Embed Size (px)
Citation preview

Child psyChiatry and developmental disorders
Behaviour disorders in children and adolescentsrichard harrington
sean maskey
AbstractBehaviour disorders in children are common, particularly in boys, and
cause significant social, academic and personal impairment. young chil-
dren frequently recover from mild forms, but severe early-onset conduct
disorder is persistent and very costly to the individual, their family and
society. the causes are multifactorial and the intervention is psychoso-
cial and, in older children, needs to be complex. hyperkinetic disorder is
an early-onset biologically-based disturbance of attention, concentration
and motor activity that causes pervasive impairment of function. atten-
tion deficit hyperactivity disorder is a broader concept including children
with milder and less pervasive difficulties. treatment is multidisciplinary
and usually involves medication, typically a stimulant. Untreated, the
likely outcomes are poor academic performance, conduct disorder and
substance misuse. the long-term benefits of medication are less clear.
Keywords adolescent; attention deficit hyperactivity disorder; child;
conduct; disruptive behaviour; hyperkinetic; methylphenidate; opposi-
tional; parenting; psychiatry; violence
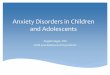
Behaviour disorders are often called externalizing or disruptive childhood disorders; the typical complainant is someone else, contrasting with internalizing disorders that primarily distress the self (Figure 1).
Conduct disorders
Clinical features: conduct disorders (CDs) are characterized by frequent or severe antisocial behaviour that lasts for at least 6 months. In young children, the clinical picture is dominated by markedly oppositional behaviour such as defiance, hostility and disruptiveness that is outside the normal range (opposi-tional-defiant disorder). In older age groups, behaviours such as stealing, truancy, fighting, lying and running away are seen. In
Richard Harrington MD FRCPsych originally wrote this contribution. He
was Professor of Child and Adolescent Psychiatry in the Academic
Department of Child and Adolescent Psychiatry at the Royal
Manchester Children’s Hospital, Manchester, UK. It has been updated
by Sean Maskey for this edition.
Sean Maskey FRCPsych is a Consultant Child and Adolescent Psychiatrist
at the Michael Rutter Centre, South London and Maudsley NHS
Foundation Trust, London, UK. He works with children and young
people who are adopted, fostered or in care proceedings, and under-
eights with conduct disorder. Competing interests: none declared.
mediCine 36:9 48
the most severe cases, fire setting or cruelty to animals or other children may occur. Conduct disorder is usually associated with poor peer relationships, but sometimes occurs in children who are generally well integrated into their peer group. It may also be secondary to other mental or physical disorders.
Co-morbidity and differential diagnosis: conduct disorder is strongly associated with learning disability and specific develop-mental disorders; about one-third of affected children have read-ing difficulties. Hyperkinetic disorder is frequently co-morbid with CD as hyperkinetic conduct disorder. CD is occasionally the result of organic brain disorder, such as epilepsy or acquired brain injury. Short lived but sometimes intense behavioural dis-turbance - adjustment disorder - may follow from upsetting life events such as loss of a parent or other major upset. Aggression and violence may be a non-specific response to emotional dis-tress, triggered by a neurotic disorder such as obsessive com-pulsive disorder or it may instrumental in achieving control over the situation, for example by coercing a parent to comply with a an anorexic’s calorie avoidance. The emotional arousal and heightened threat perception of post traumatic stress dis-order may mimic CD. Children who are being severely mal-treated, abused or neglected may present only with significant behavioural symptoms. It is essential therefore to understand the genesis of the behaviour, fully assess the psychiatric status of the child and understand the family context (see also pages 475–477). A child’s experience of severe or chronic disruption or disturbance of parenting may lead to the child developing a set of behaviours - attachment disorders - that seem to enhance autonomous self preservation, in contrast to social interdepen-dence. The child is over-friendly but intolerant of ordinary social rebuffs, they may show heightened arousal and fear, ‘frozen watchfulness’ and poor emotional control, and frequent violence when distressed.
Epidemiology and aetiology: CD occurs in about 6%1 of all chil-dren aged 5–16 years. The prevalence increases during adoles-cence and it is twice as common in boys as in girls. Conduct disorder is not the same as, but frequently leads to, delinquency (offending behaviour which in an adult would lead to crimi-nal conviction), which is much more common and exhibits a greater male preponderance. There are well-recognized factors which increase the risks of CD; social adversity, parental discord,
• parent training programmes are the evidence-based
intervention for conduct disorders in younger children
• life-course persistent conduct disorder is just that; small boys
do not ‘grow out of it’
• medication is of proven efficacy in adhd but effects may not
persist in the long term
• Genes and gene x environment interactions are emerging
areas of research
What’s new?
2 © 2008 elsevier ltd. all rights reserved.

Child psyChiatry and developmental disorders
Adolescent onset
Lifetime persistent
Socialized
Excessivemovement
Out of seat
FidgetyHyperactivity
Attention
Restless
Short span
Distractible
Impulsivity
MedicationPTSD
Psychosis
Mood disorders
Acquired brain injury
Otherdisorders
Atomoxetine
Dexamphetamine
Methylphenidate
Diagnostictriad
HD/ADHD
Reckless
Interruptsand calls out
Difficultytaking turn
Younger age
Non-violent
Unsocialized
Confined to the home
Comt
Genetics
Peergroup
CD
CD
ADHD
Up to 50%antisocial personality
Delinquency
CDODD
Substance misuse
Injury
Poor academic attainments
Parenting style
Social adversity
Learning difficulty
Parental criminality
Domesticviolence
Intrauterine
Smokingand ADHD
Witness
Victim
Often resolveODD
Adjustmentdisorder
Behaviour disturbance/behavioural regression is
typical childhood response to:divorce/loss of parent,
illness and other disruption
Primary
Outcomes
Secondary
Predisposinginfluences
Childhoodbehaviourdisorders
Childhoodbehaviourdisorders
Course
A ‘map’ of childhood behaviour disorders
CD, conduct disorder; HD, hyperkinetic disorder; ADHD, attention deficit hyperactivity disorder; ODD, oppositional defiant disorder;
PTSD, post-traumatic stress disorder.
Figure 1
reconstituted families and stepchildren in the home, poor educa-tion (parent and child), and locality, although not necessarily inner-city. Parents are often inconsistent in applying rules and are commonly critical and rejecting of the child. CD is increas-ingly also shown to be heritable. Three patterns emerge: child-hood limited, adolescent onset, (typically lasting about 3 years), and life course persistent (early onset and continuing into adult life). Young people with CD are often rejected by their non-anti-social peers and therefore usually associate with delinquent peer groups where the behaviour may be a sub-cultural norm, a pat-tern characteristic of adolescent onset. The unsocialized group will typically have early onset, associated neurodevelopmental problems and more persistent and severe behaviour problems.
mediCine 36:9 4
Biological factors are generally considered less important than social factors. However, genetic influences can have a role. Recently, genetic and, more importantly, gene environment interactions2 have been demonstrated and are promising areas for future research (see also pages 493–495).
Prognosis: the outcome in CD varies. Young people with few symptoms and good peer relationships, the common presentation of oppositional defiant disorder, usually fare well even without treatment. Those with onset in early childhood, poor peer rela-tionships and many different conduct symptoms are at a 40–50% risk of personality disorder in adulthood. Almost all adults with antisocial personality disorder suffered CD as children. Mortality
83 © 2008 elsevier ltd. all rights reserved.

Child psyChiatry and developmental disorders
from suicide, accidents and diseases related to lifestyle factors, such as smoking and drinking, is increased. Conduct disorder is also a risk factor for many mental disorders in adulthood. Childhood-onset disorders may remit; even with severe CD, 50% do not grow into adults with antisocial personality disorder, or other adverse adult outcomes.4
Management: the National Institute for Health and Clinical Excellence (NICE) recommends group-based parent training programmes5 based on social learning theory for behavioural difficulties in children developmentally aged 12 years or under. These techniques, such as the Parent Child Game,6 have a structured content and attend to the parent–child relationship, enhancing sensitive responding (i.e. emotional attunement to the child, appreciating the child’s perspective and responding con-tingently). It also teaches assertive discipline (i.e. the consistent use of age-appropriate, clear commands and responses to the child that are contingent on the child’s behaviour, so maximiz-ing the fit of parental expectations and producing suitable limits, rewards and punishments). The benefits of such programmes have been shown to continue for at least 1 year.
Treatment for adolescents with established CD is more diffi-cult. However, there is evidence that shows intensive structured programmes, such as Functional Family Therapy, may be benefi-cial. Medication is of little value in reducing antisocial behaviour, though the doctor may have a role in diagnosing and treating comorbid disorders, such as depression and substance abuse, and in ensuring that these young people have access to health care. Teenagers with conduct disorder are at high risk of physical problems, such as sexually transmitted infections and alcohol-related or drug-related conditions.
Children with CD commonly cause substantial disruption in school and the community, so it is important to work closely with other agencies such as Youth Inclusion Teams and the Courts. Children with CD are 10 times more likely to be excluded from school, in addition to problems with truancy, their educa-tional attainments are poor. Children who are severely disturbed may benefit from placement in a special school or residential setting. It is hoped that the focus on evidence-based parenting programmes by the National Academy of Parenting Practitioners3 will greatly improve the availability and accessibility of effective treatment programmes.
Hyperkinetic disorders
Clinical features: hyperkinetic disorder (HD) is characterized by early onset of overactive behaviour (e.g. fidgeting, ‘always on the go’), impulsiveness (e.g. giving answers to questions in class before being asked, running into the road) and marked inatten-tion (e.g. easily distracted, unable to concentrate on school work or other tasks that he or she does not find engaging) (Table 1). The diagnosis requires that the impairment should start before 5 years, be pervasive (e.g. home and classroom), and persist over time. The commonly used term attention deficit hyperactivity dis-order (ADHD) requires some symptoms, rather than impairment, to be pervasive. Hyperkinetic disorder is difficult to diagnose in the under-5s, because there is a wide normal variation in activity levels in this group. Several other abnormalities are associated with the disorder, including developmental and various learning difficulties.
mediCine 36:9 48
Comorbidity and differential diagnosis: the increased arousal of anxiety disorders may mimic ADHD, however, it can usu-ally be differentiated by the situation-specific nature. In autis-tic spectrum disorders, overactive behaviour is common but the social interaction is typically very different. The attention getting behaviours of CD may obscure the diagnosis of HD and the con-ditions frequently co-occur. Moreover HD predisposes to later conduct disorder. Tourette’s syndrome is frequently comorbid. Acquired brain injury may be causal or a result of HD behav-iours. Similarly, it is all too easy to assume that the behavioural difficulties of a child with a chronic history of abuse and neglect are a result of their experiences, ignoring the easily treated hyperkinetic component. However, the emotional dysregulation of attachment disorders and complex post-traumatic stress disor-der may mimic HD.
Epidemiology and aetiology: the estimated prevalence of HD varies widely (from 1.5% in the UK2 to 5% for ADHD in the USA). Boys are six times more likely to have the disorder than girls. Recently, similar impairments have been recognized in adults.
Brain dysfunction resulting from diverse biological processes is important in the aetiology. A recent imaging study showed a delay in cortical maturation. Genetic variation in the dopa-mine neurotransmitter systems may underlie executive function deficits in sustained attention, planning and the ability to delay gratification. ADHD and particularly HD are highly heritable conditions.
Hyperkinetic syndrome is more common in children and ado-lescents with learning difficulties, even when corrected for devel-opmental age, and is common following head injury.
Prognosis: hyperkinetic children become less active during ado-lescence, but remain more active than their peers. Follow-up studies suggest that they are at increased risk of CD, substance misuse and delinquency later in life. Some hyperkinetic children become impulsive and overactive adults.
Components of hyperactivity
Attention deficit
• Fails to give attention
• does not listen
• easily distracted
• Forgetful
Hyperactivity
• excessive movement
• Fidgeting
• difficulty playing quietly
• talks excessively
Impulsivity
• often acts without thinking
• reckless
• difficulty taking turns
• interrupts others
Table 1
4 © 2008 elsevier ltd. all rights reserved.

Child psyChiatry and developmental disorders
Management: primary care assessment should exclude physi-cal and developmental problems and a general screening questionnaire, such as the Strengths and Difficulties Question-naire7 (SDQ) will help clarify issues. The condition should be managed by a multidisciplinary approach, covering psychologi-cal, parental, educational and medical interventions enabling the development of a treatment strategy that is acceptable to the child and his parents (Table 2). Parenting programmes are important for the pre-school child. Many parents have tried vari-ous diets, and there is no reason not to continue these if they are not restrictive and the parents feel that they have helped.Methylphenidate – the multimodal treatment of ADHD (MTA)
trial has clearly shown the benefit of methylphenidate over careful behavioural treatment at one and two years follow-up. The longer term open follow-on study is more complex; there was no differ-ence in outcome by initial treatment. However, many of the chil-dren in the unmedicated arm were on methylphenidate at 3 years and some of those initially on medication had stopped and medica-tion compliance was variable, compromising analysis by treatment intention. Current evidence suggests that stimulants have relatively few serious side effects and, certainly for HD, but less clearly for ADHD the risk:benefit ratio is in favour of treatment as recom-mended by the NICE technology appraisal.8 Appetite suppression is a significant risk and so monitoring of weight and height is essential. The pressor effect may increase pulse and blood pres-sure. Recently a number of modified release forms of methylphe-nidate have been made available. These greatly reduce the burden of medication on children and their schools and careful match-ing of the drug profile with individual circumstances is beneficial. Dexamphetamine like methylphenidate is a central stimulant and has similar side effects. It is licensed for use in children aged three and above, although when medication is necessary, the clinician’s familiarity with methylphenidate may be preferable to licensed use. It is typically a second preference medication and may be less epileptogenic in children with poorly controlled epilepsy.
nICe guidelines on the treatment of AdHd
• methylphenidate, dexamphetamine and atomoxetine are
recommended in hd
• methylphenidate is not licensed for use in children less than
6 years of age, or for those with anxiety, tics, heart disease
or glaucoma; use with caution in epilepsy and substance
dependence. a specialist may prescribe dexamphetamine for
a child aged 4 or over
• the diagnosis of attention deficit disorder should be
made by a child psychiatrist or paediatrician with relevant
expertise; diagnosis should involve the parents and school
• treatment with medication should be started only by a
child psychiatrist or an experienced paediatrician; the Gp
may monitor and continue medication under shared care
arrangements
• Choice of medication depends on the symptom and
the individual risk/side effect profile; where there is no
preference, the cheapest option should be used
Table 2
mediCine 36:9 48
Atomoxetine is a recently licensed non-stimulant medication that is also recommended by NICE as a first-line treatment.
Mixed disorders of conduct and emotions
A mixture of emotional and behavioural problems characterize these conditions. About 20% of depressed children also have CD (so-called ‘depressive conduct disorder’). Depression is usually secondary to the CD, or to one of the consequences of CD (e.g. parental criticism of the child). Treatment is symptomatic. The prognosis is usually determined more by the conduct disorder than by the depression. The incidence of self-harm is high. ◆
ReFeRenCes
1 Green h, mcGinnity a, meltzer h, Ford t, Goodman r. mental health
of children and young people in Great Britain. Basingstoke: palgrave
macmillan houndmills, 2004. available at: http://www.statistics.gov.
uk/downloads/theme_health/GB2004.pdf (accessed 2 Feb 2008).
2 Caspi a, mcClay J, moffitt te, et al. role of genotype in the cycle of
violence in maltreated children. Science 2002; 297: 851–54.
3 http://www.parentinguk.org/
4 odgers Cl, Caspi a, Broadbent Jm. prediction of differential adult
health burden by conduct problem subtypes in males. Arch Gen
Psychiatry 2007; 64: 476–84.
5 national institute for health and Clinical excellence. parent-training/
education programmes in the management of children with conduct
disorders. technology appraisal. london: niCe, 2006.
6 Forehand r, mcmahon r. helping the non-compliant child. new york:
the Guildford press, 2003.
7 Goodman r. the strengths and difficulties questionnaire: a research
note. J Child Psychol Psychiatry 1997; 38: 581–86.
8 national institute for health and Clinical excellence.
methylphenidate, atomoxetine and dexamfetamine for attention
deficit hyperactivity disorder (adhd) in children and adolescents.
review of technology appraisal 13. london: niCe, 2006.
FuRTHeR ReAdIng
earls F, mezzacappa e. Conduct and oppositional disorders. in:
rutter m, taylor e, eds. Child and adolescent psychiatry: modern
approaches. 4th edn. oxford: Blackwell science, 2002; 419–36.
henggeler sW, Borduin Cm. Family therapy and beyond. a
multisystemic approach to teaching the behavior problems of
children and adolescents, pacific Grove: Brooks-Cole, 1990.
taylor e, döpfner m, sergeant J, et al. european clinical guidelines for
hyperkinetic disorder – first upgrade. Eur Child Adolesc Psychiatry
2004; 13(suppl 1): 1–8.
Practice points
• early intervention improves the outcome in conduct disorders
• Children with established conduct disorder are at high risk of
personality problems and delinquency later in life
• the diagnosis of hyperkinetic disorder requires that
impairment is present in more than one situation
• stimulants and atomoxetine are effective treatments for
hyperkinetic disorder and adhd
5 © 2008 elsevier ltd. all rights reserved.