Embed Size (px)
Citation preview
Best Practices forProtecting EMS Responders
duringTreatment and Transport ofVictims of Hazardous Substance Releases
OSHA 3370-11 2009
Occupational Safety and Health Act of 1970“To assure safe and healthful working conditionsfor working men and women; by authorizingenforcement of the standards developed underthe Act; by assisting and encouraging the States intheir efforts to assure safe and healthful workingconditions; by providing for research, information,education, and training in the field of occupationalsafety and health.”
This publication provides a general overview of aparticular standards-related topic. This publicationdoes not alter or determine compliance responsibilitieswhich are set forth in OSHA standards, and theOccupational Safety and Health Act. Moreover,because interpretations and enforcement policymay change over time, for additional guidance onOSHA compliance requirements, the reader shouldconsult current administrative interpretations anddecisions by the Occupational Safety and HealthReview Commission and the courts.
Material contained in this publication is in the publicdomain and may be reproduced, fully or partially,without permission. Source credit is requestedbut not required.
This information will be made available to sensoryimpaired individuals upon request. Voice phone:(202) 693-1999; teletypewriter (TTY) number: 1-877-889-5627.
Best Practices forProtecting EMS Responders
during Treatment and Transport ofVictims of Hazardous Substance Releases
Occupational Safety and Health AdministrationU.S. Department of Labor
OSHA 3370-112009
Cover photo courtesy of Dr. John Hick
This document is not a standard or regulation, and it creates no new legal obligations. It containsrecommendations as well as descriptions of mandatory safety and health standards. The recom-mendations are advisory in nature, informational in content, and are intended to assist employers inproviding a safe and healthful workplace. The Occupational Safety and Health Act requires thatemployers to comply with safety and health standards promulgated by OSHA or by a state with anOSHA-approved state plan. In addition, the Act’s General Duty Clause, Section 5(a)(1), requiresemployers to provide their employees with a workplace free from recognized hazards likely to causedeath or serious physical harm. Employers may be cited for violating mandatory safety and healthstandards or other OSH Act requirements, including the General Duty Clause.
2
Occupational Safety andHealth Administration
Acknowledgements
Numerous individuals, agencies and organizationsassisted in the development of this publication.OSHA wishes to express its deepest appreciation tothe following for their significant contributions to thisguide.
American Ambulance AssociationAmerican Medical ResponseAgency for Toxic Substances and Disease Registry,
Emergency ResponseBoston Emergency Medical ServicesDepartment of Homeland Security,
Federal Emergency Management Agency,National Emergency Training Center
Emergency Nurses AssociationEnMagine, Inc.Hennepin County Medical Center,
Dept of Emergency MedicineElsevier Public Safety,
Journal of Emergency Medical ServicesNational Association of EMS EducatorsNational Association of EMS PhysiciansNational Institute for Occupational Safety and
HealthNew York City Fire DepartmentNorth Shore – LIJ Health System,
Center for Emergency Medical Services,Special Operations Division
Objective Safety, LLCU.S. Department of Health and Human ServicesU.S. Department of TransportationU.S. Environmental Protection Agency
The following agencies and organizations reviewedand provided comments:
Emergency Nurses AssociationEnMagine, Inc.Hennepin County Medical Center,
Department of Emergency MedicineNational Association of EMS EducatorsNational Association of EMS PhysiciansNational Association of State EMS OfficialsNational Institute for Occupational Safety and
Health, Emergency Preparedness andResponse Coordination Office
New Jersey Department of Health and SeniorServices, Division of EpidemiologyEnvironmental and Occupational Health
New York City Fire Department,Office of Medical Affairs
National Institutes of Health/National Instituteof Environmental Health Sciences,Worker Education Training Branch
North Shore – LIJ Health System,Center for Emergency Medical Services
Objective Safety, LLCU.S. Agency for Toxic Substances and Disease
Registry, Emergency ResponseU.S. Department of Homeland Security,
Federal Emergency Management AgencyU.S. Department of Health and Human ServicesU.S. Department of Transportation

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3
ContentsAcronyms 6
Executive Summary 7
Introduction 9
Scope and Objectives 9
Purpose 11
Organization of this Guide 11
Determinants of Training and PPE:Personnel Roles, Hazard Assessmentsand Emergency Response Plans 12
EMS Responder’s Role in the Community 12
Defining the EMS Responder Role inCommunity Response: Factors toEvaluate, Contacts, Information Sourcesand Special Considerations 12
The Value of Open Dialogue 14
The EMS Hazard Assessment 14
Requirement and Purpose 14
Sources of Hazard Assessment Informationin the Community 15
Include EMS Responder Health and SafetyExperience in Hazard Assessments 16
Incorporating EMS Responder Preparationinto an Effective Emergency Response Plan 16
Training 18
Background 18
Summary of Existing Training Guidelinesfor EMS Responders 18
Applicability of HAZWOPER Training toEMS Responders 18
EMS Responder Roles RequiringHAZWOPERTraining 20
First Responder Awareness Level Training 20Training Duration,Topics and Competencies 20Annual Refresher Training 21
First Responder Operations Level Training 21Training Duration 21Option to Demonstrate Competence 22Topics for Training or Demonstrationof Competency 22Annual Refresher Training 22Associated Training 22
Associated Training – PPE 23Associated Training – Respiratory Protection 23
Sources of Training and Curricula 23
EMS Responder Roles that RequireNo HAZWOPER Training 24
Skilled Support Personnel 24
Relevance of Other HAZWOPER TrainingLevels to EMS Responders 25
Conclusions Regarding EMSTraining 25
Personal Protective Equipment 26
Using OSHA’s Rationale for HazardAssessment and PPE Selection 26
PPE Selection Based on ReasonablyAnticipatedWorst-Case Scenarios 26
RequiredWritten Documentation forRespirator and PPE Selection Processes 27
Assessing the Need for Respiratory Protection 27
Respiratory Protection Required for EMSResponders 27
Types of Respiratory Protection Available 27
National Institute for Occupational Safetyand Health (NIOSH) Approval and Chemical,Biological, Radiological, Nuclear (CBRN)Certifications 28
Respiratory Protection for an Identified orCharacterized Hazard 28
Other Requirements Related to RespiratoryProtection 28
Gloves, Boots and Garments 28
Gloves and Boots 28
Protective Garments 29
Modifying PPE Selections Based onAvailable Information 30
Proper Size and Fit of PPE 31
Considerations for Effectively Using,Maintaining and Storing PPE 31
Conclusions Regarding Personal ProtectiveEquipment 31
Summary of OSHA’s Recommendationsfor Training and PPE 32
Best Practices for Pre-Transport PatientDecontamination 35
Removing Contaminated Clothing andPersonal Effects 35
Cleansing with Soap andWater 35
Assistance for Non-Ambulatory andAmbulatory Patients 36

4
Occupational Safety andHealth Administration
Decontamination in LowWater Situations 37
Vehicle and Equipment Decontamination 38
Discovering that a Patient in the Ambulanceis Contaminated 38
Detection Equipment 39
Detection Instruments 39
Ionizing Radiation Meters 39
Chemical and Biological Agent DetectionEquipment 40
Methamphetamine Detection Equipment 42
Conclusion 44
Appendix AGlossary 45
Appendix BReferences 48
Appendix CAdditional Sources of Information 54
Appendix DExamples of Mutual Aid Agreementsand Templates 55
Appendix EUsing Hazardous Substances EmergencyEvents Surveillance System (HSEES)Information in Community HazardEvaluations – A Review 56
Evaluation of Data from the Early 1990s 57
Rural/agricultural area compared to allother non-rural areas 58
Appendix FSpecial Considerations for ResponsesInvolving Methamphetamine Laboratories 59
Appendix GClandestine Drug Labs –First Responder Awareness Card 64
Appendix HTraining Curricula Options 66
Training Curricula for EMS Responders 66
Tips for Successful EMS ResponderHAZWOPER Training Programs 68
Appendix IHospital Incident Command System 69
Excerpt from Hospital Incident SystemGuidebook 69
Appendix J
Summary of Respirator Types andSelection Information 71
Summary of Respirator Types andCharacteristics 71
Advantages and Disadvantages of VariousTypes of Respiratory Protection 72
Advantages and Disadvantages of VariousRespirator Facepiece Styles 73
OSHA Assigned Protection Factors forRespiratory Protective Devices 74
Respirators for IDLH Atmospheres 75
Respirators for Atmospheres that areNot IDLH 75
Appendix KThermal Stress: Working inHot or Cold Environments 76
Heat Stress and Strain 76
Cold Stress and Hypothermia 76
Appendix LDecontamination Foam andBarrier Cream 77
Appendix MExamples of PPE Donningand Doffing Sequences 78
Appendix NGeneral Description and Discussion ofthe Levels of Protection and ProtectiveGear 79
Appendix OOccupational Health HazardExperience of EMS Responders 83
Background/Overview 83
Review of the Literature on Risks toEMS Responders 83
Experience of EMS Responders Exposedto Hazardous Substances 83
EMTs at the Tokyo Subway SarinGas Attacks 83
Hazardous Substances EmergencyEvents Surveillance (HSEES) Datafor EMS Responders 84
Other Reports of EMS Responder Injuryduring Hazardous Substance Releases 88
Risk to EMS Responders of Injury andIllness from Causes Other than HazardousSubstance Exposure 89
Appendix PIndustry Characteristics that AffectHow EmployersTrain and ProtectTheir Employees 92
The Roles of NHTSA and States 92
Applicability of Federal and State OSHAHAZWOPER Standards and OtherRegulations 93
The Influence of Overlapping OrganizationalDemographics of EMS Responders 93
Appendix QSources of Help in AddressingBiological Agent Issues 95
Concern about Needlesticks and BiologicalAgents 95
List ofTables
Table 1. Results of Simulation Tests onSeveral Chemical Suits 30
Table 2. Training, Respiratory Protection,and PPE for EMS Responders 32
Table E-1. HSEES Reported Event ParametersDuring 1993-2000 58
Table F-1. Reported MethamphetamineLaboratory Seizures, 1997-2005 59
Table F-2. Number and Percentages ofFirst Responders Who Sustained Injuriesduring Emergency Events Associatedwith Illicit Methamphetamine Laboratoriesby Type of Injury 61
Table F-3. Chemical Hazards Encountered atMethamphetamine Laboratories 62
Table J-1. Summary of Respirator Typesand Characteristics 71
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5
Table J-2. Advantages and Disadvantagesof Various Types of Respiratory Protection 72
Table J-3. Advantages and Disadvantagesof Various Respirator Facepiece Styles 73
Table J-4. Assigned Protection Factors 74
Table N-1. PPE Levels of Protection 80
List of Figures
Figure 1. How to Use Table 2 34
Figure 2. How to Do a Survey for Radiation 41
Figure F-1. Distribution of U.S. ClandestineMethamphetamine Lab Incidents byState – 2004 60
Figure O-1. HSEES Injury Disposition –for Hazardous Substances EmergencyEvents Surveillance in 2004 85
Figure O-2. Release Type for Incidents atWhich EMS Responders Were Injured(HSEES 2002-2007) 86
Figure O-3. Frequency of Specific SymptomsAmong EMT/EMS Injured at Scenes withHazardous Substance Release (HSEES2002-2006) 87
Figure O-4. Chemical Categories Associatedwith Hazardous Substance Release –Scenes at Which EMT/EMS Were Injured(HSEES 2002-2006) 87
OSHA Assistance 97
OSHA Regional Offices 99
6
Occupational Safety andHealth Administration
AcronymsAPF Assigned protection factor
APR Air-purifying respirator
ASR Atmosphere supplying respirator
ATSDR Agency for Toxic Substances andDisease Registry
CBRN Chemical, biological, radiological, ornuclear [agent or substance]
CBRNE Chemical, biological, radiological,nuclear, or explosive [agent or sub-stance]
CDC Centers for Disease Control andPrevention
CERCLA Comprehensive EnvironmentalResponse, Compensation, andLiability Act
CFR Code of Federal Regulation
EMS Emergency Medical Services
EMT Emergency medical technicians[of all levels]
ERP Emergency response plan
HAZCOM Hazard Communication(29 CFR 1910.120)
HAZMAT Hazardous material
HAZWOPER Hazardous Waste Operations andEmergency Response (29 CFR1910.120)
HEPA High efficiency particulate air[filtration system]
HICS Hospital Incident Command System
HSEES Hazardous Substances EmergencyEvents Surveillance
HVA Hazard vulnerability analysis
IDLH Immediately dangerous to lifeor health
ICS Incident command system
IC Incident commander
JCAHO Joint Commission on Accreditationof Healthcare Organizations
LEPC Local emergency planning committee
LERP Local emergency response plan
NFPA National Fire Protection Association
NHTSA National Highway Traffic SafetyAdministration
NIOSH National Institute for OccupationalSafety and Health
NIMS The National Incident ManagementSystem
NRC Nuclear Regulatory Commission
PPE Personal protective equipment
PAPR Powered air-purifying respirator
SCBA Self-contained breathing apparatus
SAR Supplied-air respirator
SERP State emergency response plan
TB Tuberculosis
TSCA Toxic Substances Control Act of 1976
See Appendix A for glossary of terms

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7
Executive Summary
In 2005, OSHA published the Best Practices forHospital-Based First Receivers guide that providedguidance for those healthcare facilities that receiveand treat victims of hazardous substance releases.At the request of stakeholders that participated inthe development of that guide, OSHA has devel-oped a similar guide for emergency medical service(EMS) responders who provide medical assistanceduring an incident involving a hazardous substancerelease. This guide is intended for employers ofEMS responders and discusses the measures theseemployers need to take to protect their EMS respon-ders from becoming additional victims while on thefront line of medical response.
ScopeEMS responders are broadly defined here as theindividuals who provide pre-hospital emergencymedical care and patient transportation. Some EMSresponders are also assigned duties that supportpatient care, including patient decontamination. Forthe purpose of this guide, the term EMS responderrefers to all levels of emergency medical personnelinvolved in incident response (e.g., emergency med-ical technicians [EMTs], paramedics, and others whoperform similar duties). While many EMS respon-ders are cross-trained (e.g., EMT and firefighter),this guide applies to these workers only when theyare functioning as EMS responders.
The Employer’s RolePreplanning helps employers ensure that theirworkers have adequate training and personal pro-tective equipment (PPE) for the incidents in whichthe workers are expected to participate. Criticalsteps for the employer involve determining the EMSresponder’s expected role in a reasonably anticipat-ed worst-case scenario, identifying the hazards thatare associated with the EMS responder’s assignedduties, and developing an emergency response plan(ERP) that spells out how the EMS responder will beprepared (through training and PPE) to safely fulfillthose duties (OSHA Instruction CPL-02-02-073,Emergency Responses to Hazardous SubstanceReleases, Aug. 27, 2007).
OSHA’s RecommendationsOSHA’s recommendations on minimum trainingand PPE for EMS responders assisting patients athazardous substance release sites generally followregulatory requirements contained in paragraph (q)of OSHA’s Hazardous Waste Operations and
Emergency Response (HAZWOPER) standard (29Code of Federal Regulations [CFR] 1910.120) andassociated guidelines and interpretive letters. Insome instances, OSHA also recommends that, as abest practice, employers consider offering instruc-tion to certain EMS responders who would not oth-erwise receive HAZWOPER training under regulato-ry requirements, but who OSHA believes might findthemselves in a situation where this training wouldallow them to make better decisions to protect boththemselves and other EMS personnel.
Table 2 at pg. 32 of this guide summarizes theserequirements and best practices for EMS respon-ders who might be assigned to assist patients undercertain situations.
For example, if an EMS responder would beassigned to provide:
• medical assistance in an environment that ispotentially immediately dangerous to life andhealth (IDLH), whether in the hot or the warmzone, then the employer must provide HAZWOP-ER first responder operations level training, aself-contained breathing apparatus (SCBA) asrespiratory protection and Level A or Level BPPE, in accordance with OSHA requirements (29CFR 1910.120(q)(3)(iv) and Appendix B of thatstandard). This level of protection may be modi-fied by the incident commander (IC) as informa-tion becomes available. By definition, activitiessuch as treating contaminated patients anddecontaminating patients occur in the warmzone. The hot, warm, and cold zones are definedin Appendix A.
• medical assistance only in the cold zone, assist-ing uncontaminated or thoroughly decontami-nated patients during a hazardous substancerelease event, then OSHA strongly recommendsthat, as a minimum, employers provide HAZ-WOPER first responder awareness level training.OSHA also suggests that the next higher level ofHAZWOPER training, first responder operationslevel, be provided to these workers as an appro-priate “best practice” because of the possibilityof incomplete decontamination or inaccuratetriage performed by others. Regardless of thelevel of training, the minimum respiratory pro-tection for workers in the cold zone would beonly that needed for infection control purposes.
• emergency transport for uncontaminatedpatients during emergencies involving an IDLHenvironment or the release of an unknown/
8
Occupational Safety andHealth Administration
uncharacterized hazardous substance, thenOSHA strongly recommends HAZWOPER firstresponder awareness level training or, preferablyfirst responder operations level training.
• uncontaminated patient transport at an incidentonly after the hazardous substance is adequatelycharacterized, OSHA recommends that theseworkers receive hazard communication training,or as a best practice, first responder awarenesslevel training. The minimum respiratory protec-tion would be only that needed for infection con-trol purposes.
• inter-facility transport only (i.e., never respond to911 calls), then if such a worker is unexpectedlycalled upon to respond to an emergency involv-ing a hazardous substance release, OSHArequires that the worker must be trained as“skilled support personnel” (29 CFR1910.120(q)(4)). The employer should confirmthat no contracts or cooperative arrangementsexist that could result in workers responding tothe site of an emergency involving a hazardousmaterial. Such agreements would indicate thatthese duties are expected, and, therefore, theresponders should be appropriately trained inadvance.
Best Practices Guide ContentThe first section of this guide offers employers sug-gestions for obtaining information that will helpthem determine the roles that their workers mayplay in an emergency response. This section alsoprovides information to help employers assess thehazards their workers may encounter in the event ofa hazardous substance release incident. This sectionconcludes with identifying information that shouldbe included in the ERP.
The next two sections provide best practices ontraining and equipping EMS responders duringtreatment and transport of potentially contaminatedvictims. Table 2 presents best practice recommen-dations for levels of training and PPE for EMSresponders. Employers may incorporate these train-ing and PPE levels into their ERPs, citing this bestpractices document as the basis for those selec-tions.
A final section addresses hazardous substancedecontamination. Although EMS responders mightnot be assigned to a community’s decontaminationteam, they should understand the process if theyare to recognize ineffective decontamination proce-dures that could result in improperly decontaminat-ed patients – patients that EMS responders could beexpected to treat and/or transport. Furthermore,OSHA believes that during a mass casualty incident,EMS responders could be assigned to assist withdecontamination and would need to know how toperform effective patient decontamination.
Appendices to this guide provide supplementalinformation and examples related to issues raisedby this guide.
The Web site URLs cited in this document wereeffective as of the date of publication. Be awarethat URLs are often changed. If the Web siteURL does not work, go to the home page of theorganization. This can usually be done bydeleting all of the URL characters after the firstforward slash. For instance, if the site ishttp://www.cdc.gov/niosh/docs/2005-100/, thehome page would be located at www.cdc.gov.You may then be able to find the web page ofinterest by following links on the home page.
Introduction
Emergency medical services (EMS) responders area critical part of the nation’s emergency responsesystem and the front line of medical response. Theyprovide medical treatment at the scene of an inci-dent and are often among the first group of respon-ders to arrive. As a result, EMS responders are alsolikely to be present on the scene before hazards arebrought fully under control and before situationalawareness is complete. Incident sites routinely con-tain evolving hazards that can harm emergencyresponders. This Best Practices document address-es the special conditions presented by dangeroussubstances released at the site of an emergencyresponse and discusses the measures employersneed to take to protect their EMS responders frombecoming additional victims at sites involving haz-ardous substances.
This guide offers the employers of EMS respon-ders suggestions on how to determine the rolestheir workers will perform in the event of a haz-ardous substance release incident. Employers areexpected to protect their EMS responders bypreparing them for their roles in hazardous sub-stance response with appropriate training and PPE.Worker training and PPE provided should corre-spond, so that each EMS responder is equippedwith PPE that will allow that employee to work safe-ly in the role for which he or she is trained.
The basic steps for achieving appropriate EMSworker protection include:1) The employer determines the EMS responder’s
expected role in reasonably anticipated worst-case scenarios.
2) The employer conducts a hazard assessment toidentify the anticipated hazards associated withthe EMS responder’s role.
3) The employer develops an ERP that spells outhow the EMS responder will be prepared tosafely perform the responder’s anticipated role.The plan should indicate the level of trainingthat the EMS responder should receive and thetype of PPE that will be provided to that respond-er.This document consolidates existing OSHA poli-
cy and guidance on training and PPE for EMSresponders and is intended to help EMS respon-ders save lives without becoming additional vic-tims.1
Scope and ObjectivesEMS responders are broadly defined here as theindividuals who provide pre-hospital emergencymedical care. EMS responder activities can encom-pass all levels of patient emergency care, treatment,or transport provided at the incident location orbetween that location and the receiving hospital orother healthcare facility (i.e., inter-facility transporta-tion). Depending on the community in which theyserve, some EMS responders are also expected toassist with other related duties that support patientcare, including patient decontamination.
EMS Responders: For the purposes of this docu-ment, the term EMS responder refers to all levels ofemergency medical personnel involved in incidentresponse. Thisgroup includesemergency medicaltechnicians (EMTs)of various levels,paramedics, andothers who performthe duties of anEMT or paramedic,regardless of their job title or employment status.These individuals serve as the “public’s emergencymedical safety net” and will continue to do so asthe EMS system evolves in the future (NHTSA,2000).2
These recommendations are best suited forthose individuals for whom providing medicalcare is a primary mission. Others may benefitfrom these recommendations, but might alsohave additional training that expands their capa-bilities during emergencies involving hazardousmaterials.
This best practices document is not intended toadvise other responders (e.g., firefighters,police) when they perform work beyond theduties of an EMS responder.
AllWorkers Functioning as EMS Responders:This guide is intended for employers of EMSresponders of all types. This document is equallyrelevant to EMS responders who are volunteers,full- or part-time workers, and personnel of agen-
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9
1 The existing OSHA policy and guidance appear in OSHAstandards and letters of interpretation cited throughout thisdocument.
2 From: NHSTA, undated. EMS Education Agenda for theFuture. Last accessed May 19, 2007. Available at www.nhtsa.dot.gov/people/injury/ems/EdAgenda/final/agenda600.htm#core.
Phot
oco
urte
syof
Jenn
iferLy
den

cies, fire departments, or hospitals while they areproviding the services of an EMS responder at anincident site or during patient transport.3 Al-thoughmany EMS responders are cross-trained or holdmultiple qualifications (e.g., EMT and firefighter orHAZMAT team member), OSHA considers thisguide relevant to these individuals only while theyare performing the duties of an EMS responder. It isnot applicable when an EMS responder who iscross-trained as a firefighter or HAZMAT teammember is performing work to fight a fire or “han-dle or control actual or potential leaks or spills ofhazardous substances requiring possible closeapproach to the substance.”
Hazardous Substance Release: Emergencyresponse to a hazardous substance release isdefined here as it is in OSHA’s Hazardous WasteOperations and Emergency Response (HAZWOPER)standard:
“…a response effort by employees from out-side the immediate release area or by otherdesignated responders (i.e., mutual aidgroups, local fire departments, etc.) to anoccurrence which results, or is likely to result,in an uncontrolled release of a hazardous sub-stance. Responses to incidental releases ofhazardous substances where the substancecan be absorbed, neutralized, or otherwisecontrolled at the time of release by employeesin the immediate release area, or by mainte-nance personnel are not considered to beemergency responses within the scope of this[HAZWOPER] Standard. Responses to releasesof hazardous substances where there is nopotential safety or health hazard (i.e., fire,explosion, or chemical exposure) are not con-sidered to be emergency responses” (29 CFR1910.120(a)(3)).
OSHA acknowledges the dynamic tension thatexists between the need to provide expedientmedical treatment (including taking patients to asite where they can receive more advanced care)and the need to protect the medical care provider.
This document focuses on reasonably anticipat-ed worst-case scenarios with the understandingthat these situations will be relatively rare.Nevertheless, the associated preparation willbenefit employers and EMS responders any timepatients require emergency medical assistance atthe scene of a hazardous substance release.
Hazards and Routes of Exposure: This guidespecifically covers protection for EMS respondersduring responses to releases of chemicals, radio-logical particles, and biological agents that result inpatients who may need emergency on-scene med-ical care, decontamination, and/or transportationfrom the scene of the release to the hospital. Whensuch hazardous substances are present, EMSresponders may become exposed to the sub-stances through direct airborne or physical contactwith the contaminant at the scene, or through sec-ondary contact while caring for a patient whobecame contaminated with the substance at thescene.4
At the Scene of the Release: This guide focuseson protecting EMS responders who answer re-quests for emergency medical care at (or in closeproximity to) the scene of the hazardous substancerelease. For this purpose, OSHA has placed anemphasis on EMS response to a release of harmfulchemicals, radiological materials, or biologicalagents – such as an anthrax spore powder – duringthe initial release (i.e., when the release is discov-ered at the time of the incident). This documentdoes not address cases where the scene of therelease is unknown, or where the scene was identi-fied only later through epidemiological methods,when EMS responders would no longer be requiredat the scene. Furthermore, this document does notcover EMS responder protections for infectiousagents when a release is identified retrospectivelyonly after the identification of sick individuals. Thislatter category includes infectious agents such asthose causing highly pathogenic avian influenza,severe acute respiratory syndrome (SARS), plague,smallpox, or tularemia, when spread by natural,insidious, or clandestine release.5 In these cases,OSHA recommends that employers consult CDC for
1 0
Occupational Safety andHealth Administration
3 See Appendix P for further discussion of OSHA jurisdictionover public employees.
4 Hazardous substance is defined as any substance exposurethat may result in adverse effects on the health or safety ofemployees. This includes substances defined under Section101(14) of CERCLA; biological or disease-causing agents thatmay reasonably be anticipated to cause death, disease, orother health problems; any substance listed by the U.S.Department of Transportation as hazardous material under 49CFR 172.101 and appendices; and substances classified as haz-ardous waste. See 1910.120(a)(3).5 As a special case, release of an infectious disease would becovered by this document if a known intentional or accidentalrelease occurred at a known location, so that an incident sceneis recognized at the time of the release. As a rule of thumb, akey test is the question: “Would immediate surface or victimdecontamination affect the course of the incident?” If theanswer is “no”– because victims who were at the scene havealready become infected – then CDC guidelines for handlinginfectious disease incidents will be more relevant than thesebest practices from OSHA.
information on EMS responder protections. For abrief discussion of biological agents and a list ofuseful Web sites, see Appendix Q – Sources of Helpin Addressing Biological Agent Issues.
PurposeEmployers of EMS responders will find this docu-ment useful during development of hazard evalua-tions and ERPs. The purpose of this guide is toestablish best practices that EMS employers canimplement to help EMS responders save lives with-out becoming additional victims. To this end, thedocument will help inform employers about:
• The relevance of OSHA’s HAZWOPER standardto EMS responders.
• Methods for obtaining information on the typesof hazardous substance release events that thelocal community is preparing to address.
• The importance of identifying responder rolesand responsibilities in the community (includingthose under mutual aid agreements).
• Important topics to consider while developingan ERP.
• OSHA’s recommendations and requirements fortraining and PPE when EMS responders’ rolesinclude the potential for response to incidentsinvolving hazardous substance(s).
Organization of this GuideOSHA’s Best Practices for Protecting EMSResponders during Treatment and Transport ofVictims of Hazardous Substance Releases is
organized into seven sections, including thisintroduction and a brief conclusion.
The next sections provide background andsupport for OSHA recommendations on trainingand PPE (including respiratory protection) forEMS responders who could reasonably be antici-pated to respond to an event involving a haz-ardous substance release.
A summary of training and PPE is then provid-ed with a summary table (Table 2) to look up therecommended minimum training and PPE neededfor EMS responders assigned to specific roles andunder a range of anticipated conditions. Employ-ers may cite this information when conductinghazard evaluations required by OSHA standardson respiratory protection and PPE. See Figure 1 atpg. 34 for simple instructions on using the sum-mary table.
The final section reviews topics related topatient and responder decontamination. AlthoughEMS responders in many communities are notroutinely assigned to decontamination teams,they need to be prepared to identify improper orinadequate decontamination in patients theyreceive. Additionally, OSHA believes that it isnaive to assume that some EMS responderswould not be tasked with decontamination duringan event that involves mass casualties.
This guide is supplemented with appendicesthat provide additional details on topics intro-duced in the text, including a detailed glossaryand a list of the references cited throughout thedocument and its appendices.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 1 1
Determinants of Trainingand PPE: Personnel Roles,Hazard Assessments andEmergency Response Plans
OSHA considers appropriate worker preparation toencompass both training and PPE. To determinenecessary training and PPE, the employer mustunderstand all workers’ roles and the associatedhazards. EMS responders should be adequatelytrained for their role in emergency response duringhazardous substance events. Furthermore, eachworker’s training and PPE should be compatible, sothat the EMS responder is equipped with PPE thatwill allow that individual to work safely in the rolefor which that he or she is trained.
The basic steps for determining necessary train-ing and PPE include:1) The employer determines the EMS responder’s
expected role in a reasonably anticipated worst-case scenario.
2) The employer conducts a hazard assessment toidentify any anticipated hazards associated withthe EMS responder’s role during such a re-sponse.
3) The employer develops an ERP that spells outhow the EMS responders will be prepared tosafely perform their anticipated roles. The planshould indicate the level of training that the EMSresponders should receive and the type of PPEthat will be provided to those responders.This section outlines regulations, information
sources and prudent practices that shape employ-ers’ decisions about EMS responder preparation.The decisions that employers make about EMSresponder roles, training and PPE should be out-lined in the employers’ ERPs.
EMS Responder’s Role in the CommunityOSHA standards and letters of interpretationrequire employers to tailor EMS responder trainingand PPE to (1) the duties that EMS responders are“expected” to perform, and (2) the expected haz-ards that EMS responders can reasonably be antici-pated to encounter while performing those duties.Thus, both the duties and the hazards must bedefined in order to reasonably establish trainingand protection for an EMS responder.
If multiple persons are down (i.e., incapacitated)in a public area and there is no obvious trauma,then [a HAZWOPER trained EMS responder]
should immediately suspect a chemical expo-sure or attack. EMS responders without properPPE should never enter such an area, or if theydo enter before realizing the problem, theyshould immediately exit while only removingthose closest to the exit (OSHA StakeholderComments, 2006).
Specifically, in a 1991 letter of interpretationOSHA clarified that EMS personnel should betrained in accordance with the responsibilities theywill be expected to assume during an emergencyresponse as described in the community emer-gency response plan (OSHA, 1991-McNamara).Furthermore, OSHA’s Personal ProtectiveEquipment standard requires that the employerselect appropriate PPE based on the hazards thatare present, or likely to be present, including fore-seeable emergencies (see Personal ProtectiveEquipment for additional information on requiredwritten documentation associated with the PPE andrespiratory protection selection processes). Whenspecific hazards cannot be identified in advance,OSHA expects that employers will consider the rea-sonably anticipated “worst-case employee expo-sure scenarios” (OSHA, 2002-Hayden).
The following two sections discuss factors thatemployers of EMS responders should considerwhen evaluating their workers’ roles in emergencyresponse events and the hazards that EMS respon-ders encounter while performing their jobs.
Defining the EMS Responder Role in CommunityResponse: Factors to Evaluate, Contacts,Information Sources and Special ConsiderationsThe employer is ultimately responsible for deter-mining the duties to which individual EMS respon-ders could be assigned. By defining workers’ rolesto address community expectations, the employerwill be better able to anticipate how to prepare theirEMS responders for these roles and any associatedhazardous conditions.
As a first step toward identifying EMS responderroles, the employer should determine whether ornot its workers would be made available to respondto an emergency. For some employers of EMSresponders involved in 911 response this is an easydecision. Other employers might find this more dif-
1 2
Occupational Safety andHealth Administration

ficult to answer. For instance, some employersmight employ EMS responders who never respondto an emergency, but rather work as inter-facilitytransport EMTs, transferring patients between med-ical facilities. As a guideline, OSHA recommendsthat employers train and prepare their workers torespond to an emergency if the employers areparty to existing contracts (e.g., with the county ormunicipality) that call for the employers to partici-pate in emergency response in the event of a disas-ter. Furthermore, if employers are covered by a dis-aster mutual aid agreement or cooperative arrange-ment with other emergency services providers orcommunities, then the employers should preparetheir workers accordingly.
Having determined that their workers mightrespond to an emergency, employers should findout how and under what circumstances the com-munity expects the EMS providers to respond. Thisinformation will help employers determine the rolesto which they will assign their personnel.
“The emergency response plan for the jurisdictionshould clearly define who will be responsible fordecontaminating victims during an emergencyresponse.The emergency medical service person-nel should be trained in accordance with theresponsibilities they will be expected to assumeduring an emergency response as described in thecommunity emergency response plan.” (OSHA,1991-McNamara).
Employers of EMS responders can easilydescribe their workers’ day-to-day duties, but theymight find it more difficult to anticipate the actionsand hazards associated with EMS responder dutiesin the event of a mass casualty event, in the face ofa new threat, or during a large-scale disaster involv-ing several communities. These roles are typicallybased on community emergency response plan-
ners’ decisions, which are in part based upon per-ceived risks, resources, availability of other respon-ders, and to some extent, the influence or percep-tions of the broader community (e.g., citizens, busi-nesses, news media).
By understanding the needs and expectations ofcommunity leaders, emergency planners, otherresponders, and typical citizens, employers can bet-ter anticipate how and where they may be asked toengage their workers under various emergency cir-cumstances.
The expectations of the community (as express-ed by its emergency planners) may be assessedfrom several perspectives:
• What role does the community expect an indi-vidual EMS service provider to fill?
• What actions and tasks does the communityexpect EMS responders to fill?
• Under what circumstances will these responsi-bilities be performed?
• Where within the continuum of hazard responsezones does the community expect EMS respon-ders to respond?
• What actions does the community expect theEMS responder to take when they encountercontaminated patients?
• Does the community provide detection equip-ment and expect EMS responders to use it (e.g.,ionizing radiation detectors, chemical detectors)?
• How many EMSresponders, if any,need to be pre-pared to functionin the most dan-gerous areas (e.g.,the hot zone) com-pared to the num-bers of EMSresponders needed in areas with reduced or nopotential for hazardous substance exposure? Arean adequate number of properly trained andequipped fire- or HAZMAT-team based EMSresponders available to fill this need?
• What additional training is required to prepareEMS responders to meet possible situationsthey could encounter during emergencyresponse?
• Who will treat patients in the warm zone?
Specifically, the EMS employer should workwith the local emergency management agency,Local Emergency Planning Committee (LEPC), fire
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 1 3
Phot
oco
urte
syof
Fran
kCal
ifano
Phot
oco
urte
syof
Jenn
iferLy
den
department, HAZMAT team, police, and otherresponse partners consistent with the state andlocal government structure, to determine:
• Who will be performing decontamination activi-ties and to what extent?
• Who will remove victims from the hot zone?
• Who will treat victims trapped in a dangerousarea?6
• Who will transport patients removed from thescene once first responders assess them?
• Who will be available as backup, if needed?
As an additional step, it is important to workwith the community to define expectations of wherein the danger continuum (from release site to a safeand clean area) the EMS responders could performtheir designated tasks.
Unless they have addressed these questions inadvance with the community, employers of EMSresponders will find themselves making difficultdecisions at the last minute under emergency con-ditions. Undefined or unwritten expectations canhinder EMS providers’ ability to make good deci-sions and might result in responders arriving on thescene unprepared or poorly equipped.
“Whatever roles are chosen, it should be clearthat SOME agency in the community has theresponsibility and training to provide patientcare in the warm zone (at least) and is properlyequipped to do so. This could be an issue if thecommunity has a fire department without med-ical responsibilities/training and they are the onlyones with Level B PPE.” (OSHA StakeholderComments, 2006).
The Value of Open DialogueCommunity planners should ensure that EMSresponders participate in discussions of emergencypreparedness and exercises involving mutual aid.The better the community’s organizations and itscitizens understanding of the strengths and limita-
tions of their EMS system, the more realistic thecommunity’s expectations will be during an actualemergency. Additionally, employers that fosteropen and trusting dialogue between themselvesand these community groups during day-to-dayoperations will find it easier to share valuable infor-mation in times of crisis. In the midst of a disaster,that shared information might help remind commu-nity members of both the greatest strengths andthe realistic limitations of their EMS responders.This could help protect employers from being pres-sured by the demands of unrealistic communityexpectations into providing EMS responders foractivities for which they are not properly trained orequipped.
Background information for media might includeanswers to:• Why are some responders equipped and
trained to one level, while others are preparedat a different level? How does this benefit thecommunity?
• What are the benefits and limitations of differ-ent types of protective equipment that an EMSresponder might use?
• Which categories of responders provide rescuein hazardous areas, and why were they select-ed for this role?
A specific example of a proactive practice forcommunication would be employers who promotedialogue with the media. Emergency responders,including EMS responders, can help media repre-sentatives before a disaster occurs by providinguseful background information to help the mediaunderstand how EMS responders work and whatconditions put them at undue risk. It is also impor-tant for citizens to understand how the risk to thecommunity increases when EMS responders andambulances must be taken out of commission dueto contamination, injury, or illness. Employersmight consider training media spokespersons whocan help disseminate this message. During anemergency, however, communication with themedia must be with one voice through the incidentcommand system (ICS) structure.7
The EMS Hazard AssessmentRequirement and PurposeEmployers must conduct hazard assessments toidentify the expected hazards associated with EMS
1 4
Occupational Safety andHealth Administration
6 Also attempt to answer questions such as, “In this communi-ty, where is the line drawn between attempting to save a vic-tim and maintaining the safety and health of the EMT (…and ofthe second EMT who would attempt to save the first EMT)?” Isthat line set at a realistic point? Clearly defined expectationshelp employers communicate these expectations to employ-ees, who may require supportive training. It is counterintuitivefor a medic (regardless how unqualified) to stand back andNOT respond to a victim in need of rescue. In a hazardous sub-stance incident, however, the danger may be increased ifunqualified individuals respond unsafely. EMS respondersmust be trained and equipped to safely perform their duties inthe environments they will encounter.
7 The Hospital Incident Command System (HICS), an ICS forhospital/healthcare organizations is described in Appendix I.

responders’ roles in responses to reasonably antici-pated worst-case scenarios in the community. Thesehazard assessments are required, for example, byOSHA’s Personal Protective Equipment standard(1910.132(d)(2)) and give the employer the informa-tion needed to select PPE (i.e., eye, hand, foot, headprotection) that is suitable for the EMS responders’work conditions. The employer must produce awritten certification that the hazard assessment hasbeen conducted (see page 27 for further discussionof the necessary documentation).
EMS responders must also consider anticipatedairborne hazards when selecting respiratory protec-tion for EMS responders. Factors to considerinclude identifying the substance, making a reason-able estimate of exposure levels, and predicting thecontaminant’s chemical state and physical form.When it is not possible to identify the contaminantor estimate worker exposure levels, the employermust consider the atmosphere to be immediatelydangerous to life and health (IDLH). (29 CFR1910.134(d)(1)(iii)). As discussed in the section,Summary of OSHA’s Recommendations for Trainingand PPE, both PPE and respiratory protection areprescribed for IDLH environments by the HAZWOP-ER standard, which requires an SCBA respirator andLevel A or Level B PPE, as defined by Appendix B ofthe HAZWOPER standard.
Not all EMS responders must be equipped towork in an IDLH environment. In particular, EMSresponders may wear lower levels of respiratoryprotection and PPE in areas where the IncidentCommander has determined that an IDLH environ-ment does not exist. In that case, EMS respondersmust wear respiratory protection and PPE at least asprotective as that which the Incident Commanderhas determined necessary to protect them from thehazards that exist in the area. Frequently, the PPEand respiratory protection permitted at these timesis less cumbersome, more comfortable, and lesscostly than that required for work in IDLH environ-ments.
It is for the purpose of identifying protectiveequipment suitable for these reduced hazard situa-tions that the employer must perform the mostdetailed hazard assessments and respiratory hazardevaluations. The information they gather will helpemployers who wish to equip their EMS respondersin this manner with the information needed tochoose respiratory protection and PPE that will pro-vide reasonable protection under the range of non-IDLH conditions workers are most likely toencounter in their assigned roles. Fortunately,although the employer is ultimately responsible forensuring that its EMS responders are adequately
protected, much of the information needed to selectthe protective equipment is available from othersources within the community.
Sources of Hazard Assessment Informationin the CommunityNumerous resources are available to employers ofEMS responders regarding hazards for which thecommunity expects to prepare. In seeking hazardassessment information, employers should placeemphasis on obtaining information most relevant toEMS responders. One particularly good place tostart, which does not require original research, iswith a local hospital’s Hazard Vulnerability Analysis(HVA).8 Drawing on the hazard assessment findingsof other organizations and experts will save timeand speed the process of determining what trainingand PPE are necessary, as well as aiding in the cre-ation of the employers’ ERP.
LEPCs are community planning organizationsthat most likely have as members employers ofEMS responders and other experts involved inemergency management.9 There is no requirementfor a community to form an LEPC, but there are anumber of benefits including access to low or no-cost training and other preparedness activities. Oneof the requirements LEPCs must fulfill is to conducta community hazard assessment. The HazardousMaterials Emergency Planning Guide, publishedby the National Response Team and available at:www.nrt.org, provides guidance on how to performthese assessments. This process may help employ-ers prepare their own hazard assessment if neces-sary. Where mutual aid agreements increase thepossibility of EMS personnel responding to other
8 The Joint Commission on Accreditation of HospitalOrganizations (JCAHO) requires that accredited hospitalsdevelop and review an HVA. In a 2004 survey, 84 percent of575 hospitals reported having completed a collaborative threatand vulnerability analysis of the community (Barbara et al.,2006). When asked, “Do you perceive your hospital to be atincreased risk for any of the following hazards or threats(check all that apply),” 76 percent of the 575 respondents listed“hazardous materials” as a perceived risk at their hospital,while 47 percent listed “terrorism” and 26 percent listed“nuclear concerns.” For comparison, risks associated withsevere weather (e.g., floods, tornados, and winter storms)were mentioned by 42 percent, 62 percent, and 67 percent ofthe hospitals, respectively. Describing a weakness of the study,the authors reported that slightly more than half of the hospi-tals that responded to the survey were located in urban areasand 35 percent were trauma centers. Small, rural, and unac-credited hospitals were less likely to have responded and sothey were underrepresented in the survey results. A lack of his-toric experience with certain types of events (e.g., terrorism)also limits the strength of this subjective information.9 Visit http://yosemite.epa.gov/oswer/lepcdb.nsf/HomePage?openForm to see listings for LEPCs by location.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 1 5
communities, employers should also consider thehazards which those other communities perceive asincreased risks.
Information provided by community memberscan be used to concentrate or supplement areas ofconcern suggested by public information sources,such as the Hazardous Substances EmergencyEvents Surveillance (HSEES) system database.10
Review of these data suggest the types of substancerelease incidents most likely to result in exposuresand casualties (Hall et al., 1994; Hall et al., 1995; Hallet al., 1996; Berkowitz et al., 2004; Kaye et al., 2005).Appendix E contains a summary of these analyses.When reviewing the HSEES information, however,employers should note that some of the HSEESdata analyses and similar sources predate theSeptember 11, 2001 attack on the World Trade Centerand do not include consideration of terrorism.
Other sources of information on community haz-ards include:• Local HAZMAT teams.
• EPA’s Envirofacts (www.epa.gov/enviro/index_java.html).
• The spill reports database of the NationalResponse Center (available through www.nrt.orgor at www.nrc.uscg.mil/index.html).
• Community right-to-know information availablefrom the LEPC or the State Emergency ResponseCommission.
• National Fire Incident Reporting System avail-able from the U.S. Fire Administration atwww.usfa.dhs.gov/fireservice/nfirs.
Other local organizations can also provide infor-mation gathered from their activities. Examples ofthese resources include the local or state fire mar-shal, local health authorities, and county agricultureagents. On a national scale, the Homeland SecurityCouncil and U.S. Department of Homeland Securityhave published a list of 15 scenarios, considered“the worst-case” situations for which the nationneeds to prepare. Hazardous substance release isamong them (Homeland Security Council, 2005).While these scenarios may be too broad for individ-
ual employers to use in planning to protect EMSresponders, the employers may find these scenariosreferenced in community plans.
Include EMS Responder Health and SafetyExperience in Hazard AssessmentsOSHA permits the use of industry and companyexperience in the hazard assessment. Appendix O –Occupational Health Hazard Experience of EMSResponders – contains information on the publishedexperiences of EMS responders, both during haz-ardous substance release events and during routineresponses. When conducting hazard assessmentsfor EMS responders, employers may draw upon thisinformation, then supplement it with informationrelated to anticipated local conditions. Theseemployers may also incorporate information ontheir own health and safety experience (e.g., fromoccupational injury and illness records or otheremployer records).
Incorporating EMS ResponderPreparation into an EffectiveEmergency Response Plan
Emergency response plans describe policies andprocedures developed by employers, based on theroles EMS responders will serve and the hazardassessments associated with these roles in the com-munity. An OSHA compliance instruction notes thatif employers have chosen to have their own workersrespond to releases that would require an emer-gency response, the employers must develop emer-gency response capabilities that are appropriate totheir individual situations (OSHA, 2007-CPL-02-02-073). Employers’ ERPs must describe the steps thatthe employers have taken to prepare all of theirworkers (in this case EMS responders) who wouldbe expected to respond in the event of a hazardoussubstance release.
Employers must have an ERP that explains whatsteps are being taken to be sure that all of theirEMS responders:• Are adequately trained for their intended job
duties.• Are properly equipped for the intended tasks.• Are capable of responding in a safe manner.• Are managed by competent leaders.
(OSHA CPL-02-02-073, 2007)
In evaluating ERPs, OSHA looks for signs of aneffective program, including (but not limited to):
10 Also in 1989, the Agency for Toxic Substances and DiseaseRegistry (ATSDR) implemented an active state-based haz-ardous substances emergency events surveillance system(HSEES) in an attempt to adequately characterize the publichealth consequences of hazardous substance releases. A haz-ardous substance emergency event is defined as uncontrolledor illegal releases or threatened releases of chemicals or theirhazardous by-products. The HSEES database collects informa-tion on events, chemicals, victims, injuries and evacuations.Analysis of the HSEES data helps identify risk factors associat-ed with hazardous substances releases.
1 6
Occupational Safety andHealth Administration
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 1 7
• Pre-emergency planning and coordination, suchas integration with a local or state emergencyresponse plan (LERP or SERP).
• Identification of the types of hazardous sub-stance release emergencies that would requireresponse.
• Clearly defined personnel roles.
• Clear lines of communication.
• Worker training that is consistent with theirroles.
• Procedures to be followed if personnel or equip-ment require decontamination.
• Selection of PPE for personnel performingdecontamination.
• An inventory of PPE and emergency responseequipment, including instructions for use, theirlimitations, and the circumstances under whichthey will be used.
• Procedures for critiquing responses (to helpimprove future responses).
The previous sections suggested methods employ-ers can use to identify their workers’ anticipatedroles in emergency responses involving hazardoussubstance releases. The following sections are in-tended to help employers consider the HAZWOPERtraining and PPE needs of their EMS respondersbased on their anticipated roles and responsibilities.

1 8
Occupational Safety andHealth Administration
Training
BackgroundSummary of Existing Training Guidelinesfor EMS RespondersThe U.S. Department of Transportation’s (DOT),National Highway Traffic Safety Administration(NHTSA) developed a National StandardCurriculum (NSC) for EMTs at all provider levels.These guidelines constitute the basic nationalentry-level training requirements for EMS respon-ders, accepted by most states, while leaving theoption for state and local authorities to tailor theguidelines to best meet local needs. NHTSA’s NSCintroduces the topic of hazardous substances andresponse associated with hazardous substancereleases, but does not automatically prepare EMSresponders to meet the expected levels of compe-tence required by OSHA’s HAZWOPER standard,nor does it provide information relevant to localcommunity emergency response plans (OSHA,2004-Gantt). To meet the requirement for emer-gency first responder HAZWOPER training at eitherthe awareness or operations level, the trainer must:• Augment the NSC with additional hazardous
substance response information.
• Tailor the training to the individual worker’sassigned duties.
• Augment the operations level training durationto meet minimum HAZWOPER requirements(see Training Duration, below [for FirstResponder Operations Level]).
Other organizations also offer supplementaltraining for EMS responders. Examples include thetraining activities for DOT’s Hazardous MaterialsEmergency Preparedness program, the FederalEmergency Management Agency’s (FEMA)Emergency Management Institute course offerings,and the National Institute of Environmental HealthSciences’ (NIEHS) Worker Environmental TrainingProgram. These programs also require tailoring toinclude local community response plans to ensurethat EMS responders understand their assignedduties.
Applicability of HAZWOPER Training toEMS RespondersThe scope of paragraph (q) of OSHA’s HAZWOPERstandard (or the parallel state standards in stateswith OSHA-approved State Plans) covers “emer-gency response operations for releases of, or sub-
stantial threats of releases of, hazardous sub-stances without regard to the location of the haz-ard.” (29 CFR 1910.120(a)(1)(v)). Specifically, para-graph (q) covers employers whose workers areengaged in emergency response no matter where itoccurs, unless those workers are engaged in haz-ardous waste site operations.11
HAZWOPER paragraph (q) outlines require-ments for advance planning, training, medicalmonitoring and PPE for emergency responders.Several specific categories of emergency responsepersonnel are defined in this paragraph, includingfirst responder awareness level and first responderoperations level. OSHA’s compliance directive forparagraph (q) specifically includes “emergencymedical services” responding to a hazardous sub-stance release area.
OSHA has clarified that the HAZWOPER standardonly applies to emergency releases, or substantialthreats of releases, of hazardous substances.“HAZWOPER does not necessarily apply to everyincident in which an individual requiring medicaltreatment is contaminated with [a] hazardous sub-stance. OSHA cannot require HAZWOPER trainingfor incidents outside the scope of the standard,although such training may be beneficial.” (OSHA,1995-Nechis). The scope of the HAZWOPER stan-dard does not cover “incidental releases,” releasesthat are limited in quantity and pose no emergencyor significant threat to the safety and health ofworkers in the immediate vicinity.
An example is a tanker truck receiving a loadof HAZMAT at a tanker truck loading station.At the time of the accidental spill, the productcan be contained by employees in the imme-
11 The exceptions indicate that paragraph (q) does not apply toactivities at uncontrolled hazardous waste sites that are onEPA's National Priority Site List (NPL), cleanup operations atsites covered by the Resource Conservation and Recovery Actof 1976 (RCRA), voluntary cleanup operations at sites recog-nized by federal, state, local or other governmental bodies asuncontrolled hazardous waste sites, and operations involvinghazardous waste that are conducted at treatment, storage, dis-posal (TSD) facilities regulated by 40 CFR Parts 264 and 265pursuant to RCRA; or by agencies under agreement with U.S.EPA to implement RCRA regulations (see paragraphs (a)(1)(i)through (a)(1)(iv) of 29 CFR 1910.120). The standard goes on tostate that only paragraph (q) of the standard applies to emer-gency response activities unless the response involves anidentified hazardous waste site (29 CFR 1910.120(a)(2)(iv)).Other provisions of the HAZWOPER standard do not apply toemergency response operations except where paragraph (q)specifically refers to the other provisions.

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 1 9
diate vicinity and cleaned up utilizingabsorbent without posing a threat to the safe-ty and health of employees.Thus, this situa-tion is considered an incidental release, not anemergency release covered by HAZWOPER(OSHA, 2007-CPL-02-02-073).
The principles of risk assessment, PPE, deconta-mination and training apply equally.
As further clarification, OSHA explains inAppendix A of the HAZWOPER compliancedirective that personnel responding to anoverturned aircraft leaking jet fuel would likelybe performing emergency response due to thesignificant and uncontrolled hazards posed bythe aircraft and jet fuel.These personnel wouldbe conducting operations such as fire fighting,passenger rescue and working to stop therelease of jet fuel. However, a fuel spill from atanker truck that can be absorbed, neutralizedor otherwise controlled by employees in theimmediate release area through the placementof absorbent pads may qualify as an incidentalrelease, providing that there are no significanthealth or safety hazards (OSHA, 2007-CPL-02-02-073).12
Regarding acts of terrorism and natural disas-ters, an OSHA directive on the HAZWOPER stan-dard explains that, while employers are notrequired to prepare specifically for terrorist events(which are considered unforeseeable workplaceemergencies),13 employers must prepare for emer-gencies that release hazardous substances, regard-less of the cause of the release.
The release of chemicals or hazardous sub-stances into a workplace, whether caused byan accidental release or by a terrorist eventwould…be considered a hazardous substance(HAZMAT) incident. All emergency respondersand employees performing emergencyresponse efforts for such releases would,therefore, fall under 1910.120(q).The level ofemergency responder training must be basedon the duties and functions to be performedby each responder.
Workplaces located in areas prone to naturalphenomena, such as earthquakes, floods, tor-nadoes, and hurricanes, and potentially sub-ject to a ‘substantial threat of release of haz-ardous substances’ are covered by 1910.120.The ERP required in 1910.120(q)(1) must in-clude responses to emergencies caused bysuch natural phenomena.The requirement ofthe ERP clearly states in paragraph (q)(1), thatemergency response plans ‘shall be devel-oped and implemented to handle anticipatedemergencies prior to the commencement ofemergency response operations.’ This meansthat employers in areas prone to natural phe-nomena should anticipate whether such natu-ral phenomena are likely to cause releases ofhazardous substances and, if so, to incorpo-rate emergency response procedures to suchnatural phenomenon in their ERP (OSHA CPL02-02-073, 2007).
Medical personnel, including EMS responders,are not typically first on the scene, but becauseEMS responders do usually respond in the firstphase of an incident, they are likely to be involvedat the scene of an emergency during the initial riskassessment, rather than having the advantage of afully characterized hazard assessment when theyarrive. Although many scenes initially consideredto potentially involve a hazardous substance re-lease can be quickly reclassified, EMS responderssent to the scene of an emergency must be appro-priately trained to work in a suspect environment.This means that EMS responders need instructionon how to think beyond the confines of “medicalcare” so they can work safely and function as partof the incident command system (ICS). At anyevolving emergency scene, EMS responders’ dutiesmight range from keeping themselves out of situa-tions that present a hazard and are beyond thecapacity of their level of training or available pro-tective equipment, to contributing observations andinformation about the patient’s condition that willinfluence triage decisions and help decision-makersbetter characterize the hazards at the site.14 Theseconsiderations point to the need for first responderawareness level training as a minimum.
12 Other OSHA standards will still apply, such those as for hazardcommunication (29 CFR 1910.1200), permissible exposure limits(29 CFR 1910.1000), respiratory protection (29 CFR 1910.134), andpersonal protective equipment (29 CFR 1910.132).13 “OSHA does not consider terrorist events to be foreseeableworkplace emergencies for purposes of standards requiringemployers to anticipate and prepare for such emergencies.”(OSHA, CPL 02-02-073, 2007).
14 For example, patients treated by the EMS responder mightexhibit signs and symptoms that suggest the presence or identity(i.e., raise the index of suspicion) of a hazardous substancerelease.

2 0
Occupational Safety andHealth Administration
First on the Scene
The situation of an EMS responder arriving firston the scene could arise more or less frequentlydepending on the experience and practices inthat community.
For example, first responders in some commu-nities may be obliged to stop if they happenupon a transportation accident that has justoccurred. The accident might involve a haz-ardous substance release. Furthermore, somecommunities dispatch EMS responders, ratherthan police or firefighters, to certain medical911 calls, but it is possible that those calls couldinvolve hazardous substances that were notreported during the 911 call.
If, in the initial stages of a response, the EMSresponder could temporarily be the decision-maker at the site until a more qualified incidentcommander arrives, then that EMS responderrequires both first responder operations leveltraining [29 CFR 1910.120(q)(6)(ii)] and incidentcommander training (29 CFR 1910.120(q)(6)(v)).
Some EMS responders should have additional-levels of training. Although not normally the case,occasions exist when EMS responders could be thefirst to arrive on a scene (see above text box, Firston the Scene). In this case, the EMS respondercould have interim authority as the initial incidentcommander (IC) for the brief period between inci-dent discovery and the time that a correctly trainedIC arrives at the scene. The EMS responders whocould find themselves performing this role needadditional instruction on how to think beyond theconfines of medical care (see above box “First onthe Scene”). Furthermore, specific EMS respondersmight be designated to provide special services,such as rescue, decontamination, or treatment oftrapped patients in an area of higher hazard. Theseindividuals also require, at a minimum, firstresponder operations level training. Online trainingresources on the National Incident ManagementSystem (NIMS) and the Incident Command System(ICS) are available through the Federal EmergencyManagement Agency (FEMA) Website.15
EMS Responder Roles RequiringHAZWOPER Training
First Responder Awareness Level TrainingFirst responder training at the awareness level is the
minimum level of training required for EMS respon-ders who respond to emergencies (including 911calls) and might be first on the scene of an emer-gency, but would not be expected to treat or handlea contaminated patient (OSHA, 1991-McNamara).These EMS responders would not be designated toserve in any capacity on a decontamination team atthe site of the emergency release, nor would theyenter an area where contaminants could be present.This group of EMS responders would be responsiblefor notifying authorities if they encountered suspecthazardous substances at a scene and are expectedto stay alert to signs that a release might haveoccurred, but would not attempt to rescue patientsor treat contaminated patients (OSHA, 1991-McNamara). Rather, these EMS responders wouldwait for other properly trained and equipped firstresponders to bring thoroughly decontaminatedpatients to a safe area where the EMS responderscould treat them. A higher level of training (HAZ-WOPER first responder operations level training) isrequired if an EMS responder could be assigned torescue, treat, or participate in decontamination ofvictims of a hazardous substance release, or providethese services under any mutual aid agreement oremployer contract with the community. OSHA doesnot believe that all EMS responders need to betrained to treat contaminated victims (OSHA, 1992-Chapman); however, those who will perform thisservice must be properly trained to do so. Firstresponder awareness level training should ade-quately prepare EMS responders to use professionaljudgment to distinguish between the situations forwhich the responder is qualified to act and thosewhich require a higher level of training and PPE.
Training Duration,Topics and CompetenciesFirst responder training requirements for the aware-ness level appear under 29 CFR 1910.120(q)(6)(i).This section does not require a specific minimumtraining duration, but outlines topics that must becovered (competencies the worker must acquire). Inthe HAZWOPER compliance directive, OSHA men-tions that although the standard does not set a min-imum number of hours for this training, “suchcourses often run from 4 to 12 hours” (OSHA, 2007-CPL-02-02-073). The HAZWOPER standard allows analternative to the first responder awareness leveltraining requirement. Training can be waived if theworker has had sufficient experience to objectivelydemonstrate competency in specific areas. Therequired training topics (or areas of competency)are listed in 29 CFR 1910.120(q)(6)(i), or the parallelState Plan standards, and include:15 To access NIMS and ICS online training, go to
http://www.fema.gov/emergency/nims/nims_training.shtm#0.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 2 1
fulfill the refresher training requirement.
First Responder Operations LevelTrainingEmployers must provide HAZWOPER first respon-der operations level training to designated EMSresponders who are expected to treat patientsbefore they are thoroughly decontaminated. Thisincludes EMS responders who perform decontami-nation, which could bring the EMS responder intocontact with contaminated individuals (OSHA, 1991-McNamara; OSHA, 1992-Levitin). It also includesEMS responders who “enter the danger area toperform rescue or treat contaminated victims.”(OSHA, 1995-Nechis).
Training DurationTraining requirements for first responder operationslevel appear under 29 CFR 1910.120 (q)(6)(ii), whichindicates a minimum training duration of 8 hoursand outlines topics to be covered (competenciesthe worker must acquire). Both the required compe-tencies and training time for medical personneltrained at first responder operations level were con-firmed in an interpretive letter (OSHA, 2003-Bolt).OSHA, however, allows these topics (but not theminimum training time) to be tailored to bettermeet the needs of first responders. Training that isrelevant to the required competencies countstoward the 8-hour requirement, even if the trainingis provided as a separate course. For example,training on PPE that will be used during patientdecontamination activities may be applied towardsthe 8-hour minimum first responder operationslevel training requirement, regardless of whetherthe PPE training is conducted as part of a specificHAZWOPER training course or as part of anothertraining program (OSHA, 1992-Levitin).
First responder awareness level training com-pleted by a worker also counts towards that individ-ual’s 8-hour requirement for first responder trainingat the operations level. This point is clarified in aletter of interpretation issued by OSHA:
“…if you spend two hours training employeesin the required competencies for FirstResponder Awareness Level as described in 29CFR 1910.120(q)(6)(i)(A)-(F), then you wouldneed to spend at least six additional hours train-ing employees in the required competencies forFirst Responder Operations Level as describedin 29 CFR 1910.120(q)(6)(ii)(A)-(F). Depending onthe employees’ job duties and prior educationand experience, more than eight hours of train-ing may be needed.” (OSHA, 2003-Bolt).
• An understanding of what hazardous substancesare, and their associated risks during an inci-dent.16
• An understanding of the potential outcomesassociated with an emergency created whenhazardous substances are present.
• The ability to recognize the presence of haz-ardous substances in an emergency.
• The ability to identify the hazardous substances,if possible.
• An understanding of their role in the employer’semergency response plan, including site securityand control and the DOT Emergency ResponseGuidebook.
• The ability to realize the need for additionalresources and to make appropriate notificationsto the communications center.
Although not required, OSHA recommends as abest practice that training include information onrisk assessment and risk management to enableEMS responders to understand and identify the lim-itations of their expected role.
• Recognizing the types of situations that couldinclude a hazardous substance release.
• Placards, labels, common hazard rating schemes(e.g., National Fire Protection Association [NFPA]hazard warning diamond) and other indicatorsof hazardous substances.
• Recognizing signs or symptoms of hazardoussubstance exposure in patients and responders.
• The steps the EMS responder is expected to takeif a scene or patient is discovered to be contami-nated with a hazardous substance (or substancesuspected of being hazardous).
• The extent and limitations of the EMS respon-der’s training and PPE (what they are and arenot prepared to do).
Annual RefresherTrainingAnnual refresher training is required for workerstrained at the first responder awareness level. Theclass content must be adequate to maintain theEMS responder’s competence, and the employermust document the training or the method used todemonstrate the EMS responder’s competence.Employers may also use actual or drill responses to
16 As noted previously, a hazardous substance is any substanceto which exposure may result in adverse effects on health orsafety of workers. This includes biological agents, substanceslisted by U.S. DOT as hazardous materials, and substances classi-fied as hazardous wastes. See Appendix A – Glossary for a moredetailed definition.
• Recognizing signs and symptom of exposure tohazardous substances that they could encounterat emergency response scenes in jurisdictionsthey might cover (including those areas coveredby mutual aid agreements).
• Assessing site safety, including risks to EMSresponders.
• Specific training on hazardous risk assessmentduring encounters with contaminated patients.
• Selecting and using appropriate PPE. (See para-graphs below titled AssociatedTraining – PPEand AssociatedTraining – RespiratoryProtection.)
• Employing patient decontamination procedures.(See Best Practices for Pre-ambulance PatientDecontamination, below.)
Annual RefresherTrainingAnnual refresher training at the first responderoperations level is required under 1910.120(q)(8)(i),or the parallel State Plan standards; however, thelength of the refresher training is not specified.Instead, the standard requires that workers trainedat the first responder operations level shall receiveannual refresher training of sufficient content andduration to maintain their competencies, or shalldemonstrate competency in those areas at leastyearly. Employers may also use actual or drillresponses to fulfill the refresher training require-ment.
Documenting HowTraining Requirements AreMet : Employers of EMS responders must docu-ment that initial and refresher training was per-formed, or alternatively, keep a record of how theEMS responder demonstrated competence in therequired areas. This is particularly important when-ever workers are allowed to satisfy any portion ofthe training requirement through other relatedtraining or through demonstration of competence.The HAZWOPER standard requires, and an OSHAletter of interpretation confirms, that the employermust certify in writing the comparable training ordemonstrated competencies (OSHA, 2003-Bolt).
AssociatedTrainingThe following subsections briefly describe trainingthat employers must provide EMS responders whouse PPE and/or respiratory protection. This trainingcan count towards the 8-hour requirement for firstresponder operations level training.
Option to Demonstrate CompetenceAs with first responder awareness level training, theHAZWOPER standard allows workers to demon-strate competence in specific areas as an alternativeto the 8-hour training requirement (29 CFR1910.120(q)(6)(ii)). OSHA reaffirmed this point in aletter of interpretation (OSHA, 2003-Bolt). However,it is important to recognize that in the typical EMSresponder setting, it might be difficult to ensurethat workers have sufficient experience to waive allthe training requirements. Many EMS responderslack extensive experience with higher levels of res-piratory protection along with, as the studies citedin Appendix O demonstrate, performance of decon-tamination activities.
Topics forTraining or Demonstrationof CompetencyThe HAZWOPER standard requires that workerstrained at the first responder operations level shallhave received at least 8 hours of training or havehad sufficient experience to objectively demon-strate competency (e.g., in exercises and drills) inthe following areas (1910.120(q)(6)(ii)):
All of the topics previously listed for first respon-der training at the awareness level, plus the addi-tional topics listed here.
• Knowledge of the basic hazard and risk assess-ment techniques.
• Knowledge of how to select and use proper PPE.[A critical aspect is knowing both when PPE isuseful, and under what circumstances it willNOT provide adequate protection.]
• An understanding of basic hazardous materialsterms.
• Knowledge of how to perform basic control,containment, and/or confinement operationswithin the capabilities of the resources and PPEavailable.
• Knowledge of how to implement basic decon-tamination procedures.
• An understanding of the relevant standard oper-ating procedures and termination procedures.
Although not required, OSHA recommends asa best practice that training topics be tailored toreflect EMS responders’ anticipated duties andmight include details such as:
• Understanding the community emergency oper-ations plan and EMS responders’ role in theresponse, including who will provide decontami-nation services.
2 2
Occupational Safety andHealth Administration
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 2 3
It is also important that the level of training becompatible with the PPE that is provided to EMSresponders. Over-equipping workers mayencourage them to attempt activities beyond thelevel for which they are trained. If workersrequire a higher level of protection, considerwhether a higher level of training, includingHAZWOPER training, is also needed.
AssociatedTraining – PPEThe first responder operations level training relatedto the use of PPE must include topics as required byOSHA’s PPE standard (29 CFR 1910.132). Under thisstandard, training must be provided to each workerwho is required to use PPE. At a minimum, thattraining must cover the following:
• Recognizing when PPE is necessary.
• Identifying what PPE is necessary.
• Demonstrating how to properly put on, remove,adjust, and wear PPE.
• Understanding the limitations and hazards ofPPE.
• Understanding the proper care, maintenance,useful life and disposal of PPE.
Workers must demonstrate their understandingof the training by showing that they can use the PPEproperly, prior to wearing it in the workplace.Refresher training is required when the worker can-not demonstrate proficiency in the proper care anduse of the PPE, when changes in the workplace ren-der the previous training inadequate, or whenchanges in the type of PPE to be used render theprevious training inadequate. The employer mustmaintain a written record of worker PPE training. Itis the employer’s responsibility to assess the fullrange of the EMS responder’s expected duties andprovide PPE and PPE training accordingly. Thisassessment must include the worker’s expected roleduring reasonably anticipated worst-case scenarios.
AssociatedTraining – Respiratory ProtectionFirst responder training at the operations level alsomust include training required by OSHA’sRespiratory Protection standard (29 CFR 1910.134),or the parallel State Plan standards. Specifically, anyworker who must wear a respirator must be trainedin the proper use and limitations of that device priorto its use in the workplace. The training must becomprehensive enough that the worker is able todemonstrate knowledge of the seven training topicsspecified in the standard and outlined below. Theworker also must be able to demonstrate compe-
tence in wearing the complete PPE ensemble,including respirator, protective garment, gloves,boots, and any other safety equipment required forthe worker’s role. Refresher training is required atleast annually, or sooner if changes in the workplaceor type of respirator render previous training inade-quate. Refresher training is also required if theworker does not demonstrate proficiency in theproper care and use of the respirator, or at anyother time when retraining appears necessary toensure safe respirator use.
At a minimum, training under OSHA’sRespiratory Protection standard must cover the fol-lowing topic areas:
• The nature of the respiratory hazard, and why arespirator is needed.
• Respirator capabilities, limitations and conse-quences if the respirator is not used correctly.
• How to handle respirator malfunctions and otheremergencies.
• How to inspect, put on, remove, use and checkseals on the respirator.
• How to maintain the respirator face/face sealintegrity (e.g., through proper grooming, clean-ing, and correct use).
• Maintenance and storage procedures.
• When to change cartridges on air purifying respi-rators (APRs).
• Additional prescribed procedures relating toSCBAs (if used), such as monthly inspectionsand ensuring breathing air quality.
• How to recognize medical signs and symptoms thatmay limit or prevent effective use of a respirator.
• General requirements of the respiratory protec-tion program.
Sources of Training and CurriculaSeveral examples of HAZWOPER first responderoperations level training curricula are available foremployers preparing EMS responders to conductdecontamination activities. Examples include theHazardous Materials andTerrorist IncidentPrevention Curriculum Guidelines (HMEP, 1996).However, these curricula are not necessarilydesigned as 8-hour presentations. Many curriculaare longer, while others are shorter and intended foruse when workers are able to demonstrate compe-tence in specific areas. See Appendix H for an addi-tional discussion on options for first responder train-ing at the awareness and operations levels for EMSpersonnel.
2 4
Occupational Safety andHealth Administration
If employees who only provide inter-facility trans-port are unexpectedly called on to aid a contami-nated victim, those individuals may be consid-ered skilled support personnel and receive specialon-the-spot training.
However, if repeatedly called upon to treat acci-dent victims contaminated from HAZWOPER inci-dents, the EMS employer must train and desig-nate the employees to the First ResponderOperations Level (OSHA, Nechis, 1995).
(See the related discussion of skilled support per-sonnel, below).
First responder training is offered at both theawareness and operations levels through a numberof public and private organizations. An increasingnumber of hospitals offer (or coordinate) local class-es tailored to medical personnel.17
EMS Responder Roles that RequireNo HAZWOPER TrainingAs noted previously, if an employer has not agreedto be designated in a state or local emergencyresponse plan to respond to a hazardous substancerelease, then the employer may not have any obliga-tion to train workers under the HAZWOPER standard(OSHA, 1995-Nechis). For example, employers arenot obliged to provide HAZWOPER training to anEMS responder whose work involves only patienttransport between medical treatment facilities, aslong as no agreements exist that could increasethe EMS responder’s involvement in emergencyresponse including hazardous substances.
It also bears repeating that employers may notdesignate an EMS responder as exempt from HAZ-WOPER training if it is anticipated that the EMSresponder could suddenly be activated to provide911 response. This prohibition holds even for “strict-ly medical” 911 calls – since some of these calls caninvolve unanticipated hazardous substance release(e.g., scenes that upon arrival are discovered toinvolve a methamphetamine laboratory). Similarly,an EMS responder cannot be exempt from HAZ-WOPER training if the employer has entered into amutual aid agreement that could result in the EMSresponder responding to an emergency or a 911 call,or if the employer has signed support contracts ormade arrangements with the community, localorganizations, or neighboring communities that
could result in the EMS responder being sent to thesite of an emergency.
Because a worker without HAZWOPER trainingmight not be equipped to identify the presence of ahazardous condition and make the decision to stayaway, an untrained EMS responder who happensupon the scene of an emergency should not ap-proach the site.
Skilled Support PersonnelThe HAZWOPER standard allows for the case wherea worker is not expected to serve in an emergencyresponse capacity, but nevertheless is suddenlycalled upon (e.g., as a one-time occurrence) to pro-vide emergency care at a scene involving hazardoussubstance release. When this occurs, the worker istermed skilled support personnel. An EMS respon-der who has been exempt from HAZWOPER trainingby the employer (such as those discussed above),but is unexpectedly called on to aid a contaminatedpatient, or perform other work at the scene of a haz-ardous substance release, is considered skilled sup-port personnel. Other examples of skilled supportpersonnel include a medical specialist or a trade per-son, such as an electrician. These individuals mustreceive expedient orientation to site operations,immediately prior to providing such services (OSHA,1997-Whittaker). An EMS responder without HAZ-WOPER training might treat and transport patientsthat have been “…totally and thoroughly decontami-nated and removed from the danger zone. However,in this case, while working as skilled support person-nel, these EMS responders should be given an initialbriefing at the site…” prior to providing this service(OSHA, 1991-McNamara). This briefing would alsobe needed for EMS responders trained at the firstresponder awareness level, who are suddenly calledupon to provide decontamination services, whichwould require first responder training at the opera-tions level. The briefing for skilled support personnelis intended to provide the individual with informa-tion necessary to safely do a specific job at a specificincident site and typically assumes no prior HAZ-WOPER training.
The following quotation from an OSHA letter ofinterpretation emphasizes this important point:
“…if an EMS [squad] is not designated in anyemergency response plan, but finds that they arerepeatedly called upon to treat accident victimscontaminated from a HAZWOPER incident, theseworkers cannot be considered skilled supportpersonnel and the EMS employer must train anddesignate the workers to the First ResponderOperations Level.” (OSHA, 1995-Nechis).
17 Additional resources to assist with the development of trainingcan be found at: www.osha.gov/SLTC/emergencypreparedness/index.html.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 2 5
When an EMS responder is unexpectedly calledupon to respond to a hazardous substance incidentas skilled support personnel, the EMS respondermust receive an orientation that provides informa-tion on:
• Nature of the hazard (if known).
• Expected duties.
• Appropriate use of PPE.
• Other appropriate safety and health precautions(e.g., decontamination procedures).
If a respirator will be needed, these personnel alsomust be medically cleared for respirator use beforethe respirator is worn. An acceptable fit test andproper grooming to ensure a good face/facepieceseal is required if the responder will wear a tight-fit-ting respirator. These steps are required by 29 CFR1910.134 (Respiratory Protection), or the parallelState Plan standards.
While a just-in-time briefing during the responseis the only required training for these personnel,time and resource limitations inherent in a crisis like-ly will diminish the effectiveness of such training.This is another reason why employers of EMSresponders should diligently consider the broadrange of conditions under which their workersmight be called to serve and provide an appropriatelevel of HAZWOPER training.
An employer cannot allow workers to be desig-nated as skilled support personnel as an alterna-tive to providing appropriate, initial, and refresh-er HAZWOPER training.
Relevance of Other HAZWOPER TrainingLevels to EMS RespondersAn OSHA letter of interpretation discusses the rolesof EMS responders and other emergency respon-ders at the scene of a hazardous substance release.“Standard emergency medical practice dictates thatEMS personnel are to survey the accident scene andremain away from the hazard area until it is safe toapproach. In the case of a HAZWOPER roadwayemergency, the incident needs to be brought under
control by more highly skilled emergency respon-ders before it would be permissible for EMS person-nel, including those certified at the first responderoperations level, to enter to perform rescue or pro-vide medical treatment.” (OSHA, 1995-Nechis).
First responder training beyond the operationslevel is not necessary for worker activities that arerestricted to medical treatment and decontamina-tion. However, many EMS responders have qualifi-cations at higher levels of HAZWOPER training.These are EMS personnel who elect to be cross-trained to serve an expanded role (e.g., firefighter,HAZMAT team member), and might receive otherlevels of HAZWOPER training as needed in supportof those additional roles. For example, firefighterscommonly obtain additional education to qualify asEMS responders (in addition to continuing to qualifyas firefighters) and some EMS personnel are trainedat the Hazardous Materials Technician or HazardousMaterials Specialist level to serve on special HAZ-MAT teams. Any HAZWOPER training that an EMSresponder receives beyond the first responder oper-ations level would be to support the role of firefight-er or HAZMAT team member. The EMS respondermight, in the capacity of firefighter, enter dangerousareas to perform non-medical activities such as con-trolling a hazardous substance release or performingrescue, for which the higher level of HAZWOPERtraining is required.
Conclusions Regarding EMS TrainingEmployers must use the information at their disposalto make informed decisions regarding suitable levelsof HAZWOPER training for their EMS personnel.Although there may be some EMS personnel forwhom HAZWOPER training is not necessary, OSHAbelieves that after a critical review of communityexpectations and community threats, most employerswill find that at a minimum first responder awarenesslevel training is appropriate for all their EMS respon-ders and that some of these personnel also requirefirst responder operations level training. In somecommunities, contract language referring to HAZ-WOPER initial and refresher training will promoteEMS personnel qualifications in this regard.
Personal ProtectiveEquipment
Using OSHA’s Rationale for HazardAssessment and PPE Selection
The best practices presented in this document indi-cate the minimum PPE that OSHA generally antici-pates will be needed to protect EMS respondersunder various conditions. However, as with anygeneralized protection, OSHA’s PPE selection forEMS personnel offers more protection againstsome hazards than others. If an employer or inci-dent commander determines that EMS responderscould reasonably anticipate encountering a specificknown hazard, the employer or incident command-er also must determine whether this generalizedprotection must be supplemented to more fullyprotect against the specific hazard.
In order to complete the hazard assessment andPPE selection process, each employer must consid-er the role the EMS responders will play in thecommunities in which they might be called upon tooperate. Employers should also consider additionalinformation available from community sourcesregarding the range of hazards that EMS respon-ders could encounter during reasonably anticipatedworst-case scenarios (OSHA, 2002-Hayden). Whenthese sources point to a specific substance or situa-tion from which the employer should protect EMSresponders, the employer must confirm that PPEselection provides effective protection against thathazard. In rare situations, the employer may find itnecessary to augment the PPE specified in this doc-ument for unknown hazards in order to help ensureprotection against specific known hazards (e.g., bytailoring glove selection to address an identified,specific hazard, or by stocking additional supplies).
Employers must adopt a more specialized levelof protection (such as atmosphere-supplying respi-rators [ASR]) when the EMS responder’s role in thecommunity or hazard assessment indicates that ahigher level of protection is necessary, such aswhen EMS responders could be subjected to anenvironment immediately dangerous to life andhealth (IDLH).
PPE Selection Based on ReasonablyAnticipated Worst-Case ScenariosPPE selection will vary based on the working con-ditions of EMS personnel. OSHA suggests thatemployers of EMS personnel provide workerswith the minimum PPE that will offer protectionagainst a reasonably anticipated worst-case sce-
2 6
Occupational Safety andHealth Administration
nario, including catastrophic or terrorist incidents.It is important to note, however, that the mini-mum PPE for the reasonably anticipated worst-case scenario may differ between locales. Forexample, after evaluating (1) the roles that theseresponders could be called upon to fill in thecommunity and (2) the reasonably anticipatedhazards that EMS responders could encounter intheir community, an EMS employer should reviewthese best practices and select the minimum PPEthat would protect against the most serious credi-ble situations.
“If only one level or type of PPE will be avail-able, it is appropriate for that PPE to coverthe worst-case situation. EMS agencies mightalso wish to provide other types of PPE forless-than worst-case situations (e.g., the haz-ard is identified and risk is reduced). If anadequate level of PPE is not carried on theambulance, the agency needs to have a pro-vision for getting it to the site where it isneeded.” (OSHA Stakeholder Comments,2006)
For most employers of EMS responders, thereasonably anticipated worst-case scenario is like-ly to involve the release of unidentified or unchar-acterized hazardous substances with potential forsecondary contamination. In many areas, theworst case could include the possibility that theunidentified substance would be a CBRNE sub-stance. Where community expectations restrictthe EMS responders to treating patients only afterthe hazardous substance is characterized, or totreating only patients who have been thoroughlydecontaminated by other EMS personnel (e.g.,properly equipped HAZMAT team members), thenthe most serious exposure scenario might onlyinvolve characterized or identified hazardous sub-stances, or possibly limited quantities of partiallycharacterized hazardous substances. OSHA, how-ever, believes that in most communities, certainEMS responders cannot be assured of such a lim-ited role during a widespread mass casualty inci-dent. As a result, PPE selection for EMS respon-ders in these communities should be based onthe need to provide decontamination at the sceneof the incident and the need to offer emergencymedical services before the hazardous substancehas been characterized. The number of EMSresponders who should be trained and equipped
with PPE allowing them to provide decontamina-tion services will depend on the community’sexpectations and Hazard Vulnerability Analysis.
Employers should keep in mind that once ahazardous substance is identified or character-ized, the PPE can be adjusted to appropriate lev-els, as determined by the incident commander.Employers should be prepared to provide adjust-ed PPE suitable for the most common anticipatedsituations in the community.
Required Written Documentation forRespirator and PPE Selection ProcessEmployers selecting respiratory protection andPPE must consider factors outlined in OSHA’sRespiratory Protection standard (29 CFR 1910.134)and Personal Protective Equipment standard (29CFR 1910.132). For both respirators and PPE, aprimary selection factor is the hazards that work-ers are likely to encounter and both standardscontain requirements for written documentation(see text box - Written Documentation of HazardAssessment for PPE Selection). Several otherselection factors are listed in the following sub-sections and details on all factors are provided inthe respective OSHA standards.
Written Documentation of HazardAssessment for PPE Selection
Under 1910 Subpart I, the employer mustperform a hazard assessment to select appro-priate personal protective equipment for thehazards that are present, or likely to be pres-ent, including foreseeable emergencies. Thehazard assessment must be in the form of awritten certification as described in 29 CFR1910.132(d)(2).
The employer shall verify that therequired workplace hazard assessmenthas been performed through a writtencertification that identifies the workplaceevaluated; the person certifying that theevaluation has been performed; and thedate(s) of the hazard assessment.Thewritten certification must also clearlyidentify the document as the certificationof hazard assessment.
The hazard assessment provision appliesonly to 29 CFR 1910.133 (eye and face protec-tion), 1910.135 (head protection), 1910.136(foot protection), and 1910.138 (hand protec-tion). Although it does not apply to 29 CFR1910.134 (respiratory protection) and1910.137 (electrical protective devices), the
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 2 7
Respiratory Protection standard does containspecific requirements for evaluating respira-tory hazards. The employer must includeprocedures for selecting respirators in thewritten respiratory protection program asdescribed in 29 CFR 1910.134. As part of theselection process:
The employer shall identify and evaluatethe respiratory hazard(s) in the workplace;this evaluation shall include a reasonableestimate of employee exposures to respi-ratory hazard(s) and an identification ofthe contaminant's chemical state andphysical form.Where the employer can-not identify or reasonably estimate theemployee exposure, the employer shallconsider the atmosphere to be IDLH. (29CFR 1910.134(d)(1)(iii))
Assessing the Need forRespiratory Protection
Respiratory Protection Required forEMS RespondersRespiratory protection requirements are welldefined for specific emergency response situations.OSHA’s HAZWOPER standard and letters of inter-pretation dictate the levels of protection that OSHArequires for EMS responders in cases of high haz-ard and when the hazard is very low. The respirato-ry hazard evaluation that employers conduct helpsthem define the types of respiratory protection thatincident commanders are most likely to designateat scenes once the hazard is adequately character-ized. Employers of EMS responders who could becalled upon to play a role in emergency responsemust equip their workers to work safely in theirassigned roles (OSHA, CPL 02-02-073, 2007).
Types of Respiratory Protection AvailableAppendix J provides an overview of respiratoryprotection types, facepieces, and their associatedadvantages and disadvantages. Employers of EMSresponders should consult Appendix J while con-sidering the respiratory protection that their work-ers would need to perform specific emergencyresponse roles. Practical matters, such as how toensure that the correct respiratory protection isavailable at the scene, need to be considered aspart of the emergency response plan. OSHAbelieves that EMS responders will not be able towork safely if they are designated to fill roles forwhich the required PPE will not necessarily be onhand.

National Institute for Occupational Safetyand Health (NIOSH) Approval and Chemical,Biological, Radiological, Nuclear (CBRN)CertificationsRespiratory protection for EMS responders mustalways be of a type approved by NIOSH. Addition-ally, in any location where CBRN substances are athreat, the respirator should also be NIOSH-ratedfor use in CBRN environments. In addition, CBRNrespirators offer advantages of having passed addi-tional testing to assure ruggedness and structuraldurability.
Respiratory Protection for an Identifiedor Characterized HazardThe incident commander is responsible for deter-mining an appropriate level of respiratory protec-tion for EMS responders at emergency scenesinvolving the release of a known hazardous sub-stance(s), or entry into the dangerous area of thescene after the substance is characterized. However,in some circumstances, OSHA’s HAZWOPER stan-dard prescribes the level of protection. Specifically,an SCBA respirator is required when an IDLHatmosphere is present, including occasions whenthe hazardous substance is unidentified or informa-tion is inadequate to rule out an IDLH environment.OSHA’s Respiratory Protection standard requiresthat for an IDLH environment the SCBA must beconfigured as a full facepiece pressure demandSCBA certified by NIOSH for a minimum service lifeof thirty minutes, or as a combination full facepiecepressure demand supplied-air respirator (SAR) withauxiliary self-contained air supply (29 CFR 1910.134(d)(2)(i)(A) and (B)). Furthermore, Appendix B of theHAZWOPER standard indicates that where an IDLHenvironment is present, Level A or Level B PPE arerequired, depending on whether the hazardincludes a substance that can be absorbed or ishazardous to the skin (requiring Level A) or not(Level B permitted). For a description of these PPElevels, see Appendix N – General Description andDiscussion of the Levels of Protection andProtective Gear.
Other Requirements Related toRespiratory ProtectionIf EMS responders will need to wear respiratoryprotection, OSHA requires that the employer devel-op a respiratory protection program that explainshow the employer meets the requirements outlinedin OSHA’s Respiratory Protection standard (29 CFR1910.134). The program must cover topics such asthe procedures used for selecting respirators; how
medical evaluations and fit testing are provided;methods for ensuring that respirators are properlyused, cleaned and maintained; worker training; andhow the program’s effectiveness is evaluated.
Gloves, Boots and GarmentsAs is the case with respiratory protection, the actualconditions will dictate the level and type of PPErequired to protect an EMS responder. Some con-siderations for gloves, boots and protective clothingare presented in the following sections. Regardlessof the selection, the provisions of the BloodbornePathogens standard (29 CFR 1910.1030) wouldapply. As previously discussed, the employer mustcertify that a hazard assessment has been per-formed as part of the PPE selection process.
Gloves and BootsNo single glove or boot material will protect againstevery substance. Base the selection on the type andextent of anticipated contact with hazardous sub-stances. Consider the type of substances, the effectof dermal exposure, patient symptoms, and thelikely interventions that contaminated patientsmight require, then select protective gear that bestallows critical patient treatments while fully protect-ing the EMS provider.
Most glove manufacturers offer detailed guidesto glove materials and their chemical resistance.Butyl rubber gloves generally provide better protec-tion than nitrile gloves for chemical warfare agentsand most toxic industrial chemicals that are morelikely to be involved in a terrorist incident, althoughthe converse applies to some industrial chemicals.Foil-based gloves are highly resistant to a widevariety of hazardous substances and could also beconsidered when determining an appropriate pro-tective ensemble. Employers of EMS respondersmust select materials that cover the specific sub-stances that the employer has determined that EMSresponders reasonably might encounter. However,given the broad scope of potential contaminants,OSHA considers it important for employers toselect materials that protect against a wide range ofsubstances. A double layer of gloves, made of twodifferent materials, or foil-based gloves will resistthe broadest range of chemicals.
A combination of gloves, for example, butylgloves worn over inner nitrile gloves, is often thebest option for use by EMS responders duringemergencies and mass casualties involving haz-ardous substances. However, responders areadvised to select the combination that best meets
2 8
Occupational Safety andHealth Administration

their specific needs. Between gloves that offer ade-quate worker protection, select the model(s) thatminimize impact on delivering the types of patientinterventions that are most likely to be needed.
Glove thickness is measured in mils, with ahigher number of mils indicating a thicker glove (1mil equals 1/1000 of an inch). Using commonexamples, exam gloves are often approximately 4mil, while general-purpose household (kitchen)gloves are 12–16 mil, and heavy industrial glovesmight be 20 to 30 mil.
Depending on the dexterity needed by the EMSresponder, the glove selection can be modified toallow for the use of a glove combination that isthinner than that usually recommended for the bestprotection. As an example, the U.S. Army Centerfor Health Promotion and Preventive Medicine(USACHPPM) recommends that medical personnelworking with patients potentially contaminated withchemical warfare agents or toxic industrial chemi-cals wear a combination of chemical protectivegloves, such as butyl rubber gloves over innernitrile gloves (USACHPPM, 2003a). Because thickergloves offer greater protection, USACHPPM recom-mends a butyl glove with a minimum thickness of14 mil (over a 4 or 5 mil nitrile glove). However,with increased thickness comes greater loss ofmanual dexterity and hand fatigue. When advancedmedical procedures must be performed beforedecontamination, thicker gloves might be too awk-ward, and, therefore, it might be necessary to use abutyl rubber glove of 7 mil over the nitrile glove, ora 14 mil butyl rubber glove alone (USACHPPM,2003a).
When manual dexterity is required, a 14 milbutyl glove, or a 7 mil butyl glove over a 4 to5 mil nitrile glove, may be the best options;however, these gloves should be changedfrequently to minimize the chance of expo-sure if gloves tear, abrade, or are chemicallydegraded. (OSHA Stakeholder Comments,2006).
Hendler et al. (2000), as cited in USACHPPM(2003a), conducted a study to determine the effectof full PPE (including 12-mil “tactile” gloves and afull facepiece mask) on intubation performance.Clinicians wearing this equipment could performendotracheal intubation effectively (i.e., the tubewas inserted in sufficient time), but the proceduredid take longer than it would have without PPE.Intubation delays would cause subsequent deconta-mination procedures and medical treatment to bedelayed by a corresponding amount of time. Some
incidents may have injured patients in such a waythat routine emergency care cannot be rendereduntil the patient is decontaminated to assure ade-quate protection to the medical team.
If sterility is required and decontamination is notpossible before performing medical procedures, adouble layer of disposable 4 to 5 mil nitrile glovesmight be the best option (USACHPPM, 2003a). Notall sources recommend double gloves; for example,the U.S. Army Soldier and Biological ChemicalCommand’s (SBCCOM) [now called the Research,Development and Engineering Command, or RDE-COM] Domestic Preparedness Program (DPP) rec-ommends butyl rubber gloves for personnel per-forming decontamination operations and casualtycare (SBCCOM, 2000). Among the sterile glovesreadily available, those made of nitrile offer the bestresistance to the widest range of substances.Thinner gloves fail (deteriorate, tear, rip) more rap-idly than thicker gloves and, therefore, if they mustbe used, these gloves should be inspected andchanged more frequently. Thinner gloves should bechanged when contaminated or as soon as feasibleif they are torn, punctured, or when their ability tofunction as a barrier is compromised.18
In general, the same material selected for gloveswill also be appropriate for boots. Because bootwalls tend to be thicker than gloves, boots of anymaterial are likely to be more protective thangloves of the same material. Military vinyl over-shoes (designed to be worn over combat boots) arenow commercially available at competitive costsand have been approved by the military for protec-tion against chemical warfare agents.
Protective GarmentsThe optimal garment materi-al for EMS responders willvary depending on theresponder’s role and shouldbe a subject of the employ-er’s hazard assessment.Except for particularly harshclimates, standard uniformsmay be sufficient for EMSresponders in the cold zone.As discussed below, theselection is more complex for responders whocould find themselves in the warm zone. SeeAppendix K for links to additional information on
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 2 9
18 For additional information on recommended glove materialsand chemical breakthrough of specific substances, see theNIOSH Recommendations for Chemical Protective Clothing: ACompanion to the NIOSH Pocket Guide to Chemical Hazards.Available at www.cdc.gov/niosh/ncpc/ncpc2.html
Phot
oco
urte
syof
Fran
kCal
ifano

associated with an actual first responder chemicalresponse (but did not involve physical acts, such aspatient handling or handling needles and injections,that would likely be required of EMS responders)(SBCCOM, 2003). Results are summarized in Table 1.
Table 1.
Results of SimulationTests on Several Chemical Suits
Suit Configuration # SuitsTested Protection Factor
Standard [Police] Uniform 2 2
Tyvek® Protective Wear Suit 4 4
Tychem® 9400 ProtectiveSuit 4 17
Kappler® Tychem CPF4Protective Suit 4 18
Tychem® SL Protective Suit 5 24
Tyvek® ProTech F ProtectiveSuit 5 42
Source: SBCCOM, 2003.
The ability of protective garment fabric to with-stand physical abrasion and tearing is also impor-tant. If their role could involve assisting non-ambu-latory contaminated patients or victims trapped inthe hot zone, EMS responders might subject theprotective garments to physical stresses that shouldbe considered in garment selection. The NFPAStandard No. 1994 on Protective Ensemble for FirstResponders to CBRN Terrorism Incidents offers cri-teria for evaluating the performance of protectivegarments, including detailed specifications forbursting, puncture and tear resistance, as well asgarment seam specifications (NFPA, 2007).
Additionally, the Interagency Board has begunpublishing a list of standard products, includingPPE, for use in national emergencies (IAB, 2007).
As a rule of thumb, if the employer has deter-mined that an EMS responder’s role in a responsecould involve using SCBA, the responder shouldalso be outfitted with broad spectrum chemicalprotective clothing. However, chemical protectiveclothing is generally semi- or impermeable. Any-time an EMS responder wears semi-permeableor impermeable clothing, the risk of heat stressincreases substantially. See Appendix K for a dis-cussion of thermal stress on EMS responders work-ing in hot and cold environments.
Modifying PPE Selections Based onAvailable InformationFlexibility in prescribing respiratory protection andPPE is particularly important. Employers of EMSresponders must be prepared to provide their work-
3 0
Occupational Safety andHealth Administration
thermal stress and working in cold and hot condi-tions, including working in chemical protectivesuits.
In the warm zone, EMS responders will needgarments that protect against a wide range ofchemicals in liquid, solid, or vapor form (phase).Because EMS responders might become contami-nated with liquid or solid (dust) contaminantsthrough physical contact with a contaminatedpatient, the ideal fabric will repel chemicals.Additionally, the optimal garment will restrict thepassage of vapors, both through the suit fabric andthrough openings in the suit. Finally, optimal cloth-ing is also sufficiently flexible, durable, and light-weight for long-term wear (up to several hours)during physically active work.
A variety of broad-spectrum protective fabricsand designs may be appropriate, depending on thesituations and hazards that the employer antici-pates EMS responders reasonably might be expect-ed to encounter. Several commercially availableproducts include: Tyvek® F, Tychem® CPF3, Tychem®
CPF4, Tychem® BR, Tychem® LV, Tychem® SL,Zytron® 100, Zytron® 200, Zytron® 300, Zytron® 400,Zytron® 500, and Zytron® 600, ProVent® 10,000, andDuraVent® 2.8. Note, however, that OSHA does nottest, endorse, or recommend specific products.Before selecting products or materials, contact themanufacturer for specific application guidance.
Fabric and suit manufacturers can provide labo-ratory testing information regarding specific materi-als.19 For example, Tyvek® F has been tested exten-sively by military organizations and accredited test-ing laboratories. As another example, the SBCCOM(now called RDECOM) DPP tested vapor-blockingproperties of six different protective suits in a simu-lated, high-vapor environment. In the results tabu-lated below, the Tyvek® F suit (ProTech model)offered a protection factor of 42 (vapor levels out-side the suit were 42 times higher than inside thesuit), which was approximately twice the protectionthan was provided by the next best performingsuits. Traditional Tyvek® (protection factor of 4) wastwice as protective as a standard police uniform(protection factor of 2). These suits were tested byplacing sensors for the test vapor under the suits at17 specific body locations. Volunteers wore the pro-tective gear while performing the activities normally
19 Some chemical-protective fabric manufacturers provide Web-based services for comparing their products. For example, chem-ical permeation and recommended usage charts for DuPont’sTychem® line and related fabric types appear at www2.dupont.com/NOWApp/DPPRequestGateway/0/pct/?command=ACProductComparisonHome and Kappler’s Zytron fabrics are compared atwww.kappler.com/techdata_main.html.

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3 1
ers with respiratory protection and PPE that is atleast as effective as that which the incident com-mander might dictate for the situations EMSresponders could reasonably be expected to en-counter in their designated roles. The employer’sERP should include information on the PPE that theemployer will make available to workers. Becausethis guide recommends Levels A and B for most sit-uations involving EMS responders, such protectionprovides adequate eye protection. Therefore, addi-tional discussion on eye protection is not warranted.
Proper Size and Fit of PPEThe size and fit of PPE is as important as selectingappropriate materials and configurations. Poorly fit-ting respirators, gloves, footwear, or protective cloth-ing offer a reduced level of protection. Specifically,ill-fitting equipment might gape, leak, fall off, causetripping, or create other serious safety hazards.Employers must consider fit in the selection of pro-tective gear for EMS responders, as required byOSHA’s General Requirements for personal protec-tive equipment (29 CFR 1910.132(d)(1)(iii)). EMSresponders who wear tight-fitting respirators must befit tested before the first time they wear the respiratorin the field and again each year. See RespiratoryProtection for an Identified or CharacterizedChemical Hazard, above, for a summary of addition-al requirements associated with respiratory protec-tion.
Considerations for Effectively Using,Maintaining and Storing PPEOnce PPE decisions have been made, the employershould obtain PPE in adequatequantities and sizes to meet theneeds of those EMS responderswho will wear the equipment.Consider protective gear com-patibility when making purchas-es, so that one piece of equip-ment does not interfere with thefunctioning of another. PPE usedto prevent hazardous materialexposure (e.g., a respirator)must be compatible with othersafety equipment required for injury prevention (e.g.,protective eyewear or a helmet). However, planningand purchasing decisions alone will not protect EMSresponders.
Many types of PPE, such as respiratory protection(excluding filtering facepieces) require ongoinginspection, maintenance, worker training, medicalmonitoring, and recordkeeping. For additional infor-mation on this topic, consult OSHA’s standard on
Respiratory Protection (29 CFR 1910.134) and OSHA’sSmall Entity Compliance Guide for RespiratoryProtection at www.osha.gov/Publications/secgrevcurrent.pdf.
EMS responders who are asked to perform activ-ities or work in areas for which they are notequipped should bring this to the attention of theIC (or designated safety officer).
In accordance with OSHA’s PPE standards, and asdiscussed in the Training section of this guide, work-ers must be trained to use PPE effectively and to rec-ognize when PPE will not provide adequate protec-tion. EMS providers risk injury if they becomeexposed to dangerous substances due to a falsesense of security when using incorrect PPE, or whenwearing PPE improperly (Hick, 2007).
Community expectations for EMS providers’ activi-ties and the areas in which they will work must takeinto consideration each employer’s decision aboutworkers’ roles, how PPE is distributed, where equip-ment is stored, and how the employer determines themanner in which personnel are trained to react.Experience has shown that when proper PPE is notreadily available, EMS responders are reluctant to pullback and wait for better equipped providers to arrive.Instead, EMS personnel tend to provide medical res-cue and care without appropriate PPE, thus exposingthemselves to a higher risk (rather than compromis-ing patient care, they compromise their own safety)(Hick, 2007). Personnel training must be adequate toensure that EMS providers fully understand their limi-tations (and those of their training and equipment). IfEMS providers might encounter contaminatedpatients seeking medical assistance, provide medicalcare in a contaminated area or to contaminatedpatients, or be called upon to support fire departmentdecontamination efforts, these individuals must betrained and equipped to do these jobs safely.
Conclusions Regarding PersonalProtective EquipmentCarefully considered EMS responder PPE goeshand-in-hand with the responder’s training; onlywith proper training will EMS responders be able toidentify hazardous substance release conditions andunderstand the limits within which they can worksafely with their available PPE. Determining trainingand PPE needs in advance through a hazard assess-ment will permit employers of EMS responders toensure that their workers are prepared for the inci-dents in which they are expected to participate. ThePPE offered to EMS responders should correspondto both the type of training they are provided and to
Phot
oco
urte
syof
Fran
kCal
ifano
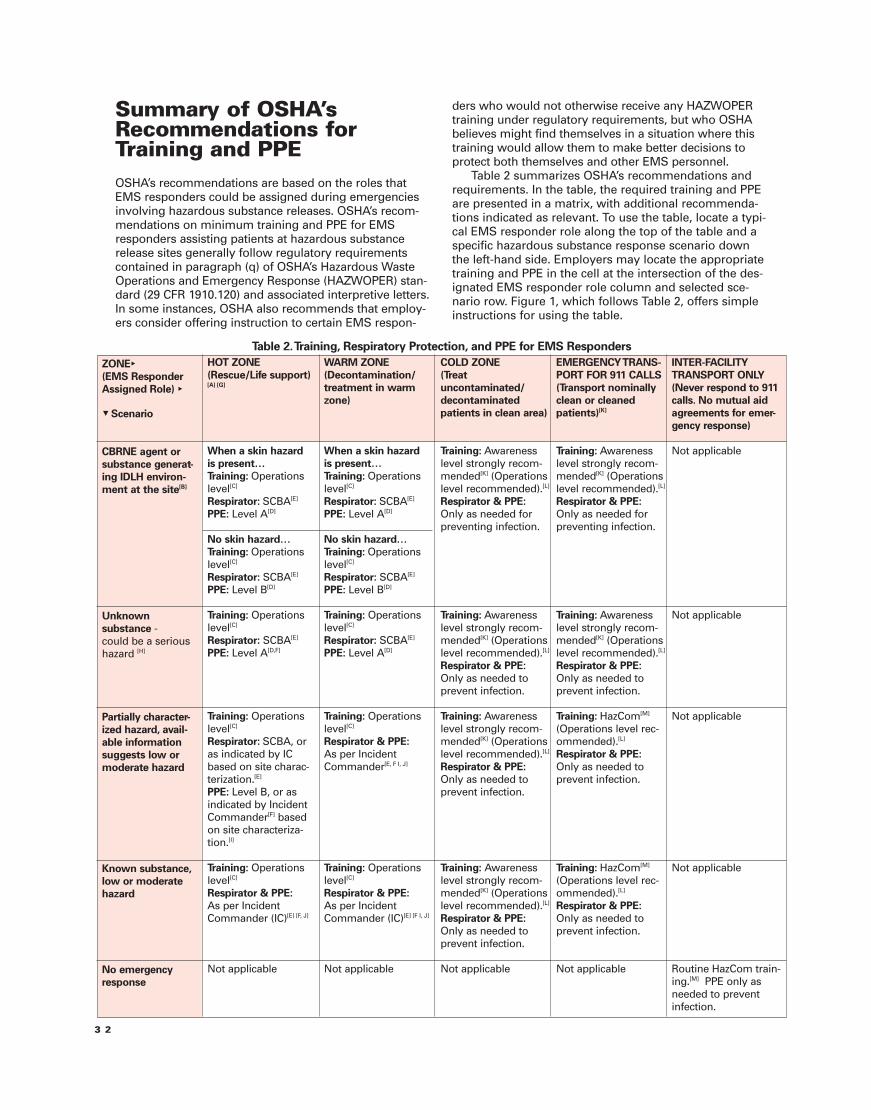
Summary of OSHA’sRecommendations forTraining and PPEOSHA’s recommendations are based on the roles thatEMS responders could be assigned during emergenciesinvolving hazardous substance releases. OSHA’s recom-mendations on minimum training and PPE for EMSresponders assisting patients at hazardous substancerelease sites generally follow regulatory requirementscontained in paragraph (q) of OSHA’s Hazardous WasteOperations and Emergency Response (HAZWOPER) stan-dard (29 CFR 1910.120) and associated interpretive letters.In some instances, OSHA also recommends that employ-ers consider offering instruction to certain EMS respon-
3 2
ders who would not otherwise receive any HAZWOPERtraining under regulatory requirements, but who OSHAbelieves might find themselves in a situation where thistraining would allow them to make better decisions toprotect both themselves and other EMS personnel.
Table 2 summarizes OSHA’s recommendations andrequirements. In the table, the required training and PPEare presented in a matrix, with additional recommenda-tions indicated as relevant. To use the table, locate a typi-cal EMS responder role along the top of the table and aspecific hazardous substance response scenario downthe left-hand side. Employers may locate the appropriatetraining and PPE in the cell at the intersection of the des-ignated EMS responder role column and selected sce-nario row. Figure 1, which follows Table 2, offers simpleinstructions for using the table.
ZONE►(EMS ResponderAssigned Role) ►
▼ Scenario
CBRNE agent orsubstance generat-ing IDLH environ-ment at the site[B]
Unknownsubstance -could be a serioushazard [H]
Partially character-ized hazard, avail-able informationsuggests low ormoderate hazard
Known substance,low or moderatehazard
No emergencyresponse
HOT ZONE(Rescue/Life support)[A] [G]
When a skin hazardis present…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
No skin hazard…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level B[D]
Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D,F]
Training: Operationslevel[C]
Respirator: SCBA, oras indicated by ICbased on site charac-terization.[E]
PPE: Level B, or asindicated by IncidentCommander[F] basedon site characteriza-tion.[I]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander (IC)[E] [F, J]
Not applicable
WARM ZONE(Decontamination/treatment in warmzone)
When a skin hazardis present…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
No skin hazard…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level B[D]
Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander[E, F I, J]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander (IC)[E] [F I, J]
Not applicable
COLD ZONE(Treatuncontaminated/decontaminatedpatients in clean area)
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed forpreventing infection.
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Not applicable
EMERGENCYTRANS-PORT FOR 911 CALLS(Transport nominallyclean or cleanedpatients)[K]
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed forpreventing infection.
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: HazCom[M]
(Operations level rec-ommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: HazCom[M]
(Operations level rec-ommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Not applicable
INTER-FACILITYTRANSPORT ONLY(Never respond to 911calls. No mutual aidagreements for emer-gency response)
Not applicable
Not applicable
Not applicable
Not applicable
Routine HazCom train-ing.[M] PPE only asneeded to preventinfection.
Table 2.Training, Respiratory Protection, and PPE for EMS Responders
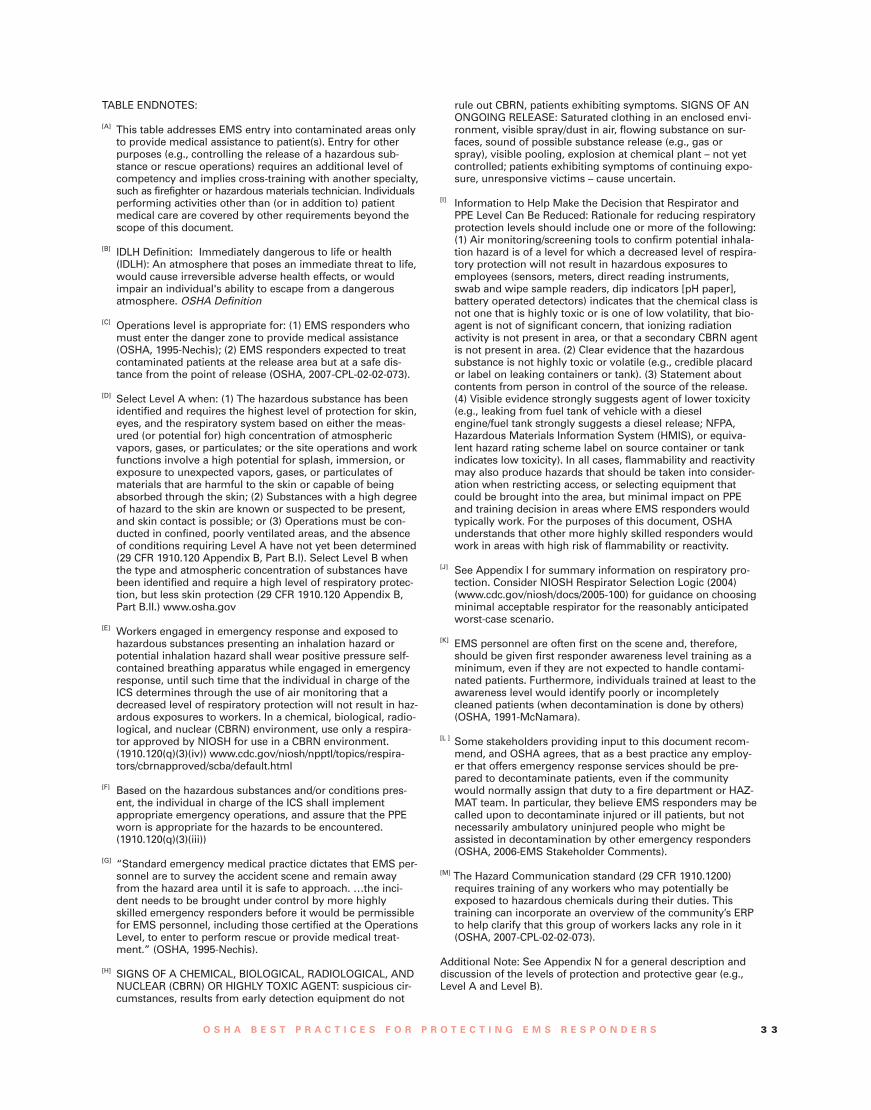
TABLE ENDNOTES:
[A] This table addresses EMS entry into contaminated areas onlyto provide medical assistance to patient(s). Entry for otherpurposes (e.g., controlling the release of a hazardous sub-stance or rescue operations) requires an additional level ofcompetency and implies cross-training with another specialty,such as firefighter or hazardous materials technician. Individualsperforming activities other than (or in addition to) patientmedical care are covered by other requirements beyond thescope of this document.
[B] IDLH Definition: Immediately dangerous to life or health(IDLH): An atmosphere that poses an immediate threat to life,would cause irreversible adverse health effects, or wouldimpair an individual's ability to escape from a dangerousatmosphere. OSHA Definition
[C] Operations level is appropriate for: (1) EMS responders whomust enter the danger zone to provide medical assistance(OSHA, 1995-Nechis); (2) EMS responders expected to treatcontaminated patients at the release area but at a safe dis-tance from the point of release (OSHA, 2007-CPL-02-02-073).
[D] Select Level A when: (1) The hazardous substance has beenidentified and requires the highest level of protection for skin,eyes, and the respiratory system based on either the meas-ured (or potential for) high concentration of atmosphericvapors, gases, or particulates; or the site operations and workfunctions involve a high potential for splash, immersion, orexposure to unexpected vapors, gases, or particulates ofmaterials that are harmful to the skin or capable of beingabsorbed through the skin; (2) Substances with a high degreeof hazard to the skin are known or suspected to be present,and skin contact is possible; or (3) Operations must be con-ducted in confined, poorly ventilated areas, and the absenceof conditions requiring Level A have not yet been determined(29 CFR 1910.120 Appendix B, Part B.I). Select Level B whenthe type and atmospheric concentration of substances havebeen identified and require a high level of respiratory protec-tion, but less skin protection (29 CFR 1910.120 Appendix B,Part B.II.) www.osha.gov
[E] Workers engaged in emergency response and exposed tohazardous substances presenting an inhalation hazard orpotential inhalation hazard shall wear positive pressure self-contained breathing apparatus while engaged in emergencyresponse, until such time that the individual in charge of theICS determines through the use of air monitoring that adecreased level of respiratory protection will not result in haz-ardous exposures to workers. In a chemical, biological, radio-logical, and nuclear (CBRN) environment, use only a respira-tor approved by NIOSH for use in a CBRN environment.(1910.120(q)(3)(iv)) www.cdc.gov/niosh/npptl/topics/respira-tors/cbrnapproved/scba/default.html
[F] Based on the hazardous substances and/or conditions pres-ent, the individual in charge of the ICS shall implementappropriate emergency operations, and assure that the PPEworn is appropriate for the hazards to be encountered.(1910.120(q)(3)(iii))
[G] “Standard emergency medical practice dictates that EMS per-sonnel are to survey the accident scene and remain awayfrom the hazard area until it is safe to approach. …the inci-dent needs to be brought under control by more highlyskilled emergency responders before it would be permissiblefor EMS personnel, including those certified at the OperationsLevel, to enter to perform rescue or provide medical treat-ment.” (OSHA, 1995-Nechis).
[H] SIGNS OF A CHEMICAL, BIOLOGICAL, RADIOLOGICAL, ANDNUCLEAR (CBRN) OR HIGHLY TOXIC AGENT: suspicious cir-cumstances, results from early detection equipment do not
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3 3
rule out CBRN, patients exhibiting symptoms. SIGNS OF ANONGOING RELEASE: Saturated clothing in an enclosed envi-ronment, visible spray/dust in air, flowing substance on sur-faces, sound of possible substance release (e.g., gas orspray), visible pooling, explosion at chemical plant – not yetcontrolled; patients exhibiting symptoms of continuing expo-sure, unresponsive victims – cause uncertain.
[I] Information to Help Make the Decision that Respirator andPPE Level Can Be Reduced: Rationale for reducing respiratoryprotection levels should include one or more of the following:(1) Air monitoring/screening tools to confirm potential inhala-tion hazard is of a level for which a decreased level of respira-tory protection will not result in hazardous exposures toemployees (sensors, meters, direct reading instruments,swab and wipe sample readers, dip indicators [pH paper],battery operated detectors) indicates that the chemical class isnot one that is highly toxic or is one of low volatility, that bio-agent is not of significant concern, that ionizing radiationactivity is not present in area, or that a secondary CBRN agentis not present in area. (2) Clear evidence that the hazardoussubstance is not highly toxic or volatile (e.g., credible placardor label on leaking containers or tank). (3) Statement aboutcontents from person in control of the source of the release.(4) Visible evidence strongly suggests agent of lower toxicity(e.g., leaking from fuel tank of vehicle with a dieselengine/fuel tank strongly suggests a diesel release; NFPA,Hazardous Materials Information System (HMIS), or equiva-lent hazard rating scheme label on source container or tankindicates low toxicity). In all cases, flammability and reactivitymay also produce hazards that should be taken into consider-ation when restricting access, or selecting equipment thatcould be brought into the area, but minimal impact on PPEand training decision in areas where EMS responders wouldtypically work. For the purposes of this document, OSHAunderstands that other more highly skilled responders wouldwork in areas with high risk of flammability or reactivity.
[J] See Appendix I for summary information on respiratory pro-tection. Consider NIOSH Respirator Selection Logic (2004)(www.cdc.gov/niosh/docs/2005-100) for guidance on choosingminimal acceptable respirator for the reasonably anticipatedworst-case scenario.
[K] EMS personnel are often first on the scene and, therefore,should be given first responder awareness level training as aminimum, even if they are not expected to handle contami-nated patients. Furthermore, individuals trained at least to theawareness level would identify poorly or incompletelycleaned patients (when decontamination is done by others)(OSHA, 1991-McNamara).
[L ] Some stakeholders providing input to this document recom-mend, and OSHA agrees, that as a best practice any employ-er that offers emergency response services should be pre-pared to decontaminate patients, even if the communitywould normally assign that duty to a fire department or HAZ-MAT team. In particular, they believe EMS responders may becalled upon to decontaminate injured or ill patients, but notnecessarily ambulatory uninjured people who might beassisted in decontamination by other emergency responders(OSHA, 2006-EMS Stakeholder Comments).
[M] The Hazard Communication standard (29 CFR 1910.1200)requires training of any workers who may potentially beexposed to hazardous chemicals during their duties. Thistraining can incorporate an overview of the community’s ERPto help clarify that this group of workers lacks any role in it(OSHA, 2007-CPL-02-02-073).
Additional Note: See Appendix N for a general description anddiscussion of the levels of protection and protective gear (e.g.,Level A and Level B).
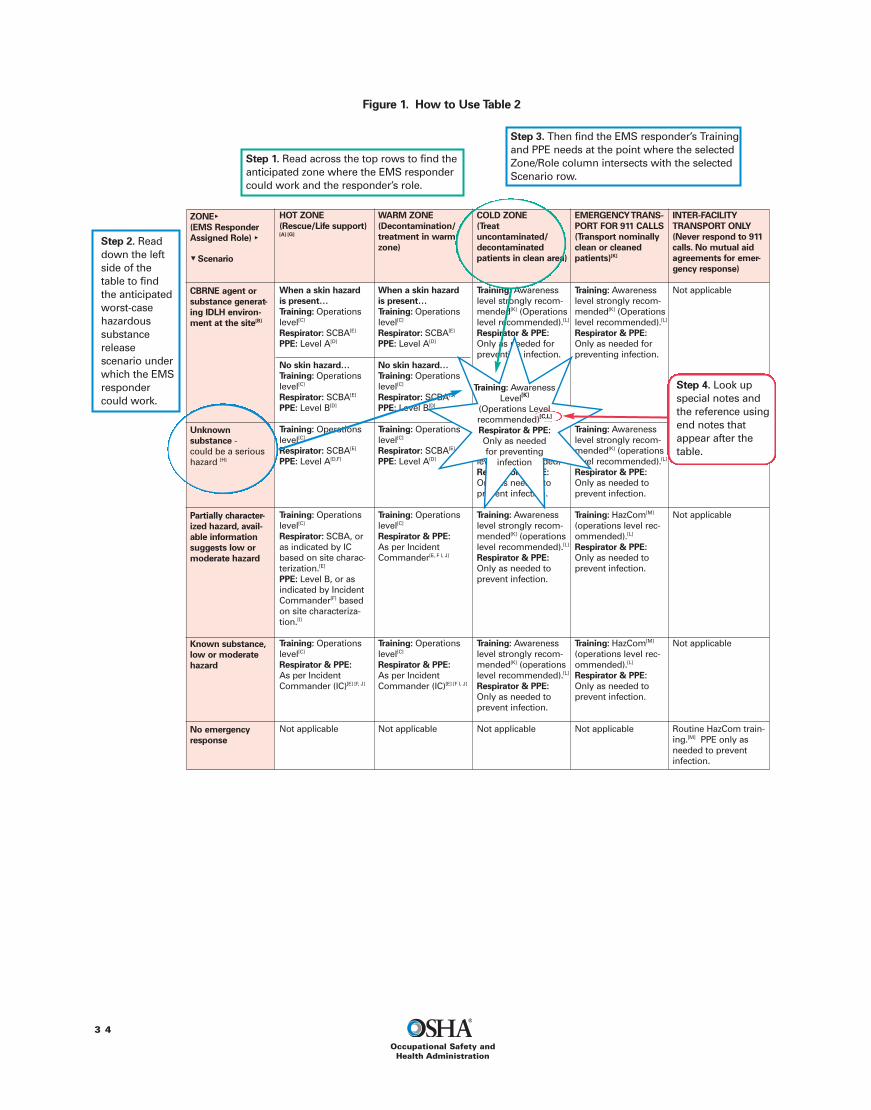
ZONE►(EMS ResponderAssigned Role) ►
▼ Scenario
CBRNE agent orsubstance generat-ing IDLH environ-ment at the site[B]
Unknownsubstance -could be a serioushazard [H]
Partially character-ized hazard, avail-able informationsuggests low ormoderate hazard
Known substance,low or moderatehazard
No emergencyresponse
HOT ZONE(Rescue/Life support)[A] [G]
When a skin hazardis present…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
No skin hazard…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level B[D]
Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D,F]
Training: Operationslevel[C]
Respirator: SCBA, oras indicated by ICbased on site charac-terization.[E]
PPE: Level B, or asindicated by IncidentCommander[F] basedon site characteriza-tion.[I]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander (IC)[E] [F, J]
Not applicable
WARM ZONE(Decontamination/treatment in warmzone)
When a skin hazardis present…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
No skin hazard…Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level B[D]
Training: Operationslevel[C]
Respirator: SCBA[E]
PPE: Level A[D]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander[E, F I, J]
Training: Operationslevel[C]
Respirator & PPE:As per IncidentCommander (IC)[E] [F I, J]
Not applicable
COLD ZONE(Treatuncontaminated/decontaminatedpatients in clean area)
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed forpreventing infection.
Training: Awarenesslevel strongly recom-mended[K] (operationslevel recommended)[L].Respirator & PPE:Only as needed toprevent infection.
Training: Awarenesslevel strongly recom-mended[K] (operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: Awarenesslevel strongly recom-mended[K] (operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Not applicable
EMERGENCYTRANS-PORT FOR 911 CALLS(Transport nominallyclean or cleanedpatients)[K]
Training: Awarenesslevel strongly recom-mended[K] (Operationslevel recommended).[L]
Respirator & PPE:Only as needed forpreventing infection.
Training: Awarenesslevel strongly recom-mended[K] (operationslevel recommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: HazCom[M]
(operations level rec-ommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Training: HazCom[M]
(operations level rec-ommended).[L]
Respirator & PPE:Only as needed toprevent infection.
Not applicable
INTER-FACILITYTRANSPORT ONLY(Never respond to 911calls. No mutual aidagreements for emer-gency response)
Not applicable
Not applicable
Not applicable
Not applicable
Routine HazCom train-ing.[M] PPE only asneeded to preventinfection.
3 4
Occupational Safety andHealth Administration
Figure 1. How to Use Table 2
Step 2. Readdown the leftside of thetable to findthe anticipatedworst-casehazardoussubstancereleasescenario underwhich the EMSrespondercould work.
Step 1. Read across the top rows to find theanticipated zone where the EMS respondercould work and the responder’s role.
Step 3. Then find the EMS responder’s Trainingand PPE needs at the point where the selectedZone/Role column intersects with the selectedScenario row.
Step 4. Look upspecial notes andthe reference usingend notes thatappear after thetable.
Training: AwarenessLevel[K]
(Operations Levelrecommended)[C,L]
Respirator & PPE:Only as neededfor preventing
infection
Best Practices forPre-Transport PatientDecontamination
Patient decontamination is critical to patient safety,to the protection of EMS personnel, and to continu-ing EMS operations. Many communities placeresponsibility for decontamination activities on thefire department or incident response personnel,without directly involving EMS responders. Othercommunities ask EMS responders to assist with theprocess. Some stakeholders providing input to thisdocument recommended that any employer thatoffers emergency response services should be pre-pared to decontaminate patients, even if the com-munity would normally assign that duty to a firedepartment or HAZMAT team. In particular, theybelieve EMS responders may be called upon todecontaminate injured or ill patients, but not neces-sarily ambulatory uninjured people who might beassisted in decontamination by other emergencyresponders (OSHA, 2006-EMS StakeholderComments).20
Regardless of which responders will performdecontamination, OSHA believes that EMS respon-ders who might be sent to the scene of a releasewill be better prepared to recognize an inadequate-ly decontaminated patient if they understand thebasic decontamination process, even if these EMSresponders are not expected to be involved inpatient decontamination.
As a best practice, OSHA recommends thatemployers provide information on decontaminationpractices to all EMS responders who could beassigned a role in a hazardous substance response.Additional detailed training on performing decontami-nation is required for EMS responders whom theemployer has designated to perform decontamination.
Current accepted decontamination practicesfocus on removing the patient’s clothing, cleansingwith soap and water, then rinsing. When thesesteps are followed carefully, patient exposure is sig-nificantly decreased and patients pose less risk toEMS personnel, transport vehicles and equipment.
Removing Contaminated Clothingand Personal EffectsStudies estimate that removing contaminated cloth-ing can reduce the quantity of contaminant associ-ated with victims by an estimated 75 to 90 percent
(Macintyre et al., 2000; Vogt, 2002; USACHPPM,2003a).21 Modeling studies that help quantify expo-sures during decontamination and patient handlingactivities suggest that victims’ clothing can hold asignificant amount of contaminant. Removing con-taminated clothing as soon as possible will reduceboth patient and responder exposure levels (Schultzet al., 1995; Georgopoulos et al., 2004). The soonercontaminated clothing and effects are removed theless these potential sources will contribute to expo-sure levels.
Clothing and personal items that are contami-nated should be sealed in double plastic bags toeliminate them as a source of continuing exposure.
Many community plans provide for somepatient privacy and protection from harsh weatherduring decontamination. The plans also often callfor the provision of tags to label bagged personalbelongings with the owners’ names. These provi-sions can help improve patients’ compliance withdecontamination procedures.
Cleansing with Soap and WaterDecontamination with soap and water remains thebest practice for most contaminants under most cir-cumstances of mass decontamination. Initial rinsingcan often be started quickly and will help physicallyremove water-soluble and particulate contaminants,while a soap that dissolves grease will help removeother substances.
Hurst (1997) notes that “the most important andmost effective decontamination after any chemicalor biological exposure is that decontaminationdone within the first minute or two after exposure”and that “after years of research world wide, simpleprinciples that consistently produce good resultsare still recommended.” Specifically, timely physi-cal removal of the contaminating substance is criti-cal. However, “which decontamination method isused is not as important as how and when it isused.” (Hurst, 1997).
OSHA realizes that, although generally considereda beneficial practice, 5 minutes of flushing with
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3 5
20 The stakeholders feel, however, that it makes less sense to sug-gest that EMS responders decontaminate ambulatory uninjuredpeople (OSHA EMS Stakeholder Comments, 2006).
21 The percentage of contaminant reduction depends on the typeof clothing the victim was wearing when exposed. The estimatesmay be somewhat lower (down to 50 percent) for victims wear-ing short pants or skirts and higher (up to 94 percent) for victimsexposed to biological warfare agents while wearing protectivemilitary uniforms (USACHPPM, 2003a).

rinse water may not always be practical in the field.It serves primarily as a benchmark to guide deci-sion making. USACHPPM recommends 1-minuterinsing from head to toe with tepid water (slightlywarm, not hot) after removal of contaminated cloth-ing, followed by a more thorough decontaminationby washing with a soap with good surfactant prop-erties (e.g., a liquid soap such as hand dishwashingdetergent), tepid water and soft sponges. Avoid stiffbrushes and vigorous scrubbing, which can dam-age the skin and increase the chance that the con-taminant would be absorbed by the patient’s skin.USACHPPM recommends these procedures formost classes of contaminants, except reactivemetal dusts, for which a soft dry brush should beused to remove most of the material from the skin.(USACHPPM, 2003a).
Assistance for Non-Ambulatory andAmbulatory PatientsNon-ambulatory patients can require a substantialproportion of the decontamination team’s time andeffort. EMS responders designated as decontamina-tion team members are likely to experience thegreatest exposures while assisting these patients.22
The team members should take steps to identifypossible sources of contamination and limit theirexposure to those sources, as well as the exposureof patients and any EMS responders who mayassist the patients later. For example, it is possibleto use specific procedures for removing patients’clothing to minimize both decontamination teamand patient exposures. One such procedure is touse blunt-nose scissors to cut away clothing, ratherthan pulling it off. Practical exercises have shownthat seatbelt cutters also work well for removingclothing and further reduce the chance of accidentalinjury.23 In contrast, tugging on clothing can pro-duce a wringing action that might distribute con-taminant on the patient, decontamination teammembers, and the surrounding area (in addition tounnecessarily shifting a patient who may havespinal injuries). As noted previously, once removed,the clothing should be immediately placed into asealed container.
Some communities may ask ambulatorypatients to assist by performing some of the decon-tamination steps themselves. Specifically, minimal-
3 6
Occupational Safety andHealth Administration
ly exposed patients who are able can help by re-moving their own clothing and personal effects.They may even begin wetting and cleansing them-selves, although these and subsequent stepsshould be supervised (if not performed) by aresponder trained in decontamination procedures.When ambulatory patients assist with these initialdecontamination steps during large-scale incidents,decontamination of all patients may be more expe-dient, and the risks to responders (e.g., from han-dling contaminated clothing) are reduced.
The methods decontamination team membersuse to decontaminate themselves and remove(doff) PPE also impact their own exposure. ATSDR(2001) and Appendix M offer examples of proce-dures used by some teams.
EMS responders might find the following reviewof basic decontamination steps helpful:
1) Activate the emergency decontaminationplan.
2) Learn as much as possible (as soon as possi-ble) about the location of patients, the con-taminant, its hazards, and associated symp-toms. Previous arrangements with other firstresponder agencies can improve how infor-mation flows to responders.
3) Arrange for decontamination equipment tobe delivered to a suitable location. Some sys-tems are heavy and cumbersome – in addi-tion to the need for an adequate area of rela-tively level ground, consider factors such asvehicular access to deliver equipment andalso eventually to provide ambulance serviceto patients who require it.
4) Activate the decontamination system andassemble the decontamination team. Theseindividuals should be pre-designated by thecommunity plan so that they will be properlytrained and have drilled with the availableequipment prior to the emergency. Also inadvance, the community should consider theneed for staffing multiple decontaminationlines (for responders, ambulatory patients,and non-ambulatory patients; or males andfemales), which can increase patient compli-ance and/or process efficiency. Consider bywhom and where decontamination for criti-cally ill/injured patients will be performed.
5) Perform any medical monitoring (e.g., vitalsigns) of decontamination team members, ifspecified by the community or EMS agencyplan.
6) Put on PPE.
22 OSHA understands that decontamination teams will consist offirefighters, HAZMAT team members, and/or EMS personnel whoare FULLY qualified to do so and are wearing adequate protectiveequipment.23 Seatbelt cutters are not as useful for cutting through thick tapearound responder’s boots; shears work better for this type of material.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3 7
7) Triage patients to determine which individualsrequire decontamination and provide criticalmedical treatment to stabilize them beforedecontamination.
8) Direct or assist patients (ambulatory and non-ambulatory) in removing contaminated cloth-ing and securing personal property as soonas possible (within minutes of arrival).
9) Place clothing and other contaminated itemsin a plastic bag that can be sealed (or whenavailable, place items in an approved haz-ardous waste container and cover). Ensurethat waste bags/containers are isolated andremain outdoors so that the items are not acontinuing source of exposure.
10) Perform gross decontamination with water(extensive amounts, if available), such as froma hose. More time-consuming technical decon-tamination may be necessary to completelyremove contaminant. This more thoroughdecontamination procedure involves washingpatients using soap, with good surface-activeproperties (i.e., soaps that help oil dissolve inwater), and water (preferably tepid water toimprove patient compliance). Pay particularattention to the back and hair on the head orbody. Make sure that hair wash water fallsaway from the body, if possible. Remove allobvious contamination on a patient with gentleblotting or brushing, never rub or irritate theskin. Avoid abrasive materials (such as “gritty”soaps). This step should also include copiousrinsing, especially when dealing with acids orbases. [See discussion, below.] Ambulatorypatients may be able to clean themselvesunder direction of the decontamination team.
11) Inspect patients to evaluate the effectivenessof decontamination. Guide decontaminatedpatients to the medical treatment area (awayfrom any possible contamination). Returninadequately decontaminated patients to theshower area and repeat cleansing.
12) Decontaminate equipment and the decontam-ination system (if not disposable).
13) Decontamination team removes PPE anddecontaminates themselves. The order inwhich PPE is removed during responderdecontamination can help minimize addition-al exposure. See Appendix M for an exampleof a sequence for putting on (donning),decontaminating, and removing (doffing) PPE.
14) Patient inspection provides a final check toensure that contaminant is not carried intoclean areas.
Decontamination procedures, like PPE use, canbe modified once the contaminant is identified;decontamination team members who are cleansingpatients to remove known contaminants can tailorprocedures as appropriate. For example, a longerrinse might be beneficial for contamination in theeyes, or for contamination involving corrosive,sticky, or oil-soluble substances. Organizations suchas the Centers for Disease Control and Prevention(CDC) and the U.S. Department of HomelandSecurity offer specific recommendations for de-contaminating patients exposed to individual haz-ards, such as ionizing radiation (CDC, 2003; U.S.Department of Homeland Security, 2003).24
Determining the adequacy of decontaminationefforts is a recurring issue in community prepared-ness discussions. If it was known that patients wereexposed to nerve agents and a decontaminationteam had access to appropriate testing media (e.g.,surface testing tapes), this confirmation could behelpful. Although contaminant detection equipmentis available for certain other hazardous substances(such as radiological hazards), in most cases confir-mation that a patient has been carefully washed bya trained decontamination team still offers the bestassurance of safety for EMS responders, vehiclesand equipment. As previously discussed, OSHAstrongly recommends that employers train to thefirst responder awareness level all EMS responderswho could transport decontaminated patients froma hazardous substance emergency site, and as abest practice train them as first responders at theoperations level.
Decontamination in LowWater SituationsDecontamination with extensive amounts of waterremains the preferred method; however, for lowwater situations, other methods can help physicallyremove contaminant from patients. Several militaryand civilian organizations are investigating deconta-mination aids for use in situations when little or nowater is available or when cold weather makeswater less practical. These methods include target-ed application of available water, bulk absorbentsand reactive foams.
Once contaminated clothing is removed, spotdecontamination can be performed using littlewater targeted to the skin that was originallyexposed (typically the hands and head/hair). Usingthis method, it might be possible to perform gross
24 The International Commission on Radiological Protection(ICRP) and the National Council on Radiation Protection andMeasurements (NCRP) also offer guidance for radiological inci-dents.

decontamination with a hand-pump sprayer and afew gallons of water.
Hurst (1997) reviewed decades of literature ondecontamination methods and noted that an appli-cation of flour, followed by wet tissue wipes offerssome benefit in reducing the amount of chemicalsubstances left on the skin. Nevertheless, bulk dryabsorbents tend to be most useful (and have tradi-tionally been used) for decontaminating large sur-face areas and points where contaminant haspooled. The best absorbent for a job depends onthe contaminant, but any non-reactive substancewith a large porous surface area has potential toserve as a sorbent. Materials considered by the U.S.Army for use in cold weather would also serveunder conditions where little water is available; sug-gested practices for conducting gross decontamina-tion include blotting patients with sorbent sub-stances such as paper towels, flour, sand, dirt, an oilabsorbent, or diatomaceous earth (Fuller’s earth)with the intent of removing harmful material fromthe patient as quickly as possible (SBCCOM, 2002).As noted previously, patients’ clothing should beremoved as soon as possible to achieve the maxi-mum benefit.
Gross decontamination with sorbent should befollowed up as soon as feasible with a warm waterwash. Various foams and creams may play a role inthe future, but at this time these products are notapproved for use on human skin (see Appendix L -Decontamination Foam and Barrier Cream).
Vehicle and Equipment DecontaminationPrevention is the best policy for protecting vehiclesfrom contamination. Some industrial chemicals canbe neutralized,but many willbe difficult toremove fromporous materi-als and cracks/crevices in theinterior. If con-taminated, thevehicle may need to be taken out of service.
Decontamination of non-porous equipmentmaterials follows a similar process to decontamina-tion of skin (wash with extensive amounts of waterand soap, rinse thoroughly, inspect carefully),although equipment can be scrubbed. Porous mate-rials are more difficult to clean effectively and mostlikely will need to be discarded with other wastefrom the response and decontamination effort. AnOSHA letter of interpretation advises eliminating or
minimizing soft plush surfaces where they mightneed to be decontaminated later (OSHA, 1994-Bays).
Discovering that a Patient in theAmbulance is ContaminatedEMS providers should make every effort to preventambulances from becoming contaminated.Contamination of an ambulance, and the EMS per-sonnel associated with it, could cause them to beremoved from service and decrease the availabilityof these critical resources. Representatives of theEMS community requested guidance in addressingthis possible scenario.
OSHA believes that prevention is the first lineof defense for preserving emergency medicalresources. EMS responders should communicatewith other first responders and decontaminationteams regarding the extent of patient exposure andthe decontamination processes used to cleanpatients. This information will help ambulanceoperators ensure that only uncontaminated/cleanpatients are loaded into the vehicle. EMS respon-ders who suspect residual contamination on apatient should not hesitate to suggest that thepatient be returned to the wash area for additionalcleaning.
In practice, however, it is possible that EMS per-sonnel could discover evidence of contaminationassociated with a patient who is already beingtransported, although that patient was believed tobe clean.25 In this situation, efforts should focus onminimizing further spread of the contaminant andon (further) decontamination. Ambulance operatorsshould take the following steps:
En Route
• Notify the receiving hospital that the incomingpatient shows evidence of possible contamina-tion so that decontamination procedures can beactivated.
• Verify that all clothing and personal effects arecompletely removed and sealed in plastic bags(double layer).
• Take available steps to contain the spread of con-tamination to vehicle and personnel (e.g., wrappatient in disposable tarp or blanket if allowedby patient care protocol).
3 8
Occupational Safety andHealth Administration
25 It is also possible that EMS responders might be instructed totransport a contaminated patient. In this case, the respondersshould confirm that the incident commander is aware that suchan action may cause the ambulance and crew to be taken out ofservice.
Phot
oco
urte
syof
Fran
kCal
ifano

• Alert the incident site that a patient in transitshows signs of contamination (describe the evi-dence) so that ongoing patient handling anddecontamination procedures at the site can bemodified appropriately.
Upon Arrival at the Receiving Hospital
• Treat EMS responders as victims, requiringdecontamination and/or treatment, until it is pos-sible to confirm that they have not suffered illeffects.
• Remove the ambulance from service and arrangeto have it surveyed immediately to determinewhether it can be placed back in service.
Certain ambulance designs can help reduceexposure to airborne contaminants, but do not pre-vent exposure. For example, NIOSH investigatorsresearching tuberculosis (TB) exposure controlsevaluated the effectiveness of supplemental highefficiency particulate air (HEPA) filtration systems inambulances (NIOSH, 1996).26 In tests conductedunder similar conditions, airborne particles werecleared more rapidly from the air inside an ambu-lance equipped with supplemental HEPA filtrationthan from an ambulance without HEPA filtration.Furthermore, testing showed that “particle clearancecould be improved with the use of the rear vent fan”(turned to the “high” setting) in combination withfresh air provided through the ambulance’s mainheating and cooling system. Running the rear ventfan provided some particle clearance even in anambulance that was not fitted with HEPA filters, inpart because running the vent fan increased airexchange in the ambulance. With the main heatingand cooling system, HEPA filtration system, and rearvent all running, the volume of air in the rear com-partment of the ambulance was replaced at a rate ofalmost once per minute (56 air changes per hour).The investigators note that “while supplementalengineering controls such as [HEPA filtration] canimprove particulate clearance in the ambulance, theywill not eliminate the potential for exposure….”When HEPA filtration systems are used, consult themanufacturer to determine the optimal testing andmaintenance schedule (NIOSH, 1996).
Detection EquipmentDetection InstrumentsNumerous instruments allow EMS responders todetect contaminant levels with varying degrees ofprecision. Easy-to-use ionizing radiation meters per-
form well during emergency medical responsesand may be used to evaluate both contaminatedpatients/equipment and the effectiveness of decon-tamination processes. EMS responders face agreater challenge in identifying chemically or bio-logically contaminated individuals at the scene, bothbefore and after decontamination procedures.
The first indication of the need to activate thedecontamination team might come from firstresponders who identify contaminated individualsthrough an initial interview, by visual observation,by the presence of indicative odors, and throughsigns that a substance appears to be affectinghealth. After a patient has been through the decon-tamination system, to confirm cleanliness, EMSresponders currently rely primarily on visual inspec-tion and the extent to which the patient followedprescribed showering procedures. Ionizing radiationdetectors effectively contribute valuable screeninginformation. In contrast, for most chemical sub-stances the currently available simple, portablechemical detection equipment can supplementthese methods, but do not replace them.
Ionizing Radiation MetersIonizing radiation occurs in three major forms –alpha, beta, and gamma radiation.27 Most radiologi-cal substances emit one or more of these forms ofradiation. Of the three, alpha radiation, in general,has the highest energy and is most hazardous ifingested or inhaled, but presents minimal hazardoutside the body. Beta radiation (typically with lessenergy) can cause skin burns at close range (i.e.,skin contamination). Patients can become contami-nated with alpha- or beta-emitting radioactive mate-rials if these materials are released during a haz-ardous substance incident. Inhalation and ingestionof these particles can be greatly reduced by remov-ing contaminated clothing and washing thoroughly(EPA RERT, 2007).
Two different exposure scenarios are possible forphoton/gamma radiation, which exists in the formof energy that passes through the body, causingdamage to organs and tissues in its path. Thesource of gamma radiation could be either (1)gamma-emitting radioactive materials (contami-nants released during a hazardous substance inci-dent), or (2) a discrete gamma-emitting source ofradiation. In the first case, decontamination proce-dures will help remove the gamma-emitting materi-als from skin, which will reduce the radiation expo-sure, and subsequently the risk, to patients and
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 3 9
26 HEPA filters are capable of removing 99.97 percent of the parti-cles that are less than 0.3 microns in diameter (the most pene-trating – or worst case – size).
27 Photon radiation types include gamma radiation, x-radiation,and “bremsstrahlung” (a type of electromagnetic energy).

responders. In the second case, if only photon/gamma radiation is released from a specific discretesource and no gamma-emitting material contami-nants (e.g., dusts) are involved, then gamma radia-tion will be emitted through the area exposingpatients (and responders) in the area until thesource is removed from the area or shielded with anappropriate material such as lead. Exposure can becontrolled by moving the patient to a safe location.When the source of gamma emission is removed orshielded, the gamma radiation exposure will alsostop. Patients who were initially exposed by theemitting source may have lingering health effectsfrom that initial exposure, but will not have addi-tional exposure after the gamma-emitting source isremoved. These patients may not benefit fromdecontamination procedures unless they are con-taminated with other substances that need to beremoved. Likewise, EMS responders will not experi-ence gamma radiation exposure if they arrive onthe scene after the discrete gamma-emitting sourceis removed.
It is important that ionizing radiation meters (andassociated probes) used by EMS responders beselected based on the types of radiological materi-als with which patients could be contaminated. Ifradiation is suspected, a health physicist should beconsulted (EPA RERT, 2007).
Relatively reliable and easy-to-use instrumentsare available for measuring beta and gamma formsof ionizing radiation (e.g., survey meters fitted witha Geiger-Mueller detector or “GM probe,” of whicha “pancake” probe is one common example). Thistype of instrument typically functions as a ratemeter and provides a reading in the units of “countsper minute” in analog or digital form. 28 For evaluat-ing patient contamination, EMS responders mightfind it helpful to have access to a rate meter with a“scaler” feature. A scaler displays an integrated dig-ital readout for a preset sample period, selected bythe operator, at a point of potential contamination(e.g., a patient’s hair). The integrated digital readoutis easy to compare to readings from other parts ofthe body or to background readings taken at a dis-tance from the patient.
Because these probes are sensitive to gamma, x,alpha, and beta radiations, they will always detectthe natural background radiation levels. Unless fullyshielded, they do not read zero, even in an environ-ment that is not radiologically contaminated. For
this reason, GM probe values are more useful forcomparing contamination levels at different specificpositions (i.e., comparing a point of suspected con-tamination to a non-contaminated point) rather thanfor checking radiation levels against specific fixedcriteria (EPA RERT, 2007).29 The U.S. Department ofHealth and Human Services’ Radiological EventMedical Management Web site contains detailedinformation on the use of GM meters during patientcontamination evaluations and other helpful guid-ance for providing medical services during a radio-logical emergency (see http://remm.nlm.nih.gov/index.html). Figure 2, at page 41, adapted from thatWeb site, describes how to use a radiation meter toconduct a survey for radioactive contamination on apatient or an emergency responder.
These same GM meters will detect alpha radia-tion to a limited extent, but are less sensitive formonitoring the presence of low-level alpha detec-tion during decontamination procedures. Whenalpha radiation is present, a survey meter with analpha scintillation probe is preferable for evaluatingthe alpha radiation. Alpha detectors are best usedby an experienced operator under the direction of ahealth physicist. These professionals will also bebetter equipped to determine whether more thanone type of radiation is present (e.g., alpha andbeta, or beta and gamma).
Decontamination after a radiological materialsevent involves mechanical removal of the radioac-tive particles from the individual. The process caninclude washing, wiping, or irrigating the area. Thedecontamination team should take care not to scruband abrade the skin. Once decontamination hasbeen performed, the area should be resurveyedwith a survey meter and appropriate probe. Decon-tamination efforts should continue until there is nomeasurable decrease in the count rate.
Chemical and Biological AgentDetection EquipmentThere is no single ideal chemical or biological agentmeter (or even two or three meters) that will meetall the needs of EMS responders. The requirementsof this group of responders are particularly highbecause EMS responders have restricted space tocarry equipment, are generally not hazardous sub-
4 0
Occupational Safety andHealth Administration
28 GM meters, such as the popular Ludlum Model 12 rate meterand equivalents are readily available from commercial sourcesand may come equipped with a range of optional features. A900-volt model will likely be most practical for EMS responders(EPA RERT, 2007).
29 DOE has specific criteria for fixed and removable contamina-tion values in 10 CFR 835 Appendix D, summarized on theLawrence Berkeley National Laboratory Web site at http://uclbl.org/ehs/orps/pdf/radContamination.pdf. The Radiological EventMedical Management Web site, http://remm.nlm.gov/remm_RadPhysics.htm#pag, lists allowable limits of radiation for thegeneral public and radiation workers, and guidelines for radiationresponse worker exposure.
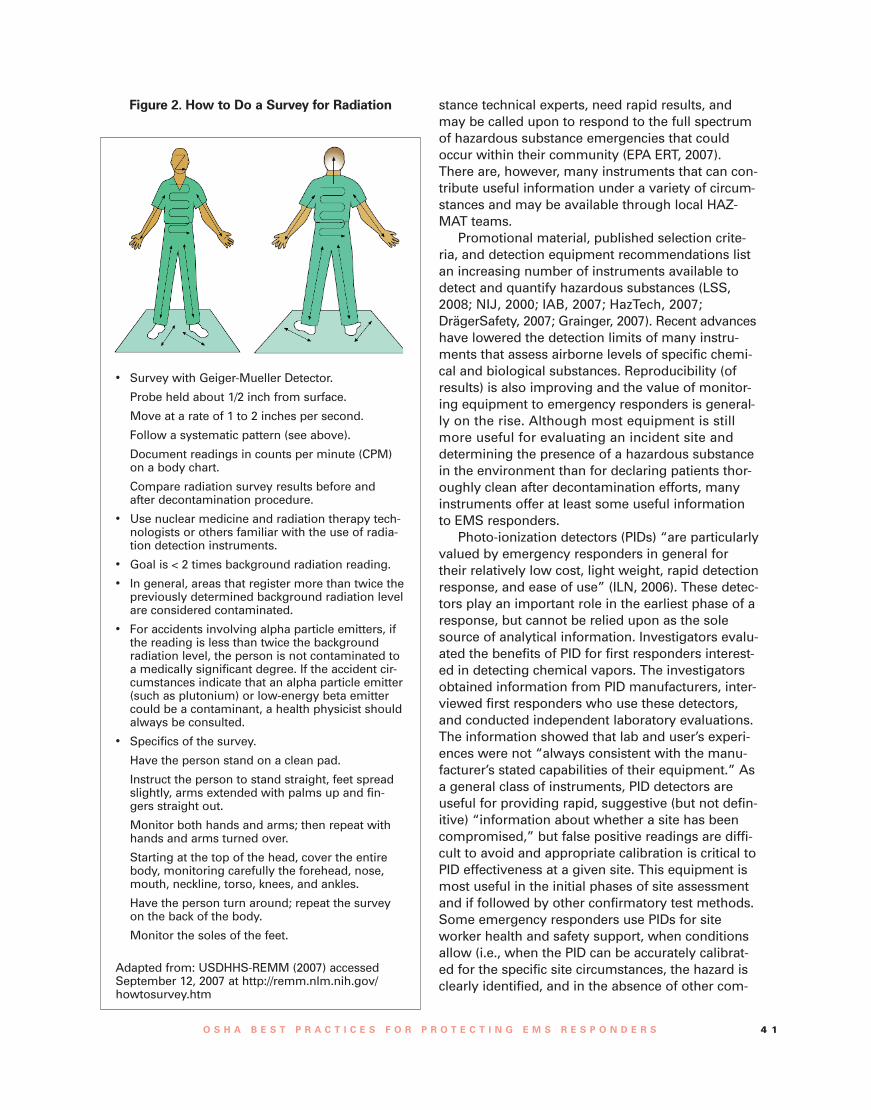
stance technical experts, need rapid results, andmay be called upon to respond to the full spectrumof hazardous substance emergencies that couldoccur within their community (EPA ERT, 2007).There are, however, many instruments that can con-tribute useful information under a variety of circum-stances and may be available through local HAZ-MAT teams.
Promotional material, published selection crite-ria, and detection equipment recommendations listan increasing number of instruments available todetect and quantify hazardous substances (LSS,2008; NIJ, 2000; IAB, 2007; HazTech, 2007;DrägerSafety, 2007; Grainger, 2007). Recent advanceshave lowered the detection limits of many instru-ments that assess airborne levels of specific chemi-cal and biological substances. Reproducibility (ofresults) is also improving and the value of monitor-ing equipment to emergency responders is general-ly on the rise. Although most equipment is stillmore useful for evaluating an incident site anddetermining the presence of a hazardous substancein the environment than for declaring patients thor-oughly clean after decontamination efforts, manyinstruments offer at least some useful informationto EMS responders.
Photo-ionization detectors (PIDs) “are particularlyvalued by emergency responders in general fortheir relatively low cost, light weight, rapid detectionresponse, and ease of use” (ILN, 2006). These detec-tors play an important role in the earliest phase of aresponse, but cannot be relied upon as the solesource of analytical information. Investigators evalu-ated the benefits of PID for first responders interest-ed in detecting chemical vapors. The investigatorsobtained information from PID manufacturers, inter-viewed first responders who use these detectors,and conducted independent laboratory evaluations.The information showed that lab and user’s experi-ences were not “always consistent with the manu-facturer’s stated capabilities of their equipment.” Asa general class of instruments, PID detectors areuseful for providing rapid, suggestive (but not defin-itive) “information about whether a site has beencompromised,” but false positive readings are diffi-cult to avoid and appropriate calibration is critical toPID effectiveness at a given site. This equipment ismost useful in the initial phases of site assessmentand if followed by other confirmatory test methods.Some emergency responders use PIDs for siteworker health and safety support, when conditionsallow (i.e., when the PID can be accurately calibrat-ed for the specific site circumstances, the hazard isclearly identified, and in the absence of other com-
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 4 1
• Survey with Geiger-Mueller Detector.
Probe held about 1/2 inch from surface.
Move at a rate of 1 to 2 inches per second.
Follow a systematic pattern (see above).
Document readings in counts per minute (CPM)on a body chart.
Compare radiation survey results before andafter decontamination procedure.
• Use nuclear medicine and radiation therapy tech-nologists or others familiar with the use of radia-tion detection instruments.
• Goal is < 2 times background radiation reading.
• In general, areas that register more than twice thepreviously determined background radiation levelare considered contaminated.
• For accidents involving alpha particle emitters, ifthe reading is less than twice the backgroundradiation level, the person is not contaminated toa medically significant degree. If the accident cir-cumstances indicate that an alpha particle emitter(such as plutonium) or low-energy beta emittercould be a contaminant, a health physicist shouldalways be consulted.
• Specifics of the survey.
Have the person stand on a clean pad.
Instruct the person to stand straight, feet spreadslightly, arms extended with palms up and fin-gers straight out.
Monitor both hands and arms; then repeat withhands and arms turned over.
Starting at the top of the head, cover the entirebody, monitoring carefully the forehead, nose,mouth, neckline, torso, knees, and ankles.
Have the person turn around; repeat the surveyon the back of the body.
Monitor the soles of the feet.
Adapted from: USDHHS-REMM (2007) accessedSeptember 12, 2007 at http://remm.nlm.nih.gov/howtosurvey.htm
Figure 2. How to Do a Survey for Radiation

peting substances that could cause false PID read-ings).
The formal report on the evaluation of PID usefor first responders…
…indicates that PIDs should always be part ofa decision-making context in which other quali-tative and more definitive tests and instru-ments are used to confirm a finding.The per-formance of PIDs, as observed by users andquantified by independent testing, may affectthe ability to make correct field decisions (ILN,2006).30
Other types of detectors are also available foruse with some constraints. Like PIDs, flame ioniza-tion detectors (FID) can be used primarily as ascreening tool, but with verification by other evalua-tion methods. This is because FIDs are subject tointerference by other substances and even humidity.Bulky, but still portable, (shoulder-carried) atomicabsorption and gas chromatograph instruments canprovide more precise and accurate levels of detec-tion and/or chemical specificity. Although theseinstruments often require operators with more spe-cialized training and need careful calibration toobtain meaningful results, HAZMAT teams usingthis equipment may be able to provide EMS respon-ders with useful information on hazardous sub-stance identification and concentration.
User-friendly equipment of adequate sensitivityis available for certain specific agents typically usedas chemical weapons. HAZMAT teams in manycommunities have acquired a selection of handhelddetection meters designed to detect parts per billion(ppb) levels of specific chemical “nerve and blisteragents” used as chemical weapons (e.g., organ-ophosphates and mustard agent) and other sub-stances. Additionally, some of the current broad-spectrum detection devices are capable of detectingclasses of agents (if not the individual agent) withreasonable sensitivity and accuracy. In some cases,other analyses of the basic properties of a sub-stance may provide useful information about itspotential to be toxic, corrosive, volatile or flamma-ble, even when the identity or airborne concentra-tion remain unknown (OSHA, 2006-StakeholderComments).
EMS stakeholders who advised OSHA on thisproject note that the potentially small residualcontaminant on clothing and skin prior todecontamination often cannot be detectedefficiently with current technology. It is evenmore difficult to identify a handheld detectionmethod that will assure that decontaminationefforts have been adequate (except in casesof radiation release).
“There is no foolproof chemical detector andwe are far from having a foolproof biologicalagent detector.” False readings continue to bea problem, with relatively harmless chemicalstriggering an alarm (OSHA StakeholderComments, 2006). At this time, good supervi-sion of the washing process remains a morereliable indicator of good decontamination.
To the extent that they become available, EMSresponders might also find chemical detection tapesand swabs useful for assessing the types of persist-ent, highly toxic, modestly volatile or non-volatileCBRNE agents that could cling to a patient’s cloth-ing, or to the patient’s body once contaminatedclothing has been removed (EPA ERT, 2007).
Employers of EMS responders should considermeeting with HAZMAT teams to obtain an overviewof the strengths and weaknesses of the detectionequipment available to the teams with which theywould work in the event of an emergency release.Together they should determine the utility of theseinstruments to support EMS responder functions.Keep in mind that EMS responder training and pow-ers of observation to identify cases of contamina-tion still remain a critical element of their defense.
Methamphetamine Detection EquipmentTo assist law enforcement officials who go on siteduring investigation or decontamination of illegalmethamphetamine laboratories, NIOSH researchershave developed field methods to detect the pres-ence of methamphetamine on surfaces, personneland PPE. These methods will help detect the pres-ence of the drug in illicit laboratories and evaluatethe effectiveness of decontamination procedures.NIOSH reports that:
“A prominent manufacturer of sampling tech-nologies has commercialized two low-cost,NIOSH-designed field methods to help firstresponders, public health officials, and remedi-ation workers quickly detect the presence ofmethamphetamine on various environmentalsurfaces.The sampling technique can be usedto detect trace levels of the illicit drug on sur-
4 2
Occupational Safety andHealth Administration
30 Appendix B of the source document contains interviews withnine community incident commanders regarding the specificdetection equipment they take to sites and how they use theinformation the detectors provide. See “Data for First ResponderUse of Photoionization Detectors for Vapor Chemical Constituents”(ILN/EXT -05-00165 (Rev 1), Idaho National Laboratory(November 2006). Accessed September 4, 2007 at:www.inl.gov/technicalpublications/Documents/3589641.pdf.

faces, or used to evaluate decontaminationefforts or clearance” (NIOSH, 2006).
The first method involves a “colorimetric testthat detects the presence of methamphetamineresidue on surfaces from 15 to 5000 micro-grams/100 cm2. Results should not be used forclearance purposes.” The second method is a set of“semi-quantitative immunoassay tests that detectlow levels of methamphetamine residue on sur-
faces. They may be used to determine the need forcleaning in a specific area or the need for furthercleaning onsite to reach state cleanup guidelines”(SKC, 2006). The manufacturer notes that somestates and counties require lab results from quanti-tative wipe sampling before issuing a reentry certifi-cate after cleanup efforts. In addition to screeningtests, laboratory analyses are also available.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 4 3

Conclusion
These best practices are intended to help EMSresponders’ employers investigate and identify inadvance of an incident the roles that their workerscan be expected to play during a hazardous sub-stance release event in their community (includingunder conditions of a mutual aid agreement).Employers should use the information in this guidewhen conducting hazard assessments to determineworker PPE and training needs. The hazard assess-ments are based in part on worker roles and on thetypes of hazardous substance releases for which the
community is preparing. The anticipated role ofworkers and the related hazard assessments shouldhelp guide the employers’ decisions about how toprepare their EMS responders to work as safely asis reasonably possible during treatment and trans-port of victims of hazardous substance releases.
In determining appropriate PPE and training fortheir EMS responders, employers should refer tothe Summary of OSHA’s Recommendations forTraining and PPE section of this guide (at pg. 32).
4 4
Occupational Safety andHealth Administration

Appendix A
GlossaryAir-purifying respirator (APR): A respirator that usesfilters, cartridges, or canisters to cleanse the air.
Atmosphere supplying respirator (ASR): A respiratorthat provides clean air from an uncontaminatedsource to the facepiece. Examples include supplied-air (airline) respirators, SCBA, and combination sup-plied-air/SCBA.
Assigned protection factor (APF): A rating assignedto a respirator style by OSHA. This rating indicatesthe level of protection most workers can expectfrom properly worn, maintained, and fitted respira-tors used under actual workplace conditions. AnAPF of 1,000 indicates that the concentration of con-taminant inside the facepiece would be 1,000 timeslower than the concentration in the surrounding air.A respirator with an APF of 1,000 will providegreater protection than a respirator with an APF of100. (Note:The APF should not be confused with asimilar measure, the “fit factor,” obtained duringquantitative fit testing. Fit factors, which tend to behigher numbers, provide a relative indication ofhow well a respirator fits an individual, but do notrepresent the level of protection the respiratorwould provide in the workplace.)
Awareness level: See first responder awarenesslevel.
CBRN: Chemical, biological, radiological, or nuclear[agent or substance].
CBRNE: Chemical, biological, radiological, nuclear,or explosive [agent or substance].
Cold zone: Area free of contamination. Equipmentand people leaving the hot zone should be decon-taminated prior to arriving at the cold zone. If a haz-ardous substance from patients or equipment con-taminates the cold zone, the area is redefined as awarm zone.
Decontaminate (or decontamination): The processof removing hazardous substance contaminationfrom a patient, equipment or other material. Seealso Gross Decontamination and TechnicalDecontamination.
Doff: To take off or remove (e.g., PPE).
Don: To put on, in order to wear (e.g., PPE).
EMS: Emergency medical services. The emergencymedical service system can encompass all levels ofpatient emergency care, treatment or transport.
EMS responder: Individual trained to answer publicsafety requests for emergency medical care. In-cludes all levels of emergency medical technicians
(EMTs) and paramedics. For the purposes of thisdocument, the term EMS responder also includesindividuals cross-trained or holding multiple qualifi-cations (e.g., firefighter, hazardous materials teammember, police officer) only at the time that theyare performing the duties of an EMT or paramedic.
EMT: Emergency medical technicians of all levels(EMT-Basic, EMT-Intermediate, EMT-Paramedic).
ERP: Emergency response plan.
First responder: Personnel who have responsibilityto initially respond to emergencies. Some examplesare firefighters, HAZMAT team members, law en-forcement officers, lifeguards, forestry personnel,EMTs, and other public service personnel. In thecase of hazardous materials incidents, these person-nel typically respond at the site where the incidentoccurred.
First responder awareness level: Individuals whomight reasonably be anticipated to witness or dis-cover a hazardous substance release and who havebeen trained to initiate an emergency responsesequence by notifying the proper authorities of therelease. They would take no further action beyondnotifying the authorities. [OSHA HAZWOPERStandard, 29 CFR 1910.120(q)(6)(i)].
First responder operations level: Individuals whorespond to releases or potential releases of haz-ardous substances as part of the initial response tothe site for the purpose of protecting nearby per-sons, property, or the environment from the effectsof the release. These individuals shall have receivedat least 8 hours of training or have sufficient experi-ence to objectively demonstrate competency in spe-cific critical areas. [OSHA HAZWOPER Standard, 29CFR 1910.120(q)(6)(ii)].
Gross decontamination: The process of removingclothing and/or a water rinsing of the naked body toquickly remove the majority of hazardous substancecontamination from a patient. Also called primary,or expedient decontamination.
HAZCOM: OSHA’s Hazard Communication standard[29 CFR 1910.1200].
HAZMAT: Hazardous material.
HAZWOPER: OSHA’s Standard on Hazardous WasteOperations and Emergency Response, 29 CFR1910.120. In particular, paragraph (q) of this stan-dard covers employers whose workers are engagedin emergency response to hazardous substancereleases.
Hazard response zones: Any of the three areas des-ignated to indicate the degree of hazard and loca-
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 4 5

tion of response activities. The three zones are hotzone, warm zone, and cold zone. Consult the glos-sary entry for the individual zone for a moredetailed definition.
Hazard vulnerability analysis (HVA): The identifica-tion of potential emergencies and direct and indirecteffects these emergencies may have on the organi-zation’s operations and the demand for its services.
Hazardous Substance: Any substance exposure towhich may result in adverse effects on the health orsafety of workers. This includes substances definedunder Section 101(14) of CERCLA; biological or dis-ease-causing agents that may reasonably be antici-pated to cause death, disease, or other health prob-lems; any substance listed by the U.S. Departmentof Transportation as hazardous material under 49CFR 172.101 and appendices; and substances classi-fied as hazardous waste.
Hazardous Substances Emergency EventsSurveillance System (HSEES): A state-based systemoperated by the Agency for Toxic Substances andDisease Registry (ATSDR) since 1989. The system isintended to help characterize the public health con-sequences of hazardous substance releases.Approximately one-third of the U.S. states currentlyparticipate by collecting and submitting information.The HSEES database stores information on events,chemicals, victims, injuries and evacuations.
Hospital incident command system (HICS): Anexample of an optional NIMS-based ICS tailoredspecifically for use by hospitals and designed tofunction in conjunction with other common ICSsused by emergency response agencies (e.g., FireService Incident Command System). See Appendix Ifor additional information.
Hot zone: An area in and immediately surroundinga hazardous substance release. It is assumed topose an immediate health risk to all persons, includ-ing EMS responders.
IDLH: Immediately dangerous to life or healthmeans an atmospheric concentration of any toxic,corrosive or asphyxiant substance that poses animmediate threat to life or would interfere with anindividual's ability to escape from a dangerousatmosphere. NIOSH publishes a list of IDLH concen-trations for various substances. NIOSH has set theIDLH levels based on several toxicity criteria, whichgive priority to 30-minute acute data that demon-strates the concentration that is lethal to 50 percentof laboratory animals in 30 minutes.
Incident command system (ICS): A flexible organi-zational structure which provides a basic expand-able system adapted by the Department ofHomeland Security as the common emergency
response organizational structure throughout thenation.
Incident commander (IC): The individual who holdsoverall responsibility for incident response andmanagement.
JCAHO: Joint Commission on Accreditation ofHealthcare Organizations.
LEPC: Local Emergency Planning Committee.
Mass casualty: “A combination of patient numbersand patient care requirements that challenge orexceed a community’s ability to provide adequatepatient care using day-to-day operations” (Barberaand MacIntyre, 2003).
NFPA: National Fire Protection Association.
NHTSA: National Highway Traffic SafetyAdministration, an organization under the U.S.Department of Transportation (U.S. DOT).
NIMS: The National Incident Management System,established by the U.S. Department of HomelandSecurity as a standardized management approachto incident response, including the NIMS-based ICS,that all responders will use to coordinate and con-duct response actions.
Paramedic: An Emergency Medical Technician –Paramedic level. A person who is trained to giveemergency medical treatment or assist medical pro-fessionals in providing advanced life support.
Personal protective equipment (PPE): Examplesinclude protective suits, gloves, foot covering, respi-ratory protection, hoods, safety glasses, gogglesand face shields.
Powered air-purifying respirator (PAPR): A respiratorthat uses a battery-powered blower to force airthrough a filter or purifying cartridge before blowingthe cleaned air into the respirator facepiece.
Self-contained breathing apparatus (SCBA): A respi-rator that provides fresh air to the facepiece from acompressed air tank (usually worn on the worker’sback).
Skilled support personnel: Personnel, not necessari-ly an employer's own workers, who are skilled inthe operation of certain equipment, such as mecha-nized earthmoving or digging equipment or craneand hoisting equipment, and who are needed tem-porarily to perform immediate emergency supportwork that cannot reasonably be performed in atimely fashion by an employer's own workers, andwho will be or may be exposed to the hazards at anemergency response scene [from 1910.120(q)(4)].
Supplied-air respirator (SAR): A respirator that pro-vides breathing air through an airline hose from anuncontaminated compressed air source to the face-
4 6
Occupational Safety andHealth Administration

piece. The facepiece can be a hood, helmet, or tightfitting facepiece.
Technical decontamination: The process of using acleansing agent to completely clean a patient. Thecleansing agent is typically soap and water, butmight include other solvents. Technical decontami-nation (also called secondary, or precautionarydecontamination) is more thorough, but also moretime-consuming than gross decontamination.
Triage: The process of screening and classifyingsick, wounded, or injured persons to determine pri-ority needs in order to ensure the efficient use ofmedical personnel, equipment and hospitals.
Warm zone: The area surrounding the hot zone,where primary contamination is not expected butwhere personnel must use protective clothing andequipment to avoid hazardous substance exposurefrom contaminated victims. People and items aredecontaminated in this zone as they return from thehot zone and before being released to the cold zone.The warm zone is located between the hot zone andthe cold zone, with consideration of environmentalfactors such as wind direction and geographic con-ditions.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 4 7
Appendix B
ReferencesExposure 29 CFR 1910.120. Hazardous Waste
Operations and Emergency Response standard,29 CFR 1910.120, Code of Federal Regulations.
Adams, D. & Elliot, T. 2006. Impact of safety needledevices on occupationally acquired needlestickinjuries: a four-year prospective study. Journalof Hospital Infection 64:50-55.
AHRQ. 2005. Development of models for emer-gency preparedness – personal protective equip-ment, decontamination, isolation/quarantine,and laboratory capacity (AHRQ Pub. No. 05-0099). U.S. Department of Health and HumanServices, Agency for Healthcare Research andQuality (AHRQ). August. Accessed at: www.ahrq.gov/research/devmodels
ANSI/ASSE. 2006. ANSI/ASSE Z15.1 standard onSafe Practices for Motor Vehicle Operators.American National Standards Institute (ANSI)with the American Society of Safety Engineers(ASSE). February. Available at http://webstore.ansi.org/RecordDetail.aspx?sku=ANSI/ASSE%20Z15.1-2006
ATSDR. 2001. Managing Hazardous MaterialsIncidents (Volume 1) – Emergency MedicalServices: A Planning Guide for the Managementof Contaminated Patients. U.S. Department ofHealth and Human Services, Agency for ToxicSubstances and Disease Registry (ATSDR).Accessed September 20, 2007 at: www.atsdr.cdc.gov/mhmi/#bookmark05
ATSDR. 2004. Hazardous Substances EmergencyEvents Surveillance (HSEES) – Annual Report2004. U.S. Department of Health and HumanServices, Agency for Toxic Substances andDisease Registry (ATSDR). Accessed September1, 2007 at: www.atsdr.cdc.gov/HS/HSEES/annual2004.html
ATSDR. 2007. E-mail communications betweenATSDR statisticians and ERG regarding“Statistician Inquiry” – HSEES database resultsfor EMT/EMSs. U.S. Department of Health andHuman Services, Agency for Toxic Substancesand Disease Registry (ATSDR). August 8 and 9.
Baker et al. 2006. EMS helicopter crashes: Whatinfluences fatal outcome? Annals of EmergencyMedicine 47(4). April.
Barg. 2004. Breaking down barriers: Collaborativeeducation drives collective change. Article onInternet Web site for the Office of the FireMarshall, Province of Ontario, Canada. October4. Accessed February 11. www.ofm.gov.on.ca/english/FireService/announcements/2004/Breaking%20Down%20Barriers.asp
Berrios-Torres, S.I. et al. (2003). World Trade Centerrescue worker injury and illness surveillance,New York, 2001. Am J Prev Med 25(2): 79-87.
Berkowitz, Z., et al. (2004). Hazardous substancesreleases causing fatalities and/or people trans-ported to hospitals: rural/agricultural vs. otherareas. Prehospital Disaster Med 19(3): 213-20.
Boal W.L., Hales, T., Ross, C.S. 2005. Bloodbornepathogens among firefighters and emergencymedical technicians. Prehosp Emerg Care. Apr-Jun; 9(2):236-247.
Burgess, et al. 2002. Medical surveillance of clan-destine drug laboratory investigators. J OccupEnviron Med. 44(2):184-9 (abstract only).(February).
Caldicott, et al. 2005. Clandestine drug laboratoriesin Australia and the potential for harm.Australian and New Zealand Journal of PublicHealth 29(2):155-162.
CA EMSA. 2006. Hospital Incident CommandSystem Guidebook. Accessed May 21, 2007 at:www.emsa.cahwnet.gov/hics/hics%20guidebook%20and%20glossary.pdf
CDC. 2003. Interim Guidelines for HospitalResponse to Mass Casualties from aRadiological Incident. Centers for DiseaseControl and Prevention (CDC), U.S. Departmentof Health and Human Services. December.
Cone, D.C., McNamara R.M. 1998. Injuries to emer-gency medicine residents on EMS rotations.Prehosp Emerg Care. Apr-Jun; 2(2):123-6.
Cydulka, R.K., Emerman C.L., et al. 1997. Stress lev-els in EMS personnel: a national survey.Prehospital Disaster Med. Apr-Jun; 12(2):136-40.
DHHS. 2006. Maps of methamphetamine drugseizure. Department of Health and HumanServices, www.MethResources.gov Web Site.Accessed September 4, 2006 at: www.methre-sources.gov/AudienceInfoTypeResult.aspx?AudId=1&InfoId=2
4 8
Occupational Safety andHealth Administration
DrägerSafety. 2007. Fire and Emergency Services.Internet web page for DrägerSafety. AccessedSeptember 3 at: www.draeger.com/ST/internet/US/en/index.jsp
Ellen, S. 2003. Personal Decon. Military MedicalTechnology – On-line Archives, 7(4) (June).Accessed September 4, 2006 at: www.military-medical-technology.com/article.cfm?DocID=130
EMS Insider, 2006. Ambulance safety gainsmomentum. EMS Insider, Vol. 24(6). June.
EnviroFoam. 2008. Internet Web site forEnviroFoam Technologies, Inc., Huntsville,Alabama. Accessed June 30, 2008 at: www.envirofoam.com/EasyDecon/FactSheet.aspx?ID=17
EPA-ERT. 2007. Personal communication between arepresentative of the U.S. EnvironmentalProtection Agency (U.S. EPA) EmergencyResponse Team (ERT), Las Vegas, Nevada andERG. August 30.
EPA RERT. 2007. Personal communication betweena representative of the U.S. EnvironmentalProtection Agency (U.S. EPA) RadiologicalEmergency Response Team (RERT), Las Vegas,Nevada and ERG. September 11.
E-Z-EM. 2006. What is RSDL? Internet Web site forRSDecon. E-Z-EM, Inc., Lake Success, New York.Accessed September 5 at: www.rsdecon.com
FEMA, 2007. National emergency responder cre-dentialing – EMS job titles (FEMA 509-3). FederalEmergency Management Agency. July. AccessedSeptember 10, 2007 at: www.fema. gov/pdf/emergency/nims/ems_jobtitle_112906.pdf
Georgopoulos, P.G., et al. 2004. Hospital responseto chemical terrorism: personal protective equip-ment, training, and operations. AmericanJournal of Industrial Medicine 46(5):432-445.November.
Gershon R.R., et al. 1995 Review of accidents/injuries among emergency medical servicesworkers in Baltimore, Maryland. PrehospitalDisaster Med. Jan-Mar;10(1):14-8.
Grainger. 2007. Online catalog - chemical detectionequipment. Grainger, Inc. Accessed September 3at: www.grainger.com/images/firstresponderfaxform.pdf
Green et al. 2005. Reducing vehicle crash-relatedEMS worker injuries through improvements inrestraint system. Presentation at the XVII WorldCongress on Safety and Health at Work,Orlando, FL. September 18-22.
Hall, H.I., et al. 1994. "Surveillance of hazardoussubstance releases and related health effects."Arch Environ Health 49(1): 45-8.
Hall, H.I., et al. 1995. "Health effects related toreleases of hazardous substances on theSuperfund priority list." Chemosphere 31(1):2455-61.
Hall, H.I., et al. 1996. "Public health consequencesof hazardous substance releases." Toxicol IndHealth 12(2): 289-93.
HazTech Systems. 2007. Internet Web site forHazCat. HazTech Systems, Inc., Mariposa, CA.Accessed September 3 at: www.hazcat.com
Hick, J.L., et al. 2003. Protective equipment forhealthcare facility decontamination personnel:regulations, risks, and recommendations.Annals of Emergency Medicine 42(3):370-380.September.
Hick, J.L. 2007. Personal communication betweenDr. Hick and ERG regarding comments on thedraft Best Practices Document for EMTs Exposedto Hazardous Substances. October.
HMEP. 1996. HMEP Hazardous Materials andTerrorist Incident Response CurriculumGuidelines and the companion HMEP HazardousMaterials and Terrorist Incident PreventionCurriculum Guidelines. June 5. http://search.fema.gov/search?q=+DOT+HMEP+Curriculum+Guide++&sort=date%3AD%3AL%3Ad1&output=xml_no_dtd&ie=UTF-8&oe=UTF-8&client=usfa&proxystylesheet=usfa&site=usfa&btnG.x=7&btnG.y=5
Homeland Security Council. 2005. NationalPlanning Scenarios. April. [Draft copy] accessedFebruary 11, 2007. http://media.washingtonpost.com/wp-srv/nation/nationalsecurity/earlywarning/NationalPlanningScenariosApril2005.pdf
Horton, D.K., Berkowitz, Z., W.E. Kaye. 2003.Secondary contamination of ED personnel fromhazardous materials events, 1995-2001. Am JEmerg Med 21:199-204. May.
Horton et al. 2008. Secondary contamination ofmedical personnel, equipment, and facilitiesresulting from hazardous materials events,2003–2006. Disaster Medicine and Public HealthPreparedness, 2(2):104-113.
Houser et al. 2004. Emergency Responder Injuriesand Fatalities: An Analysis of Survey Data(Technical Report). Document number TR-100-NIOSH. Rand, Santa Monica, California. (March).
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 4 9
Hurst, C.G. 1997. Decontamination. Chapter 15 inMedical Aspects of Chemical and BiologicalWarfare. Published by Department of the Army,Office of The Surgeon General, Borden Institute.Accessed March 30, 2008 at: www.bordeninstitute.army.mil/published_volumes/chemBio/Ch15.pdf
IAB. 2007. Standardized Equipment List (SEL),InterAgency Board for EquipmentStandardization and Interoperability (IAB).http://www.iab.gov/Documents.aspx
Ilhan et al. 2006. Long working hours increase therisk of sharp and needlestick injury in nurses:the need for new policy implication. Journal ofAdvanced Nursing 56(5):563 – 568.
“Data for First Responder Use of PhotoionizationDetectors for Vapor Chemical Constituents”(ILN/EXT -05-00165 (Rev 1), Idaho NationalLaboratory (November 2006). AccessedSeptember 4, 2007 at: www.inl.gov/technicalpublications/Documents/3589641.pdf
Kahn, C.A., Pirrallo, R.G., Kuhn, E.M. 2001.Characteristics of fatal ambulance crashes in theUnited States: an 11-year retrospective analysis.Prehosp Emerg Care. Jul-Sep;5(3):261-9.
Kales, S.N., et al. 1997. Injuries caused by haz-ardous materials accidents. Ann Emerg Med30(5): 598-603.
Kaye, W.E., M.F. Orr, et al. (2005). “Surveillance ofhazardous substance emergency events: identi-fying areas for public health prevention.” Int JHyg Environ Health 208(1-2): 37-44.
LaTourrette, et al. 2003. Protecting EmergencyResponders, Volume 2: Community views ofsafety and health risks and personal protectionneeds. Rand, Santa Monica, California.Document number MR-1646-NIOSH.
Levick, N. 2006. Hazard analysis and vehicle safetyissues for emergency medical service vehicles:where is the state of the art? Session 732.Presentation at American Society of SafetyEngineers Conference, Seattle, WA. June.Accessed at: www.objectivesafety.net/LevickASSEPDC2006.pdf
LSS. 2008. Safety and Industrial Catalog 7FQ(First Edition). Laboratory Safety Supply (LSS),Janesville, WI.
Macintyre, A.G., et al. 2000. Weapons of MassDestruction Events with ContaminatedCasualties: Effective Planning for Health CareFacilities. JAMA 283(2):242-249. January 12.
Maguire, B.J., et al. 2002. Occupational Fatalities inEmergency Medical Services: A Hidden Crisis.Ann Emerg Med 40(6): 625-632.
Maguire, B.J., et al. 2005. Occupational injuriesamong emergency medical services personnel.Prehosp Emerg Care. Oct-Dec;9(4):405-11.
Martyny, et al. 2005. Chemical exposures associatedwith clandestine methamphetamine laboratoriesusing the hypophosphorous and phosphorousflake method of production. National JewishMedical Research Center, Division of Environ-mental and Occupational Health Sciences,Denver, Colorado. (September 23) AccessedSeptember 4, 2006 at: www.njc.org/pdf/meth-hypo-cook.pdf#search=%22%22medical%20surveillance%20of%20Clandestine%20drug%20laboratory%20investigators%22%20Burgess%202002%22
Mechem, C.C., et al. 2002. Injuries from assaults onparamedics and firefighters in an urban emer-gency medical services system. Prehosp EmergCare. Oct-Dec;6(4):396-401.
Miller, N., Gudmestad, T., & Eisenberg, M. 2005.Development of model infectious disease proto-cols for fire and EMS personnel. PrehospitalEmergency Care 9:326 – 332.
MMWR. 2000. Public health consequences amongfirst responders to emergency events associatedwith illicit methamphetamine laboratories--selected states, 1996-1999. MMWR Morb MortalWkly Rep 49(45): 1021-4.
MMWR. 2003. Ambulance crash-related injuriesamong emergency medical services workers –United States, 1991-2002. Mortality andMorbidity Weekly Report (MMWR). 52(8):154-6.February 28. Accessed September 10, 2007 at:www.cdc.gov/mmwr/PDF/wk/mm5208.pdf
MMWR. 2005. Public health consequences fromhazardous substances acutely released duringrail transit--South Carolina, 2005; selectedStates, 1999-2004. MMWR Morb Mortal WklyRep 54(3): 64-7.
Mock, E.F., Wrenn K.D., et al. 1999. Anxiety levels inEMS providers: effects of violence and shiftsschedules. Am J Emerg Med. Oct;17(6):509-11.
Modec. 2008. Product promotional materials on theInternet Web site for Modec, Inc., Denver,Colorado. Accessed June 30, 2008 at:www.deconsolutions.com.
5 0
Occupational Safety andHealth Administration
Narad, R.A. 1998. An inventory of ambulance serv-ice regulatory programs in California.Prehospital Disaster Med. Jan-Mar;13(1):49-54.
NDIC. 2004. Methamphetamine LaboratoryIdentification and Hazards – Fast Facts –Questions and Answers, NDIC Product No. 2004-L0559-001. National Drug Intelligence Center(NDIC), U.S. Department of Justice. AccessedSeptember 4, 2006. www.usdoj.gov/ndic/pubs7/7341/7341p.pdf
NDIC. 2006. National Drug Threat Assessment 2006(Table 4). National Drug Intelligence Center(NDIC), U.S. Department of Justice. AccessedSeptember 4, 2006 at: www.dea.gov/concern/18862/meth.htm
NFPA. 2007. NFPA 1994 Standard on protectiveensembles for first responders to CBRN terror-ism incidents. National Fire ProtectionAssociation (NFPA), Quincy, MA.
NFPA. 2008. NFPA 1852 Standard on selection, care,and maintenance of open-circuit self-containedbreathing apparatus (SCBA). National FireProtection Association (NFPA), Quincy, MA.
NHTSA. 2000. Emergency Medical ServicesEducation Agenda for the Future – A SystemsApproach (document number HS808 711).National Highway Traffic Safety Administration,U.S. Department of Transportation (U.S. DOT).July. Accessed February 11, 2007 at www.nhtsa.dot.gov/people/injury/ems/EdAgenda/final/index.html
NIJ. 2000. Guide for the Selection of ChemicalAgent and Toxic Industrial Material DetectionEquipment for Emergency First Responders –Volumes I & II (NIJ Guide 100-00). NationalInstitute of Justice, U.S. Department of Justice.June. http://ncjrs.org/pdffiles1/nij/184449.pdf
NIOSH. 2006. Two NIOSH-designed methods fordetecting methamphetamine now commerciallyavailable. NIOSH e-New, 4(3) (July). NationalInstitute for Occupational Safety and Health(NIOSH), Cincinnati, OH. Accessed September 4,2006 at: www.cdc.gov/niosh/enews/enewsV4N3.html
NIOSH. 1996. Health hazard evaluation report 95-0031-2601 – University of Medicine and Dentistryof New Jersey, University Hospital, Newark,New Jersey. National Institute for OccupationalSafety and Health (NIOSH), Cincinnati, OH.October.
Nishiwaki, Y., et al. 2001. Effects of sarin on thenervous system in rescue team staff membersand police officers 3 years after the Tokyo sub-way sarin attack. Environ Health Perspect109(11): 1169-73.
Okumura, et al. 1998. The Tokyo subway sarinattack: disaster management, Part 1: Communityemergency response. Acad Emerg Med 5(6):613-7.
Okumura, T., et al. 2003. The chemical disasterresponse system in Japan. Prehospital DisasterMed 18(3): 189-92.
OSHA. 1991-Borwegen. Letter of InterpretationAddressed to Mr. William Borwegen, ServiceEmployees International Union, AFL-CIO, Re:HAZWOPER EPA and OSHA jurisdictional issues.December 18. Accessed April 6, 2004 atwww.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=20500
OSHA. 1991-McNamara. Letter of Interpretationaddressed to Mr. Edward McNamara, ExecutiveDirector, Central Massachusetts EmergencyMedical Systems Corporation. RE: Trainingrequirements for emergency medical personnel.(June14) www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=20302
OSHA. 1992-Chapman. Letter of Interpretationaddressed to The Honorable Jim Chapman, U.S.House of Representatives. RE: Background ofStandards. (November 20) www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=20942
OSHA. 1992-Levitin. Letter of Interpretationaddressed to Howard Levitin, MD. RE: Trainingrequirements for hospital personnel involved inan emergency response of a hazardous sub-stance. (October 27). www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=20911
OSHA. 1994-Bays. Letter of Interpretationaddressed to Mr. Robert Bays, Sr., HuntingtonLaboratories, Inc. RE: Decontamination of plushcarpet surface after a spill. (June 10). www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=21511
OSHA. 1995-Nechis. Letter of Interpretationaddressed to Barry Nechis, President, RescueTechnology. RE: The OSHA Hazardous Waste
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5 1
Operations and Emergency Response (HAZ-WOPER) regulation. (August 28) AccessedSeptember 10, 2007 at: www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=21901
OSHA. 1996-Grassley. Letter of Interpretationaddressed to The Honorable Charles E. Grassley,U.S. Senate. RE: Regulations for VolunteerRescue and Ambulance Squads. (June 11)www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=22193
OSHA. 1997-Whittaker. Letter of InterpretationAddressed to Mr. Thomas Whittaker, NewEngland Hospital Engineer's Society, RE:Emergency response training requirements forhospital staff. (April 25) Accessed April 6, 2004at www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=22393
OSHA. 1997-Killen. Letter of Interpretationaddressed to Bill Killen, Director, Navy Fire andEmergency Services. RE: Fire fighter personalprotective clothing issues. (August 28)www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=22467
OSHA. 2001-BBP Preamble/Final Rule. OccupationalExposure to Bloodborne Pathogens; Needlestickand Other Sharps Injuries; Final Rule. FederalRegister 66:5317-5325 (January 18).www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=FEDERAL_REGISTER&p_id=16265
OSHA. 2002-Hayden. Letter of Interpretationaddressed to CPT Kevin Hayden, ActingCommanding Officer, State of New JerseyEmergency Management Section. RE: Trainingand PPE requirements for hospital staff thatdecontaminate victims/patients. (December 2)www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=24523
OSHA. 2003-Bolt. Letter of Interpretation Addressedto Mike Bolt, RE: HAZWOPER training require-ments for hospital staff who decontaminatechemically contaminated patients. (April 22)Accessed April 6, 2004 at www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=24605
OSHA. 2004-Gantt. Letter of Interpretationaddressed to Mr. Ron Gantt, Trainer/consultant,
5 2
Occupational Safety andHealth Administration
Safety Compliance Management, Inc. RE:Acceptability of using computer-based (on-line)training for the HAZWOPER 40-hour classroomtraining. (August 16) www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=24985
OSHA. 2005. OSHA Best Practices for Hospital-Based First Receivers of Victims from MassCasualty Incidents Involving the Release ofHazardous Substances. January. AccessedSeptember 21, 2007 at: www.osha.gov/dts/osta/bestpractices/firstreceivers_hospital.pdf
OSHA. 2006-Stakeholder Comments. Commentsreceived in response to OSHA stakeholder meet-ing and review of draft Best Practices Documentfor EMTs Exposed to Hazardous Substances.
OSHA. 2007. Pandemic Influenza Preparedness andResponse Guidance for Healthcare Workers andHealthcare Employers: www.osha.gov/Publications/OSHA_pandemic_health.pdf
OSHA. 2007-CPL 02-02-073. OSHA Instruction –inspection procedures for 29 CFR 1910.120 and1926.65, paragraph (q): Emergency Response toHazardous Substance Release. August. AccessedSeptember 10, 2007, at www.osha.gov/OshDoc/Directive_pdf/CPL_02-02-073.pdf
Peate, W.F. 2001. Preventing needlesticks in emer-gency medical system workers. J Occup EnvironMed. June; 43(6):554-575.
Pennsylvania Department of Health. 2004. Thenational study to prevent blood exposure inparamedics preliminary results. March.Accessed June 6, 2007 at: www.dsf.health.state.pa.us/health/lib/health/ems/natl_bloodstudy.pdf
Rischitelli, G., et al. 2001. The risk of acquiring hep-atitis B or C among public safety workers: A sys-tematic review. American Journal of PreventiveMedicine 20(4):299-306.
SBCCOM. 2000a. Guidelines for Responding to aChemical Weapons Incident. DomesticPreparedness Chemical Team, U.S. Army Soldierand Biological Chemical Command (now knownas the Research, Development and EngineeringCommand [RDECOM]). http://transit-safety.volpe.dot.gov/training/Archived/EPSSeminarReg/CD/documents/Weapons/cwirp_guidelines.pdf.
SBCCOM. 2002. Guidelines for cold weather massdecontamination during a terrorist chemicalagent incident. U.S. Army Soldier BiologicalChemical Command (now known as theResearch, Development and Engineering
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5 3
Command [RDECOM]) . (January). AccessedMarch 28, 2008 at: www.edgewood.army.mil/downloads/cwirp/ECBC_cwirp_cold_weather_mass_decon.pdf
SBCCOM. 2003. Guidelines for Use of PersonalProtective Equipment by Law EnforcementPersonnel During a Terrorist Chemical AgentIncident. U.S. Army Soldier and BiologicalChemical Command (now known as theResearch, Development and EngineeringCommand [RDECOM]). Original June 2001.Revised July 2003. http://stinet.dtic.mil/dticrev/PDFs/ada435808.pdf.
Schultz, M., Cisek, J., and Wabeke, R. 1995.Simulated exposure of hospital emergency per-sonnel to solvent vapors and respirable dust dur-ing decontamination of chemically exposedpatients. Annals of Emergency Medicine.26(3):324-329. September.
Schwartz, R.J., Benson L., Jacobs, L.M. 1993. Theprevalence of occupational injuries in EMTs inNew England. Prehospital Disaster Med. Jan-Mar;8(1):45-50.
SKC. 2006. Product promotional material forMethCheck and MethAlert – “Meth residuedetectives”. SKC, Inc. Eighty-Four, Pennsylvania.Accessed September 4, 2006 at: www.meth-wipe.com
Umbrell, C. 2006. Tweakers, snakes, and cold medi-cine – health and safety during illegal drug labcleanup. Synergist 17(1):32-36. AmericanIndustrial Hygiene Association (AIHA), Fairfax,Virginia. (January). Accessed September 4, 2006at: www.aiha.org/1documents/PR/Synergist-Meth%20Feature-Jan%2006.pdf#search=%22NIOSH%20Methamphetamine%20PPE%22
USACHPPM. 2003a. Personal Protective EquipmentGuide for Military Medical Treatment FacilityPersonnel Handling Casualties from Weapons ofMass Destruction and Terrorism Events(Technical Guide 275). U.S. Army Center forHealth Promotion and Preventive Medicine.August. http://chppm-www.apgea.army.mil/documents/TG/TECHGUID/TG275new.pdf
USDHHS-REMM. 2007. Radiological Event MedicalManagement Web site. U.S. Department ofHealth and Human Services. AccessedSeptember 12 at http://remm.nlm.nih.gov/index.html
USFA/IAFC. 2006. Policies and Procedures forEmergency Vehicle Safety (including model forcustomization). Department of HomelandSecurity, U.S. Fire Administration (USFA) withthe International Association of Fire Chiefs(IAFC). Accessed September 10, 2007 at:www.iafc.org/displaycommon.cfm?an=1&subarticlenbr=602
Vogt, B.M. and J.H. Sorrensen. 2002. How clean issafe? Improving the effectiveness of decontami-nation of structures and people following chemi-cal and biological incidents – Final Report(ORNL/TM-2002/178). Prepared by OakridgeNational Laboratory for the U.S. Department ofEnergy. October. Accessed September 2004 athttp://emc.ornl.gov/EMCWeb/EMC/PDF/How_Clean_is_Safe.pdf
Walter, F.G., et al. 2003. Hazardous materialsresponses in a mid-sized metropolitan area.Prehosp Emerg Care 7:214-218. Apr-Jun.

5 4
Occupational Safety andHealth Administration
Appendix C
Additional Sources of InformationInter Agency Board for Equipment Standardizationand Interoperability – general information and linksto related sites, such as the Responder KnowledgeBase, at www.iab.gov
• InterAgency Board – Standard Equipment List(personal protective equipment)www.iab.gov/Download/sel_section1_2006.pdf
• Radiological Event Medical Management Website, at www.remm.nlm.gov

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5 5
Appendix D
Examples of Mutual Aid Agreementsand TemplatesThis Appendix provides three examples of mutualaid agreements and templates for agreementsbetween service providers and communities. Theexample from Westchester County, NY contains asubstantial amount of detail, while another exam-ple, from the Iowa Department of Public Health, isbrief and to the point. Many other formats andarrangements exist and many are publicly availableon the Internet (For example, conduct an Internetsearch using key words such as: Mutual Aid EMT; orMutual Aid memorandum of agreement EMT)
Emergency Management Assistance Compacts(EMACs) serve a similar purpose for mutual aidbetween states and can help fulfill the function ofmutual aid agreements. For information on intrastatemutual aid and model intrastate legislative language,see www.emacweb.org.
Westchester County, NY Mutual Aid agreement[View at: www.westchestergov.com/emergserv/EMS/PDF_files/mutualaidplandec03-v5.pdf]
Template for mutual aid agreement provided by theIowa Department of Public Health (IDPH)[View at: www.idph.state.ia.us/ems/common/pdf/mutual_aid_agreement.pdf]
Washington State Inter-county Mutual Aid omnibusAgreementTemplate[View at: http://emd.wa.gov/plans/documents/MutualAidHandbook.pdf]

Appendix E
Using Hazardous Substances EmergencyEvents Surveillance System (HSEES)Information in Community HazardEvaluations – A Review
Case Study – How communities and industriescan use the HSEES system information toreduce events (primary prevention) and informemergency responders as part of secondaryprevention (excerpt from Kaye et al. 2005).
Ammonia
BackgroundDuring 1996-2001, ammonia releases constitut-ed 6.2% of all releases reported to HSEES. Theammonia events were also 68% more likely toresult in more victims than expected based onthe percentage of all events in that category.Because of the prevalence of victims duringthese events, ammonia releases have been tar-geted for prevention in many states.
Primary preventionAs part of primary prevention efforts that tar-geted industry, Texas offered to provide fre-quent spillers with their own HSEES data. Afood processing company responded byrequesting their spill data. From the data theydiscovered that two facilities they had just pur-chased had never reported any chemical releas-es to either HSEES or the Nuclear RegulatoryCommission (NRC). The two facilities apparent-ly were lax in maintaining release records [a sit-uation that could be easily corrected].
To reduce the risk of employee exposure andminimize losses due to contaminated processedfoods, this company also implemented manyprocess safety measures in all 13 of its Texasfacilities. These measures included:
• Training on good workplace safety practicesfor both new and veteran employees.
• Designing and implementing pollution pre-vention systems to capture released ammo-nia by way of a water recovery system, ratherthan create fugitive plant emissions.
The company specifically used HSEES data toevaluate the cyclic nature of ammonia (refriger-ant) releases and found that there was a higherfrequency of releases during the summer, whenoutside temperatures were greater than 100°F.Engineering controls were added to the refrig-eration systems to compensate for higher sea-sonal pressure, thereby reducing the frequencyof releases. A periodic inspection and mainte-nance schedule minimized component failuresbefore they occurred. By the end of 1999, anautomated early warning ammonia detectionsystem was installed in each company process-ing facility.
Secondary preventionBecause of the prevalence of ammonia-relatedinjuries, many of the states participating in theHSEES system have chosen to target the pro-ducers, transporters, and handlers of ammoniafor secondary prevention of injuries. The farmbelt states particularly target their preventionactivities around ammonia because of the largequantities of ammonia fertilizers used. Onesuch state is Minnesota, which analyzed itsammonia release data and produced an articleaimed at health and safety personnel (Southeret al., 2000) and first responders (Souther et al.,2002). These articles contained additional infor-mation about ammonia and possible healtheffects from exposure, how to respond to anammonia release safely, and first-aid tips ifexposure occurs. Calls from fire departmentsfor more information were received after thearticles were published. The articles were usedduring training of fire department personnel,and techniques described in the article areactively used by fire department personnelwhen responding to ammonia releases.
5 6
Occupational Safety andHealth Administration

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5 7
In 1989, the Agency for Toxic Substances andDisease Registry (ATSDR) implemented an activestate-based hazardous substances emergencyevents surveillance system (HSEES) in an attemptto adequately characterize the public health conse-quences of hazardous substance releases. A haz-ardous substance emergency event (herein called“event”) is defined as uncontrolled or illegal releas-es or threatened releases of chemicals or their haz-ardous by-products. The HSEES collects informa-tion on events, chemicals, victims, injuries andevacuations. Analysis of the HSEES data helpsidentify risk factors associated with hazardous sub-stances releases.
A knowledge of risk factors can be useful whendeveloping public safety interventions and canimpact the guidelines and policies aimed at reduc-ing the number of events (primary prevention) andthe morbidity and mortality associated with suchevents (secondary prevention) (Kaye et al., 2005).
Using the HSEES system, participating stateshave been able to develop prevention outreachactivities such as awareness training of first respon-ders, primary prevention of spills, and secondaryprevention of related injuries and deaths. One suchcase, involving ammonia, has been excerpted fromKaye et al. (2005) and is presented in the inset,above.
Following are several additional studies thathave reviewed the HSEES system data and providevaluable trend analysis information that might helpemployers in planning for common incident typesin their areas. These examples also further illustratethe type of information available from the HSEESsystem.
Evaluation of Data from the Early 1990sHall et al. (1994, 1995, and 1996) studied the resultsof events reported to the HSEES system fromJanuary 1, 1990, through December 31, 1992.General trends resulting from the reported haz-ardous releases are briefly summarized below.
EventsThe majority (72%) of events occurred at fixed facil-ities (e.g., industrial sites, schools, farms, etc.) whilethe remaining (28%) were transportation-related(e.g., surface, air, or water transport). (Hall et al.1994 & 1996). Spills (72%) and fires (10%) account-ed for the majority of release types while theremaining events resulted from explosions andother types of releases (Hall et al., 1995). Over half(55%) of the events occurred in areas with industrialor commercial land use with an additional quarter
of events taking place in areas classified as rural(Hall et al. 1994 & 1996). Even fewer events arereported for residential areas. Most events occurredon weekdays and typically took place between thehours of 6 a.m. to 6 p.m. Fewer events occurred onthe weekends.
ChemicalsIn the majority of events, only one chemical wasreleased. The most frequently released chemicalswere herbicides (19%), volatile organic compounds(17%), acids (12%), and ammonias (13%) with theremaining substance categories all below 10%.(Hall et al. 1994 & 1996). In events with victims,acids, volatile organic compounds, and ammoniaswere most often released, while an increased num-ber of herbicide releases occurred in transportationevents.
VictimsOn the whole, workers (64%) were injured more fre-quently than the general public (22%) or firstresponders (14%) (e.g., firefighters, police officers,or hazardous materials or emergency responseteams) (Hall et al. 1994 &1996). Typically in trans-portation-related events, fewer (10%) of the victimsinvolved were from the general public (Hall et al.1994 &1996). Most events were associated with alimited number of injuries. For example, half of theevents resulted in just one injured person and onequarter of the remaining events resulted in twoinjured people. The majority of those injured tend-ed to be male with a mean age in the mid-thirties(Hall et al., 1994 & 1995).
InjuriesSome victims sustained more than one type ofinjury from an event. The most frequently reportedinjuries were respiratory irritation (40%) and eyeirritation (27%), followed by nausea (10%) (Hall etal., 1994 &1996). In transportation events, victimsalso commonly received trauma injuries and chem-ical burns. Injuries associated with death were trau-ma, chemical burns, thermal burns, heat stress, car-diac arrest and asphyxiation. Hall et al. (1994)reported that 62% of the victims, including all thevictims from the general public, did not use anytype of personal protective equipment. Treatmenteither occurred on-scene or at the hospital.
EvacuationsEvacuations were ordered for between 13-14% ofthe events occurring between 1990 and 1992 with amajority of the evacuations ordered by a public offi-
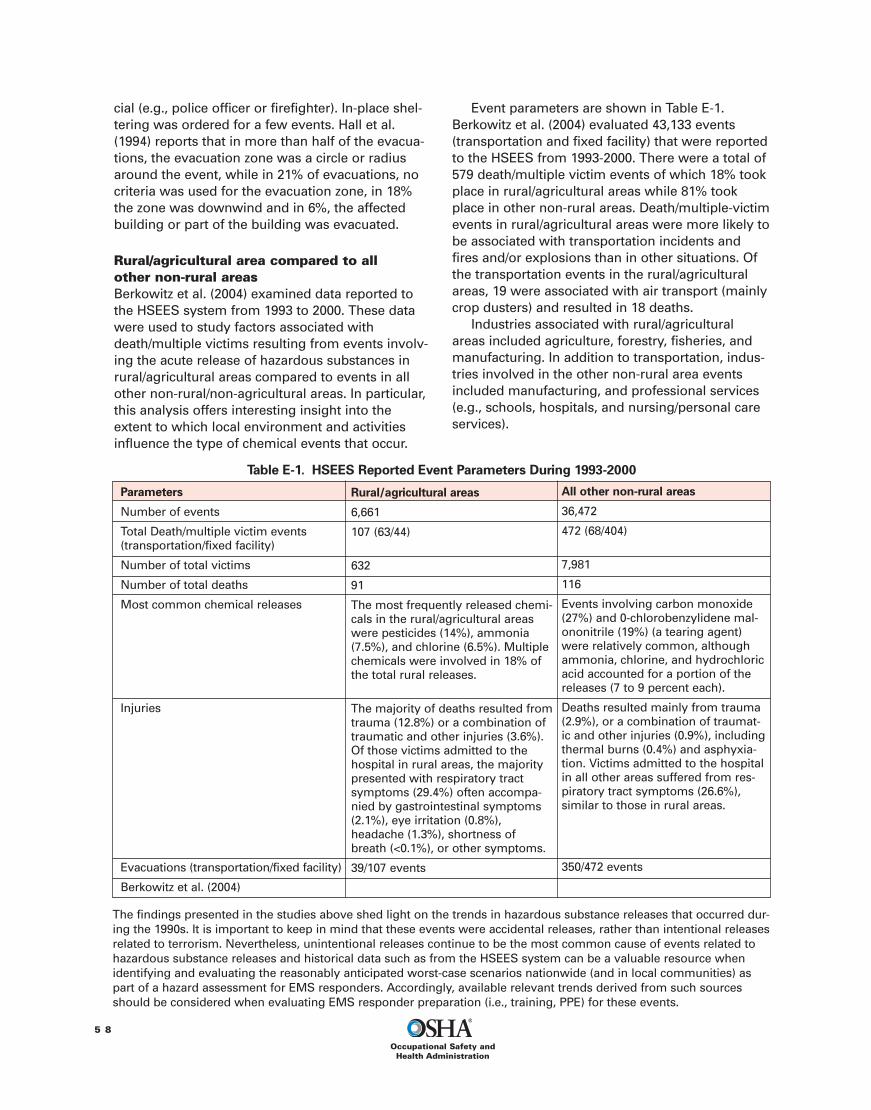
cial (e.g., police officer or firefighter). In-place shel-tering was ordered for a few events. Hall et al.(1994) reports that in more than half of the evacua-tions, the evacuation zone was a circle or radiusaround the event, while in 21% of evacuations, nocriteria was used for the evacuation zone, in 18%the zone was downwind and in 6%, the affectedbuilding or part of the building was evacuated.
Rural/agricultural area compared to allother non-rural areasBerkowitz et al. (2004) examined data reported tothe HSEES system from 1993 to 2000. These datawere used to study factors associated withdeath/multiple victims resulting from events involv-ing the acute release of hazardous substances inrural/agricultural areas compared to events in allother non-rural/non-agricultural areas. In particular,this analysis offers interesting insight into theextent to which local environment and activitiesinfluence the type of chemical events that occur.
Event parameters are shown in Table E-1.Berkowitz et al. (2004) evaluated 43,133 events(transportation and fixed facility) that were reportedto the HSEES from 1993-2000. There were a total of579 death/multiple victim events of which 18% tookplace in rural/agricultural areas while 81% tookplace in other non-rural areas. Death/multiple-victimevents in rural/agricultural areas were more likely tobe associated with transportation incidents andfires and/or explosions than in other situations. Ofthe transportation events in the rural/agriculturalareas, 19 were associated with air transport (mainlycrop dusters) and resulted in 18 deaths.
Industries associated with rural/agriculturalareas included agriculture, forestry, fisheries, andmanufacturing. In addition to transportation, indus-tries involved in the other non-rural area eventsincluded manufacturing, and professional services(e.g., schools, hospitals, and nursing/personal careservices).
5 8
Occupational Safety andHealth Administration
Parameters
Number of events
Total Death/multiple victim events(transportation/fixed facility)
Number of total victims
Number of total deaths
Most common chemical releases
Injuries
Evacuations (transportation/fixed facility)
Berkowitz et al. (2004)
Rural/agricultural areas
6,661
107 (63/44)
632
91
The most frequently released chemi-cals in the rural/agricultural areaswere pesticides (14%), ammonia(7.5%), and chlorine (6.5%). Multiplechemicals were involved in 18% ofthe total rural releases.
The majority of deaths resulted fromtrauma (12.8%) or a combination oftraumatic and other injuries (3.6%).Of those victims admitted to thehospital in rural areas, the majoritypresented with respiratory tractsymptoms (29.4%) often accompa-nied by gastrointestinal symptoms(2.1%), eye irritation (0.8%),headache (1.3%), shortness ofbreath (<0.1%), or other symptoms.
39/107 events
All other non-rural areas
36,472
472 (68/404)
7,981
116
Events involving carbon monoxide(27%) and 0-chlorobenzylidene mal-ononitrile (19%) (a tearing agent)were relatively common, althoughammonia, chlorine, and hydrochloricacid accounted for a portion of thereleases (7 to 9 percent each).
Deaths resulted mainly from trauma(2.9%), or a combination of traumat-ic and other injuries (0.9%), includingthermal burns (0.4%) and asphyxia-tion. Victims admitted to the hospitalin all other areas suffered from res-piratory tract symptoms (26.6%),similar to those in rural areas.
350/472 events
The findings presented in the studies above shed light on the trends in hazardous substance releases that occurred dur-ing the 1990s. It is important to keep in mind that these events were accidental releases, rather than intentional releasesrelated to terrorism. Nevertheless, unintentional releases continue to be the most common cause of events related tohazardous substance releases and historical data such as from the HSEES system can be a valuable resource whenidentifying and evaluating the reasonably anticipated worst-case scenarios nationwide (and in local communities) aspart of a hazard assessment for EMS responders. Accordingly, available relevant trends derived from such sourcesshould be considered when evaluating EMS responder preparation (i.e., training, PPE) for these events.
Table E-1. HSEES Reported Event Parameters During 1993-2000
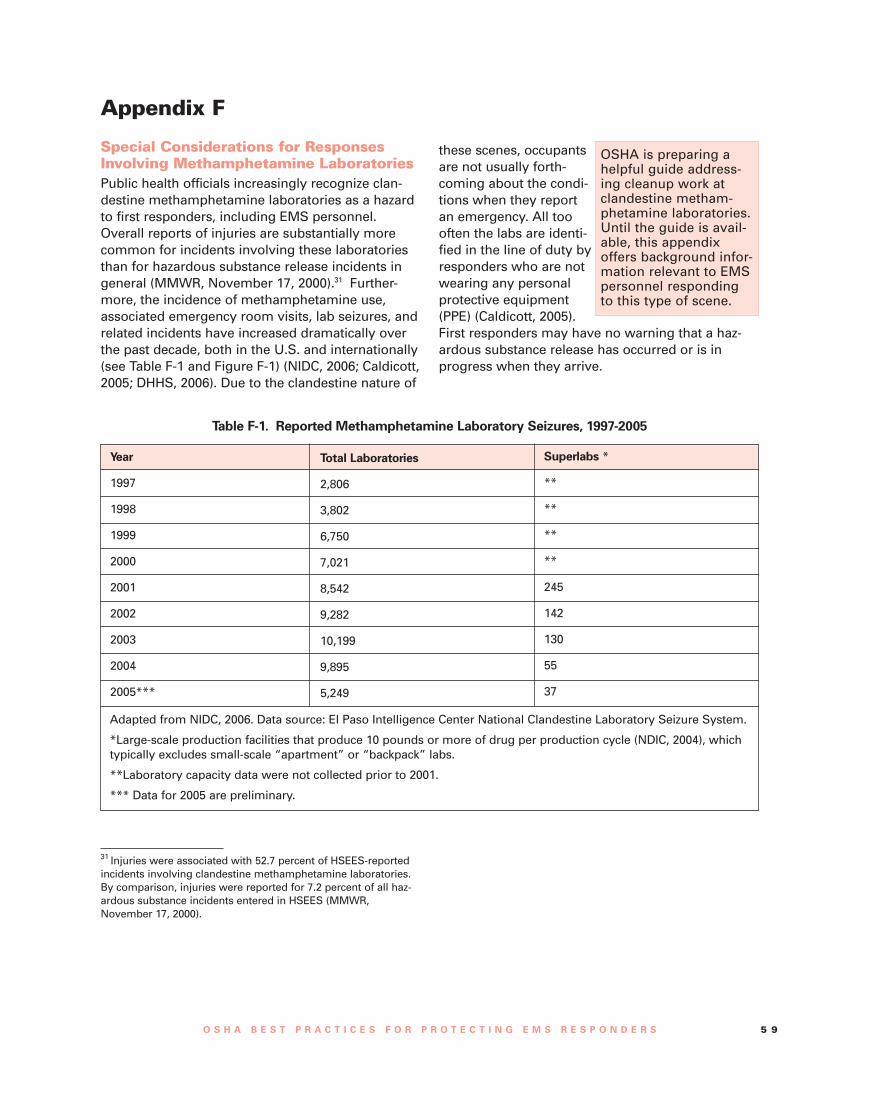
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 5 9
Appendix F
Special Considerations for ResponsesInvolving Methamphetamine LaboratoriesPublic health officials increasingly recognize clan-destine methamphetamine laboratories as a hazardto first responders, including EMS personnel.Overall reports of injuries are substantially morecommon for incidents involving these laboratoriesthan for hazardous substance release incidents ingeneral (MMWR, November 17, 2000).31 Further-more, the incidence of methamphetamine use,associated emergency room visits, lab seizures, andrelated incidents have increased dramatically overthe past decade, both in the U.S. and internationally(see Table F-1 and Figure F-1) (NIDC, 2006; Caldicott,2005; DHHS, 2006). Due to the clandestine nature of
these scenes, occupantsare not usually forth-coming about the condi-tions when they reportan emergency. All toooften the labs are identi-fied in the line of duty byresponders who are notwearing any personalprotective equipment(PPE) (Caldicott, 2005).First responders may have no warning that a haz-ardous substance release has occurred or is inprogress when they arrive.
OSHA is preparing ahelpful guide address-ing cleanup work atclandestine metham-phetamine laboratories.Until the guide is avail-able, this appendixoffers background infor-mation relevant to EMSpersonnel respondingto this type of scene.
Year
1997
1998
1999
2000
2001
2002
2003
2004
2005***
Total Laboratories
2,806
3,802
6,750
7,021
8,542
9,282
10,199
9,895
5,249
Superlabs *
**
**
**
**
245
142
130
55
37
Adapted from NIDC, 2006. Data source: El Paso Intelligence Center National Clandestine Laboratory Seizure System.
*Large-scale production facilities that produce 10 pounds or more of drug per production cycle (NDIC, 2004), whichtypically excludes small-scale “apartment” or “backpack” labs.
**Laboratory capacity data were not collected prior to 2001.
*** Data for 2005 are preliminary.
31 Injuries were associated with 52.7 percent of HSEES-reportedincidents involving clandestine methamphetamine laboratories.By comparison, injuries were reported for 7.2 percent of all haz-ardous substance incidents entered in HSEES (MMWR,November 17, 2000).
Table F-1. Reported Methamphetamine Laboratory Seizures, 1997-2005
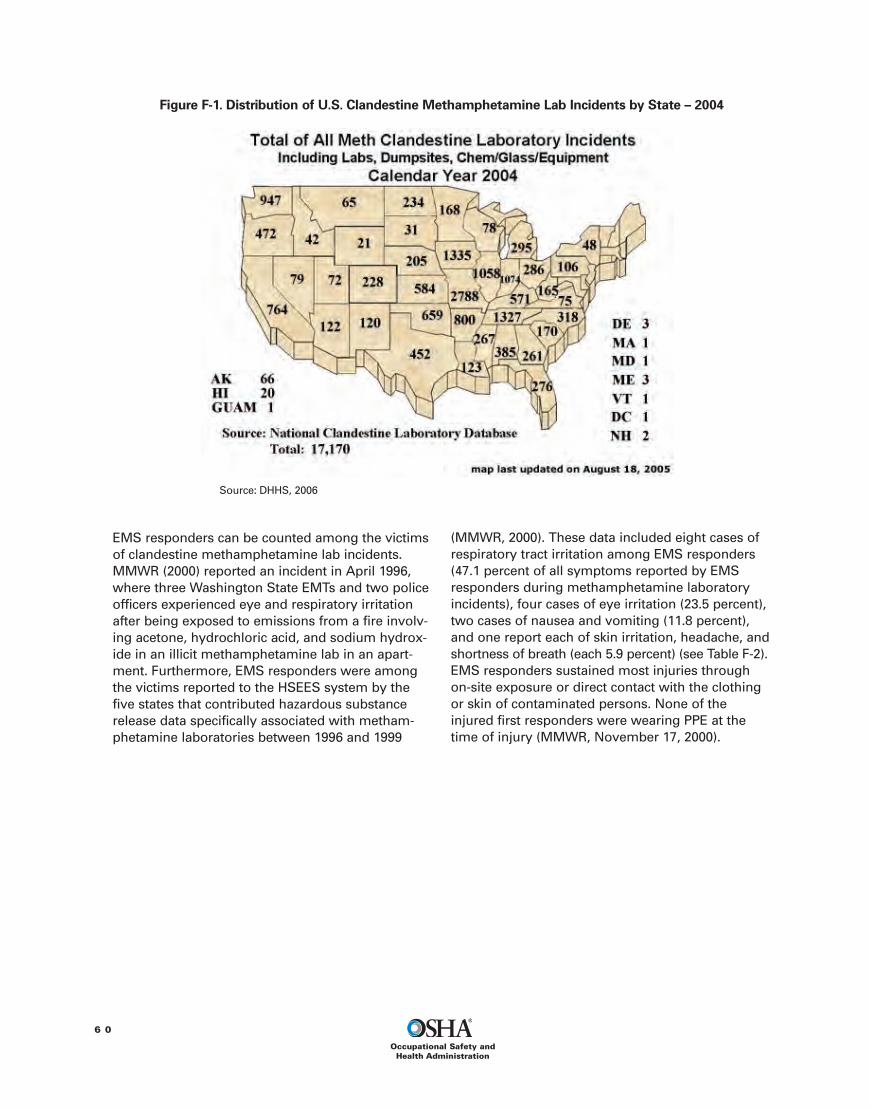
EMS responders can be counted among the victimsof clandestine methamphetamine lab incidents.MMWR (2000) reported an incident in April 1996,where three Washington State EMTs and two policeofficers experienced eye and respiratory irritationafter being exposed to emissions from a fire involv-ing acetone, hydrochloric acid, and sodium hydrox-ide in an illicit methamphetamine lab in an apart-ment. Furthermore, EMS responders were amongthe victims reported to the HSEES system by thefive states that contributed hazardous substancerelease data specifically associated with metham-phetamine laboratories between 1996 and 1999
(MMWR, 2000). These data included eight cases ofrespiratory tract irritation among EMS responders(47.1 percent of all symptoms reported by EMSresponders during methamphetamine laboratoryincidents), four cases of eye irritation (23.5 percent),two cases of nausea and vomiting (11.8 percent),and one report each of skin irritation, headache, andshortness of breath (each 5.9 percent) (see Table F-2).EMS responders sustained most injuries throughon-site exposure or direct contact with the clothingor skin of contaminated persons. None of theinjured first responders were wearing PPE at thetime of injury (MMWR, November 17, 2000).
6 0
Occupational Safety andHealth Administration
Figure F-1. Distribution of U.S. Clandestine Methamphetamine Lab Incidents by State – 2004
Source: DHHS, 2006
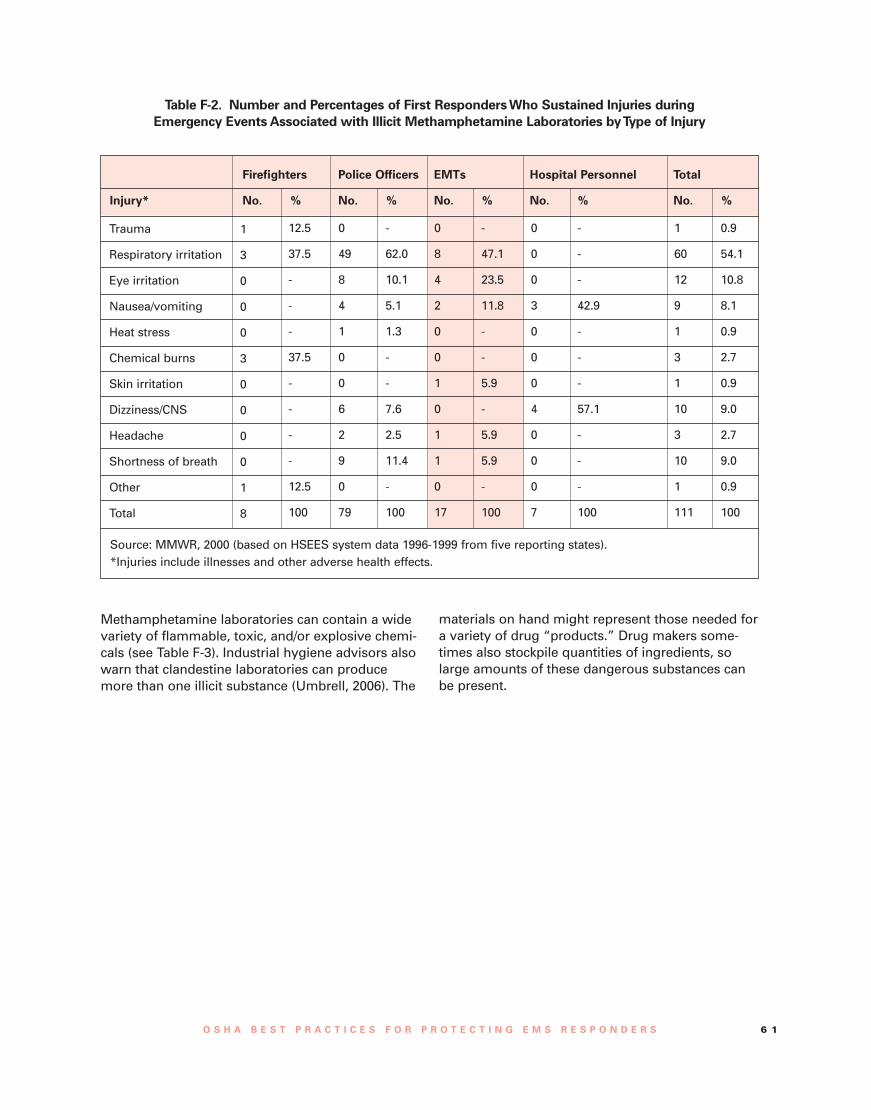
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 6 1
Table F-2. Number and Percentages of First RespondersWho Sustained Injuries duringEmergency Events Associated with Illicit Methamphetamine Laboratories byType of Injury
Trauma
Respiratory irritation
Eye irritation
Nausea/vomiting
Heat stress
Chemical burns
Skin irritation
Dizziness/CNS
Headache
Shortness of breath
Other
Total
1
3
0
0
0
3
0
0
0
0
1
8
Firefighters Police Officers EMTs Hospital Personnel Total
Injury* No. % No. % No. % No. % No. %
12.5
37.5
-
-
-
37.5
-
-
-
-
12.5
100
0
49
8
4
1
0
0
6
2
9
0
79
-
62.0
10.1
5.1
1.3
-
-
7.6
2.5
11.4
-
100
0
8
4
2
0
0
1
0
1
1
0
17
-
47.1
23.5
11.8
-
-
5.9
-
5.9
5.9
-
100
-
-
-
42.9
-
-
-
57.1
-
-
-
100
1
60
12
9
1
3
1
10
3
10
1
111
0.9
54.1
10.8
8.1
0.9
2.7
0.9
9.0
2.7
9.0
0.9
100
0
0
0
3
0
0
0
4
0
0
0
7
Source: MMWR, 2000 (based on HSEES system data 1996-1999 from five reporting states).*Injuries include illnesses and other adverse health effects.
Methamphetamine laboratories can contain a widevariety of flammable, toxic, and/or explosive chemi-cals (see Table F-3). Industrial hygiene advisors alsowarn that clandestine laboratories can producemore than one illicit substance (Umbrell, 2006). The
materials on hand might represent those needed fora variety of drug “products.” Drug makers some-times also stockpile quantities of ingredients, solarge amounts of these dangerous substances canbe present.

6 2
Occupational Safety andHealth Administration
These substances and additional compounds,such as the phosphine gas and hydrogen chlorideemitted when they are mixed or heated, presentserious hazards to the skin, eyes, respiratory tract,central nervous system (CNS), and various targetorgans.
Neither medical surveillance nor occupationalexposure results are available for EMS respondersexposed to hazardous substances during clandes-tine drug lab response. Limited information, howev-er, is available for other responders in related situa-tions. Burgess et al. (2002) evaluated annual med-ical surveillance records for the period 1991 to 1998for 40 California law enforcement drug laboratoryinvestigators (methamphetamine laboratoriesaccount for most drug laboratory investigations.)During the investigations, the officers understoodthe hazards of the situation they would encounterand sometimes took precautions such as wearingrespiratory protection, but also typically spent aconsiderably longer period of time in the laborato-
Table F-3. Chemical Hazards Encountered at Methamphetamine Laboratories
Chemical
Pseudoephedrine
Acetone/ethyl alcohol
Freon
Anhydrous ammonia
Red phosphorus
Hypophosphorous acid
Lithium metal
Hydriodic acid
Iodine crystals
Phenylpropanolamine
Hazards
Ingestion of doses greater than 240 mg causes hypertension, arrhythmia, anxiety, dizzi-ness, and vomiting. Ingestion of doses greater than 600 mg can lead to renal failure andseizures.
Extremely flammable, posing a fire risk in and around the laboratory. Inhalation oringestion of these solvents causes severe gastric irritation, narcosis, or coma.
Inhalation can cause sudden cardiac arrest or severe lung damage.
A colorless gas with pungent, suffocating odor. Inhalation causes edema of the respira-tory tract and asphyxia. Contact with vapors damages eyes and mucous membranes.
May explode as a result of contact or friction. Ignites if heated above 260oC. Vapor fromignited phosphorus severely irritates the nose, throat, lungs, and eyes.
Extremely dangerous substitute for red phosphorus. If overheated, deadly phosphinegas is released. Poses a serious fire and explosion hazard.
Extremely caustic to all body tissues. Reacts violently with water and poses a fire orexplosion hazard.
A corrosive acid with vapors that are irritating to the respiratory system, eyes, and skin.If ingested, causes severe internal irritation and damage that may cause death.
Gives off vapor that is irritating to respiratory system and eyes. Solid form irritates theeyes and may burn skin. If ingested, causes severe internal damage.
Ingestion of doses greater than 75 mg causes hypertension, arrhythmia, anxiety, anddizziness. Quantities greater than 300 mg can lead to renal failure, seizures, stroke, anddeath.
Source: DEA Office of Diversion Control (NDIC, 2004).
ries than would an EMS responder responding to anemergency.
The study results found a median annual declineof 40 milliliters (ml) per year in the officers’ lungfunction (average 64 ±138 ml/year), measured asforced expiratory volume in 1 second (FEV1). “For34 subjects with valid exposure data, longer dura-tion use of respiratory protection was associatedwith a less rapid decline in FEV1, whereas lack ofrespiratory protection during the processing phaseof laboratory investigation was associated with amore rapid annual decline.” The authors recom-mended “more assiduous use of respiratory protec-tion” (Burgess et al., 2002). Results of blood testsadministered as part of routine medical surveillancesuggest no significant longitudinal changes inparameters, including serum alanine aminotrans-ferase, serum aspartate aminotransferase, hemoglo-bin, and white cell count, “although plateletsdeclined slightly.”
Other investigators in Colorado noted a lack of

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 6 3
• Regardless of whether a cook is being conductedat the time of entry, it is likely that most itemsand individuals in the vicinity of the cook will becontaminated with methamphetamine.
• If a methamphetamine cook has been conductedwithin a building, chemicals from the cook willhave spread not only in the specific area of thecook but throughout the building. This is espe-cially true of hydrogen chloride and metham-phetamine.
• If a methamphetamine cook has been conductedwithin a building, all children within that buildingare likely to have been exposed to methamphet-amine and other chemicals and should be con-sidered as exposed and contaminated.
• If any law enforcement or emergency servicespersonnel are to be entering a building suspect-ed of being a clandestine methamphetamine lab-oratory, they should enter only with self-con-tained breathing apparatus and complete skinprotection unless it is known that the lab has notbeen in recent operation and that all of thechemicals are under control. In the opinion of theauthors, it is not likely that these conditions willbe known prior to entry in most cases. We there-fore suggest that all initial entries be made withthe PPE previously mentioned.
• After the suspected laboratory is known to beout of operation and the chemicals are in a sta-ble condition, then investigators could reducethe respiratory protection portion of the PPE to afull-face air-purifying respirator with organicvapor, acid gas, and P100 combination car-tridges.
• All law enforcement officers and emergencyservices personnel should be made aware of thehigh potential for exposure to methampheta-mine contamination and trained in the methodsto reduce the “take home” levels of metham-phetamine. Testing at the scene on a periodicbasis should be used to verify that personnel arenot being contaminated on-scene.
• Decontamination of all items taken out of thesuspected laboratory should be conducted.Efforts should be made to reduce contaminationtransfer outside of the laboratory and periodictesting should be conducted to assure that per-sonnel and items are being adequately decon-taminated.”
information about airborne concentrations of haz-ardous substances in active methamphetamine lab-oratories. This type of exposure information is nec-essary to ensure that first responders are adequate-ly protected when they enter such an environment.As a step toward characterizing the potential forexposure, the researchers conducted extensiveindustrial hygiene area and personal air monitoringduring controlled drug “cooking” experiments. Forthis experiment, the two “cooks,” both forensicchemists, used two different, but common, meth-amphetamine production methods. One cook usedhypophosphorous, while the other used flake phos-phorous, both of which are substitutes for red phos-phorus (typical of another common method). Theresearchers also obtained wipe samples used toevaluate the extent to which hazardous substanceswere deposited on surfaces. These experimentswere conducted in realistic settings: the bathroomand living area of condemned structures similar tothose often used as drug laboratories (Martyny etal., 2005).
The results of these tests showed that short-termexposure levels to hazardous substances in a func-tioning methamphetamine laboratory can be elevat-ed to a level that can cause acute and chronic healtheffects. Although personal exposure levels were nottypically in the IDLH range, short-term phosphinelevels as high as 62.3 ppm were recorded in theimmediate cooking area (on the table). This exceedsthe IDLH for phosphine of 50 ppm. Furthermore,individuals who have been “cooking” methamphet-amine can carry significant surface contamination.The findings also indicate that surfaces throughoutthe structure can be contaminated with metham-phetamine even after a single cooking cycle(Martyny et al., 2005).
Based on their sampling results, Martyny et al.(2005) offered several conclusions relevant to EMSresponders responding to the scene involving amethamphetamine laboratory. These are quotedhere:• “If a methamphetamine cook is being conducted
and the hypophosphorous manufacturingmethod is used, then exposure to levels ofhydrogen chloride that exceed current occupa-tional levels are likely.
• During the cook, it is possible that exposures tohydrogen chloride will exceed levels consideredby NIOSH to be immediately dangerous to life orhealth (IDLH).
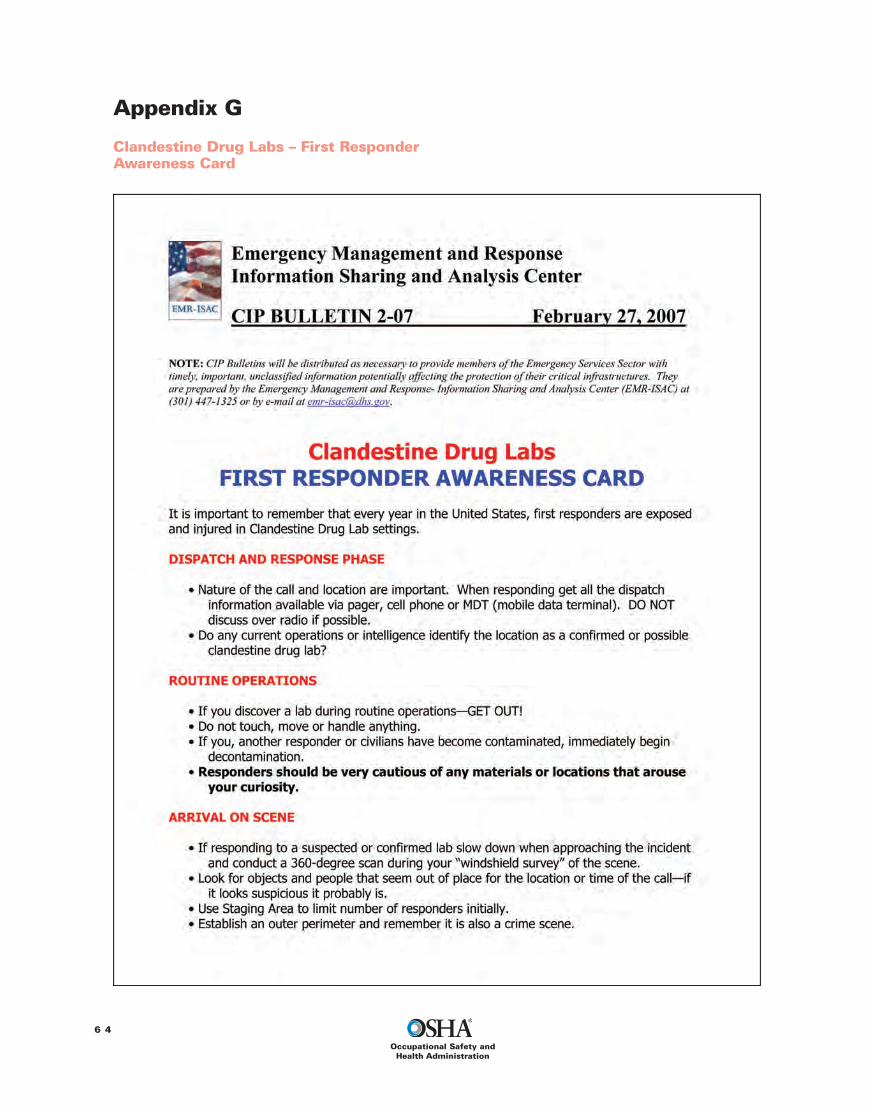
Appendix G
Clandestine Drug Labs – First ResponderAwareness Card
6 4
Occupational Safety andHealth Administration
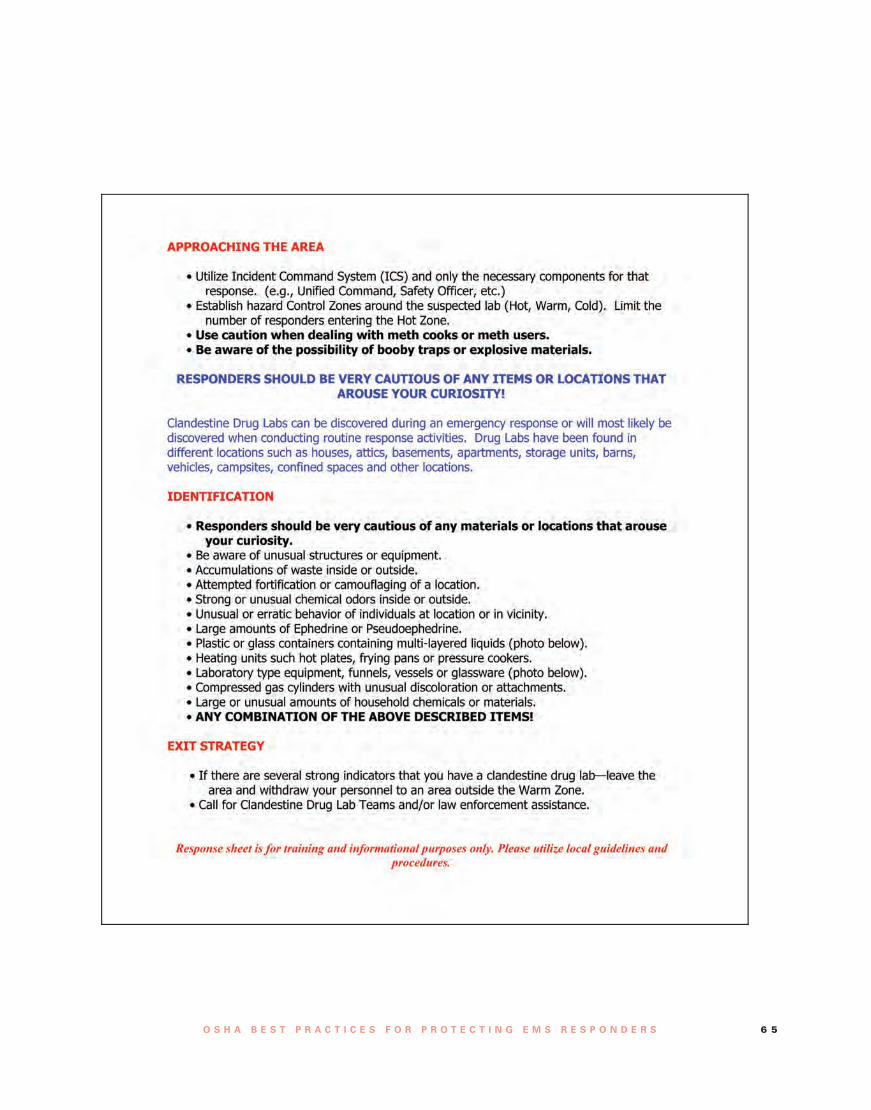
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 6 5

Appendix H
Training Curricula OptionsTraining Curricula for EMS RespondersBackgroundThe National Highway Traffic Safety Administration(NHTSA) curricula for EMS responders introducessome topics relevant to HAZWOPER first respondertraining. As noted in Appendix P, however, (see dis-cussion of the roles of NHTSA and states in EMSresponder training), that curricula does not in itselfmeet OSHA’s requirements because it lacks informa-tion on relevant local community conditions.Furthermore, depending on how the NHTSA cur-riculum is offered, it might not meet the required 8-hour HAZWOPER training duration for first respon-der operations level.
The National Fire Protection Association (NFPA)offers an extensive list of competencies that supple-ment OSHA’s requirements for EMS responders’HAZWOPER training at the first responder aware-ness and operations levels (as well as higher levels).Specifically, the non-regulatory NFPA 472 providesdetailed recommendations for competencies NFPAbelieves are important for all first responders (e.g.,firefighters, police, EMS) who work at the aware-ness or operations levels (NFPA-742, 2008). A com-panion standard (also non-regulatory), NFPA 473,suggests additional areas of competence specificallytailored for EMS personnel (NFPA-473, 2008).
Two non-regulatory (optional) NFPA stan-dards suggest training topics that can beincluded in HAZWOPER training for EMSresponders. These two standards are:• NFPA 472 Standard for Competence ofResponders to Hazardous Materials/Weapons of Mass Destruction Incidents(2008)
• NFPA 473 Standard for Competence forEMS Personnel Responding to HazardousMaterials/Weapons of Mass DestructionIncidents (2008)
OSHA says of these and other NFPA standards(such as NFPA 471 – Recommended Practice forResponding to Hazardous Material Incidents):
In general, employers of emergency responseorganizations who follow the NFPA standardsshould be in compliance with 29 CFR1910.120(q). It is important that the applicableportions of all related standards be followed.(OSHA, 2007-CPL-02-02-073).As an example, OSHA notes that NFPA 471 no
longer addresses the position of “safety officer,”
although another NFPA standard (NFPA 1500 –Standard on Fire Department Occupational Safetyand Health Program) does. A designated safety offi-cer, however, is mandatory in the HAZWOPER stan-dard. OSHA would consider the absence of a safetyofficer as a failure to comply with the standard(OSHA, 2007-CPL-02-02-073). Employers who useNFPA standards are ultimately responsible forensuring that they are providing training or allowingemployees to demonstrate competence that meetsOSHA’s requirements.
The following sections provide an outline ofsome of the competencies presented in NFPA 472and NFPA 473 that are most relevant to EMSresponders. Each competency includes a brief sum-mary of how responder competence is evaluated. Ingeneral, although not precisely aligned with OSHA’scompetencies for first responders at the awarenessand operations levels, an EMS responder thatdemonstrated competence in each of the areas list-ed by NFPA would likely also in the process demon-strate OSHA’s required competencies, as long as thescenarios used for discussion are provided with theHAZWOPER competencies in mind. Consult theNFPA’s standards for complete listings of the indi-vidual competencies and specific details of NFPA’srecommendations for demonstrating competence.
Select Examples of Core Competencies forFirst Responder Awareness Level PersonnelRecommended in NFPA 472:
Detecting the presence of hazardous materials(responder is requested to identify situations wherehazardous materials are present, provide numerousexamples of hazardous materials categories, identi-fy specific types of container marking; perform exer-cises involving material safety data sheets (MSDSs)and shipping papers, and identify indicators of pos-sible criminal activity relating to various types ofhazardous substances or sites).
Surveying hazardous materials and collectingrelated information (responder is requested toname hazardous materials described in exampleincidents, describe methods for determining sub-stance names, and look up information in a stan-dard reference book).
Initiating protective actions (responder isrequested to identify basic information from scenar-ios and plans, including the role of individuals atfirst responder awareness level, appropriate precau-tions and PPE (from given lists), and security meas-ures).
6 6
Occupational Safety andHealth Administration

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 6 7
Initiating the notification process (responder isrequested to identify details related to notification inprovided scenarios).
Select Examples of Core Competencies forFirst Responder Operations Level PersonnelRecommended in NFPA 472:
Competencies listed for first responder aware-ness level personnel.
Surveying hazardous material incidents (respon-der is requested to discuss hazardous materialscontainers/packaging, possible materials releaseand site conditions for example scenarios, and fromprovided lists pick the correct answers to relatedquestions).
Describing response objectives and identifyingactions (responder is requested to describe expo-sures that could be avoided and risks to respondersunder different scenarios or for different hazardclasses).
Determine suitability of PPE and decontamina-tion issues (responder is requested to decidewhether available PPE is adequate for example situ-ations, describe various SCBA and protective cloth-ing configurations, and exhibit knowledge aboutdecontamination methods, equipment, and issues).
Scene control and preserving evidence (respon-der is requested to identify criteria and techniquesfor establishing scene control, allowing personnel towork, and preserving evidence under various inci-dent site conditions).
Initiating the ICS (responder is requested todemonstrate ICS initiation for a given scenario’s ERPand identify various elements of an ICS).
Using PPE (responder is requested to identify ordiscuss various factors that are critical to correctlyusing PPE, such as when to use a buddy system,control of thermal stress, and how to clean andinspect PPE).
Select Examples of Competencies for Basic LifeSupport and Advanced Life Support PersonnelRecommended in NFPA 473:
The non-regulatory NFPA 473 is intended for“EMS personnel who respond to incidents involvinghazardous materials or weapons of mass destruc-tion.” NFPA 473 also assumes that these EMSresponders “are trained to meet at least the corecompetencies of the operations level responders”as presented in NFPA 472 (NFPA-473, 2008). It isunderstood that in any area of competence involv-ing direct patient care, the EMS responder’s activi-ties must be within the scope of practice and train-ing of the individual responder.
NFPA 473 is aligned along EMS responder quali-
fications to provide basic life support (BLS) oradvanced life support (ALS), rather than along firstresponder awareness or operations level trainingrequirements. Some employers might link BLS andALS qualifications to workers roles requiring firstresponder operations level training and first respon-der awareness level training, respectively. Otheremployers, however, might designate worker rolesalong different lines, depending on conditions in thecommunity and the employers’ response plans.Although most NFPA 473 competencies for bothBLS and ALS personnel are similar (or identical),there are a few differences and these are indicatedby an asterisk (*) and notation summarizing the dif-ference.
The following summary provides a number ofexamples of the types of competencies included inNFPA 473 specifically for EMS responders. Again,consult the NFPA’s standards for complete listingsof the individual competencies and specific detailsof NFPA’s recommendations for demonstratingcompetence.
Surveying hazardous materials incidents(responder is requested to describe details of identi-fication, spread of contamination, effects or treat-ment for a range of physical, chemical and biologi-cal hazard types). [*ALS responder is also asked todiscuss how site and patients should be observedfor signs of exposure.]32
Collecting and interpreting hazard and responseinformation (responder is requested to discussmethods for gathering information about an inci-dent and the health effects of any hazardous materi-als involved). [*ALS responder is also asked to iden-tify ways to determine whether secondary devicesor other hazards might be present at the scene.]
Identifying high risk areas for potential expo-sures (responder is requested to assimilate giveninformation from a variety of sources and determineareas where exposure is likely to occur.)
Incident communications (responder is request-ed to identify effective ways to communicate in sup-port of the response plan).
Role of the BLS level responder [*or ALS levelresponder] (responder is requested to describe theICS and how EMS responders function in perform-ing specific duties within the system).
Determining the nature of the incident and pro-viding medical care (responder is requested to dis-cuss various modes and effects on patients of haz-ardous substance exposure during incidents). [*ALS
32 An asterisk (*) indicates a notable difference in this competen-cy for BLS responders compared to what is expected of ALSresponders.

responder is expected to determine the physical andtoxicological/symptomatic characteristics of sub-stances to which a patient could be exposed.]
Decontamination (responder is requested todetermine or identify specific aspects of decontami-nation procedures presented in a model plan andassociated standard operating procedures (SOPs).[*ALS responder is expected to be able to executespecific tasks that form major components of thedecontamination phase of a sample ERP and associ-ated SOPs, for individual and mass decontamina-tion scenarios.]
Preserving evidence (responder is requested todetermine whether criminal acts are involved inexample incidents and identify ways of safeguard-ing evidence while providing medical care).
Medical support for incidents (responder isrequested to describe or demonstrate how to createand execute various aspects of a medical monitor-ing plan for responders wearing PPE). [*ALSresponder is asked to do the same for responderswearing chemical protective suits.]
Tips for Successful EMS ResponderHAZWOPER Training ProgramsSuccessful first responder training at the awarenessand operations levels depends on effective curriculaand on teaching methods that are compatible withadult learners who are probably not accustomed tospending time in a classroom.
One technique for drafting a successful trainingprogram involves starting by outlining lectures andexercises that will provide participants with the
tools they need to successfully “demonstrate com-petency” to perform the expected job functionssafely and effectively. Once the curricula addressesthose needs, details about laws, standards, and reg-ulatory requirements can be incorporated into thetraining program where they are most relevant.
Experienced trainers keep students engaged inlearning by organizing the curricula to alternate lec-ture periods and hands-on practical sessions.Sometimes this means that some basic informationneeds to be shifted later in the course to allow ahands-on skill-development session (e.g., PPE use)to be inserted between lecture sessions. Instructorscan help improve the learning experience by tailor-ing course material so it is related to participants’work and life experience. The more interactive thecourse, the more easily students will learn.
OSHA permits EMS responders who receive firstresponder training (or demonstration of compe-tence) at the awareness level to count it towards theoperations level training requirements. This meansthat an employer may be able to offer just oneclass, with the first responder awareness level stu-dents attending only the first portion of the class.
OSHA allows flexibility in how EMS responderscomplete the initial and annual refresher trainingrequirements. Those who are able to satisfy part orall of their HAZWOPER training requirement bydemonstrating competence may be offered oppor-tunities to do so as part of organized training ses-sion, drills, and exercises. OSHA also allows work-ers who participate in critiques after incidents tocount that experience toward their training.
6 8
Occupational Safety andHealth Administration
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 6 9
Appendix I
Hospital Incident Command SystemEmployers of EMS responders must work closelywith hospitals and other organizations during a haz-ardous substance release that affects patients. Theemployers should be familiar with incident com-mand system structures used in their communities,including the Hospital Incident Command System(HICS) updated from the earlier version (hospitalemergency incident command system – HEICS) in2006. HICS is published by the California EmergencyMedical Services Authority (EMSA). The followingexcerpt from the HICS Guidebook is provided as anintroduction to this 2006 version and is followed byHICS Section 4.7.2 – Fire and Emergency MedicalServices.
Excerpt from Hospital IncidentCommand System Guidebook:ForwardHospitals throughout the United States confronta myriad of operational and fiscal challenges ona daily basis. To effectively manage emergen-cies, whether external (e.g., fires, earthquakes) orinternal (e.g., child abductions, utility failure),hospitals must invest the time and necessaryfunds to ensure adequate preparations are inplace. Recent events such as the September 11,2001 terrorism attacks, the Severe AcuteRespiratory Syndrome (SARS) outbreak in 2004,and the Gulf Coast hurricanes of 2006 demon-strated the importance of hospital preplanningand personnel training.
Since its inception in the late 1980s, theHospital Emergency Incident Command System(HEICS) served as an important emergency man-agement foundation for hospitals in the UnitedStates. We recognized the value and importanceof using an incident management system, notonly in emergency situations but also in dailyoperations, preplanned events, and non-emer-gent situations. Therefore, the HEICS IV Project,sponsored by the California Emergency MedicalServices Authority, has evolved to becomeHICS—the Hospital Incident Command System—a comprehensive incident management systemintended for use in both emergent and non-emergent situations.
The HEICS IV project is not intended to be theonly answer to a hospital’s emergency prepared-ness needs. However, we believe this Guidebookand the accompanying materials can play a
major role in advancing institutional prepared-ness while providing needed local, state, andnational standardization of hospital emergencyresponse and recovery.
We believe the new Hospital IncidentCommand System has built upon the benefitsand successes of the original HEICS and pro-vides hospitals of all sizes with tools needed toadvance their emergency preparedness andresponse capability—both individually and as amember of the broader response community.
Fire and Emergency Medical Services - Section4.7.2Fire departments, private ambulance providers,air medical services, and a governing EmergencyMedical Services (EMS) entity all have significantroles and interface with hospitals in the UnitedStates.
Fire departments provide any or all of the fol-lowing services: first responder basic life support(BLS) and/or advance life support (ALS) medicalcare; ambulance transport; hazmat response;and search and rescue.
Private ambulance companies provide BLSand/or ALS transport for 911 responses; inter-facility transports; and standby for prescheduledevents, hazmat events, or search and rescueevents.
EMS governing entities (which may be firedepartments) provide medical direction to pre-hospital emergency medical technicians (EMTs)and paramedics and system oversight for allambulance activities, to include licensure,inspection, and approval or agreement for oper-ating areas. The medical oversight often extendsto the interface between pre-hospital and hospi-tal EMS, and in many communities this entityacts as the disaster coordinator/manager in alarge-scale emergency.
Hospitals should also be familiar with airmedical services that may be used and have anindividual or community plan for how best tocoordinate multiple requests for assistance.Planning consideration should be given to howhelicopters or fixed wing aircraft can assist withpersonnel, patient, and equipment/supply trans-port if necessary.
During an emergency, EMS (which we defineas the combination of any of the servicesdescribed above) can be expected to bring a sig-

nificant segment of the involved population tothe hospital for medical care. For this reason,information-sharing procedures must be wellknown by both parties, and dependable andredundant communication systems and technol-ogy must be in place and properly used.
Hospitals should also be familiar with theircommunity multiple/mass casualty plan, includ-ing appropriate response codes and terminology,as well as the triage, treatment, and transporta-tion practices to be employed. EMS personnelshould have a fundamental understanding ofhow the hospital will respond, including whatinformation is needed to declare a disaster, alter-native travel routes into the facility, and wheretriage and decontamination will be conducted.
Preplanning should also address issues such aswhat personnel supplementation can be provid-ed by either party, including trained decontami-nation team supplementation, and how responseinformation will be shared. In addition to patienttransport and possible staff and equipment aug-mentation, EMS responds when the hospitalitself is the scene of an incident; plans for suchresponse should also be mutually developed.
More Information:More information on the Hospital IncidentCommand System can be found at www.emsa.ca.gov/HICS/default.asp (accessed July 10,2009).
7 0
Occupational Safety andHealth Administration
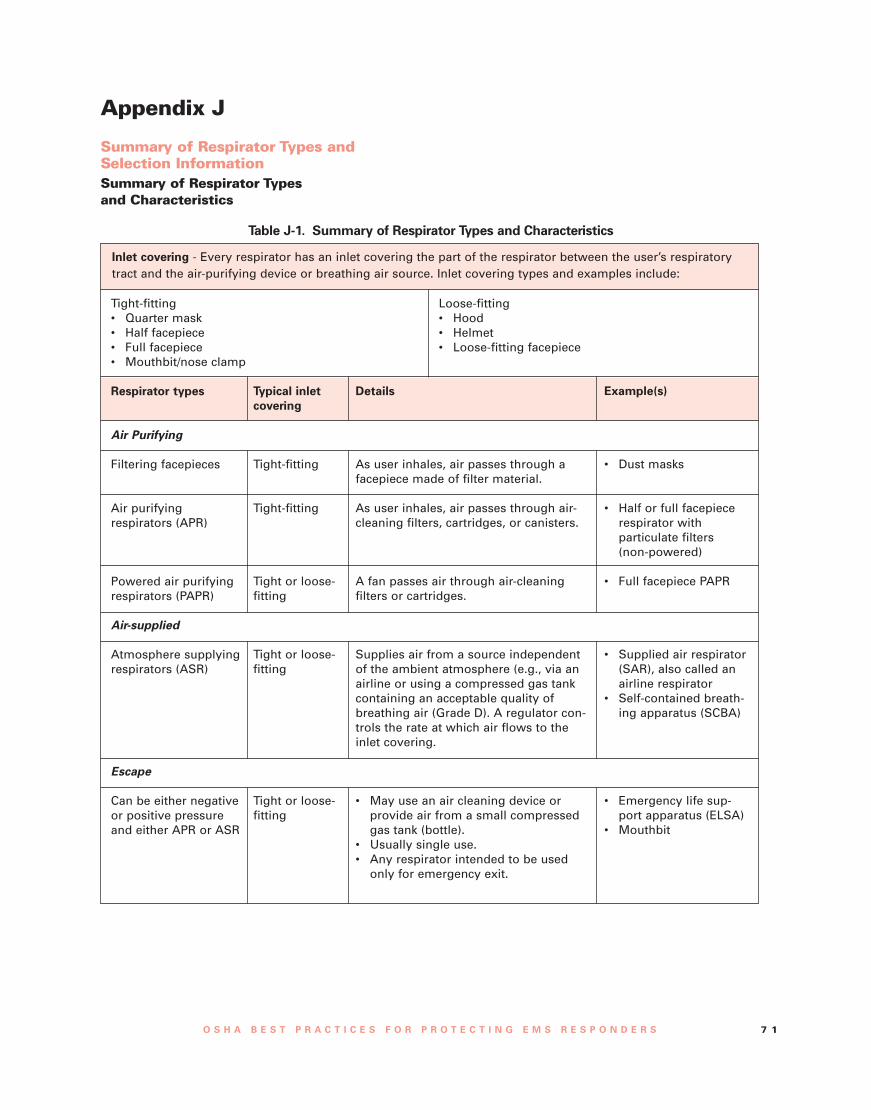
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7 1
Appendix J
Summary of Respirator Types andSelection InformationSummary of Respirator Typesand Characteristics
Table J-1. Summary of Respirator Types and Characteristics
Inlet covering - Every respirator has an inlet covering the part of the respirator between the user’s respiratorytract and the air-purifying device or breathing air source. Inlet covering types and examples include:
Tight-fitting• Quarter mask• Half facepiece• Full facepiece• Mouthbit/nose clamp
Loose-fitting• Hood• Helmet• Loose-fitting facepiece
Respirator types
Air Purifying
Filtering facepieces
Air purifyingrespirators (APR)
Powered air purifyingrespirators (PAPR)
Air-supplied
Atmosphere supplyingrespirators (ASR)
Escape
Can be either negativeor positive pressureand either APR or ASR
Typical inletcovering
Tight-fitting
Tight-fitting
Tight or loose-fitting
Tight or loose-fitting
Tight or loose-fitting
Details
As user inhales, air passes through afacepiece made of filter material.
As user inhales, air passes through air-cleaning filters, cartridges, or canisters.
A fan passes air through air-cleaningfilters or cartridges.
Supplies air from a source independentof the ambient atmosphere (e.g., via anairline or using a compressed gas tankcontaining an acceptable quality ofbreathing air (Grade D). A regulator con-trols the rate at which air flows to theinlet covering.
• May use an air cleaning device orprovide air from a small compressedgas tank (bottle).
• Usually single use.• Any respirator intended to be used
only for emergency exit.
Example(s)
• Dust masks
• Half or full facepiecerespirator withparticulate filters(non-powered)
• Full facepiece PAPR
• Supplied air respirator(SAR), also called anairline respirator
• Self-contained breath-ing apparatus (SCBA)
• Emergency life sup-port apparatus (ELSA)
• Mouthbit
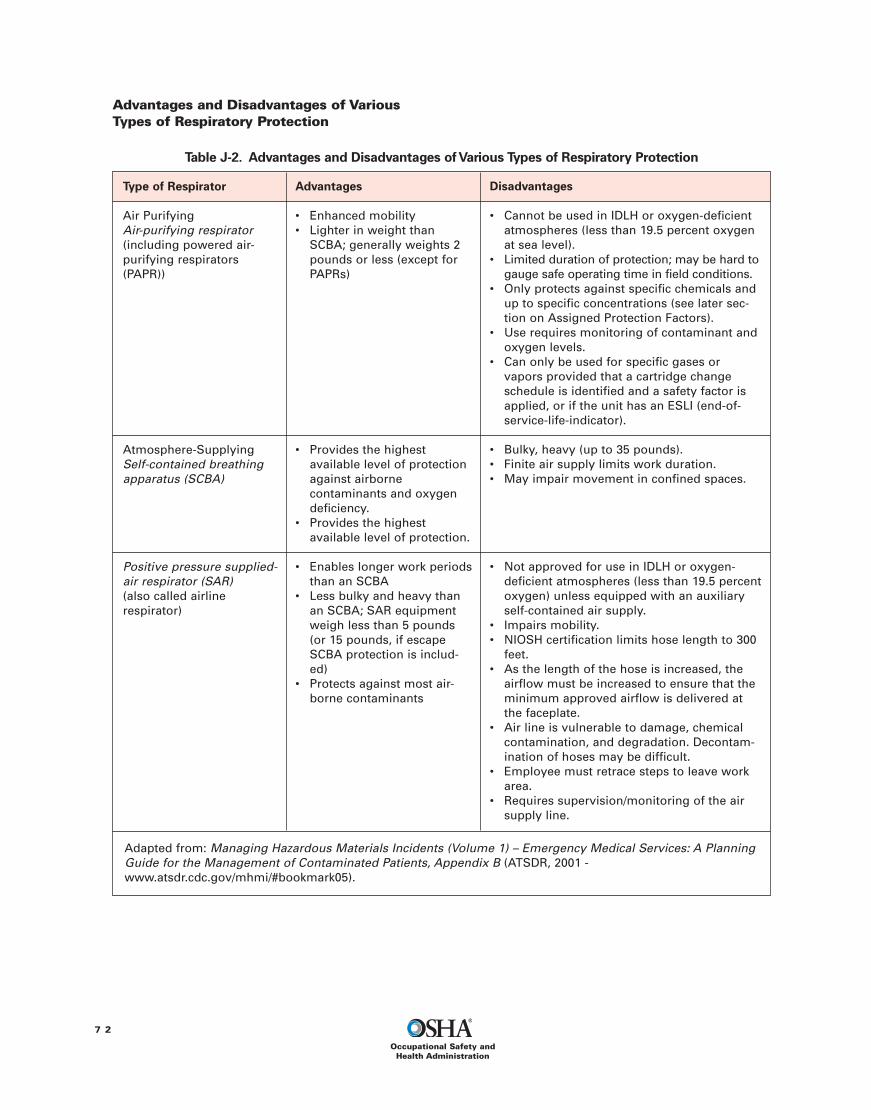
Advantages and Disadvantages of VariousTypes of Respiratory Protection
7 2
Occupational Safety andHealth Administration
Table J-2. Advantages and Disadvantages ofVarious Types of Respiratory Protection
Type of Respirator
Air PurifyingAir-purifying respirator(including powered air-purifying respirators(PAPR))
Atmosphere-SupplyingSelf-contained breathingapparatus (SCBA)
Positive pressure supplied-air respirator (SAR)(also called airlinerespirator)
Advantages
• Enhanced mobility• Lighter in weight than
SCBA; generally weights 2pounds or less (except forPAPRs)
• Provides the highestavailable level of protectionagainst airbornecontaminants and oxygendeficiency.
• Provides the highestavailable level of protection.
• Enables longer work periodsthan an SCBA
• Less bulky and heavy thanan SCBA; SAR equipmentweigh less than 5 pounds(or 15 pounds, if escapeSCBA protection is includ-ed)
• Protects against most air-borne contaminants
Disadvantages
• Cannot be used in IDLH or oxygen-deficientatmospheres (less than 19.5 percent oxygenat sea level).
• Limited duration of protection; may be hard togauge safe operating time in field conditions.
• Only protects against specific chemicals andup to specific concentrations (see later sec-tion on Assigned Protection Factors).
• Use requires monitoring of contaminant andoxygen levels.
• Can only be used for specific gases orvapors provided that a cartridge changeschedule is identified and a safety factor isapplied, or if the unit has an ESLI (end-of-service-life-indicator).
• Bulky, heavy (up to 35 pounds).• Finite air supply limits work duration.• May impair movement in confined spaces.
• Not approved for use in IDLH or oxygen-deficient atmospheres (less than 19.5 percentoxygen) unless equipped with an auxiliaryself-contained air supply.
• Impairs mobility.• NIOSH certification limits hose length to 300
feet.• As the length of the hose is increased, the
airflow must be increased to ensure that theminimum approved airflow is delivered atthe faceplate.
• Air line is vulnerable to damage, chemicalcontamination, and degradation. Decontam-ination of hoses may be difficult.
• Employee must retrace steps to leave workarea.
• Requires supervision/monitoring of the airsupply line.
Adapted from: Managing Hazardous Materials Incidents (Volume 1) – Emergency Medical Services: A PlanningGuide for the Management of Contaminated Patients, Appendix B (ATSDR, 2001 -www.atsdr.cdc.gov/mhmi/#bookmark05).
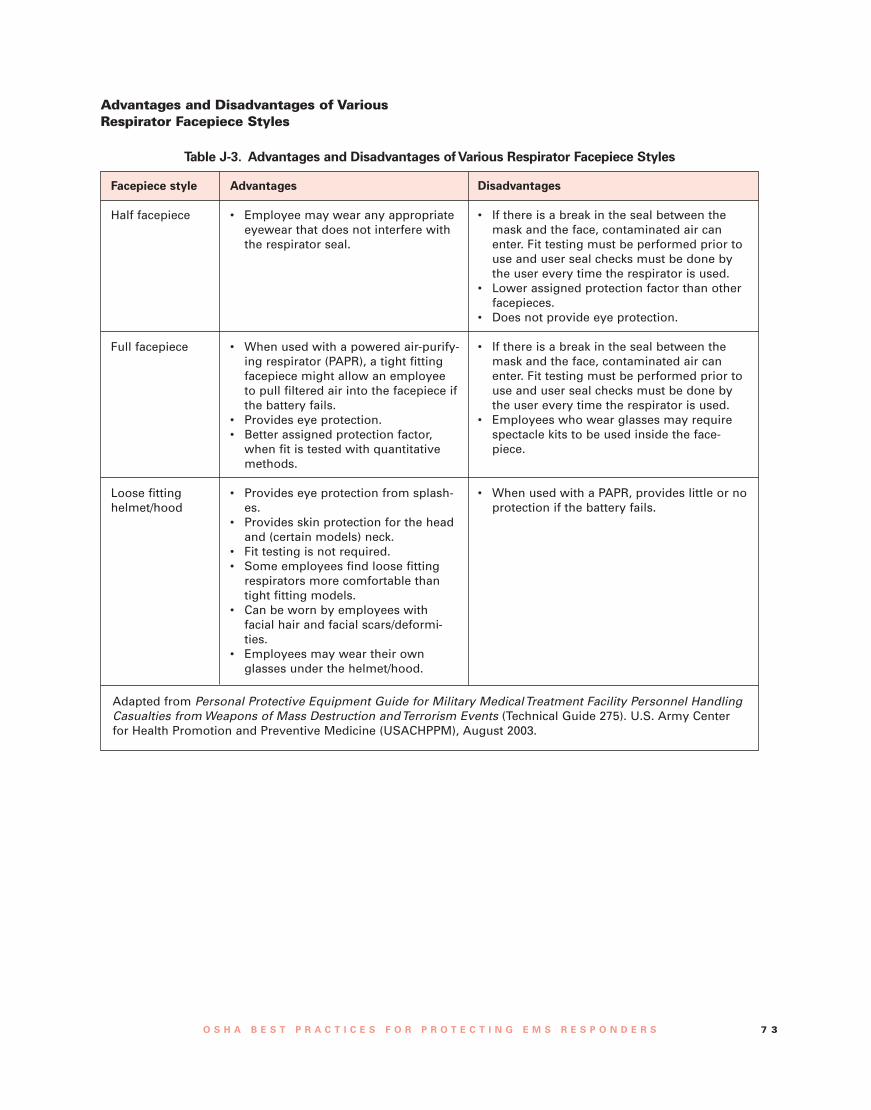
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7 3
Advantages and Disadvantages of VariousRespirator Facepiece Styles
Table J-3. Advantages and Disadvantages ofVarious Respirator Facepiece Styles
Facepiece style
Half facepiece
Full facepiece
Loose fittinghelmet/hood
Advantages
• Employee may wear any appropriateeyewear that does not interfere withthe respirator seal.
• When used with a powered air-purify-ing respirator (PAPR), a tight fittingfacepiece might allow an employeeto pull filtered air into the facepiece ifthe battery fails.
• Provides eye protection.• Better assigned protection factor,
when fit is tested with quantitativemethods.
• Provides eye protection from splash-es.
• Provides skin protection for the headand (certain models) neck.
• Fit testing is not required.• Some employees find loose fitting
respirators more comfortable thantight fitting models.
• Can be worn by employees withfacial hair and facial scars/deformi-ties.
• Employees may wear their ownglasses under the helmet/hood.
Disadvantages
• If there is a break in the seal between themask and the face, contaminated air canenter. Fit testing must be performed prior touse and user seal checks must be done bythe user every time the respirator is used.
• Lower assigned protection factor than otherfacepieces.
• Does not provide eye protection.
• If there is a break in the seal between themask and the face, contaminated air canenter. Fit testing must be performed prior touse and user seal checks must be done bythe user every time the respirator is used.
• Employees who wear glasses may requirespectacle kits to be used inside the face-piece.
• When used with a PAPR, provides little or noprotection if the battery fails.
Adapted from Personal Protective Equipment Guide for Military MedicalTreatment Facility Personnel HandlingCasualties fromWeapons of Mass Destruction andTerrorism Events (Technical Guide 275). U.S. Army Centerfor Health Promotion and Preventive Medicine (USACHPPM), August 2003.
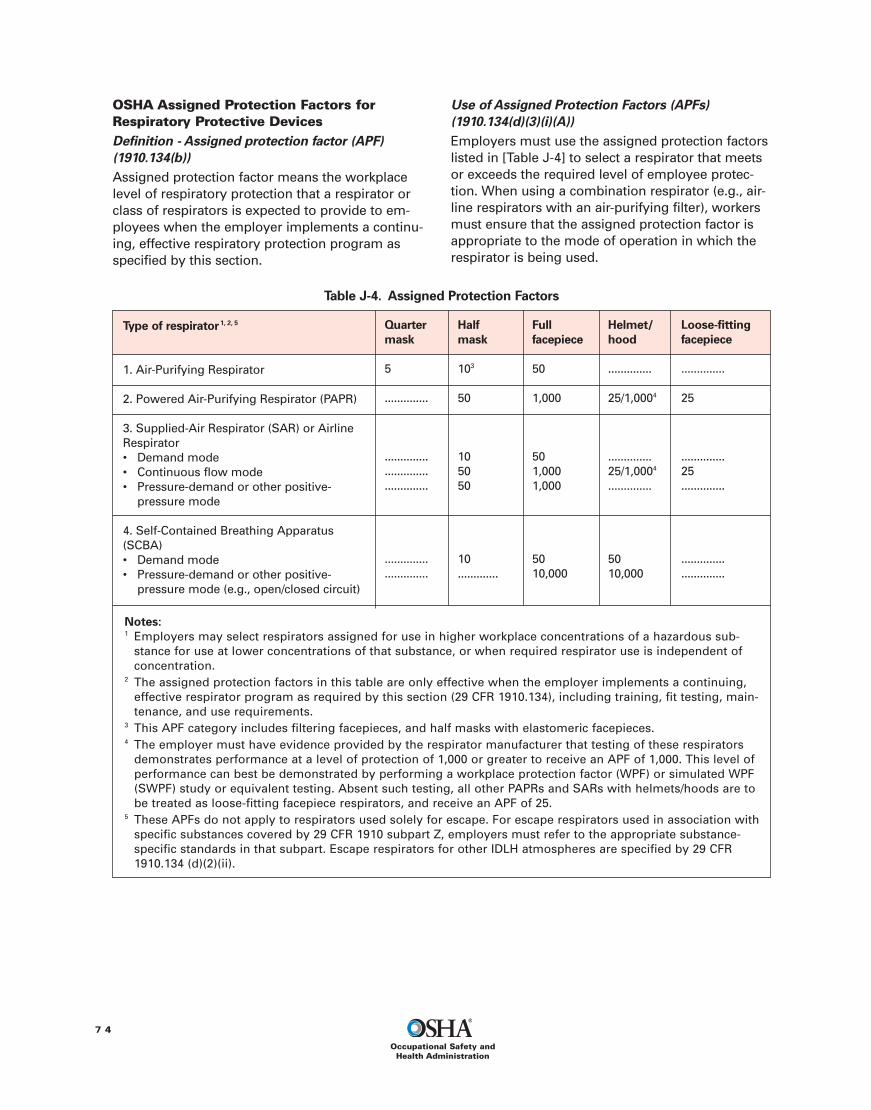
OSHA Assigned Protection Factors forRespiratory Protective DevicesDefinition - Assigned protection factor (APF)(1910.134(b))Assigned protection factor means the workplacelevel of respiratory protection that a respirator orclass of respirators is expected to provide to em-ployees when the employer implements a continu-ing, effective respiratory protection program asspecified by this section.
Use of Assigned Protection Factors (APFs)(1910.134(d)(3)(i)(A))Employers must use the assigned protection factorslisted in [Table J-4] to select a respirator that meetsor exceeds the required level of employee protec-tion. When using a combination respirator (e.g., air-line respirators with an air-purifying filter), workersmust ensure that the assigned protection factor isappropriate to the mode of operation in which therespirator is being used.
7 4
Occupational Safety andHealth Administration
Table J-4. Assigned Protection Factors
Type of respirator1, 2, 5
1. Air-Purifying Respirator
2. Powered Air-Purifying Respirator (PAPR)
3. Supplied-Air Respirator (SAR) or AirlineRespirator• Demand mode• Continuous flow mode• Pressure-demand or other positive-
pressure mode
4. Self-Contained Breathing Apparatus(SCBA)• Demand mode• Pressure-demand or other positive-
pressure mode (e.g., open/closed circuit)
Quartermask
5
..............
..............
..............
..............
..............
..............
Loose-fittingfacepiece
..............
25
..............25..............
..............
..............
Notes:1 Employers may select respirators assigned for use in higher workplace concentrations of a hazardous sub-
stance for use at lower concentrations of that substance, or when required respirator use is independent ofconcentration.
2 The assigned protection factors in this table are only effective when the employer implements a continuing,effective respirator program as required by this section (29 CFR 1910.134), including training, fit testing, main-tenance, and use requirements.
3 This APF category includes filtering facepieces, and half masks with elastomeric facepieces.4 The employer must have evidence provided by the respirator manufacturer that testing of these respirators
demonstrates performance at a level of protection of 1,000 or greater to receive an APF of 1,000. This level ofperformance can best be demonstrated by performing a workplace protection factor (WPF) or simulated WPF(SWPF) study or equivalent testing. Absent such testing, all other PAPRs and SARs with helmets/hoods are tobe treated as loose-fitting facepiece respirators, and receive an APF of 25.
5 These APFs do not apply to respirators used solely for escape. For escape respirators used in association withspecific substances covered by 29 CFR 1910 subpart Z, employers must refer to the appropriate substance-specific standards in that subpart. Escape respirators for other IDLH atmospheres are specified by 29 CFR1910.134 (d)(2)(ii).
Halfmask
103
50
105050
10.............
Fullfacepiece
50
1,000
501,0001,000
5010,000
Helmet/hood
..............
25/1,0004
..............25/1,0004
..............
5010,000

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7 5
Respirators for IDLH AtmospheresSelected Excerpts from 29 CFR 1910.134 – OSHA’sstandard on Respiratory Protection
Hazard Evaluation (1910.134(d)(1)(iii))The employer shall identify and evaluate the res-piratory hazard(s) in the workplace; this evalua-tion shall include a reasonable estimate ofemployee exposures to respiratory hazard(s)and an identification of the contaminant's chemi-cal state and physical form.Where the employercannot identify or reasonably estimate theemployee exposure, the employer shall considerthe atmosphere to be IDLH.
The employer shall select respirators from a suf-ficient number of respirator models and sizes sothat the respirator is acceptable to, and correctlyfits, the user. (1910.134(d)(1)(iv))
Respirators for IDLH atmospheres (1910.134(d)(2))The employer shall provide the following respi-rators for employee use in IDLH atmospheres:
A full facepiece pressure demand SCBA certifiedby NIOSH for a minimum service life of thirtyminutes, or
A combination full facepiece pressure demandsupplied-air respirator (SAR) with auxiliary self-contained air supply.
Respirators provided only for escape from IDLHatmospheres shall be NIOSH-certified for escapefrom the atmosphere in which they will be used.
All oxygen-deficient atmospheres shall be con-sidered IDLH. Exception: If the employer demon-strates that, under all foreseeable conditions, theoxygen concentration can be maintained withinthe ranges specified [inTable II of the standard],then any atmosphere-supplying respirator maybe used.
Respirators for Atmospheres that areNot IDLHRespirators for atmospheres that are not IDLH(1910.134(d)(2)).The employer shall provide a respirator that isadequate to protect the health of the employeeand ensure compliance with all other OSHAstatutory and regulatory requirements, underroutine and reasonably foreseeable emergencysituations.
Choosing APR Cartridges that Offer ProtectionAgainst a Wide Range of Contaminants
The combination of high efficiency (P-100) partic-ulate filters plus organic vapor (OV) cartridges inwhat has come to be known as “stacked car-tridges” will protect against many of the air-borne hazards that EMTs might encounter (e.g.,toxic dusts, biological agents, radioactive particu-lates, organophosphates and other pesticides,and solvents).33 Acid gas and amine cartridgesadd an additional level of protection from gaseswhich have been implicated in at least one caseof healthcare worker injury.34
33 For PAPRs the equivalent to a P-100 filter is the high efficiency(HE) filter.34 Despite the number of carbon monoxide victims treated at hos-pitals, it is not anticipated that EMS responders would benefitfrom specialty cartridges that remove carbon monoxide from air.There are no reported cases of healthcare workers being injuredthrough secondary contamination from victims of carbonmonoxide poisoning (Horton et al., 2003; Hick et al., 2003; Walteret al., 2003). If the source of carbon monoxide is producing anongoing release, appropriately trained responders equipped withSCBA will need to control the release and evacuate victims.

Appendix K
Thermal Stress: Working in Hot or ColdEnvironmentsHeat Stress and StrainEMS responders must work in a wide variety of hotor hot and humid environments. Comfort is not theonly issue in working in such environments. Workerswho are suddenly exposed to working in a hot envi-ronment face additional and generally avoidablehazards to their safety and health. Chemical protec-tive clothing can add an extra burden by reducingair circulation on the skin and limiting the body’snatural ability to cool itself as sweat evaporates.Extended use of respiratory protection can also hin-der a worker’s ability to replenish fluids by drinking,putting the worker at greater risk. The employershould provide detailed instructions on preventivemeasures and adequate protection necessary toprevent heat stress. Detailed guidance on preven-tive measures can be found in the following docu-ments.
NIOSH Publication No. 86-112 – Working in HotEnvironments provides basic general informationfor employers and employees on thermal stressfrom working in hot environments. Access this pub-lication at www.cdc.gov/niosh/hotenvt.html#protective
The problems of thermal stress and chemical pro-tective clothing are outlined in paragraph X of
OSHA’s Technical Manual, Section VII, Chapter 1 –Chemical Protective Clothingwww.osha.gov/dts/osta/otm/otm_viii/otm_viii_1.html
Cold Stress and HypothermiaDust EMS responders who assist patients duringincidents involving cold weather may be subject tocold exposure, which can affect performance andultimately lead to hyperthermia. Wet conditions(including sweat) and wind can exacerbate the situ-ation. Decontamination procedures often meangreater exposure to water and removal of clothesresulting in greater exposure to cold and wind.Effective alternate decontamination methods shouldbe considered in extremely cold climates.
The U.S. Army Technical Bulletin TB-MED 508 –Prevention and Management of Cold-weatherInjuries offers details on cold stress management.Section 3-2 provides guidance on avoidinghypothermia, while Section 3-6 offers suggestionsfor PPE use and decontamination in very coldweather. Although intended for military troops, theadvice (e.g., straps on the respirator mask must notbe too tight, as this will reduce blood flow to theskin of the face and can cause frostbite) applies toany worker wearing protective gear at extremelylow temperatures. www.usariem.army.mil/download/tbmed508.pdf
7 6
Occupational Safety andHealth Administration

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7 7
Appendix L
Decontamination Foam and Barrier CreamDecontamination foams have been the subject ofresearch by Sandia National Laboratories. Thesefoams are effective for use on equipment againstcertain biological and chemical contaminants.These products have been licensed for commercialproduction (EnviroFoam, 2008; Modec, 2008). Thefoams have not been approved for use on humanskin.
For certain weapons of chemical, biological, radi-ological, nuclear, or explosive (CBRNE) contami-nants (nerve and blister agents, specifically),Reactive Skin Decontamination Lotion (RSDL) offerssome benefit but has some inherent risk. The FDAhas approved this lotion for use on human skin.According to the product distributor, the U.S. mili-tary is conducting efficacy testing and recently
began permitting local police, fire departments,emergency medical teams, and the other organiza-tions to use the lotion (E-Z-EM, 2006).
Another product under development by the mili-tary, Skin Exposure Reduction Paste AgainstChemical Warfare Agents (SERPACWA), is alsointended for use on human skin (Ellen, 2003). Thisproduct functions as a barrier cream when appliedbefore any opportunity for exposure occurs. Thecream is intended to protect military personnel fromadverse effects if a small amount of contaminantpenetrates through “hastily donned full-body pro-tective gear.” It is hoped that a related product(active topical skin protectant), also under develop-ment, will offer greater protection. Neither of theseproducts is FDA approved.
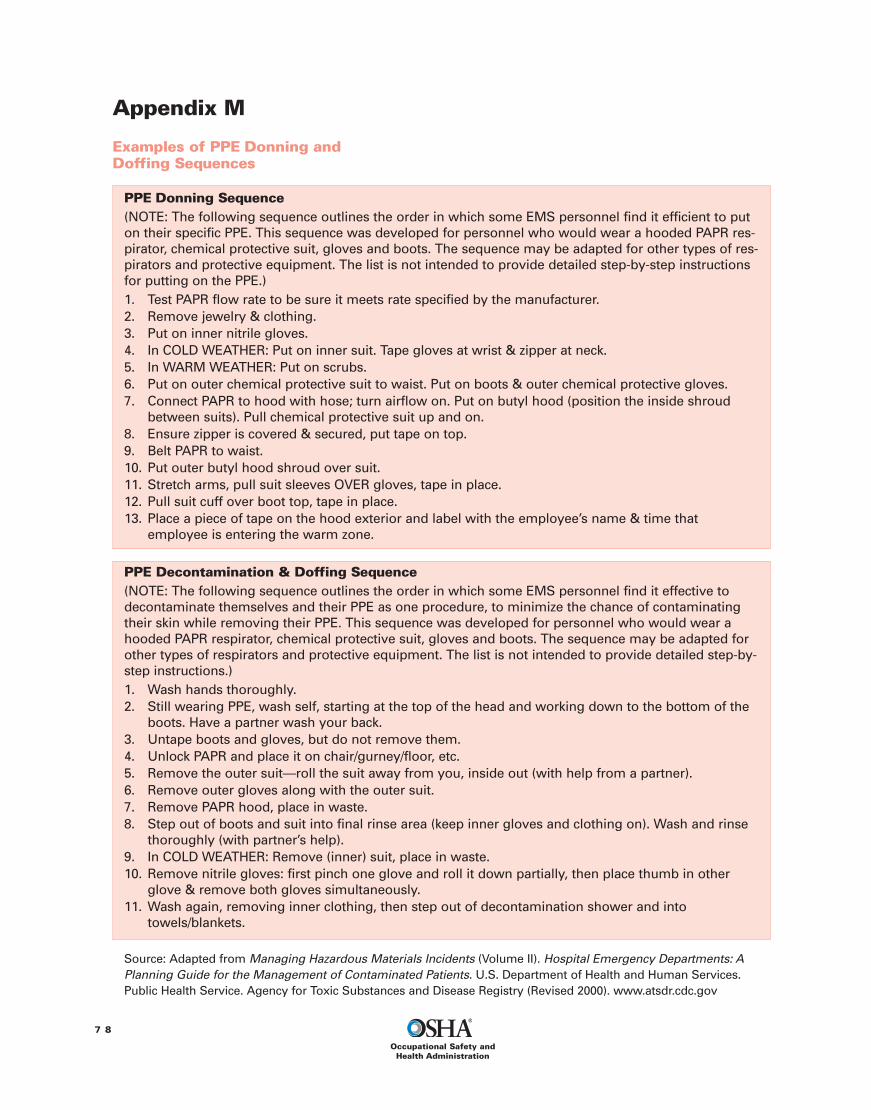
Appendix M
Examples of PPE Donning andDoffing Sequences
7 8
Occupational Safety andHealth Administration
PPE Donning Sequence(NOTE: The following sequence outlines the order in which some EMS personnel find it efficient to puton their specific PPE. This sequence was developed for personnel who would wear a hooded PAPR res-pirator, chemical protective suit, gloves and boots. The sequence may be adapted for other types of res-pirators and protective equipment. The list is not intended to provide detailed step-by-step instructionsfor putting on the PPE.)1. Test PAPR flow rate to be sure it meets rate specified by the manufacturer.2. Remove jewelry & clothing.3. Put on inner nitrile gloves.4. In COLD WEATHER: Put on inner suit. Tape gloves at wrist & zipper at neck.5. In WARM WEATHER: Put on scrubs.6. Put on outer chemical protective suit to waist. Put on boots & outer chemical protective gloves.7. Connect PAPR to hood with hose; turn airflow on. Put on butyl hood (position the inside shroud
between suits). Pull chemical protective suit up and on.8. Ensure zipper is covered & secured, put tape on top.9. Belt PAPR to waist.10. Put outer butyl hood shroud over suit.11. Stretch arms, pull suit sleeves OVER gloves, tape in place.12. Pull suit cuff over boot top, tape in place.13. Place a piece of tape on the hood exterior and label with the employee’s name & time that
employee is entering the warm zone.
PPE Decontamination & Doffing Sequence(NOTE: The following sequence outlines the order in which some EMS personnel find it effective todecontaminate themselves and their PPE as one procedure, to minimize the chance of contaminatingtheir skin while removing their PPE. This sequence was developed for personnel who would wear ahooded PAPR respirator, chemical protective suit, gloves and boots. The sequence may be adapted forother types of respirators and protective equipment. The list is not intended to provide detailed step-by-step instructions.)1. Wash hands thoroughly.2. Still wearing PPE, wash self, starting at the top of the head and working down to the bottom of the
boots. Have a partner wash your back.3. Untape boots and gloves, but do not remove them.4. Unlock PAPR and place it on chair/gurney/floor, etc.5. Remove the outer suit—roll the suit away from you, inside out (with help from a partner).6. Remove outer gloves along with the outer suit.7. Remove PAPR hood, place in waste.8. Step out of boots and suit into final rinse area (keep inner gloves and clothing on). Wash and rinse
thoroughly (with partner’s help).9. In COLD WEATHER: Remove (inner) suit, place in waste.10. Remove nitrile gloves: first pinch one glove and roll it down partially, then place thumb in other
glove & remove both gloves simultaneously.11. Wash again, removing inner clothing, then step out of decontamination shower and into
towels/blankets.
Source: Adapted from Managing Hazardous Materials Incidents (Volume II). Hospital Emergency Departments: APlanning Guide for the Management of Contaminated Patients. U.S. Department of Health and Human Services.Public Health Service. Agency for Toxic Substances and Disease Registry (Revised 2000). www.atsdr.cdc.gov

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 7 9
Appendix N
General Description and Discussion of theLevels of Protection and Protective GearThis appendix, taken from Appendix B of OSHA’sHAZWOPER standard (29 CFR 1910.120) and adapt-ed with additional information from Appendix C ofATSDR (2001), sets forth information about personalprotective equipment (PPE) protection levels thatmay be used to assist employers in complying withthe PPE requirements of the HAZWOPER standard.
As required by the HAZWOPER standard, PPEmust be selected which will protect employeesfrom the specific hazards which they are likely toencounter during their work.
Selection of the appropriate PPE is a complexprocess which should take into consideration a vari-ety of factors. Key factors involved in this processare identification of the hazards, or suspected haz-ards; the routes by which employees could beexposed to the potential hazard (inhalation, skinabsorption, ingestion, and eye or skin contact); andthe performance of the PPE materials (and seams)in providing a barrier to these hazards. The amountof protection provided by PPE is material- and haz-ard-specific. That is, protective equipment materialswill protect well against some hazardous sub-stances and poorly, or not at all, against others. Inmany instances, protective equipment materialscannot be found which will provide continuous pro-tection from the particular hazardous substance. Inthese cases, the PPE must be changed or work muststop before breakthrough time is reached (55 FR14074, Apr. 13, 1990).
Other factors in this selection process to be con-sidered are matching the PPE to the employee's
work requirements and task-specific conditions. Thedurability of PPE materials, such as tear strengthand seam strength, should be considered in relationto the employee's tasks. The effects of PPE in rela-tion to heat stress and task duration are a factor inselecting and using PPE. In some cases layers ofPPE may be necessary to provide sufficient protec-tion, or to protect expensive PPE inner garments,suits, or equipment.
The more that is known about the hazards at thesite, the easier the job of PPE selection becomes. Asmore information about the hazards and conditionsat the site becomes available, the site supervisorcan make decisions to upgrade or downgrade thelevel of PPE to match the tasks at hand.
The following are guidelines which an employercan use to begin the selection of the appropriatePPE. As noted above, the site information may sug-gest the use of combinations of PPE selected fromthe different protection levels (i.e., A, B, C, or D) asbeing more suitable to the hazards of the work. Itshould be cautioned that the listing below does notfully address the performance of the specific PPEmaterial in relation to the specific hazards at the jobsite, and that PPE selection, evaluation and reselec-tion is an ongoing process as sufficient informationabout the hazards and PPE performance is obtained.
Personal protective equipment is divided intofour categories based on the degree of protectionafforded. Table N-1 presents the recommendedequipment, suggestions for when it should be used,and limiting criteria associated with this level ofPPE.
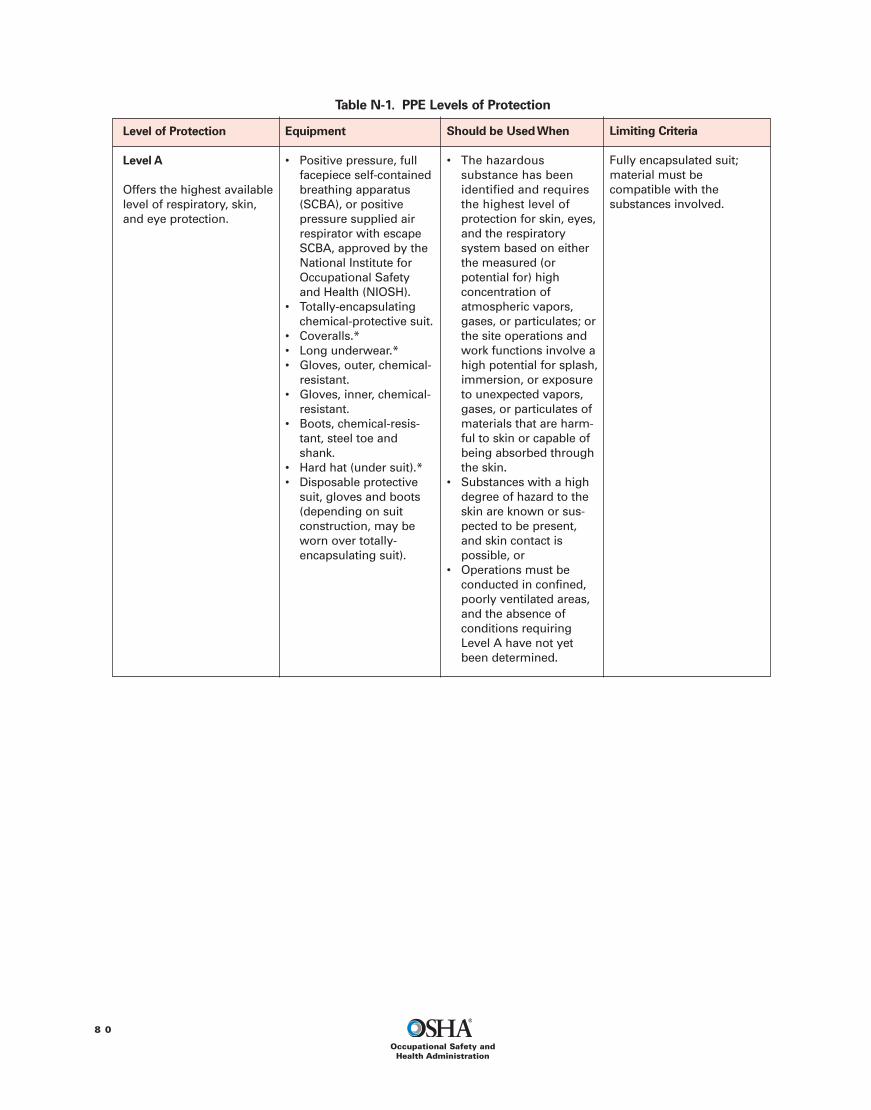
8 0
Occupational Safety andHealth Administration
Table N-1. PPE Levels of Protection
Level of Protection
Level A
Offers the highest availablelevel of respiratory, skin,and eye protection.
Equipment
• Positive pressure, fullfacepiece self-containedbreathing apparatus(SCBA), or positivepressure supplied airrespirator with escapeSCBA, approved by theNational Institute forOccupational Safetyand Health (NIOSH).
• Totally-encapsulatingchemical-protective suit.
• Coveralls.*• Long underwear.*• Gloves, outer, chemical-
resistant.• Gloves, inner, chemical-
resistant.• Boots, chemical-resis-
tant, steel toe andshank.
• Hard hat (under suit).*• Disposable protective
suit, gloves and boots(depending on suitconstruction, may beworn over totally-encapsulating suit).
Should be UsedWhen
• The hazardoussubstance has beenidentified and requiresthe highest level ofprotection for skin, eyes,and the respiratorysystem based on eitherthe measured (orpotential for) highconcentration ofatmospheric vapors,gases, or particulates; orthe site operations andwork functions involve ahigh potential for splash,immersion, or exposureto unexpected vapors,gases, or particulates ofmaterials that are harm-ful to skin or capable ofbeing absorbed throughthe skin.
• Substances with a highdegree of hazard to theskin are known or sus-pected to be present,and skin contact ispossible, or
• Operations must beconducted in confined,poorly ventilated areas,and the absence ofconditions requiringLevel A have not yetbeen determined.
Limiting Criteria
Fully encapsulated suit;material must becompatible with thesubstances involved.
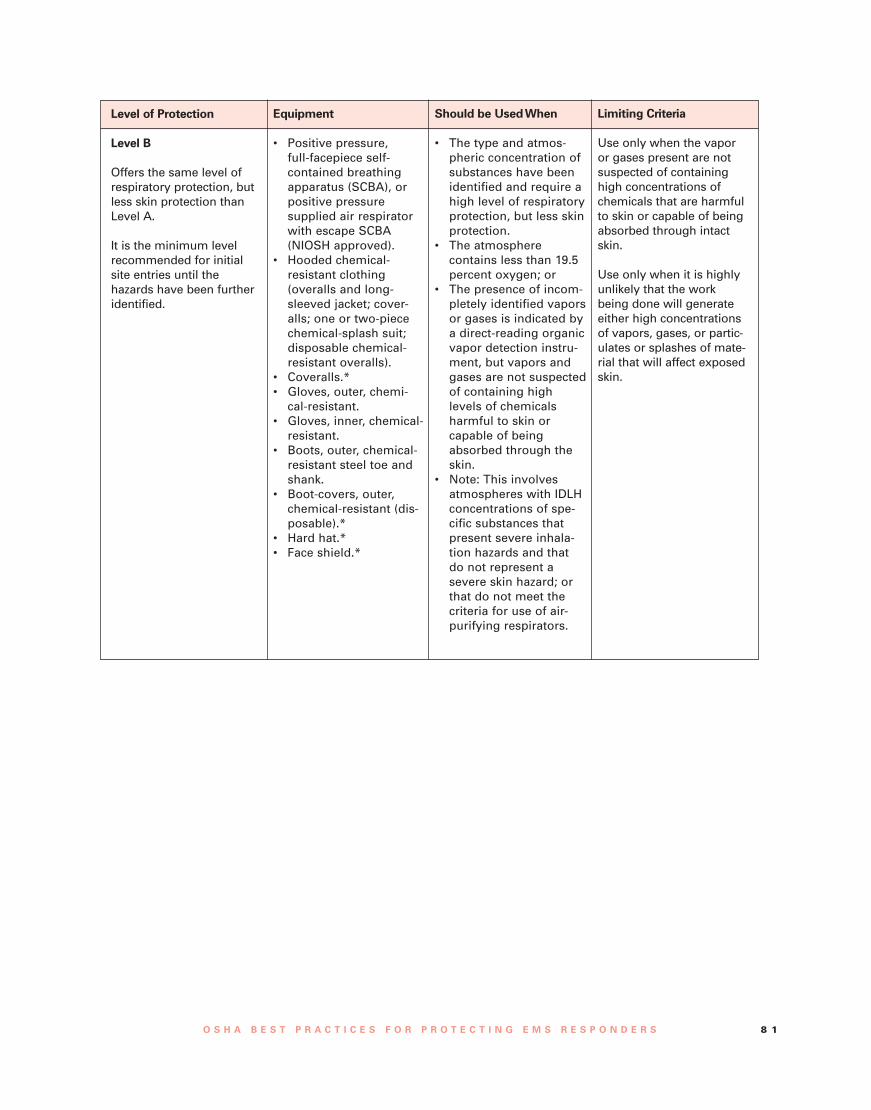
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 8 1
Level of Protection
Level B
Offers the same level ofrespiratory protection, butless skin protection thanLevel A.
It is the minimum levelrecommended for initialsite entries until thehazards have been furtheridentified.
Equipment
• Positive pressure,full-facepiece self-contained breathingapparatus (SCBA), orpositive pressuresupplied air respiratorwith escape SCBA(NIOSH approved).
• Hooded chemical-resistant clothing(overalls and long-sleeved jacket; cover-alls; one or two-piecechemical-splash suit;disposable chemical-resistant overalls).
• Coveralls.*• Gloves, outer, chemi-
cal-resistant.• Gloves, inner, chemical-
resistant.• Boots, outer, chemical-
resistant steel toe andshank.
• Boot-covers, outer,chemical-resistant (dis-posable).*
• Hard hat.*• Face shield.*
Should be UsedWhen
• The type and atmos-pheric concentration ofsubstances have beenidentified and require ahigh level of respiratoryprotection, but less skinprotection.
• The atmospherecontains less than 19.5percent oxygen; or
• The presence of incom-pletely identified vaporsor gases is indicated bya direct-reading organicvapor detection instru-ment, but vapors andgases are not suspectedof containing highlevels of chemicalsharmful to skin orcapable of beingabsorbed through theskin.
• Note: This involvesatmospheres with IDLHconcentrations of spe-cific substances thatpresent severe inhala-tion hazards and thatdo not represent asevere skin hazard; orthat do not meet thecriteria for use of air-purifying respirators.
Limiting Criteria
Use only when the vaporor gases present are notsuspected of containinghigh concentrations ofchemicals that are harmfulto skin or capable of beingabsorbed through intactskin.
Use only when it is highlyunlikely that the workbeing done will generateeither high concentrationsof vapors, gases, or partic-ulates or splashes of mate-rial that will affect exposedskin.
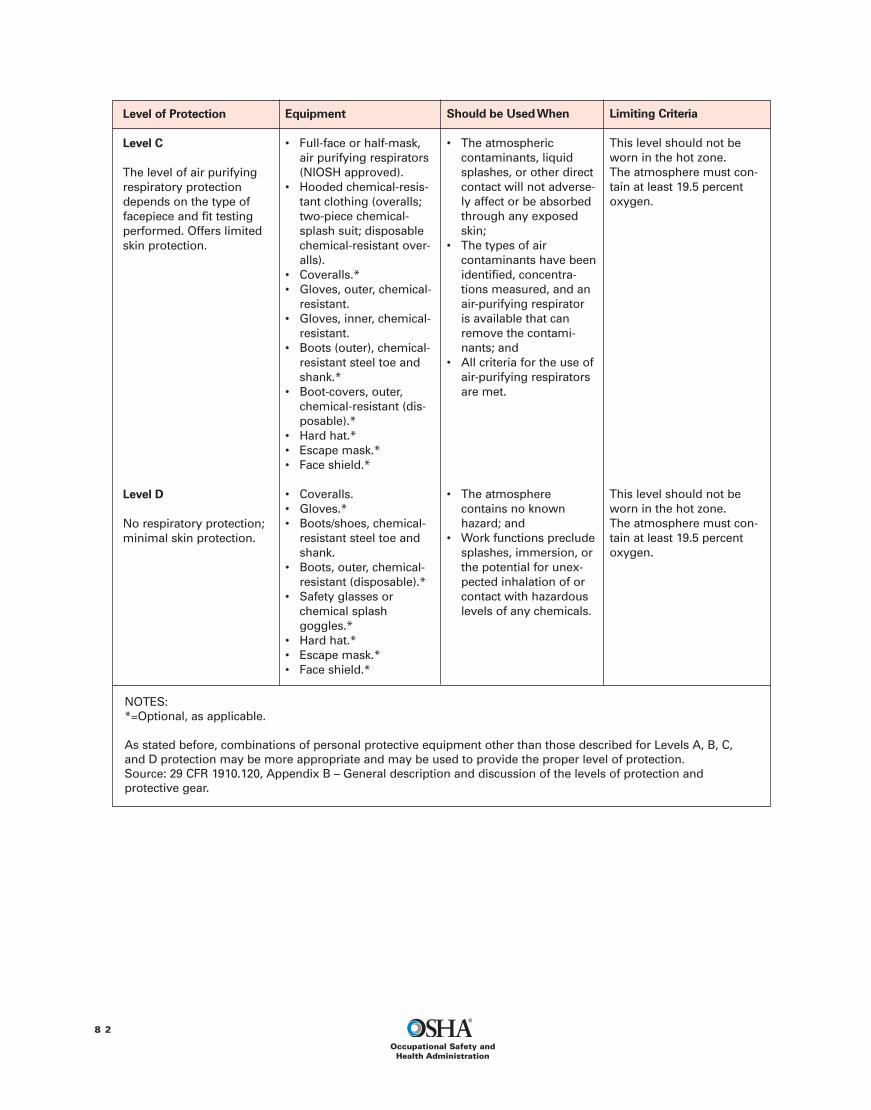
8 2
Occupational Safety andHealth Administration
Level of Protection
Level C
The level of air purifyingrespiratory protectiondepends on the type offacepiece and fit testingperformed. Offers limitedskin protection.
Level D
No respiratory protection;minimal skin protection.
Equipment
• Full-face or half-mask,air purifying respirators(NIOSH approved).
• Hooded chemical-resis-tant clothing (overalls;two-piece chemical-splash suit; disposablechemical-resistant over-alls).
• Coveralls.*• Gloves, outer, chemical-
resistant.• Gloves, inner, chemical-
resistant.• Boots (outer), chemical-
resistant steel toe andshank.*
• Boot-covers, outer,chemical-resistant (dis-posable).*
• Hard hat.*• Escape mask.*• Face shield.*
• Coveralls.• Gloves.*• Boots/shoes, chemical-
resistant steel toe andshank.
• Boots, outer, chemical-resistant (disposable).*
• Safety glasses orchemical splashgoggles.*
• Hard hat.*• Escape mask.*• Face shield.*
Should be UsedWhen
• The atmosphericcontaminants, liquidsplashes, or other directcontact will not adverse-ly affect or be absorbedthrough any exposedskin;
• The types of aircontaminants have beenidentified, concentra-tions measured, and anair-purifying respiratoris available that canremove the contami-nants; and
• All criteria for the use ofair-purifying respiratorsare met.
• The atmospherecontains no knownhazard; and
• Work functions precludesplashes, immersion, orthe potential for unex-pected inhalation of orcontact with hazardouslevels of any chemicals.
Limiting Criteria
This level should not beworn in the hot zone.The atmosphere must con-tain at least 19.5 percentoxygen.
This level should not beworn in the hot zone.The atmosphere must con-tain at least 19.5 percentoxygen.
NOTES:*=Optional, as applicable.
As stated before, combinations of personal protective equipment other than those described for Levels A, B, C,and D protection may be more appropriate and may be used to provide the proper level of protection.Source: 29 CFR 1910.120, Appendix B – General description and discussion of the levels of protection andprotective gear.

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 8 3
Appendix O
Occupational Health Hazard Experienceof EMS RespondersBackground/OverviewEmployers’ decisions regarding worker protectionmust begin with an evaluation of the hazards towhich workers might be exposed. A review of theliterature shows that EMS responders are subject tomany of the same occupational safety and healthhazards as are workers in other transportation,medical, and public service occupations. EMSresponders are subject to hazardous substanceexposures as well as numerous other hazards,including back injuries, automobile crashes, assault,stress, bloodborne pathogens, and injuries to theextremities, eyes, and ears.
Review of the Literature on Risks toEMS RespondersExperience of EMS Responders Exposed toHazardous SubstancesEMS responders routinely respond to sites wherehazardous substance releases have occurred. Theresponders can become exposed to hazardous sub-stances when they provide medical treatment atthese sites or at locations where contaminated per-sons, equipment, or vehicles have been moved afterthe release. Although most studies of hazardoussubstance exposure only looked at the broadergroup of emergency service providers (includingvarious combinations of firefighters, police, EMTs,HAZMAT teams, and in some cases emergencyroom personnel), several reports provided detailedinformation specific to EMS responders.35 OSHA hassummarized those reports in the following section.
EMTs at theTokyo Subway Sarin Gas AttacksThe experience of EMTs was specifically document-ed for the Tokyo subway sarin gas attacks of 1995.In that disaster, officials dispatched 1,364 EMTs and131 ambulances (plus some minivans) to 15 affect-ed subway stations, from which they transported688 of the 4,000 victims who eventually were seenat area hospitals. A review of incident records indi-cated that 135 (9.9%) of the EMTs showed acutesymptoms and received medical treatment at hospi-tals.36 The authors did not indicate whether EMTs
entered the contaminated subway areas, but indi-cated that they did assist contaminated victims.Most of the affected EMTs “started having symp-toms during transportation, and it is suspected thatthey were exposed in ambulances to the vaporizedsarin from victims’ clothes.” (Okumura et al., 1998).The EMTs “wore standard work clothing without res-piratory protection” and “ventilation in ambulancesand minivans at first was poor” because windowswere closed, although these were later opened toimprove the ventilation in transport vehicles.37
Okumura et al. (1998) note that it is important toconsider several additional factors when evaluatingthe experience of EMTs during this disaster, includ-ing the lack of proper patient decontamination, theduties performed by EMTs in Japan, and the ratio ofvictims that arrived at the hospital via ambulancecompared to other forms of transportation. Theseadditional factors are described in more detail here:• Lack of decontamination: Little or no effort was
made to decontaminate victims before transport-ing them (Okumura et al., 1998). If performed,these types of decontamination activities mighthave significantly reduced victim exposure lev-els, particularly because many victims experi-enced continued exposure while they waited incrowded, enclosed rooms before being treated athospitals. While earlier efforts to decontaminatethe victims would likely have reduced EMT expo-sures during victim transport, the act of deconta-mination might have contributed to the exposureof EMTs who assisted victims with washing andundressing. Sarin off-gassing from abandonedcontaminated clothing could also have continuedto present a source of exposure to EMTs in thearea. EMTs would have required additional pre-cautions to operate safely.
• EMT duties: Okumura et al. (2004) point outthat “Under Japanese law, only physicians areallowed to perform endotracheal intubation andadminister medications to victims of a chemicalattack at the site of the incident.” In Japan, emer-gency response physicians can be dispatched forthis purpose (in contrast, EMS personnel in theU.S. are often authorized to perform intubation).Hick et al. (2003) also reviewed the literaturedescribing this incident and noted that the health-care employees most affected were several35 Historically, “general-population sources [of injury and illness
data] contain information on police and firefighters, but EMS per-sonnel are not typically broken out.” (Houser et al., 2004).36 The authors did not elaborate on the symptoms, but imply thatthe acute symptoms were considered possible effects of sarinexposure.
37 An important consideration for those planning EMS responderprotection is that “even in the absence of risk, the perceived riskwithout PPE can lead to symptoms and compromise workflow.”Hick (2007).

8 4
Occupational Safety andHealth Administration
physicians who spent up to 40 minutes attempt-ing to resuscitate the initial victims of the inci-dent. As might be expected, the medical person-nel most affected provided treatment involvingextended close contact with the most critically illvictims – who were also likely to have been themost highly exposed and perhaps the most high-ly contaminated.
• Victim transportation to the hospital: Recordsfrom one Tokyo hospital indicate that, while thegreatest number of victims arrived by foot, thepercentage who arrived by taxi (24 percent of allvictims arriving at that hospital) was more thanthree times the number transported by ambu-lance (7 percent). Another 13 percent arrived byprivate vehicles (Okumura et al., 1998). Althoughit might be assumed that the most severely ex-posed and affected victims were transported byambulance, two of the three reported cardiacarrest cases were transported by private vehiclesthat happened to be passing the subway stationshortly after the incident (Okumura et al., 1998).Although victims were triaged at the subway sta-tions, some victims worsened during transport,suggesting greater or continuing exposures. Thissuggests that if more victims had been transport-ed by ambulance, more EMTs might have experi-enced the effects of exposure. A follow-up evalu-ation of rescue team members and police officers,made 2 to 3 years after they had been exposed tosarin in the Tokyo incident, suggested a decline inmemory function independent of traumatic stresssymptoms. The authors were not able to deter-mine whether the effect was due to direct neuro-toxicity of sarin (Nishiwaki et al., 2001).
Hazardous Substances Emergency EventsSurveillance (HSEES) Data for EMS RespondersHorton et al. (2003 and 2008) and ATSDR (2004 and2007) reported on the experience of EMTs respond-ing to events recorded in the Hazardous SubstancesEmergency Events Surveillance (HSEES) system.38
For the purposes of this database, a hazardous sub-stance was any substance (i.e., chemical, biological,or radiological) that could reasonably be expectedto cause an adverse health effect. Events involving
only petroleum are excluded by HSEES. Hazardoussubstance emergency events were defined as “actu-al, uncontrolled, or illegal releases of a hazardoussubstance(s) that had to be removed, cleaned up, orneutralized according to federal, state, or local law.”Victims of such events were defined as “personssustaining at least one injury or symptom (i.e., res-piratory irritation) or death as a result of the event.”
The HSEES data for seven years from 1995through 2001 show that EMTs constituted one-halfof one percent (0.5 percent) of all reported victimsof hazardous substance emergency events (13,173total victims from more than 44,000 events) record-ed during this period. Altogether, 72 EMT injurieswere reported.39 The 13,173 total victims also includ-ed 190 volunteer firefighters, 273 career firefighters,437 police officers, and 32 hospital personnel, indi-cating that first responders (of all types) accountedfor a notable number victims injured during report-ed events of this period (Horton et al., 2003).
A subsequent report reviewed the frequencywith which medical treatment and decontaminationwere provided during HSEES events. These HSEESdata indicate that medical treatment (first aid) wasprovided (presumably by EMS responders in mostcases) for 262 injuries sustained by individuals athazardous substance release sites in the year 2004(ATSDR, 2004). Figure O-1, reprinted from ATSDR(2004), contrasts this value to the 1,039 hazardoussubstance release site injuries treated in hospitals.These figures suggest that EMS responders arebeing called to some scenes to treat patients, butthat the vast majority of victims injured in haz-ardous substance release events are being trans-ported or otherwise finding their way to hospitalsfor treatment (in some cases, possibly in addition totreatment at the scene).
Decontamination is performed infrequently, butis somewhat more likely to occur at the scene of therelease than at medical facilities. “Of the 1,766(96.0%) victims [in 2004 for whom decontaminationstatus was reported to HSEES], 1,483 (84.0%) werenot decontaminated, 157 (8.9%) were decontaminat-ed at the scenes, 101 (5.7%) were decontaminatedat medical facilities, and 25 (1.4%) were decontami-nated at both the scenes and medical facilities.”(ATSDR, 2004).
Victims who were decontaminated in 2004 werenot necessarily injured. “For events in which unin-jured persons were decontaminated, the mediannumber of uninjured decontaminated individuals
38 The HSEES system data were collected by the Agency for ToxicSubstances and Disease Registry (ATSDR). The 16 reportingstates included (grouped by geographical area): Alabama,Mississippi, Texas, Iowa, Missouri, Minnesota, Wisconsin, NewYork, New Jersey, Rhode Island, New Hampshire, North Carolina,Colorado, Oregon, Washington, and Utah (Horton et al., 2003;Berkowitz et al., 2004). Two additional states, Florida andMichigan, began reporting in 2006 (Horton et al., 2008). Not allstates participated for the full period.
39 Horton et al. (2003) reported that 3,453 of these approximately44,000 events involved injured victims; however, the total num-ber of EMTs responding to these events is not known.
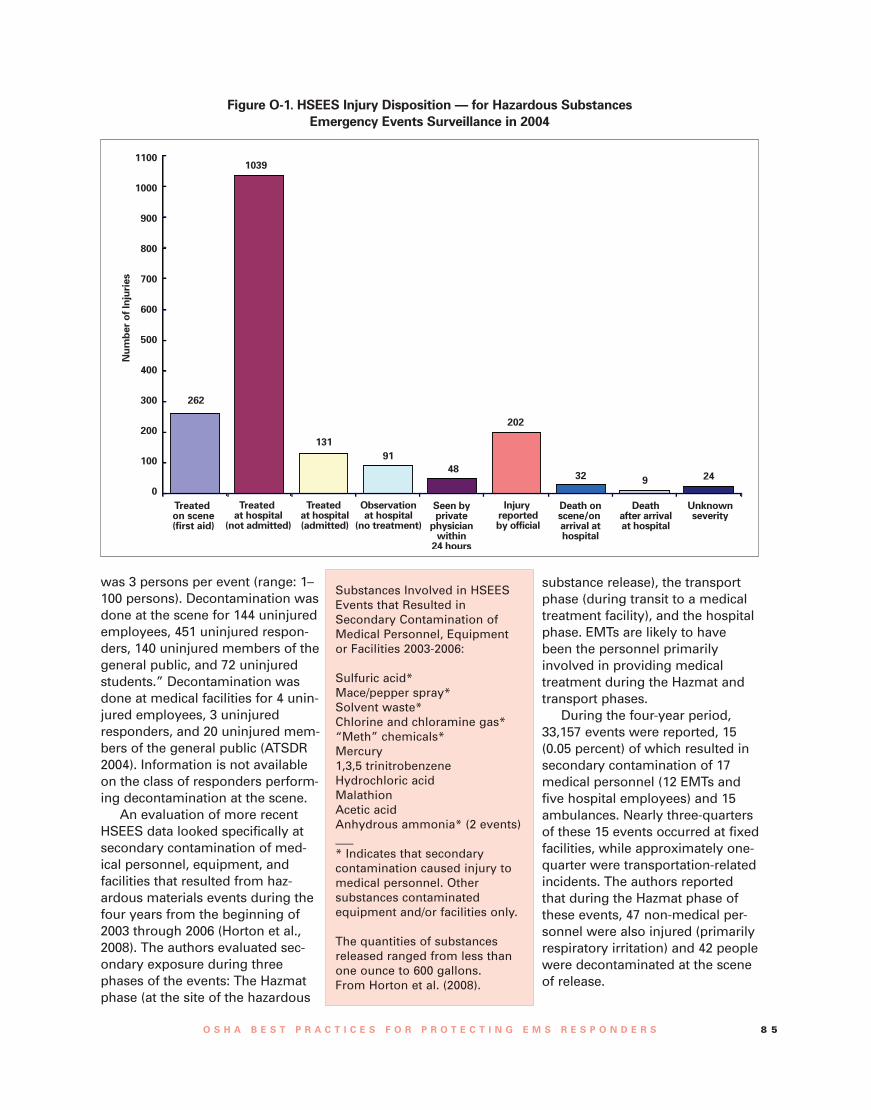
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 8 5
was 3 persons per event (range: 1–100 persons). Decontamination wasdone at the scene for 144 uninjuredemployees, 451 uninjured respon-ders, 140 uninjured members of thegeneral public, and 72 uninjuredstudents.” Decontamination wasdone at medical facilities for 4 unin-jured employees, 3 uninjuredresponders, and 20 uninjured mem-bers of the general public (ATSDR2004). Information is not availableon the class of responders perform-ing decontamination at the scene.
An evaluation of more recentHSEES data looked specifically atsecondary contamination of med-ical personnel, equipment, andfacilities that resulted from haz-ardous materials events during thefour years from the beginning of2003 through 2006 (Horton et al.,2008). The authors evaluated sec-ondary exposure during threephases of the events: The Hazmatphase (at the site of the hazardous
substance release), the transportphase (during transit to a medicaltreatment facility), and the hospitalphase. EMTs are likely to havebeen the personnel primarilyinvolved in providing medicaltreatment during the Hazmat andtransport phases.
During the four-year period,33,157 events were reported, 15(0.05 percent) of which resulted insecondary contamination of 17medical personnel (12 EMTs andfive hospital employees) and 15ambulances. Nearly three-quartersof these 15 events occurred at fixedfacilities, while approximately one-quarter were transportation-relatedincidents. The authors reportedthat during the Hazmat phase ofthese events, 47 non-medical per-sonnel were also injured (primarilyrespiratory irritation) and 42 peoplewere decontaminated at the sceneof release.
Figure O-1. HSEES Injury Disposition — for Hazardous SubstancesEmergency Events Surveillance in 2004
Substances Involved in HSEESEvents that Resulted inSecondary Contamination ofMedical Personnel, Equipmentor Facilities 2003-2006:
Sulfuric acid*Mace/pepper spray*Solvent waste*Chlorine and chloramine gas*“Meth” chemicals*Mercury1,3,5 trinitrobenzeneHydrochloric acidMalathionAcetic acidAnhydrous ammonia* (2 events)___* Indicates that secondarycontamination caused injury tomedical personnel. Othersubstances contaminatedequipment and/or facilities only.
The quantities of substancesreleased ranged from less thanone ounce to 600 gallons.From Horton et al. (2008).
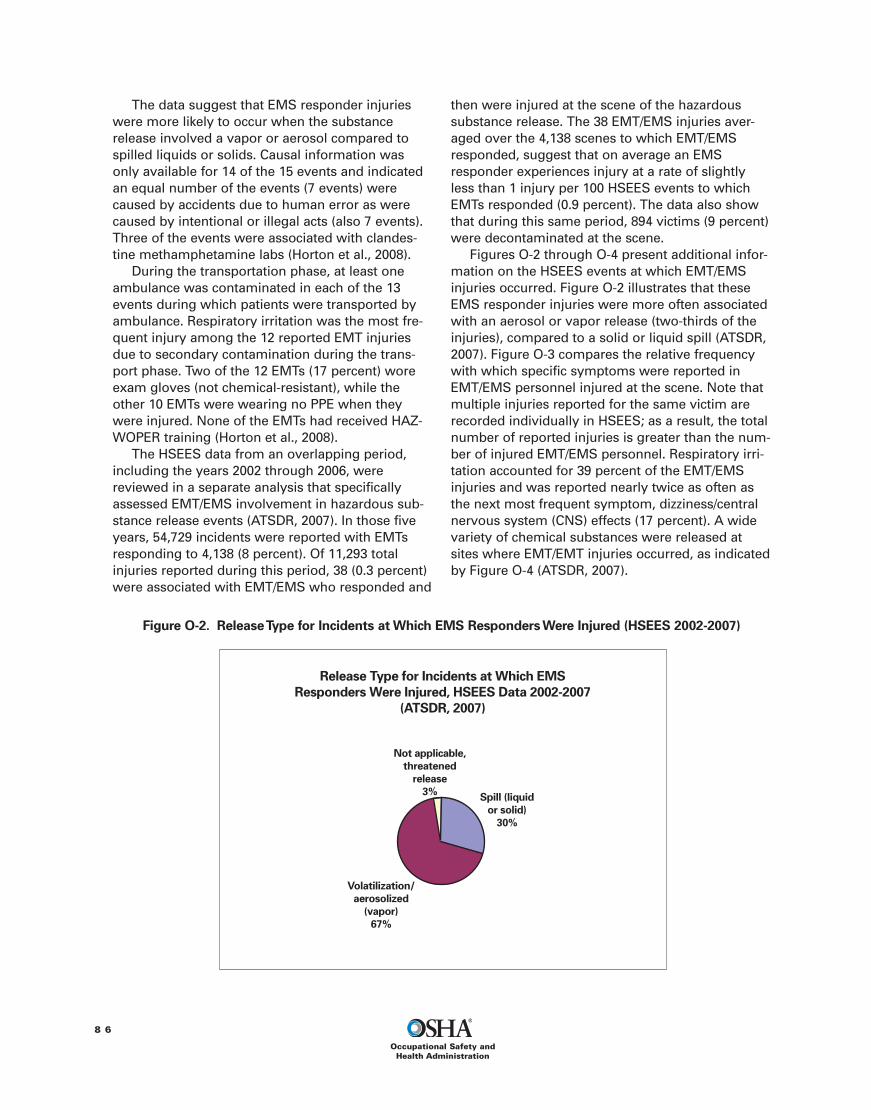
8 6
Occupational Safety andHealth Administration
The data suggest that EMS responder injurieswere more likely to occur when the substancerelease involved a vapor or aerosol compared tospilled liquids or solids. Causal information wasonly available for 14 of the 15 events and indicatedan equal number of the events (7 events) werecaused by accidents due to human error as werecaused by intentional or illegal acts (also 7 events).Three of the events were associated with clandes-tine methamphetamine labs (Horton et al., 2008).
During the transportation phase, at least oneambulance was contaminated in each of the 13events during which patients were transported byambulance. Respiratory irritation was the most fre-quent injury among the 12 reported EMT injuriesdue to secondary contamination during the trans-port phase. Two of the 12 EMTs (17 percent) woreexam gloves (not chemical-resistant), while theother 10 EMTs were wearing no PPE when theywere injured. None of the EMTs had received HAZ-WOPER training (Horton et al., 2008).
The HSEES data from an overlapping period,including the years 2002 through 2006, werereviewed in a separate analysis that specificallyassessed EMT/EMS involvement in hazardous sub-stance release events (ATSDR, 2007). In those fiveyears, 54,729 incidents were reported with EMTsresponding to 4,138 (8 percent). Of 11,293 totalinjuries reported during this period, 38 (0.3 percent)were associated with EMT/EMS who responded and
then were injured at the scene of the hazardoussubstance release. The 38 EMT/EMS injuries aver-aged over the 4,138 scenes to which EMT/EMSresponded, suggest that on average an EMSresponder experiences injury at a rate of slightlyless than 1 injury per 100 HSEES events to whichEMTs responded (0.9 percent). The data also showthat during this same period, 894 victims (9 percent)were decontaminated at the scene.
Figures O-2 through O-4 present additional infor-mation on the HSEES events at which EMT/EMSinjuries occurred. Figure O-2 illustrates that theseEMS responder injuries were more often associatedwith an aerosol or vapor release (two-thirds of theinjuries), compared to a solid or liquid spill (ATSDR,2007). Figure O-3 compares the relative frequencywith which specific symptoms were reported inEMT/EMS personnel injured at the scene. Note thatmultiple injuries reported for the same victim arerecorded individually in HSEES; as a result, the totalnumber of reported injuries is greater than the num-ber of injured EMT/EMS personnel. Respiratory irri-tation accounted for 39 percent of the EMT/EMSinjuries and was reported nearly twice as often asthe next most frequent symptom, dizziness/centralnervous system (CNS) effects (17 percent). A widevariety of chemical substances were released atsites where EMT/EMT injuries occurred, as indicatedby Figure O-4 (ATSDR, 2007).
Figure O-2. ReleaseType for Incidents at Which EMS RespondersWere Injured (HSEES 2002-2007)
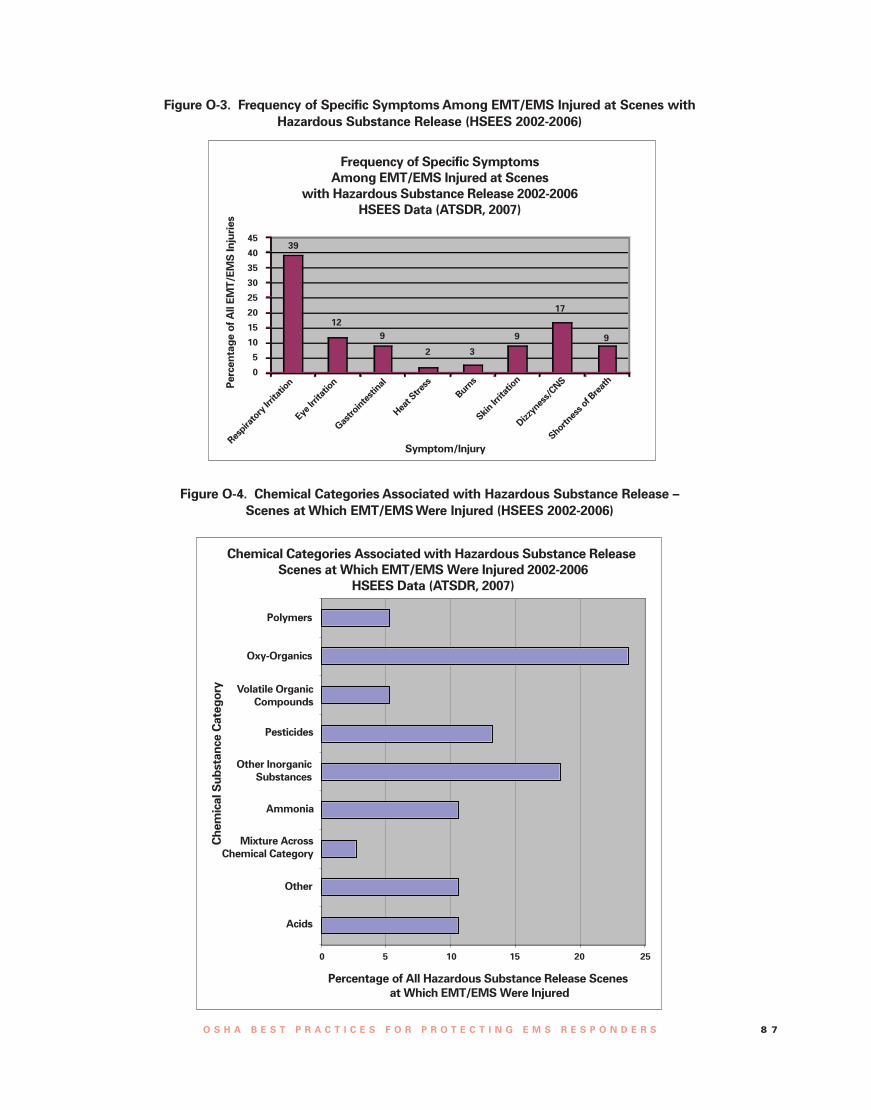
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 8 7
Figure O-3. Frequency of Specific Symptoms Among EMT/EMS Injured at Scenes withHazardous Substance Release (HSEES 2002-2006)
Figure O-4. Chemical Categories Associated with Hazardous Substance Release –Scenes at Which EMT/EMSWere Injured (HSEES 2002-2006)
39
129
2 3
9
17
9
0 5 10 15 20 25

8 8
Occupational Safety andHealth Administration
Other Reports of EMS Responder Injury duringHazardous Substance ReleasesThe published literature contains several other reportsof hazardous substance effects on EMS personnelresponding to clandestine drug laboratories, acts ofterrorism, and transportation incidents in the U.S.
Response to clandestine methamphetamine lab-oratories presents an increasing source of haz-ardous substance exposure, injuries, and illnessesto EMS responders in jurisdictions where these labsare prevalent. “Substances used in the metham-phetamine laboratories are often corrosive, explo-sive, flammable, and toxic and can cause fires,explosions, and other uncontrolled reactions.”(MMWR, November 17, 2000). The results aredevastating to laboratory occupants, emergencyresponders, and the local public.
Berkowitz et al. (2004) analyzed HSEES databetween 1993 and 2000 and found that the ninereports of EMS responders injured during haz-ardous substance release events all occurred innon-rural areas. This trend is in contrast to the find-ing that emergency responders in general (and vol-unteer firefighters in particular) were three timesmore likely to be injured in rural/agricultural areasthan in other areas. The report continues:
“Of note was the large proportion of victimswho were responders, mainly police officersand EMTs, in the events involving drug labora-tories. More than half of these events involvedfire and/or explosion, and almost all injuredpolice officers and EMTs did not wear personalprotective clothes.These circumstances indi-cate that responders typically are very vulnera-ble to hazardous exposures.They often enterthe event area with little knowledge of thechemicals involved, and they do not have theproper protection that may prevent contactwith these chemicals.” (Berkowitz et al., 2004)
Although injuries resulted from only 7.2 percentof all the hazardous substance incidents reported byfive states to the HSEES system during 1996 to1999, injuries resulted from a much higher portion(52.7 percent) of incidents when methamphetamineprocessing was a factor at the incident scene(MMWR, November 17, 2000).40 In one incident inApril 1996, three Washington State EMTs and twopolice officers experienced eye and respiratory irri-tation after being exposed in an apartment to emis-sions from a fire involving acetone, hydrochloricacid, and sodium hydroxide in an illicit metham-
phetamine lab. Overall, symptoms reported by EMSresponders across all five states included eightcases of respiratory tract irritation (47.1 percent ofEMS responders reported symptoms), four cases ofeye irritation (23.5 percent), two cases of nauseaand vomiting (11.8 percent), and one report each ofskin irritation, headache, and shortness of breath(each 5.9 percent). “EMTs sustained most injuriesthrough onsite exposure or direct contact with theclothing or skin of contaminated persons.... None ofthe injured first responders was wearing personalprotective equipment at the time of injury.”(MMWR, November 17, 2000). The associatedMMWR editorial noted that “standard uniformsworn by police officers, EMTs, and hospital person-nel provided little or no chemical/respiratory protec-tion.” See Appendix G for additional discussion ofresponse to clandestine methamphetamine labora-tories.
EMS personnel who responded to the WorldTrade Center rescue effort in 2001 visited healthcarefacilities 183 times. The most common complaintswere musculoskeletal injuries (38 cases), headache(21 cases), respiratory effects other than acute infec-tion (18 cases), eye irritation or injury (17 cases),and skin problems (11 cases) (Berrios-Torres et al.,2003). Most of the affected EMS responders weretreated and released; there were no fatalities amongthis group and only one EMS responder was admit-ted to a hospital. The authors could not determineincident rates for these injuries and illnesses be-cause the total number of individuals working in thecapacity of EMS responder during the response wasnot recorded. This study evaluated injuries and ill-nesses for which various groups of first responderswere treated and results do not reflect the numberof firefighters who died in the World Trade Centerdisaster.
Other studies shed light on exposure patterns ofemergency response personnel in general (not spe-cific to EMS responders). One review of injuriescaused by hazardous materials accidents inMassachusetts between 1990 and 1996 found that“when injuries did occur, they were more frequentlyamong civilians (25 percent of the incidents) thanpublic service personnel (7 percent of the incidents).Inhalation exposure was more common [among thepublic] than dermal exposure, while injury to publicservice personnel involved only minor muscu-loskeletal injuries.” (Kales et al., 1997).
Six first responders were among 44 peopleinjured in Texas when a tanker car was puncturedduring a train derailment in 2004. “At least 60,000pounds of chlorine (as released gas) reacted withsodium hydroxide to form sodium hypochlorite,
40 The five states were Iowa, Minnesota, Missouri, Oregon, andWashington.

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 8 9
killing two people. [EMS] personnel were amongthe first responders at the scene.” (MMWR, 2005).Eighty first responders were decontaminated afterresponding to the event.
Compared to the amount of information avail-able for firefighters and police, relatively few reportsprovide injury and illness statistics specifically forEMS responders. The more general emergencyresponder information, however, has some inferen-tial value. A Rand report (Houser et al., 2004) ratesthe applicability of available emergency servicescasualty data (for firefighters, police, etc.) to EMSresponders.41 The report classifies the relevance ofgeneral emergency services data to the experienceof EMS responders as “medium” for fatal and non-fatal injury and illness. On the other hand, for HAZ-MAT incidents, the applicability of general emer-gency services data to the experience of EMSresponders is rated as “high,” suggesting that theauthor considered many of the determinants of haz-ardous materials exposure similar for responders invarious specialties (e.g., fire, HAZMAT, medical, andpolice).
Risk to EMS Responders of Injury and Illness fromCauses Other than Hazardous Substance ExposureAs shown in the previous section, hazardous sub-stance exposure is a real concern for EMS respon-ders, but is far from the only concern. For compari-son, this section describes other causes of injuryand illnesses in EMS responders (i.e., not related tohazardous substances).
Injury and illness statistics support the need forsafer work practices. In a survey of registered EMTsin New England, Schwartz et al. (1993) describedself-reported injury rates (for back, stress, assault,hearing loss, eye injury, ambulance collision, etc.).42
The average prevalence rates, standardized to thenumber of occurrences per 100 full-time equivalent(FTE) EMTs per year, were highest for stress thatinterfered with the job (prevalence rate of 27.1),back injury (25.4), and injuries to extremities (23.7).Over half the back injuries resulted in lost workdays,the average being 25 days, and the range from 2 to180 days. EMTs reported being assaulted at a rate of20.3 occurrences per 100 FTE EMTs/year and beinginvolved in an ambulance collision at a prevalencerate of 9.9 occurrences per 100 FTE EMTs/year. Eyeinjury (due to foreign objects or chemicals) andhearing loss were reported less frequently, withprevalence rates of 3.4 and 6.0, respectively; howev-er, even these values potentially represent a largenumber of affected individuals, considering thatthere were over 38,000 registered EMTs at the timethat this survey was conducted.43
Gershon et al. (1995) also investigated accidentsand injuries among EMS responders in the early1990s. In this case, the research evaluated medicalcharts for EMS responders employed by a countyfire department, which conducted approximately32,000 emergency responses in 1992. EMS employ-ees filed 226 injury reports: 23 percent related tosprains, 20 percent to strains, and 15 percent inresponse to exposure to body fluids. The back (20percent) and respiratory tract (15 percent) were thesites most frequently injured. “Most incidents werecaused by stretcher mishaps, especially duringtransport of heavy patients.”
In a more recent retrospective review, Maguire etal. (2005) studied on-duty injury reports recordedbetween 1998 and 2002 for two EMS agencies thatwere the sole 9-1-1 EMS providers in large urbanareas (civilian, non-firefighting). Agency employeeslogged over 2.8 million hours and experienced 489reported injuries over the period studied (227 ofthese involved lost work time). The overall injuryrate was 34.6 per 100 FTEs/year, with sprains,strains, and tears the most frequent category ofinjury, and the back the most frequently injured site.The authors conclude, “Our findings have shownthat the rate of injuries among EMS workers washigher than the rate for any private industry pub-lished by the [Department of Labor] in 2000.”
Other investigators also found that transporta-tion-related crashes and assaults contributed sub-stantially to EMS responder injury rates, with EMSresponders accounting for 33 percent of fatalities
41 For example, the authors analyzed how closely study findingsbased on data covering the combined experience of firefighters,police, and other types of emergency responders (defined as“general emergency services data”) would track the actual expe-rience of EMS responders. The authors rated EMS personnel’srisk of fatal injury or illness (e.g., due to collapse of a burningstructure or gunfire) as lower than that of firefighters and police,while the hazardous materials exposure of EMS personnel wasrated as more similar (but not necessarily identical) to that of fire-fighters and police.42 Questionnaires were mailed to a random sample (2 percent) ofall registered EMTs in Vermont, New Hampshire, Rhode Island,Maine, Connecticut, and Massachusetts. Fifty-six percent of the786 surveys were successfully returned. The average responderwas 35 years old with 8 years on the job (ranging from less than1 year to 36 years of EMT experience) (Schwartz et al., 1993).Note that the low return rate is a possible source of bias in thestudy, which could have lead to an over-representation of injuryrates as EMTs who had been injured might be more likely toreturn the survey.
43 The authors were not able to determine the proportion of allregistered EMTs that were full-time, part-time, or not activelyworking in the field. The survey respondents, however, workedan average of 33 hours per week.

9 0
Occupational Safety andHealth Administration
associated with ambulance occupants in crashes.The authors cited inconsistent seatbelt/restraint useas a weak point in EMS responder vehicular safety(MMWR, February 28, 2003). Kahn et al. (2001)reviewed fatal ambulance crash records from 1987to 1997, confirming that the most serious or fatalinjuries occurred in the rear (compared to the frontdriver compartment) and were associated withimproperly restrained occupants. The authors alsofound that 41 percent of ambulance drivers hadpoor driving records and 16 percent had been citedfor traffic violations.
EMS responders also experience elevated occu-pational mortality and ground transportation-relatedfatalities that are a significant factor in the estimatedfatality rate for EMS personnel. For this group, thefatality rate from all causes was 12.7 deaths per100,000, more than twice the national average of 5.0deaths per 100,000 for the same period (Maguire etal., 2002; MMWR, February 28, 2003). The authorsreviewed three independent fatality databases fromapproximately 1992 to 1997 and estimated therewere 114 EMS employee fatalities during those 6years, including at least 67 ground transportation-related fatalities, 19 air ambulance crash fatalities,13 deaths resulting from cardiovascular incidents,10 homicides, and 5 deaths due to other causes(Maguire et al., 2002). Citing more recent data fromthe National EMS Memorial Service, Houser et al.(2004) reported that causes of EMS employee line-of-duty fatalities from 1998 to 2001 were due to air-craft accidents (57 percent, primarily from rescuehelicopter crashes), motor vehicle accidents (26 per-cent), heart attacks/stress (7 percent), and other (11percent).
Injuries and fatalities are not limited to employ-ees. Students and trainees are similarly affected.Cone and McNamara (1997) surveyed emergencymedicine residency programs and concluded,“Injuries sustained by [emergency medical residentsin the field] during EMS rotations are uncommonbut nontrivial, with several serious injuries and onefatality reported.”
The problem of assaults on EMS responders hasbeen receiving increasing attention. Mechem et al.(2002) analyzed an occupational injury database atthe Philadelphia Fire Department (PFD) and foundthat 4 percent of occupational injuries were due toassaults. Among 1,100 employee injury reportsfrom 1996 to 1998, the authors identified 35 involv-ing assaults on paramedics and an additional nineinvolving assaults on firefighters. Forty-one percentof the assaults occurred during patient care activi-ties, and in 82 percent of the cases, the employee
sought medical treatment. Twenty-six (59 percent)of the assaults were classified as intentional and 17(38 percent) were considered unintentional (definedas “patient in an altered mental status”). “The find-ing that far more paramedics than firefighters wereassaulted is noteworthy, given that at the time thePFD employed almost ten times as many firefight-ers as paramedics.” The same authors reviewedseveral other studies, which suggested similartrends: 61 to 90 percent of EMS providers had beenthe victim of abuse or a violent act, or been assault-ed on the job, usually by a patient, a patient’s familymember, or a bystander.
Despite the levels of assault, when Mock et al.(1999) studied the effects of violence and shiftschedules on EMS providers, results suggested thatthe providers were no more anxious than the gener-al working public. Cydulka et al. (1997), however,found that stress levels were “very high” among
Promoting Ambulance Safety
Ambulance safety advocates recommend amulti-tiered approach to addressing the highEMS responder vehicle-related injury and deathrates. The following are some examples:
One specialist advocates an interdisciplinaryapproach including better access to EMS acci-dent and injury statistics, increased applicationof automotive safety principles to ambulancedesign, wearing helmets in the back of anambulance (until other safety features areimplemented), driver feedback with “black box”technology, incorporating Intelligent Transpor-tation System technology into ambulances, con-sideration of ergonomics in crashworthinessresearch, improvements in fleet management/policy, and relevant standards to guide theseprocesses (Levick, 2006; EMS Insider, 2006).
Green, et al. (2005) conducted computer model-ing and crash testing to identify potential solu-tions to the high EMS employee injury rate andfound opportunities for improvements in ambu-lance restraints, seat design, cabin geometry,and padding.
Ambulance safety is advanced by recent publi-cations, such as the U.S. Fire Administration’sPolicies and Procedures for Emergency VehicleSafety, which includes a customizable modelpolicy (USFA/IAFC, 2006) and the AmericanNational Standards Institute’s ANSI/ASSE Z15.1standard on Safe Practices for Motor VehicleOperators (ANSI/ASSE, 2006).

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9 1
the 22 percent of the National Association ofEmergency Medical Technicians (NAEMT) member-ship who returned a survey, which had been sent toall members. These authors cited a number of rea-sons ranging from job dissatisfaction to personnelshortages.
EMS responders are also subject to bloodbornepathogen exposures. Needlesticks and other percu-taneous injuries resulting in exposure to blood orother potentially infectious materials are a concerndue to the high frequency of their occurrence andthe potential severity of the health effects associatedwith exposure. When these injuries involve expo-sure to infectious agents, affected EMS respondersare at risk of contracting disease. Exposed individu-als may also suffer from adverse side effects ofdrugs used for post-exposure prophylaxis and frompsychological stress due to the threat of infectionfollowing an exposure incident (OSHA, 2001-BBPPreamble). Surprisingly, there is some evidence thatEMS responders’ rate of zero-conversion for the
hepatitis C virus (HCV), due to needlesticks, is simi-lar to that of the general population. The authorshypothesize that this is a combination of the“healthy worker syndrome” (i.e., unhealthy employ-ees leaving the profession), plus some level ofincreased risk due to activities associated with theEMS responder profession (compared to the gener-al population), resulting in a neutral risk ratio (Boalet al., 2004). A separate study reported that needle-stick rates were lower for EMS personnel using self-retracting lancets than other types (Peate, 2001).
These studies show the breadth of risks thatEMS responders face in the line of duty. These per-sonnel are exposed to substantial hazards frommotor vehicle crashes, sprains and strains, on-the-job violence, and other significant sources of injuryand illness. Comprehensive efforts to improve theoccupational health and safety of EMS respondersmust address these factors, but should also pro-mote adequate preparation for hazardous substancescenarios.
9 2
Occupational Safety andHealth Administration
Appendix P
Industry Characteristics that Affect HowEmployers Train and Protect theirEmployeesA multitude of EMS industry characteristics affecthow employers make decisions about training andprotecting EMS responders.
Characteristics of the EMS Industry
• The array of regulatory organizations withjurisdiction over EMS responders and theagencies for which they work.
• The diversity of state-specific certification,training, and regulatory requirements and theapplicability of OSHA’s HAZWOPER standard(or the equivalent in State plan states) to EMSagencies.
• The overlap between career and volunteerEMS providers.
• The overlap between public and privateambulance agencies.
• The overlap between inter-facility transportingambulance services and emergency responseservices.
• The mechanism and sources used to fundEMS and the extent of such funding.
• The unique paradigms under which EMSagencies operate in order to accomplish theirimportant public health and emergency medi-cine missions.
• The mutual aid agreements between EMSagencies and other organizations/jurisdictions.
• The influence of ad hoc in-the-field decisionson EMS responder health and safety.
• The employer’s and contracting municipality’sdiligence in complying with OSHA or statehealth and safety regulations.
• The close relationship between this industryand hospital-based emergency services, firedepartments, and hazardous materials re-sponse teams.
• The role EMS agencies play in 9-1-1 response.• The local community’s expectations regarding
EMS.• The diverse conditions under which EMS
responders could work.• The “terms of art” unique to this and closely
related industries.• The need to make informed decisions quickly
based on initial information that may beincomplete.
• The limited equipment/storage space avail-able on an ambulance.
• The challenges of treating patients whileensuring personal safety and health.
This appendix examines three specific strengthsand challenges faced by the EMS industry includ-ing its relationship with the U.S. Department ofTransportation’s (DOT) National Highway TrafficSafety Administration (NHTSA); the applicability offederal and state OSHA HAZWOPER standards andother regulations; and the complexity created byoverlapping organizational demographics of EMSresponders has on the industry. Although state andfederal government organizations play a large role,local EMS provider demographics also can affectthe way employers implement EMS responderhealth and safety programs.
The Roles of NHTSA and StatesNHTSA develops the National Standard Curriculum(NSC), which is voluntarily adopted by the states tomeet their individual needs. States then licenseEMS responders and provide oversight of initial andongoing training requirements. Typically, an EMSresponder who is properly trained to the NSC, isevaluated to be competent, and meets other staterequirements, is then eligible to be licensed by thestate to practice.
NHTSA’s NSC provides the framework for anationally recommended minimum standard forEMS responder education. The curricula may besupplemented by additional resources and educa-tion, some of which are also available as trainingcourse outlines from NHTSA. NHTSA does not,however, dictate the amount of time trainers ina state will spend instructing on a given topic.Although objective and didactic material in the NSCcontain most of the elements of OSHA’s standardon Hazardous Waste Operations and EmergencyResponse (HAZWOPER) training, the material doesnot meet the requirements for HAZWOPER training.Specifically, to meet HAZWOPER requirements, thestandard curricula would need to be customized to(1) include information relevant to local communityconditions and (2) provide students with adequatetraining time to meet the HAZWOPER trainingrequirements (e.g., 8 hours for operations leveltraining). As a national program the NSC does notinclude information on specific local communityconditions, nor does it specify training time require-ments for those elements that could serve as thebasis for meeting the general HAZWOPER trainingrequirements.
The current EMS education system has limita-tions. According to an advisory panel, a more for-mal national EMS training program could provide

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9 3
greater consistency across the U.S. (NHTSA, 2000).The advisory panel listed hazardous materials inci-dents as one of 22 core content categories, althoughcompatibility with HAZWOPER training require-ments is not specifically listed as an objective. Arevised system, called the National EMS EducationStandards is currently under development. The newsystem is expected to offer a more structured corecontent and credentialing process that will also beeasier to adapt as the need arises.
The U.S. is not alone in updating EMS trainingstandards and considering competency of EMS per-sonnel who could respond to a hazardous materialrelease. An EMS training system in Canada, imple-mented by the Minister of Health and Long-termCare in the Province of Ontario, Canada, is alreadyincorporating a high degree of standardization intothe province-wide standards for EMS training, vehi-cles, and equipment. While this structure might notbe practical in the U.S., certain aspects may serveas illustrative examples when EMS decision makersreview local, regional, state, and federal standards.In particular, since the events of September 11,2001, policies dictate that “when an incident in-volves the response to hazardous materials… theexpectation is that all municipal and communityresponse agencies (fire, police, and emergencymedical services) throughout the province have thecapacity to respond… in keeping with the aware-ness level as defined by the National Fire ProtectionAssociation Standard 472 (NFPA 472): Standardfor Professional Competence of Responders toHazardous Materials Incidents (2002, Edition). Thismeans that all responders should be able to recog-nize the presence of hazardous materials and takeappropriate safety precautions, secure the scene ofthe incident, and call the appropriate authorities forassistance.” (Barg, 2004).
Applicability of Federal and State OSHA HAZ-WOPER Standards and Other RegulationsEmergency responders at the site of a hazardoussubstance release are covered under OSHA’s HAZ-WOPER standard, or the parallel OSHA-approvedState Plan standard.44 Emergency responders,including firefighters, law enforcement, and EMSpersonnel, are often employees of local, municipal,or state governments or effectively acting in thatcapacity under a contract or other agreement.
Although Federal OSHA's standards and enforce-ment authority do not extend to such state and localgovernments, these employers and employees arecovered by the 26 states that operate OSHA-approv-ed State Plans and, in states without State Plans, bythe U.S. Environmental Protection Agency (EPA)with regard to HAZWOPER (29 CFR 1910.120).45
State Plan programs set and enforce standards,such as those for HAZWOPER and RespiratoryProtection, which are identical to or “at least aseffective as” Federal OSHA standards, and, there-fore, may have more stringent or supplementalrequirements. State Plan standards apply to stateand local government employees and, in somecases, to volunteers. EPA's HAZWOPER parallelstandard was adopted to cover public sectoremployees in states without OSHA-approved StatePlans who otherwise would not be covered by theFederal OSHA standard, including volunteers whowork for a government agency engaged in emer-gency response, such as firefighters. For consisten-cy, OSHA interprets the HAZWOPER standard forEPA. Federal OSHA administers the safety andhealth program for the private sector in the remain-ing states and territories, and also retains authoritywith regard to safety and health conditions forFederal employees throughout the nation (OSHA,1991-Borwegen).
Employers of EMS responders are also regulatedunder numerous and diverse local programs. Narad(1998) conducted an inventory of ambulance serviceregulatory programs in California and noted that“California has a variety of regulatory programs forambulance services; these are shared among thestate, county, and city governments, as well asmulti-county agencies. The types of regulatory pro-grams and the standards used vary widely aroundthe state.” This pattern is duplicated to some degreein each of the 50 states across the U.S. Although itis beyond the scope of this document to discussindividual local programs, employers need to beaware of them and communicate with local pro-gram administrators to address any conflictsbetween local programs and state or federalrequirements.
The Influence of Overlapping OrganizationalDemographics of EMS RespondersOne method of describing EMS responder activitiesis to divide them according to functional roles(those who respond to emergencies and those who44 In a letter of interpretation OSHA explained that public employ-
ee EMTs in State Plan programs must be covered by approvedstate OSHA standards. The extent to which volunteers are cov-ered in State Plan programs depends on state law and policy(OSHA, 1996 – Grassley).
45 In states without OSHA-approved State Plans, state and localgovernment employees are covered with regards to HAZWOPERunder EPA’s 40 CFR Part 311.

9 4
Occupational Safety andHealth Administration
do not). Other divisions can be made according tothe type of organization the EMS responder worksfor, how many hours per week the responder works,or whether the responder is a volunteer.
Many EMS responders are considered “inter-facility transporting EMS responders” and primarilytransfer patients to and from medical facilities undernon-emergency conditions. Many of these EMSresponders do not respond to 9-1-1 calls as a regu-lar part of their jobs. In contrast, most of theremaining EMS responders do work in an emer-gency-response capacity at least some of the time.These two EMS responder groups have substantial-ly different risk of encountering a hazardous sub-stance during their normal duties.
EMS responders can be further subdivided into(1) EMS personnel for whom providing medical carebefore the patient arrives at a healthcare facility isthe primary duty and (2) EMS responders who arecross-trained as firefighters, hazardous materialsteam members, or law enforcement officers.46 In thelatter case, the EMS responders’ medical dutiessupplement the other related profession. EMSresponders in both groups might experience similarranges of hazards while performing medical care(regardless of what hazards they might encounterwhen filling the other role(s) for which they arecross-trained). Among fire-based EMS responders,“the integration with firefighters and associatedemphasis on safety and access to quality equipmentmay lead to fire-based EMS systems experiencingfewer shortcomings in their [PPE] options”(LaTourrette et al., 2003).
The cross-trained EMS responders may haveadditional training and qualifications (e.g., to wear ahigher level of respiratory protection) than EMSresponders who perform only medical responseactivities. Those additional qualifications are relatedto requirements of the EMS responders’ other occu-pational expectations and are not a traditional stan-dard requirement for medical emergency responseactivities.
EMS responders may work for public, private, orcontract agencies, fire departments, hospitals, orother types of organizations. This makes it difficultto fully characterize the EMS industry and has impli-cations for how OSHA and EPA regulations areapplied.
Finally, EMS responders may work full-time orpart-time, or they may work on a strictly voluntarybasis. An undefined number of EMS respondersmaintain their certification, but do not actually prac-tice (i.e., they work in a different field).
In summary, EMS responders are a diversegroup. Their risks vary with their primary and sec-ondary roles. OSHA recognizes that this diversity ofroles and risks must be taken into considerationwhen identifying best practices and recommenda-tions. Additionally, state and local jurisdictions havea good deal of freedom to tailor programs to localneeds; however, the number and variability of localinfluences affecting an individual EMS responderagency can lead to numerous requirements whichare sometimes confusing.
46 Approximately “40 percent of EMS response is provided by firedepartments (after Karter, 2001), with independent agencies and,to a smaller extent, hospitals, private firms, and law enforcementagencies making up the remaining 60 percent.” (LaTourrette etal., 2003).
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9 5
Appendix Q
Sources of Help in Addressing BiologicalAgent IssuesHazardous substance release events could includethe immediately identified (or announced) release ofbiological agents. When the hazard assessmentsuggests that hazardous substance releases in theregion could involve biological agents, employers ofEMS responders should plan to protect their work-ers from these agents.
Biological agents generally occur in the form ofviruses, bacteria, and substances produced by bio-logical agents (e.g., ricin). Some are infectiousagents, while others cause health effects throughother processes, such as toxicity. In the event thatthe biological agent is a viral variant with a highpatient mortality rate (e.g., a pandemic influenza),EMS responders should assume (until confirmedotherwise) that the virus is spread by airbornetransmission (i.e., as an aerosol) as well as bydroplets. EMS responders will require respiratoryprotection (minimum N95).46 This level of respirato-ry protection is also appropriate for bacteriologicalagents such as tuberculosis (TB), commonly spreadby infectious process.
OSHA’s standard on bloodborne pathogens (29CFR 1910.1030) sets forth requirements for protect-ing workers, including EMS responders, from thistype of biological agent (e.g., Hepatitis B).
More detailed information on addressing theissues surrounding biological agent exposures anddisease spread by infectious processes are availableat the following sources:
• Pandemic flu: www.pandemicflu.gov
• Preparing for a Bioterrorist Attack: Legal andAdministrative Strategies: www.cdc.gov/ncidod/eid/vol9no2/02-0538.htm
• CDC Disease Listings (look up general and tech-nical information on disease agents [infectiousand otherwise] from anthrax to yersiniosis):www.cdc.gov/ncidod/dbmd/diseaseinfo/default.htm
• OSHA’s Pandemic Influenza Preparedness andResponse Guidance for Healthcare Workers andHealthcare Employers: www.osha.gov/Publications/OSHA_pandemic_health.pdf
• OSHA Regulations: Bloodborne Pathogens stan-dard (29 CFR 1910.1030): www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=10051
• NIOSH page on Eye Protection for InfectionControl: www.cdc.gov/niosh/topics/eye/eye-infectious.html
• CDC Infection Control Guidelines: www.cdc.gov/ncidod/dhqp/guidelines.html
• OSHA Safety and Health Topics page on possiblehazards and solutions for healthcare workers athealthcare facilities and elsewhere (includesinformation relevant to EMS responders):www.osha.gov/SLTC/healthcarefacilities/recognition.html
• OSHA Safety and Health Topics page forEmergency Responders: www.osha.gov/SLTC/emergencypreparedness/responder.html#First
• NIOSH guidelines for healthcare workers andhealthcare facilities: www.cdc.gov/niosh/hcwold0.html
• CDC Emergency Response and Preparednesspage on ricin: http://www.bt.cdc.gov/agent/ricin
Concern about Needlesticks andBiological AgentsNeedlesticks are one of the greatest sources of con-cern for EMS responders under normal conditionsand the need for concern is potentially even greaterduring incidents involving biological agents. In thecourse of their job duties, EMS responders arepotentially subject to exposure to blood and otherpotentially infectious material (OPIM). This increasestheir risk of exposure to bloodborne diseases, suchas hepatitis B and C and human immunodeficiencyvirus (HIV) (Adams & Elliot, 2006; Boal et al., 2005;Peate, 2001; Rischitelli et al., 2001). EMS respondersare also exposed to airborne infectious diseases,like meningococcal meningitis and tuberculosiswhich have serious health effects (Miller et al.,2005). Exposed individuals may also suffer fromadverse side effects of drugs used for post-exposureprophylaxis and from psychological stress due tothe threat of infection following an exposure inci-dent (OSHA, 2001-BBP Preamble). Because EMS
46 Airborne transmission, as occurs in tuberculosis, is spreadthrough small infectious particles such as droplet nuclei. Unlikethe larger droplets, these very small airborne droplet nuclei canbe readily disseminated by air currents to susceptible individuals.They can travel significant distances and can penetrate deep intothe lung to the alveoli where they can establish an infection. Thepresence of significant airborne transmission would indicate theneed for ventilation procedures and respiratory protectiongreater than that afforded by a surgical mask, e.g., a NIOSH-certified N95 or higher respirator.

9 6
Occupational Safety andHealth Administration
responder work is performed in uncontrolled, emer-gency environments, usually dealing with trauma orsudden onset of illness, there is a greater potentialfor needlesticks or blood exposure to occur (Boal etal., 2005; Peate, 2001).
Preliminary results of a national study to preventblood exposure in paramedics by the PennsylvaniaDepartment of Health determined that blood expo-sures occurred through (1) needle or lancet stick, (2)cuts from sharp objects, (3) blood in eyes, nose ormouth, (4) uncooperative or combative patient bites(skin break) and (5) blood on non-intact skin(Pennsylvania Department of Health, 2007). Twenty-two percent of the paramedics reported at least oneexposure to blood and an additional seven percentreported more than one blood exposure in the lasttwelve months of service (Pennsylvania Departmentof Health, 2007).
EMS responders do not always report the expo-sure. The Pennsylvania study cited reasons for non-report as:
• The paramedic did not consider the exposuresignificant or forgot about the exposure.
• The paramedic determined that he/she was toobusy and reporting involved too much paper-work.
• The paramedic did not want to be reprimanded.
• The paramedic was worried that somebodywould find out about the exposure.
• The paramedic thought that the company rarelytook action when a worker is exposed.
The critical concept in this kind of responderwork is the need to focus on prevention of exposureto blood and OPIM (Boal et al., 2005). A review ofliterature determined that combinations of strate-gies reduced needlestick injuries for healthcareemployees. Enhanced training on sharps education,safe needle choice, a uniform approach to exposureplans with concise treatment protocol, and limitinglong work hours have been cited as actions thatdecrease needlestick injuries (Adams & Elliot, 2006;Ilhan et al., 2006; Miller et al., 2005; Peate, 2001).

O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9 7
OSHA Assistance
OSHA can provide extensive help through a variety ofprograms, including technical assistance about effec-tive safety and health programs, state plans, work-place consultations, and training and education.
Safety and Health ManagementSystem GuidelinesEffective management of worker safety and healthprotection is a decisive factor in reducing the extentand severity of work-related injuries and illnesses andtheir related costs. In fact, an effective safety andhealth management system forms the basis of goodworker protection, can save time and money, increaseproductivity and reduce employee injuries, illnessesand related workers’ compensation costs.
To assist employers and workers in developingeffective safety and health management systems,OSHA published recommended Safety and HealthProgram Management Guidelines (54 Federal Register(16): 3904-3916, January 26, 1989). These voluntaryguidelines can be applied to all places of employmentcovered by OSHA.
The guidelines identify four general elements criti-cal to the development of a successful safety andhealth management system:• Management leadership and worker involvement,• Worksite analysis,• Hazard prevention and control, and• Safety and health training.
The guidelines recommend specific actions, undereach of these general elements, to achieve an effectivesafety and health management system. The FederalRegister notice is available online at www.osha.gov.
State ProgramsThe Occupational Safety and Health Act of 1970 (OSHAct) encourages states to develop and operate theirown job safety and health plans. OSHA approves andmonitors these plans. Twenty-five states, Puerto Ricoand the Virgin Islands currently operate approvedstate plans: 22 cover both private and public (state andlocal government) employment; Connecticut, Illinois,New Jersey, New York and the Virgin Islands cover thepublic sector only. States and territories with their ownOSHA-approved occupational safety and health plansmust adopt standards identical to, or at least as effec-tive as, the Federal OSHA standards.
Consultation ServicesConsultation assistance is available on request toemployers who want help in establishing and main-taining a safe and healthful workplace. Largely fundedby OSHA, the service is provided at no cost to the
employer. Primarily developed for smaller employerswith more hazardous operations, the consultationservice is delivered by state governments employingprofessional safety and health consultants. Comprehen-sive assistance includes an appraisal of all mechanicalsystems, work practices and occupational safety andhealth hazards of the workplace and all aspects of theemployer’s present job safety and health program. Inaddition, the service offers assistance to employers indeveloping and implementing an effective safety andhealth program. No penalties are proposed or cita-tions issued for hazards identified by the consultant.OSHA provides consultation assistance to the employ-er with the assurance that his or her name and firmand any information about the workplace will not beroutinely reported to OSHA enforcement staff. Formore information concerning consultation assistance,see OSHA’s website at www.osha.gov.
Strategic Partnership ProgramOSHA’s Strategic Partnership Program helps encour-age, assist and recognize the efforts of partners toeliminate serious workplace hazards and achieve ahigh level of worker safety and health. Most strategicpartnerships seek to have a broad impact by buildingcooperative relationships with groups of employersand workers. These partnerships are voluntary rela-tionships between OSHA, employers, worker repre-sentatives, and others (e.g., trade unions, trade andprofessional associations, universities, and other gov-ernment agencies).
For more information on this and other agencyprograms, contact your nearest OSHA office, or visitOSHA’s website at www.osha.gov.
OSHATraining and EducationOSHA area offices offer a variety of information serv-ices, such as technical advice, publications, audiovisu-al aids and speakers for special engagements. OSHA’sTraining Institute in Arlington Heights, IL, providesbasic and advanced courses in safety and health forFederal and state compliance officers, state consult-ants, Federal agency personnel, and private sectoremployers, workers and their representatives.
The OSHA Training Institute also has establishedOSHA Training Institute Education Centers to addressthe increased demand for its courses from the privatesector and from other federal agencies. These centersare colleges, universities and nonprofit organizationsthat have been selected after a competition for partici-pation in the program.
OSHA also provides funds to nonprofit organiza-tions, through grants, to conduct workplace trainingand education in subjects where OSHA believes there
9 8
Occupational Safety andHealth Administration
is a lack of workplace training. Grants are awardedannually.
For more information on grants, training and edu-cation, contact the OSHA Training Institute, Directorateof Training and Education, 2020 South ArlingtonHeights Road, Arlington Heights, IL 60005, (847) 297-4810, or see Training on OSHA’s website atwww.osha.gov. For further information on any OSHAprogram, contact your nearest OSHA regional officelisted at the end of this publication.
Information Available ElectronicallyOSHA has a variety of materials and tools available onits website at www.osha.gov. These include electronictools, such as Safety and HealthTopics, eTools, ExpertAdvisors; regulations, directives and publications;videos and other information for employers and work-ers. OSHA’s software programs and eTools walk youthrough challenging safety and health issues andcommon problems to find the best solutions for yourworkplace.
OSHA PublicationsOSHA has an extensive publications program. Fora listing of free items, visit OSHA’s website at
www.osha.gov or contact the OSHA PublicationsOffice, U.S. Department of Labor, 200 ConstitutionAvenue, NW, N-3101, Washington, DC 20210; tele-phone (202) 693-1888 or fax to (202) 693-2498.
Contacting OSHATo report an emergency, file a complaint, or seekOSHA advice, assistance, or products, call (800) 321-OSHA or contact your nearest OSHA Regional or Areaoffice listed at the end of this publication. The tele-typewriter (TTY) number is (877) 889-5627.
Written correspondence can be mailed to the near-est OSHA Regional or Area Office listed at the end ofthis publication or to OSHA’s national office at: U.S.Department of Labor, Occupational Safety and HealthAdministration, 200 Constitution Avenue, N.W.,Washington, DC 20210.
By visiting OSHA’s website at www.osha.gov, youcan also:• File a complaint online,• Submit general inquiries about workplace safety
and health electronically, and• Find more information about OSHA and occupa-
tional safety and health.
O S H A B E S T P R A C T I C E S F O R P R O T E C T I N G E M S R E S P O N D E R S 9 9
OSHA Regional Offices
Region I(CT*, ME, MA, NH, RI, VT*)JFK Federal Building, Room E340Boston, MA 02203(617) 565-9860
Region II(NJ*, NY*, PR*, VI*)201 Varick Street, Room 670New York, NY 10014(212) 337-2378
Region III(DE, DC, MD*, PA, VA*, WV)The Curtis Center170 S. Independence Mall WestSuite 740 WestPhiladelphia, PA 19106-3309(215) 861-4900
Region IV(AL, FL, GA, KY*, MS, NC*, SC*, TN*)61 Forsyth Street, SW, Room 6T50Atlanta, GA 30303(404) 562-2300
RegionV(IL*, IN*, MI*, MN*, OH, WI)230 South Dearborn StreetRoom 3244Chicago, IL 60604(312) 353-2220
RegionVI(AR, LA, NM*, OK, TX)525 Griffin Street, Room 602Dallas, TX 75202(972) 850-4145
RegionVII(IA*, KS, MO, NE)Two Pershing Square2300 Main Street, Suite 1010Kansas City, MO 64108-2416(816) 283-8745
RegionVIII(CO, MT, ND, SD, UT*, WY*)1999 Broadway, Suite 1690PO Box 46550Denver, CO 80202-5716(720) 264-6550
Region IX(AZ*, CA*, HI*, NV*, and American Samoa,Guam and the Northern Mariana Islands)90 7th Street, Suite 18-100San Francisco, CA 94103(415) 625-2547
Region X(AK*, ID, OR*, WA*)1111 Third Avenue, Suite 715Seattle, WA 98101-3212(206) 553-5930
*These states and territories operate their ownOSHA-approved job safety and health programsand cover state and local government employeesas well as private sector employees. TheConnecticut, Illinois, New Jersey, New York andVirgin Islands plans cover public employees only.States with approved programs must have stan-dards that are identical to, or at least as effectiveas, the Federal OSHA standards.
Note: To get contact information for OSHA AreaOffices, OSHA-approved State Plans and OSHAConsultation Projects, please visit us online atwww.osha.gov or call us at 1-800-321-OSHA.