort to improve the quality of care for oncology patients and to provide a consistent message across the care continuum, bridging this gap will be necessary.
% of Oncology Staff Who Understood Their Organization’s Educational Process at Children’s
Hospital & Medical Center
Less than half of the oncology staff surveyed felt they fully understood Children’s Hospital’s educational curriculum in addition to knowing their role in teaching newly diagnosed patients
Developing a curriculum across the continuum boosts consistency
Standardizing the delivery of education enhances patient understanding
Appointing a dedicated oncology educator ensures resource relevancy High
light
s
39%
Improvement to Staff Familiarity with Oncology Resources and Educational Process at Children’s Hospital & Medical Center
Pre-Implementation Post-Implementation
37%
67%
39%
74%
Resources Process

17COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: “Following Chemotherapy” Caregiver Educational Handout Chemotherapy can cause a variety of side effects among children, such as nausea, vomiting, and fatigue—symptoms that usually reflect illness and can drive considerable concern. To ensure that patients and their caregivers leave a chemotherapy treatment with understanding of their care at Children’s Hospital & Medical Center, caregivers are given an educational handout. This document describes how to carefully dispose of clothing or bedding that comes into contact with the child’s bodily fluids, food preparation, sun protection, and nail care, among other suggestions.
For additional insight on how other organizations have improved the care experience of oncology patients, download The Academy’s white paper, “Expanding Survivorship Care with Persistent Follow-Up and Individualized Treatment,” from the Analyst Advisory page of the members-only web portal
Excerpt from Children’s Hospital & Medical Center’s Caregiver Educational Handout
Disclaimer: This document is not intended to be a substitute for, nor does it constitute, professional medical advice. Always seek the advice of a physician or other qualified health provider with any questions you may have regarding a medical condition. Do not delay seeking professional medical advice due to something you have read in this document.
Copyright © 2016 by Children’s Hospital & Medical Center
Returning to School Going to school is an important part of helping your child feel “normal.” We can help to ease the transition for children returning to school. Timing for when your child can return to school will be based on their diagnosis and type of treatment. In general, your child should have an ANC >500 to return to school. There may be times throughout therapy in which we anticipate your child’s counts to be dropping. During those times we may decide it would be best to keep your child home from school. This can be discussed with your provider. Fertility
The radiation and chemotherapy that are used to treat cancer can sometimes cause problems with your child’s ability to get pregnant or make someone pregnant, also known as fertility. You can talk with your health care team about how likely it is for their treatment to affect fertility. They may be able to offer some options for fertility preservation or ways to make it more likely for your child to have a baby in the future.
Caring for Your Child
Disclaimer: This document is not intended to be a substitute for, nor does it constitute, professional medical advice. Always seek the advice of a physician or other qualified health provider with any questions you may have regarding a medical condition. Do not delay seeking professional medical advice due to something you have read in this document.
Copyright © 2016 by Children’s Hospital & Medical Center
Bodily Fluids
Chemotherapy drugs can come out of your child’s body fluids (urine, stool, vomit and semen). Family members should always wear gloves before coming into contact with your child’s body fluids for at least 48 hours after the chemotherapy has been given. If your child accidentally soils clothing or bedding with any body fluids within 48 hours of receiving chemotherapy, wash the soiled laundry twice in hot water separately from other laundry. When you are at home, flush the toilet twice with the lid down after your child uses the restroom during the 48 hours after receiving chemotherapy. If your child wears diapers, double-bag the soiled diapers and dispose of them immediately. Nail Care
Your child’s fingernails and toe nails should be kept trimmed by using nail clippers, an emery board or cuticle scissors. Discourage nail biting and thumb sucking as they both can be a source of infection. Never let your child tear nails or hang nails.
Sun Protection Chemotherapy will make your child’s skin extremely sensitive to sun. To avoid sunburn, your child should wear sunscreen and a hat year-round and limit the amount of time s/he spends in direct sunlight. Food Preparation
You usually will not need to make any major changes in your child’s diet during therapy. It is recommended to avoid unnecessary exposure to bacteria in foods while your child’s immune system is suppressed. This includes avoiding raw or undercooked meat, unpasteurized dairy products, raw honey and uncooked Brewer’s yeast. In addition, wash all fruits and vegetables thoroughly and avoid any expired food or any food with visible mold. Most milk and yogurt, as well as some cheeses, are pasteurized and are safe to eat.
Caring for Your Child

19
Best Practices in Patient Care ExperiencePROMOTING A HIGHLY ENGAGED ATMOSPHERE FOR PATIENTS

20 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
Along with highly trained and dedicated doctors, nurses, and other medical staff, many procedures and practices in hospitals and health systems are aided by today’s technology advancements. By utilizing new equipment such as video conferencing stations that make telemedicine visits possible, electronic health records that document patients’ history, and ultraviolet germicidal irradiation that disinfects patient rooms, technology has made caring for patients and their families more efficient for healthcare professionals.
Nonetheless, technology has also resulted in growing complexity of care for some patients and has given all consumers of healthcare services the ability to share their care experiences instantaneously with almost anyone. Internet databases and advice forums can confuse patients or even lead to patients disengaged from their care through a mistaken belief that internet sources are as valuable as the services offered at their hospital or health system. Ultimately, any effort to improve the care experience must take into consideration the difficulties of ensuring patient engagement, especially in our socially minded, information-laden world.
In truth, encouraging patient engagement can be approached in a wide variety of ways, and for some organizations, has led to notable improvements in experience and patient outcomes. For example, offering complementary counselor meetings upon discharge to raise awareness of vital follow-up visits for chronic conditions, such as heart failure or COPD, can lead to a decrease in readmissions.
Likewise, engagement can also be improved by implementing patient and family advisory councils, where community members can share their thoughts and concerns about the care they are receiving with service excellence and quality healthcare personnel. By expanding follow-up care and strengthening relationships based on compelling communication between physicians, patients, and family, healthcare organizations can offer a better overall experience.
Engaging patients is not a simple task, and even the best efforts of many leading organizations have left some patients feeling disinterested in care processes. The experiences and insights of industry innovators, however, offer guidance that can help other organizations limit “exit points”—opportunities for patients to disengage from their caregivers and their care—and create more effective points of entry through which to reengage. The tactics that follow share such experiences and may be a useful first step for organizations striving to better engage patients across the continuum.
IntroductionPractice 2: Promoting a Highly Engaged Atmosphere for Patients
When surveying the experienced hospital leadership that makes up its Insights Council, the New England Journal of Medicine Catalyst reported that they believed fewer than one in 10 patients were highly engaged
42%
29%
20%
9%
1–24 25–49 50–74 75–100Low Engagement High Engagement
Engagement Levels of Patients at Their Facilities According to New England Journal of Medicine (NEJM) Catalyst Insights Council Members
Source: Massachusetts Medical Society (2016)
21COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
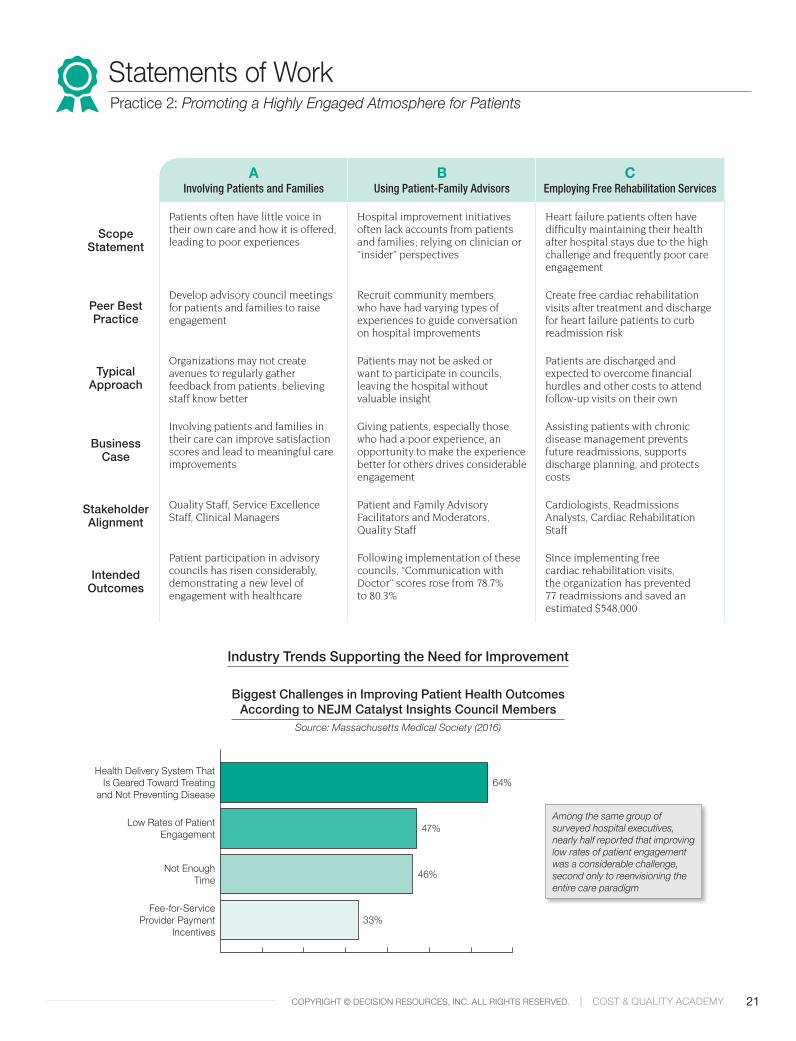
AInvolving Patients and Families
BUsing Patient-Family Advisors
CEmploying Free Rehabilitation Services
Scope Statement
Patients often have little voice in their own care and how it is offered, leading to poor experiences
Hospital improvement initiatives often lack accounts from patients and families; relying on clinician or “insider” perspectives
Heart failure patients often have difficulty maintaining their health after hospital stays due to the high challenge and frequently poor care engagement
Peer Best Practice
Develop advisory council meetings for patients and families to raise engagement
Recruit community members who have had varying types of experiences to guide conversation on hospital improvements
Create free cardiac rehabilitation visits after treatment and discharge for heart failure patients to curb readmission risk
Typical Approach
Organizations may not create avenues to regularly gather feedback from patients, believing staff know better
Patients may not be asked or want to participate in councils, leaving the hospital without valuable insight
Patients are discharged and expected to overcome financial hurdles and other costs to attend follow-up visits on their own
Business Case
Involving patients and families in their care can improve satisfaction scores and lead to meaningful care improvements
Giving patients, especially those who had a poor experience, an opportunity to make the experience better for others drives considerable engagement
Assisting patients with chronic disease management prevents future readmissions, supports discharge planning, and protects costs
Stakeholder Alignment
Quality Staff, Service Excellence Staff, Clinical Managers
Patient and Family Advisory Facilitators and Moderators, Quality Staff
Cardiologists, Readmissions Analysts, Cardiac Rehabilitation Staff
Intended Outcomes
Patient participation in advisory councils has risen considerably, demonstrating a new level of engagement with healthcare
Following implementation of these councils, “Communication with Doctor” scores rose from 78.7% to 80.3%
Since implementing free cardiac rehabilitation visits, the organization has prevented 77 readmissions and saved an estimated $548,000
Statements of WorkPractice 2: Promoting a Highly Engaged Atmosphere for Patients
Industry Trends Supporting the Need for Improvement
Biggest Challenges in Improving Patient Health Outcomes According to NEJM Catalyst Insights Council Members
Source: Massachusetts Medical Society (2016)
Among the same group of surveyed hospital executives, nearly half reported that improving low rates of patient engagement was a considerable challenge, second only to reenvisioning the entire care paradigm
64%
47%
46%
33%
Health Delivery System That Is Geared Toward Treating
and Not Preventing Disease
Low Rates of Patient Engagement
Not Enough Time
Fee-for-Service Provider Payment
Incentives

22 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• After having success in its main hospital-based patient and family advisory councils, Gundersen Health System—headquartered in La Crosse, Wisconsin—has created additional councils at 11 of its regional clinics to give rural patients and families the opportunity to be more engaged in their healthcare
• Under supervision of the system’s Service Excellence Department, 8–12 community members meet at their respective clinics quarterly, where they will enjoy a light supper before discussing topics regarding but not limited to patient education and marketing, behaviors of healthcare staff, and even billing practices
• Requiring that members make a one to three year commitment to the council allows strong bonds and friendships to materialize among council participants and the meeting facilitator, which can encourage passionate discussions; when community participants of the advisory councils are more comfortable with each other and the facilitator, more honest and, ultimately, more useful feedback can be garnered on hospital and health system practices
• Following a printed agenda, meetings begin with members stating what they think is working well at the clinic, such as new electronic check-in kiosks, and conversely, opportunities for improvement, which could be items ranging from physical facility improvements to increasing the number of patients participating in advanced care planning in the clinical setting
• Maintaining 11 different regional councils with 12 diverse members each enables these staff-selected individuals to act as liaisons within their communities, promoting these positive patient experiences through word-of-mouth and explaining that their questions are answered and their advice for improvement is heard
Involving Patients and Families Through CouncilsPractice 2: Promoting a Highly Engaged Atmosphere for Patients
Business ChallengeA Gap Between Expected and Actual Communication for Patients and Their ProvidersThe emotional investment aspect of providing healthcare can be a difficult challenge for many providers to balance, requiring sincerity, empathy, and professionalism. In many cases, providers may be warned by teachers or mentors not to get too emotionally connected with their patients, to limit the chance of burnout or distress if an adverse event occurs. Unfortunately, this can cause a negative impact on the patient’s experience and may leave individuals questioning their overall level of trust in their doctor.
Relatively few organizations have standardized and systematized processes for such interactions outside of the immediate patient care experience. Though the challenges of setting up such a process—patient and family advisory councils, for example—can be difficult, the benefits can distinctly outweigh the costs.
% of Patients Desiring Provider Listening vs. Patients Reporting Being Listened To
Source: Institute of Medicine Discussion Paper (2012)
With a nearly 20% gap between what patients expect and receive from providers, healthcare organizations must realize the importance of fielding patient concerns
Employ dedicated service excellence practitioners
Building trustworthy relationships among members assists in care
Holding insightful regional meetings increases word-of-mouth outreachHigh
light
s
% Increase of Patient and Family Advisory Councils from 2013–2016 at Gundersen Clinics and Partner Organizations
Expected Listening
Actual Listening
80%
61%
By nearly doubling the amount of patient and family advisory councils at Gundersen clinics and partner organizations in a three-year span, the health system has shown confidence in these council meetings to increase patient engagement, satisfaction, and morale
Increase in Councils90%
23COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Patient and Family Advisory Council ContractTo increase patient experience and engagement, facilitating advisory councils to hear healthcare concerns, improvement ideas, and overall feedback from patients and their families can be effective. In order to maintain high levels of discussion, a signed contract can serve as a written record to which members can refer if they need reminding of their consents and obligations.
The following document is a sample member contract shared by Gundersen Health System as part of their patient and family advisory councils. This contract is used as an agreement between members and council facilitators to ensure confidentiality of the council, responsible actions as a representative of Gundersen Health System, and constant support of the council work. It also states the intent of the council, which is to serve as a venue for patients and families to provide input into policy and program development at Gundersen Health System.
For further details on modern efforts to garner more patient feedback and engagement, download the white paper, “Opening Communication Through Social Media to Obtain Patient Feedback,” from the Analyst Advisory page of the members-only web portal
Gundersen Health System’s Patient and Family Advisory Council Member Contract
Cost & Quality Academy
Copyright © Healthcare Business Insights. All Rights Reserved.
Gundersen Health System’s Patient and Family Advisory Council Member Contract
In order to provide a more complete care experience, hospitals continue to strive to raise patient engagement and involvement in their health decisions. Increased patient engagement can be garnered in numerous ways, including the utilization of patient and family advisory councils that engage community members to share ideas regarding policy and program development in their community healthcare realm. In order to gain greater insight into these patient and family advisory councils, The Academy conducted an interview with Gundersen Health System.
The following document is a sample member contract shared by Gundersen Health System for its patient and family advisory council members. This contract outlines commitements that both community council members and Gundersen Health System employees must agree to, such as giving thoughtful and pertinent patient feedback and respecting the confidentiality of the council.
Gundersen Health System Patient and Family Advisory Council
Member Contract As a member of the Gundersen Patient and Family Advisory Council, I agree to:
1. Commit to a minimum of one year of regular attendance of meetings 2. Respect the confidentiality of the Council and of Gundersen 3. Conduct myself as a responsible representative of Gundersen 4. Give thoughtful and pertinent feedback, responding to email requests within 48 hours
Gundersen contracts to:
1. Consistently support the Council work and its members 2. Give reasonable notice if there is a change in plan or schedule 3. Respect the confidentiality of the Council 4. Use advisors time wisely and effectively
Council Member Signature__________________________________________ Date_____ Council Member Name _____________________________________________________ Gundersen Employee Signature _______________________________________________________________Date_____
Gundersen Health System Patient and Family Advisory Council

24 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Through an effort to actively engage community members in quality initiatives, Lowell General Hospital—a 434-bed acute care facility in Lowell, Massachusetts—established a patient and family advisory council (PFAC) allowing for an organized two-way conversation between the community and the hospital that elicits changes based on firsthand care experiences
• Using advertising, pamphlets, a website, and word of mouth, the PFAC recruits and incorporates individuals into the committee who have had varied experiences at the hospital, creating a group comprised of people with diverse perspectives toward the inpatient stay
• A nominating chair vets applicants who will then meet with guests to learn about the responsibilities of the council and are later assigned a “committee buddy” to help educate them about the typical expectation and time commitments of the PFAC
• Assembling six times a year, council members discuss a standardized agenda on quality improvement, patient education, and annual priorities; additionally, an open agenda roundtable offers the opportunity to discuss more wide-ranging topics such as hospital improvement, visitation policies, communication tools, continuity of care, and social services
• Much of a PFAC member’s time is used to advocate for the council and present initiatives in their own social circles which has led to the formation of strong bonds between members and their communities with improved healthcare engagement as the product
Using Patient-Family Advisors to Center Care on PatientsPractice 2: Promoting a Highly Engaged Atmosphere for Patients
Business ChallengeCapturing All Voices in the Continuum of CareTo understand the total value of healthcare, suggestions and considerations must be taken from more than solely physicians or other clinical staff. However, within many hospital committees and oversight groups, healthcare providers sometimes represent the majority, offering a limited perspective toward the assessment of quality improvement initiatives. This creates an incomplete narrative of healthcare practices and risks limiting the perspectives of providers when it comes to honest criticism and opportunities for legitimate, long-term improvement.
For patients in such a hospital or health system, care practices and the related experience may seem to stagnate or obvious problems—at least to the patient’s observations—may not be solved. Thus the involvement of patients and their families or caregivers continues to be an opportunity for sincere improvement of practices.
% of Hospitals Adopting Patient and Family Advisory Councils
Source: The American Hospital Association’s Health Research & Educational Trust (2016)
Despite the considerable potential value of direct patient to provider interaction to drive better care quality and experience, a wide majority of hospitals throughout the nation have not adopted the use of patient and family advisory councils
Recruiting active community members evokes suggestions
Create opportunities for both structured and open discussion
Ensure council members advocate for initiatives in their social groupsHigh
light
s
No Councils
Some Units
60.6%
13.4%
Hospital-Wide
No Data
25.0%
1.0%
“Always” HCAHPS Scores Across Three Questions at Lowell General Hospital During PFAC Integration
Source: Lowell General Hospital (2016)
78.8% 80.8% 78.7% 80.3%
62.1% 64.0%
2015Communication
with Nurse
2016 2015Communication
with Doctors
2016 2015Communication About Medicine
2016

25COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Patient Family Advisory Council ApplicationRecruiting patients and family members to participate in hospital committees requires hospital staff to take greater efforts than simply informing an individual about a group. Patient information must be gathered and considerations made for the type of group membership that will result from those included. The following document is a sample application shared with The Academy by Lowell General Hospital that provides fields for any needed information and attempts to gauge the interest and reasoning for applicants in being a part of the patient family advisory council.
For more information on Lowell General Hospital’s efforts with patient and family advisory councils, download the white paper, “Increasing Community Engagement with Care Initiatives Through Active Patient and Family Presence on Hospital Councils,” from the Analyst Advisory page of the members-only web portal
Lowell General Hospital’s Patient Family Advisory Council Application

26 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• To improve clinical outcomes and reduce its heart failure readmissions, the Regional Medical Center (RMC) in Orangeburg, South Carolina, began a process of internal review and discussion that led to a growing awareness that cardiac rehabilitation visits were a potent force in favor of long-term improvement in heart failure patients’ health
• As cardiac rehabilitation staff are better able to develop strong relationships with patients—due to weekly visits and a focus on building the patients toward success—RMC sought a way to regularly engage heart failure patients in rehabilitation, ultimately deciding that offering these visits for free would drive higher usage and could prevent some readmissions
• The plan approved by hospital leadership allowed for patients treated and discharged for heart failure to receive two weekly cardiac rehabilitation visits for one month at no cost; considered Stage IV participants in rehabilitation, the cost for these visits was underwritten by the hospital
• To facilitate usage of the new free visits, RMC educated its staff hospitalwide and developed a custom electronic order that alerts rehabilitation staff upon submission
• Further, patients are provided an informational packet about rehabilitation during their hospitalization and have their first free visit entered into their discharge instructions; thanks to these efforts, RMC has exceeded its goal of at least 25% of patients referred attending a minimum four of eight visits; as a result, RMC has prevented 77 readmissions since May 2013 with an estimated savings $548,000
Employing Free Cardiac Rehabilitation ServicesPractice 2: Promoting a Highly Engaged Atmosphere for Patients
Business ChallengeStrategically Combating Symptom Management for Heart Failure PatientsAs one of the most costly chronic diseases both financially and in terms of lost life, heart failure presents countless challenges for hospitals and health systems as they strive to ensure positive, long-lasting patient outcomes despite numerous roadblocks. Perhaps chief among the difficulties posed by heart failure is the simple fact that care for the disease never truly ends. Even when the patient is discharged following diagnosis or an acute episode, multiple care maintenance requirements follow them home or to a skilled nursing facility. Moreover, whether due to ignorance, forgetfulness, fear of costs, or a willful desire to avoid healthcare services altogether, it is not uncommon for heart failure patients to miss vital follow-up appointments.
The results of these factors are clear. Care for these patients is costly, readmission rates high, and mortality all too common. Patient engagement with care for such a condition is core to lasting success, but overcoming barriers to care and maintaining that engagement long term pose considerable challenges.
% of Patients Participating in Cardiac Rehabilitation Services
of All Those EligibleSource: American Heart Association (2013)
While services that can improve the health of heart failure patients in the long term, such as cardiac rehabilitation, can be extremely beneficial, only one in five patients make use of them
Offering a free service may provide considerable return on investment
Utilize staff that can build meaningful patient relationships
Providing information up front ensures opportunity for engagementHigh
light
s
Volume of Participants Versus Readmissions in the Cardiac Rehabilitation Program at RMC
Participants Readmissions
<20%
17
4
22
4
17
1
FY 130
26
FY 14 FY 15 FY 16 Through Sept

27COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Heart Failure Subphase Order SetManaging a heart failure patient during their stay requires structure, coordination, and organization to ensure successful clinical outcomes. The following document is a sample physician order set shared by Regional Medical Center that acts as part of its electronic physician order set for initiating cardiac rehabilitation services. The order includes categories to ensure patients receive all needed ancillary cardiac rehabilitation services including dietary and pharmacy consultations.
For greater insight into other means to reduce heart failure readmissions, watch or download the Virtual Conference presentation, “Reducing Heart Failure Readmissions – A Case Study in Improving Care Through a Standardized, Team-Based Approach,” from the Events page of the members-only web portal
Cost & Quality Academy
Copyright © Healthcare Business Insights. All Rights Reserved.
The Regional Medical Center’s Heart Failure Subphase Order Set Source: The Regional Medical Center (Effective 6/29/2015)
Heart Failure Subphase Patient Care Heart Failure Education
T;N, q12h Standard Consults Dietary Consult
t;n, Heart Failure Management Pharmacy Consultant
CHF Medication Management review - interdisciplinary team management and teaching. Consult to Cardiac Rehabilitation
t;n, HF Monitoring Case Management Consult
t;n, Routine, Heart failure Management Communication Order MD to Nursing
t;n, Heart Failure Management- One time Home Health visit Referral to Discharge Clinic
t;n, follow up within 3 days of discharge from the hospital *Report Legend: DEF - This order sentence is the default for the selected order GOAL - This component is a goal IND - This component is an indicator INT - This component is an intervention IVS - This component is an IV Set NOTE - This component is a note Rx - This component is a prescription SUB - This component is a sub phase
Regional Medical Center’s Heart Failure Subphase Order Set

29
Best Practices in Patient Care ExperienceREDUCING STRESSORS AND MISCOMMUNICATION TO BOLSTER PATIENT SATISFACTION
30 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
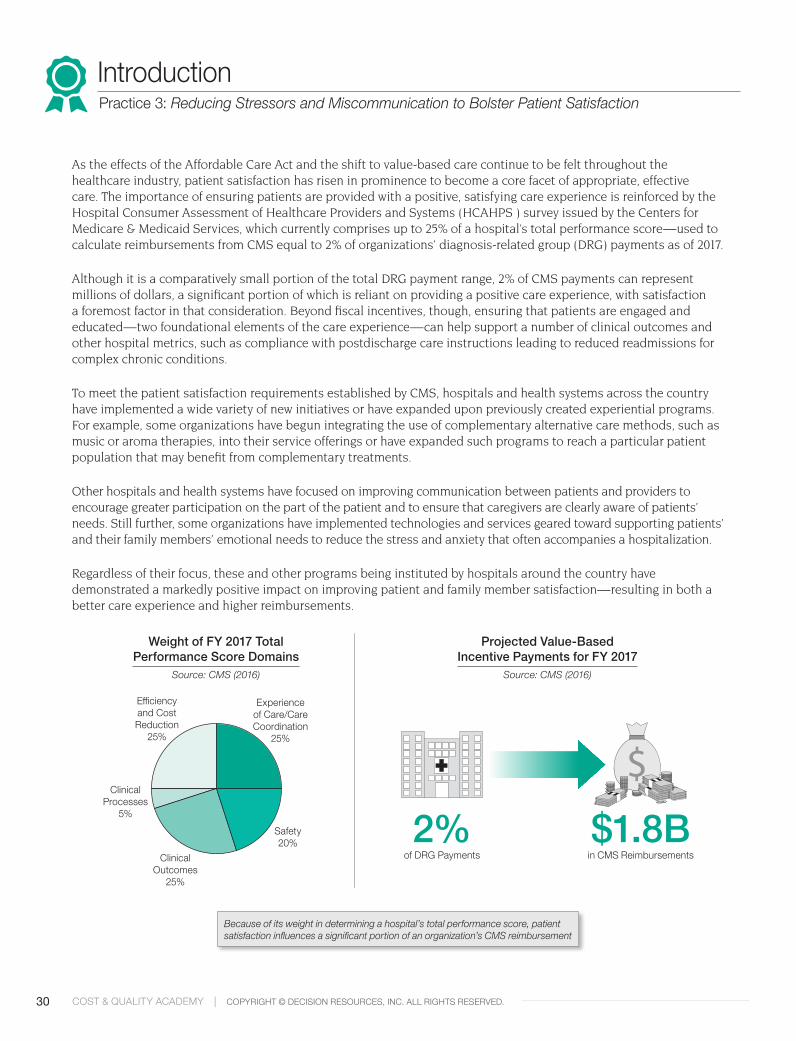
As the effects of the Affordable Care Act and the shift to value-based care continue to be felt throughout the healthcare industry, patient satisfaction has risen in prominence to become a core facet of appropriate, effective care. The importance of ensuring patients are provided with a positive, satisfying care experience is reinforced by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS ) survey issued by the Centers for Medicare & Medicaid Services, which currently comprises up to 25% of a hospital’s total performance score—used to calculate reimbursements from CMS equal to 2% of organizations’ diagnosis-related group (DRG) payments as of 2017.
Although it is a comparatively small portion of the total DRG payment range, 2% of CMS payments can represent millions of dollars, a significant portion of which is reliant on providing a positive care experience, with satisfaction a foremost factor in that consideration. Beyond fiscal incentives, though, ensuring that patients are engaged and educated—two foundational elements of the care experience—can help support a number of clinical outcomes and other hospital metrics, such as compliance with postdischarge care instructions leading to reduced readmissions for complex chronic conditions.
To meet the patient satisfaction requirements established by CMS, hospitals and health systems across the country have implemented a wide variety of new initiatives or have expanded upon previously created experiential programs. For example, some organizations have begun integrating the use of complementary alternative care methods, such as music or aroma therapies, into their service offerings or have expanded such programs to reach a particular patient population that may benefit from complementary treatments.
Other hospitals and health systems have focused on improving communication between patients and providers to encourage greater participation on the part of the patient and to ensure that caregivers are clearly aware of patients’ needs. Still further, some organizations have implemented technologies and services geared toward supporting patients’ and their family members’ emotional needs to reduce the stress and anxiety that often accompanies a hospitalization.
Regardless of their focus, these and other programs being instituted by hospitals around the country have demonstrated a markedly positive impact on improving patient and family member satisfaction—resulting in both a better care experience and higher reimbursements.
IntroductionPractice 3: Reducing Stressors and Miscommunication to Bolster Patient Satisfaction
Because of its weight in determining a hospital’s total performance score, patient satisfaction influences a significant portion of an organization’s CMS reimbursement
Projected Value-Based Incentive Payments for FY 2017
Source: CMS (2016)
Weight of FY 2017 Total Performance Score Domains
Source: CMS (2016)
Experience of Care/Care Coordination
25%
Clinical Outcomes
25%
Safety 20%
Clinical Processes
5%
Efficiency and Cost Reduction
25%
of DRG Payments2%
in CMS Reimbursements$1.8B

31COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ACalming Music Therapy
Interventions
BImproving Communication
CMinimizing Stress Through
Patient Tracking
Scope Statement
Discomfort stemming from injury and sickness may negatively influence perceptions of care
A lack of organizational focus and awareness of current state on patient satisfaction may impact care on the frontline
Uncertainty over a patient’s status and location may heighten familial stress and thereafter decrease patient satisfaction
Peer Best Practice
Offer holistic services such as music therapy to address the full spectrum of patient needs and improve satisfaction
Adopt multiple electronic surveys and dashboards to provide more comprehensive feedback data
Provide patient families with up-to-date patient status and location information via an anonymized video board
Typical Approach
Staff can often overlook patients’ emotional needs in favor of supporting physical comfort, leaving anxiety and stress unaddressed
Organizations focus on national reporting standards instead of also looking at hospital-specific measures, limiting patient satisfaction information
Health systems prioritize tasks that directly impact patients at the bedside and often forego providing real-time patient status and location changes to waiting families
Business Case
Enriching patients’ hospital experience assists in improving HCAHPS scores, thereby subsequently impacting reimbursements
Maintaining a focus on satisfaction improves patient engagement, contributing to better clinical outcomes
Ensuring a patient’s family is informed throughout their hospital stay can improve both their and the patient’s satisfaction
Stakeholder Alignment
Music Therapists, Nurses, Physicians
Administrators, Quality Department Staff, Physicians, Nurses
Surgeons, Nurses, Patient and Guest Relations Staff Members
Intended Outcomes
Providing services to address patients’ foundational emotional and mental discomforts can assist with symptom management and improve HCAHPS scores
Sustaining communication about the patient experience between clinic leadership and providers, while also improving key CGCAHPS measures increased overall CGCAHPS value from 72.9% to 78.9%
Making individuals in the waiting room aware of related patient status updates without directly consuming staff time can bolster the satisfaction of all parties involved
Statements of WorkPractice 3: Reducing Stressors and Miscommunication to Bolster Patient Satisfaction
Industry Trends Supporting the Need for Improvement
Average “Top Box” HCAHPS Score in 2015 at Participating U.S. HospitalsSource: CMS (2016)
Although many hospitals and health systems have dedicated time and resources to improving HCAHPS domains, there is still considerable room for improvement
82%
80%
68%
65%
Communication with Doctors
Communication with Nurses
Responsiveness of Staff
Communication About Medications
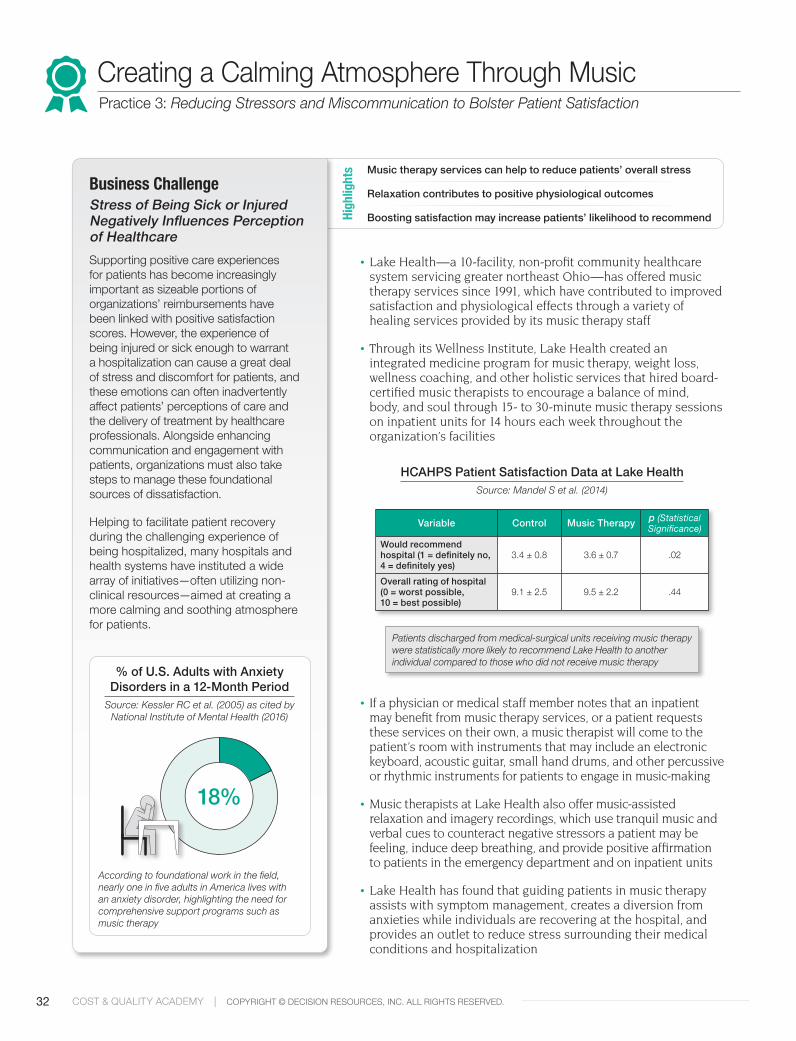
32 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Lake Health—a 10-facility, non-profit community healthcare system servicing greater northeast Ohio—has offered music therapy services since 1991, which have contributed to improved satisfaction and physiological effects through a variety of healing services provided by its music therapy staff
• Through its Wellness Institute, Lake Health created an integrated medicine program for music therapy, weight loss, wellness coaching, and other holistic services that hired board-certified music therapists to encourage a balance of mind, body, and soul through 15- to 30-minute music therapy sessions on inpatient units for 14 hours each week throughout the organization’s facilities
• If a physician or medical staff member notes that an inpatient may benefit from music therapy services, or a patient requests these services on their own, a music therapist will come to the patient’s room with instruments that may include an electronic keyboard, acoustic guitar, small hand drums, and other percussive or rhythmic instruments for patients to engage in music-making
• Music therapists at Lake Health also offer music-assisted relaxation and imagery recordings, which use tranquil music and verbal cues to counteract negative stressors a patient may be feeling, induce deep breathing, and provide positive affirmation to patients in the emergency department and on inpatient units
• Lake Health has found that guiding patients in music therapy assists with symptom management, creates a diversion from anxieties while individuals are recovering at the hospital, and provides an outlet to reduce stress surrounding their medical conditions and hospitalization
Creating a Calming Atmosphere Through MusicPractice 3: Reducing Stressors and Miscommunication to Bolster Patient Satisfaction
Business ChallengeStress of Being Sick or Injured Negatively Influences Perception of HealthcareSupporting positive care experiences for patients has become increasingly important as sizeable portions of organizations’ reimbursements have been linked with positive satisfaction scores. However, the experience of being injured or sick enough to warrant a hospitalization can cause a great deal of stress and discomfort for patients, and these emotions can often inadvertently affect patients’ perceptions of care and the delivery of treatment by healthcare professionals. Alongside enhancing communication and engagement with patients, organizations must also take steps to manage these foundational sources of dissatisfaction.
Helping to facilitate patient recovery during the challenging experience of being hospitalized, many hospitals and health systems have instituted a wide array of initiatives—often utilizing non-clinical resources—aimed at creating a more calming and soothing atmosphere for patients.
% of U.S. Adults with Anxiety Disorders in a 12-Month Period
Source: Kessler RC et al. (2005) as cited by National Institute of Mental Health (2016)
According to foundational work in the field, nearly one in five adults in America lives with an anxiety disorder, highlighting the need for comprehensive support programs such as music therapy
Music therapy services can help to reduce patients’ overall stress
Relaxation contributes to positive physiological outcomes
Boosting satisfaction may increase patients’ likelihood to recommend High
light
s
Variable Control Music Therapy p (Statistical Significance)
Would recommend hospital (1 = definitely no, 4 = definitely yes)
3.4 ± 0.8 3.6 ± 0.7 .02
Overall rating of hospital (0 = worst possible, 10 = best possible)
9.1 ± 2.5 9.5 ± 2.2 .44
Patients discharged from medical-surgical units receiving music therapy were statistically more likely to recommend Lake Health to another individual compared to those who did not receive music therapy
HCAHPS Patient Satisfaction Data at Lake HealthSource: Mandel S et al. (2014)
18%

33COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Music Therapy Treatment Plan and Documentation RecordLong employed by a small number of hospitals and health systems, music therapy has demonstrated a positive impact on improving patients’ mood and morale, reducing anxiety, and assisting with pain management. This music therapy treatment plan from Lake Health serves as a method of documenting individual sessions and includes a large list of interventions that can be employed, goals for the session, and areas for comments specific to the patient and reason for the session. Additionally, it includes spaces for documenting and tracking outcomes including patient pain, mood, vocal feedback, anxiety, and sadness, as well as post-session heart rate and blood pressure.
For further details on Lake Health’s music therapy program, download the Academy’s white paper, “Creating a Calming Atmosphere Through the Use of Music Therapy Interventions,” from the Analyst Advisory page of the members-only web portal
Lake Health’s Music Therapy Treatment Plan
Lake Health Music Therapy Treatment Plan Label Page 2 of 2
MT_NU9081_612
AFFECT Before After
Affect MT Rated □ Smiling □ Neutral □ Frown/Grimace □ Clenched Teeth/Tension
□ Smiling □ Neutral □ Frown/Grimace □ Clenched Teeth/Tension
Affect Comments: VOCAL Before After
Vocal MT Rated
□ Positive □ Neutral/No Vocal □ Crying/Moaning □ Screaming/Yelling
□ Positive □ Neutral/No Vocal □ Crying/Moaning □ Screaming/Yelling
Vocal Comments: ANXIETY Before After
Anxiety MT Rated
□ Yes □ No
□ Yes □ No
Anxiety Comments: SADNESS Before After
Sadness MT Rated
□ Yes □ No
□ Yes □ No
Sadness Comments: Post Session BP: /
Post-Session HR:
□ Designated care partner present □ Other person present
Name and Relationship:
Patient agreed to music therapist return: □ Yes □ No If patient did not agree to music therapist return, why? If music therapist did not offer return visit why? Outpatient music therapy offered: □ Yes □ No If Yes, patient agreed to follow-up contact: □ Yes □ No Outpatient follow-up Comments: Evaluation Comments (including patient quotations): Signature: Date: Time:
Lake Health Music Therapy Treatment Plan Label Page 1 of 2
MT_NU9081_612
Purpose of Visit: □ Screening □ Assessment □ Follow-Up □ Neurologic Music Therapy Session
Length Session (min):
Reason for Patient Admission: Source of Referral: □ Case Manager □ Care Coordinator □ Clergy □ Family Member □ Hospice □ Nursing □ Patient Request □ Physician □ PT/OT □ Speech Referral Reason:
Assessment Comments (Including Patient Quotations):
Baseline BP / N/A
Baseline HR N/A
Goals: (check all that apply) □ Calm/Soothe Anxiety □ Divert from Pain □ Elevate Mood □ Emotional/Spiritual Support □ Induce Sleep □ Memory Sharing/Reminiscence □ Offset Sadness □ Orient to time, place and self □ Positive Stimulation □ Procedural Support □ Promote Movement □ Relaxation □ Relieve Stress □ Self Expression □ Other; See Goals Comment □ Sensorimotor Training □ Speech and Language Training □ Cognition Training Goals Comment: Interventions: (Check all that apply) □ Drawing to Music □ Improvisation □ Lyric Analysis □ Music Assisted Relaxation □ Music Diversion □ Music Instrument Playing □ Personal music listening Instruction □ Song Requests □ Songwriting □ Therapeutic Listening □ Therapeutic Singing □ Verbal Processing □ Other, See Interventions Comment □ TIMP Therapeutic Instrumental Music Performance □ PSE Patterned Sensory Enhancement □ RAS Rhythmic Auditory Stimulation □ MIT Melodic Intonation Therapy □ OMREX Oral Motor and Respiratory Exercises □ VIT Vocal Intonation Therapy □ MUSTIM Musical Speech Stimulation □ DSLM Developmental Speech and Language Training Through Music □ RCS Rhythmic Speech Cuing □ SYCOM Symbolic Communication Training Through Music □ MNT Music Neglect Training □ MSOT Music Sensory Orientation Training □ APT Auditory Perception Training □ MACT Musical Attention Control Training □ MMT Musical Mnemonics Training □ MEFT Musical Executive Functions Training □ MPC Music Psychotherapy and Counseling Interventions Comments:
Music Preferences: □ Big Band □ Blues □ Broadway □ Classical □ Country □ Easy Listening □ Folk □ Jazz □ Oldies □ Pop □ Patriotic □ Polka □ No Rap □ No Country □ Spiritual □ No Musical Preference □ No Spiritual □ Rock □ Spiritual Music Preference Comments: Outcomes: (Check all that apply) □ Calm/Soothe Anxiety □ Divert from Pain □ Elevate Mood □ Emotional/Spiritual Support □ Induce Sleep □ Memory Sharing Reminiscence □ Offset Sadness □ Orient to time, place and self □ Positive Stimulation □ Promote Movement □ Procedural Support □ Promote Movement □ Relaxation □ Relieve Stress □ Self Expression □Other, See Outcomes Comment
Outcomes Comments:
Evaluation: PAIN Before After
MT/PT Rated (0,1,2,3,4,5,6,7,8,9,10)
0 = No Pain; 10 = Worst Pain
N/A
N/A
Pain Comments:
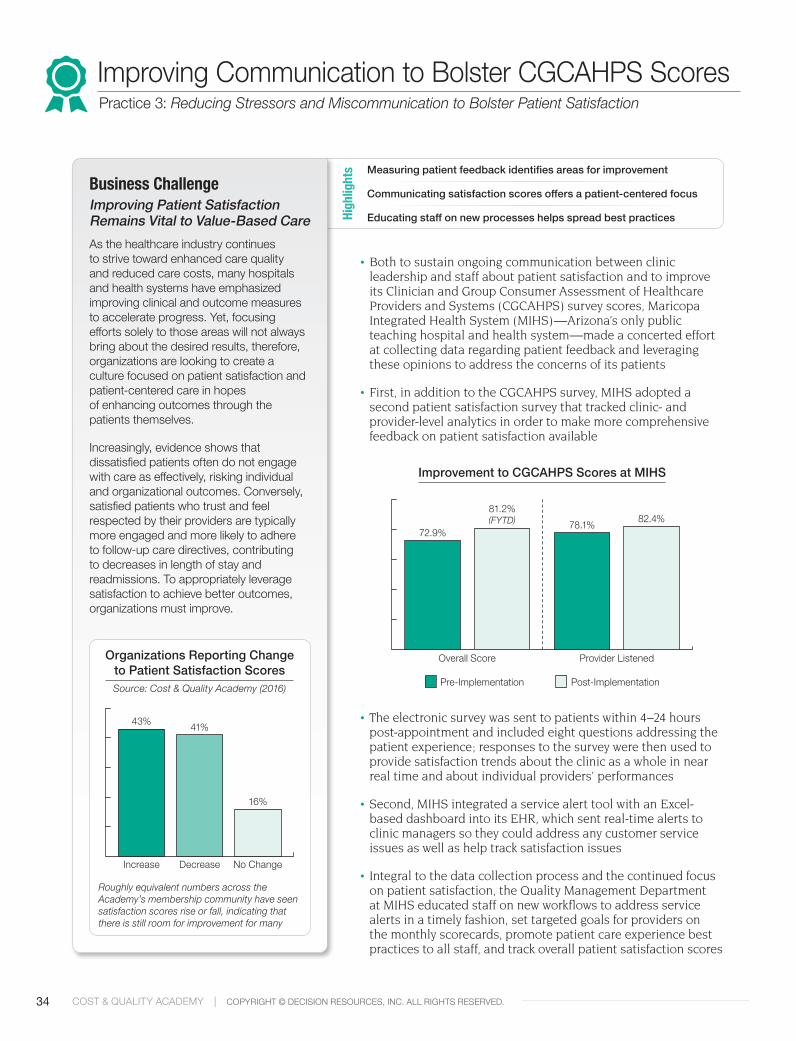
34 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Both to sustain ongoing communication between clinic leadership and staff about patient satisfaction and to improve its Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CGCAHPS) survey scores, Maricopa Integrated Health System (MIHS)—Arizona’s only public teaching hospital and health system—made a concerted effort at collecting data regarding patient feedback and leveraging these opinions to address the concerns of its patients
• First, in addition to the CGCAHPS survey, MIHS adopted a second patient satisfaction survey that tracked clinic- and provider-level analytics in order to make more comprehensive feedback on patient satisfaction available
• The electronic survey was sent to patients within 4–24 hours post-appointment and included eight questions addressing the patient experience; responses to the survey were then used to provide satisfaction trends about the clinic as a whole in near real time and about individual providers’ performances
• Second, MIHS integrated a service alert tool with an Excel-based dashboard into its EHR, which sent real-time alerts to clinic managers so they could address any customer service issues as well as help track satisfaction issues
• Integral to the data collection process and the continued focus on patient satisfaction, the Quality Management Department at MIHS educated staff on new workflows to address service alerts in a timely fashion, set targeted goals for providers on the monthly scorecards, promote patient care experience best practices to all staff, and track overall patient satisfaction scores
Improving Communication to Bolster CGCAHPS ScoresPractice 3: Reducing Stressors and Miscommunication to Bolster Patient Satisfaction
Business ChallengeImproving Patient Satisfaction Remains Vital to Value-Based CareAs the healthcare industry continues to strive toward enhanced care quality and reduced care costs, many hospitals and health systems have emphasized improving clinical and outcome measures to accelerate progress. Yet, focusing efforts solely to those areas will not always bring about the desired results, therefore, organizations are looking to create a culture focused on patient satisfaction and patient-centered care in hopes of enhancing outcomes through the patients themselves.
Increasingly, evidence shows that dissatisfied patients often do not engage with care as effectively, risking individual and organizational outcomes. Conversely, satisfied patients who trust and feel respected by their providers are typically more engaged and more likely to adhere to follow-up care directives, contributing to decreases in length of stay and readmissions. To appropriately leverage satisfaction to achieve better outcomes, organizations must improve.
Organizations Reporting Change to Patient Satisfaction ScoresSource: Cost & Quality Academy (2016)
Roughly equivalent numbers across the Academy’s membership community have seen satisfaction scores rise or fall, indicating that there is still room for improvement for many
Measuring patient feedback identifies areas for improvement
Communicating satisfaction scores offers a patient-centered focus
Educating staff on new processes helps spread best practicesHigh
light
s
Increase Decrease
43% 41%
No Change
16%
Improvement to CGCAHPS Scores at MIHS
Pre-Implementation Post-Implementation
72.9%
81.2% (FYTD) 78.1% 82.4%
Overall Score Provider Listened
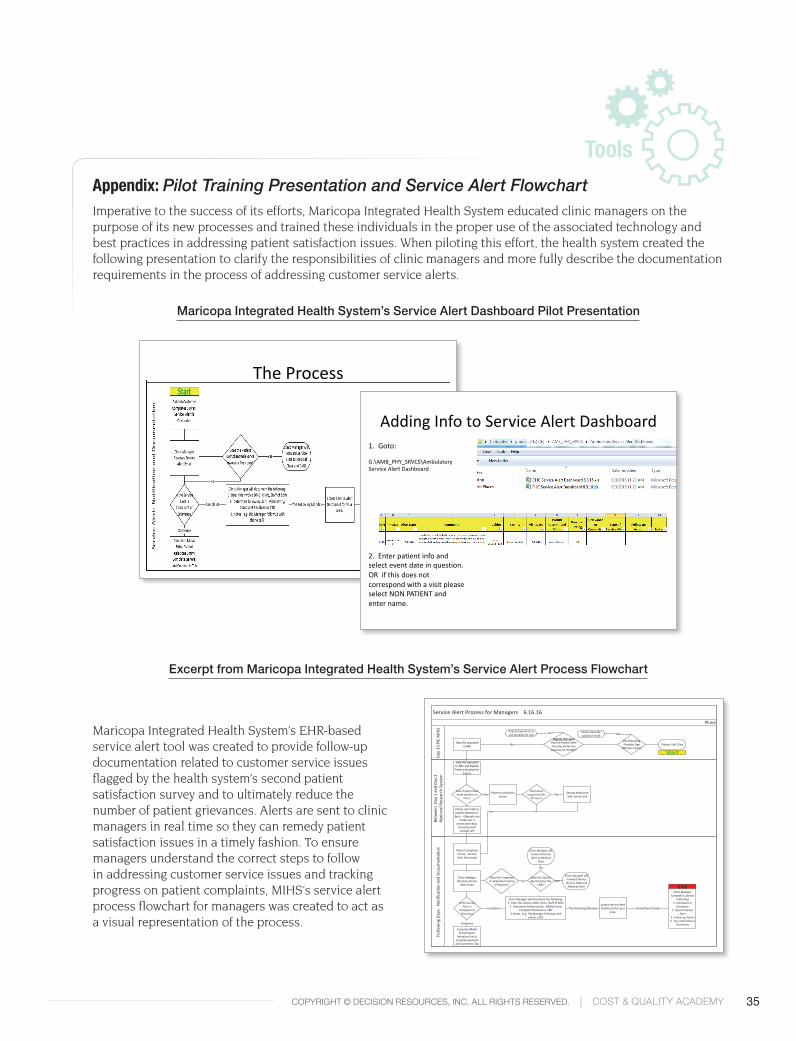
35COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Pilot Training Presentation and Service Alert FlowchartImperative to the success of its efforts, Maricopa Integrated Health System educated clinic managers on the purpose of its new processes and trained these individuals in the proper use of the associated technology and best practices in addressing patient satisfaction issues. When piloting this effort, the health system created the following presentation to clarify the responsibilities of clinic managers and more fully describe the documentation requirements in the process of addressing customer service alerts.
Maricopa Integrated Health System’s EHR-based service alert tool was created to provide follow-up documentation related to customer service issues flagged by the health system’s second patient satisfaction survey and to ultimately reduce the number of patient grievances. Alerts are sent to clinic managers in real time so they can remedy patient satisfaction issues in a timely fashion. To ensure managers understand the correct steps to follow in addressing customer service issues and tracking progress on patient complaints, MIHS’s service alert process flowchart for managers was created to act as a visual representation of the process.
Excerpt from Maricopa Integrated Health System’s Service Alert Process Flowchart
Maricopa Integrated Health System’s Service Alert Dashboard Pilot Presentation
Service Alert Process for Managers 6.16.16
Day
1 EP
IC M
IHS
Betw
een
Day
1 a
nd D
ay 2
Na
tiona
l Res
earc
h Sy
stem
Follo
win
g Da
ys:
Notif
icatio
n an
d Do
cum
enta
tion
Phase
Phone call made to patient between 6-8pm. Attempts are
made over 3 consecutive days.
Voicemail with number left
Does Patient have email address on
file s?
Patient is emailed a surveyYes
No
Patient Completes Survey. Service Alert Generated
Yes
Data file uploaded to NRC and Eligible Patient Sampled for
Survey
Clinic Manager Receives Service
Alert Email
Does the Compliant or Grievance involve
a Physician?
Complete Midas Entry(Patient
Relations Entry)Complete General
and Comments Tab
Does the Service Alert Involve the
CMD? Yes
Is the Service Alert a
Complaint or Grievance
NO
Grievance
Access Service Alert Dashboard for your
area.
Clinic Manager will document the following:1. Does this involve DMG, Clinic, Staff of Both
2. Determine follow-up Axn: Midas Entry/Complaint Resolved or TBD
3. Notes (e.g. Did Manager followup with phone call?)
Complaint The Following Monday
Clinic Manager Complete Columns
Indicating 1. Complaint or
Grievance 2. Type of Service
Alert 3. Follow-up Action 4. Any other Notes/
Comments
Shared Excel Sheet
Start
End
Eligible OutreachHas the Patient Seen Provider within the
previous 12 months?
Patient Visit Clinic
Patient Experience is not sampled for visit
Did Attending Provider Sign
off/Close Chart?
Data file uploaded to NRC
Patient Data file upload on hold NOYes
No
Clinic Manager will Forward Service Alert to Medical
Chair
Yes
Clinic Manager will Forward Service
Alert to CMD and Medical Chair
Second email sent with survey Link
Did patient respond within
72 hours?No
TheProcess
AddingInfotoServiceAlertDashboard1.Goto:
G:\AMB_PHY_SRVCS\AmbulatoryServiceAlertDashboard
2.Enterpatientinfoandselecteventdateinquestion.ORifthisdoesnotcorrespondwithavisitpleaseselectNONPATIENTandentername.
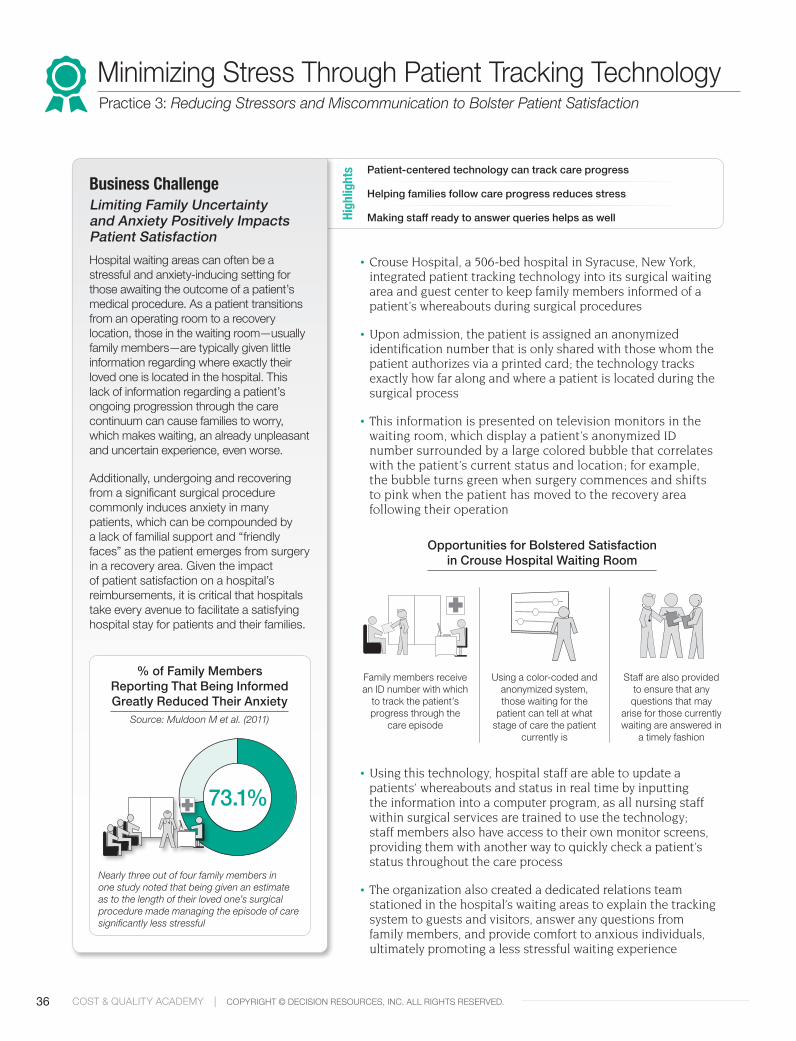
36 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
• Crouse Hospital, a 506-bed hospital in Syracuse, New York, integrated patient tracking technology into its surgical waiting area and guest center to keep family members informed of a patient’s whereabouts during surgical procedures
• Upon admission, the patient is assigned an anonymized identification number that is only shared with those whom the patient authorizes via a printed card; the technology tracks exactly how far along and where a patient is located during the surgical process
• This information is presented on television monitors in the waiting room, which display a patient’s anonymized ID number surrounded by a large colored bubble that correlates with the patient’s current status and location; for example, the bubble turns green when surgery commences and shifts to pink when the patient has moved to the recovery area following their operation
• Using this technology, hospital staff are able to update a patients’ whereabouts and status in real time by inputting the information into a computer program, as all nursing staff within surgical services are trained to use the technology; staff members also have access to their own monitor screens, providing them with another way to quickly check a patient’s status throughout the care process
• The organization also created a dedicated relations team stationed in the hospital’s waiting areas to explain the tracking system to guests and visitors, answer any questions from family members, and provide comfort to anxious individuals, ultimately promoting a less stressful waiting experience
Minimizing Stress Through Patient Tracking TechnologyPractice 3: Reducing Stressors and Miscommunication to Bolster Patient Satisfaction
Opportunities for Bolstered Satisfaction in Crouse Hospital Waiting Room
Family members receive an ID number with which
to track the patient’s progress through the
care episode
Using a color-coded and anonymized system, those waiting for the
patient can tell at what stage of care the patient
currently is
Staff are also provided to ensure that any questions that may
arise for those currently waiting are answered in
a timely fashion
Business ChallengeLimiting Family Uncertainty and Anxiety Positively Impacts Patient SatisfactionHospital waiting areas can often be a stressful and anxiety-inducing setting for those awaiting the outcome of a patient’s medical procedure. As a patient transitions from an operating room to a recovery location, those in the waiting room—usually family members—are typically given little information regarding where exactly their loved one is located in the hospital. This lack of information regarding a patient’s ongoing progression through the care continuum can cause families to worry, which makes waiting, an already unpleasant and uncertain experience, even worse.
Additionally, undergoing and recovering from a significant surgical procedure commonly induces anxiety in many patients, which can be compounded by a lack of familial support and “friendly faces” as the patient emerges from surgery in a recovery area. Given the impact of patient satisfaction on a hospital’s reimbursements, it is critical that hospitals take every avenue to facilitate a satisfying hospital stay for patients and their families.
% of Family Members Reporting That Being Informed Greatly Reduced Their Anxiety
Source: Muldoon M et al. (2011)
Nearly three out of four family members in one study noted that being given an estimate as to the length of their loved one’s surgical procedure made managing the episode of care significantly less stressful
Patient-centered technology can track care progress
Helping families follow care progress reduces stress
Making staff ready to answer queries helps as wellHigh
light
s
73.1%

37COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED. | COST & QUALITY ACADEMY
ToolsAppendix: Sample Operating Room Tracer CardEven after patient tracking monitors are installed, visitors and caregivers waiting for word on a patient may not immediately understand how they are supposed to use the technology. This sample operating room tracker card utilized by Crouse Hospital explains the purpose of the patient tracking monitors posted in the guest waiting areas and provides the family with the unique identifying number of the given patient so that the family may track progress through the surgical process. It also defines and describes the different levels of the surgical process and provides directions to family members who may have further questions.
For additional tactics to improve the satisfaction of patients and their families during or following operations, download The Academy’s white paper, “Enhancing Throughput and Satisfaction with a Patient Departure Lounge,” from the Analyst Advisory page of the members-only web portal
Crouse Hospital’s Operating Room Tracer Card
Questions? Please ask the Guest Services Receptionist to assist you with any questions you may have on the status of your loved one.
RED Patient is in Preoperative Holding Area
BLUE Patient is in Operating Room
GREEN Surgery has begun
PINK Patient is in Post-Anesthesia Care Unit (Recovery Room)
ORANGEPatient has left Post-Anesthesia Care Unit and is being moved to a nursing unit
To Family Members and Guests of Witting Surgical Center Patients:The Witting Surgical Center guest areas have display screens that will allow you to track the progress of your loved one as they go through the surgical process.
Please take note of this unique number: __________. It will appear on a bubble on the monitor. This number is only identifiable to you or anyone you wish to share it with.
The bubble on the monitor will change color, indi-cating where the patient is in the surgical process.

39
Healthcare Business InsightsACADEMY COMMUNITIES

40 COST & QUALITY ACADEMY | COPYRIGHT © DECISION RESOURCES, INC. ALL RIGHTS RESERVED.
Academy CommunitiesHealthcare Business Insights
Cost & Quality Academy
The Cost & Quality Academy membership community provides Chief Quality Officers, Chief Nursing Officers, Chief Medical Officers, and their managers with resources to assist in the transition to a value-based care environment, care delivery improvement, disease management, and care quality and patient satisfaction initiatives.
Information Technology Academy
The Information Technology Academy membership community serves Chief Information Officers and departmental leadership responsible for IT and clinical informatics governance, infrastructure management, support networks, and application deployment, security, and optimization.
Revenue Cycle Academy
The Revenue Cycle Academy membership community serves Chief Financial Officers, Revenue Cycle Vice Presidents and Directors, and all other revenue cycle leaders who oversee patient access, documentation, charge capture, coding, and billing & collections processes.
Supply Chain Academy
The Supply Chain Academy membership community serves Chief Financial Officers, Chief Purchasing Officers, and their management teams in planning & forecasting, purchasing & sourcing, contracting, and materials management & logistics processes.
Healthcare Business Insights enables healthcare providers to improve their business outcomes through best practice research, industry insights, and implementation resources. Each HBI Academy is focused on distinct business functions, providing hospital and health system members with numerous offerings intended to help them improve the way they do business.
Physician Network Academy
The Physician Network Academy membership community serves leaders focused on physician engagement, alignment, and cohesion—from Chief Medical Officers and Chief Transformation/Integration Officers to vice presidents, directors, and managers over the physician network or medical group.
888.700.5223
healthcarebusinessinsights.com





























