Embed Size (px)
DESCRIPTION
Benign Disease of the Genital Tract
Citation preview
Benign Gynecologic Lesions
By Dr Hossam El Sokkary
Lecturer of obst&gynaecology
Benign Lesions of the Genital
Tract
• lesions of the vulva, vagina, cervix, uterine corpus, ovaries and fallopian tubes
Benign Characteristics:1. slow-growing2. well-circumscribed 3. not associated with hemorrhage, necrosis or evidence of
widespread dissemination (metastasis)4. no constitutional signs and symptoms of weight loss and
anorexia
• a tissue biopsy is needed to make a specific diagnosis.
Topic Objectives
1. To describe and discuss the more common lesions and conditions of the female genital tract
2. To discuss their pathophysiology, as well as their corresponding treatment
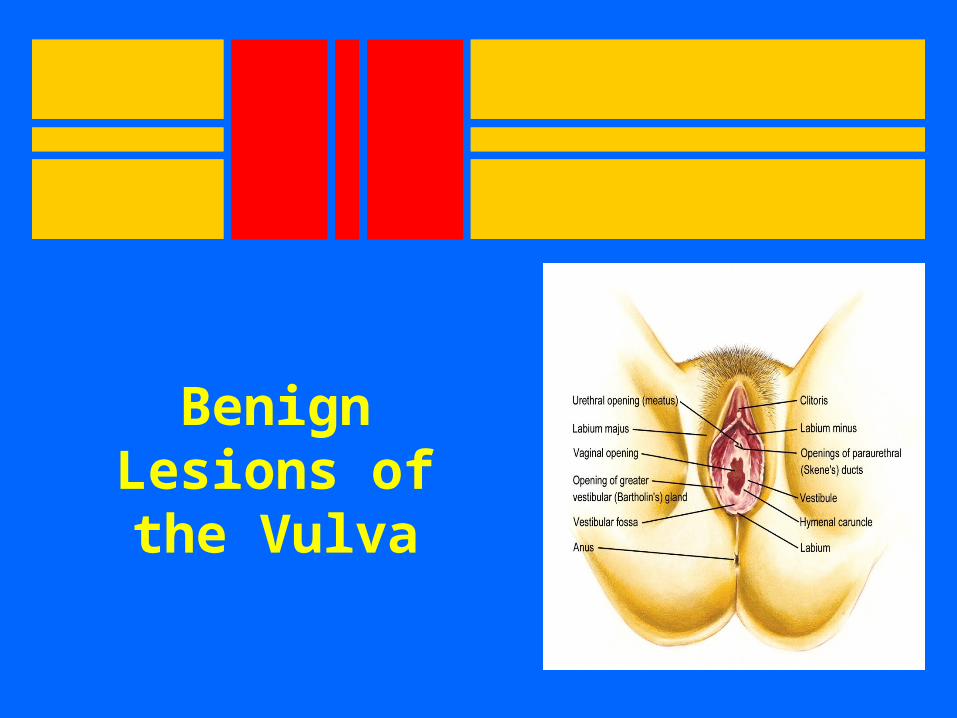
Benign Lesions of the
Vulva
Urethral Caruncle
• fleshy outgrowth of the distal edge of the urethra• frequently in postmenopausal women • must be differentiated from urethral carcinomas • generally small, single and sessile but may be
pedunculated and grow to be 1 to 2 cm in diameter
• tissue is soft, smooth, friable and bright red and initially appears as an eversion of the urethra
Urethral Caruncle
• believed to arise from an ectropion of the posterior urethral wall associated with retraction and atrophy of the postmenopausal vagina
• histologically composed of transitional and stratified squamous epithelium with loose connective tissue
Urethral Caruncle
• Growth is secondary to chronic irritation
• Symptoms may be variable– mostly asymptomatic– dysuria frequency, and urgency
Urethral Caruncle
• differential diagnosis• primary carcinoma of the urethra • prolapse of the urethral mucosa
• not a precursor for urethral carcinoma
• diagnosis is established by biopsy under local anesthesia
Urethral Caruncle
Treatment– Initially
1. oral or topical estrogen 2. avoidance of irritation
– cryosurgery, laser therapy, fulguration, or operative excision
– following operative destruction - a foley catheter should be left in place for 48 to 72 hours
– follow-up is necessary to ensure that the patient does not develop urethral stenosis
Urethral Prolapse
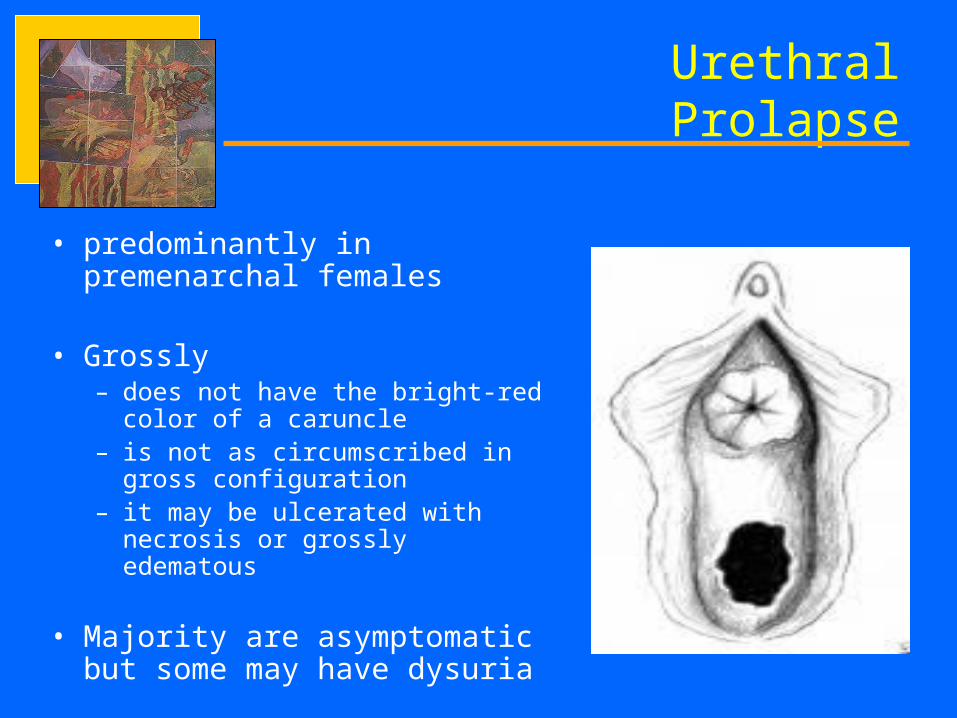
• predominantly in premenarchal females
• Grossly– does not have the bright-red color of
a caruncle – is not as circumscribed in gross
configuration – it may be ulcerated with necrosis or
grossly edematous
• Majority are asymptomatic but some may have dysuria
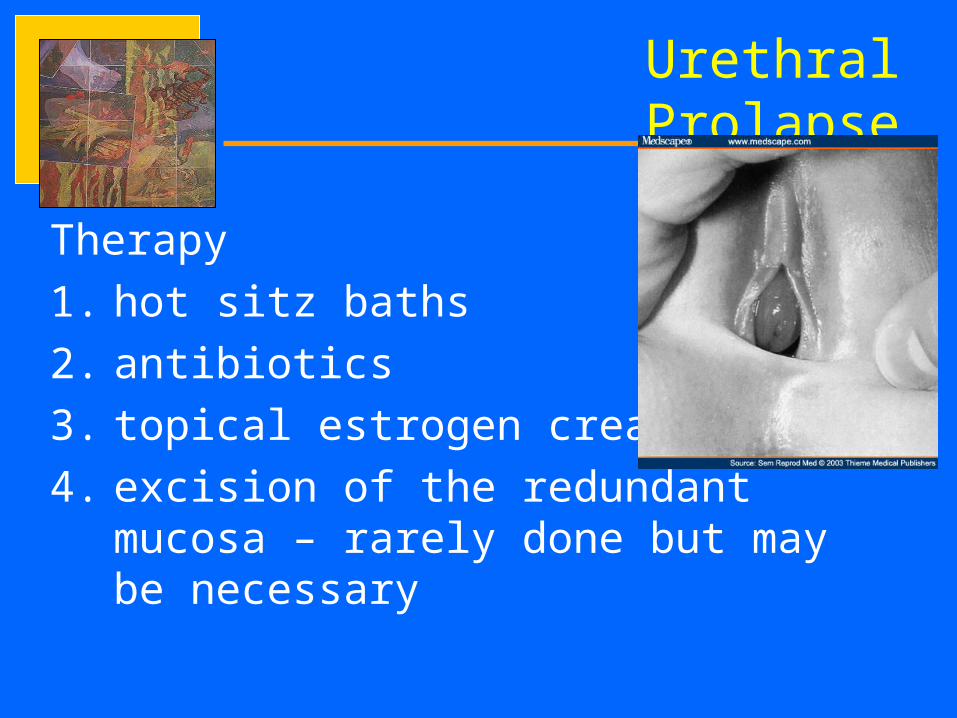
Urethral Prolapse
Therapy
1. hot sitz baths
2. antibiotics
3. topical estrogen cream
4. excision of the redundant mucosa – rarely done but may be necessary
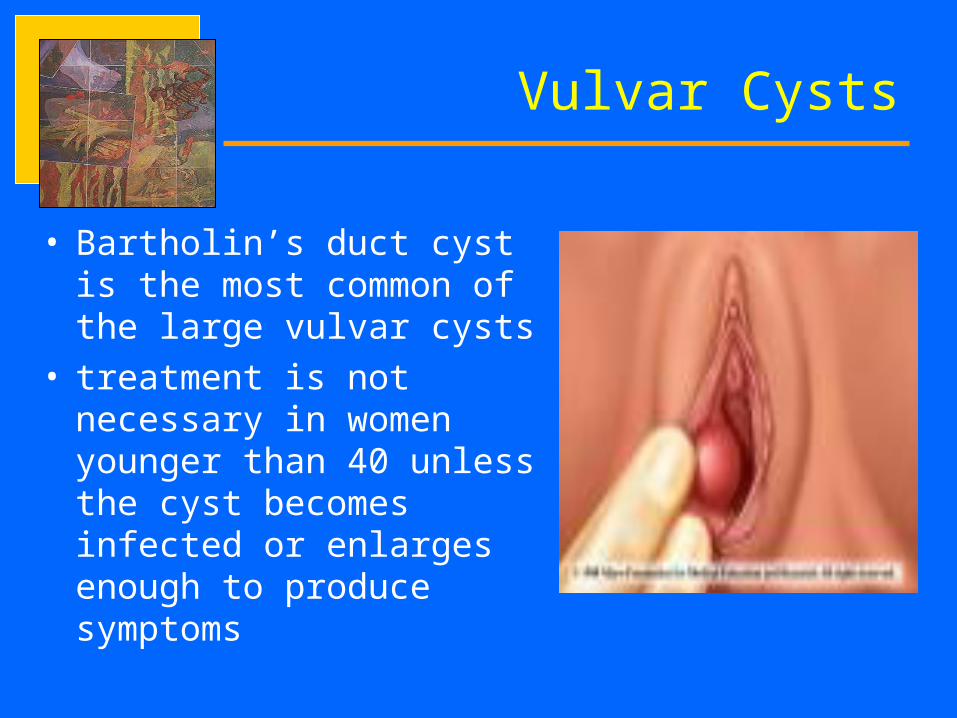
Vulvar Cysts
• Bartholin’s duct cyst is the most common of the large vulvar cysts
• treatment is not necessary in women younger than 40 unless the cyst becomes infected or enlarges enough to produce symptoms
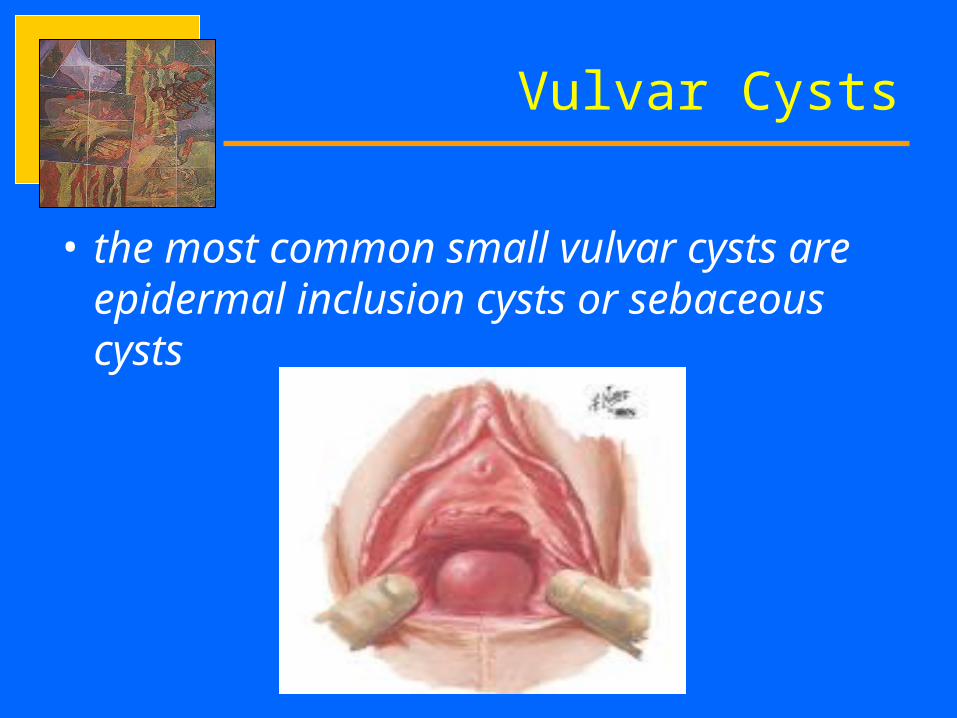
Vulvar Cysts
• the most common small vulvar cysts are epidermal inclusion cysts or sebaceous cysts
Sebaceous Cysts
• located immediately beneath the epidermis• mostly discovered on the anterior half of the
labia majora• multiple, freely movable, round, slow growing,
and nontender with firm consistency• grossly appear white or yellow with caseous
contents on cut section• local scarring of the adjacent skin sometimes
occurs when rupture of the contents of the cyst produces inflammatory reaction in the subcutaneous tissue.
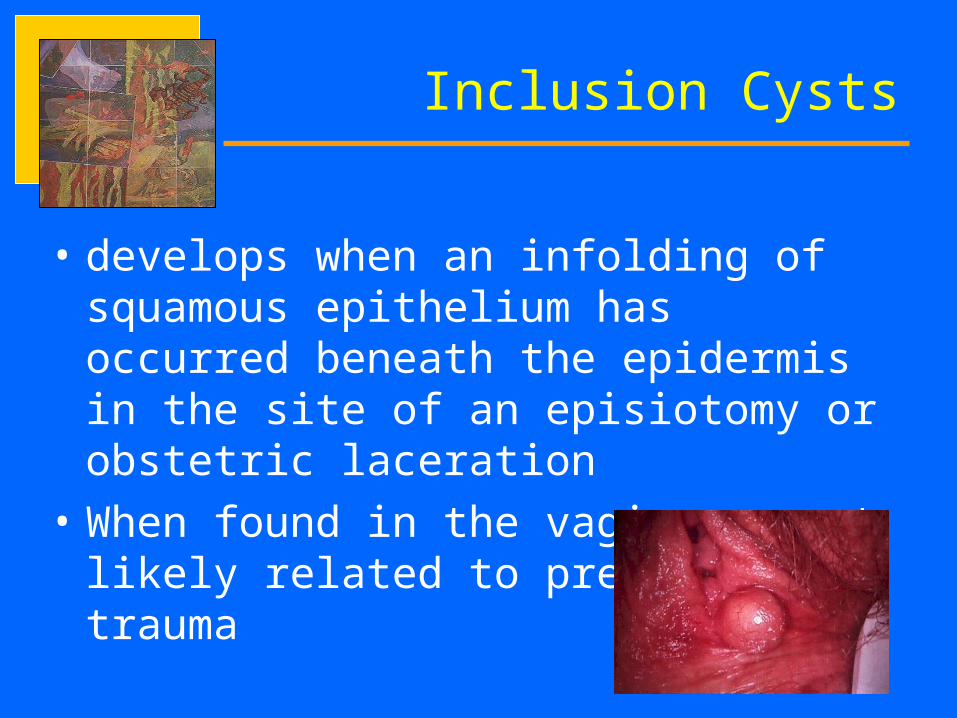
Inclusion Cysts
• develops when an infolding of squamous epithelium has occurred beneath the epidermis in the site of an episiotomy or obstetric laceration
• When found in the vagina – most likely related to previous trauma
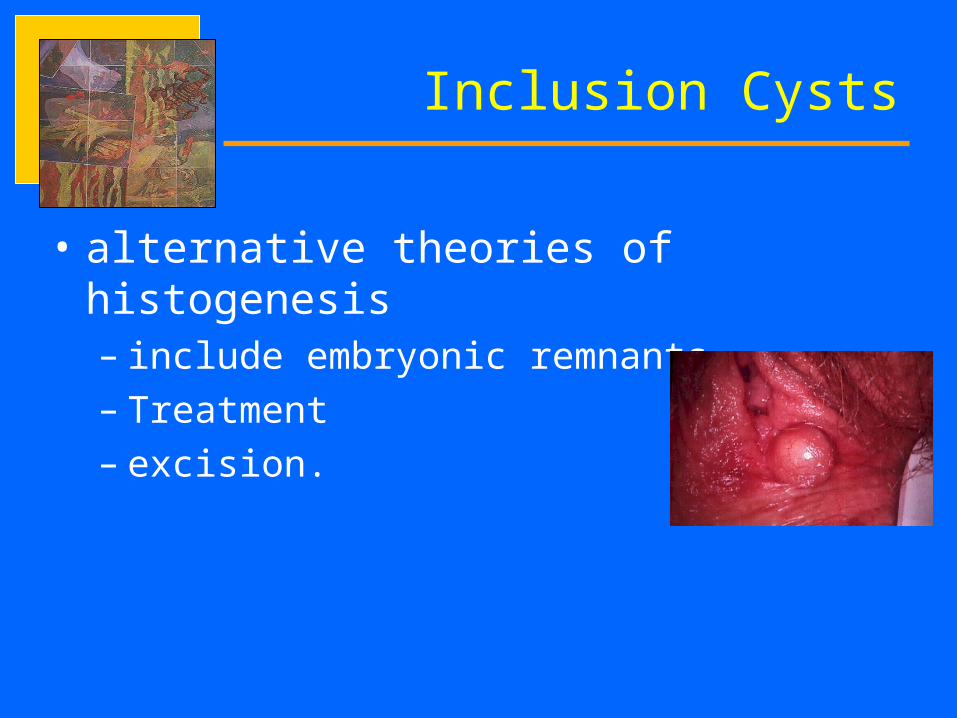
Inclusion Cysts
• alternative theories of histogenesis – include embryonic remnants – Treatment– excision.
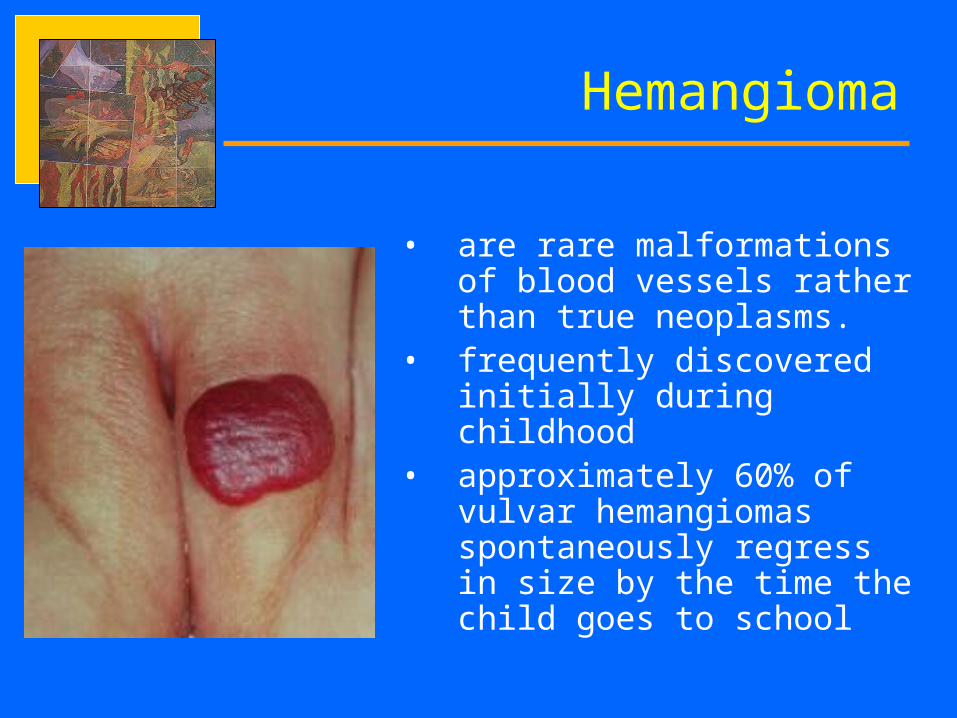
• are rare malformations of blood vessels rather than true neoplasms.
• frequently discovered initially during childhood
• approximately 60% of vulvar hemangiomas spontaneously regress in size by the time the child goes to school
Hemangioma
• appear histologically as predominantly thin-walled capillaries arranged randomly and separated by thin connective tissue septa.
• most are asymptomatic
• may occasionally become ulcerated and bleed
Hemangioma
Fibroma
• most common benign solid tumor of the vulva• commonly found in the labia majora• occur in all age groups• have smooth surface and distinct contour• with low grade potential for becoming malignant• smaller fibromas are asymptomatic • large tumors may produce chronic pressure
symptoms or acute pain• treatment - operative removal if the fibromas
are symptomatic and/or continue to grow

Lipoma
• benign, slow growing, circumscribed tumors of fat cells arising from the subcutaneous tissue of the vulva.
• second most frequent benign vulvar mesenchymal tumor
• most lipomas are discovered in the labia majora and are superficial in location
• malignant potential is extremely low
Endometriosis
• Rare in the vulva• firm, small nodule or nodules • varies from a few millimeters to several centimeters in
diameter • found at the site of an old, healed obstetric laceration,
episiotomy site, an area of operative removal of a Bartholin’s cyst, or along the canal of Nuck
• Pathophysiology– secondary to metaplasia– retrograde lymphatic spread,
Endometriosis
• commonly present with introital pain and dyspareunia
• classic history - cyclic discomfort and enlargement of the mass during menses
• Treatment– wide excision or laser vaporization depending
on the size of the mass
• Recurrence after treatment are common

Hematoma
• usually secondary to blunt trauma - (straddle injury)
• spontaneous hematomas are rare and usually occur from rupture of a varicose vein during pregnancy or the postpartum period
Hematoma
• Management – usually conservative unless the hematoma is
greater than 10 cm in diameter or is rapidly expanding
– direct pressure may be applied to control the bleeding
– compression and application of an ice pack to the area
– Identification and ligation of bleeders if the hematoma continues to expand
Dermatologic Lesions
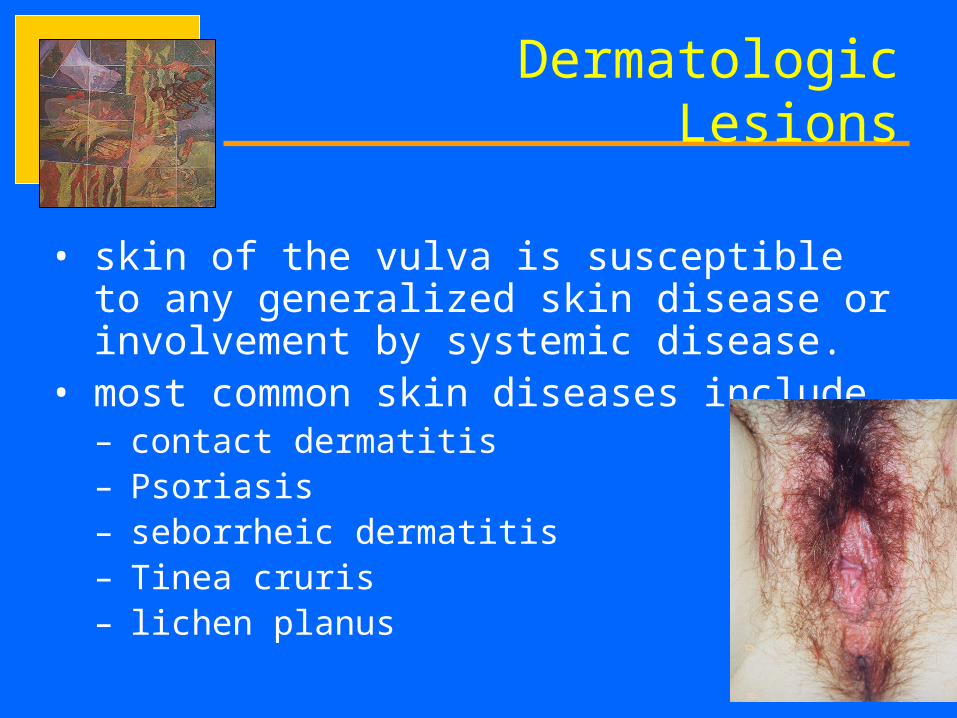
• skin of the vulva is susceptible to any generalized skin disease or involvement by systemic disease.
• most common skin diseases include– contact dermatitis– Psoriasis– seborrheic dermatitis– Tinea cruris – lichen planus
Dermatologic Lesions
• majority are scalelike rashes and usually presents with pruritus
• diagnosis and treatment are often obscured or modified by the environment of the vulva
Vulvar Edema
• may be a symptom of either local or generalized disease
• Most common causes:– secondary reaction to inflammation
– lymphatic blockage
Benign Lesions of the
Vagina
Urethral Diverticulum
• a saclike projection arising from the posterior urethra• often present as a mass of the anterior vaginal wall• symptoms are identical to lower urinary tract infection
• Diagnosis:• ascending cystourethrography • cystourethroscopy. • Treatment:
– Excisional surgery in acute infection
Inclusion Cyst
• most common cystic structures of the vagina• usually discovered in the posterior or lateral
walls of the lower third of the vagina• common in parous women• often results from birth trauma or gynecologic
surgery• majority are asymptomatic• if symptomatic, excisional biopsy is indicated
Tampon Problems
• risks with its usage:– vaginal ulcers– toxic shock syndrome from toxins produced by
Staphylococcus aureus
• associated with microscopic epithelial changes• the classic “forgotten” tampon presents with a
foul vaginal discharge and occasional spotting• Treatment: broad spectrum antibiotic
Local Trauma
• Coitus is the most frequent etiology
• most common injury is a transverse tear of the posterior fornix
• Manifests with profuse or prolonged vaginal bleeding
• Management: – prompt suturing under adequate anesthesia
Benign Lesions of the
Cervix
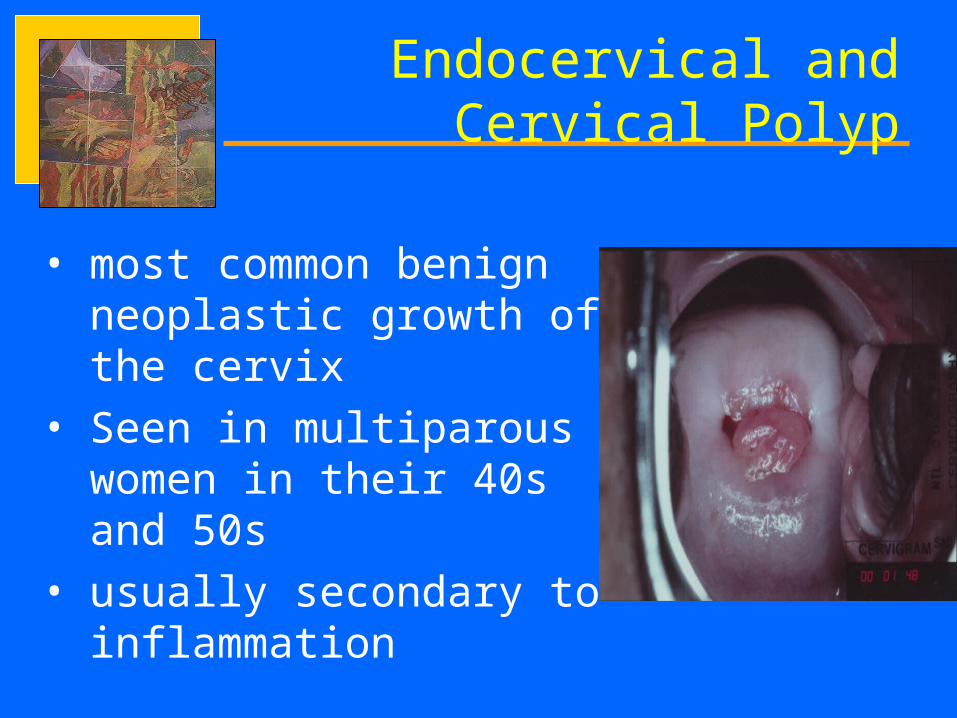
Endocervical and Cervical Polyp
• most common benign neoplastic growth of the cervix
• Seen in multiparous women in their 40s and 50s
• usually secondary to inflammation
Endocervical and Cervical Polyp
• Symptoms– classic symptom is intermenstrual bleeding– many are asymptomatic – recognized for the first time during a routine
speculum examination
Endocervical and Cervical Polyp
• Management– Polypectomy may be an office procedure– most can be managed by grasping the base of the
polyp with an appropriately sized clamp. – The polyp is avulsed with a twisting motion and sent
to the pathology for microscopic evaluation.– if bleeding ensues, the base may be treated with
chemical cautery, electrocautery, or cryocautery
Nabothian Cysts
• so common that they are considered a normal feature of the adult cervix
• retention cysts of endocervical glands occurring due to obstruction of the gland duct
• asymptomatic
Cervical Lacerations
• frequently occur with both normal and abnormal deliveries• vary from minor superficial lacerations to extensive full-
thickness lacerations
Management• Acutely bleeding cervical lacerations should be suturedComplications• extensive cervical lacerations especially those involving the
endocervical stroma may lead to incompetence of the cervix during a subsequent pregnancy
Cervical Myomas
• smooth, firm masses similar to myomas of the uterus
• may become pedunculated and protrude through the external os of the cervix
• diagnosis is by inspection and palpation
management – observation/ expectant management– medical therapy with GnRH agonists – myomectomy or hysterectomy
Cervical Stenosis
• most often occurs in the region of the internal os
• may be divided into congenital or acquired• causes of acquired cervical stenosis:
– Operative (i.e. cone biopsy, cautery)– Radiation– Infection– Neoplasia
Cervical Stenosis
Symptoms– in premenopausal women: dysmenorhea,
pelvic pain, amenorrhea and infertility– postmenopausal women are usually
asymptomatic– diagnosis is established by inability to
introduce a 1 to 2 mm dilator into the uterine cavity
Benign Lesions of the
Uterus
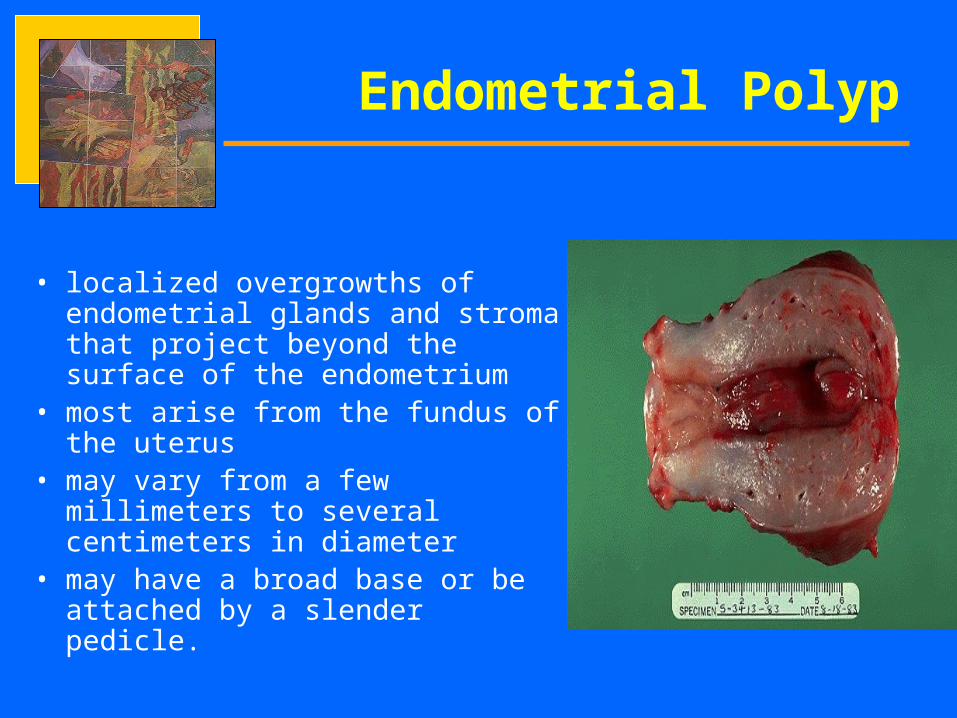
• localized overgrowths of endometrial glands and stroma that project beyond the surface of the endometrium
• most arise from the fundus of the uterus
• may vary from a few millimeters to several centimeters in diameter
• may have a broad base or be attached by a slender pedicle.
Endometrial Polyp
• peak incidence between ages 40 and 49• associated with endometrial hyperplasia
– unopposed estrogen may be the cause– May be associated with chronic administration
of tamoxifen
• majority are asymptomatic• those that are symptomatic are associated
with a wide range of abnormal bleeding patterns.
Endometrial Polyp
Components 1. endometrial glands
2. endometrial stroma
3. central vascular channels
Endometrial Polyp
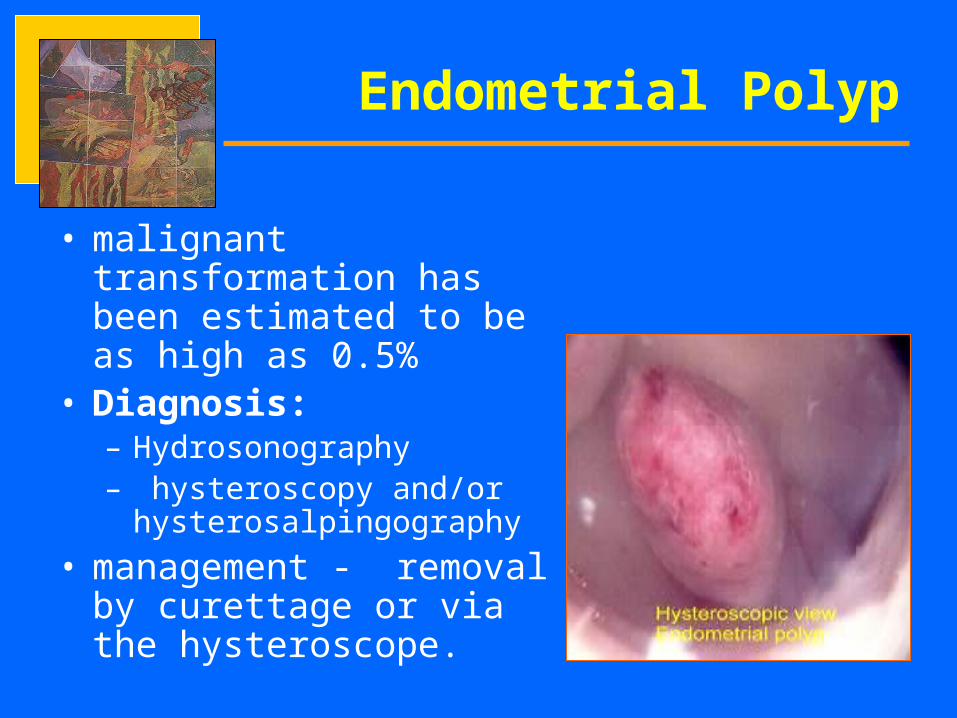
• malignant transformation has been estimated to be as high as 0.5%
• Diagnosis:– Hydrosonography– hysteroscopy and/or
hysterosalpingography
• management - removal by curettage or via the hysteroscope.
Endometrial Polyp
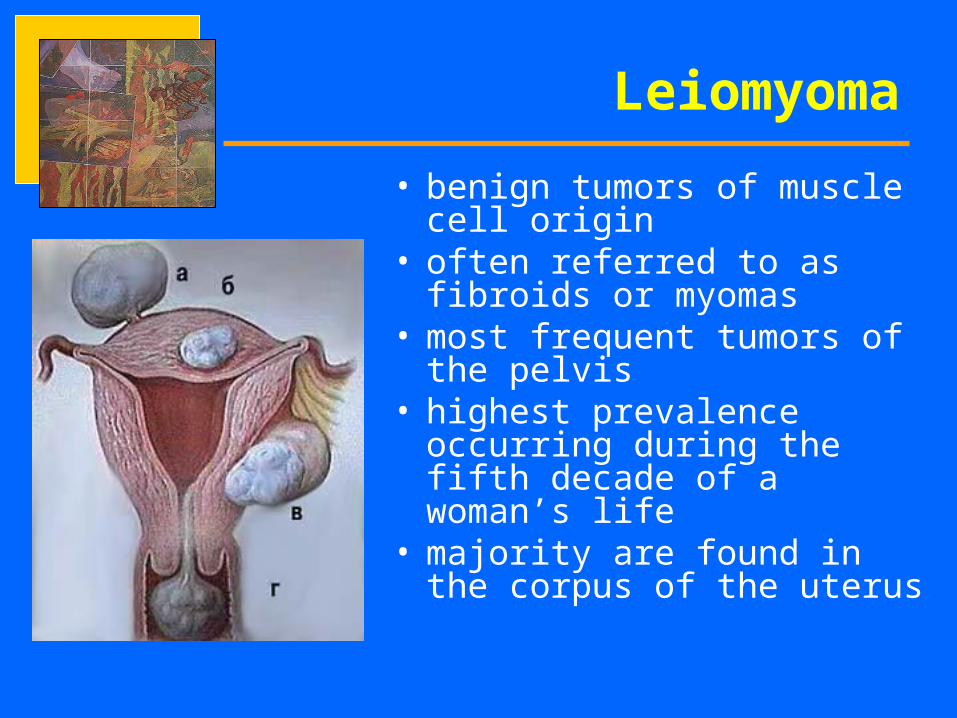
• benign tumors of muscle cell origin
• often referred to as fibroids or myomas
• most frequent tumors of the pelvis
• highest prevalence occurring during the fifth decade of a woman’s life
• majority are found in the corpus of the uterus
Leiomyoma
Leiomyoma
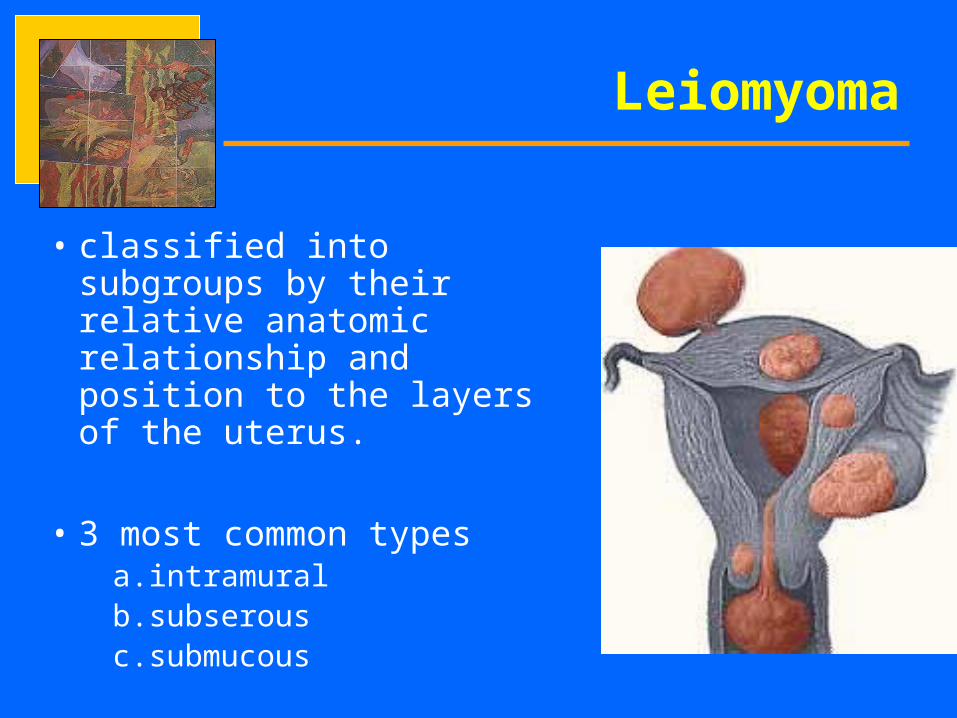
• classified into subgroups by their relative anatomic relationship and position to the layers of the uterus.
• 3 most common types a.intramuralb.subserousc.submucous
Leiomyoma
• submucosal tumors – associated with abnormal vaginal bleeding or
distortion of the uterine cavity that may produce infertility or abortion
• subserosal myomas give the uterus its knobby contour during pelvic examination
• parasitic myoma - myoma that outgrows its blood supply and obtains a secondary blood supply from another organ
• broad ligament myoma – results from lateral growth of myoma
Leiomyoma
Etiology
• each tumor results from an original single muscle cell (monoclonal theory)
• somatic mutation of normal myometrium to leiomyomas influenced by estrogen.
Leiomyoma
• never before menarche
• most diminish in size following menopause with the reduction of a significant amount of circulating estrogen.
• often enlarge during pregnancy and occasionally enlarge secondary to oral contraceptive therapy.
Leiomyoma
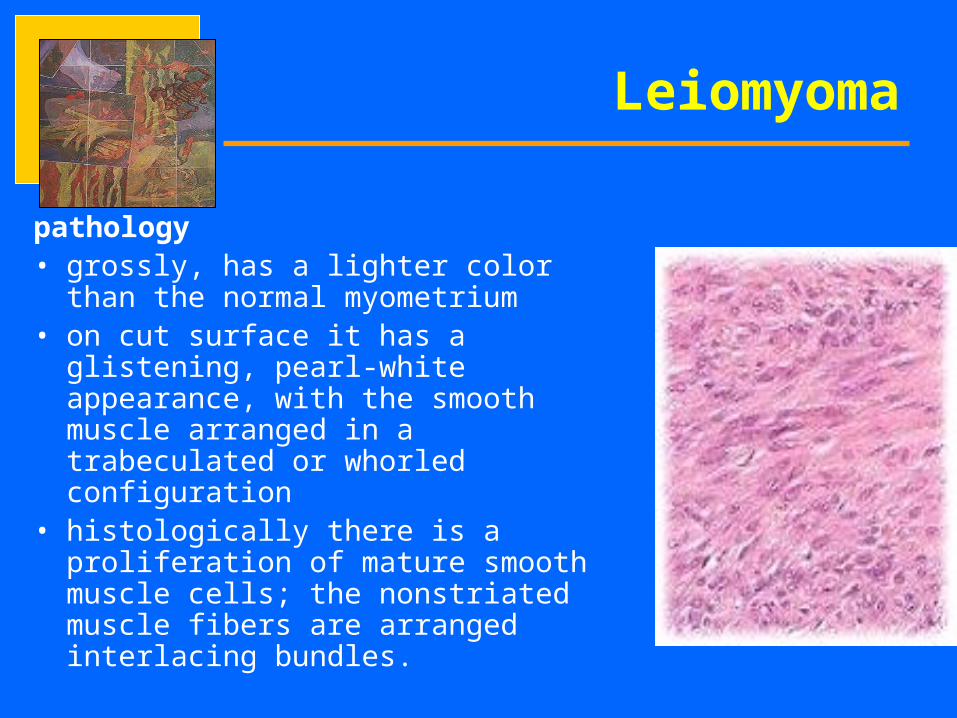
pathology• grossly, has a lighter color than the
normal myometrium• on cut surface it has a glistening, pearl-
white appearance, with the smooth muscle arranged in a trabeculated or whorled configuration
• histologically there is a proliferation of mature smooth muscle cells; the nonstriated muscle fibers are arranged interlacing bundles.
Leiomyoma
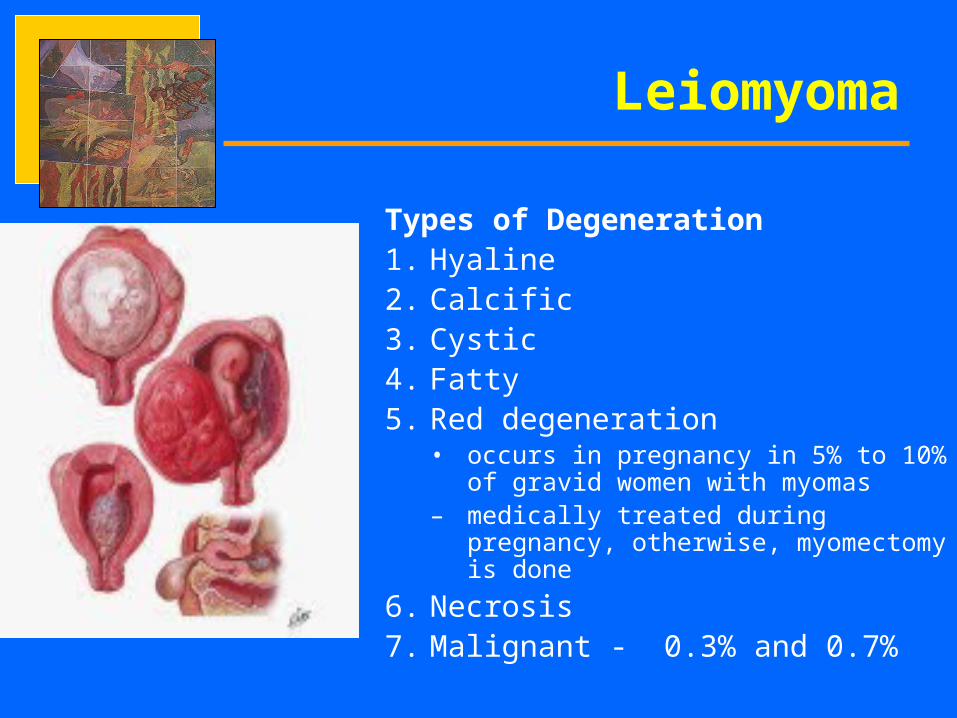
Types of Degeneration1. Hyaline2. Calcific3. Cystic4. Fatty5. Red degeneration
• occurs in pregnancy in 5% to 10% of gravid women with myomas
– medically treated during pregnancy, otherwise, myomectomy is done
6. Necrosis7. Malignant - 0.3% and 0.7%
Leiomyoma
symptoms• most common are pressure from an enlarging
pelvic mass, pain and abnormal uterine bleeding• severity of symptoms is usually related to the
number, location, and size of the myomas• majority are asymptomatic• rapid growth after menopause is a disturbing
symptom
Leiomyoma
diagnosis1. pelvic examination2. Ultrasound
management• if small, symptomatic, judicious observation is made• at first discovery, a pelvic examination at 6 month
intervals to determine the rate of growth should be done• women with abnormal bleeding and leiomyomas should
be investigated thoroughly for concurrent problems such as endomterial hyperplasia
• surgery when persistently symptomatic
Leiomyoma
Medical Management• Medical treatment involves reduction in the size of the myoma by
reducing the level of estrogen and progesterone• e.g.GnRh agonists
Advantages1. Facilitate easier surgery2. induction of amenorrhea
Disadvantages1. degeneration of some leiomyomas, necessitating piece-meal
enucleation at myomectomy2. hypoestrogenic side effects (e.g. trabecular bone loss, vasomotor
flushes)3. cost
Leiomyoma
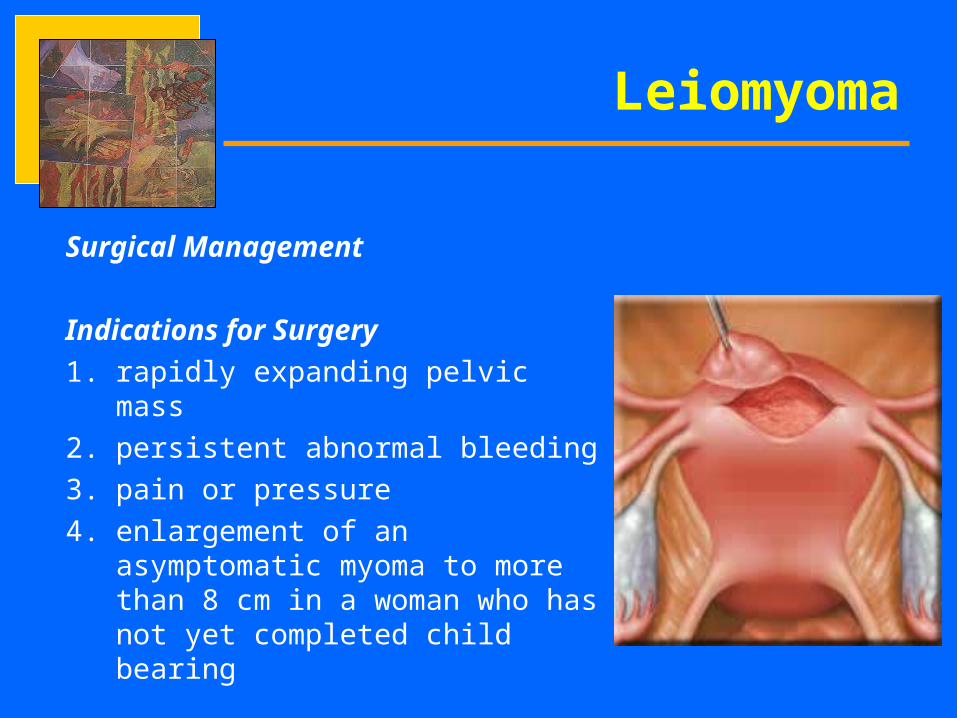
Surgical Management
Indications for Surgery
1. rapidly expanding pelvic mass
2. persistent abnormal bleeding
3. pain or pressure
4. enlargement of an asymptomatic myoma to more than 8 cm in a woman who has not yet completed child bearing
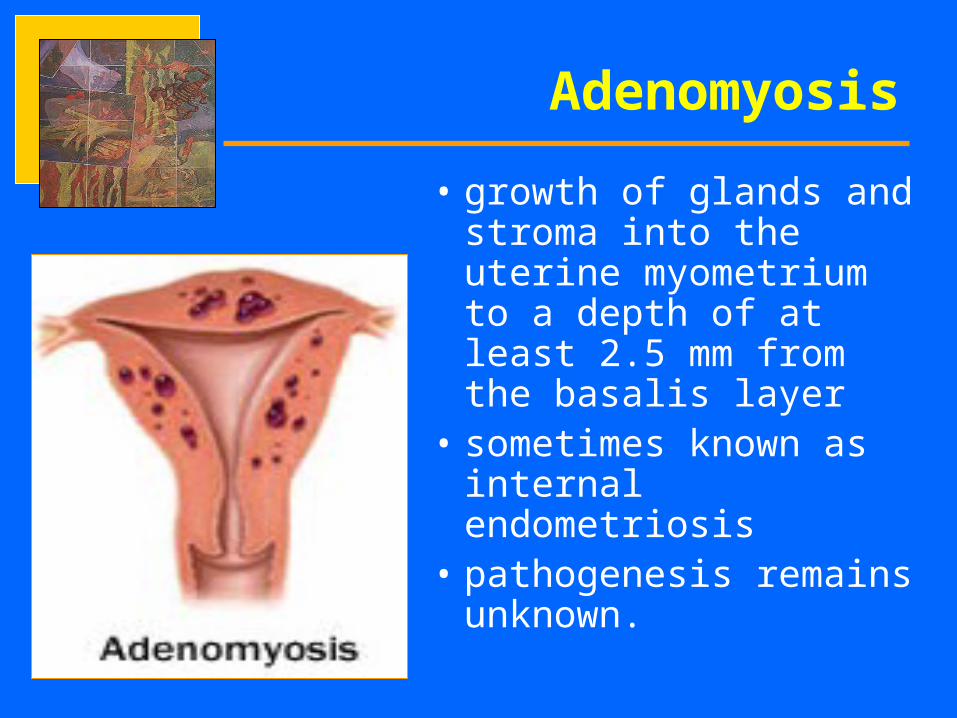
• growth of glands and stroma into the uterine myometrium to a depth of at least 2.5 mm from the basalis layer
• sometimes known as internal endometriosis
• pathogenesis remains unknown.
Adenomyosis
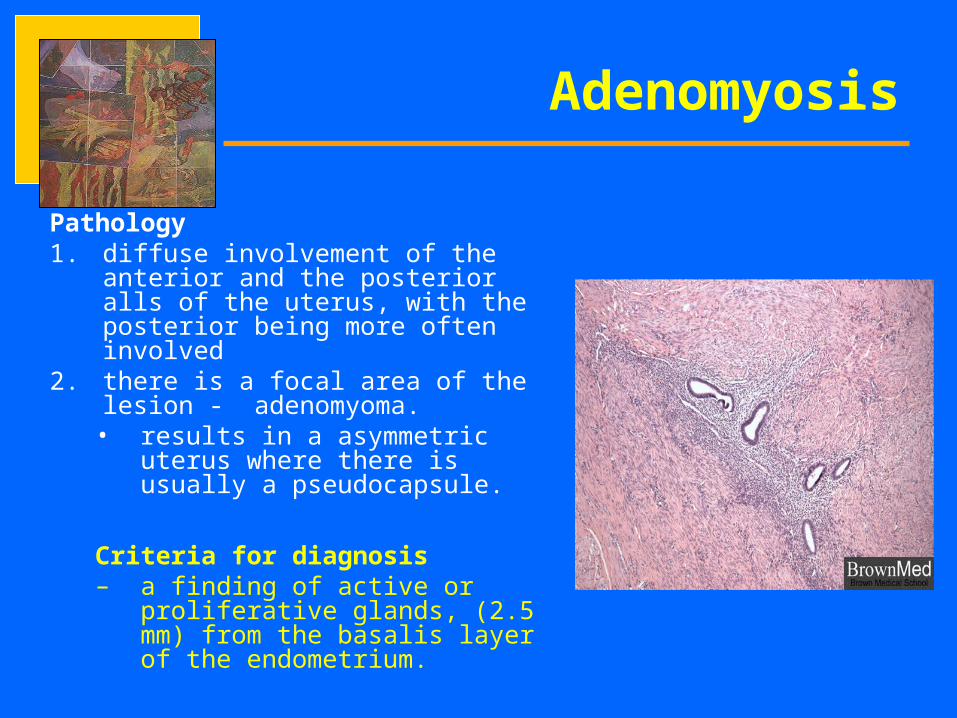
Pathology1. diffuse involvement of the anterior
and the posterior alls of the uterus, with the posterior being more often involved
2. there is a focal area of the lesion - adenomyoma.
• results in a asymmetric uterus where there is usually a pseudocapsule.
Criteria for diagnosis– a finding of active or proliferative
glands, (2.5 mm) from the basalis layer of the endometrium.
Adenomyosis
Adenomyosis
Diagnosis• majority of women are asymptomatic• May present with secondary
dysmennorhea and menorrhagia. severity of symptoms increases proportionally with depth of invasion and penetration.
• Usually presents with uterine enlargement palpated through pelvic examination
• Ultrasound is helpful in diagnosis.
Adenomyosis
Treatment• no satisfactory
proven medical treatment for adenomyosis.
• Hysterectomy is the definitive treatment
Benign Lesions of the
Ovaries
• most frequent cystic structure in normal ovaries
• arises from temporary variation of a normal physiologic process
• may result from either – the dominant mature follicle’s
failing to rupture (persistent follicle) or
– an immature follicle’s failing to undergo the normal process of atresia.
• most commonly found in young, menstruating women
Follicular Cysts
• majority are asymptomatic • May be discovered during ultrasound imaging of the pelvis or a
routine pelvic examination • May also present with signs and symptoms of ovarian enlargement
and therefore must be differentiated from a true ovarian neoplasm
Management• Conservative observation• majority disappear spontaneously by either reabsorption of the cyst
fluid or silent rupture within 4 to 8 weeks on initial diagnosis• persistent ovarian mass necessitates operative intervention to
differentiate it from a true neoplasm of the ovary• cystectomy and oophorectomy
Follicular Cysts
• less common than follicular cysts, but clinically more important
• minimum of 3 cm in diameter• may be associated with either
normal endocrine function or prolonged secretion of progesterone.
• associated menstrual pattern may be normal, delayed menstruation or amenorrhea
• vary from being asymptomatic to those causing catastrophic and massive intraperitoneal bleeding with rupture.
Corpus Luteum Cyst
Differential Diagnosis1. ectopic pregnancy2. ruptured endometrioma 3. adnexal torsion
Management• Conservative if unruptured• With persistent bleeding - treatment is
cystectomy.
Corpus Luteum Cyst
• least common of the three types of physiologic ovarian cysts
• almost always bilateral and produce moderate to massive enlargement of the ovaries
• Seen in 50% of molar pregnancies and 10% of choriocarcinoma
• also discovered in the latter months of pregnancies often with conditions that produce a large placenta, such as twins, diabetes and Rh sensitization
Theca Lutein Cysts
• Luteoma of pregnancy– not a true neoplasm but rather a specific,
benign, hyperplastic reaction of ovarian theca lutein cells
Theca Lutein Cysts
• produce vague symptoms, such as pressure in the pelvis
• presence is established by palpation and often confirmed by ultrasound examination
• treatment is conservative
Theca Lutein Cysts
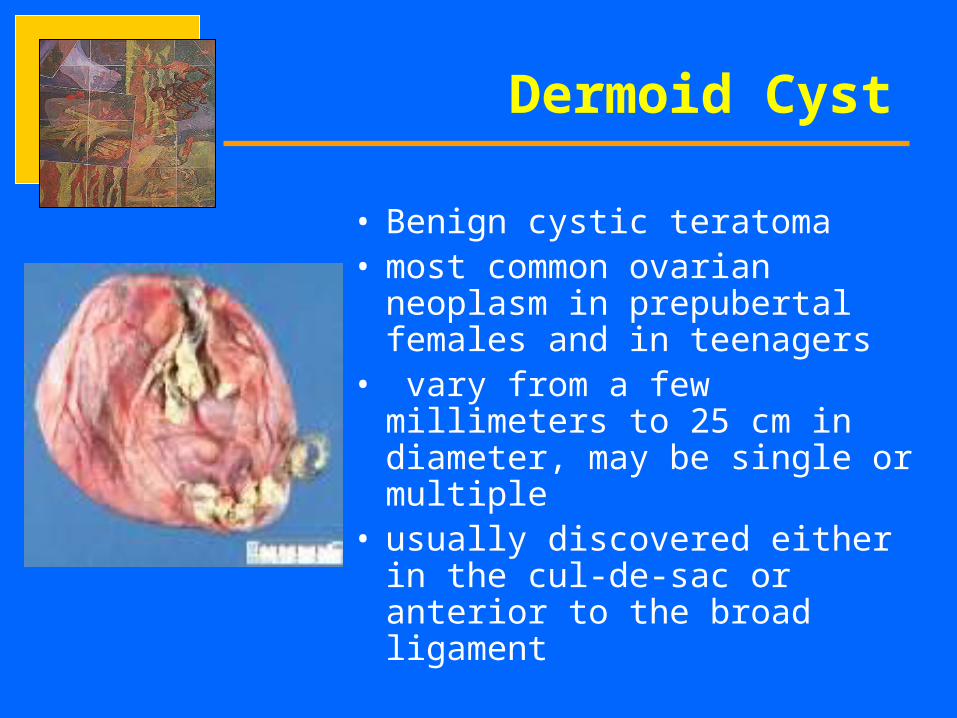
• Benign cystic teratoma• most common ovarian neoplasm
in prepubertal females and in teenagers
• vary from a few millimeters to 25 cm in diameter, may be single or multiple
• usually discovered either in the cul-de-sac or anterior to the broad ligament
Dermoid Cyst
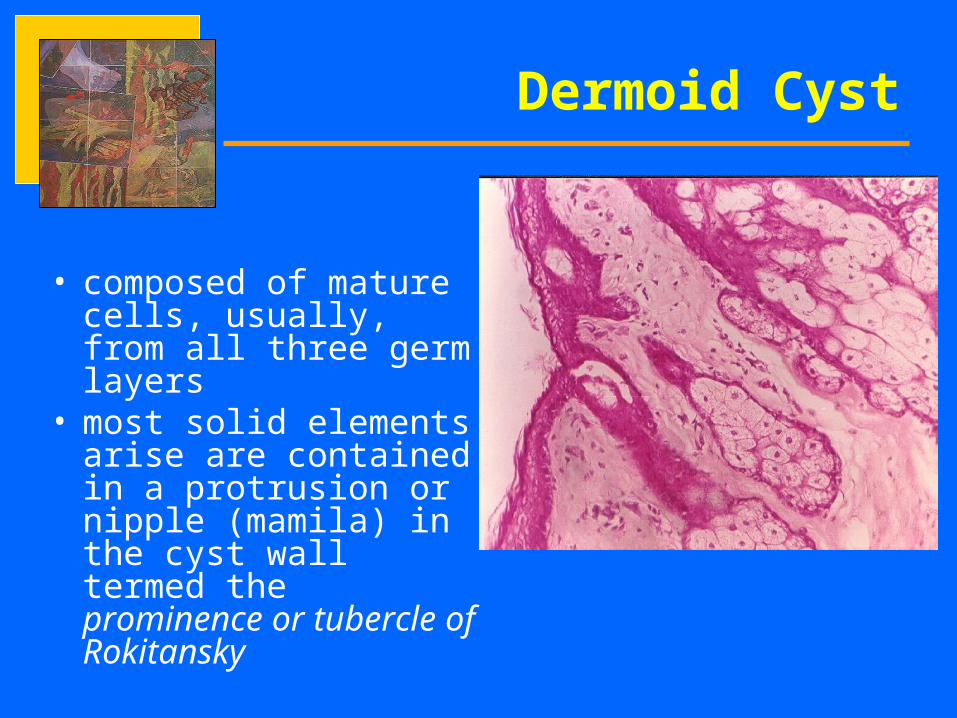
• composed of mature cells, usually, from all three germ layers
• most solid elements arise are contained in a protrusion or nipple (mamila) in the cyst wall termed the prominence or tubercle of Rokitansky
Dermoid Cyst
• adult thyroid tissue is discovered microscopically in approximately 12% of benign teratomas
• Struma ovarii – teratoma in which the thyroid tissue has
overgrown other elements and is the predominant tissue
Dermoid Cyst
• presenting symptoms include pain, sensation of pelvic pressure• 50% to 60% are asymptomatic • Some are discovered during a routine pelvic examination,
coincidentally visualized by an abdominal x-ray or ultrasound examination
management• cystectomy with preservation of as much normal ovarian tissue as
possible
Complications 1. Torsion2. Rupture3. Infection4. Hemorrhage5. malignant degeneration
Dermoid Cyst
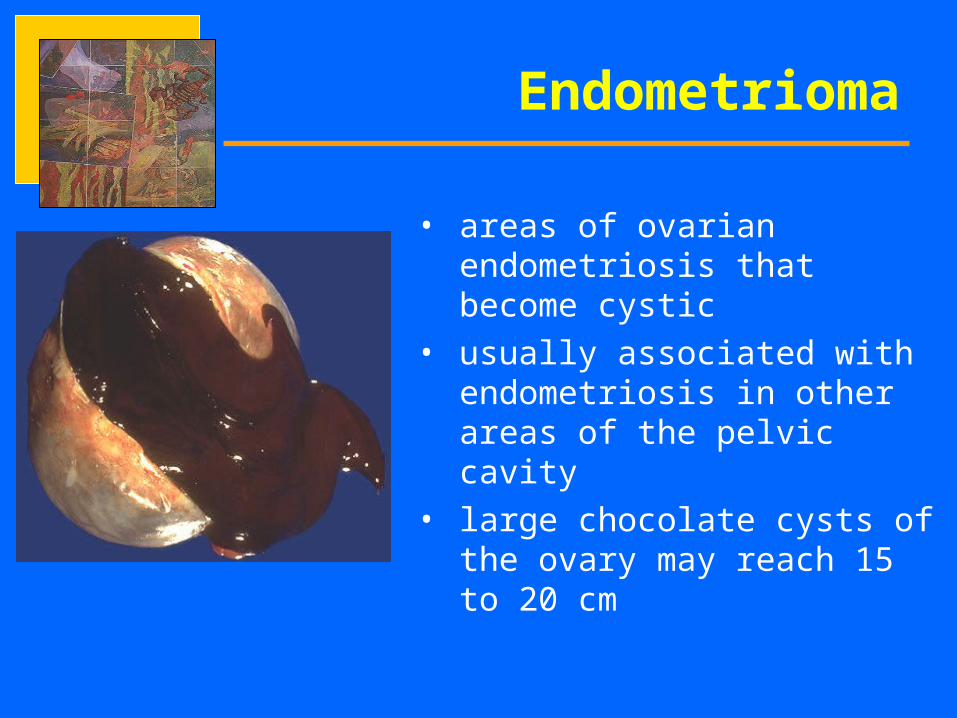
• areas of ovarian endometriosis that become cystic
• usually associated with endometriosis in other areas of the pelvic cavity
• large chocolate cysts of the ovary may reach 15 to 20 cm
Endometrioma
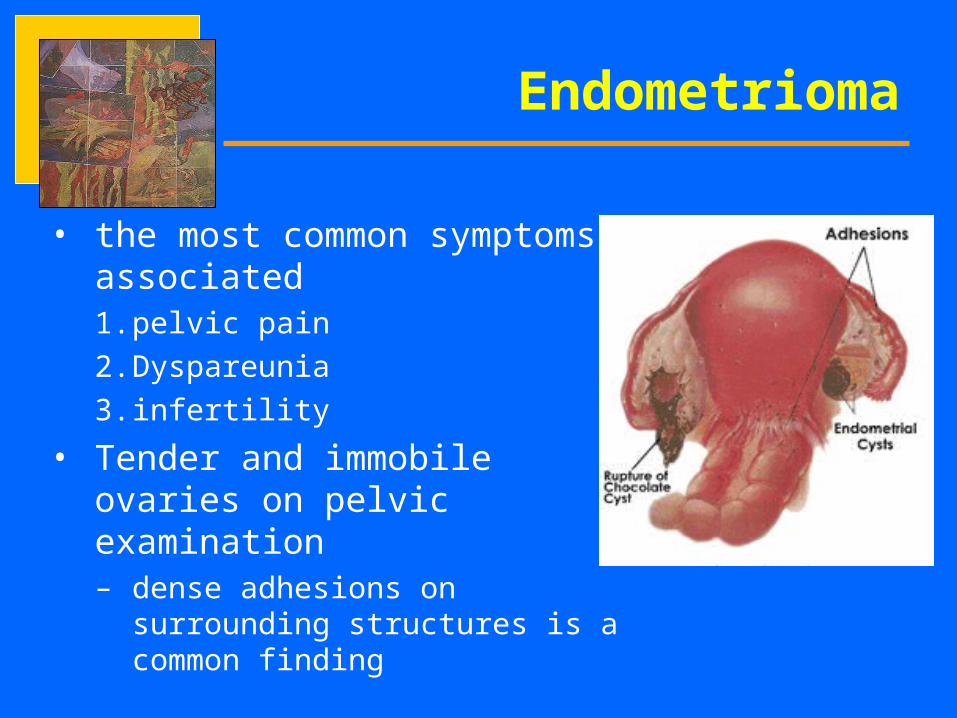
• the most common symptoms associated1. pelvic pain
2. Dyspareunia
3. infertility
• Tender and immobile ovaries on pelvic examination– dense adhesions on surrounding
structures is a common finding
Endometrioma

management
• medical therapy is rarely successful in treating ovarian endometriosis
• surgical therapy is complicated by formation of de novo and recurrent adhesions
Endometrioma
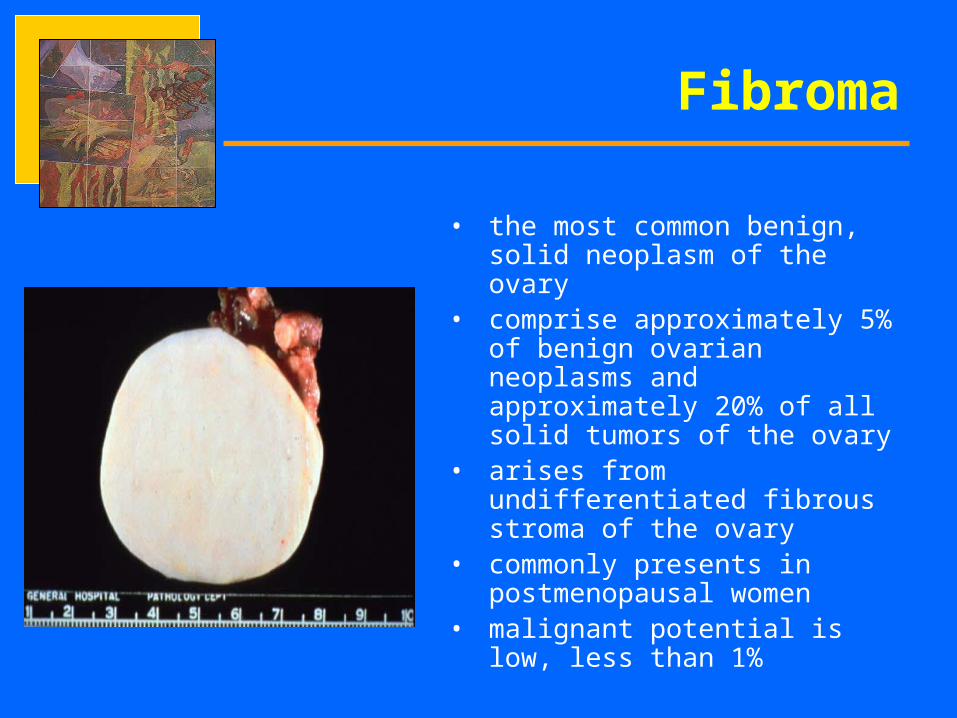
• the most common benign, solid neoplasm of the ovary
• comprise approximately 5% of benign ovarian neoplasms and approximately 20% of all solid tumors of the ovary
• arises from undifferentiated fibrous stroma of the ovary
• commonly presents in postmenopausal women
• malignant potential is low, less than 1%
Fibroma
• Manifest with pressure symptoms and abdominal enlargement
• Meigs’ syndrome– the association of an ovarian fibroma, ascites and hydrothorax– both resolve after the removal of an ovarian tumor
management• Exploratory operation• in postmenopausal women, often a bilateral salpingo-
oophorectomy and total abdominal hysterectomy are performed
Fibroma
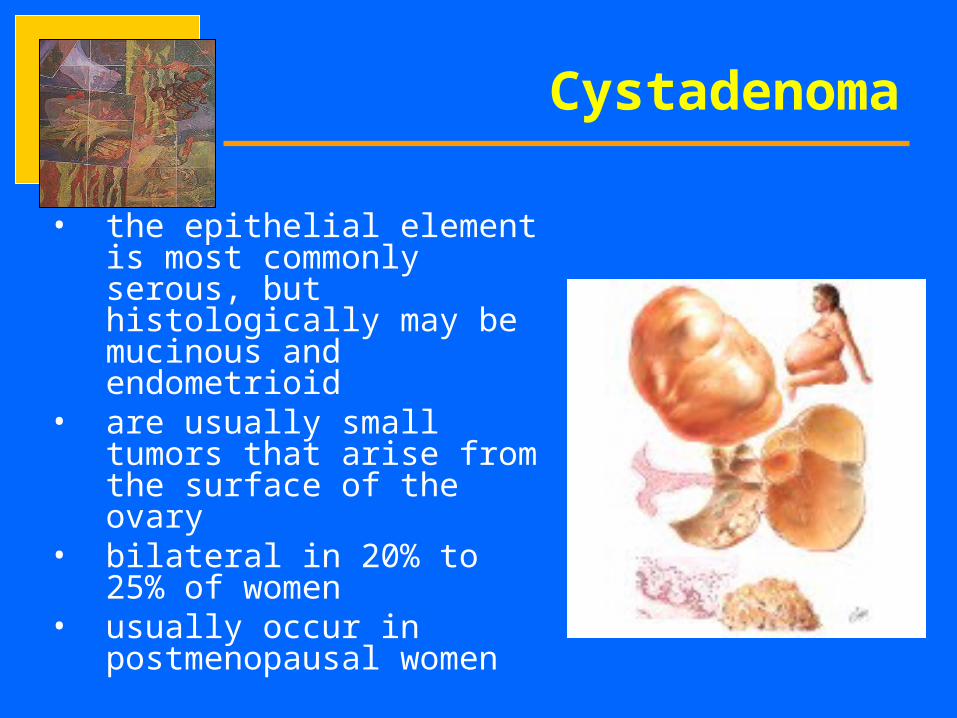
• the epithelial element is most commonly serous, but histologically may be mucinous and endometrioid
• are usually small tumors that arise from the surface of the ovary
• bilateral in 20% to 25% of women
• usually occur in postmenopausal women
Cystadenoma
• smaller tumors are asymptomatic or pelvic operations.• large tumors may cause pressure symptoms, rarely
adnexal torsion.
Management• postmenopausal women: bilateral salpingo-
oophorectomy and total abdominal hysterectomy• in younger women: simple excision of the tumor and
inspection of the contralateral ovary is appropriate
Cystadenoma
• a complication of benign ovarian tumors in the postmenopausal woman
• important cause of acute lower abdominal and pelvic pain
• commonly affects both fallopian tube and ovaries• pregnancy appears to predispose women to adnexal
torsion
Symptoms• Acute abdominal and pelvic pain• nausea and vomiting• fever
Torsion
management
• conservative operation for young women– laparoscope or via laparotomy
• with severe vascular compromise - unilateral salpingo-oophorectomy
Torsion
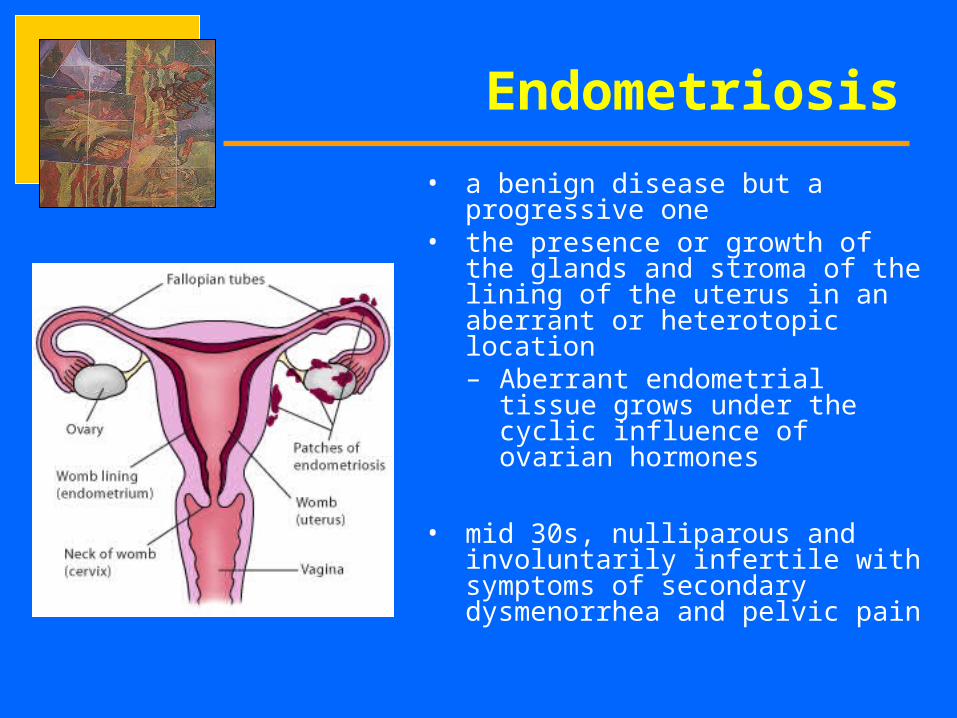
• a benign disease but a progressive one
• the presence or growth of the glands and stroma of the lining of the uterus in an aberrant or heterotopic location– Aberrant endometrial tissue
grows under the cyclic influence of ovarian hormones
• mid 30s, nulliparous and involuntarily infertile with symptoms of secondary dysmenorrhea and pelvic pain
Endometriosis
1. RETROGRADE MENSTRUATION– pelvic endometriosis is secondary to implantation of endometrial cells
shed during menstruation2. METAPLASIA
– arises from the metaplasia of coelomic epithelium or proliferation of embryonic rests.
3. LYMPHATIC AND VASCULAR METASTASIS– endometrial tissue is transplanted via lymphatic pathways and the
vascular system. 4. IATROGENIC DISSEMINATION5. IMMUNOLOGIC CHANGES
– the altered function of the immune-related cells are directly involved on the pathogenesis of endometriosis
6. GENETIC PREDISPOSITION
Etiology of Endometriosis
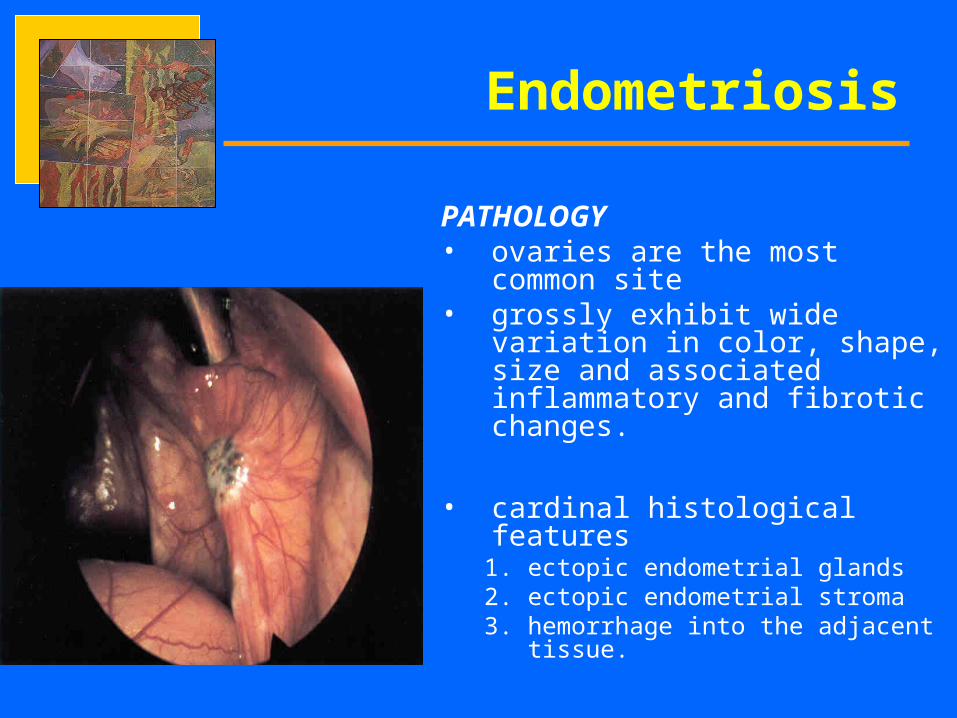
PATHOLOGY• ovaries are the most common
site• grossly exhibit wide variation in
color, shape, size and associated inflammatory and fibrotic changes.
• cardinal histological features 1. ectopic endometrial glands2. ectopic endometrial stroma 3. hemorrhage into the adjacent
tissue.
Endometriosis
Signs and Symptoms– Classic symptoms include cyclic pelvic pain and
infertility.– Pelvic pain is often inversely proportional to the
amount of endometriosis.– cyclic pelvic pain is related to the sequential swelling
and the extravasations of blood and menstrual debris in to the surrounding tissue and mediated by prostaglandins and cytokines
– Dyspareunia– GI and urinary symptoms– classic pelvic findings of a retroverted uterus with
scarring and tenderness posterior to the uterus
Endometriosis
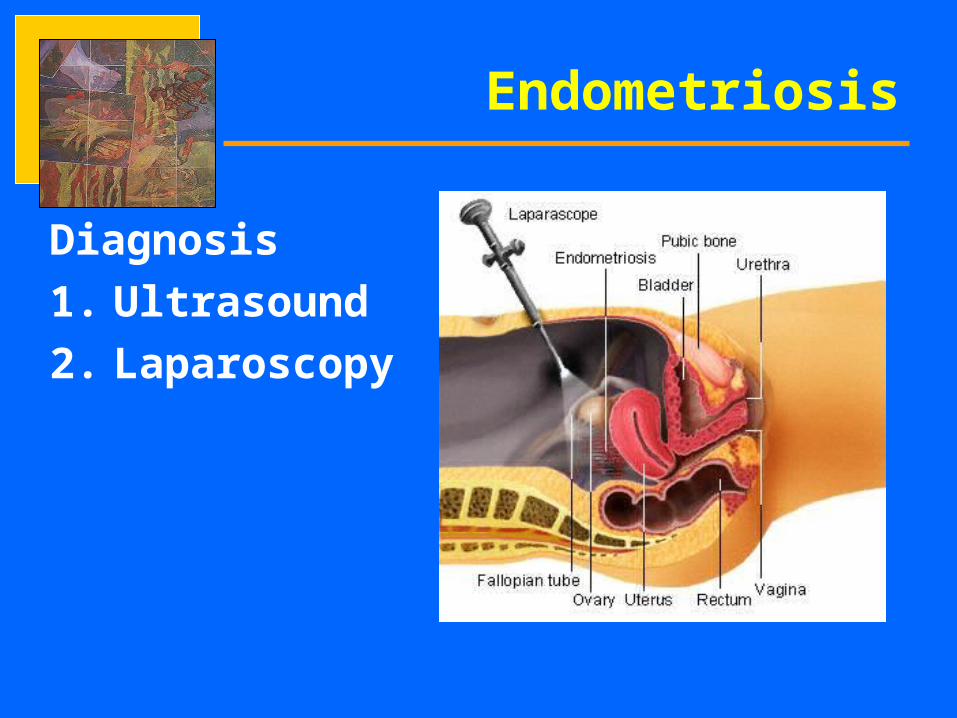
Diagnosis
1. Ultrasound
2. Laparoscopy
Endometriosis
Goals of Management
1.relief of pain
2.promotion of fertility
• Primary long term goal in management is to prevent progression of the disease process
Endometriosis
Endometriosis
Medical Management– primary goal of hormonal treatment is
induction of amenorhea.– DOES NOT provide a long lasting cure of the
disease
Endometriosis
Medications for Endometriosis
1. Danazol
2. GnRH Agonists*
3. Oral contraceptives
4. Medroxyprogesterone acetate (DMPA)
Endometriosis
SURGICAL THERAPY
• Often occurs concurrently during laparoscopy to establish diagnosis • only option after failed medical treatment• for women who have moderate to severe endometriosis• Conservative surgery has as its goal the removal of macroscopic
visible areas of endometriosis with preservation of fertility.
Types of Surgical Therapy Used1. laparoscopy2. laser3. Total hysterectomy with ovarian preservation4. total abdominal hysterectomy with bilateral salpingo
oophorectomy.
Thank you!