Embed Size (px)
Citation preview

Behavior of Eosinophil Leukocytes in Acute Inflammation
II. EOSINOPHIL DYNAMICSDURINGACUTEINFLAMMATION
DAVDA. BASS
From the Nuffield Department of Clinical Medicine, University of Oxford,Oxford, England
A B ST R A C r The marked diminution in the numberof circulating eosinophils, which has been shown tooccur during acute bacterial infections, is a distinctiveaspect of eosinophil physiology and of the host responseto acute infection. The mouse rendered eosinophilic byinfection with trichinosis provides a suitable model forstudy of the eosinopenic response induced by acute in-flammation. The alterations in eosinophil dynamics as-sociated with acute inflammatory reactions in trichinousmice were studied with pneumococcal abscesses, withEscherichia coli pyelonephritis, with Coxsackie viralpancreatitis, and with acute subcutaneous inflammationdue to turpentine. Each of these stimuli of acute inflam-mation markedly suppressed the eosinophilia of trichi-nosis. This suggests that the eosinopenia is a responseto the acute inflammatory process rather than the re-sponse to a specific type of pathogen.
These studies apply quantitative techniques to as-certain the effects of acute inflammation on eosinophilproduction in bone marrow and on distribution of eosino-phils in the peripheral tissues. From these observations,it is apparent that the initial response to acute inflamma-tion includes a rapid drop in numbers of circulatingeosinophils, a rapid accumulation of eosinophils at theperiphery of the inflammatory site, and an inhibition ofegress of eosinophils from the bone marrow. With pro-longation of the inflammatory process, inhibition ofeosinopoiesis occurs.
INTRODUCTION
One of the most distinctive properties of eosinophilleukocytes is the dramatic fall in the number of circu-lating eosinophils that occurs during an acute infection.
Dr. Bass was a recipient of a grant from the Common-wealth Fund. His present address is the Department of In-ternal Medicine, University of Texas Southwestern Medi-cal School, Dallas, Tex. 75235.
Received for publication 18 February 1975 and in revisedform 17 June 1975.
This eosinopenia of acute infection has been assumedto be a secondary expression of adrenal glucocorti-costeroid stimulation produced by the stress of the in-fection. Hence, the phenomenon has not been re-exam-ined since 1934, when Spink described suppression ofthe eosinophilia of trichinosis in guinea pigs withstaphylococcal, tuberculous, or trypanosomal infections(1). Recent studies from this laboratory demonstratedthat mice with trichinosis develop a reproducible eosino-philia that provides a suitable base line for the study ofeosinopenia induced by acute inflammatory processes(2, 3). The suppression of the eosinophilia of trichinosisduring pneumococcal infection was found to occur in-dependently of adrenal stimulation and in adrenalecto-mized mice (3). These studies indicated that the eosino-penia that occurs during acute infection cannot be as-cribed solely to adrenal stimulation and that it repre-sents a distinctive aspect of the host response to acuteinfection.
Previous studies demonstrated an eosinopenic re-sponse during acute bacterial infections (1-3). Thepresent studies show that acute inflammation caused byviral pancreatitis and by subcutaneous injection ofturpentine produces a similar decrease in numbers ofcirculating eosinophils.
Before undertaking studies to define the mechanismand physiologic significance of the eosinopenic responseto acute infection, it was desirable to apply currentlyavailable quantitative techniques to define further thenature of the phenomenon. The possibilities included thefollowing: (a) a peripheral sequestration of eosinophilsby localization in such sites as the inflammatory region,the draining lymph nodes, or the spleen, by diffuse in-travascular margination, or by destruction of eosino-phils; (b) a suppression of egress of mature eosino-phils from the bone marrow; and (c) a suppression ofeosinophil production. The current studies examine thesepossibilities.
The Journal of Clinical Investigation Volume 56 October 1975* 870-879870

METHODS
Unless stated, the experimental methods are the same asdescribed previously (3).
Animals. Inbred C3H/mg mice Were obtained in a
pathogen-free condition from the Medical Research CouncilLaboratory Animal Centre, Carshalton, Surrey, Englandand Scientific Agribusiness Consultants International Ltd.,Braintree, England.
Bone marrow preparation. Quantitative cell counts onfemoral bone marrow were performed by a modificationof the method of Chervenick et al. (4). The mice wereanesthetized with ether, peripheral blood was sampled, andthe mice were then killed by cervical dislocation. Bothfemurs were removed and cleaned of attached muscle.Femoral ends were removed by carefully nibbling with boneforceps until the marrow cavity was just exposed. A no. 23needle was inserted in the distal end and 2 ml of (Eagle's)minimal essential medium (MEM) I (Biocult Labs, Glas-gow, Scotland) containing 5 U of heparin/ml was forcedthrough the cavity, expelling most of the marrow as aplug. The fluid was then drawn back and forth through thefemur to remove any remaining cells. A free cell sus-
pension was made by drawing the entire sample through ano. 23 needle several times. The cells from both femurswere pooled. The total white cell count and eosinophilcount of the 2 ml of fluid were then determined as forwhole blood. The eosinophil counts were made within 20min of diluting marrow suspensions in counting fluid, assome of the immature marrow cells would not lyse. Al-though such cells were at first easily distinguished by theirsize and lack of uptake of eosin, they later absorbed enoughdye to make identification less certain. For differentialcounts, one or two drop samples of the marrow preparationwere spun in a cytocentrifuge (Shandon Ltd., London) at500 g for 5 min onto microscope slides previously acid-alco-hol cleaned. These were stained with hematoxylin andBiebrich scarlet and examined as previously described (5).
Labeling of bone marrow cells with [WH]thymidine. In-cubation with [PH]thymidine in vitro provided an indicationof the number of marrow cells synthesizing DNA (a re-flection of the "mitotic pool"). Suspensions of femoralmarrow cells were prepared as described and 10%o fetalbovine serum (Biocult Labs) was added to the medium.This technique of bone marrow preparation provided a
suspension of cells with greater than 95% viability as dem-onstrated by trypan blue exclusion. To each 2-ml marrowsuspension, 1 t&Ci of [3H]thymidine (45 Ci/mmol, TheRadiochemical Centre, Amersham, England), in 50 ul ofMEMwas added, and the samples were then incubated at370C in a water bath with gentle horizontal agitation for1 h exactly. To stop uptake of thymidine, 15 ml of coldMEMwas added to each tube, and the samples werewashed three times with 15-ml aliquots of MEMwithcentrifugation at 400 g for 10 min between washings.Finally, several cytocentrifuge preparations on microscopeslides were made from each sample as described above.These were fixed in methanol and lightly stained withHarris' hematoxylin (staining with hematoxylin beforeautoradiograph preparation reduced the chance of later lossof emulsion granules during staining). The preparationswere dipped in nuclear emulsion K2 (Millford Ltd., Essex,England) which had been melted at 500C and diluted 1: 1.5with distilled water. Slides were then held at 40C for 3wk in light-tight boxes. They were developed in Kodak
'Abbreviation used in this paper: MEM, minimal essen-tial medium.
D19 solution (Kodak Ltd., Hemel Hempstead, Herts.,England) and fixed with standard biosulfate hypo. Theywere then stained with Biebrich scarlet as described belowand examined on the same day. Differential counts oflabeled and unlabeled cells were made and a minimum of200 cells of the specific cell type under study was counted(500 cells in the case of the marrows from eosinophilic
mice).Pneumococcal infection. Production of a 2.5-ml subcu-
taneous air pouch and inoculation with 2 X 108 log-phasetype 3 pneumococci were performed as described previously(3). This was satisfactory for acute experiments, but sur-vival of the mice was too short for more chronic study.As observed previously in rats (6), a curtailment of bac-terial growth by sulfapyridine resulted in a balance betweenhost defenses and bacterial virulence prolonging the infec-tious process without killing the mice. A dose of 25 mgsulfapyridine (MayandBaker, Dagenham, Essex, England)was given orally under light anesthesia by means of in-tubation with a blunted no. 11 needle, beginning at 9 hafter bacterial inoculation and continuing at intervals of12 h. Mice thus treated appeared only slightly ill, ranfreely about the cage, and ate sufficiently to maintainweight. After 4 days these mice had developed a ring ofedematous, gelatinous, subcutaneous material up to 2 mminthickness that contained 4 X 10' pneumococci/g and fre-quently extended completely around the abdomen. Therewas continuous bacteremia from 18 h onward, with 10'4108organisms/ml of blood. Histologically, all organs (lung,liver, spleen, and kidney) were free of evidence of local-ized inflammatory processes or abscesses. During treatmentwith sulfapyridine, this huge bacterial load had remark-ably little apparent effect on the mice.
Reproducible cure of the pneumococcal infections wasproduced by the administration of 4-mg doses of procainepenicillin (Distaquaine G, Dista Products Ltd., Liverpool)subcutaneously at 12-h intervals for four doses.
Staphylococcal infection. Staphylococcus aureus typePS80 was supplied by Dr. Parker (Public Central HealthLaboratories, Colindale, London). This organism was storedon an agar slope at 40C. When a culture was required, itwas first grown overnight on blood agar and one colonywas inoculated into 15 ml brain-heart infusion broth andincubated at 37°C for 6 h with agitation.
Reproducible abscesses were produced by subcutaneousimplantation of small plugs of compressed cotton dust im-pregnated with staphylococci by the method of Noble (7).With an inoculum of 10' organisms, the mice developedsmall abscesses 3-6 mmin diameter which progressed over2-5 days to form a small necrotic slough of skin, abscessdrainage, and eventual healing. There were no instances ofdisseminated staphylococcal infection.
Corsackie viral pancreatitis. Coxsackie B4 virus wassupplied by Dr. D. R. Gamble (Coxsackie Reference Lab-oratory, Public Health Laboratories, Westpark Hospital,Epsom, Surrey, England) in a mouse torso suspension ofthe eighth passage of a suspension of pancreas in sucklingmice. It had a titer of 1046 LDw in newborn mice, andproduced massive necrosis of pancreatic acinar tissue. Forinfections in 7-wk-old C3H/mg mice, an intraperitoneal in-fective dose of 50 ud of a 10-' dilution was selected andproduced an active pancreatitis in all animals inoculated,with an eventual mortality of 30%o. After an incubationperiod of 8 days, the mice appeared mildly ill (ruffling offur). Mice sacrificed at this stage had multiple scatteredareas of acute pancreatic inflammation without histologicallyapparent involvement of the liver or myocardium. Deaths
Eosinophils in Acute Inflammation 871

FEV
E TX \T
Z - \EOSINOPHILS 2°0 /400- -2.0 E
ax 200 / K3 I0~~~~~~~~~z~~~~~~OIOHL/522 EO0I.PH LS
w
21 23 25DAYS of TRICHINOSIS
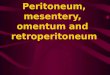
FIGURE 1 Eosinophil counts in the peripheral blood andtotal eosinophils in the femoral bone marrow in mice be-tween 21 and 27 days after oral inoculation with Trichinellaspiralis larvae (mean+LSEM). The shaded area representsthe normal range for total marrow eosinophils in C3H/mgmice.
occurred b'etween the 8th and 13th days. By the 15th day,inflammation had subsided but several mice had developedprogressive wasting and had no identifiable pancreatic tis-sue when autopsied. When the same inoculum was givento mice on the 15th day of oral trichinosis, they followeda more severe course. After 8 days the mice becameabruptly ill and 9 of 12 succumbed by the 13th day. Autop-sies demonstrated only acute pancreatic inflammation with-out involvement of the liver or myocardium; areas of acuteinflammation also existed in some parts of the perivenal fatand omental fat, presumably due to release of pancreaticenzymes.
Splenectomyt. After anesthetizing with Nembutal, theabdomen was opened anteriorly. A cotton wool swab wasinserted and twisted gently to secure the omentum. Asthis was pulled out, the spleen followed. Splenic hilar ves-selIs and splenogastric ligament were ligated and severed.Peritoneum was closed with a 4/0 silk suture and the skinrepaired with 9-mm steel clips ( Autoclips, Clay-Adams,Inc., Parsippany, N. J.).
Histological methods. Tissues for histological studywere fixed in 10%o buffered formal saline for 24 h, washedseveral times in 70% alcohol, and processed on an auto-matic Histokinette machine for embedding. They were sec-tioned at 5 ttm. thickness, dried overnight at 45 °C, de-waxed in xylene, passed through 100, 95, and 70% alcoholand into water. They were then strained with standardEhrlich's hematoxylin. The counterstain was the followingmodification of the standard Biebrich scarlet method. Theuse of Biebrich scarlet has proven very valuable foridentification of eosinophils in tissues in most species (n.g.,see reference 5, for use in rat tissues). Mouse eosinophilsstain less well than those of other species and in thestandard method the stain is likely to be lost during thedecolorization process. The sections were stained for aminimum of 30 min in a saturated solution of water-soluble Biebrich scarlet in Strenson glycine-NaOH bufferat pH 9.2. They were very briefly washed in water, passedquickly through 70, 95, and1002o alcohol with a 1-minmaximum in each solution, and finally into xylene beforemounting. This results intentionally in somewhat inade-quate decolorization with a mild pink color remaining in
the cytoplasm of most cells, a red color to any red cellspresent, and a brilliant crimson in the granules of eosino-phils. For staining of films of cells such as marrow prepa-rations, the procedure was the same except that passagethrough alcohol was limited to a 10-s dip in 70% alcohol,quickly followed by washing with water and drying.
Basic experimental design. As discussed previously (3),a study of stimuli which induce tosinophil leukopenia re-quires the availability of a predictable and reproducibleeosinophilia as a base line to facilitate statistcal analysis ofthe changes in the leukocyte population. The second peakof eosinophilia induced by trichinosis in mice was used inmost of the experiments in the study. Migration of trichi-nella larvae from the intestinal tract occurs before andduring the first peak of eosinophilia (8). Acute inflamma-tory stimuli were superimposed after larval migration tostriated muscles, thus minimizing any possible effect onthe trichinella infection itself. The usual procedure was todetermine the animals' response on day 22 of trichinosis,at which time the eosinophil level is beginning to rise(Fig. 1). Having verified that the eosinophilic responsewas underway, the animals were randomized and the in-flammatory stimuli were applied. Experimental and controlgroups were compared on days 23 and 24 of trichinosisat the expected height of eosinophilia. This timing was also*advantageous for studying changes within the bone marrow,as the marrow eosinophils remain at a constant level dur-ing this period (Fig. 1).
RESULTS
Normal values. Normal hematological values inC3H/mg mice are shown in Table I. As has been notedpreviously, these are characterized by a low resting stateof eosinophil production, as shown in both peripheralblood and bone marrow.
Responses of peripheral blood eosinophils to inflam-matory stimuli. Coxsackie B4 pancreatitis provided amodel of viral infection characterized by predominantlyacute inflammatory response. The inoculum of Cox-sackie B4 virus that was chosen produced pancreatitisin mice after a reproducible incubation period of 7-8days. The mice were therefore inoculated on day 15 oftrichinosis, so that the anticipated peak eosinophil re-sponse would coincide with the onset of pancreatitis.Although the majority of infected mice displayed mini-mal signs of systemic illness on days 7 and 8 of theinfection, the eosinophilia of trichinosis was completelysuppressed at that time (Fig. 2).
Turpentine provided a noninfectious acute inflamma-tory stimulus. The effect of injecting 0.1 ml of turpen-tine subcutaneously on day 22 of trichinosis is shown inFig. 3. As with acute infectious processes, a dramaticfall in circulating eosinophils occurred promptly andpersisted for several days.
Studies on localization of eosinophils during eosino-penia induced by acute inflammation. The studies ofchanges in peripheral blood have shown a remarkablyrapid fall in the number of circulating eosinophils afterinduction of an acute inflammatory process. This was
872 D. A. Bass

TABLE IHematological Values in Normal C3H/mg Mice
Numberof mice Mean SD SEM
Peripheral bloodEosinophils/mm3 90 65.2 29.8 3.5Neutrophils/mm3 21 2,139 1,085 236Lymphocytes/mm3 21 4,958 2,237 488
Bone marrow: total cellsEosinophils/femur X 10-5 14 0.774 0.254 0.068Neutrophils/femur X 10-5 11 90.9 29.5 8.9
Bone marrow: [3H]thymidine labeledEosinophils/femur X 10-5 8 0.206 0.066 0.023Neutrophils/femur X 10-5 12 15.5 6.35 1.83
especially apparent in the early response to pneumococcalabscess (3). The rapidity of the fall in circulatingeosinophils suggests that a sudden peripheral sequestra-tion may be an early manifestation of acute inflammation.The site of this postulated sequestration has not beendetermined, but the most probable sites would be thespleen (9-12), the inflammatory lesion itself (13) orits draining lymph nodes (14), or diffuse intravascularmargination.
To investigate the role of the spleen, mice were sple-nectomized on day 21 of trichinosis. On day 22, theirperipheral eosinophil counts were found to be 1,480±236 eosinophils/mm8 (mean ±SEM, n = 12 mice),more than twice that of their nonsplenectomized litter-
mates. Pneumococcal abscesses were established at11:00 p.m. on day 22 of trichinosis and eosinophils werecounted 10 h later (Fig. 4). The resultant eosinopeniain the splenectomized mice, a drop from 1,497 to 24±9/mm3, was even greater than that seen for normal ani-mals studied concomitantly, i.e., from 540 to 90+15/mm3. Rather than aborting the mechanism of eosino-penia, the removal of the spleen and its store of matureeosinophils had enhanced it.
The possibility that eosinophils might be drawn intothe lymph nodes draining the site of the acute inflam-
1, 800 =
1, 600-
700
600
EE
E-
0:z
LA
500
400
300
200
100
1, 400
I
+f )Ij(8)
Saline
I
EE
-i
00cn0
L"
1, 200-
1, 000k800-
600 H'I
Coxsackie B4
, (12)
14 15 21 22 23 24 25DAYS OF TRICHINOSIS
FIGURE 2 Eosinophil counts of mice given intraperitonealCoxsackie B4 on the 15th day of trichinosis (1) (mean+SEM).
a I i n e
(8)
400h
200(6)
I22 23 24 25 26
DAYS OF TRICHINOSIS
FIGURE 3 Eosinophil counts in the peripheral blood ofmice injected subcutaneously with 0.1 ml of turpentine onday 22 of trichinosis (4^) (mean+SEM).
Eosinophils in Acute Inflammation 873

2$00
EE
0
z0^-i
CL.so
La
2P00
l,600
1,200
800
400
21 22 23
DAYS OF TRICHINOSIS
FIGURE 4 Eosinophil counts in the peripheral blood ofmice given splenectomy on day 21 (.1) and subcutaneousair-pouch injection with pneumococci or saline on day 22of trichinosis (4I) (mean±SEM).
matory process was examined histologically. Mice onday 23 of trichinosis, with a peripheral eosinophilia ofover 1,000/mm3, were given pneumococcal abscessesover the dorsal thoracic region. 8 h later, the axillarynodes were dissected and processed for staining withhematoxylin and Biebrich scarlet. There were relativelyfew eosinophils demonstrable in the nodes of the controlmice and no appreciable accumulation of eosinophilsin the nodes from the mice with the pneumococcal abscess.
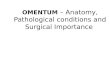
Eosinophils appeared to congregate around theperiphery of the acute inflammatory response in histo-logical sections of mice with pneumococcal abscessesor Coxsackie viral pancreatitis. However, the wide-spread nature of the pneumococcal infection and the ex-tensive but irregular involvement of the pancreas inCoxsackie pancreatitis made it difficult to quantify thisphenomenon. In contrast, subcutaneous abscess formedby a small plug of cotton dust impregnated with staphy-lococci provided a localized acute inflammatory lesionthat could be excised en bloc and subjected to moreprecise histopathological examination. Subcutaneouscotton-plug abscesses were produced in mice on day 23of trichinosis with peripheral eosinophil counts over1,000/mm3. 7 h later, the regions containing the cottonplugs were excised and processed for histological study.Sections through the abscess center were prepared witha thickness of 5 /m and stained with hematoxylin andBiebrich scarlet. It was observed that numerous eosino-phils had already accumulated at the region of the ab-scess site. To estimate the distribution of polymorphonu-clear leukocytes in several regions of the inflammatorylesion, neutrophils and eosinophils were enumerated withthe help of an eyepiece reticle that had been calibrated
with a stage micrometer and covered an area of 0.11mm2. The numbers of cells found within such areas atvarying distances from the abscess center are shown inFig. 5. The data are shown for only one tissue section,but a similar distribution was found in each of the eightabscesses examined. Immediately adjacent to the cottonplug, neutrophils and eosinophils were numerous andwere present in a ratio similar to that observed in theperipheral blood before establishing the abscesses. Theabsolute numbers of neutrophils rapidly diminished asthe distance from the abscess center increased. In con-trast, the number of eosiuophils increased at the periph-ery of the inflammatory l)rocess. In each of the eightabscesses examined, the number of eosinophils wasgreater at the periphery (2.5-3.5 mmfrom the abscess)than near the abscess center.
An estimate of the total number of eosinophils at theabscess site was derived from the above data by assum-ing that the subcutaneous abscess had the shape of a halfsphere with a concentration of eosinophils varying withdistance from the abscess center as shown in Fig. 5.Such an estimate would suggest that 7 X 106 eosinophilshad accumulated at the abscess site 7 h after inoculation.The eosinophil count of the same mouse at the time ofinoculation was 1,600/mm3, indicating a total circulatingpool of approximately 2.2 X 106 eosinophils. It appearsthat the number of eosinophils found at the abscess sitemay be sufficient to account for the initial drop in num-bers of circulating eosinophils after induction of anacute infection.
Responses of marrow eosinophils to inflammatorystimuli. As the characteristic alterations in peripheral
EOS NOPH LS
NEUTROPHLS
.. Ecs
772 63 20 18 46
j 11 10 47 I 132 288
88, 86 30 12 14
FIGURE 5 Distribution of eosinophils and neutrophils nearan abscess of 7 h duration. The cotton plug, impregnatedwith staphylococci, was inserted subcutaneously in a mousewith eosinophilia. Cell counts are for areas of 0.11 mm'.Section thickness, 5 Am.
874 D. A. Bass

blood during acute inflammation involve a reduction inthe circulating eosinophils of sudden onset but prolongedduration, possible changes in marrow might include ces-sation of egress of mature eosinophils into the blood orcessation of eosinophil production or both, or no changein production or egress of marrow eosinophils, reflectinga peripheral phenomenon. The initial studies of eosino-phil kinetics were performed with mice stimulated bytrichinosis to a stage of predictable eosinophilia so thatstatistically significant changes in eosinophil countscould be more easily documented. Quantitative techniquesfor marrow analysis were used in all experiments.
The effect of pneumococcal abscesses on total marroweosinophil populations as a function of time after pneu-mococcal infection was determined using a total of 75experimental and control mice with trichinosis (Fig. 6).The duration of the acute pneumococcal infection wasvaried by adjusting the time of bacterial inoculation sothat marrow sampling in all mice could be done at thesame time of day on either day 23 or 24 of trichinosis,thereby assuring constant marrow eosinophil counts inthe controls. The eosinophil counts of the stimulatedmarrow in these trichinous control animals were 30times the mean of counts from unstimulated mouse mar-rows. Nevertheless, during the first 36 h of acute pneu-mococcal infection, a further doubling of the total mar-row eosinophils was observed. This was followed by adecline in marrow eosinophil counts toward normallevels during the next 72 h.
The early increase in marrow eosinophils after pneu-mococcal infection could be due either to sudden cessa-tion of egress of mature eosinophils from the marrowor to a burst of eosinophil proliferation. If the phenome-non were due to an inhibition of marrow egress withresultant increase in the number of mature eosinophils,the number of eosinophils synthesizing DNAshould beunaffected. In contrast, a stimulation of eosinopoiesis
3. 0 -
2. 5 _
2. 0 _
1. 5 r
1. 0 _
0. 5
0 0.5 1 1.5 2 2.5 3 3.5
DAYS OF PNEUMOCOCCALINFECTION
FIGURE 6 Total femoral marrow eosinophilsa subcutaneous pneumococcal infection prolesulfapyridine treatment (mean±SEM). All mexamined on the 23rd or 24th day of trichino
(5) No bacterialinfection
(5) Pneumococci
4 4.5
in mice withinged duringarrows were
Isis.
25
20
W-
In
LA
W-
-CI.-
15
10
3. 0 °2
-n
2. 0 0z
-i
m
z
-
0 0.5 1 1.5 2 2.5 3
DAYS OF PNEUMOCOCCALINFECTION
FIGURE 7 Total marrow eosinophils (U) and marroweosinophils labeled in vitro with [3H] thymidine (*) inmice with pneumococcal infection prolonged by treatmentwith sulfapyridine (mean± SEM). All marrows were ex-amined on the 23rd or 24th day of trichinosis.
should be reflected by an increasing number of eosino-phils synthesizing DNA, which could be estimated bypulse-labeling with [5H]thymidine (5). The precedingexperiment with pneumococcal abscess was thereforerepeated, but in addition, uptake of [5H]thymidine bymarrow eosinophils after incubation for 1 h in vitrowith [2H]thymidine and autoradiograph preparationwas measured. The changes in total marrow eosinophilswere the same as previously observed. In contrast, thenumber of eosinophils labeled with [2H]thymidine didnot increase, but remained constant for the first 36 hand then fell rapidly toward normal levels (Fig. 7).Thus, the initial rise in marrow eosinophils was notaccompanied by increased eosinophil production, butappeared to be due to an increase in the number of non-dividing eosinophils, presumably because of reducedegress of mature cells into the blood. Inhibition of mar-row eosinophil production was a late event, and becameprominent only after the first 36 h of acute infection.
The animal with trichinosis is in an unusual state ofstimulation of eosinophil production. The induction ofan acute inflammation inhibits this process and bothmarrow eosinophil production and total marrow eosino-phil counts declined toward normal. To study the effect
Eosinophilis in Acute Inflammation 875
2w=D
xCL0FV)0
3cCc0w-C
_ Elf-

(8)
/ \ / T~~OTALg w ~~~~~EOSNOPH LS
[3H]THYMIDINE- %x.LABELED EOSINOPHILS + (8)
0 1 2 3
DAYS OF PNEUMOCOCCALINFECTION
TOTALNEUTROPHLS
4
(8)
(8) _
NEUTROPH LS
0 1 2 3 4
DAYS OF PNEUMOCOCCALABSCESS
FIGURE 8 Total and [3H] thymidine-labeled eosinneutrophils in normal mice with pneumococcalprolonged by treatment with sulfapyridine (mea
of turpentine provide an opportunity to test whether ornot the events observed in the marrow occur after otherinflammatory stimuli. Mice were studied on day 23 or
0.4 24 of trichinosis and the interval between inoculation ofthe acute inflammatory agent and sampling of the bone
0. 30 < 2 marrow was varied as in the previous experiments.L !t Pyelonephritis was induced by unilateral ureteral liga-
0.20 ° I tion and immediate intrarenal inoculation of 105 E. colias described previously (3). The initial rise in marrow
^ eosinophils varied in magnitude with the different in-flammatory stimuli (Fig. 9). The height of this transientrise was most marked with pneumococcal infection,moderate with E. coli pyelonephritis, and negligible withturpentine injection. Nevertheless, all were sufficientlypowerful stimuli of acute inflammation to bring aboutmarked depression of eosinopoiesis within 3 days.
Resumption of eosinophilia after cessation of acuteinflammation. To determine whether or not the sup-
= pression of eosinophilia by inflammation is reversible,25 . the effects of penicillin therapy on eosinophil responses
! to pneumococcal infection were studied. Pneumococcalair-pouch abscesses were established in mice on day 22
5 E of trichinosis. Six groups of mice were used so that no
~ animal would have its blood sampled more frequentlyj.I, ~ than at 18-h intervals. The first of four injections of
5 Z penicillin was administered 12 h after infection (Fig.10). The eosinophil levels continued to fall during thefirst 6 h of therapy, but then rose over the next 6 htoward the level of the uninfected controls. Thus, the
ophils and suppressive effects of acute inflammation on the eosino-infection philia of trichinosis is rapidly reversible when the in-
Ln+SEM). flammatory stimulus is removed.
of acute pneumococcal infection on unstimulated mar-
row, experiments were performed exactly as before, ex-
cept that nontrichinous mice free of previous inflamma-tory or hypersensitivity processes were used. Both thetotal marrow eosinophil counts and eosinophil mitoticpool were studied simultaneously (Fig. 8). A transientrise in total marrow eosinophils was observed duringthe 24 h after infection. This was accompanied by a
brief but significant increase in the population of eosino-phils synthesizing DNA (P < 0.05), and this early in-crease in dividing eosinophils was comparable to thesimultaneous early increase in neutrophil production(Fig. 8). After this brief stimulation, however, theeosinophil production declined to less than 40% of"resting" control levels, although the total marrow
eosinophil counts gradually increased. This accumulationof nondividing eosinophils may reflect greater inhibitionof egress than of production of marrow eosinophils.
The preceding experiments on marrow eosinophilchanges were all performed with the test system ofsubcutaneous pneumococcal abscess. The models ofacute E. coli pyelonephritis and subcutaneous injection
0
I
x
LJ
-.
z
V10
LA
CK
tY
3. 0
2. 5
2. 0
1. 5
1. 0
0. 5
0 1 1.5 2 2.5 3 3.5
DAYS OF ACUTE INFLAMMATION
FIGURE 9 Total marrow eosinophils in mice with trichino-sis subjected to prolonged pneumococcal infection (0),E. coli pyelonephritis (A), subcutaneous turpentine (*),or subcutaneous saline ([]). Marrows were all examinedon the 23rd or 24th day of trichinosis. Each point is themean of five to eight mice.
876 D. A. Bass
1.50 -
1.25 [-
1. 00 H
0. 75 H
0.50 [
0. 25
100 r-
75 [-
50 V
25 F
I'C.
cx
IEw
.tLA
m0-0
Ln0
3.1
0,x
I.-
2
-1, C,
Ix
w
.tLA
wC-)
a-0
M
z
:3.0CyI=
0

Pneumococcus
,Penclci
EEE-.
CL0z
0
9 a.m. 9 a.m. 9 a.m. 9 a.m.22 23 24 25
DAYS OF TRICHINOSIS
FIGURE 10 Resumption of eosinophilia with cure of thepneumococcal infection (mean±SEM). Mice on day 22 oftrichinosis given pneumococcal abscess. Penicillin adminis-tered 12 h later. Eosinophil changes in controls due to di-urnal variation.
DISCUSSION
These experiments have again confirmed that an acuteinflammatory process may obliterate a high eosinophiliawith a rapid return of eosinophil counts into the normalrange. The eosinopenic responses to pneumococcal ab-scess and to E. coli pyelonephritis (3) and to Cox-sackie viral pancreatitis demonstrate that the effect isnot due to infection with a specific pathogen or to theelaboration of any known toxin. The effect of turpentinesuggests that it is not dependent on infection by a liv-ing organism. The one common element in the severalmodels examined appears to be the host response, theacute inflammatory reaction and the systemic reactionsinduced by it.
The eosinopenic response to acute inflammation is re-markably rapid. The induction of a subcutaneous pneu-mococcal abscess was observed to produce an 80% fall inthe peripheral eosinophil counts within 6 h (3). Aftersplenectomy, the eosinopenic response was even moredramatic, the peripheral eosinophil counts falling morethan 98% in 10 h. Although the blood transit time of
eosinophils is not known for the mouse, studies in therat have demonstrated it to be between 6.6 and 19.2 h(12, 15). Unless the blood transit half-life of theeosinophil in the mouse is remarkably rapid, the possi-bility that the rapid onset of peripheral eosinopenia isdue solely to a blockade of bone marrow egress ofeosinophils appears untenable. Alternatives would beperipheral intravascular margination of eosinophils or arapid mobilization of these cells into peripheral tissuesduring the response to acute inflammation.
The purpose of the study of eosinophil changes inperipheral tissues was to observe such possible sites ofearly localization of eosinophils. The spleen is thoughtto act as a storage site for eosinophils (9-11) and cancontract after epinephrine administration to releaseeosinophils into the circulation. Spry (12), while study-ing rat eosinophil kinetics, found that eosinophils ap-peared to lodge in the spleen for a final period of matu-ration before progressing on to the tissues. The rapideosinopenic response occurring in animals with splenec-tomy suggests that the spleen, rather than providing asite of sequestration during acute inflammation, probablyreleases eosinophils during the process and helps todampen the effect of acute inflammation. Eosinophils areknown to enter an area of inflammation in a mannersimilar to that of neutrophils (13). The large numbersof eosinophils observed in the vicinity of the acutestaphylococcal abscess may be sufficient to explain therapid decline in the numbers of these cells in the periph-eral circulation.
The observation that eosinophils collect at the periph-ery of the inflammatory process is compatible with previ-ous histological studies of acute (16, 17) and granulo-matous (18, 19) inflammation. Steele and Wilhelm (17)in a study of chemically induced inflammation observedthat, "compared with the neutrophils, eosinophils havea tendency to accumulate rather deeper in the dermis(than the neutrophils) and further from obviously dam-aged tissue. They are also more numerous in the lateralborders of the lesion as though they were spectators ofthe struggles of the neutrophils rather than participants."Both eosinophils and neutrophils emigrate into the vi-cinity of an inflammatory stimulus by diapedesis (13).The peripheral concentration of eosinophils and centralconcentration of neutrophils in abscesses might be ex-plained in part by a more sluggish response of eosino-phils to neutrophil chemotactic agents (20). This hy-pothesis suggests that neutrophils move rapidly to theinflammatory center, perform their function and becomeless motile (21, 22) or die, therefore accumulating atthe abscess center. In contrast, eosinophils move moreslowly toward the chemotactic stimuli at the abscess.Moreover, those found there do not display partial de-granulation or histological signs of dying, and may be
Eosinophi1i- in Acute Inflammation 877
ii I I |,Xn/x,/z/////Za

able to continue their random motility without accumu-lating in large numbers at the abscess center. If this hy-pothesis were true, a relatively even dispersion of eo-sinophils throughout the inflammatory region would beexpected. In fact, however, the greatest concentration ofeosinophils occurred 2.5-3.5 mmfrom abscesses of onlya 0.4-mm radius and was peripheral to the capillariesnearest the abscess. This quantitative increase in eosino-phils distal to the site of initial emigration of inflamma-tory cells suggests that the eosinophils are specificallyattracted to the periphery of the inflammatory process.Although several substances have been described thatare chemotactic for eosinophils, none has been shownto be responsible for such a localization of eosinophilsaway from the center of the inflammatory stimulus.
Eosinophils have recently been found to produce asubstance which inhibits histamine release by basophils(23) and also to produce an arylsulphatase that inacti-vates slow-reacting substance of anaphylaxis (24). Theneutralization of these well-characterized mediators ofinflammation as well as the localization of eosinophilsin the periphery of the inflammatory process stronglysupport a teleological speculation proposed in 1914 (18):the eosinophil serves a homeostatic function by inacti-vating byproducts of inflammation or by reducing sensi-tivity to further inflammatory stimuli, thus helping tocontain the inflammatory process.
The initial bone marrow-eosinophil response to acuteinflammation involved an increase in total numbers ofmarrow eosinophils without an apparent concomitantincrease in eosinophil production. This suggests the oc-currence of an inhibition of egress of eosinophils fromthe bone marrow. The rapidity and magnitude of thisinitial increase in total marrow eosinophils appears todepend on the intensity of the acute inflammatory proc-ess and the state of stimulation to eosinopoiesis of themarrow. It did not become definite in the resting marrowuntil the 3rd and 4th days of the acute inflammation. Inthe mouse with trichinosis, the effect is dramatic duringpneumococcal infection, is appreciable during E. colipyelonephritis, and is minimal during turpentine-inducedsubcutaneous inflammation. The mechanism of this ap-parent inhibition of marrow egress is unknown. A possi-bility to be considered is that a massive release of neu-trophils from the marrow (see Fig. 7) prevents the con-comitant escape of eosinophils, but such a selective com-petition between these two cell types for the innumerablepossible points of egress from the marrow lacunae intothe blood during the early response to acute inflamma-tion seems unlikely. More probable is the interruptionof an active process, the normal stimulation for eosino-phil release, whatever that may be.
Tn the presence of acute inflammation, eosinophilproduction eventually declines in both the resting and
stimulated bone marrow. This decline could be due toany of three processes: (a) inhibition of a pre-existingstimulus to eosinophil production, (b) a direct effect ondividing eosinopllils, (c) an effect on the unrecognizableeosinophil precursors, the "stem cells," which might bediverted from eosinophil to neutrophil production. Thedata available cannot distinguish between these possiblemechanisms.
The previous observations of Morgan and Beeson(2) demonstrated a similar eventual decrease in totalmarrow eosinophils as a response to inflammation; how-ever, the early accumulation of marrow eosinophils wasnot observed during that study. This apparent discrep-ancy may be due to differences in the experimental pro-duction of pyelonephritis and the timing of marrowsampling. The earlier study delayed the inoculation ofE. coli until 24 h after ureteral ligation and consideredthis point "time zero." The first marrow samples weretaken 48 h later, which would already be somewhat intothe depressive phase of the pyelonephritis curve. Fur-thermore, the preceding surgery may have caused suffi-cient stress and inflammation to initiate the chain ofevents of eosinopenia. Although returning to prior levelsin the controls, the marrow events would be maintainedby the pyelonephritis. The first marrow samples, 72 hafter laparotomy, would thereby be well into the de-pressive phase of marrow activity.
The cure of the pneumococcal abscess with penicillindemonstrated that the mechanisms involved in the pro-duction of eosinopenia of acute inflammation are rapidlyreversible with the cessation of the acute inflammatoryresponse. It is noteworthy that there was no suggestionof eosinophil destruction during any of the experimentsof this study nor in histological studies of the effects ofacute infection on the eosinophilic granuloma, to be re-ported at a later time.
ACKNOWLEDGMENTSI gratefully acknowledge the guidance of Professor Paul B.Beeson, who directed this study. I thank Miss Sarah Daviesfor excellent technical assistance.
This work was supported by a grant from the MedicalResearch Council.
REFERENCES1. Spink, W. W. 1934. Effects of vaccines and bacterial
and parasitic infections on eosinophilia in trichinous ani-mals. Arch. Intern. Med. 54: 805-817.
2. Morgan, J. E., and P. B. Beeson. 1971. Experimentalobservations on the eosinopenia induced by acute infec-tion. Br. J. Exp. Pathol. 52: 214-220.
3. Bass, D. A. 1975. Behavior of eosinophil leukocytes inacute inflammation. I. Lack of dependence on adrenalfunction. J. Clin. Invest. 55: 1229-1236.
4. Chervenick, P. A., D. R. Boggs, J. C. Marsh, G. E.Cartwright, and M. M. Wintrobe. 1968. Quantitative
878 D. A. Bass

studies of blood and bonie marrow neutrophils in nor-mial miice Atm. J. Phvsiol. 215: 353-360.
5. Spry, C. J. F. 1971. Mechanism of eosinophilia. V.Kinetics of normal and accelerated eosinopoiesis. CellTissue Kinet. 4: 351-364.
6. Wood, W. B., Jr., and E. N. Irons. 1946. Studies onthe mechanism of recovery in pneumococcal pneumonia.II. The effect of sulphonamide therapy upon the pul-monary lesion of experimental pneumonia. J. Exp. Med.84: 365-376 + plates 11-14.
7. Noble, W. C. 1965. The production of subcutaneousstaphylococcal skin lesions in mice. Br. J. Exp. Pathol.46: 254-262.
8. Walls, R. S., R. L. Carter, E. Leuchars, and A. J. S.Davies. 1973. The immunol)athology of trichinosis inT-cell deficient mice. Clin. Exp. Inimitnol. 13: 231-242.
9. McDermott, W. V., E. G. Fry, J. R. Brobeck, and C.N. H. Long. 1950. Mechanism of control of adreno-corticotrophic hormone. Yale J. Biol. Med. 23: 52-66.
10. Dury, A. 1950. Leukocyte picture of the rat: relation ofadrenal and spleen. Am. J. Physiol. 160: 75-82.
11. Schweizer, M. 1953. Alterations in the white blood cellpicture in normal, hypophysectomized and splenecto-mized guinea pigs during mild stress and following epi-nephrine injection. Enidocrinology. 53: 293-300.
12. Spry, C. J. F. 1971. Mechanism of eosinophilia. VI.Eosinophil mobilization. Cell Tisste Kinet. 4: 365-374.
13. Marchesi, V. T., and H. W. Florey. 1960. Electronmicrographic observations on the 'emigration of leuko-cytes. Q. J. Exp. Physiol. Cogn. Med. Sci. 45: 343-348 + Figs. 1-28.
14. Litt, M. 1964. Eosinophils and antigen-antibody reac-tions. Ann. N. Y. Acad. Sci. 116: 964-985.
15. Foot, E. C. 1965. Eosinophil turnover in the normalrat. Br. J. Ilaceiatol. 11: 439-445.
16. Glaser, R. J., and W. B. Wood, Jr. 1951. Patlhogeniesisof streptococcal pneumonia in the rat. Arch. Pathol. 52:244-252.
17. Steele, R. H., and D. L. Wilhelm. 1970. The inflamma-tory reaction in chemical injury. III. Leukocytosis andother histological changes induced by superficial injury.Br. J. Exp. Pathol. 51: 265-279.
18. Schwartz, E. 1914. Die Lehre von der allgemeinen und5rtlichen Eosinophilie. Ergeb. Allg. Pathol. Pathol.Anat. 17: 137-787.
19. Boyer, M. H., C. J. F. Spry, P. B. Beeson, and W. H.Sheldon. 1971. Mechanism of cosinophilia. IV. Thepulmonary lesion resulting from intravenous injectionof Trichinella spiralis. Yale J. Biol. Med. 43: 351-357.
20. Ward, P. A. 1969. Chemotaxis of human eosinophils.Am. J. Pathol. 54: 121-128.
21. Bryant, R. E., R. M. Des Prez, and D. E. Rogers.1967. Studies on human leukocyte motility. II. Effectsof bacterial endotoxin on leukocyte migration, adhesive-ness and aggregation. Yale J. Biol. Med. 40: 192-204.
22. Williams, K. E., and M. N-I. Walters. 1968. Inhibitionof leukocytic emigration after phagocytosis. J. Pathol.Bacteriol. 95: 167-174.
23. Hubscher, T. 1975. Role of the eosinophil in allergicreactions. I. EDI-an eosinophil-derived inhibitor ofhistamine release. J. Immunol. 114: 1379-1388.
24. Wasserman, S. I., E. J. Goetzl, and K. F. Austen. 1975.Inactivation of slow reacting substance of anaphylaxisby human eosinophil arylsulphatase. J. Imiimuol. 114:645-649.
Eo.sitophils in Acute Inflammation 879