Embed Size (px)
Citation preview

Behavioral Distinctions in Children with Reading Disabilities and/or ADHD
STEWART PISECCO, PH.D., DAVID B. BAKER, PH.D., PHIL A. SILVA, PH.D., O.B.E., AND MARK BROOKE, B.A.(HoNs.)
ABSTRACT
Objective: To investigate behavioral distinctions between children with reading disabilities (RD) and attention-deficit hyperactivity disorder (ADHD). Method: A four-group mixed design consisting of children with reading disabilities only (RD only), reading disabilities and ADHD (RD/ADHD), ADHD only, and a comparison group was used. Differences
between parent reports, from age 5 to 15 years, and teacher reports, from age 5 to 13 years, were examined on measures of hyperactive and antisocial behaviors. Results: The analyses indicated that, at home, children from the ADHD only and RD/ADHD groups exhibited significantly more hyperactive behaviors than children from the RD only
and comparison groups. At school, children from the RD only, ADHD only, and RD/ADHD groups typically exhibited significantly more hyperactive and antisocial behaviors than children from the comparison group. With regard to antisocial behaviors, children from the RD/ADHD group exhibited significantly more antisocial behaviors than children from any
other group. Conclusions: The results of the study indicate that children from these groups may exhibit either a “pervasive” or “situational” presentation of behavioral problems, a finding which suggests that in conducting an evalua-
tion of ADHD it is important to obtain both parent and teacher reports of problem behaviors. J. Am. Acad. Child Adolesc. Psychiatry, 1996, 35( 1 1):1477-1484. Key Words: attention-deficit hyperactivity disorder, reading disability, epidemiology.
One of the most consistent findings in the childhood psychopathology literature is that children with reading disabilities frequently present with additional psychiat- ric disorders (Hinshaw, 1992; McGee et al., 1986; Semrud-Clikeman et al., 1992; Williams et al., 1990; Williams and McGee, 1994). For instance, Williams et al. (1990) examined the relationship between risk factors and behavioral and emotional disorders in 11- year-old children and found that reading problems
Accepted April 24, 1996 Dr. Pisecco is Assistant Projssor, University o f Houston; Dr. Baker is
Associate Proj&sor, University o f North Texas: Dr. Silva is Director and Mr. Brooke is Biostatistician, Dunedin Multidisciplinary Health and Development Research Unit (DMHDRU), University of Otago Medical School, New Zealand
Dr. Pisecco’s work was compk-ted while on a Fulbright Grant hnded by the New Zealand- United States Educational Founahtion. This research was ah0 supported by grants from the NIMH (MH45070 to Terrie Mofitt and MH49414 to Avshalom Carpi). Dr. Silva and the DMHDRU are supported by the New Zealand Health Research Council. Special thanks to Terrie Mofitt, Avshalom Carpi, and anonymous reviewers for editorial comments.
Reprint requests to Dr. Pisecco, University of Houston, College of Education, Department o f Educational Psychoingy, Houston, 7X 77204-5071.
0890-8567/96/3511-1477$03.00/001996 by the American Academy of Child and Adolescent Psychiatry.
successfully predicted the coexistence of another psychi- atric disorder. Others have reported that the presence of a behavioral disorder is the most common long- term association with reading difficulties (McGee et al., 1988a). In an attempt to distinguish between the type of disruptive disorder and its association with reading difficulties, Anderson et al. (1989) failed to find a relationship between aggressive conduct disorder and poor reading. However, an association between conduct disorder and reading difficulties has been documented when conduct disorder was paired with attention-deficit hyperactivity disorder (ADHD) (McGee et al., 1988~). This has led researchers to suggest that reading disabilities are most commonly associated with ADHD. This hypothesized association has been well documented (Frick et al., 1991; Hinshaw, 1992), with conservative comorbidity estimates of ap- proximately 23% (Semrud-Clikeman et al., 1992).
The co-occurrence of ADHD and reading difficulties is so frequent that some have begun to question the nature of this relationship (Hinsaw, 1992; Jorm et al., 1986; McGee and Share, 1988; McGee et al., 1986;
J . A M . ACAD. C H I L D ADOLESC. PSYCHIATRY, 35:11, NOVEMBER 1996 1477
PISECCO ET AL
Waldie and Spreen, 1993; Williams et al., 1990, Wil- liams and McGee, 1994). For example, McGee and Share (1988) suggested that reading disorders lead to the development of ADHD behaviors. In contrast, DuPaul and Stoner (1994) noted that others have proposed that ADHD leads to the manifestation of reading difficulties. These debates typify the two most common causality hypotheses. The first is the sugges- tion that disorder A causes disorder B. The second hypothesis is that disorder B causes disorder A.
Pennington et al. (1993) put forth an additional hypothesis which suggests that in some cases disorder A could cause symptoms of disorder B to manifest without the full occurrence of disorder B. They refer to this as the phenocopy hypothesis. In an attempt to find support for their hypothesis and to identify cogni- tive distinctions between these two groups, Pennington et al. (1993) compared and contrasted the performance of various groups (i.e., reading disabilities [RD] only, ADHD only, ADHD and RD, and control groups) on two different domains. Domain A consisted of phonological processing measures and domain B con- sisted of executive functioning measures. They found that for the phonological processing domain, the RD only and RD/ADHD groups’ performance was im- paired compared with the ADHD only and control group. However, on the executive functioning measures the RD only and RD/ADHD groups’ performance was normal. In contrast, the ADHD only group performed worse on the executive measures than did the RD only and RD/ADHD groups. Since the performance of the RD/ADHD group was more consistent with the performance of the RD only group, they concluded that the ADHD symptomatology is likely secondary to the reading disability. Their results support the phenocopy hypothesis, a hypothesis which suggests that reading disorders may cause symptoms of ADHD to manifest without the development of the full syn- drome. Pennington and colleagues’ (1 993) conclusions are interesting in that they could explain the high comorbidity of ADHD symptoms in the reading dis- ability population while at the same time preserving the validity of the ADHD diagnosis. However, it should be noted that other attempts to identify such distinctions have failed (McGee et al., 1988b).
By identifying distinctions between children with reading disabilities and those with ADHD it is possible
to document the independent validity of each diagnos- tic criterion. While the majority of such attempts have focused on phonological and cognitive differences, efforts to identify other areas of distinction are also important. For instance, if ADHD is to be thought of as an independent disorder, then it would be reason- able to suggest that children with ADHD would present with different behaviors at home and school than would children with reading disabilities. However, if McGee and Share’s suggestion that reading disabilities lead to the development of ADHD-like symptoms is correct, then there would be few, if any, behavioral differences between the two groups. To determine which behav- ioral characteristics are attributable to a diagnosis of ADHD or to the presence of a reading disability, it would be important to use a four-group mixed design, with the groups consisting of children with reading disabilities only (RD only), children with reading disa- bilities and ADHD (RD/ADHD), children with ADHD only, and a comparison group. As well as including an index of ADHD symptoms, it would also be important to include an index of antisocial behaviors because children with ADHD and reading difficulties frequently exhibit such behaviors. Research specifically focused on behavioral distinctions between children with reading disabilities only, children with reading disabilities and ADHD, children with ADHD only, and a comparison group is limited.
The purpose of this study was to investigate behav- ioral distinctions, on parent and teacher reports, be- tween four groups of children (RD only, RD/ADHD, ADHD only, and a comparison group) from early childhood to mid-adolescence. O n the basis of a review of the literature, we expected the following results: (1) On parent reports, children from the RD/ADHD and ADHD only groups will exhibit significantly more ADHD and antisocial behaviors than children from the RD only and comparison groups. (2) On teacher reports, children from the RD only, RD/ADHD, and ADHD only groups will exhibit elevated levels of ADHD and antisocial behaviors than children from the comparison group.
METHOD
Subjects
Subjects were children involved in the Dunedin (New Zealand) Multidisciplinary Health and Development Study. The cohort’s
1478 J . AM. ACAD. C H I L D A D O L E S C . PSYCHIATRY, 35:11 , N O V E M B E R 1 9 9 6

BEHAVIORAL DISTl NCTIONS
history has been described by Silva (1990). The study is a longitudi- nal investigation of the health, development, and behavior of a complete cohort of consecutive births between April 1, 1972, and March 31, 1973, in Dunedin, New Zealand. Perinatal data were obtained at birth. When the children were traced for follow-up at 3 years of age, 1,039 children were deemed eligible for inclusion in the longitudinal study. Since then, follow-ups have been conducted biannually. The sample consisted of subjects predominantly of European ancestry (fewer than 2% were Polynesian) and is therefore comparable with similar white samples from other English-speaking Western cultures. McGee (1985) has compared children who were lost to the study at each age with those remaining by age 11 years and found no systematic differences in social class, IQ, or a variety of behavioral variables.
Instruments
Reading Ability. At ages 7 , 9, 11, 13, 15, and 18 years, the children completed the Burt Word Reading Test-Revised (New Zealand Council for Research in Education, 1981). The Burt Word Reading Test is a word-recognition reading test normed for New Zealand children. In format it resembles the American Wide Range Achievement Test of reading. The Burt Word Reading Test is considered a very consistent measure, with test-retest reliability coefficients ranging from .95 to .99 and internal consistency coefficients ranging from .96 to .97.
Behavior Ratings. When the children were aged 5 years their parents completed form A and when they were aged 7 years their teachers completed form B of the Rutter Child Scales (RCS) (Rutter et al., 1970). The RCS-A consists of 31 items describing three types of problem behaviors: aggressiveness, hyperactivity, and anxiety-worry. The items were coded by the parents, who described the behavior as follows: does not apply (0), applies somewhat (l) , or certainly applies (2). The a coefficients are .81 for the aggressiveness scale, .74 for the hyperactivity scale, and .59 for the anxiety-worry scale. The RCS-B consists of 26 items and covers the same areas of behaviors as the parent version and is completed in the same manner. The ci coefficients for the aggressiveness, hyperactivity, and anxiety-worry scales are .83, 3 2 , and .72, respec- tively. At ages 9 and 11, three items were included which measured additional inattentive and hyperactive behaviors (McGee et al., 1985). When the children were aged 13 years, the teachers com- pleted the RCS-B. However, when the children were aged 13 and 15 years the parents completed the Revised Behavior Problem Checklist (RBPC) (Quay and Peterson, 1987), which contains more extensive and age-appropriate items than the Rutter scales. The RBPC consists of 89 items of which 77 load on four major subscales. Each item is rated: does not apply (0), applies somewhat ( l ) , or certainly applies (2). The major subscales are Conduct Disorder, Socialized Aggression, Inattentive, and Hyperactivity. Each scale consists of 11 to 22 items, and the scales have yielded a coefficients ranging from .82 to .94. For the purposes of this study the Socialized Aggression, Inattentive, and Hyperactivity scales of the RBPC were computed to examine the occurrence of antisocial and ADHD behaviors.
Procedure
All children were categorized on the basis of their reading scores and behavioral ratings when they were 11 years old.
RD Only Group. Typically the identification of reading disorders relies on a discrepancy between the child’s reading level and ability, with ability being represented by the child‘s score on an intelligence
test (Semrud-Clikeman et al., 1992). The basic assumption that drives such an approach is best illustrated by Burt’s (1937) argument that ‘‘ . . . capacity must obviously limit content. It is impossible for a pint jug to hold more than a pint of milk and it is equally impossible for a child’s educational attainment to rise higher than his educable capacity” (p. 477). Share et al. (1989) tested that assumption and found that rates of progress and levels of achieve- ment clearly indicate that I Q does not set a limit on reading progress, even in children with extremely low IQs. They concluded that the use of I Q tests to determine achievement potential in reading appears unjustified.
Consequently, a child was considered reading-disabled if he or she obtained a reading score that was at least 1.5 standard deviations below the total ( n = 925) sample’s average reading score. In addition, children in this group did not meet the diagnostic criteria for any type of psychiatric disorder. Since we did not use the standard discrepancy approach to identify reading disability in this study, children in this group will be referred to as having a reading disability rather than a disorder.
ADHD Only. Three sources existed for the report of symptoms meeting DSM-III criteria for ADD. These sources included self- reported symptoms as assessed with the Diagnostic Interview Sched- ule for Children-Child Version (DISC-C) (Costello et al., 1982) and parent and teacher reports of inattention and hyperactivity from the Rutter scales A and B. Each child was individually interviewed by a child psychiatrist with the DISC-C. An ADHD diagnosis was made if two of the three possible reporters provided independent consensus report of all DSM-Illcriteria, if one reporter met the full criterion and another met some of the criteria, or if one reporter alone provided all symptoms to meet the diagnostic criteria (for a complete description of this method and the results see Anderson et al., 1989).
ADHD/RLI Group. Children in this group met the criteria for ADHD as described above and had a reading score that was at least 1.5 standard deviations below the mean of the sample.
Comparison Group. Children in this group did not meet the criteria for either a reading disability or ADHD and were free from any other handicapping condition.
Identification of the Groups
O n the basis of the above criteria, 43 children had ADHD. Thirty-six of those 43 subjects were male and 7 were female. As a result of the low number of females with ADHD the subsequent analyses were limited to males. Of those 36 males with ADHD, 19 were identified as reading-disabled and 17 as “normal” readers. Of the 19 subjects from the ADHD/RD group, 6 also met the criteria for either a conduct or oppositional defiant disorder. O f the 17 subjects with ADHD only, 8 also met the criteria for either a conduct or oppositional defiant disorder. Of the remaining members of the sample, 57 were reading-disabled and 269 qualified for the comparison group.
RESULTS
All raw data were transformed to Zscores, to make interscale comparisons possible. Therefore, all data presented in the tables are Z scores unless otherwise specified. All group contrasts were done using the Schefle method.
J. AM. ACAD. C H I L D A D O L E S C . PSYCHIATRY, 35:11, N O V E M B E R 1996 1479
PISECCO ET AL.
Parent Behavioral Ratings
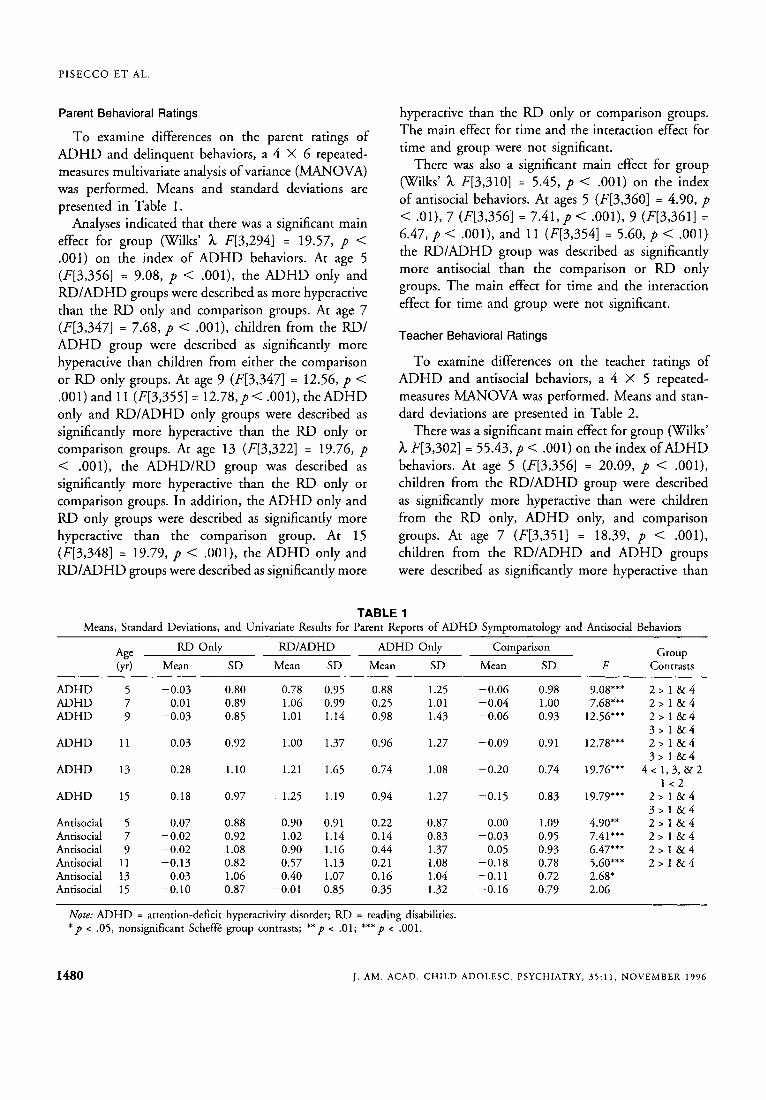
T o examine differences on the parent ratings of ADHD and delinquent behaviors, a 4 X 6 repeated- measures multivariate analysis of variance (MANOVA) was performed. Means and standard deviations are presented in Table 1.
Analyses indicated that there was a significant main effect for group (Wilks' h F[3,294] = 19.57, p < .OOl ) on the index of ADHD behaviors. At age 5 (F[3,356] = 9.08, p < .001), the ADHD only and RD/ADHD groups were described as more hyperactive than the RD only and comparison groups. At age 7 (F[3,347] = 7.68, p < .001), children from the RD/ ADHD group were described as significantly more hyperactive than children from either the comparison or RD only groups. At age 9 (F[3,347] = 12.56, p < .001) and 11 (F[3,355] = 1 2 . 7 8 , ~ < . O O l ) , the ADHD only and RD/ADHD only groups were described as significantly more hyperactive than the RD only or comparison groups. At age 13 (F[3,322] = 19.76, p < .001), the ADHD/RD group was described as significantly more hyperactive than the RD only or comparison groups. In addition, the ADHD only and RD only groups were described as significantly more hyperactive than the comparison group. At 15 (F[3,348] = 19.79, p < .001), the ADHD only and RD/ADHD groups were described as significantly more
hyperactive than the RD only or comparison groups. The main effect for time and the interaction effect for time and group were not significant.
There was also a significant main effect for group (Wilks' h F[3,310] = 5.45, p < .001) on the index of antisocial behaviors. At ages 5 (F[3,360] = 4.90, p < . O l ) , 7 (F[3,356] = 7 . 4 1 , ~ < .OOl ) , 9 (F[3,361] = 6.47, p < .001), and 11 (F[3,354] = 5.60, p < . O O l ) the RD/ADHD group was described as significantly more antisocial than the comparison or RD only groups. The main effect for time and the interaction effect for time and group were not significant.
Teacher Behavioral Ratings
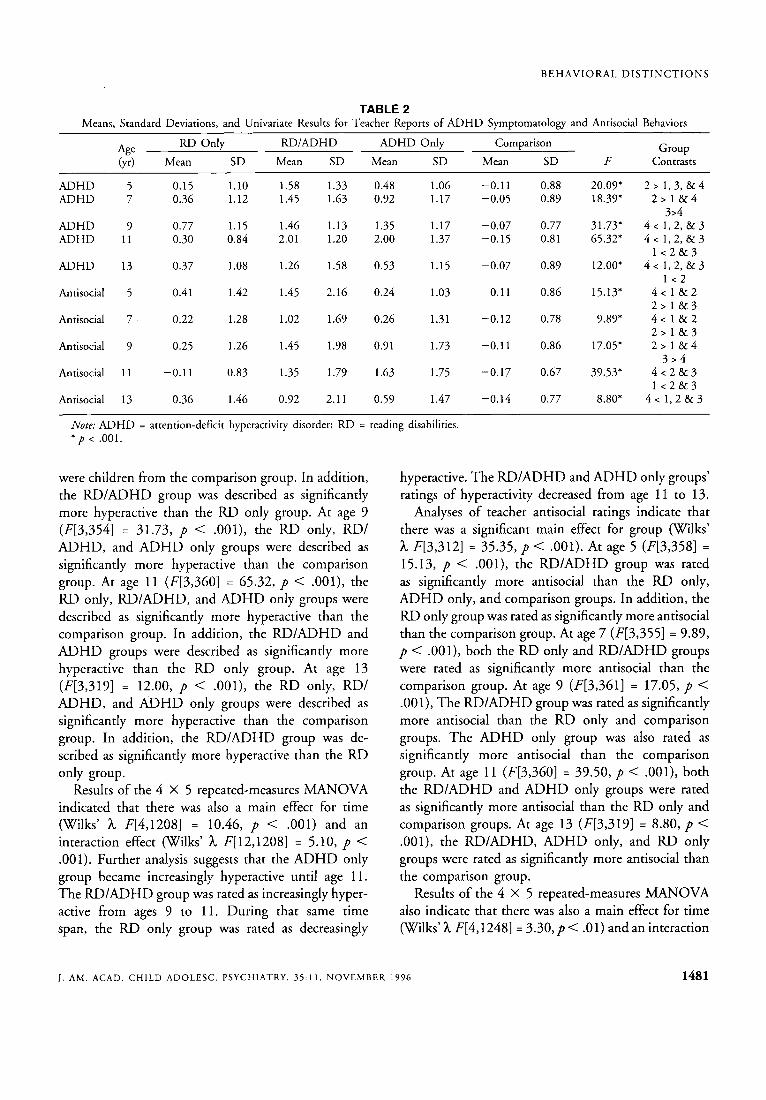
To examine differences on the teacher ratings of ADHD and antisocial behaviors, a 4 X 5 repeated- measures MANOVA was performed. Means and stan- dard deviations are presented in Table 2.
There was a significant main effect for group (Wilks' h F[3,302] = 55.43, p < .001) on the index of ADHD behaviors. At age 5 (F[3,356] = 20.09, p < . O O l ) , children from the RD/ADHD group were described as significantly more hyperactive than were children from the RD only, ADHD only, and comparison groups. At age 7 (F[3,351] = 18.39, p < .001), children from the RD/ADHD and ADHD groups were described as significantly more hyperactive than
TABLE 1 Means, Standard Deviations, and Univariate Results for Parent Reports of ADHD Symptomatology and Antisocial Behaviors
Comparison Group RD Only RD/ADHD ADHD Only Age (yr) Mean SD Mean SD Mean SD Mean SD F Contrasts
ADHD ADHD ADHD
ADHD
ADHD
ADHD
Antisocial Antisocial Antisocial Antisocial Antisocial Antisocial
5 -0.03 0.80 0.78 0.95 0.88 1.25 7 0.01 0.89 1.06 0.99 0.25 1.01 9 -0.03 0.85 1.01 1.14 0.98 1.43
11 0.03 0.92 1.00 1.37 0.96 1.27
13 0.28 1.10 1.21 1.65 0.74 1.08
15 0.18 0.97 1.25 1.19 0.94 1.27
5 0.07 0.88 0.90 0.91 0.22 0.87 7 -0.02 0.92 1.02 1.14 0.14 0.83 9 -0.02 1.08 0.90 1.16 0.44 1.37
11 -0.13 0.82 0.57 1.13 0.21 1.08 13 0.03 1.06 0.40 1.07 0.16 1.04 15 -0.10 0.87 -0.01 0.85 0.35 1.32
-0.06 -0.04 -0.06
-0.09
-0.20
-0.15
0.00 -0.03
0.05 -0.18 -0.11 -0.16
0.98 1 .oo 0.93
0.91
0.74
0.83
1.09 0.95 0.93 0.78 0.72 0.79
~~
9.08"' 7.68"'
12.56"'
12.78"'
19.76'''
19.79'''
4.90" 7.41"' 6.47"' 5.60"' 2.68' 2.06
~ ~~~ ~
2 > 1 & 4 2 > 1 & 4 2 > 1 & 4 3 > 1 & 4 2 > 1 & 4 3 > 1 & 4
4 < 1,3,&2 1 < 2
2 > 1 & 4 3 > 1 & 4 2 > 1 & 4 2 > 1 & 4 2 > 1 & 4 2 > 1 & 4
Note: ADHD = attention-deficit hyperactivity disorder; RD = reading disabilities. ' p < .05, nonsignificant Scheffk group contrasts; " p < .01; '"p < .001.
1480 J . AM. ACAD. C H I L D ADOLESC. PSYCHIATRY, 35:11 , NOVEMBER 1996
BEHAVIORAL D I S T I N C T I O N S
TABLE 2 Means, Standard Deviations, and Univariate Results for Teacher Reports of ADHD Symptomatology and Antisocial Behaviors
Group RD Only RD/ADHD ADHD Only Comparison Age (yr) Mean SD Mean SD Mean SD Mean SD F Contrasts
ADHD ADHD
ADHD ADHD
ADHD
Antisocial
Antisocial
Antisocial
Antisocial
Antisocial
5 7
9 11
13
5
7
9
11
13
0.15 1.10 1.58 0.36 1.12 1.45
0.77 1.15 1.46 0.30 0.84 2.01
0.37 1.08 1.26
0.41 1.42 1.45
0.22 1.28 1.02
0.25 1.26 1.45
-0.1 1 0.83 1.35
0.36 1.46 0.92
1.33 1.63
1.13 1.20
1.58
2.16
1.69
1.98
1.79
2.1 1
0.48 1.06 0.92 1.17
1.35 1.17 2.00 1.37
0.53 1.15
0.24 1.03
0.26 1.31
0.9 1 1.73
1.63 1.75
0.59 1.47
-0.11 -0.05
-0.07 -0.15
-0.07
-0.11
-0.12
-0.1 1
-0.17
-0.14
0.88 0.89
0.77 0.8 1
0.89
0.86
0.78
0.86
0.67
0.77
20.09' 18.39"
3 1.73* 65.32"
12.00*
15.13"
9.89'
17.05"
39.53*
8.80'
2 > 1 , 3 , & 4 2 > 1 & 4
3>4 4 < 1 , 2 , & 3 4 < 1 , 2 , & 3
1 < 2 & 3 4 < 1 , 2 , & 3
1 < 2 4 < 1 & 2 2 > 1 & 3 4 < 1 & 2 2 > 1 & 3 2 > 1 & 4
3 > 4 4 < 2 & 3 1 < 2 & 3
4 < 1 , 2 8 2 3
Note: ADHD = attention-deficit hyperactivity disorder; RD = reading disabilities. * p < .001.
were children from the comparison group. In addition, the RD/ADHD group was described as significantly more hyperactive than the RD only group. At age 9 (F[3,3541 = 31.73, p < .OOl), the RD only, RD/ ADHD, and ADHD only groups were described as significantly more hyperactive than the comparison group. At age 11 (F[3,360] = 65.32, p < .OOl), the RD only, RD/ADHD, and ADHD only groups were described as significantly more hyperactive than the comparison group. In addition, the RD/ADHD and ADHD groups were described as significantly more hyperactive than the RD only group. At age 13 (F[3,319] = 12.00, p < .OOl ) , the RD only, RD/ ADHD, and ADHD only groups were described as significantly more hyperactive than the comparison group. In addition, the RD/ADHD group was de- scribed as significantly more hyperactive than the RD only group.
Results of the 4 X 5 repeated-measures MANOVA indicated that there was also a main effect for time (Wilks' h F[4,1208] = 10.46, p < .001) and an interaction effect (Wilks' h F[12,1208] = 5.10, p < .001). Further analysis suggests that the ADHD only group became increasingly hyperactive until age 1 1. The RD/ADHD group was rated as increasingly hyper- active from ages 9 to 11. During that same time span, the RD only group was rated as decreasingly
hyperactive. The RD/ADHD and ADHD only groups' ratings of hyperactivity decreased from age 11 to 13.
Analyses of teacher antisocial ratings indicate that there was a significant main effect for group (KVilks' h F[3,312] = 35.35, p < .OOl) . At age 5 (F[3,358] =
15.13, p < .001), the RD/ADHD group was rated as significantly more antisocial than the RD only, ADHD only, and comparison groups. In addition, the RD only group was rated as significantly more antisocial than the comparison group. At age 7 (F[3,355] = 9.89, p < .001), both the RD only and RD/ADHD groups were rated as significantly more antisocial than the comparison group. At age 9 (F[3,361] = 17.05, p < .001), The RD/ADHD group was rated as significantly more antisocial than the RD only and comparison groups. The ADHD only group was also rated as significantly more antisocial than the comparison group. At age 11 (F[3,360] = 39.50, p < .OOl ) , both the RD/ADHD and ADHD only groups were rated as significantly more antisocial than the RD only and comparison groups. At age 13 (F[3,319] = 8.80, p < .OOl ) , the RD/ADHD, ADHD only, and RD only groups were rated as significantly more antisocial than the comparison group.
Results of the 4 X 5 repeated-measures MANOVA also indicate that there was also a main effect for time (Wilks' h F[4,1248] = 3 . 3 0 , ~ < . O l ) and an interaction
J. AM. ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 5 : 1 1 , N O V E M B E R 1996 1481

PISECCO ET AL.
effect (Wilks’ h F[12,1248] = 4 . 8 1 , ~ < .001). Analysis of the interaction suggests that the ADHD only group was rated as increasingly more antisocial until the age of 11. From ages 1 1 to 13, antisocial ratings for the ADHD only group decreased in severity. Antisocial ratings for the RD only group decreased in severity from ages 9 to 11. However, their antisocial ratings increased from ages 11 to 13.
DISCUSSION
The purpose of this study was to investigate behav- ioral distinctions, on parent and teacher reports of ADHD and antisocially related behaviors, between four groups of children (RD only, RD/ADHD, ADHD only, and a comparison group) from early childhood to mid-adolescence. This particular design allows for distinctions to be made between which behaviors are characteristic of a diagnosis of ADHD and which are characteristic of reading difficulties. Overall there was general support for the hypothesis that situational and pervasive groups would be identified. However, the groups of children with situational and pervasive prob- lems fluctuated as a function of the specific behavior being monitored.
O n parent reports of ADHD-related behaviors, from the ages of 5 to 15, the ratings for the RD/ADHD and ADHD only groups were typically significantly higher than those of the RD only and comparison groups. The only exceptions were at ages 7 and 13. Overall, these results suggest that the ADHD behaviors exhibited, at home, by the RD/ADHD group are primarily attributable to their ADHD diagnosis. For parent antisocial ratings, the aforementioned hypothesis was also supported. The results suggest that the antiso- cial tendencies of the RD/ADHD group are unlikely to be solely attributable to their reading difficulties or ADHD diagnosis.
The results of the analyses of intergroup differences on the teacher behavioral reports are more complex than the results of the analyses for the parent ratings. These results suggest that, for a particular group of children, reading difficulties may lead to the manifesta- tion or exacerbation of ADHD-like symptoms. In addition, it would seem that both reading disabilities and the presence of ADHD behaviors may be associated with the manifestation or exacerbation of antisocial behaviors.
Also noteworthy is the finding that at school both groups exhibited elevated levels of antisocial behaviors at varying times. One possible interpretation would be that both reading problems and ADHD may lead to the development or exacerbation of antisocial behav- iors at school but likely in reaction to different stimuli. For example, children with reading difficulties may exhibit more antisocial behaviors as a result of their inability to master academic tasks, while children with ADHD may exhibit antisocial behaviors as a result of their inattentive, impulsive, and hyperactive tendencies.
In comparing the parent and teacher reports it becomes apparent that at times the ratings are inconsis- tent. As Cohen et al. (1990) noted, in the past parent- teacher discrepancies were thought to be a function of low rating scale reliability. However, they go on to suggest that parent-teacher discrepancies are more likely a function of the heterogeneity of the population. Others have also suggested that there are likely two groups of children who present with behavioral disor- ders, a situational group and a pervasive group (Good- man and Stevenson, 1989; Schachar et al., 1981). This suggestion has clear implications for the results of this study.
For instance, one group of children exhibited the full ADHD behavioral syndrome. These children would meet a “pervasive” ADHD diagnostic criteria in that they exhibited symptomatology across a variety of situations. The pervasive presentation of symptom- atology is an important consideration in making an appropriate diagnosis (American Psychiatric Associa- tion, 1994). This group would include children from the RD/ADHD and ADHD only groups. Pennington et al. (1993) concluded that children from the RD/ ADHD group manifested ADHD symptomatology in reaction to reading problems. Their conclusion implies that these children do not exhibit the full ADHD syndrome and clashes with the results of this study.
Analyses of our behavioral data suggest that neither malady is the result of the other, but rather children from the RD/ADHD group may actually be afflicted with both conditions. These children are likely to be representative of a small subtype, who Pennington et al. (1993) referred to as possessing both disorders. That children from this group would meet a pervasive criterion is not surprising because inclusion in the ADHD group required independent consensus from two reporters.
1482 J . AM. A C A D . CHILD A D O L E S C . PSYCHIATRY, 35:11, N O V E M B E R 1996

B E H AVI 0 RAL D I S T I N C T I 0 N S
The presence of a situational group may have signifi- cant implications for both clinical practice and research. In this study children from the RD only group exhibited ADHD symptoms only at school. As mentioned, their reading difficulties may have led to the manifestation of ADHD-like symptoms. This finding would be con- sistent with past suggestions that ADHD symptomatol- ogy is often secondary to reading problems (McGee and Share, 1988) and that the presentation of ADHD- related behaviors may be affected by environmental influences (Barkley, 199 1). This has clear clinical impli- cations because a large number of children are typically referred for ADHD evaluations by their school. This finding also confirms the importance of obtaining behavioral ratings from both the child’s parents and his or her teachers and ruling out the presence of a learning problem when reporter discrepancies are noted. For researchers it is important to clarify and validate distinctions between those children who exhibit situational and those who exhibit pervasive ADHD characteristics. Research in the treatment of ADHD may especially benefit from this distinction.
Differences between a situational and pervasive pre- sentation may also be valid for the presentation of antisocial behaviors. As was mentioned earlier, the RD only and ADHD only groups exhibited elevated levels of antisocial behaviors at varying times. Such behaviors are likely a result of situational influences, as these children did not have elevated levels of antisocial behav- iors at home. As suggested, the development of such behaviors at school may be a reaction to differing demands.
In addition, there are those children, with both reading problems and ADHD, who exhibit characteris- tics of a “pervasive” behavioral disorder. This group of children would likely consist of individuals to whom Moffitt (1 993) referred as “life-course persistent delin- quents.” As mentioned earlier, their behavior is unlikely solely attributable to reading problems or ADHD. The pervasive nature of their problems would also rule out the solo influence of the school environment. Consequently, additional factors may place these chil- dren further at risk for the development of delinquency, such as neurological influences, temperament, family adversity, or other unidentified variables.
Before concluding it is important to consider the limitations of this study. The first limitation is that the sample consisted predominantly of subjects of
European ancestry. Consequently, the generalization of these findings to individuals from other ethnic minorities may be limited. Second, as with any longitu- dinal study, it is important to consider the impact of a cohort effect, which may further limit the generaliza- tion of the data. Finally, it is also important to recognize that the parent and teacher rating forms used in this study lack validity indicators. Consequently, it is impos- sible to know the absolute accuracy with which the respondents completed the forms. This limitation is one that is not unique to this study because the majority of parent and teacher forms do not have validity scales. One reassuring note in regard to this last limitation is that this particular sample has a long history of revealing personal information and in each incidence their confidentiality has never been compromised.
In conclusion, the results of this study support the hypothesis that there are behavioral distinctions between children with reading difficulties and those with ADHD. More specifically, we were able to identify a group of children who suffer from pervasive problems related to ADHD and other behavioral problems. In addition, it should be noted that there seem to be situational variables that may lead to the manifestation of symptoms related to an ADHD diagnosis and other disruptive problems. This particular finding supports McGee and Share’s (1988) suggestion that reading problems may lead to the manifestation of ADHD behaviors and Pennington and colleagues’ (1 993) phe- nocopy hypothesis. These results also highlight the need for a comprehensive evaluation that includes both parent and teacher behavioral reports when making a decision about the diagnosis of ADHD.
REFERENCES
American Psychiatric Association (1 994), Diagnostir and Statistical Manual of Mental Disorders, 4th edition (DSM-II.3. Washington, DC: American Psychiatric Association
Anderson J, Williams S, McGee R, Silva P (1989), Cognitive and social correlates of DSM-III disorders in preadolescent children. ] A m Acad Child Adolesc Psychiatry 283342-846
Barkley RA (1991), Diagnosis and assessment of attention deficit hyperactiv- ity disorder. Compr Ment Health Care 1:27-43
Burt C (1937), The Backward Child. London: University of London Press Cohen M, Becker MG, Campbell R (1990), Relationship among four
methods of assessment of children with ADHD. 1 Sch Psychol 28: 189-202
Costello A, Edelbrock C, Was R, Kessler M, Klaric SA (1982), Diagnostic Interview Schedule f . r Children (DISC; contract RFP-DB-8 1-0027). Bethesda, MD: National Institute of Mental Health
DuPaul GT, Stoner G (1994), ADHD in the Schooh: Assessment and Intervention Strategies. New York: Guilford
J . AM. ACAD. C H I L D A D O L E S C . PSYCHIATRY, 35:11, N O V E M B E R 1996 1483

P I S E C C O E T AL.
Frick PJ, Kamphaus RW, Lahey BB et al. (19911, Academic underachieve- ment and the disruptive behavior disorders. J Consult Clin Psychol 59:289-294
Goodman R, Stevenson J (1989), A twin study of hyperactivity: I . An examination of hyperactivity scores and categories derived from Rutter teacher and parent questionnaires. J Child Psychol Psychiatry 30:671-689
Hinshaw SP (1992), Externalizing behavior problems and academic under- achievement in childhood and adolescence: causal relationships and underlying mechanisms. Psychol Bull 11 1: 127-1 55
Jorm AF, Share DL, Matthews R, Maclean R (1986), Behaviour problems in specific reading retarded and general reading backward children: a longitudinal study. J Psychol Psychiatry 27:33-43
McGee R (1985), Response Rates at Phase XI of the Dunedin Multidiscipli- nary Health and Development Study. Report from the Dunedin Multi- disciplinary Health and Development Research Unit, Otago Medical School, Dunedin, New Zealand
McGee R, Share DL (1988), Attention deficit disorder-hyperactivity and academic failure: which comes first and what should be treated? J Am Acad Child Adolesc Psychiatry 27:318-325
McGee R, Share D, Mofitt TE, Williams S, Silva PA (1988a), Reading disability, behaviour problems and juvenile delinquency. In: Individual Differences in Children and Adolescents: International Research Perspectives, Saklofske D, Eysenck S, eds. London: Hodder and Stoughton, pp 158-172
McGee R, Williams S, Bradshaw J, Chapel JL, Robins A, Silva PA (1985), The Rutter scale for completion by teachers: factor structure and relationship with cognitive abilities and family adversity for a sample of New Zealand children. J Child Psychol Psychiatry 26:727-739
McGee R, Williams S, Mofitt TE, Anderson J (1988b), A comparison of 13-year-old boys with attention deficit and/or reading disorder on neuro-psychological measures. J Abnorm Child Psychol 17:37-53
McGee R, Williams S, Share DL, Anderson J, Silva PA (1986), The relationship between specific reading retardation, general reading back- wardness and behavioural problems in a large sample of Dunedin
boys: a longitudinal study from five to eleven years. J Child Psychol Psychiatry 27:597-610
McGee R, Williams S, Silva PA (1988c), Slow starters and long-term backward readers: a replication and extension. Br J Educ Psychol
Mofitt TE (1993), “Life-course-persistent” and “adolescent-limited” anti- social behavior: a developmental taxonomy. Psychol Rev 100:679-70 1
New Zealand Council for Research in Education (1981), The Burt Word Reading Test, 1981 New Zealand Revision. Wellington: Lithoprint
Pennington BF, Groisser D, Welsh MC (1993), Contrasting cognitive deficits in attention deficit hyperactivity disorder versus reading disabil- ity. Dev Psychol 29:511-523
Quay HC, Peterson DR (1987), Manualfor the Revised Behavior Problem Checklist. Coral Gables, FL: University of Miami
Rutter M, Tizard J, Whitmore K (1970), Education, Health, and Behavior. London: Longman
Schachar R, Rutter M, Smith A (1981), The characteristics of situationally and pervasively hyperactive children: implications for syndrome defini- tion. J Child Psychol Psychiany 4:375-392
Semrud-Clikeman M, Biederman J, Sprich-Buckrninister S, Lehaman BK, Faraone SV, Norman D (1992), Comorbidity between ADDH and learning disability: a review and report in a clinically referred sample. J Am Acad Child Adolesc Psychiaty 31:439-448
Share DL, McGee R, Silva PA (1989), I Q and reading progress: a test of the capacity notion of IQ. J A m Acad ChildAdolesc Psychiatry 28:97-100
Silva PA (1990), The Dunedin Multidisciplinary Health and Development Study: a fifteen year longitudinal study. Paediatr Perimt Epidzmiol 4:96-127
Waldie K, Spreen 0 (1993), The relationship between learning disabilities and persisting delinquency. J Learn Disaabil26:417-423
Williams S, Anderson J, McGee R, Silva PA (1990), Risk factors for behavioral and emotional disorder in preadolescent children. J A m Acad Child Adoksc Psychiatry 29:413-419
Williams S , McGee R (1994), Reading attainment and juvenile delinquency. J Child Psychol Psychiany 35:441-459
58:330-337
1484 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:11, NOVEMBER 1996





























