Embed Size (px)
Citation preview
Evidence Summary #22-2-9 ARCHIVED 2017
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO)
Best Practices for Oncologic Pathology Secondary Review: Central Nervous System (CNS) Tumours
Alexander Boag, Glenn G Fletcher, Sidney Croul, Gerard Jansen,
James Perry, Aaron Pollett, and John Srigley *
Report Date: June 26, 2014
An assessment conducted in October 2017 ARCHIVED Evidence Summary
22-2-9. This means that the document will no longer be maintained but may still
be useful for academic or other information purposes. The PEBC has a formal and
standardized process to ensure the currency of each document
(PEBC Assessment & Review Protocol)
This Evidence Summary is part of an eleven-report series.
Please refer to #22-2-M for background and methodology.
#22-2-M: Methods and Overview
#22-2-1: Breast Cancer
#22-2-2: Gastrointestinal Cancers
#22-2-3: Genitourinary Cancers
#22-2-4: Gynecologic Cancers
#22-2-5: Head and Neck Cancers
#22-2-6: Hematologic Cancers
#22-2-7: Lung Cancer
#22-2-8: Cutaneous Melanoma and Other Skin Cancers
#22-2-9: Central Nervous System (CNS) Tumours
#22-2-10: Bone and Soft Tissue Cancers (Sarcoma)
* Author affiliations are given in Appendix I
For information about the PEBC and the most current version of all reports, please visit the
CCO Web site at http://www.cancercare.on.ca/ or contact the PEBC office at: Phone: 905-527-4322 ext. 42822 Fax: 905 526-6775 E-mail: [email protected]
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 1
QUESTION What types of specimens suspected to be or diagnosed as central nervous system (CNS)
tumours should or should not have a routine secondary pathology review? INTRODUCTION
This report is part of a series of reports on pathology secondary review in cancer diagnosis. The reader should consult document #22-2-M: Methods and Overview for a more detailed background to the project, definitions and limitations of secondary review, and the methodology used. Only a brief summary of the methods is given below, along with any details specific to this subproject.
METHODS
The evidence-based reports developed by CCO Program in Evidence-Based Care (PEBC) use the methods of the Practice Guidelines Development Cycle (1). For this project, the core methodology used to develop the evidentiary base was the systematic review. For this project, the core methodology used to develop the evidentiary base was the systematic review. Evidence was selected and key details extracted by GF of the PEBC.
The body of evidence in this review is primarily comprised of comparative studies on interobserver accuracy or agreement. The systematic review is intended to promote evidence-based practice in Ontario, Canada. The PEBC is supported by the Ontario Ministry of Health and Long-Term Care through CCO. All work produced by the PEBC is editorially independent from the Ministry. Definition of Secondary Pathology Review
In this series of documents, secondary pathology review is defined as the review of pathology specimens by a second pathologist that is usually initiated at the request of the patient or treating clinician, multidisciplinary case conference (MCC) process, quality control protocol, or as standard practice to review all cases at a cancer centre prior to treatment. Consultation or review at the request of the primary pathologist or prior to finalization of the primary pathologist’s report is NOT included in this definition. Literature Search Strategy and Study Selection Criteria
Details of the search strategy and inclusion/exclusion criteria are provided in report #22-2-M of this series and only a brief summary is included here. In December 2009, a search for practice guidelines was conducted in the National Guideline Clearing House (USA), National Institute for Health and Clinical Excellence (NICE, UK), Scottish Intercollegiate Guidelines Network (SIGN), American Society of Clinical Oncology (ASCO), National Comprehensive Cancer Network (NCCN, USA), National Health and Medical Research Council (NHMRC, Australia), New Zealand Guidelines Group (NZZG), Canadian Medical Association’s CMA Infobase: Clinical Practice Guidelines, Association of Directors of Anatomic and Surgical Pathology, College of American Pathologists (CAP), and the Canadian Association of Pathologists (CAP-ACP). The SAGE Directory of Cancer Guidelines was searched in May 2012.
MEDLINE and EMBASE databases were searched from 1995 to May 7, 2013. Articles with terms related to both pathology (including cytology or histology) and diagnostic discrepancy were retrieved. For inclusion in this report, articles had to include review of the same samples by a second pathologist (excluding review at the original pathologist’s request), be related to the diagnosis of neurologic cancer, and report on diagnostic discrepancy or agreement between two (or more) pathologists.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 2
RESULTS For neurologic cancers, the search resulted in 37 articles, of which eight were
reproducibility studies. The 29 studies (2-30) that report agreement or disagreement between initial and secondary pathology review are summarized in Table 1. There are an additional five studies that include neurologic cancer along with other cancers (31-35). While data was not extracted from the reproducibility studies, these may be of interest to some readers and address specialized areas of pathologic interpretation and especially areas where more research or standardization is necessary. The publications are therefore listed separately in Appendix II.
Almost all of the studies reported had secondary pathology review by a neuropathologist. Aldape et al (3) found that specimens initially diagnosed by a general pathologist had a 26% discrepancy rate (4.4% major), while those initially diagnosed by a neuropathologist had a 12% discrepancy rate (1.1% major). Several studies found discrepancies even among neuropathologists and involved additional neuropathologists in case of discrepancies among the primary and secondary review (2,7,15,21,28). Gupta et al (6) reported 17% discrepancy between the institutional neuropathologist and the central review neurooncopathologist.
For brain or spinal cord biopsies performed due to suspicion of neoplastic disease, Bruner et al (2) reported a 32% discrepancy rate in cases referred for treatment, including 6% major (immediate alternation of therapy, quality of life, resources) and 21% discrepancy when including change in care or prognosis. Kronz et al (31) performed a mandatory secondary review on all CNS specimens and found 3% rate of major errors, which would modify therapy or prognosis. Aldape et al (3) reported the clinical significance of discrepancies for glioma resection. They reported a 3.7% major discrepancy rate (4.4% when initially reviewed at a community hospital by a general pathologist and 1.1% when initially reviewed at an academic institution by a neuropathologist). Most studies in the evidence base involve a central pathology review for eligibility in chemotherapy or chemoradiotherapy trials and do not indicate the type of sample (biopsy or resection) or clinical significance.
The systematic review did not include any studies on secondary review for CNS metastases, metastases with an unknown primary, or primary central nervous system lymphoma (PCNSL). Guidelines
The NCCN guideline on CNS cancers (36) recommends review by an experienced neuropathologist, while NICE (37,38) recommends care by a multidisciplinary team including a pathologist who is registered as a neuropathologist or histopathologist, has specialist expertise in neuro-oncology, and takes part in the national External Quality Assurance scheme for neuropathology organised by the British Neuropathological Society. The surgical options include stereotactic biopsy or debulking procedure, subtotal resection, or maximal safe resection, while chemotherapy is effective for subtypes such as anaplastic oligodendrogliomas. Pathologic diagnosis is critical and often difficult to determine accurately.
The Children’s Cancer and Leukaemia Group (CCLG) guideline on intracranial meningioma in children and young people (39) recommends central pathology review for brain tumours to allow for consistency in the diagnosis, availability of tumour material for further research studies, and, ultimately, an increase in the knowledge base regarding this rare tumour in childhood. A neuropathologist should be part of the multidisciplinary team. The British Committee for Standards in Haematology (40) recommends that PCNSL and primary intraocular lymphoma (PIOL) be confirmed histologically and subjected to central pathological review due to the rarity of PCNSL and usually scanty diagnostic material.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 3
Stereotactic biopsy is the preferred surgical procedure, and there is no role for surgical resection. The British Neuro-oncology Society (41) recommends the diagnosis of suspected PCNSL or PIOL in a centre with a team including ocular pathology and hematopathology specialists and access to relevant immunocytochemical and molecular techniques. Pathologists should participate in relevant diagnostic external quality assessment schemes, such as that provided by the British Neuropathological Society and by the British Association of Ophthalmic Pathology. Typically these patients will be under the care of both a neuroscience and lymphoma multidisciplinary team (MDT). Primary CNS lymphoma of T-cell type (T-CNSL) is often a very difficult histological diagnosis, and an experienced neuropathologist, ocular pathologist and/or a hematopathologist should be involved in the investigation of these cases. In addition to immunohistochemistry, T-cell receptor studies may help to confirm the diagnosis.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 4
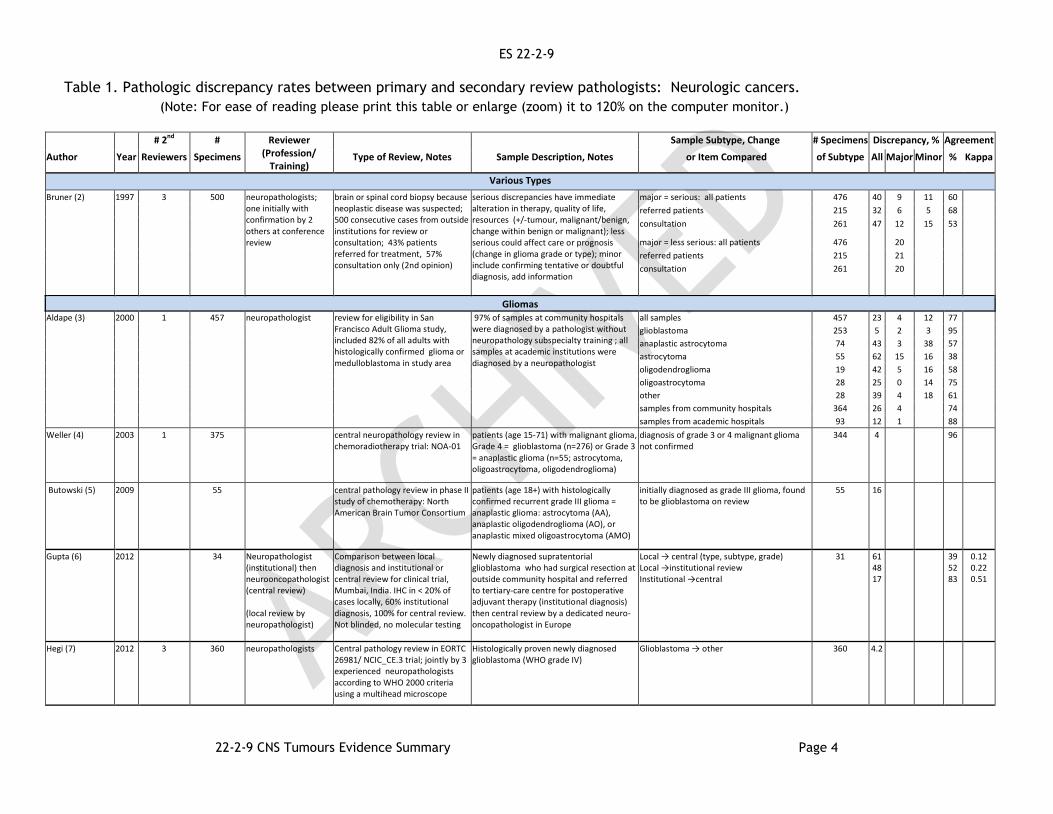
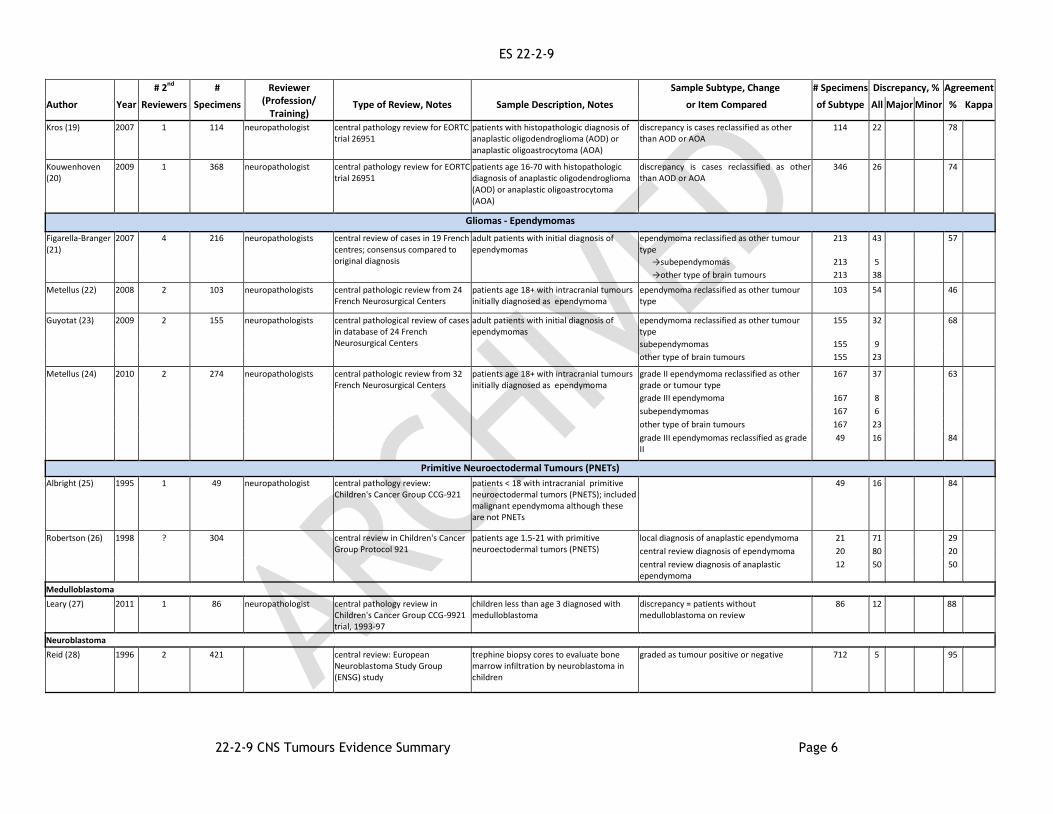
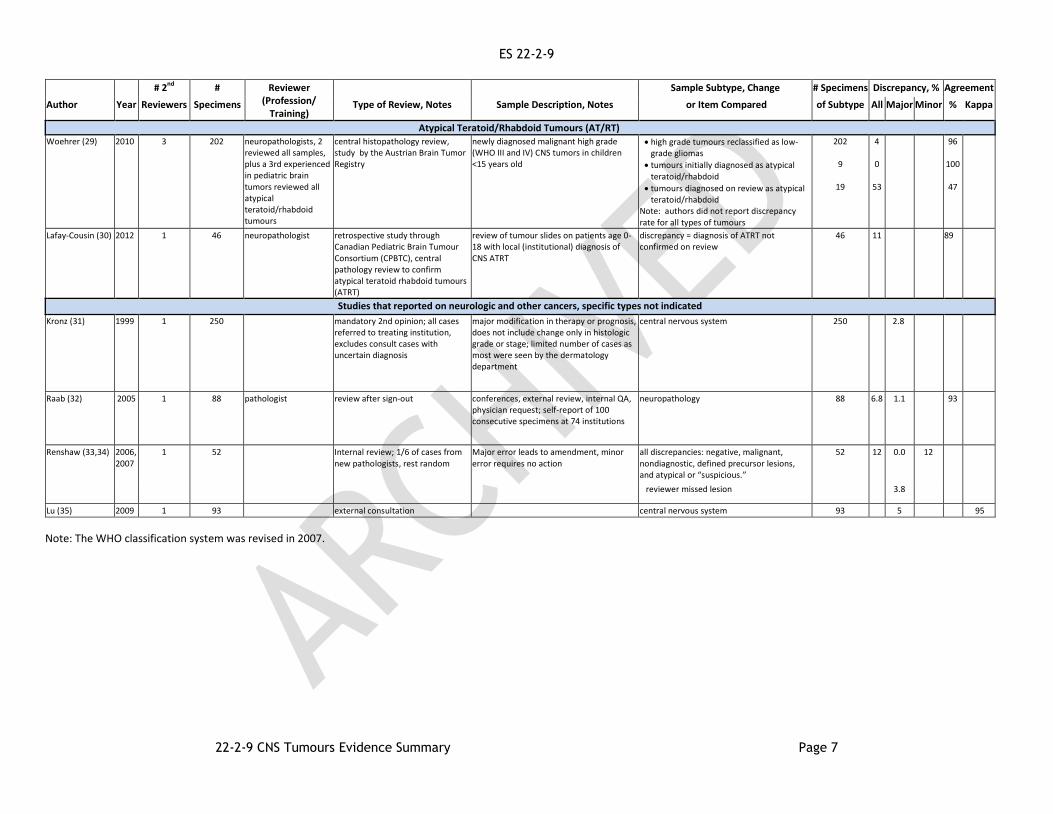
Table 1. Pathologic discrepancy rates between primary and secondary review pathologists: Neurologic cancers.
(Note: For ease of reading please print this table or enlarge (zoom) it to 120% on the computer monitor.)
# 2nd # Reviewer
(Profession/ Training)
Sample Subtype, Change # Specimens Discrepancy, % Agreement
Author Year Reviewers Specimens Type of Review, Notes Sample Description, Notes or Item Compared of Subtype All Major Minor % Kappa
Various Types
Bruner (2) 1997 3 500 neuropathologists; one initially with confirmation by 2 others at conference review
brain or spinal cord biopsy because neoplastic disease was suspected; 500 consecutive cases from outside institutions for review or consultation; 43% patients referred for treatment, 57% consultation only (2nd opinion)
serious discrepancies have immediate alteration in therapy, quality of life, resources (+/-tumour, malignant/benign, change within benign or malignant); less serious could affect care or prognosis (change in glioma grade or type); minor include confirming tentative or doubtful diagnosis, add information
major = serious: all patients 476 40 9 11 60
referred patients 215 32 6 5 68
consultation 261 47 12 15 53
major = less serious: all patients 476 20
referred patients 215 21
consultation 261 20
Gliomas Aldape (3) 2000 1 457 neuropathologist review for eligibility in San
Francisco Adult Glioma study, included 82% of all adults with histologically confirmed glioma or medulloblastoma in study area
97% of samples at community hospitals were diagnosed by a pathologist without neuropathology subspecialty training ; all samples at academic institutions were diagnosed by a neuropathologist
all samples 457 23 4 12 77
glioblastoma 253 5 2 3 95
anaplastic astrocytoma 74 43 3 38 57
astrocytoma 55 62 15 16 38
oligodendroglioma 19 42 5 16 58
oligoastrocytoma 28 25 0 14 75
other 28 39 4 18 61
samples from community hospitals 364 26 4 74
samples from academic hospitals 93 12 1 88
Weller (4) 2003 1 375 central neuropathology review in chemoradiotherapy trial: NOA-01
patients (age 15-71) with malignant glioma, Grade 4 = glioblastoma (n=276) or Grade 3 = anaplastic glioma (n=55; astrocytoma, oligoastrocytoma, oligodendroglioma)
diagnosis of grade 3 or 4 malignant glioma not confirmed
344 4 96
Butowski (5) 2009 55 central pathology review in phase II study of chemotherapy: North American Brain Tumor Consortium
patients (age 18+) with histologically confirmed recurrent grade III glioma = anaplastic glioma: astrocytoma (AA), anaplastic oligodendroglioma (AO), or anaplastic mixed oligoastrocytoma (AMO)
initially diagnosed as grade III glioma, found to be glioblastoma on review
55 16
Gupta (6) 2012 34 Neuropathologist (institutional) then neurooncopathologist (central review) (local review by neuropathologist)
Comparison between local diagnosis and institutional or central review for clinical trial, Mumbai, India. IHC in < 20% of cases locally, 60% institutional diagnosis, 100% for central review. Not blinded, no molecular testing
Newly diagnosed supratentorial glioblastoma who had surgical resection at outside community hospital and referred to tertiary-care centre for postoperative adjuvant therapy (institutional diagnosis) then central review by a dedicated neuro-oncopathologist in Europe
Local → central (type, subtype, grade) Local →institutional review Institutional →central
31 61 48 17
39 52 83
0.12 0.22 0.51
Hegi (7) 2012 3 360 neuropathologists Central pathology review in EORTC 26981/ NCIC_CE.3 trial; jointly by 3 experienced neuropathologists according to WHO 2000 criteria using a multihead microscope
Histologically proven newly diagnosed glioblastoma (WHO grade IV)
Glioblastoma → other 360 4.2
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 5
# 2nd # Reviewer (Profession/
Training)
Sample Subtype, Change # Specimens Discrepancy, % Agreement
Author Year Reviewers Specimens Type of Review, Notes Sample Description, Notes or Item Compared of Subtype All Major Minor % Kappa
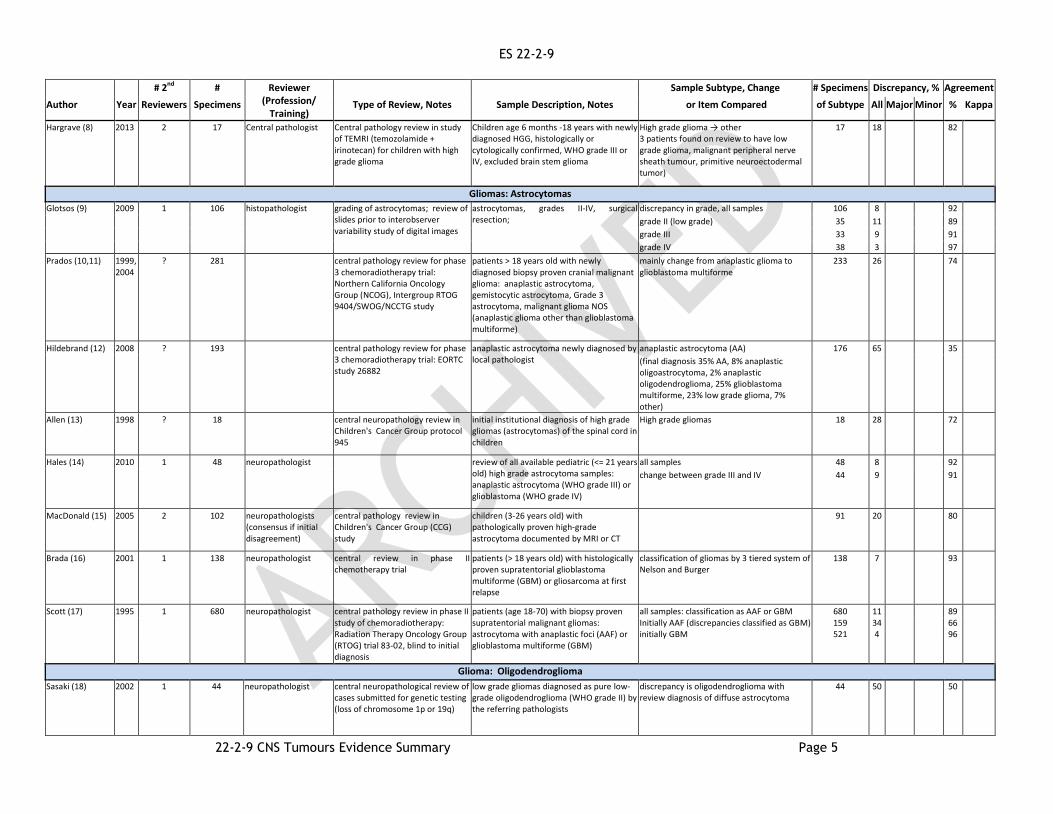
Hargrave (8) 2013 2 17 Central pathologist Central pathology review in study of TEMRI (temozolamide + irinotecan) for children with high grade glioma
Children age 6 months -18 years with newly diagnosed HGG, histologically or cytologically confirmed, WHO grade III or IV, excluded brain stem glioma
High grade glioma → other 3 patients found on review to have low grade glioma, malignant peripheral nerve sheath tumour, primitive neuroectodermal tumor)
17 18 82
Gliomas: Astrocytomas
Glotsos (9) 2009 1 106 histopathologist grading of astrocytomas; review of slides prior to interobserver variability study of digital images
astrocytomas, grades II-IV, surgical resection;
discrepancy in grade, all samples 106 8 92
grade II (low grade) 35 11 89
grade III 33 9 91
grade IV 38 3 97
Prados (10,11) 1999, 2004
? 281 central pathology review for phase 3 chemoradiotherapy trial: Northern California Oncology Group (NCOG), Intergroup RTOG 9404/SWOG/NCCTG study
patients > 18 years old with newly diagnosed biopsy proven cranial malignant glioma: anaplastic astrocytoma, gemistocytic astrocytoma, Grade 3 astrocytoma, malignant glioma NOS (anaplastic glioma other than glioblastoma multiforme)
mainly change from anaplastic glioma to glioblastoma multiforme
233 26 74
Hildebrand (12) 2008 ? 193 central pathology review for phase 3 chemoradiotherapy trial: EORTC study 26882
anaplastic astrocytoma newly diagnosed by local pathologist
anaplastic astrocytoma (AA) 176 65 35
(final diagnosis 35% AA, 8% anaplastic oligoastrocytoma, 2% anaplastic oligodendroglioma, 25% glioblastoma multiforme, 23% low grade glioma, 7% other)
Allen (13) 1998 ? 18 central neuropathology review in Children's Cancer Group protocol 945
initial institutional diagnosis of high grade gliomas (astrocytomas) of the spinal cord in children
High grade gliomas 18 28 72
Hales (14) 2010 1 48 neuropathologist review of all available pediatric (<= 21 years old) high grade astrocytoma samples: anaplastic astrocytoma (WHO grade III) or glioblastoma (WHO grade IV)
all samples 48 8 92
change between grade III and IV 44 9 91
MacDonald (15) 2005 2 102 neuropathologists (consensus if initial disagreement)
central pathology review in Children's Cancer Group (CCG) study
children (3-26 years old) with pathologically proven high-grade astrocytoma documented by MRI or CT
91 20 80
Brada (16) 2001 1 138 neuropathologist central review in phase II chemotherapy trial
patients (> 18 years old) with histologically proven supratentorial glioblastoma multiforme (GBM) or gliosarcoma at first relapse
classification of gliomas by 3 tiered system of Nelson and Burger
138 7 93
Scott (17)
1995
1
680
neuropathologist
central pathology review in phase II study of chemoradiotherapy: Radiation Therapy Oncology Group (RTOG) trial 83-02, blind to initial diagnosis
patients (age 18-70) with biopsy proven supratentorial malignant gliomas: astrocytoma with anaplastic foci (AAF) or glioblastoma multiforme (GBM)
all samples: classification as AAF or GBM Initially AAF (discrepancies classified as GBM) initially GBM
680 159 521
11 34 4
89 66 96
Glioma: Oligodendroglioma
Sasaki (18) 2002 1 44 neuropathologist central neuropathological review of cases submitted for genetic testing (loss of chromosome 1p or 19q)
low grade gliomas diagnosed as pure low-grade oligodendroglioma (WHO grade II) by the referring pathologists
discrepancy is oligodendroglioma with review diagnosis of diffuse astrocytoma
44 50 50
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 6
# 2nd # Reviewer (Profession/
Training)
Sample Subtype, Change # Specimens Discrepancy, % Agreement
Author Year Reviewers Specimens Type of Review, Notes Sample Description, Notes or Item Compared of Subtype All Major Minor % Kappa
Kros (19) 2007 1 114 neuropathologist central pathology review for EORTC trial 26951
patients with histopathologic diagnosis of anaplastic oligodendroglioma (AOD) or anaplastic oligoastrocytoma (AOA)
discrepancy is cases reclassified as other than AOD or AOA
114 22 78
Kouwenhoven (20)
2009 1 368 neuropathologist central pathology review for EORTC trial 26951
patients age 16-70 with histopathologic diagnosis of anaplastic oligodendroglioma (AOD) or anaplastic oligoastrocytoma (AOA)
discrepancy is cases reclassified as other than AOD or AOA
346 26 74
Gliomas - Ependymomas
Figarella-Branger (21)
2007 4 216 neuropathologists central review of cases in 19 French centres; consensus compared to original diagnosis
adult patients with initial diagnosis of ependymomas
ependymoma reclassified as other tumour type
213 43 57
→subependymomas 213 5
→other type of brain tumours 213 38
Metellus (22) 2008 2 103 neuropathologists central pathologic review from 24 French Neurosurgical Centers
patients age 18+ with intracranial tumours initially diagnosed as ependymoma
ependymoma reclassified as other tumour type
103 54 46
Guyotat (23) 2009 2 155 neuropathologists central pathological review of cases in database of 24 French Neurosurgical Centers
adult patients with initial diagnosis of ependymomas
ependymoma reclassified as other tumour type
155 32 68
subependymomas 155 9
other type of brain tumours 155 23
Metellus (24) 2010 2 274 neuropathologists central pathologic review from 32 French Neurosurgical Centers
patients age 18+ with intracranial tumours initially diagnosed as ependymoma
grade II ependymoma reclassified as other grade or tumour type
167 37 63
grade III ependymoma 167 8
subependymomas 167 6
other type of brain tumours 167 23
grade III ependymomas reclassified as grade II
49 16 84
Primitive Neuroectodermal Tumours (PNETs)
Albright (25) 1995 1 49 neuropathologist central pathology review: Children's Cancer Group CCG-921
patients < 18 with intracranial primitive neuroectodermal tumors (PNETS); included malignant ependymoma although these are not PNETs
49 16 84
Robertson (26) 1998 ? 304 central review in Children's Cancer Group Protocol 921
patients age 1.5-21 with primitive neuroectodermal tumors (PNETS)
local diagnosis of anaplastic ependymoma 21 71 29
central review diagnosis of ependymoma 20 80 20
central review diagnosis of anaplastic ependymoma
12 50 50
Medulloblastoma
Leary (27) 2011 1 86 neuropathologist central pathology review in Children's Cancer Group CCG-9921 trial, 1993-97
children less than age 3 diagnosed with medulloblastoma
discrepancy = patients without medulloblastoma on review
86 12 88
Neuroblastoma
Reid (28) 1996 2 421 central review: European Neuroblastoma Study Group (ENSG) study
trephine biopsy cores to evaluate bone marrow infiltration by neuroblastoma in children
graded as tumour positive or negative 712 5 95
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 7
# 2nd # Reviewer (Profession/
Training)
Sample Subtype, Change # Specimens Discrepancy, % Agreement
Author Year Reviewers Specimens Type of Review, Notes Sample Description, Notes or Item Compared of Subtype All Major Minor % Kappa
Atypical Teratoid/Rhabdoid Tumours (AT/RT)
Woehrer (29) 2010 3 202 neuropathologists, 2 reviewed all samples, plus a 3rd experienced in pediatric brain tumors reviewed all atypical teratoid/rhabdoid tumours
central histopathology review, study by the Austrian Brain Tumor Registry
newly diagnosed malignant high grade (WHO III and IV) CNS tumors in children <15 years old
high grade tumours reclassified as low-grade gliomas
tumours initially diagnosed as atypical teratoid/rhabdoid
tumours diagnosed on review as atypical teratoid/rhabdoid
Note: authors did not report discrepancy rate for all types of tumours
202
9
19
4
0
53
96
100
47
Lafay-Cousin (30) 2012 1 46 neuropathologist retrospective study through Canadian Pediatric Brain Tumour Consortium (CPBTC), central pathology review to confirm atypical teratoid rhabdoid tumours (ATRT)
review of tumour slides on patients age 0-18 with local (institutional) diagnosis of CNS ATRT
discrepancy = diagnosis of ATRT not confirmed on review
46 11 89
Studies that reported on neurologic and other cancers, specific types not indicated
Kronz (31) 1999 1 250 mandatory 2nd opinion; all cases referred to treating institution, excludes consult cases with uncertain diagnosis
major modification in therapy or prognosis, does not include change only in histologic grade or stage; limited number of cases as most were seen by the dermatology department
central nervous system 250 2.8
Raab (32) 2005 1 88 pathologist review after sign-out conferences, external review, internal QA, physician request; self-report of 100 consecutive specimens at 74 institutions
neuropathology 88 6.8 1.1 93
Renshaw (33,34) 2006, 2007
1 52 Internal review; 1/6 of cases from new pathologists, rest random
Major error leads to amendment, minor error requires no action
all discrepancies: negative, malignant, nondiagnostic, defined precursor lesions, and atypical or “suspicious.”
52 12 0.0 12
reviewer missed lesion 3.8
Lu (35) 2009 1 93 external consultation central nervous system 93 5 95
Note: The WHO classification system was revised in 2007.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 8
DISCUSSION Almost all of the included studies had secondary review by a neuropathologist,
and we believe this appropriate. In Ontario most CNS tumours are initially reviewed by a neuropathologist or pathologist with special interest in neuropathology. Secondary review is done by a neuropathologist, regardless of the qualification of the primary pathologist. The conclusion is consistent with the NCCN guideline (36), which recommends review by an experienced neuropathologist, and with the NICE) (37,38) and the CCLG (39) guidelines that recommend an MDT including a neuropathologist or histopathologist with expertise in neuro-oncology who takes part in the external neuropathology quality assurance scheme.
The articles by Bruner and by Kronz (2,31) are considered relevant to Canadian practice. The study by Bruner et al (2) is one of the most relevant as it did not use highly selected patients, and it reported on the clinical significance of discrepancies. It included consecutive cases with brain or spinal cord biopsy because neoplastic disease was suspected and found 32% discrepancy for referred patients and 47% discrepancy for samples sent for consultation. For the referred patients, there was a serious discrepancy in 6%, less serious change that could affect care or prognosis in 21%, and minor discrepancy including confirmation of tentative diagnosis or reporting of additional information in 5% of cases. Kronz et al (31) performed mandatory secondary review on all CNS specimens and found a 3% rate of errors which would modify therapy or prognosis (major errors).
Most of the other studies in Table 1 used central pathology review to verify the diagnosis for inclusion into chemotherapy or chemoradiotherapy trials and involved highly selected subgroups of patients. These studies reported relatively high discrepancies in diagnosis but did not indicate the type of sample (biopsy or resection) or clinical significance. The authors of this review considered these studies as not giving much information regarding the need for secondary pathology review in routine pathology practice.
Despite these limitations, the large discrepancy rates in CNS type or grade among all the trials support the conclusion that all CNS biopsies and resections, including samples initially evaluated to be non-diagnostic, should have a secondary pathology review. Unlike other disease sites, the brain and spinal cord are not easily accessible and, therefore, rebiopsying is uncommon. It is essential to get as much information as possible from the first biopsy, including samples considered non-diagnostic or suboptimal. Neuropathology practice is low volume/high complexity, and thus the secondary review of all samples is considered both clinically justified and feasible.
The systematic review did not include any studies on a secondary review for CNS metastases. The experience of the authors is that the secondary review changes treatment for some patients and that, due to sample complexity and low specimen volume (number of cases), it is easier to review all the samples than to determine which subset of samples would most benefit.
While no studies dealt with metastases of unknown primary or PCNSL, some special considerations are noted. Cases of unknown primary are difficult to diagnose. Some may be CNS tumours, and, therefore, secondary review by a neuropathologist should occur. As broad expertise is often required, consultation with a general anatomic pathologist or other specialist should also be considered. PCNSL cases require review by both neuropathologists and lymphoma pathologists. This is consistent with the British Neuro-Oncology Society (41) recommendation that biopsy samples of suspected PCNSL and PIOL be examined in centres or by network teams
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 9
with suitably qualified neuropathologists, hematopathologists, and ocular pathology specialists and access to relevant immunohistochemistry (IHC) and molecular techniques.
Several studies found discrepancies even among neuropathologists and involved additional neuropathologists in case of discrepancies among the primary and secondary review (2,7,15,21,28). This finding is indicative of the complexity of some of the cases. The experience of the authors is that the MDT of neuropathologists, neuro-oncologists, and neurosurgeons and others at the treatment centre works very closely together and interprets nuances and finer details that may affect treatment but are often not identified from external pathology reports. Currently all case conference and quality assurance data do not appear in patient records. While these issues may be addressed in the future, at the current time a neuropathology review at the treatment center is recommended, even for cases that have already had secondary review elsewhere. CONCLUSIONS
Secondary pathology review of CNS specimens should be conducted by a neuropathologist.
All CNS biopsies and resections, including samples initially evaluated to be non-diagnostic, should be considered for secondary pathology review.
Secondary pathology review should be considered for all CNS metastases.
Metastases with an unknown primary should have secondary pathology review by a neuropathologist. Consultation with a general anatomic pathologist or other specialist should be considered.
PCNSL cases should be reviewed by a neuropathologist and have secondary pathology review by a lymphoma pathologist.
Pathology review should be considered at the treatment centre prior to treatment.
UPDATING This series of evidence summaries on secondary pathology review will be
considered current for three years. The evidence summaries will then be designated as archived and indicated as such on the CCO website. These reports will not undergo annual assessment. They will not be updated unless required as the basis of a new guideline by the Pathology and Laboratory Medicine Program (PLMP). CONFLICT OF INTEREST
In accordance with the PEBC Conflict of Interest (COI) Policy, the authors were asked to disclose potential COIs. Potential COIs that were declared are summarized in Appendix I. The COIs declared did not disqualify any individuals from performing their designated role in the development of this review, in accordance with the PEBC COI Policy. To obtain a copy of the policy, please contact the PEBC office by email at ccopgi.mcmaster.ca
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 10
ACKNOWLEDGEMENTS AND AUTHORSHIP
The Pathology & Medicine Program and the Working Group would like to thank the following individuals for their assistance in developing this report:
Dr. John Srigley, Dr. Sandy Boag, Glenn Fletcher, Dr. Suhas Joshi, Dr. Mahmoud Khalifa, and Dr. Brendan Mullen for taking the lead in the overall pathology secondary review project.
Melissa Brouwers, Sheila McNair, Hans Messersmith, Homa Keshavarz, and Rovena Tey for providing feedback on draft versions.
Denise Kam for providing research assistance and for managing communication among the working group and with the reviewers.
Julia Shen for conducting a data audit.
Carol De Vito for copyediting.
Jennifer Hart and Dana Wilson-Li of Cancer Care Ontario. A complete list of the members of the Best Practices for Oncologic Pathology
Secondary Review: Hematologic Cancers Working Group with their affiliations and conflict of interest information is provided in Appendix 1.
Funding
The PEBC is a provincial initiative of Cancer Care Ontario supported by the Ontario Ministry of Health and Long-Term Care. All work produced by the PEBC is editorially independent from the
Ontario Ministry of Health and Long-Term Care.
Copyright This report is copyrighted by Cancer Care Ontario; the report and the illustrations herein may
not be reproduced without the express written permission of Cancer Care Ontario. Cancer Care Ontario reserves the right at any time, and at its sole discretion, to change or revoke this
authorization.
Disclaimer Care has been taken in the preparation of the information contained in this report.
Nonetheless, any person seeking to apply or consult the report is expected to use independent medical judgment in the context of individual clinical circumstances or seek out the
supervision of a qualified clinician. Cancer Care Ontario makes no representation or guarantees of any kind whatsoever regarding the report content or use or application and disclaims any
responsibility for its application or use in any way.
Contact Information For information about the PEBC and the most current version of all reports,
please visit the CCO website at http://www.cancercare.on.ca/ or contact the PEBC office at:
Phone: 905-527-4322 ext. 42822 Fax: 905 526-6775 E-mail: [email protected]

ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 11
REFERENCES
1. Browman GP, Levine MN, Mohide EA, Hayward RS, Pritchard KI, Gafni A, et al. The
practice guidelines development cycle: A conceptual tool for practice guidelines development and implementation. J Clin Oncol. 1995;13(2):502-12.
2. Bruner JM, Inouye L, Fuller GN, Langford LA. Diagnostic discrepancies and their clinical impact in a neuropathology referral practice. Cancer. 1997;79(4):796-803.
3. Aldape K, Simmons ML, Davis RL, Miike R, Wiencke J, Barger G, et al. Discrepancies in diagnoses of neuroepithelial neoplasms: The San Francisco Bay Area Adult Glioma Study. Cancer. 2000;88(10):2342-9.
4. Weller M, Muller B, Koch R, Bamberg M, Krauseneck P, Neuro-Oncology Working Group of the German Cancer Society. Neuro-Oncology Working Group 01 trial of nimustine plus teniposide versus nimustine plus cytarabine chemotherapy in addition to involved-field radiotherapy in the first-line treatment of malignant glioma. J Clin Oncol. 2003;21(17):3276-84.
5. Butowski N, Lamborn KR, Lee BL, Prados MD, Cloughesy T, DeAngelis LM, et al. A North American brain tumor consortium phase II study of poly-ICLC for adult patients with recurrent anaplastic gliomas. J Neurooncol. 2009;91(2):183-9.
6. Gupta T, Nair V, Epari S, Pietsch T, Jalali R. Concordance between local, institutional, and central pathology review in glioblastoma: Implications for research and practice: A pilot study. Neurol India. 2012;60(1):61-5.
7. Hegi ME, Janzer R-C, Lambiv WL, Gorlia T, Kouwenhoven MCM, Hartmann C, et al. Presence of an oligodendroglioma-like component in newly diagnosed glioblastoma identifies a pathogenetically heterogeneous subgroup and lacks prognostic value: Central pathology review of the EORTC_26981/NCIC_CE.3 trial. Acta Neuropathol (Berl). 2012;123(6):841-52.
8. Hargrave D, Geoerger B, Frappaz D, Pietsch T, Gesner L, Cisar L, et al. A phase II single-arm study of irinotecan in combination with temozolomide (TEMIRI) in children with newly diagnosed high grade glioma: A joint ITCC and SIOPE-brain tumour study. J Neurooncol. 2013;113(1):127-34.
9. Glotsos D, Georgiadis P, Kostopoulos S, Daskalakis A, Kalatzis I, Ravazoula P, et al. A pilot study investigating the minimum requirements necessary for grading astrocytomas remotely. Anal Quant Cytol Histol. 2009;31(5):262-8.
10. Prados MD, Scott C, Sandler H, Buckner JC, Phillips T, Schultz C, et al. A phase 3 randomized study of radiotherapy plus procarbazine, CCNU, and vincristine (PCV) with or without BUdR for the treatment of anaplastic astrocytoma: A preliminary report of RTOG 9404. Int J Radiat Oncol Biol Phys. 1999;45(5):1109-15.
11. Prados MD, Seiferheld W, Sandler HM, Buckner JC, Phillips T, Schultz C, et al. Phase III randomized study of radiotherapy plus procarbazine, lomustine, and vincristine with or without BUdR for treatment of anaplastic astrocytoma: Final report of RTOG 9404. Int J Radiat Oncol Biol Phys. 2004;58(4):1147-52.
12. Hildebrand J, Gorlia T, Kros JM, Afra D, Frenay M, Omuro A, et al. Adjuvant dibromodulcitol and BCNU chemotherapy in anaplastic astrocytoma: Results of a randomised European Organisation for Research and Treatment of Cancer phase III study (EORTC study 26882). Eur J Cancer. 2008;44(9):1210-6.
13. Allen JC, Aviner S, Yates AJ, Boyett JM, Cherlow JM, Turski PA, et al. Treatment of high-grade spinal cord astrocytoma of childhood with '8- in-1' chemotherapy and radiotherapy: A pilot study of CCG-945. J Neurosurg. 1998;88 (2):215-20.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 12
14. Hales RK, Shokek O, Burger PC, Paynter NP, Chaichana KL, Quinones-Hinojosa A, et al. Prognostic factors in pediatric high-grade astrocytoma: The importance of accurate pathologic diagnosis. J Neurooncol. 2010;99 (1):65-71.
15. MacDonald TJ, Arenson EB, Ater J, Sposto R, Bevan HE, Bruner J, et al. Phase II study of high-dose chemotherapy before radiation in children with newly diagnosed high-grade astrocytoma: Final analysis of Children's Cancer Group Study 9933. Cancer. 2005;104(12):2862-71.
16. Brada M, Hoang-Xuan K, Rampling R, Dietrich PY, Dirix LY, Macdonald D, et al. Multicenter phase II trial of temozolomide in patients with glioblastoma multiforme at first relapse. Ann Oncol. 2001;12(2):259-66.
17. Scott CB, Nelson JS, Farnan NC, Curran WJ, Jr., Murray KJ, Fischbach AJ, et al. Central pathology review in clinical trials for patients with malignant glioma. A Report of Radiation Therapy Oncology Group 83-02. Cancer. 1995;76(2):307-13.
18. Sasaki H, Zlatescu MC, Betensky RA, Johnk LB, Cutone AN, Cairncross JG, et al. Histopathological-molecular genetic correlations in referral pathologist-diagnosed low-grade "oligodendroglioma". J Neuropathol Exp Neurol. 2002;61(1):58-63.
19. Kros JM, Gorlia T, Kouwenhoven MC, Zheng P-P, Collins VP, Figarella-Branger D, et al. Panel review of anaplastic oligodendroglioma from European Organization For Research and Treatment of Cancer Trial 26951: Assessment of consensus in diagnosis, influence of 1p/19q loss, and correlations with outcome. J Neuropathol Exp Neurol. 2007;66(6):545-51.
20. Kouwenhoven MCM, Gorlia T, Kros JM, Ibdaih A, Brandes AA, Bromberg JEC, et al. Molecular analysis of anaplastic oligodendroglial tumors in a prospective randomized study: A report from EORTC study 26951. Neuro Oncol. 2009;11(6):737-46.
21. Figarella-Branger D, Metellus P, Barrie M, Maues de Paula A, Fernandez C, Polivka M, et al. Intracranial ependymomas in adult patients. Diagnosis and histological prognostic factors. [French]. Neurochirurgie. 2007;53 (2-3 SUPPL. PART 1):76-84.
22. Metellus P, Figarella-Branger D, Guyotat J, Barrie M, Giorgi R, Jouvet A, et al. Supratentorial ependymomas: Prognostic factors and outcome analysis in a retrospective series of 46 adult patients. Cancer. 2008;113(1):175-85.
23. Guyotat J, Metellus P, Giorgi R, Barrie M, Jouvet A, Fevre-Montange M, et al. Infratentorial ependymomas: Prognostic factors and outcome analysis in a multi-center retrospective series of 106 adult patients. Acta Neurochir (Wien). 2009;151(8):947-60.
24. Metellus P, Guyotat J, Chinot O, Durand A, Barrie M, Giorgi R, et al. Adult intracranial WHO grade II ependymomas: Long-term outcome and prognostic factor analysis in a series of 114 patients. Neuro Oncol. 2010;12(9):976-84.
25. Albright AL, Wisoff JH, Zeltzer P, Boyett J, Rorke LB, Stanley P, et al. Prognostic factors in children with supratentorial (nonpineal) primitive neuroectodermal tumors. A neurosurgical perspective from the Children's Cancer Group. Pediatr Neurosurg. 1995;22(1):1-7.
26. Robertson PL, Zeltzer PM, Boyett JM, Rorke LB, Allen JC, Geyer JR, et al. Survival and prognostic factors following radiation therapy and chemotherapy for ependymomas in children: A report of the children's cancer group. J Neurosurg. 1998;88 (4):695-703.
27. Leary SES, Zhou T, Holmes E, Geyer JR, Miller DC. Histology predicts a favorable outcome in young children with desmoplastic medulloblastoma: A report from the children's oncology group. Cancer. 2011;117(14):3262-7.
28. Reid MM, Roald B. Central review of bone marrow biopsy specimens from patients with neuroblastoma. J Clin Pathol. 1996;49(8):691-2.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 13
29. Woehrer A, Slavc I, Waldhoer T, Heinzl H, Zielonke N, Czech T, et al. Incidence of atypical teratoid/rhabdoid tumors in children: A population-based study by the Austrian Brain Tumor Registry, 1996-2006. Cancer. 2010;116(24):5725-32.
30. Lafay-Cousin L, Hawkins C, Carret AS, Johnston D, Zelcer S, Wilson B, et al. Central nervous system atypical teratoid rhabdoid tumours: The Canadian Paediatric Brain Tumour Consortium experience. Eur J Cancer. 2012;48(3):353-9.
31. Kronz JD, Westra WH, Epstein JI. Mandatory second opinion surgical pathology at a large referral hospital. Cancer. 1999;86(11):2426-35.
32. Raab SS, Nakhleh RE, Ruby SG. Patient safety in anatomic pathology: Measuring discrepancy frequencies and causes. Arch Pathol Lab Med. 2005;129(4):459-66.
33. Renshaw AA, Gould EW. Comparison of disagreement and amendment rates by tissue type and diagnosis: Identifying cases for directed blinded review. Am J Clin Pathol. 2006;126(5):736-9.
34. Renshaw AA, Gould EW. Measuring errors in surgical pathology in real-life practice: Defining what does and does not matter. Am J Clin Pathol. 2007;127(1):144-52.
35. Lu ZF, Yin HL, Du J, Shi QL, Li NY, Jin XZ, et al. Analysis of 12 206 cases of external pathology consultation. [Chinese]. Zhonghua bing li xue za zhi [Chinese Journal of Pathology] 2009;38(10):678-81.
36. Nabors LB, Ammirati M, Bierman PJ, Brem H, Butowski N, Chamberlain MC, et al. NCCN clinical practice guidelines in oncology (NCCN Guidelines®): Central nervous system cancers Version 1.2012. Fort Washington (PA): National Comprehensive Cancer Network; 2012 [cited 2012 May 31].
37. National Collaborating Centre for Cancer (Developed for NICE), Bridger P, Elyan S, Baker M, Britton J, Carpenter K, et al. Guidance on cancer services. Improving outcomes for people with brain and other CNS tumours. The manual. London (UK): National Institute for Health and Clinical Excellence (NICE); 2006 [cited 2012 May 31]. Available from: http://www.nice.org.uk/nicemedia/pdf/CSG_brain_manual.pdf.
38. National Collaborating Centre for Cancer (Developed for NICE). Guidance on cancer services. Improving outcomes for people with brain and other CNS tumours. The evidence review. London (UK): National Institute for Health and Clinical Excellence (NICE); 2006 [cited 2012 May 31]. Available from: http://www.nice.org.uk/nicemedia/pdf/CSG
39. Traunecker H, Mallucci C, Grundy R, Pizer B, Saran F. Children's Cancer and Leukaemia Group (CCLG): Guidelines for the management of intracranial meningioma in children and young people. Br J Neurosurg. 2008;22(1):13-25; discussion 4-5.
40. British Committee for Standards in Haematology, Marcus R, Hodson D, Coupland S, Bessell E, Mead B, et al. Guidelines on the diagnosis and management of adult patients with primary CNS lymphoma (PCNSL) and primary intra-ocular lymphoma (PIOL). London (UK): British Committee for Standards in Haematology; 2007 [cited 2012 May 31]. Guideline No.: HO/16. . Available from:
www.bcshguidelines.com/documents/PCNSL__bcsh_2007.pdf. 41. British Neuro-Oncology Society. Guidelines on the diagnosis and management of
primary CNS and intra-ocular lymphoma (PCNSL). British Neuro-Oncology Society/NCAT Rare Tumour Guidelines. London (UK): British Society for Haematology; 2011 Jun [cited 2013 Feb 15]. Available from: http://www.bnos.org.uk/documents/rare_tumours_guidelines/CNS%20Lymphoma%20Guidelines.pdf.
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 14
Appendix I. Members of the Pathology Secondary Review Working Group.
Pathology Secondary Review Working Group: Neurologic Cancer
Dr. Alexander (Sandy) Boag, Service Chief, Anatomic Pathology, Department of
Pathology, Kingston General Hospital; Associate Professor, Pathology and Molecular
Medicine, Queens University, Kingston
Dr. Sidney Croul, Head, Department of Neuropathology, Princess Margaret Hospital,
University Health Network, Toronto; Professor, Laboratory Medicine and Pathobiology,
University of Toronto
Dr. Gerard Jansen, Neuropathologist, Department of Pathology and Laboratory
Medicine, The Ottawa Hospital; Director Neuropathology Laboratory Services and
Associate Professor in Neuropathology, Department of Pathology and Laboratory
Medicine, University of Ottawa
Dr. James Perry, Neuro-oncologist and Division Head Neurology, Sunnybrook Health Sciences Centre; Associate Professor of Neurology, University of Toronto
Dr. Aaron Pollett, Pathologist, Mount Sinai Hospital, Toronto; Assistant Professor, Laboratory and Medicine and Pathobiology, University of Toronto; Chair, Pathology and Laboratory Medicine Program (PLMP), Cancer Care Ontario
Dr. John Srigley, Pathologist and Chief of Laboratory Medicine, Credit Valley Hospital, Mississauga; Professor (part-time), Pathology and Molecular Medicine, McMaster University; Chair (until April 2013), Pathology and Laboratory Medicine Program (PLMP), Cancer Care Ontario
Glenn Fletcher, Health Research Methodologist, PEBC, Cancer Care Ontario/McMaster
University, Hamilton, Ontario
Denise Kam, Research Assistant, PEBC, Cancer Care Ontario/McMaster University,
Hamilton, Ontario
Jennifer Hart, Manager - Clinical Programs, Cancer Care Ontario, Toronto, Ontario
Dana Wilson-Li, Policy and Research Analyst, Pathology and Laboratory Medicine
Program, Cancer Care Ontario, Toronto, Ontario
No conflicts of interest were declared by the Working Group members
ES 22-2-9
22-2-9 CNS Tumours Evidence Summary Page 15
Appendix II. Reproducibility studies (data not extracted).
1. Coons SW, Johnson PC, Scheithauer BW, Yates AJ, Pearl DK. Improving diagnostic
accuracy and interobserver concordance in the classification and grading of primary gliomas. Cancer. 1997;79(7):1381-93.
2. Ellison DW, Kocak M, Figarella-Branger D, Felice G, Catherine G, Pietsch T, et al. Histopathological grading of pediatric ependymoma: Reproducibility and clinical relevance in European trial cohorts. J Negat Results Biomed. 2011;10:7.
3. Giannini C, Scheithauer BW, Weaver AL, Burger PC, Kros JM, Mork S, et al. Oligodendrogliomas: Reproducibility and prognostic value of histologic diagnosis and grading. J Neuropathol Exp Neurol. 2001;60(3):248-62.
4. Gilles FH, Tavare CJ, Becker LE, Burger PC, Yates AJ, Pollack IF, et al. Pathologist interobserver variability of histologic features in childhood brain tumors: Results from the CCG-945 study. Pediatr Dev Pathol. 2008;11(2):108-17.
5. Grzybicki DM, Liu Y, Moore SA, Brown HG, Silverman JF, D'Amico F, et al. Interobserver variability associated with the MIB-1 labeling index: High levels suggest limited prognostic usefulness for patients with primary brain tumors. Cancer. 2001;92(10):2720-6.
6. Mittler MA, Walters BC, Stopa EG. Observer reliability in histological grading of astrocytoma stereotactic biopsies. J Neurosurg. 1996;85(6):1091-4.
7. Prayson RA, Agamanolis DP, Cohen ML, Estes ML, Kleinschmidt-DeMasters BK, Abdul-Karim F, et al. Interobserver reproducibility among neuropathologists and surgical pathologists in fibrillary astrocytoma grading. J Neurol Sci. 2000;175(1):33-9.
8. Prayson RA, Castilla EA, Hembury TA, Liu W, Noga CM, Prok AL. Interobserver variability in determining MIB-1 labeling indices in oligodendrogliomas. Ann Diagn Pathol. 2003;7(1):9-13.