Embed Size (px)
Citation preview

Benzodiazepine-induced reduction in activity mirrorsdecrements in cognitive and psychomotor performance
Jean Dawson1*, Julia Boyle1, Neil Stanley1, Sigurd Johnsen1, Ian Hindmarch2 and Debra J. Skene3
1HPRU Medical Research Centre, Faculty of Health and Medical Sciences, University of Surrey, Guildford, UK2Emeritus Professor, Faculty of Health and Medical Sciences, University of Surrey, Guildford, UK3Centre for Chronobiology, Faculty of Health and Medical Sciences, University of Surrey, Guildford, UK
Objective To assess whether actigraphy is sensitive to benzodiazepine-induced changes in cognitive and psychomotorperformance and sleep.Methods Healthy young volunteers (n¼ 23; 11 males), were randomised to a double-blind, placebo-controlled, crossovertrial. Actigraphy was used to record motor activity continuously. Following dosing at 18.00 h with 2.5mg lorazepam (LZP),psychomotor and cognitive assessments were made at hourly intervals post-dose for 4 h and after sleep at 14.5 h post-dose.Results Activity levels were significantly reduced after LZP for 5 h post-dose (p¼ 0.0104), during sleep (5–13 h)(p< 0.02) and the following morning, 13–14.5 h post-dose (p< 0.02). At the same time cognitive and psychomotorperformance was also significantly impaired (p< 0.05). LZP also significantly increased actigraphic sleep efficiency andsleep per cent (p< 0.02).Conclusion This study showed that activity levels were significantly reduced following dosing with a benzodiazepine andthese changes coincided with impairment of cognitive and psychomotor performance. Actigraphy, therefore, appears to beable to reflect the psychopharmacological effects of a benzodiazepine in changes in daytime function and nocturnalbehaviour, which, without waking the subject, is beyond the power of conventional psychometrics. Copyright# 2008 JohnWiley & Sons, Ltd.
key words—actigraphy; cognitive performance; psychomotor performance; benzodiazepine
INTRODUCTION
The development of actigraphy has allowedrest-activity patterns to be measured in difficultpopulation groups. Whilst polysomnography (PSG)remains the gold standard for assessing sleep, acti-graphy has offered a cheaper, less intrusive alternative,which has the added advantage of being able tomonitor rest and activity patterns for longer periods oftime in situations where an intensive in-houseassessment of sleep would be difficult.
Actigraphy is widely accepted as a non-invasivetool for assessing sleep-wake patterns in differentgroups of subjects (Ancoli-Israel et al., 2003; Littner
et al., 2003; Sadeh et al., 1995), including insomnia(Hauri and Wisbey, 1992; Lichstein et al., 2006),sleep-related breathing (Acebo and LeBourgeois,2006), children (Acebo et al., 2005), restless legs(King et al., 2005), depression (Raoux et al., 1994;Royant-Parola et al., 1986) and circadian rhythmdisorders (Lockley et al., 1999). There are howeverrelatively few studies to show that actigraphy canreliably measure the daytime and night-time effects ofa CNS drug (Stanley, 2003). Whether actigraphtechnology is sensitive to the sedating effects ofmedication and how accurately actigraphy is able totrack drug pharmacokinetics (PK) and pharmacody-namics remains to be substantiated.Traditionally the evaluation of psychotropic drug
effects has been conducted utilising psychometric testbatteries to assess daytime cognition and psychomotorfunctioning (Fairweather et al., 1996; Hindmarch,1980; Hindmarch et al., 2005) whilst night-time sleep
human psychopharmacologyHum. Psychopharmacol Clin Exp 2008; 23: 605–613.
Published online 20 June 2008 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/hup.961
*Correspondence to: J. Dawson, HPRU Medical Research Centre,Faculty of Health and Medical Sciences, University of Surrey,Egerton Road, Guildford GU2 7XP, UK. Tel: þ44-1483-689797;Fax: þ44-1483-689790. E-mail: [email protected]
Copyright # 2008 John Wiley & Sons, Ltd.
Received 28 November 2007
Accepted 14 May 2008

has been evaluated with PSG to assess changes insleep architecture (Grozinger et al., 1998; Saletu et al.,1991).Activity monitoring allows information on the same
variable for both daytime and nocturnal behaviours.Changes in daytime activity levels may reflectincreased sedation – a common unwanted side effectof some centrally acting compounds. Psychometricassessments have shown that a number of cognitivefunctions are adversely affected by increased sedationincluding information processing, memory and atten-tion (Hindmarch et al., 2001; Patat et al., 1987;Soo-ampon et al., 2004).Actigraphy has been used to assess the effect of
drugs on sleep and daytime behaviour in studies ofsedatives (Borbely et al., 1988; Mattmann et al.,1982), antidepressants (Fairweather et al., 1996;Stanley and Hindmarch, 1997; Stanley et al., 1999),hypnotics (Borbely et al., 1983; Takahashi et al.,2003), antihistamines (Hindmarch et al., 1999; Roehrset al., 2000; Shamsi et al., 2001) and stimulants(Hindmarch et al., 2000). Many hypnotics, antianxietyagents and antihistamines reduce activity duringwakefulness (Borbely et al., 1983; Takahashi et al.,2003) and impair mental ability and alertness in theacute phase of drug administration (Kawahara et al.,2002; Kiang et al., 2003). Drug-induced reduction inactivity has been studied in ‘spontaneous’ activity(Kiang et al., 2003) (i.e. activity during periods of freeactivity) and there are some data to suggest thatactigraphy is able to detect ‘hangover effects’(Borbely, 1984; Borbely et al., 1988; Kawaharaet al., 2002; Klosch et al., 2001; Stanley, 1997;Takahashi et al., 2003).The 1,4-benzodiazepines have well-known sedative
properties (van Laar et al., 2001) and a dose of 2.5mgof LZP was used in this study for its known ability todisrupt psychomotor and cognitive function. The aimof this study was to assess the utility of actigraphy inmonitoring the psychopharmacological activity of atypical benzodiazepine on daytime and night-timebehaviour.
METHODS
Study design
The data presented here were taken from a largerclinical trial involving two other experimental treat-ments but since the purpose of this report is toinvestigate the utility of a particular investigationaltechnique only the results of the study treatments forplacebo and 2.5mg lorazepam (LZP; recommended
daily dose as a hypnotic 1–2mg at bedtime) arepresented. The original design was a four-waydouble-blind crossover with each subject acting astheir own control and treatments given in accordancewith a balanced Latin-square design. Data from twoconsecutive 24 h periods are presented here for bothLZP and placebo.
Prior to dosing subjects were housed for 24 h for apre-treatment period for baseline measurements.Subjects received two single oral doses of medicationduring each study period, all treatments were suppliedin identical gelatine capsules with each oral dose takenat 18:00 h on Day 1 and repeated at 18:00 h on Day 2of each study period. The consecutive four studyperiods were separated by a 6-day washout period andthe inter-session interval between placebo and LZPranged from 6 to 20 days depending on the random-isation sequence. Psychometric tests were conductedduring the pre-treatment period (Day 1) for trainingand familiarisation, Day 1 at 08:00 and 17:00 h forbaseline and hourly after dosing commencing at19:00 h. Blood sampling for PK samples occurred onDay 2 from 18:00 to 22:00 h. Subjects were permittedto read, play board and computer games and watchtelevision during the periods of free time. The studyplan is shown in Figure 1.
Subjects
Twenty-four subjects were randomised. Data wereobtained for 23 healthy, Caucasian volunteers(11 males) with a mean age (�SD) of 27.3 (�5.3)years. Health status was determined via GeneralPractitioner (GP) consent and a medical and clinicalphysiological examination. According to the inc-lusion/exclusion criteria subjects were included in thestudy if they were non-smokers, and were moderatedrinkers of alcohol (no more than 40 g of alcohol perday), tea, coffee and caffeinated beverages (no morethan 6 cups per day) and were not taking anyconcomitant medication (except oral contraceptiveswhere applicable). Volunteers were requested toabstain from caffeine and alcohol 24 h before andon study days, alcohol and drugs of abuse non-usewere confirmed. Written informed consent wasobtained from all volunteers together with the consentof their GP to participate in the trial. The study wasapproved by the Ethics Committee of the South WestSurrey Health Authority. Volunteers were instructed toavoid late-nights and adhere to their usual time in bed(minimum 6–8 h sleep) before each of the studyperiods.
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
606 j. dawson ET AL.

MEASURES
Actigraphy
Volunteers were required to wear Actiwatches1 AW4(Cambridge Neurotechnology Ltd, UK) on theirnon-dominant wrist continuously for 3 days duringeach of the placebo and LZP study periods. Thesesmall wristwatch sized electronic devices measure andrecord physical movement with a piezo-electronicaccelerometer which detects motion and is set up torecord the integration of intensity, amount andduration of movement in all directions. A signalvoltage is generated which is converted and stored asan activity count in the memory unit of the actigraph.Activity was captured in 1min epochs and the datapooled into 30min bins. The mean activity per minutefor each 30min bin was calculated from dosing at18:00 h, and was analysed during the psychometrictesting periods in the acute phase after dosing, duringthe sleep period and immediately upon waking for anyresidual effects. Each 30min period where subjectswere permitted to choose their activity was referred toas ‘spontaneous’ activity and each 30min periodduring which the psychometric tests were performedwas referred to as ‘controlled’ activity. Motor activityduring sleep was automatically measured usingSleepwatch1 software (version 1.8) and its validatedsleep/wake algorithm (Oakley, 1997). The sleep/wakealgorithm uses the activity data recorded by theActiwatch in a series of linked calculations todetermine sleep and wakefulness. In the default
medium sensitivity setting for each 1-min epoch ascore of 40 activity counts is identified as ‘awake’whereas a score below 40 activity counts is identifiedas ‘sleep-like’. All data were captured electronically.During the sleep period activity is scored using the
algorithm to calculate the sleep variables. Minuteswhere zero activity has occurred are identified asimmobile minutes and are used to automaticallydetermine sleep start which is recorded as the time ofthe first epoch of 10 consecutive immobile minutesafter lights out. Sleep variables derived from theactigraphic data included the following: Sleeppercentage: percentage of ‘sleep-like’ activity (epochswith below 40 counts) from sleep start to sleep end,less any awake time; sleep efficiency: percentage of‘sleep-like’ activity from lights out to lights on(23:00–07:00 h), less any time awake; number of sleepbouts; and fragmentation index: calculated fromthe percentage of time spent moving and immobileminutes during sleep, higher scores> 50 indicatefragmented sleep. A sleep bout is a period ofundisturbed (by awakenings) sleep during the con-solidated sleep period. Each night will have a numberof sleep bouts and a reduction in the number of sleepbouts or the fragmentation index indicates a morerestful sleep.
Subjective evaluation
Line Analogue Rating Scales (LARS) were employedas a measure of the subjective effects of the
Figure 1. Plan to illustrate the study protocol. Drug administration (X) arrival (A) departure (D) sleep period 23:00–07:00 h, continuousactigraphy (. . .) psychometric testing (P), PK sampling 18:00–22:00 h
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
benzodiazepine-induced reduction in activity 607

medication. The mean scores of ratings of the‘tiredness’, ‘drowsiness’ and ‘alertness’ factors weretaken as a measurement of perceived sedation(Gudgeon and Hindmarch, 1983).
Psychometrics
Cognitive and psychomotor performance, measured ina 30min test battery, included a choice reaction time –HICKS H-CRT (CRT) (variables including recog-nition reaction time (RRT), motor reaction time(MRT) and total reaction time (TRT) – which is thesum of RRTandMRT) (Hindmarch and Tiplady, 1994;Sherwood and Kerr, 1993) and a continuous trackingtask (CTT) (Hindmarch, 1987; Kerr et al., 1996;Parkin et al., 1998) with variables including trackingerror (CTT-ERR) and tracking reaction time(CTT-RT) (Hindmarch et al., 1983). The cognitivetests outlined above are known to be sensitive tothe impairing effects of psychotropic compounds(Hindmarch et al., 2005; Kyriakopoulos et al., 1978).Pre-study training was provided on the psycho-
metric test battery (Parkin et al., 1999) to reducepractice and learning effects and a pre-study base-line was obtained on the day prior to dosing. Datawere collected from the psychometric tests at 1.5, 2.5,3.5, 4.5, and 14.5 h post-dose on the first day oftreatment only.
Statistical analysis
The data for the placebo and LZP were extracted fromthe larger four-treatment study and analysed separ-ately as a two-treatment data set. An analysis ofvariance was conducted with mean activity as thedependent variable; treatment and study period asfixed effects, and time (within subject and studyperiod) as a repeated measure and with SP(POW)variance-covariance matrix, with subject as a randomeffect. Baseline values, taken prior to each studyperiod, were used as a covariate to minimise any ordereffects in the study periods.Individual LZP versus placebo comparisons were
performed using the LSMEANS option for estimatingdifferences of SAS PROC MIXED (StatisticalAnalysis Software SAS1 PC, Version 9.1, SASInstitute, North Carolina, USA) which providedinformation on estimates, 95% confidence limits,and p-values for each time point. No test multiplicitysignificance adjustment was made at any stage in theanalysis. The results were analysed by the REMLmethod in SAS PROC MIXED with ‘subject’ as arandom effect, whereby the non-missing observations
for subjects with just one missing value are used in theestimation.
Comparison of the effect of LZP and placebo wasconducted separately for each day divided into threetime segments, 0–5 h (18:00–23:00 h) for acute effectsof the medication, 5–13 h (23:00–07:00 h) for evalu-ation during the overnight sleep period and 13–14.5 h(07:00–08:30 h) post-dose for residual effects.
A Pearson’s correlation matrix was produced toidentify any relationship between the activity levelsand the psychomotor performance. As data were takenfrom a larger four treatment study, a test forsignificance as an explanatory variable of the sequencecategory effect was performed, however no statisticalsignificance was found.
RESULTS
The total number of subjects that were randomisedwas 24, 1 subject was withdrawn prior to testing and2 subjects completed only one of the selectedtreatments, therefore the maximum number ofsubjects included in the analysis was 23.
Actigraphy
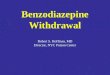
There was a significant main effect of treatmentfollowing dosing (0–5 h) on the first day of treatment(p¼ 0.0104) for LZP compared with placebo(Figure 2a). Post-hoc analysis revealed that therewas a significant effect of treatment on ‘spontaneous’activity at 3 h post-dose, with LZP reducing activitycompared with placebo (p< 0.01). Although activitylevels 0–4 h post-dose on the second day of treatmentwere also reduced overall, there was no significanteffect of treatment (Figure 2b).
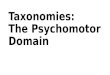
During the sleep periods 5–13 h post-dose(23:00–07:00 h) there was a significant reduction inactivity on both nights following LZP (p< 0.02 and0.001, respectively) (Figure 3a and b). For both nightspost-hoc analysis showed a significant (p< 0.001)reduction in activity compared with placebo, 5.5 hpost-dose, i.e. just after lights out. The followingmorning 13–14.5 h post-dose (07:00–08:30 h) althoughthere was a significant main effect of treatment afterthe first dose with LZP reducing (p< 0.02) activity(Figure 2a), there was no significant difference at anydistinct time point.
Sleep variables
The various actigraphically-derived sleep variables(Table 1) show that for nights 1 and 2 LZP
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
608 j. dawson ET AL.

significantly increased percentage sleep (p< 0.05)and sleep efficiency (p< 0.01) compared to placebo.LZP also significantly reduced the number of sleepbouts during both nights (p< 0.05) compared toplacebo. A trend towards a reduction in the fragmenta-tion index following LZP was observed only on night 1(p¼ 0.0633).
Cognitive and psychomotor function
The subjective evaluation of sedation was measuredwith LARS. There was a significant effect of treatmentfor the overall comparison of LZP versus placebo
(p< 0.05). Post-hoc analysis revealed a significantincrease in subjective sedation with LZP at 4.5 hpost-dose on the first night (p< 0.0001), comparedwith placebo (Figure 4a).Overall there was a significant effect of treatment on
the performance of the CRT and CTT. LZP causedsignificant increases in TRT, the response time to theperipheral stimulus component of the CTT-RT, and inthe tracking error component CTT-ERR (p< 0.0001).Post-hoc analysis revealed a significant effect of LZPcompared with placebo on the individual time points(p< 0.05) as shown in Figure 4b–d. However, therewas no significant correlation, between activity at 3 h
Figure 2. Time course of effect of placebo (&) and LZP 2.5mg (&) on activity as measured by actigraphy on (a) Day 1 and (b) Day 2.There was an overall significant effect of treatment on Day 1 (p< 0.02), post-hoc tests revealed a significant effect at 3 h post-dose(�p< 0.01) compared to placebo. Data are presented as mean�SEM (n¼ 23) (#¼ psychometric test point, controlled activity)
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
benzodiazepine-induced reduction in activity 609

post-dose and the 3.5 h post-dose time point of thecognitive performance tests although the correlationbetween CTT-ERR and activity approached signifi-cance (p¼ 0.08).
DISCUSSION
Statistically significant effects of LZP on activity,actigraphically derived sleep variables and psycho-motor performancewere observed in the present study.These current findings in agreement with otheractigraphic studies conducted with different druggroups (Kiang et al., 2003; Roehrs et al., 2000;Stanley, 1997; Stanley and Hindmarch, 1997; Taka-hashi et al., 2003) show that reduced overt behaviouralactivity detected by actigraphy is reflected in both the
Figure 3. Time course of effect of placebo (&) and LZP 2.5mg (&) on activity during sleep on (a) Night 1 and (b) Night 2 as measured byactigraphy. There was an overall significant effect of treatment (p< 0.02) on both nights, post-hoc tests revealed a significant effect at 5.5 hpost-dose (��p< 0.001) compared to placebo. 5.5 h post-dose corresponds to 23:00–23:30 h. Data are presented as mean�SEM (n¼ 23)
Table 1. Effect of LZP and placebo on actigraphic sleep variables
Variable
Night 1 Night 2
PlaceboLorazepam2.5mg Placebo
Lorazepam2.5mg
Percentage sleep 88� 1 91� 1� 89� 1 92� 1�
Number of sleepbouts
28� 2 22� 2�� 27� 2 22� 2�
Fragmentationindex
26� 2 21� 2 25� 3 21� 2
Sleep efficiency 86� 1 90� 1�� 87� 2 91� 1��
Data are provided as sleep variables calculated with the SleepwatchAlgorithm and presented as mean�SEM (n¼ 23).�p< 0.05.��p< 0.01 versus corresponding placebo.
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
610 j. dawson ET AL.

psychometric and subjective assessments of sedation,psychomotor performance, general information pro-cessing skills and arousal. There was a significanteffect of treatment on Day 1, LZP reduced activitycompared to placebo, with a statistically significantreduction at 3 h post-dose corresponding with the tmax
of the drug (Papini et al., 2006). Although this wasthe only time point that was significantly different anoverall reduction in activity compared to placebo isreflected in the shape of the curve (Figure 2a)indicating that LZP caused a global reduction inactivity levels which was indicative of the time courseof action of the drug. It is feasible that the stimulatingeffect of the cognitive and psychomotor performancetests may have masked the actual reduction in activity.
There was no overall significant effect of treatmentfollowing the second dose of LZP. During this time inplace of the psychometric tests, PK samples weretaken with subjects lying on their beds and psycho-metric tests were not performed as data would bedifficult to collect and interpret accurately. Althoughthe shape of the curve (Figure 2b) reflects an overallreduction in activity following LZP administration theconcomitant PK procedure is likely to have affectedthe activity levels in both treatments.Cognitive and psychomotor performance were also
reduced 0–5 h post-dose with significant impairmentsin performance at 2.5, 3.5 and 4.5 h (p< 0.01) forCRT-TRT, CTT-ERR and CTT-RT. Although cogni-tive performance was significantly impaired and
Figure 4. Time course of effect of placebo (&) and LZP 2.5mg (&) on (a) sedation component of LARS, (b) total reaction time (TRT) ofCRT (c) reaction time of CTT and (d) tracking error CTT-ERR. There was an overall significant effect of treatment (p< 0.05) on allpsychometric tests. Post-hoc tests revealed significant effects at 2.5, 3.5, 4.5 and 14.5 h post-dose (� p< 0.05, �� p< 0.01) compared toplacebo. Data are presented as mean�SEM (n¼ 23)
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
benzodiazepine-induced reduction in activity 611

activity levels significantly reduced during 3–3.5 hpost-dose, a Pearson’s correlation using the 3 hactivity data and the 3.5 h psychometric data failedto show any significant correlations, although thecorrelation of CTT-ERR and activity approachedsignificance (p¼ 0.08). The reason for this lack ofcorrelation is not known although it suggests thatperhaps the psychometric tests are more sensitive tochanges in performance and should be considered asthe gold standard for assessment of daytime function-ing. The current results however do show that reducedactivity levels coincided with changes in psychometricperformance and therefore may be of use in situationswhere psychometric testing is not feasible such as infield studies.In terms of night-time effects of LZP compared with
placebo a previous study showed that LZP alters sleeparchitecture as determined by PSG by reducing sleeplatency and number of awakenings, whilst increasingtotal sleep time (TST) (Saletu et al., 1990). In thepresent study the actigraphic analysis of the sleepperiod following LZP administration revealed signifi-cant reductions in activity levels at the beginning ofthe sleep period together with significant increases inthe actigraphic sleep variables of sleep efficiency andsleep per cent and significant decreases in the numberof sleep bouts. This clearly indicates that the presentactigraphy data are consistent with previous PSGfindings of the effect of LZP and highlight thebeneficial use of actigraphy in assessing objectivesleep quality.As single doses of psychoactive drugs have varied
durations of action, it is important to establish themaximum duration of impairment in order to providesafety data when prescribing. If a hypnotic taken to aidsleep has residual or hangover effects in the morningclearly this may be a safety hazard. Previous studies(Borbely et al., 1988; Mattmann et al., 1982;Takahashi et al., 2003) have shown that actigraphyis useful in providing data on residual effects, byshowing a reduction in activity levels following singledosing. In the present study activity levels were alsoreduced the morning after waking with a significantreduction in overall activity 1.5 h after waking (14.5 hpost-dose) clearly demonstrating a residual morninghangover effect of LZP 2.5mg. This hangover effectwas also confirmed by the psychomotor impairmentobserved in the morning. Interestingly, althoughsubjects demonstrated impaired cognition and activitylevels were reduced they reported no subjectivesedation on the LARS, volunteers thus being unawareof the residual effects of LZP on their ability tofunction. Actigraphy may therefore be useful in
patient studies where psychometric testing is notfeasible to investigate hangover effects as it appearsthat volunteers are not reliable in rating their ownlevels of sedation.
CONCLUSION
In conclusion, the current study provides furtherevidence that actigraphy is sensitive to the sedatingeffects of a benzodiazepine. A reduction in beha-vioural activity post-dose, during the sleep period andthe following morning confirms that actigraphy is ableto detect the acute and residual effects of a hypnoticdrug. The current data also show that actigraphy mayprovide a sensitive indication of the time course ofaction of a psychoactive drug although further fieldstudies will be necessary to fully validate this methodas a useful tool in psychopharmacology.
ACKNOWLEDGEMENTS
The data in this paper were used with the permission ofServier (France) who funded the original study carriedout at the University of Surrey, UK.
REFERENCES
Acebo C, Sadeh A, Seifer R, Tzischinsky O, Hafer A, CarskadonMA. 2005. Sleep/wake patterns derived from activity monitoringand maternal report for healthy 1- to 5-year-old children. Sleep28: 1568–1577.
Acebo C, LeBourgeois MK. 2006. Actigraphy. Respir Care ClinN Am 12: 23–30.
Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W,Pollak CP. 2003. The role of actigraphy in the study of sleep andcircadian rhythms. Sleep 26: 342–392.
Borbely AA, LoepfeM,Mattmann P, Tobler I. 1983.Midazolam andtriazolam: hypnotic action and residual effects after a singlebedtime dose. Arzneimittelforschung 33: 1500–1502.
Borbely AA. 1984. Ambulatory motor activity monitoring to studythe timecourse of hypnotic action. Br J Clin Pharmacol 18:83S–86S.
Borbely AA, Youmbi-Balderer G, Jaggi-Schwarz K. 1988. Zolpi-dem (10mg and 20mg): hypnotic action and residual effects aftera single bedtime dose. In Imidazopyridines in Sleep Disorders,Sauvenet JP, Langer SZ, Morselli PL (eds) Raven Press: NewYork; 205–210.
Fairweather DB, Ashford J, Hindmarch I. 1996. Effects of fluvox-amine and dothiepin on psychomotor abilities in healthy volun-teers. Pharmacol Biochem Behav 53: 256–259.
Grozinger M, Kogel P, Roschke J. 1998. Effects of lorazepam on theautomatic online evaluation of sleep EEG data in healthy volun-teers. Pharmacopsychiatry 31: 55–59.
Gudgeon AC, Hindmarch I. 1983. Midazolam: effects on psycho-motor performance and subjective aspects of sleep and sedation innormal volunteers. Br J Clin Pharmacol 16: 121–126.
Hauri PJ, Wisbey J. 1992. Wrist actigraphy in insomnia. Sleep 15:293–301.
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
612 j. dawson ET AL.

Hindmarch I. 1980. Psychomotor function and psychoactive drugs.Br J Clin Pharmacol 10: 189–209.
Hindmarch I, Subhan Z, Stoker MJ. 1983. The effects of zimeldineand amytriptyline on car driving and psychomotor performance.Acta Psychiatr Scand 68: 141–146.
Hindmarch I. 1987. Three antidepressants (amytriptyline, dothiepin,fluoxitine), with and without alcohol, compared to placebo ontests of psychomotor ability related to car driving. Hum Psycho-pharmacol 2: 177–183.
Hindmarch I, Tiplady B. 1994. A comparison of the psychometriceffects of remoxipride with those of haloperidol, thioridazine andlorazepam in healthy volunteers. Hum Psychopharmacol 9:43–49.
Hindmarch I, Shamsi Z, Stanley N, Fairweather DB. 1999.A double-blind, placebo-controlled investigation of the effectsof fexofenadine, loratadine and promethazine on cognitive andpsychomotor function. Br J Clin Pharmacol 48: 200–206.
Hindmarch I, Rigney U, Stanley N, Quinlan P, Rycroft J, Lane J.2000. A naturalistic investigation of the effects of day-longconsumption of tea, coffee and water on alertness, sleep onsetand sleep quality. Psychopharmacology (Berl) 149: 203–216.
Hindmarch I, Patat A, Stanley N, Paty I, Rigney U. 2001. Residualeffects of zaleplon and zolpidem following middle of the nightadministration five hours to one hour before awakening. HumPsychopharmacol 16: 159–167.
Hindmarch I, Trick L, Ridout F. 2005. A double-blind, placebo- andpositive-internal-controlled (alprazolam) investigation of the cog-nitive and psychomotor profile of pregabalin in healthy volun-teers. Psychopharmacology (Berl) 183: 133–143.
Kawahara R, Nishimura S, Inagaki Y, Taenaka N, Kawahara H.2002. Actigraphic assessment of the preoperative hypnoticeffects of brotizolam and zopiclone. Acta Anaesthesiol Belg53: 27–31.
Kerr JS, Powell J, Hindmarch I. 1996. The effects of reboxetine andamitriptyline, with and without alcohol on cognitive function andpsychomotor performance. Br J Clin Pharmacol 42: 239–241.
Kiang M, Daskalakis ZJ, Christensen BK, Remington G, Kapur S.2003. Actigraphic measurement of the effects of single-dosehaloperidol and olanzapine on spontaneous motor activity innormal subjects. J Psychiatry Neurosci 28: 293–299.
King MA, Jaffre MO, Morrish E, Shneerson JM, Smith IE. 2005.The validation of a new actigraphy system for the measurement ofperiodic leg movements in sleep. Sleep Med 6: 507–513.
Klosch G, Gruber G, Anderer P, Saletu B. 2001. Activity monitoringin sleep research, medicine and psychopharmacology. Wien KlinWochenschr 113: 288–295.
Kyriakopoulos AA, Greenblatt DJ, Shader RI. 1978. Clinical phar-macokinetics of lorazepam: a review. J Clin Psychiatry 39: 16–23.
Lichstein KL, Stone KC, Donaldson J, et al. 2006. Actigraphyvalidation with insomnia. Sleep 29: 232–239.
Littner M, Kushida CA, Anderson WM, et al. 2003. Standards ofPractice Committee of the American Academy of Sleep Medi-cine. Practice parameters for the role of actigraphy in the study ofsleep and circadian rhythms: an update for 2002. Sleep 26:337–341.
Lockley SW, Skene DJ, Arendt J. 1999. Comparison betweensubjective and actigraphic measurement of sleep and sleeprhythms. J Sleep Res 8: 175–183.
Mattmann P, Loepfe M, Scheitlin T, et al. 1982. Day-time residualeffects and motor activity after three benzodiazepine hypnotics.Arzneimittelforschung 32: 461–465.
Oakley NR. 1997. Validation with polysomnography of the Sleep-watch sleep/wake scoring algorithm used by the Actiwatch activitymonitoring system. Technical Report to Mini-Mitter Co., Inc.
Parkin C, Fairweather DB, Shamsi Z, Stanley N, Hindmarch I. 1998.The effects of cigarette smoking on overnight performance.Psychopharmacology (Berl) 136: 172–178.
Parkin C, Kerr JS, Hindmarch I. 1999. The effects of practice onchoice reaction time and critical flicker fusion threshold. HumPsychopharmacol 12: 65–70.
Patat A, Klein MJ, Hucher M. 1987. Effects of single oral doses ofclobazam, diazepam and lorazepam on performance tasks andmemory. Eur J Clin Pharmacol 32: 461–466.
Papini O, Bertucci C, da Cunha SP, dos Santos N, Lanchote V. 2006.Quantitative assay of lorazepam and its metabolite glucoronide byreverse-phase liquid chromatography-tandem mass spectrometryin human plasma and urine samples. J Pharm Biomed Anal 40:389–396.
Raoux N, Benoit O, Dantchev N, et al. 1994. Circadian pattern ofmotor activity in major depressed patients undergoing anti-depressant therapy: relationship between actigraphic measuresand clinical course. Psychiatry Res 52: 85–98.
Roehrs T, Turner L, Roth T. 2000. Effects of sleep loss on wakingactigraphy. Sleep 15: 793–797.
Royant-Parola S, Borbely AA, Tobler I, Benoit O, Widlocher D.1986. Monitoring of long-term motor activity in depressedpatients. Br J Psychiatry 149: 288–293.
Saletu B, Frey R, Grunberger J, Krupka M, Anderer P, Musch B.1990. Sleep laboratory studies on single dose effects of suriclone.Br J Clin Pharmacol 30: 703–710.
Saletu B, Frey R, Krupka M, Anderer P, Grunberger J, Wolf SR.1991. Sleep laboratory studies on the single-dose effects ofserotonin reuptake inhibitors paroxetine and fluoxetine on humansleep and awakening qualities. Sleep 14: 439–447.
Sadeh A, Hauri PJ, Kripke DF, Lavie P. 1995. The role of actigraphyin the evaluation of sleep disorders. Sleep 18: 288–302.
Shamsi Z, Kimber S, Hindmarch I. 2001. An investigation into theeffects of cetirizine on cognitive function and psychomotorperformance in healthy volunteers. Eur J Clin Pharmacol 56:865–871.
Sherwood N, Kerr JS. 1993. The reliability, validity and pharma-cosensitivity of four psychomotor tests. In Human Psychophar-macology Measures and Methods, Hindmarch I, Stonier PD(eds). John Wiley & Sons: Chichester; 4: 1–14.
Soo-ampon S, Wongwitdecha N, Plasen S, Hindmarch I, Boyle J.2004. Effects of word frequency on recall memory followinglorazepam, alcohol, and lorazepam alcohol interaction in healthyvolunteers. Psychopharmacology (Berl) 176: 420–425.
Stanley N, Hindmarch I. 1997. Actigraphy can measure antidepres-sant-induced daytime sedation in healthy volunteers. Hum Psy-chopharmacol 12: 437–443.
Stanley N. 1997. Actigraphy in psychopharmacology. In HumanPsychopharmacology Measures and Methods, Hindmarch I,Stonier PD (eds). John Wiley & Sons: Chichester; 6: 67–93.
Stanley N, Fairweather DB, Hindmarch I. 1999. Effects of fluoxetineand dothiepin on 24-hour activity in depressed patients. Neurop-sychobiology 39: 44–48.
Stanley N. 2003. Actigraphy in human psychopharmacology: Areview. Hum Psychopharmacol 18: 39–49.
Takahashi T, Okajima Y, Otsubo T, et al. 2003. Comparison ofhangover effects among triazolam, flunitrazepam and quazepamin healthy subjects: a preliminary report. Psychiatry Clin Neuro-sci 57: 303–309.
van Laar M, Volkerts E, VerbatenM. 2001. Subchronic effects of theGABA-agonist lorazepam and the 5-HT2A/2C antagonist ritan-serin on driving performance, slow wave sleep and daytimesleepiness in healthy volunteers. Psychopharmacology (Berl)154: 189–197.
Copyright # 2008 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2008; 23: 605–613.DOI: 10.1002/hup
benzodiazepine-induced reduction in activity 613