Embed Size (px)
Citation preview
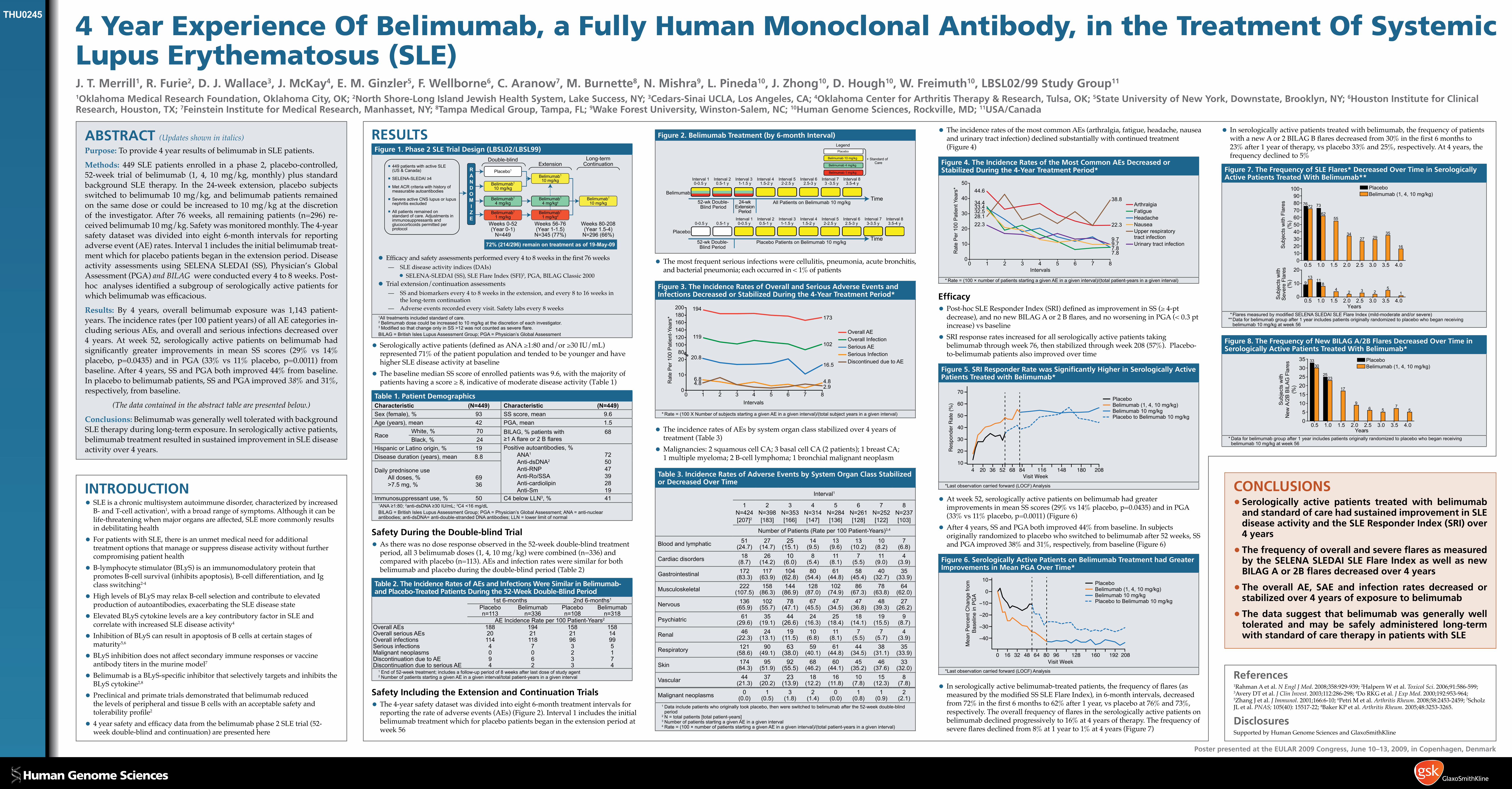
4 Year Experience Of Belimumab, a Fully Human Monoclonal Antibody, in the Treatment Of Systemic Lupus Erythematosus (SLE) J. T. Merrill1, R. Furie2, D. J. Wallace3, J. McKay4, E. M. Ginzler5, F. Wellborne6, C. Aranow7, M. Burnette8, N. Mishra9, L. Pineda10, J. Zhong10, D. Hough10, W. Freimuth10, LBSL02/99 Study Group11
1Oklahoma Medical Research Foundation, Oklahoma City, OK; 2North Shore-Long Island Jewish Health System, Lake Success, NY; 3Cedars-Sinai UCLA, Los Angeles, CA; 4Oklahoma Center for Arthritis Therapy & Research, Tulsa, OK; 5State University of New York, Downstate, Brooklyn, NY; 6Houston Institute for Clinical Research, Houston, TX; 7Feinstein Institute for Medical Research, Manhasset, NY; 8Tampa Medical Group, Tampa, FL; 9Wake Forest University, Winston-Salem, NC; 10Human Genome Sciences, Rockville, MD; 11USA/Canada
ABSTRACT (Updates shown in italics)Purpose: To provide 4 year results of belimumab in SLE patients.
Methods: 449 SLE patients enrolled in a phase 2, placebo-controlled, 52-week trial of belimumab (1, 4, 10 mg/kg, monthly) plus standard background SLE therapy. In the 24-week extension, placebo subjects switched to belimumab 10 mg/kg, and belimumab patients remained on the same dose or could be increased to 10 mg/kg at the discretion of the investigator. After 76 weeks, all remaining patients (n=296) re-ceived belimumab 10 mg/kg. Safety was monitored monthly. The 4-year safety dataset was divided into eight 6-month intervals for reporting adverse event (AE) rates. Interval 1 includes the initial belimumab treat-ment which for placebo patients began in the extension period. Disease activity assessments using SELENA SLEDAI (SS), Physician’s Global Assessment (PGA) and BILAG were conducted every 4 to 8 weeks. Post-hoc analyses identified a subgroup of serologically active patients for which belimumab was efficacious.
Results: By 4 years, overall belimumab exposure was 1,143 patient-years. The incidence rates (per 100 patient years) of all AE categories in-cluding serious AEs, and overall and serious infections decreased over 4 years. At week 52, serologically active patients on belimumab had significantly greater improvements in mean SS scores (29% vs 14% placebo, p=0.0435) and in PGA (33% vs 11% placebo, p=0.0011) from baseline. After 4 years, SS and PGA both improved 44% from baseline. In placebo to belimumab patients, SS and PGA improved 38% and 31%, respectively, from baseline.
(The data contained in the abstract table are presented below.)
Conclusions: Belimumab was generally well tolerated with background SLE therapy during long-term exposure. In serologically active patients, belimumab treatment resulted in sustained improvement in SLE disease activity over 4 years.
INTRODUCTION•SLE is a chronic multisystem autoimmune disorder, characterized by increased
B- and T-cell activation1, with a broad range of symptoms. Although it can be life-threatening when major organs are affected, SLE more commonly results in debilitating health
•For patients with SLE, there is an unmet medical need for additional treatment options that manage or suppress disease activity without further compromising patient health
•B-lymphocyte stimulator (BLyS) is an immunomodulatory protein that promotes B-cell survival (inhibits apoptosis), B-cell differentiation, and Ig class switching2-4
•High levels of BLyS may relax B-cell selection and contribute to elevated production of autoantibodies, exacerbating the SLE disease state
•Elevated BLyS cytokine levels are a key contributory factor in SLE and correlate with increased SLE disease activity4
•Inhibition of BLyS can result in apoptosis of B cells at certain stages of maturity5,6
•BLyS inhibition does not affect secondary immune responses or vaccine antibody titers in the murine model7
•Belimumab is a BLyS-specific inhibitor that selectively targets and inhibits the BLyS cytokine2,8
•Preclinical and primate trials demonstrated that belimumab reduced the levels of peripheral and tissue B cells with an acceptable safety and tolerability profile2
•4 year safety and efficacy data from the belimumab phase 2 SLE trial (52-week double-blind and continuation) are presented here
RESULTSFigure 1. Phase 2 SLE Trial Design (LBSL02/LBSL99)
Placebo1
Belimumab1
1 mg/kg
Belimumab1
4 mg/kg
Belimumab1
10 mg/kg
Belimumab1
1 mg/kg2
Belimumab1
4 mg/kg2
Belimumab1
10 mg/kg
Belimumab1
10 mg/kg
Weeks 0-52(Year 0-1)
N=449
Weeks 56-76(Year 1-1.5)
N=345 (77%)
Weeks 80-208(Year 1.5-4)
N=296 (66%)
ExtensionRANDOMIZE
Double-blind
72% (214/296) remain on treatment as of 19-May-09
Long-termContinuation449 patients with active SLE
(US & Canada)
SELENA-SLEDAI ≥4
Met ACR criteria with history ofmeasurable autoantibodies
Severe active CNS lupus or lupusnephritis excluded
All patients remained onstandard of care. Adjustments inimmunosuppressants and glucocorticoids permitted per protocol
•Efficacy and safety assessments performed every 4 to 8 weeks in the first 76 weeks — SLE disease activity indices (DAIs)•SELENA-SLEDAI (SS), SLE Flare Index (SFI)3, PGA, BILAG Classic 2000
•Trial extension/continuation assessments — SS and biomarkers every 4 to 8 weeks in the extension, and every 8 to 16 weeks in
the long-term continuation — Adverse events recorded every visit. Safety labs every 8 weeks
1All treatments included standard of care. 2 Belimumab dose could be increased to 10 mg/kg at the discretion of each investigator. 3ModifiedsothatchangeonlyinSS>12wasnotcountedassevereflare.BILAG=BritishIslesLupusAssessmentGroup;PGA=Physician’sGlobalAssessment
•Serologically active patients (defined as ANA ≥1:80 and/or ≥30 IU/mL) represented 71% of the patient population and tended to be younger and have higher SLE disease activity at baseline
•The baseline median SS score of enrolled patients was 9.6, with the majority of patients having a score ≥ 8, indicative of moderate disease activity (Table 1)
Table 1. Patient DemographicsCharacteristic (N=449) Characteristic (N=449)Sex(female),% 93 SSscore,mean 9.6Age(years),mean 42 PGA,mean 1.5
RaceWhite,% 70 BILAG,%patientswith 68
≥1Aflareor2BflaresBlack,% 24HispanicorLatinoorigin,% 19 Positiveautoantibodies,%
ANA1 72 Anti-dsDNA2 50 Anti-RNP 47 Anti-Ro/SSA 39 Anti-cardiolipin 28 Anti-Sm 19
Diseaseduration(years),mean 8.8
Dailyprednisoneuse Alldoses,% 69 >7.5mg,% 36
Immunosuppressantuse,% 50 C4belowLLN3,% 411ANA≥1:80;2anti-dsDNA≥30IU/mL;3C4<16mg/dLBILAG=BritishIslesLupusAssessmentGroup;PGA=Physician’sGlobalAssessment;ANA=anti-nuclearantibodies;anti-dsDNA=anti-double-strandedDNAantibodies;LLN=lowerlimitofnormal
Safety During the Double-blind Trial
•As there was no dose response observed in the 52-week double-blind treatment period, all 3 belimumab doses (1, 4, 10 mg/kg) were combined (n=336) and compared with placebo (n=113). AEs and infection rates were similar for both belimumab and placebo during the double-blind period (Table 2)
Table 2. The Incidence Rates of AEs and Infections Were Similar in Belimumab- and Placebo-Treated Patients During the 52-Week Double-Blind Period
1st6-months 2nd6-months1
Placebon=113
Belimumabn=336
Placebon=108
Belimumabn=318
AE Incidence Rate per 100 Patient-Years2
Overall AEs 188 194 158 158Overall serious AEs 20 21 21 14Overall infections 114 118 96 99Seriousinfections 4 7 3 5Malignant neoplasms 0 0 2 1Discontinuation due to AE 9 6 3 7Discontinuation due to serious AE 4 2 3 4
1 Endof52-weektreatment;includesafollow-upperiodof8weeksafterlastdoseofstudyagent2 NumberofpatientsstartingagivenAEinagiveninterval/totalpatient-yearsinagiveninterval
Safety Including the Extension and Continuation Trials
•The 4-year safety dataset was divided into eight 6-month treatment intervals for reporting the rate of adverse events (AEs) (Figure 2). Interval 1 includes the initial belimumab treatment which for placebo patients began in the extension period at week 56
References 1Rahman A et al. N Engl J Med. 2008;358:929-939; 2Halpern W et al. Toxicol Sci. 2006;91:586-599;
3Avery DT et al. J Clin Invest. 2003;112:286-298; 4Do RKG et al. J Exp Med. 2000;192:953-964; 5Zhang J et al. J Immunol. 2001;166:6-10; 6Petri M et al. Arthritis Rheum. 2008;58:2453-2459; 7Scholz JL et al. PNAS; 105(40): 15517-22; 8Baker KP et al. Arthritis Rheum. 2005;48:3253-3265.
Disclosures Supported by Human Genome Sciences and GlaxoSmithKline
CONCLUSIONS•Serologically active patients treated with belimumab
and standard of care had sustained improvement in SLE disease activity and the SLE Responder Index (SRI) over 4 years
•The frequency of overall and severe flares as measured by the SELENA SLEDAI SLE Flare Index as well as new BILAG A or 2B flares decreased over 4 years
•The overall AE, SAE and infection rates decreased or stabilized over 4 years of exposure to belimumab
•The data suggest that belimumab was generally well tolerated and may be safely administered long-term with standard of care therapy in patients with SLE
Poster presented at the EULAR 2009 Congress, June 10–13, 2009, in Copenhagen, Denmark
THU0245
Figure 2. Belimumab Treatment (by 6-month Interval)
Time
Belimumab
Placebo
Interval 10-0.5 y
Interval 20.5-1 y
Interval 31-1.5 y
Interval 41.5-2 y
Interval 52-2.5 y
Interval 62.5-3 y
Interval 10-0.5 y
Interval 20.5-1 y
Interval 31-1.5 y
Interval 41.5-2 y
Interval 52-2.5 y
Interval 62.5-3 y0-0.5 y 0.5-1 y
Placebo
Belimumab 1 mg/kg
Belimumab 4 mg/kg
Belimumab 10 mg/kg
Legend
+ Standard ofCare
52-wk Double-Blind Period
Placebo Patients on Belimumab 10 mg/kg
Time52-wk Double- 24-wkExtension
PeriodBlind Period
All Patients on Belimumab 10 mg/kg
Interval 73 -3.5 y
Interval 83.5-4 y
Interval 73-3.5 y
Interval 83.5-4 y
•The most frequent serious infections were cellulitis, pneumonia, acute bronchitis, and bacterial pneumonia; each occurred in < 1% of patients
Figure 3. The Incidence Rates of Overall and Serious Adverse Events and Infections Decreased or Stabilized During the 4-Year Treatment Period*
80100120140160180200
0
10
20
Intervals
Rat
e P
er 1
00 P
atie
nt-Y
ears
*
1 2 3 4 5 6 7 80
102
173
2.94.8
16.5
119
194
4.86.8
20.8
Overall AE
Serious AEOverall Infection
Serious InfectionDiscontinued due to AE
* Rate=(100XNumberofsubjectsstartingagivenAEinagiveninterval)/(totalsubjectyearsinagiveninterval)
•The incidence rates of AEs by system organ class stabilized over 4 years of treatment (Table 3)
•Malignancies: 2 squamous cell CA; 3 basal cell CA (2 patients); 1 breast CA; 1 multiple myeloma; 2 B-cell lymphoma; 1 bronchial malignant neoplasm
Table 3. Incidence Rates of Adverse Events by System Organ Class Stabilized or Decreased Over Time
Interval1
1 N=424 [207]2
2 N=398 [183]
3 N=353 [166]
4 N=314 [147]
5 N=284[136]
6 N=261[128]
7 N=252 [122]
8 N=237 [103]
NumberofPatients(Rateper100Patient-Years)3,4
Bloodandlymphatic 51(24.7)
27(14.7)
25(15.1)
14 (9.5)
13 (9.6)
13 (10.2)
10 (8.2)
7 (6.8)
Cardiac disorders 18 (8.7)
26(14.2)
10 (6.0)
8 (5.4)
11 (8.1)
7 (5.5)
11 (9.0)
4 (3.9)
Gastrointestinal 172(83.3)
117(63.9)
104(62.8)
80(54.4)
61(44.8)
58(45.4)
40(32.7)
35(33.9)
Musculoskeletal 222 (107.5)
158(86.3)
144(86.9)
128(87.0)
102 (74.9)
86(67.3)
78(63.8)
64(62.0)
Nervous 136(65.9)
102 (55.7)
78(47.1)
67(45.5)
47(34.5)
47(36.8)
48(39.3)
27(26.2)
Psychiatric 61(29.6)
35(19.1)
44(26.6)
24(16.3)
25(18.4)
18(14.1)
19(15.5)
9 (8.7)
Renal 46(22.3)
24(13.1)
19(11.5)
10 (6.8)
11 (8.1)
7 (5.5)
7 (5.7)
4 (3.9)
Respiratory 121 (58.6)
90(49.1)
63(38.0)
59(40.1)
61(44.8)
44(34.5)
38(31.1)
35(33.9)
Skin 174(84.3)
95(51.9)
92(55.5)
68(46.2)
60(44.1)
45(35.2)
46(37.6)
33 (32.0)
Vascular 44(21.3)
37(20.2)
23 (13.9)
18(12.2)
16(11.8)
10 (7.8)
15(12.3)
8 (7.8)
Malignant neoplasms 0 (0.0)
1 (0.5)
3 (1.8)
2 (1.4)
0 (0.0)
1 (0.8)
1 (0.9)
2 (2.1)
1 Dataincludepatientswhooriginallytookplacebo,thenwereswitchedtobelimumabafterthe52-weekdouble-blindperiod
2N=totalpatients[totalpatient-years]3 Number of patients starting a given AE in a given interval4Rate=(100×numberofpatientsstartingagivenAEinagiveninterval)/(totalpatient-yearsinagiveninterval)
•The incidence rates of the most common AEs (arthralgia, fatigue, headache, nausea and urinary tract infection) declined substantially with continued treatment (Figure 4)
Figure 4. The Incidence Rates of the Most Common AEs Decreased or Stabilized During the 4-Year Treatment Period*
0
10
20
30
40
50
0 1 2 3 4 5 6 7 8Intervals
Rat
e P
er 1
00 P
atie
nt Y
ears
* 44.6
34.433.432.528.122.3
Arthralgia
Headache
Upper respiratorytract infectionUrinary tract infection
Fatigue
Nausea
38.8
22.3
9.79.77.87.8
*Rate=(100×numberofpatientsstartingagivenAEinagiveninterval)/(totalpatient-yearsinagiveninterval)
Efficacy
•Post-hoc SLE Responder Index (SRI) defined as improvement in SS (≥ 4-pt decrease), and no new BILAG A or 2 B flares, and no worsening in PGA (< 0.3 pt increase) vs baseline
•SRI response rates increased for all serologically active patients taking belimumab through week 76, then stabilized through week 208 (57%). Placebo-to-belimumab patients also improved over time
Figure 5. SRI Responder Rate was Significantly Higher in Serologically Active Patients Treated with Belimumab*
Res
pond
er R
ate
(%)
4 20 36 52 68 84 116 148 180 20810
20
30
40
50
60
70
Visit Week
PlaceboBelimumab (1, 4, 10 mg/kg)Belimumab 10 mg/kgPlacebo to Belimumab 10 mg/kg
*Lastobservationcarriedforward(LOCF)Analysis
•At week 52, serologically active patients on belimumab had greater improvements in mean SS scores (29% vs 14% placebo, p=0.0435) and in PGA (33% vs 11% placebo, p=0.0011) (Figure 6)
•After 4 years, SS and PGA both improved 44% from baseline. In subjects originally randomized to placebo who switched to belimumab after 52 weeks, SS and PGA improved 38% and 31%, respectively, from baseline (Figure 6)
Figure 6. Serologically Active Patients on Belimumab Treatment had Greater Improvements in Mean PGA Over Time*
10
Visit Week
Mea
n Pe
rcen
t Cha
nge
from
Base
line
in P
GA
0 16 32 48 64 80 96 128 160 192 208
−40
−30
−20
−10
0PlaceboBelimumab (1, 4, 10 mg/kg)Belimumab 10 mg/kgPlacebo to Belimumab 10 mg/kg
*Lastobservationcarriedforward(LOCF)Analysis
•In serologically active belimumab-treated patients, the frequency of flares (as measured by the modified SS SLE Flare Index), in 6-month intervals, decreased from 72% in the first 6 months to 62% after 1 year, vs placebo at 76% and 73%, respectively. The overall frequency of flares in the serologically active patients on belimumab declined progressively to 16% at 4 years of therapy. The frequency of severe flares declined from 8% at 1 year to 1% at 4 years (Figure 7)
•In serologically active patients treated with belimumab, the frequency of patients with a new A or 2 BILAG B flares decreased from 30% in the first 6 months to 23% after 1 year of therapy, vs placebo 33% and 25%, respectively. At 4 years, the frequency declined to 5%
Figure 7. The Frequency of SLE Flares* Decreased Over Time in Serologically Active Patients Treated With Belimumab**
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.00
102030405060708090
100
7672 73
6255
3427 29
35
16Sub
ject
s w
ith F
lare
s(%
)
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.00
10
20
913
811
42 3 2
51
Years
Sub
ject
s w
ithS
ever
e Fl
ares
(%)
PlaceboBelimumab (1, 4, 10 mg/kg)
*FlaresmeasuredbymodifiedSELENASLEDAISLEFlareIndex(mild-moderateand/orsevere) **Dataforbelimumabgroupafter1yearincludespatientsoriginallyrandomizedtoplacebowhobeganreceiving
belimumab10mg/kgatweek56
Figure 8. The Frequency of New BILAG A/2B Flares Decreased Over Time in Serologically Active Patients Treated With Belimumab*
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.005
101520253035 33
30
2523
17
96 5
75
Years
Sub
ject
s w
ithN
ew A
/2B
BIL
AG
Fla
res
(%)
PlaceboBelimumab (1, 4, 10 mg/kg)
*Dataforbelimumabgroupafter1yearincludespatientsoriginallyrandomizedtoplacebowhobeganreceivingbelimumab10mg/kgatweek56





























