Embed Size (px)
Citation preview
Ben BermanNASA Ames Research Center/San Jose State
University
Key Dismukes NASA Ames Research Center
Loukia LoukopoulosNASA Ames Research Center/San Jose State
University
Human Factors in Aviation ConferenceSan Antonio, Texas
March 6, 2007
Cognitive Limitations and Vulnerabilities on the Flight Deck:
What Can We Do?
“Most Airline Accidents Attributed to Crew Error”
What does this mean?
– Why do highly skilled pilots make fatal errors?
– How should we think about the role of errors in accidents?
Draw upon cognitive science research on skilled performance of human operators
Broken Bolt vs.
Unflipped Switch
• Physical causes leave characteristic traces• No such thing for human performance• “Why” drops out, for good reason• Can never know with certainty why accident crew
made specific errors--but can determine why the population of pilots is vulnerable
• Put “why” back into the analysis with informed perspective
Approach
• Reviewed NTSB reports of the 19 U.S. airline accidents between 1991-2001 attributed primarily to crew error
• Followed the approach of NTSB (1994)
• Asked: Why might any airline crew in situation of accident crew – knowing only what they knew – be vulnerable?
Hindsight Bias
• Knowing the outcome of an accident flight reveals what the crew should have done differently
• But: accident crew does not know the outcome– They respond to situation as they perceive it at the
moment
• Presumption has to be that more underlies an error than lack of skill or motivation
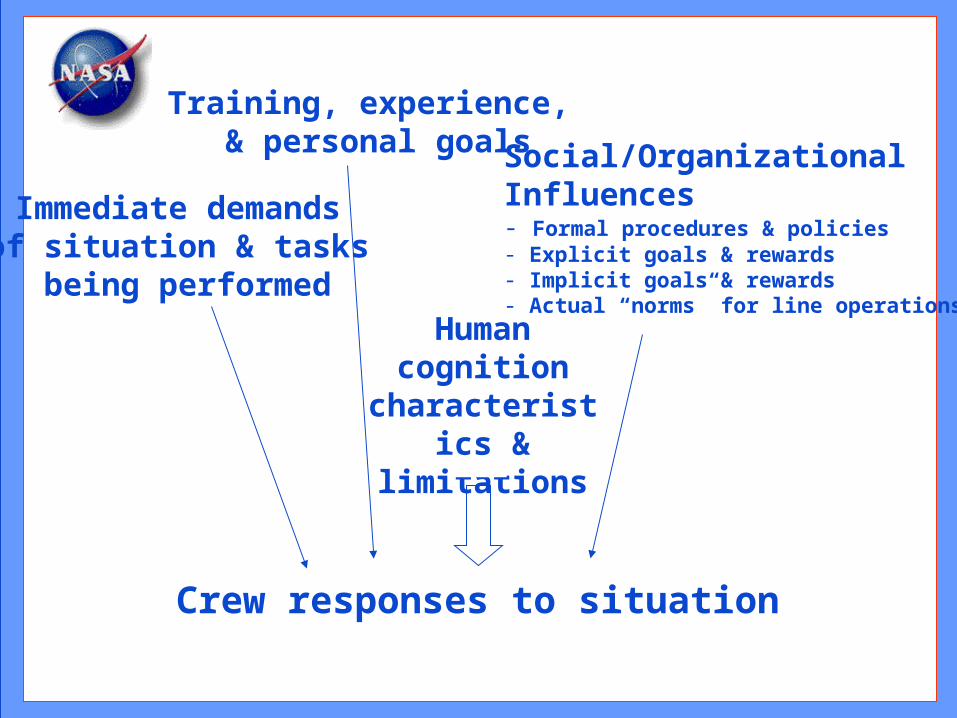
Immediate demands of situation & tasks
being performed
Training, experience, & personal goals Social/Organizational
Influences- Formal procedures & policies- Explicit goals & rewards- Implicit goals & rewards- Actual “norms” for line operations
Human cognition
characteristics & limitations
Crew responses to situation
American 903May 12, 1997
West Palm Beach, Florida• Airbus 300/600 in its initial descent for Miami
• Airplane leveled, slowed, and began a holding pattern at 16,000 feet
• Uncontrolled roll and pitch oscillations; steep descent; recovered with one serious injury/damage to the tail that was discovered much later
• Probable cause: “The flight crew’s failure to maintain adequate airspeed during level-off which led to an inadvertent stall, and their subsequent failure to use proper stall recovery techniques”
• Contributing factor: “The flight crew’s failure to properly use the autothrottle”
American 903:Sequence of Events
• Autothrottle became disconnected during descent from cruise--not clear why, and not noticed or remembered by the crew
• Autopilot captured 16,000 feet and pitched up to maintain altitude, so airspeed decreased
• Vibration and buffeting began that the crew attributed to turbulence
• Airplane stalled and departed controlled flight
• Crew recovered below 13,000 feet, proceeded to safe landing in Miami
American 903:Dim Cues, Missing Cues,
and Hints
• Autothrottle disconnection did not have salient annunciation
– Dim cue (compared to autopilot, for example)
– Crews often do not notice unexpected mode changes
• Autothrottles had tripped off on other flights
– Hint about accidents from everyday operations
• Crew might have disconnected autothrottle without thinking about it or remembering
– Automaticity
American 903:Out of the Loop, Missing Cues,
and the Wrong Procedure
• Neither pilot noticed the airspeed loss until well below maneuvering speed
– Vulnerability from being out of the active control loop
– Crew expected aircraft to slow, just not that much
• Stall warning did not activate prior to stall
– Dependence on missing cue
• Crew performed wind shear recovery rather than stall recovery
– Primed to think about thunderstorms
– Training for wind shear and min-altitude approach to stall recovery
– Again, absence of timely stall warning
American 903:Lessons
• Tendency toward degraded monitoring of normally reliable automation is rooted in basic human cognitive vulnerabilities
– Simply cautioning pilots to monitor more carefully will not greatly reduce vulnerability, by itself.
• Snowball effect of one error producing overload that undermines error-trapping and results in more errors
• Missing cues can be extremely hazardous
• Concept of reliability on the flight deck
– Variability of performance
– Two pilots, redundant procedures, several warning systems, and an airplane: goal is to keep errors from sneaking through all those layers of cheese
Each Accident Has Unique Surface Features and
Combinations of Factors
• Countermeasures to surface features of past accidents will not prevent future accidents
• Must examine deep structure of accidents to find common factors
Cross-Cutting Factors Contributing to Crew Errors
• Situations requiring rapid response • Challenges of managing concurrent tasks
• Equipment failure and design flaws
• Misleading or missing cues normally present
• Stress
• Shortcomings in training and/or guidance
• Social/organizational issues
• Plan continuation bias
Situations requiring rapid response
• Nearly 2/3 of 19 accidents
• Examples: upset attitudes, false stick shaker activation after rotation, anomalous airspeed indications at rotation, autopilot-induced oscillation at Decision Height, pilot-induced oscillation during flare
• Very rare occurrences, but high risk
• Surprise is a factor
• Inadequate time to think through situation– Automatic response required from pilot
Cross-Cutting Factors
Challenges of managing concurrent tasks
• Workload high in some accidents (e.g., Little Rock, 1999)
– Overloaded crews failed to recognize situation getting out of hand (“snowball effect”): losing the ability to recognize that they were overloaded
– Monitoring and cross-checking suffered
– Crews became reactive instead of proactive/strategic
• But: adequate time available for all tasks in many accidents– Inherent cognitive limitations in switching attention:
preoccupation with one task of many; forgetting to resume interrupted or deferred tasks
Cross-Cutting Factors
Stress
• Stress is normal physiological/behavioral response to threat
• Acute stress hampers performance– Narrows attention (“tunneling”)– Reduces working memory capacity
• Combination of surprise, stress, time pressure, and concurrent task demands can be lethal setup
Cross-Cutting Factors
Social/Organizational Issues
• Actual norms may deviate from Flight Operations Manual
• Accident crew judgment & decision-making may not differ from non-accident crews in similar situations:– Lincoln Lab study: Penetration of storm cells on approach not uncommon– Other flights may have landed or taken off without difficulty a minute or two
before accident flight
– Little data available on extent to which accident crews’ actions are typical/atypical
• Competing pressures not often acknowledged– Implicit messages from company may conflict with formal guidance
• e.g. on-time performance vs. conservative response to ambiguous situations
– Pilots may not be consciously aware of influence of internalized competing goal
Cross-Cutting Factors
Plan continuation bias (e.g., Burbank, 2000)
• Unconscious cognitive bias to continue original plan in spite of changing conditions
• Appears stronger as one nears completion of activity (e.g., approach to landing)– Why are crews reluctant to go-around?
• Bias may prevent noticing subtle cues indicating original conditions have changed
• Reactive responding is easier than proactive thinking
• Default plan always worked before
Cross-Cutting Factors
Implications and
Countermeasures:The Individual
• Vulnerabilities are inherent in our human cognition
– Limitations, biases
• Effects extend to error trapping mechanisms
– Monitoring subject to task shedding under workload
– Checklists automatized, subject to slips/omissions
• Recognize realistic rather than theoretical performance of humans in generating errors as they work, and in catching errors
Implications and
Countermeasures:The Aviation System
• Accept the variability of human performance
– Because someone makes an error does not make them deficient or complacent
– Errors are inevitable
– Recognize that errors are probabilistic
• Society’s demand for reliability is nearly unlimited
– Focus on net system reliability, made up of:
• Reliability of each error trapping mechanism
• Independence of error trapping mechanisms to prevent the holes in the swiss cheese from lining up: (e.g., landing checklist initiation cued by callout to extend the gear)
Implications and
Countermeasures:The Aviation System (cont’d)
• Causal attribution to individual can distract attention from underlying cause and prevention
• Remediation lies with the system
– Guard against “don’t do that anymore” prescriptions
– No evidence of Bad Apple theory
– All other remediation requires more difficult changes in the system
Net System Reliability: “Okay, what can we do?”
• Treat monitoring and crosschecking as being as important as anything else we do
• Suggestions for training & checking:– Cut down on negative training (e.g., continuing
unstabilized approaches in sim makes plan continuation bias stronger on the line
– Teach pilots to monitor, give them the opportunity to practice in the sim
– Build at least one realistic challenge and decision into every sim session
– Teach how to manage workload, practice in the sim
“What can we do?”(continued)
• Procedures design review– Match human characteristics and limitations– Independence
• Equipment design review– Match human characteristics and limitations
• Safety Change:– Heed the hints--the next accident is trying to warn you
about itself right now• AA903, AA1340, CAL1943
– How to separate the wheat from the chaff?
Dismukes, R. K., Berman, B.A., & Loukopoulos, L. L. The Limits of Expertise: Rethinking Pilot Error and the
Causes of Airline Accidents.
www.ashgate.com
More information on NASA Human Factors Research:
http://human-factors.arc.nasa.gov/his/flightcognition/
This research was partially funded by NASA’s Aviation Safety Program and by the FAA (Eleana Edens, Program Manager).
What else can we do?