Embed Size (px)
Citation preview

I
“A STUDY TO EVALUATE THE EFFECTIVENESS OF
BEHAVIOR CHANGE COMMUNICATION ON KNOWLEDGE
AND PRACTICE REGARDING PREVENTION OF STROKE
AMONG EARLY DETECTED HYPERTENSIVE PATIENTS
ATTENDING OPD’S AT TERTIARY CARE HOSPITAL,
DHARWAD”.
BY
Ms. KOTAPURI. PRATHYUSHA
DISSERTATION
Submitted to
SHRI DHARMASTHALA MANJUNATHESWARA UNIVERSITY,
DHARWAD, KARNATAKA
In partial fulfillment of the requirements for the degree of
MASTER OF SCIENCES IN MEDICAL SURGICAL NURSING
Under the Guidance of
MRS. RENUKA.BAGEWADI M.Sc(N)
Assistant Professor, Medical-Surgical Nursing
SDM UNIVERSITY Institute of Nursing Sciences
Dharwad-580009
Karnataka, INDIA.
2021

II

III

IV
V

VI
Dedicated to my beloved
Late Ms. Munigeti. Steffy Debora
You’re always remembered

VII
ACKNOWLEDGEMENT
I take this opportunity to put down on paper, my gratitude to numerous people who
stood by my side, guiding, helping and encouraging me in this achievement.
First and foremost I thank the Lord Almighty for the abundant mercy and continuous
grace showered upon me to complete this study successfully.
I owe my philosophical honor to Poojya Shri D. Veerendra Heggadeji , Chancellor,
SDM University Dharwad, for giving me this opportunity to undertake this study in
this esteemed Institution.
I convey my deepest thanks Dr. Niranjan Kumar, Vice-Chancellor SDM Hospital
Dharwad for giving me this opportunity to undertake this study.
It‟s my immense pleasure and privilege to express my deep sense of gratitude to
Prof. David. A. Kola M.Sc (N) SDMU IONS, for his inspiration, motivation, constant
guidance, valuable suggestions whose enthusiasm and guidance inspired me to work
tirelessly and come up with the best results. My mentor, whose keen interest in giving
the best to his Students, indeed blessed to be guided by him.
I‟m extremely grateful to my guide. It gives me immense pleasure in extending my
heartfelt thanks to Mrs. Renuka. Bagewadi M.Sc (N) ,Assistant Professor, Medical
Surgical Nursing, SDMU for her support, encouragement, guidance, valuable
suggestions and constant support which helped me to complete the study successfully.
I convey my gratitude to my co-guide Mr. Tilak. Joshi M.Sc (N), Department of
Community Health Nursing. For his valuable guidance encouraging and helping me to
complete this study.
I express my heartfelt thanks to all my teachers of SDMIONS for their valuable
suggestions, constant support and guidance to carry out my study successfully.
I express my gratitude to Dr. Kiran. Aithal Prof & HOD, Dept. General Medicine
SDMCMSH and Dr. S. B. Javali Statistician for their guidance and suggestions in the
completion of this study.

VIII
My heartfelt thanks to Librarian Akshara Library and Library staff, Nursing office
Staff SDMUINS for providing me their timely assistance and encouragement
throughout the study.
I convey my deep sense of thanks to my Parents Mr. K. L. Nathan & Mrs. Sumathi,
Mr. P. Shyam Rao & Mrs. Annamary, for their motivation, encouragement and
support throughout my studies & enabled me to complete my study successfully.
Date: Signature of the candidate
Place: Dharwad (Ms. Kotapuri. Prathyusha)

IX
LIST OF ABBREVIATION USED
BCC - Behavior Change Communication
HTN - Hypertension
OPD‟s - Out patient department

X
ABSTRACT
Background of the study
Stroke is the second major leading cause of mortality worldwide. It is one of
the public health concerns. The incidence of stroke in general population is 154 per
1,00,000 in India. 12% of strokes occur in above 40 years. 34% of strokes occur in
people younger than 65years old. The most effective way to reduce the morbidity and
mortality in stroke is prevention by teaching.
Objectives
To assess the existing knowledge and practice of early detected hypertensive
patients regarding prevention of stroke.
To evaluate the effectiveness of BCC regarding prevention of stroke.
To find the association between pre-test knowledge and practice scores with
selected socio-demographic variables.
Methods
Conceptual framework of the study, an Integrative Model of Behavior Prediction
Fishbein. M. & Yzer. MC. (2003) was applied to Pre-experimental one group pre-test
and post-test research design using Non probability purposive sampling technique 40
early detected hypertension patients were selected. Pre-test was conducted using
structured knowledge questionnaire and practice checklist followed by intervention
(BCC) session on maintenance of positive health. On 7th day post-test was conducted
using the same tool. Results were analyzed using descriptive and inferential statistics.
Results
In the post-test majority 35(87.5%) had adequate knowledge and 2(5%)
moderate knowledge while in the pre-test 25(62.5%) had inadequate knowledge and
10(25%) had moderate knowledge. Depicted that majority 20(50%) had poor practice
in pre-test where as in post-test 31(77.5%) had practice towards maintenance of
positive health. Therefore these results proved the effectiveness of BCC on improving
knowledge and practice in prevention of stroke.

XI
Interpretation & Conclusion
The study concludes that, there was significant increase in Knowledge and practice in
maintenance of positive health. Hence, BCC is proved to be effective in bringing the
change.

XII
TABLE CONTENTS
SL.NO CONTENT PAGE NO
1 INTRODUCTION 1-4
2 OBJECTIVES 5-10
3 REVIEW OF LITERATURE 11-20
4 METHODOLOGY 21-28
5 RESULT 29-41
6 DISCUSSION 42-45
7 CONCLUSION 46-48
8 SUMMARY 49-51
9 BIBLIOGRAPHY 52-55
10 ANNEXURES 56-117

XIII
LIST OF TABLES
SL.NO TABLES PAGE NO
1 Frequency and percentage distribution according to Socio
demographic variables
30-31
2 Mean, Standard deviation and Mean percentage of Pre and
Post–test Knowledge scores
35
3 Mean, Standard deviation and Mean percentage of pre and
post -test practice scores
35
4 Levels of Knowledge scores 36
5 Levels of Practice scores 36
6 Comparison of pretest and post- test knowledge scores by
dependent „t‟ test
37
7 Comparison of pretest and post -test practice scores by
dependent „t‟ test
37
8 Association between Pre- test Knowledge with selected Socio
demographic Variables
39
9 Association between pre- test level of Practice with
demographic variables
40-41

XIV
LIST OF FIGURES
SL.NO FIGURES PAGE
NO
1 Conceptual framework of the study 11
2 Schematic representation of the research process 29
3 Comparison of pre-test and post-test knowledge score by
dependent paired „t‟ test
37
4 Depicting that post-test knowledge is higher than pretest
knowledge
37
5 Showing the percentage of post-test skill practice is higher than
pretest practice by paired „t‟ test
37
XV
LIST OF ANNEXURES
ANNEXURE CONTENT PAGE NO
1 Consent Form for the patients 55-56
2 Letter requesting Opinion & suggestion from expert
for validity of the tool
57-58
3 Content validation Certificate 59
4 Evaluation criteria checklist for validation of tool 60-62
5 Letter seeking permission 63
6 Letter seeking Research permission 64
7 List of the Experts 65
8 Structured knowledge question and knowledge practice
checklist English version
66-74
9 Lesson plan English version 75-95
10 Structured knowledge question and practice checklist
Kannada version & Lesson plan Kannada version
96-117

1
1. INTRODUCTION
“Sometimes what you don’t know can kill you,
but putting knowledge into action can save your life”
-ASH
Hypertension is a most leading cause of death among adult population, the reasons are
either these adults are unaware of their condition or negligence / non-compliance with
the treatment regimen. Assuming one day missing the medication does not impact
much on health. Not recognizing it brings many complications and sometimes leading
to morality too. Where in, Hypertension is the most important modifiable risk factor
to prevent complications such as coronary heart disease (the leading cause of death),
stroke (the second leading cause), congestive heart failure, end-stage renal disease,
and peripheral vascular disease. Therefore, Health Care Professional must not only
identify and treat patients with hypertension but also promote a healthy and
preventive strategy to decrease the prevalence of hypertension in the general
population.1
Looking into gravity of the situation health care professionals specially nurses play a
vital role in sustaining the life of this population and preventing life threatening
complications. Indian Council of Medical Research (2015) mentions that among all
complications related to Hypertension Stroke is a major cause for loss of life, limbs
and speech in India, claiming 9.3lakh cases of stroke and 6.4lakhs deaths due to
stroke among less than 45 years of age. Annually deaths as well as disability are
counted together, then India have lost 63lakhs of disability-adjusted life in 2004.
Estimate reports that 1.6million cases of stroke occurred in India annually, at least
one-third of them become disabled.2
WHO estimates (2015) suggest that by 2050, 80% stroke cases in the world would
occur in low-middle-income countries mainly India and China. This is the reason why
India has now come out with national guidelines for Stroke Management. Prepared by
Dr. Kameshwar Prasad, director of AIIMS' clinical epidemiology unit, along with
doctors from Nizam's Institute of Medical Sciences Hyderabad, Command Hospital
Lucknow and PGI Chandigarh, the guidelines cover the management of stroke from

2
onset to chronic care and focus is on patients with first stroke or recurrent strokes.
These guidelines may be used by all health professionals/ health care planners
involved in the management of the patients with stroke. The secondary objectives of
the guidelines are to identify areas of gaps in knowledge and practice stimulates
research in each area though these guidelines are available, but have not reached to
the people.2
WHO report (2009) on “Why health communication is important in public health
because there are many threats to global public health (through diseases and
environmental calamities) are rooted in human behavior . Effective communication is
vital for an orchestrated response to a public health crisis. Communication as defined
by Adler and Rodman refers to the process of human beings responding to the
symbolic behavior of other persons. The three major components: communication is
human, communication is a process and communications are symbolic highlighted.2
Hence Communication serves an instrumental role that helps acquire knowledge and
practice in fulfilling ritualistic function, it reflects individuals as members of a social
community. Health communication attempts to persuade the affected group to engage
in certain behavior through accessing information. Intervention measures to change
behaviors in the affected group in an area of concern and must be fully supported by
both the government and nongovernmental organizations.3
NEED FOR THE STUDY
“We are the Custodians of our bodies, we must take action to employee healthy
lifestyle habits to prevent, reduce and or manage disease and illness”
- Bridgette L Collins
Stroke is one of the major leading causes of death and disability worldwide. About
70% of strokes are occurring in low-middle class countries, and high blood pressure is
the main risk factor of stroke that happens due to its poor recognition of stroke
prevention methods. Furthermore over the four decades, the stroke incidence in low-
middle class countries has doubled. Even though stroke is preventable through the
simple modifiable risk factors, recent literature shows that people with hypertension
were four times more likely to have stroke than those with normal blood pressure.

3
Additionally, about 80% of people who have high blood pressure were attacked by
stroke.4
According to the World Health Organization report (2017) in Ethiopia, stroke was the
second leading cause of death. (6.23%) and it was a massive financial burden not only
for patients but also for society as a whole. Therefore equipping the public with
appropriate knowledge and practice will be the key tip in stroke prevention activities.4
Health risks are influenced by human behavior thus affecting other aspects of life. For
instance, a society that is invaded with health problems is at risk of being
underdeveloped thus the need of behavior change. Behavior change has become a
central aim of the public health and health promotion interventions, as the influence of
prevention within the health services has increased. It is a very important aspect in
health communication and issued as an intervention measure across a wide range of
health problems. Behavior change communication (BCC) is an interactive process of
any intervention with Individuals, communities and / or societies (as integrated with
an overall program) to develop communication strategies to promote positive
behaviors which are appropriate to their settings. Strategic use of communication to
promote positive health outcomes is based on proven theories and models of behavior
change.5
Behavior Change Communication is a process of working with individual through
different communication channels to promote positive health behaviors and support
them to maintain positive health behaviors taken on. Behavior change is a complex
process motivated by many factors including, a person‟s awareness of the need to
change, understanding of the benefits of such change, belief and confidence in his
ability to change. Behavior change communication employs a systematic process that
involves formative research and behavior analysis, communication planning,
implementation, and monitoring and evaluation. In addition, the audiences are
carefully segmented, messages and materials are pre-tested, and both mass media and
interpersonal channels are used to achieve defined behavioral objectives. To be
successful BCC must move people from awareness to action by motivating them to
believe that health benefits will be obtained by changing behavior and by increasing
individual‟s sense of controls over his own health behavior choices.6

4
According to Newson et al. (2013) “Behavior change is positioned as in reducing the
risk of illness and individual‟s adaption towards avoiding it”. Furthermore health
transition is influenced by determinants and behavior change for a better need.7
Milgromisist that any successful communications program aimed at changing
behavior must be grounded in theory. She further states health programs and
companion communications campaigns should find components of at least one
behavior-change theory. Most of the studies revealed that change of behavior differ
across range of factors. Individual perceptions, beliefs or emotions affect decision-
making towards behavior change. Interpersonal factors such as family influences like
social support and relationship also affects individual decision-making. Community
norms influence how people make decision regarding health issues. Structural factors
such as the economic status of the country, political climate laws enforcement and
policies also affects behavior change of an individual. Some behaviors are so tightly
woven into social norms (e.g. smoking) that an ecological approach targeting the
individual, as well as their community and broader environment, is critical.8
Descriptive study conducted on Knowledge regarding prevention of stroke in
Kottayam with a total number of (1248) people surveyed. 476(38.1%) were prevalent
in hypertension. Among the randomly selected 60 people with hypertension,
47(78.3%) of the patients had inadequate knowledge,13(21.7%) had moderate
knowledge and none of them had adequate knowledge regarding prevention of stroke.
Most of the people had poor knowledge on hypertension and prevention of stroke.
Study concluded that though there was more prevalence of hypertension and most of
them had inadequate knowledge on prevention of stroke and there is a need to make
the people aware about the complications of hypertension and its prevention aspects.9
The investigator from her personal experience during her clinical postings and review
of literatures' identified that most of the patients with hypertension admitted in
hospital were not aware of the various risk factors leading to hypertension and its
complications which could have been easily prevented. If they have adequate
knowledge about blood pressure and have a positive attitude towards blood pressure
control. Hence, the investigator felt the need to conduct a study to evaluate the
effectiveness of behavior change communication on knowledge and practice
regarding prevention of stroke among early detected hypertensive patient.

5
2. OBJECTIVES
The objective or research project summarizes what is too be achieved by the
study. This chapter deals with the objectives of the study, operational definitions and
hypothesis of the study, limitations and conceptual framework.
OBJECTIVES OF THE STUDY
To assess the existing knowledge and practice of early detected hypertensive
patients regarding prevention of stroke.
To evaluate the effectiveness of Behaviour change communication regarding
prevention of stroke.
To find the association between pre-test knowledge, practice scores and
selected socio-demographic variables.
OPERATIONAL DEFINATIONS
Behaviour Change Communication (BCC)
In this study Behavior Change Communication is a process of working with
individual through different communication channels to promote positive
health behaviors and support them to maintain positive health behaviors taken
on. Behavior change is a complex process motivated by many factors
including, a person‟s awareness of the need to change, understanding of the
benefits of such change, belief and confidence in his ability to change.
Behavior change communication employs a systematic process that involves
formative research and behavior analysis, communication planning,
implementation, and monitoring and evaluation.
Knowledge
In this study knowledge refers to bringing awareness among study subjects
regarding to the diet, drug and exercises to be practiced in maintenance of
normal level of blood pressure at any given point of time for prevention of
stroke. Further the attempt will be made by the investigator to enhance the
knowledge by subjecting them to the validated structured teaching program
delivered through the process of behaviour change communication.

6
Practice
In this study practice refers to application of gained knowledge to the
activities of daily living in controlling and maintaining normal blood pressure
by using a tool designed, developed and validated by investigator for
preventing the stroke includes
Maintenance of healthy dietary pattern.
Taking the medicine, right dose at right time as prescribed.
Doing regular physical exercises and reducing the stress as learned
through structured teaching program delivered by the investigator.
Early detected hypertensive patients
In this study, early detected hypertensive patients refers to confirmed
diagnosis of hypertension certified by physician and on treatment with in 1
year at the time of data collection.
Evaluate the effectiveness
In this study, evaluate the effectiveness refers to the statistical comparison
made between the pre and post-test knowledge and practice responses
received from study subjects to know the impact of behaviour change
communication in prevention of stroke.
HYPOTHESIS
H1: The mean post-test knowledge scores of patients with hypertension
attending OPD's will be significantly higher than the mean pre-test knowledge
scores at 0.05 level of significance.
H2: There will be significant association between pre-test knowledge scores
and selected social-demographic variables.
H3: The mean post-test practice scores of patients with hypertension attending
OPD's will be significantly higher than the mean pre-test practice scores at
0.05 level of significance.
H4: There will be significant association between pre-test practice scores and
selected social-demographic variables.

7
VARIABLES UNDER STUDY
INDEPENDENT VARIABLES: Behavioral change communication
regarding prevention of stroke among early detected hypertensive patients.
DEPENDENT VARIABLES: Knowledge and practice of hypertensive
patients regarding prevention of stroke.
LIMITATIONS
The study is conducted with sample size in a limited period considering the
selective aspects. Hence the results of the study cannot be generalized.
CONCEPTUAL FRAME WORK
The conceptual framework is the soul of every research project. It includes
more than one theory as well as concepts and empirical findings from the literatures.
It is used to show the relationship among ideas and how to relate to the research
study. It is a representation of a system, made of the composition of concepts which
are used to help people know, understand, or stimulate a subject the model represents.
Where in Nursing is the resource in the environment that can influence the health of a
person through use of the process of inquiry, caring and practice which increases the
quality of interaction.
Introduction
The conceptual framework applied to the study is by taking the concepts of
Integrative theory. The theory incorporates the elements of 3 widely used theories
(which guide the proposed study to appreciate the effect of Behavior Change
Communication Intervention). As the theory proposes that human being is the system
and is always in complex interaction and influence of the interaction directs the
system to behave accordingly.
Hypertension is not the disease. It can be controlled through lifestyle
modification and not merely by the drugs.
In the present generation more number of adults is affected by hypertension
which has mainly influenced by life styles. Hence to guide the proposed study An
Integrative Model of Behavior Prediction Fishbein, M. & Yzer, MC. (2003).
Therefore the proposed study intended to know the impact of Behavior Change
8
Communication on lifestyle modification in preventing anticipated complication
mainly the stroke.
This model consists of the following concepts which are explaining the
interrelationship between the concepts directing towards maintenance of positive
health.
Distal Variables
Behavioral beliefs and outcome valuations
Normative beliefs and motivation to comply
Efficacy beliefs
Attitudes
Perceived norms
Self-efficacy
Skills
Intention
Environmental constraints
Behavior
INPUT
In the proposed study subjects are hypertensive patients whose physiological
condition influenced by the distal variables. Such as demographics, culture, attitude,
personality and media leading to maladaptive behavior and affecting the complains.
* In this study Behavioral beliefs refers to non-adhering to the prescribed treatment
and not maintaining dietary regimen and lifestyle required for positive health.
* Normative beliefs refer to the lack of motivation, Acceptance of self and Evaluation
of self-behavior of the subjects.

9
* In this study Efficacy beliefs refers to maladaptive behavior influenced by socio
demographic variables and subjects are Inevitable towards positive thoughts and
positive health.
In the present study subjects were selected and explained regarding the
procedure thereafter informed consent was taken from the subjects, meanwhile pre-
test was conducted with the help of structured knowledge questionnaire and practice
checklist.
THROUGHPUT
With these predictions and with the help of pretest the investigator made an
attempt to identify the causes of the behavior such as
* In this study Attitudes refers to the mixed feelings of the subjects as they may
follow, decide to take medication regularly in maintaining the balance required for
positive health.
* In this study Perceived norms refers to voluntary responses towards a particular
action in maintaining healthy life.
* In this study Self efficacy refers as subjects are encouraged to take the corrective
actions to reach the goal by the investigator, peer group and family members.
Based on the findings of the input, interventions were designed, developed
related to attitudes, perceived norms & self-efficacy. Hence developed to change the
attitude in maintaining healthy behavior and follow the instructions of physician and
investigator. Meanwhile Behavior Change Communication session was conducted
and continuous contact was maintained in order to reinforce the information and clear
the doubts if any.
BCC
It refers to, giving information to the subjects regarding lifestyle modification (drug,
diet and exercise) helps to modify their behavioral beliefs, attitudes for a healthy
outcome.
One is to one ratio contact continued till the post test.
Group discussion to motivate each other.

10
Teaching by lecture cum discussion method, using AV aids (Charts,
pamphlets) regarding Hypertension and prevention of stroke.
So as to improve the knowledge and practice skills of the subjects to obtain a
better health.
Post-test will be implemented by using the same structured knowledge
questionnaire and knowledge practice checklist skill to know the impact of
behavior and effectiveness of BCC session.
* In this study Skill refers to practicing the lifestyle modification which includes drug,
diet and exercise and the practices implemented by the study subjects after the BCC
session.
* In this study Intentions refers to achieve a desired outcome treatment to maintain a
healthy lifestyle and achieve practical skills in appropriate learning experiences with
responses to clarification of doubts and subjects determination to achieve positive
health.
* In this study Environmental constraints refers to subject‟s positive attitude to elicit a
change.
OUTPUT
It refers to the study subjects gain in knowledge and practice in prevention of
stroke related to their behavior and practice towards maintaining a positive health
with complete lifestyle modification and gets acquainted in maintaining a good
quality of life by substituting negativity with positive outcome.
In this study the effectiveness of BCC session is tested by interrelated
elements such as input, throughput and output from the post test conducted.

11
Distal variables
Demographics
age
education
occupation
monthly income
type of family
diet
family history
Culture
Myths and beliefs affecting
quality of life.
Attitudes
Emotional instability
influenced by conditioned
response.
Personality
Impact of personality in
maintaince of healthy
lifestyle.
Other individual variables
Maladaptive behavior and
compliance.
Exposure to media
Influence of media and peer
group
Behavioral beliefs and
outcome valuations
-non adhering to the
prescribed treatment.
-not maintaining dietary
regimen and lifestyle
required to positive
health.
Normative beliefs and
motivation to comply
-lack of motivation
-Acceptance of self.
-Evaluation of self.
Efficacy beliefs
-Maladaptive behavior
influenced by socio
demographic variables.
-Inevitable towards
positive thoughts and
positive health.
Attitudes
-subjects may follow,
decide to take
medication regularly.
Self-efficacy
- Subject are
encouraged to take
the corrective
actions to reach the
goal.
Intention
1. To achieve a desired
outcome.
2. Treatment modalities to
follow.
3. Maintain a healthy
lifestyle.
4. Achieve practical
skills.
5. Appropriate learning
experiences in responses
to clarification of doubts.
Skills
1. Practicing the
lifestyle modification
which includes drug,
diet and exercise.
An Integrative Model of Behavior Prediction Fishbein,M. & Yzer,MC.(2003).
Environmental constraints
1. Modifying the cause.
2. Eliciting the behavior
patterns.
Behavior
1. Positive
reinforcement
towards health
with complete
lifestyle
modification.
2. Gets
acquainted in
maintaining a
good quality of
life.
3. Substitute
negativity with
positive
outcome.
INPUT THROUGHPUT
P
O
S
T
T
E
S
T
B
C
C
Perceived norms
-voluntary responses
towards a particular
action in
maintaining healthy
life.
OUTPUT
Figure- 1

12
3. REVIEW OF LITERATURE
Review of literature is the key step in the research process and comprehensive
summary of previous research studies. It helps to lay the foundation by being
supportive study. The investigator search of the existing literature and organizing as
follows under various sub sections:
a) Literature related to knowledge and practice of early detected
hypertensive patients regarding prevention of stroke.
b) Literature related to effectiveness of Behaviour change communication
regarding prevention of stroke.
c) Literature related to association between pre-test knowledge and practice
scores with selected socio-demographic variables.
a) Literature related to knowledge and practice of early detected
hypertensive patients regarding prevention of stroke.
A cross sectional study was conducted on “High blood pressure among
primary care patients with known hypertension”. This study recurred 530
completed surveys, 26% of respondents did not know that most of the time
people with high Blood pressure do not feel it. 22% either were not sure
whether anything could be done to prevent high blood pressure or believe that
there is nothing that can be done. 19% either believe taking medications will
cure high Blood pressure or not sure whether it will. 22% (95%CI 19-26) of
respondents had overall lower hypertension knowledge. The study concluded
that patients may need to be taught the difference between curing hypertension
and treating it will medications. Efforts to educate the public that lifestyle
modifications can prevent hypertension and that it usually causes no
symptoms need to continue.10
A cross- sectional study was conducted on “Knowledge, attitude and
practice of hypertension among hypertensive patients” at Puducherry, India
(October to December 2018). 200 hypertensive patients were selected as
samples. The questionnaire given consists of 16 questions on knowledge-5,
Attitude-5, Practice-6. In this study 40.5% were males and 59.5% were
females. The results revealed that74% had knowledge regarding hypertension,

13
attitude 94%, physical activity 77%, and only 9% were practicing exercise.
The study concluded that lacks of knowledge, positive attitude and practice
was observed except for practice of regular exercise.11
A cross-sectional study was conducted on “To assess knowledge,
attitude and practices regarding lifestyle risk factors in patients with
hypertension” at PIMS Jalandhar, Punjab. Samples of 200 hypertensive
patients were selected. A simple random technique is used. Out of 200 patients
110 (55%) were females, 90(45%) were males. 170 were already on
hypertensive treatment and 30 were newly diagnosed. A Pre-Experimental
One Group Pre-test Post-test research design is used. The result shows that
159 (79.5%) had knowledge about hypertension, 169 (84.5%) knew about
preventive measures. Attitude 198 (99%) were ready to take preventive
measures. Practice 137 (68.50%) have decreased salt intake. 45 (22.5%)
patients were consuming alcohol and tobacco. The study concluded there is a
need to increase awareness and generate motivation through IEC campaigns to
encourage communities to adopt a lifestyle with regular activity.12
A study conducted on (2019) “Effectiveness of hypertension
prevention program on Information among Employees” at Tamilnadu, India.
A selected of 120 samples with hypertension. Aim of the study was to prevent
hypertension by Intervention Programme through awareness regarding
lifestyle modification and maintaining normal blood pressure. Purposive
sampling technique is used. The result suggests that difference between the
pre-test and post-test knowledge score was high in paired t test (11.69) than
the table value t (118) _>3.37, p> 0.001. Significant difference between pre-
test and post-test knowledge score at 0.1%level. The study concluded that it
helps to determine the need for continuing education programme.13
A cross- sectional study conducted on “Assess the prevalence of
hypertension and knowledge regarding the prevention of stroke” at Chennai
Tamilnadu. Simple random sampling technique was used, 1248 people were
selected randomly. The result showed that out of 60 samples 47 (78.3%) has
inadequate knowledge, 13 (21.7%) has moderate knowledge and none had
adequate knowledge regarding prevention of stroke. The study concluded that
there is a need to make people aware about the complications and prevention
aspects.14

14
A comparative survey design study conducted on “Awareness and
attitude towards stroke and its prevention among hypertensive and non-
hypertensive” at Ernakulum, Kerala (2017). Non-probability convenient
sampling technique was used. 140 samples were selected out of these 70 were
hypertensive and 70 were non-hypertensive. The data collection tool consists
of structured questionnaire with awareness 20 questions; 10statements were of
attitude towards stroke and its prevention. The result shows that the awareness
score non-hypertensive (12) was relatively higher than the hypertensive (12),
similarly attitude score hypertensive people (32) were relatively higher than
(31) non-hypertensive. The study reveals that awareness regarding stroke and
prevention was average even among hypertensive hence there is a need for
education for high risk Group.15
A study conducted on “Knowledge, attitude and practice of general
population towards Hypertension at Gandhinagar Gujarat. Random sampling
technique was used. 500 were the samples selected. Validated questions were
adopted. The data collection tool consists of 20 questionnaires, of which 8
questions on knowledge, 5 on attitude and 6 questions were on practice. The
result showed that Attitude (45.2%), practice (5%) and (98%) had knowledge.
Hence, the study concluded that they had good knowledge but, poor attitude
and practice, there is a need for health education, repeated reinforcement and
motivation to bring positive change in attitude and practice.16
A cross sectional study was conducted in the age group of 30-59 years
males attending Medicine Outpatient Department in Sri Ramachandra Medical
College and Hospital, Chennai in November 2013 using an interview
schedule. Result shows that Among 100 males with hypertension, 34% were
in the age group of less than 50 years and 64% had hypertension for less than
5 years. Nearly 84% had knowledge about influence of smoking and alcohol
on hypertension and 82% had knowledge about at least 3 dietary factors which
control hypertension. About 70% of males were aware that more than 30
minutes of physical activity/day is needed to control hypertension. 89% were
physically active for more than 30 minutes/day, 72% did not consume alcohol,
89% were nonsmokers but 25% were adding extra salt in their diet and none of

15
them increased fiber intake. Study concludes that Dietary modification
practices were less among hypertensive males.17
Prospective family-based cohort study, 573 families were included
with 997 participants aged >30 years. Self-structured and standardized
questionnaire tool was used. Study results revealed that prevalence of
hypertension was 43%. Higher in women than men (43.7% vs. 41.4%). In
total, 78% (86.2% in women, 62.9% in men) were aware of their hypertension.
Among those aware, 60.4% (63.5% in women, 52.6% in men) of the
participants were on treatment, and hypertension was controlled in 75.1%
(77.5% women, 68% in men) of them treatment. Prevalence was less in
regular exercise versus those who did moderate exercise (32% vs. 45.7%) and
among nonsmokers versus smokers (42.2% vs. 46.6%). Study concludes
prevalence of hypertension in Kerala is high. Although awareness is quite
high, there is a need to improve the people with hypertension taking
treatment.18
A cross-sectional study assessed knowledge, attitude and practice of
exercise for blood pressure control among Nigerian patients with
hypertension. 150 (male, 66 and female, 84) patients with 20 years and older
participated. A structured questionnaire on socio-demographic, knowledge,
attitude and practice of exercise for blood pressure control was selected Data
were analyzed using descriptive and inferential statistics at 0.05 Alpha level.
90 (60.0%) had poor exercise practice. A majority, 101 (67.3%) had poor
knowledge of exercise, 39 (26.0%) had positive attitude towards exercise.
There were significant associations between knowledge of exercise and level
of education (28.337; p=0.001), attitude ( 38.297; p=0.001) and practice of
exercise (12.757; p=0.001) respectively. Significant association was found
between knowledge and socio-economic status (χ2=19.192; p=0.001)
and attitude (χ2=25.634; p=0.001). Study concluded Practice was low
which was significantly influenced by poor knowledge and negative attitude
towards exercise practice for blood pressure control.19

16
b) Literature related to effectiveness of Behaviour change communication
regarding prevention of stroke.
A cross-sectional study was conducted with 333 adults of
hypertension; samples were selected using multistage sampling. Interview
method was obtained with structured questionnaires. The questionnaires used
in this study included the Health-Promoting Lifestyle Profile II (HPLP II),
Hypertension Knowledge-Level Scale (HK-LS), Self-Rated Abilities for
Health Practices Scale (SRAHP), Barriers to Health-promoting Behavior
Scales (BAS), Benefits to Health-Promoting Behavior Scales (BES),
Multidimensional Scale of Perceived Social Support (MSPSS) and Situational
Influences Questionnaire (SIQ). Using multiple linear regressions data was
analyzed. Result showed that 36.9% variation in health-promoting behavior
among adults with hypertension with six variables education, knowledge, self-
efficacy, perceived barriers, social support and situational influences
(adjusted R2 = 0.369). Study concluded good-quality education will increase
the level of health-promoting behavior. Situational influences and support
from family and friends can also influence the adult's attempts to change their
health behaviour.20
A study conducted with 322 adult hypertensive participants who had
been on treatment for at least three consecutive months were randomized into
two groups. Using semi-structured questionnaire an interview and clinical
parameters were measured on pre- and post-intervention. The intervention
group was given teaching regarding lifestyle behaviors, regular exercise,
eating adequate fruits and vegetables, moderate alcohol intake and cessation of
smoking. Results shows that Post-intervention, among the intervention group
22.4%, 71.4% and 100%, as compared with the control group at 6.2%, 41.0%
and 87.6%, met recommendations for physical activity, fruit and vegetable
consumption and alcohol consumption. The difference in each category was
statistically significant (p < 0.001). However, the difference in smoking habits
between the two groups (83.9% vs. 79.5%) was not statistically significant (p
= 0.313). study concluded Lifestyle modifications had an effective treatment
modality for hypertension. It is desirable that primary care physicians devise

17
and implement clinical and public health strategies that promote and maintain
a combination of pharmacologic interventions and lifestyle modifications.21
A cross-sectional study was conducted among 205 hypertensive
patients in Durame and Nigist Elleni Mohamed Memorial General Hospitals in
Sothern Nation and Nationality People Representative (SNNPR), Using
simple random technique samples were selected. The study revealed that 56
(27.3%) of the patients practiced recommended lifestyle modifications. The
study found that age (Adjusted Odds Ratio [AOR] = 0.27, 95% Confidence
Interval [CI]:0.13-0.61), educational status (AOR = 2.00,95% CI:1.33-6.75),
monthly income (AOR = 2.46, 95% CI:1.32-4.63), years since diagnosis
(AOR = 2.48, 95%CI: 1.32-4.69), and co-morbidity (AOR = 0.28,95% CI:
0.13-0.61) were factors significantly associated with lifestyle modification
practice (p < 0.05). Study concluded lifestyle modification practices among
hypertensive patients were low in this study. Therefore, Patients should be
educated on the recommended lifestyle modifications that may help patients to
control f their blood pressure.22
A cross-sectional study was conducted with 350 participants using BP
readings from three consecutive months. Purposive technique was used with a
structured interview pretested questionnaire with components derived from the
World Health Organization. Result shows mean age was 67± 11.38 years.
Males made up 35% of the participants and BP control was achieved in 41.4%
of the patients. Only 5.1% of the participants reported adherence to all the
recommended lifestyle behaviors. Low adherence rates were reported for diet,
medication, and physical activity. Bivariate analysis showed that BP (p< 0.1).
Logistic regression analysis revealed that participants BP by 40% (AOR: 0.6;
95% CI: 0.4– 0.9).Study concluded that there was Overall, adherence to the
recommended lifestyle behaviors which are known to be effective in
controlling BP was poor. Health workers should include comprehensive health
education messages on the importance of compliance with dietary, medication,
and physical exercise recommendations when counseling patients..23
A descriptive cross sectional study design was conducted in Lumbini
Medical College Teaching Hospital (LMCTH). A total of 63 patients attending

18
Medical outpatient clinic who were diagnosed as hypertensive at least two
months before the interview were included. Data were collected from 22nd
February 2015 to 21st March 2015 by interview method using a questionnaire
consisting of a combination of structured and semi-structured questions. The
study revealed that non-vegetarian decreased from 95.2% to 74.6% after
diagnosis. Lifestyle modification criteria like amount of salt intake, smoking,
and alcohol consumption were significantly reduced whereas physical exercise
and stress reduction activity were significant increased. Study concluded
Majority of the patients has changed their lifestyle after diagnosis of
hypertension.24
A cross sectional study involving adult hypertensive patients who
presented during a medical screening exercise. Structured pre-tested
questionnaire was used for data collection with 101 individuals. Results show
that 58 (57.4%) males and 43 (42.6%) females. Mean age was 56.7±12 years
with a range of 27 to 84 years. 87.1% were unaware that regular exercise is
part of lifestyle modification while 60% are unaware of the need for
moderation of alcohol intake. More than 80% are unaware of the roles of
vegetables, fruits, unsaturated oil and reduction in diary food intake in the
control of BP. Among 88 participants with some knowledge of salt restriction,
68.2% practiced it. 8.6%, 7.5%, 32.3%, 12.9% and 6.5% of those with
knowledge of regular exercise, weight reduction, alcohol moderation, fruit
intake and cigarette smoking respectively. There was a negative correlation
between the level of practice. Study concluded Awareness level and practice
of lifestyle modification in blood pressure control among the studied cohort is
poor. Concerted strategies need to be taken to improve these.25
A cross–sectional study conducted at the Hypertensive clinic of
Murtala Muhammad Specialist Hospital, Kano, and North – Western Nigeria.
Structured pre-tested questionnaire was used for data collection with 104
participants. Questions were on socio-demographic characteristics,
knowledge, perception and practice of various lifestyle-modification
measures. Results show 51 (49%) males and 53 (51%) females. Mean age was
56 ±11.7 years, with a range of 24 to 90 years. 92% were aware that regular

19
exercise is part of lifestyle modification while 81% are aware about salt
restriction. Only 9% and 13% of the participants are aware of the roles of
unsaturated oil and reduction in diary food intake in the control of BP.
Overall, 33(31.7%) of the patients had good knowledge, 40(38.5%) average
knowledge and 31 (30%) poor knowledge. Despite the positive attitude
towards lifestyle measures, only 59(56.7%) had good adherence. Study
concluded level of knowledge and practice of lifestyle modification low.
Concerted strategies are required to increase the awareness, knowledge and
practice of the lifestyle-modification.26
A cross-sectional study among 230 patients with essential hypertension
in the Family Medicine clinic in a tertiary hospital using a structured pretested
questionnaire. Results revealed that (149; 64.8%) were educated on lifestyle
practices by health workers. Abstaining from tobacco products (230; 100%)
and drinking alcohol (230; 100%) were the most used lifestyle practices.
Dietary fruit consumption (93; 40.4%) and engagement in physical activity for
thirty minutes per day (35; 15.2%) were the least used lifestyle practices.
Study concludes alcohol consumption and tobacco products were not
practiced. Dietary fruit consumption and engagement in physical activity were
not popular lifestyle practices. It is recommended that primary care clinicians
inquire about unhealthy lifestyles during clinical consultations as well as
motivate hypertensive patients to adopt and adhere to appropriate lifestyle
modifications.27
A cross-sectional study was conducted among hypertensive patients
above 30 years of age attending O.P.D. at Sir Sunder Lal Hospital, Banaras
Hindu University. A semi- structured questionnaire was used to collect data.
Study results revealed that half (54.7%) of the patients were non-vegetarian
before diagnosis and after diagnosis the proportion of non-vegetarian study
subjects reduced by 14%. Similarly, the reduction in consumption of meat,
eggs, salt, ghee and oil (mustard, sunflower) by hypertensive patients was also
noted. Likewise, smoking and consumption of alcohol was also reduced after
diagnosis of hypertension. However physical activity increased among 30% of
the respondents. Study concludes that Most of the patients changed their

20
lifestyle after diagnosis of hypertension. There were many recommended
lifestyle changes but this study showed that even after diagnosis of
hypertension only few lifestyle changes were adopted.28
A cross-sectional study was conducted in Sikkim Manipal Institute of
Medical Sciences. Attending medicine OPD aged >18 years from Jan 1st 2017
to Jan 15th
, 2017 were selected. Semi structured questionnaire interview was
regarding knowledge of life style interventions. Study results revealed (n =
100), 60 patients had adequate knowledge (>50%) and 40 patients had
inadequate (<50%) knowledge. Significant association between educational
background and knowledge on lifestyle interventions was present. Urban
population was more aware as compared to rural population Blood pressure
was significantly under control in the aware population. Study concluded that
Patients knowledge on lifestyle interventions for the management of blood
pressure is important. The rural population and uneducated people have
inadequate knowledge on lifestyle modifications of hypertension. Structured
teaching programs are needed to improve awareness about the lifestyle
changes.29
c) Literature related to association between pre-test knowledge and practice
scores with selected socio-demographic variables.
An Interventional study conducted with 292 first visit patients with
hypertension. 142 were randomly assigned to a Control group (C) and 150 to
an Intervention group (I). 10 multiple-choice questionnaires were developed to
evaluate the effect of the intervention on lifestyle modification. Patients were
given the questionnaire, had their BP measured and drug therapy registered
before educational intervention and 12 months later. Group I patients
participated in the focus group and in the role play 2 and 4 months,
respectively, after recruitment. Group C patients received the oral
information. Main outcome measure Blood pressure values and lifestyle
modification. Results shows 150 interventional patients, 58 participated in
both focus group and role play, 30 participated only in focus group and the
remaining 62 never participated. After 12 months, BP decreased more
markedly in group I than in group C, with P < 0.001 for both. Significant

21
improvement of lifestyle modification after 12 months of follow-up
concerning some aspects in both groups. Study findings show that a
motivational approach is a powerful tool for achieving better blood pressure
control and is an essential skill 30
A study conducted with (516) patients were interviewed using a semi
structured questionnaire on patients knowledge, side effects, frequency,
medicines and life style modification. Study results revealed 193 (37%) were
males and 323 (63%) were females. 184 (36%) had middle school education.
201 (39%) were aware of side effects of medicines dispensed for the
management of hypertension whereas 490 (95%) knew the frequency of
administering anti-hypertensive medicine. The mean anti-hypertensive
knowledge score obtained was 2.6221 [SD: 1.30816] out of 5. 320 (62%) and
195 (37%) of respondents were aware of lifestyle modification such as
reducing dietary salt intake and avoiding cigarette smoking. Study concluded
Patient‟s knowledge on the administration of medicines and lifestyle practices
was average. There is the need for counseling and monitoring of hypertensive
patients with regard to their therapy (both medicines and lifestyle practices) 31

22
4. METHODOLOGY
Research methodology is a systemic way of organizing reliable data for a
problem. This chapter deals with Research approach, research design , research
setting , population, sample and sampling technique, development and description of
the tool, data collection procedure, pilot study and plan for data analysis.
RESEARCH APPROACH
Quantitative Evaluate Research Approach was used to conduct the proposed study.
RESEARCH DESIGN
Pre experimental one group Pre-test Post-test design research design was adopted.
PRE-TEST EXPERIMENT POST-TEST
O1 X O2
KEYS:
O1- Pre-test assessment of knowledge and practice regarding prevention of stroke.
X- Behavior Change Communication on knowledge and practice regarding prevention
of stroke.
O2- Post-test assessment of knowledge and practice regarding prevention of stroke.
SETTINGS: The study was conducted Medicine OPD‟s, At Tertiary care Hospital
Dharwad.
POPULATION: Hypertensive patients.
METHODS OF DATA COLLECTION
SAMPLE: 40
SAMPLING TECHNIQUE:
Non-probability purposive sampling technique was adapted to select the
samples for this proposed study.
SAMPLE SIZE:
Sample size for this proposed study was 40 hypertensive patients.

23
INCLUSION CRITERIA:
Male patients
Patients who are in the age group of 35-55 years.
Patients who are willing to participate in this study.
Early detected hypertensive patients attending OPD‟s. [who are diagnosed
with in a span of 1 year].
Patients Who can read and write either English or Kannada language.
EXCLUSION CRITERIA:
Patients who had history of stroke.
Patients who have complication (Coronary artery Disease, Renal Disease,
Peripheral vascular Disease).
SELECTION OF DEVELOP OF INSTRUMENT:
SELECTION OF TOOL
Tool is an instrument prepared by the investigator to collect the
information required to answer the questions raised in the study.
DEVELOPMENT OF THE TOOL:
A tool was designed, developed and validated by the investigator after going
through
Review of literature
Preparation of blue print
Discussion and suggestion from subject experts and guide.
DESCRIPTION OF TOOL:
o Section I : Socio-demographic Proforma
o Section II : Structured Knowledge Question
PART I : Pre- Contemplation
PART II : Contemplation
PART III : Preparation
o Section III : Practice questionnaire checklist

24
In present study structured knowledge questionnaires and practice checklist was
prepared by the investigator “Evaluate the effectiveness of behavior change
communication on knowledge and practice regarding prevention of stroke” . The tool
was further classified into following sections:
Section I: Socio-demographic Proforma
It consists of 8 items related to demographic variables of hypertensive patients
who are certified as hypertensive by the physician and on treatment with in 1 year to
the time of data collection.
Section II: Structured Knowledge Question
PART I: Pre- Contemplation
It consisted of 6 questions; these data were used to collect the data
from participants.
PART- II: Contemplation
It consists of 4 questions; these data were used to collect the data from
participants.
PART-III Preparation
Consists of 4 questions; these data were used to collect the data from
participants.
Section III: Knowledge Questionnaire Practice Checklist
It consists of 22 items; these data were used to collect the data from
participants.
SCORING AND INTERPRETATION OF KNOWLEDGE
The tool consisted of 14 items on knowledge, 22 items on practice checklist. Each
right answer carried „1‟ mark and wrong answer carried „0‟ mark. Further
categorization of the level of knowledge was done as following as

25
Inadequate knowledge 0-4
Moderate knowledge 5-9
Adequate knowledge 10-14
SCORING AND INTERPRETATION OF PRACTICE
Knowledge questionnaire practice checklist
Good 15-22
Average 7-14
Poor 0-6
CONTENT VALIDITY:
Content validity of the tool refers to the degree of which an instruments
measures, what is supposed to measure. In order to obtain content validity, prepared
instruments along with problem statement, operational definition and blue print were
submitted to 6 experts from the field of Medical Surgical Nursing department. The
experts gave their valuable suggestions. The necessary change in the tool was made
by incorporating suggestions given by experts according to the feasibility, before
conducting of pilot study.
PILOT STUDY:
Pilot study was conducted in selected Tertiary care hospital Dharwad from
08th
March 2021 to 16th
March 2021. To find out the reliability of the tool and
effectiveness of learning teaching programme in terms of enhancement of knowledge
and practice regarding prevention of stroke so as to decide their stability for the final
study. The investigator used purposive sampling technique to select the samples from
the total population. 10 samples were selected for the study and these 10 samples
were excluded for the main study.
The pre-test was administered by using structured questionnaire followed by
Behavior change communication session. After7 days, the post test was administered
by using the same structured questionnaire for evaluating the effectiveness of

26
Behavior change communication session on knowledge and practice regarding
prevention of stroke.
RELIABILITY:
Reliability of an instrument is the degree of consistency with which it
measures the attribute it is supposed to measure.
Reliability of the tool was assessed by collecting data from 10 hypertensive
patients; attending medicine OPD‟s at Tertiary care hospital Dharwad. Using (Karl
Pearson‟s correlation co-efficient) to find the internal consistency. The reliability co-
efficient of correlation of the knowledge tool was found to be r= 0.90. The reliability
co-efficient of correlation of practice tool was found to be r=0.87. Hence the tool was
found statistically reliable for the study.
Development of behavior change communication teaching program on
knowledge and practice regarding prevention of stroke among early detected
hypertensive patients
The teaching programme was designed, developed and validated based on the
review of the literature, research literature and the objectives stated in the teaching
plan.
The following steps were adopted to develop the behavior change communication
teaching programme.
Preparation of BCC teaching programme
Planning for teaching
Identification and stating of objectives in Behavioral terms
The teaching objectives were identified and written in behavioral terms depending on
the needs of the learner.
Selection of the Content
The content of Behavior change communication in prevention of stroke among
early detected hypertensive patients was selected through literature search and in
27
consultation with the guide and experts. The content was analyzed into sub topics and
they were broken down into elements.
Selection and preparation of appropriate Audio-Visual Aids
Flash cards, charts, banners, were considered appropriate to increase the
impact of teaching.
Determining Teaching and Learning Activities
Teaching and learning activities were determined well in advance and includes the
following:
Creating interest by motivation and reinforcement
Discussion
Planning to Implement the Behavior change communication teaching
programme
The time and date was planned and it was decided to implement the BCC
teaching programme.
Informing the participants
It was planned to inform the patients and was taken consent.
PROCEDURE FOR DATA COLLECTION:
The investigator was obtained permission and ethical clearance from the
Institutional Ethical Committee and from the Medicine OPD‟s Department of
Tertiary Care Hospital Dharwad.
Subjects were selected according to the Selection Criteria and were assured
the Confidentiality of the sample.
Informed written consent was obtained from all the subjects who were
participating in the study.
Subjects were selected by using Non-Probability Purposive sampling
technique.
On Day1, Pretest was done. To know the knowledge and practice regarding
prevention of stroke.

28
On the same Day1 BCC teaching was given with the help of lecture using
flash cards, charts and handouts for teaching subjects regarding prevention of
stroke.
After 7 days Post-test was conducted with the help of pre-test questionnaires
to know the effectiveness.
DATA ANALYSIS PLAN:
Data Analysis was collected by descriptive and inferential statistics.
By organizing the data on a master sheet.
Tabulation of data corresponding to the Socio-demographic variables such as
frequency, percentage, mean, standard deviation.
Paired „t‟ test was used to evaluate the effectiveness of behavior Change
Communication on knowledge and practice regarding prevention of stroke
among early detected hypertensive patients.
Chi-square test was used to find the association between Pre-test knowledge
scores and socio-demographic variables.
The findings were presented in form of graphs and tables.

29
RESEARCH PROCESS
RESEARCH APPROACH
RESEARCH DESIGN
RESEARCH SETTING
RESEARCH POPULATION
SAMPLING TECHNIQUE
SAMPLE SIZE
PRE-TEST
POST-TEST
ANALYSIS
TOOL USED FOR DATA
COLLECTION
Quantitative Evaluate Research
Pre experimental One group Pre-test Post-
test
Early Detected Hypertensive patients.
Medicine OPD‟s, of Tertiary care teaching
Hospital
Non-probability purposive sampling
technique
40
Structured knowledge questionnaires and
practice checklist
To assess the level of knowledge and
practice towards maintenance of positive
health
Pre-test data
Posttest after BCC on maintenance of
positive health
-Comparison of results of pre-test & post-
test. Descriptive & inferential statistics
Paired„t‟ test. Finding and conclusion.
STATISTICAL ANALYSIS
INTERPRETATION OF
DATA & DISCUSSION
BEHAVIOR CHANGE COMMUNICATION
Figure 2
30
5. RESULTS
This chapter deals with a logical presentation of the empirical results after
completing the data analysis. It includes tabulated results, results of hypothesis tests,
graphs and figures.
OBJECTIVES
To assess the existing knowledge and practice of early detected hypertensive
patients regarding prevention of stroke.
To evaluate the effectiveness of Behaviour change communication regarding
prevention of stroke.
To find the association between pre-test knowledge and practice scores with
selected socio-demographic variables.
HYPOTHESIS:
H1: The mean post-test knowledge scores of patients with hypertension
attending OPD's will be significantly higher than the mean pre-test knowledge
scores at 0.05 level of significance.
H2: There will be significant association between pre-test knowledge scores
and selected socio-demographic variables.
H3: The mean post-test practice scores of patients with hypertension attending
OPD's will be significantly higher than the mean pre-test practice scores at
0.05 level of significance.
H4: There will be significant association between pre-test practice scores and
selected social-demographic variables.
Presentation of the data
The data is presented in three sections under the following headings:
SECTION-I: Deals with description of the subjects according to the socio-
demographic characteristics of hypertensive people attending OPD's at tertiary care
hospital.
SECTION-II: Analysis is applied to depict effectiveness of Behavior change
Communication(BCC) on maintenance of positive health.

31
SECTION-III: Deals with analysis to find the association between pre-test knowledge
and practice scores with selected socio-demographic variables.
SECTION-I :
Table 1: Frequency and percentage distribution of patients according to socio-
demographic variables.
Sl.no Demographic variables Frequency(f) (Percentage)%
1 Age groups
35-40yrs 9 22.5%
41-45yrs 9 22.5%
46-50yrs 14 35%
51-55yrs 8 20%
2 Educations
SSLC 15 37.5%
PUC 9 22.5%
Degree 16 40%
3 Occupations
Employee 21 52.5%
Business 6 15%
Skilled worker 13 32.5%
4 Monthly income
Rs. 8000-Rs. 10000 13 32.5%
Rs. 10001-Rs.15000 14 35%
32
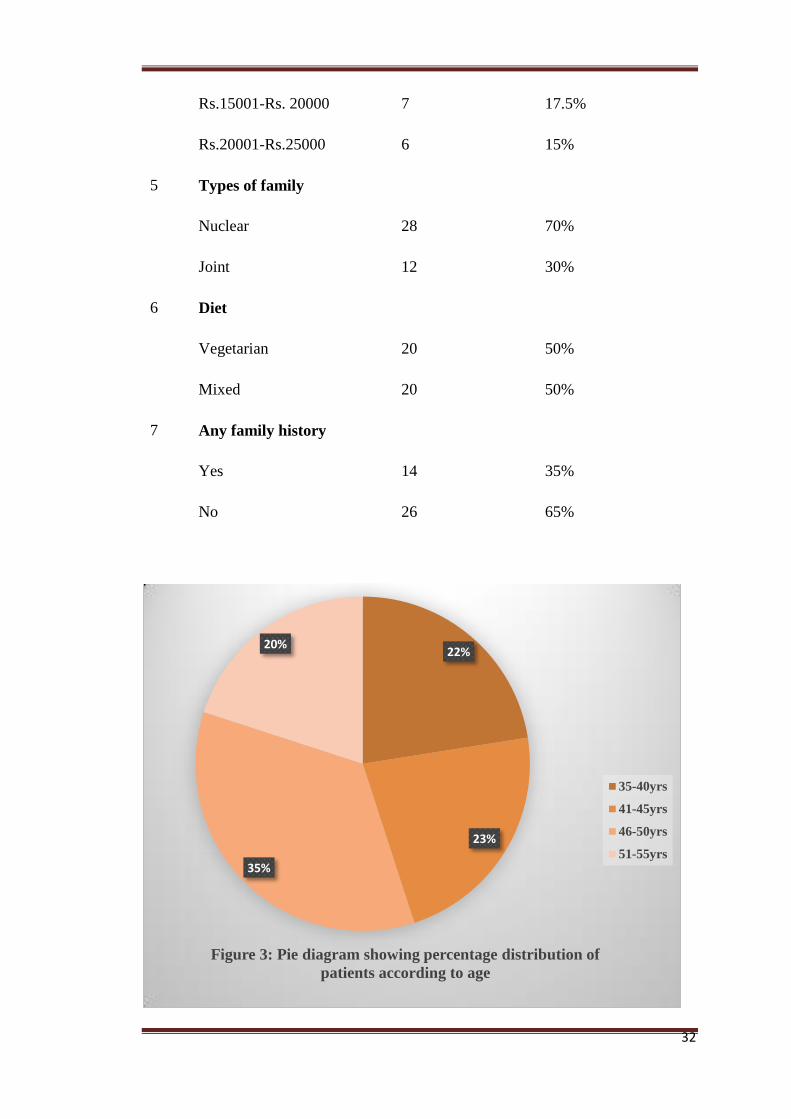
Rs.15001-Rs. 20000 7 17.5%
Rs.20001-Rs.25000 6 15%
5 Types of family
Nuclear 28 70%
Joint 12 30%
6 Diet
Vegetarian 20 50%
Mixed 20 50%
7 Any family history
Yes 14 35%
No 26 65%
22%
23%
35%
20%
Figure 3: Pie diagram showing percentage distribution of
patients according to age
35-40yrs
41-45yrs
46-50yrs
51-55yrs

33
Figure 3 : Indicated that majority of the subjects 14 (35%) belonged to the age
group of 46-50 years.
Figure 4 : Maximum subjects 16(40%) have attained Degree.
Figure 5 : Majority of the subjects 21(52.2%) were Employees.
SSLC
15
PUC
9
Degree
16
0
2
4
6
8
10
12
14
16
18
SSLC PUC Degree
Figure 4 : Column diagram showing percentage distributionof
patients according to Educational qualifications.
21
6
13
52.50%
15% 32.50%
Figure 5: Cylindrical diagram showing percentage distribution
of patients according to Occupation
frequency percentage

34
Figure 6 : Maximum 14(35%) monthly income of the subjects was between
Rs. 10001-Rs.15000 per month.
Figure 7: Majority of the subjects 28 (70%) belongs to Nuclear family.
Rs. 8000-Rs.
10000
32.50%
Rs. 10001-
Rs.15000
35.00%
Rs.15001-Rs.
20000
17.50%
Rs.20001-
Rs.25000
15.00%
Figure 6: Pie diagram showing percentage distribution of patients according to Monthly Income
Nuclear
28 (70%)
Joint
12 (30%)
0
5
10
15
20
25
30
Figure7: Column diagram showing percentage distribution of
patients according to Type of family

35
Figure 8: While 20 (50%) were vegetarian, 20(50%) were mixed diet.
Figure 9: Majority of the subjects 26 (65%) were not having any family
history.
Vegetarian
50.00%
Mixed
50.00%
Figure 8: Pie diagram showing percentage ditribution of
patients according to Diet
Vegetarian Mixed
14
35%
26
65%
frequency percentage
Figure 9: Pyramid diagram showing percentage ditribution of
patients according to family history
Yes No

36
SECTION-II
Analysis is applied to depict effectiveness of Behavior change Communication(BCC)
on maintenance of positive health.
Table 2: Mean, Standard deviation and Mean percentage of Pre and Post–test
Knowledge scores of patients on maintenance of positive health
n=40
Mean Median Standard
Mean
% Min.
Max.
deviation score
score
Pre- Test 5.23 4.5 3.47 13.07 2 13
Post-Test 10.7 11 2.43 26.75 5 14
Table 2 : Describes that the mean post-test knowledge scores were(26.75%) and the
mean pre-test scores were(13.07%) mentioning the impact of BCC in the
improvement of the knowledge.
Table 3: Mean, Standard deviation and Mean percentage of pre and posttest practice
scores of the patients on maintenance of positive health.
n=40
Mean Median Standard Min. Max.
Mean
%
deviation score score
Pre- Test 7.38 7.5 2.87 1 5 18.45
Post-Test 13.4 13 2.81 12 18 33.5
Table3 : Shows that the mean post-test practice scores were (33.5%) while the mean
pre-test scores (18.45%), indicating that BCC was effective in changing the practice
of the students in positive direction.

37
Table 4 a. Levels of Knowledge scores
Pre-test Post-test
Frequency (F) Percentage (%) Frequency (F) Percentage (%)
Inadequate 25 62.5 3 7.5
Moderate 10 25 2 5
Adequate 5 12.5 35 87.5
Table 4.a. and Figure 10: Depicted that in the posttest 35 (87.5%) has adequate
knowledge and 2 (5%) had moderate knowledge while in the pre-test 25 (62.5%) had
inadequate knowledge and 10 (25%) had moderate knowledge.
Table 4.b. Levels of Practice scores.
Pre-test Post-test
Frequency
(F)
Percentage
(%)
Frequency
(F)
Percentage
(%)
Poor 20 50 4 10
Average 15 37.5 3 7.5
Good 5 12.5 31 77.5

38
Table 4.b. and Figure 11: Depicted that majority 20 (50%) had poor practice in pre-
test where as in post-test 31 (77.5%) had practice towards maintenance of positive
health.
Table 5.a: Comparison of pretest and posttest knowledge scores by dependent „t‟ test
Mean SD Mean
Diff.
SD Diff. t-value P-value
Pre-test 5.23 3.47
Post-test 10.7 2.43 5.48 3.8 9.1058 <0.001, HS
Table 5.a. shows that, the two tailed „P‟ value is less than 0.0001 by conventional
criteria, this difference is considered to be extremely statistically significant.
Table 5.b. Comparison of pretest and post-test practice scores by dependent„t‟ test
Mean SD Mean
Diff.
SD Diff. t-value P-value
Pre-test 7.38 2.87
Post-test 13.4 2.81 6.03 4.3 8.8626 <0.001, HS
20
50% 4 10%
15
37.50% 3
7.50%
5 12.50%
31
77.50%
Figure 11 : Cyindrical diagram showing the
distributionn of percentage of pre and post test level
of practice scores
Poor
Average
Good

39
Table 5.b. and Figure 13 shows that , the two tailed „P‟ value is less than 0.0001 by
conventional criteria, this difference is considered to be extremely statistically
significant.
SECTION-III
Association between Pre-test Knowledge and Practice with selected Socio
demographic Variables.
Table 8.a: Association between Pre-test Knowledge with selected Socio demographic
Variables.

40
Sl.No Demographic characteristics Chi-
square Df
p-
value
Level of
significant
1 Age groups
35-40yrs
2.212 9 0.53 NS
41-45yrs
46-50yrs
51-55yrs
2 Educations
SSLC
11.963 4 0.003 S PUC
Degree
3 Occupations
Employee
3.533 4 0.171 NS
Business
Skilled worker
4 Monthly income
Rs. 8000-Rs. 10000
3.302 9 0.347 NS
Rs. 10001-Rs.15000
Rs.15001-Rs. 20000
Rs.20001-Rs.25000
5 Types of family
Nuclear
4.977 1 0.026 S Joint
6 Diet
Vegetarian
0.143 1 0.705 NS
Mixed
7 Any family history
Yes
9.341 1 0.002 S No
* Significant

41
Data presented in table 8.a. shows that the significant association in the Education,
Type of family and Family History with pre-test knowledge scores at 0.05 level of
significance.
Table 8 .b :Association between pre test level of Practice with demographic
characteristics.
Sl.No Demographic characteristics Chi-
square Df p-value Level of significant
1 Age groups
35-40yrs
3.65 9 0.302 NS 41-45yrs
46-50yrs
51-55yrs
2 Educations
SSLC
2.415 4 0.299 NS PUC
Degree
3 Occupations
Employee
0.433 4 0.805 NS Business
Skilled worker
4 Monthly income
Rs. 8000-Rs. 10000
2.108 9 0.55 NS Rs. 10001-Rs.15000
Rs.15001-Rs. 20000
Rs.20001-Rs.25000
5 Types of family
Nuclear
0.008 1 0.928 NS Joint
6 Diet
Vegetarian 0.173 1 0.677 NS
Mixed

42
7 Any family history
Yes
0.154 1 0.695 NS
No
*Not significant
Data presented in table 8.b. shows that their is no significant association with pre-test
practice scores at 0.05 level of significance.

43
6. DISCUSSION
This chapter the findings of the study have been discussed with reference to
the objectives and hypotheses stated in Chapter II along with the findings of the other
study.
MAJOR FINDINGS OF THE STUDY
To achieve the set objectives of the study forty subjects were selected by
applying sampling criteria.
Majority of the subjects 14 (35%) belonged to the age group of 46-50 years.
Maximum subjects 16 (40%) have attained Degree.
Majority of the subjects 21(52.2%) were Employees.
Maximum 14 (35%) monthly income of the subjects was between Rs. 10001-
Rs.15000 per month.
Majority of the subjects 28 (70%) belongs to Nuclear family.
While 20 (50%) were vegetarian, 20 (50%) were mixed diet.
Majority of the subjects 26 (65%) were not having any family history.
The mean post-test knowledge scores were (26.75%) and the mean pre-test scores
were (13.07%) mentioning the impact of BCC in the improvement of the
knowledge.
The mean post-test practice scores were (33.5%) while the mean pre-test scores
(18.45%), indicating that BCC was effective in changing the practice of the
students in positive direction.
The post-test 35 (87.5%) has adequate knowledge and 2 (5%) had moderate
knowledge while in the pre-test 25 (62.5%) had inadequate knowledge and 10
(25%) had moderate knowledge.
Majority20 (50%) had poor practice in pre-test where as in post-test 31 (77.5%)
had practice towards maintenance of positive health.

44
The two tailed „P‟ value is less than 0.0001 by conventional criteria, this difference is
considered to be extremely statistically significant. The two tailed „P‟ value is less
than 0.0001 by conventional criteria, this difference is considered to be extremely
statistically significant.
The significant association in the Education, Type of family and Family History
with pre-test knowledge scores at 0.05 level of significance.
Data presented in table 8.b. shows that there is no significant association with
pre-test practice scores at 0.05 level of significance.
DISCUSSION
The findings of the study are organized under the following headings for the
purpose of discussion.
1. Findings related to socio-demographic variables of the patients.
2. Findings related to effectiveness of Behavior Change Communication (BCC) on
maintenance of positive health.
3. Findings related to association between the existing pre-test knowledge scores of
the patients with selected socio-demographic variables.
4. Findings related to association between the existing pre-test practice scores of the
patients with selected socio-demographic variables.
FINDINGS RELATED TO SOCIO DEMOGRAPHIC DATA OF THE
PATIENTS (TABLE 1)
For the proposed study, a sample size comprising of forty Early detected
Hypertensive patients attending Medicine OPD‟s at Tertiary care hospital Dharwad.
The findings (table 1) of the study suggested that all the (40) subjects were
between the age group of 35-55years of age of whom 15 (37.5%) have completed
SSLC, 16 (40%) degree and 9 (22.5%) have done PUC.

45
Majority of the subjects 21 (52.2%) were Employees, 13 (32.5%) were skilled
workers and 6 (15%) were doing Business. Maximum 14 (35%) monthly income of
the subjects was between Rs.10001-Rs.15000 per month. 13 (32.5%) Rs.8000-Rs.
10000, 7 (17.5%) Rs.15001-Rs. 20000, 6 (15%) Rs.20001- Rs.25000. Types of
family Nuclear 28 (70%), Joint 12 (30%). Diet Vegetarian 20 (50%), Mixed 20
(50%). Any family history Yes 14 (35%), No 26 (65%).
FINDINGS RELATED TO EFFECTIVENESS OF BEHAVIOR CHANGE
COMMUNICATION ON MAINTENANCE OF POSITIVE HEALTH.
In the pre-test out of 40 Hypertensive subjects 25 (62.5%) had inadequate, 10
(25%) had moderate and 5 (12.5%) had adequate level of knowledge. While majority
20 (50%) had poor practice, 15 (37.5%) had average and only 5 (12.5%) had good
level of practice scores in pre-test. Where as in the post-test 35 (87.5%) has adequate
knowledge and 2 (5%) had moderate knowledge and 31 (77.5%) had good practice, 3
(7.5%) had average practice towards maintenance of positive health.
Further the computed „t‟ value on knowledge (9.10) and practice (8.8626) found to
be greater than table values at 0.05 level significance confirms that BCC has made
true difference in enhancing the knowledge and changing the practice of the
Hypertensive patients in the maintenance of positive health . Hence H1 is accepted.
FINDINGS RELATED TO ASSOCIATION BETWEEN THE EXISTING PRE-
TEST KNWOLEDGE AND PRACTICE OF THE HYPERTENSIVE
PATIENTS WITH SELECTED SOCIO DEMOGRAPHIC VARIABLES.
To achieve the objective 3 the collected pre-test data was further subjected to
analysis to find an association with socio-demographic variable. The computed X2
results (X2
cal >X2
Tab) revealed that there was statistical significant association at
0.05 level of significance association in the Education, Type of family and Family
History with pre-test knowledge scores of Hypertensive patients, Hence H2 was
accepted and in rest of the case H2 is rejected.
In case of practice, the calculated X2
results (X2
cal >X2
Tab) revealed that there
was statistical significant association at 0.05 level of significance association. In all
the socio-demographic data H2 was rejected.

46
The above findings proved that students were not aware and lack of knowledge and
practice on maintenance of positive health the investigator reasonably concludes that
enhancement in knowledge and practice towards positive change was occurred only
after BCC session on maintenance of positive health.

47
7. CONCLUSION
This chapter deals with the conclusions drawn and its implications of the study
on the different aspects of nursing, such as nursing practice, nursing administration,
nursing education and nursing research, limitations and recommendations. It clarifies
the limitations of the study and suggests recommendations for further research.
Based on the findings of the study, the following conclusions were drawn.
1. As it assumed, that the pre-test findings of the study revealed that the
knowledge scores of the patients on maintains of positive health were average and
attitude score were not fully favorable.
2. Since the above findings did not correlate with each other giving clear
indications that the health maintenance behavior of the patients is inappropriate and
need for the intervention. Hence after extensive review of literature and the opinion of
the experts and investigator‟s personal experience it was planned to use and find the
effectiveness of behavior change communication (BCC) as a mode of intervention.
3. The findings of the post-test result revealed that there were significant
improvement in the level of knowledge and practice on maintenance of positive
health. Hence it is concluded that the BCC in equipping the appropriate knowledge
and practice as a mode of intervention found to be effective.
4. Further it also revealed that socio-demographic characteristics of the
subjects do not have much interfere in the maintenance of positive health. Thus it is
concluded that the behavior of the individual is dependent on knowledge and practice.
IMPLICATIONS OF THE STUDY
The implications of the study could be discussed under four broad areas, as follows,
Nursing practice
Nursing administration
Nursing education
Nursing research.
48
Nursing practice:
National development depends on individual‟s health. As individuals are
considered to be the change in the society they need to be provided with appropriate
Information Education Communication (IEC) which will further improve their health
seeking behavior. Based on the final results of the study. Clearly indicates that nurses
play vital role in prevention of diseases through counseling. Behavior Change
Communication proved to be effective and appropriate method for delivering health
message to the individual‟s, who attend OPD‟s at tertiary care hospital.
Nursing Administration:
The study emphasized the need for Behavior Change Communication on
maintenance of positive health to improve the health of the patients in their day today
life. The nurse administrators can equip the health personnel in delivering appropriate
health message according to situations, level of understanding of the consumers
through proper planning and implementation.
Nursing education:
Along with the care provider‟s, as leaders and managers of health care team
plays a role of educator and counselor. Hence these advance methods of IEC should
be incorporated in the hospital settings.
Nursing research:
This present study conducted by the investigator can be a source to make the
health education methods refined in order to the people in the community and it can
be used for critique or for comparison.
LIMITATIONS
The study is limited to Hypertensive patients at tertiary care hospital,
1. The broad generalization of the findings of the study cannot be made due to
the small size of sample and investigator was unable to reach their place of residence
limited time.

49
2. The instrument used for the study is designed and developed by the
investigator for the purpose of achieving set of objectives of the study. Hence it is not
a standardized tool.
3. The study did not assess the self-reported practice of patients on
maintenance of positive health.
4. The Behavior Change Communication is long process because it takes
several months to Change Behavior so continues monitoring and assessment are
needed in different phases.
RECOMMENDATIONS
On the basis of the findings the study, following recommendation are made.
A similar study on larger sample for a longer period of time with precise
sampling technique would be more pertinent.
An experimental study can be undertaken with a control group for comparison
of the results to be more precise in the following subjects at the place of their
residence.
An comparative study may be conducted between rural and urban people.

50
8. SUMMARY
This chapter presents a brief summary of the research study. The present study
pre-experimental in nature was undertaken with the purpose to evaluate the
effectiveness of Behavior Change Communication (BCC) on maintenance of positive
health among the Hypertensive patients attending Medicine OPD‟s in tertiary care
hospital at Dharwad.
The study was aimed at accomplishing the following objectives.
To assess the existing knowledge and practice of early detected hypertensive
patients regarding prevention of stroke.
To evaluate the effectiveness of Behaviour change communication regarding
prevention of stroke.
To find the association between pre-test knowledge and practice scores with
selected socio-demographic variables.
The conceptual framework selected for this study was based on an integrative
Model of Behavior Prediction by Fishbein, M. & Yzer, MC.(2003). It is based on
Behavioral beliefs, attitude toward the behavior, normative belief, subjective norm
and perceived behavioral control, with each predictor weighted for its importance in
relation to the behavior and population of interest.
The study assumed that the knowledge influences practice exhibited through
actions. The lack of knowledge of Early detected hypertensive patients in
maintenance of positive health has influenced their practices leading them towards
harmful or ignorance practice and it is also assumed that Behavioral Change
Communication (BCC) will have a significant impact on patients health behavior.
The study was confined to Hypertensive patients attending Medicine OPD‟s in
tertiary care hospital, Dharwad.
The extensive review of literature directed the investigator to prepare the BCC
material on Knowledge questionnaire and knowledge practice questionnaire checklist.

51
A pre-experimental one group pre-test post-test design utilized to achieve the
overall and comprehensive purpose. Samples were collected by using Non-probability
purposive sampling technique.
Content validity of the designed tool and Behavior Change Communication
material was obtained through expert judgment.
The pilot study was conducted at Hypertensive patients attending Medicine
OPD‟s in tertiary care hospital Hypertensive patients attending Medicine OPD‟s in
tertiary care Hospital from 8th
March 2021 to 16th
March 2021to know the feasibility
of the main study and establish reliability of the tool and BCC, keeping in mind the
cultural characteristics and rituals as same as to the final setting of the study. The
reliability of the tool and BCC was established by computing the coefficient ( r ) of
internal consistency for both structured knowledge questionnaire and practice were
r=0.90 and r=0.87 respectively, using split half technique which indicates that the tool
is reliable.
The main study was undertaken from 15th April 2021 to 30th
May 2021 in
Medicine OPD‟s in tertiary care hospital, Dharwad after obtaining a formal
permission from Vice Chancellor and HOD of Medicine Department.
The pre and post test data was collected by using above instrument of the
study. Behavior Change Communication was administered to the students at the end
of pre-test and the investigator kept personal contact with individual patients till the
post-test, providing explanations and demonstration. Clearing doubts I order to bring
changes in their health behavior. The post-test was conducted on the seventh day of
intervention.
The data generated through the pre-test and post-test was tabulated and
analyzed by using descriptive and inferential statistics to achieve the set objectives of
the study.

52
9. BIBILOGRAPHY
1. Goldman Rena. Effects of hypertension on body [cited on 2020 January 31].
Available from: https://www.healthline.com/health/high-blood-pressure-
hypertension/effect-on-body#1
2. Jayalakshmi.Effectiveness of self-instructional module on knowledge
regarding prevention of stroke among hypertensive patients. In a selected
hospital at Madurai district; 2016; [cited on 2020 February 25]. Available
from:http://repository-tnmgrmu.ac.in/2416/1/3001228jayalakshmih.pdf.
3. https://courses.lumenlearning.com/atd-hostos-interpersonalrelations-
1/chapter/introduction-to-communication/
4. Tibebu NS, Emiru TD, Tiruneh CM, Nigat AB, Abate MW, Demelash AT.
Knowledge on Prevention of Stroke and Its Associated Factors Among
Hypertensive Patients at Debre Tabor General Hospital: An Institution-Based
Cross-Sectional Study. Risk Manag Healthc Policy. 2021;14:1681-1688
https://doi.org/10.2147/RMHP.S303876
5. Behavior Change Communication for the Prevention and Treatment of STDs.
Arlington, VA: AIDSCAP/Family Health International, 1997.Available from:
doi: 10.2471/BLT.08.056713
6. Gurupada K P, David A Kola. Effectiveness of Behavior Change
Communication (BCC) on maintenance of positive health among the students
of Rural Higher Primary Schools. International Journal of Nursing Education
and Research. 2019; 7(4): 535-538Available from : DOI No: 10.5958/2454-
2660.2019.00118.2
7. Newson, R.S., Lion, R., Crawford, R.J. et al. Behaviour change for better
health: nutrition, hygiene and sustainability. BMC Public Health 13, S1
(2013). https://doi.org/10.1186/1471-2458-13-S1-S1
8. Milgrom, K.The Role of Health Communications in Behavior Change.2015.
Available from :
https://www.google.com/search?rlz=1C1CHBD_enIN886IN886&ei=AGmQX
tvTBv2V4-EP-
v6OyAM&q=.++The++Role++of++Health++Communications++in++Behavi
or++Change.2015&oq=.++The++Role++of++Health

53
9. Missiriya, Sahbanathul.(2017). Assess the prevalence of hypertension and
knowledge regarding the prevention of stroke. Asian Journal of
Pharmaceutical and Clinical Research.
DOI:10.22159/ajpcr.2017.v10i8.18558
10. Viera AJ, Cohen LW, Mitchell CM, Sloane PD. “High blood pressure
knowledge among primary care patients with known hypertension: a North
Carolina Family Medicine Research Network (NC-FM-RN) study. J Am
Board Fam Med.2008;21(4):300-308. Available from:
DOI: https://doi.org/10.3122/jabfm.2008.04.070254
11. Rajan J, Sakthibalan M, Raj GM, Mangaiarkkarasi A. Knowledge, attitude and
practice of hypertension among hypertensive patients in a tertiary care
teaching hospital. Int Journal of Basic and Clinical Pharmacology 2019;
8:1013-1018. Available from:DOI: http://dx.doi.org/10.18203/2319-
2003.ijbcp20191593
12. Mitra Y, Singh G and Vij A To assess knowledge , attitude and practices
regarding lifestyle risk factors in patients with hypertension, coming to
Medicine O.P.D. at PIMS Jalandhar. HECS International Journal of
Community Health and Medical Research- 2017;3(4):14-20.
13. C. Sasi Sulochana, Sharmila Jansi Rani. Effectiveness of Hypertension
Prevention Program on Information among Employees at Kanaya Kumari
District, Tamil Nadu. Int. J. Nur. Edu. and Research. 2019; 7(4):458-462.
Available from : DOI No: 10.5958/2454-2660.2019.00102.9
14. Sreejesh K P, Athira K S, Heydey Green M J. Awareness and attitude towards
stroke and its prevention among Hypertensive and Non- hypertensive people.
Asian Journal Of Pharmaceutical and Clinical Research 2018; 11(3): 39-42.
[last cited on 2020 April 06]
Available from: DOI https://doi.org/10.22159/ajpcr.2017.v10i8.18558
15. Missriya Ma, S., and J. John. “Assess The Prevalence Of Hypertension And
Knowledge Regarding The Prevention Of Stroke”. Asian Journal of
Pharmaceutical and Clinical Research, Vol. 10, No. 8, Aug. 2017, Pp. 177-
180. Available from: DOI https://doi.org/10.22159/ajpcr.2017.v10i8.18558
16. Pragnesh Parmar, et‟al. Study of knowledge, attitude and practice of general
population of Gandhinagar towards hypertension. International Journal of
Current Microbiology and Applied Sciences (IJCMAS).2014;3(8);680-685.

54
Available from: DOI : https://www.ijcmas.com/vol-
38/Pragnesh%20Parmar,%20et%20al.pdf
17. Vanitha D, Anitha Rani.M Knowledge and Practice on lifestyle modifications
among males with hypertension. Indian J Comm Health. 2015; 27, 1: 143-149.
18. M. D. Saju, Komal Preet Allagh, Lorane Scaria, Shinto Joseph, Jotheeswaran
Amuthavalli Thiyagarajan, "Prevalence, Awareness, Treatment, and Control
of Hypertension and Its Associated Risk Factors: Results from Baseline
Survey of SWADES Family Cohort Study", International Journal of
Hypertension, vol. 2020, Article
ID 4964835, 7 pages, 2020. https://doi.org/10.1155/2020/4964835
19. Awotidebe, T., Adedoyin, R., Rasaq, W., Adeyeye, V., Mbada, C., Akinola,
O., & Otwombe, K. (2014). Knowledge, attitude and Practice of Exercise for
blood pressure control: A cross-sectional survey. Journal of Exercise Science
and Physiotherapy, 10(1), 1–
10.https://search.informit.org/doi/10.3316/informit.755688598487763
20. Giena, Vike Pebri et al. “Predictors of health-promoting behaviour among
older adults with hypertension in Indonesia.” International journal of nursing
sciences vol. 5,2 201-205. 14 Apr. 2018, doi:10.1016/j.ijnss.2018.04.002
https://doi.org/10.1016/j.ijnss.2018.04.002
21. AO Ayodapo & TAV Olukokun (2019) Lifestyle counselling and behavioural
change: role among adult hypertensives in a rural tertiary institution, South
African Family Practice, 61:3, 91-96, DOI: 10.1080/20786190.2019.1569453
22. Buda, E.S., Hanfore, L.K., Fite, R.O. et al. Lifestyle modification practice and
associated factors among diagnosed hypertensive patients in selected
hospitals, South Ethiopia. Clin Hypertens 23, 26 (2017).
https://doi.org/10.1186/s40885-017-0081-1
23. Tozivepi SN, Takawira S, Chikaka E, Mundagowa P, Chadambuka EM,
Mukora-Mutseyekwa F. The Nexus Between Adherence to Recommended
Lifestyle Behaviors and Blood Pressure Control in Hypertensive Patients at
Mutare Provincial Hospital, Zimbabwe: A Cross-Sectional Study. Patient
Prefer Adherence. 2021;15:1027-1037https://doi.org/10.2147/PPA.S306885
24. Nepal P, Dhungana B. Lifestyle modification after diagnosis of hypertension
in patients visiting Lumbini Medical College Teaching Hospital. Journal of
Lumbini Medical College, 2015;3(1):12-5. doi: 10.22502/jlmc.v3i1.62

55
25. Okwuonu C.G, Emmanuel C.I, Ojimadu N.E. Perception and practice of
lifestyle modification in the management of hypertension among
hypertensives in south-east Nigeria. Int J Med Biomed Res 2014;3(2):121-131
doi: http://dx.doi.org/10.14194/ijmbr.3.2.8
26. http://www.medicinearticle.com/JMR_201732_10.pdf
27. Dan- Jumbo, Alali & Dienye,Paul & Nnadi, Nnenna & Uriah, Simon. (2021).
Lifestyle practices among hyperetensive patients attending the Family
Medicine Clinic in a tertiary hospital in Nigeria.GSC Advanced Research and
Reviews. 6. 050-060.
DOI: https://doi.org/10.30574/gscarr.2021.6.2.0021
28. Verma, P. et al. “Assessment of Extent of Lifestyle Modification among
Diagnosed Patients of Hypertension Attending Tertiary Care
Hospital.” International Journal of Medical and Health Sciences 4 (2015):
196-201.https://www.semanticscholar.org/paper/Assessment-of-Extent-of-
Lifestyle-Modification-of-Verma-
Manushi/aae837701e1a6c22187a2b49a133273b8ed4fdc2
29. Dhakal M, Dhakal O. A hospital based cross sectional study to evaluate
awareness of lifestyle interventions among hypertensive patients in Sikkim
(North-Eastern State of India). Int J Med Res Rev [Internet]. 2017Apr.30
[cited 2021Jul.1];5(4):421-8 https://doi.org/10.17511/ijmrr.2017.i04.08
30. Scala, D., D‟Avino, M., Cozzolino, S. et al. Promotion of behavioural change
in people with hypertension: an intervention study. Pharm World Sci 30, 834–
839 (2008). https://doi.org/10.1007/s11096-008-9235-2
31. Marfo,Afia.(2014). Ghanaian hypertensive patients understanding of their
medicines and lifestyles modification for managing hypertension. International
Journal of Pharmacy and Pharmaceutical Sciences.6. 165-170
https://innovareacademics.in/journal/ijpps/Vol6Issue4/8781.pdf

56
10. ANNEXURES
CONSENT FORM FOR THE PATIENTS
Dear respondent,
I Ms. Kotapuri. Prathyusha 2nd
year Nursing Student of Shri Dharmasthala
Manjunatheswara University Institute of Nursing Sciences Dharwad. In partial
fulfillment of the course requirement, I have to undertake a research project to Shri
Dharmasthala Manjunatheswara University Institute of Nursing Sciences Dharwad.
The title of my project is,
“A STUDY TO EVALUATE THE EFFECTIVENESS OF BEHAVIOR
CHANGE COMMUNICATION ON KNOWLEDGE AND PRACTICE
REGARDING PREVENTION OF STROKE AMONG EARLY DETECTED
HYPERTENSIVE PATIENTS ATTENDING OPD’S AT TERTIARY CARE
HOSPITAL, DHARWAD.”
The purpose of this study is to evaluate the effectiveness of behavior change
communication designed by the investigator on knowledge and practice regarding
prevention of stroke among early detected hypertensive patients attending OPD‟s at
tertiary care hospital, Dharwad, thus to evaluate the knowledge and practice of the
early detected hypertensive patients and to update the knowledge and practice during
the study.
You are requested to participate in this study following are the details of the study.
On Day1, Pretest will be conducted to assess the pre-interventional knowledge
and practice. (per day 5 patients will be taken)
Patient will be given an appointment to attend the teaching and demo on
prevention of stroke.
On the same Day1 BCC teaching will be given with the help of lecture using flash
cards, charts and handouts.
Meanwhile, after the teaching session, the patients can also clear their doubts; if
any, by discussing with the investigator. (For those 5 subjects, taken on the same
day teaching will be given).
• Post-test will be conducted on 7th
day of intervention to find out the effectiveness
of behavior change communication.

57
I assure you that the information given by you will be kept strictly confidential
and used only for the study purpose. If you are willing to participate in this study
please sign the consent form given below.
Place: Yours Sincerely
Date: Ms. Kotapuri. Prathyusha
2nd
year M.Sc Nursing Student.
I HERE BY VOLUNTEER AND CONSENT TO PARTICIPATE IN THIS STUDY,
I HAVE READ THE CONSENT OR IT HAS BEEN READ TO MY OWN
LANGUAGE. THE STUDY HAS BEEN FULLY EXPLAINED TO ME AND I
HAVE BEEN TOLD BY THE INVESTIGATOR TO CONTACT HER
PERSONALLY FOR CLARIFICATION OF THE DOUBTS / QUESTIONS OR
WITHDRAW MY SELF FROM THE STUDY AT ANY TIME.
Participants name
and address
Participants
signature
Researcher name
Researcher
signature
Date
Date
I have been informed of the purpose of the study and I voluntarily give my consent to
participate in the study.
Place: Signature of the respondent
Date: Name:
58
LETTER REQUESTING OPINION AND SUGGESTION FROM
EXPERT FOR VALIDITY OF RESEARCH TOOL
From,
Ms. Kotapuri .Prathyusha
II year M.Sc Nursing
Shri Dharmasthala Manjunatheswara University‟s
Institute of Nursing Sciences, Dharwad-580009
To,
Respected sir/Madam
Subject: Request for expert opinion and suggestion to establish content validity of
the research tool.
I, Ms. Kotapuri . Prathyusha, II year M.Sc Nursing [(Medical Surgical
Nursing)] specialty, [(Critical Care Nursing)] student of Shri Dharmasthala
Manjunatheswara University Institute of Nursing Sciences Dharwad, has selected the
topic titled “A STUDY TO EVALUATE THE EFFECTIVENESS OF
BEHAVIOR CHANGE COMMUNICATION ON KNOWLEDGE AND
PRACTICE REGARDING PREVENTION OF STROKE AMONG EARLY
DETECTED HYPERTENSIVE PATIENTS ATTENDING OPD’S AT
TERTIARY CARE HOSPITAL, DHARWAD”. For the dissertation to be
submitted to Shri Dharmasthala Manjunatheswara University Institute of Nursing
Sciences Dharwad, as a partial fulfillment of Master of Science in Nursing
Programme.
May I request you to go through the items and give your valuable suggestions
and opinions to develop the content validity of the tool. Kindly suggest
modifications, additions, if any, in the remark columns.

59
I also request you to certify regarding your validation in the enclosed format. I
will be grateful to your honorable work. Anticipating a favorable response at the
earliest.
I have enclosed the following for your reference:
Statement of the problem, Objectives of the study, operational definitions and
hypothesis.
Demographic data and Observational checklist to evaluate knowledge and
practice.
Evaluative criteria checklist
Content validity certificate
Lesson plan
Thanking you,
Date: Yours Sincerely,
Place: Sattur, Dharwad [Ms. Kotapuri. Prathyusha]

60
CONTENT VALIDATION CERTIFICATE
This is to certify that the tool describing the Knowledge questionnaires prepared by
Ms. Kotapuri. Prathyusha. II year M.Sc Nursing, Shri Dharmasthala Manjunatheswara
University Institute of Nursing Sciences Dharwad. To be used in her study title “A
Study To Evaluate The Effectiveness Of Behavior Change Communication On
Knowledge And Practice Regarding Prevention Of Stroke Among Early
Detected Hypertensive Patients Attending OPD’s At Tertiary Care Hospital,
Dharwad”.
My comments on following :
Tool :
Adequate of tool measure objectives :
Organization of tool :
Feasibility of tool :
Date: Signature & seal of expert
Place: Designation and address

61
EVALUATION CRITERIA CHECKLIST FOR VALIDATION OF TOOL
INSTRUCTIONS:
Please review the items in the tool and give your suggestions regarding accuracy,
relevance and appropriateness of the context. Kindly please tick mark ( ) in the
appropriate column. If there are any suggestions or comments please mention in the
remark column.
Section-I:
Consists of socio-demographic data, it consists of 8 items for obtaining
information about selected base line data.
Section-II:
Structured knowledge question,
PART-I: PRE- CONTEMPLATION
It consists of 6 questions for evaluating the knowledge on hypertension.
PART-II: CONTEMPLATION
Consists knowledge questions on stroke. It consists of 4 questions on
knowledge of Stroke.
PART-III: PREPARATION
It consists of 4 questions on prevention of stroke.
INTERPRETATION OF COLUMN:
Column 1- Relevant
Column-2 Needs modifications
Column-3 Not relevant
Section-III:
KNOWLEDGE PRACTICE QUESTIONNAIRE- CHECKLIST
Consists of 22 items on knowledge practice
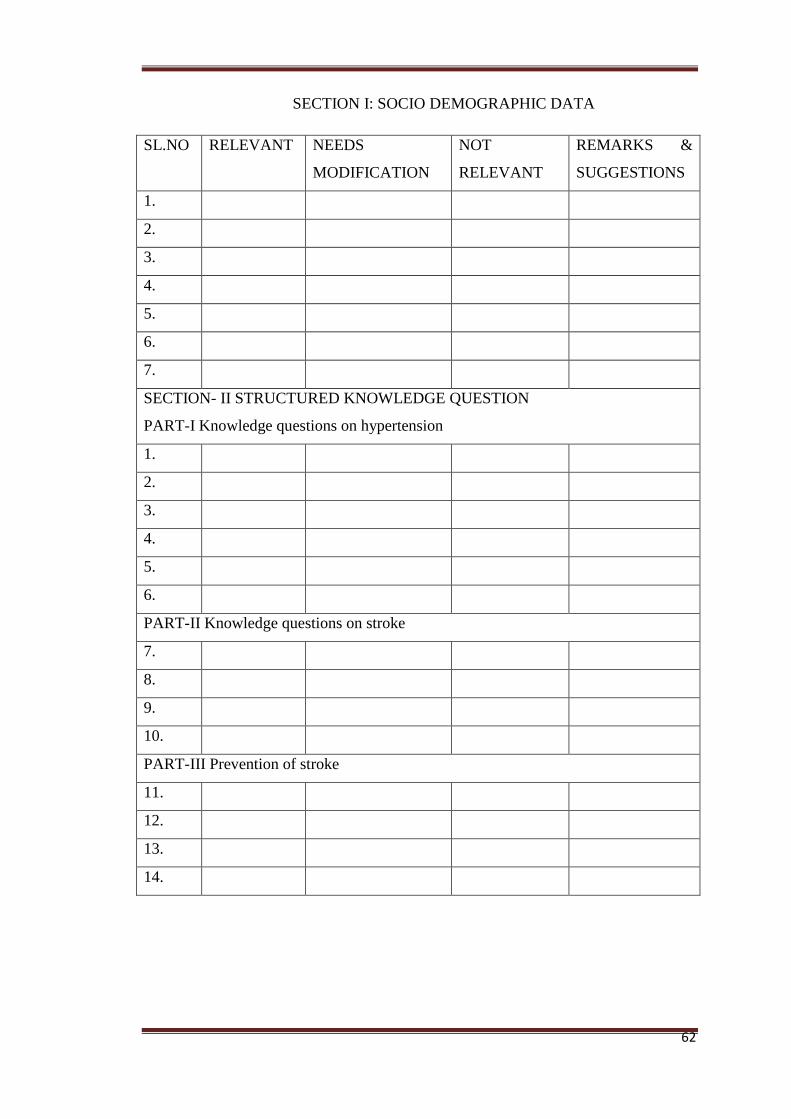
62
SECTION I: SOCIO DEMOGRAPHIC DATA
SL.NO RELEVANT NEEDS
MODIFICATION
NOT
RELEVANT
REMARKS &
SUGGESTIONS
1.
2.
3.
4.
5.
6.
7.
SECTION- II STRUCTURED KNOWLEDGE QUESTION
PART-I Knowledge questions on hypertension
1.
2.
3.
4.
5.
6.
PART-II Knowledge questions on stroke
7.
8.
9.
10.
PART-III Prevention of stroke
11.
12.
13.
14.

63
Section-III:
KNOWLEDGE PRACTICE QUESTIONNAIRE- CHECKLIST
SL.NO RELEVANT NEEDS
MODIFICATION
NOT
RELEVANT
REMARKS &
SUGGESTIONS
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.

64
LETTER SEEKING PERMISSION

65
LETTER SEEKING RESEARCH PERMISSION

66
LIST OF EXPERTS
Mr. Basavant. Dhudum Prof. (Mrs). Suchitra. Rathod
Associate.Prof D.Y. Patil‟s College of Nursing,
Dept.Medical Surgical Nursing, Kasaba Bawada,
Bharati Vidyapeeth College of Nursing, Kolhapur.
Sangli.
Prof. Prasanna. Deshpande Mrs. Preeti. Bhupal
Prof & Principal Prof & HOD Medical Surgical Nursing ,
KLE‟S Institute of Nursing Sciences, KLE‟S Institute of Nursing Sciences,
Anokola. Belagavi.
Prof. (Mr). Samuel Fernandis Dr. Sanjay. M. Peerapur
Pricipal Principal
HOD Dept. Medical Surgical Nursing KLE‟S Institute of Nursing Sciences,
Miraj Medical Center, Miraj. Hubli.

67
SECTION 1
SOCIO DEMOGRAPHIC PROFORMA
1. Age in years [ ]
2. Education [ ]
3. Occupation [ ]
4. Monthly income of the family in rupees [ ]
5. Type of family
a) Nuclear [ ]
b) Joint [ ]
6. Diet
a) Vegetarian [ ]
b) Mixed diet [ ]
7. Any family history of hypertension
a) Yes [ ]
b) No [ ]

68
SECTION -2
STRUCTURE KNOWLEDGE QUESTION
INSTRUCTIONS:
Dear participants
1. Kindly read the following questions and follow the instructions.
2. Select and tick the most appropriate answer from options given
below each question.
3. Please note that it is important to answer to all questions.
4. Correct answer will be scored 1 mark and wrong answer is scored
0 marks.
CODE NO :- DATE :-
PART-I: PRE- CONTEMPLATION
1. Hypertension leads to
a) Cancer [ ]
b) Shock [ ]
c) Stroke [ ]
d) Tuberculosis [ ]
2. Does smoking lead to
a) Kidney Failure [ ]
b) Stroke [ ]
c) Liver Failure [ ]
d) Respiratory Failure [ ]

69
3. What is hypertension commonly called as?
a) Stunt killer [ ]
b) Stealing killer [ ]
c) Secret killer [ ]
d) Silent killer [ ]
4. Which is the important way for Stress management?
a) Proper rest [ ]
b) Healthy diet [ ]
c) Listen to music [ ]
d) All the above [ ]
5. A measure to maintain healthy weight
a) Drink plenty of fluids [ ]
b) Proper rest and sleep [ ]
c) Physical activity [ ]
d) All the above [ ]
6. Regular blood pressure monitoring is done to
a) Detect the early symptoms of complications [ ]
b) Start the medication [ ]
c) Get checked only when you get sick /illness [ ]
d) Get checked every for every 6months [ ]

70
PART-II: CONTEMPLATION
7. What is stroke?
a) Heart attack [ ]
b) Liver failure [ ]
c) Brain attack [ ]
d) Kidney failure [ ]
8. How does stroke happen?
a) Blood clot in the brain [ ]
b) Blood clot in the heart [ ]
c) Blood clot in the kidneys [ ]
d) Blood clot in the lungs [ ]
9. What are the main symptoms of stroke?
a) Headache, nausea and vomiting [ ]
b) Fever, nausea and seizure [ ]
c) Diarrhea, fever and coma [ ]
d) All of the above [ ]
10. How hypertension produce stroke?
a) It strains, weakens and damages the blood vessels [ ]
b) It relaxes the blood vessels [ ]
c) It increases the cholesterol level [ ]
d) It increases the hemoglobin level in the blood [ ]

71
PART-III: PREPARATION
11. The salt intake of hypertensive patients should be
a) Stopped [ ]
b) Limited [ ]
c) Increased [ ]
d) Sodium intake is not related with Hypertension [ ]
12. Which is the diet not suitable for high blood pressure?
a) Fruits [ ]
b) Dairy foods [ ]
c) Mixed diet [ ]
d) Salty foods [ ]
13. How many hours a person must sleep in a day?
a) 4-5 hours [ ]
b) 6-7 hours [ ]
c) 7-8 hours [ ]
d) 9-10 hours [ ]
14. The daily recommended minutes of exercise to maintain normal blood
pressure is
a) 10-20 minutes [ ]
b) 20-30 minutes [ ]
c) 30-40 minutes [ ]
d) 60-70 minutes [ ]

72
KNOWLEDGE PRACTICE QUESTIONNAIRE- CHECKLIST
Content
Yes No Not
Applicable
1. I take prescribed medications regularly in
time.
2. Taking prescribed medication helps to
maintain normal level of blood pressure
3. I always undergo routine health checkup.
4. A person must drink minimum 8 glasses of
water a day
5. I perform 30 minutes of moderate exercise
daily in a week for (5days).
6. A person has to do exercises 3 to 4 times in
a week.
7. I check my weight regularly.
8. I always take low fatty foods only.
9. Frequent consumption of junk foods affects
in maintaining normal blood pressure.
10. I always follow the food timings regularly.
11. I include fruits and vegetables in my diet.
12. I include 1-2 (0.35grams) table spoon of salt
in my diet.

73
13. Reducing the salt intake helps to control
high blood pressure.
14. I eat a balanced diet.
15. I will limit the alcohol intake.
16. I will quit smoking.
17. I will cut back on coffee.
18. I will do meditation to reduce my stress
level.
19. A person who is diagnosed with high blood
pressure should avoid lifting weight or
heavy objects.
20. A person with stroke needs immediate
hospitalization.
21. Lifestyle modification is the first step in
managing normal blood pressure
22. I will do activities such as walking and
gardening to increase physical activity
levels.
Scoring and Interpretation
The tool consisted of 14 items on knowledge, 22 items on practice checklist. Each
right answer carried „1‟ mark and wrong answer carried „0‟ mark. Further
categorization of the level of knowledge was done as following as

74
Inadequate knowledge 0-4
Moderate knowledge 5-9
Adequate knowledge 10-14
SCORING AND INTERPRETATION OF PRACTICE
Knowledge questionnaire practice checklist
Good 15-22
Average 7-14
Poor 0-6
KEY ANSWERS
SECTION-2 STRUCTURE KNOWLEDGE QUESTION
1-C 8-A
2- B 9-D
3-D 10-A
4-D 11-B
5-D 12-D
6-C 13-C
7-C 14-B

75
LESSON PLAN
Name of the teacher : Miss. KOTAPURI. PRATHYUSHA
Topic : Prevention of Stroke among early detected Hypertensive patients.
Group : Patients attending the OPDs (Medicine OPD)
Place : Tertiary Care Hospital Dharwad.
Method of teaching : Lecture cum discussion
AV Aids : Flash cards, Charts and Banners.
Time : 45 Minutes
GENERAL OBJECTIVES:
At the end of the teaching the patient will be able to gain in depth knowledge and practice regarding prevention of stroke.
SPECIFIC OBJECTIVES:
At the end of teaching patient will be able to :
Explain review of anatomy and physiology of brain and heart.
Definition of hypertension
Lists the causes of hypertension
Explains the signs and symptoms of high blood pressure

76
Enumerates the complication of hypertension
Definition of stroke
List out the causes of stroke
How hypertension causes hemorrhagic stroke
Enlist the symptoms of stroke
Explain the preventive measures for stroke.

77
SPECIFIC
OBJECTIVES
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
A.V AIDS EVALUA
TION
2
minutes
Introduces the topic
INTRODUCTION
Life style diseases are set of diseases usually
related to our changing urban way of life. The
Important factors contributing to these disorders
are two much work, too much stress, round the
clock working hours, bad eating habits, and
sedentary life with little or no exercise. In many
diseases our life style may be an important
causative factor or may aggravate there disease.
One of the important life style related disease is
hypertension.
Introduces the
topic
Listens and
participates in
discussion

78
4minutes Explains the
anatomy and
physiology of brain
and heart
ANATOMY AND PHYSIOLOGY OF
BRAIN AND HEART
BRAIN
The brain, together with the spinal cord,
makes up the Central nervous system (CNS).
This is the „control centre‟ that coordinates
the body‟s function. The human brain is
hugely interconnected but three major
components can be identified: The Cerebrum,
Brainstem, and Cerebellum. This is the
„control centre‟ that co ordinates the body‟s
function.
Explains the
anatomy and
physiology
Listens and
observes the
flash card and
chart
Flash
cards,
charts
What are the parts of the brain?

79
HEART
The heart is a hollow organ that pumps blood
throughout the blood vessel by repeated,
rhythmic contraction. The adult human heart has
mass of between 250 and 350 grams and is
about the size of a fist. It is situated in the left
side of chest cavity. The average human heart,
beating at 72 beats per minute. The main
function of heart is circulation.

80
BLOOD PRESSSURE
Blood pressure is the force of blood pushing up
against the blood vessel walls. The higher the
pressure the harder the heart has to pump and it
increases the work load of heart.
A blood pressure reading appears to be 2
numbers. The first and higher of the two is a
measure of systolic pressure is the peak pressure
in the arteries, which occurs near the end of the
cardiac cycle when the ventricles are
contracting. Diastolic pressure is the minimum
pressure in the arteries, which occurs near the
beginning of the cardiac cycle when the
ventricles are filled with blood.
The blood pressure usually is measured with a
small, portable instrument called a blood
pressure cuff( sphygmomanometer). Unit is the
millimeters of mercury (mm Hg).
Explaining
Listening
Charts,
flash
cards.

81
2minutes Defines the term
hypertension
HYPERTENSION
Hypertension, also referred to as high blood
pressure, is a condition in which arteries have
persistently elevated blood pressure. Every time
the human heart beats, it pumps blood to the
whole body through the arteries.
High blood pressure is called “silent killer”
because it often causes no symptoms for many
years, even decades.
Recommendations of joint national
committee on prevention detection evaluation,
treatment of high blood pressure, the
classification of blood pressure for adults aged
18 years or older as follows.
Defines the
term
hypertension
Listens and
observes the
chart and
flash card
Charts,
flash
cards.
What is hypertension?

82
People with more than two blood pressure
readings of 140/90 or higher, are said to have
high blood pressure. If the pressure remains
high, your doctor will probably begin treatment.
2minutes Lists the causes of
hypertension CAUSES
The exact causes of hypertension are usually
unknown these include:
Obesity or being overweight
Diabetes
Smoking
Sedentary lifestyle
Lack of physical activity
High levels of salt intake
Insufficient calcium, potassium, and
magnesium consumption
Vitamin D deficiency
High levels of alcohol consumption.
Explains the
causes of
hypertension
Listens
observes the
flash cards
Flash cards
List down the causes of hypertension?

83
Stress
Aging
Medicines such as birth control pills
Genetics and a family history of
hypertension
Chronic kidney disease
Adrenal and thyroid problems or tumors
2minutes Lists the symptoms
of high blood
pressure
SYMPTOMS OF HIGH BLOOD
PRESSURE
One of the most dangerous aspects of
hypertension is that may not know that you have
it. The main symptoms are severe headache,
dizziness, blurred vision.
Explains the
symptoms of
hypertension
Listens and
observes
charts
charts List down the symptoms of high blood pressure.

84
3minutes Discusses the
complications of
hypertension
COMPLICATIONS
One of the main complication which occur due
to uncontrolled hypertension is stroke. The main
organs affected by hypertension are heart, eye
and kidney.
Enumerates
the
complications
of
hypertension
Listens and
observes
charts
charts List down the complications.

85
3minutes Defines the term
stroke STROKE
Stroke is the second leading cause of death
worldwide.
A stroke. Or cerebrovascular (CVA) is the
Rapid Loss Of Brain Function Due To
disturbance in the blood supply to the brain.
This can be used due to ischemia (lack of blood
flow ) caused by blockage (thrombosis, arterial
embolism ), or a hemorrhage.
Stroke is a medical emergency and can cause
permanent neurological damage and death. High
blood pressure is the most important modifiable
risk factor of stroke.
The patient may suddenly lose the ability to
speak, there may be memory problems, or one
side of the body can become paralyzed. If a
person has paralysis on right side of body, left
side of brain is affected.
Defines stroke Listens and
observes
charts
chart What is stroke?
5minutes Explains the
incidence INCIDENCE
According to WHO, high blood pressure
contributes more than 12.7 million of stroke
worldwide .Stroke deaths in India reached 9.2%
of total deaths
Explains the
incidence
Listens What’s the incidence rate?
7minutes Lists the types of
hypertension TYPES
The two main types of stroke include ischemic
stroke and hemorrhagic stroke.
Explains the
types of
hypertension
Listens and
observes
cards
Flash cards List the types
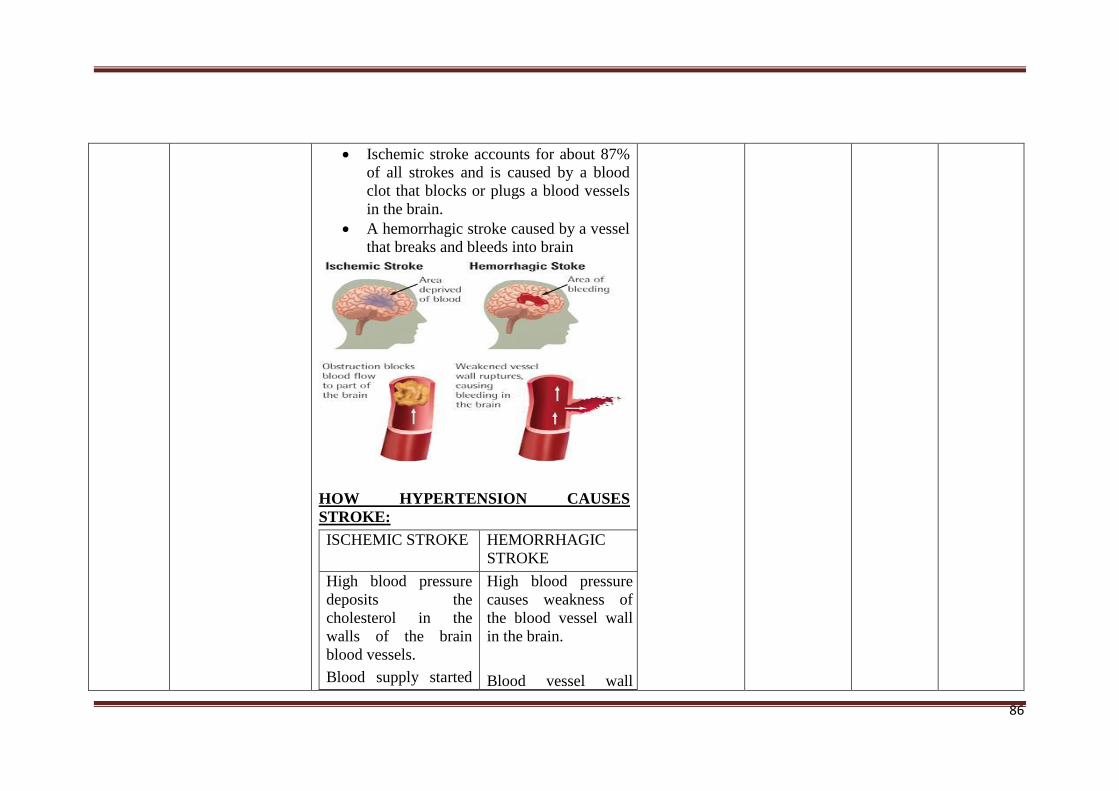
86
Ischemic stroke accounts for about 87%
of all strokes and is caused by a blood
clot that blocks or plugs a blood vessels
in the brain.
A hemorrhagic stroke caused by a vessel
that breaks and bleeds into brain
HOW HYPERTENSION CAUSES
STROKE:
ISCHEMIC STROKE HEMORRHAGIC
STROKE
High blood pressure
deposits the
cholesterol in the
walls of the brain
blood vessels.
Blood supply started
High blood pressure
causes weakness of
the blood vessel wall
in the brain.
Blood vessel wall

87
to reduce. Blood cells
trapped over the
cholesterol deposited
area.
Gradually, blood
vessel perimeter
reduces.
stretch and become
balloon shaped.
Continues high blood
pressure rupture the
weakened blood
vessel.
Alteration in the blood supply of brain causes in
metabolism changes within 30 seconds
Metabolism interrupted within 2 min
Brain cells activity reduced and dies within
5min
3minutes Discuss the
symptoms SYMPTOMS
a) Face dropping
b) Arm/leg weakness,
c) Speech difficulty
d) Paralysis or numbness in any part of the
body
e) Nausea and vomiting
f) Difficulty in walking
g) Irregular breathing
h) Loss of consciousness
Discusss the
symptoms
Listens and
observes
charts
charts List down the symptoms?

88
10minutes Explains the
prevention of
stroke
PREVENTION
Many factors help to reduce blood pressure
there by preventing the risk of stroke.
1.DASH-DIET PLAN
a) The DASH eating plan is based on2000
calories a day.
b) The low salt dietary approaches to stop
hypertension on are proven to lower
blood pressure<2g/day Sodium),(5g/day
Salt) in adults. This diet is not only rich
Explains the
prevention of
stroke
Listens and
observes
cards
Flashcards,
charts
List down the prevention?
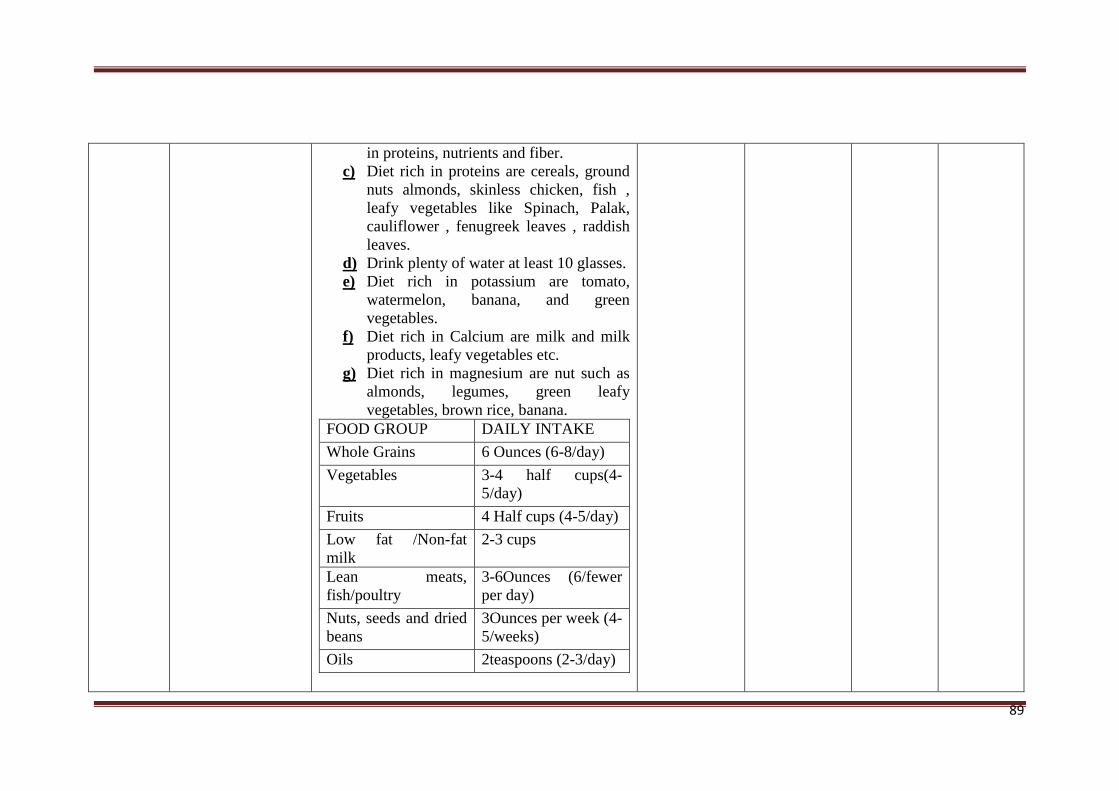
89
in proteins, nutrients and fiber.
c) Diet rich in proteins are cereals, ground
nuts almonds, skinless chicken, fish ,
leafy vegetables like Spinach, Palak,
cauliflower , fenugreek leaves , raddish
leaves.
d) Drink plenty of water at least 10 glasses.
e) Diet rich in potassium are tomato,
watermelon, banana, and green
vegetables.
f) Diet rich in Calcium are milk and milk
products, leafy vegetables etc.
g) Diet rich in magnesium are nut such as
almonds, legumes, green leafy
vegetables, brown rice, banana.
FOOD GROUP DAILY INTAKE
Whole Grains 6 Ounces (6-8/day)
Vegetables 3-4 half cups(4-
5/day)
Fruits 4 Half cups (4-5/day)
Low fat /Non-fat
milk
2-3 cups
Lean meats,
fish/poultry
3-6Ounces (6/fewer
per day)
Nuts, seeds and dried
beans
3Ounces per week (4-
5/weeks)
Oils 2teaspoons (2-3/day)

90
DRUG :
You should always take blood pressure
medications as prescribed by the
physician.
Never skip a dose/ abruptly stop taking
your blood pressure medications.
Suddenly stopping blood pressure drugs,
can cause a sharp increase in blood
pressure (rebound hypertension).
Daily maintain the timings while taking
medication and report to the physician if
any side effects like Giddiness/Vertigo,
Headache.
2. EXERCISE REGULARLY
People should be indulged in normal physical
activities to get significant healthy benefits.
Exercises will lower blood pressure by an
average of 5-10mmHg.Daily exercising for 20-
30 minutes very good. Some of the regular
exercises which can be done regularly.
AEROBIC EXERCISES:
These are the activities involving large
muscles done for the extended period of time,
that makes the lungs and heart work for harder.
It can be done for weight loss, also will provide
cardiovascular benefits. Examples are walking,
cycling swimming, jogging etc. for 5-

91
7days/week.
3.QUIT SMOKING
Smoking increases blood pressure because
Nicotine is a stimulant and it narrows the lumen
of blood vessels. Smoking raises blood pressure
from 5-10mmHg or more
4.REDUCE STRESS
a) Go for a walk 30-45 minutes/day
92
b) Call a good friend
c) Listen to music
d) Drink cup of coffee
5.REDUCE SALT INTAKE
Obesity can lead to disease such as diabetes
mellitus type2, high blood cholesterol. The body
mass index (BMI) should be 20-25. If BMI is
calculated as wt./ht m2.
The most effective method for weight loss is
reducing the number of calories consumed while
burning the calories through physical activity.
You can achieve this either by cutting back on
your food intake, by increasing physical
activity, or ideally, by doing both.
6.MANAGING HIGH BLOOD PRESSURE
High blood pressure usually has no warning
signs. Therefore, it is important that you have

93
regular blood pressure checks. Regular blood
pressure monitoring is done to detect the early
symptoms of complications.
7.LIMIT THE INTAKE OF ALCOHOL
Alcohol is a targeted culprit in boosting blood
pressure hypertension makes your heart work
harder than the normal, increase the stress on
your heart muscle which, cause irregular
heartbeats high blood pressure can also lead to
putting you at high risk for stroke.

94
8.GET ENOUGH SLEEP
In a recent study, both systolic and diastolic
blood pressure was higher in people who slept
less than 8 hours at night. Sleep helps to
regulate stress hormones and maintains health of
nervous system.
2minutes CONCLUSION
Hypertension can be controlled by the life style
modification. The health should be maintained
by person to avoid ill effects, because
prevention is better than cure.
BIBILOGRAPHY
1. Lewis text book of medical surgical nursing
(13th edn)Elsevier New Delhi, (2013)1466-
1489
2. Brunner and Siddarth medical surgical
nursing (10th edn) LWW
Philadelphia,(2007),1891-1971

95
3. Joyce M. Black medical surgical nursing (7th
edn) Elsevier New Delhi, (2007)
4. Nettina. Ms Lippincott manual of nursing
practice (8th edn) jaypee brother medical
publishers New Delhi,(2006),490-493
5.Susan L Woods cardiac nursing. (5th edn) ,
Lippincott Williams & Wilkins Philadelphia.
(2005)

96
gÉÆÃVUÀ½UÉ PÀ£ÉìAmï ¥sÁªÀiïð DwäÃAiÀÄ ¥ÀæwªÁ¢, £Á£ÀÄ «Ä¸ï. PÉÆÃl¥ÀÄj ¥ÀævÀÄåµÁ 2£Éà ªÀµÀð ²æà zsÀªÀÄð¸ÀܼÀ ªÀÄAdÄ£ÁxÉñÀégÀ «±Àé«zÁå®AiÀÄzÀ
£À¹ðAUï «zÁåyð zsÁgÀªÁqÀ, PÉÆøïð CªÀ±ÀåPÀvÉAiÀÄ ¨sÁUÀ±ÀB ¥ÀÆtðUÉƽ¸ÀÄ«PÉAiÀÄ°è £Á£ÀÄ ²æà zsÀªÀÄð¸ÀܼÀ
ªÀÄAdÄ£ÁxÉñÀégÀ «±Àé«zÁå®AiÀÄzÀ £À¹ðAUï ¸ÉÊ£Àì¸ï zsÁgÀªÁqÀUÉ ªÀÄgÀÄ¥ÀqÉAiÀÄÄ«PÉ AiÉÆÃd£ÉAiÀÄ£ÀÄß
PÉÊUÉƼÀî¨ÉÃPÁVzÉ.
£À£Àß AiÉÆÃd£ÉAiÀÄ ²Ã¶ðPÉAiÉÄAzÀgÉ, “ªÀvÀð£ÉAiÀÄ §zÀ¯ÁªÀuÉAiÀÄ ¸ÀAªÀºÀ£À ¥ÀjuÁªÀÄPÁjvÀéªÀ£ÀÄß ªÀiË®åªÀiÁ¥À£À ªÀiÁqÀĪÀ AiÀiÁªÀÅzÉà eÁÕ£ÀzÀ §UÉÎ ªÀÄvÀÄÛ
C sÁå¸ÀzÀ §UÉÎ ªÉÆzÀ¯Éà ¥ÀvÉÛ ºÀZÀѯÁV®è, C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ gÉÆÃVUÀ½UÉ ¥ÀjuÁªÀÄPÁjAiÀiÁVzÉ, zsÁgÀªÁqÀ
vÀÈwÃAiÀÄ DgÉÊPÉ D ÀàvÉæAiÀÄ°è N¦rUÉ ºÁdgÁUÀĪÀ ÉÃUÀ£É ¥ÀvÉÛAiÀiÁzÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ gÉÆÃVUÀ¼À°è ¥Á±ÀéðªÁAiÀÄÄ
vÀqÉUÀlÄÖªÀ §UÉÎ.”
F CzsÀåAiÀÄ£ÀzÀ £ÀAvÀgÀzÀ ºÀAvÀzÀ°èAiÉÄà ªÀiË®åªÀiÁ¥À£À ªÀiÁqÀ¨ÉÃPÁUÀÄvÀÛzÉ. eÁÕ£À ªÀÄvÀÄÛ C sÁå¸ÀzÀ PÀÄjvÀÄ vÀ¤SÁ¢üPÁj «£Áå¸ÀUÉƽ¹zÀ ªÀvÀð£ÉAiÀÄ §zÀ¯ÁªÀuÉAiÀÄ ¸ÀAªÀºÀ£À.
»ÃUÁV ¨ÉÃUÀ£É ¥ÀvÉÛAiÀiÁzÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ gÉÆÃVUÀ¼À eÁÕ£À ªÀÄvÀÄÛ C¨sÁå ÀªÀ£ÀÄß ªÀiË®åªÀiÁ¥À£À ªÀiÁqÀ®Ä
ªÀÄvÀÄÛ eÁÕ£À ªÀÄvÀÄÛ C¨sÁå¸ÀªÀ£ÀÄß £À«ÃPÀj¸À®Ä CzsÀåAiÀÄ£ÀzÀ ¸ÀªÀÄAiÀÄzÀ°è, F CzsÀåAiÀÄ£ÀzÀ°è ¨sÁUÀªÀ»¸À®Ä
¤ªÀÄä£ÀÄß «£ÀAw¸À¯ÁVzÉ CzsÀåAiÀÄ£ÀzÀ «ªÀgÀUÀ¼ÀÄ.
¢£À 1 gÀAzÀÄ, ¥ÀƪÀð¨sÁ« ªÀÄzsÀå¹ÜPÉ eÁÕ£À ªÀÄvÀÄÛ C¨sÁå¸ÀªÀ£ÀÄß ¤tð¬Ä À®Ä ¥ÉæmÉ ïÖ £ÀqÉ À¯ÁUÀÄvÀÛzÉ.
(¢£ÀPÉÌ 5 gÉÆÃVUÀ¼À£ÀÄß vÉUÉzÀÄPÉƼÀî¯ÁUÀÄvÀÛzÉ)
gÉÆÃVUÉ «°AiÀÄ£ÀÄß ¤ÃqÀ¯ÁUÀĪÀÅzÀÄ ¥Á±ÀéðªÁAiÀÄÄ vÀqÉUÀlÄÖ«PÉ PÀÄjvÀÄ ¨ÉÆÃzsÀ£É ªÀÄvÀÄÛ qɪÉÆUÉ
ºÁdgÁUÀ®Ä £ÉêÀÄPÁw
CzÉà ¢£À ©¹¹ ¥sÁèöåµï PÁqïðUÀ¼ÀÄ, ZÁmïðUÀ¼ÀÄ ªÀÄvÀÄÛ PÀgÀ¥ÀvÀæUÀ¼À£ÀÄß §¼À¹PÉÆAqÀÄ G¥À£Áå¸ÀzÀ
¸ÀºÁAiÀÄ¢AzÀ ¨ÉÆÃzsÀ£É ¤ÃqÀ¯ÁUÀĪÀÅzÀÄ.
KvÀ£ÀäzsÉå, ¨ÉÆÃzsÀ£Á C¢üªÉñÀ£ÀzÀ £ÀAvÀgÀ, gÉÆÃVUÀ¼ÀÄ vÀªÀÄä C£ÀĪÀiÁ£ÀUÀ¼À£ÀÄß ¸ÀºÀ
vÉgÀªÀÅUÉƽ¸À§ºÀÄzÀÄ; AiÀiÁªÀÅzÁzÀgÀÆ EzÀÝgÉ, vÀ¤SÁ¢üPÁjAiÉÆA¢UÉ ZÀað¸ÀĪÀ ªÀÄÆ®PÀ
£ÀqÀªÀ½PÉAiÀÄ §zÀ¯ÁªÀuÉ.
£ÀqÀªÀ½PÉAiÀÄ §zÀ¯ÁªÀuÉAiÀÄ ¸ÀAªÀºÀ£À ¥ÀjuÁªÀÄPÁjvÀéªÀ£ÀÄß PÀAqÀÄ »rAiÀÄ®Ä ºÀ¸ÀÛPÀë¥ÀzÀ 7£ÉÃ
¢£ÀzÀAzÀÄ ¥ÉÆøïÖmɸïÖ «® C£ÀÄß £ÀqÉ À¯ÁUÀÄvÀÛzÉ.

97
¤ÃªÀÅ ¤ÃrzÀ ªÀiÁ»wAiÀÄ£ÀÄß zÀÈqsÀªÁV «±Áé¸ÁºÀðªÁV Ej¸À¯ÁUÀĪÀÅzÀÄ JAzÀÄ ¤ªÀÄUÉ ¨sÀgÀªÀ É ¤Ãr,
¤ÃªÀÅ F CzsÀåAiÀÄ£ÀzÀ°è ¨sÁUÀªÀ»¸À®Ä ¹zÀÝjzÀÝgÉ zÀAiÀÄ«lÄÖ M¦àUÉUÉ À» ªÀiÁr.
vÀªÀÄä «±Áé¹,
PÉÆÃl¥ÀÄj ¥ÀævÀÄåµÁ 2£Éà ªÀµÀðzÀ JA.J¸ï.¹.
£À¹ðAUï «zÁåyð ¸ÀܼÀ : ¢£ÁAPÀ :
F CzsÀåAiÀÄ£ÀzÀ°è ¥ÀjµÀÌj¸À®Ä ªÁ®AnÃgï ªÀÄvÀÄÛ PÀ£ÉìAmï. EzÀÄ £À£Àß ¸ÀéAvÀ ¨sÁµÉUÉ N¢zÉ CxÀªÁ
n N¢zÉ. £À£ÀUÉ ¸ÀA¥ÀÆtðªÁV «ªÀj À¯ÁVzÉ ªÀÄvÀÄÛ AiÀiÁªÀÅzÉà ¸ÀªÀÄAiÀÄzÀ°è CzsÀåAiÀÄ£À¢AzÀ £À£Àß ¸ÀéAvÀ
¸ÀºÁAiÀÄ¢AzÀ qËmïUÀ¼ÀÄ / ¥Àæ±ÉßUÀ½UÉ E£Éé¹ÖUÉÃlgï ªÀÄÆ®PÀ £Á£ÀÄ ºÉýzÉÝãÉ.
sÁUÀªÀ»¸ÀĪÀªÀgÀ ºÉ¸ÀgÀÄ ªÀÄvÀÄÛ
sÁUÀªÀ»¸ÀĪÀªÀgÀ «¼Á¸À
sÁUÀªÀ»¸ÀĪÀªÀgÀ
À»
ÀA±ÉÆÃzsÀPÀgÀ ºÉ¸ÀgÀÄ
¸ÀA±ÉÆÃzsÀPÀgÀ
À»
¢£ÁAPÀ ¢£ÁAPÀ
CzsÀåAiÀÄ£ÀzÀ GzÉÝñÀzÀ §UÉÎ w½¸À ÁVzÉ ªÀÄvÀÄÛ CzsÀåAiÀÄ£ÀzÀ°è £À£Àß M¦àUÉ PÀrªÉÄ «ªÀgÀªÀ£ÀÄß
¸ÀéAiÀÄA¥ÉæÃgÀuɬÄAzÀ ¤ÃqÀÄvÉÛãÉ.
¥ÀæwªÁ¢AiÀÄ ¸À»
ºÉ¸ÀgÀÄ ¸ÀܼÀ : ¢£ÁAPÀ :

98
C£ÀħAzsÀ – 1
«¨sÁUÀ 1 - ¸ÉƹAiÉÆ qɪÉÆUÁæ¦üPï ¥ÉÆæ¥sÁªÀiÁð
1) ªÀµÀð¥ÀÆwð ªÀAiÀĸÀÄì [ ]
2) ²PÀët [ ]
3) GzÉÆåÃUÀ [ ]
4) PÀÄlÄA§zÀ ªÀiÁ¹PÀ DzÁAiÀÄ [ ]
5) PÀȶ ¥ÀæPÁgÀ
C) ¥ÀgÀªÀiÁtÄ [ ]
D) dAn [ ]
6) DºÁgÀ
C) ¸À¸ÁåºÁj [ ]
D) «Ä±Àæ DºÁj [ ]
7) C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ AiÀiÁªÀÅzÉà PÀÄlÄA§zÀ EwºÁ¸À
C) ºËzÀÄ
(PÀÄlÄA§zÀ AiÀiÁgÁzÀgÀÆ EzÀÝgÉ ¤¢ðµÀ×¥Àr¹)
[ ]
D) E®è [ ]

99
«¨sÁUÀ – 1
gÀZÀ£É eÁÕ£À ¥Àæ±Éß ¸ÀÆZÀ£ÉUÀ¼ÀÄ DwäÃAiÀÄ ¨sÁUÀªÀ»¸ÀĪÀªÀgÀÄ 1) zÀAiÉĬÄAzÀ PɼÀV£À ¥Àæ±ÉßUÀ¼À£ÀÄß N¢ ªÀÄvÀÄÛ ÀÆZÀ£ÉUÀ¼À£ÀÄß C£ÀĸÀj¹
2) ¥Àæw ¥Àæ±ÉßUÉ PɼÀUÉ ¤ÃrgÀĪÀ DAiÉÄÌUÀ½AzÀ ºÉZÀÄÑ ÀÆPÀÛªÁzÀ GvÀÛgÀªÀ£ÀÄß DAiÉÄ̪ÀiÁr ªÀÄvÀÄÛ
nPï ªÀiÁr
3) J¯Áè ¥Àæ±ÉßUÀ½UÉ GvÀÛj¸ÀĪÀÅzÀÄ ªÀÄÄRå JA§ÄzÀ£ÀÄß zÀAiÀÄ«lÄÖ UÀªÀĤ¹
4) ¸ÀjAiÀiÁzÀ GvÀÛgÀªÀ£ÀÄß 1 CAPÀ ªÀÄvÀÄÛ vÀ¥ÀÄà GvÀÛgÀªÀ£ÀÄß 0 CAPÀUÀ¼À£ÀÄß UÀ½ À¯ÁUÀÄvÀÛzÉ.
PÉÆÃqï ÀASÉå: ¢£ÁAPÀ:
¨sÁUÀ – 1 : ¥ÀƪÀð - ¸ÀA¥ÀPÀð
1) C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ CAzÀgÉ
C) PÁå£Àìgï [ ]
D) DWÁvÀ [ ]
E) ¥Á±ÀéðªÁAiÀÄÄ [ ]
F) PÀëAiÀÄ [ ]
2) zsÀƪÀÄ¥Á£ÀªÀÅ
C) ªÀÄÆvÀæ¦AqÀ ªÉÊ¥sÀ®å [ ]
D) ¥Á±ÀéðªÁAiÀÄÄ [ ]

100
E) AiÀÄPÀÈwÛ£À ªÉÊ¥sÀ®å [ ]
F) G¹gÁlzÀ vÉÆAzÀgÉ [ ]
3) C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¸ÁªÀiÁ£ÀåªÁV
C) ¸ÀÖAmï Q®ègï [ ]
D) gÀºÀ¸Àå PÉƯÉUÁgÀ [ ]
E) gÀºÀ¸Àå PÉƯÉUÁgÀ [ ]
F) ¸ÉʯÉAmï Q®ègï [ ]
4) MvÀÛqÀ ¤ªÀðºÀuÉUÉ EzÀÄ ¥ÀæªÀÄÄR ªÀiÁUÀðªÁVzÉ
C) ¸ÀjAiÀiÁzÀ «±ÁæAw [ ]
D) DgÉÆÃUÀåPÀgÀ DºÁgÀ [ ]
E) ¸ÀAVÃvÀªÀ£ÀÄß D°¹ [ ]
F) ªÉÄð£À J¯Áè [ ]
5) DgÉÆÃUÀåPÀgÀ vÀÆPÀªÀ£ÀÄß PÁ¥ÁrPÉƼÀî£ÀÄß MAzÀÄ C¼ÀvÉ
C) ¸ÁPÀµÀÄÖ zÀæªÀUÀ¼À£ÀÄß PÀÄr¬Äj [ ]
D) ¸ÀjAiÀiÁzÀ «±ÁæAw ªÀÄvÀÄÛ ¤zÉæ [ ]
E) zÉÊ»PÀ ZÀlĪÀnPÉ [ ]
F) ªÉÄð£À J¯Áè [ ]

101
6) ¤AiÀÄ«ÄvÀªÁV gÀPÀÛzÉÆvÀÛqÀzÀ ªÉÄðéZÁgÀuÉAiÀÄ£ÀÄß ªÀiÁqÀ¯ÁUÀÄvÀÛzÉ
C) vÉÆqÀPÀÄUÀ¼À DgÀA©üPÀ ®PÀëtUÀ¼À£ÀÄß ¥ÀvÉÛ ªÀiÁr [ ]
D) OµÀ¢üUÀ¼À£ÀÄß ¥ÁægÀA©ü¹ [ ]
E) ¤ÃªÀÅ C£ÁgÉÆÃUÀåPÉÌ M¼ÀUÁzÁUÀ ªÀiÁvÀæ ¥ÀjÃQë¹ [ ]
F) ¥Àæw 6 wAUÀ½UÉƪÉÄä ¥Àæw ¥Àj²Ã°¹ [ ]
¨sÁUÀ – 2 : aAvÀ£É
7) ¸ÉÆÖçÃPï JAzÀgÉãÀÄ
C) ºÀÈzÀAiÀiÁWÁvÀ [ ]
D) AiÀÄPÀÈwÛ£À ªÉÊ¥sÀ®å [ ]
E) «ÄzÀĽ£À zÁ½ [ ]
F) ªÀÄÆvÀæ¦AqÀ ªÉÊ¥sÀ®å [ ]
8) ¥Á±ÀéðªÁAiÀÄÄ ºÉÃUÉ ÀA¨sÀ«¸ÀÄvÀÛzÉ
C) ªÉÄzÀĽ£À°è gÀPÀÛ ºÉ¥ÀÄàUÀlÄÖ«PÉ [ ]
D) ºÀÈzÀAiÀÄzÀ°è gÀPÀÛ ºÉ¥ÀÄàUÀlÄÖ«PÉ [ ]
E) ªÀÄÆvÀæ¦AqÀzÀ°è gÀPÀÛ ºÉ¥ÀÄàUÀlÄÖ«PÉ [ ]
F) ±Áé¸ÀPÉÆñÀzÀ°è gÀPÀÛ ºÉ¥ÀÄàUÀlÄÖ«PÉ [ ]

102
9) ¸ÉÆÖçÃPï
C) vÀ¯É£ÉÆêÀÅ, ªÁPÀjPÉ ªÀÄvÀÄÛ ªÁAw [ ]
D) dégÀ, ªÁPÀjPÉ ªÀÄvÀÄÛ ¸É¼ÀªÀÅ [ ]
E) Cw¸ÁgÀ, dégÀ ªÀÄvÀÄÛ PÉÆêÀiÁ [ ]
F) ªÉÄî£À J¯Áè [ ]
10) C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ ¥Á±ÀéðªÁAiÀÄĪÀ£ÀÄß ºÉÃUÉ GvÁࢸÀÄvÀÛzÉ
C) J°Ö vÀ½UÀ¼ÀÄ, gÀPÀÛ£Á¼ÀUÀ¼À£ÀÄß zÀħð®UÉƽ¸ÀÄvÀÛzÉ ªÀÄvÀÄÛ ºÁ¤UÉƽ¸ÀÄvÀÛªÉ [ ]
D) n gÀPÀÛ£Á¼ÀUÀ¼À£ÀÄß ¸Àr®UÉƽ¸ÀÄvÀÛzÉ [ ]
E) EzÀÄ PÉƯɸÁÖç¯ï ªÀÄlÖªÀ£ÀÄß ºÉaÑ ÀÄvÀÛzÉ [ ]
F) EzÀÄ gÀPÀÛzÀ°è£À »ªÉÆÃUÉÆèé£ï ªÀÄlÖªÀ£ÀÄß ºÉaÑ ÀÄvÀÛzÉ [ ]
¨sÁUÀ – 3 : vÀAiÀiÁj
11) C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ gÉÆÃVUÀ¼À G¥ÀÄà ¸ÉêÀ£ÉAiÀÄÄ
C) ¤°è¹ [ ]
D) ¹Ã«ÄvÀ [ ]
E) ºÉZÁÑVzÉ [ ]
F) ¸ÉÆÃrAiÀÄA ¸ÉêÀ£ÉAiÀÄÄ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀPÉÌ ¸ÀA§A¢ü¹®è [ ]

103
12) EzÀÄ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀPÉÌ ¸ÀÆPÀÛªÀ®èzÀ DºÁgÀªÁVzÉ
C) ºÀtÄÚUÀ¼ÀÄ [ ]
D) qÉÊj DºÁgÀUÀ¼ÀÄ [ ]
E) «Ä±Àæ DºÁgÀ [ ]
F) G¥ÀÄà DºÁgÀUÀ¼ÀÄ [ ]
13) M§â ªÀåQÛAiÀÄÄ ¢£ÀzÀ°è JµÀÄÖ UÀAmÉUÀ¼À PÁ® ªÀÄ®UÀ¨ÉÃPÀÄ
C) 4 – 5 UÀAmÉUÀ¼ÀÄ [ ]
D) 6 – 7 UÀAmÉUÀ¼ÀÄ [ ]
E) 7 – 8 UÀAmÉUÀ¼ÀÄ [ ]
F) 9 – 10 UÀAmÉUÀ¼ÀÄ [ ]
14) ¸ÁªÀiÁ£Àå gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß PÁ¥ÁrPÉƼÀî®Ä zÉÊ£ÀA¢£À ²¥sÁgÀ¸ÀÄ ªÀiÁrzÀ
ªÁåAiÀiÁªÀÄ
C) 10 – 20 ¤«ÄµÀUÀ¼ÀÄ [ ]
D) 20 – 30 ¤«ÄµÀUÀ¼ÀÄ [ ]
E) 30 – 40 ¤«ÄµÀUÀ¼ÀÄ [ ]
F) 60 – 70 ¤«ÄµÀUÀ¼ÀÄ [ ]

104
¤ªÀðºÀuÉ ¥ÀæªÀiÁt
PÀæ. ¸ÀA. «ªÀgÀUÀ¼ÀÄ ºËzÀÄ E®è
1 £Á£ÀÄ ¤UÀ¢vÀ OµÀ¢üUÀ¼À£ÀÄß ¸ÀªÀÄAiÀÄPÉÌ ¤AiÀÄ«ÄvÀªÁV vÉUÉzÀÄPÉƼÀÄîvÉÛãÉ
2 ¤UÀ¢vÀ OµÀ¢üUÀ¼À£ÀÄß vÉUÉzÀÄPÉƼÀÄîªÀÅzÀÄ ¸ÁªÀiÁ£Àå ªÀÄlÖzÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß
PÁ¥ÁrPÉƼÀî®Ä ¸ÀºÁAiÀÄ ªÀiÁqÀÄvÀÛzÉ
3 £Á£ÀÄ AiÀiÁªÁUÀ®Æ ¢£À¤vÀåzÀ DgÉÆÃUÀå vÀ¥Á¸ÀuÉUÉ M¼ÀUÁUÀÄvÉÛãÉ.
4 M§â ªÀåQÛAiÀÄÄ ¢£ÀPÉÌ PÀ¤µÀ× 8 UÁè¸ï ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ
5 £Á£ÀÄ ªÁgÀzÀ°è (5 ¢£ÀUÀ¼ÀÄ) ¥Àæw¢£À 30 ¤«ÄµÀUÀ¼À ªÀÄzsÀåªÀÄ ªÁåAiÀiÁªÀĪÀ£ÀÄß ªÀiÁqÀÄvÉÛ£É
6 M§â ªÀåQÛAiÀÄÄ ªÁgÀzÀ°è 3 jAzÀ 4 ¨Áj ªÁåAiÀiÁªÀÄ ªÀiÁqÀ¨ÉÃPÁUÀÄvÀÛzÉ
7 £Á£ÀÄ ¤AiÀÄ«ÄvÀªÁV £À£Àß vÀÆPÀªÀ£ÀÄß ¥Àj²Ã°¸ÀÄvÉÛãÉ
8 £Á£ÀÄ AiÀiÁªÁUÀ®Æ PÀrªÉÄ PÉÆ©â£À DºÁgÀªÀ£ÀÄß ªÀiÁvÀæ vÉUÉzÀÄPÉƼÀÄîvÉÛãÉ
9 dAPï ¥sÀÄqïUÀ¼À£ÀÄß DUÁUÉ ¸Éë¸ÀĪÀÅzÀjAzÀ ¸ÁªÀiÁ£Àå gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß
PÁ¥ÁrPÉƼÀÄîvÀÛzÉ
10 £Á£ÀÄ AiÀiÁªÁUÀ®Æ DºÁgÀ ¸ÀªÀÄAiÀĪÀ£ÀÄß ¤AiÀÄ«ÄvÀªÁV C£ÀĸÀj ÀÄvÉÛãÉ
11 £À£Àß DºÁgÀzÀ°è ºÀtÄÚUÀ¼ÀÄ ªÀÄvÀÄÛ vÀgÀPÁjUÀ¼À£ÀÄß ¸ÉÃj¸ÀÄvÉÛãÉ
12 £À£Àß DºÁgÀzÀ°è 1-2 (0.35 UÁæA) mÉç¯ï ZÀªÀÄZÀ G¥Àà£ÀÄß ¸ÉÃj¸ÀÄvÉÛãÉ
13 G¦à£ÀA±ÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀĪÀÅzÀÄ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¤AiÀÄAwæ¸À®Ä ¸ÀºÁAiÀÄ ªÀiÁqÀÄvÀÛzÉ
14 £Á£ÀÄ ¸ÀªÀÄvÉÆð£À DºÁgÀªÀ£ÀÄß ¸Éë¸ÀÄvÉÛãÉ
15 £Á£ÀÄ D¯ÉÆÌúÁ¯ï ¸ÉêÀ£ÉAiÀÄ£ÀÄß «ÄwUÉƽ¸ÀÄvÉÛãÉ
16 £Á£ÀÄ zsÀƪÀÄ¥Á£ÀªÀ£ÀÄß vÀåf¸ÀÄvÉÛãÉ
17 £Á£ÀÄ PÁ¦üAiÀÄ£ÀÄß PÀrvÀUÉƽ¸ÀÄvÉÛãÉ

105
18 £À£Àß MvÀÛqÀzÀ ªÀÄlÖªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ®Ä £Á£ÀÄ zsÁå£À ªÀiÁqÀÄvÉÛãÉ
19 C¢üPÀ gÀPÀÛzÉÆvÀÛqÀzÀ gÉÆÃVUÀ¼ÀÄ vÀÆPÀ CxÀªÁ zsÁgÀªÁqÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß
JvÀÄÛªÀÅzÀ£ÀÄß vÀ¦à¸À ÉÃPÀÄ
20 ¥Á±ÀéðªÁAiÀÄÄ EgÀĪÀ ªÀåQÛUÉ vÀPÀët D¸ÀàvÉæUÉ zÁR®Ä ªÀiÁqÀĪÀ CUÀvÀå«zÉ
21 fêÀ£À ±ÉÊ° ªÀiÁ¥ÁðqÀÄ ¸ÁªÀiÁ£Àå gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¤ªÀð»¸ÀĪÀ ªÉÆzÀ® ºÀAvÀªÁVzÉ
22 zÉÊ»PÀ ZÀlĪÀnPÉAiÀÄ ªÀÄlÖªÀ£ÀÄß ºÉaÑ À®Ä £Á£ÀÄ ªÁQAUï ªÀivÀÄÛ vÉÆÃlUÁjPÉ ªÀÄÄAvÁzÀ ZÀlĪÀnPÉUÀ¼À£ÀÄß ªÀiÁqÀÄvÉÛãÉ

106
¸ÀªÀÄAiÀÄ ¤¢ðµÀ× GzÉÝñÀUÀ¼ÀÄ
«µÀAiÀÄ ²PÀëPÀgÀ ZÀlĪÀnPÉ
PÀ¯ÉAiÀÄĪÀªÀgÀ ZÀlĪÀnPÉ
J.«.Kqïì ªÀiË®åªÀiÁ¥À£À
02 ¤«ÄµÀ
«µÀAiÀĪÀ£ÀÄß ¥ÀjZÀ¬Ä¸ÀÄvÀÛzÉ
¥ÀjZÀAiÀÄ
fêÀ£À ±ÉÊ°AiÀÄ PÁ¬Ä¯ÉUÀ¼ÀÄ ¸ÁªÀiÁ£ÀåªÁV £ÀªÀÄä §zÀ¯ÁUÀÄwÛgÀĪÀ
£ÀUÀgÀ fêÀ£À «zsÁ£ÀPÉÌ ¸ÀA§A¢ü¹zÀ gÉÆÃUÀUÀ¼À UÀÄA¥ÁVzÉ. F
PÁ¬Ä¯ÉUÀ½UÉ PÁgÀtªÁUÀĪÀ ¥ÀæªÀÄÄR CA±ÀUÀ¼ÀÄ ºÉZÀÄÑ MvÀÛqÀ,
UÀrAiÀiÁgÀzÀ PÉ®¸ÀzÀ ¸ÀªÀÄAiÀĪÀ£ÀÄß ¸ÀÄvÀÄÛªÀÅzÀÄ, PÉlÖ DºÁgÀ ¥ÀzÀÞw
ªÀÄvÀÄÛ PÀrªÉÄ CxÀªÁ ªÁåAiÀiÁªÀÄ«®èzÀ d£À fêÀ£À. C£ÉÃPÀ
PÁ¬Ä¯ÉUÀ¼À°è £ÀªÀÄä fêÀ£À ±ÉÊ°AiÀÄÄ MAzÀÄ ¥ÀæªÀÄÄR
PÁgÀtªÁUÀĪÀ CA±ÀªÁVgÀ§ºÀÄzÀÄ CxÀªÁ C°è gÉÆÃUÀªÀ£ÀÄß
G®âtUÉƽ¸À§ºÀÄzÀÄ. fêÀ£À±ÉÊ°UÉ ¸ÀA§A¢ü¹zÀ ¥ÀæªÀÄÄR
PÁ¬Ä¯ÉAiÉÄAzÀgÉ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ
«µÀAiÀĪÀ£ÀÄß ¥ÀjZÀ¬Ä¸ÀÄvÀÛzÉ
PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ
¨sÁUÀªÀ»¸ÀÄ«PÉ
04 ¤«ÄµÀ
ªÉÄzÀļÀÄ ªÀÄvÀÄÛ ºÀÈzÀAiÀÄzÀ
CAUÀgÀZÀ£Á±Á¸ÀÛç ªÀÄvÀÄÛ
±ÀjÃgÀ±Á¸ÀÛçªÀ£ÀÄß «ªÀj¹
ªÉÄzÀļÀÄ ªÀÄvÀÄÛ ºÀÈzÀAiÀÄzÀ CAUÀgÀZÀ£Á±Á¸ÀÛç ªÀÄvÀÄÛ ±ÀjÃgÀ±Á ÀÛç
¨É£ÀÄߺÀÄjAiÉÆA¢UÉ ªÉÄzÀļÀÄ PÉÃAzÀæ £ÀgÀªÀÄAqÀ®ªÀ£ÀÄß gÀƦ¸ÀÄvÀÛzÉ.
EzÀÄ zÉúÀzÀ PÁAiÀÄðªÀ£ÀÄß ¸ÀªÀÄ£ÀéAiÀÄUÉƽ¸ÀĪÀ ¤AiÀÄAvÀæt
PÉÃAzÀæªÁVzÉ. ªÀiÁ£ÀªÀ£À ªÉÄzÀļÀÄ CwÃvÀªÁV ¥ÀgÀ ÀàgÀ ¸ÀA§AzsÀ
ºÉÆA¢zÉ DzÀgÉ ªÀÄÆgÀÄ ¥ÀæªÀÄÄR CA±ÀUÀ¼À£ÀÄß UÀÄgÀÄw¸À§ºÀÄzÀÄ.
¸ÉgɧæªÀiï, ¨ÉæöÊ£ï ¹¸ÀÖªÀiï ªÀÄvÀÄÛ ¸ÉgÉ É®èªÀiï. EzÀÄ zÉúÀzÀ
PÁAiÀÄðªÀ£ÀÄß ¸ÀªÀÄ£ÀéAiÀÄUÉƽ¸ÀĪÀ ¤AiÀÄAvÀæt PÉÃAzÀæªÁVzÉ.
CAUÀgÀZÀ£Á±Á¸ÀÛç ªÀÄvÀÄÛ
±ÀjÃgÀ±Á¸ÀÛçªÀ£ÀÄß «ªÀj ÀÄvÉÛãÉ
PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ
£ÉÆÃqÀĪÀÅzÀÄ
107
ºÀÈzÀAiÀÄ
ºÀÈzÀAiÀĪÀÅ mÉƼÁîzÀ CAUÀªÁVzÀÄÝ, gÀPÀÛ£Á¼ÀzÀÄzÀÝPÀÆÌ gÀPÀÛªÀ£ÀÄß
¥ÀÄ£ÀgÁªÀwðvÀ, ®AiÀħzÀÞ ¸ÀAPÉÆÃZÀ£ÀzÀ ªÀÄÆ®PÀ ¥ÀA¥ï
ªÀiÁqÀÄvÀÛzÉ. ªÀAiÀĸÀÌ ªÀiÁ£ÀªÀ ºÀÈzÀAiÀĪÀÅ 250 jAzÀ 350
UÁæAUÀ¼ÀµÀÄÖ zÀæªÀågÁ²AiÀÄ£ÀÄß ºÉÆA¢gÀÄvÀÛzÉ ªÀÄvÀÄÛ EzÀÄ ªÀÄĶÖAiÀÄ
UÁvÀæªÀ£ÀÄß ºÉÆA¢gÀÄvÀÛzÉ. EzÀÄ JzÉAiÀÄ PÀĺÀgÀzÀ JqÀ¨sÁUÀzÀ°èzÉ.
ªÀiÁ£ÀªÀ ºÀÈzÀAiÀĪÀÅ ¤«ÄµÀPÉÌ 72 §rvÀUÀ¼À£ÀÄß ºÉÆqÉAiÀÄÄvÀÛzÉ.
ºÀÈzÀAiÀÄzÀ ªÀÄÄRå PÁAiÀÄðªÉAzÀgÉ gÀPÀÛ¥ÀjZÀ®£É.
«ªÀj ÀÄvÉÛÃ£É PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ
£ÉÆÃqÀĪÀÅzÀÄ
gÀPÀÛzÉÆvÀÛqÀ
gÀPÀÛzÉÆvÀÛqÀªÀÅ gÀPÀÛ£Á¼ÀUÀ¼À UÉÆÃqÉUÀ¼À «gÀÄzÀÞ gÀPÀÛªÀ£ÀÄß vÀ¼ÀÄîªÀ
±ÀQÛAiÀiÁVzÉ. ºÉaÑ£À MvÀÛqÀªÀÅ ºÀÈzÀAiÀĪÀ£ÀÄß PÀptªÁV ¥ÀA¥ï
ªÀiÁqÀ¨ÉÃPÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ CzÀÄ ºÀÈzÀAiÀÄzÀ PÉ®¸ÀzÀ ºÉÆgÉ
ºÉaÑ ÀÄvÀÛzÉ. gÀPÀÛzÉÆvÀÛqÀ NzÀÄ«PÉ 2 ¸ÀASÉåUÀ¼ÀAvÉ PÀAqÀħgÀÄvÀÛzÉ.
JgÀqÀgÀ°è ªÉÆzÀ® ªÀÄvÀÄÛ ºÉaÑ£ÀzÀÄ ¹¸ÉÆÖ°Pï MvÀÛqÀzÀ
C¼ÀvÉAiÀiÁVzÀÄÝ, C¥ÀzsÀªÀĤUÀ¼À°è£À PÀ¤µÀ× MvÀÛqÀªÁVzÀÄÝ, EzÀÄ
PÀĺÀgÀUÀ¼ÀÄ gÀPÀÛ¢AzÀ vÀÄA©zÁUÀ ºÀÈzÀAiÀÄ ZÀPÀæzÀ ¥ÁægÀA¨sÀzÀ §½
¸ÀA¨sÀ« ÀÄvÀÛzÉ. gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¸ÁªÀiÁ£ÀåªÁV gÀPÀÛzÉÆvÀÛqÀzÀ PÀ¥sï
(¹ÖUÉÆäêÀÄ£ÉÆëÄÃlgï) JA§ ¸ÀtÚ ¥ÉÆÃlð§¯ï G¥ÀPÀgÀt¢AzÀ
C¼ÉAiÀįÁUÀÄvÀÛzÉ. AiÀÄÄ£Àmï ¥ÁzÀgÀ ÀzÀ «Ä°«ÄÃlgï (mmHg)
¸ÀgÁ¸Àj 5-10 JAJAºÉZïf PÀrªÉÄ ªÀiÁqÀÄvÀÛzÉ. 30 ¤«ÄµÀUÀ¼À
«ªÀj ÀÄvÉÛÃ£É PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ
£ÉÆÃqÀĪÀÅzÀÄ

108
PÁ® zÉÊ£ÀA¢£À ªÁåAiÀiÁªÀÄ vÀÄA¨Á M¼ÉîAiÀÄzÀÄ, ¤AiÀÄ«ÄvÀªÁV
ªÀiÁqÀ§ºÀÄzÁzÀ PÉ®ªÀÅ ¤AiÀÄ«ÄvÀ ªÁåAiÀiÁªÀÄUÀ¼ÀÄ, JgÉÆéPï
ªÁåAiÀiÁªÀÄUÀ¼ÀÄ «¸ÀÛøvÀ CªÀ¢üUÉ ªÀiÁrzÀ zÉÆqÀØ ¸ÁßAiÀÄÄUÀ¼À£ÀÄß
M¼ÀUÉÆAqÀ ZÀlĪÀnPÉUÀ¼ÀÄ EªÀÅ. EzÀÄ ±Áé¸ÀPÉÆñÀ ªÀÄvÀÄÛ
ºÀÈzÀAiÀĪÀ£ÀÄß UÀnÖAiÀiÁV PÉ®¸À ªÀiÁqÀÄvÀÛzÉ. vÀÆPÀ £ÀµÀÖPÉÌ EzÀ£ÀÄß
ªÀiÁqÀ§ºÀÄzÀÄ, ºÀÈzÀAiÀÄgÀPÀÛ£Á¼ÀzÀ ¥ÀæAiÉÆÃd£ÀUÀ¼À£ÀÄß ¸ÀºÀ ¤ÃqÀÄvÀÛzÉ.
ªÁQAUï, ¸ÉÊQèAUï, FdÄ, eÁVAUï EvÁå¢ GzÁºÀgÀuÉUÀ¼ÀÄ
zsÀƪÀÄ¥Á£ÀªÀ£ÀÄß ©r
zsÀƪÀÄ¥Á£ÀªÀÅ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ºÉaÑ ÀÄvÀÛzÉ KPÉAzÀgÉ ¤PÉÆÃn£ï
MAzÀÄ GvÉÛÃdPÀªÁVzÉ ªÀÄvÀÄÛ EzÀÄ gÀPÀÛ£Á¼ÀUÀ¼À ®ÄªÉÄ£ï C£ÀÄß
¸ÀAPÀÄavÀUÉƽ¸ÀÄvÀÛzÉ. zsÀƪÀÄ¥Á£ÀªÀÅ 5-10 CxÀªÁ ºÉaÑ£ÀzÀjAzÀ
gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ºÉaѸÀÄvÀÛzÉ.
MvÀÛqÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁr
¢£ÀPÉÌ 30-45 ¤«ÄµÀ £ÀrUÉUÉ ºÉÆÃV
GvÀÛªÀÄ ¸ÉßûvÀ£À£ÀÄß PÀgÉ ªÀiÁr
¸ÀAVÃvÀªÀ£ÀÄß D°¹

109
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ JAzÀÆ PÀgÉAiÀįÁUÀÄvÀÛzÉ,
EzÀgÀ°è C¥ÀzsÀªÀĤUÀ¼ÀÄ ¤gÀAvÀgÀªÁV gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ºÉaÑ ÀÄvÀÛªÉ.
ªÀiÁ£ÀªÀ£À ºÀÈzÀAiÀÄ §rzÁUÀ¯É¯Áè CzÀÄ C¥ÀzsÀªÀĤUÀ¼À ªÀÄÆ®PÀ
Erà zÉúÀPÉÌ gÀPÀÛªÀ£ÀÄß ¥ÀA¥ï ªÀiÁqÀÄvÀÛzÉ. C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß
¸ÉʯÉAmï Q®ègï JAzÀÄ PÀgÉAiÀįÁUÀÄvÀÛzÉ. KPÉAzÀgÉ EzÀÄ C£ÉÃPÀ
ªÀµÀðUÀ½AzÀ zÀ±ÀPÀUÀ¼ÀªÀgÉUÉ AiÀiÁªÀÅzÉà gÉÆÃUÀ®PÀëtUÀ¼À£ÀÄß GAlÄ
ªÀiÁqÀĪÀÅ¢®è. vÀqÉUÀlÄÖ«PÉ ¥ÀvÉÛ ªÀiË®åªÀiÁ¥À£À, C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ
aQvÉì, 18 ªÀµÀð ªÀAiÀĹì£À ªÀAiÀĸÀÌjUÉ CxÀªÁ »jAiÀÄgÀÄ.
gÀPÀÛzÉÆvÀÛqÀzÀ ªÀVÃðPÀgÀt PÀÄjvÀÄ dAn gÁ¶ÖçÃAiÀÄ ¸À«ÄwAiÀÄ
²¥sÁgÀ¸ÀÄUÀ¼ÀÄ F PɼÀV£ÀAvÉ.
140/90 CxÀªÁ CzÀQÌAvÀ ºÉaÑ£À gÀPÀÛzÉÆvÀÛqÀzÀ ªÁZÀ£ÀUÉÆöÖAiÀÄ£ÀÄß
ºÉÆA¢gÀĪÀ d£ÀgÀÄ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ºÉÆA¢zÁÝgÉAzÀÄ
ºÉüÀ¯ÁUÀÄvÀÛzÉ. MvÀÛqÀ ºÉZÁÑVzÀÝgÉ ¤ªÀÄä ªÉÊzÀågÀÄ §ºÀıÀB
aQvÉìAiÀÄ£ÀÄß ¥ÁægÀA©ü ÀÄvÁÛgÉ.
PÁgÀtUÀ¼ÀÄ:
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ ¤RgÀªÁzÀ PÁgÀtUÀ¼ÀÄ ¸ÁªÀiÁ£ÀåªÁV EªÀÅUÀ¼À°è
¸ÉÃjªÉ.
¨ÉÆdÄÓ CxÀªÁ C¢üPÀ vÀÆPÀ
ªÀÄzsÀĪÉÄúÀ
110
zsÀƪÀÄ¥Á£À
dqÀ fêÀ£À±ÉÊ°
zÉÊ»PÀ ZÀlĪÀnPÉ PÉÆgÀvÉ
G¥ÀÄà ¸ÉêÀ£ÉAiÀÄ ºÉaÑ£À ªÀÄlÖ
¸ÁPÀµÀÄÖ PÁå°ëAiÀÄA, ¥ÉÆmÁå²AiÀÄA ªÀÄvÀÄÛ ªÉÄVß²AiÀÄA
§¼ÀPÉ
«l«Ä£ï r PÉÆgÀvÉ
ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è C¯ÉÆÌúÁ¯ï ¸ÉêÀ£É
MvÀÛqÀ
ªÀAiÀĸÁìzÀ
d£À£À ¤AiÀÄAvÀæt ªÀiÁvÉæUÀ¼ÀAvÀºÀ OµÀ¢üUÀ¼ÀÄ
C¢PÀ gÀPÀÛzÉÆvÀÛqÀzÀ eÉ£ÉnPïì ªÀÄvÀÄÛ PÀÄlÄA§zÀ EwºÁ¸À
¢ÃWÀðPÁ®zÀ ªÀÄÆvÀæ¦AqÀ PÁ¬Ä¯É
ªÀÄÆvÀæd£À£ÁAUÀ ªÀÄvÀÄÛ xÉÊgÁAiÀiïØ ÀªÀĸÉåUÀ¼ÀÄ CxÀªÁ
UÀqÉØUÀ¼ÀÄ

111
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀzÀ ®PÀëtUÀ¼ÀÄ
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀzÀ CvÀåAvÀ C¥ÁAiÀÄPÁj CA±ÀªÉAzÀgÉ CzÀÄ
¤ªÀÄä°èzÉ JAzÀÄ w½¢gÀ§ºÀÄzÀÄ. wêÀæ vÀ¯É£ÉÆêÀÅ, vÀ¯ÉwgÀÄUÀÄ«PÉ,
zÀ馅 ªÀÄAzÀªÁUÀĪÀÅzÀÄ EzÀgÀ ¥ÀæªÀÄÄR ®PÀëtUÀ¼ÁVªÉ
vÉÆqÀPÀUÀ¼ÀÄ
C¤AiÀÄAwæPÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ¢AzÁV GAmÁUÀĪÀ MAzÀÄ ªÀÄÄRå
vÉÆqÀPÀÄ ¥Á±ÀéðªÁAiÀÄÄ. C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ¢AzÀ §¼À®ÄwÛgÀĪÀ
ªÀÄÄRå CAUÀUÀ¼ÀÄ ºÀÈzÀAiÀÄ, PÀtÄÚ ªÀÄvÀÄÛ ªÀÄÆvÀæ¦AqÀ
¥Á±ÀéðªÁAiÀÄÄ
¥Á±ÀéðªÁAiÀÄÄ «±ÀézÁzÀåAvÀ ¸Á«UÉ JgÀqÀ£Éà ¥ÀæªÀÄÄR PÁgÀtªÁVzÉ
¸ÉÆÖçÃPï CxÀªÁ ¸ÉgÉ ÉÆæªÁ¸ÀÄÌ®gï JAzÀgÉ ªÉÄzÀĽUÉ gÀPÀÛ
¥ÀÆgÉÊPÉAiÀÄ°è£À CqÀZÀuɬÄAzÁV ªÉÄzÀĽ£À PÁAiÀÄðZÀlĪÀnPÉAiÀÄ
vÀéjvÀ £ÀµÀÖ. vÀqÉUÀlÄÖ«PÉ (zsÀA©¹£ï, C¥ÀzsÀªÀĤAiÀÄ JA¨Á°¸ÀªÀiï)
CxÀªÁ gÀPÀÛ¸ÁæªÀ¢AzÀ GAmÁUÀĪÀ EµÉÌëÄAiÀiÁ (gÀPÀÛzÀ ºÀj«£À
PÉÆgÀvÉ)UÉ EzÀ£ÀÄß §¼À¸À§ºÀÄzÀÄ. ¥Á±ÀéðªÁAiÀÄÄ ªÉÊzÀåQÃAiÀÄ
vÀÄvÀÄð¹Üw ªÀÄvÀÄÛ EzÀÄ ±Á±ÀévÀ £ÀgÀªÉÊeÁÕ¤PÀ ºÁ¤ ªÀÄvÀÄÛ ¸Á«UÉ
PÁgÀtªÁUÀ§ºÀÄzÀÄ. C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ ¥Á±ÀéðªÁAiÀÄÄ«£À ¥ÀæªÀÄÄR
ªÀiÁ¥Àðr¸À§ºÀÄzÁzÀ C¥ÁAiÀÄPÁj CA±ÀªÁVzÉ gÉÆÃVAiÀÄÄ
EzÀÝQÌzÀÝAvÉ ªÀiÁvÀ£ÁqÀĪÀ ¸ÁªÀÄxÀåðªÀ£ÀÄß PÀ¼ÉzÀÄPÉƼÀÀÄzÀÄ,
ªÉĪÉÆj ¸ÀªÀĸÉåUÀ½gÀ§ºÀÄzÀÄ CxÀªÁ zÉúÀzÀ MAzÀÄ §¢

112
¥Á±ÀéðªÁAiÀÄÄ«UÉ M¼ÀUÁUÀ§ºÀÄzÀÄ. M§â ªÀåQÛAiÀÄÄ zÉúÀzÀ
§®¨sÁUÀzÀ°è ¥Á±ÀéðªÁAiÀÄÄ ºÉÆA¢zÀÝgÉ ªÉÄzÀĽ£À JqÀ¨sÁUÀªÀÅ
¥ÀjuÁªÀÄ ©ÃgÀÄvÀÛzÉ.
WÀl£ÉUÀ¼ÀÄ
WHO ¥ÀæPÁgÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ «±ÀézÁzÀåAvÀ 12.7 zÀ±À®PÀëPÀÆÌ
ºÉZÀÄÑ ¥Á±ÀéðªÁAiÀÄÄUÀ¼À£ÀÄß ¤ÃqÀÄvÀÛzÉ. ¨sÁgÀvÀzÀ°è ¥Á±ÀéðªÁAiÀÄÄ
¸ÁªÀÅUÀ¼À°è 9.2% vÀ®Ä¦zÉ.
jÃw:
¸ÉÆÖçÃPï JgÀqÀÄ ªÀÄÄRå «zsÀUÀ¼ÀÄ EµÉÌ«ÄPï ¸ÉÆÖçÃPï.
EµÉÌëÄPï ¸ÉÆÖçÃPï J¯Áè ¥Á±ÀéðªÁAiÀÄÄUÀ¼À°è ¸ÀĪÀiÁgÀÄ 87% £À¶ÖzÉ
ªÀÄvÀÄÛ EzÀÄ gÀPÀÛ ºÉ¥ÀÄàUÀlÄÖ«PɬÄAzÀ GAmÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ CzÀÄ
ªÉÄzÀĽ£À gÀPÀÛ£Á¼ÀªÀ£ÀÄß ¤§ðA¢ü¸ÀÄvÀÛzÉ CxÀªÁ ¥ÀèUï ªÀiÁqÀÄvÀÛzÉ.
ºÀqÀV¤AzÀ GAmÁUÀĪÀ gÀPÀÛ¸ÁæªÀzÀ ¥Á±ÀéðªÁAiÀÄÄ ªÀÄÄjzÀÄ
ªÉÄzÀĽUÉ gÀPÀÛ¸ÁæªÀªÁUÀÄvÀÛzÉ.
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ ¥Á±ÀéðªÁAiÀÄÄ«UÉ ºÉÃUÉ PÁgÀtªÁUÀÄvÀÛzÉ
EµÉÌ«ÄPï ¸ÉÆÖçÃPï
ªÉÄzÀĽ£À gÀPÀÛ£Á¼ÀUÀ¼À UÉÆÃqÉUÀ¼À°è PÉƯɸÁÖç¯ï£À°è C¢üPÀ
gÀPÀÛzÉÆvÀÛqÀ ÀAUÀæºÀªÁUÀÄvÀÛzÉ.
gÀPÀÛ ¥ÀÆgÉÊPÉ PÀrªÉÄAiÀiÁUÀ®Ä ¥ÁægÀA©ü¹vÀÄ. PÉƯɸÁÖç¯ï

113
¤PÉëÃ¥À ¥ÀæzÉñÀzÀ ªÉÄÃ¯É ¹QÌ©zÀÝ gÀPÀÛ PÀtUÀ¼ÀÄ.
PÀæªÉÄÃt gÀPÀÛ£Á¼ÀUÀ¼À ¥Àj¢üAiÀÄÄ PÀrªÉÄAiÀiÁUÀÄvÀÛzÉ.
ºÉªÀÄgÁfPï ÉÆÖçÃPï
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ ªÉÄzÀĽ£À°è gÀPÀÛ£Á¼ÀzÀ UÉÆÃqÉAiÀÄ
z˧ð®åPÉÌ PÁgÀtªÁUÀÄvÀÛzÉ
gÀPÀÛ£Á¼ÀzÀ UÉÆÃqÉ »Vι §®Æ£ï DPÁgÀPÉÌ §gÀÄvÀÛzÉ
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ zÀħð®UÉÆAqÀ gÀPÀÛ£Á¼ÀªÀ£ÀÄß
czÀæUÉƽ¸ÀÄvÀÛzÉ . ªÉÄzÀĽ£À gÀPÀÛ¥ÀÆgÉÊPÉAiÀÄ°è£À
§zÀ¯ÁªÀuÉAiÀÄÄ ZÀAiÀiÁ¥ÀZÀAiÀÄ QæAiÉÄAiÀÄ°è 30
¸ÉPÉAqÀÄUÀ¼À°è §zÀ¯ÁUÀÄvÀÛzÉ. ZÀAiÀiÁ¥ÀZÀAiÀÄ QæAiÉÄÃAiÀÄÄ 2
¤«ÄµÀUÀ¼À°è CqÀZÀuÉAiÀiÁVzÉ. ªÉÄzÀĽ£À PÉÆñÀUÀ¼À
ZÀlĪÀnPÉ 5 ¤«ÄµÀUÀ¼À°è PÀrªÉÄAiÀiÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ
¸ÁAiÀÄÄvÀÛzÉ.
®PÀëtUÀ¼ÀÄ
¥sÉøï qÁæ¦AUï
vÉÆüÀÄ / PÁ®Ä z˧ð®å
ªÀiÁw£À vÉÆAzÀgÉ
zÉúÀzÀ AiÀiÁªÀÅzÉà ¨sÁUÀzÀ°è ¥Á±ÀéðªÁAiÀÄÄ CxÀªÁ
114
ªÀÄgÀUÀlÄÖ«PÉ
ªÁPÀjPÉ
£ÀqÉAiÀÄ®Ä vÉÆAzÀgÉ
C¤AiÀÄ«ÄvÀ G¹gÁl
¥ÀæeÉÕAiÀÄ £ÀµÀÖ
vÀqÉUÀlÄÖ«PÉ
¥Á±ÀéðªÁAiÀÄÄ C¥ÁAiÀĪÀ£ÀÄß vÀqÉUÀlÄÖªÀ ªÀÄÆ®PÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß
PÀrªÉÄ ªÀiÁqÀ®Ä C£ÉÃPÀ CA±ÀUÀ¼ÀÄ ¸ÀºÁAiÀÄ ªÀiÁqÀÄvÀÛªÉ
1. qÁå±ï-qÀAiÀÄmï AiÉÆÃd£É
w£ÀÄߪÀ AiÉÆÃd£É ¢£ÀPÉÌ 2000 PÁå¯ÉÆÃjUÀ¼À£ÀÄß DzsÀj¹zÉ
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¤°è¸À®Ä PÀrªÉÄ G¥ÀÄà DºÁgÀ
«zsÁ£ÀUÀ¼ÀÄ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀÄvÀÛzÉ JAzÀÄ
¸Á©ÃvÁVzÉ. F DºÁgÀzÀ°è ¥ÉÆæÃnãï, ¥ÉÆõÀPÁA±ÀUÀ¼ÀÄ
ªÀÄvÀÄÛ £Áj£ÀA±ÀUÀ¼ÀÄ ªÀiÁvÀæªÀ®è
¹jzsÁ£ÀåUÀ¼ÀÄ, £É®UÀqÀ É, ¨ÁzÁ«Ä, ZÀªÀÄðgÀ»vÀ PÉÆý,
«ÄãÀÄ, ¥Á®PÀ, ºÀÆPÉÆøÀÄ, ªÉÄAvÉå J ÉUÀ¼ÀÄ, ªÀÄÆ®AV
J¯ÉUÀ¼ÀAvÀºÀ ¸ÉƦà£À vÀgÀPÁjUÀ¼ÀÄ ¥ÉÆæÃnãïUÀ¼À°è
¸ÀªÀÄÈzÀÞªÁVªÉ. ¸ÁPÀµÀÄÖ ¤ÃgÀÄ, PÀ¤µÀÖ 10 UÁè¸ï PÀÄr¬Äj
¥ÉÆmÁ²AiÀÄA ¸ÀªÀÄÈzÀÞªÁVgÀĪÀ DºÁgÀªÉAzÀgÉ mÉƪÉÄmÉÆÃ,
115
PÀ®èAUÀr, ¨Á¼ÉºÀtÄÚ ªÀÄvÀÄÛ ºÀ¹gÀÄ vÀgÀPÁjUÀ¼ÀÄ.
PÁå°ìAiÀÄA ¸ÀªÀÄÈzÀÞªÁVgÀĪÀ DºÁgÀªÉAzÀgÉ ºÁ®Ä ªÀÄvÀÄÛ
ºÁ°£À GvÀà£ÀßUÀ¼ÀÄ, ¸ÉÆ¥ÀÄà vÀgÀPÁjUÀ¼ÀÄ.
ªÉÄVß²AiÀÄA ¸ÀªÀÄÈzÀÞªÁVgÀĪÀ DºÁgÀªÉAzÀgÉ ¨ÁzÁ«Ä,
¢ézÀ¼À zsÁ£ÀåUÀ¼ÀÄ, ºÀ¹gÀÄ ¸ÉÆ¥ÀÄà vÀgÀPÁjUÀ¼ÀÄ, PÀAzÀÄ CQÌ,
¨Á¼ÉºÀtÄÚ
2. ¤AiÀÄ«ÄvÀªÁV ªÁåAiÀiÁªÀÄ ªÀiÁr
UÀªÀÄ£ÁºÀð DgÉÆÃUÀåPÀgÀ ¥ÀæAiÉÆÃd£ÀUÀ¼À£ÀÄß ¥ÀqÉAiÀÄ®Ä d£ÀgÀÄ
¸ÁªÀiÁ£Àå zÉÊ»PÀ ZÀlĪÀnPÉUÀ¼À°è ¥Á¯ÉÆμÀî¨ÉÃPÀÄ. ªÁåAiÀiÁªÀÄUÀ¼ÀÄ
gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀÄvÀÛzÉ
G¥ÀÄà ÉêÀ£ÉAiÀÄ£ÀÄß PÀrªÉÄ ªÀiÁr
¸ÀÆÜ®PÁAiÀÄvÉAiÀÄ qÀAiÀiÁ©n¸ï ªÉÄ°èl¸ï mÉÊ¥ï 2, C¢üPÀ gÀPÀÛzÀ
PÉƯɸÁÖç¯ï£ÀAvÀºÀ PÁ¬Ä¯ÉUÉ PÁgÀtªÁUÀ§ºÀÄzÀÄ. ¨Ár ªÀiÁ¸ï
EAqÉPïì 20-25 DVgÀ¨ÉÃPÀÄ. EzÀ£ÀÄß JAzÀÄ ¯ÉPÀÌ ºÁQzÀgÉ zÉÊ»PÀ
ZÀlĪÀnPÉAiÀÄ ªÀÄÆ®PÀ PÁå¯ÉÆÃjUÀ¼À£ÀÄß ¸ÀÄqÀĪÁUÀ ¸Éë¸ÀĪÀ
PÁå¯ÉÆÃjUÀ¼À ¸ÀASÉåAiÀÄ£ÀÄß PÀrªÉÄ ªÀiÁqÀĪÀÅzÀÄ vÀÆPÀ £ÀµÀÖPÉÌ CvÀåAvÀ
¥ÀjuÁªÀÄPÁj «zsÁ£ÀªÁVzÉ. zÉÊ»PÀ ZÀlĪÀnPÉAiÀÄ£ÀÄß ºÉaÑ ÀĪÀ
ªÀÄÆ®PÀ CxÀªÁ JgÀqÀ£ÀÆß ªÀiÁqÀĪÀ ªÀÄÆ®PÀ ¤ªÀÄä DºÁgÀ
¸ÉêÀ£ÉAiÀÄ£ÀÄß PÀrvÀUÉƽ ÀĪÀ ªÀÄÆ®PÀ ¤ÃªÀÅ EzÀ£ÀÄß
¸Á¢ü¸À§ºÀÄzÀÄ.

116
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ¤ªÀð»¸ÀĪÀÅzÀÄ
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀ ¸ÁªÀiÁ£ÀåªÁV AiÀiÁªÀÅzÉà JZÀÑjPÉ aºÉßUÀ¼À£ÀÄß
ºÉÆA¢gÀĪÀÅ¢®è. DzÀÝjAzÀ ¤ÃªÀÅ ¤AiÀÄ«ÄvÀªÁV gÀPÀÛzÉÆvÀÛqÀ
vÀ¥Á¸ÀuÉ £ÀqÉ ÀĪÀÅzÀÄ ªÀÄÄRå. vÉÆqÀPÀÄUÀ¼À DgÀA©üPÀ ®PÀëtUÀ¼À£ÀÄß
PÀAqÀÄ»rAiÀÄ®Ä ¤AiÀÄ«ÄvÀªÁV gÀPÀÛzÉÆvÀÛqÀ ªÉÄðéZÁgÀuÉAiÀÄ£ÀÄß
ªÀiÁqÀ¯ÁUÀÄvÀÛzÉ.
D ÉÆÌúÁ¯ï ¸ÉêÀ£ÉAiÀÄ£ÀÄß «ÄwUÉƽ¹
gÀPÀÛzÉÆvÀÛqÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß ºÉaÑ ÀĪÀ°è D¯ÉÆÌúÁ¯ï
GzÉÝòvÀ C¥ÀgÁ¢ü, ¤ªÀÄä ºÀÈzÀAiÀĪÀÅ ¸ÁªÀiÁ£ÀåQÌAvÀ PÀptªÁV
PÉ®¸À ªÀiÁqÀÄvÀÛzÉ, C¤AiÀÄ«ÄvÀ ºÀÈzÀAiÀÄ §rvÀUÀ½UÉ PÁgÀtªÁUÀĪÀ
¤ªÀÄä ºÀÈzÀAiÀÄ ¸ÁßAiÀÄÄ«£À ªÉÄÃ¯É ¤ªÀÄä MvÀÛqÀªÀ£ÀÄß ºÉaÑ ÀÄvÀÛzÉ,
C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀÅ ¸ÀºÀ ¥Á±ÀéðªÁAiÀÄÄ«UÉ ºÉaÑ£À
C¥ÁAiÀĪÀ£ÀÄßAlÄ ªÀiÁqÀÄvÀÛzÉ.
¸ÁPÀµÀÄÖ ¤zÉæ ¥ÀqɬÄj:
EwÛÃa£À CzsÀåAiÀÄ£ÀªÉÇAzÀgÀ°è ¹¸ÉÆÖðPï ªÀÄvÀÄÛ qÀAiÀiÁ¸ÉÆÖðPï
gÀPÀÛzÉÆvÀÛqÀ JgÀqÀÆ gÁwæ 8 UÀAmÉUÀ½VAvÀ PÀrªÉÄ ªÀÄ®VzÀÝ d£ÀgÀ°è
ºÉZÁÑVvÀÄÛ. MvÀÛqÀzÀ ºÁªÉÆÃð£ÀÄUÀ¼À£ÀÄß ¤AiÀÄAwæ¸À®Ä ¤zÉæ ¸ÀºÁAiÀÄ
ªÀiÁqÀÄvÀÛzÉ ªÀÄvÀÄÛ £ÀgÀªÀÄAqÀ®zÀ DgÉÆÃUÀåªÀ£ÀÄß PÁ¥ÁrPÉƼÀÄîvÀÛzÉ.
wêÀiÁð£À
fêÀ£À±ÉÊ°AiÀÄ ªÀiÁ¥ÁðqÀÄUÀ½AzÀ C¢üPÀ gÀPÀÛzÉÆvÀÛqÀªÀ£ÀÄß

117
¤AiÀÄAwæ¸À§ºÀÄzÀÄ. PÉlÖ ¥ÀjuÁªÀÄUÀ¼À£ÀÄß vÀ¦à¸À®Ä ªÀåQÛ¬ÄAzÀ
DgÉÆÃUÀåªÀ£ÀÄß PÁ¥ÁrPÉƼÀî¨ÉÃPÀÄ, KPÉAzÀgÉ UÀÄt¥Àr¸ÀĪÀÅzÀQÌAvÀ
vÀqÉUÀlÄÖ«PÉ GvÀÛªÀĪÁVzÉ.
UÀæAxÀ¸ÀÆa
ªÉÊzÀåQÃAiÀÄ ±À¸ÀÛçaQvÉìAiÀÄ ±ÀıÀÆæµÉAiÀÄ ¯É«£ï ¥ÀoÀå ¥ÀÄ ÀÛPÀ
(13 £Éà DªÀÈwÛ) J®ì«ðAiÀÄgï £ÀªÀ zɺÀ° (2013)
§æ£Àßgï ªÀÄvÀÄÛ ¸ÀÄqÁØxÀð ªÉÊzÀåQÃAiÀÄ ±À¸ÀÛçaQvÉìAiÀÄ ±ÀıÀÆæµÉ
(10 DªÀÈwÛ) J®Ø§Æèöå, qÀ§Æèöå, ¦ü¸ÀqÉ°áAiÀiÁ (2007)
eÁAiÀiïì JA PÀ¥ÀÄà ªÉÊzÀåQÃAiÀÄ ªÀÄvÀÄÛ ±À¸ÀÛçaQvÉìAiÀÄ ±ÀıÀÆæµÉ
(7 £Éà DªÀÈwÛ) J®ì«ðAiÀÄgï £ÀªÀ zɺÀ° (2007)
£Ànð£Á JAJ¸ï °¦Ö£ÁÌmï £À¹ðAUï C¨sÁå¸ÀzÀ PÉʦr
(8 £Éà DªÀÈwÛ) eÉæà §æzÀgï ªÉÄrPÀ¯ï ¥À©èµÀ¸Àð £ÀªÀzɺÀ°
(2006)
¸ÀĸÁ£ï J¯ï ªÀÅqïì PÁrðAiÀiÁPï £À¹ðAUï (5 £Éà DªÀÈwÛ)
°¦Ö£ÁÌmï «°AiÀĪÀiïì.