Embed Size (px)
Citation preview
27/11/2015
1
BELGIANCONSENSUS MEETINGon TRAVEL MEDICINE
June 26, 2015
Belgian Scientific Study Group on Travel
Medicine
Pr. A. Van Gompel Dr U Maniewski (ITG)Pr. F. Jacobs (Hôp. Erasme, ULB)
Pr. P. Lacor & Dr L Seyler (UZ-Brussel) Dr. Ph. Leonard (CHU-ULg)
Pr. W. Peetermans (U.Z. - K.U.Leuven) Pr. S. Callens(UZ.- U.Gent) Dr. S.Quoilin (iph.fgov.be)
Dr.P. Soentjens (Belgian Defence)Pr. B. Vandercam (CHU. St. Luc, UCL)
Pr. Y. Van Laethem & Dr C Martin (CHU. St. Pierre, ULB)PART 2 version 25/11/15

27/11/2015
2
REPORTBELGIAN CONSENSUS MEETING on TRAVEL MEDICINE
June 26, 2015 – PART 2
2015
• The consensus meeting was chaired by A. Van Gompel and Y, Van Laethem
• Secretary of the meeting was P Lacor• A preliminary PowerPoint, prepared by A. Van Gompel,
was presented• The discussion and recommendations of the
meeting are included in this finale presentation.• The ESSENTIAL SLIDES (pdf-version) & the
CONSENSUS BROCHURE (in Dutch and French) highlighting the proposals for changes will been sent to all participants. May be used for teaching.
• These documents will serve as a proposal for approval by the governmental Belgian Health Council – section Vaccinations, on 17-09-2015
• Responsable final redaction : A. Van Gompel
PART 1• 1.a - Vaccination for Yellow Fever• 1.b - Malaria
PART 2• 2.A - Other vaccinations• 2.B - TD, other infections, …., • 2.C - VARIA
2015

27/11/2015
3
Anaphylaxis • Anaphylaxis following administration of a
vaccine (after excluding severe allergy by medical history) is extremely rare.
• 15' of observation (in the waiting room or in the hall of the travel clinic) is a safety rule after vaccination
• Nr. 8802 Hoge Gezondheidsraad = Conseil Supérieur de la Santé 4/7/2012
– http://tinyurl.com/HGR-8802-anafylaxie– http://tinyurl.com/CSS-8802-anaphylaxie
2015
Basic Vaccinations - Tetanus-diphteria-pertussis- Poliomyelitis- Measles mumps rubella
2014

27/11/2015
4
Tetanus-Diphtheria-Pertussis
2014
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
d’une dose unique de rapp

27/11/2015
5
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
6
2015
2015

27/11/2015
7
Primovaccinatie met dTp(a) ? In de bijsluiter wordt de primovaccinatiemet het dTp(a)-vaccin niet vermeld.Ook de aanbeveling van de HogeGezondheidsraad vermelden daaroverniets.Een studie uit 2007 onderzocht bijvolwassenen ouder dan 40 jaar die devoorbije 20 jaar geen tetanus of difterievaccinhadden gekregen of waarvan devaccinatiestatus onbekend was, de efficiëntievan dTp(a) en dTp(a)-IPV-vaccins.Eén maand na de toediening van 3 dosissen,bedroeg het niveau van beschermendeantistoffen 99%. Bij gebrek aan dT kan dTp(a) dus worden gebruikt voor primovaccinatie. Indien ook bescherming tegen polio nodig is, kan dTp(a)-IPV gebruikt worden
Primovaccination avec le dTp(a) ?
Ni la notice, ni les recommandations duConseil Supérieur de la Santé ne mentionnentla possibilité d’une primovaccinationavec le dTp(a).Cependant, une étude publiée en2007 a montré chez 99% des vaccinésl’obtention de taux séroprotecteurscontre le tétanos et la diphtérie après uneprimovaccination à l’aide du dTp(a) (3doses), chez des adultes de plus de 40ans (en absence de données vaccinalesou avec un dernier rappel datant de plusde 20 ans).En cas d’indisponibilté du dT, par exemple lors d’une rupture de stock, l’administration du dTp(a) pourrait donc être utilisé en primovaccination. En cas de nécessité d’une protection contre la poliomyélite, dTp(a)-IPV peut être utilisé,
Theeten H et al, Primary vaccination of adults with reduced antigen-content diphtheria-tetanusacellular pertussis or dTpa-inactivated poliovirus vaccines compared to diphtheria-tetanus-toxoid vaccines. Current medical research and opinion. Vol. 23, n° 11, 2007 : 2729-2739.
2014
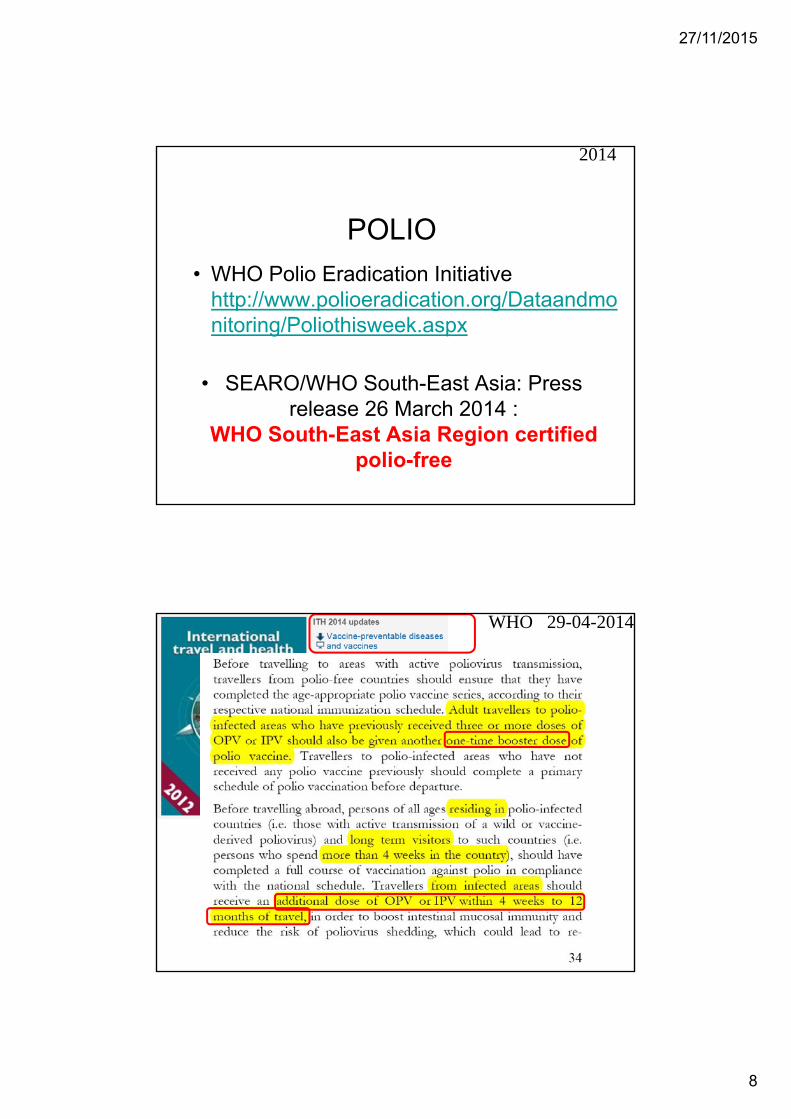
POLIO
2015
27/11/2015
8
POLIO
• SEARO/WHO South-East Asia: Press release 26 March 2014 :
WHO South-East Asia Region certified polio-free
2014
• WHO Polio Eradication Initiative http://www.polioeradication.org/Dataandmonitoring/Poliothisweek.aspx
WHO 29-04-2014

27/11/2015
9
WHO 29-04-2014
2014

27/11/2015
10
July 2015(since 24/04/15)

27/11/2015
11
Sept 2015(since 04/08/15)
25-11- 2015(since 03/09/15)

27/11/2015
12
Imovax Polio ®
Revaxis ®
Boostrix IPV ®
=also Polio
Clearly mention that this is polio-vaccination

27/11/2015
13
Travel Vaccinations
1. Hepatitis A 2. Hepatitis B 3. Typhoid fever4. Rabies5. Meningococcal meningitis6. Japanese encephalitis7. TBE - FSME
2014
HEPATITIS A
Immunodepressed traveler should – if possible - receive the complete series
(2 / 3 doses) before leave(+ antibodytiter)
2014

27/11/2015
14
2014
Results: • The final study population consisted of
53 patients treated with • TNFi (n 15),TNFi & MTX (n 21) or MTX (n 17)
months after the 1st dose % of the patients that had attained seroprotection
1 10%6 33%months after the 2nd dose1 83%6 72%
at month 24 86%
2014

27/11/2015
15
Conclusions: • Two doses of hepatitis A vaccine at a 6-
month interval provided protection for most immunosuppressed RA patients.
• A single dose does not seem to afford sufficient protection to this group of patients.
2014
2014

27/11/2015
16
2015
2015

27/11/2015
17
HEPATITIS B
Immunodepressed …..
2015
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
18
2015
2015

27/11/2015
19
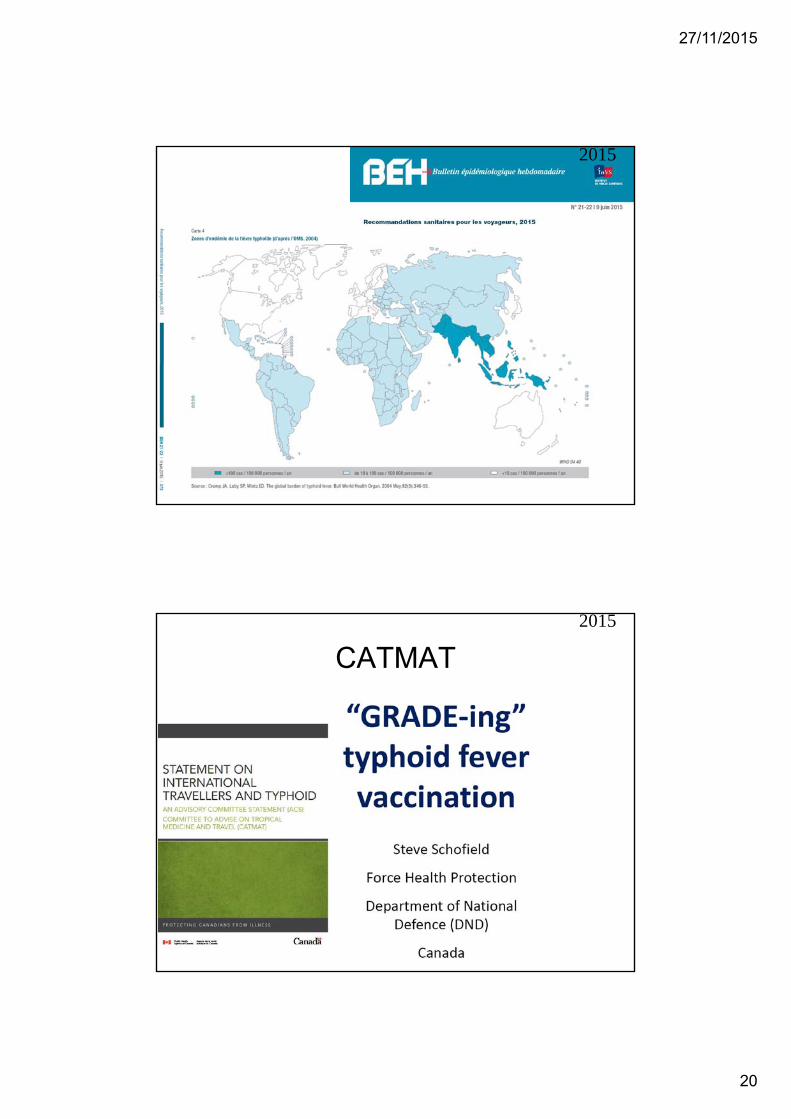
TYPHOID FEVER
25-11-2015
Vaccination against typhoid fever
• Stock of vaccine against typhoid fever depleted– Typhim ®– Typherix ® is available – but in limited
quantities– Vivotif ® is barely or not available
2015
27/11/2015
20
2015
CATMAT 2015

27/11/2015
21
CATMAT
2015
Extract from CatMat 2014 = Canadian guidelines
The strongest and most consistent predictor of typhoid risk in travellers is destination of travel. The estimated risk of developing travel associated typhoid is about:
– 1/3,000 travellers for travel to the South Asia (= high risk) • South Asia is defined as Afghanistan, Bangladesh, Bhutan, India,
Nepal, Maldives, Pakistan, and Sri Lanka. • Among these countries, the large majority (≥ 90%) of cases of typhoid
among travellers were reported from India, Pakistan and Bangladesh
– 1/50,000-100,000 for travel to Sub-Saharan Africa, North Africa and the Middle East, or South America (= intermediate risk)
– < 1/300,000 for travel to the Caribbean and Central America (= low risk).
27/11/2015
22
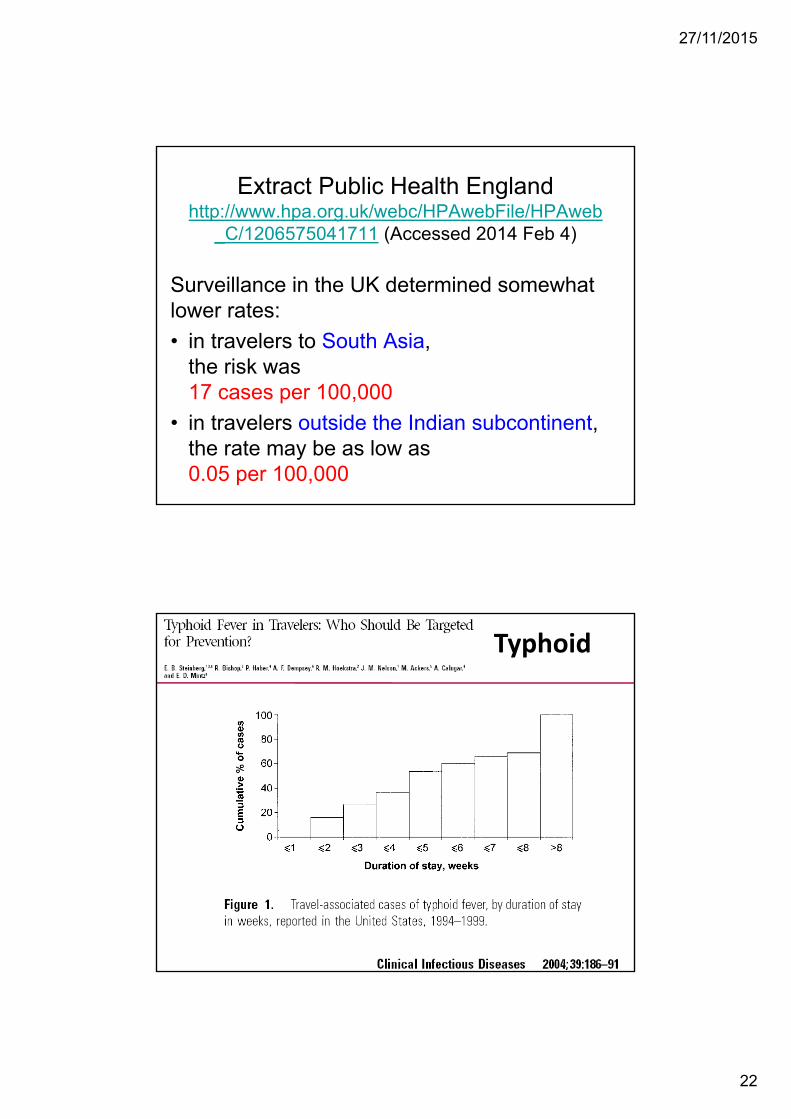
Extract Public Health England http://www.hpa.org.uk/webc/HPAwebFile/HPAweb
_C/1206575041711 (Accessed 2014 Feb 4)
Surveillance in the UK determined somewhatlower rates: • in travelers to South Asia,
the risk was 17 cases per 100,000
• in travelers outside the Indian subcontinent, the rate may be as low as 0.05 per 100,000
Typhoid

27/11/2015
23
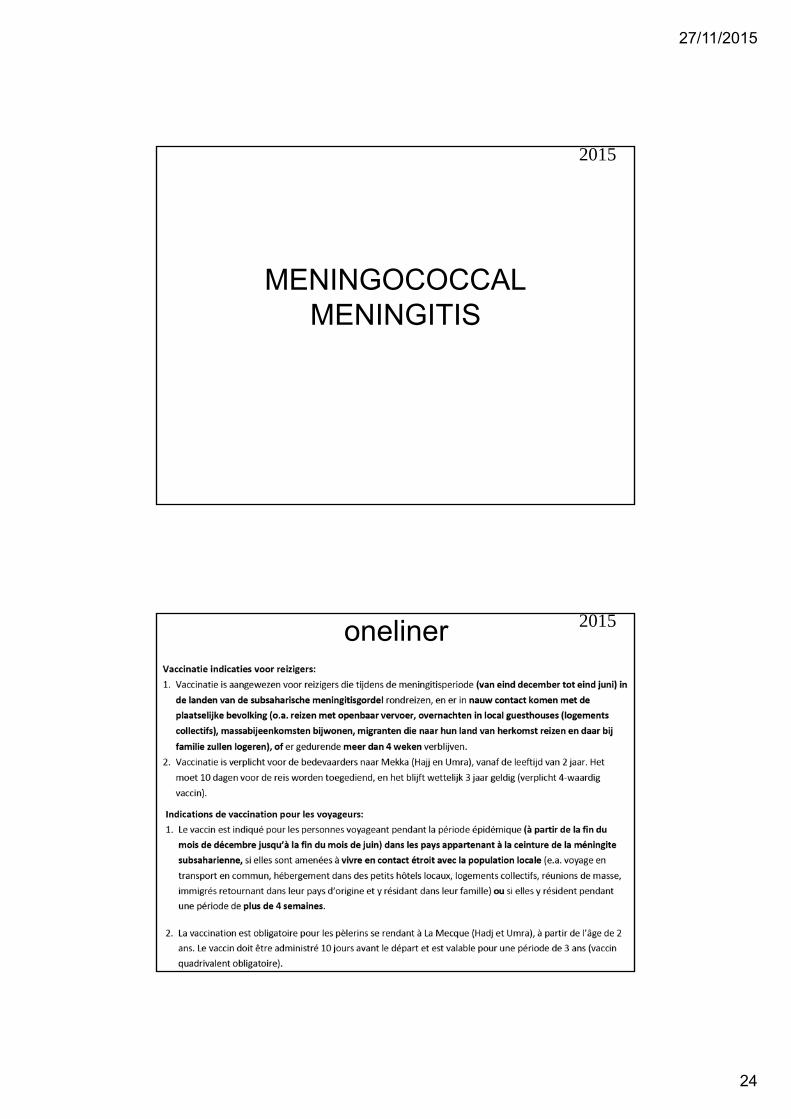
New onelinerOLD : Vaccinatie wordt aangeraden• voor tropenreizen langer dan 3 weken OF • voor avontuurlijke reizen, zelfs indien korter dan 3 weken.
PROPOSAL FOR A NEW ONE:
•la vaccination contre la fièvre typhoïde est surtout conseillée pour les voyages de plus de trois semaines vers le sous-continent indien
• la vaccination contre la fièvre typhoïde est à considérer pour les voyages aventureux dans de mauvaises conditions sanitaires vers les pays tropicaux ou subtropicaux ou pour les immigrés et leurs enfants qui retournent dans leur pays tropical d’origine pour visiter la famille et les connaissances.
25-11-2015
• vaccination against typhoid fever is particularlyadvisable for trips longer than 3 weeks duration to the Indian subcontinent
•vaccination against typhoid fever can be considered in case of an adventurous trip in poor sanitary conditions to tropical or subtropical countries or for immigrants when they return to their homeland to visit friends and relatives.
• vaccinatie tegen buiktyfus is vooral aangeraden voor reizen langer dan 3 weken naar het Indisch subcontinent
• vaccinatie tegen buiktyfus kan overwogen worden voor avontuurlijke reizen in slechte hygiënische omstandigheden in tropische of subtropische landen of voor migranten en hun kinderen die terugkeren naar hun land van herkomst op bezoek bij familie of vrienden.
2015
27/11/2015
24
MENINGOCOCCAL MENINGITIS
2015
oneliner 2015

27/11/2015
25
2014
2014

27/11/2015
26
RABIES
2015
2013
From 31- 05 - 2013 on:no booster after 1 year or later is advisedanymore for at least 20-30 yearsafter the basic series of 3 shots (1-7-21/28) in persons with normal immunity
2012
27/11/2015
27
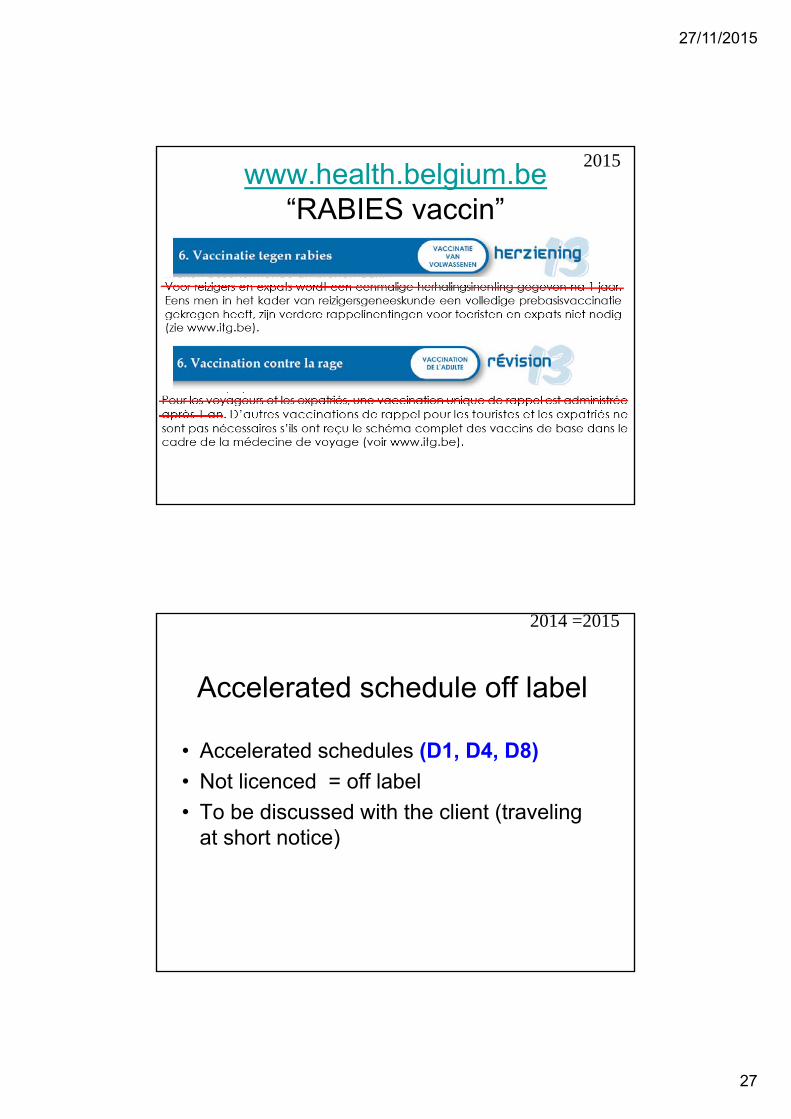
www.health.belgium.be“RABIES vaccin”
2015
Accelerated schedule off label
• Accelerated schedules (D1, D4, D8) • Not licenced = off label• To be discussed with the client (traveling
at short notice)
2014 =2015

27/11/2015
28
NECTM 5 Bergen Norway 2014 Jelinek LECTURE & POSTER
accelerated pre-exposure purifiedChick-embryo cell-culture rabies
vaccine for travelers
2014
2014

27/11/2015
29
2015
Background: • For individuals traveling at short notice to rabies and Japanese encephalitis (JE) endemic countries, concomitant administration of travel
vaccines within a short period is often required.
Methods: • The aim of this study was to determine whether an accelerated (one-week: Days 1 + 8) pre-
exposure rabies (Rabipur, Novartis Vaccines) vaccination regimen administered concomitantlywith a Japanese encephalitis (JE) vaccination (Ixiaro, Valneva) regimen, is non-inferior to the standard (four-week: Days 1, 8, 29) rabies regimen administered alone or concomitantly with the JE vaccine.
• Healthy adults (18 to 65 years) were randomized into Rabies & JE-Standard, Rabies + JE-Accelerated, Rabies-Standard and JE-Standard groups.
• Relative immunogenicity for rabies in each regimen was assessed using the rapid fluorescent focus inhibition test.
• Safety was evaluated up to and including Day 57.
Results: • Non-inferior immunogenicity for rabies was established between the Rabies + JE accelerated
group compared to both the Rabies-Standard and Rabies & JE-Standard groups;• as well as between the Rabies + JE-Standard regimen and the Rabies-Standard regimen. • By Day 57, adequate neutralizing levels were achieved by 97- 100% of subjects across all groups.• Adverse events (AEs) were comparable for all groups.
Conclusions: • An accelerated pre-exposure rabies and JE vaccination regimen is non-inferior to the standard
four-week rabies regimen and may thus provide a more convenient regimen for individuals traveling to endemic countries at short notice.
2015
27/11/2015
30
Travel medicine Seminar 19 /11/15 “Travel medicine Seminar 20 years later”
MILITAIR HOSPITAAL as in 1995 14.00-14.05 Introduction
14.05-14.35 Yellow fever vaccination issues CHARLOTTE MARTIN
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedulesPATRICK SOENTJENS
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines STEVEN CALLENS
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrheaLUCIE SEYLER
16.25- 16.50 Malaria: when prevention is not clear-cutULA MANIEWSKI
16.50-17.15 Traveller's ThrombosisPETER VERHAMME
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ? FONS & YVES
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009
JAPANESE ENCEPHALITIS
2015

27/11/2015
31
Oneliners• Les indications de vaccination
restent limitées: • voyageurs séjournant plus de
3-4 semaines dans les campagnes des zones endémiques, vivant proche des villages et des fermes dans les zones de rizières et d’élevages porcins.
• ….• Ce vaccin doit également être
proposé pour les expatriés vivant en pays d’endémie, même si leur domicile est en ville.
• De indicatie voor de vaccinatie blijft beperkt:
• reizigers die minstens 3-4 weken rondtrekken op het platteland in endemisch gebied, die in de dorpen en op boerderijen logeren, vooral in gebieden waar natte rijstvelden zich nabij varkenskwekerijen bevinden.
• …..• Deze vaccinatie moet
eveneens voorgesteld worden aan personen die gaan wonen in endemische gebieden, zelfs indien ze in de stad wonen.
2015

27/11/2015
32
Oneliners
• Des mesures préventives contre les piqûres de moustiques dès la tombée de la nuit et la nuit, sont une alternative valable à la vaccination.
• Beschermende maatregelen tegen muggenbeten vanaf de beginnende avondschemering zijn een doeltreffend alternatief!
2015
Accelerated schedule
• NECTM5 Accelerated schedules (D1, D8) • 2014 : not licenced = off label• To be discussed with the client
• EMA approves accelerated schedule:
2014
2015
27/11/2015
33
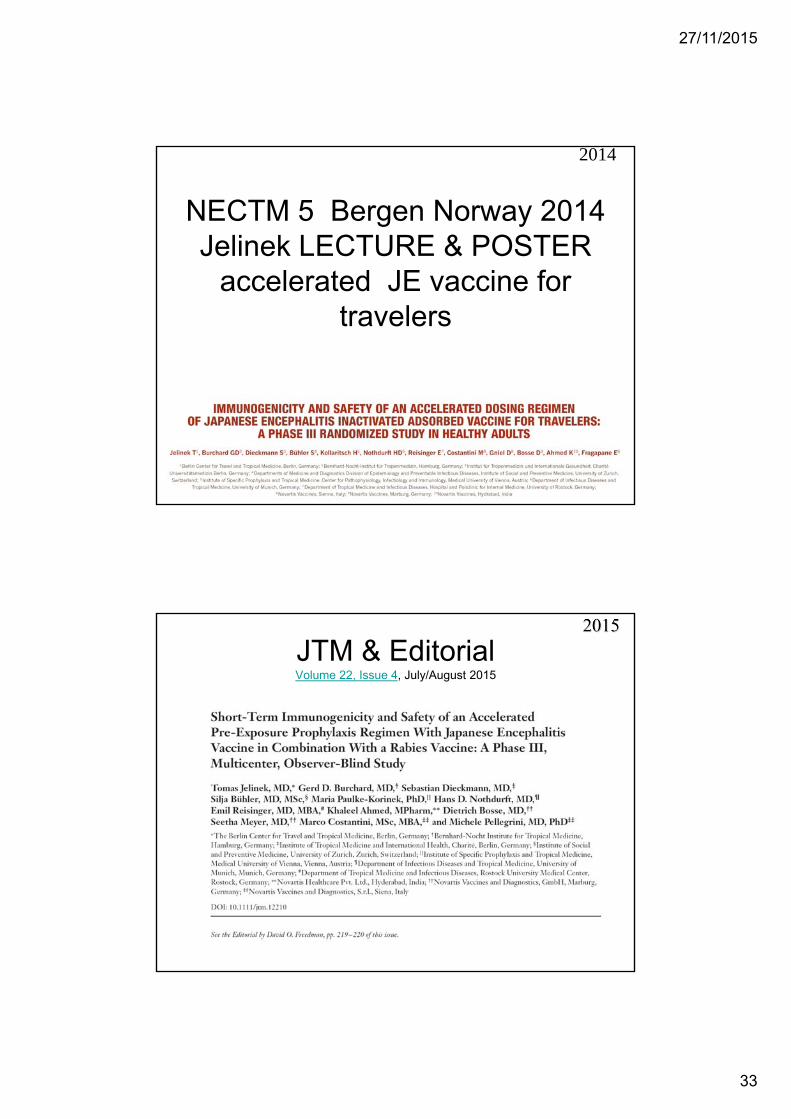
NECTM 5 Bergen Norway 2014 Jelinek LECTURE & POSTER
accelerated JE vaccine for travelers
2014
JTM & EditorialVolume 22, Issue 4, July/August 2015

27/11/2015
34
JTM & EditorialVolume 22, Issue 4, July/August 2015
From: Membre-smv [mailto:[email protected]] On Behalf Of BOUCHAUD OlivierSent: donderdag 25 juni 2015 16:14To: [email protected]: [Membre-smv] schéma court vaccin encéphalite japonaise
2015

27/11/2015
35
From: Mar Faraco via International Society of Travel Medicine [mailto:[email protected]] Sent: woensdag 26 augustus 2015 12:56Subject: RE: TravelMed : Japanese Encephalitis vaccine - last minute traveller
2015
“the rapid schedule for IXIARO was autorized by EMA (European Medicines Agency) this August, just in case you have at least 1 week to vaccinate this particular traveller http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000963/WC500037287.pdfIt is 2 dosis in days 0-7, but with the precaution to have both doses at least 7 days before departure (as normal schedule), to achieve immunity”
Last updated 13/08/2015
Duration immunity after full schedule Ixiaro ® ?
27/11/2015
36
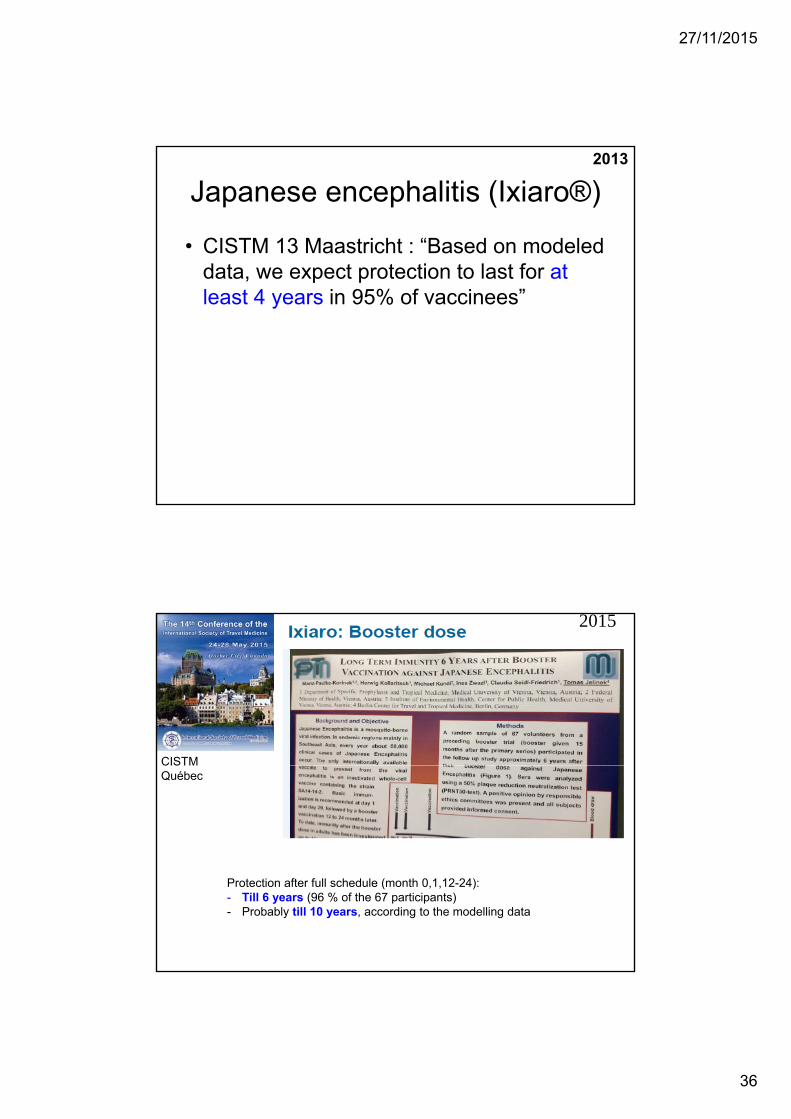
Japanese encephalitis (Ixiaro®)
• CISTM 13 Maastricht : “Based on modeled data, we expect protection to last for at least 4 years in 95% of vaccinees”
2013
CISTMQuébec
2015
Protection after full schedule (month 0,1,12-24):- Till 6 years (96 % of the 67 participants)- Probably till 10 years, according to the modelling data

27/11/2015
37
PO03.10Long Term Immunity 6 Years after Booster Vaccination against Japanese EncephalitisM. Paulke-Korinek1, H. Kollaritsch1, M. Kundi2, I. Zwazl1, C. Seidl-Friedrich1, T. Jelinek3
1Medical University Vienna, Department of Specific Prophylaxis and Tropical Medicine, Vienna,Austria, 2Medical University Vienna, Institute of Environmental Health, Center for Public Health,
Vienna, Austria, 3Berlin Center for Travel and Tropical Medicine, Berlin, Germany
Background and Objective: Japanese Encephalitis is a mosquito-borne viral infection. In endemic• regions mainly in Southeast Asia, every year about 68,000 clinical cases of Japanese Encephalitis• occur. The only internationally available vaccine to prevent from the viral encephalitis is an inactivated• whole-cell vaccine containing the strain SA14-14-2. Basic immunization is recommended at day 1 and• day 29, followed by a booster vaccination 12 to 24 months later. To date, immunity after the booster• dose in adults has been investigated up to 12 months. This study was initiated to assess antibody• decline and to predict long-term duration of seroprotection.Method: A random sample of 70 volunteers from a preceding booster trial (booster given 15 months• after the primary series, 45% of originally vaccinated) was invited to the follow up study and 67 (96%)• participated approximately 6 years after their booster dose against Japanese Encephalitis. Sera were• analyzed using a 50% plaque reduction neutralization test (PRNT50-test). A positive opinion by• responsible ethics committees was present and all subjects provided informed consent.Result: Six years after the last booster dose, geometric mean titer was still 148 (95% CI:107 to 207),• and 96% of the tested subjects had antibody titers above PRNT50 values of 10, the surrogate level of• protection according to WHO. Antibody titers generally were lower in subjects aged 50 years and• older. Yellow fever vaccination and vaccination against TBE had no significant effects on antibody• titers against Japanese Encephalitis.Conclusion: Long-term protection against Japanese Encephalitis after basic immunization and one• booster dose against Japanese Encephalitis up to 6 years could be shown in the majority of subjects.• This implies that a second booster may not be necessary for at least 6 years after the first booster.Conflict of Interest: The study was supported by Valneva, Austria
2015 Final publication of these data available online since 30 May 2015

27/11/2015
38
Background: • Japanese Encephalitis (JE) virus occurs in wide regions of Asia with over 3 billion people living in areas at risk for JE. • An estimated 68,000 clinical cases of JE occur every year, and vaccination is the most effective prophylactic measure. • One internationally licensed vaccine containing the inactivated JEvirus strain SA14-14-2 is Ixiaro® (Valneva, Austria). • According to recommendations, basic immunizationconsists of vaccinations on day 0, day 28, and a booster dose 12–24 months later. • Protection in terms of neutralizing antibody titers has been assessed up to 12 months after the third dose of the vaccine.• The current investigation was designed to evaluate antibody decline over time and to predict long-termduration of seroprotection after a
booster dose
Method: • In a preceding trial, volunteers received basic immunization (day 0, day 28) and one
booster dose against JE 15 months later. A follow up blood draw 6 years following their booster dose was carried out in 67 subjects. For antibody testing, a 50% plaque reduction neutralization test (PRNT50-test) wasused. PRNT50values of 10 and above are surrogate levels of protection according to WHO standards
Result: • Seventy-six months following the booster dose, 96% of the tested subjects had
PRNT50 titers of 10 or higher. • Geometric mean titer (GMT) was 148 (95% CI confidence interval: 107–207). • Antibody titers were lower in volunteers 50 years of age and older. • Vaccination history against other flaviviruses (yellowf ever or tick borne encephalitis)
did not significantly influence PRNT50titers. • A two-step log-linear decline model predicted protection against JE of approximately
14 years after the booster dose.Conclusion: • Six years after a booster dose against JE, long-term protection could be
demonstrated.• According to our results, further booster doses should be scheduled 10 years
following the first booster dose.
2015
Ixiaro ® is available in Belgium since the summer of 2010
A first booster has been given 12-24 months after the start of the primovaccination.
So in the summer of 2017 the first clients for a second booster may show up.
What will be the advice ? 6 years ? 10 years ? we will wait EMA
EMA 13/08/2015 (website consulted 01/10/2015) “Data on the need for further booster doses are not available”
2015
Ixiaro ® is not available in many countries in Asia, but it might be available under another name : e.g. JEEV (from India), Jespect (from Australia)
Other inactivated Vero cell-derived vaccines are produced in Asia : e.g., Genovax® (Bharat Biotech India), …

27/11/2015
39
Live JE vaccines in Asia • 1 injection for “lifelong” protection (20 y ? 30 y ?)
- BUT longterm immunogenicity data are limited - in children a second injection might be indicated
• Might be useful for expats • Different types / very variable local prices :
– live attenuated (Chengdu – made in China)
– live recombinant - chimeric (Imojev® - made by Novartis-Australia)
2015
Scientific details :
TBE FSME
2015

27/11/2015
40
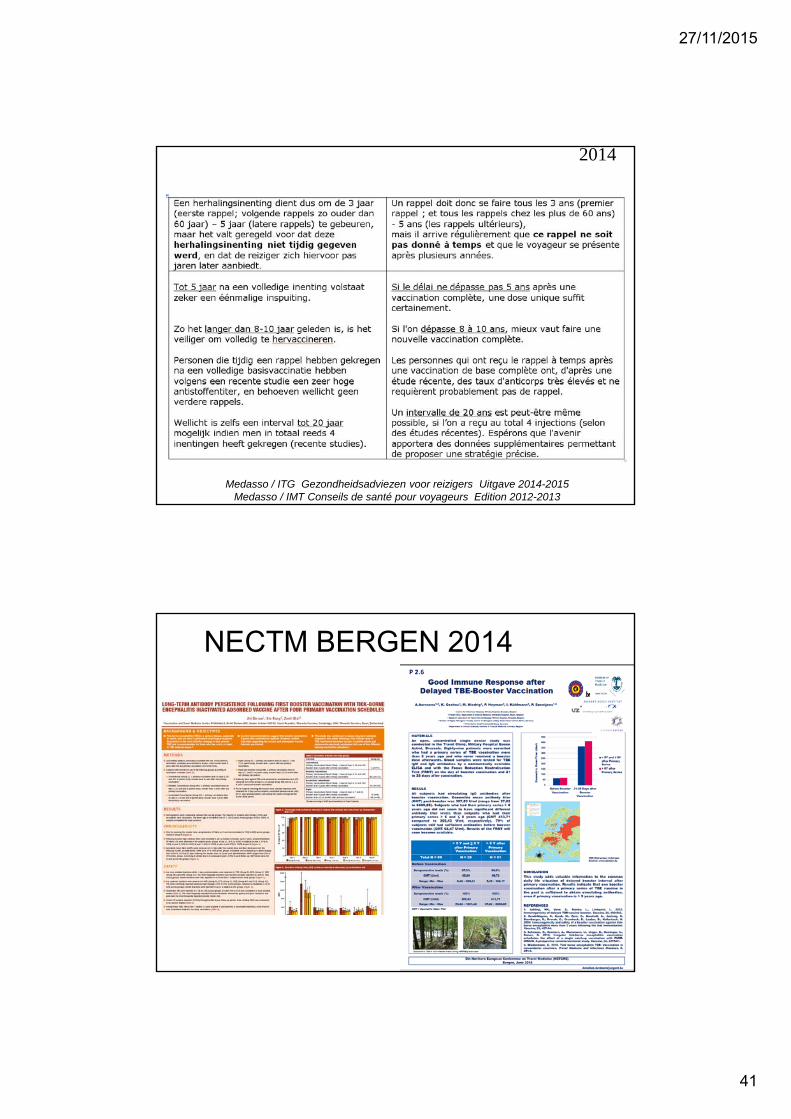
2014 = 15
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
27/11/2015
41
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
2014
NECTM BERGEN 2014

27/11/2015
42
CISTMQuébec
2015
“The serological response is thought to persist after the first booster dose. Therefore, it probably is never necessary to re-vaccinate with a complete series if one was administered before”
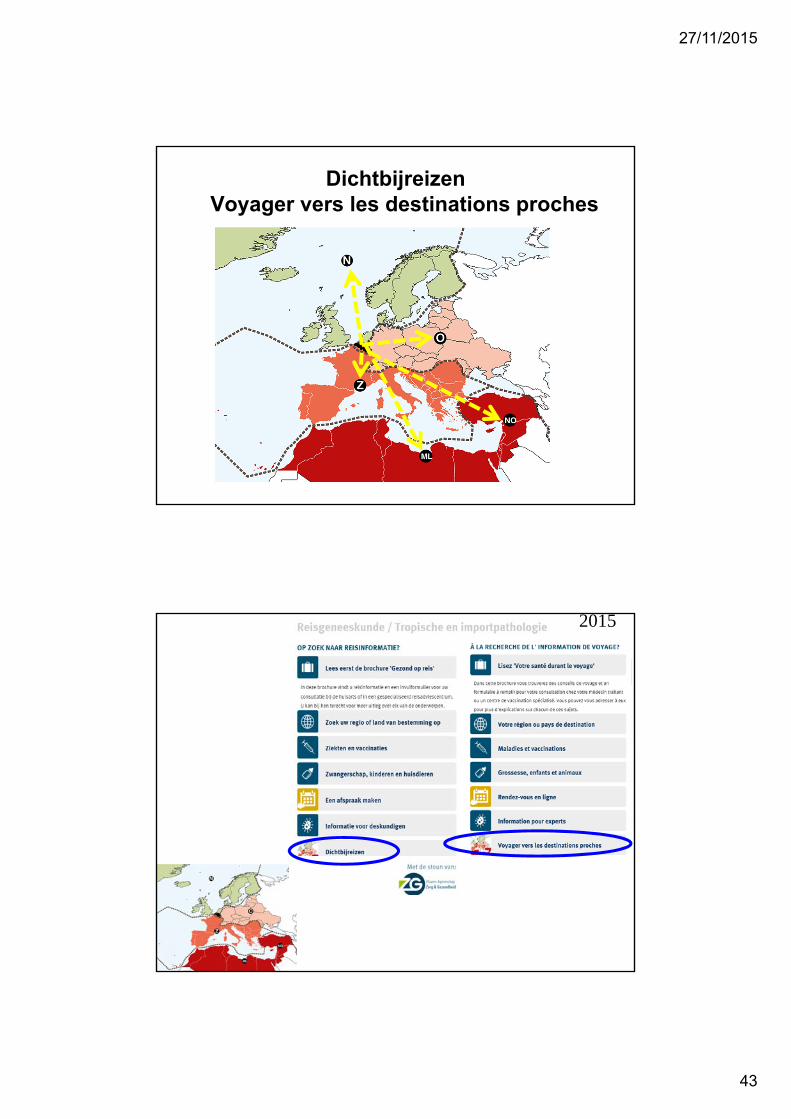
DichtbijreizenVoyager vers les destinations proches
27/11/2015
43
DichtbijreizenVoyager vers les destinations proches
2015

27/11/2015
44
PART 1• 1.A - Vaccination for Yellow Fever• 1.B - Malaria
PART 2• 2.A - Other vaccinations• 2.B - TD, other infections, …., • 2.C - VARIA
2015

27/11/2015
45
2015

27/11/2015
46
Background• More than 300 million travelers visit regions with poor hygiene annually. A significant percentage of
them become colonized by resistant intestinal bacteria such as extended-spectrum beta-lactamase–producing Enterobacteriaceae (ESBL-PE) and may transmit the strains to others and to medical care settings when they return home. .
Methods• Stool samples were collected from 430 Finns before and after traveling outside Scandinavia. • All specimens were analyzed for ESBL- and carbapenemase-producing Enterobacteriaceae (CPE). • Questionnaires were used to survey volunteers about use of antimicrobials as well as other potential
risk factors.
Results • 21 % (90/430) of the travelers became colonized by ESBL-PE -
none by CPE. • Were identified as independent predisposing risk factors
(1) Geographic region (2) occurrence of travelers’ diarrhea (TD) (3) age (4) use of antimicrobial (AB) for TD
Antimicrobials Increase Travelers’ Risk of Colonization by Extended-Spectrum Betalactamase-Producing Enterobacteriaceae
• 11 % of those in subgroup TD−AB−, 21% in TD+AB−, and 37% in TD+AB+ acquired ESBL-PE.
• The risk proved to be highest in South Asia (46%); 23% became colonized in subgroup TD−AB−, 47% in TD+AB−, and 80% in
TD+AB+. • In Southeast Asia, the rates were 14%, 37%, and 69%, respectively.
Antimicrobials Increase Travelers’ Risk of Colonization by Extended-Spectrum Betalactamase-Producing Enterobacteriaceae
21 % (90/430) of the travelers became colonized by ESBL-PESouth Asia (46%) Southeast Asia
TD−AB−, 11% 23% 14%TD+AB−, 21% 47% 37%TD+AB+ 37% 80% 69%
Conclusions• TD and antimicrobials for TD proved to be independent risk factors,
with up to 80% of TD+AB+ travelers contracting ESBL-PE. • In modern pre-travel counseling for those visiting high-risk regions,
travelers should be advised against taking antibiotics for mild or moderate TD.

27/11/2015
47
2015
2015

27/11/2015
48
2015
2015

27/11/2015
49
2015
2015

27/11/2015
50
2015
2015

27/11/2015
51
2015
2015

27/11/2015
52
2015
2015

27/11/2015
53
2015
2015
27/11/2015
54
2015
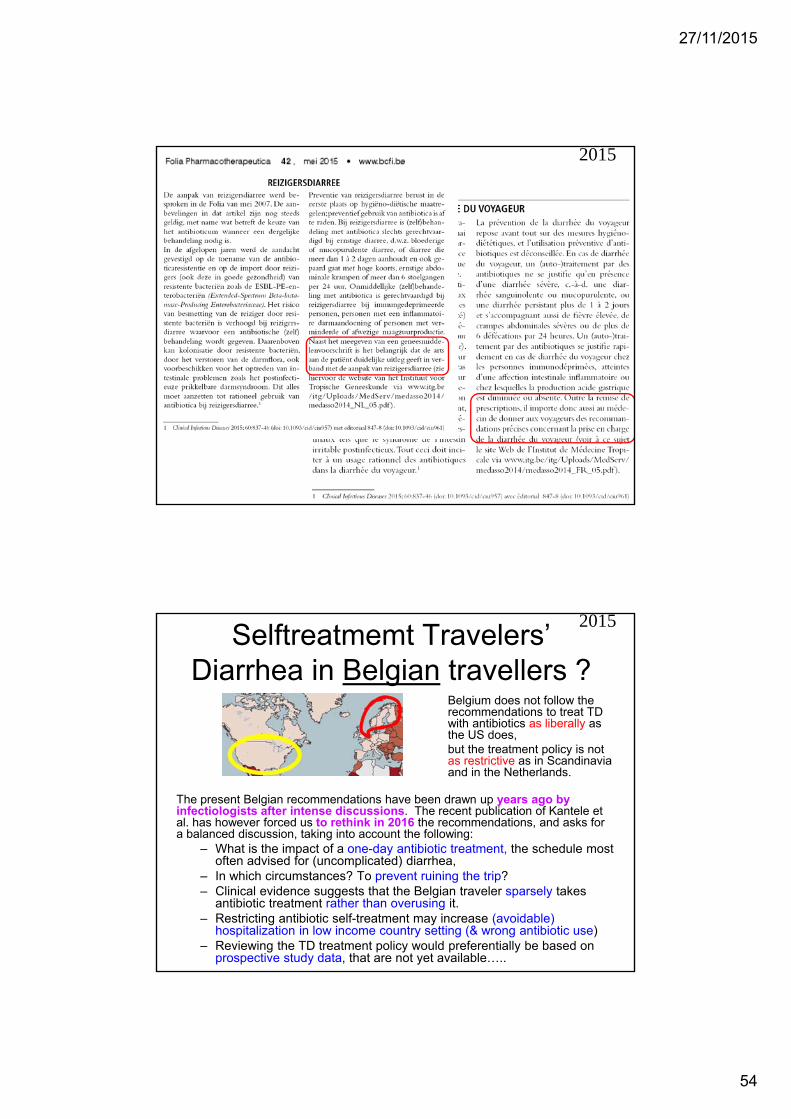
Selftreatmemt Travelers’ Diarrhea in Belgian travellers ?
2015
The present Belgian recommendations have been drawn up years ago by infectiologists after intense discussions. The recent publication of Kantele et al. has however forced us to rethink in 2016 the recommendations, and asks for a balanced discussion, taking into account the following:
– What is the impact of a one-day antibiotic treatment, the schedule most often advised for (uncomplicated) diarrhea,
– In which circumstances? To prevent ruining the trip?– Clinical evidence suggests that the Belgian traveler sparsely takes
antibiotic treatment rather than overusing it.– Restricting antibiotic self-treatment may increase (avoidable)
hospitalization in low income country setting (& wrong antibiotic use)– Reviewing the TD treatment policy would preferentially be based on
prospective study data, that are not yet available…..
Belgium does not follow the recommendations to treat TD with antibiotics as liberally as the US does, but the treatment policy is not as restrictive as in Scandinavia and in the Netherlands.

27/11/2015
55
2015
Quid role in travel medicine ?
2013

27/11/2015
56
Travel medicine Seminar 19 /11/15 “Travel medicine Seminar 20 years later”
MILITAIR HOSPITAAL as in 1995 14.00-14.05 Introduction
14.05-14.35 Yellow fever vaccination issues CHARLOTTE MARTIN
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedulesPATRICK SOENTJENS
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines STEVEN CALLENS
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrheaLUCIE SEYLER
16.25- 16.50 Malaria: when prevention is not clear-cutULA MANIEWSKI
16.50-17.15 Traveller's ThrombosisPETER VERHAMME
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ? FONS & YVES
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009
Chikungunya
2015

27/11/2015
57
2014
Eurosurveillance, Volume 19, Issue 28, 17 July 2014
2015
CDC

27/11/2015
58
Dengue
2015
2014=5

27/11/2015
59
Although rather “suboptimal” efficacySanofi-vaccine will be available in endemic regions end 2015 ???
2015
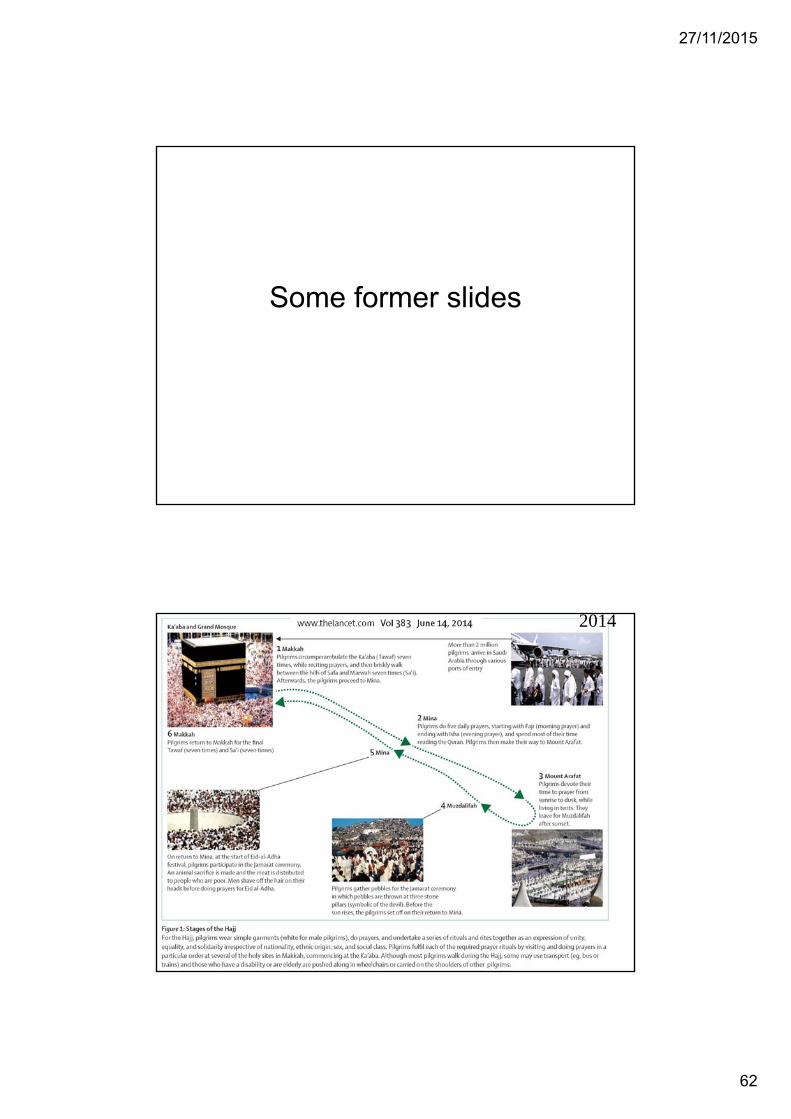
Hajj
2014 = 2015
No change of the health advice in • 2014• 2015 (= 20/9-25/9)

27/11/2015
60
2015
2015

27/11/2015
61
General advice for Mecca pilgrims -required/recommended vaccines• Vaccination with a tetravalent, conjugated ACYW135
meningococcal vaccine is required to obtain a visa.
• Available vaccines in Belgium: Nimenrix® and Menveo®
• The unconjugated 4-valent meningococcal vaccine is not available anymore in pharmacy (July 2013) – it might still be available in the travel clinics and be used in pilgrims
• It remains unclear if children till the age of 2 years are obliged to be vaccinated, but it correct to vaccinate also the little children – on the other hand, see further : children under 12 yrs are discouraged to come to Mecca.
2013 = 2014 = 2015
General advice for Mecca pilgrims -required/recommended vaccines• Incompletely vaccinated individuals should update
their vaccine status.• Vaccination against the seasonal flu is
recommended when available (around mid-September, the pilgrimage starts October 4th).
• Pneumococcal vaccine for the known risk groups• Hepatitis A vaccination is recommended,
depending on age and medical history.• For journeys exceeding 3 weeks stay, a
vaccination against typhoid fever may be advisable.
2013 = 2014 = 2015
27/11/2015
62
Some former slides
2014

27/11/2015
63
Kingdom of Saudi Arabia Ministry of Health
Health Regulations for travellers to Saudi Arabia for Umrah &
Pilgrimage (Hajj)-1435 (2014).
2014
2014

27/11/2015
64
http://www.who.int/wer/2013/wer8832.pdf
Varia– Hajj 2013
Varia– Hajj
MEKKA http://www.hajinformation.com/main/p3001.htm -
• meningococcal vaccine remain obligatory• influenza vaccine remain imperatively
advised
2013

27/11/2015
65
2012
… & Mers
2015

27/11/2015
66
2014

27/11/2015
67
Promedmail - Morocco 19-6-2014• Advice not to go on the Hadj … !!
2014
27/11/2015
68
Because of the MERS-Cov : The Saudi Ministry of Health
recommends that people• aged over 65 years and • those with chronic diseases (e.g. heart disease, kidney disease,
respiratory disease, diabetes) and • pilgrims with immune deficiency (congenital and acquired), • malignant and • terminal illnesses, • pregnant women and • children aged under 12 years
planning to come for Hajj and Umra this year, to postpone the performance of the Hajj and Umra for their own safety.
2013
Schistosomiasis Corsica ?
2015

27/11/2015
69
2014
EID sept 2014 Letter
2015 “ …Until today, no cases had been identified with exposure in 2014. None of 3 534 Bulinus snails in the Cavu River tested in summer 2014 were infected. In addition, 38 bathing sites in 19 other rivers in Corsica were investigated for the presence of snails. Bulinus snails were found in two bathing sites in Solenzara, two sites in Osu and one site in Tarcu. None were found positive for Schistosoma spp.” ECDC risk-assessment 23-7-2015
The swimming ban in Cavu River was lifted on 4 June 2015.Surveillance for schistosomiasis is still ongoingDr J. Clerinx ITG/IMT
2014

27/11/2015
70
PART 1• 1.a - Vaccination for Yellow Fever• 1.b - Malaria
PART 2• 2.A - Other vaccinations• 2.B - TD, other infections, …., • 2.C - VARIA
2015
27/11/2015
71
Travel medicine Seminar 19 /11/15 “Travel medicine Seminar 20 years later”
MILITAIR HOSPITAAL as in 1995 14.00-14.05 Introduction
14.05-14.35 Yellow Fever Immunization: where are we up to now?CHARLOTTE MARTIN
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedulesPATRICK SOENTJENS
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines STEVEN CALLENS
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrheaLUCIE SEYLER
16.25- 16.50 Malaria: when prevention is not clear-cutULA MANIEWSKI
16.50-17.15 Traveller's ThrombosisPETER VERHAMME
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ? FONS & YVES
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009
END
2015





























