Embed Size (px)
Citation preview
655 West 12th Avenue
Vancouver, BC V5Z 4R4
Tel 604.707.2400
Fax 604.707.2441
www.bccdc.ca
BC Influenza Prevention Policy: a discussion of the evidence
2013
2
B.C.’s Enhanced Influenza Protection Policy, 2013
Discussion of the evidence supporting the enhanced influenza protection policy
A. Background
Influenza can be a serious contagious disease spread by droplet transmission through close contact with an infected individual. According to the Public Health Agency of Canada, nationally there are between 2000 and 4000 deaths per year from influenza and its complications. Infected individuals are highly contagious and can transmit influenza for 24 hours before they are symptomatic. Among vaccine-preventable diseases, influenza causes by far the most deaths, outpacing all other vaccine preventable diseases combined. Hospitalized patients and residents of long term care are frequently more vulnerable to influenza than members of the general population. Influenza in vulnerable groups, especially the elderly, the very young and the immunosuppressed, is associated with significant morbidity and mortality; however, the influenza vaccine is less effective in preventing influenza in these same groups than it is in healthy people.
Healthcare workers have been implicated as the source of influenza infection in healthcare settings. Vaccination of healthcare workers will reduce their risk of getting influenza and spreading it to patients, other healthcare workers or their families. The most effective strategy for preventing influenza is annual vaccination. Influenza vaccine is safe and effective.
The wearing of masks can serve as a method of source control of infected healthcare workers who may have no symptoms. Masks may also protect unvaccinated healthcare workers from as yet unrecognized infected patients or visitors with influenza. Other infection control measures such as rapid identification of ill patients, hand hygiene, cough etiquette, restrictions on work and visiting, and the use of anti-viral medications all help, but vaccination remains the cornerstone of efforts to control influenza transmission.
In the face of this information, in 2012, British Columbia (BC) became the first province in Canada to implement a province-wide condition-of-service influenza prevention policy, including the requirement that health care workers (HCWs) either receive the seasonal influenza vaccine or wear a mask while in patient care areas for the duration of the influenza season. The decision was made by the Leadership Council of BC (which includes health authority CEOs and the Deputy Minister of Health) on the advice of the Provincial

3
Health Officer. The policy was disseminated widely and documents were developed to support managers and other leaders in implementation of the policy. During the implementation of the policy there were several issues that came up around evidence in the literature to support aspects of the policy. This paper addresses the most common issues that arose and reviews the evidence on each.
1. What is the burden of influenza morbidity and mortality in the community and in healthcare settings?
Influenza infection is common - depending on the year and on exposure risk (e.g. whether there are children in the family), between 3% and 30% of unvaccinated healthy adults develop influenza infection annually (1,2). Influenza virus is shed by persons before they develop symptoms of influenza, and by persons who are asymptomatically infected (3,4). Vaccination prevents approximately 60% of these infections (5). However, many different respiratory viruses can cause a range of infection from very mild (a runny nose for a few hours) to much more severe (high fever for days, and persistent cough with profound fatigue for weeks). In temperate climates, influenza is responsible for 20-35% of "influenza-like illness" in unvaccinated adults during an average winter influenza season (6,7). In Canada, the proportion of influenza-like illness that is due to influenza is highest during influenza season (a 10-16 week period that occurs at some time between November and April), intermediate during the winter, non-influenza season, and lowest during the summer (8).
An important difference between influenza and other viruses which cause upper respiratory tract infection is that influenza is more commonly associated with complications, most commonly secondary bacterial infection and exacerbations of underlying chronic heart and lung disease (1). These complications of influenza are what are primarily responsible for the mortality associated with influenza. Because of this, influenza is the most common infectious disease cause of death in North America, and is among the top 10 infectious disease causes of total burden of serious illness among Canadians (9).
Every year in BC we have outbreaks of influenza in healthcare settings; many of these are in long term care homes (LTC) where the resident population is particularly vulnerable. Public health and infection control programs in BC have focused much attention on reducing the risk in LTC by vaccinating residents, encouraging vaccination of healthcare workers and visitors and volunteers and developing strong protocols for early detection and response to outbreaks. Despite comprehensive, multifaceted programs to encourage HCW immunization in LTC, rates of immunization remain low, ranging between 49-68% from 2003/04 to 2011/12; far lower than the target of 80% coverage (10). Rates in residents in
4
LTC by contrast have been consistently high, ranging from 89-93% in the same timeframe. Every year we have experienced outbreaks in LTC that lead to severe illnesses and deaths in this most vulnerable population.
The impact of influenza on HCW and patients in hospitals and the transmission of influenza within a hospital are difficult to measure for a number of reasons. Patients in hospital are a much more transient population with median lengths of stay of 3-5 days in most hospitals Thus, patients exposed in the hospital may not develop symptoms until after their discharge; they may not be tested for influenza, and the source of their infection is likely to remain unrecognized. Longer stay patients may have underlying cardiorespiratory illness that make it difficult to identify the cause of worsening symptoms; and there are many potential causes of new fever and/or respiratory symptoms in hospitalized patients. Such patients are rarely tested for influenza or other respiratory viruses. Influenza is difficult to diagnose at admission in older, chronically ill adults, and unrecognized cases may also serve as potential sources of spread. Hospital (or nosocomial) outbreaks are not uncommon and may be substantially underreported (11). Having said that, the impact in hospitals from the outbreaks that have been reported in the literature is substantial. In a review of nosocomial influenza that included detailed review of 12 reported nosocomial influenza outbreaks, the length of the outbreak ranged from 2-69 days (median 7 days) and reported infection rates in patients ranged from 3-50% on the wards where the outbreak was detected and 0.7-20% in the entire hospital(15). The case fatality rate varies depending on the patient population affected, but average 16% in acute care hospitals – though they can be much higher in special populations such as transplant or ICU patients where the mortality can be 33-60% (12, 13).
There are many factors which affect how much impact influenza will have in any given season. One main factor is the circulating strain with influenza AH1N1 and B strains more likely to affect children and influenza A H3N2 having more severe effects on the elderly. In years when H3N2 is the predominant circulating strain of influenza, outbreaks in LTC and in elderly populations, both in the community and in hospital, can be particularly severe.
2. What is the mortality from influenza?
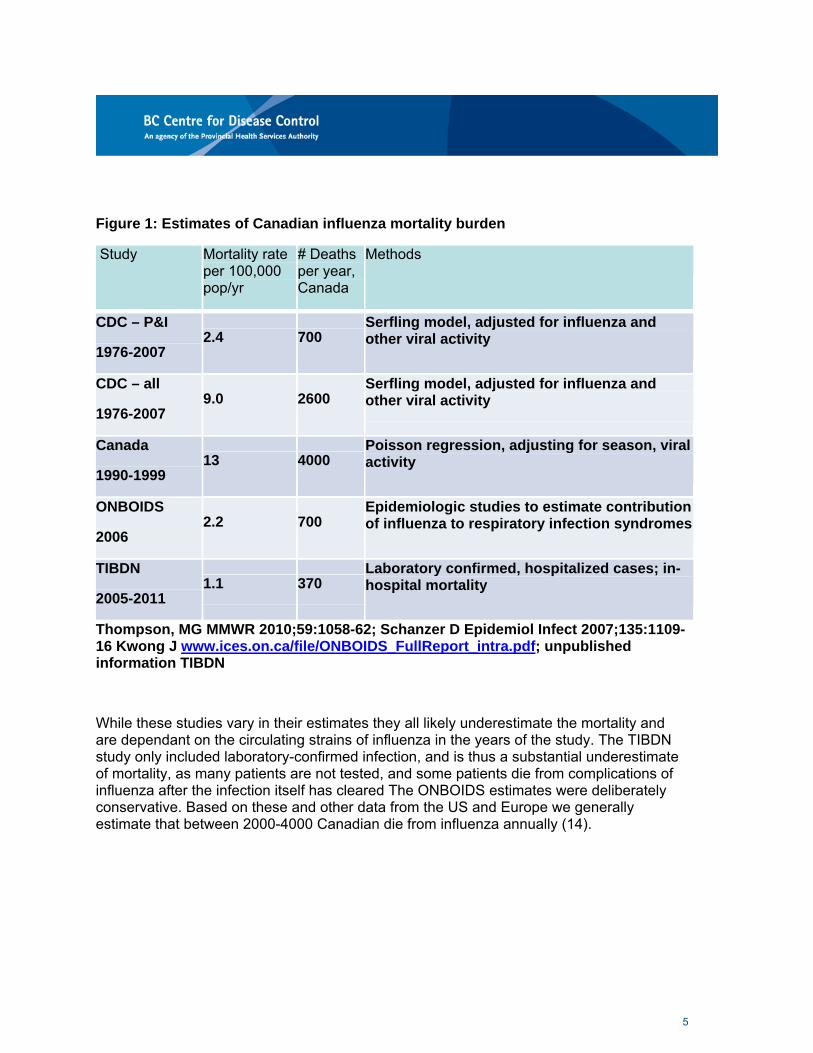
For some of the reasons described above, mortality is difficult to measure directly. Many people with influenza do not seek medical attention for their influenza illness, but may be admitted to hospital or have complications from the infection or from worsening of their underlying illness. Most of these people are not tested for influenza even though it may play an important contributing role in their illness. Several studies have estimated the mortality in Canada from influenza using a variety of methods (Figure 1).
5
Figure 1: Estimates of Canadian influenza mortality burden
Study Mortality rate per 100,000 pop/yr
# Deaths per year, Canada
Methods
CDC – P&I
1976-2007 2.4 700
Serfling model, adjusted for influenza and other viral activity
CDC – all
1976-2007 9.0 2600
Serfling model, adjusted for influenza and other viral activity
Canada
1990-1999 13 4000
Poisson regression, adjusting for season, viral activity
ONBOIDS
2006 2.2 700
Epidemiologic studies to estimate contribution of influenza to respiratory infection syndromes
TIBDN
2005-2011 1.1 370
Laboratory confirmed, hospitalized cases; in-hospital mortality
Thompson, MG MMWR 2010;59:1058-62; Schanzer D Epidemiol Infect 2007;135:1109-16 Kwong J www.ices.on.ca/file/ONBOIDS_FullReport_intra.pdf; unpublished information TIBDN
While these studies vary in their estimates they all likely underestimate the mortality and are dependant on the circulating strains of influenza in the years of the study. The TIBDN study only included laboratory-confirmed infection, and is thus a substantial underestimate of mortality, as many patients are not tested, and some patients die from complications of influenza after the infection itself has cleared The ONBOIDS estimates were deliberately conservative. Based on these and other data from the US and Europe we generally estimate that between 2000-4000 Canadian die from influenza annually (14).
6
3. What is the evidence that vaccinating healthcare workers protects patients? What about the Cochrane review that concludes there is no benefit to patients in long term care?
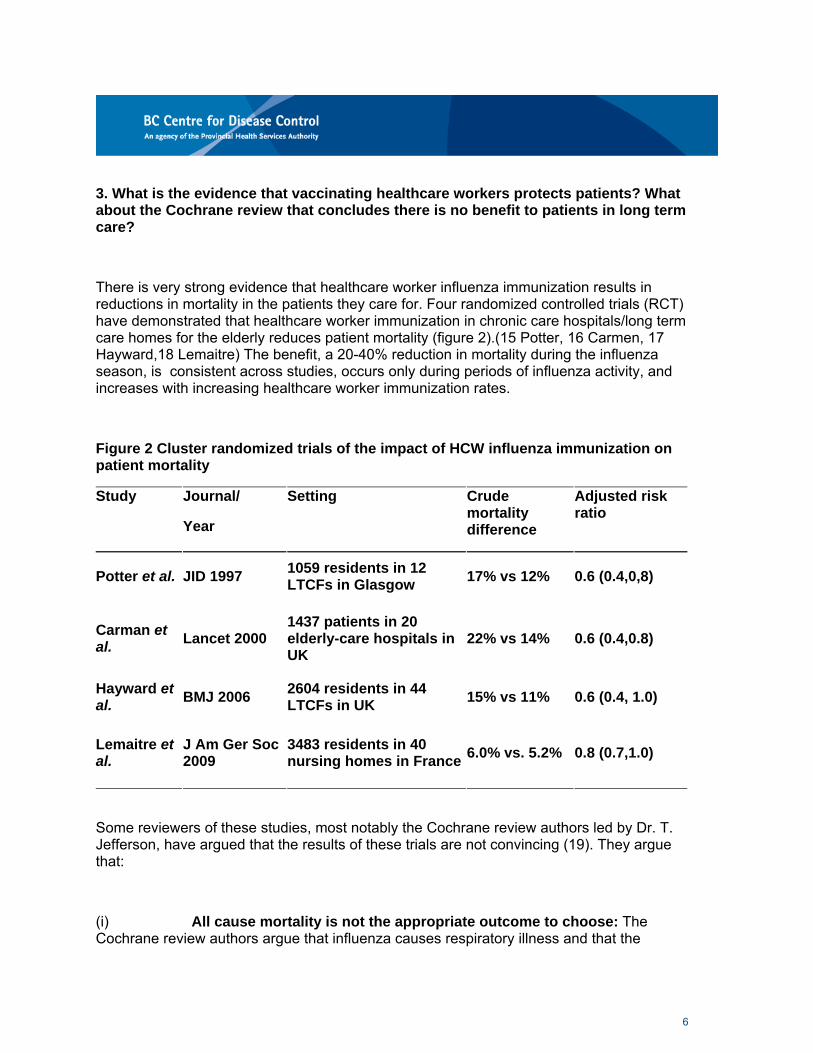
There is very strong evidence that healthcare worker influenza immunization results in reductions in mortality in the patients they care for. Four randomized controlled trials (RCT) have demonstrated that healthcare worker immunization in chronic care hospitals/long term care homes for the elderly reduces patient mortality (figure 2).(15 Potter, 16 Carmen, 17 Hayward,18 Lemaitre) The benefit, a 20-40% reduction in mortality during the influenza season, is consistent across studies, occurs only during periods of influenza activity, and increases with increasing healthcare worker immunization rates.
Figure 2 Cluster randomized trials of the impact of HCW influenza immunization on patient mortality
Study Journal/
Year
Setting Crude mortality difference
Adjusted risk ratio
Potter et al. JID 1997 1059 residents in 12 LTCFs in Glasgow
17% vs 12% 0.6 (0.4,0,8)
Carman et al.
Lancet 2000 1437 patients in 20 elderly-care hospitals in UK
22% vs 14% 0.6 (0.4,0.8)
Hayward et al.
BMJ 2006 2604 residents in 44 LTCFs in UK
15% vs 11% 0.6 (0.4, 1.0)
Lemaitre et al.
J Am Ger Soc 2009
3483 residents in 40 nursing homes in France
6.0% vs. 5.2% 0.8 (0.7,1.0)
Some reviewers of these studies, most notably the Cochrane review authors led by Dr. T. Jefferson, have argued that the results of these trials are not convincing (19). They argue that:
(i) All cause mortality is not the appropriate outcome to choose: The Cochrane review authors argue that influenza causes respiratory illness and that the

7
outcome should be some form of respiratory illness. In clinical trials, all cause mortality is always the most important outcome (20) -- what is most clinically relevant is whether patients are alive at the end of a study. Survival/mortality is also the best outcome to measure, because the measurement is much less likely to be subject to bias than measurement for other outcomes and will almost always be unaffected by whether assessors are blind to the intervention. The reason that all cause mortality is rarely used as an outcome is that clinical trials almost always have to be very large (and thus very expensive) when this outcome is chosen. Thus, we use "intermediate measures" which permit greater efficiency in trial design. In this particular circumstance, when the original RCT (Potter et al.) demonstrated an effect on resident all cause mortality during influenza season with an achievable sample size, all cause mortality was clearly most appropriate primary outcome for later studies.
(ii) The effect size is too large: it is not possible that preventing influenza would result in this reduction in all cause mortality. It is true that a part of the reason why we have four randomized controlled trials of this intervention, when we would normally believe evidence and change practice after one or two RCTs, is because the effect size is larger than almost all clinicians and scientists thought it would be. The UK Health Protection Agency specifically commissioned Dr. Hayward's study to conclusively demonstrate whether the effect measured in the previous two RCTs was real, because it seemed to large to be true. However, as noted above, the effect that has been measured is consistent across trials. In Carman et al.'s study, the degree of protection was shown to increase as vaccination increased, and in Hayward et al.'s study, the protection could only be measured during influenza season, and in the year when there was substantial influenza activity. In addition, in looking at the studies, the absolute decrease in mortality is greatest in the study populations with the highest baseline mortality. The consistent, reproducible and large effect seen in these randomized controlled trials support the effectiveness of influenza vaccination against mortality.
There are no data on the incidence of influenza infection or the case fatality rate in these vulnerable populations; based on other data and expert opinion we would expect that about 1.3% of vaccinated nursing home residents in Canada would die each year of influenza (an incidence of infection of 16% and a 8% case fatality rate) (2,21-24), such that if increasing the vaccination rate of HCWs by 40% prevented 60% of deaths, the reduction in absolute mortality would be about 0.8%. This is almost exactly what was measured in the study of Lemaitre et al. in a similar population (18). In more vulnerable populations, the effect size would be even larger, such as in the British studies in which the population had higher baseline mortality rates (15-17).
8
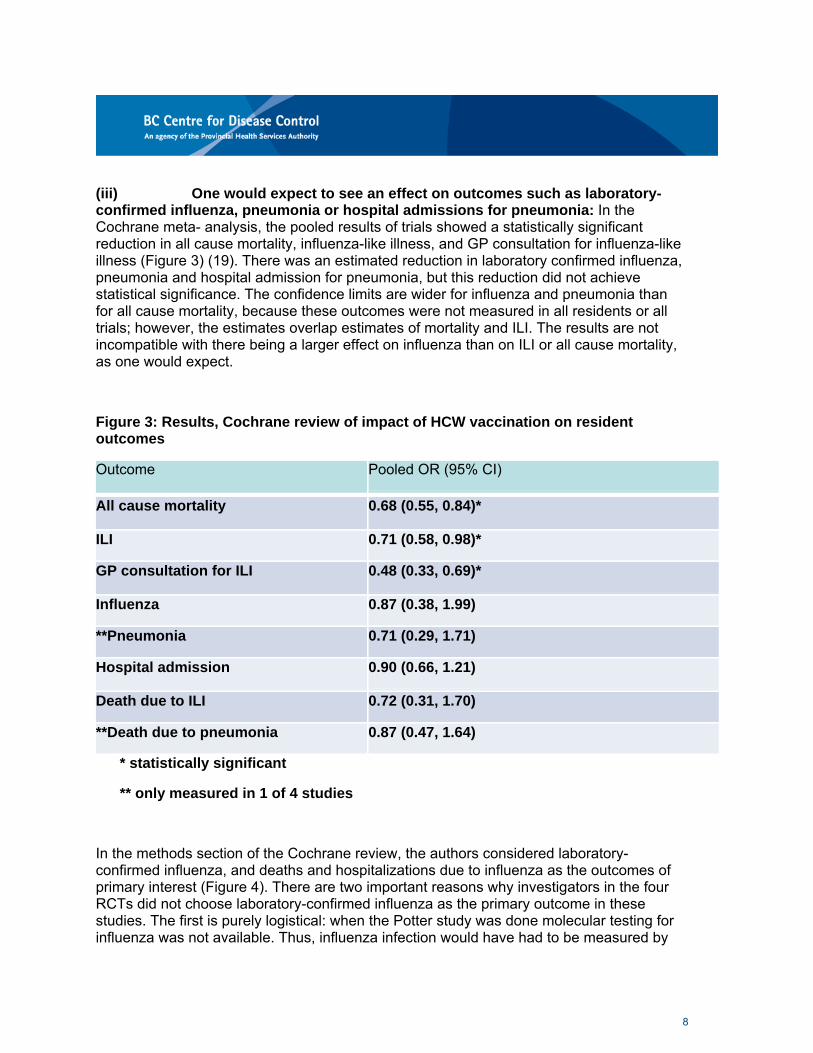
(iii) One would expect to see an effect on outcomes such as laboratory-confirmed influenza, pneumonia or hospital admissions for pneumonia: In the Cochrane meta- analysis, the pooled results of trials showed a statistically significant reduction in all cause mortality, influenza-like illness, and GP consultation for influenza-like illness (Figure 3) (19). There was an estimated reduction in laboratory confirmed influenza, pneumonia and hospital admission for pneumonia, but this reduction did not achieve statistical significance. The confidence limits are wider for influenza and pneumonia than for all cause mortality, because these outcomes were not measured in all residents or all trials; however, the estimates overlap estimates of mortality and ILI. The results are not incompatible with there being a larger effect on influenza than on ILI or all cause mortality, as one would expect.
Figure 3: Results, Cochrane review of impact of HCW vaccination on resident outcomes
Outcome Pooled OR (95% CI)
All cause mortality 0.68 (0.55, 0.84)*
ILI 0.71 (0.58, 0.98)*
GP consultation for ILI 0.48 (0.33, 0.69)*
Influenza 0.87 (0.38, 1.99)
**Pneumonia 0.71 (0.29, 1.71)
Hospital admission 0.90 (0.66, 1.21)
Death due to ILI 0.72 (0.31, 1.70)
**Death due to pneumonia 0.87 (0.47, 1.64)
* statistically significant
** only measured in 1 of 4 studies
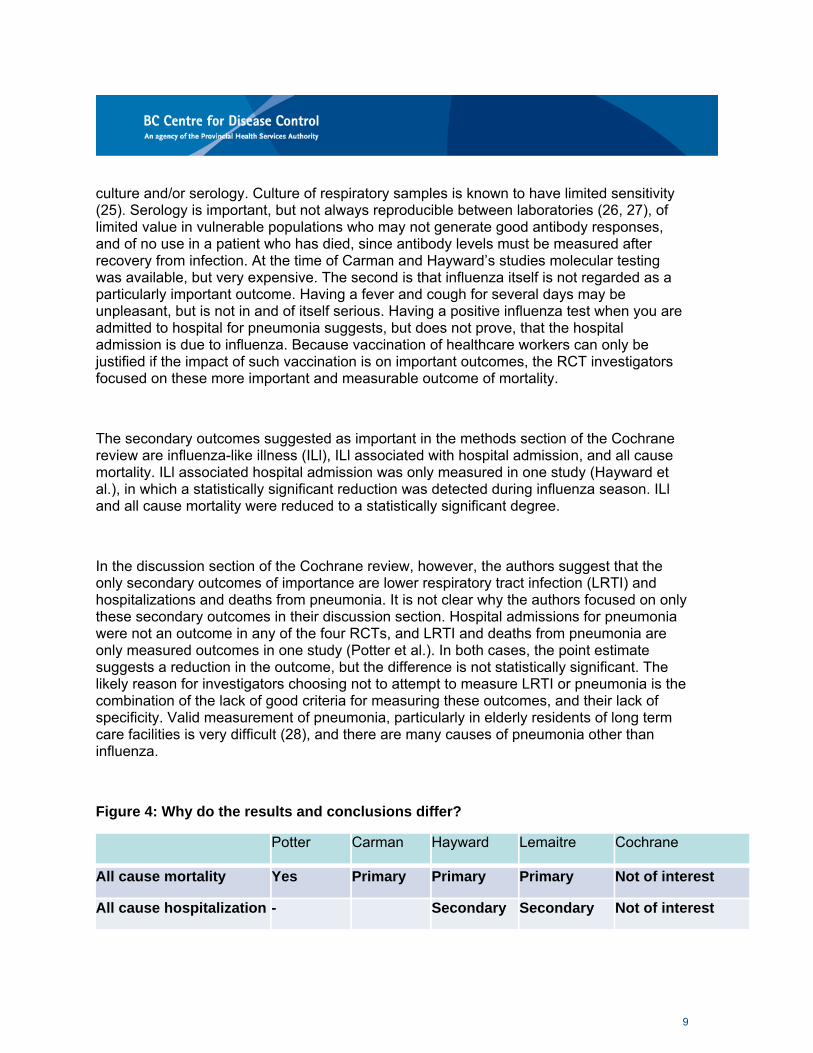
In the methods section of the Cochrane review, the authors considered laboratory-confirmed influenza, and deaths and hospitalizations due to influenza as the outcomes of primary interest (Figure 4). There are two important reasons why investigators in the four RCTs did not choose laboratory-confirmed influenza as the primary outcome in these studies. The first is purely logistical: when the Potter study was done molecular testing for influenza was not available. Thus, influenza infection would have had to be measured by
9
culture and/or serology. Culture of respiratory samples is known to have limited sensitivity (25). Serology is important, but not always reproducible between laboratories (26, 27), of limited value in vulnerable populations who may not generate good antibody responses, and of no use in a patient who has died, since antibody levels must be measured after recovery from infection. At the time of Carman and Hayward’s studies molecular testing was available, but very expensive. The second is that influenza itself is not regarded as a particularly important outcome. Having a fever and cough for several days may be unpleasant, but is not in and of itself serious. Having a positive influenza test when you are admitted to hospital for pneumonia suggests, but does not prove, that the hospital admission is due to influenza. Because vaccination of healthcare workers can only be justified if the impact of such vaccination is on important outcomes, the RCT investigators focused on these more important and measurable outcome of mortality.
The secondary outcomes suggested as important in the methods section of the Cochrane review are influenza-like illness (ILl), ILl associated with hospital admission, and all cause mortality. ILl associated hospital admission was only measured in one study (Hayward et al.), in which a statistically significant reduction was detected during influenza season. ILl and all cause mortality were reduced to a statistically significant degree.
In the discussion section of the Cochrane review, however, the authors suggest that the only secondary outcomes of importance are lower respiratory tract infection (LRTI) and hospitalizations and deaths from pneumonia. It is not clear why the authors focused on only these secondary outcomes in their discussion section. Hospital admissions for pneumonia were not an outcome in any of the four RCTs, and LRTI and deaths from pneumonia are only measured outcomes in one study (Potter et al.). In both cases, the point estimate suggests a reduction in the outcome, but the difference is not statistically significant. The likely reason for investigators choosing not to attempt to measure LRTI or pneumonia is the combination of the lack of good criteria for measuring these outcomes, and their lack of specificity. Valid measurement of pneumonia, particularly in elderly residents of long term care facilities is very difficult (28), and there are many causes of pneumonia other than influenza.
Figure 4: Why do the results and conclusions differ?
Potter Carman Hayward Lemaitre Cochrane
All cause mortality Yes Primary Primary Primary Not of interest
All cause hospitalization - Secondary Secondary Not of interest
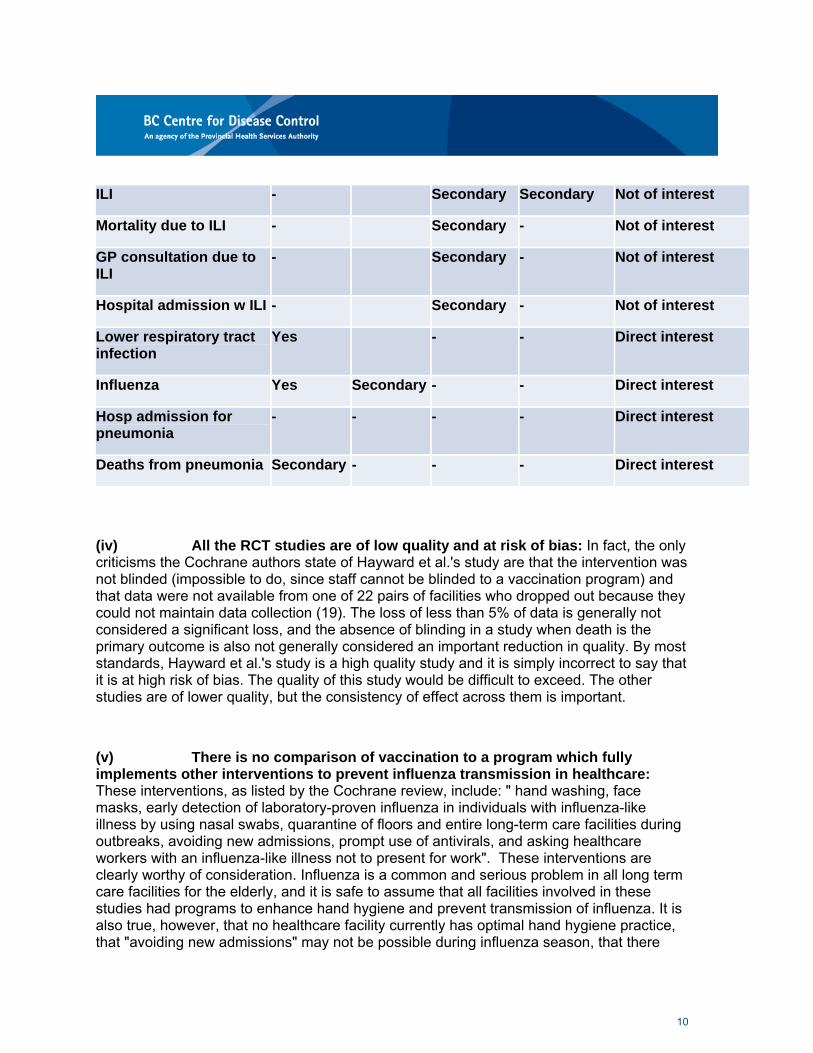
10
ILI - Secondary Secondary Not of interest
Mortality due to ILI - Secondary - Not of interest
GP consultation due to ILI
- Secondary - Not of interest
Hospital admission w ILI - Secondary - Not of interest
Lower respiratory tract infection
Yes - - Direct interest
Influenza Yes Secondary - - Direct interest
Hosp admission for pneumonia
- - - - Direct interest
Deaths from pneumonia Secondary - - - Direct interest
(iv) All the RCT studies are of low quality and at risk of bias: In fact, the only criticisms the Cochrane authors state of Hayward et al.'s study are that the intervention was not blinded (impossible to do, since staff cannot be blinded to a vaccination program) and that data were not available from one of 22 pairs of facilities who dropped out because they could not maintain data collection (19). The loss of less than 5% of data is generally not considered a significant loss, and the absence of blinding in a study when death is the primary outcome is also not generally considered an important reduction in quality. By most standards, Hayward et al.'s study is a high quality study and it is simply incorrect to say that it is at high risk of bias. The quality of this study would be difficult to exceed. The other studies are of lower quality, but the consistency of effect across them is important.
(v) There is no comparison of vaccination to a program which fully implements other interventions to prevent influenza transmission in healthcare: These interventions, as listed by the Cochrane review, include: " hand washing, face masks, early detection of laboratory-proven influenza in individuals with influenza-like illness by using nasal swabs, quarantine of floors and entire long-term care facilities during outbreaks, avoiding new admissions, prompt use of antivirals, and asking healthcare workers with an influenza-like illness not to present for work". These interventions are clearly worthy of consideration. Influenza is a common and serious problem in all long term care facilities for the elderly, and it is safe to assume that all facilities involved in these studies had programs to enhance hand hygiene and prevent transmission of influenza. It is also true, however, that no healthcare facility currently has optimal hand hygiene practice, that "avoiding new admissions" may not be possible during influenza season, that there

11
continue to be uncertainties about the best use of antivirals, and that HCWs are known to work when ill regularly, and despite policies that suggest that they should not (29, 30, 31). It is also true that, despite systematic implementation (and regulation) of programs with these elements to prevent influenza in BC and other Canadian long term care facilities for at least the last two decades, and >90% influenza vaccination rates in residents, influenza outbreaks and sporadic cases of influenza continue to cause significant morbidity and mortality in residents (32, 33, 34). It is most likely that, because of the limitations associated with both these methods of protection and vaccination, we will only achieve best protection of patients if both vaccination and all of these other interventions are implemented as effectively as possible.
In September 2013, an additional systematic review of the evidence was published by Ahmed et al (35). They identified four cluster randomized trials and four observational trials conducted in long-term care or hospital settings, including the four RCTs reviewed in Cochrane. In their meta-analysis pooled risk ratios for all-cause mortality were 0.71 (95% CI: 0.59, 0.85) and for influenza-like-illness 0.58 (95% CI: 0.46, 0.73). They used GRADE methodology to evaluate the quality of the evidence and rated it as moderate for the overall effect of HCP vaccination on mortality and morbidity in patients. Their conclusions were that HCW influenza vaccination can enhance patient safety. An accompanying editorial (36) reviews the differences between the Cochrane review and the Ahmed review including the issue of delay in mortality post influenza infection and the difficulty in using laboratory confirmed influenza because of laboratory methods that were insensitive in older patients or the lack of laboratory testing in the studies reviewed. The editorial concludes that “given the dire consequences that outbreaks can have in institutional settings, the known safety and efficacy of current vaccines, and the strong evidence that vaccinating a segment of the population can protect unvaccinated persons who are in contact with the vaccinees, the meta-analysis by Ahmed et al. offers additional reassurance that the threshold for action has been reached or surpassed”.
Thus, careful review of the data from these RCTs, and review of the criticisms that have been advanced, results in a clear conclusion that increasing vaccination rates in healthcare workers results in reduced all cause mortality during influenza season. In addition to the data from these RCTs, observational studies have found that the risk of influenza and influenza outbreaks decreases as the immunization rate of staff increases.(37, 38) Additional evidence of protection of close contacts by vaccinating people against influenza is found in studies of school-based vaccination programs (39, 40), in a randomized controlled trial of vaccination of children in Hutterite communities (41), which demonstrated that vaccination of 83% of 3-15 year olds in intervention communities, not only protected the vaccinated children but also reduced confirmed influenza by 61% in non-vaccinated community members, and in an ecologic study of school-based influenza vaccination programs in Japan (42).

12
In sum, there is no question that influenza vaccination of healthcare workers providing care for residents/patients in long term care protects residents from significant morbidity and mortality. This reduction is achieved by preventing the introduction of influenza into these facilities by staff, and by reducing the risk of transmission of influenza among staff and between staff and patients.
5. These studies have been in long-term care facilities. What about in acute care and community care setting?
The relevant differences between acute/community care settings and long term care facilities for the elderly are that some patients may not be as compromised as long term care facility residents, and that they may be more likely to have exposures to influenza external to patient care. However, the biologic rationale for healthcare worker immunization does not vary from one healthcare setting to another and many patients in acute care hospitals and in the community are as vulnerable, if not more vulnerable, as those in long term care. There is evidence in acute care hospitals that transmission of influenza occurs between and among patients and healthcare workers, and that vaccination of staff protects patients from hospital-acquired pneumonia. Influenza outbreaks in acute care are common, and healthcare worker attack rates mirror and sometimes exceed patient attack rates in these outbreaks.(11,43-54) Two observational cohort studies have found that lower healthcare worker immunization rates were associated with higher rates of laboratory-confirmed hospital acquired influenza (55,56), and transmission of influenza-like illness among and between healthcare workers and patients in acute care hospitals was common (57). Not included in the reviews above is a recent cluster-randomized trial in the Netherlands that showed increased healthcare provider influenza immunization was associated with decreased influenza and/or pneumonia in hospital patients (58).
There is no question that vaccination of health care workers will prevent transmission of influenza from them to the patients they care for, whatever the setting. Because of the potential for other exposures to influenza in patients in the community, the protection afforded by vaccinating health care providers in community and acute care hospital settings is likely less than that provided by vaccinating health care providers in residential long term care. However, the effect size in residential long term care is so large that it is very likely the benefit in all settings is clinically significant.
4. How effective is the current vaccine at preventing influenza? What about reports that it is not sufficiently effective to make it ‘mandatory’ for HCW?

13
The degree to which influenza immunization protects people depends very much on the age and immune status of the recipient although in all cases the vaccine provides better protection from infection and leads to less severe illness in those vaccinated than those who are not vaccinated. Many studies have shown that those for whom the vaccine is recommended (people over age 65, adults and children with chronic medical conditions, infants) are the very populations in whom the vaccine is less effective. On the other hand, the effectiveness in healthy adults generally ranges from 60-90% depending on the match with the circulating strains (59). This commonly quoted range comes primarily from a Cochrane review (this is a separate Cochrane review from the one which reviewed the evidence on HCW immunization referenced above but was conducted by the same group) estimate of trivalent inactivated vaccine (TIV) efficacy in healthy adults when the vaccine strain matched the circulating strains and circulation was high, as quoted in the Canadian National Advisory Committee on Immunization Statement on Seasonal Influenza Vaccine for 2012-2013 (59, 60). The overall estimate of trivalent inactivated influenza vaccine efficacy -- averaged over all seasons and all strains of influenza -- from this Cochrane review is 70% (95% confidence interval: 56%-80%) (60).
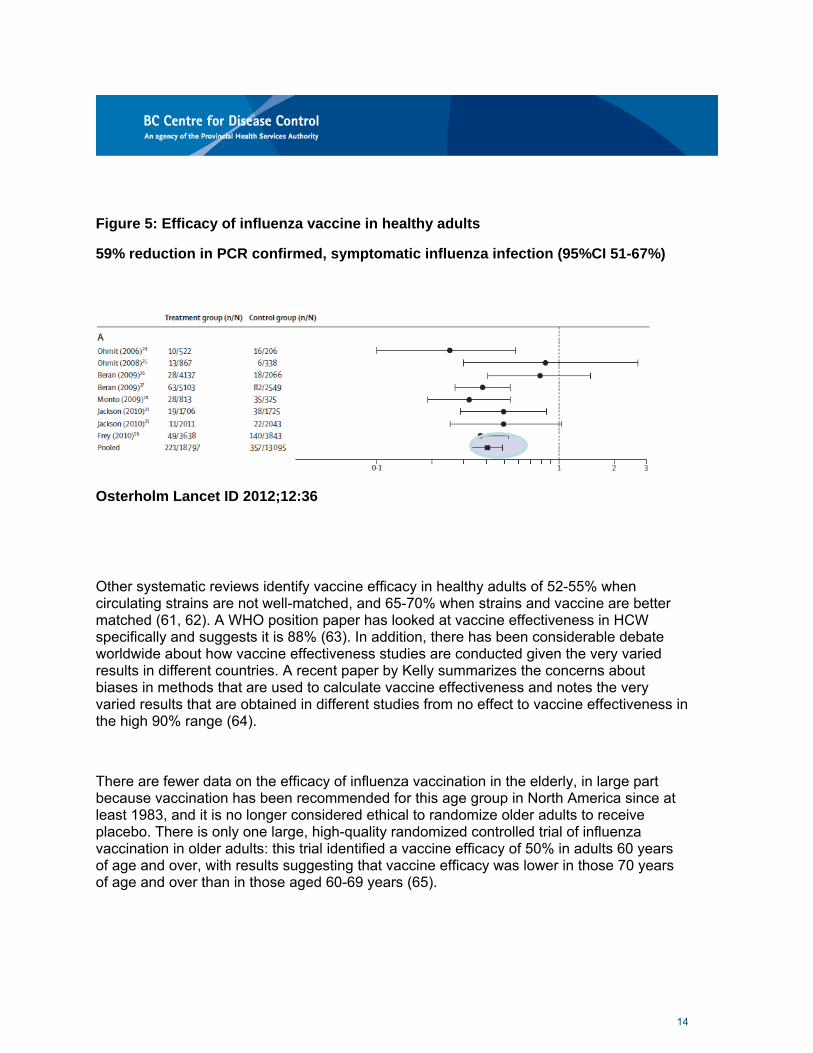
Recently a systematic review of vaccine effectiveness was completed by Osterholm that suggested that the effectiveness was closer to 59% in healthy adults and that there was no evidence to support it being effective in elderly people at all (5). This study used very restrictive criteria for assessment of influenza vaccine efficacy and effectiveness, and as such, did not consider many of the papers typically considered in such analyses. However, many feel this review provides a better estimate because it only included trials using PCR detection of influenza as an outcome and thereby avoided the bias associated with measuring infection serologically. PCR is also more sensitive than previous methods; because it may detect milder illness with shedding of less virus, and because vaccine reduces the severity of influenza, vaccination may be less protective against illness that is culture positive as compared to illness that is PCR positive. Osterholm et al.'s overall estimate of TIV efficacy on average over all seasons and strain matches was 59% (95% confidence interval 51-67%)( Figure 5) (5), consistent with the findings of the Cochrane review; the confidence intervals between the two studies overlap meaning they are not statistically significantly different.
In addition, they concluded that data supported ‘breakthrough’ illness in vaccinated individuals was less severe than in those who were unvaccinated. The conclusions from the Osterholm paper highlighted the need for a new generation of more highly effective and cross protective vaccines that can be manufactured rapidly to address the ongoing public health burden caused by seasonal influenza and the potential global effect of a severe pandemic. In the meantime they called for optimal use and support for the current vaccines as the best intervention available for seasonal influenza.
14
Figure 5: Efficacy of influenza vaccine in healthy adults
59% reduction in PCR confirmed, symptomatic influenza infection (95%CI 51-67%)
Osterholm Lancet ID 2012;12:36
Other systematic reviews identify vaccine efficacy in healthy adults of 52-55% when circulating strains are not well-matched, and 65-70% when strains and vaccine are better matched (61, 62). A WHO position paper has looked at vaccine effectiveness in HCW specifically and suggests it is 88% (63). In addition, there has been considerable debate worldwide about how vaccine effectiveness studies are conducted given the very varied results in different countries. A recent paper by Kelly summarizes the concerns about biases in methods that are used to calculate vaccine effectiveness and notes the very varied results that are obtained in different studies from no effect to vaccine effectiveness in the high 90% range (64).
There are fewer data on the efficacy of influenza vaccination in the elderly, in large part because vaccination has been recommended for this age group in North America since at least 1983, and it is no longer considered ethical to randomize older adults to receive placebo. There is only one large, high-quality randomized controlled trial of influenza vaccination in older adults: this trial identified a vaccine efficacy of 50% in adults 60 years of age and over, with results suggesting that vaccine efficacy was lower in those 70 years of age and over than in those aged 60-69 years (65).

15
The Cochrane review identified three other randomized controlled trials of influenza vaccine in the elderly, and did not include one other randomized trial in older adults for reasons that are not clear (66). The Cochrane review concluded that, based on randomized controlled trials, the efficacy of influenza vaccine in older adults was 58% (95% Cl 34%-73%); all trials were in well-matched seasons (5). This estimate is based largely on the Govaert study (65), and is likely applicable to adults between 65 and 70 years old. This data suggest that the effect of vaccination is significantly reduced in older adults, who are also known to have reduced immune response to vaccination. The estimate of an overall reduction by 50% considering all adults aged >65 years compared to healthy adults is probably a reasonable estimate.
The immune response to influenza vaccine is also known to be reduced in populations of patients who are immunosuppressed, to an extent which suggests that clinical protection will be reduced (67,68). Again, because vaccination is recommended for immunosuppressed patients, most ethics committees will not permit randomization to placebo. While there are a number of studies demonstrating that vaccine is protective in different populations of patients (69,70); there are too few data to permit comparison of the estimates of the effectiveness of vaccine in the prevention of illness due to influenza with similar illness in healthy adults. What is clear is that the vaccine provides good protection in healthy adults and much more modest protection in the population that needs it most, those at risk for severe illness or death from influenza.
5. What is the rationale for requiring HCW who are not vaccinated to wear a mask? What is the evidence that wearing a mask will prevent influenza transmission?
Having healthcare providers wear a mask during influenza season will also provide some protection to their patients and to themselves. The primary purpose of having health care providers wear a mask is to prevent transmission from them to their patients at times when they are shedding virus (prior to symptom onset, if they are working while ill, or if they are asymptomatically infected).
Immunization is clearly superior in terms of protection from influenza as the vaccine needs only be received once in the season and it protects the HCW at work and in the community (providing individual protection for the HCW and their family/contacts in the community as well as in the work setting). Wearing a mask will only protect the patient for the short encounter in the healthcare setting. Two types of studies are available to consider the protection afforded by masks (surgical or procedure masks) and respirators. Experimental

16
studies measure influenza virus concentrations in different particle sizes in the air and in people's airways, and have asked whether masks prevent both egress and ingress of particles containing influenza.
There is good evidence that surgical masks reduce the concentration of influenza virus expelled into the ambient air (a 3.4 fold overall reduction in a recent study) when they are worn by someone shedding influenza virus (71,72). There is also evidence that surgical masks reduce exposure to influenza in experimental conditions (73). There is disagreement in the literature as to whether N95 respirators reduce expelled virus more effectively than surgical masks (71,74,75). The extent that N95 respirators add protection to surgical masks to prevent exposure to influenza virus in droplets or aerosols is currently uncertain: there is some evidence that they improve protection (75), but whether the increase is clinically significant is unknown. One pivotal study (76) randomized nurses to wearing either a surgical mask or an N95 respirator when patients required droplet-contact precautions for viral respiratory illness (including influenza) in an acute care facility. The study found no difference in rates of influenza infection in the two groups of nurses, suggesting that masks and respirators provided equal protection against transmission of influenza. In addition, the degree of protection depends on exactly which surgical mask and which N95 respirator, and whether the respirator is fit tested or not.
Clinical studies have also suggested that masks, in association with hand hygiene, may have some impact on decreasing transmission of influenza infection (77-79, 80). These studies are not definitive as they all had limitations. The household studies are limited by that fact that mask wearing did not start until influenza had been diagnosed and the patient/household was enrolled in the study, such that influenza may have been transmitted prior to enrolment. A study in student residences is limited by the fact that participants wore their mask for only approximately 5 hours per day. Two systematic reviews of the cumulative studies conclude that there is evidence to support that wearing of masks or respirators during illness protects others, and a very limited amount of data to support the use of masks or respirators to prevent becoming infected (81, 82). One concluded: "the effectiveness of masks and respirators is likely linked to early, consistent and correct usage".(82)
In summary, there is evidence supporting the use of wearing of masks to reduce transmission of influenza from health care workers to patients. It is not conclusive, and not of the quality of evidence that supports influenza vaccination. Based on current evidence, patient safety would be best ensured by requiring healthcare providers to be vaccinated if they provide care during periods of influenza activity. However, if healthcare workers are unvaccinated, wearing masks almost certainly provides some degree of protection to their patients. There is also a potential for mask wearing to provide a benefit to the HCW by
17
providing a barrier to them contacting respiratory viruses (including influenza) or bacteria from an infectious patient (frequently with unrecognized infection).
References
1. Nicholson KG, Human Influenza, Chapter 5 in Textbook of Influenza, Nicholson KG, Webster RG, and Hay AJ, eds. Blackwell Science, 1998, pp 181-206.
2. Nguyen-Van-Tam JS. Epidemiology of influenza. Chapter 17 in Textbook of Influenza, Nicholson KG, Webster RG, and Hay AJ, eds. Blackwell Science, 1998, pp 181-206.
3. Freitas FT, Cabral AP, Barros EN, Burigo MJ, Prochnow RD, Silva LA, Widdowson MA, Sobel J. Pre-symptomatic transmission of pandemic influenza H1N1 2009: investigation of a family cluster, Brazil. Epidemiollnfect. 2013 Apr;141(4):763-6
4. Lau LL, Cowling BJ, Fang VJ, Chan KH, Lau EH, Lipsitch M, Cheng CK, Houck PM, Uyeki TM, Peiris JS, Leung GM. Viral shedding and clinicalillness in naturally acquired influenza virus infections. J Infect Dis. 2010 May 15;201(10):1509-16.
5. Osterholm MT, Kelley NS, Sommer A, Belongia EA. Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet Infect Dis. 2012 Jan;12(1):36-44.
6. Noh JY, Song JY, Cheong HJ, Choi WS, Lee J, Lee JS, Wie SH, Jeong HW, Kim YK,Choi SH, Han SB, So BH, Kim H, Kim WJ. Laboratory surveillance of influenza-like illness in seven teaching hospitals, South Korea: 2011-2012 season. PLoS One. 2013 May 22;8(5):e64295.
7. Wallace LA, Collins TC, Douglas JD, Mcintyre S, Millar J, Carman WF. Virological surveillance of influenza-like illness in the community using PCR and serology. J Clin Viral. 2004 Sep;31(1):40-5.
8. Boivin G, Hardy I, Tellier G, Maziade J. Predicting influenza infections during epidemics with use of a clinical case definition. Clin Infect Dis. 2000Nov;31(5):1166-9.
9. Kwong JC, Crowcroft NS, Campitelli MA et al. Ontario Burden of Infectious Diseases Study. Ontario Agency for Health Protection and Promotion and the Institute for Clinical and Evaluative Sciences, Ontario, Canada. Available at: http:/ /www.ices.on.ca/file/ONBOIDS FullReport intra.pdf. Accessed January 21, 2012
10. http://www.bccdc.ca/dis-cond/a-z/_f/Flu/statsres/default.htm
18
11. Salgado CD, Farr BM, Hall KK, Hayden FG. Influenza in the acute hospital setting Lancet Infectious Diseases 2002; 2: 145–55.
12. Anonymous, Centers for Disease Control and Prevention. Suspected nosocomial influenza cases in an intensive care unit. Morb Mortal Wkly Rep 1988;37: 3–4.
13. Weinstock D, Eagan J, Malak S, Rogers M, Wallace H, Kiehn T et al. Control of influenza A on a bone marrow transplant unit. Infect Control Hosp Epidemiol 2000; 21:730–32.
14. Statement on Seasonal Influenza Vaccine for 20 11 - 2012- Canada Communicable Disease Report Monthly- Public Health Agency of Canada [Internet]. [cited 21 June 2013). Available from: http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/ll vol37/acs-dcc-5/indexeng.php#footnote97
15. Potter J, Stott DJ, Roberts MA, Elder AG, O'Donnell B, Knight PV, Carman WF. Influenza vaccination of health care workers in long-term-care hospitals reduces the mortality of elderly patients. J Infect Dis. 1997 Jan;175(1):1-6.
16. Carman WF, Elder AG, Wallace LA, McAulay K, Walker A, Murray GD, Stott DJ. Effects of influenza vaccination of health-care workers on mortality of elderly people in long-term care: a randomised controlled trial. Lancet. 2000 Jan 8;355(9198):93-7.
17. Hayward AC, Harling R, Wetten S, Johnson AM, Munro S, Smedley J, Murad S, Watson JM. Effectiveness of an influenza vaccine programme for care home staff to prevent death, morbidity, and health service use among residents: cluster randomised controlled trial. BMJ. 2006 Dec 16;333(7581):1241.
18. Lemaitre M, Meret T, Rothan-Tondeur M, Belmin J, Lejonc JL, LuquelL, Piette F, Salam M, Verny M, Vetel JM, Veyssier P, Carrat F. Effect of influenza vaccination of nursing home staff on mortality of residents: a cluster-randomized trial. JAm Geriatr Soc.2009;57(9):1580-6
19. Thomas RE, Jefferson T, Lasserson TJ. Influenza vaccination for healthcare workers who work with the elderly. Cochrane Database of Systematic Reviews 2010, Issue 2. Art. No.: CD005187. DOl: 10.1002/14651858.CD005187.pub3.
20. Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schinemann HJ; GRADE Working Group. What is "quality of evidence" and why is it important to clinicians? BMJ. 2008 May3;336(7651):995-8.
21. Nicholson KG, Kent J, Hammersley V. Influenza A among community-dwelling elderly persons in Leicestershire during winter 1993-4; cigarette smoking as a risk factor and the efficacy of influenza vaccination. EpidemiolInfect. 1999 Aug 1;123(1):103-8.
22. Utsumi M, Makimoto K, Quroshi N, Ashida N. Types of infectious outbreaks and their impact in elderly care facilities: a review of the literature. Age Ageing. 2010 May;39(3):299-305.
19
23. Gaillat J, Dennetiere G, Raffin-Bru E, Valette M, Blanc MC. Summer influenza outbreak in a home for the elderly: application of preventive measures. J Hasp Infect. 2008 Nov;70(3):272-7.
24. Loeb M, McGeer A, McArthur M, Peeling RW, Petrie M, Simor AE. Surveillance for outbreaks of respiratory tract infections in nursing homes. CMAJ. 2000 Apr 18;162(8):1133-7.
25. Cho CH, Chulten B, Lee CK, Nam MH, Yoon SY, Lim CS, Cho Y, Kim YK. Evaluation of a novel real-time RT-PCR using TOCE technology compared with culture and Seeplex RV15 for simultaneous detection of respiratory viruses. J Clin Viral. 2013 Aug;57(4):338-42.
26. Stephenson I, Das RG, Wood JM, Katz JM. Comparison of neutralising antibody assays for detection of antibody to influenza A/H3N2 viruses: an international collaborative study. Vaccine. 2007 May 16;25(20):4056-63.
27. Wood JM, Gaines-Das RE, Taylor J, Chakraverty P. Comparison of influenza serological techniques by international collaborative study. Vaccine. 1994 Feb;12(2):167-74.
28. Loeb MB, Carusone SB, Marrie TJ, Brazil K, Krueger P, Lohfeld L, Simor AE, Walter SD. lnterobserver reliability of radiologists' interpretations of mobile est radiographs for nursing home-acquired pneumonia. JAmMed Dir Assoc. 2006 Sep;7(7):416-9.
29. Lester RT, McGeer A, Tomlinson G, Detsky AS. Use of, effectiveness of, and attitudes regarding influenza vaccine among house staff. Infect Control Hasp Epidemiol. 2003 Nov;24(11):839-44.
30. Turnberg W, Daniell W, Duchin J. Influenza vaccination and sick leave practices and perceptions reported by health care workers in ambulatory care settings. Am J Infect Control. 2010 Aug;38(6):486-8.
31. Coleman BL, Boggild AK, Drews SJ, Li Y, Low DE, McGeer AJ. Respiratory illnesses in Canadian health care workers: a pilot study of influenza vaccine and oseltamivir prophylaxis during the 2007/2008 influenza season. Influenza Other Resp Viruses. 2011 Nov;5(6):404-8.
32. Ontario influenza bulletin, 2010-11 season weeks 40-41; available at: http: I lwww.publichealthontario.ca/ en/DataAndAnalytics/ Documents/ lnfluenza%20Bulletin -Weeks%2040 41.pdf.
33. Mahmud SM, Thompson LH, Nowicki DL, Plourde PJ. Outbreaks of influenza-like illness in long-term care facilities in Winnipeg, Canada. Influenza Other Respi Viruses. 2012 Nov12. [Epub ahead of print]
34. McGeer A, Green KA, Plevneshi A, Shigayeva A, Siddiqi N, Raboud J, Low DE; Toronto Invasive Bacterial Diseases Network. Antiviral therapy and outcomes of influenza requiring hospitalization in Ontario, Canada. Clin Infect Dis. 2007 Dec 15;45(12):1568-75.
20
35. Ahmed F, Lindley Mc, Allred N, Weinbaum C and Grohskop L. Effect of influenza vaccination of health care personnel on morbidity and mortality among patients: systematic review and grading of evidence. Clinical Infectious Diseases 2013; downloaded from http://cid.oxfordjournals.org/on September 20, 2013.
36. Griffin M R. Influenza vaccination of health acre workers: making the Grade for action. Clinical Infectious Diseases 2013; downloaded from http://cid.oxfordjournals.org/on September 20, 2013.
37. Stevenson CG, McArthur MA, Naus M, Abraham E, McGeer AJ. Prevention of influenza and pneumococcal pneumonia in Canadian long-term care facilities: how are we doing? CMAJ. 2001 May 15;164(10):1413-9.
38. Shugarman LR, Hales C, Setodji CM, Bardenheier B, Lynn J. The influence of staff and resident immunization rates on influenza-like illness outbreaks in nursing homes. J Am Med Dir Assoc. 2006 Nov;7(9):562-7.
39. King JC Jr, Stoddard JJ, Gaglani MJ,Moore KA, Magder L, McClure E, Rubin JD, Englund JA, Neuzil K. Effectiveness of school-based influenza vaccination. N Engl J Med. 2006 Dec 14;355(24):2523-32.
40. Monto AS, Davenport FM, Napier JA, Francis T, Jr. Effect of vaccination of a school�age population upon the course of an A2�Hong Kong influenza epidemic. Bull World Health Organ. 1969;41(3):537�542.
41. Loeb M, Russell ML, Moss L, Fonseca K, Fox J, Earn DJ, Aoki F, Horsman G, Van Caeseele P, Chokani K, Vooght M, Babiuk L, Webby R, Walter SD. Effect of Influenza vaccination of children on infection rates in Hutterite communities: a randomized trial. JAMA. 2010 Mar10;303(10):943-50.
42. Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M. The Japanese experience with vaccinating schoolchildren against influenza. N Engl J Med. 2001 Mar 22;344(12):889-96.
43. Voirin N, Barret B, Metzger MH, Vanhems P. Hospital-acquired influenza: a synthesis using the Outbreak Reports and Intervention Studies of NosocomialInfection (ORION) statement. J Hosp Infect. 2009 Jan;71(1):1-14.
44. Gooskens J, Jonges M, Claas EC, Meijer A, van den Broek PJ, Kroes AM. Morbidity and mortality associated with nosocomial transmission of oseltamivir-resistant influenza A(H1N1) virus. JAMA. 2009 Mar 11;301(10):1042-6.
45. Bearden A, Friedrich TC, Goldberg TL, Byrne B, Spiegel C, Schult P, Safdar N. An outbreak of the 2009 influenza a (H1N1) virus in a children's hospital. Influenza Other Respi Viruses. 2012 Sep;6(5):374-9.
21
46. Pollara CP, Piccinelli G, Rossi G, Cattaneo C, Perandin F, Corbellini S, Tomasi DD, Bonfanti C. Nosocomial outbreak of the pandemic Influenza A (H1N1) 2009 in critical hematologic patients during seasonal influenza 2010-2011: detection of oseltamivir resistant variant viruses. BMC Infect Dis. 2013 Mar 7;13:127.
47. Chan MC, Lee N, Ngai KL, Wong BC, Lee MK, Choi KW, Lai RW, Chan PK. A. Pre-seasonal hospital outbreak of influenza pneumonia caused by the drift variant A/Victoria/361 /2011- like H3N2 viruses, Hong Kong, 2011. J Clin Viral. 2013 Mar;56(3):219-25.
48. Grund S, Roggendorf M, Schweiger B. Outbreak of influenza virus A/H1N1 in a hospitalward for immunocompromised patients. Arch Viral. 2010 Nov;155(11):1797-80.
49. lioka F, Sada R, Maesako Y, Nakamura F, Ohno H. Outbreak of pandemic 2009 influenza AIH1N1 infection in the hematology ward: fatal clinical outcome of hematopoietic stem cell transplant recipients and emergence of the H275Y neuraminidase mutation. lnt J Hematol. 2012 Sep;96(3):364-9.
50. Fanella ST, Pinto MA, Bridger NA, Bullard JM, Coombs JM, Crockett ME, Olekson KL, Poliquin PG, Van Caeseele PG, Embree JE. Pandemic (H1N1) 2009 influenza in hospitalized children in Manitoba: nosocomial transmission and lessons learned from the first wave. Infect Control Hosp Epidemiol. 2011 May;32(5):435-43
51. Tsagris V, Nika A, Kyriakou D, Kapetanakis I, Harahousou E, Stripeli F, Maltezou H, Tsolia M. Influenza A/H1N1/2009 outbreak in a neonatal intensive care unit. J Hosp Infect. 2012 May;81(1):36-40
52. Apisarnthanarak A, Puthavathana P, Kitphati R, et al. Outbreaks of Influenza A Among Nonvaccinated Healthcare Workers: Implications for Resource-Limited Settings. Infect Control Hosp Epidemiol, 2008; 29(8):777-780.
53. Sagrera X, Ginovart G, Raspall F, Rabella N, Sala P, Sierra M, Demestre X, Vila C. Outbreaks of influenza A virus infection in neonatalintensive care units. Pediatr Infect Dis J. 2002 Mar;21(3):196-200.
54. Cunney R, Bialachowski A, Thornley D, Smaill F, Pennie R. An outbreak of influenza A in a neonatalintensive care unit. Infect Control Hosp Epidemiol 2000;21:449-454.
55. Benet T, Regis C, Voirin N, Robert 0, Lina B, Cronenberger S, Comte B, Coppere B, Vanhems P. Influenza vaccination of healthcare workers in acute-care hospitals: a case- control study of its effect on hospital-acquired influenza among patients. BMC Infect Dis. 2012 Feb 1;12(1):30.
56. Salgado CD, Giannetta ET, Hayden FG, Farr BM. Preventing nosocomial influenza by improving the vaccine acceptance rate of clinicians. Infect ControlHosp Epidemiol. 2004 Nov;25(11):923-8.

22
57. Vanhems P, Voirin N, RocheS, Escuret V, Regis C, Gorain C, Pires-Cronenberger S, Giard M, Lina B, Najioullah F, Barret B, Pollissard L, David S, Crozet MN, Comte B, Hirschel B, Ecochard R. Risk of influenza-like illness in an acute health care setting during community influenza epidemics in 2004-2005, 2005- 2006, and 2006-2007: a prospective study. Arch Intern Med. 2011 Jan 24;171(2):151-7.
58. Riphagen-Dalhuisen J, Burgerhof JG, Frijstein G, van der Geest-Blankert AD, Danhof-Pont MB, de Jager HJ, Bos AA, Smeets EE, de Vries MJ, Gallee PM, Hak E. Hospital-based cluster randomised controlled trial to assess effects of a multi-faceted programme on influenza vaccine coverage among hospital healthcare workers and nosocomial influenza in the Netherlands, 2009 to 2011. Euro Surveill. 2013;18(26):pii=20512.
59. National Advisory Committee on Immunization. Statement on Seasonal Influenza Vaccine for 2012-2013. CCDR 2012;38:ACS-2. Available at: http:/ /www.phac-aspc.gc.ca/ publicat/ ccdr-rmtc/ 12vol38/ acs-dcc-21assets/ pdf I acs-dcc-2 -eng.pdf
60. Jefferson T, Di Pietrantonj C, Al-Ansary LA, Ferroni E, Thorning S, Thomas RE. Vaccines for preventing influenza in the elderly. Cochrane Database of Systematic Rev;ews 2010, Issue 2. Art. No.: CD004876. DOl: 10.1002/14651858.CD004876.pub3.
61.Tricco AC, Chit A, Soobiah C, Hallett D, Meier G, Chen MH, Tashkandi M, Bauch CT, Loeb M. Comparing influenza vaccine efficacy against mismatched and matched strains: a systematic review and meta-analysis. BMC Med. 2013 Jun 25;11(1):153.
62. DiazGranados CA, Denis M, Plotkin S. Seasonalinfluenza vaccine efficacy and its determinants in children and non-elderly adults: a systematic review with meta-analyses of controlled trials. Vaccine. 2012 Dec 17;31(1):49-57.
63. WHO (2012). Vaccines against Influenza. WHO position paper – November 2012. Weekly Epidemiological Record, 47: 461-476.
64. Kelly H, Steffens I. Complexities in assessing the effectiveness of inactivated influenza vaccines. Euro Surveill. 2013;18(7):pii=20403. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20403
65. Govaert TM, Thijs CT, Masurel N, Sprenger MJ, Dinant GJ, Knottnerus JA. The efficacy of influenza vaccination in elderly individuals. A randomized double-blind placebo-controlled trial. JAMA. 1994 Dec 7;272(21):1661-5
66. Praditsuwan R, Assantachai P, Wasi C, Puthavatana P, Kositanont U. Theefficacy and effectiveness of influenza vaccination among Thai elderly persons living in the community. J Med Assoc Thai. 2005 Feb;88(2):256-64.
67. Beck CR, McKenzie BC, Hashim AB, Harris RC; University of Nottingham lnfluenzaand the lmmunoCompromised (UNIIC) Study GroupN, guyen-Van-Tam JS. Influenza vaccination for immunocompromised patients: systematic review and meta- analysis by etiology. J Infect Dis. 2012 Oct;206(8):1250-9.
23
68. Ljungman P. Vaccination of immunocompromised patients. Clin Microbiol lnfect. 2012 Oct;18 Suppl5:93-9.
69. Machado CM, Cardoso MR, da Rocha IF, Boas LS, Dulley FL, Pannuti CS. The benefit of influenza vaccination after bone marrow transplantation. Bone Marrow Transplant. 2005 Nov;36(10):897-900
70. Magnani G, Falchetti E, Pollini G, Reggiani LB, Grigioni F, Coccolo F, Potena L, Magelli C, Sambri V, Branzi A. Safety and efficacy of two types of influenza vaccination in heart transplant recipients: a prospective randomised controlled study. J Heart Lung Transplant. 2005 May;24(5):588-92.
71. Milton DK, Fabian MP, Cowling BJ, Grantham ML, McDevitt JJ. Influenza virus aerosols in human exhaled breath: particle size, culturability, and effect of surgical masks. PLoS Pathog. 2013 Mar;9(3):e1003205.
72. Johnson DF, Druce JD, Birch C, Grayson ML. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis. 2009 Jul15;49(2):275-7.
73. Makison Booth C, Clayton M, Crook B, Gawn JM. Effectiveness of surgical masks against influenza bioaerosols. J Hosp Infect. 2013 May;84(1):22-6.
74. Mansour MM, Smaldone GC. Respiratory source control versus receiver protection: impact of facemask fit. J AerosolMed Pulm Drug Deliv. 2013 Jun;26(3):131-7.
75. Harnish DA, Heimbuch BK, Husband M, Lumley AE, Kinney K, Shaffer RE, Wander JD. Challenge of N95 filtering facepiece respirators with viable H1N1 influenza aerosols. Infect Control Hosp Epidemiol. 2013 May;34(5):494-9.
76. Loeb M, Dafoe N, Mahony J, John M, Sarabia A, Glavin V, Webby R, Smieja M, Earn DJ, Chong S, Webb A, Walter SD. Surgical mask vs N95 respirator for preventing influenza among health care workers: a randomized trial. JAMA. 2009 Nov 4;302(17):1865-71.
77. Cowling BJ, Chan KH, Fang VJ, Cheng CK, Fung RO, Wai W, Sin J, Seto WH, Yung R, Chu DW, Chiu BC, Lee PW, Chiu MC, Lee HC, Uyeki TM, Houck PM, Peiris JS, Leung GM. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009 Oct 6;151(7):437-46.
78. Aiello AE, Perez V, Coulborn RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial. PLoS One. 2012;7(1):e29744. doi: 10.1371 /journal.pone.0029744.
79. Simmerman JM, Suntarattiwong P, Levy J, Jarman RG, Kaewchana S, Gibbons RV, Cowling BJ, Sanasuttipun W, Maloney SA, Uyeki TM, Kamimoto L, Chotipitayasunondh T. Findings from a household randomized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand. Influenza Other Resp Viruses. 2011 Jul;5(4):256-67.

24
80. Suess T, Remschmidt C, Schink SB, Schweiger B, Nitsche A, Schroeder K, Doellinger J, Milde J, Haas W, Koehler I, Krause G, Buchholz U. The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Germany, 2009-2011.BMC Infect Dis. 2012 Jan 26;12:26
81. Cowling BJ, Zhou Y, lp DK, Leung GM, Aiello AE. Face masks to prevent transmission of influenza virus: a systematic review. Epidemiollnfect. 2010 Apr;138(4):449-56.
82. Bin-Reza F, Lopez Chavarrias V, Nicoll A, Chamberland ME. The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence. Influenza Other Respi Viruses. 2012 Jul;6(4):257-67.
Prepared by: Dr Bonnie Henry, BCCDC
Acknowledgments: Dr Allison McGeer, Mt Sinai Hospital, Toronto for her
generous provision of expertise and material that was used extensively in this
discussion paper.