Embed Size (px)
Citation preview

Volumen IV No.3 Septiembre 2005
Current Treatment Options forNeovascular Age-Related Macular DegenerationSSuussaannnnaa SS.. PPaarrkk,, MMDD PPhhDD
Intraocular Lens Power Calculationfor Cataract Extraction after Corneal Refractive SurgeryVVaahhiidd FFeeiizz,, MMDD
Behçet's Disease and HyperprolactinemiaHHeelleennaa PPrrooeennççaa MMDD,, CCiiddaalliinnaa FFeerrrreeiirraa MMDD,, MMaarrggaarriiddaa MMiirraannddaa MMDD,, LLuuííss MMeettzznneerr SSeerrrraa PPhhDD,, AA.. CCaassttaannhheeiirraa--DDiinniiss PPhhDD
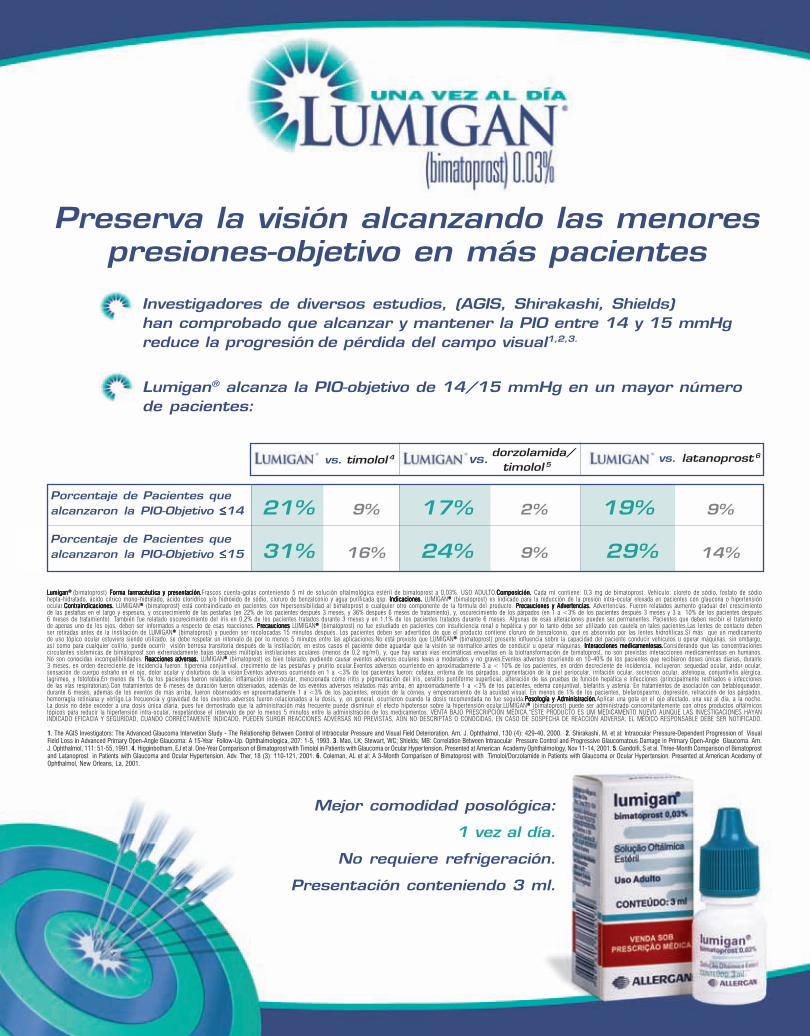
1. The AGIS Investigators: The Advanced Glaucoma Intervetion Study - The Relationship Between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophthalmol, 130 (4): 429-40, 2000. 2. Shirakashi, M. et al: Intraocular Pressure-Dependent Progression of VisualField Loss in Advanced Primary Open-Angle Glaucoma: A 15-Year Follow-Up. Ophthalmologica, 207: 1-5, 1993. 3. Mao, LK; Stewart, WC; Shields, MB: Correlation Between Intraocular Pressure Control and Progressive Glaucomatous Damage in Primary Open-Angle Glaucoma. Am.J. Ophthalmol, 111: 51-55, 1991. 4. Higginbotham, EJ et al. One-Year Comparison of Bimatoprost with Timolol in Patients with Glaucoma or Ocular Hypertension. Presented at American Academy Ophthalmology, Nov 11-14, 2001. 5. Gandolfi, S et al. Three-Month Comparison of Bimatoprostand Latanoprost in Patients with Glaucoma and Ocular Hypertension. Adv. Ther, 18 (3): 110-121, 2001. 6. Coleman, AL et al: A 3-Month Comparison of Bimatoprost with Timolol/Dorzolamide in Patients with Glaucoma or Ocular Hypertension. Presented at American Acedemy ofOphthalmol, New Orleans, La, 2001.
Preserva la visión alcanzando las menorespresiones-objetivo en más pacientes
Mejor comodidad posológica:
1 vez al día.
No requiere refrigeración.
Presentación conteniendo 3 ml.
LLLLLumiganumiganumiganumiganumigan® ® ® ® ® (bimatoprost) Forma farmacéutica y prForma farmacéutica y prForma farmacéutica y prForma farmacéutica y prForma farmacéutica y presentación.esentación.esentación.esentación.esentación.Frascos cuenta-gotas conteniendo 5 ml de solución oftalmológica estéril de bimatoprost a 0,03%. USO ADULTO.Composición. Composición. Composición. Composición. Composición. Cada ml contiene: 0,3 mg de bimatoprost. Vehículo: cloreto de sódio, fosfato de sódiohepta-hidratado, ácido cítrico mono-hidratado, ácido clorídrico y/o hidróxido de sódio, cloruro de benzalconio y agua purificada qsp. Indicaciones.Indicaciones.Indicaciones.Indicaciones.Indicaciones. LUMIGAN®®®®® (bimatoprost) es indicado para la reducción de la presión intra-ocular elevada en pacientes con glaucona o hipertensiónocular.Contraindicaciones.Contraindicaciones.Contraindicaciones.Contraindicaciones.Contraindicaciones. LUMIGAN®®®®® (bimatoprost) está contraindicado en pacientes con hipersensibilidad al bimatoprost o cualquier otro componente de la fórmula del producto. Pr Pr Pr Pr Precauciones y Adverecauciones y Adverecauciones y Adverecauciones y Adverecauciones y Advertencias.tencias.tencias.tencias.tencias. Advertencias. Fueron relatados aumento gradual del crescimientode las pestañas en el largo y espesura, y oscurecimiento de las pestañas (en 22% de los pacientes después 3 meses, y 36% después 6 meses de tratamiento), y, oscurecimiento de los párpados (en 1 a <3% de los pacientes después 3 meses y 3 a 10% de los pacientes después6 meses de tratamiento). También fue relatado oscurecimiento del íris en 0,2% de los pacientes tratados durante 3 meses y en 1,1% de los pacientes tratados durante 6 meses. Algunas de esas alteraciones pueden ser permanentes. Pacientes que deben recibir el tratamientode apenas uno de los ojos, deben ser informados a respecto de esas reacciones. PrPrPrPrPrecaucionesecaucionesecaucionesecaucionesecauciones LUMIGAN®®®®® (bimatoprost) no fue estudiado en pacientes con insuficiencia renal o hepática y por lo tanto debe ser utilizado con cautela en tales pacientes.Las lentes de contacto debenser retiradas antes de la instilación de LUMIGAN®®®®® (bimatoprost) y pueden ser recolocadas 15 minutos después. Los pacientes deben ser advertidos de que el producto contiene cloruro de benzalconio, que es absorvido por las lentes hidrofílicas.Si más que un medicamentode uso tópico ocular estuviera siendo utilizado, se debe respetar un intervalo de por lo menos 5 minutos entre las aplicaciones.No está previsto que LUMIGAN®®®®® (bimatoprost) presente influencia sobre la capacidad del paciente conducir vehículos u operar máquinas, sin embargo,así como para cualquier colírio, puede ocurrir visión borrosa transitoria después de la instilación; en estos casos el paciente debe aguardar que la visión se normalice antes de conducir u operar máquinas. Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Considerando que las concentracionescirculantes sistemicas de bimatoprost son extremadamente bajas después múltiplas instilaciones oculares (menos de 0,2 ng/ml), y, que hay varias vías encimáticas envueltas en la biotransformación de bimatoprost, no son previstas interacciones medicamentosas en humanos.No son conocidas incompatibilidades. R R R R Reacciones adversas.eacciones adversas.eacciones adversas.eacciones adversas.eacciones adversas. LUMIGAN®®®®® (bimatoprost) es bien tolerado, pudiendo causar eventos adversos oculares leves a moderados y no graves.Eventos adversos ocurriendo en 10-40% de los pacientes que recibieron doses únicas diarias, durante3 meses, en orden decreciente de incidencia fueron: hiperenia conjuntival, crecimento de las pestañas y prurito ocular.Eventos adversos ocurriendo en aproximadamente 3 a < 10% de los pacientes, en orden decreciente de incidencia, incluyeron: sequedad ocular, ardor ocular,sensación de cuerpo estraño en el ojo, dolor ocular y distúrbios de la visión.Eventos adversos ocurriendo en 1 a <3% de los pacientes fueron: cefalea, eritema de los párpados, pigmentación de la piel periocular, irritación ocular, secreción ocular, astenopia, conjuntivitis alérgica,lagrimeo, y fotofobia.En menos de 1% de los pacientes fueron relatadas: inflamación intra-ocular, mencionada como iritis y pigmentación del íris, ceratitis puntiforme superficial, alteración de las pruebas de función hepática e infecciones (principalmente resfriados e infeccionesde las vías respiratorias).Con tratamientos de 6 meses de duración fueron observados, además de los eventos adversos relatados más arriba, en aproximadamente 1 a <3% de los pacientes, edema conjuntival, blefaritis y astenia. En tratamientos de asociación con betabloqueador,durante 6 meses, además de los eventos de más arriba, fueron observados en aproximadamente 1 a <3% de los pacientes, erosión de la córnea, y empeoramiento de la acuidad visual. En menos de 1% de los pacientes, blefarospasmo, depresión, retracción de los párpados,hemorragia retiniana y vértigo.La frecuencia y gravedad de los eventos adversos fueron relacionados a la dosis, y, en general, ocurrieron cuando la dosis recomendada no fue seguida.Posología y Administración.Posología y Administración.Posología y Administración.Posología y Administración.Posología y Administración.Aplicar una gota en el ojo afectado, una vez al día, a la noche.La dosis no debe exceder a una dosis única diaria, pues fue demostrado que la administración más frecuente puede disminuir el efecto hipotensor sobre la hipertensión ocular.LUMIGAN®®®®® (bimatoprost) puede ser administrado concomitantemente con otros productos oftálmicostópicos para reducir la hipertensión intra-ocular, respetándose el intervalo de por lo menos 5 minutos entre la administración de los medicamentos. VENTA BAJO PRESCRIPCIÓN MÉDICA.“ESTE PRODUCTO ES UM MEDICAMENTO NUEVO AUNQUE LAS INVESTIGACIONES HAYANINDICADO EFICACIA Y SEGURIDAD, CUANDO CORRECTAMENTE INDICADO, PUEDEN SURGIR REACCIONES ADVERSAS NO PREVISTAS, AÚN NO DESCRIPTAS O CONOCIDAS, EN CASO DE SOSPECHA DE REACCIÓN ADVERSA, EL MÉDICO RESPONSABLE DEBE SER NOTIFICADO.
vs. timolol 4 vs. latanoprost6
Porcentaje de Pacientes quealcanzaron la PIO-Objetivo ≤≤≤≤≤14 21% 9% 17% 2% 19% 9%
Porcentaje de Pacientes quealcanzaron la PIO-Objetivo ≤≤≤≤≤15 31% 16% 24% 9% 29% 14%
dorzolamida/ timolol 5vs.
®®®
Lumigan® alcanza la PIO-objetivo de 14/15 mmHg en un mayor númerode pacientes:
Investigadores de diversos estudios, (AGIS, Shirakashi, Shields)han comprobado que alcanzar y mantener la PIO entre 14 y 15 mmHgreduce la progresión de pérdida del campo visual1,2,3.

VISIONPAN-AMERICA 1: :
Septiembre 2005
provecho esta oportunidad editorial para hacer algunas consideraciones
sobre los próximos eventos a suceder dentro de la organización de
Asociación Panamericana de Oftalmología.
Del 31 de Julio al 3 de agosto del presente año se llevará a cabo, en
la ciudad de Chihuahua , México, el Curso Panamericano que organiza la
Sociedad Mexicana de Oftalmología. Este es ya un curso tradicional, que
en forma bienal se lleva a cabo en la República Mexicana y que la
sociedad de ese país honra, en memoria del Dr. Feliciano Palomino Dena,
ex presidente de la Asociación Panamericana de Oftalmología, con el
nombre del Panamericanismo.
Los días 2 y 3 de septiembre la Asociación Panamericana de Oftalmo-
logía organiza un curso panamericano regional en la ciudad de Tucumán,
Argentina. Este curso organizado por el Dr. Arturo Maldonado Bas y la
Doctora Bateman, esta dirigido al oftalmólogo en práctica general y
abarca la actualidad en distintos
aspectos de nuestra práctica profe-
sional. El Dr. Maldonado Bas, en cum-
plimiento con los objetivos de estos
cursos regionales, ha convocado a los
oftalmólogos de la región y esperamos
una nutrida asistencia y el éxito de las
finalidades del curso.
Como es tradicional, en Octubre
de este año, la Asociación Paname-
ricana de Oftalmología tendrá su reu-
nión anual en Chicago, durante las
actividades de la Academia Americana de Oftalmología. Les invitamos
a todos a que asistan a este evento académico y que compartan con
nosotros sus experiencias e inquietudes.
Del 19 al 12 de febrero, en la Ciudad de São Paulo, Brasil, se llevará
a cabo el Congreso Mundial de Oftalmología. A invitación del Interna-
cional Council de Oftalmología, la Asociación Panamericana de Oftal-
mología, decidió reunir sus esfuerzos y sumarse, en forma de congreso
extraordinario, al Congreso Mundial. De esta manera, en el año 2006,
sucederá, simultáneamente el Congreso Panamericano de Oftalmología.
Su presidente, el Dr. Newton Kara, ha sumado sus esfuerzos a los que
empeña el Dr. Rubens Belfort, Presidente del Congreso Mundial, para
que este evento tenga una asistencia Panamericana importante y dar a
conocer a nuestra Asociación al resto de la oftalmología mundial.
Finalmente del 23 al 25 de abril del 2006, se llevará a cabo en Lima,
Perú. Un curso dirigido a los encargados de las residencias de oftal-
mología de la región norte del cono sur. Este curso es el producto del
esfuerzo conjunto de la Asociación Panamericana de Oftalmología ( PAAO y
PAOF y PACUPO ), del Internacional Council of Ophthalmology y de su
Fundación, de la AUPO,( Association for University Proffesors in
Ophthalmology ) y del generoso patrocinio de Laboratorios ALCON. El
curso esta dirigido a enseñar a enseñar y su foro tratará sobre los
principales problemas que enfrentan las residencias médicas y de cómo
resolverlos. Bajo la Organización regional del Dr. Juan Verdaguer y del
coordinador del Curso el Dr. Antonio Roca, se han ya comprometido la
asistencia todos los directores de los cursos de residencia de la Repú-
blica del Perú y Bolivia y se ha convocado a todos aquellos interesados
en este tema.
Esperamos que estos esfuerzos nos conduzcan a enseñar mejor y en
mejores condiciones, la oftalmología a nuestros residentes.
De esta manera la Oftalmología Panamericana crece y se consolida.
would like to take this editorial opportunity to consider some of the
events happening soon within the Pan-American Association of
Ophthalmology.
From July 31 to August 3 of this year, the Curso Panamericano
organized by the Mexican Society of Ophthalmology will take place in
Chihuahua, Mexico.
This is a traditional course that occurs every two years in the Mexican
Republic and that the people of this country honor in memory of Dr. Feli-
ciano Palomino Dena, ex-president of the Pan-American Association of
Ophthalmology.
On September 2nd and 3rd, the Pan-American Association of
Ophthalmology is organizing a regional Pan-American course in Tucumán,
Argentina. This course, organized by Dr. Arturo Maldonado Bas and Dr.
Bateman, is focused on ophthalmology in general practice and includes
current issues in our professional practice. Dr. Maldonado Bas, in accor-
dance with the objectives of these regional courses, has summoned the
ophthalmologists of the region, and we expect a considerable attendance
and success in meeting the goals of the course.
As is traditional, in October of this year, the Pan-American Association
of Ophthalmology will have its annual meeting in Chicago, during the
events of the American Academy of Ophthalmology. We invite all of you
to attend this academic event and to share with us your experiences and
concerns.
From the 12th to the 19th of February in São Paulo, Brazil, the World
Ophthalmology Congress (W.O.C) will take place. At the invitation of the
International Council of Ophthalmology, the Pan-American Association of
Ophthalmology decided to join forces and add an additional congress as
the W.O.C. In this way, in the year 2006, the Pan-American Congress of
Ophthalmology will occur simultaneously. Its president, Dr. Newton Kara,
has joined forces with Dr. Rubens Belfort, president of the World Con-
gress, in order to promote Pan-American attendance and to introduce
our Association to the rest of the world.
Finally, from the 23rd to the 25th of April 2006, a couse geared to those
in charge of ophthalmology residencies of the northern region of the
southern cone will take place in Lima, Peru. This course is the product of
the joint efforts of the Pan-American Association of Ophthalmology (PAAO
and PAOF and PACUPO), the International Council of Ophthalmology and
its foundation, and the Association for Univerisity Professors of Ophthal-
mology (AUPO), with the generous sponsorship of Alcon Laboratories.
This course is oriented to teaching how to teach, and its focus will be the
pricipal problems facing medical residencies and how to solve them.
Under the regional Organization of Dr. Juan Verdaguer and Dr. Antonio
Roca, coordinator of the Course, all of the residency directors of the
Republic of Peru and Bolivia have already committed to attend and have
summoned everyone interested in this area.
We hope that these efforts lead to better teaching and better conditions
for our ophthalmology residents.
In this way, Pan-American Ophthalmology will grow and strengthen.
MENSAJE DEL PRESIDENTE
A I
Enrique GrauePresidente de la Asociación Panamericanade Oftalmología.
PRESIDENT’S MESSAGE

Septiembre 2005
VISIONPAN-AMERICA2: :
proveito esta oportunidade editorial para fazer algumas considerações
sobre os próximos eventos dentro da organização da Associação Pan-
Americana de Oftalmologia.
De 31 de Julho a 3 de Agosto deste ano, se realizará, na cidade de
Chihuahua, no México, o Curso Panamericano organizado pela Sociedade
Mexicana de Oftalmologia. Este já é um curso tradicional, que se realiza
na República Mexicana bienalmente e que a sociedade deste país honra,
em memória do Dr. Feliciano Palomino Dena, ex-presidente da Asociação
Pan-Americana de Oftalmologia, com o nome de Panamericano.
Nos dias 2 e 3 de setembro a Associação Pan-Americana de Oftalmologia
organiza um curso panamericano regional na cidade de Tucumán, na
Argentina. Este curso, organizado pelo Dr. Arturo Maldonado Bas e pela
Dra. Bateman, é dirigido ao oftalmologista geral e abordará a atualidade
dos distintos aspectos de nossa prática profissional. O Dr. Maldonado Bas,
cumprindo os objetivos destes cursos regionais, convocou os oftalmolo-
gistas da região e esperamos uma expressiva participação e o êxito na
realização das finalidades do curso.
Como é tradicional, em Outubro deste ano, a Associação Pan-
Americana de Oftalmologia terá a sua reunião em Chicago, durante as
atividades da Academia Americana de Oftalmologia. Convidamos todos a
comparecerem a este evento acadêmico e a compartilharem conosco as
suas experiências e inquietudes.
De 19 a 12 de Fevereiro, na cidade de São Paulo, no Brasil, se
realizará o Congreso Mundial de Oftalmología. A convite do Internacional
Council of Ophthalmology, a Associação Pan-Americana de Oftalmologia
decidiu-se a reunir esforços e somar-se, na forma de congresso
extraordinário, ao Congresso Mundial. Desta maneira, no ano de 2006,
acontecerá simultaneamente o Congresso Panamericano de Oftalmologia.
O seu Presidente, o Dr. Newton Kara, somou seus esforços aos
empenhados pelo Dr. Rubens Belfort, Presidente do Congreso Mundial,
para que este evento tenha uma participação Panamericana importante e
mostre a nossa Associação aos outros participantes da oftalmologia
mundial.
Finalmente, de 23 a 25 de abril de 2006, se realizará em Lima, no Perú.
Um curso dirigido aos encarregados pelas residências em Oftalmologia na
região norte do cono sul. Este curso é fruto de um esforço conjunto da
Associação Pan-Americana de Oftalmologia (PAAO, PAOF e PACUPO), do
Internacional Council of Ophthalmology e de sua Fundación, da AUPO,
(Association for University Professors of Ophthalmology) e do generoso
patrocínio dos Laboratorios ALCON. O curso visa ensinar a ensinar e o seu
foro tratará sobre os principais problemas que enfrentam as residências
médicas e como resolvê-los. Sob a organização regional do Dr. Juan
Verdaguer e do coordenador do curso, o Dr. Antonio Roca, já se compro-
meteram a participar todos os diretores de cursos de residência da República
do Perú e Bolivia e se convocou todos os interessados neste tema.
Esperamos que estes esforços nos conduzam a ensinar melhor, e em
melhores condições, a oftalmologia a nossos residentes.
Desta maneira a Oftalmología Panamericana cresce e se consolida.
Atentamente,
Sincerely,
Atenciosamente,
Enrique GrauePresidente de la Asociación Panamericana de Oftalmología.President Pan-American Association of Ophthalmology.Presidente Associação Pan-Americana de Oftalmologia.
UMA MENSAGEM DO PRESIDENTE
A
Current Treatment Options for
Neovascular Age-RelatedMacular DegenerationSSuussaannnnaa SS.. PPaarrkk,, MMDD PPhhDDAssociate Professor of Clinical Ophthalmology.Retina Service.Department of Ophthalmology & Vision ScienceUniversity of California, Davis4860 Y Street, Suite 2400, Sacramento, CA 95817Tel. (916) 734-6544FAX. (916) 734-6197E-mail: [email protected]
ge-related macular degeneration (AMD) is the leading cause of
irreversible vision loss in the elderly population in the United
States. Currently, 1.75 million Americans have vision loss from advanced
AMD in at least one eye.1 Most cases of severe vision loss occur from
complications of neovascular or "wet" AMD which occur in 15% of
patients with AMD.2 Several new treatments for neovascular AMD have
become available recently to reduce the risk of further vision loss and
potentially improve vision. This article is an overview of the current
treatments options for neovascular AMD.
Macular Laser Photocoagulation
Macular laser photocoagulation is the treatment of choice among
patients with wet AMD with a well-defined, extrafoveal choroidal neovas-
cular membrane, i.e. lesions greater than 200 microns from the fovea
(Figure 1). The goal of thermal laser photocoagulation is to directly
coagulate the neovascular membrane and prevent it from bleeding or
growing into the fovea. The result is a non-selective thermal damage to
the neovascular tissue and the overlying retina which can result in a
scotoma corresponding to the area treated. The Macular Photocoagu-
lation Study (MPS) showed that focal laser treatment of a well-defined,
extrafoveal choroidal neovascular membrane decreased the risk of
severe vision loss when compared to untreated eyes.3 However, 54% of
treated patients had loss of vision during the 5 year follow-up period from
recurrent neovascular AMD which eventually involved the fovea.
A similar treatment benefit was noted by the MPS group for patients
with well-defined, juxtafoveal neovascular AMD, i.e. lesion extending
within 200 microns from the fovea but not involving the fovea.4 However,
32% of treated eyes had persistent neovascularization during the first 6
weeks and 45% had recurrent neovascularization during the 5 year
follow-up period.
Among patients with subfoveal choroidal neovascular membrane from
AMD, laser photocoagulation resulted in an increase in risk of severe
vision loss at 3 months follow-up although a small treatment benefit was
noted at 24 months following treatment.5 Most patients with visual acuity
of 20/100 or better at baseline lost vision as a result of the treatment.
Based on these observations, macular laser photocoagulation is not
recommended in patients with a subfoveal choroidal neovascular
membrane if the visual acuity is 20/200 or better (Figure 2). Similarly, in
patients with juxtafoveal neovascular AMD where the lesion is too close
to the fovea to allow complete treatment without affecting the fovea, an
alternative treatment should be considered if the visual acuity is 20/200
or better.
A
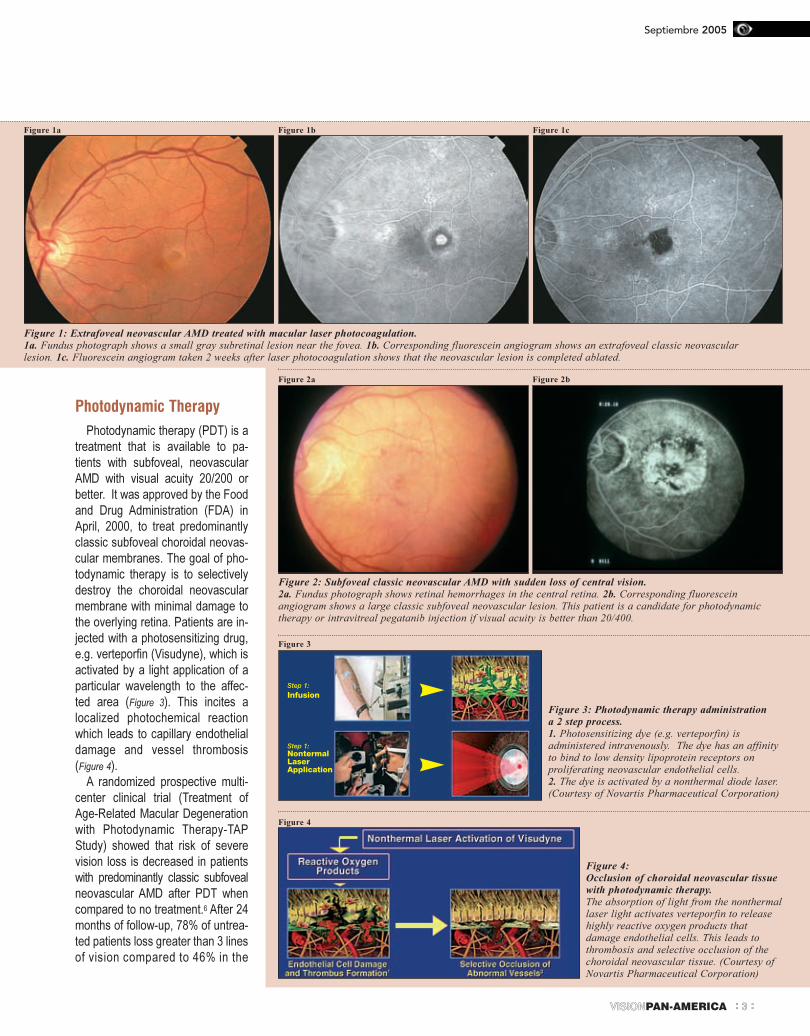
Photodynamic Therapy
Photodynamic therapy (PDT) is a
treatment that is available to pa-
tients with subfoveal, neovascular
AMD with visual acuity 20/200 or
better. It was approved by the Food
and Drug Administration (FDA) in
April, 2000, to treat predominantly
classic subfoveal choroidal neovas-
cular membranes. The goal of pho-
todynamic therapy is to selectively
destroy the choroidal neovascular
membrane with minimal damage to
the overlying retina. Patients are in-
jected with a photosensitizing drug,
e.g. verteporfin (Visudyne), which is
activated by a light application of a
particular wavelength to the affec-
ted area (Figure 3). This incites a
localized photochemical reaction
which leads to capillary endothelial
damage and vessel thrombosis
(Figure 4).
A randomized prospective multi-
center clinical trial (Treatment of
Age-Related Macular Degeneration
with Photodynamic Therapy-TAP
Study) showed that risk of severe
vision loss is decreased in patients
with predominantly classic subfoveal
neovascular AMD after PDT when
compared to no treatment.6 After 24
months of follow-up, 78% of untrea-
ted patients loss greater than 3 lines
of vision compared to 46% in the
VISIONPAN-AMERICA 3: :
Septiembre 2005
Figure 1: Extrafoveal neovascular AMD treated with macular laser photocoagulation.
1a. Fundus photograph shows a small gray subretinal lesion near the fovea. 1b. Corresponding fluorescein angiogram shows an extrafoveal classic neovascularlesion. 1c. Fluorescein angiogram taken 2 weeks after laser photocoagulation shows that the neovascular lesion is completed ablated.
Figure 1a Figure 1b Figure 1c
Figure 2a
Figure 3
Figure 4
Step 1:
Infusion
Step 1:NontermalLaserApplication
Figure 2b
Figure 2: Subfoveal classic neovascular AMD with sudden loss of central vision.
2a. Fundus photograph shows retinal hemorrhages in the central retina. 2b. Corresponding fluoresceinangiogram shows a large classic subfoveal neovascular lesion. This patient is a candidate for photodynamictherapy or intravitreal pegatanib injection if visual acuity is better than 20/400.
Figure 3: Photodynamic therapy administration
a 2 step process.
1. Photosensitizing dye (e.g. verteporfin) isadministered intravenously. The dye has an affinityto bind to low density lipoprotein receptors onproliferating neovascular endothelial cells.2. The dye is activated by a nonthermal diode laser.(Courtesy of Novartis Pharmaceutical Corporation)
Figure 4:
Occlusion of choroidal neovascular tissue
with photodynamic therapy.
The absorption of light from the nonthermallaser light activates verteporfin to releasehighly reactive oxygen products thatdamage endothelial cells. This leads tothrombosis and selective occlusion of thechoroidal neovascular tissue. (Courtesy ofNovartis Pharmaceutical Corporation)
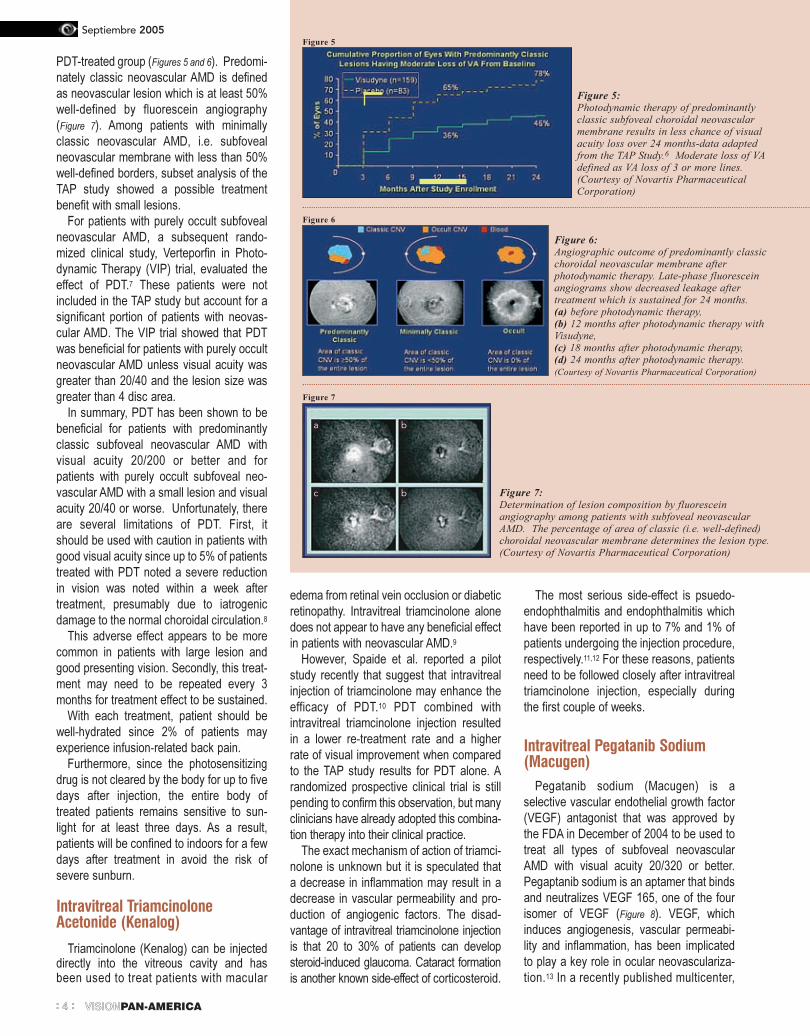
PDT-treated group (Figures 5 and 6). Predomi-
nately classic neovascular AMD is defined
as neovascular lesion which is at least 50%
well-defined by fluorescein angiography
(Figure 7). Among patients with minimally
classic neovascular AMD, i.e. subfoveal
neovascular membrane with less than 50%
well-defined borders, subset analysis of the
TAP study showed a possible treatment
benefit with small lesions.
For patients with purely occult subfoveal
neovascular AMD, a subsequent rando-
mized clinical study, Verteporfin in Photo-
dynamic Therapy (VIP) trial, evaluated the
effect of PDT.7 These patients were not
included in the TAP study but account for a
significant portion of patients with neovas-
cular AMD. The VIP trial showed that PDT
was beneficial for patients with purely occult
neovascular AMD unless visual acuity was
greater than 20/40 and the lesion size was
greater than 4 disc area.
In summary, PDT has been shown to be
beneficial for patients with predominantly
classic subfoveal neovascular AMD with
visual acuity 20/200 or better and for
patients with purely occult subfoveal neo-
vascular AMD with a small lesion and visual
acuity 20/40 or worse. Unfortunately, there
are several limitations of PDT. First, it
should be used with caution in patients with
good visual acuity since up to 5% of patients
treated with PDT noted a severe reduction
in vision was noted within a week after
treatment, presumably due to iatrogenic
damage to the normal choroidal circulation.8
This adverse effect appears to be more
common in patients with large lesion and
good presenting vision. Secondly, this treat-
ment may need to be repeated every 3
months for treatment effect to be sustained.
With each treatment, patient should be
well-hydrated since 2% of patients may
experience infusion-related back pain.
Furthermore, since the photosensitizing
drug is not cleared by the body for up to five
days after injection, the entire body of
treated patients remains sensitive to sun-
light for at least three days. As a result,
patients will be confined to indoors for a few
days after treatment in avoid the risk of
severe sunburn.
Intravitreal TriamcinoloneAcetonide (Kenalog)
Triamcinolone (Kenalog) can be injecteddirectly into the vitreous cavity and hasbeen used to treat patients with macular
edema from retinal vein occlusion or diabetic
retinopathy. Intravitreal triamcinolone alone
does not appear to have any beneficial effect
in patients with neovascular AMD.9
However, Spaide et al. reported a pilot
study recently that suggest that intravitreal
injection of triamcinolone may enhance the
efficacy of PDT.10 PDT combined with
intravitreal triamcinolone injection resulted
in a lower re-treatment rate and a higher
rate of visual improvement when compared
to the TAP study results for PDT alone. A
randomized prospective clinical trial is still
pending to confirm this observation, but many
clinicians have already adopted this combina-
tion therapy into their clinical practice.
The exact mechanism of action of triamci-
nolone is unknown but it is speculated that
a decrease in inflammation may result in a
decrease in vascular permeability and pro-
duction of angiogenic factors. The disad-
vantage of intravitreal triamcinolone injection
is that 20 to 30% of patients can develop
steroid-induced glaucoma. Cataract formation
is another known side-effect of corticosteroid.
The most serious side-effect is psuedo-
endophthalmitis and endophthalmitis which
have been reported in up to 7% and 1% of
patients undergoing the injection procedure,
respectively.11,12 For these reasons, patients
need to be followed closely after intravitreal
triamcinolone injection, especially during
the first couple of weeks.
Intravitreal Pegatanib Sodium(Macugen)
Pegatanib sodium (Macugen) is a
selective vascular endothelial growth factor
(VEGF) antagonist that was approved by
the FDA in December of 2004 to be used to
treat all types of subfoveal neovascular
AMD with visual acuity 20/320 or better.
Pegaptanib sodium is an aptamer that binds
and neutralizes VEGF 165, one of the four
isomer of VEGF (Figure 8). VEGF, which
induces angiogenesis, vascular permeabi-
lity and inflammation, has been implicated
to play a key role in ocular neovasculariza-
tion.13 In a recently published multicenter,
Septiembre 2005
VISIONPAN-AMERICA4: :
Figure 5
Figure 5:Photodynamic therapy of predominantlyclassic subfoveal choroidal neovascularmembrane results in less chance of visualacuity loss over 24 months-data adaptedfrom the TAP Study.6 Moderate loss of VAdefined as VA loss of 3 or more lines.(Courtesy of Novartis PharmaceuticalCorporation)
Figure 6
Figure 6:Angiographic outcome of predominantly classicchoroidal neovascular membrane afterphotodynamic therapy. Late-phase fluoresceinangiograms show decreased leakage aftertreatment which is sustained for 24 months.(a) before photodynamic therapy,(b) 12 months after photodynamic therapy withVisudyne,(c) 18 months after photodynamic therapy,(d) 24 months after photodynamic therapy.(Courtesy of Novartis Pharmaceutical Corporation)
Figure 7
Figure 7:Determination of lesion composition by fluoresceinangiography among patients with subfoveal neovascularAMD. The percentage of area of classic (i.e. well-defined)choroidal neovascular membrane determines the lesion type.(Courtesy of Novartis Pharmaceutical Corporation)
a b
bc

randomized prospective clinical study,
intravitreal injection of pegatanib sodium
resulted in a decrease in the rate of vision
loss from subfoveal neovascular AMD,
regardless of lesion type, when compared
to sham treatment.14 It was administered
every six weeks for one year but treatment
benefit was noted as early as 3 month, i.e.
after 2 injections.
It is unclear at the present time whether
this treatment is superior to photodynamic
therapy. In fact, 25% of the patients in the
study were treated concurrently with photo-
dynamic therapy. Unlike triamcinolone,
there is no risk of steroid-glaucoma. The
risk of endophthalmitis and cataract forma-
tion from the trauma of repeat injection re-
mains a potential limitation of this therapy.
Vitreous Surgery for NeovascularAMD.
Two surgical approaches to treating neo-
vascular AMD have been explored in the
last twelve years. These treatments have
become less popular in recent years with
the advent of PDT and anti-VEGF therapy.
Surgical removal of the subfoveal cho-
roidal neovascular tissue is technically
possible and can result in significant visual
improvement in some patients.15
Unfortunately, most patients experience
progressive visual decline despite surgery.
Surgical translocation of the macula such
that the macula is moved to a new area with
a healthier underlying retinal pigment epi-
thelium has also been tried in a couple of
clinical centers.16 Significant improvement in
vision has been reported in some of these
patients. The limitation of this latter surgery
is the risk of retinal detachment and diplopia
following surgery. Whether these surgical
treatments have a better long-term visual
outcome than PDT or anti-VEGF therapy
is unknown.
SUMMARY
The treatment option for neovascular
AMD is expanding with the advent of new
pharmacologic agents and photodynamic
therapy. Several other pharmacologic a-
gents are currently being investigated as
possible new treatments. As newer agents
become available, the treatment regimen
for neovascular AMD will become more
complex. At the current time, it is unclear
which treatment alone or in combination will
prove to be most beneficial for neovascular
AMD.
Figure 8
Figure 8:VEGF cascade leading toneovascular AMD is inhibited byPegatanib Sodium. (Courtesy ofNovartis PharmaceuticalCorporation)
VISIONPAN-AMERICA 5: :
Septiembre 2005
"This work was supported in part by a generous grant from Research to Prevent Blindness, Inc. New York, NY"
1. Friedman DS, O'Colmain BJ, Munoz B, et al, for the Eye DiseasesPrevalence Research Group. Prevalence of age-related macular degene-ration in the United States. Arch Ophthalmol. 2004; 122: 564-572.2.Macular Photocoagulation Study Group. Risk factor for choroidal neo-vascularization in the second eye of patients with juxtafoveal or subfovealchoroidal neovascularization secondary to age-related macular degene-ration. Arch Ophthalmol. 1997; 115: 741-747.3.Macular Photocoagulation Study Group. Argon laser photocoagulationfor neovascular maculopathy. Five-year results from randomized clinicaltrials. Arch Ophthalmol. 1991; 109: 1109-1114.4.Macular Photocoagulation Study Group. Laser photocoagulation for jux-tafoveal choroidal neovascularization: five-year results from randomizedclinical trials. Arch Ophthalmol. 1994; 112: 500-509.5.Macular Photocoagulation Study Group. Laser photocoagulation ofsubfoveal neovascular lesions in age-related macular degeneration. Resultsof a randomized clinical trial. Arch Ophthamol. 1991; 109: 1220-1231.6.Treatment of Age-Related Macular Degeneration with PhotodynamicTherapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidalneovascularization in age-related macular degeneration with verteporfin:two-year results of 2 randomized clinical trials-TAP report 2. ArchOphthalmol. 2001; 119: 198-207.7.Blinder KJ, Bradley S, Bressler NM, et al, for the Treatment of Age-Related Macular Degeneration With Photodynamic Therapy (TAP) andVerteporfin in Photodynamic Therapy (VIP) Study Groups. Effect of lesionsize, visual acuity, and lesion composition on visual acuity change with andwithout verteporfin therapy for choroidal neovascularization secondary toage-related macular degeneration: TAP and VIP report no. 1. Am JOphthamol. 2003; 136: 407-418.8.Arnold JJ, Blinder KJ, Bressler NM, et al, for the Treatment of Age-Related Macular Degeneration With Photodynamic Therapy (TAP) Study
Group. Acute severe visual acuity decrease after photodynamic therapy withverteporfin: case reports from randomized clinical trials-TAP and VIPreport no. 3. Am J Ophthalmol. 2004; 137: 683-696.9.Gillies MC, Simpson JM, Luo W, et al. A randomized clinical trial of asingle dose of intravitreal triamcinolone acetonide for neovascular age-related macular degeneration: one-year results. Arch Ophthalmol. 2003;121: 667-673.10. Spaide RF, Sorenson J, Maranan L. Combined photodynamic therapy withverteporfin and intravitreal triamcinolone acetonide for choroidal neovas-cularization. Ophthalmology. 2003; 110: 1517-1525.11. Roth DB, Chieh J, Spirn MJ, Green SN, et al. Noninfectious endophthal-mitis associated with intravitreal triamcinolone injection. Arch Ophthalmol2003; 121: 1279-1282.12. Moshfeghi DM, Kaiser PK, Scott IU, et al. Acute endophthamitisfollowing intravitreal triamcinolone acetonide injection. Am J Ophthalmol.2003; 136: 791-796.13. Krzystolik MG, Afshari MA, Adamis AP, et al. Prevention of experi-mental choroidal neovascularization with intravitreal antivascularendothelial growth factor antibody fragment. Arch Ophthalmol. 2002; 120:338-346.14. Gragoudas ES, Adamis AP, Cunningham ET, Jr, et al, for the VEGFInhibition Study in Ocular Neovascularization Clinical Trial Group. Pe-gaptanib for neovascular age-related macular degeneration. N Engl J Med.2004; 351: 2805-2816.15. Thomas MA, Grand MG, Williams DF, et al. Surgical management ofsubfoveal choroidal neovascularization. Ophthalmology. 1992; 99: 952-968.16. American Academy of Ophthalmology. Macular translocation. Ophthal-mology. 2000; 107: 1015-1018.
REFERENCES:

Septiembre 2005
VISIONPAN-AMERICA6: :
Intraocular Lens Power Calculation for Cataract Extraction
after Corneal Refractive SurgeryVVaahhiidd FFeeiizz,, MMDDAssistant ProfessorDepartment of Ophthalmology & Vision ScienceUnviersity of California, Davis4860 Y Street Suite 2400, Sacramento, CA 95817Tel: 916-734-6603Fax: 916-734-6992
INTRODUCTIONAs corneal refractive surgery has evolved from incisional
techniques such as radial keratotomy (RK) to more accurate and
predictable methods of excimer laser keratectomy, these procedures
have gained wide popularity amongst patients and ophthalmic
surgeons.1 Alongside this evolution, the early post-refractive surgery
patients have become older and are beginning to enter the age at
which development of visually significant cataracts occurs. This, in
turn, has increased awareness of the shortcomings of standard
methods of intraocular lens (IOL) power determination.
Early experience with cataract removal and lens implantation in
post-keratorefractive surgery eyes resulted in highly unexpected
refractive surprises. IOL implantation in post-RK eyes and post-
myopic excimer eyes has consistently shown a trend toward
underestimation of IOL power and hyperopic refractive surprises
after cataract surgery.2-4 Data from cataract surgery after corneal
hyperopic refractive procedures are limited but there have been
reports of a possible trend toward overestimation of IOL power and
myopic surprises after cataract surgery.5
While it is not entirely clear what the exact source of these errors is
or whether there is one cause or multiple reasons, most physicians
agree that the majority of these miscalculations can be contributed
to inaccurate measurement of the central corneal power. In other
words, the central corneal power as measured by standard
keratometry or topography, overestimates the true corneal power,
which in turn results in intraocular lens power underestimation and
subsequent hyperopia.6
Since standard keratometry and topography are routinely used
with excellent results in eyes without prior refractive surgery, these
clinical observations after refractive surgery have been somewhat
puzzling. However, through the work of a number of clinical
researchers, analysis of individual steps that are normally
incorporated into corneal power measurements has resulted in a
better understanding of these erroneous measurements. These
findings in turn have resulted in recommendations for modification of
standard IOL power calculations to improve outcomes in post
refractive surgery patients.
The following sections of this article include a brief review of these
error sources and ways to compensate for them.
Sources of Error
Standard keratometry or topography does
not directly gauge central corneal power but
rather a radius of curvature in the para-
central 2-3 mm of the cornea.7 This is
accomplished by projecting mires to the
para-central cornea form several light
sources. The radius of curvature, in millime-
ters, is then determined by the measure-
ment of the distance between the reflected
images from the para-central cornea. In
doing so, a basic supposition is made that
the power of the para-central cornea is a
close approximation of the central corneal
refractive power. Furthermore, in order for
the measurements to be clinically useful,
they have to be converted to optical power
in diopters, which is accomplished by
utilizing an optical refractive index. The re-
fractive index is assumed to be constant for
all corneas with a value of 1.3375.6,7
While all of these postulations are
clinically valid in normal virgin corneas, they
may not be applicable to corneas after
refractive surgery. In post-RK eyes, with
small optical zones of 2-3 mm, the central
cornea is significantly flatter than the para-
central cornea and the actual measured
para-central power overestimates the cen-
tral corneal power.
The situation is somewhat different in
eyes after myopic LASIK or PRK where
large optical zones are routinely used. In
these cases, while the para-central radius of
curvature is expected to be a fairly good
approximation of the central radius of
curvature, the effective refractive index of
the cornea has changed.6,8 To make matters
more complicated, the change in effective
refractive index is also variable depending
on the amount of tissue ablated.9
Other factors may also contribute to IOL
power miscalculations. Among these is the
relationship between the anterior chamber
depth and the corneal refractive power,
which is used by most formulas (e.g. SRK-
T, Holladay) to predict an effective lens
position and can have a profound effect on
the final refraction after cataract surgery.
After corneal refractive surgery, this re-
lationship is altered but the formulas have not
been modified to compensate for this change.10
Approaches to Decrease IOLPower Errors
While there are a number of methods
proposed by different authors with the aim
of decreasing IOL power errors, these all fall
within two main categories. Those that
require some knowledge of pre-refractive
surgery corneal power and those that can
be used independently of values prior to
refractive surgery.
The first group includes clinical history
method, double K method, and nomogram
adjustment.10-12 While the use of these
methods has been shown to improve accu-
racy to varying degrees, the major shortco-
ming is the reliance on pre-refractive
surgery values that may not be available to
the ophthalmologist who is performing the
cataract extraction, usually years later.
The second group includes the hard
contact lens method and use of newer
topography systems such as OrbscanTM
(Baush & Lomb) to improve accuracy of
central corneal power measurements. Each of the various methods is briefly
described and discussed below.
VISIONPAN-AMERICA 7: :
Septiembre 2005
Clinical History Method
In this method, the change in spherical
equivalent induced by refractive surgery is
determined. In cases of eyes after myopic
refractive surgery, this value is subtracted
from average corneal power prior to refrac-
tive surgery. This calculated corneal power,
generally lower than the measured post-
refractive surgery values, is then used in
conjunction with axial length to determine
the IOL power.11
While not tested in large clinical trials,
several small case series have shown
improvement in refractive outcomes of
cataract extraction after refractive surgery
with this approach.13,14 It does, however,
require knowledge of pre-refractive surgery
values including refraction and keratometry,
that may not always be available. In addi-
tion, while the original authors recommen-
ded using the change in refraction at the
corneal plane, recent studies have shown
that refractive change at the spectacle
plane further improves outcomes.15
This method has been utilized for eyes
after RK, as well as eyes after LASIK and
PRK with varying degrees of success.13, 14
Double K Method
Aramberri10 proposed a modified formula
where pre-refractive surgery Ks are used to
estimate effective lens position (ELP) and
post-refractive surgery Ks are used to
determine IOL power taking into account the
ELP. In addition, the author recommends
further modifying the measured keratometry
values using clinical history method as
described above. It is therefore not a truly
independent method but a further modifica-
tion of the clinical history method. No large
case studies of outcomes using this method
have been published.
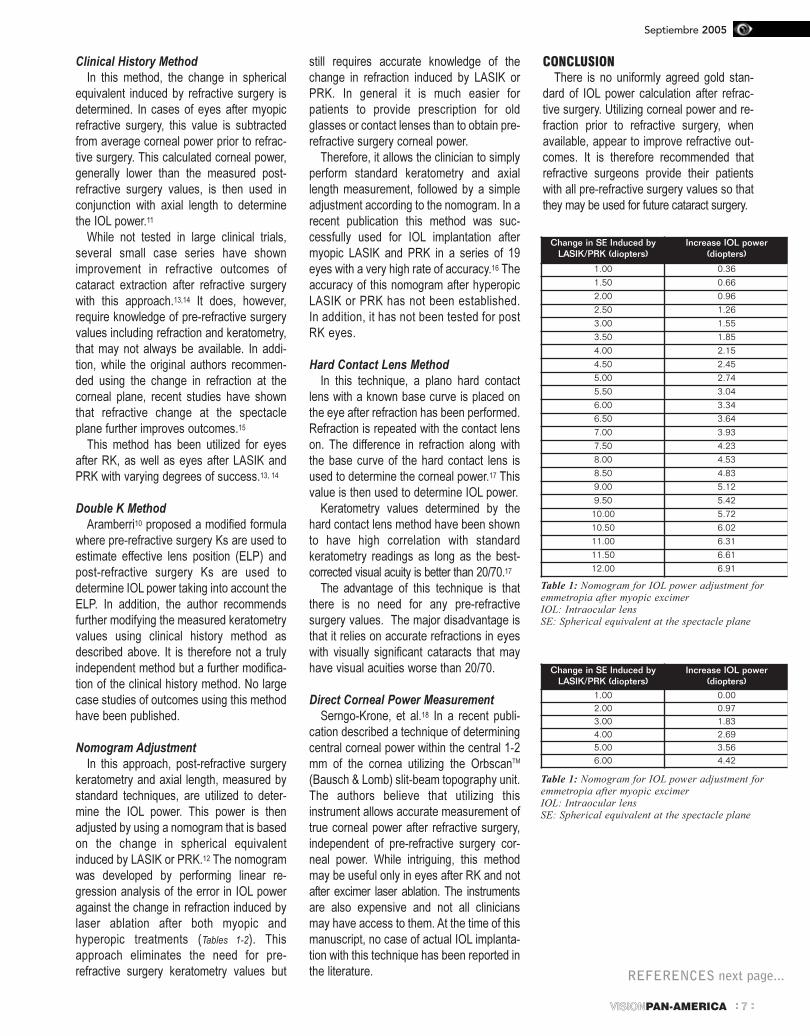
Nomogram Adjustment
In this approach, post-refractive surgery
keratometry and axial length, measured by
standard techniques, are utilized to deter-
mine the IOL power. This power is then
adjusted by using a nomogram that is based
on the change in spherical equivalent
induced by LASIK or PRK.12 The nomogram
was developed by performing linear re-
gression analysis of the error in IOL power
against the change in refraction induced by
laser ablation after both myopic and
hyperopic treatments (Tables 1-2). This
approach eliminates the need for pre-
refractive surgery keratometry values but
still requires accurate knowledge of the
change in refraction induced by LASIK or
PRK. In general it is much easier for
patients to provide prescription for old
glasses or contact lenses than to obtain pre-
refractive surgery corneal power.
Therefore, it allows the clinician to simply
perform standard keratometry and axial
length measurement, followed by a simple
adjustment according to the nomogram. In a
recent publication this method was suc-
cessfully used for IOL implantation after
myopic LASIK and PRK in a series of 19
eyes with a very high rate of accuracy.16 The
accuracy of this nomogram after hyperopic
LASIK or PRK has not been established.
In addition, it has not been tested for post
RK eyes.
Hard Contact Lens Method
In this technique, a plano hard contact
lens with a known base curve is placed on
the eye after refraction has been performed.
Refraction is repeated with the contact lens
on. The difference in refraction along with
the base curve of the hard contact lens is
used to determine the corneal power.17 This
value is then used to determine IOL power.
Keratometry values determined by the
hard contact lens method have been shown
to have high correlation with standard
keratometry readings as long as the best-
corrected visual acuity is better than 20/70.17
The advantage of this technique is that
there is no need for any pre-refractive
surgery values. The major disadvantage is
that it relies on accurate refractions in eyes
with visually significant cataracts that may
have visual acuities worse than 20/70.
Direct Corneal Power Measurement
Serngo-Krone, et al.18 In a recent publi-
cation described a technique of determining
central corneal power within the central 1-2
mm of the cornea utilizing the OrbscanTM
(Bausch & Lomb) slit-beam topography unit.
The authors believe that utilizing this
instrument allows accurate measurement of
true corneal power after refractive surgery,
independent of pre-refractive surgery cor-
neal power. While intriguing, this method
may be useful only in eyes after RK and not
after excimer laser ablation. The instruments
are also expensive and not all clinicians
may have access to them. At the time of this
manuscript, no case of actual IOL implanta-
tion with this technique has been reported in
the literature.
CONCLUSIONThere is no uniformly agreed gold stan-
dard of IOL power calculation after refrac-
tive surgery. Utilizing corneal power and re-
fraction prior to refractive surgery, when
available, appear to improve refractive out-
comes. It is therefore recommended that
refractive surgeons provide their patients
with all pre-refractive surgery values so that
they may be used for future cataract surgery.
Change in SE Induced byLASIK/PRK (diopters)
Increase IOL power(diopters)
1.00 0.361.50 0.662.00 0.962.50 1.263.00 1.553.50 1.854.00 2.154.50 2.455.00 2.745.50 3.046.00 3.346.50 3.647.00 3.937.50 4.238.00 4.538.50 4.839.00 5.129.50 5.4210.00 5.7210.50 6.0211.00 6.3111.50 6.6112.00 6.91
Change in SE Induced byLASIK/PRK (diopters)
Increase IOL power(diopters)
1.00 0.002.00 0.973.00 1.834.00 2.695.00 3.566.00 4.42
Table 1: Nomogram for IOL power adjustment foremmetropia after myopic excimerIOL: Intraocular lensSE: Spherical equivalent at the spectacle plane
Table 1: Nomogram for IOL power adjustment foremmetropia after myopic excimerIOL: Intraocular lensSE: Spherical equivalent at the spectacle plane
REFERENCES next page...

Septiembre 2005
VISIONPAN-AMERICA8: :
Behçet's Disease and HyperprolactinemiaHHeelleennaa PPrrooeennççaa MMDD,, CCiiddaalliinnaa FFeerrrreeiirraa MMDD,, MMaarrggaarriiddaa MMiirraannddaa MMDD,, LLuuííss MMeettzznneerr SSeerrrraa PPhhDD,,AA.. CCaassttaannhheeiirraa--DDiinniiss PPhhDDCentro de Estudos das Ciências da Visão - Faculdade de Medicina de LisboaClínica Universitária de Oftalmologia - Hospital de Santa MariaAvenida Professor Egas Moniz1649-035 Lisboa - PortugalPlease address all correspondence to Helena Proença at the above address or [email protected] authors have no financial interest in the material discussed in this paper
INTRODUCTION:Rolactin (PRL) is a circulating hormone usually known by its important role in lactation. It's a
polipeptide chain secreted by pituitary gland. Its secretion is hypothalamus controlled by
inhibitory factors, like dopamine, and stimulatory factors such as thyrotropin releasing hor-
mone. There is also feedback by numerous circulating factors.
There has been a remarkable development of prolactin's physiopathological role
knowledge, specially concerning immunology.
There is conclusive scientific evidence of prolactine's functions as a cytokine1.
Prolactin is thimogenic and thereby influences immune cells' proliferation and differen-
tiation.
Prolactin-specific receptors have been identified on B and T lymphocytes, monocytes and
natural-killer cells. There is a structural homology between receptors for PRL and for interleukins
2 and 6. Lymphocytes have also been shown to secrete a prolactin-like substance. It has
been proven that hypophysectomised rats are immuno-compromised and PRL introduction
can restore their imune function1.
Cyclosporin A competes directly for prolactin binding sites on human lymphocytes. It also
stimulates prolactin production. Both these mechanisms are responsible for cyclosporin A
induced hyperprolactinemia and immuno-suppression.
Dopaminergic agonists that suppress serum prolactin are presently enroled on clinical trials
for autoimmune diseases treatment and organ transplant rejection prevention2.
At last, abnormal serum prolactin levels are related to many immunologic diseases:
systemic lupus erythematosus, autoimmune uveitis, thyroid disease, Reiter's syndrome3,
psoriatic arthritis, juvenile chronic arthritis, Sjogren's syndrome, sclerodermia, derma-
tomyositis, multiple sclerosis, Behçet's syndrome among other1.
In summary, prolactin from both pituitary and lymphocyte's origin plays an essential role in
white blood cells' proliferation and function.
Prolactin is a cytokine showing biphasic nature of immunomodulatory effect: hypo-
prolactinemia and hyperprolactinemia can both lead to immunocompromise.
Purpose: To report the clinical picture and
outcome of Behçet's Disease with hyperpro-
lactinemia.
Methods: We report a case of an 18-year-
old female who presented with monocular
decreased visual acuity two days before.
Results: The fundus examination revealed
papilitis and mild posterior vitritis OS.
Serologic analysis revealed hyperprolacti-
nemia, HLA B51 positive. Brain computed
tomography and magnetic resonance imaging
excluded intracraneal patology. Vitreous
humor Polymerase-Chain-Reaction was ne-
gative for common pathogens.
Conclusions: This case suggests the role
of prolactin in immunoregulation and patho-
genesis of Behçet’s Disease. We suggest
serum prolactin measu-rement in atypical
Behçet’s Disease suspect.
Key Words: Behçet’s disease, hyper-
prolactinemia, immunoregulation, auto-immune
diseases.
Case report:
An 18-year-old Caucasian female was
referred to our department for analysis of
unilateral decreased visual acuity and
uveitis two starting two days before.The patient had previously been healthy,
used no medications or other substances
and had no known previous disease.
She mentioned transient episodes of
cutaneous rash and headaches. She denied
oral or genital recorrent ulceration, galac-
torrhea or amenorrhea.
She had no family history of autoimmune
disorders.
1. Sandoval HP, de Castro LE, Vroman DT, Solomon KD.Refractive Surgery Survey 2004. J Cataract Refract Surg. 2005Jan;31(1):221-33.2. Hamilton DR, Hardten DR. Cataract surgery in patients withprior refractive surgery. Curr Opin Ophthalmol 2003;14:44-53.3. Seitz B, Langenbucher A, Nguyen NX, et al. Underestimationof intraocular lens power after myopic photorefractivekeratectomy. Ophthal-mology 1999; 106:693-7024. Gimbel HV, Sun R, Kay GB. Refractive error in cataractsurgery after previous refractive surgery. J Cataract Refract Surg2000;26:142-4.5. Wang L, Jackson DW, Koch DD. Methods of estimating cornealrefractive power after hyperopic laser in situ keratomileusis. JCataract Refract Surg. 2002 Jun; 28(6):954-616. Seitz B, Langenbucher A. Intraocular lens calculations statusafter corneal refractive surgery. Curr Opin Ophthalmol. 2000Feb;11(1):35-46. Review.7. Maeda N, Klyce SD, Smolek MK, McDonal MB. Disparitybetween keratometry-style readings and corneal power within thepupil after refractive surgery for myopia. Cornea 1997;16:517-5248. Feiz V, Mannis MJ. Intraocular lens power calculation aftercorneal refractive surgery. Curr Opin Ophthalmol. 2004Aug;15(4):342-9. Review9. Seitz B, Langenbucher A, Nguyen NX, et al. Underestimationof intra-ocular lens power after myopic photorefractivekeratectomy. Ophthalmology 1999; 106:693-70210. Aramberri J. Intraocular lens power calculation after cornealrefractive surgery: double-K method. J Cataract Refract Surg. 2003Nov;29(11):2063-811. Holladay JT. Consultations in refractive surgery [comment]Refract Corneal Surg 1989; 5:20312. Feiz V, Mannis MJ, Garcia-Ferrer F, Kandavel G, DarlingtonJK, Kim E, Caspar J, Wang JL, Wang W. Intraocular lens powercalculation after laser in situ keratomileusis for myopia andhyperopia: a standardized approach. Cornea. 2001 Nov;20(8):792-7.13. Wang L, Booth MA, Koch DD. Comparison of intraocular lenspower calculation methods in eyes that have undergone laser-assistedin-situ kerato-mileusis.Trans Am Ophthalmol Soc. 2004; 102:189-96;discussion 196-7.14. Odenthal MT, Eggink CA, Melles G, Pameyer JH, GeerardsAJ, Beekhuis WH. Intraocular lens power calculation for cataractsurgery after photorefractive keratectomy. Arch Ophthalmol. 2003Jul;121(7):1071.15. Hoffer KJ. Calculating intraocular lens power after refractivecorneal surgery. Arch Ophthalmol. 2002 Apr;120(4):500-1.16. Zeh WG, Koch DD. Comparison of contact lens overrefractionand standard keratometry for measuring corneal curvature in eyeswith lenticular opacity. J Cataract Refract Surg. 1999 Jul;25(7):898-90317. Sonego-Krone s, Lopez-Moreno G, Beaujon-Balbi OV, et al. Adirect method to measure the power of the central cornea aftermyopic laser in situ keratomileusis. Arch Ophthalmol 2004;122:159-66
REFERENCES:
"This work was supported in part
by a generous grant from Research
to Prevent Blindness, Inc.
New York, NY"
VISIONPAN-AMERICA 9: :
Septiembre 2005
Figure 1
Figure 3
Figure 2
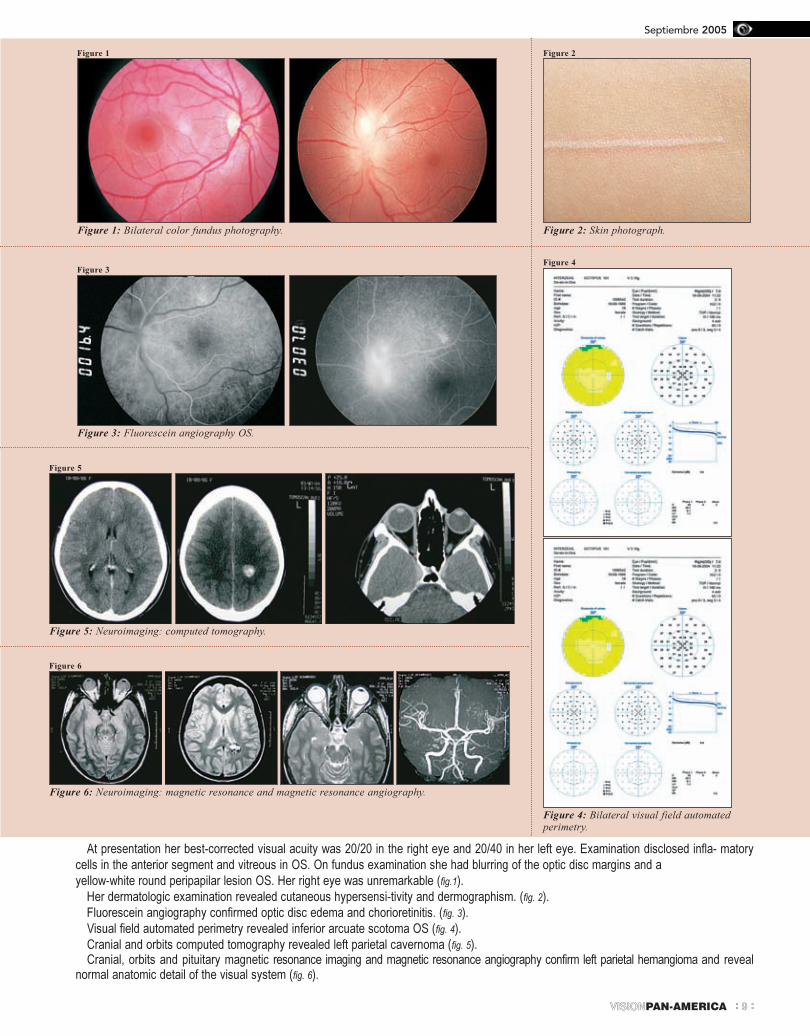
Figure 1: Bilateral color fundus photography.
Figure 3: Fluorescein angiography OS.
Figure 5
Figure 6
Figure 5: Neuroimaging: computed tomography.
Figure 6: Neuroimaging: magnetic resonance and magnetic resonance angiography.
Figure 2: Skin photograph.
Figure 4
Figure 4: Bilateral visual field automatedperimetry.
At presentation her best-corrected visual acuity was 20/20 in the right eye and 20/40 in her left eye. Examination disclosed infla- matory
cells in the anterior segment and vitreous in OS. On fundus examination she had blurring of the optic disc margins and a
yellow-white round peripapilar lesion OS. Her right eye was unremarkable (fig.1).
Her dermatologic examination revealed cutaneous hypersensi-tivity and dermographism. (fig. 2).
Fluorescein angiography confirmed optic disc edema and chorioretinitis. (fig. 3).
Visual field automated perimetry revealed inferior arcuate scotoma OS (fig. 4).
Cranial and orbits computed tomography revealed left parietal cavernoma (fig. 5).Cranial, orbits and pituitary magnetic resonance imaging and magnetic resonance angiography confirm left parietal hemangioma and reveal
normal anatomic detail of the visual system (fig. 6).
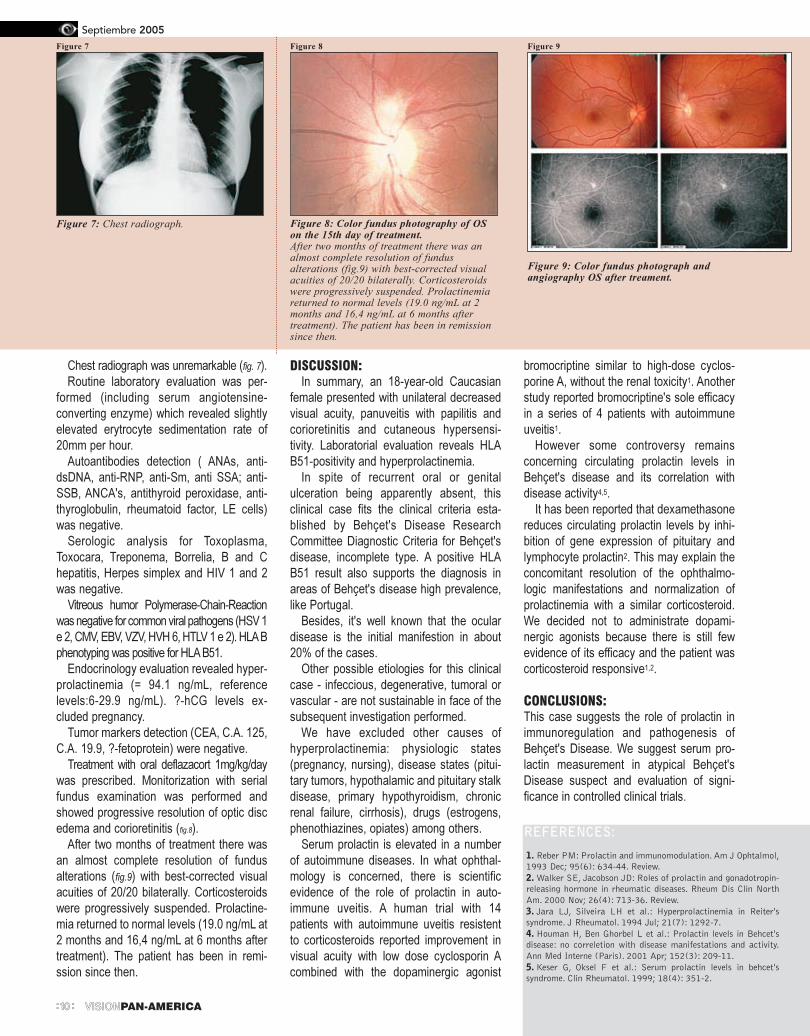
Chest radiograph was unremarkable (fig. 7).
Routine laboratory evaluation was per-
formed (including serum angiotensine-
converting enzyme) which revealed slightly
elevated erytrocyte sedimentation rate of
20mm per hour.
Autoantibodies detection ( ANAs, anti-
dsDNA, anti-RNP, anti-Sm, anti SSA; anti-
SSB, ANCA's, antithyroid peroxidase, anti-
thyroglobulin, rheumatoid factor, LE cells)
was negative.
Serologic analysis for Toxoplasma,
Toxocara, Treponema, Borrelia, B and C
hepatitis, Herpes simplex and HIV 1 and 2
was negative.
Vitreous humor Polymerase-Chain-Reaction
was negative for common viral pathogens (HSV 1
e 2, CMV, EBV, VZV, HVH 6, HTLV 1 e 2). HLAB
phenotyping was positive for HLA B51.
Endocrinology evaluation revealed hyper-
prolactinemia (= 94.1 ng/mL, reference
levels:6-29.9 ng/mL). ?-hCG levels ex-
cluded pregnancy.
Tumor markers detection (CEA, C.A. 125,
C.A. 19.9, ?-fetoprotein) were negative.
Treatment with oral deflazacort 1mg/kg/day
was prescribed. Monitorization with serial
fundus examination was performed and
showed progressive resolution of optic disc
edema and corioretinitis (fig.8).
After two months of treatment there was
an almost complete resolution of fundus
alterations (fig.9) with best-corrected visual
acuities of 20/20 bilaterally. Corticosteroids
were progressively suspended. Prolactine-
mia returned to normal levels (19.0 ng/mL at
2 months and 16,4 ng/mL at 6 months after
treatment). The patient has been in remi-
ssion since then.
DISCUSSION:In summary, an 18-year-old Caucasian
female presented with unilateral decreased
visual acuity, panuveitis with papilitis and
corioretinitis and cutaneous hypersensi-
tivity. Laboratorial evaluation reveals HLA
B51-positivity and hyperprolactinemia.
In spite of recurrent oral or genital
ulceration being apparently absent, this
clinical case fits the clinical criteria esta-
blished by Behçet's Disease Research
Committee Diagnostic Criteria for Behçet's
disease, incomplete type. A positive HLA
B51 result also supports the diagnosis in
areas of Behçet's disease high prevalence,
like Portugal.
Besides, it's well known that the ocular
disease is the initial manifestion in about
20% of the cases.
Other possible etiologies for this clinical
case - infeccious, degenerative, tumoral or
vascular - are not sustainable in face of the
subsequent investigation performed.
We have excluded other causes of
hyperprolactinemia: physiologic states
(pregnancy, nursing), disease states (pitui-
tary tumors, hypothalamic and pituitary stalk
disease, primary hypothyroidism, chronic
renal failure, cirrhosis), drugs (estrogens,
phenothiazines, opiates) among others.
Serum prolactin is elevated in a number
of autoimmune diseases. In what ophthal-
mology is concerned, there is scientific
evidence of the role of prolactin in auto-
immune uveitis. A human trial with 14
patients with autoimmune uveitis resistent
to corticosteroids reported improvement in
visual acuity with low dose cyclosporin A
combined with the dopaminergic agonist
bromocriptine similar to high-dose cyclos-
porine A, without the renal toxicity1. Another
study reported bromocriptine's sole efficacy
in a series of 4 patients with autoimmune
uveitis1.
However some controversy remains
concerning circulating prolactin levels in
Behçet's disease and its correlation with
disease activity4,5.
It has been reported that dexamethasone
reduces circulating prolactin levels by inhi-
bition of gene expression of pituitary and
lymphocyte prolactin2. This may explain the
concomitant resolution of the ophthalmo-
logic manifestations and normalization of
prolactinemia with a similar corticosteroid.
We decided not to administrate dopami-
nergic agonists because there is still few
evidence of its efficacy and the patient was
corticosteroid responsive1,2.
CONCLUSIONS:This case suggests the role of prolactin in
immunoregulation and pathogenesis of
Behçet's Disease. We suggest serum pro-
lactin measurement in atypical Behçet's
Disease suspect and evaluation of signi-
ficance in controlled clinical trials.
Figure 7
Figure 7: Chest radiograph.
Figure 8 Figure 9
Figure 8: Color fundus photography of OSon the 15th day of treatment.After two months of treatment there was analmost complete resolution of fundusalterations (fig.9) with best-corrected visualacuities of 20/20 bilaterally. Corticosteroidswere progressively suspended. Prolactinemiareturned to normal levels (19.0 ng/mL at 2months and 16,4 ng/mL at 6 months aftertreatment). The patient has been in remissionsince then.
Figure 9: Color fundus photograph andangiography OS after treament.
Septiembre 2005
VISIONPAN-AMERICA10: :
1. Reber PM: Prolactin and immunomodulation. Am J Ophtalmol,1993 Dec; 95(6): 634-44. Review.2. Walker SE, Jacobson JD: Roles of prolactin and gonadotropin-releasing hormone in rheumatic diseases. Rheum Dis Clin NorthAm. 2000 Nov; 26(4): 713-36. Review.3. Jara LJ, Silveira LH et al.: Hyperprolactinemia in Reiter'ssyndrome. J Rheumatol. 1994 Jul; 21(7): 1292-7.4. Houman H, Ben Ghorbel L et al.: Prolactin levels in Behcet'sdisease: no correletion with disease manifestations and activity.Ann Med Interne (Paris). 2001 Apr; 152(3): 209-11.5. Keser G, Oksel F et al.: Serum prolactin levels in behcet'ssyndrome. Clin Rheumatol. 1999; 18(4): 351-2.
REFERENCES:

romotion of scientific and cultural exchange among ophthalmologists in the Americas is a major goal
of PAAO. To that end, the Paul Kayser Scholarship provides funds on a competitive basis for US
residents and fellows to gain experience in Latin America. I was very lucky to benefit from this program and
I want to share my story in the hope of encouraging further exchange.
After choosing Peru as my destination, I contacted Dr. Francisco Contreras, a former PAAO president
and a prominent Peruvian ophthalmologist. He put me in touch with Johannes Kohler, a German doctor who
founded an eye clinic in the town of Abancay with the help of a catholic charity. Dr. Kohler, in turn, was very
gracious in inviting me to work with him for 2 weeks. By May, I was ready to go, sporting a large bottle of
SPF40 sunblock and a 15 kilo bag of surgical supplies kindly donated by Alcon Laboratories.
Abancay is a lively, dusty Andean town of roughly 65,000 people. This is one of the poorest parts of Peru
and as such, the clinic headed by Dr. Kohler is the only eye-care center serving the entire region. Dr. Kohler
picked me up from Cusco and we traversed the rollercoaster of a road that cuts through the mountains to
Abancay in 4 jolly hours. Still dizzy from the drive, I took lodging at the local convent and met the staff at the
clinic. Dr. Kohler works with 3 local nurses who juggle the roles of technicians, surgical assistants, social
workers, Quechua translators and miracle workers at large. Their dedication and professionalism impressed
me immediately upon starting work.
Each day we attended patients at the clinic: old farmers with 'count fingers' cataracts, adults with
pterigia, kids with uncorrected myopia, rural folk with fungal keratitis, retirees with presbyopia, etc. There was
the patient with pan-uveitis and severe retinal arteriolitis of unclear etiology that we sent for a systemic work-
up, and the boy with keratoconus and acute hydrops whose mother cried when we told her that a trip to Lima
was necessary for a corneal transplant. Tuesday we worked in the operating room where I learned that not
every surgical suite is equipped with a phaco machine or even an endless supply of disposable surgical
gowns. On Saturday, we drove to screen patients in a mountain community whose residents rarely make it
to Abancay. Lest you think this trip was all work, we ventured for hikes in the mountains and sampled tasty
Andean cuisine.
This trip provided my first glimpse of eye care in Latin America. The benefit to me as an ophthalmologist
in training and to the people I visited was tremendous. I returned with the anticipation that I can strengthen
my connection with doctors in Peru and donate my time and skills on a regular basis in the future. For now,
I hope that more US ophthalmologists establish relationships with our colleagues to the South.
Julie Freidlin, MD
Ophthalmology Resident, 2006
University of Illinois at Chicago
as enfermedades de la superficie ocular son actualmente reconocidas como una categoría de importancia en el campo de la cornea y las enfermedades
externas. Para el oftalmólogo de habla hispana no hay texto más completo y científicamente válido que Superficie Ocular por José Benítez del Castillo
y sus colegas de la Universidad Complutense de Madrid. Con contribuciones de muchos autores de España, Estados Unidos, Japón, Reino Unido, Italia,
Alemania, Argentina, Chile y Francia, este notable texto de 49 capítulos abarcan los tópicos de las enfermedades de la superficie ocular desde la anatomía
básica y estudios de laboratorio hasta actuales y aun experimentales procedimientos quirúrgicos.
El texto es municioso y claro. Se inicia con un capítulo de la anatomía funcional de la superficie ocular, luego los autores continúan con la actual
clasificación de las enfermedades de la superficie ocular. Capítulos de Ojo Seco están seguidos por un grupo de capítulos sobre el párpado que incluye
anormalidades anatómicas y enfermedades inflamatorias. Los capítulos siguientes cubren virtualmente todas las enfermedades de la superficie ocular inclu-
yendo lentes de contacto y superficie ocular, enfermedades iatrogénicas, cirugía refractiva y enfermedades de la superficie ocular, distrofias corneales, pterí-
gion, tumores de superficie, síndromes mucocutaneos, conjuntivitis infecciosa, degeneración corneal anterior y cinco capítulos de diversas causas de keratitis.
El último grupo de capítulos se refiere a terapia médica y quirúrgica. Hay excelentes y completos capítulos de lágrimas artificiales, terapia hormonal,
agentes anti-inflamatorios, higiene palpebral, anti-metabolitos, suero autólogo, lentes terapéuticos y medicaciones sistémicas para las enfermedades de la
superficie ocular. Los capítulos de terapia quirúrgica incluyen secciones de queratectomía fototerapéutica, alteraciones palpebrales, adhesivos corneales,
transplante de membrana amniótica, injertos limbares, keratoplastia lamelar, prostokeratoplastia y una expansión ex-vivo de células madres para
transplantes, entre otros tópicos. El minucioso y bien escrito texto se complementa con bellas fotografías y claras e ilustrativas tablas.
Los autores han producido un notable hito de referencia que seguramente será una obra mayor de este tema en la lengua castellana.
Mark J. Mannis, MD
José M. Benítez del Castillo Sánchez MD.,
Juan A. Durán de la Colina MD. y María Teresa Rodríguez Ares MD.
Editorial: Sociedad Española de Oftalmología 2004
VISIONPAN-AMERICA 11: :
Septiembre 2005
P
L
MMaakkiinngg ccoonnnneeccttiioonnss:: tthhee PPaauull KKaayysseerr SScchhoollaarrsshhiipp
BBooookk RReevviieewwSSuuppeerrffiicciiee OOccuullaarr
Septiembre 2005
VISIONPAN-AMERICA12: :
Visión Pan-América es la publicación oficial de la Asociación
Panamericana de Oftalmología. La publicación está particularmente
interesada en recibir manuscritos que sean cortas revisiones de
materias novedosas de interés para los oftalmólogos miembros de
la Asociación. Además de las revisiones, la publicación está intere-
sada en artículos acerca de nuevas técnicas quirúrgicas, nuevas
terapias médicas, y casos de correlacion clinico-patológica.
Información de Presentación:Los manuscritos deben enviarse electrónicamente al jefe de
redacción, Mark J. Mannis, MD a [email protected] o puede
enviarse vía el correo a:
Mark J. Mannis, MD,
Department of Ophthalmology
University of California,
Davis 4860 Y Street, Suite 2400
Sacramento, CA 95817
U.S.A
Si se envía el trabajo por correo, este debe ir tanto impreso (a
máquina,etc.) y en forma electrónica (CD, etc.). Todas las presen-
taciones deben ser publicaciones originales que no se hayan
publicado en otra parte. Las presentaciones pueden ser escritas en
idioma español, inglés, portugués o francés. Todos los trabajos
deben tener un resumen en inglés y en español.
Formato de Presentación:Los trabajos presentados no deben sobrepasar las 1500 palabras
(seis páginas escritas a doble espacio) más las referencias.
Las referencias deben ser incluidas como una lista en una página
separada al final del manuscrito con referencias citadas codificadas
al texto en el orden de aparición.
El siguiente formato debe usarse para las referencias:
Jones JS, García TL, Perrero M. Retinopatía Diabética en Bolivia.
Córnea, 1996; 26 (2): 341 - 343.
Smith DJ, Caldera MC, Chang N, Ferrer RJ. Managing Trauma
Ocular. Hofstra y Publicadores de Kennimore, Londres, 1989.
Se aceptan figuras de color y deben enviarse en PICT, TIFF o
formato de JPEG. El formato de Powerpoint no es aceptable.
La página del título debe incluir lo siguiente:
(1) el nombre completo de cada autor (es decir, nombre, apellido y
la inicial media si usa,) y el grado académico más alto; (2) la ciudad,
estado, y país en que el trabajo se llevó a cabo; (3) el nombre y
dirección del autor para recibir pedidos de separata; (4) declaración
de los autores si existe o no interés financiero en un producto citado
o utilizado en el trabajo.
Vision Pan-America is the official publication of the Pan-American
Association of Ophthalmology. The publication is particularly in-
terested in receiving manuscripts that are short state–of-the-art
review papers that will be of interest to the practicing PAAO member
ophthalmologist. In addition to review articles, the publication is
interested in articles on new surgical techniques, medical therapies,
and case reports that emphasize clinicopathologic correlations.
Submission information:Manuscripts should be submitted electronically to the Editor-in-
Chief, Mark J. Mannis, MD at [email protected] or can be sent
via mail to:
Mark J. Mannis, MD,
Department of Ophthalmology
University of California,
Davis 4860 Y Street, Suite 2400
Sacramento, CA 95817
U.S.A
All submissions must be provided in electronic form as well as
written manuscript form if mailed. All submissions must be original
publications that have not been published elsewhere. Submissions
can be in Spanish, English, Portuguese or French. All papers should
be preceded by an abstract in either English or Spanish.
Submission Format:Papers submitted should be no longer than 1500 words (six double
–spaced type-written pages) plus references.
References should be included as a list on a separate page at the
end of the manuscript with cited references keyed to the text in the
order of appearance.
The following format should be used for referenced papers:
Jones JS, García TL, Perrero M. Diabetic retinopathy in Bolivia.
Cornea, 1996; 26 (2): 341- 343.
Smith DJ, Caldera MC, Chang N, Ferrer RJ. Managing Ocular
Trauma. Hofstra and Kennimore Publishers, London, 1989.
Color figures are encouraged and should be submitted in PICT, TIFF
or JPEG format. Powerpoint format is not acceptable.
The title page should include the following:
(1) each author's full name (i.e., first name, middle initial if used, and
last name) and highest degree; (2) city, state, and country in which
work was carried out; (3) name and address of author to receive
reprint requests; (4) statement about the authors' proprietary or
financial interest in a product or lack thereof.
:::: IInnssttrruucccciioonneess aa llooss AAuuttoorreess
:::: IInnssttrruuccttiioonnss ttoo AAuutthhoorrss
Imp
reso
po
r P
rin
ter
Co
lom
bia
na
S.A
.