Embed Size (px)
DESCRIPTION
May-June 2015 BCNU is United for Safe Patient Care
Citation preview

UPDATEBRITISHCOLUMBIANURSES’ UNION
BURNED OUT: WORKLOAD STUDY REVEALS HIGH LEVELS OF EMOTIONAL EXHAUSTION
SPECIAL PULL-OUT REPORT: GRIEVANCE SETTLEMENT SETS PATH TO IMPROVED STAFFING
UPDATEUPDATEBRITISHUPDATEUPDATECOLUMBIAUPDATEUPDATENURSES’ UPDATEUPDATEUNIONUPDATEW
WW
.BC
NU
.OR
GM
AY/
JUN
E 2
015
SPEC
IAL
HEALT
H &
SAFE
TY
ISSUE
BCNU IS UNITED FOR SAFE PATIENT CARE
CONVENTION 2015
BCNU IS UNITED FOR SAFE PATIENT CARE
CONVENTION 2015
SPEC
IAL
HEALT
H
PROUD TO BE NURSES Central Vancouver region’s Jeana Dagasdas and Okanagan Similkameen region’s Celine Smith are committed to safe patient care.
NATIONAL NURSING WEEK
MAY 11–17, 2015
With you every STEP of the way
> INTERNATIONAL NURSES DAY MAY 12 > LPN DAY MAY 13

UPDATE MAGAZINE May/June 2015 3
CONTENTS
SAFETY FIRST
FEATURE
UPFRONT
DEPARTMENTS
UPDATE VOL 34 NO2 • MAY/JUNE 2015
20
OH&S CHAMPIONS University of BC Hospital nurse Jocelyn McCord and Vancouver General Hospital nurse Dallas Gogal both worked to successfully ensure that Vancouver Coastal Health Authority implement an enforceable surgical smoke evacuation policy for its operating rooms.
Read about how BCNU members are making their workplaces safer for themselves and their patients.
6 Check InNews, updates and current events.
8 Birthing Unit Crisis Surrey Memorial Hospital nurses ring the alarm on chronic understaffi ng.
9 Care Model Changes Island nurses document the risks to safe patient care.
10 Committed to Their WorkLong-term care nurses address their unique challenges ahead of bargaining.
12 Burned OutBCNU workload survey reveals high levels of emotional exhaustion.
13 Convention ReportA virtual rally for safe patient care was one of the highlights of this year’s gathering.
5 PRESIDENT’S REPORT
32 YOUR PENSION
34 PRFS WORK
36 WHO CAN HELP?
37 COUNCIL PROFILE
38 OFF DUTY
Special Pull-out Report
Learn about the recent staffi ng
grievance sett lement that
sets the tone for productive
bargaining in the year ahead. p. 13
Special Pull-out Report
Special Pull-out Report
Special Pull-
Learn about the recent staffi ng
grievance
>Message From Your President >NEW Fast-Track Staffing Dispute Process >$5 Million In Specialty Education Funding
www.bcnu.org
STAFFING GRIEVANCE SETTLEMENT
Special Report
APRIL 2015
> INTERNATIONAL NURSES DAY MAY 12 > LPN DAY MAY 13
4
MISSION STATEMENTBCNU protects and advances
the health, social and economic
well-being of our members
and our communities.
BCNU UPDATE is published by the
BC Nurses’ Union, an independent
Canadian union governed by a council
elected by our 42,000 members. Signed
articles do not necessarily represent
offi cial BCNU policies.
EDITORLew MacDonald
CONTRIBUTORS
Juliet Chang, Laura Comuzzi,
Sharon Costello, David Cubberley,
Monica Ghosh, Gayle Duteil, Gary Fane,
Shawn Leclair, Michelle Livaja,
Robert Macquarrie, Sherry Parkin,
Cindy Paton, Catherine Pope
PHOTOS
David Cubberley, Lew MacDonald,
Catherine Pope
CONTACT USBCNU Communications Department
4060 Regent Street
Burnaby, BC, V5C 6P5
PHONE 604.433.2268
TOLL FREE 1.800.663.9991
FAX 604.433.7945
TOLL FREE FAX 1.888.284.2222
BCNU WEBSITE www.bcnu.org
EMAIL EDITOR [email protected]
MOVING? Please send change of address to
Publications Mail Agreement
40834030
Return undeliverable
Canadian addresses to BCNU
4060 Regent Street
Burnaby, BC, V5C 6P5
UPDATEMAGAZINE
BC Nurses’ Union
When you move, please let BCNU know your new address so we can keep sending you the Update, election information and other vital union material. Give us your home email address and we’ll send you the latest BCNU bulletins and news releases. And if you’ve changed your name, please let us know.
MOVING? NEW EMAIL?
Please contact the Membership Department by email at [email protected] or by phone at 604-433-2268 or 1-800-663-9991
STAY CONNECTED

UPDATE MAGAZINE May/June 2015 5
PRESIDENT’S REPORT the list. As this issue of Update went to
press, another Hillside nurse was assaulted, and Interior Health has fi nally posted a safety offi cer at the facility 24-7. (Turn to page 23 for the full story and learn more about BCNU’s new policy on violence protection.)
I am also very pleased that BCNU has won a major sett lement which resolves thousands of safe staffi ng grievances. Th e details can be found in the special pull-out insert on page 13. BCNU has secured $2 million for breaches of the contract, which will be distributed to individuals and groups of members who fi led griev-ances. Another $5 million in funding has been secured for specialty education and there is now a fast-track process to resolve nurses’ staffi ng issues. It won’t solve every staffi ng issue at every site, but it improves the process and makes health authorities more accountable.
Th is signifi cant achievement could not have happened without the dedication and perseverance of our members. You rose to the call for collective action, took the time to fi le thousands of grievances demanding safe patient care and made change happen!
Occupational health and safety is the focus of this month’s magazine. In addi-tion to violence prevention, there are stories about rural transport nurses’ work to secure safety management systems and Vancouver Coastal Health OR nurses’ successful push for an enforceable smoke evacuation policy.
As always, members are making a diff er-ence on many of these issues by speaking up and working with union reps to defend their right to a safe and healthy workplace.
I want to thank each and every one of you for your hard work and dedication. Th e recent grievance sett lement and health min-istry commitments are just the beginning, and one more step on our path to a new and bett er contract for all BC nurses. update
SAFE NURSES EQUALS SAFE PATIENT CARE
GAYLE DUTEIL
A S YOU READ THIS, CHANCES ARE THAT A NURSE TODAY somewhere in BC has been assaulted while on the job. Nurses everywhere, every day, are subjected to physical, verbal or emotional abuse while trying to provide safe patient care.
Violent att acks on health care workers have increased 70 percent in the last ten years. Th is is unacceptable, and defi nitely not part of the job. No nurse should ever have to suff er because of a lack of safety offi cers, personal alarms or adequate training.
Over the last number of months, we have worked hard to convince provincial health authorities that they must make worksites safer. Th e BCNU team has presented our demands in countless meetings with the health minister and senior offi cials from the government and health employers. We have also raised public awareness by engaging the media.
Finally we seem to be gett ing somewhere.Th e government has now agreed to move forward with a plan to address some of
BCNU’s concerns. Four sites out of the twelve we identifi ed as needing immediate att ention are now being reviewed by the health ministry. Hillside Psychiatric Centre in Kamloops, where many nurses have been injured by patients over the years, is fi rst on P
HO
TO: A
LEX
IS S
ULL
IVA
N W
ALT
ER
S

6
Several BC nursing students were recently elected to top posi-tions in this year’s Canadian Nursing Students’ Association elections. North Island College’s Dawn Tisdale was elected president, Langara College School of Nursing’s Terrace Desnomie was elected vice president and Langara College School of Nursing’s Tonie Castro was elected director of communications.
If you are contacted by the Canada Revenue Agency (CRA) regarding the union dues amount you have claimed on your 2014 income tax return you should provide them with the following: 1. Your T4 (or T4s if more than
one was received) – this shows the amount of union dues your employer has deducted from your salary and submitted to BCNU for the tax year indicated.
2. The receipt you received from CRNBC or CLPNBC as proof of payment of your annual membership fee.
In most instances this
should satisfy any CRA inves-tigation audit regarding your union dues and professional fees.
If the CRA requests proof that the union dues noted on your T4 were paid to BCNU you should contact the payroll department of your employer and request a brief letter noting that they remitted the dues to BCNU in tax year 2014 on your behalf. BCNU does not issue receipts for proof of union dues noted on your T4.
More information on annual union and professional dues claims can be found on CRA’s website.
NEWS FROM AROUND THE PROVINCE
CHECK INHARM REDUCTION
DUES AND TAXES
CNSA ELECTIONS
SAFE INJECTIONS SAVE LIVES BCNU and other organizations are working hard to support the continued operation of Vancouver’s Insite – Canada’s only stand-alone supervised drug injection facility. But the federal government has consistently opposed the harm reduction strategy on which Insite is based.
A HOUSE OF COMMONS BILL THAT PASSED last month will impede the operations of supervised consumption sites such as Vancouver’s Insite and endanger severely addicted Canadians, according to nurses and other community health professionals.
Bill C-2, the Respect for Communities Act, consists of a host of new regulations that will make it much more difficult for a com-munity service provider to open a harm reduction site. The new legislation will also complicate the process by which existing sites have to apply annually for an exemption from the Controlled Drugs and Substances Act to operate.
The move flies in the face of a 2011 Supreme Court of Canada ruling where the court found that supervised injection sites save lives and that the federal health minister’s failure to provide an exemp-tion was in violation of drug users’ constitutional rights to life and security of the person.
Under Bill C-2, facilities that wish to run a supervised consump-tion site must meet a lengthy list of requirements, including: a letter from the head of the local police force; statistics and other informa-tion on crime, public nuisance and inappropriately discarded drug paraphernalia in the vicinity of the site; and a report on consultations with “a broad range of community groups.”
The Canadian Nurses Association says it is “disappointed” that the bill was passed in the House and “concerned” by the Conservative government’s so-called “tough-on-crime” position.
“A government truly committed to public health and safety would enhance access to prevention and treatment services instead of building more barriers,” the association, which represents 135,000 registered nurses, said in a statement last month. update
OTTAWA THREATENS INSITE – AGAIN
INTENT TO LEAVE The percentage of nurses who reported that they were “somewhat likely” to leave their current job within the next year.
44% 25% 40%
VITAL SIGNS Numbers that matter
CAREER CHOICE The percentage of nurses who reported that they were “very satisfied” with being a nurse.
Recently surgical BCNU members reported only moderate levels of satisfaction when it came to working in their cur-rent job. Nurses cited workload and management practices as the primary reasons for intent to leave their current positions. Nurses were satisfied overall with their career choice despite the working conditions.
CURRENT JOB The percentage of nurses who reported that they were “moderately satisfied” with their current job.
Source: BC Nurses’ Workload Impact Study (2014) MacPhee, M, et al. Published by the University of British Columbia and the BC Nurses’ Union
NURSES’ JOB SATISFACTION

UPDATE MAGAZINE May/June 2015 7
MAKING HEALTH CARE LEADERSHIP AN ELECTION ISSUEWhen the federal govern-ment announced cuts to health care funding in 2011, many Canadians vowed to make sure that voters would not forget the decision.
Duncan Home and Community Centre nurse Ted Gamble reminded people of the Harper govern-ment’s polices when he wrote to the Vancouver Sun on the one-year anniversary of the March 31, 2014 expiry of the federal-provincial health accords that had secured Ottawa’s
funding contribution.“The [Harper] govern-
ment will not negotiate a new health care agreement between the federal and provincial governments. The private sector is lobby-ing our governments, suc-
cessfully it seems, to allow it more access to our public health care system. This issue needs to be at the forefront of the federal election, and I encourage all constituents to question all the political party
candidates on this issue,” wrote the BCNU Pacif ic Rim region member in a letter published April 2.
MAKING NEWS BCNU in the headlines
FIRST CONTRACTINDEPENDENT BARGAINING
GOOD DEAL Ayre Manor Lodge
workers (from left) Anna Campbell,
Terri McKinty, Linda Quigley and Janice
Leask are happy with the fi rst collective
agreement they signed on March 31.
Ted Gamble
#SAFEPATIENTCARE BCNU’s North East region held a mini rally during its March 27 regional meeting in Prince George. Members pictured, from left: University Hospital of Northern BC steward Victoria MacDonald, UHNBC steward Shannon Sluggett, UHNBC steward and Joint Occupational Health and Safety committee member Jen Coleman and UHNBC full-time steward Judi Dindayal.
A FIRST CONTRA CT COVERING 65 BCNU members at Ayre Manor Lodge in Sooke was ratifi ed on March 31 by 100 percent. Th e three-year agree-ment, retroactive to July 2014, improves wages, paid leave, and benefi ts, and establishes strong new
language on bullying and harassment.Under the contract that has now been ratifi ed by the Sooke
Elderly Citizens Housing Society (SECHS), housekeepers, servers and prep cooks will receive a $1.00 per hour increase, while wages for all classifi cations will rise by 2.5 percent on July 1 and another 2 percent on July 1, 2016. Members will also receive a signing bonus of $250 for full-time, and $125 for part-time. Casuals who have worked more than fi ve shift s since July 1, 2014 will receive $75.
Statutory holidays have been increased from 10 to 12 per year, with Christmas paid as a super stat at twice regular pay. Th e contract also increases sick leave to up to eight days a year, accrued fully in January (under a former independent contract it had to be accrued month-by-month).
BCNU was certifi ed to bargain on behalf of all the workers on July 15, 2014. Th e four-member bargaining committ ee, led by BCNU negotiator Laura Anderson, showed patience and deter-mination throughout long negotiations, which also included mediation.
“I think members are really happy with the gains in this contract,” said bargaining committ ee member Janice Leask. “Th ey like the harassment language, and the night shift are happy they’re going to get paid for their meal breaks.”
Since 2008 Ayre Manor Lodge has provided 25 assisted living apartments and 32 residential complex care suites. Th e lodge was initially operated on contract by Beckley Farm Lodge Society, but SECHS assumed direct control in 2014 and BCNU now represents all classifi cations at the facility, including housekeepers, cooks, serv-ers, care workers and nurses. update
Ayre Manor Lodge employees see improved wages, benefi ts and holidays

8
BIRTHING UNIT CRISIS
IMAGINE A SITUATION WHERE you work an entire shift running from medical event to medical event with no time for mental or physical breaks, being unable to
complete your charting until aft er the shift ends, and fi nally being reduced to tears be-fore heading home due to the overwhelm-ing workload.
Now imagine that, instead of being a one-off event, this is considered part of a normal shift at your worksite. Th is is the reality for the more than 100 regular nurses who work at Surrey Memorial Hospital’s Family Birthing Unit (SMH FBU).
Every year, some 4,200 babies are born here.
Th e SMH FBU is the busiest mater-
in active labour and needing immediate one-to-one nursing care. She also noted that the unit is expected to deal with many high risk deliveries requiring multiple nurses to provide appropriate care and monitoring. But short staffi ng has led to admission delays and incomplete assess-ments, and an inability to provide patients with adequate post-partum education.
SMH doctors joined nurses in testifying at the hearing about their concerns for the safety of their patients.
Cooley is also worried about her employer’s ability to recruit and retain staff for a ward that has seen an exodus of some 30 regular nurses in the past two years. “We’ve lost so many amazing nurses and we now have a lot of junior staff on the unit – and it’s hard to support them when it’s such a busy place,” she says. “So it’s very hard on new people as well.”
She says it feels like managers are more focused on the budget than meeting guide-lines and following the contract.
“Many of the nurses don’t feel sup-ported,” says Cooley. “Th ey don’t see more nurses being trained and educated. Th ey don’t see the lines and shift s being fi lled, so working short just places extra workload on them – and they choose to go to other obstetrical units in the lower mainland where working conditions are bett er.”
Th is only compounds the problem, she says. “You can work in a diff erent birthing unit in Fraser Health and it’s way less busy and bett er staff ed.”
In the meantime, Cooley is doing her best to support her team. “Always ask for help, always fi ll out PRFs and always tell your PCC when you’re feeling your practice or patient care is being aff ected,” is her mes-sage to nurses working short.
Fixing the problems at the FBU is now a top priority as the BCNU works with provincial health employers to resolve all outstanding safe staffi ng grievances related to the 2012 provincial collective agreement (see the special pull-out report on p. 13). Th e progress made so far is a testament to nurses at SMH and other worksites who continue to fi ght for safe patient care every day. update
SARE CARE NOW! Surrey Memorial Hospital patient care coordinator Janet Cooley and former full-timesteward Nicole Ng are seeking concrete solutions to remedy the chronic staffi ng problems in the hospital’s maternity ward.
babies are born here. Th e SMH FBU is the busiest mater-
nity ward in the province. Th e unit is also a non-refusal site with its own operating room designed to accept high-risk pregnan-cies. It’s not a place for the faint of heart. But despite the unit’s size and importance to the region, nurses here are constantly overworked, and patients aren’t gett ing the care they deserve.
Nurses have been ringing alarm bells for the past two years due to chronic understaff -ing, and report that managers regularly staff the unit with only 14 to 15 nurses on the night shift when the baseline staffi ng requires 21. RN absences are regularly not replaced.
Janet Cooley is a 17-year nurse and patient care coordinator at SMH. She’s proud of the work she and others do under the circumstances. “We have an amazing team and everyone works really hard and really well together,” she says. But Cooley also knows that staff are experiencing
physical and mental stress, burnout and sometimes provide sub-standard care to their patients.
Nurses have responded by fi ling several grievances over the employer’s
refusal to properly staff for patient demand and to baseline levels. At
a recent arbitration hearing, Cooley testifi ed that the
level of acuity and patient demand can change at any moment, with up to 10 patients coming to the unit
SURREY MEMORIAL HOSPITAL
STAFFING NIGHTMARE SEES EXODUS OF 30 NURSES OVER THE PAST 2 YEARS

UPDATE MAGAZINE May/June 2015 9
THE TWO SCHOOL BUSES that pulled up outside Victo-ria’s Royal Jubilee Hospital on March 26 were fi lled with nurses determined to send a
strong message to Island Health Authority board members during its public meeting.
Led by BC Nurses’ Union South Islands region co-chairs Adriane Gear and Lynnda Smith, some 100 nurses outside the hospital carried signs that read “Safe Patient Care.”
Once inside, nurses presented the board with 2,000 petitions demanding an indepen-dent review of the deeply fl awed care model (dubbed Care Delivery Model Redesign, or CDMR) which has caused so many prob-lems for nurses and patients on Vancouver Island. Th e latest batch of petitions come in addition to the 27,000 signatures already given to Island Health over the year-and-a-half since CDMR was introduced.
Each board member was also given a personally addressed lett er reminding them of their own vision statement in which they
nurses from meeting their professional stan-dards and providing safe patient care.
Th is information will be presented in affi davits during upcoming arbitration hearings where the union will provide evidence of specifi c instances of lapses in patient safety due to excessive workloads, including: • Th e inability to provide medications in a
timely manner.• Th e inability to complete patient assess-
ments and adequately monitor patients. • Th e inability to complete charting and
care plans.Nurses have reported that these types
of situations are all associated with an increased risk of adverse patient outcomes.
“Island Health has repeatedly said there is no evidence of serious problems with the care model,” says BCNU Pacifi c Rim region chair Jo Salken. “But nurses at Nanaimo Hospital deal with problems in providing safe patient care every single day.”
Th e union is hoping that the sched-
NURSES DELIVER STRONG MESSAGE TO ISLAND HEALTHBCNU has documented more than 100 instances where new care model prevented nurses from meeting their professional standards
“aspire to the highest degree of quality and safety.”
“How can you endorse replacing nurses with care aides in a context of rising patient acuity?” read the lett ers. “How can less nursing care be a safe response to more complex patient needs? And how can cut-ting over 48,000 annual nursing hours in Nanaimo (26 FTEs) and up to 186,000 annual hours (100 FTEs) in Victoria be said to improve care for patients whose complex illnesses require more – not less – nursing att ention?”
Gear told the board that when nurses tell Island Health leadership that they can’t meet their professional standards, they’ve been told to “lower their standards.” Island Health CEO Brendan Carr dismissed these concerns, claiming management would never ask people not to comply with profes-sional standards.
However, BCNU has now documented more than 100 instances where the new care model has prevented Vancouver Island
CARE MODEL CHANGES

10
BCNU MEMBERS WHO WORK in long-term care facilities across the province have been meeting to prepare for contract negotiations so employers and policy makers clearly
understand their issues at the bargaining table. Th is winter, the BCNU wrapped up a series
of dinner meetings organized to hear fi rst-hand about the challenges that the more than 6,000 BCNU members working in long-term care face. More than 300 members participated in 18 meetings across the province. And for many of the participants it was their fi rst BCNU meeting.
BCNU Vice President Christine Sorensen, Treasurer Mabel Tung and BCNU long-term care Bargaining Committ ee rep Liz Ilczaszyn facilitated many of the dinners. Th ey were joined by other BCNU regional chairs and staff .
Th e lack of accessible long-term care services is a serious issue, and it’s one that policy makers cannot aff ord to ignore as BC’s population ages and more people require full-time home and community health care services. Seniors’ advo-cates have been speaking out about the issue on behalf of patients (see sidebar: BC Seniors’ Advocate calls for improved home and commu-nity care services).
No one is more aware of the challenges fac-ing the long-term care sector than the nurses and other health care workers who provide care daily, and BCNU members raised many common themes in the course of the meetings. Th ese included:• Chronic underfunding: nurses report that
government neglect and the lack of a provin-cial/national long-term care strategy has led to the problems they are experiencing in their workplaces.
• Increasing resident acuity: nurses report facing daily challenges and obstacles as they provide care to an increasingly complex resi-dent population.
• Short staffi ng and heavy workload: long-term care nurses have heavy workloads and high nurse-to-patient ratios. Th ey oft en feel they are doing litt le more than “putt ing out fi res” and don’t have the opportunity to build relationships with residents, and this puts health outcomes at risk.
• Communication challenges: heavy work-loads cause communication problems with
uled arbitration will resolve key issues in Nanaimo, including:• A ruling on the extent to which
an employer can cut nurse staff -ing levels without impacting their professional standards.
• A ruling that will require the employer to re-establish nursing positions on CDMR units where professional standards aren’t being met.
• An acknowledgement that Island Health changed its care model without seeking nurses’ input.
• An acknowledgement that CDMR has impacted nurses’ work-life balance, resulting in decreased job satisfaction and increased mental health prob-lems, such as moral distress.Unfortunately, Island Health
continues to deny that the care model has serious fl aws, and nurses say that problems providing safe patient care while understaff ed persist.
According to Salken, Nanaimo Regional General Hospital’s fl oor fi ve is a heavy medical and stroke fl oor that is oft en short four nurses. “Nurses just don’t want to work any ‘extra’ in an environment where it puts them into moral distress because they’re unable to provide quality care,” she explains, noting that professional responsibility forms are being used in response to the situation. “PRFs continue to be fi lled out by nurses who are not meeting their standards.”
Salken points to Island Health’s creation of a Critical Care Outreach Team (CCOT) as evi-dence that CDMR isn’t working. CCOT is supposed to “provide early intervention to prevent a patient from going into cardio-pulmonary arrest,” she says. But she believes it’s recognition that there have been poor outcomes for patients on CDMR units. update
CALLING FOR ACTION Victoria nurse Ariel Allen says the lack of staff in every classifi cation is the biggest problem facing the long-term care sector.
LONGTERM CARE MEMBERS PREPARE FOR BARGAININGMEETINGS HIGHLIGHT THE UNIQUE CHALLENGES FACING MEMBERS WHO PROVIDE SENIORS’ CARE ACROSS THE PROVINCE

UPDATE MAGAZINE May/June 2015 11
residents, managers and families. Nurses want more education to create positive environments that combine clinical care with family engagement. Many also said that managers aren’t connected to front-line employees and don’t under-stand nurses’ experiences.
• Fair compensation: long-term care nurses have a wide body of knowledge and provide health services to residents with multiple issues. But they feel that their work and their unique body of nursing knowledge is neither valued nor appreciated by managers, other members of their profession or co-workers. LPNs in particular felt that they should be fairly compen-sated for their nursing work.
A riel Allen is a Victoria RN who works at two long-term care facili-ties. She’s also worked in oncology and in
end-of-life care. Allen attended one of the BCNU bargaining meetings for long-term care members.
“I love having the same resident day after day and getting to know them and their family,” says Allen. “I want to help residents maintain the best possible quality of life for the time they have.”
She says that when she worked in acute care facilities she liked the patient acuity but didn’t like having four to six new patients every day. “In residential [long-term] care I have the best of both worlds,” says Allen. “Patient acuity is high so I get to expand my nursing knowledge, and I also get to build caring relationships with residents and their families that are so important to my practice.”
Allen says that long-term care nurses need broad knowledge about different fields of health care like oncology, renal, palliative, emer-gency, cardiac, neuro and mental
The BC Seniors’ Advocate has just released a report about improvements that are urgently needed in seniors’ health care services. The advocate’s recommendations echo the sug-gestions of many long-term care nurses who attended the BCNU’s dinner meetings recently.
The advocate made three key recommendations:
1. More community supports are necessary to keep seniors in their homes longer. Up to 15 percent of long-term care residents were prematurely admitted and should have stayed at home with community support.
Supporting healthier seniors in their homes will improve their health and free more space in residential facilities for those who really need it. Then, less complex patients can move out of acute care facilities into appropriate placements. This would reduce costs and lower hospital congestion.
2. Better use of medication in residential
care. Drugs are over-used, especially anti-psychotics and antidepressants.
In BC long-term care, the following statis-tics are troubling:• 34 percent of residents have been pre-
scribed antipsychotic drugs, while only 4.1 percent have been diagnosed with a psychiatric disorder.
• 47.1 percent of residents have been pre-scribed antidepressant drugs, while only 24.5 percent have been diagnosed with depression.
3. More physical, occupational, speech and recreational therapy are needed. BC lags behind Alberta and Ontario in these areas by a signif icant margin.
Alberta provides almost double the amount of recreational therapy and Ontario provides almost f ive times more physical therapy.
Read the full report at www.SeniorsAdvocateBC.ca
BC SENIORS’ ADVOCATE CALLS FOR IMPROVED HOME AND COMMUNITY CARE SERVICES
health because the acuity is so high. For Allen, the rewards of the job
are overshadowed by what she sees as the biggest problem in long-term care today: the lack of staff in every classification. In addition to needing more nurses, residents also need more physical and occupational therapy to keep them active and socially stimulated, she explains.
“The lack of staff actually pushes up costs to the health care system,” says Allen. “More physical occupa-tional therapy would reduce falls and injuries, and more recreation would reduce depression and patient outbursts. Better recreation would also reduce the amount of medica-tion residents take.”
Allen points to visionary seniors’ care policies in countries like Holland that keep seniors stimu-lated and active. “It astonishes me that we’re not following models like that,” she says. “They’re doing things the right way and it’s the kind of setting I want for my parents and grandparents if they need residential care.”
The information gathered during the course of the BCNU long-term care dinner meetings makes it clear that members working in this sector need more resources, and that mes-sage will be delivered to employ-ers and policy makers in contract negotiations. Our system needs to prepare for – and can easily accom-modate with appropriate planning – the growing number of baby boomers who will need long-term care services.
Allen says that baby boomers and those who don’t yet require care should demand better services to ensure they are available when they need them too. “The boomers that are approaching the system need to say ‘this isn’t the way we should be treated in our golden years – this system needs to change.’” update

12
BURNED OUT
LAST YEAR, OVER 2,000 BCNU members responded to a comprehensive survey conducted by researchers from UBC’s School of Nursing. Th e
objective was to build on existing research on nurses’ perceptions about their work environments.
Th e research unequivocally supports BCNU’s call for increased staffi ng. Nurses across sectors believe there has been a deterioration in quality and safety stan-dards within their organizations. Th e report fi nds that staffi ng is insuffi cient and there is simply too much work to do. On average nurses leave three to four essential tasks undone on their shift s.
BCNU will certainly be bringing these fi ndings to the bargaining table in the coming months, and Nurses’ Bargaining Association nego-tiators will cite this research to assist in the larger campaign for safe patient care.
However, an equally trou-bling fi nding is the survey’s insight into nurses’ mental health. High levels of emotional exhaustion were reported in every sector, as well as reports of post-traumatic stress. Many nurses also reported sleep disturbances and panic att acks. And instead of using profes-sional help as a way to deal with work-related stress, the majority of respon-dents’ coping strategies involved the use of informal supports, such as friends, family, exercise and hobbies.
BC NURSES’ WORKLOAD IMPACT STUDY REVEALS HIGH LEVELS OF EMOTIONAL EXHAUSTION
Dr. Maura MacPhee is the study’s principal researcher. She says that when nurses are consistently unable to carry out essential tasks, while also perceiving a real compromise to their professional standards, they get burned out.
MacPhee notes that over 45 percent of survey respondents reported high levels of emotional exhaustion, while 40 percent indicated that they intended to leave their jobs within the next year – and that’s a problem.
“Employers need to take note, because there’s a big correlation between nurse burnout – when they say they’re emo-tionally exhausted – and their desire to leave,” she says. “Sometimes they leave their current job, and sometimes they will
leave the whole nursing profession – so it is important that health care administra-tors look at those things and try to do what they can to improve nurses’ work environ-ment so that they don’t get burned out and they don’t leave.” Over 50 percent of nurses cited burnout as the main reason for their intent to leave, according to the report.
Not surprisingly, over 40 percent of sur-vey respondents reported that they were dissatisfi ed with their current job. When asked to identify the particular workload factors associated with their dissatisfac-tion, nurses cited emotional exhaustion, short-staffi ng, and a lack of time to com-plete necessary nursing tasks as primary culprits. Th ey also cited interruptions dur-
ing care delivery and documenta-tion as factors infl uencing their job satisfaction and levels of emotional exhaustion.
Health employers who are fi nd-ing diffi culties fi lling regular full-time positions should also note that of those respondents who worked part-time or casual, over one-third stated that they chose to work fewer hours because they felt that full-time work was too demanding.
Th e report should serve as a wake-up call for policy-makers and health employers. Th ere’s
no question that nurses are committ ed to safe patient care, but there is clear evidence that, without the necessary support, they are sacrifi cing their own well-being in the process. update
MENTAL HEALTH
fi ndings to the bargaining table in the
no question that nurses are committ ed to
To learn more about the study, please visit: www.bcnwis.net
Complete the confidential online survey at: www.bcnwis.net
Your password is: _______
UBC nurse researchers are partnering with BCNU to
document the impact of workload on nurses’ physical,
emotional and mental health as well as on patient safety.
Together with a random sample of nurses, you are invited
to take part in the study.
Survey participants will be entered in a draw to win a
Mini iPad or 1 of 5 $ 100 gift cards.
PARTICIPATE !
COMPREHENSIVE FINDINGS The detailed information on nurses’ work environments gathered in last year’s survey provides invaluable insight into the factors aff ecting BCNU members’ job satisfaction.
UNITED FOR SAFE PATIENT
CARESocial media networks lit up last month with the mes-sage “United for Safe Patient Care.” Th e occasion was BCNU’s fi rst ever “virtual rally” that took place during this year’s convention. Th e action succeeded in get-ting convention delegates to really make some online noise about nurses’ commit-ment to safe patient care.
CONVENTION 2015
MEMBERS WITH A MESSAGE BCNU’s virtual rally saw hundreds of nurses broadcasting their call for safe patient care.

14
WELCOME ADDRESS BCNU Executive Councillor Dan Murphy addresses delegates for the first time since BCNU’s merger with the Union of Psychiatric Nurses.
BARGAINING REPORT BCNU’s Executive Director of Negotiations and Strategic Development Gary Fane gives delegates an update on preparations for provincial bargaining in 2015.
Nurses used social media to reach thousands of people with their message without ever leaving the convention floor. The action involved the mass uploading of pictures and pre-recorded video clips pro-moting the message to Facebook sites for sharing with friends, family and beyond.
Rally organizers primed the pump dur-ing the week with teaser pics of BCNU executive members holding Safe Patient Care signs, posted to Our Nurses Matter – BCNU’s popular Facebook site with over 17,000 followers.
Photo and video booths were set up at convention to generate individual and group photos and video clips for upload-ing to the Our Nurses Matter page, and for sharing with members’ personal networks from there.
Delegates launched a clear message in cyberspace that nurses are indeed united for safe patient care.
PRESIDENT’S MESSAGEThe virtual rally marked the final day of BCNU’s thirty-fourth annual conven-
tion, which ran from Feb. 23–25. BCNU President Gayle Duteil kicked off the event with a powerful message for the over 500 delegates gathered in Vancouver for the event.
She said that when it comes to talking about conditions in BC’s heath care facili-ties, it’s nurses’ voices that tell the real story.
“All of you know that the patients lin-ing the hallways, the tub rooms and the emergency departments, and the elderly in the community who are waiting for assess-ments – they are not statistics.”
Duteil thanked del-egates for their unrelenting advocacy on behalf of their patients, and in the face of an employer who does not want to listen. “But these are the stories that matter, she said, “and we will tell them with our voices because we must tell them.”
She reported that the min-istry of health finally appears to be listening to nurses’ voices, and told delegates that the provincial govern-ment and health employers met recently to address the workload and patient care issues that BCNU stewards and activists have been con-
tinually raising.Duteil congratulated delegates on the
filing of over 4,200 grievances in just six weeks – a coordinated effort that should leave no doubt nurses are indeed united for safe patient care. “You folks did this – you helped get employers’ attention to get them to do what they should have done two years ago: implement a fairly negotiated agreement.”
The government has since indicated that it now plans to work constructively with nurses to resolve outstanding issues con-tained in the 2012–2014 contract. “I’m so very pleased that we’re finally making prog-ress, that nurses’ and patients’ voices will be heard.” (See special pull-out report on p. 13 that provides highlights of the grievance set-tlement reached with the government and health employers following convention).
Duteil also reminded delegates that –despite the ongoing advocacy and effort of the union to advance the occupational health and safety of its members – employ-ers are still not getting the message when it comes to protecting nurses from violent
“I’m so very pleased that we’re finally making progress, that nurses’ and patients’ voices will be heard.” BCNU PRESIDENT GAYLE DUTEIL
BRINGING NURSES TOGETHER BCNU President Gayle Duteil kicks off this year’s convention with a strong message of unity and hope for all nurses who are fighting for safe patient care.

UPDATE MAGAZINE May/June 2015 15
HUMAN RIGHTS & EQUITY The BCNU Human Rights and Equity Caucus met during convention to discuss current issues and prioritize its work in the year ahead. One urgent issue on their agenda was the federal Bill C-279, which is being delayed in the Senate. Bill C-279 incorporates transgender rights in the Canadian Human Rights Code and in the Hate Crimes provisions of the Criminal Code of Canada. Passed in the House of Commons in March 2013, the bill could die on the order paper if senators continue to delay its passage. Committee members, from left: Walter Lumamba, Mabel Tung, Catherine Clutchey, Kath-Ann Terrett, Kelly Woywitka, Jessica Celeste, Lori Pearson, Cynthia Reid, Jonathan Karmazinuk, Roni Lokken and Sherry Ridsdale.
“I wanted to learn about the decision making process and the running of the business – to be able to bring that back to my colleagues in public health in Campbell River, where vacation backfill has been an issue.”
FIRST-TIME DELEGATES’ VIEWSWHY DID YOU ATTEND CONVENTION THIS YEAR?
RYAN UNGERThompson North Okanagan
“I’m hoping to learn about how BCNU performs its business. I went to the f irst-time delegates’ session and learned a lot about how meetings are done.”
DEANNA ROMMSimon Fraser
“I’m actually quite proud to be a BCNU member, and that’s why I came. I feel support coming from everywhere, from my co-chair to the president – from the top on down.”
CAROLYN HUTTONPacific Rim
and aggressive patients.“We have waited too long for the
government and health authorities to take action, and our nurses have the broken jaws to prove it,” she said, before announc-ing that BCNU has created a new policy which will provide a range of supports for nurses who are physically or psycho-logically hurt. This includes the option of support for legal action taken by a nurse who has been injured on the job and who wishes to press charges against the attacker.
Duteil took the opportunity to welcome members of the Union of Psychiatric Nurses into the BCNU family, and noted that nurses are all too aware of the mental health challenges facing health care work-ers and their patients.
She said BCNU’s leadership in the
development of mental health strategy informed by the voice and experience of frontline nurses will go a long way to addressing this pressing social problem.
“We will create solutions and offer ideas as we help to address this overwhelming problem for patients with mental health issues.”
Duteil called on delegates to keep build-ing on their successes as they advance the profession of nursing and continue to provide some of the most complex and compassionate care available.
“Because at the end of the day we will find strength in unity,” she said, “one voice – united for safe patient care.”
PROVINCIAL LOBBY REPORTOn the second day of convention del-

16
egates heard from union vice president and provincial lobby coordinator Christine Sorensen, who remarked that a huge bonus of her many responsibilities is the time she gets to spend “working with members, hearing from members, and meeting with members.”
A highpoint for such contact was this year’s community bargaining outreach that saw Sorensen travel to 11 sites across BC and meet with some 880 community nurses. This consultation process identified issues from safety, violence and post-traumatic stress, to vacation backfill, job security and technology, all of which are being fed back into the community bargain-ing table.
Sorensen also praised the many local campaigns undertaken by the union’s 16 regional lobby coordinators. She mentioned BCNU’s rural and remote health care postcard (where over 3,500 cards calling for improvements were sent to Christy Clark) and support for the Single Mothers’ Alliance of BC’s child support clawback campaign as examples of lobbying success. “Small grassroots efforts can make for amaz-
ing results,” she said.Sorensen also blasted the Association
of Registered Nurses of BC (ARNBC) for pretending to be “our voice” while being run by “management and educators” and avoiding engaging with working nurses. Speaking defiantly, Sorensen said, “BCNU has over 42,000 members and we are proud to be the true voice of professional nursing in this province.”
RETIRING ACTIVISTS THANKEDSeveral retiring activists were recognized this year for their dedication and com-mitment to the union. Members also bid fond farewell to former BCNU President Debra McPherson, who served the union for over 18 years. Other outgoing activists thanked included East Kootenay region’s Patt Shuttleworth, Okanagan Similkameen region’s Laurie Munday, Fraser Valley region’s Linda Pipe, Interior Health LPN rep Janet Van Doorn, North East region’s
Jackie Nault, Central Vancouver region’s Margaret Dhillon, South Islands region’s Margo Wilton and South Fraser Valley region’s Lisa Walker. Duteil extended them best wishes on behalf of all BCNU members.
KEYNOTE SPEAKER MARGARET TRUDEAUDelegates attending this year’s convention were treated to Margaret Trudeau as the event’s keynote speaker.
Best known as the former wife of the late Prime Minister Pierre Elliott Trudeau, today the 66-year-old mother of five speaks about her experiences living with bipolar disorder as her way of encouraging others to better understand mental illness and to get help.
Trudeau spoke candidly about her life-long experience with mental illness. She recalled her healthy childhood in North Vancouver, and the changes she first began to notice as a young student. She told dele-
ACTIVISTS’ FAREWELL Several retiring activists were recognized this year for their dedication and commitment to the union. Members also bid fond farewell to former BCNU President Debra McPherson, who served the union for over 18 years. From left: Patt Shuttleworth, Laurie Munday, Linda Pipe, Janet Van Doorn, Jackie Nault, Margaret Dhillon, Margo Wilton and Lisa Walker.
PATIENT’S VOICE Keynote speaker Margaret Trudeau speaks candidly about her life-long experience with mental illness.

UPDATE MAGAZINE May/June 2015 17
gates about the lack of support she received when experiencing her first bout of depres-sion after the birth of her second child, and the onset of her episodes of mania.
Of all the ups and downs in her life, Trudeau told the convention that her low-est point came with the accidental death of her third son in 1998.
The tragedy sent her into deep depres-sion and isolation. “I was finished, I had no hope. I was physically ill, I was mentally destroyed,” she said.
Trudeau spoke about how she emerged from the darkness after being hospitalized
again in 2001, when she was first diagnosed with bipolar disorder, and of the benefit of the medical treatment she received that has given her new happiness and balance.
“It was the kindness and care of the nurses who helped me get back on my feet, who helped me recover, and who gave me the ability to want to live,” she said.
Trudeau noted the value in being proac-tive to ensure a successful recovery.
“You have to make the decision that you want to be better,” was her message to other individuals struggling with mental illness. “Don’t dismiss the idea that you can have a beautiful, wonderful, productive and purposeful life.”
Throughout her talk, Trudeau stressed the importance of self-care and nurturing the mind and the body with a healthy diet, exercise and sleep.
BYLAWS AND RESOLUTIONSDelegates to this year’s convention spent significant time debating proposed bylaw amendments and resolutions that members brought to the floor.
Delegates defeated a motion that proposed limiting the number of con-
secutive terms an officer could serve in the same position to no more than two. Delegates also voted against approving a bylaw amendment that would change the composition of the Nomination Committee from five regular members to three standing members and two auxiliary members.
Delegates rejected a resolution that called for an end to BCNU’s organizing of psychiatric nurses who are members of other unions and turned down a resolution that would reduce the president’s severance allowance to one week’s pay for every one year of service.
Delegates voted in favour of an emer-gency resolution calling for the continua-tion of salary reimbursement for members taking the Building Union Strength (BUS) course.
An emergency resolution calling on the BCNU to push for the federal government’s adoption of the United Nations Outcome Document upholding the rights of indig-enous people was referred to Council for consideration, as was an emergency resolution calling for BCNU to support family work-life balance by allowing all employees fair and reasonable vacation leave during school holidays. update
STUDENT NURSES MEET BCNU student members from seven BC nursing programs met during convention’s Young Nurses’ Network luncheon to discuss issues such as bursaries and the new National Council Licensure Examination (NCLEX). Back row: (l-r) Kelsey Hollett, Joseph Zeller, Gina Neumann, Diana Henson, Holly Gale. Middle row: (l-r) BCNU Council student liaison Sharon Sponton, Nadine McGinity, Jessica Wakeling, Catherine Miller, Regina Leung, Sarra Smeaton, BCNU education officer Lois Pierik. Front row: (l-r) Fiona Chiu, Autumn McIvor, Wendy Chan.
“BCNU has over 42,000 members and we are proud to be the true voice of professional nursing in this province.” BCNU VICE PRESIDENT CHRISTINE SORENSEN

18
1. BCNU Young Nurses’ Network provincial chair Catherine Clutchey and Central Vancouver region’s Isabelle Bertrand chat at the YNN booth. 2. East Kootenay region’s Nancy Silzer calls for extended OH&S call centre hours. 3. BCNU President Gayle Duteil presents LPN survey winner and Central Vancouver region member Catriona Busutil with an iPad Mini. 4. Delegates Manjit Bains, Harwinder Gill, Bernie Wright and Jessica Celeste. 5. 50-50 draw winner Georgina Lapointe receives prize from retired member Teresa Meierhofer. All funds raised went to BCNU’s Nurses’ Education Fund. 6. BCNU LGBT caucus chair Cynthia Reid smiles with Coastal Mountain chair Kath-Ann Terrett. 7. Delegates wear pink shirts to celebrate Anti-Bullying Day on Feb. 25. 8. Simon Fraser region’s Sherry Ridsdale and South Islands region’s Louise Laroche at the Aboriginal Leadership Circle booth. 9. BCNU’s Workers of Colour caucus met over lunch on Wednesday to talk about priorities in the year ahead. 10. Shaughnessy Heights region members rock it ‘80s style at the convention dance night hosted by the East Kootenay region. From left: Anne Shields, Eve Seto and Merissa Lacsamana. 11. Retired Pacifi c Rim region member Brenda Hill sells 50-50 draw tickets to Central Vancouver region’s Gulzar Hassan. 12. South Islands region’s Lenny Balaiah speaks to the need for more mental health resources in long-term care facilities. 13. North East region’s Cynthia Marquez participates in convention photo shoot. 14. Delegates Desta Azale, Sharon Sharp, unidentifi ed member, Malou Cordero, Menchie Rosales, Cedric Soriano and Christina Isidro take a break at the BCNU Communications Department booth. 15. Coastal Mountain region’s Amy Orodio poses with keynote speaker Margaret Trudeau. 16. South Fraser Valley region’s Cathy Robinson spins the Wheel of Fortune with Central Vancouver region’s Rae Wooffi ndin at the LGBT caucus booth. 17. South Fraser Valley region’s Rod Isidro and RIVA region’s Romy de Leon join BCNU Men in Nursing group chair Walter Lumamba at the MiN booth.
1 2
3
7
8
tickets to Central Vancouver region’s Gulzar Hassan. South Islands region’s Lenny Balaiah speaks to the need for more mental health resources in long-term care facilities. 13. convention photo shoot. Sharp, unidentifi ed member, Malou Cordero, Menchie Rosales, Cedric Soriano and Christina Isidro take a break at the BCNU Communications Department booth. Coastal Mountain region’s Amy Orodio poses with keynote speaker Margaret Trudeau. Cathy Robinson spins the Wheel of Fortune with Central Vancouver region’s Rae Wooffi ndin at the LGBT caucus booth. region’s Romy de Leon join BCNU Men in Nursing group chair Walter Lumamba at the MiN booth.
77
88
4
5
CONVENTION POSTCARDS
6

UPDATE MAGAZINE May/June 2015 19
9
1312
10
17
15
14
11
16
TTh e days of smoking in hospitals, or any work-place for that matt er, are long gone. Th e health risks of tobacco are well-established, and the over-all awareness of the importance of air quality and proper ventilation has made buildings much safer work environments than they were in the past.
NO SMOKING
Now imagine working in a modern hos-pital in BC and being expected to routinely inhale a toxic plume of smoke, live viruses, live bacteria, toxic gases and human tissue in the course of your duties.
Th is is the reality facing many operating room nurses and other health care profes-sionals working in BC hospitals today.
Th e toxins, which include things like the Human Papillomavirus, are produced when a heat-generating procedure is performed on human tissue. Th is includes electro-cautery and laser surgery. Th e plume is a part of the environment during operative and invasive procedures. And as lasers and electrosurgery become commonplace, the health of nurses and other perioperative practitioners is increasingly at risk.
Yet, since the mid-1970s, the body of evidence documenting the hazardous com-ponents of surgical plume has continued to grow. Plumes are now proven to be carcino-genic, mutagenic and fetogenic, and since 1996 there have been requirements mandat-ing surgical plume evacuation in BC’s occu-pational health and safety regulations.
However, it wasn’t until March of this year before the Vancouver Coastal Health Authority – home to some of the busiest ORs in the province – implemented an enforceable smoke evacuation policy that obligates managers to provide smoke evacu-ation on all of its units. And it likely would not have happened without the diligence and determination of BCNU members.
Vancouver General Hospital OR nurse Dallas Gogal is a member of the hospital’s Joint Occupational Health and Safety Committ ee. A nurse for the past 14 years, he joined the committ ee in 2013. Gogal says he’s seen a lot of surgical smoke in his time, and inhaled a lot of it too.
“I’ve known for a decade that this stuff wasn’t good for you,” he says of the surgical smoke that he was exposed to. “What I didn’t know was there were laws to ensure that we shouldn’t be breathing this.”
SPECIAL FOCUS ON SAFETY
VANCOUVER COASTAL OPERATING ROOM NURSES PUSH FOR ENFORCEABLE POLICIES TO PROTECT THEM FROM TOXIC SURGICAL SMOKE

Gogal says he learned more about surgi-cal smoke at a BCNU OH&S workshop. “I and the other members [of the JOHS committ ee] were quite upset when we learned about the actual law and found out we’ve been here completely unpro-tected,” he says. “And that’s prett y unac-ceptable – that’s when we had to move forward.”
Members learned that the only way to eliminate surgical plume as an occu-pational health hazard is to ensure that facilities consistently use smoke evacua-tion systems with special air fi lters. N95 respirators used alone are not eff ective.
Gogal and other nurses on the VGH JOHS committ ee discovered that, while their employer had a policy that instructed using smoke evacuators for all surgeries, it was deemed “non-enforce-able” on the grounds that there were either not enough available units to cover all ORs, or that there were legal obstacles in the procurement process required to install additional machines.
Undeterred, the BCNU JOHS commit-tee members, with the support of union staff , worked on a proposal for an enforce-able policy that the committ ee would send to management for a response. Workplace JOHS committ ees are made up of employee and employer reps, and it’s not always an easy task to reach the consensus needed to make a policy rec-ommendation to management. But that’s what Gogal and his colleagues were able to achieve, and in January the JOHS sent a 21-day lett er of offi cial recommendation to VGH management for a response.
U nbeknownst to Gogal, operating room nurses at UBC Hospital were ad-dressing similar concerns, and the VGH nurses’
eff orts to establish a policy, if success-ful, would apply to all workplaces in the
Vancouver Coastal Health Authority (VCHA). Th e timing could not have been bett er.
Jocelyn McCord is the operating room nurse coordinator at UBC Hospital and has worked in ORs for the majority of her 35-year career.
She says that nurses were not taught about the perils of surgical plumes when she was in school and it wasn’t until she joined the Perioperative Registered Nurses’ Association of BC in 2006 that she received formal education about sur-gical smoke and became more aware of the risks.
UBC Hospital is a major surgical day-care centre, with eight operating rooms and 800 staff , including 270 physicians and 450 nurses. Approximately 1,600 hip and knee replacement surgeries are performed each year, and surgical plumes are a daily reality at the facility.
When McCord began to advocate for consistent smoke evacuation, she discov-ered that the primary barriers she faced were technological and fi nancial.
She says that surgeons and nursing staff were not comfortable using the existing old, noisy and bulky smoke evacuation equipment designed to att ach to their surgical tools, and which could block their view while working.
“Th e physicians felt that they didn’t have proper visualization in their surgical fi eld with the smoke evacuation equip-ment provided,” she explains, adding that surgeries went ahead with no smoke evacuation whatsoever. “But surgeons said they would evacuate smoke if they were given a proper cauterizing pencil that provides smoke evacuation while allowing adequate, safe surgical fi eld visualization.”
In 2012 McCord spoke with equip-ment vendors and discovered that a range of cauterizing pencils are available, and that these were already being used
While most commonly encountered in operating rooms, surgical plume can be produced anywhere heat generating pro-cedures are employed on human tissue, including day surgery, labour and delivery, ICU/PICU/NICU, interventional radiol-ogy, emergency departments, outpatient clinics, etc.
If you work in any of these settings, you may have experienced plume-related symptoms, including:
• Nausea• Sore throat• Nasal/sinus congestion• Bronchospasm• Asthma/allergy• Headache• Ocular irritation• Excessive fatigue
While these symptoms can be tran-sient, and may clear when you leave the workplace, however they are indicative of an exposure.
If you have concerns:• Inform your manager/supervisor and
the Joint Occupational Health and Safety steward or representative at your worksite.
• Report the hazard as soon as pos-sible using the employee incident reporting process at your worksite, e.g. Employee Call Center, elec-tronic, or paper employee incident report.
• Participate in the incident inves-tigation process with the Joint Occupational Health and Safety steward/representative at your workplace.
• You can also f ile a lack of safe work-place grievance.
• You may follow the steps for Refusal of Unsafe Work.
HAVE YOU BEEN EXPOSED TO SURGICAL PLUME?

22
staff at UBC as soon as she learned about it.“UBC Hospital was one of the last hospi-
tals in the country to get on board to fi nally implement a policy and make equipment available,” she says. “And that didn’t happen until March 2.”
G ogal and McCord’s experi-ences illustrate that it’s possible to eff ect change with diligence and perseverance. In both cases management
initially resisted their initiatives, but chose to work with staff through the JOHS com-mitt ee to achieve a resolution. Both nurses also had to work with colleagues – both BCNU members and other health care workers – and get their support in helping achieve their goals.
Th e new policy has been in place for two months, and Gogal says he is pleased with its implementation so far.
“As far as I am aware, we are at 100 percent compliance now,” he says. “I’ll give credit to management. Th ey’ve brought another company in and expanded their range of [smoke evacuation] options that can be used by the surgeons – and that addressed a lot of the surgeon group’s concerns.”
He also notes that the available range of smoke evacuation tools means there is no longer an excuse for a surgeon or anyone else to avoid using one of the products.
Gogal’s message to other members who have an occupational health and safety concern? “Find your JOHS committ ee, meet your rep and realize that you can work through the committ ee,” he says. “It’s your venue for working together with the employer to solve something.”
Gogal is also happy for his team to serve as an example for others. “If there are members in other parts of the province suff ering from surgical smoke issues, they should know that there are many places like Vancouver General that have successfully solved the problem,” he says. “You can be protected and still be in surgery, and every-body can be winners, right?” update
Meanwhile, the members at VGH had met with success. In February, VGH management announced a new policy and brought 16 new smoke evacuator machines on site so that all operating rooms have adequate evacuation. Th e policy came into eff ect March 2.
“It was more challenging than I expected,” confesses Gogal on the JOHS committ ee’s eff orts to establish the policy. “But I’m glad it’s over. However hard it was to get it going, everybody walks away as a winner because of it.”
McCord sent the new VCHA policy out to
SPECIAL FOCUS ON SAFETY
OH&S CHAMPIONS University of BC Hospital nurse Jocelyn McCord and Vancouver General Hospital nurse Dallas Gogal both worked to successfully ensure that Vancouver Coastal Health Authority implemented an enforceable surgical smoke evacuation policy for its operating rooms.
EXPERIENCING SYMPTOMS? DO THE FOLLOWING:• Report the exposure as soon as possible using the employee incident reporting process at your worksite, e.g. employee call center, electronic, or
paper employee incident report.• Register on the WorkSafeBC exposure registry if you have experienced an
exposure.• If you develop surgical smoke-related illnesses f ile a WSB claim in case of
required treatment and/or time loss.
in other hospitals within the health authority and the the province. McCord then approached hospital manage-ment who initially agreed to the trial use of the new equipment. However, it was not long before equipment managers decided that the product was too expen-sive, and could not be provided to some hospitals without off ering to all.
“It was denied on that basis,” she says.
McCord raised the issue with her workplace JOHS commit-tee and received support from BCNU staff on how to cor-rectly document concerns and keep them on the employer’s agenda.
She’s not surprised that the momentum for changes at UBC which picked up last year happened independently from the initiative that nurses were taking at VGH.
“A lot happens in isolation,” she says, indicating that many policies are applied inconsistently across the health authority. “I found out that Lions Gate and Richmond Hospital have been using a smoke evacu-ation pencil for the past four years,” she recalls, “so I suspected that this was just [UBC] management not wanting to spend the money – because the other sites appar-ently seemed to have managed it without requiring a [formal enforcement] policy.”

UPDATE MAGAZINE May/June 2015 23
SAFE NURSES = SAFE PATIENT CARE The BCNU bus was on hand for a March 10 news conference at Abbotsford Regional Hospital to call for action after an ER nurse at the facility was savagely attacked, suff ering serious trauma and injury. Back row: Chilliwack General Hospital steward Mike Goerzen, Fraser Valley region PRF advocate Janice Young, BCNU President Gayle Duteil, Abbotsford Regional Hospital full-time steward Elvira Martens, ARH nurse Robin Price, former BCNU Executive Councillor Will Offl ey and ARH steward Doris Rettich. Front row: ARH stewards Kathi Dempsey, Heather Quayle and Ravi Kochar, and Fraser Valley region chair Katherine Hamilton.
HEALTH AUTHORITIES MUST IMPROVE NURSES’ SAFETY NOW
The chronic levels of prevent-able workplace violence that BCNU members have been consistently reporting is a clear indication that serious action is
required on the part of the provincial govern-ment and health employers to address this occupational health and safety issue. And the BC Nurses’ Union has made violence one of its top priorities as it prepares for collective bargaining in the year ahead.
“We will not have a new collective agree-ment signed until the issue of violence is
offi cials, Duteil has received a lett er from Deputy Minister of Health Stephen Brown committ ing to address the problems:
“…the government will commence work linked to your proposal on ensuring the safety and security of nurses working in high risk mental health care services with a view to taking some practical concrete steps to make real improvements in the sites you have identifi ed.”
Duteil says any changes can’t come soon enough for nurses on the front lines. “Nurses put themselves at risk every day while trying to provide safe patient care. Many violent att acks can be prevented by increasing safety offi cers, and providing personal alarms, specialized training and appropriate staffi ng levels for the patients’ care needs, especially those who are aggressive or violent.”
Health Minister Terry Lake reiterated the government’s commitment at a recent violence prevention summit of health care leaders in Richmond that was att ended by BCNU. “We can’t accept that violence is part of the job – it’s a huge challenge and we’ve got lots of work to do,” said Lake.
(Sadly, as Update went to press, another nurse was viciously att acked at Hillside Centre in Kamloops. Duteil called for imme-diate action, and aft er meeting with Lake and Interior Healthy Authority manangent, a 24-7 safety offi cer was posted to the worksite.)
Th e Ministry of Health has promised to consider all of the solutions that BCNU has proposed and has committ ed to a plan that will begin by gathering information from four sites out of the 12 that BCNU has identifi ed as needing immediate att ention. Th ese include:• Forensic Psychiatric Hospital, Coquitlam• Hillside Centre at Royal Inland Hospital,
Kamloops• Seven Oaks Tertiary Mental Health
Facility, Victoria• Abbotsford Regional Hospital
Abbotsford is one of many sites in BC where nurses have felt unsafe at work. In March a nurse was assaulted while triaging a
addressed,” said BCNU President Gayle Duteil at a March 10 news conference organized in response to the problem. She indicated that unsafe staffi ng levels are at the root of much of the violence that nurses are experiencing, and until health authorities begin honouring their 2012 contract com-mitments to maintain baseline staffi ng levels and replace nurses when required, it will be very diffi cult to move forward.
Th e union’s warning got the att ention of the government, and now, aft er numer-ous meetings with government and health
BCNU CALL FOR VIOLENCE-FREE WORKPLACES FINALLY GETS GOVERNMENT’S ATTENTION
BREAKING POINT
continued on page 25

24
so that added an additional obstacle of placement,” she notes.
It was Herrington’s steward who sug-gested she make contact with the BCNU Enhanced Disability Management Program (EDMP) representative from her region.
Jointly administered by the employer and the union, the EDMP is a pro-active, customized disability management program designed to help members off work or
G wen Herrington began studying to become an RN shortly aft er graduating as an LPN in 2002. Th e Dawson Creek nurse wanted more
knowledge – and a life-changing diagnosis of kidney disease in 2005 gave her the mo-tivation to fi nish the RN program as soon as possible. “As an LPN, the work was too physically demanding,” she explains. “But as an RN I could work part-time as a liaison nurse while still having enough kidney function to be an eff ective nurse.”
However, in 2012 Herrington needed to go on long-term disability as her kidney function decreased to the point that she needed dialysis and could no longer work as a liaison nurse at Dawson Creek Home and Community Care due to the fatigue.
Herrington was on dialysis for over two years before receiving a transplant in July 2014. “A wonderful friend, who is also a nurse donated to me,” she says. “Th e trans-plant is a gift of life, but more specifi cally it is the gift of MY life back – I would encour-age people to donate.”
Last February Herrington received the good news from her physician that she was approved to return to work. But the transi-tion came with challenges. Herrington’s decreased immune system required that she work in an environment where she wouldn’t be exposed to very sick patients. “My position was eliminated in my absence,
ENHANCED DISABILITY MANAGEMENT PROGRAM HELPS ILL AND INJURED MEMBERS RETURN TO WORK
COLLABORATIVE SUPPORT
EDMP COMING TO AFFILIATE WORKSITES IN 2015 EDMP has been fully implemented for all BCNU members who are employees of a Health Authority. Starting in May 2015 EDMP will be implemented into aff iliate worksites through a graduated roll-out. Watch your email and bulletin boards for more details of when it is being implemented at your aff iliate worksite.
struggling at work due to an occupational or non-occupational illness or injury.
Th e regional BCNU EDMP repre-sentative works collaboratively with the employee and disability management professional to address all barriers to a return to work through the development of an individualized case management plan. Th e plan may include medical intervention, transitional work, a graduated return to work, workplace modifi cations and voca-tional rehabilitation and/or retraining.
Herrington says she was vaguely aware of the program, but admits that she made some assumptions about what it was. “I didn’t ever think it would apply to my own needs.”
Aft er meeting with Wanda Veer, the BCNU EDMP rep for her region, and employer representatives, Herrington says that options opened up for her, and she found herself pleased with how quickly things progressed. “A teleconference was set up immediately, and when we ended the call a plan of action and schedule for future meetings was in place,” she recalls. Th e manager and EDMP team reviewed options where there were vacan-cies and identifi ed those that would suit Herrington’s abilities.
From start to fi nish it took Herrington less than six weeks to know that she would be returning to work in public health on a part-time basis, although she notes that it can oft en take several months to accommo-date members in the program. She says that on her fi rst day back to work, her manager and co-workers could not have been more supportive.
Herrington says the approach of both her employer and union was cooperative and
CUSTOMIZED ASSISTANCE Dawson Creek nurse Gwen Herrington took advantage of the Enhanced Disability Management Program to help her transition back to work after a long-term disability. She encourages any nurse needing support returning to work to contact the program.
SPECIAL FOCUS ON SAFETY

UPDATE MAGAZINE May/June 2015 25
patient in the ER. Without warning, the patient lunged across the desk and attacked the nurse, who was left with stitches and an eye injury requiring surgery.
Following extensive media coverage about the incident, a third safety officer was finally hired to protect staff in the ER. In addition, new safety barriers have been put in place in the triage area.
Nurses at the facility say it’s been a long battle just to obtain these few necessary protections. “We have been asking for increased security since 2011,” says BCNU Fraser Valley region chair Katherine Hamilton. “The situation had become so bad nurses were afraid to come to work. We were so frustrated, we contacted the media and after that a few changes were finally made.”
The progress in Abbotsford and the recent commitment from the government are promising, but the risk of violent attacks and injury remains, and all members are reminded to use existing tools to address the problem.
“BCNU members need to know that there are many supports available to address their safety concerns,” says Duteil, who reminded nurses that Joint Occupational Health and Safety Committees, griev-ances and professional responsibility forms (PRFs) are just some of the ways that members can work together to improve safety for them-selves, their co-workers and their patients.
“We will continue to advocate for improved staffing levels and demand that BC health authorities and affiliates take responsibility for safety and follow through on their legal requirements,” she says. update
• All regular employees who are off work for one day with a work-related illness or injury, or f ive consecutive shifts with a non-work related illness or injury, participate in the program.
• Casual employees and regular employees who are struggling but continue to work may self-refer.
• Case Management Plans are developed collaboratively between the disability management professional, the employee and BCNU EDMP representative. Plans reasonably address all barriers to return to work including medical, personal, vocational and/or workplace.
• All confidential medical information is protected.
Health Care and Social Services
56%
Education 10%
Hospitality and Leisure Service
6%
Public Administration 6%
Retail 6%
Transportation and Related Services
5%
Other 11%
supportive. “I could tell that everyone was seek-ing the best for me.” She encourages any nurse need-ing support returning to work to contact EDMP. “It can make a difference.”
If you are struggling at work with occupational or non-occupational illness or injury, contact your steward or regional EDMP representative about self-referring to EDMP. update
EDMP HIGHLIGHTS
In response to the ongoing lack of support for injured nurses, BCNU is developing a policy to provide assistance to members who have been hurt on the job due to violence. This includes both physical and psychologi-cal harm caused by workplace violence.
BCNU will support members in a variety of ways in their time of need. The draft policy, which Council has approved in principle, will:
• Establish a 1-800 hotline for
nurses injured on the job.• Defend and assist all mem-
bers – including casuals – who are injured on the job due to workplace violence according to the provisions of the collective agreement.
• Provide limited f inancial support for employment income lost while awaiting WorkSafeBC claims to be processed (to be reimbursed by member once claim processed).
• Provide support for mental and physical health.
“The purpose of this policy is to assist members in their time of need and to ensure that employers adhere to their obli-gations,” says BCNU President Gayle Duteil. “Nurses need and deserve better protection from violent and aggressive patients.”
Duteil also reports that BCNU intends to assist nurses who wish to pursue legal action against an attacker. update
BY THE NUMBERS VIOLENCE IN HEALTH CARE
WorkSafeBC claims• There has been a 70% increase in health care claims in the
past ten years. • 42% of all injured worker claims in health care are in long-
term care.• 70% of claims are made by women over the age of 35.
NEW BCNU POLICY OFFERS HELP FOR NURSES INJURED ON THE JOB DUE TO VIOLENCE
How does health care compare to other sectors?
BREAKING POINT continued from page 23
Source: WorkSafeBC

26 SPECIAL FOCUS ON SAFETY
A LAX SAFETY CULTURE AND A RECENT SPATE OF INJURIES HAVE NURSES WORKING AT THE PROVINCE’S MAJOR PSYCHIATRIC FACILITY RINGING THE ALARM ABOUT WORKPLACE HEALTH AND SAFETY
tals in BC, with 7 percent of staff reporting injuries versus 4.1 percent in other facilities.
Like every employer in BC, FPH is obliged by law to take comprehensive steps to elimi-nate or minimize the risks of injury to its workforce. But FPH’s management, despite seeing a much higher-than-average ratio of violent incidents and being ordered repeat-edly by WorkSafeBC to comply with occupa-tional health and safety regulations, appears reluctant to make safety its top priority.
In fact, staff have said it feels like their employer’s concern with budgets has trumped its commitment to provide quality care to clients, optimize the therapeutic relationship between nurses and patients, and protect nurses from assault on the job. A new staffi ng model in place since 2013 that reduced baseline staffi ng and scrambled shift s is widely felt to have seriously compro-mised the continuity of care.
“Regular shift patt erns lead to safe care by supporting therapeutic outcomes,” says FPH nurse and BCNU steward Ron Morley. “Familiarity has a therapeutic value, and therapeutic rapport leads to safety
Imagine what it’s like working with the most clinically challenging patients in British Columbia while wondering that if things go sideways, management will not have your back.
Or what it’s like to head home at the end of each shift feeling lucky that you didn’t get injured on the job that day.
Th at’s the grim reality faced by some 190 registered psychiatric nurses and registered nurses at BC’s Forensic Psychiatric Hospital (FPH) in Coquitlam. Th ese BCNU mem-bers, along with about 250 other health care workers, care for unpredictable, potentially violent patients at the 190-bed facility.
FPH is where people who have committ ed serious crimes, but deemed unfi t to stand trial due to mental illness, are sent for treat-ment. Nurses and other health care workers play a key role in the therapies designed to enable these patients to eventually return to society. But the nature of this population means the potential for violence and risk of injury to staff is ongoing. According to WorkSafeBC, the hospital’s injury rate is 75 percent higher than other acute care hospi-
because the patients trust you.”Staff report that the switch to a scheduling
structure that sees nurses working diff erent shift s on diff erent units, and with absences fi lled from a fl oat pool of nurses who are oft en not adequately oriented – has led to instability in therapeutic relationships, with negative implications for workplace safety.
“Back when we had four-on, two-off , there was always continuity of care and people knew what was going on,” says 20-year nurse Carole Anne Pominville. “Now we’re exhausted, we’re swinging shift s too much, we’re always with diff erent people.”
“When it was ward-based, you knew every patient on your unit, and their history,” she explains. “Now, with the number of on-call and relief [staff ], it’s a whole diff erent story.”
Staff say the recent staffi ng model changes have only served to aggravate stress levels and feelings of insecurity in a workplace where safety training remains erratic and when violent incidents occur all too frequently. And tensions have been compounded by the fact that repeated orders, warnings and a major fi ne issued by WorkSafeBC to address health and safety have largely been ignored.
“Th ere appears to be fundamental problem with the way this facility is being managed,” says BCNU President Gayle Duteil. “Th e employer needs to start listening to nurses’ safety concerns and taking WorkSafeBC orders seriously.”
The Forensic Psychiatric Hospital falls under the administrative jurisdiction of the Provincial Health Services
Authority (PHSA), but the operational and clinical management is provided on contract by the Forensic Psychiatric Services Com-mission (FPSC). Responsibility for ensuring a safe, healthy workplace thus falls on two parties, yet neither appears to be taking the role as seriously as provincial legislation requires.
Systemic neglect of safety at FPH fi rst came to light aft er a serious stabbing incident in September 2012, where a patient with a known history of violence was alone with a
THE MOST DANGEROUS HOSPITAL IN BC

UPDATE MAGAZINE May/June 2015 27
therapist and allowed access to a large unse-cured knife. A subsequent WorkSafeBC investigation revealed just how lacking the culture of safety was at FPH.
Morley, first on the scene following the stabbing, says the incident reveals manage-ment’s blatant disregard for worker safety. Ultimately, WorkSafeBC found FPH in total breach of its obligations to eliminate or min-imize the risk of violence to its workforce. In April 2014, it issued four orders setting out detailed measures to ensure compliance with provincial regulations.
Despite being directed to implement the measures without delay, Morley reports that only some of the required steps have been taken, and nearly a year later FPH is still resisting coming into full compliance.
A December 2014 WorkSafeBC inves-tigation report on subsequent incidents identified further violations of provincial regulations. FPSC was then assessed a fine of $75,000 because the employer:• “failed to take sufficient precautions for
the prevention of work-related injuries”• “[had] not maintained a safe workplace or
safe working conditions”• “did not exercise due diligence to prevent
these circumstances”Dr. Johann Brink, Clinical Director of
Psychiatry at the facility, disputed the basis for the fine, claiming in a letter that the report “does not take into account changes made since the incidents,” which he listed. However, WorkSafeBC had closely assessed those changes and found that many were inadequate or incomplete.
WorkSafeBC then issued an administra-tive warning, this time to the PHSA, regard-ing management’s failure to bring FPH into compliance. Noting it had established grounds to assess another fine, WorkSafeBC opted instead for a formal warning as “the appropriate course of action to motivate your firm [PHSA] to comply with the Act”.
Finding motivation to proactively protect its workers appears to be an ongoing chal-lenge for FPH management, and PHSA is still silent on the matter. In response to the employer’s delaying tactics, BCNU filed a
Single Employer Policy Dispute (SEPD) grievance on Jan. 12 over PHSA’s continuing failure to minimize the risk of violence to staff at FPH. The dispute alleges that PHSA is:• Not providing appropriate staffing for
patient acuity.• Failing to ensure that seclusion/post-
seclusion work practices are done in a safe and appropriate manner.
• Failing to address particular weapons infractions (Plexiglas, rope, X-ACTO blades, lamp parts) appropriately.
Practices relating to the use of seclu-sion rooms at FPH provide some of the clearest examples of how
management continues to stubbornly resist changes that would remove or greatly diminish safety risks. Seclusion rooms are used to isolate and settle patients who pose an immediate risk to themselves or others, so there is a heightened risk of violence towards staff especially if they are alone with patients.
In just over a year, five workers have been injured providing food to patients in seclusion, and there were 26 reported cases of aggression that did not result in injury. In September 2014, the hospital’s Joint
MAKING SURE SAFETY COMES FIRST Forensic Psychiatric Hospital Joint Occupational Health and Safety Committee members (from left) Philip Oosterman, Carole Anne Pominville and Ron Morley say recent staffing model changes have increased stress levels and feelings of insecurity in their workplace.
Occupational Health and Safety Committee ( JOHS) formally asked the employer to install pass-through food slots on seclusion room doors to avoid individual contact with unsettled patients.
Management rejected this request on grounds that shielding workers from violence in this way would somehow be “detrimental to creating a positive therapeutic milieu for assessing, treating and rehabilitating persons with severe mental illness.” They proposed instead that a set of secondary controls to reduce risk be explored, which the JOHS declined because they don’t address risk, and opted instead to bring WorkSafeBC back in to
resolve the issue.A subsequent WorkSafeBC inspection
and incident review endorsed the viability of pass-through food slots as an interim control while dismissing management’s arguments against this solution. WorkSafeBC’s report also reminded FPH of its obligation to eliminate or minimize the risk of violence and ensure that its current practices do not contravene OH&S regulation 4.29 (b). WorkSafeBC ordered FPH to review and revise procedures accordingly and to prepare a Notice of Compliance report by March 31.
The date has come and gone. Neither BCNU, worksite stewards nor the JOHS committee have received the report as required by law. And to date, the employer appears to have taken no action to bring FPH into compliance. It would seem that stalling, delay or outright refusal to mini-mize risks to workers continues to be the entrenched mindset at FPH.
“Nurses’ occupational health and safety is a major priority for the union,” says Duteil. “The failure of this employer to protect their workforce when dealing with dangerous patients is shameful. We will be supporting our members in this dispute and advocating strongly for safe patient care.” update
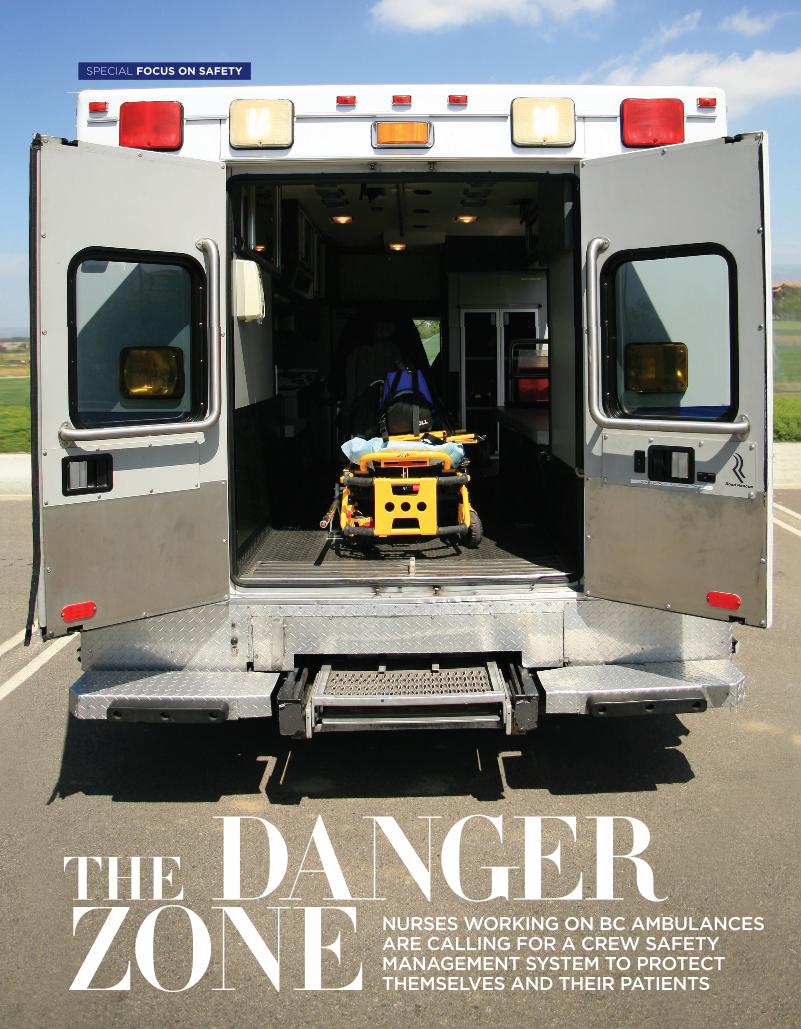
2828
THE DANGER ZONE NURSES WORKING ON BC AMBULANCES
ARE CALLING FOR A CREW SAFETY MANAGEMENT SYSTEM TO PROTECT THEMSELVES AND THEIR PATIENTS
SPECIAL FOCUS ON SAFETY

UPDATE MAGAZINE May/June 2015 29
High Acuity Response Team (HART) nurses att end to acute patients in rural and remote health sites, either stabilizing them
to avoid transfer or transporting them by ambulance to a higher level of care.
Nurses like Kim Brown have tons of experience saving lives in ambulances. But a 2014 ambulance crash switched her role from HART nurse to ambulance patient in a terrifying vehicle rollover that happened in the blink of an eye.
Th e July 2014 accident that could have killed Brown and the crew was entirely pre-ventable because the risks that preceded the crash were clearly visible at the time.
Brown started her night shift on July 23 in the high-acuity unit at Trail’s Kootenay Boundary Regional Hospital. At about 2:00 a.m. the BC Ambulance Service (BCAS) dispatched her and a paramedic crew to Nelson’s Kootenay Lake Hospital to move a critically ill patient to Kelowna. Just before they left Nelson one of the paramedics told BCAS they were fatigued. Th e crew was sent anyway.
Th ey left Nelson for the two-hour drive to Grand Forks where they planned to meet a Penticton-based crew who would take the patient to Kelowna. But that plan would change along the way.
“Just outside of Grand Forks, BCAS told us we had to drive another hour and meet the Penticton crew in Midway,” says Brown. “Th at adds another two hours to our shift by the time we get home.”
BCAS knew that some of the crew felt very tired, but still extended the transport. And during the journey one paramedic radioed BCAS three times to report that they felt fatigued.
Brown’s crew made it safely to Midway and handed over the patient to the next crew. Th en they started their three-hour journey home to Trail. But three hours of driving on an already long day can create a dangerous situation.
“We were about 10K from Trail when I felt the ambulance veer right and leave the
road,” says Brown, who was sitt ing in the back of the ambulance. “It happened so fast that all I remember is rolling around uncontrollably, and equipment was crash-ing around me.”
Th e ambulance skidded off the road and rolled down a 50-foot ravine. Th e batt ered vehicle lodged against a tree that stopped it from rolling further.
“I didn’t lose consciousness and when the ambulance stopped rolling I smelled fuel and smoke,” says Brown. “Th e back exits were crushed, and the driver was unconscious and blocking the exit window into the front cabin. I was trapped in the ambulance, and didn’t know if the fuel would explode.”
A passing motorist arrived at the scene and removed the unconscious driver from the cab. Th en Brown crawled to safety through a window into the cab. Th e rollover had scatt ered their equipment and cell phones so they couldn’t call for emergency services.
Th e motorist used his cell phone to call for help, and a fi re truck and two ambu-lances arrived quickly at the accident scene.
In less than 15 minutes, Brown’s role switched from being a high-acuity transport nurse to an ambulance patient. She was off work for almost eight months because of spinal fractures she sustained in the roll-over. Th ere were no shoulder harnesses in the ambulance’s back seats that could have prevented this injury.
Brown says that in hindsight she sees a whole chain of events that conspired to cre-ate an unsafe situation for the crew. Th ere were clear warning signs at the beginning of their journey and at points along the way that the transport was becoming unsafe.
A crew safety management system (see sidebar p. 30) would have mitigated some of the following danger signs: • Before the crew left Nelson one of the
paramedics reported they were feeling very fatigued. Currently, crews don’t have the safety protocols to collectively monitor their safety or the authority to change plans if circumstances are gett ing unsafe.
• On three separate occasions a para-medic reported they were gett ing more fatigued. A safety management system would empower the crew to pull over and rest until another crew is found to fi nish the transport.
• Th e paramedics had transported a critically-ill patient earlier that day which increased their fatigue. Th at should have been considered before they were sent on a lengthy transport.
• Transferring the patient in Midway and refueling in Grand Forks were natural points for a crew safety discussion. Th ose discussions didn’t happen because there’s no protocol for the crew to assess safety at enroute points.Clear standard operating procedures that
focus on crew safety could have prevented this accident at multiple points along the way. And 10 months aft er the accident the Interior Health Authority still hasn’t implemented a safety management system for HART nurses.
“We need to be very careful not to blame individual staff members for events like this because nurses, paramedics and BCAS staff are all working hard in tough conditions,” says Brown. “Th e problem is systemic. IHA and BCAS need to implement protocols to keep us safe and help us make alternate plans when circumstances are gett ing unsafe.”
Scott Lamont is a Trail-based HART
“It happened so fast that all I remember is rolling around uncontrollably and equipment was crashing around me.” HART NURSE KIM BROWN

30
nurse with more than 20 years of experience transporting critically ill patients in Canada and the U.S. He’s also fl ight board certifi ed as a Certifi ed Flight Registered Nurse (CFRN) in the U.S. to provide emergency and critical care in an air transport environment.
Lamont’s experience as an emer-gency transport nurse in northern Canada and New Mexico gives him a broad perspective on what safety should look like for BCAS staff and the nurses who work with them.
“In New Mexico we used stan-dardized protocols to assess crew and patient safety before we left the sending facility and at points along the transport route,” says Lamont. “It’s inconceivable that airline crews wouldn’t have safety protocols to fol-low at every point in their journey, and ambulance crews shouldn’t be any diff erent.”
Lamont says employers must implement safety protocols that reduce risks for transport nurses and paramedics. Industry-standard safety management systems would fi x many of the problems they see every day.
Some of the protocols Lamont suggests include:• Using pre-departure briefi ngs where factors
like patient safety, road conditions, equip-ment checks and transport duration are all discussed in advance.
• Establishing a clear decision-making authority about who gets to make “go or no-go” decisions, or when plans need to be adjusted during transport.
• Implementing a minimum equipment list that says “no-go” if important items are damaged or missing.
• Assessing when it’s safe to leave the hospital whenever hospital management pressure staff to transport patients as quickly as pos-sible (transporting patients right away isn’t always the best decision because weather conditions, roads, crew fatigue and equip-ment failures might mean it’s bett er to keep the patient where they are).
Lamont is unequivocal in his demand for action. “We need a comprehensive safety management system that brings HART nurses, hospital staff and BCAS employees onto the same page to focus on crew safety. Until we have that, the risks to crews and patients will keep multiplying,” he says.
BCNU has advocated for Kim Brown’s acci-dent investigation to be fi nalized, so that the void in the overall safety regime can be fi xed.
“If IHA won’t do the right thing and imple-ment a transport safety management system then nurses need to know they have a legal right to refuse unsafe work,” says BCNU President Gayle Duteil, who is watching the BCAS/IHA accident investigation carefully. “If nurses believe there are risks along the transport route they can simply refuse to go, or refuse to continue,” she says. “Th e law is clear – no one is required to put themselves in unsafe conditions and BCNU will support our members’ right to refuse all unsafe work.”
Lamont stresses that what happened to Kim Brown could happen to any nurse in BC who’s transporting a patient. “We need to be sure that safety measures are in place for all nurses travel-ling in ambulances.” update
The Commission on Accreditation for Medical Transport Systems (CAMTS) sets industry-leading benchmarks for safety standards in the U.S. It also accredits medical transport systems in Canada, the UK and South Africa.
Patient transport systems can-not be CAMTS accredited unless they have clearly defined crew safety management systems.
Employers should include the following procedures and equip-ment in crew safety systems: • Structured protocols to evalu-
ate road conditions, weather forecasts, crew fatigue/rest, equipment status, transport duration and patient acuity before leaving the hospital, and at points during the transport.
• Clear roles and responsibili-ties on the crew and with BCAS dispatch to collectively make safety decisions and adjust plans when dangers emerge.
• Training on the right to refuse unsafe work.
• Training HART nurses, BCAS staff and hospital manage-ment to focus on transport crew safety as well as patient well-being.
• Up-to-date safety equipment in ambulances such as f ixed satellite phones in the back of the ambulance, GPS or satellite tracking systems, ‘black-box’ recordings, helmets and adjust-able seats so nurses can treat patients while they’re in lap and shoulder restraints.
KEEPING SAFE ON THE ROADCrew Safety Management Systems are industry benchmarks in the US
NARROW ESCAPE The wreckage of a July 2014 ambulance rollover near Grand Forks that nearly claimed the life of trans-port nurse Kim Brown highlights the need for improved crew safety management systems.
SPECIAL FOCUS ON SAFETY

UPDATE MAGAZINE May/June 2015 31
STANDING UP FOR MEDICAREBC Nurses’ Union members joined with public health care supporters across the country March 31 in a national day of action calling for federal leadership in health care.
NATIONAL DAY OF ACTION BCNU MEMBERS ACROSS BC RALLY IN SUPPORT OF PUBLIC HEALTH CARE, CALL FOR FEDERAL LEADERSHIP
MEDICARE
MARCH 31 MARKED THE one-year anniversary of the expiration of the 2004 – 2014 Health Accord – an important deal that set funding and health care service delivery agreements between the federal and provin-cial and territorial governments.
Th e Harper Conservatives’ refusal to negotiate a new deal
1. South Fraser Valley region lobby coordinator Walter Lumamba at a rally of health care workers at Surrey Memorial Hospital. 2. Dawson Creek Hospital nurse Connie Schmakeit. 3. Nanaimo Regional General Hospital Nurse Sharon Fulton (l) is joined by a retired vacationing nurse from Alberta at a rally in Nanaimo. 4. West Kootenay region members joined a rally in Nelson. From left: Sarah Crossley, Jessie Renzie, Colleen Driscoll, Angela Falk and Chantal Robert. 5. Thompson North Okanagan region members Diane Lingren, Tracy Musey and Brenda Boynton rally at Royal Inland Hospital. 6. North West region lobby coordinator Kathy Buell is joined by Wendy Onofrenchuk and Ingrid Overbeek in a visit to the Terrace offi ces of Skeena-Bulkley Valley MP Nathan Cullen. 7. Dawson Creek Hospital nurse Amanda Chmelyk and UNBC student nurse Sheena Muir. 8. Dawson Creek Hospital nurse Shallyn Kocis shows her support for public health care. 9. South Fraser Valley regional executive members Michelle Sordal, Melissa Lee and Jonathan Karmazinuk visited the offi ce of Surrey-Fleetwood MP Nina Grewal.
1 2 3
7
8
9
4
5
6
with the provinces has signaled a historic shift away from the federal government’s leader-ship role in health care policy and fi nancing. Th is was an unfortunate decision, especially considering that the 2004 deal was designed to rectify years of federal underfunding during the 1990s.
BC Nurses’ Union members joined with public health care supporters across the country in a national day of action to remind the federal government that Canadians will not forget Ott awa’s betrayal, which will see $36 billion worth of health care cuts come into eff ect aft er this year’s federal election.
Nurses and others are con-cerned that the lack of federal leadership in health care will lead to 14 diff erent health care systems, with access depending on where patients live and their ability to pay.
“Canada is facing an impor-tant next step in our medicare history,” says BCNU President
Gayle Duteil. “We need to tell Ott awa that that everyone – provincial and territorial gov-ernments, First Nations and the federal government – should come together to negotiate a health care accord that delivers bett er, more effi cient, quality public health care.
“We have an aging popula-tion and demand for health care is increasing – unless federal funding is stable and adequate, our cherished public system is in danger.”
Th is year’s federal election is currently scheduled for October 19, but the government may call an election at any time before this date. update

32
Your PensionSECURING YOUR FUTURE
ciary for a set period, or it may pay a lump sum payment to your estate.
To increase your pension, you can increase your sal-ary and/or your pensionable service.
Your Member Benefit Statement also notes your pensionable earnings (Section 5) and your pensionable ser-vice for the previous calendar year (Section 4). If you want to review your pensionable service history or estimate what your pension might be, based on your current personal information, you can access the “My Account” page on the BC Pension Corporation website and use the General Pension Estimator tool.
Not all earnings are pension-able. For example, straight time earnings are pensionable, but overtime is not.
If you’re a member of the MPP and the PSPP and work for more than one employer, you will contribute on all earn-
ANSWERS TO YOUR PENSION QUESTIONS
ings but will not accrue more than 12 months of pensionable service in one year. However, the total salary will be used to calculate your five year highest average salary.
Why does my Member Benefit Statement show
less than 12 months of pensionable service when I work full time and never take unpaid leaves?
If you work the full number of shifts assigned
to you in a year, or contribute for the first 20 unpaid leave days (150 hours), your pensionable service should be 12 months if you are full time.
There are legitimate rea-sons why you may be short pensionable service such as: you took more hours off than what was in your bank (such as vacation or sick leave bank); you swapped shifts and didn’t complete the swap; you really did take an unpaid leave; or you had a change in rotation
mid-year and lost time. The fact that you are paid in January for shifts worked in the previous year should not result in a shortfall in service.
If you feel that your pension-able service is not reported cor-rectly, contact your employer. If you disagree with the report from your employer, contact your steward for assistance.
I take time off without pay (Leaves of Absence – LOA)
during the year. Can I contrib-ute to my pension when I am on an LOA and is my employer required to contribute?
Article 37 of the Provincial Collective
Agreement (Leave – General), or Article 34 (Leave – Unpaid) under the Facilities Collective Agreement, requires employers to continue paying pension contributions for the first 20 days (150 hours) of an unpaid leave of absence provided you continue to pay your contribu-tions. The 20 days is pro-rated for part-time employees.
If you don’t continue your contributions, the employer isn’t required to pay their portion.
If I take an LOA, must I inform my employer in
writing that I wish to continue paying my portion of pension contributions?
Yes, you must advise the employer you wish to
continue your pension contri-butions with each unpaid LOA. Before leaving, complete a purchase of service application form and submit it to your employer.
If you’ve been working in BC’s public health care and social services system (health authorities and affiliates, and community social service agencies) chances are you’re part of the Municipal Pension Plan (MPP) or the Public Service Pension Plan (PSPP).
Even if retirement is the furthest thing from your mind, it’s a good idea to have an understanding of how your pension plan works, and make sure you are getting the most of this important benefit.
Here are the answers to some of our members’ most frequently asked questions about the MPP and PSPP, the two plans to which most BCNU members belong.
How is my retirement benefit calculated and how
do I know how much I will receive when I retire?
Your actual pension benefit at retirement is
not based on contributions. It is based on a formula that takes into consideration your age and your spouse’s age (if any) at retirement, your Highest Average Salary (HAS), your years of pensionable service and the pension option you choose at retirement.
Section 2 of your Member Benefit Statement provides an estimate of your monthly pen-sion benefit at retirement.
Once you become vested – after two years of contributory service – the plan will give you a lifetime pension, starting when you retire. After your death, depending on what kind of pension option you chose, the plan may continue to pay pension benefits to your spouse (if you have one) for his or her life time or to another benefi-
UPDATE MAGAZINE May/June 2015 33
Keep a copy of the purchase of service application form for your records.
For any unpaid leaves over 20 days, you must apply for a purchase of service if you want to include them in your years of pensionable service. Your employer is not required to pay a portion of the purchase cost.
I work part time at one facility and started casual
in another. Do I have to contribute to the pension plan as a casual?
If you are a member of the Municipal
Pension Plan with one employer and start working with another employer, the second employer must enroll you in the Plan at the date of hire.
I am quitt ing my job and starting to work with
another employer who off ers the MPP. Do I have to wait another three months to be eligible for enrolment if I take a regular job or meet the criteria again if I take a casual position?
No. As long as you are hired within 30 days from
your termination date, your new employer must enrol you in the plan as a new regular or casual employee.
I belong to the MPP now and want to take a casual
job with another plan employer. What happens to my pension at the second employer?
As you are already a contributing member of
the Municipal Pension Plan, your new employer is required to enrol you in the Plan immediately.
I plan to quit my job and get a job with another Plan
employer. What happens to my pension?
Your contributions remain in the plan. Under
the MPP, if you get a job with another plan employer within 30 calendar days, your employer is required to enrol you in the Plan immediately. Under the PSPP, if you get a job with another plan employer and kept your seniority rights, you will be enrolled immediately.
If you don’t get a job with another Plan you’ll be provided with a number of options. You can always keep your funds in
the plan and apply for a pen-sion later on.
Can I defer my pension?
Yes. If you termi-nate employment
prior to being able to start your pension, you can defer the benefi t until a later
date. For example, if you terminate employ-
ment at age 50, you can leave your funds in the plan
and begin to draw your pension as early as age 55.
I chose a Single Life Pension, guaranteed for 15
years and have a dependent child that is on my Post Retirement Group Benefi ts. What happens to the benefi ts if I die prior to the guarantee period?
Your dependent can remain covered by
PRGBs until the end of the guarantee period only. If your benefi ciary is not listed as a dependent with benefi t coverage, they will not be able to enrol.
What is the Retiree Benefi t Program and how do I
apply?Th e RBP is for members who belonged to the
Nurses’ Bargaining Association (NBA) collective agreement at the time of their retirement.
Since 2009, the program has reimbursed up to 50 percent of the MSP premiums that pen-sion plan retirees pay for this benefi t. Twice yearly, enrolled program members receive a cheque from BCNU which refl ects 50 percent of out-of-pocket costs of MSP premiums that are no longer covered by public pension plans. Th is amount is adjusted yearly based on the MSP monthly premiums.
Eventually, the union hopes to negotiate all BCNU mem-bers into this program.
For more information on eli-gibility and how to apply, email retireebenefi [email protected] or phone 604-433-2268 (toll free 1-800-663-9991). update
contribute to the pension plan as a casual?
If you are a member of the Municipal
Pension Plan with one employer and start working with another employer, the second employer must enroll you in the Plan at the date of hire.
casual employee. get a job with another Plan employer. What happens to my pension?
Your contributions remain in the plan. Under
the MPP, if you get a job with another plan employer within 30 calendar days, your employer is required to enrol you in the Plan immediately. Under the PSPP, if you get a job with another plan employer and kept your seniority rights, you will be enrolled immediately.
If you don’t get a job with another Plan you’ll be provided with a number of options. You can always keep your funds in
the plan and apply for a pen-sion later on.
Can I defer my pension?
prior to being able to start your pension, you can defer the benefi t until a later
date. For example, if you terminate employ-
ment at age 50, you can leave your funds in the plan

34
PRFsIN THE WORKPLACE
PRFS WORK Campbell River Hospital stewards Nancy Boulet and Devon Hilsden say a strong focus on patient safety has led to a healthy working relationship with managers.
JOINT EFFORT NURSES AND MANAGERS AT CAMPBELL RIVER HOSPITAL ARE IMPROVING HEALTH CARE BY BUILDING RELATIONSHIPS IN THE PRF PROCESS
ing a strong working relation-ship with hospital management. “Management is eager to hear nurses’ feedback because we all want the best patient outcomes and higher patient safety,” says Hilsden. “Th ey take the PRF process seriously and we all want to make this a good workplace.”
“When just one nurse fi lls out a PRF it can encourage others to do the same – then issues get identifi ed and resolved, and people learn that PRFs are not a punitive process,” explains Boulet. “Solving PRFs locally avoids escalating workplace
problems to the Senior Review Committ ee.”
Hilsden, an LPN, says that the PRF process was unfamiliar to her and her colleagues before they joined BCNU. However, she soon became an advocate of the PRFs when she learned how eff ective they could be. “I had to encourage my colleagues at fi rst,” she says. “But early successes impacted them and helped them trust the process.”
One of those early PRF successes was the creation of a checklist for patients admitt ed to the transitional care unit that helped defi ne which patients were suitable for the hospital’s LPN and care aide unit. “Th e checklist keeps patients safe, avoids risks to LPNs’ licences and teaches others about LPNs’ scope of practice,” says Hilsden.
Th e CRH nurses are also proud of another PRF suc-cess that improved everyone’s safety almost overnight. “We’re a small hospital with only one secure ER room,” says Boulet. “One weekend we were very short-staff ed and aft er a safety incident we discovered that security guards could be called in to help. Now, calling them is a standard practice at the hospital.”
To keep the process on track Hilsden supports all LPNs who fi ll out PRFs. “I’m there to help my peers when they need it,” she says. “Before LPNs joined BCNU I was hesitant to get involved with my union. But when LPNs moved to the
CAMPBELL RIVER HOSPITAL nurses have successfully used the Professional Responsibility Form process to improve staff and patient safety and build solution-focused relationships.
BCNU members’ PRFs are even informing safety and design decisions for the new 95-bed hospital that is being constructed in the city. Th is level of collaboration turns the process into a gold mine of both clinical and process information.
Nancy Boulet and Devon Hilsden are nurses and BCNU stewards at CRH who are build-

UPDATE MAGAZINE May/June 2015 35
nurses’ union I became a steward and I’m enjoy-ing the experience. It’s so important for our union to support LPNs’ practice issues, and now that we’re in BCNU we should use that support.”
The steward team at CRH discusses PRFs regularly. BCNU stewards, clinical coordinators and the site director all attend PRF Committee meetings where discussions are structured to reduce stress. “The director thanks each nurse who fills out a PRF and that makes people feel comfortable and supported instead of nervous,” says Hilsden.
The stewards keep detailed information about all PRFs, and the data is shared with the facil-ity director who uses the information to make good decisions for nurses and patients.
Boulet and Hilsden say it’s a joint effort to find solutions in PRF meetings. Patient safety is always at the front of everyone’s mind. And when management really hears workload or staffing concerns it’s a win-win for everyone.
“Patient safety is the reason for every PRF that nurses have submitted,” says Boulet. “When we’re over census or the flu hits then PRFs come in fast and reflect those critical situations. The collabora-tive approach we have with management means nurses feel they have a voice and aren’t just numbers in the system.”
For years Boulet didn’t know a lot about the RN contract or her union. “I’ve worked at CRH for 28 years now and I’m in my 35th year of nursing,” she says. “After 25 years of nursing, I took a keener interest in BCNU because I wanted the contract followed and nurses treated fairly. I like it when nurses have a say in things and the PRF process gives them a structured way to do that and to protect their licence.”
Hilsden says that Boulet has been her mentor and go-to person for any PRF questions. “We remind members who approach us that they’re not alone – we take calls 24-7 and are always there for our members.” update
MANY PROFESSIONAL concerns that members address using the PRF process are resolved at the local level. This is a good thing – and it shows that PRFs can be an effective tool to address patient care and other practice issues.
But if nurses and managers are unable to f ind a solution, a PRF can be forwarded to the Senior Review Committee (SRC) for a f inal recommendation. The SRC was created in 2012 and hears presentations at worksites province-wide. This joint commit-tee’s goal is to f ind solutions that are unanimous and binding.
BCNU Pacific Rim region’s Rachel Kimler is one of the union’s representatives on the SRC. While relatively new to the role, she’s been involved with PRFs for many years as a worksite steward at Cowichan District Hospital in Duncan.
The SRC consists of one union and one employer rep: it’s either Kimler or BCNU West Kootenay region’s Paul Moffat, and the chief nursing officer of the health authority for the worksite in question.
BCNU professional advocacy off icers on staff provide Kimler or Moffat with the background and history of a unit before they meet with members. The BCNU reps use this information to help members prepare a presentation
that they will make to the SRC. “I’ll go to the nurses’ work-
site and spend a few hours with them. Basically, I’m making sure I have clarity and that I have a full appreciation of the issues they’re dealing with,” explains Kimler.
She says the SRC is also benefi-cial for health authority managers who may not have a full apprecia-tion of the workplace issues from the distance of their offices.
“When the chief nursing offi-cers are hearing nurses’ pre-sentations, they’re hearing from the frontline workers how these issues are impacting them on a daily basis,” says Kimler. “And I think it can really hit a nerve with them.”
After hearing from nurses first-hand, the SRC meets and aims to find mutual ground for a recom-mendation that, if unanimous, becomes binding. “There’s a lot of push to find that mutual ground,” says Kimler. “Binding recom-mendations have a lot more teeth because the union signs off on it and so does the employer – so in many respects it’s very much like contract negotiations, but at a much more local level.”
The SRC plays an important role that Kimler is proud to be a part of. “I see PRFs as a posi-tive way to engage nurses and to make positive workplace changes – the SRC is just the next level in that process.” update
FINDING SOLUTIONSSenior Review Committee is an important step in the PRF process
For more details on the PRF process and information on how to use PRFs at your worksite visit the BCNU website.
36
COASTAL MOUNTAINKath-Ann TerrettChairC [email protected]
EAST KOOTENAYLori PearsonChairC [email protected]
FRASER VALLEYKatherine HamiltonChairC [email protected]
NORTH EASTVeronica (Roni) LokkenChairC [email protected]
NORTH WESTSharon SpontonChairC [email protected]
OKANAGAN-SIMILKAMEENRhonda CroftChair C [email protected]
PACIFIC RIMJo SalkenChairC [email protected]
RIVALauren VandergrondenChairC [email protected]
SHAUGHNESSY HEIGHTSClaudette JutChairC [email protected]
SIMON FRASERLiz IlczaszynCo-chairC [email protected]
Debbie PiccoCo-chairC [email protected]
SOUTH FRASER VALLEYJonathan KarmazinukCo-chairC [email protected]
Michelle Sordal Co-chairC [email protected]
SOUTH ISLANDSAdriane GearCo-chairC [email protected]
Lynnda Smith Co-chairC [email protected]
THOMPSON NORTH OKANAGANTracy Quewezance Chair C 250-320-8064 [email protected] VANCOUVER METROMeghan FriesenChairC [email protected]
WEST KOOTENAYLorne Burkart ChairC [email protected]
CONTACT YOUR STEWARDS For all workplace concerns contact your steward. REGIONAL REPS If your steward can’t help, or for all regional matters, contact your regional rep. EXECUTIVE COMMITTEE For all provincial, national or union policy issues, contact your executive committee.
BCNU CAN. Here’s how you can get in touch with the right person to help you.
Who Can Help? BCNU IS HERE TO
SERVE MEMBERS
PRESIDENTGayle DuteilC [email protected]
VICE PRESIDENTChristine SorensenC [email protected]
TREASURERMabel TungC [email protected]
EXECUTIVE COUNCILLORDeb DucharmeC [email protected]
EXECUTIVE COUNCILLORDan MurphyC [email protected]
EXECUTIVE COUNCILLORVacant
EXECUTIVE COMMITTEE
REGIONAL REPS
CENTRAL VANCOUVER Judy McGrathCo-chairC [email protected]
Marlene GoertzenCo-chairC [email protected]

UPDATE MAGAZINE May/June 2015 37
WHEN MARLENE Goertzen decides she wants a challenge, she really knows how to choose them. Th e BCNU Central Vancouver region co-chair was at the forefront of the union’s historic organizing cam-paign that successfully allowed over 7,000 of the province’s licensed practical nurses to move from the Facilities Bargaining Association to BCNU in 2012. “I felt so strongly that nurses needed to be together,” she says.
Goertzen has learned a lot about nurses’ rights and benefi ts since becoming a BCNU activist. “Like a nurse looking aft er your patients, that’s how we look aft er our union members,” is how she describes her role as a regional chair.
“Before I became involved with BCNU I knew some parts of my contract, but not all of
BRINGING NURSES TOGETHER CENTRAL VANCOUVER CO-CHAIR MARLENE GOERTZEN
EMPOWERING MEMBERS “BCNU is there to help you be the best nurse you can be,” says Central Vancouver co-chair Marlene Goertzen.
QUICK FACTS NAME Marlene Goertzen.GRADUATED Vancouver Community College 2002. UNION POSITIONCentral Vancouver co-chair. WHY I SUPPORT BCNU? The union looks after members the way a nurse looks after their patients.
Council Profi leHERE’S WHO’S WORKING FOR YOU
it, and not in depth,” she says. “When I became a steward, I felt that members counted on me to know the contract. And I under-stand how they feel because I was in their place once, so now I’m here for them with the informa-tion they need.”
Goertzen says she wanted to continue her leadership role aft er the successful LPN campaign. “By the time we were part of BCNU, I felt I needed to see things through,” she explains. “We convinced a lot of LPNs that it was important to join BCNU, so I had to take responsibility for members that followed us.”
In 2012 Goertzen was elected as an LPN representative on BCNU Council, and she says it was natural progression to run for a regular Council position when her term expired last year.
Currently on leave from her
position at a Richmond long-term care facility, Goertzen fi rst completed her nursing education at the Vancouver Vocational Institute (the precursor to today’s Vancouver Community College (VCC)) in February 1977, and received her nursing upgrade certifi cate at VCC in 2002.
Aft er working in maternity, pediatrics, orthopaedic and medical-surgical wards, Goertzen says she found her “right place” working in palliative care.
Goertzen is a member of BCNU’s Bursary Committ ee, which provides funding for nurses who want to advance their education. She also sits on the Member Engagement, Steward Recruitment and Retention Committ ee, which works to ensure that future leaders are supported in their roles within their union.
Goertzen also sits on BCNU’s Bargaining Committ ee. As one of the LPN reps tasked with comparing both the Nurses’ Bargaining Association and Facilities Bargaining Association contracts line-by-line, her knowledge now informs BCNU’s provincial bargaining objectives.
“BCNU cares about health care and about nurses,” says Goertzen when asked about what keeps her motivated. “Th e union is there to help you be the best nurse you can be. It supports our education and our practice, and binds all nurses together with a common goal for health care in BC and in Canada,” she says. “I’m amazed to be given this opportunity and responsibility – and I’m using it to improve the lot of all nurses.” update

38 UPDATE MAGAZINE May/June 2015
MARATHON RUNNER RACHEL KIMLER IS FOCUSED ON HEALTH AND WELLNESS
Off DutyMEMBERS AFTER HOURS
WHEN MANY OF US HIT our mid-forties, we start to ease up on our fitness efforts. Our aching bodies usually tell us that it’s time to change our routines.
For Nanaimo’s Rachel Kimler, however, the transi-tion to middle-age became the motivation to ramp-up her exercise regime.
Five years ago, the Cowichan District Hospital nurse decided to complete a marathon. To tackle the goal, she started training for a half-marathon. It was difficult at first. “I would build up to the distance, and then get injured or sick,” she recalls. “I would be side-lined for a while and need to start all over again.” But eventually, her perseverance paid off.
In May 2010, Kimler crossed the finish line of her first half-marathon. “It was a feeling of relief and satisfaction,” she says “I knew that if I could accom-plish this, I could move forward with my ultimate goal of com-pleting a full marathon.”
Kimler completed several more half-marathons that year including an event in Las Vegas.
She says that training to run a marathon’s distance of 42.1 km requires her to run five days
a week. Often she will run by herself, but she also enjoys the company of her local running store club.
“Besides the safely factor of running with a group, the social element has been a big part of my life. When you’re running
with some of the same people for hours at a time, you forge some really strong bonds,” she says. “The running commu-nity is very supportive of one another.”
This fact was evident to Kimler during the 2013 Boston marathon. A major race that requires runners to qualify to participate, Kimler completed the infamously hard course just three minutes shy of her personal best time and was elated to be part of this incred-
ible marathon experience.
However, just as she and a fellow Nanaimo racer were collecting post-race cloth-ing they heard two large bangs that sounded like canons. Because Boston was celebrating Patriot’s Day, the noises didn’t alarm them. But moments later, chaos erupted with police run-ning in differ-ent directions, helicopters above and subways shut down. They, along with the rest of the world, soon discovered that bombs had been planted on
the route, killing three people and injuring an estimated 264 others.
After several heart-stopping hours, Kimler was re-united with her husband. She says the experience was surreal. People from her running community in Nanaimo were texting back and forth, fearing for their loved ones’ safety. Before the tragedy unfolded, Kimler had been impressed with the num-ber of Bostonians who came out to support the runners. And the way people responded in the wake of disaster has made her proud of the running community.
Despite her accomplish-ments, Kimler admits she can be unmotivated, and that without goal setting, she could easily slip into couch potato mode. She says that being surrounded by a fit healthy group of co-workers keeps her on track. “We are supportive of one another and have like-minded ideas on health and wellness.”
Kimler has now completed 10 half-marathons and five marathons including Boston and Chicago. So what’s next? In the running community there are six major events around the world that are thought to be the ultimate accomplishments in marathons. With Boston and Chicago under her belt, she says she has New York, London, Berlin and Tokyo to go. update
CROSSING THE FINISH LINE BCNU Pacific Rim region nurse Rachel Kimler says her community of marathon runners supports her in achieving her fitness goals.

NATIONAL ABORIGINAL DAYJUNE 21, 2015
BCNU A
boriginal Leadership Circle
PM 40834030
SAFETY & HEALTH WEEK
MAY 3–9, 2015
Delivering safe patient care means working in a safe and healthy environment.





























