Embed Size (px)
Citation preview
Beausoleil, Muskoka & Rama
CME 2010
Agenda
• Didactic:– STEMI update– TOR– King LT– Anaphylaxis
• Skills– Neonatal Resuscitation– Cardiac arrest & KING LT– Breath sounds– IM injection– IV start, fluid and dextrose administration
• Scenarios• KAT
General Housekeeping
• Did your name, address, telephone, cell phone or email change since the last CME?
• If so please fill out a medic info sheet!
THANK YOU
Auditing Housekeeping
• Please ensure the use of – 010 Vital signs code.
• Document Vital signs pre and post each medication administration on the ACR, not as a group at the bottom of the ACR
• Do not use a procedure code (i.e. 615 NTG) when you are ruling out NTG administration. Use 030 ALS assessment
What do I attach to the ACR?
From the LP15 printouts:
• Vital sign log• ECG with O2Sat waveform (Plethysmograph)
• All 12 Lead ECG’s with patients name recorded on each ECG.
TIME = Cardiac Muscle
• Likely to be older (74 v 67)Likely to be older (74 v 67)
• Women (49% v 38%)Women (49% v 38%)
• Diabetic (33% v 25%)Diabetic (33% v 25%)
• Prior heart failure (26% v 12%)Prior heart failure (26% v 12%)
• Longer delay to assessment (8% v Longer delay to assessment (8% v 5%)5%)
• Less likely to be diagnosed (22% v Less likely to be diagnosed (22% v 50%)50%)
• Less likely to receive treatment Less likely to receive treatment (25% v 74%)(25% v 74%)
• Most likely to die (23% v 9%)Most likely to die (23% v 9%)
Patient Presentation 33% of patients with confirmed MI present with S & S other than chest discomfort. This group compared with those that present with chest discomfort are:
Pre-Hospital 12 Lead• Perform a history and physical exam• Patients ≥40 kg with signs and symptoms
of cardiac ischemia you must acquire a 12 lead ECG
– Software will interpret findings• STEMI positive ECG• LP 12 *****Acute MI Suspected******• LP 15*** Meets ST Elevation MI Criteria****
• STEMI negative ECG All other statements
12 Lead ECG acquisition
• Must be performed on all patients presenting with signs and symptoms of cardiac ischemia
• Must input age and sex
12 Lead ECG acquisition
• 3 ECGs will be done on these patients:– First on scene as early as possible– Second prior to departure– Third upon arrival at medical facility
TORWhen to call the BHP for
termination of resuscitation?
Medical TOR (page 42)
• Age > 18 years old• No ALS procedures• Cardiac in nature• 3 No shocks on scene
• Witnessed by EMS or Fire?• Any shocks delivered?• Was there a ROSC?
• YES or uncertain = continue resuscitation & transport• NO = continue resuscitation and PATCH to BHP for
medical TOR & continue transport.
Trauma TOR (page 23 & 24)
Trauma TOR• Age > 16 years old• Blunt trauma = Big pads
– Shock delivered, transport– No shock, No pulse, HR>0, transport– No shock, No pulse, No HR, patch for trauma TOR
• Penetrating trauma = Petite pads (Electrodes)– HR >0, ED <20 minutes, transport– HR >0, ED >20 minutes, patch for trauma TOR– HR 0, patch for trauma TOR
• Trauma patients that have received a TOR after a patch are to be left on the scene.
King LT
Click on video to start
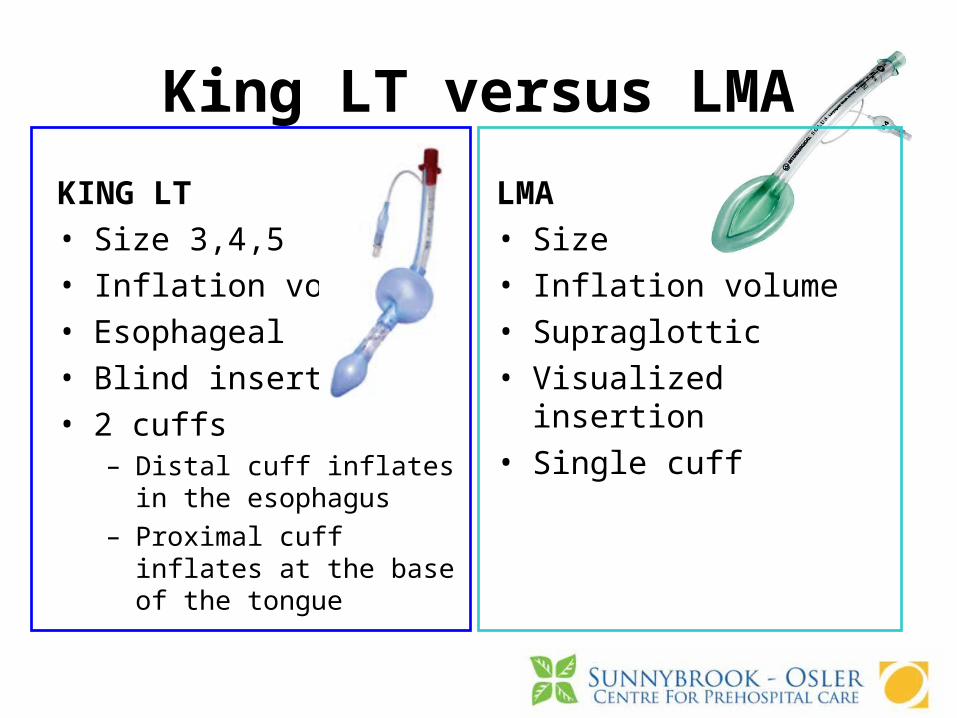
King LT versus LMA
KING LT• Size 3,4,5• Inflation volume• Esophageal• Blind insertion• 2 cuffs
– Distal cuff inflates in the esophagus
– Proximal cuff inflates at the base of the tongue
LMA• Size• Inflation volume• Supraglottic• Visualized insertion• Single cuff
Neonatal Resuscitation
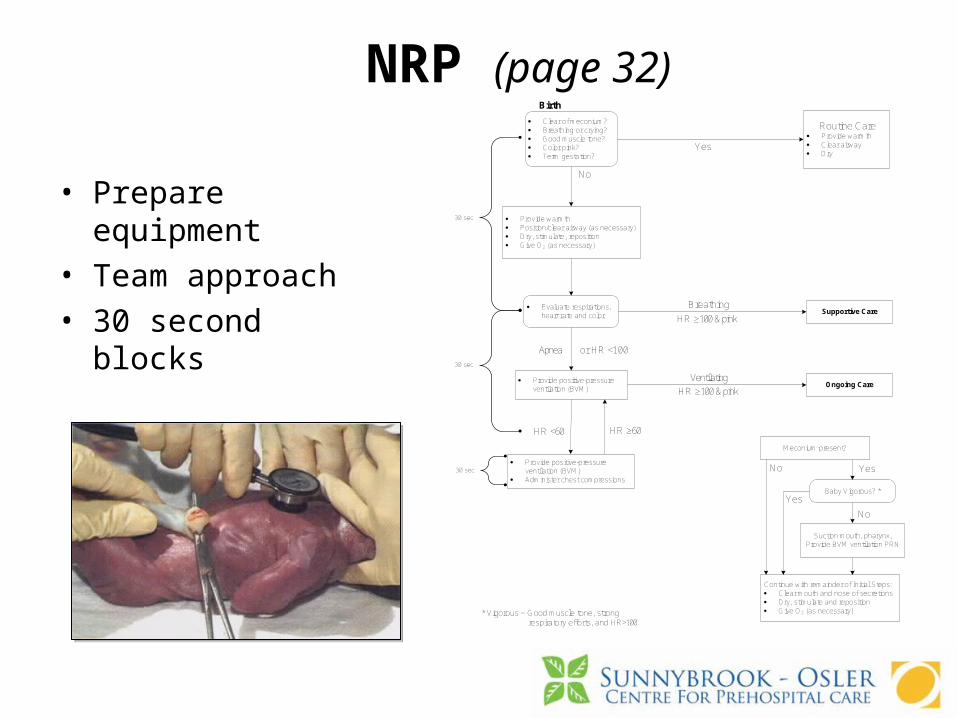
NRP (page 32)
• Prepare equipment• Team approach• 30 second blocks
· Clear of meconium?· Breathing or crying?· Good muscle tone?· Color pink?· Term gestation?
· Provide warmth· Position/clear airway (as necessary)· Dry, stimulate, reposition· Give O2 (as necessary)
Routine Care· Provide warmth· Clear airway· Dry
· Evaluate respirations, heart rate and color
Supportive Care
· Provide positive-pressure ventilation (BVM)
Ongoing Care
· Provide positive-pressure ventilation (BVM)
· Administer chest compressions
Meconium present?
Baby Vigorous? *
Suction mouth, pharynx, Provide BVM ventilation PRN
Continue with remainder of Initial Steps:· Clear mouth and nose of secretions· Dry, stimulate and reposition· Give O2 (as necessary)
Birth
HR ≥60
or HR <100
HR <60
Apnea
Yes
Breathing
HR ≥100 & pink
HR ≥100 & pinkVentilating
No
No
No
Yes
Yes
* Vigorous = Good muscle tone, strong respiratory efforts, and HR>100
30 sec
30 sec
30 sec
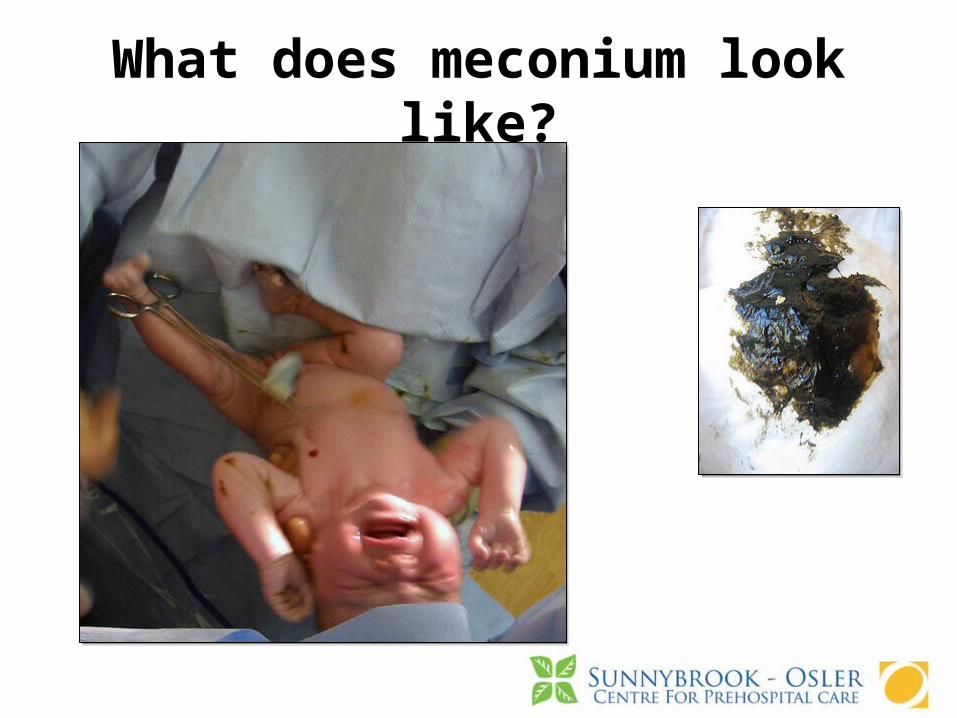
What does meconium look like?
ANAPHYLAXIS REVIEW
Continuing Education
Outline
• Definition
• Incidence
• Pathophysiology
• Signs and Symptoms
• Diagnosis
• Indication for Epinephrine SQ/IM
• Case Presentation
Definition of Anaphylaxis
• A systemic reaction to a protein (antigen)• Caused by the release of immunoglobulin
E (IgE) • IgE acts on mast cells and basophils • Mast cells and basophils release
chemical mediators; including histamine• Histamine and other inflammatory agents
act on smooth muscle, connective tissue and mucous glands
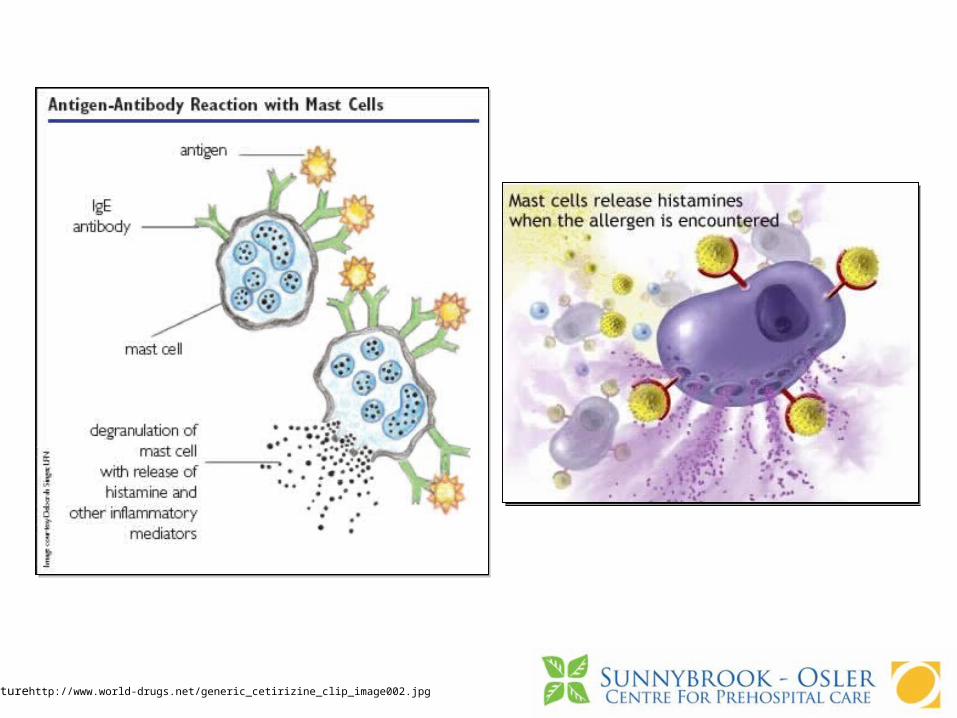
Picturehttp://www.world-drugs.net/generic_cetirizine_clip_image002.jpg
Incidence
• Difficult to get true numbers
• Many reactions are mild and not reported or misdiagnosed
• Up to 15% of population may be at risk
Pathophysiology
• Anaphylactic and Anaphylactoid reactions occur due to the systemic release of chemical mediators from mast cells and basophils
• Histamine is the primary mediator involved in urticaria, bronchospasm and anaphylactic shock
Pathophysiology
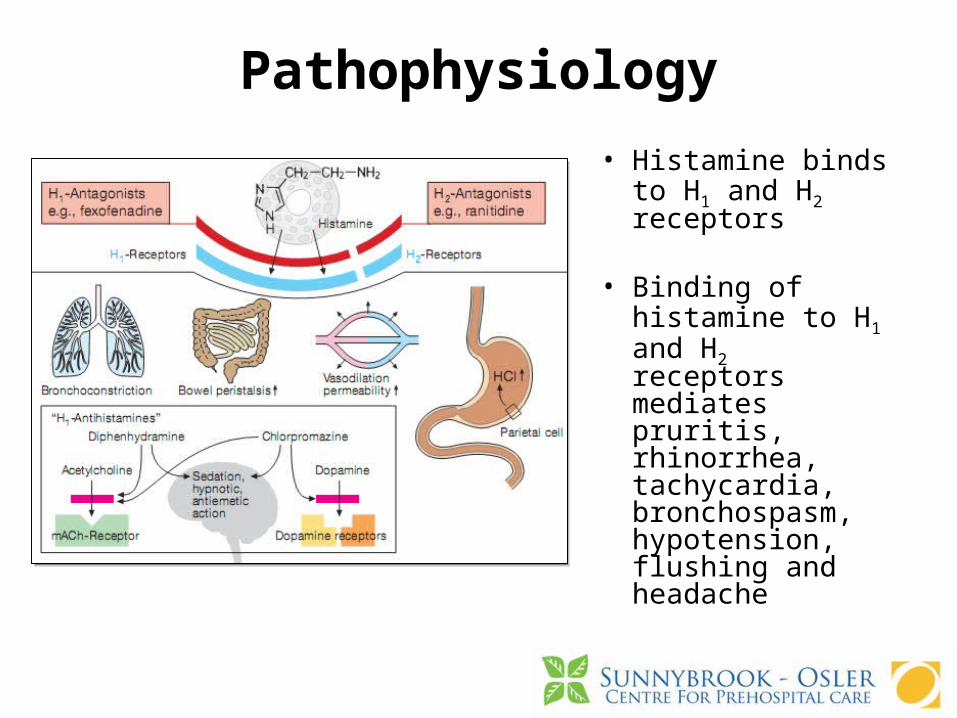
• Histamine binds to H1 and H2 receptors
• Binding of histamine to H1 and H2 receptors mediates pruritis, rhinorrhea, tachycardia, bronchospasm, hypotension, flushing and headache
Signs and Symptoms
Skin:• Itching, Urticaria• Angioedema, flushing
Respiratory:• Hoarseness, stridor• Dyspnea, wheezing, rhinitis
GI:• Nausea, vomiting• Cramping, diarrhea

Pictures: http://healthsymptomspictures.com/wp-content/uploads/2009/11/anaphylaxis.jpg
Signs and Symptoms
Cardiovascular:• Dizziness,Chest Pain (uncommon)• Tachycardia, hypotensionNeurologic:• Headache, • decreased LOA (due to hypotension +/-
hypoxia),• seizures-uncommon

Signs and Symptoms• Skin findings are the most common BUT up
to 20% of patients do not have hives or other skin symptoms
• Respiratory symptoms are the second most common
• deaths result from severe bronchospasm and airway and laryngeal edema
Diagnosis
Diagnosis is made clinically:
• History of exposure to possible allergen followed by development of symptoms consistent with anaphylaxis
• Development of urticaria, laryngeal edema, bronchospasm and/or hypotension with other signs associated with anaphylaxis
• Rebound reactions can occur up to 24 hours later
Treatment ?
• First line is Epinephrine SQ/IM• Other treatments: antihistamines,
corticosteroids, bronchodilators, IV fluids without administration of epinephrine fail to prevent or relieve severe anaphylaxis
• Epinephrine in the setting of anaphylaxis has greater benefit than risk
What are the Indications for Epi SQ/IM
• Confirmed or suspected exposure to a probable allergen
• Signs and symptoms of a severe anaphylactic reaction– Involvement of more than one body system– E.g.: Urticaria and nausea– E.g.: shortness of breath with wheezing
and facial edema– OR any airway symptoms
Case Presentation
• 8 year old female began to have shortness of breath with wheezing and tightness in her throat while running a race at school
• EMS is called 20 minutes later because the patient’s symptoms have not subsided and the patient now has a hoarse voice
• Has had a similar reaction in the past but there was no specific allergen found
• Pulse: 132, Resp: 24, BP: 80/62
Diagnosis?
Treatment?

QUESTIONS
Jeopardy