Embed Size (px)
Citation preview

Eur J Vasc Endovasc Surg (2014) -, 1e11
REVIEW
Beneficial Effects of Pre-operative Exercise Therapy in Patients with anAbdominal Aortic Aneurysm: A Systematic Review
S. Pouwels a,b, E.M. Willigendael c, M.R.H.M. van Sambeek a, S.W. Nienhuijs d, P.W.M. Cuypers a, J.A.W. Teijink a,b,*
a Department of Vascular Surgery, Catharina Hospital, Michelangelolaan 2, 5602 ZA Eindhoven, The Netherlandsb Department of Epidemiology, CAPHRI Research School, Maastricht University, Maastricht, The Netherlandsc Department of General and Vascular Surgery, Medical Centre Alkmaar, Alkmaar, The Netherlandsd Department of General Surgery, Catharina Hospital, Eindhoven, The Netherlands
* CoCatharNetherE-ma1078
Surgeryhttp:
PleaseSystem
WHAT THIS PAPER ADDS
This review provides an overview of the current evidence on pre-operative exercise therapy in patients with anabdominal aortic aneurysm (AAA; with or without indication for surgical repair). Pre-operative exercise therapyhas potential beneficial effects on such variables as physical fitness, reduction in cardiovascular risk factors, post-operative complications, length of stay, and recovery. Further research is needed to investigate the mosteffective pre-operative exercise program for patients with AAA.Objective/background: The impact of post-operative complications in abdominal aortic aneurysm (AAA) surgeryis substantial, and increases with age and concomitant co-morbidities. This systematic review focuses on thepossible effects of pre-operative exercise therapy (PET) in patients with AAA on post-operative complications,aerobic capacity, physical fitness, and recovery.Methods: A systematic search on PET prior to AAA surgery was conducted. The methodological quality of theincluded studies was rated using the Physiotherapy Evidence Database scale. The agreement between thereviewers was assessed with Cohen’s kappa.Results: Five studies were included, with a methodological quality ranging from moderate to good. Cohen’skappa was 0.79. Three studies focused on patients with an AAA (without indication for surgical repair) withphysical fitness as the outcome measure. One study focused on PET in patients awaiting AAA surgery and onestudy focused on the effects of PET on post-operative complications, length of stay, and recovery.Conclusion: PET has beneficial effects on various physical fitness variables of patients with an AAA. Whether thisleads to less complications or faster recovery remains unclear. In view of the large impact of post-operativecomplications, it is valuable to explore the possible benefits of a PET program in AAA surgery.� 2014 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.Article history: Received 21 July 2014, Accepted 14 October 2014, Available online XXXKeywords: Abdominal aortic aneurysm, Abdominal surgery, Complications, Exercise training, Physical fitness,
Preconditioning
INTRODUCTION
The development of an abdominal aortic aneurysm (AAA) isage related, and affects approximately 7.5% of men and3.0% of women.1 Surgical intervention (open reconstructionor endovascular) is the only treatment effective in
rresponding author. J.A.W. Teijink, Department of Vascular Surgery,ina Hospital, Michelangelolaan 2, 5602 ZA Eindhoven, Thelands.il address: [email protected] (J.A.W. Teijink).-5884/$ e see front matter � 2014 European Society for Vascular. Published by Elsevier Ltd. All rights reserved.//dx.doi.org/10.1016/j.ejvs.2014.10.008
cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeatic Review, European Journal of Vascular and Endovascular Surgery (2
preventing AAA rupture and aneurysm related death. Ingeneral, this treatment is reserved for AAAs >55 mm indiameter and >50 mm in men and women, respectively.2
Surgical intervention, especially open repair, results in sig-nificant hemodynamic stress and an increased oxygen de-mand in the peri- and post-operative period.3,4 A minimumlevel of aerobic capacity and physical fitness is required tomaintain an adequate response to the physical stressinduced by surgical intervention.
The majority of patients with an AAA eligible for repairare >65 years of age. Relatively fit octogenarians present-ing with large AAAs are no longer an exception.5e7 Togetherwith the advancing age of AAA patients comes a poorer
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

2 S. Pouwels et al.
functional capacity due to multiple co-morbidities and anincreased risk for post-operative complications.7,8
An extensive cardiopulmonary co-morbidity is present inthis population compared with the population requiringnon-vascular major abdominal surgery (coronary disease orcongestive heart failure, w50%; hypertension, 30e50%;chronic obstructive pulmonary disease, 30e40%; chronicrenal disease, w5%; cerebrovascular disease, w6%).5e8 (5-8) Surgery can also induce a decline in functional capacity(especially in the elderly), which has detrimental effects ongeneral health.5e8 By improving the physical condition,peri-operative complications might be prevented. In thenon-surgical population there is evidence demonstratingthe beneficial effects of exercise on improving fitness inpatients with cardiorespiratory disease.9e12 There isincreasing evidence that pre-operative exercise therapy(PET) is effective in reducing post-operative complicationsand length of hospital stay after surgical interventions.13e16
However, the effectiveness of PET might vary betweendifferent surgical interventions, as well as patient pop-ulations.13e16 A different approach in the design of PETprograms seems necessary; however, evidence for a specificdesign is still lacking.
A recent systematic review by Valkenet et al. (17) showedthat PET programs can be effective in reducing post-operative complications and length of hospital stay.17
However, this study did not include any subgroup analysisbetween different patient groups and their specific surgicalinterventions. For example, a patient with colorectal cancerhas, owing to pre-operative chemoradiation, a limited pre-operative time span for a PET program compared with apatient scheduled for an elective AAA repair. Also, there isno evidence for the effectiveness of different PET programs.So far, the level of evidence is insufficient to have a pref-erence for an endurance training program or a strengthprogram, or a combination of both. Each specific patientpopulation could need a specific program in a specific timeframe.
A systematic review of PET in AAA surgery and the effecton post-operative complications, aerobic capacity, physicalfitness, and recovery was carried out in an attempt toanswer the following research questions: (1) What is theeffect of an exercise program in patients with an AAA oriliac artery aneurysm (IAA) (with or without an indicationfor surgical repair) on aerobic fitness and physical param-eters?; (2) What is the effect of PET in patients with an AAAor IAA scheduled for surgical repair on the post-operativecomplications and the length of hospital stay?
METHODS
A systematic literature search was performed. The popula-tion of interest was patients with an AAA or IAA, and pa-tients scheduled for surgical repair of an AAA or IAA. Theintervention studied was PET (in case of patients scheduledfor surgical repair) or an exercise program (in case of pa-tients without an indication for surgical repair) comparedwith standard care (no exercise program). Outcome
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
measures were aerobic capacity, physical fitness, post-operative complications, length of stay, and recovery.
PubMed, Embase, MEDLINE, The Cochrane Library, PEDro,CINAHL, and Web Of Knowledge were searched from theearliest date of each database up to May 2014. The searchfor publications was performed using the following searchstring: ([“Abdominal Aortic Aneurysm” {MeSH} OR EVAR ORopen repair]) AND (“Physical Therapy Modalities” [MeSH]OR physical therapy OR physiotherapy OR “Exercise”[MeSH] OR exercise).
S.P. and E.M.W., who were both blinded to the authors ofpapers and titles of journals, separately screened andselected studies on the basis of title and abstract. Afterprimary selection, both authors reviewed the full text of theselected studies and, based on the established selectioncriteria, determined suitability for inclusion. For furthereligible studies, cross references were screened. Disagree-ments were solved by discussion with each other and thesenior author (J.A.W.T.) until consensus was reached.
Inclusion criteria
The inclusion criteria for the studies were as follows: (i) arandomized controlled or prospective cohort trial; (ii)eligible participants were all patients with an AAA or IAA(without indication for surgical repair) and were scheduledfor surgical repair of an AAA or IAA; (iii) the interventionconsisted of a PET program, which was defined as a struc-tured regimen of physical activities (either a standaloneregimen, home based, or supervised) for specific thera-peutic goals to gain or increase musculoskeletal and/orcardiovascular and/or respiratory function; (iv) reportedoutcome measurements were improvement of aerobic ca-pacity and/or physical fitness, post-operative complications,length of stay, and recovery.
Rating of methodological quality was conducted usingthe Physiotherapy Evidence Database (PEDro) scale.18,19
The PEDro scale has 11 criteria, with a maximum score of10 (range 0e10) as the first item (the specification of theeligibility criteria) is not included in the total score. Twoauthors (S.P. and E.M.W.) separately rated the methodo-logical quality of each included study, according to thePEDro scale, and the following classification was used: ascore of <4 indicated poor methodological quality, between4 and 5 fair quality, 6e8 good quality, and 9e10 excellentquality.20
The level of agreement between the authors wasassessed by a Cohen’s kappa score, which was determinedas follows: <0.20 poor agreement; 0.21e0.40 fair agree-ment; 0.41e0.60 moderate agreement; 0.61e0.80 goodagreement; 0.81e1.00 very good agreement.21
Exercise physiology definitions
In exercise physiology and in this systematic reviewdifferent terms will be used to describe and measure theeffect of a PET program. Two different terms are often used:physical activity and physical fitness.22 Physical activity isdefined as any bodily movement produced by skeletal
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

Pre-operative Exercise Therapy in Patients with AAA 3
muscles, which results in energy expenditure. The amountof energy required to accomplish activity can be measuredin kilojoules (kJ) or kilocalories (kcal).22
Physical fitness or “being physically fit” is defined as “theability to carry out daily tasks with vigor and alertness,without undue fatigue and with ample energy to enjoy lei-sure time pursuits and to meet unforeseen emergencies”.22
For measuring the effect of PET programs, a variety ofterms can be used. The most commonly used terms are“aerobic threshold”, “ventilatory threshold”, and “VO2
peak”.23 When the body uses energy, two systems are used:(i) the aerobic system, which uses oxygen and burns car-bohydrates and fats; (ii) the anaerobic system, whichdoesn’t require oxygen. The aerobic threshold is the level ofeffort at which anaerobic energy pathways start to be asignificant part of the energy production.23
VO2 peak is defined as the highest value of VO2 attainedat the particular test, most commonly an incremental orhigh energy test, designed to bring the subject to the limitof tolerance.23
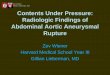
Figure 1. Preferred Reporting Items for Systematic R
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
The ventilatory threshold is the point during exercise atwhich pulmonary ventilation becomes disproportionatelyhigh with respect to the oxygen consumption. This point isbelieved to be the onset of use of the anaerobicpathway.23
RESULTS
The primary literature search produced 712 results,including 40 duplicates. After screening of the titles andabstracts, eight studies were found to be possibly relevantand underwent a full text critical appraisal, which resultedin three being excluded. One study was only available inDanish,24 one was a research protocol,25 and one was aninvited commentary.26
Fig. 1 summarizes the search results. The methodologicalquality of the included studies ranged from moderate togood, indicated by the PEDro scale (Table 1). A Cohen’skappa of 0.79 reflected a good agreement between theauthors (S.P. and E.M.W.). Table 2 gives an overview of theresults of the included studies.
eviews and Meta-Analyses (PRISMA) flowchart.
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

Table 1. Assessment of methodological quality using the Physiotherapy Evidence Database (PEDro) score.18
Study Criteriaa
1 2 3 4 5 6 7 8 9 10 11 TotalDronkers et al., 200830 � � � � e e � � � � � 8Kothmann et al., 200929 � � � � e e e � � � � 7Myers et al., 201028 � � � � e e e � � � � 7Barakat et al., 20143 � e e � e e e � � � � 5Tew et al., 201227 � � � � e e e � � � � 7
a PEDro criteria: (1) specification of eligibility criteria (this criterion was not counted for the final score); (2) random allocation; (3) con-cealed allocation; (4) prognostic similarity at baseline; (5) participant blinding; (6) therapist blinding; (7) outcome assessor blinding; (8)>85% follow up of at least one key outcome; (9) intention to treat analysis; (10) between or within group statistical comparison; (11) pointestimates of variability provided.18
4 S. Pouwels et al.
Three of the included studies investigated an exerciseprogram in patients with an AAA (without indication forsurgical repair),27e29 with a duration ranging from 6 weeksto 12 months. Barakat et al. studied a PET program for 6consecutive weeks in patients awaiting elective infrarenalAAA repair.3 Dronkers et al. studied an inspiratory muscletraining program for at least 2 weeks before surgery inpatients awaiting elective AAA repair.30
Effects of an exercise program in patients with an AAA,without indication for surgical repair
Compliance. Tew et al. found a 94% compliance rate to anexercise program (three sessions a week for a period of 12consecutive weeks), with 371 of 396 sessions attended.27
Physical fitness parameters. Three studies investigatedphysical fitness parameters. Myers et al. found a significantincrease in exercise time in the intervention group after 12months training (from 495.8 � 182.0 s to 701.2 � 209.0 s;p ¼ .01 between groups).28 The peak VO2 did not differbetween baseline values and after 12 months of training,and between groups (exercise group: 18.5 � 5.9 mL/kg/minto 20.0 � 5.5 mL/kg/min; control group: 21.6 � 7.8 mL/kg/min to 20.2 � 7.9 mL/kg/min (p ¼ .29 between groups)).28
Kothmann et al. found a 10% increase in aerobicthreshold (equivalent to 1.1 mL O2/kg/min) after 6 weeks ofsupervised exercise training, between the intervention andcontrol group.29
Tew et al. showed that the ventilatory threshold (from12.8 � 2.4 mL/kg/min to 15.3 � 3.9 mL/kg/min) increasedin the intervention group after pre-operative training for 12consecutive weeks.27 Between groups there was a signifi-cant difference in ventilatory threshold (p ¼ .02). Therewere no significant changes in both groups for peak valuesof heart rate, blood lactate, perceived exertion, and respi-ratory exchange ratio (p > .05).27
Training intensity.Myers et al. reported training intensity asa percentage of target heart rate.28 Each patient docu-mented their heart rate in a diary. Over the year, heart raterecordings documented a mean training intensity of98 � 7%. Training intensity did not differ between homebased or supervised exercise training (average heart rate99 � 7% of the target and 97 � 8% of the target,respectively).28
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
Effects of pre-operative exercise therapy in patientsscheduled for surgical repair of an AAA
Compliance. Barakat et al. reported a minimum attendanceof the supervised exercise program classes during 6 weeksof 70%,3 with 12 of the 20 patients attending 100% of theclasses.
Physical fitness parameters. After a three training sessionsa week program for 6 consecutive weeks, Barakat et al.showed that peak VO2 significantly improved, from 18.2 mL(range 15.4e19.9 mL) O2/kg/min to 19.9 mL (range 17.1e21.1 mL) O2/kg/min (p ¼ .05).3 The aerobic threshold alsoimproved significantly, from 12.2 mL (range 10.5e14.9 mL)O2/kg/min to 14.4 mL (range 12.3e15.4 mL) O2/kg/min(p ¼ .023).3
Post-operative complications. Dronkers et al. investigatedthe effects of an inspiratory muscle training program con-sisting of six sessions a week for 6 weeks prior to surgery in20 patients at high risk for post-operative pulmonarycomplications.30 Dronkers et al. reported the developmentof atelectasis in eight patients in the control group andthree in the intervention group (p ¼ .07).30 The atelectasiswas evident on the chest Xrays for a median of 1.5 days inthe control group and of 0 days in the intervention group(p ¼ .07).30
Respiratory function. Before AAA surgery, Dronkers et al.found no change in mean maximal inspiratory pressure(MIP; from 68 � 19 cmH2O to 72 � 22 cmH2O [p ¼ .32])after 6 weeks of pre-operative inspiratory muscle training inthe intervention group.30 Over the same period the meanMIP in the control group changed from 83 � 15 cmH2O to80 � 24 cmH2O (p ¼ .60). There was also no significantdifference between the groups (p ¼ .29).30
Before surgery, the mean inspiratory muscle enduranceincreased significantly from 32 � 8 cmH2O to 43 � 9 cmH2O(p ¼ .05) after pre-operative training in the interventiongroup and from 39 � 10 cmH2O to 43 � 9 cmH2O (p ¼ .36)in the control group. There were no significant differencesbetween both groups (p ¼ .12).30
Patient satisfaction. In the intervention group of the studyof Dronkers et al.,30 eight patients completed a question-naire 2 weeks after discharge. The questionnaire showedhigh patient motivation to complete the pre-operative
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

Table 2. Overview of included studies.
Study (þdesign) Participants Intervention Primary outcomemeasure
Study resultsn (M/F) Characteristics I: n (age [y] � SD)
C: n (age � SD)Treatment Comparison
Dronkers et al.,2008 (RCT)30
20 (5/15) Candidates forelective AAA athigh risk of PPCs
I: 10.0 (59.0 � 6.0)C: 10.0 (70.0 � 6.0)
IMT, starting at20% of thepatients Pi-max,6 days a week,15 min per sessionfor at least 2 weeks
Instruction indiaphragmaticbreathing,incentivespirometry,forced expirationtechniques(defined asusual care)
Post-operativepulmonarycomplicationsMIME afterinspiratorymuscle trainingCompliance
Atelectasis:
� I: 3� C: 8� p ¼ .07
Duration of atelectasis:
� I: 0 days� C: 1.5 days� p ¼ .07
Increase MIME beforesurgery:
� I: 32 � 8 to43 � 14 cmH2O(p ¼ .05)
� C: 39 � 10 to43 � 9 cmH2O(p ¼ .36)
� no differencebetween groups(p ¼ .12)
Kothmann et al.,2009 (RCT)29
25 (20/5) Patients with AAAunder surveillance(<5.5 cm onabdominalultrasound)
I: 17.0 (69.5 � ?)C: 8.0 (69.4 � ?)
6 weeks hospitalbased exerciseprogram. Twosupervised sessionsper week, whichconsisted of 30min exercise on astatic bicycle
Regular care Change inaerobic threshold
AT:
� 10% increase(equivalent to1.1 ml O2/kg/min)in interventiongroup comparedwith control(p ¼ .01)
Continued
Pre-operative
ExerciseTherap
yin
Patients
with
AAA
5
Pleasecite
thisarticle
inpress
as:Po
uwels
S,etal.,B
eneficialEffects
ofPre-o
perative
ExerciseTherap
yin
Patientswith
anAbdominalA
ortic
Aneu
rysm:A
Systematic
Review
,Europ
eanJournal
ofVascu
larandEndovascu
larSurgery
(2014),http
://dx.d
oi.org/10.1016/j.ejvs.2014.10.008

Table 2-continued
Study (þdesign) Participants Intervention Primary outcomemeasure
Study resultsn (M/F) Characteristics I: n (age [y] � SD)
C: n (age � SD)Treatment Comparison
Myers et al.,2010 (RCT)28
57 (53/4) Patients with AAA(<5.5 cm)
I: 26.0 (73.1 � 6.0)C: 31.0 (70.4 � 9.0)
Exercise training(supervised orat home, orcombination). Goalof training was toachieve a meanenergy expenditureof 2000 kcal/wk. Thesupervised sessionsincluded treadmillcycle ergometry, stairclimbing, ellipticaltraining, and rowingthree times weeklyfor 45 min followedby 10 min of resistancetraining
Regular care Mean energyexpenditureExercise capacityRisk markersbefore andafter training
� I: mean energyexpenditure of2269 � 1207kcal/wk. Increasedexercise capacity(42% increase intreadmill time,24% increase inestimatedmetabolicequivalents,p ¼ .01)
� Between I and Cp ¼ .08 forexercise capacityand estimatedmetabolicequivalents
� I: significantreduction inCRP1 comparedwith C (p ¼ .05)
6S.
Pouwels
etal.
Pleasecite
thisarticle
inpress
as:Po
uwels
S,etal.,B
eneficialEffects
ofPre-o
perative
ExerciseTherap
yin
Patientswith
anAbdominalA
ortic
Aneu
rysm:A
Systematic
Review
,Europ
eanJournal
ofVascu
larandEndovascu
larSurgery
(2014),http
://dx.d
oi.org/10.1016/j.ejvs.2014.10.008

Barakat et al.,2014 (PCCS)3
20 (17/3) Patients scheduledfor electiveinfrarenal AAAinterventions(open orendovascular)
I: 20.0 (74.9 � 5.9) Supervised pre-operativeexercise program for atotal of 6 weeks, 3sessions per week.Each exercise sessioncomprised of a totalof 1 h, consisting of6e8 different exercises,including: heel raises,cycle ergometer, step-ups,arm weights, kneeextensions, chair sit-ups,knee flexions, and gradedtreadmill exercise, witha 5 min warm up/cooldown routine at thebeginning/end of eachsession
Exercise capacity(measured as VO2
peak and aerobicthreshold)Compliance
VO2 peak:
� Before: 18.2ml/kg/min (range15.4e19.9ml/kg/min)
� After: 19.9 ml/kg/min (17.1e21.1ml/kg/min)
� p ¼ 0.05
AT:
� Before: 12.2 ml/kg/min (range10.5e14.9 ml/kg/min)
� After: 14.4 ml/kg/min (range12.3e15.4 ml/kg/min)
� p ¼ .02
Time at AT:
� Before: 137.0 s(range 86.8e234.5 s)
� After: 200.5 s(range 93.8e397.5 s)
� p ¼ .05
Total time:
� Before: 379.0 s(233.3e653.3 s)
� After: 603.5 s(406.5e715.0 s)
� p < .01
Continued
Pre-operative
ExerciseTherap
yin
Patients
with
AAA
7
Pleasecite
thisarticle
inpress
as:Po
uwels
S,etal.,B
eneficialEffects
ofPre-o
perative
ExerciseTherap
yin
Patientswith
anAbdominalA
ortic
Aneu
rysm:A
Systematic
Review
,Europ
eanJournal
ofVascu
larandEndovascu
larSurgery
(2014),http
://dx.d
oi.org/10.1016/j.ejvs.2014.10.008

Table 2-continued
Study (þdesign) Participants Intervention Primary outcomemeasure
Study resultsn (M/F) Characteristics I: n (age [y] � SD)
C: n (age � SD)Treatment Comparison
Tew et al.,2012 (RCT)27
25 (21/4) Patients with anasymptomatic,infrarenal AAA30e50 mm indiameter
I: 11.0 (71.0 � 8.0)C: 14.0 (74.0 � 6.0)
Supervised exercisetraining three times aweek, for 12 consecutiveweeks. Each sessionconsists of a mixtureof treadmill walkingand cycle ergometry for35e45 min
Standard care(encouragementto exercise only)
Exercise capacity(measured as VO2
peak and aerobicthreshold)Cardiovascularrisk markers
Ventilatory threshold:I: Baseline12.8 � 2.4 ml/kg/minAfter 12 weeks15.3 � 3.9 ml/kg/minC: Baseline12.2 � 3.3 ml/kg/minAfter 12 weeks12.2 � 3.1 ml/kg/min(p ¼ .02 between Iand C after 12 weeks)VO2 peak:I: Baseline19.3 � 4.5 ml/kg/minAfter 12 weeks21.1 � 6.7 ml/kg/minC: Baseline17.9 � 5.4 ml/kg/minAfter 12 weeks18.0 � 5.7 ml/kg/min(p ¼ .18 between I andC after 12 weeks)SBP:I: Baseline149.0 � 25.0 mmHg After12 weeks 138.0 � 20.0 mmHgC: Baseline152.0 � 26.0 mmHg After12 weeks 148.0 � 15.0 mmHg(p ¼ .10 between I and Cafter 12 weeks)hs-CRP:I: Baseline1.4 � 1.1 mg/L After12 weeks 0.9 � 0.9 mg/LC: Baseline2.3 � 1.5 mg/L After 12weeks 2.6 � 1.6 mg/L(p ¼ .01 between I and Cafter 12 weeks)
Note. M ¼male; F ¼ female; I ¼ intervention; C ¼ control; RCT ¼ randomized controlled trial; PCCS ¼ prospective cohort comparative study; AAA ¼ abdominal aortic aneurysm; PPC ¼ post-operative pulmonary complications; IMT ¼ inspiratory muscle training, Pi-max ¼ maximum inspiratory pressure; MIME ¼ mean inspiratory muscle endurance; CRP ¼ C-reactive protein;AT ¼ aerobic threshold; VO2 peak ¼ maximum oxygen uptake; SBP ¼ systolic blood pressure; hs-CRP ¼ high sensitivity CRP.
8S.
Pouwels
etal.
Pleasecite
thisarticle
inpress
as:Po
uwels
S,etal.,B
eneficialEffects
ofPre-o
perative
ExerciseTherap
yin
Patientswith
anAbdominalA
ortic
Aneu
rysm:A
Systematic
Review
,Europ
eanJournal
ofVascu
larandEndovascu
larSurgery
(2014),http
://dx.d
oi.org/10.1016/j.ejvs.2014.10.008

Pre-operative Exercise Therapy in Patients with AAA 9
intervention, but revealed no influence on the quality of lifeof the PET program.
DISCUSSION
This systematic review highlights the current evidence onthe effects of PET and other exercise programs in patientswith an AAA (with and without indication for surgicalrepair). The studies report on the measured effects of PETon aerobic capacity, physical fitness, post-operative com-plications, length of stay, and duration of recovery. Themethodological quality of the five included studies rangedfrom moderate to good.
Recently, two studies reviewed the effect of PET onphysiological function,31 complications, and recovery aftersurgery.17 They both concluded that the evidence forbeneficial effects of PET was limited. The major disadvan-tage of these studies was a very heterogeneous patientpopulation with non-comparable PET programs.
Positive effects of pre-operative PET programs (endur-ance or cardiopulmonary) have been described in the AAApopulation and the elderly in general. PET reduces the riskof all cause (peri-operative) mortality and morbidity in theAAA patient population owing to an improvement of car-diopulmonary fitness.32,33 Also, pre-operative fitness levelsare associated with higher survival rates in patients un-dergoing open surgical AAA repair and other majorabdominal surgery.34,35
PET can be beneficial in various types of surgery and mayreduce post-operative complications. The incidence of post-operative (pulmonary) complications varies, depending ontheir definition and type of surgery. The reported incidenceof post-operative pulmonary complications varies between5% and 30%.36,37 Post-operative complications are the pri-mary reason for post-operative morbidity and mortality andincreased length of hospital stay, medical consumption, andhealthcare costs.36e39 In the case of pulmonary complica-tions, atelectasis predisposes a patient to more clinicallyrelevant complications, such as pneumonia.40 Atelectasisoccurring from the second post-operative day onward isconsidered to affect blood oxygenation and bronchialmucus production.36
Several studies in different surgical specialties investi-gated whether PET reduces post-operative complicationsand improves physical fitness. Two studies reported positiveresults on PET-induced improved pre-operative physicalfitness in patients awaiting lung resection surgery.13
Two additional studies showed reduced post-operativecomplications and length of hospital stay in cardiac sur-gery after a PET program (pre-operative pulmonary phys-iotherapy and exercise training).15
The available literature on the effects of PET on importantprimary endpoints like post-operative complications, lengthof hospital stay, and duration of recovery all suffer from thesame difficulties. The PET protocols used are diverse. Isthere any evidence for an optimal effective training pro-gram in a potentially high risk (elderly) patient group? Onthe matter of the training intensity, evidence suggests that
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
continuous exercise at a higher intensity leads to greaterimprovements of the aerobic threshold.40e42 Also, very highintensity interval training is more effective than continuousmoderate exercise training.25,43 A superior training effect ofexercise training at 95% of the peak heart rate comparedwith an exercise regimen at 70% of the peak heart rate hasbeen reported.43 Evidence suggests that with respect to thelength of the training, regular exercise for the duration of atleast 12 weeks at a moderate intensity significantly im-proves the level of fitness in elderly people.44,45
Patient safety during the exercise program in this elderlypopulation has been studied and records a risk of seriousadverse events of approximately 1:10,000 with exercisetesting in high risk patients.46 Recently, Gommans et al.reported a low risk of adverse events in an exercise popu-lation of patients with peripheral arterial disease undergo-ing a supervised exercise therapy program.47
Future perspectives
The specific goal of pre-operative exercise training is toprepare patients for surgery in the best possible way toreduce complications, length of stay, and healthcare costs.This is the first systematic review on the effects of PET inAAA surgery, but with only five heterogeneous studieseligible for inclusion there is room and a necessity for futureresearch. Current evidence shows PET in AAA surgery haspotential beneficial effects. To be able to perform highquality future research, definitions of PET, including exerciselength, intensity, and method, should be determined andcompared.
Future improvements in standards of care and optimalpre-operative preparation should not only focus of thesurgical team and the hospital organization, but also onincorporating the active role of the patient.
CONCLUSION
PET may have beneficial effects on various physical fitnessvariables in patients with an AAA. Whether this leads tofewer complications or faster recovery remains promisingbut unclear, because of the great heterogeneity and smallsample size of the included studies. In view of the largeimpact of post-operative complications, it would be valu-able to explore the possible benefits of a PET program inAAA surgery.
FUNDING
None.
CONFLICT OF INTEREST
None.
REFERENCES
1 Lederle FA, Johnson GR, Wilson SE. The aneurysm detectionand management study screening program: validation cohortand final results. Aneurysm Detection and Management Vet-erans Affairs Cooperative Study Investigators. Arch Intern Med2000;160:1425e30.
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

10 S. Pouwels et al.
2 Baxter BT, Terrin MC, Dalman RL. Medical management ofsmall abdominal aortic aneurysms. Circulation 2008;117:1883e9.
3 Barakat HM, Shahin Y, Barnes R, Gohil R, Souroullas P, Khan J,et al. Supervised exercise program improves aerobic fitness inpatients awaiting abdominal aortic aneurysm repair. Ann VascSurg 2014;28:74e9.
4 Older P, Hall A. Clinical review: how to identify high-risk sur-gical patients. Crit Care 2004;8:369e72.
5 Pol RA, Zeebregts CJ, van Sterkenburg SMM, Reijnen MMPJ.Thirty-day outcome and quality of life after endovascularabdominal aortic aneurysm repair in octogenarians based onthe Endurant Stent Graft Natural Selection Global PostmarketRegistry. J Vasc Surg 2012;56:27e35.
6 Visser L, Pol RA, Tielliu IFJ, van den Dungen JJAM, Zeebregts CJ.A limited and customized follow-up seems justified afterendovascular abdominal aneurysm repair in octogenarians.J Vasc Surg 2014;59:1232e40.
7 Karthikesalingam A, Holt PJ, Vidal-Diez A, Ozdemir BA,Poloniecki JD, Hinchliffe RJ, et al. Mortality from rupturedabdominal aortic aneurysms: clinical lessons from a comparisonof outcomes in England and the USA. Lancet 2014;383:963e9.
8 De Martino RR, Goodney PP, Nolan BW, Robinson WP, Farber A,Patel VI, et al. Optimal selection of patients for electiveabdominal aortic aneurysm repair based on life expectancy.J Vasc Surg 2013;58:589e95.
9 Anderson JM. Rehabilitating elderly cardiac patients. West JMed 1991;154:573e8.
10 Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM.Regular physical activity reduces hospital admission and mor-tality in chronic obstructive pulmonary disease: a populationbased cohort study. Thorax 2006;61:772e8.
11 Dorn J, Naughton J, Imamura D, Trevisan M. Results of amulticenter randomized clinical trial of exercise and long-termsurvival in myocardial infarction patients: the National Exerciseand Heart Disease Project (NEHDP). Circulation 1999;100:1764e9.
12 Belardinelli R, Paolini I, Cianci G, Piva R, Georgiou D, Purcaro A,et al. Exercise training intervention after coronary angioplasty:the ETICA trial. J Am Coll Cardiol 2001;37:1891e900.
13 Bobbio A, Chetta A, Ampollini L. Pre-operative pulmonaryrehabilitation in patients undergoing lung resection for non-small cell lung cancer. Eur J Cardiothorac Surg 2008;33:95e8.
14 Hulzebos E, Helders P, Favie N, De Bie R, Brutel de la R, vanMeeteren N. Pre-operative intensive inspiratory muscletraining to prevent post-operative pulmonary complications inhigh-risk patients undergoing CABG surgery: a randomizedclinical trial. JAMA 2006;296:1851e7.
15 Herdy A, Marcchi P, Vila A. Pre- and post-operative cardiopul-monary rehabilitation in hospitalized patients undergoing cor-onary artery bypass surgery: a randomized controlled trail. AmJ Phys Med Rehabil 2008;87:714e9.
16 Jones L, Peddle C, Eves N. Effects of presurgical exercisetraining on cardiorespiratory fitness among patients undergo-ing thoracic surgery for malignant lung lesions. Cancer2007;110:590e8.
17 Valkenet K, van de Port I, Dronkers J, de Vries W, Lindeman E,Backx F. The effects of pre-operative exercise therapy on post-operative outcome: a systematic review. Clin Rehabil 2011;25:99e111.
18 Mosely AM, Herbert RD, Sherrington C. Evidence for physio-therapy practice: a survey of the Physiotherapy EvidenceDatabase (PEDro). Aust J Physiother 2002;48:43e9.
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
19 Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M.Reliability of the PEDro scale for rating quality of randomizedcontrolled trials. Phys Ther 2003;83:713e21.
20 Foley NC, Teasell RW, Bhogal SK, Speechley MR. Stroke reha-bilitation evidence-based review: methodology. Top StrokeRehabil 2003;10:1e7.
21 Altman D. Practical statistics for medical research. London:Chapman & Hall; 1991.
22 Caspersen CJ, Powell KE, Christenson GM. Physical activity,exercise, and physical fitness: definitions and distinctions forhealth-related research. Public Health Rep 1985;100:126e31.
23 Ghosh AK. Anaerobic threshold: its concept and role inendurance sport. Malays J Med Sci 2004;11:24e36.
24 Kjaer M, Krogsgaard MR, Magnusson P. Elective surgeryreconvalescence after pre-operative physical training. UgeskrLaeger 2009;171:2920e2 [in Danish].
25 Tew GA,Weston M, Kothmann E, Batterham AM, Gray J, Kerr K,et al. High-intensity interval exercise training before abdominalaortic aneurysm repair (HIT-AAA): protocol for a randomisedcontrolled feasibility trial. BMJ Open 2014;4.
26 Honnesh S, Goosen L, Adams N, Forni L, Lavies N, Venn R. Ef-fect of short-term exercise training on aerobic fitness in pa-tients with abdominal aortic aneurysms. Br J Anaesth2010;104:265e6.
27 Tew GA, Moss J, Crank H, Mitchell PA, Nawaz S. Enduranceexercise training in patients with small abdominal aorticaneurysm: a randomized controlled pilot study. Arch Phys MedRehabil 2012;93:2148e53.
28 Myers JN, White JJ, Narasimhan B, Dalman RL. Effects of ex-ercise training in patients with abdominal aortic aneurysm:preliminary results from a randomized trial. J CardiopulmRehab Prev 2010;30:374e83.
29 Kothmann E, Batterham AM, Owen SJ, Turley AJ, Cheesman M,Parry A, et al. Effect of short-term exercise training on aerobicfitness in patients with abdominal aortic aneurysms: a pilotstudy. Br J Anaesth 2009;103:505e10.
30 Dronkers J, Veldman A, Hoberg E, van der Waal C, vanMeeteren N. Prevention of pulmonary complications afterupper abdominal surgery by pre-operative intensive inspiratorymuscle training: a randomized controlled pilot study. ClinRehabil 2008;22:134e42.
31 Lemanu D, Singh P, MacCormick A, Arroll B, Hill A. Effect of pre-operative exercise on cardiorespiratory function and recoveryafter surgery: a systematic review. World J Surg 2013;37:711e20.
32 Freiberg MS, Arnold AM, Newman AB, Edwards MS,Kraemer KL, Kuller LH. Abdominal aortic aneurysms, increasinginfrarenalaortic diameter, and risk of total mortality and inci-dent cardiovasculardisease events: 10-year follow-up data fromthe Cardiovascular Health Study. Circulation 2008;117:1010e7.
33 Jack S, West M, Grocott MP. Perioperative exercise training inelderly subjects. Best Pract Res Clin Anaesthesiol 2011;25:461e72.
34 Carlisle J, Swart M. Mid-term survival after abdominal aorticaneurysm surgery predicted by cardiopulmonary exercisetesting. Br J Surg 2007;94:966e9.
35 Older P, Hall A, Hader R. Cardiopulmonary exercise testing as ascreening test for perioperative management of major surgeryin the elderly. Chest 1999;116:355e62.
36 Brooks Brunn JA. Post-operative atelectasis and pneumonia.Heart Lung 1995;24:94e115.
37 Hamel MB, Henderson WG, Khuri SF, Daley J. Surgical out-comes for patients aged 80 and older: morbidity and mortality
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008

Pre-operative Exercise Therapy in Patients with AAA 11
from major noncardiac surgery. J Am Geriatr Soc 2005;53:424e9.
38 Davies JM. Pre-operative respiratory evaluation and manage-ment of patients for upper abdominal surgery. J Biol Med1991;64:329e49.
39 Fleischmann KE, Goldman L, Young B, Lee TH. Association be-tween cardiac and noncardiac complications in patients un-dergoing noncardiac surgery: outcomes and effects on lengthof stay. Am J Med 2003;115:515e20.
40 Duggan M, Kavanagh BP. Pulmonary atelectasis: a pathogenicperioperative entity. Anesthesiology 2005;102:838e54.
41 Gaskill SE, Walker AJ, Serfass RA, Bouchard C, Gagnon J,Rao DC, et al. Changes in ventilatory threshold with exercisetraining in a sedentary population: the HERITAGE Family Study.Int J Sports Med 2001;22:586e92.
42 Siafakas NM, Mitrouska I, Bouros D, Georgopoulos D. Surgeryand the respiratory muscles. Thorax 1999;54:458e65.
43 Wisløff U, Støylen A, Loennechen JP, Bruvold M, Rognmo Ø,Haram PM, et al. Superior cardiovascular effect of aerobic
Please cite this article in press as: Pouwels S, et al., Beneficial Effects of Pre-opeSystematic Review, European Journal of Vascular and Endovascular Surgery (2
interval training versus moderate continuous training in heartfailure patients: a randomized study. Circulation 2007;115:3086e94.
44 Fabre C, Masse-Biron J, Ahmaidi S, Adam B, Prefaut C. Effec-tiveness of individualized aerobic training at the ventilatorythreshold in the elderly. J Gerontol A Biol Sci Med Sci 1997;52:260e6.
45 Takeshima N, Tanaka K, Kobayashi F, Watanabe T, Kato T. Ef-fects of aerobic exercise conditioning at intensities corre-sponding to lactate threshold in the elderly. Eur J Appl PhysiolOccup Physiol 1993;63:138e43.
46 Hill J, Timmis A. Exercise tolerance testing. Br Med J 2002;324:1084e7.
47 Gommans LN, Saarloos R, Scheltinga MR, Houterman S, deBie RA, Fokkenrood HJ, et al. Editor’s choicedthe effect ofsupervision on walking distance in patients with intermittentclaudication: a meta-analysis. Eur J Vasc Endovasc Surg2014;48:169e84.
rative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A014), http://dx.doi.org/10.1016/j.ejvs.2014.10.008