Embed Size (px)
Citation preview

Belief Assessment as a Component of Curriculum Planning: Cigarette Smoking as an Example*
Stephen Roberts
Smokers, in comparison to non- smokers, have quite different beliefs and values about smoking cigarettes. Differences occur in areas such as health, dependency and relaxation.
Due to the many problems attributed to cigarette use, considerable effort has been invested in health education for the purposes of both preventing non- smokers from starting to smoke and encouraging smokers to quit smoking. These educational efforts have not been overwhelmingly successful. Although the percentage of adolescent males who smoke cigarettes appears to have declined slightly over the last few years, the proportion of young females who smoke has risen.‘
Health education obviously cannot be singled out as the primary culprit in the unhealthy rise of female adolescent smoking, but there would appear to be a number of weaknesses in present-day programs which, if attended to, could increase the effectiveness of the educator’s efforts. A number of these problems, as discussed by Cornacchia, Smith and Bentel’ are as follows: ( I ) emphasis on “the acquisi- tion of pharmacological or physiological information without consideration of psychological, sociological and spiritual aspects,” (2) insufficient consideration of student involvement and (3) lack of adequate procedures to measure the effectiveness of programs.
It is the purpose of this paper to present a meth- odology which, if used by the educator, will help cir- cumvent the aforementioned weaknesses by supplying the following information: (1) specific salient beliefs and evaluations students have about the smoking of cigarettes (or any other behavior), (2) the relative strength of these beliefs and evaluations *This paper was originally presented at the 107th annual meeting of the American Public Health Association, New York, NY, November, 1979.
as held by the students and (3) those beliefs and evaluations on which smokers and non-smokers are most different. These findings, which are based on the perceptions of students, can serve as part of the foundation for relevant curriculum development. This particular approach is meant to be a supplement to - not a substitute for - traditional curriculum development.
METHOD It has been found in previous research that (1)
attitude is in many cases related to behavior) and (2) attitude toward a behavior is highly related to an individual’s beliefs that the behavior in question will lead to certain consequences, weighted (multiplied) by her evaluation of those consequences.’ Although no attempts have been made in this study to reaffirm either of the above relationships, it was considered appropriate to examine those specific beliefs and evaluations related to cigarette smoking in order to gain further understanding of why young women d o or do not smoke, For the purpose of this investigation, “belief” was defined as a subjective probability statement linking a consequence to a behavior. In other words, belief was seen as the likeli- hood that a particular consequence (eg, cancer) would occur as a result of smoking. Evaluation was a measure of whether the respondent felt that the con- sequence was good or bad.
Participants in the study included 142 eighteen and nineteen-year-old women enrolled at a large mid- western university. The subjects were selected randomly from residence halls.
To assess student perceptions about cigarette smoking, an initial open-ended elicitation question- naire was given to a sub-sample (different from the final sample) of 20 eighteen and nineteen-year-old college women. The questions asked were as follows: 1. What d o you think are the advantages of smoking cigarettes? adequate procedures 2. What d o you think are the disadvantages of smok- ing cigarettes? effectiveness.
One of the weaknesses of present-day health programs is a lack of
to measure their
DECEMBER 1980 THE JOURNAL OF SCHOOL HEALTH 555
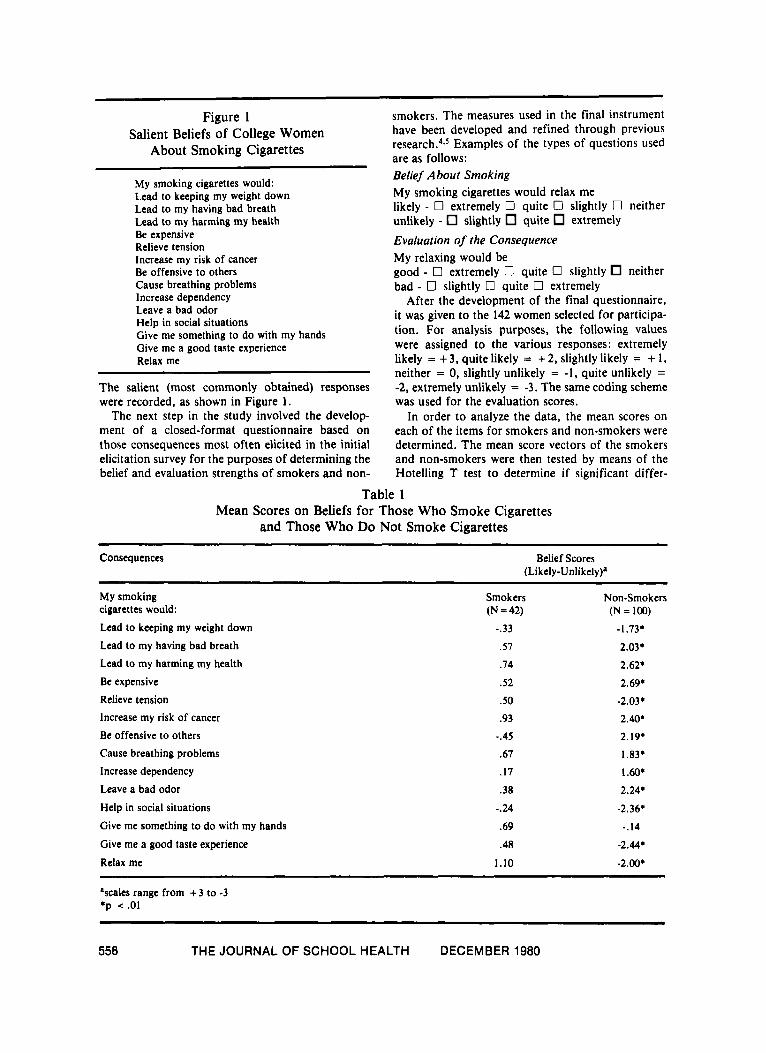
Figure 1 Salient Beliefs of College Women
About Smoking Cigarettes
My smoking cigarettes would: Lead to keeping my weight down Lead to my having bad breath Lead to my harming my health Be expensive Relieve tension Increase my risk of cancer Be offensive to others Cause breathing problems Increase dependency Leave a bad odor Help in social situations Give me something to do with my hands Give me a good taste experience Relax me
The salient (most commonly obtained) responses were recorded, as shown in Figure 1.
The next step in the study involved the develop- ment of a closed-format questionnaire based on those consequences most often elicited in the initial elicitation survey for the purposes of determining the belief and evaluation strengths of smokers and non-
smokers. The measures used in the final instrument have been developed and refined through previous r e ~ e a r c h . ~ . ~ Examples of the types of questions used are as follows: Belief About Smoking My smoking cigarettes would relax me likely - 0 extremely 0 quite 0 slightly 0 neither unlikely - slightly quite extremely Evaluation of the Consequence My relaxing would be good - 0 extremely 0 quite 0 slightly neither bad - 0 slightly 0 quite 0 extremely
After the development of the final questionnaire, it was given to the 142 women selected for participa- tion. For analysis purposes, the following values were assigned to the various responses: extremely likely = + 3, quite likely = + 2, slightly likely = + 1, neither = 0, slightly unlikely = -1, quite unlikely = -2, extremely unlikely = -3. The same coding scheme was used for the evaluation scores.
In order t o analyze the data, the mean scores on each of the items for smokers and non-smokers were determined. The mean score vectors of the smokers and non-smokers were then tested by means of the Hotelling T test to determine if significant differ-
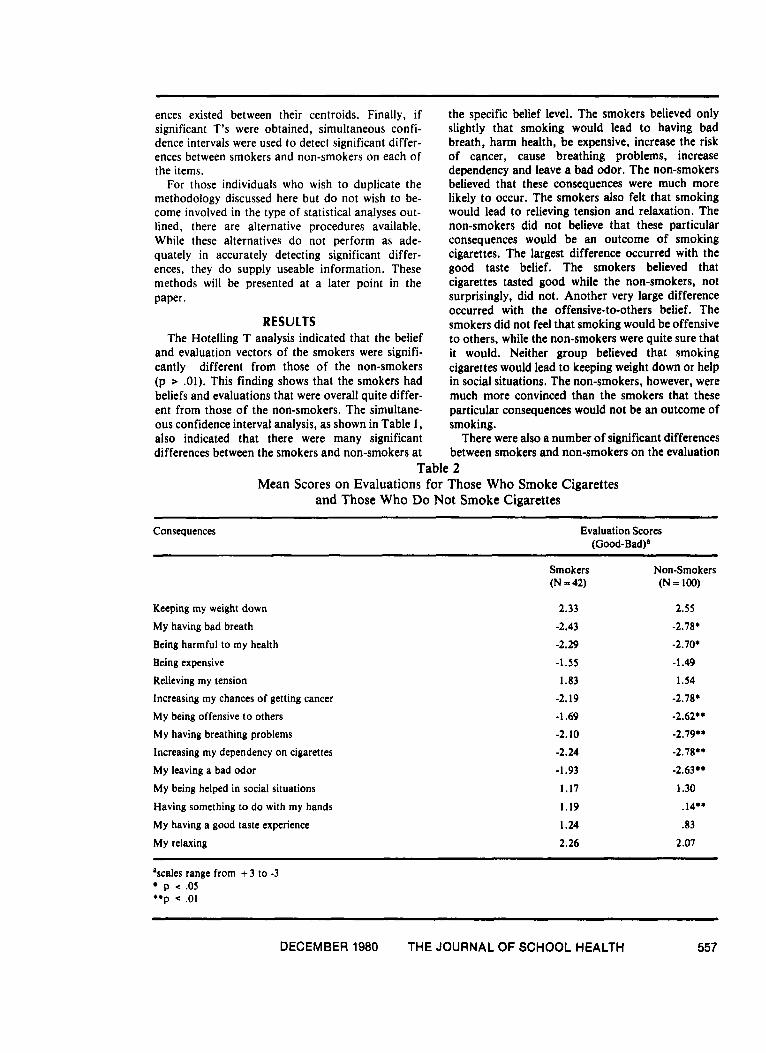
Table 1 Mean Scores on Beliefs for Those Who Smoke Cigarettes
and Those Who Do Not Smoke Cigarettes
Consequences Belief Scores (Li kely-Unlikely)*
My smoking cigarettes would: Lead to keeping my weight down Lead to my having bad breath Lead to my harming my health Be expensive Relieve tension Increase my risk of cancer Be offensive to others Cause breathing problems Increase dependency Leave a bad odor Help in social situations Give me something to do with my hands Give me a good taste experience
Relax me
Smokers (N = 42)
-.33
.57
.74
.52
.50
.93
-.45
.67
.17
.38
-.24
.69
.48
1.10
Non-Smokers (N = 100)
- I .73* 2.03.
2.62+
2.69+
-2.03.
2.40.
2.19.
1.83+
1 .a* 2.24.
-2.36.
-.14
-2.44.
-2.00+
ascales range from + 3 to -3 +p .2 .01
556 THE JOURNAL OF SCHOOL HEALTH DECEMBER 1980
ences existed between their centroids. Finally, if significant T's were obtained, simultaneous confi- dence intervals were used to detect significant differ- ences between smokers and non-smokers on each of the items.
For those individuals who wish to duplicate the methodology discussed here but d o not wish to be- come involved in the type of statistical analyses out- lined, there are alternative procedures available. While these alternatives do not perform as ade- quately in accurately detecting significant differ- ences, they d o supply useable information. These methods will be presented at a later point in the paper.
RESULTS The Hotelling T analysis indicated that the belief
and evaluation vectors of the smokers were signifi- cantly different from those of the non-smokers (p .01). This finding shows that the smokers had beliefs and evaluations that were overall quite differ- ent from those of the non-smokers. The simultane- ous confidence interval analysis, as shown in Table 1, also indicated that there were many significant differences between the smokers and non-smokers a t
the specific belief level. The smokers believed only slightly that smoking would lead t o having bad breath, harm health, be expensive, increase the risk of cancer, cause breathing problems, increase dependency and leave a bad odor. The non-smokers believed that these consequences were much more likely to occur. The smokers also felt that smoking would lead to relieving tension and relaxation. The non-smokers did not believe that these particular consequences would be an outcome of smoking cigarettes. The largest difference occurred with the good taste belief. The smokers believed that cigarettes tasted good while the non-smokers, not surprisingly, did not. Another very large difference occurred with the offensive-to-others belief. The smokers did not feel that smoking would be offensive t o others, while the non-smokers were quite sure that it would. Neither group believed that smoking cigarettes would lead t o keeping weight down or help in social situations. The non-smokers, however, were much more convinced than the smokers that these particular consequences would not be an outcome of smoking.
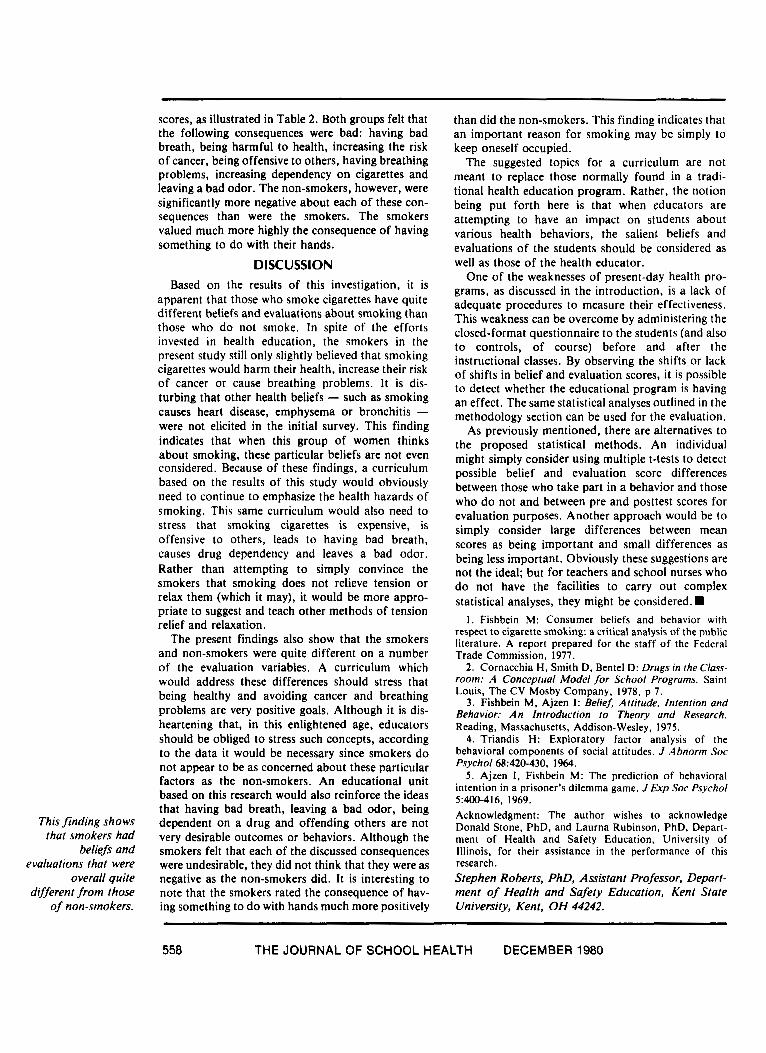
There were also a number of significant differences between smokers and non-smokers on the evaluation
Table 2 Mean Scores on Evaluations for Those Who Smoke Cigarettes
and Those Who Do Not Smoke Cigarettes ~ ~~
Consequences Evaluation Scores (Good-Bad)a
Keeping my weight down My having bad breath Being harmful to my health Being expensive Relieving my tension Increasing my chances of getting cancer My being offensive to others My having breathing problems Increasing my dependency on cigarettes My leaving a bad odor My being helped in social situations Having something to do with my hands My having a good taste experience My relaxing
Smokers (N = 42)
2.33
-2.43
-2.29
-1.55
1.83
-2.19
-1.69
-2.10
-2.24
-1.93
1.17
1.19
1.24
2.26
Non-Smokers (N = 100)
2.55
-2.78.
-2.70.
-1.49
1.54
-2.78.
-2.62..
-2.79..
-2.78..
-2.63
1.30
.I4**
.83
2.07
'scales range from + 3 to -3 p < .05
**p < .01
DECEMBER 1980 THE JOURNAL OF SCHOOL HEALTH 557
This finding shows that smokers had
beliefs and evaluations that were
overall quite different from those
of non-smokers.
scores, as illustrated in Table 2. Both groups felt that the following consequences were bad: having bad breath, being harmful to health, increasing the risk of cancer, being offensive to others, having breathing problems, increasing dependency on cigarettes and leaving a bad odor. The non-smokers, however, were significantly more negative about each of these con- sequences than were the smokers. The smokers valued much more highly the consequence of having something to d o with their hands.
DISC U SSlON Based on the results of this investigation, it is
apparent that those who smoke cigarettes have quite different beliefs and evaluations about smoking than those who d o not smoke. In spite of the efforts invested in health education, the smokers in the present study still only slightly believed that smoking cigarettes would harm their health, increase their risk of cancer or cause breathing problems. It is dis- turbing that other health beliefs - such as smoking causes heart disease, emphysema or bronchitis - were not elicited in the initial survey. This finding indicates that when this group of women thinks about smoking, these particular beliefs are not even considered. Because of these findings, a curriculum based on the results of this study would obviously need to continue to emphasize the health hazards of smoking. This same curriculum would also need to stress that smoking cigarettes is expensive, is offensive to others, leads to having bad breath, causes drug dependency and leaves a bad odor. Rather than attempting to simply convince the smokers that smoking does not relieve tension or relax them (which it may), it would be more appro- priate to suggest and teach other methods of tension relief and relaxation.
The present findings also show that the smokers and non-smokers were quite different on a number of the evaluation variables. A curriculum which would address these differences should stress that being healthy and avoiding cancer and breathing problems are very positive goals. Although it is dis- heartening that, in this enlightened age, educators should be obliged to stress such concepts, according to the data it would be necessary since smokers d o not appear to be as concerned about these particular factors as the non-smokers. An educational unit based on this research would also reinforce the ideas that having bad breath, leaving a bad odor, being dependent on a drug and offending others are not very desirable outcomes or behaviors. Although the smokers felt that each of the discussed consequences were undesirable, they did not think that they were as negative as the non-smokers did. It is interesting to note that the smokers rated the consequence of hav- ing something to d o with hands much more positively
than did the non-smokers. This finding indicates that an important reason for smoking may be simply to keep oneself occupied.
The suggested topics for a curriculum are not meant to replace those normally found in a tradi- tional health education program. Rather, the notion being put forth here is that when educators are attempting to have an impact on students about various health behaviors, the salient beliefs and evaluations of the students should be considered as well as those of the health educator.
One of the weaknesses of present-day health pro- grams, as discussed in the introduction, is a lack of adequate procedures to measure their effectiveness. This weakness can be overcome by administering the closed-format questionnaire to the students (and also to controls, of course) before and after the instructional classes. By observing the shifts or lack of shifts in belief and evaluation scores, it is possible to detect whether the educational program is having an effect. The same statistical analyses outlined in the methodology section can be used for the evaluation.
As previously mentioned, there are alternatives to the proposed statistical methods. An individual might simply consider using multiple t-tests to detect possible belief and evaluation score differences between those who take part in a behavior and those who d o not and between pre and posttest scores for evaluation purposes. Another approach would be to simply consider large differences between mean scores as being important and small differences as being less important. Obviously these suggestions are not the ideal; but for teachers and school nurses who d o not have the facilities to carry out complex statistical analyses, they might be considered.
I . Fishbein M: Consumer beliefs and behavior with respect to cigarette smoking: a critical analysis of the public literature. A report prepared for the staff of the Federal Trade Commission, 1977.
2. Cornacchia H, Smith D, Bentel D: Drugs in the Class- room: A Conceptual Model for School Programs. Saint Louis, The CV Mosby Company, 1978, p 7.
3. Fishbein M. Ajzen I: Belief, Attitude, Intention and Behavior: An Introduction to Theory and Research. Reading, Massachusetts, Addison-Wesley, 1975.
4 . Triandis H: Exploratory factor analysis of the behavioral components of social attitudes. J Abnorm Soc Psycho1 68:420-430, 1964.
5 . Ajzen 1. Fishbein M: The prediction of behavioral intention in a prisoner's dilemma game. J Exp SOC Psycho1
Acknowledgment: The author wishes to acknowledge Donald Stone, PhD, and Laurna Rubinson, PhD, Depart- ment of Health and Safety Education, University of Illinois, for their assistance in the performance of this research. Stephen Roberts, PhD, Assistant Professor, Depart- ment of Health and Safety Education, Kent State University, Kent, OH 44242.
5:400-416, 1969.
558 THE JOURNAL OF S C H O O L HEALTH DECEMBER 1980





























