Embed Size (px)
Citation preview

Behavioral Medicine at JoslinBehavioral Medicine at JoslinResources and Expectations for Affiliated
Programs

October 2009
Joslin Care = Team Care
• Endocrinologist• Nurse educator, CDE• Dietitian educator, CDE• Exercise physiologist
(or related degree)
• Mental health provider– Social worker– Psychologist– Psychiatrist
The Joslin Mental Health Provider’s
Orientation:
•Policy AO-20
•Come to Boston for training
•Use Psychosocial Manual (Tab A)

October 2009
How is behavioral medicine integrated at Joslin?
• People– Large staff (social worker, psychologist, psychiatrist)
• Materials– Assessment tools– Handouts (stress management, emotions)
• Classes / Support groups– Usually begin with discussions related to feelings, common
misunderstandings – You Did It – a specific class on goal setting– Blood Glucose Awareness Training (BGAT)– Support groups
• Counseling Approaches– A focus on behavioral goal setting – Understanding barriers– Patient directed action steps
• Participate in team meetings – discuss cases

October 2009
Expectations for Affiliates
• Identify, orient and use your Mental Health Provider (MHP)• Clarify roles and responsibilities:
– Attend periodic staff meetings– Attend annual Affiliate Site Visit– Conduct classes for patients/training for Joslin staff– Participate in team clinical case conferences– Conduct support groups and/or other classes – See patients individually by appointment
• Identify someone on the Affiliate staff who will be the primary link to the MHP (to forward Joslin related materials, updates, etc)

October 2009
Joslin Resources for Behavioral Medicine
• Psychosocial Manual• Integrated into forms, classes, materials, etc• Joslin/Boston experts
– Readings– Consultation
• Discuss your needs with your Affiliate Site Coordinator

October 2009
Psychosocial Manual – TOC (2006)
• Mental Health Unit Structure– Job descriptions– Sample marketing materials
• Curriculum and resources– Relaxation strategies
• Group Treatment• Recommended Reading
– HCP– Patients
• Geriatric Assessment
• Structured Assessments– PAID– D QOL– R-BPRS– PHQ-2/9– DDS

October 2009
PAIDProblem Areas in Diabetes
• Questionnaire (20 items) to identify areas that may be barriers / problem areas
• Can be used for type 1 or type 2 • Valid and reliable; (First published in 1995)• 5 point scale: Not a problem Serious problem• Available in Spanish• Can be scored (0 – 100)• At Joslin Clinic – completed by all new patients

October 2009
Sample PAID questions
• Not having clear and concrete goals for your diabetes care?
• Feeling discouraged with your diabetes treatment plan?
• Feeling scared when you think about living with your diabetes?
• Uncomfortable social situations related to your diabetes care? (e.g., people telling you what to eat)
• Feelings of deprivation regarding food and meals
Which of the following diabetes issues are currently a problem for you?

October 2009
Basic Screening Assessment Questions
PHQ-2 (Personal Health Questionnaire):• Over the past two weeks, how often have you been
bothered by:– Little interest or pleasure in doing things?– Feeling down, depressed or hopeless?
If an anxiety disorder is suspected:• Over the past four weeks, how often have you been
bothered by:– Feeling nervous, anxious, on edge?– Worrying a lot about different things?

October 2009
Joslin Assessment FormsHow are psychosocial concerns addressed?
• Medical:– General feeling about having diabetes– Review of systems – PSYCH– Follow-up: mental health
• Education– Assess needs: Feeling less blue or depressed– Who helps with your diabetes?– PHQ-2 questions– What gets in the way? (emotions, stress, feeling
depressed)

October 2009
What can you do to enhance this service?
• Ways to enhance your relationship• Strengthening the role of the mental health
provider

October 2009
Joslin’s Behavioral Team:Areas of Interest
• John Zrebiec, MSW– Groups, BGAT
• Ann Goebel-Fabbri, PhD– Eating Disorders, Insulin omission, Wt mngmt
• Ann Butler, PhD– Psychopharmacology
• Katie Weinger, RN, EdD– Barriers to change, driving and hypoglycemia
• Marilyn Ritholtz, PhD– Adult and adolescent therapy, depression

October 2009
Depression and Anxiety Disorders
• Depression is common– 2-3 times more common than in general population– 19% met criteria for major depressive disorder
• Twice as likely to miss medication doses– About 70% type 2 report some depression symptoms
• Linked with poorer adherence to diet, exercise, meds and higher A1C levels

October 2009
Eating and Related Disorders
• Eating disorders more common in type 1 women– 2.4 times higher risk for developing eating disorder than
age matched women without diabetes
• Insulin restriction common in type 1– 30% insulin restrictors at baseline– Higher rates morbidity and mortality– Screening question: I take less insulin than I should
(often – sometimes – never)
Goebel-Fabbri, D.Care March 31(3):415-9, 2008

October 2009
Diabetes is a Self-Management Condition
Findings from DAWN
Adherence rates to all aspects of prescribed regimens• 19% - type 1• 16% - type 2
Identified link between BG and HCP relationships• 53% linked better BG control to good relationship• 37% linked poor control to one that wasn’t good
enough

October 2009
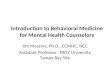
Relationship, Control and Distress DAWN - Diabetes Attitudes, Wishes and Needs
People with Diabetes Reporting Good Diabetes Control
53%
37%
Re
lati
on
sh
ip
Good Poor
People with Diabetes Reporting Diabetes Distress
25%
37%Re
lati
on
sh
ip
Good Poor

October 2009
• Insulin adherence estimates: 20-80%• Meal plan adherence: 65%• Blood glucose monitoring: 57-70%• Exercise adherence: 19-30%
• Global adherence in diabetes: 7%
Defining non-compliance in real terms

October 2009
• Clear communication counts– Patients who rated
communication as poor had an A1C 1% higher than those who assessed communication as good
– Demonstrate empathy and understanding
– The 3 important qualities of a constructive clinical relationship
Importance of the Pt-Provider Relationship

October 2009
• Communications is less about speaking than it is about listening and observing.– Barbara Anderson, PhD Former Joslin Psychologist

October 2009
Counseling Skills
• Listen! Observe.• Pay attention to your skills
– Open ended inquiry• “Tell me….” (not why)• Avoid questions requiring “yes” or “no” answers
– Reflective listening• “So, you are saying…..”• “It sounds like…..”
– Demonstrate empathy• “You seem….”• “Most people would find that hard…”
• Be positive– Focus on what can be done– Help patient set a specific goal

October 2009
Solving Problems – the Collaborative Way
• What does not work– Tell patient what to do– Provide solutions
• What does work– Let patient describe plan– Provide choices– Recognize you are both
“experts”

October 2009
Favorite Resources
• Educating Your Patient with Diabetes– Chapter by Marilyn Ritholtz
• The Art of Empowerment, 2nd Edition– Anderson, R and Funnell
• AADE Art and Science Text– Chapter 4
• Practical Psychology for Diabetes Clinicians– Anderson, B and Rubin
• 1000 Years of Wisdom– Lessons clinicians have learned from their patients