Embed Size (px)
Citation preview

BEHCET’S DISEASEBEHCET’S DISEASE
Eldad Ben-Chetrit - 2012Eldad Ben-Chetrit - 2012

BEHCET’S DISEASEBEHCET’S DISEASE
A rare multisystem, chronic disease A rare multisystem, chronic disease characterized by oral and genital characterized by oral and genital mucocutaneous ulcerations, skin rashes, mucocutaneous ulcerations, skin rashes, arthritis, thrombophlebitis, uveitis, colitis, arthritis, thrombophlebitis, uveitis, colitis, and neurologic symptoms.and neurologic symptoms.

“ “ Silk Road DiseaseSilk Road Disease””
Endemic in Japan and Northeastern Mediterranean region (Turkey & Iran)

Hulusi Behçet was a Turkish dermatologist from Istanbul (1889–1948).Described the syndrome in 1936

Other names of the syndromeOther names of the syndrome
Adamantiades’ syndrome – 1930
Behçet's disease – 1936 Adamantiades-Behçet syndrome Gilbert's syndrome - 1920

EPIDEMIOLOGYEPIDEMIOLOGY
Incidence/Prevalence:Incidence/Prevalence:
In USAIn USA 1/100, 0001/100, 000
In Japan - 670/100,000 In Japan - 670/100,000 (during the last years there is a (during the last years there is a significant decrease in this rate)significant decrease in this rate)
In Turkey - 80-320/100,000 In Turkey - 80-320/100,000

EPIDEMIOLOGYEPIDEMIOLOGY
Predominant age: 3rd to 4th decadesPredominant age: 3rd to 4th decades
Predominant sex: Male > Female; as Predominant sex: Male > Female; as frequently to twice as often. Some studies frequently to twice as often. Some studies suggest equal frequency.suggest equal frequency.

EtiologyEtiology
UnknownUnknown
Various bacteria and viruses suggestedVarious bacteria and viruses suggested (No good evidence to suggest any of them)(No good evidence to suggest any of them)
Tumor necrosis factor (TNF) thought to be Tumor necrosis factor (TNF) thought to be importantimportant
Genetic factors (HLA-B51, SNPs in IL-1)Genetic factors (HLA-B51, SNPs in IL-1)

Systemic Involvement- Systemic Involvement- MucocutaneousMucocutaneous
Oral aphthous ulceration – 100%Oral aphthous ulceration – 100%

Oral AphthaeOral Aphthae


BEHBEHÇÇET’S DISEASE ET’S DISEASE Systemic InvolvementSystemic Involvement
Genital ulceration –Genital ulceration – 60-8060-80%%

BEHBEHÇÇET’S DISEASE ET’S DISEASE Systemic InvolvementSystemic Involvement
Skin lesions – 80%Skin lesions – 80%– Erythema NodosumErythema Nodosum– Pyoderma gangrenosumPyoderma gangrenosum

Acneiform pustulosis & folliculitis

““Spontaneous” pathergy testSpontaneous” pathergy test

Pulmonary aneurysmsPulmonary aneurysms

Systemic Involvement Systemic Involvement blood vesselsblood vessels
Major vessels eg Major vessels eg superior Vena superior Vena cava obstructioncava obstruction

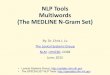
Axial T2-weighted images in acute stage of neuro-Behcet disease showing diffuse enlargement of the pons (A) with edema extending to the midbrain and right internal capsule (B). Six years later, axial T2-weighted image shows advanced atrophy of the brainstem (C), and axial T1-weighted image with gadolinium enhancement shows a small area of enhancement in the caudal midbrain (D).
CNS involvement – strokes, fits
A patient who presented with seizures and A patient who presented with seizures and hemiparesis due to cortical vein thrombosis with hemiparesis due to cortical vein thrombosis with infarctioninfarction

Ocular FeaturesOcular Features
Uveitis 70% (inflam. Uveitis 70% (inflam. of iris, ciliary body of iris, ciliary body or choroidor choroid))
Acute iritisAcute iritis
Recurrent Recurrent hypopyonhypopyon(Fluid level of WBC)(Fluid level of WBC)
The red or white eyeThe red or white eye

HYPOPYON – pus in the anterior chamber associated with uveitis

Intestinal BDIntestinal BDIntestineIntestine– Presentation similar to Crohn’s disease (CD). Presentation similar to Crohn’s disease (CD).
In pt with intestinal BD, other stigmata of BD In pt with intestinal BD, other stigmata of BD may appear latermay appear later
– Rectal and anal involvement rareRectal and anal involvement rare
– Ileocecal involvement common to Japan & Ileocecal involvement common to Japan & Turkey. Colonic involvement common in Turkey. Colonic involvement common in Europe & N. AmericaEurope & N. America

Intestinal BD contIntestinal BD cont....
– Morphology of lesions: aphthous ulcers Morphology of lesions: aphthous ulcers or deep round or oval ulcers with or deep round or oval ulcers with punched-out appearance. Longitudinal punched-out appearance. Longitudinal ulcers rareulcers rare
– Ulcers localize and appear in clustersUlcers localize and appear in clusters

The Esophagous in Behcet’s The Esophagous in Behcet’s diseasedisease

Small intestine in Behcet’s Small intestine in Behcet’s DiseaseDisease

Differential DiagnosisDifferential Diagnosis
– Reactive arthritis and other forms of Reactive arthritis and other forms of spondyloarthropathy spondyloarthropathy
– Inflammatory bowel disease (Crohn's disease Inflammatory bowel disease (Crohn's disease and ulcerative colitis) and ulcerative colitis)
– Syphilis Syphilis

Differential DiagnosisDifferential Diagnosis
– Herpes simplex Herpes simplex
– Stevens-Johnson syndromeStevens-Johnson syndrome
– Vasculitides Vasculitides
– Thrombophlebitis related to coagulation factor Thrombophlebitis related to coagulation factor deficiency deficiency

ComplicationsComplications
– Death Death (rupture of pulmonary aneurysm)(rupture of pulmonary aneurysm)
– Blindness Blindness
– Paralysis Paralysis
– Embolism/thrombosis - pulmonary, vena cava, Embolism/thrombosis - pulmonary, vena cava, peripheral peripheral
– Amyloidosis Amyloidosis

DIAGNOSISInternational Study Group Criteria 1990

INTERNATIONAL CRITERIA
Classification Tree
2006
ITR-ICBD

Revision of the International Criteria for Behcet’s Disease (ICBD 1,2,3,)
- Austria (M. Schirmer, M Baltaci), Azerbaijan (A. Isayeva), China (Y. Dong, Z. Zhang), Egypt ) S. Assaad-Khalil), France (B. Wechsler), Germany (C.C. Zouboulis, A. Altenburg), Greece (Ph. Kaklamanis), India (A. Kumar), Iran (F. Davatchi, B. Sadeghi-Abdollahi, F. Shahram, A. Nadji, C. Chams-Davatchi, H. Shams, N. Zia’I, M. Akhlagi, A.R. Jamshidi, A.K. Haghdoost), Iraq) K. Sharquie, R. Hayani ,Israel (Eldad Ben-Chetrit), Italy (I. Olivieri, C. Salvarani, N. Pipitone), Japan (Sh. Ohno, K. Namba), Jordan (W. Madanat (Libya (K. Elmuntaser( Morocco (S. Benamour), Pakistan (A. Ali), Portugal (J. Crespo, T Tribolet, C Vasconcelos, J Correia, L Carvalho, M Bastos, MJ Serra, C Resende, F Ramos, M Rosa, V Queirós, J Vedes, C. Dias, J.V. Patto, FP Duarte), Russia (Z. Alekberova, A. Elonakov), Saudi Arabia (A. Al Dalaan), Singapore (C. Yew Kuang), Spain (G. Grana Gil), Taiwan (W.C. Chen), Thailand (A. Emvalee), Tunisia (H. Houman, I. Ben Ghorbel, M. Sliti-Khanfir), Turkey (A. Boyvat), USA (K. Calamia). Coordinator: F. Davatchi. Data collection and analysis: Rheumatology Research Center, Tehran University for Medical Sciences

Table 2: Traditional format criteria
PointsPoints
Oral aphthosisOral aphthosis 11
Skin manifestationsSkin manifestations 11
Vascular lesions (arterial and Vascular lesions (arterial and venous thrombosis, aneurysm)venous thrombosis, aneurysm)
11
Pathergy phenomenon (Test)Pathergy phenomenon (Test) 11
Genital aphthosisGenital aphthosis 22
Ocular LesionsOcular Lesions 22
Behcet’s Disease: 3 or more points

PrognosisPrognosis
– Normal life expectancy, except with neurologic Normal life expectancy, except with neurologic involvementinvolvement
– Possible vision impairmentPossible vision impairment
– Improvement with ageImprovement with age

Genetics of Behcet’s diseaseGenetics of Behcet’s disease
Familial aggregationFamilial aggregation
Familial clustering is more frequent among Familial clustering is more frequent among juvenile onset (<16 Y).juvenile onset (<16 Y).
Geographic distribution – endemic areas Geographic distribution – endemic areas overlap with the ancient Silk Roadoverlap with the ancient Silk Road
BD is strongly associated with class I BD is strongly associated with class I MHC allele, HLA-B51MHC allele, HLA-B51

Genome wide associated studyGenome wide associated study

Genome-wide association study identifies variants in the MHC Genome-wide association study identifies variants in the MHC class I, IL10, and IL23R-IL12RB2 regions associated with class I, IL10, and IL23R-IL12RB2 regions associated with Behçet’s diseaseBehçet’s disease
Elaine F RemmersElaine F Remmers, Fulya Cosan, Yohei Kirino, Michael J Ombrello, Neslihan Abaci, Colleen , Fulya Cosan, Yohei Kirino, Michael J Ombrello, Neslihan Abaci, Colleen
Satorius, Julie M Le, Barbara Yang, Benjamin D Korman, Aris Cakiris, Oznur Aglar, ZelihaSatorius, Julie M Le, Barbara Yang, Benjamin D Korman, Aris Cakiris, Oznur Aglar, Zeliha
Emrence, Hulya Azakli, Duran Ustek, Ilknur Tugal-Tutkun, Gulsen Akman-Demir, Wei Chen, Emrence, Hulya Azakli, Duran Ustek, Ilknur Tugal-Tutkun, Gulsen Akman-Demir, Wei Chen,
Christopher I Amos, Michael B Dizon, Afet Akdag Kose, Gulsevim Azizlerli, Burak Erer, Oliver Christopher I Amos, Michael B Dizon, Afet Akdag Kose, Gulsevim Azizlerli, Burak Erer, Oliver
J Brand, Virginia G Kaklamani, Phaedon Kaklamanis, J Brand, Virginia G Kaklamani, Phaedon Kaklamanis, Eldad Ben-ChetritEldad Ben-Chetrit, Miles Stanford, , Miles Stanford,
Farida Fortune, Marwen Ghabra, William E R Ollier, Young-Hun Cho, Dongsik Bang, John Farida Fortune, Marwen Ghabra, William E R Ollier, Young-Hun Cho, Dongsik Bang, John
O’Shea, Graham R Wallace, Massimo Gadina, O’Shea, Graham R Wallace, Massimo Gadina, Daniel L Kastner & Ahmet GülDaniel L Kastner & Ahmet Gül
Nat Genet 2010 Nat Genet 2010

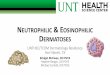
Figure 1 Behçet’s disease genome-wide association results. The −log10 P values (allelic χ2 test) for association of 311,459 autosomal SNPs in 1,215 Behçet’s disease cases and 1,278 controls from Turkey are shown segregated by chromosome and sorted by genomic position.
6
HLA-B51
IL-10
1 CPLX-1

The difference in expression of the gene The difference in expression of the gene between the disease-associated haplotype between the disease-associated haplotype and normal haplotypes – was testedand normal haplotypes – was tested

These data suggest that genetic variants These data suggest that genetic variants contributing to low IL-10 expression may contributing to low IL-10 expression may be a risk factor for Behçet’s disease.be a risk factor for Behçet’s disease.

This observation may suggest IL-10 as an This observation may suggest IL-10 as an additional therapeutic measure.additional therapeutic measure.

Behcet’s disease – treatmentBehcet’s disease – treatment
AzathioprineAzathioprine
SteroidsSteroids
ChlorambucilChlorambucil
ColchicineColchicine
CyclophosphamideCyclophosphamide
CyclosporineCyclosporine
• Tacrolimus
• IFN – α
• Thalidomide
• MTX
• Mycophenolate mofetil
• Anti – TNFα: – Infliximab
– Etanercept


Year 1998 Systematic ReviewYear 1998 Systematic Review::
ConclusionsConclusions
3232 studies were reviewed studies were reviewed
679 Behcet’s patients679 Behcet’s patients
No difference between placebo and colchicine – aphthous stomatitisNo difference between placebo and colchicine – aphthous stomatitis
Local interferon is not effective in ulcersLocal interferon is not effective in ulcers
Cyclosporin is better than colchicine for oral ulcers.Cyclosporin is better than colchicine for oral ulcers.

A double-blind trial of colchicine in Behcet's syndromeA double-blind trial of colchicine in Behcet's syndrome . . Arthritis Rheum 2001 Nov;44(11):2686-92.Arthritis Rheum 2001 Nov;44(11):2686-92.
Double blind study.Double blind study.
116 patients with joint and mucocutaneous 116 patients with joint and mucocutaneous involvement only.involvement only.
Colchicine versus placeboColchicine versus placebo
Significant improvement in treated group in Significant improvement in treated group in genital ulcers, erythema nodosum and arthritisgenital ulcers, erythema nodosum and arthritis
Treatment of mucocutaneous Treatment of mucocutaneous involvementinvolvement

Most common current treatmentMost common current treatment
PrednisonePrednisone
AzathioprineAzathioprine
MethotrexateMethotrexate
CyclosporinCyclosporin
InterferonInterferon

What is the treatmet for resistant Behcet’s Disease?
Biologics

A patient with severe Behcet’s A patient with severe Behcet’s disease – a therapeuticdisease – a therapeutic

Patient Rita MPatient Rita M..
A 48 year old lady came from Armenia due A 48 year old lady came from Armenia due to severe aphthous stomatitisto severe aphthous stomatitisA year before she started having recurrent A year before she started having recurrent oral and genital ulcers, general weakness, oral and genital ulcers, general weakness, headache, trigeminal neuralgia,headache, trigeminal neuralgia, an an episode of uveitis and elevated ESR and episode of uveitis and elevated ESR and CRPCRPShe was under colchicine treatment She was under colchicine treatment continuouslycontinuously

Patient (cont.)Patient (cont.)
She was treated with steroids with mild She was treated with steroids with mild improvement and even cyclophosphamide improvement and even cyclophosphamide (The indication is not really clear)(The indication is not really clear)
Local anesthetics and antibiotics were Local anesthetics and antibiotics were ineffective.ineffective.

Patient (Cont.)Patient (Cont.)
Following 3 weeks her situation Following 3 weeks her situation deteriorated. She could not eat due to the deteriorated. She could not eat due to the oral pains which irradiated to her left earoral pains which irradiated to her left ear
On physical examination the main findings On physical examination the main findings were 3 severe and large oral ulcerswere 3 severe and large oral ulcers
Some papulo-squamous rash over her Some papulo-squamous rash over her scalpscalp

Patient (cont.)Patient (cont.)
ESR -70ESR -70
CRP- 3.7CRP- 3.7
Hemoglobin 10.8Hemoglobin 10.8
HLA-B51 positiveHLA-B51 positive
ANA and RF – negativeANA and RF – negative
Zeil Nilssen staining negativeZeil Nilssen staining negative

Patient (cont.)Patient (cont.)
She got fluidsShe got fluids
Systemic antibioticsSystemic antibiotics
300 mg solumedrol (IV)300 mg solumedrol (IV)
No significant improvement.No significant improvement.

Patient (Cont.)Patient (Cont.)
She got 300 mg Remicade with dramatic She got 300 mg Remicade with dramatic improvement.improvement.

Patient (Cont.)Patient (Cont.)
After a few months (and having After a few months (and having discontinued the anti TNF treatment on discontinued the anti TNF treatment on her own), she was re-hospitalized because her own), she was re-hospitalized because of severe pain with a large skin lesion on of severe pain with a large skin lesion on her left leg. her left leg.

Patient (Cont.)Patient (Cont.)
A diagnosis of pyoderma gangrenosum A diagnosis of pyoderma gangrenosum was made.was made.
Topical treatment was ineffective. Topical treatment was ineffective. Therefore the patient was treated with Therefore the patient was treated with pulse solumedrol 1 gr for two successive pulse solumedrol 1 gr for two successive days and 500 mg on the third day, and she days and 500 mg on the third day, and she received 300 mg Remicade intravenously. received 300 mg Remicade intravenously.

Again, significant and quick Again, significant and quick improvement was noted regarding improvement was noted regarding
the skin lesion on her calfthe skin lesion on her calf


Patient (cont.)
Recently, she came again to our clinic because of severe mouth and right ear pain with excessive salivation, difficulties in swallowing and mild hoarseness.
The patient was not on Remicade for at least 3 months (she could not obtain this agent for logistic reasons) but instead was treated with Enbrel 25 mg twice a week.

Patient (cont.)
On physical examination the main findings through indirect laryngoscopy were narrowing of the larynx with swelling of the epiglottis (mainly on the left side) and fibrinous discharge. The arytenoid was reddish and swollen and the epiglottis was partially bitten.


Patient (cont.)
The patient was treated with three doses of solu-medrol (750 mg, 500 mg and 500 mg) and 300 mg Remicade. Following this treatment her condition improved significantly within a week

Patient (cont.)
After 12 days the swelling of the arytenoid disappeared and the vocal cord on the same side returned to its place. The pain in the ear and the ipsilateral headache diminished and the excessive salivation improved as well.

This case exemplify the potential risks of laryngeal stenosis and the difficulties in treatment – sometimes requiring surgical intervention.

Unique characteristics of the case
The present case is unique in several points: First, it describes a patient with unusual resistant Behcet's disease presenting with recalcitrant aphthous stomatitis, later with pyoderma gangrenosum and recently with severe laryngeal involvement.

Unique characteristics of the case
None of the previous reports used anti TNF blockers as a treatment for this devastating clinical condition.
Second, it shows the dependency of the disease on anti TNF treatment and its dramatic effect in ameliorating all these clinical conditions.

Unique characteristics of the case
Third, it shows that different anti TNF agents have different effects on this pathology. Etanercept was found to be ineffective in treating the severe inflammation and aphthae in the larynx, while infliximab was significantly effective.

REMICADE VERSUS ENBRELREMICADE VERSUS ENBREL
Remicade has longer half timeRemicade has longer half time
In addition to soluble TNF it binds In addition to soluble TNF it binds membrane bound TNF leading to cell – membrane bound TNF leading to cell – lysislysis

In the futureIn the future……
Anti IL-1 agentsAnti IL-1 agents
Anti IL-6 receptor – ActemraAnti IL-6 receptor – Actemra
Anti IL-17 Ab – in phase III trialsAnti IL-17 Ab – in phase III trials

THANK YOU FOR YOUR ATTENTIONTHANK YOU FOR YOUR ATTENTION
QuestionsQuestions????
![WELCOME! [] · vasculitis to gather in smaller groups for discussions on treatments and side affects. All of the sessions will include time for Q&A. Breakout Session Behcet’s disease](https://img.pdfslide.us/doc/110x75/5ff5344cc376711a4b21bb0b/welcome-vasculitis-to-gather-in-smaller-groups-for-discussions-on-treatments.jpg)












![Evidence-Based Treatment of Behcet’s Diseasewhen early onset of the disease is present (particularly under 25 years) [2,3,4]. There are different prevalences and expressions of Behcet’s](https://img.pdfslide.us/doc/110x75/5ecaecfc1515f81011769292/evidence-based-treatment-of-behcetas-when-early-onset-of-the-disease-is-present.jpg)




![Behcet’s Disease: Radiologic Diagnosis · with Behcet’s disease is the rupture of a large aortic or arterial aneurysm [17]. Venous occlusion: Deep and superficial veins thrombophlebitis](https://img.pdfslide.us/doc/110x75/5ace29797f8b9a875a8eac4b/behcets-disease-radiologic-behcets-disease-is-the-rupture-of-a-large-aortic.jpg)