Embed Size (px)
Citation preview

Behavioral Health Problems in Childhood and Adolescence:
The Power of Prevention
Jeff Jenson, PhDPhilip D. & Eleanor G. Winn Professor for
Children and Youth at RiskAssociate Dean for Research
Graduate School of Social WorkUniversity of Denver
Michael M. Davis Lecture, The Center for Health Administration Studies. University of Chicago. October 27, 2015.

Behavioral Health Problems in Childhood and Adolescence: The Evolution of Prevention
Part 1
• Prevention Practice and Policy in the US, 1960-2015– Evolution of prevention programs and approaches– Models and frameworks– Risk, protection, and public health models– Public health to prevention science– Efficacy of preventive interventions
• Youth Matters Denver Public Schools Trial• Denver Bridge Project
– Current challenges

Behavioral Health Problems in Childhood and Adolescence:
The Power of Prevention
Part 2 • Unleashing the Power of Prevention, a Grand
Challenge for Social Work– Present key findings and goals from a national plan to
advance prevention policy and practices called Unleashing the Power of Prevention
– Identify policy, education, and advocacy efforts resulting from Unleashing the Power of Prevention

The Quest for Healthy Youth Development!!

5
What can get in the way?
Anxiety Depression Autism
Alcohol, tobacco,
other drug use
Risky driving
Aggressive behavior and
conduct problems
Delinquent behavior Violence
Self-inflicted
injury
Risky sexual behavior
School dropout

The Evolution of Prevention

The Origins of Epidemiology and Prevention: Cholera, John Snow, and the Broad Street Pump
Handle, 1854

Prevention Approaches, 1960-1980 • Information dissemination approaches were common in the 1960s and 1970s
– Media was often used to provide information to children and youth• The Man with the Goodies: http://www.youtube.com/watch?v=6yS_IJl_BkE • Yogi Bear: http://www.youtube.com/watch?v=viJqk-NIPag&feature=related• Sony Bono antidrug film: http://www.youtube.com/watch?v=mkgHBWgJI3c
– More graphic and recent examples are seen in commercials aimed at preventing methamphetamine use
• Meth, Just Once: https://www.youtube.com/watch?v=zM0c7phwzL8
• Fear arousal programs exposed children and youth to the consequences of crime and drug use during the 1970s
– Scared Straight – Recent examples are seen in Beyond Scared Straight
• Alternative school programs and early forms of affective education surfaced in the 1970s
• Collectively, information dissemination, fear arousal, and alternative school strategies had little or no effect on school, drug use, or delinquent outcomes

Prevention Approaches, 1980–1990• Poor outcomes from early studies led to new prevention
strategies in the 1980s– Social learning and cognitive-behavioral theories were used to develop
interactive and skills-based programs in schools • Life Skills Training (Botvin, 1984)
• Seattle Social Development Project (Hawkins & Catalano, 1986)
• Promoting Alternative Thinking Strategies (Greenberg & Kusche, 1993)
• Early controlled trials of these approaches revealed significant effects in preventing or delaying the onset of problem behaviors– Implementation of tested strategies was largely limited to funded and
short-term investigations
• A unifying conceptual model of prevention was still lacking

Prevention Approaches, 1990–2015
• A unifying prevention framework came with the adoption of a public health approach in the 1990s
Note. Adapted from the Centers for Disease Control and Prevention, http://www.cdc.gov/
Define the problem: Surveillance
Identify causes: Risk & protective factor research
Develop and test interventions
Implement interventions
Evaluate interventions
The Public Health Approach to Prevention

Risk Factors for Child and Adolescent Problem Behavior by Level of Influence

Risk Factors for Child and Adolescent Problem Behavior by Level of Influence
Risk Factors Substance Delinquency Aggression School
Abuse Dropout_____________________________________________________________________________________________________
Peer Factors:Associating with deviant peers x
x x xRejection by conforming peers x
x x x
Environmental/Community FactorsLaws and norms favorable to antisocial behavior x x
xAvailability and access to drugs and firearms x x
xPoverty and limited economic opportunity x x
x xCommunity disorganization x
x xMedia portrayals of antisocial behavior x
xTransitions and mobility x
x x x
This table is adapted from the Social Development Research Group (Catalano, Haggerty, Hawkins, & Elgin, 2011; Hawkins, 2006; Hawkins, Catalano, & Miller, 1992) and from Jenson & Bender (2014); Jenson, Alter, Nicotera, Anthony, & Forrest-Bank (2013); Jenson & Fraser (2011); and O’Connell, Boat, & Warner (2009).

Protective Factors for Child and Adolescent Problem Behaviors by Level of Influence
Individual FactorsEmotional self-regulation
High self-esteem
Communication and language skills
Positive attitude
Temperament
Low childhood stress
Interpersonal FactorsFamily Factors:
Reliable support and discipline from parents or caregivers
Family provides structure, limits, and predictability
Caring relationships with siblings
Attachment to parents or caregivers
Support from extended family members

Protective Factors for Child and Adolescent Problem Behaviors by Level of Influence
School Factors:
Support for early learning
Access to supplemental educational services
Positive teacher expectations
Effective classroom management
School practices and policies to reduce bullying
High levels of school engagement
Peer Factors:
Ability to make friends and get along with others
Relationships with positive and prosocial peers
Environmental/Community FactorsOpportunities for education, employment, recreation
Presence and availability of mentors
Positive social norms about behavior
Physical and psychological safety
This table is adapted from Jenson, Alter, Nicotera, Anthony, & Forrest-Bank (2013); Jenson & Fraser (2011); and O’Connell, Boat, & Warner (2009).

Levels of Prevention in the Context of a Public Health Approach
• Interventions based on a public health approach apply risk and protective factors at three levels of implementation
Prevention
Primary/Universal
Secondary/Selective
Tertiary/Indicated

From Public Health to Prevention Science• The adoption of a public health framework based on risk and
protective factors contributed to what has become recognized as a science of prevention (Coie, et al., 1993)
Define the Problem
Identify Risk and
Protective Factors
Developand Test
Prevention Strategies
Assure Widespread
Adoption

What is Prevention Science?
• Prevention science includes these common characteristics – Risk and protective factors associated with a problem behavior must
be changed to prevent that behavior– Malleable risk and protective factors identified in empirical studies
are recognized as the targets of prevention– Preventive interventions should be rigorously tested in efficacy trials– Efficacious programs should be replicated, implemented with
fidelity, and tested in large-scale effectiveness trials– Effective interventions should be the focus of translation efforts
• There has been steady interest in prevention science since the late 1990s– The Society for Prevention Research was established in 1991
http://www.preventionresearch.org– Prevention Science journal created in 2004

Preventing Mental, Emotional and Behavioral Disorders Among Young People:
Progress and Possibilities
O'Connell, M.E., Boat, T., & Warner, K.E. (Eds.) (2009). Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth and Young Adults. Institute of Medicine, National Research Council.

What have we learned from 30 years of research on the
effects of preventive interventions on behavioral
health outcomes?

Prevention is Effective• Experimental trials have identified
over 50 effective interventions for promoting children’s well-being and preventing substance misuse, depression, anxiety, violence, delinquency, and other behavioral health problems…
• Scale-up and widespread implementation of prevention programs are likely to produce positive changes in young people at the population level
Jenson, J.M., & Bender, K.A. (2014). Preventing child and adolescent behavior: Evidence-based strategies in schools, families, and communities. New York: Oxford University Press.

21
Effective Prevention Programs Save Money
• Findings from cost-benefit analyses of prevention programs reveal significant financial savings associated with the implementation of preventive interventions
• Aos and colleagues at the Washington State Public Policy Institute have conducted several cost-benefit analyses of prevention programs (http://www.wsipp.wa.gov/BenefitCost)– Many evidence-based preventive interventions
show a positive benefit to cost ratio

School-Based Prevention Programs
• Social and emotional learning programs– Life Skills Training (Botvin & Griffin, 2004)
– PATHS (Greenberg, 2004)
– Second Step (Brown et al., 2012)
• School-wide strategies– Olweus Bully Prevention Program (Olweus, 1993)
• Comprehensive and integrated programs– Incredible Years (Webster-Stratton & Reid, 2010)
– Seattle Social Development Project (Hawkins et al., 2008)

School-Based Prevention:The Youth Matters
Denver Public Schools Trial

36 classrooms in14 experimental schools
27 classrooms in14 control schools
The Denver Public Schools Study: A Group-Randomized Trial
All public elementary schools in urban Denver, Colorado
Schools were stratified byrisk criteria and geography
Randomly assigned28 schools to Youth Matters or
to a no-treatment condition
Measures• Bullying and victimization (Olweus
Revised Bullying Questionnaire)• Self-reports of antisocial attitudes, peers,
antisocial conduct, depressive symptoms, school commitment
Analyses • Multilevel linear growth modeling to
examine intervention effects across 5 waves
• LCA & LTA to assess patterns of bullying

Youth Matters: A Simplified Intervention Model
Child OutcomesBullying
VictimizationAntisocial conductSocial competence
Attachment and commitment to school
School-Wide Outcomes
Bullying incidentsSuspensions
ExpulsionsClassroom disruption
Threat of Bullying or
Victimization
PositiveClassroom NormsRules about bullying
Respect for others
Communication with teachers and staff
Emotion RegulationSocial skills
Behavioral skillsCognitive skills(problem-solving;
anger control;empathy)

Selected YM Intervention Effects • Findings from multilevel growth models:
Students in experimental schools reported significantly less overall and relational bully victimization than youth in control schools at times 4 and 5
Bullying behavior decreased in both groups over time; decline in bullying was greater in YM schools at the end of the study (time 4) and one-year follow-up (time 5)
Participants in YM moved from states of bullying, victimization, and bully-victimization to being uninvolved in aggressive incidents at significantly higher rates than controls
_________________
• Williford, A., Boulton, A.J., & Jenson, J.M. (2014). Transitions between subclasses of bullying and victimization when entering middle school. Aggressive Behavior, 40, 24-41.
• Jenson, J.M., Brisson, D., Bender, K.A., & Williford, A., (2013). Effects of the Youth Matters prevention program on patterns of bullying and victimization in elementary and middle school. Social Work Research, 37, 361-374.
• Williford, A.P., Brisson, D., Bender, K.A., Jenson, J.M., & Forrest-Bank, S.S. (2011). Patterns of aggressive behavior and peer victimization from childhood to early adolescence: A latent class analysis. Journal of Youth and Adolescence, 40, 644-655.
• Jenson, J. M., Dieterich, W. A., Brisson, D., Bender, K. A., & Powell, A. (2010). Preventing childhood bullying: Findings and lessons from the Denver Public Schools Trial. Research on Social Work Practice, 20, 509-517.
• Jenson, J.M., & Dieterich, W.A. (2007). Effects of a skills-based prevention program on bullying and bully victimization among elementary school children. Prevention Science, 8, 285-296.

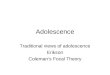
Predicted Bully Victimization Curves for Intervention
and Control Schools at One-Year Follow-up (Time 5)
0 1 2 3 4 5 6 7
-1.0
-0.5
0.0
0.5
1.0
Semester
log(B
ully
Vic
tim
Scale
- .7)
ControlIntervention
1.0
81.3
21.7
12.3
63.4
3
Bully
Vic
tim
Scale
YM-0.132, t-value = -1.953

Family-Based Prevention Programs
• Prenatal and perinatal interventions– Home visiting programs for new mothers at risk
– Nurse-Family Partnership Program (Olds et al., 2007)
• Behavioral parent training strategies– Teaching social-emotional skills to parents and their children in
groups– Coercive Family Process (Patterson, Chamberlain, & Reid, 1982)– Strengthening Families for Parents and Youth 10-14 (Spoth,
2001)
• In-home and outpatient family intervention– Families in crises to prevent out of home placement
– Multidimensional Treatment Foster Care (Chamberlain, Leve, & DeGarmo, 2007)
– Multisystemic Therapy (Henggeler et al., 1992)

Characteristics of Effective School and Family Prevention Programs
Intervention Characteristics• Effective programs…
– Target risk and protective factors for problem behavior– Use empirically-supported theoretical frameworks to inform program
design– Involve parents and children in intervention activities– Use behavioral and cognitive intervention strategies to teach social,
emotional, and cognitive skills to parents, children, and other family members
– Teach parenting skills that increase competencies in communicating, monitoring, and supervising children
– Include interactive sessions that allow for practice of newly acquired skills
– Include program activities aimed at improving parent-child relationships

Characteristics of Effective School and Family Prevention Programs
Implementation Characteristics• Effective programs…
– Specify target populations and levels of intervention– Offer interventions frequently and for long periods of
time– Receive organizational and infrastructure support from a
sponsoring community-based agency or school– Carefully consider, choose, and monitor who leads
prevention activities– Attend to issues of program adaptation that are
necessary to address cultural, gender, and other factors

Community-Based Prevention Programs• Community-based prevention strategies can be traced as far
back as the child saving movement in Chicago during the late 1800s– Early social work advocates and reformers like Jane Addams and Mary
Richmond laid the foundation for community-based prevention
• Other early influences:– The Chicago Area studies of the 1930s and 1940s by Shaw and McKay
stressed the need to understand relationships among poverty, social disorganization, immigration, and deviance
– Mobilization for Youth projects in the New York during the 1950s focused on improving community and economic opportunities for youth
• Early programs produced little in the way of positive outcomes; they did, however pave the way for later advances

Community-Based Prevention Programs• Today’s community prevention programs are often part of a
comprehensive approach that includes school and family interventions– The Harlem Children’s Zone and the Promise Neighborhood initiatives
exemplify multimodal forms of prevention
• Common program elements include:– Child care and preschool programs– School improvement strategies– Community-based health clinics– Community policing– Afterschool interventions– Policy and environmental strategies aimed at enforcing minimum
drinking ages, limiting access to drugs and weapons, and regulating the taxation and costs of alcohol and tobacco

The Denver Bridge Project:A Community-Based Prevention Program
Growing Minds. Creating Possibilities.

The Bridge Project Integrated Prevention and Early Intervention Model
Theoretical Models Goals & Interventions Outcomes
Risk and Protection
Positive Youth
Development
Community Collaboration
Goals Interventions
Enhance healthy
development
Increase positive behavior
Increase academic potential
Fosterresilience
Child & Youth Strategies• Academic support interventions• Social and emotional learning classes• Mentoring• Technology training
Community Strategies• Partnerships that foster information exchange • Reciprocity networks• Collaborative partners and networks
Intermediate Outcomes
• Reduce risk and increase protection• Increase 5 C’s of positive youth development
Long-Term Outcomes
• Positive behaviors• Academic success• Healthy emotional and social development

Selected Findings• Quasi-experimental design comparing Bridge Project participants to
youth living in other public housing communities
• Significant and positive differences in academic performance between Bridge participants and youth in other public housing communities– Higher reading scores– Better grades– Fewer absences– Higher standardized test scores
• Improvements in PYD constructs• Increase in technology skills• Improvements in social and emotional skills
See Jenson, J.M., Alter, C.F., Nicotera, N., Anthony, E.K., & Forrest-Bank, S.S. Risk, resilience, and positive youth development: Developing effective community programs for high-risk youth. Lessons from the Denver Bridge Project. (2013). New York: Oxford University Press.

Community-Based Prevention Systems• Community prevention systems have been developed in the
past two decades as a way to increase the dissemination and translation of prevention research to local communities
• Prevention systems guide community leaders and coalitions through a series of structured steps that include:– The establishment of a community board composed of local leaders,
parents, and youth – A systematic assessment of risk and protective factors for child and
adolescent problem behaviors– A review of prevalence data pertaining to problem behaviors– A process of prioritizing problem areas and setting program and
community goals– The selection, implementation, and evaluation of evidence-based
preventive interventions

Community-Based Prevention Systems• Two community prevention systems have received recognition in recent
years– Communities that Care (CTC) developed by David Hawkins, Richard Catalano, and
colleagues at SDRG– PROSPER: Promoting School-Community-University Partnerships to Enhance
Resilience developed by Richard Spoth and colleagues at Iowa State University
• CTC and PROSPER adhere to principles of prevention science, though differences exist in implementation– CTC offers extensive key leader and community board training, assessment and
survey instruments, and ongoing support to communities– PROSPER relies on existing county extension and family or consumer agents in local
settings to implement many system components
• CTC is now available through SAMHSA http://store.samhsa.gov/product/Communities-That-Care-Curriculum/PEP12-CTCPPT

How Effective are Community-Based Prevention Systems?
• CTC and PROSPER have been evaluated in group-randomized trials, CTC at the community level of assignment and PROSPER at the school district level– Both “systems” have yielded significant effects in preventing or
reducing drug use– CTC has also shown positive effects on delinquency and antisocial
conduct
• Characteristics of effective prevention systems– Adopting principles of prevention science that include the systematic
assessment of risk, protection, and problem behaviors – Building committed and sustained community boards and coalitions– Selecting and implementing evidence-based preventive interventions
with fidelity

Locating and SelectingEffective Prevention Programs
• Information about effective prevention programs is available at:
– Blueprints for Healthy Youth Development; http://www.blueprintsprograms.com
– Office of Juvenile Justice and Delinquency Prevention Model Program Guide; http://www.ojjdp.gov/MPG
– National Registry of Evidence-Based Programs and Practices, Substance Abuse and Mental Health Services Administration; http://www.nrepp.samhsa.gov
– Campbell Collaboration Library and Database; http://www.campbellcollaboration.org

Summary• Prevention has evolved from a pattern of loosely-organized
ideas, beliefs, and programs to a science based on principles of risk, protection, public health, and carefully specified interventions
• Evidence from longitudinal studies dating to the 1980s indicates that some well-implemented school, family, and community preventive interventions are effective in preventing behavioral health problems
• Significant cost savings are associated with the careful implementation of tested and effective preventive interventions

41
Yet…
• Tested and effective interventions for preventing behavioral health problems are not widely used
In fact...
• Prevention approaches that do not work or have not been evaluated are more widely used than those shown to be effective

42
How do we use knowledge gained from 30 years of
prevention research to advance practice and policy?

Ensure Healthy Development of all Youth:A Grand Challenge for Social Work
Unleashing the Power of Prevention!

44
What is Unleashing the Power of Prevention?
• Selected as a grand challenge initiative for ensuring the healthy development of all youth by the Academy of Social Work and Social Welfare in January, 2015
• A summary of evidence pertaining to behavioral health problems and an action plan aimed at increasing the widespread use of preventive interventions
• Authored by members of the Coalition for the Promotion of Behavioral Health

45
Who is the Coalition for the Promotion of Behavioral Health?
• An interdisciplinary group of prevention researchers, educators, policymakers, and practitioners who are interested in improving healthy child and youth development by….
Unleashing the Power of Prevention!!

46
Coalition for the Promotion of Behavioral Health:Steering Committee Members
Jeff Jenson, PhD, ChairPhilip D. & Eleanor G. Winn Professor for Children and Youth at RiskGraduate School of Social WorkUniversity of Denver J. David Hawkins, PhDEndowed Professor of PreventionSocial Development Research GroupSchool of Social WorkUniversity of Washington Richard Catalano, PhDBartley Dobb Professor for the Study and Prevention of ViolenceSocial Development Research GroupSchool of Social WorkUniversity of Washington
Mark Fraser, PhDJohn A. Tate Distinguished Professor School of Social WorkUniversity of North Carolina-Chapel Hill
Gilbert J. Botvin, PhD Professor EmeritusDivision of Prevention and Health BehaviorDepartment of Public HealthWeill Cornell Medical CollegeCornell University Valerie Shapiro, PhDAssistant ProfessorCo-Director, Center for Prevention Research in Social WelfareSchool of Social WelfareUniversity of California-Berkeley Kimberly Bender, PhDAssociate ProfessorGraduate School of Social WorkUniversity of Denver

Principal Coalition Authors
J. David Hawkins, PhDJeffrey M. Jenson, PhDRichard Catalano, PhDMark Fraser, PhD Gilbert J. Botvin, PhDValerie Shapiro, PhDC. Hendricks Brown, PhDWilliam Beardslee, MDDavid Brent, MDLaurel K. Leslie, MD, MPH
Mary Jane Rotheram-Borus, PhDPat Shea, MSWAndy Shih, PhDElizabeth Anthony, PhDKevin P. Haggerty, PhDKimberly Bender, PhDDeborah Gorman-Smith, PhDErin Casey, PhDSusan Stone, PhD*And the Coalition for the Promotion of Behavioral Health
47

• Unleashing the Power of Prevention is published as a Discussion Paper by the National Academy of Sciences. It is available at: http://nam.edu/perspectives-2015-unleashing-the-power-of-prevention/– Motivated by work from the Institute of Medicine Forum on the Promotion of Children’s Cognitive, Affective, and Behavioral Health
• Unleashing the Power of Prevention is available at the Academy of Social Work and Social Welfare website: http://aaswsw.org/grand-challenges-initiative/

49
Coalition Partners• Unleashing the Power of Prevention has been
recognized by:– The American Academy of Social Work and Social Welfare – The National Prevention Science Coalition– The Society for Child and Family Policy and Practice– National Association of State Mental Health Program
Directors– Center for Children, Families, and Communities – Mental Health America

50
Unleashing thePower of Prevention!
Evidence, Goals, and Opportunities

51
Unleashing the Power of Prevention:10 Year Goals!
• Reduce the incidence and prevalence of behavioral health problems in the population of young people from birth through age 24 by 20%
• Reduce racial and socioeconomic disparities in behavioral health problems by 20%

52
Action Steps and Goals1. Increase public awareness of the advances and cost
savings of effective preventive interventions that promote healthy behaviors for all– Goal: In a decade, a majority of the U.S. adult population will report
that it is possible and cost-effective to prevent behavioral health problems among children and adolescents
2. Increase the percentage of all public funds that are spent on effective prevention programs– Goal: In a decade, at least 10% of all state and federal expenditures on
the education, health, protection, and welfare of children will be allocated to effective interventions for preventing behavioral health problems

53
Action Steps and Goals3. Implement capacity-building tools that guide
communities to assess and prioritize risk and protective factors, and select evidence-based prevention programs
– Goal 1: In a decade, at least 1,000 communities in the United States will actively monitor population levels of risk and protection and behavioral health problems among young people
– Goal 2: In a decade, at least 1,000 U.S. communities will implement effective health promotion approaches and evidence-based preventive interventions

54
Action Steps and Goals4. Establish criteria for preventive interventions that are
effective, sustainable, equity-enhancing, and cost-beneficial– Goal: In a decade, all 50 states will use data from controlled studies
and cost-benefit analyses to inform policy decisions regarding investments in prevention, treatment, and control of behavioral health problems
5. Increase infrastructure to support the high-quality implementation of preventive interventions– Goal: In a decade, 25 states will have cross-agency “backbone”
organizations that provide technical assistance and monitoring services to local community organizations that provide behavioral health services for youth and their families

55
Action Steps and Goals6. Monitor and increase access of children, youth, and
young adults to effective preventive interventions– Goal: In a decade, child welfare, education, health, justice, and other
agencies in 20 states will use integrated data structures that enable cross-agency monitoring of behavioral health and preventive interventions
7. Create workforce development strategies to prepare practitioners in health and human service professions for new roles in promotion and preventive interventions – Goal: In a decade, 20 universities will include cross-disciplinary,
prevention-focused training programs in behavioral health that will include primary care medicine, nursing, psychiatry, social work, and psychology

56
The Challenge
• Joining forces across disciplines and professions and working collaboratively with policymakers and practitioners will be essential to achieving these goals

57
Unleashing the Power of Prevention: Initiatives
1. Implement healthy parenting programs in primary care settings
– Collaborating with members of the Institute of Medicine Forum on Promoting Children’s Cognitive, Affective, and Behavioral Health to scale-up tested parenting programs in primary care
– Conducting a Congressional Briefing in February, 2016 on healthy parenting in primary care with members of the National Prevention Science Coalition

58
Unleashing the Power of Prevention: Initiatives
2. Collaborate with states and communities to improve the infrastructure necessary to deliver preventive interventions
– Holding a Prevention Summit with key decision makers, elected officials, and prevention specialists in Utah in December, 2015
– Working with the Colorado Results First initiative and others to create a statewide prevention coalition guided by the goals and strategies of Unleashing the Power of Prevention

59
Unleashing the Power of Prevention: Initiatives
3. Work with university departments and communities to develop a prevention workforce in social work education
– Communities in Action collaboration between the School of Social Work, University of Washington and selected Seattle communities
– The Bridge Project collaboration between the Graduate School of Social Work, University of Denver, Denver Housing Authority, and Denver Public Schools
– Curricula for preparing prevention specialists at the University of Washington, University of Denver, University of California at Berkeley, and University of Chicago

60
• Help the Coalition for the Promotion of Behavioral Health to unleash the power of prevention!
• Work Groups: Expanding the Membership Base and Reach of the Coalition
• J. David Hawkins, PhD, Chair Workforce Development: Preparing Practitioners in Social Work and
Related Disciplines for Prevention • Kimberly Bender, PhD Chair
Conveying the Message and Goals of Unleashing the Power of Prevention
• Jeff Jenson, PhD, Chair Securing Funding to Support the Infrastructure and Advance the Goals
of Unleashing the Power of Prevention • Richard Catalano, PhD, Chair
Opportunities

61
The Prevention Pay-Off!• Effective universal, selective, and indicated preventive
interventions are available at individual, school, family, and community levels of implementation
• Scale-up and widespread implementation of prevention programs are likely to produce positive changes in young people at the population level
• Many effective programs are cost-effective
We can prevent behavioral health problems in young people before they begin!!

62
Contact Information
• Jeff Jenson Ph.D., University of Denver Chair, Coalition for the Promotion of Behavioral HealthUniversity of [email protected]