Embed Size (px)
Citation preview

Benefits and Pitfalls of Tumor VesselNormalization
Jin-Sung Park, Intae Park, and Gou Young Koh
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Lessons and Questions from Anti-VEGF-A/VEGFR2 Therapy . . . . . . . . . . . . . . . . . . . . . 52
Hallmarks of Tumor Vessel Normalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Inducing Tumor Vessel Normalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Benefits of Tumor Vessel Normalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Pitfalls of Tumor Vessel Normalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Translational Implications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
Challenges for Clinical Application . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Cross-References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
AbstractTumor vasculature has been intensively stud-ied not only to understand its role in tumorprogression and metastasis but also to discoverregulatory pro- and anti-angiogenic moleculesand cells. Until now, numerous anti-angiogenic
agents have been developed, with more thanten agents currently being administered ortested to treat patients with various typesof cancers. Despite high hopes for success,recent clinical trials have shown that theseanti-angiogenic agents are not as effective asother drugs with different targets in terms ofincreasing patient survival when used as a sin-gle agent. These unsuccessful trials have ledresearchers to reevaluate the nature of tumorvasculature and the dynamic consequences thatarise from anti-angiogenic treatments. Subse-quently, a new hypothesis was introduced,where tumor vessels were sought to be tamedand harnessed to our advantage rather than
Jin-Sung Park, Intae Park and Gou Young Koh have beencontributed equally.
J.-S. Park · I. Park · G. Y. Koh (*)Center for Vascular Research, Institute for Basic Science(IBS) and Graduate School of Medical Science andEngineering, Korea Advanced Institute of Science andTechnology (KAIST), Daejeon, South Koreae-mail: [email protected]; [email protected];[email protected]
© Springer Nature Switzerland AG 2019D. Marmé (ed.), Tumor Angiogenesis,https://doi.org/10.1007/978-3-319-33673-2_46
51

simply attempting to eliminate them, which, byitself, has shown only marginal survival bene-fit. Thus, a new avenue of research wasrevealed, and the concept “tumor vessel nor-malization” has gained considerable attentionever since. However, our knowledge in thisfield is still rather rudimentary, and much stillneeds to be accomplished in order to overcomethe pitfalls and relish the benefits of normaliz-ing tumor vessels for anticancer therapy.
KeywordsTumor vessel normalization · Tumorvasculature · Tumor microenvironment ·Enhanced drug delivery · Enhanced perfusion ·Reduced hypoxia · Anti-angiogenesis · Tie2activators
Introduction
Angiogenesis is a critical process that is drivenwith the purpose of providing every living cellwith adequate passages for nutrient and oxygensupplementation and waste removal. In cancer,angiogenesis is constantly activated to meet theunending demand of new blood vessels to matchthe unregulated growth of tumor mass, markingangiogenesis as one of themost evident phenotypichallmarks of cancer (Hanahan and Weinberg2011). Tumor growth and metastasis are largelydependent on the accompanied growth of tumorvasculature, so called tumor angiogenesis. Indeed,tumor angiogenesis has been an appealing targetfor antitumor therapy, which has been proposedmore than four decades ago (Carmeliet 2005;Fenton et al. 2004; Folkman 1971; Jain 2005;Kerbel and Folkman 2002). Ever since, numerousstrategies have been devised to block tumor angio-genesis or destroy pre-existing tumor vessels.Anti-angiogenic therapies basically reduce or“prune” growing tumor vessels. However, thisstrategy turned out to be less effective than antici-pated, mostly because the underlying cause of thepro-angiogenic drive in cancer, severe hypoxia, isactually worsened by anti-angiogenic strategies.Removing tumor vessels exacerbates tumor hyp-oxia, which ultimately generates a rebound
increase in pro-angiogenic force, ending in treat-ment resistance and failure. To circumvent thissituation, focus has shifted to alleviating hypoxia,rather than destroying tumor vasculature altogether(Jain 2014). Tumor vessel normalization is a con-cept that has emerged to overcome the shortcomingof current anti-angiogenic strategy (Carmeliet andJain 2011b). Here, we discuss the current knowl-edge and understanding of numerous ways andmechanisms to normalize tumor vasculature, whytumor vessel normalization is advantageous overtumor vessel destruction, and its potential benefitsand pitfalls in real-world applications.
Lessons and Questions from Anti-VEGF-A/VEGFR2 Therapy
The most widely studied strategy to block tumorangiogenesis is by inhibiting the interactionbetween vascular endothelial growth factor(VEGF) and its receptor VEGF receptor2 (VEGFR2), which stimulates endothelial pro-liferation, migration, permeability, and survivaland together forms the strongest agonistic axis fornew vessel formation (Chung et al. 2010; Nagyet al. 2007). More than ten drugs that targetVEGF-VEGFR2 axis have been developed andapproved for treating patients with various typesof cancers. However, despite the dramaticresponses shown in multiple preclinical animalstudies, recent clinical trials using VEGF-VEGFR2-blocking agents yielded rather disap-pointing results; randomized phase III clinicaltrials showed only a minimal survival benefit inpatients with a monotherapy of anti-angiogenicagents (anti-VEGF drugs) (Giantonio et al. 2007;Jain et al. 2006; Gligorov et al. 2014; Gilbert et al.2014). These trials clearly demonstrated the lim-itation of anti-angiogenic strategy when it isimplemented as a single treatment modality.However, the addition of cytotoxic chemothera-peutic drugs to the VEGF-A-blocking antibody,bevacizumab, led to improved patient outcomesin those with colorectal, breast, and lung cancer(Hurwitz et al. 2004; Sandler et al. 2006). Thesepuzzling results raised important questions aboutthe use of anti-angiogenic agents for treating
52 J.-S. Park et al.
cancer. Why was anti-VEGF effective in combi-nation with cytotoxic drugs, while it was unableto produce survival benefits as a monotherapy inrandomized trials? Shouldn’t anti-VEGF agentsdestroy tumor vessels and hinder the delivery ofchemotherapeutic drugs? These seemingly para-doxical results led researchers to investigate themolecular mechanism of anti-angiogenic therapyand its true effect on tumor vasculature, eventu-ally giving rise to a novel working model oftumor vasculature’s response to anti-angiogenicforce, namely, “tumor vessel normalization.”
Hallmarks of Tumor VesselNormalization
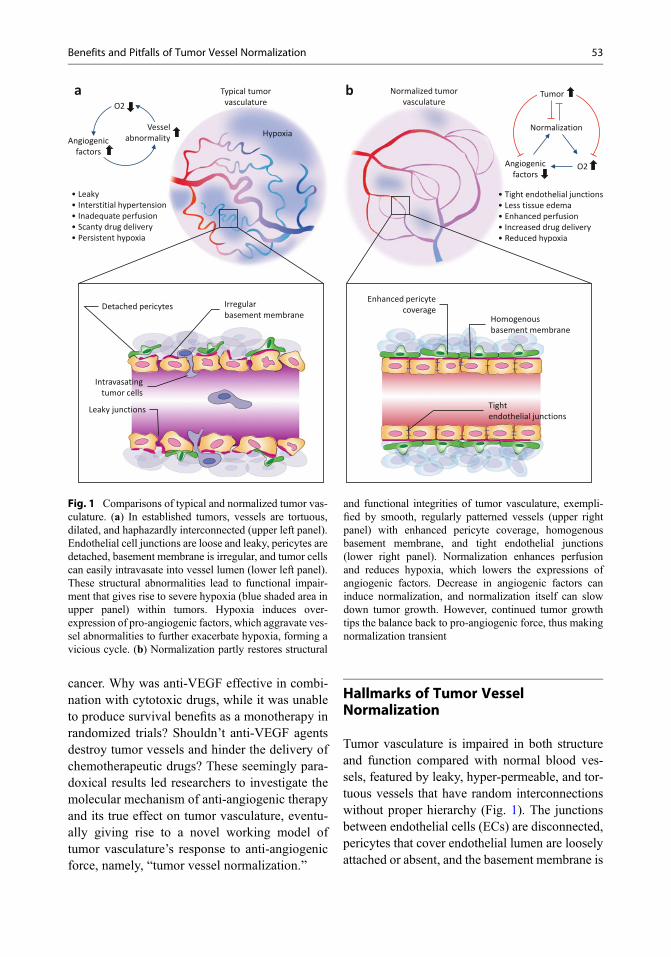
Tumor vasculature is impaired in both structureand function compared with normal blood ves-sels, featured by leaky, hyper-permeable, and tor-tuous vessels that have random interconnectionswithout proper hierarchy (Fig. 1). The junctionsbetween endothelial cells (ECs) are disconnected,pericytes that cover endothelial lumen are looselyattached or absent, and the basement membrane is
Hypoxia
O2
Angiogenicfactors
Vesselabnormality
• Leaky• Interstitial hypertension• Inadequate perfusion• Scanty drug delivery• Persistent hypoxia
• Tight endothelial junctions• Less tissue edema• Enhanced perfusion• Increased drug delivery• Reduced hypoxia
Typical tumor vasculature
Normalized tumor vasculature
Detached pericytes Irregular basement membrane
Intravasatingtumor cells
Leaky junctions
Enhanced pericyte coverage
Homogenous basement membrane
Tightendothelial junctions
a b
Normalization
Tumor
Angiogenicfactors
O2
Fig. 1 Comparisons of typical and normalized tumor vas-culature. (a) In established tumors, vessels are tortuous,dilated, and haphazardly interconnected (upper left panel).Endothelial cell junctions are loose and leaky, pericytes aredetached, basement membrane is irregular, and tumor cellscan easily intravasate into vessel lumen (lower left panel).These structural abnormalities lead to functional impair-ment that gives rise to severe hypoxia (blue shaded area inupper panel) within tumors. Hypoxia induces over-expression of pro-angiogenic factors, which aggravate ves-sel abnormalities to further exacerbate hypoxia, forming avicious cycle. (b) Normalization partly restores structural
and functional integrities of tumor vasculature, exempli-fied by smooth, regularly patterned vessels (upper rightpanel) with enhanced pericyte coverage, homogenousbasement membrane, and tight endothelial junctions(lower right panel). Normalization enhances perfusionand reduces hypoxia, which lowers the expressions ofangiogenic factors. Decrease in angiogenic factors caninduce normalization, and normalization itself can slowdown tumor growth. However, continued tumor growthtips the balance back to pro-angiogenic force, thus makingnormalization transient
Benefits and Pitfalls of Tumor Vessel Normalization 53

discontinuous, reduced, or absent. These struc-tural abnormalities hinder adequate blood flowand create spatiotemporal heterogeneity withintumor microenvironment. Moreover, leakiness invessels leads to increased interstitial fluid, whichacts in concert with proliferating cancer cells toincrease physical pressure and compress bloodand lymphatic vessels. These abnormal featuresof tumor vasculature contribute heavily to theformation of a characteristic tumor microenviron-ment that is featured by interstitial hypertension,hypoxia, and acidosis. Interstitial hypertensionacts as a barrier that hinders the delivery of ther-apeutics to the central region of tumor mass. Hyp-oxia makes tumor cells resistant to radiationtherapy and also induces numerous genes thatmake tumor cells resilient to cytotoxic drugs. Italso causes genetic instability within tumor cellsand triggers genetic mutations that make thetumor cells more malignant and prone to metasta-sis. Acidosis, combined with hypoxia, weakensthe cytotoxic functions of infiltrated immunecells. Essentially, structural and functional abnor-malities of the tumor vasculature and the resultingharsh tumor microenvironment work in tandem tohinder the effectiveness of cancer therapy. Thisimplies that tumor vasculature plays importantroles in generating a hostile tumor microenviron-ment and also suggests the possibility of improv-ing such hostility in order to maximize cancertherapy by managing and adjusting the structureand function of tumor vasculature.
Hallmarks of tumor vessel normalization arereduced mean vascular density, increased pericytecoverage, and less tortuous structure and mor-phology, which subsequently lead to functionallyimproved blood flow within tumor mass andreduced interstitial pressure and edema (Goelet al. 2012; Park et al. 2016; Viallard and Larrivee2017; Carmeliet and Jain 2011b). Because ofthese structural and functional changes of tumorvasculature, tumor vessel normalization has beengathering attention as a viable alternative to con-ventional anti-angiogenic therapy (Cully 2017;Rivera and Bergers 2015). Instead of abolishingthe blood vessels and thus the nutrients and oxy-gen supply to tumors, which aggravates tumorcharacters and antagonizes other treatments, it
was sought to reinforce them to promote syner-gism with other treatment modalities. In otherwords, normalizing tumor vessels will pave thepath for better delivery of drugs and oxygen,leading to therapeutic success. Tumor vessel nor-malization not only enhances the delivery of drugsand oxygen but also facilitates a more uniform andconcentrated distribution of these therapeutics intumor mass to ensure that a larger fraction oftumor cells is in contact with them. Furthermore,it can alleviate the inhospitable tumor microenvi-ronment to generate a friendlier setting in whichanticancer immune cells can function better. Insum, normalization alters the tumor microenvi-ronment and creates a battleground more amena-ble for treatment.
Inducing Tumor Vessel Normalization
In normal angiogenesis, stimulators of angiogen-esis temporarily outweigh inhibitors to tipthe balance between pro-angiogenic andanti-angiogenic stimuli to prompt new vesselgrowth. Once vessel growth is completed andtissue is sufficiently vascularized, the level ofangiogenic inhibitors becomes more dominantand vessels become quiescent and mature(Carmeliet and Jain 2011a; Potente et al. 2011).In tumors, rapid growth of tumor cells generates achronically hypoxic microenvironment that actsas the major driving force for the production ofpro-angiogenic activators, and thus the balance isskewed in favor of new vessel formation. Moreimportantly, unlike physiologic angiogenesis, thisimbalance between pro-angiogenic and anti-angiogenic stimuli persists, because tumor angio-genesis generates abnormal vessels that cannotcompletely resolve the underlying tissue hypoxia.This persistent hypoxia in turn generates morepro-angiogenic stimulators, and tumor vesselsbecome increasingly abnormal, thereby creatinga vicious cycle (Ziyad and Iruela-Arispe 2011;Jain 2014). Thus, it is reasonable to assume that,by blocking pro-angiogenic stimulators or modu-lating different components that affect the struc-ture and function of tumor vessel walls, onecan restore the balance of pro-angiogenic and
54 J.-S. Park et al.

anti-angiogenic stimuli and promote normaliza-tion of tumor vessels.
Mechanisms affecting tumor endothelium:Many preclinical studies demonstrated that highlevels of VEGF within tumor can induce tumorvessel abnormalities (Jain 2005, 2008). Therefore,it is reasonable to speculate that targeting VEGFsignaling by direct or indirect modulators willdecrease structural and functional abnormalitiesof tumor vessels. As expected, treatment with aVEGF-blocking antibody induced transient tumorvessel normalization, which was demonstrated byenhanced pericyte coverage, reduced vessel sizeand tortuosity, and normalized basement mem-brane (Yuan et al. 1996; Tong et al. 2004; Winkleret al. 2004; Baffert et al. 2006; Kamoun et al.2009). Mechanistically, VEGF blockade inducesupregulation of angiopoietin 1 (Angpt1), whichacts to promote tightening of EC junctions andstabilize ECs (Winkler et al. 2004). However, thesource and underlying mechanism for theupregulation of Angpt1 are still unclear. VEGFalso affects platelet-derived growth factor recep-tor β (PDGFRβ) signaling in smooth muscle cells,which are known to be critical for pericyte recruit-ment and coverage (Greenberg et al. 2008). Invarious preclinical studies, transient vessel nor-malization induced by VEGF blockade resultedin reduced interstitial fluid pressure and tissueedema (Tong et al. 2004; Kamoun et al. 2009;Dickson et al. 2007; Tailor et al. 2010), increasedperfusion along tumor vessels (Dickson et al.2007; Myers et al. 2010), and enhanced oxygenand drug delivery to the tumor core (Tong et al.2004; Winkler et al. 2004; Dickson et al. 2007;Myers et al. 2010). During this transient normal-ization window, VEGF blockade synergisticallyinhibits tumor growth with chemotherapeuticdrugs and radiation therapy, since the delivery ofdrugs and oxygen to the tumor core is enhanced.However, excessive vascular regression by pro-longed or overdosing of VEGF blockade mightcompromise the synergistic effect and antagonizethe response to radiation and chemotherapy(Fenton et al. 2004; Ma et al. 2001; Murata et al.1997). Considering the lengthy chemo- or radio-therapy regimens in the clinic, this dose-dependent effect and narrow normalization
window by VEGF blockade is an active area ofresearch.
Another example of a molecule that regulatesvessel disorganization is the oxygen sensor mole-cule prolyl hydroxylase domain-containing pro-tein 2 (PHD2) (Aragones et al. 2009; Majmundaret al. 2010). Due to the absolute requirement ofoxygen supply for cell sustenance, it is not sur-prising that a sophisticated mechanism to senseoxygen levels was devised by ECs. PHD2 is anoxygen-sensing enzyme which hydoxylates thetranscription factors, hypoxia-inducible factors(HIFs), for proteasomal degradation when oxygenconcentration is sufficient (Aragones et al. 2009;De Bock et al. 2009). Under hypoxic conditions,PHD2 is inactivated and transcription factorsHIFs are activated to induce gene expressions toincrease oxygen supply, partly via angiogenesissince VEGF-A is a well-known target gene ofHIF1α (Rey and Semenza 2010). In the aspect ofHIF1α, PHD2 downregulation should upregulateVEGF-A and subsequently induce vesselabnormalization. Perplexingly, however, endothe-lial PHD2 haplodeficiency by genetic modifica-tion in mice induced tumor vessel normalizationwithout significantly affecting vascular density orsize, while physiologic angiogenesis was largelyunaffected (Mazzone et al. 2009; De Bock et al.2013). In normalized vessels, vascular leakageand remodeling were reduced, whereas endothe-lial junction tightening and vessel maturationwere increased, leading to increased tumor perfu-sion and reduced hypoxia. In addition, endothelialjunctions formed a tight barrier against tumor cellintravasation and reduced metastasis (Mazzoneet al. 2009). These vascular changes did not affectprimary tumor growth, but reduced distant metas-tasis and also improved response to chemother-apy. Mechanistically, the molecular changes byPHD2 haplodeficiency induced an upregulationof vascular endothelial cadherin, a critical compo-nent of endothelial junctions, and also induced anupregulation of soluble FLT1, which acts as adecoy receptor that traps soluble VEGF-A(Mazzone et al. 2009; De Bock et al. 2013).
Even methods that may not seem to targettumor vasculature can also induce normalization.Metronomic chemotherapy, a method of drug
Benefits and Pitfalls of Tumor Vessel Normalization 55

delivery which administers suboptimal dose ofchemotherapeutic drugs at frequent intervals, hasalso been shown to induce tumor vessel normali-zation. The mechanism seems to involveenhanced expression of thrombospondin 1,which is a well-known inhibitor of angiogenesis(Kerbel and Kamen 2004). Aerobic exercisehas also been shown to induce normalization inpreclinical model by activating calcineurin-NFAT-TSP1 signaling pathway (Schadler et al.2016). Very interestingly, a study revealed thatthe deletion of RhoJ, a Rho GTPase enriched intumor ECs, not only inhibited tumor angiogenesisbut also induced vascular disruption (opposite totumor vessel normalization) in established tumorvessels using various murine tumor models (Kimet al. 2014), leading to significantly increasedhypoxia and necrosis that, as a result, delayedtumor growth. Thus, RhoJ in tumor ECs playsan important role in maintaining tumor vesselintegrity, and enhancing RhoJ activity couldinduce tumor vessel normalization.
Mechanisms which affect pericyte coverageand tumor vessel maturation: Typical structuralcharacteristics of normalized tumor vesselsinclude enhanced pericyte coverage, and thusmolecules that stimulate or promote mural cellcoverage of endothelial lumen can serve as impor-tant regulators of tumor vessel normalization(Carmeliet 2003; Jain 2003). The most widelystudied signaling pathway on pericyte coverageis PDGFRβ signaling axis. Its ligand PDGF-B isreleased from ECs and recruits perivascular muralcells expressing PDGFRβ. Another well-knownpericyte marker is neuron-glial antigen 2 (NG2),also known as chondroitin sulfate proteoglycan4 (CSPG4), which is a membrane proteoglycanfound on plasma membrane of diverse cell types.Genetic depletion of NG2 generated abnormaltumor vessels with reduced pericyte and basementmembrane coverage, which resulted in reducedperfusion and increased tumor hypoxia (Huanget al. 2010). Moreover, many preclinical studiesshowed that depletion of pericytes from tumorvasculature promotes metastasis, as vessel wallswithout pericytes form loose barrier that cannotblock dissemination of tumor cells (Gerhardt andSemb 2008). Lack of pericyte coverage also
correlates with metastasis in clinical settings(Yonenaga et al. 2005), and a clinical trial usingPDGFRβ blockade showed excessive fluid leak-age (Jayson et al. 2005). Interestingly, while over-expression of PDGF-D facilitates tumor growthand lymph node metastasis, it normalized tumorvasculature and enhanced drug delivery (Liu et al.2011). Clearly, further studies are required to clar-ify the benefits and pitfalls of PDGF blockade incancer treatment and vessel normalization.
Another important molecular pathwayinvolved in vessel maturation and tumor vesselnormalization is the Angpt-Tie receptor axis,which plays crucial roles in the formation of stablevasculature (Winkler et al. 2004; Augustin et al.2009; Saharinen et al. 2017). As briefly men-tioned, binding of Angpt1 – which is known tobe released by pericytes – to its receptor Tie2tightens endothelial junctions and promotes ECsurvival, whereas Angpt2 acts as a context-dependent antagonist of Tie2 that destabilizesEC and disrupts endothelial junctions (Augustinet al. 2009; Saharinen et al. 2017). Blockade ofAngpt2 induces junctional tightening of endothe-lial barrier and enhances pericyte coverage, whilereducing tumor growth and metastasis (Falconet al. 2009; Nasarre et al. 2009). Simultaneousinhibition of Angpt2 and VEGF-A by a bispecifictrap, double anti-angiogenic protein (also knownas “DAAP”), also substantially induces vesselnormalization and markedly reduces vessel leak-age in the ovarian cancer ascites model (Koh et al.2010). On the other hand, several studies soughtto activate Tie2 directly rather than inhibiting itsantagonist, Angpt2, to normalize tumor vessels.However, activating Tie2 has been much morechallenging compared with blocking Angpt2,since native Angpt1 is prone to aggregation andis largely insoluble (Cho et al. 2004; Koh 2013); itwas only recently that a potent activator of Tie2that has a long systemic half-life and minimaltoxicity was developed (Park et al. 2016; Hanet al. 2016). Activation of Tie2 in tumor ECs byan Angpt1 analog, VE-PTP inhibitor, or an acti-vating antibody induces tight endothelial junc-tions and enhances pericyte coverage, whichalleviates hypoxia and enhances the effects ofcytotoxic drugs (Hwang et al. 2009; Goel et al.
56 J.-S. Park et al.
2013; Park et al. 2016). Tie2 activation alsoreduces tumor growth and metastasis, which isthought to be the result of reduced hypoxia withinthe tumor core and enhanced pericyte coveragethat provides a stable barrier against tumor cellextravasation (Park et al. 2016). Another advan-tage of Tie2 activation stems from its uniquerelationship with Angpt2. Destabilized ECs liketumor ECs overexpress angiogenic genes likeAngpt2, ESM 1, and VEGFR2 by transcriptionalactivation of FOXO1, and Tie2 activation inhibitsthe expression of these angiogenic genes (Dalyet al. 2004, 2013; Park et al. 2017). While treat-ment of Angpt2-blocking antibody leads to arebound increase in Angpt2 expression (Mazzieriet al. 2011), Tie2 activation stably downregulatesthe angiogenic genes expressed by destabilizedECs by harnessing the inhibitory pathway builtwithin ECs. The recently developed Tie2 activat-ing antibody, angiopoietin-2 binding and Tie2activating antibody (ABTAA), takes advantageof the paradoxical relationship between Angpt2and Tie2 to induce relatively profound vessel nor-malization (Park et al. 2016). The Tie2-activatingability of ABTAA is dependent on Angpt2,whereby it binds and clusters Angpt2 to switch itfrom a Tie2 antagonist to an agonist. Subse-quently, Tie2 is activated by the ABTAA-Angpt2 complex, which downregulates theexpression of Angpt2 and breaks thepro-angiogenic cycle. Because of this uniquemode of action, adequate Tie2 activation isguaranteed even without tight regulation of a-ntibody concentration. Therefore, continuoushyper-activation of Tie2, which has been shownto promote tumor metastasis (Holopainen et al.2009), is inherently impossible because any fur-ther expression of Angpt2 is inhibited byABTAA-induced Tie2 activation; thus any excessABTAA left in the system will be inactive. Forthese reasons, Tie2 activators are gathering atten-tion as a safer alternative to anti-angiogenic agentsand for tumor vessel normalization (Fig. 2).
Regulator of G-protein signaling 5 (RGS5)also affects vessel maturation, and inhibition ofRGS5 can induce vessel normalization. RGS5 isproduced by ECs in hypoxic condition or by acti-vated pericytes (Hamzah et al. 2008). RGS
molecules block G protein-coupled receptor(GPCR) signaling, and loss of RGS5 in pancreaticislet cancer model normalizes tumor vessels withreduced leakage (Hamzah et al. 2008). RGS5-deficient tumors show uniformly distributed ves-sels, and pericytes have more mature phenotype.Influx and penetration of immune cells are alsoincreased, and adoptive transfer of immune effec-tor cells prolongs the survival of tumor-bearingmice (Hamzah et al. 2008; Nisancioglu et al.2008). Finally, a recent study highlights theimportance of metabolic profile of tumor ECsand its role in tumor vessel normalization.Tumor cells acquire a unique metabolic profileknown as “Warburg effect,” which is one of thecharacteristic hallmarks of cancer (Hanahan andWeinberg 2011). Just like tumor cells, tumor ECsalso exhibit a unique metabolic profile that issignificantly different from normal ECs(Cantelmo et al. 2016). Tumor ECs show hyper-glycolytic metabolism, and one of the enzymesinvolved in this process, 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 3 (PFKFB3),is closely linked to tumor vessel normalization.Genetic deletion or pharmacologic inhibition ofPFKFB3 from tumor ECs led to improved tumorvessel maturation and perfusion (Cantelmo et al.2016). PFKFB3 inhibition reduced the endocyto-sis of a junctional molecule, VE-cadherin, hencegenerating a tight endothelial barrier that conse-quently reduced tumor metastasis. PFKFB3 inhi-bition also enhanced pericyte coverage andreduced the expression of adhesion molecules,which is critical in regulating tumor cellintravasation/extravasation (Cantelmo et al.2016).
Mechanisms involving various types ofimmune cells: Immune cells comprise a majorcomponent of tumor microenvironment and haverecently been highlighted for their roles in pro-moting or suppressing tumor growth (De Palmaet al. 2017). Trafficking and infiltration of immunecells is largely dependent on ECs, and immunecells also interact closely with ECs to maintain itsproper function. The most widely studied immunecell type is tumor-associated macrophages(TAMs), which affect tumor angiogenesis,growth, metastasis, and also clinical outcome
Benefits and Pitfalls of Tumor Vessel Normalization 57

(De Palma et al. 2017). TAMs can change theircharacter according to external stimuli, and theirpolarization states (either M1 or M2) largelydetermine their role in tumor angiogenesis.TAMs that are polarized to M2-like phenotypeare known to promote tumor angiogenesis aswell as increase its malignancy. They can be stim-ulated to secrete various types of pro-angiogeniccytokines, and some subset of TAMs, especiallyTIE2-expressing monocytes, remain closely
attached to tumor ECs, where they modulatetumor angiogenesis and largely affect the integrityof tumor vasculature (Mazzieri et al. 2011).
Deletion of VEGF from myeloid lineage cellshas been shown to induce tumor vessel normali-zation, enhance tumor oxygenation, and enhancethe response to chemotherapy (Carretero et al.2015; Stockmann et al. 2008). Another importantangiogenic factor of the VEGF family, placentalgrowth factor (PlGF), is also known to affect
ABTAA
Angpt2
Tie2
VE-cadherin
FOXO1
Angpt2
Angpt2VEGFR2ESM1
PI3K/Akt
• EC destabilization• Destabilized EC express Angpt2• Vicious cycle continues
• Stabilized EC• Normalization of tumor vessels
PI3K/Akt
Genes for EC stabilization
PI3K/Akt
PFOXO1
Degradation
P PP P
Fig. 2 Tie2 activator takes center stage of tumor vesselnormalization. Schematic diagram depicting how Tie2activation leads to EC stabilization and tumor vessel nor-malization. Tumor ECs have insufficient pericyte coverageand lack Tie2 activation, leading to attenuated PI3 kinase-Akt signaling and enhanced FOXO1-induced upregulationof pro-angiogenic genes. Of the upregulated genes, theoverexpressed Angpt2 acts as an endothelial destabilizingfactor, and destabilized ECs further stimulate FOXO1 andits downstream pathway to produce Angpt2, creating avicious pro-angiogenic cycle. These consequently lead to
impaired vessel integrity and increased permeability. Thenewly developed Tie2 activating antibody, ABTAA(Angpt2 binding and Tie2 activating antibody), breaksthis vicious pro-angiogenic cycle by binding to Angpt2and activating Tie2. Tie2 activation by phosphorylation(P) triggers the PI3 kinase-Akt signaling, which phosphor-ylates FOXO1 for degradation. Overall, the blockade ofendothelial destabilizing factor, Angpt2, and activation ofTie2 for suppression of FOXO1 improves endothelial sta-bility with increased tight junction formation byVE-cadherin
58 J.-S. Park et al.

tumor vasculature, at least in part by modulatingTAMs. Genetic deletion of PlGF increases peri-cyte coverage and perfusion of tumor vesselswhile reducing tumor vessel leakage and vesselremodeling. PlGF downregulation by histidine-rich glycoprotein (HRG) inhibits tumor growthand metastasis and improves the efficacy of che-motherapy. By substantially downregulatingPlGF, polarization of TAM can be skewed fromM2-like phenotype to the antitumor M1-like phe-notype without affecting the number of TAMs(Rolny et al. 2011).
Eosinophil is another type of immune cell thatis closely linked to cancer. Tumor-associatedeosinophilia is frequently observed in patientswith cancer (Ishibashi et al. 2006; Nielsen et al.1999), but their role is still rather ambiguous. Arecent study revealed that intravenous transfer ofeosinophils can induce tumor vessel normaliza-tion and polarize TAMs to M1-like phenotype(Carretero et al. 2015). Eosinophils also secretevarious chemoattractants to enhance the migrationof cytotoxic T cells into tumor and play an impor-tant role in cancer rejection (Carretero et al. 2015).Neuropilin-1-expressing monocyte (NEM) isanother subset of monocytes with a role in tumorvessel normalization (Carrer et al. 2012). NEMssecrete various cytokines to promote pericyterecruitment and vascular smooth muscle cell pro-liferation, which leads to enhanced pericyte cov-erage of tumor vessels. Tumors injected withNEMs show reduced tumor growth and hypoxiaand enhanced perfusion and pericyte coverage.These data clearly demonstrate that NEMs repre-sent a novel subpopulation among monocytes thatcan induce tumor vessel normalization and inhibittumor growth (Carrer et al. 2012). T lymphocytes(helper T cells, cytotoxic T cells, regulatory Tcells, etc.) are also gaining considerable attentionas an integral part of cancer therapy, especiallyafter recent successes with immune checkpointinhibitors in cancer treatment (Huang et al. 2017;Reck et al. 2016). Tumor vasculature interactsclosely with T lymphocytes for their recruitmentand infiltration, and it has recently been shownthat normalized tumor vessels actually enhancethe delivery of cytotoxic T cells into tumor mass(Zhao et al. 2017). Another recent study also
showed that T lymphocytes actively participatein the process of tumor vessel normalization(Tian et al. 2017). The mutual regulatory loopformed by helper T cells and tumor endotheliumhighlights the importance of immune cells andtheir role in normalization of tumor vasculature.
Benefits of Tumor VesselNormalization
Tumor vessel normalization is anti-angiogenic innature: The process of tumor vessel normaliza-tion, whether by anti-VEGF agents or othernumerous methods described earlier, is thoughtto be anti-angiogenic in nature (Winkler et al.2004; Maes et al. 2014; Carmeliet and Jain2011b). The pro-angiogenic drive that acceleratestumor angiogenesis is mainly due to hypoxiawithin tumor mass, and severe hypoxia leads toenhanced expression and secretion of variouspro-angiogenic, destabilizing growth factors,including VEGF-A and Angpt2, which promotenew vessel formation. By normalizing tumor ves-sels, blood flow is increased; hence the deliveryof oxygen to the tumor core is also increased.Therefore, by significantly reducing tumorhypoxia, secretion of pro-angiogenic growthfactor will be reduced, ultimately generating a netanti-angiogenic effect. There are concerns, how-ever, that enhanced perfusion to tumor core mightactually aid the progression and proliferation oftumor mass, because more oxygen and nutrientswill be supplied by the normalized tumor vessels.On the contrary to this seemingly plausible idea,numerous preclinical studies to date concur on thefact that tumor growth tends to slow down or haltprogression instead (Carmeliet and Jain 2011b).These results can be explained by the reduction inmean vascular density and the net anti-angiogeniceffect of tumor vessel normalization, despite theincrease in perfusion through normalized vessels.Another important factor to be considered is tumorcells’ response to hypoxia. Normal cells cannottolerate persistent hypoxia, so it is natural to assumethat alleviating hypoxia by tumor vessel normali-zation should aid tumor growth. However, the hall-marks of tumor cells enable them to develop
Benefits and Pitfalls of Tumor Vessel Normalization 59

resistance against hypoxic damage, and a largenumber of studies indicate that hypoxia can actu-ally promote cancer growth (Eales et al. 2016;Semenza 2012). Finally, hypoxia triggers numer-ous growth factors including FGFs and IGFs alongwith VEGFs, which are all major drivers of tumorand EC growth. Accordingly, alleviating hypoxiacan eventually reduce the level of growth factorsthat tumors feed upon and ultimately lead to reduc-tion of tumor growth. Conclusively, tumor vesselnormalization generates an environment thatopposes tumor growth as well as provides a netanti-angiogenic effect.
Tumor vessel normalization synergizes withconventional chemotherapeutic drugs and radia-tion therapy: Another obvious and primary benefitof tumor vessel normalization strategy is that it cansignificantly increase the delivery of oxygen andconventional chemotherapeutic drugs, thus creat-ing synergistic effects in terms of tumor reductionand hopefully patient survival (McGee et al. 2010;Batchelor et al. 2013). High interstitial pressurecreated by leaky tumor vessel is a major physicalbarrier that obstructs the delivery of chemothera-peutic drugs through disorganized tumor vessels.Non-efficient perfusion and heterogeneity of tumorvessels also hinder homogeneous and effectivedelivery of drugs throughout tumor mass. Thesame applies for oxygen supply, with most tumorregions becoming hypoxic. Since the efficiency ofradiation therapy depends heavily on generatingreactive oxygen species and fixation of DNA dam-age by oxygen molecules, both of which needample amount of oxygen atoms inside tumormass, hypoxia is directly responsible for resistanceagainst radiotherapy (Barker et al. 2015). For thesereasons, tumor vessel normalization can help over-come these obstacles by reducing vessel leakagethrough tightening of endothelial junctions andenhancing pericyte coverage, thus enabling evenperfusion and distribution of drugs and oxygenthroughout the tumor mass.
Tumor vessel normalization reduces metastasis:Vessel normalization typically involves tighteningof endothelial junctions and enhanced coverage ofpericytes, thereby strengthening vessel walls.Whilemetastasis of tumor cells is a complex processinvolving numerous steps, the critical initial step is
tumor cell intravasation, which is defined as pene-tration of tumor cells into the bloodstream by pass-ing through endothelial barriers (Reymond et al.2013; Valastyan and Weinberg 2011). Since tightendothelial junctions and pericyte coverage makeendothelial barriers much more solid, normalizedtumor vessels are less susceptive to tumor cellintravasation compared with the initial unstabletumor vessel. Furthermore, tumor vessel normali-zation also contributes to reducing distant metasta-sis of tumor cells by generating amilder, less hostiletumor microenvironment with less hypoxia andlactic acidosis. Hypoxic tumor condition triggersgenetic mutations in tumor cells that turn them tobe more committed to distant metastasis (Bristowand Hill 2008; Nguyen and Massague 2007). Thus,tumor vessel normalization lessens genetic instabil-ity of tumor cells by alleviating hypoxia, ultimatelydecreasing the likelihood of the relatively mildertumor cells metastasizing to other organs.
Tumor vessel normalization assists the functionsof antitumor immune cells: The actions of tumorvessel normalization do not end in simply changingthe structure and function of tumor vasculature, butthe improved perfusion and oxygenation statusescontribute to significantly alter the whole tumormicroenvironment, including immune cells (Parket al. 2016). Hypoxia within tumor mass generatesan immune-suppressive microenvironment, whichinhibits the effects of cytotoxic CD8+ T cells andpolarizes TAMs into the pro-angiogenic M2-likephenotype. Also, the migration and extravasationof immune cells within tumor mass depend heavilyon intact ECs (Zhao et al. 2017). Indeed, tumorvessel normalization strategy has been demon-strated to synergize with immune checkpoint inhib-itor therapy (Schmittnaegel et al. 2017), increaseextravasation of adoptively transferred T cells intotumor (Shrimali et al. 2010), and sway the TAMpolarization to the antitumor M1-like phenotype(Park et al. 2016).
Pitfalls of Tumor Vessel Normalization
Tumor vessel normalization is transient: One ofthe major drawbacks of tumor vessel normaliza-tion strategy is that the effect is transient in nature.
60 J.-S. Park et al.

Tumor vessels are embedded within tumor micro-environment, which is vastly heterogeneous andundergoes dynamic changes; pro- and anti-angiogenic signaling similarly undergoes suchradical changes, and thus it is hard to keep upwith the changes and adequately modulate theangiogenic signaling to maintain a stable and con-stant state of tumor vessel within tumor mass(Fig. 3). Regardless, the transient normalizationeffect creates a narrow window of opportunity foreffective combination treatment. However, con-sidering that a general therapeutic regimen lasts atleast a month in the clinic, the few days of nor-malization window proven in preclinical studies isshort-handed for clinical application. The biggestchallenges to overcome for this strategy to havetranslational value are easy monitoring and
identification of these normalization windows inclinical settings.
Noninvasive methods for easy monitoring ofthe normalization status are still lacking: Relatedto the aforementioned pitfall, a solid evidence oftumor vessel normalization effect in patients isstill missing. Some noninvasive imaging tech-niques like magnetic resonance imaging (MRI)or positron emission tomography (PET) imagingwith 18-fluoromisonidazole provide some hints ofvessel function in patients (Emblem et al. 2014;Hormigo et al. 2007; Hernandez-Agudo et al.2016), but they only provide a single parameterof many that indicate successful tumor vesselnormalization. In addition, the inconvenience,expense, and lengthy duration of these imagingtechniques leave them impractical for repeated
High oxygen
Low oxygen
Normalization window
Excessive anti-angiogenesis:increased hypoxia
Normalized:reduced hypoxia
No changes
? Sustained normalization
Perf
usio
nO
xyge
natio
n
Hypoxic tumor
Duration of treatment
Fig. 3 Effects of tumor vessel normalization on perfusionand oxygenation of tumor. Tumor vasculature is abnormalboth in structure and function because pro-angiogenic sig-nals outweigh anti-angiogenic signals. This vascularabnormality initiates a vicious cycle as shown in Fig. 1,which ultimately generates a hypoxic tumor microenviron-ment. Enhancing anti-angiogenic signaling or inhibitingpro-angiogenic signaling can transiently restore the bal-ance between pro- and anti-angiogenic stimuli withintumor, resulting in normalization of tumor vessels.
Depending on the extent of anti-angiogenesis versus nor-malization, perfusion and oxygenation through tumor ves-sels may increase, decrease, or remain largely unchanged.The transient period when tumor perfusion and oxygena-tion increase by the normalized vessels is known as “nor-malization window.” Whether tumor vessel normalizingagents can generate sustained normalization and maintainhigh perfusion status for an extended period of timeremains to be seen
Benefits and Pitfalls of Tumor Vessel Normalization 61

use. Live imaging of tumor vessels in vivo isanother potential tool for visualization and moni-toring of normalization status, but it is only appli-cable in very specific situations and cannot easilybe translated into human practice.
Dose-dependent effect of anti-VEGF therapy:VEGF-blocking agents show different outcomesin terms of vessel normalization depending on theadministered dose (Jain 2013; Sorensen et al. 2012).Several preclinical trials using other normalizationagents had a similar problem (Maes et al. 2014;Zhang et al. 2015). This dose-dependent effect ofvessel normalization poses another challenge inapplying these strategies into diverse tumor modelsor patients. Each tumor has a unique microenviron-ment with greatly varying percentages of tumorvasculature, dependency on VEGF signaling, andlevel of angiogenic molecules among not onlytumor models but also individual patients. Thereare some tumors that are more responsive toanti-angiogenic therapy and some that are moreresistant. Moreover, the same tumor can have dif-ferent responses to anti-angiogenic drugs accordingto their current status (Bagri et al. 2010). Therefore,identifying the optimal amount of treatment is crit-ical to maximize the normalization effect, whichrequires tremendous effort and makes it difficult togeneralize the strategy unlike other treatmentoptions. In addition, VEGF blockade also affectsnormal vasculature, and suboptimal dose or admin-istration schedule of VEGF-blocking agents cancause adverse effects on cardiovascular, endocrine,and nervous systems and can also increase the riskof arterial thromboembolism (Jain et al. 2006).
No reliable serum marker: One of the reasonsthat anti-VEGF therapy showed limited benefit inclinical trials is that there is no reliable serummarker to monitor the effect of anti-angiogenictherapy during treatment. Likewise, it is impossi-ble to preselect patients who would benefit morefrom anti-angiogenic therapy while excludingthose who would be resistant. Same is true fortumor vessel normalization strategy. Due to theabsence of any method to monitor or predicttumor vessel normalization status in the clinic, itis impossible to accurately time any other thera-peutic modalities as a combination so that it isgiven exactly within the normalization window.
Novel biomarkers that are sensitive and specific tochanges in structural and functional aspects oftumor vessel would be ideal. Although numerouspreclinical studies and candidate molecules havebeen suggested, a successful target is yet to beidentified in the clinic.
Optimal time to induce vessel normalization isstill unclear: Although most preclinical studiesconcur on the fact that tumor vessel normalizationgenerally does not enhance tumor growth, thiseffect can differ depending on tumor size andprogression stages (Goel et al. 2013). Some pre-clinical studies indicate that, while normalizationstrategy is effective in early stages of tumor devel-opment, no apparent differences in tumor growthare observed when it is applied in later stageswhere tumor mass is considerably large; somenormalization strategies even promote tumorgrowth in later stages of tumor development(Hamzah et al. 2008). This dependency on tumorstages poses a difficult question in translatingnormalization into clinical settings. Again, thereare no absolute selection criteria to be certain thatpatients receiving normalization agents will actu-ally benefit from the treatment. Another aspect toconsider is that the benefits of normalization,namely, enhanced delivery of chemotherapeuticdrugs and oxygen and reduced metastasis, maynot coincide. Many preclinical studies demon-strate several of many features of tumor vesselnormalization, and not necessarily all parametersare examined in a single study. In this regard, thereis a possibility that different features of normali-zation are more evident in different stages; nor-malization in early stages may have the highestdrug delivery enhancement effect, whereas nor-malization in later stages may be most effective atreducing distant metastasis. A more thoroughinvestigation with preclinical models is requiredto describe the definite selection criteria for appli-cation of normalization strategy.
Translational Implications
It is interesting to note that the concept of tumorvessel normalization had been introduced ataround 2001 (Jain 2001), but its importance was
62 J.-S. Park et al.

never really addressed until very recent years. Incomparison, anti-angiogenic therapy was proposedmore than four decades ago, and more than tendrugs have been approved for clinical use. Thisvast time gap may explain why most evidence oftumor vessel normalization is still rooted in preclin-ical studies and why most clinical studies of vesselnormalization have applied anti-angiogenic drugs.This suggests that the translational potential oftumor vessel normalization is still in its infancyand is not yet fully explored.
Another important point to consider for thelack of translational progress of tumor vessel nor-malization strategy is related to the fact that it ishard to obtain tumor samples from patients duringcancer treatment, which is essential to monitormaturation status of tumor vessels. It is also cru-cial to consider the therapeutic goals that we hopeto achieve with the tumor vessel normalizationconcept. For example, should normalization beused as a stand-alone, first-line therapy for cancer,or, more likely, should it be used exclusively as acombination treatment modality with currentcytotoxic therapy? Should normalization beapplied to all stages of cancer progression, orshould it be limited to certain stages of cancerdevelopment, for instance, at the early stages?Accumulating evidence provide hints and direc-tions, but we still do not have a clear, directanswer to these intriguing questions. Most impor-tantly, is there any evidence of tumor vessel nor-malization in patients with cancer? Biopsysamples from human tumors show vascularabnormalities similar to those seen in preclinicalmodels usingmice, and it is a well-known fact thathuman tumors are embedded in hypoxic andacidic conditions with increased interstitial pres-sure (Willett et al. 2004, 2009 Bullitt et al. 2004;Wagemakers et al. 2010). However, in a limitedset of clinical trials, anti-VEGF therapy has beenshown to induce certain features that suggesttumor vessel normalization, including reducednumber of vessels, increased pericyte coverage,and reduced edema; this was observed after treat-ment with bevacizumab in advanced rectal cancerpatients (Willett et al. 2004, 2005, 2009).Although these parameters are similar to thoseobserved in animal models following anti-VEGF
treatment, these data must be interpreted withcaution and not be generalized, as the number ofpatients was quite limited. Also, even if theseresults suggest the existence of normalization phe-notype in bevacizumab-treated human cancer, it isunclear whether it is the normalization oranti-angiogenic effect that is responsible fortumor growth inhibition.
Studies using MRI also provide some evidenceof tumor vessel normalization in patients treatedwith anti-VEGF agents. For instance, administra-tion of cediranib (receptor tyrosine kinase inhibi-tor of VEGF receptors) to patients with recurrentglioblastoma showed reduced brain edema asmeasured by MRI (Batchelor et al. 2007, 2010).In this clinical trial, tumor vessel normalizationwas demonstrated by measuring vessel diameterand permeability. In case of brain tumors,increased permeability and breakdown of blood-brain barrier by the growing tumor can be life-threatening, as it results in increased intracranialpressure. Vessel normalization can restore theblood-brain barrier and reduce edema, which canreduce the risks of serious complications. MRIstudies further demonstrated that patients withrecurrent glioblastoma treated with cediranibshowed correlation between patient survival andvascular normalization index (changes in vascularpermeability, blood flow, microvascular volume,and circulating collagen IV, which indicatesremodeling of basement membrane) (Sorensenet al. 2009). Nevertheless, the effect ofanti-VEGF agents on tumor shrinkage and itscontribution to overall survival remain to be deter-mined. This is a particularly difficult question toanswer in the clinic because current imaging tech-niques are unable to discriminate betweendecrease in contrast (which is correlated with per-meability of vessels) and decrease in tumor size(Sorensen et al. 2008). However, there are pre-clinical studies indicating that anti-VEGF therapyprolongs overall survival of tumor-bearing miceby reducing intracranial pressure, even thoughtumor continues to grow (Kamoun et al. 2009;Claes et al. 2008). Other important questionsinclude whether the reduced permeability byanti-VEGF therapy can enhance the efficacy ofradiation therapy for patients with glioblastoma
Benefits and Pitfalls of Tumor Vessel Normalization 63
and whether tightening of BBB reduces orenhances delivery of chemotherapeutic drugs totumor mass. Thus, the clinical benefit of tumorvessel normalization in patients with glioblastomarequires further studies.
Similarly, in patients with hepatocellular carci-noma, inhibition of VEGFR resulted in decreasedblood flow and tumor progression and thus raisedthe question of whether normalization index canpredict the efficacy of therapy (Zhu et al. 2009). Inaddition to imaging, blood tests revealed that thelevel of soluble Flt1 in plasma correlates withdegree of tumor regression in patients with rectalcancer who received anti-VEGF therapy and neo-adjuvant chemoradiation therapy (Duda et al.2010). Another situation where tumor vessel nor-malization by anti-VEGF therapy was beneficialwas when VEGF blockade was combined withconventional chemotherapeutic drugs. Otherthan glioblastoma, the clinical use ofbevacizumab in patients with solid cancer is onlyapproved as a combination treatment with cyto-toxic drugs. The superior benefit conferred bycombination therapy was attributed to numerousmechanisms, one of which is the sensitization oftumor ECs to cytotoxic damage (Carmeliet 2005;Jain 2008). Enhanced delivery resulting from ves-sel normalization was also proposed to explain theoverall benefit of combination therapy. Thisexplanation is supported by preclinical studiesshowing that VEGF blockade induces deeper pen-etration of molecules by reducing hydrostaticpressure barrier across the vessel wall and alsoby enabling more even distribution of blood flowalong the tumor vessels (Jain 2005; Tong et al.2004; Dickson et al. 2007;Wildiers et al. 2003).
These evidence strongly imply that tumor vesselnormalization is a viable option as a combinationthat can be applied to clinical practice. Yet itspotentials that were demonstrated in preclinicalstudies have not been explored in humans. Forexample, in addition to cytotoxic drugs, anti-VEGF therapy improves immunotherapy in pre-clinical models by enhancing the accessibility ofimmune cells into the tumor (Shrimali et al. 2010;Schmittnaegel et al. 2017). As well as affecting thedrug delivery and immune cell infiltration, tumorvessel normalization can also make tumor cellsmore sensitive to chemotherapy by, for example,
reducing hypoxia and making the tumor cells thathave been exposed to drugs more proliferative andthus more susceptible to drug-induced damage(Jain 2005; Willett et al. 2004, 2009). In addition,normalization can improve tumor oxygenation andthus enhance the effect of radiation therapy, forwhich oxygen is crucial for the production of reac-tive oxygen species and DNA damage fixation.However, caution is needed when translating pre-clinical data into patient care since the effects seenin animal models may not occur in human cancer.For example, enhanced drug delivery by VEGFblockade is not a universal phenomenon observedin all preclinical models (Tailor et al. 2010). Fur-thermore, it is still not clear whether partial oxygenpressure (pO2) actually changes in human cancersbefore or after VEGF blockade, since measurementmethods and data are lacking. It is also unclear howlong the normalization effect sustains in patientswith different types of cancer and whether theeffect is the same in different stages of cancer.The precise mechanisms and benefits of normali-zation by bevacizumab treatment thus need to beinvestigated further.
Taken together, these clinical trials and preclin-ical studies provide some indirect but optimisticevidence indicating the possible therapeuticpotential of tumor vessel normalization in patientswith cancer. Clearly, additional randomized trialsinvolving patients with numerous types of cancersand larger patient populations need to beperformed to confirm these preliminary findings.In addition, whether tumor vessel normalizationcan actually increase oxygenation and drug deliv-ery in patients needs to be validated thoroughly.The future challenge would be to explore whetherthe aforementioned novel methods to normalizetumor vessels (other than anti-VEGF therapy) canpromote normalization in patients and whether itseffects are superior and more persistent comparedwith anti-VEGF therapy.
Challenges for Clinical Application
The approval of the VEGF blockade for clinicaluse has taught us several valuable lessons, themost important of them being the fact thatVEGF-blocking agents are mostly effective only
64 J.-S. Park et al.

when combined with cytotoxic drugs in terms ofhaving significant effects on patient survival (Jainet al. 2006; Gligorov et al. 2014; Taal et al. 2014).Increasing the dose of anti-angiogenic agents mayexhibit toxicity in normal tissues, increase tumorhypoxia, and impair drug delivery by removingtoo much blood vessels from tumor mass. How-ever, optimal administration dose and schedulingcan induce tumor vessel normalization withoutnoticeable damage to normal tissues. There arefew major challenges that must be resolved beforetumor vessel normalization strategy can be suc-cessfully translated into the clinic.
The first challenge is to validate which amongthe numerous normalization agents tested in pre-clinical trials is actually effective in patients.As numerous preclinical trials showed, any therapythat can restore the balance between pro-angiogenic and anti-angiogenic force can normal-ize tumor vessels – in theory. Whether these strat-egies could also induce normalization in humancancer remains to be shown. Ongoing translationalresearch should help us reduce the gaps in thisaspect of our current understanding of tumor andits vasculature. Important point to consider is thatmost clinical trials are designed to measure grosschanges like tumor size or overall survival and donot pay serious attention to vascular changes aftertreatment. More specific and clever designs of clin-ical trials are needed to shed light upon the vascularbiology of tumor.
The second challenge is to find a way to easilymonitor and measure normalization status inpatients using surrogate serum markers or moreadvanced imaging technologies. Identifying nor-malization window and vascular response to nor-malizing agents are paramount in planningcombination treatments and reducing potentialside effects. Measuring blood vessel density withbiopsy samples is too invasive and may notprovide functional information of tumor vessels.Current imaging techniques are expensive andhave a hard time tracking subtle changes, butthey can measure vascular permeability, bloodperfusion, and uptake of certain drugs toprovide some insight on normalization statusin a noninvasive manner. PET scan with18-fluoromisonidazole and MRI images can pro-vide some indication of tumor oxygenation status,
which might be useful in tracking normalizationwindow. Some studies indicate that the number ofcirculating ECs and their progenitors decreaseafter VEGF blockade (Duda et al. 2006; Willettet al. 2004, 2005), but it is not clear whether thisdecline coincides with vessel normalization.Serial blood sampling and measurement of mole-cules known to be involved in vessel maturationduring the course of normalization therapy canpotentially identify surrogate markers of normal-ization. However, the lack of accurate biomarkersand the impracticality of these methods makeclinical translation difficult.
The third challenge is to gain more compre-hensive knowledge on molecular and cellularmechanisms involved in tumor vessel normaliza-tion. It is still unclear whether the effects of nor-malizing agents depend on tumor size anddevelopmental stages, whether different tumorstages require different mechanisms for normali-zation, and whether different tumor stages aredifferently affected by tumor vessel normaliza-tion. Although there are concerns and few evi-dence of accelerated tumor growth by enhancedvessel function, the ultimate benefit that can beachieved by combining tumor vessel normaliza-tion with cytotoxic drugs as compared with cyto-toxic drug alone must be considered. A growingnumber of preclinical evidence are piling up, andwe need more innovative ideas on how to translatethe knowledge gained from preclinical studiesinto actual patient care.
Summary
Tumor needs to generate new blood vessels tosupport its growth and to invade or metastasizeinto other organs. This dependency on neo-vascularization led to the development of numer-ous therapeutic agents targeting tumorvasculature. The initial approach was to destroyor inhibit tumor angiogenesis, thereby starvingtumor of oxygen and nutrients. However, afternumerous failures in clinical trials to providesignificant survival benefits, focus has beenshifted to an alternative approach. Here, wediscussed the advent and recent progress of thecollective treatment tenet known as “tumor vessel
Benefits and Pitfalls of Tumor Vessel Normalization 65

normalization.” Much like the shift in the para-digm of oncoimmunology whereby research nowfocuses on removing the breaks rather than push-ing the accelerators, the concept of tumor vesselnormalization is a clever detour to the originalanti-angiogenic concept, whereby the tumor vas-culature is harnessed and utilized to our advan-tage, rather than destroying it. Numerous drugsand pathways have been revealed to induce tumorvessel normalization, and by normalizing thetumor vasculature, numerous side effects of con-ventional anti-angiogenic therapy can becircumvented. However, tons of work still remainin order to translate precious insights from pre-clinical studies into actual patient care. Whetherthese numerous regimens and drugs are equallyeffective against different types of cancers and onpatients with different stages of cancer progres-sion needs to be determined. Also, whether thereis an optimal agent to induce normalization indifferent types of cancers altogether or if normal-ization strategies must be tailored according toindividual patient is another important hurdlethat needs to be conquered. For immediate clinicalapplication, it would be ideal to develop a strategythat is persistent and not dose-dependent, giventhat the current technology cannot accuratelyobserve the characteristics of tumor vessels andthere are no biomarkers to help us calculate theoptimal dosage for each patient. A better insightinto the molecular mechanisms and developmentof optimal methods to induce and observe vesselnormalization will result in more potent and com-pelling therapies for numerous types of cancer.
Cross-References
▶Anti-angiogenic Targets: Angiopoietin andAngiopoietin Receptors
▶Biomarkers for Anti-angiogenic Therapy▶Combination of Anti-angiogenics and OtherTargeted Therapies
▶Controlling Vascular Permeability: How DoesIt Work and What Is the Impact on Normal andPathological Angiogenesis
▶Endothelial Cell-Cell Junctions in TumorAngiogenesis
▶ Imaging Tumor Angiogenesis▶Mechanisms of Anti-angiogenic Therapy▶Mechanisms of Tumor Angiogenesis▶ Pathology of Tumor Angiogenesis▶The Role of the VEGF Signaling Pathway inTumor Angiogenesis
▶The Role of VEGF in Controlling VascularPermeability
Acknowledgments We apologize for not being able tocite all of the original research articles and related refer-ences due to space limitations. Work in the authors’ labo-ratory is supported by funds from the Institute for BasicScience funded by the Ministry of Science, ICT and FuturePlanning, Korea (IBS-R025-D1).
References
Aragones J, Fraisl P, Baes M, Carmeliet P (2009) Oxygensensors at the crossroad of metabolism. Cell Metab9:11–22
Augustin HG, Koh GY, Thurston G, Alitalo K (2009)Control of vascular morphogenesis and homeostasisthrough the angiopoietin-tie system. Nat Rev MolCell Biol 10:165–177
Baffert F, Le T, Sennino B, Thurston G, Kuo CJ,Hu-Lowe D, Mcdonald DM (2006) Cellular changesin normal blood capillaries undergoing regression afterinhibition of VEGF signaling. Am J Physiol Heart CircPhysiol 290:H547–H559
Bagri A, Berry L, Gunter B, Singh M, Kasman I, DamicoLA, Xiang H, Schmidt M, Fuh G, Hollister B, Rosen O,Plowman GD (2010) Effects of anti-VEGF treatmentduration on tumor growth, tumor regrowth, and treat-ment efficacy. Clin Cancer Res 16:3887–3900
Barker HE, Paget JT, Khan AA, Harrington KJ (2015) Thetumour microenvironment after radiotherapy: mecha-nisms of resistance and recurrence. Nat Rev Cancer15:409–425
Batchelor TT, Sorensen AG, Di Tomaso E, Zhang WT,Duda DG, Cohen KS, Kozak KR, Cahill DP, Chen PJ,Zhu M, Ancukiewicz M, Mrugala MM, Plotkin S,Drappatz J, Louis DN, Ivy P, Scadden DT, Benner T,Loeffler JS, Wen PY, Jain RK (2007) AZD2171, apan-VEGF receptor tyrosine kinase inhibitor, normal-izes tumor vasculature and alleviates edema in glioblas-toma patients. Cancer Cell 11:83–95
Batchelor TT, Duda DG, Di Tomaso E, Ancukiewicz M,Plotkin SR, Gerstner E, Eichler AF, Drappatz J, HochbergFH, Benner T, Louis DN, Cohen KS, Chea H,Exarhopoulos A, Loeffler JS,MosesMA, Ivy P, SorensenAG,Wen PY, Jain RK (2010) Phase II study of cediranib,an oral pan-vascular endothelial growth factor receptortyrosine kinase inhibitor, in patients with recurrent glio-blastoma. J Clin Oncol 28:2817–2823
66 J.-S. Park et al.

Batchelor TT, Gerstner ER, Emblem KE, Duda DG,Kalpathy-Cramer J, Snuderl M, Ancukiewicz M,Polaskova P, Pinho MC, Jennings D, Plotkin SR, ChiAS, Eichler AF, Dietrich J, Hochberg FH,Lu-Emerson C, Iafrate AJ, Ivy SP, Rosen BR, LoefflerJS, Wen PY, Sorensen AG, Jain RK (2013) Improvedtumor oxygenation and survival in glioblastomapatients who show increased blood perfusion aftercediranib and chemoradiation. Proc Natl Acad Sci US A 110:19059–19064
Bristow RG, Hill RP (2008) Hypoxia and metabolism.Hypoxia, DNA repair and genetic instability. Nat RevCancer 8:180–192
Bullitt E, Ewend MG, Aylward S, Lin W, Gerig G, Joshi S,Jung I, Muller K, Smith JK (2004) Abnormal vesseltortuosity as a marker of treatment response of malig-nant gliomas: preliminary report. Technol Cancer ResTreat 3:577–584
Cantelmo AR, Conradi LC, Brajic A, Goveia J, Kalucka J,Pircher A, Chaturvedi P, Hol J, Thienpont B, TeuwenLA, Schoors S, Boeckx B, Vriens J, Kuchnio A,Veys K, Cruys B, Finotto L, Treps L, Stav-Noraas TE,Bifari F, Stapor P, Decimo I, Kampen K, De Bock K,Haraldsen G, Schoonjans L, Rabelink T, Eelen G,Ghesquiere B, Rehman J, Lambrechts D, MALIKAB, Dewerchin M, Carmeliet P (2016) Inhibition ofthe glycolytic activator PFKFB3 in endotheliuminduces tumor vessel normalization, impairs metasta-sis, and improves chemotherapy. Cancer Cell30:968–985
Carmeliet P (2003) Angiogenesis in health and disease. NatMed 9:653–660
Carmeliet P (2005) Angiogenesis in life, disease and med-icine. Nature 438:932–936
Carmeliet P, Jain RK (2011a) Molecular mechanisms andclinical applications of angiogenesis. Nature473:298–307
Carmeliet P, Jain RK (2011b) Principles and mechanismsof vessel normalization for cancer and other angiogenicdiseases. Nat Rev Drug Discov 10:417–427
Carrer A, Moimas S, Zacchigna S, Pattarini L, Zentilin L,Ruozi G, Mano M, Sinigaglia M, Maione F, Serini G,Giraudo E, Bussolino F, Giacca M (2012) Neuropilin-1identifies a subset of bone marrow Gr1- monocytes thatcan induce tumor vessel normalization and inhibittumor growth. Cancer Res 72:6371–6381
Carretero R, Sektioglu IM, Garbi N, Salgado OC,Beckhove P, Hammerling GJ (2015) Eosinophilsorchestrate cancer rejection by normalizing tumor ves-sels and enhancing infiltration of CD8(+) T cells. NatImmunol 16:609–617
Cho CH, Kammerer RA, Lee HJ, Steinmetz MO, Ryu YS,Lee SH, Yasunaga K, Kim KT, Kim I, Choi HH,Kim W, Kim SH, Park SK, Lee GM, Koh GY (2004)COMP-Ang1: a designed angiopoietin-1 variant withnonleaky angiogenic activity. Proc Natl Acad Sci U S A101:5547–5552
Chung AS, Lee J, Ferrara N (2010) Targeting the tumourvasculature: insights from physiological angiogenesis.Nat Rev Cancer 10:505–514
Claes A, Wesseling P, Jeuken J, Maass C, Heerschap A,Leenders WP (2008) Antiangiogenic compounds inter-fere with chemotherapy of brain tumors due to vesselnormalization. Mol Cancer Ther 7:71–78
Cully M (2017) Cancer: tumour vessel normalization takescentre stage. Nat Rev Drug Discov 16:87
Daly C, Wong V, Burova E, Wei Y, Zabski S, Griffiths J,Lai KM, Lin HC, Ioffe E, Yancopoulos GD, Rudge JS(2004) Angiopoietin-1 modulates endothelial cell func-tion and gene expression via the transcription factorFKHR (FOXO1). Genes Dev 18:1060–1071
Daly C, Eichten A, Castanaro C, Pasnikowski E, Adler A,Lalani AS, Papadopoulos N, Kyle AH, Minchinton AI,Yancopoulos GD, Thurston G (2013) Angiopoietin-2functions as a Tie2 agonist in tumor models, where itlimits the effects of VEGF inhibition. Cancer Res73:108–118
De Bock K, De Smet F, Leite De Oliveira R, Anthonis K,Carmeliet P (2009) Endothelial oxygen sensors regu-late tumor vessel abnormalization by instructing pha-lanx endothelial cells. J Mol Med (Berl) 87:561–569
De Bock K, Georgiadou M, Carmeliet P (2013) Role ofendothelial cell metabolism in vessel sprouting. CellMetab 18:634–647
De Palma M, Biziato D, Petrova TV (2017) Microenviron-mental regulation of tumour angiogenesis. Nat RevCancer 17:457–474
Dickson PV, Hamner JB, Sims TL, Fraga CH, Ng CY,Rajasekeran S, Hagedorn NL, Mccarville MB, StewartCF, Davidoff AM (2007) Bevacizumab-induced tran-sient remodeling of the vasculature in neuroblastomaxenografts results in improved delivery and efficacy ofsystemically administered chemotherapy. Clin CancerRes 13:3942–3950
Duda DG, Cohen KS, DI Tomaso E, Au P, Klein RJ,Scadden DT, Willett CG, Jain RK (2006) DifferentialCD146 expression on circulating versus tissue endo-thelial cells in rectal cancer patients: implications forcirculating endothelial and progenitor cells as bio-markers for antiangiogenic therapy. J Clin Oncol24:1449–1453
Duda DG, Willett CG, Ancukiewicz M, DI Tomaso E,Shah M, Czito BG, Bentley R, Poleski M, LauwersGY, Carroll M, Tyler D, Mantyh C, Shellito P, ClarkJW, Jain RK (2010) Plasma soluble VEGFR-1 is apotential dual biomarker of response and toxicity forbevacizumab with chemoradiation in locally advancedrectal cancer. Oncologist 15:577–583
Eales KL, Hollinshead KE, Tennant DA (2016) Hypoxiaand metabolic adaptation of cancer cells. Oncogenesis5:e190
Emblem KE, Farrar CT, Gerstner ER, Batchelor TT, BorraRJ, Rosen BR, Sorensen AG, Jain RK (2014) Vesselcaliber – a potential MRI biomarker of tumour responsein clinical trials. Nat Rev Clin Oncol 11:566–584
Falcon BL, Hashizume H, Koumoutsakos P, Chou J,Bready JV, Coxon A, Oliner JD, Mcdonald DM(2009) Contrasting actions of selective inhibitors ofangiopoietin-1 and angiopoietin-2 on the normalizationof tumor blood vessels. Am J Pathol 175:2159–2170
Benefits and Pitfalls of Tumor Vessel Normalization 67

Fenton BM, Paoni SF, Ding I (2004) Effect of VEGFreceptor-2 antibody on vascular function and oxygena-tion in spontaneous and transplanted tumors. RadiotherOncol 72:221–230
Folkman J (1971) Tumor angiogenesis: therapeutic impli-cations. N Engl J Med 285:1182–1186
Gerhardt H, Semb H (2008) Pericytes: gatekeepers intumour cell metastasis? J Mol Med (Berl) 86:135–144
Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ,Mitchell EP, Alberts SR, Schwartz MA, Benson AB3rd, Eastern Cooperative Oncology Group Study, E(2007) Bevacizumab in combination with oxaliplatin,fluorouracil, and leucovorin (FOLFOX4) for previ-ously treated metastatic colorectal cancer: results fromthe Eastern Cooperative Oncology Group StudyE3200. J Clin Oncol 25:1539–1544
Gilbert MR, Dignam JJ, Armstrong TS, Wefel JS,Blumenthal DT, Vogelbaum MA, Colman H,Chakravarti A, Pugh S, Won M, Jeraj R, Brown PD,Jaeckle KA, Schiff D, Stieber VW, Brachman DG,Werner-Wasik M, Tremont-Lukats IW, Sulman EP,Aldape KD, Curran WJJR, Mehta MP (2014) A ran-domized trial of bevacizumab for newly diagnosedglioblastoma. N Engl J Med 370:699–708
Gligorov J, Doval D, Bines J, Alba E, Cortes P, Pierga J-Y,Gupta V, Costa R, Srock S, De Ducla S,Freudensprung U, Mustacchi G (2014) Maintenancecapecitabine and bevacizumab versus bevacizumabalone after initial first-line bevacizumab and docetaxelfor patients with HER2-negative metastatic breast can-cer (IMELDA): a randomised, open-label, phase 3 trial.Lancet Oncol 15:1351–1360
Goel S, Wong AH, Jain RK (2012) Vascular normalizationas a therapeutic strategy for malignant and non-malignant disease. Cold Spring Harb Perspect Med 2:a006486
Goel S, Gupta N, Walcott BP, Snuderl M, Kesler CT,Kirkpatrick ND, Heishi T, Huang Y, Martin JD,Ager E, Samuel R, Wang S, Yazbek J, Vakoc BJ,Peterson RT, Padera TP, Duda DG, Fukumura D, JainRK (2013) Effects of vascular-endothelial protein tyro-sine phosphatase inhibition on breast cancer vascula-ture and metastatic progression. J Natl Cancer Inst105:1188–1201
Greenberg JI, Shields DJ, Barillas SG, Acevedo LM,Murphy E, Huang J, Scheppke L, Stockmann C, John-son RS, Angle N, Cheresh DA (2008) A role for VEGFas a negative regulator of pericyte function and vesselmaturation. Nature 456:809–813
Hamzah J, Jugold M, Kiessling F, Rigby P, Manzur M,Marti HH, Rabie T, Kaden S, Grone HJ, HammerlingGJ, Arnold B, Ganss R (2008) Vascular normalizationin Rgs5-deficient tumours promotes immune destruc-tion. Nature 453:410–414
Han S, Lee SJ, Kim KE, Lee HS, Oh N, Park I, Ko E, OhSJ, Lee YS, Kim D, Lee S, Lee DH, Lee KH, Chae SY,Lee JH, Kim SJ, Kim HC, Kim S, Kim SH, Kim C,Nakaoka Y, He Y, Augustin HG, Hu J, Song PH, KimYI, Kim P, Kim I, Koh GY (2016) Amelioration of
sepsis by TIE2 activation-induced vascular protection.Sci Transl Med 8:335ra55
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: thenext generation. Cell 144:646–674
Hernandez-Agudo E, Mondejar T, Soto-Montenegro ML,Megias D, Mouron S, Sanchez J, Hidalgo M, Lopez-Casas PP, Mulero F, Desco M, Quintela-Fandino M(2016) Monitoring vascular normalization induced byantiangiogenic treatment with (18)F-fluoromiso-nidazole-PET. Mol Oncol 10:704–718
Holopainen T, Huang H, Chen C, Kim KE, Zhang L,Zhou F, Han W, Li C, Yu J, Wu J, Koh GY, Alitalo K,He Y (2009) Angiopoietin-1 overexpression modulatesvascular endothelium to facilitate tumor cell dissemi-nation and metastasis establishment. Cancer Res69:4656–4664
Hormigo A, Gutin PH, Rafii S (2007) Tracking normaliza-tion of brain tumor vasculature by magnetic imagingand proangiogenic biomarkers. Cancer Cell 11:6–8
Huang FJ, YouWK, Bonaldo P, Seyfried TN, Pasquale EB,Stallcup WB (2010) Pericyte deficiencies lead to aber-rant tumor vascularization in the brain of the NG2 nullmouse. Dev Biol 344:1035–1046
Huang AC, Postow MA, Orlowski RJ, Mick R, Bengsch B,Manne S, Xu W, Harmon S, Giles JR, Wenz B,Adamow M, Kuk D, Panageas KS, Carrera C, Wong P,Quagliarello F,Wubbenhorst B, D'Andrea K, PaukenKE,Herati RS, Staupe RP, Schenkel JM, McGettigan S,Kothari S, George SM, Vonderheide RH, AmaravadiRK, Karakousis GC, Schuchter LM, Xu X, NathansonKL, Wolchok JD, Gangadhar TC, Wherry EJ (2017)T-cell invigoration to tumour burden ratio associatedwith anti-PD-1 response. Nature 545:60–65
Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T,Hainsworth J, Heim W, Berlin J, Baron A, Griffing S,Holmgren E, Ferrara N, Fyfe G, Rogers B, Ross R,Kabbinavar F (2004) Bevacizumab plus irinotecan,fluorouracil, and leucovorin for metastatic colorectalcancer. N Engl J Med 350:2335–2342
Hwang JA, Lee EH, Kim HW, Park JB, Jeon BH, Cho CH(2009) COMP-Ang1 potentiates the antitumor activityof 5-fluorouracil by improving tissue perfusion inmurine Lewis lung carcinoma. Mol Cancer Res7:1920–1927
Ishibashi S, Ohashi Y, Suzuki T, Miyazaki S, Moriya T,Satomi S, Sasano H (2006) Tumor-associated tissueeosinophilia in human esophageal squamous cell carci-noma. Anticancer Res 26:1419–1424
Jain RK (2001) Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combinationtherapy. Nat Med 7:987–989
Jain RK (2003) Molecular regulation of vessel maturation.Nat Med 9:685–693
Jain RK (2005) Normalization of tumor vasculature: anemerging concept in antiangiogenic therapy. Science307:58–62
Jain RK (2008) Lessons from multidisciplinary transla-tional trials on anti-angiogenic therapy of cancer. NatRev Cancer 8:309–316
68 J.-S. Park et al.

Jain RK (2013) Normalizing tumor microenvironment totreat cancer: bench to bedside to biomarkers. J ClinOncol 31:2205–2218
Jain RK (2014) Antiangiogenesis strategies revisited: fromstarving tumors to alleviating hypoxia. Cancer Cell26:605–622
Jain RK, Duda DG, Clark JW, Loeffler JS (2006) Lessonsfrom phase III clinical trials on anti-VEGF therapy forcancer. Nat Clin Pract Oncol 3:24–40
Jayson GC, Parker GJ, Mullamitha S, Valle JW,Saunders M, Broughton L, Lawrance J, Carrington B,Roberts C, Issa B, Buckley DL, Cheung S, Davies K,Watson Y, Zinkewich-PEOTTI K, Rolfe L, Jackson A(2005) Blockade of platelet-derived growth factorreceptor-beta by CDP860, a humanized, PEGylateddi-Fab’, leads to fluid accumulation and is associatedwith increased tumor vascularized volume. J ClinOncol 23:973–981
Kamoun WS, Ley CD, Farrar CT, Duyverman AM,Lahdenranta J, Lacorre DA, Batchelor TT, DITomaso E, Duda DG, Munn LL, Fukumura D,Sorensen AG, Jain RK (2009) Edema control bycediranib, a vascular endothelial growth factorreceptor-targeted kinase inhibitor, prolongs survivaldespite persistent brain tumor growth in mice. J ClinOncol 27:2542–2552
Kerbel R, Folkman J (2002) Clinical translation of angio-genesis inhibitors. Nat Rev Cancer 2:727–739
Kerbel RS, Kamen BA (2004) The anti-angiogenic basis ofmetronomic chemotherapy. Nat Rev Cancer 4:423–436
Kim C, Yang H, Fukushima Y, Saw PE, Lee J, Park JS,Park I, Jung J, Kataoka H, Lee D, Heo WD, Kim I,Jon S, Adams RH, Nishikawa S, Uemura A, Koh GY(2014) Vascular RhoJ is an effective and selective targetfor tumor angiogenesis and vascular disruption. CancerCell 25:102–117
Koh GY (2013) Orchestral actions of angiopoietin-1 invascular regeneration. Trends Mol Med 19:31–39
Koh YJ, Kim HZ, Hwang SI, Lee JE, Oh N, Jung K,Kim M, Kim KE, Kim H, Lim NK, Jeon CJ, Lee GM,Jeon BH, Nam DH, Sung HK, Nagy A, Yoo OJ, KohGY (2010) Double antiangiogenic protein, DAAP,targeting VEGF-A and angiopoietins in tumor angio-genesis, metastasis, and vascular leakage. Cancer Cell18:171–184
Liu J, Liao S, Huang Y, Samuel R, Shi T, Naxerova K,Huang P, Kamoun W, Jain RK, Fukumura D, Xu L(2011) PDGF-D improves drug delivery and efficacyvia vascular normalization, but promotes lymphaticmetastasis by activating CXCR4 in breast cancer. ClinCancer Res 17:3638–3648
Ma J, Pulfer S, Li S, Chu J, Reed K, Gallo JM (2001)Pharmacodynamic-mediated reduction oftemozolomide tumor concentrations by the angiogene-sis inhibitor TNP-470. Cancer Res 61:5491–5498
Maes H, Kuchnio A, Peric A,Moens S, Nys K, De Bock K,Quaegebeur A, Schoors S, Georgiadou M, Wouters J,Vinckier S, Vankelecom H, Garmyn M, Vion AC,Radtke F, Boulanger C, Gerhardt H, Dejana E,
Dewerchin M, Ghesquiere B, Annaert W, Agostinis P,Carmeliet P (2014) Tumor vessel normalization bychloroquine independent of autophagy. Cancer Cell26:190–206
Majmundar AJ, WONG WJ, Simon MC (2010) Hypoxia-inducible factors and the response to hypoxic stress.Mol Cell 40:294–309
Mazzieri R, Pucci F, Moi D, Zonari E, Ranghetti A,Berti A, Politi LS, Gentner B, Brown JL, Naldini L,De Palma M (2011) Targeting the ANG2/TIE2 axisinhibits tumor growth and metastasis by impairingangiogenesis and disabling rebounds of proangiogenicmyeloid cells. Cancer Cell 19:512–526
Mazzone M, Dettori D, Leite De Oliveira R, Loges S,Schmidt T, Jonckx B, Tian YM, Lanahan AA,Pollard P, Ruiz De Almodovar C, De Smet F,Vinckier S, Aragones J, Debackere K, Luttun A,Wyns S, Jordan B, Pisacane A, Gallez B, LampugnaniMG, Dejana E, Simons M, Ratcliffe P, Maxwell P,Carmeliet P (2009) Heterozygous deficiency of PHD2restores tumor oxygenation and inhibits metastasis viaendothelial normalization. Cell 136:839–851
Mcgee MC, Hamner JB, Williams RF, Rosati SF, Sims TL,Ng CY, Gaber MW, Calabrese C, Wu J, Nathwani AC,Duntsch C, Merchant TE, Davidoff AM (2010)Improved intratumoral oxygenation through vascularnormalization increases glioma sensitivity to ionizingradiation. Int J Radiat Oncol Biol Phys 76:1537–1545
Murata R, Nishimura Y, Hiraoka M (1997) An anti-angiogenic agent (TNP-470) inhibited reoxygenationduring fractionated radiotherapy of murine mammarycarcinoma. Int J Radiation Oncol Biol Phys37:1107–1113
Myers AL, Williams RF, Ng CY, Hartwich JE, DavidoffAM (2010) Bevacizumab-induced tumor vesselremodeling in rhabdomyosarcoma xenografts increasesthe effectiveness of adjuvant ionizing radiation. JPediatr Surg 45:1080–1085
Nagy JA, Dvorak AM, Dvorak HF (2007) VEGF-A andthe induction of pathological angiogenesis. Annu RevPathol 2:251–275
Nasarre P, Thomas M, Kruse K, Helfrich I, Wolter V,Deppermann C, Schadendorf D, Thurston G,Fiedler U, Augustin HG (2009) Host-derivedangiopoietin-2 affects early stages of tumor develop-ment and vessel maturation but is dispensable for laterstages of tumor growth. Cancer Res 69:1324–1333
Nguyen DX, Massague J (2007) Genetic determinants ofcancer metastasis. Nat Rev Genet 8:341–352
Nielsen HJR, Hansen U, Christensen IJ, Reimert CM,Brunner N, Moesgaard F (1999) Independent prognos-tic value of eosinophil and mast cell infiltration incolorectal cancer tissue. J Pathol 189:487–495
NisanciogluMH,MahoneyWM Jr, Kimmel DD, SchwartzSM, Betsholtz C, Genove G (2008) Generation andcharacterization of rgs5 mutant mice. Mol Cell Biol28:2324–2331
Park JS, Kim IK, Han S, Park I, Kim C, Bae J, Oh SJ,Lee S, Kim JH, Woo DC, He Y, Augustin HG, Kim I,
Benefits and Pitfalls of Tumor Vessel Normalization 69

Lee D, Koh GY (2016) Normalization of tumor vesselsby Tie2 activation and Ang2 inhibition enhances drugdelivery and produces a favorable tumor microenviron-ment. Cancer Cell 30:953–967
Park DY, Lee J, Kim J, Kim K, Hong S, Han S, kubota Y,Augustin HG, Ding L, Kim JW, Kim H, He Y, AdamsRH, Koh GY (2017) Plastic roles of pericytes in theblood-retinal barrier. Nat Commun 8:15296
Potente M, Gerhardt H, Carmeliet P (2011) Basic andtherapeutic aspects of angiogenesis. Cell 146:873–887
Reck M, Rodriguez-Abreu D, Robinson AG, Hui R,Csoszi T, Fulop A, Gottfried M, Peled N, Tafreshi A,Cuffe S, O’brien M, Rao S, Hotta K, Leiby MA,Lubiniecki GM, shentu Y, Rangwala R, Brahmer JR,Investigators K (2016) Pembrolizumab versus chemo-therapy for PD-L1-positive non-small-cell lung cancer.N Engl J Med 375:1823–1833
Rey S, Semenza GL (2010) Hypoxia-inducible factor-1-dependent mechanisms of vascularization and vascularremodelling. Cardiovasc Res 86:236–242
Reymond N, D’agua BB, Ridley AJ (2013) Crossing theendothelial barrier during metastasis. Nat Rev Cancer13:858–870
Rivera LB, Bergers G (2015) CANCER. Tumor angiogen-esis, from foe to friend. Science 349:694–695
Rolny C, Mazzone M, Tugues S, Laoui D, Johansson I,Coulon C, Squadrito ML, Segura I, Li X, Knevels E,Costa S, Vinckier S, Dresselaer T, Akerud P, DeMolM,Salomaki H, Phillipson M, Wyns S, Larsson E,Buysschaert I, Botling J, Himmelreich U, VanGinderachter JA, De Palma M, Dewerchin M,Claesson-Welsh L, Carmeliet P (2011) HRG inhibitstumor growth and metastasis by inducing macrophagepolarization and vessel normalization through down-regulation of PlGF. Cancer Cell 19:31–44
Saharinen P, Eklund L, Alitalo K (2017) Therapeutictargeting of the angiopoietin-TIE pathway. Nat RevDrug Discov 16:635–661
Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH,Dowlati A, Lilenbaum R, Johnson DH (2006)Paclitaxel-carboplatin alone or with bevacizumab fornon-small-cell lung cancer. N Engl J Med355:2542–2550
Schadler KL, Thomas NJ, Galie PA, Bhang DH, Roby KC,Addai P, Till JE, Sturgeon K, Zaslavsky A, Chen CS,Ryeom S (2016) Tumor vessel normalization after aer-obic exercise enhances chemotherapeutic efficacy.Oncotarget 7:65429–65440
Schmittnaegel M, Rigamonti N, Kadioglu E, Cassara A,Wyser Rmili C, Kiialainen A, Kienast Y, Mueller HJ,Ooi CH, Laoui D, De Palma M (2017) Dualangiopoietin-2 and VEGFA inhibition elicits antitumorimmunity that is enhanced by PD-1 checkpoint block-ade. Sci Transl Med 9:eaak9670
Semenza GL (2012) Hypoxia-inducible factors in physiol-ogy and medicine. Cell 148:399–408
Shrimali RK, Yu Z, Theoret MR, Chinnasamy D, RestifoNP, Rosenberg SA (2010) Antiangiogenic agents canincrease lymphocyte infiltration into tumor and
enhance the effectiveness of adoptive immunotherapyof cancer. Cancer Res 70:6171–6180
Sorensen AG, Batchelor TT, Wen PY, Zhang WT, Jain RK(2008) Response criteria for glioma. Nat Clin PractOncol 5:634–644
Sorensen AG, Batchelor TT, Zhang WT, chen PJ, Yeo P,Wang M, Jennings D, Wen PY, Lahdenranta J,Ancukiewicz M, Di Tomaso E, Duda DG, Jain RK(2009) A “vascular normalization index” as potentialmechanistic biomarker to predict survival after a singledose of cediranib in recurrent glioblastoma patients.Cancer Res 69:5296–5300
Sorensen AG, Emblem KE, Polaskova P, Jennings D,Kim H, Ancukiewicz M, Wang M, Wen PY, Ivy P,Batchelor TT, Jain RK (2012) Increased survival ofglioblastoma patients who respond to antiangiogenictherapy with elevated blood perfusion. Cancer Res72:402–407
Stockmann C, Doedens A, Weidemann A, Zhang N,Takeda N, Greenberg JI, Cheresh DA, Johnson RS(2008) Deletion of vascular endothelial growth factorin myeloid cells accelerates tumorigenesis. Nature456:814–818
Taal W, Oosterkamp HM, Walenkamp AME, Dubbink HJ,Beerepoot LV, Hanse MCJ, Buter J, Honkoop AH,Boerman D, De Vos FYF, Dinjens WNM, enting RH,Taphoorn MJB, Van den Berkmortel FWPJ, JansenRLH, Brandsma D, Bromberg JEC, Van Heuvel I,Vernhout RM, Van der Holt B, VAN den Bent MJ(2014) Single-agent bevacizumab or lomustine versusa combination of bevacizumab plus lomustine inpatients with recurrent glioblastoma (BELOB trial): arandomised controlled phase 2 trial. Lancet Oncol15:943–953
Tailor TD, Hanna G, Yarmolenko PS, Dreher MR,Betof AS, Nixon AB, Spasojevic I, Dewhirst MW(2010) Effect of pazopanib on tumor microenviron-ment and liposome delivery. Mol Cancer Ther9:1798–1808
Tian L, Goldstein A, wang H, Ching Lo H, Sun Kim I,Welte T, Sheng K, Dobrolecki LE, Zhang X, Putluri N,Phung TL,Mani SA, STOSSI F, Sreekumar A,ManciniMA, Decker WK, Zong C, Lewis MT, Zhang XH(2017) Mutual regulation of tumour vessel normaliza-tion and immunostimulatory reprogramming. Nature544:250–254
Tong RT, Boucher Y, Kozin SV, Winkler F, Hicklin DJ,Jain RK (2004) Vascular normalization by vascularendothelial growth factor receptor 2 blockade inducesa pressure gradient across the vasculature and improvesdrug penetration in tumors. Cancer Res 64:3731–3736
Valastyan S, Weinberg RA (2011) Tumor metastasis:molecular insights and evolving paradigms. Cell147:275–292
Viallard C, Larrivee B (2017) Tumor angiogenesis andvascular normalization: alternative therapeutic targets.Angiogenesis
Wagemakers M, Sie M, Hoving EW, Molema G, De BontES, Den Dunnen WF (2010) Tumor vessel biology in
70 J.-S. Park et al.

pediatric intracranial ependymoma. J NeurosurgPediatr 5:335–341
Wildiers H, Guetens G, De Boeck G, Verbeken E,Landuyt B, Landuyt W, De Bruijn EA, Van OosteromAT (2003) Effect of antivascular endothelial growthfactor treatment on the intratumoral uptake of CPT-11.Br J Cancer 88:1979–1986
Willett CG, Boucher Y, Di Tomaso E, Duda DG,Munn LL,Tong RT, Chung DC, Sahani DV, Kalva SP, Kozin SV,Mino M, Cohen KS, Scadden DT, Hartford AC,Fischman AJ, Clark JW, Ryan DP, Zhu AX,Blaszkowsky LS, Chen HX, Shellito PC, LauwersGY, Jain RK (2004) Direct evidence that the VEGF-specific antibody bevacizumab has antivascular effectsin human rectal cancer. Nat Med 10:145–147
Willett CG, Boucher Y, Duda DG, Di Tomaso E, munn LL,Tong RT, Kozin SV, Petit L, Jain RK, Chung DC,Sahani DV, Kalva SP, Cohen KS, Scadden DT,Fischman AJ, Clark JW, Ryan DP, Zhu AX,Blaszkowsky LS, Shellito PC, Mino-Kenudson M,Lauwers GY (2005) Surrogate markers for anti-angiogenic therapy and dose-limiting toxicities forbevacizumab with radiation and chemotherapy: contin-ued experience of a phase I trial in rectal cancerpatients. J Clin Oncol 23:8136–8139
Willett CG, Duda DG, Di Tomaso E, Boucher Y,ancukiewicz M, Sahani DV, Lahdenranta J, chungDC, Fischman AJ, lauwers GY, Shellito P, CZITOBG, Wong TZ, Paulson E, Poleski M, Vujaskovic Z,Bentley R, Chen HX, Clark JW, Jain RK (2009) Effi-cacy, safety, and biomarkers of neoadjuvantbevacizumab, radiation therapy, and fluorouracil in rec-tal cancer: a multidisciplinary phase II study. J ClinOncol 27:3020–3026
Winkler F, Kozin SV, Tong RT, Chae SS, Booth MF,Garkavtsev I, Xu L, Hicklin DJ, Fukumura D, DiTomaso E, Munn LL, Jain RK (2004) Kinetics ofvascular normalization by VEGFR2 blockade governs
brain tumor response to radiation: role of oxygenation,angiopoietin-1, and matrix metalloproteinases. CancerCell 6:553–563
Yonenaga Y, Mori A, Onodera H, Yasuda S, Oe H,Fujimoto A, Tachibana T, Imamura M (2005) Absenceof smooth muscle actin-positive pericyte coverage oftumor vessels correlates with hematogenous metastasisand prognosis of colorectal cancer patients. Oncology69:159–166
Yuan F, Chen Y, Dellian M, Safabakhsh N, Ferrara N, JainRK (1996) Time-dependent vascular regression andpermeability changes in established human tumorxenografts induced by an anti-vascular endothelialgrowth factor/vascular permeability factor antibody.Proc Natl Acad Sci U S A 93:14765–14770
Zhang H, Ren Y, Tang X, Wang K, Liu Y, Zhang L, LI X,Liu P, Zhao C, He J (2015) Vascular normalizationinduced by sinomenine hydrochloride results insuppressed mammary tumor growth and metastasis.Sci Rep 5:8888
Zhao Y, Ting K, Li J, Cogger VC, Chen J, Johansson-Percival A, Ngiow SF, Holst J, Grau GER, Goel S,Moller T, Dejana E, Mccaughan GW, Smyth MJ,Ganss R, Vadas MA, Gamble JR (2017) Targetingvascular endothelial-cadherin in tumor-associatedblood vessels promotes T cell-mediated immunother-apy. Cancer Res 77:4434–4447
Zhu AX, Sahani DV, Duda DG, Di Tomaso E,Ancukiewicz M, Catalano OA, Sindhwani V,Blaszkowsky LS, Yoon SS, Lahdenranta J,Bhargava P, Meyerhardt J, Clark JW, Kwak EL, HezelAF, Miksad R, Abrams TA, Enzinger PC, Fuchs CS,Ryan DP, Jain RK (2009) Efficacy, safety, and potentialbiomarkers of sunitinib monotherapy in advancedhepatocellular carcinoma: a phase II study. J ClinOncol 27:3027–3035
Ziyad S, Iruela-Arispe ML (2011) Molecular mechanismsof tumor angiogenesis. Genes Cancer 2:1085–1096
Benefits and Pitfalls of Tumor Vessel Normalization 71





























