Embed Size (px)
Citation preview
Proton Pump Inhibitors vs. Histamine2-Receptor
Antagonists for Stress Ulcer Prophylaxis
Battle of the Acid Suppressants
Andrew J. Burris, Pharm.D. PGY1 Pharmacy Resident
University Health System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio
February 7, 2014
Learning Objectives: 1. Describe the pathophysiology associated with stress-related mucosal disease2. Identify appropriate indications for stress ulcer prophylaxis3. Identify when stress ulcer prophylaxis should be discontinued4. Evaluate the safety and efficacy associated with histamine2-receptor antagonists and proton
pump inhibitors
Burris AJ Page 2
Stress-Related Mucosal Disease
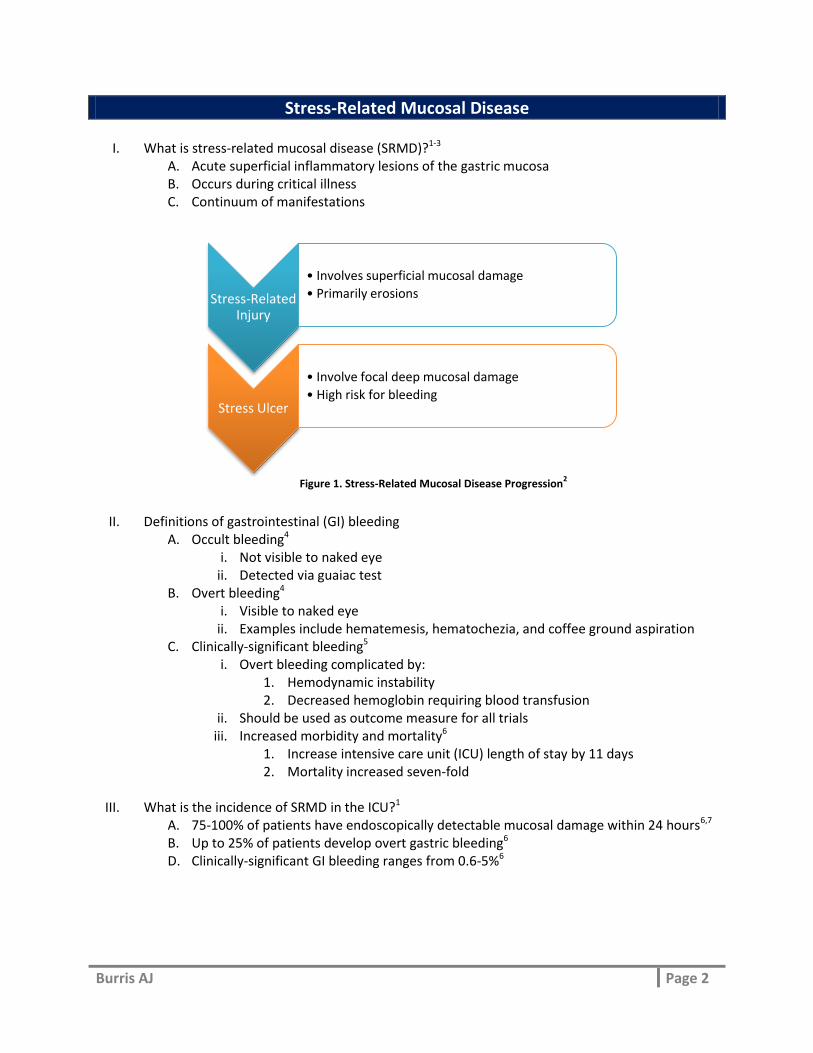
I. What is stress-related mucosal disease (SRMD)?1-3 A. Acute superficial inflammatory lesions of the gastric mucosa B. Occurs during critical illness C. Continuum of manifestations
II. Definitions of gastrointestinal (GI) bleeding A. Occult bleeding4
i. Not visible to naked eye ii. Detected via guaiac test
B. Overt bleeding4 i. Visible to naked eye
ii. Examples include hematemesis, hematochezia, and coffee ground aspiration C. Clinically-significant bleeding5
i. Overt bleeding complicated by: 1. Hemodynamic instability 2. Decreased hemoglobin requiring blood transfusion
ii. Should be used as outcome measure for all trials iii. Increased morbidity and mortality6
1. Increase intensive care unit (ICU) length of stay by 11 days 2. Mortality increased seven-fold
III. What is the incidence of SRMD in the ICU?1
A. 75-100% of patients have endoscopically detectable mucosal damage within 24 hours6,7 B. Up to 25% of patients develop overt gastric bleeding6 D. Clinically-significant GI bleeding ranges from 0.6-5%6
Stress-Related Injury
• Involves superficial mucosal damage
• Primarily erosions
Stress Ulcer
• Involve focal deep mucosal damage
• High risk for bleeding
Figure 1. Stress-Related Mucosal Disease Progression2
Burris AJ Page 3
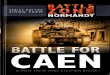
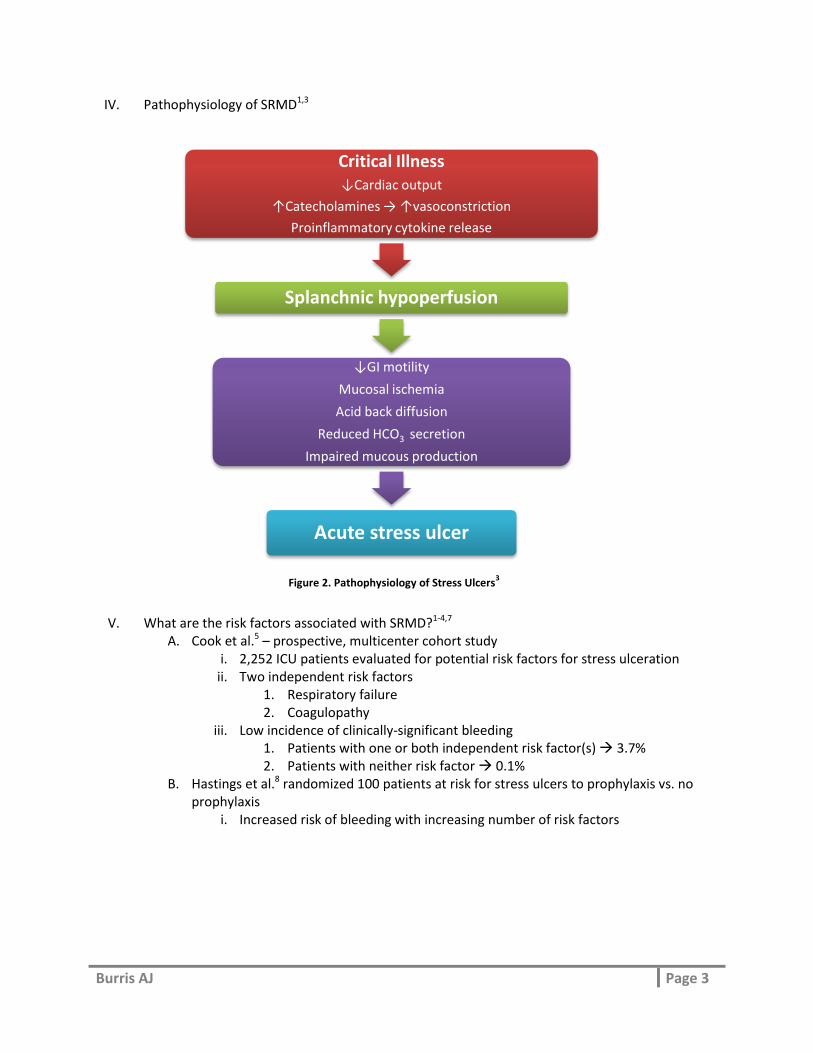
IV. Pathophysiology of SRMD1,3
V. What are the risk factors associated with SRMD?1-4,7
A. Cook et al.5 – prospective, multicenter cohort study i. 2,252 ICU patients evaluated for potential risk factors for stress ulceration
ii. Two independent risk factors 1. Respiratory failure 2. Coagulopathy
iii. Low incidence of clinically-significant bleeding 1. Patients with one or both independent risk factor(s) 3.7% 2. Patients with neither risk factor 0.1%
B. Hastings et al.8 randomized 100 patients at risk for stress ulcers to prophylaxis vs. no prophylaxis
i. Increased risk of bleeding with increasing number of risk factors
Critical Illness ↓Cardiac output
↑Catecholamines → ↑vasoconstriction
Proinflammatory cytokine release
Splanchnic hypoperfusion
↓GI motility
Mucosal ischemia
Acid back diffusion
Reduced HCO3 secretion
Impaired mucous production
Acute stress ulcer
Figure 2. Pathophysiology of Stress Ulcers3
Burris AJ Page 4
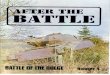
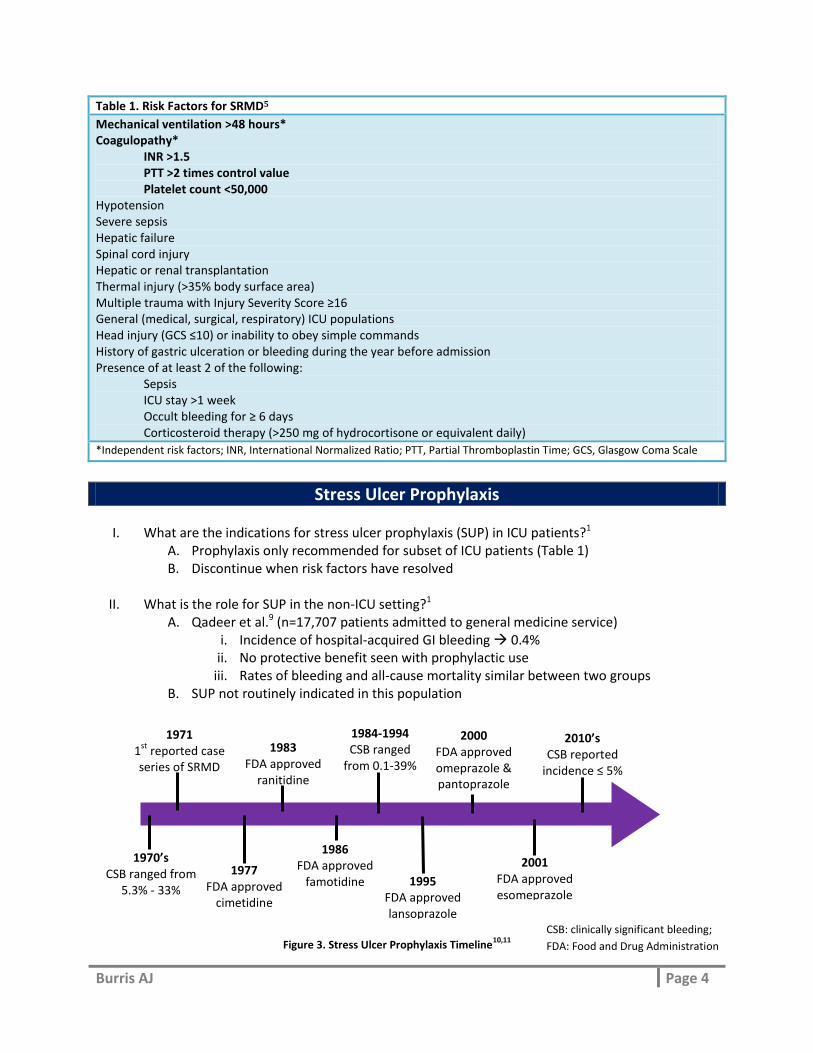
1970’s CSB ranged from
5.3% - 33%
1971 1
st reported case
series of SRMD
1977 FDA approved
cimetidine
1983 FDA approved
ranitidine
1986 FDA approved
famotidine 1995 FDA approved lansoprazole
2000 FDA approved omeprazole & pantoprazole
2001 FDA approved esomeprazole
2010’s CSB reported
incidence ≤ 5% 6%
1984-1994 CSB ranged
from 0.1-39%
Table 1. Risk Factors for SRMD5
Mechanical ventilation >48 hours* Coagulopathy*
INR >1.5 PTT >2 times control value Platelet count <50,000
Hypotension Severe sepsis Hepatic failure Spinal cord injury Hepatic or renal transplantation Thermal injury (>35% body surface area) Multiple trauma with Injury Severity Score ≥16 General (medical, surgical, respiratory) ICU populations Head injury (GCS ≤10) or inability to obey simple commands History of gastric ulceration or bleeding during the year before admission Presence of at least 2 of the following:
Sepsis ICU stay >1 week Occult bleeding for ≥ 6 days Corticosteroid therapy (>250 mg of hydrocortisone or equivalent daily)
*Independent risk factors; INR, International Normalized Ratio; PTT, Partial Thromboplastin Time; GCS, Glasgow Coma Scale
Stress Ulcer Prophylaxis
I. What are the indications for stress ulcer prophylaxis (SUP) in ICU patients?1 A. Prophylaxis only recommended for subset of ICU patients (Table 1) B. Discontinue when risk factors have resolved
II. What is the role for SUP in the non-ICU setting?1
A. Qadeer et al.9 (n=17,707 patients admitted to general medicine service) i. Incidence of hospital-acquired GI bleeding 0.4%
ii. No protective benefit seen with prophylactic use iii. Rates of bleeding and all-cause mortality similar between two groups
B. SUP not routinely indicated in this population Figure 3. Stress Ulcer Prophylaxis Timeline
10,11 CSB: clinically significant bleeding;
FDA: Food and Drug Administration
Burris AJ Page 5
III. Why did the incidence of bleeding change over time?1,4 A. Enteral feeding B. Low tidal volume ventilation C. Prompt and adequate fluid resuscitation
IV. What are the options for SUP?1-4
A. Antacids i. Mechanism of action (MOA)
1. Directly buffer or neutralize acid contents of stomach ii. Efficacy
1. Hastings et al.8 randomized 100 patients at risk for stress ulcers a. Prophylaxis with antacids vs. no prophylaxis b. Decreased bleeding rate when antacid therapy titrated to pH
>3.5 (p<0.005) iii. Limitations
1. Administered every 1-2 hours for adequate acid neutralization 2. High dose antacids increase risk of aspiration pneumonia and toxicity
a. Highest risk in patients with renal dysfunction B. Sucralfate
i. MOA 1. Adheres to epithelial cells and forms protective barrier 2. No acid-neutralizing activity
ii. Efficacy 1. Cook et al.12 randomized 1,200 ICU patients to intravenous (IV)
ranitidine vs. sucralfate a. Clinically significant GI bleeding higher in the sucralfate group
(3.8%) vs. ranitidine (1.7%) group (p=0.02) b. No significant difference in the incidence of pneumonia
iii. Limitations 1. Constipation 2. Hypophosphatemia 3. Nasogastric tube occlusion 4. Aluminum toxicity (chronic renal insufficiency) 5. Decreased absorption of concomitantly administered oral medications
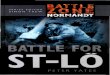
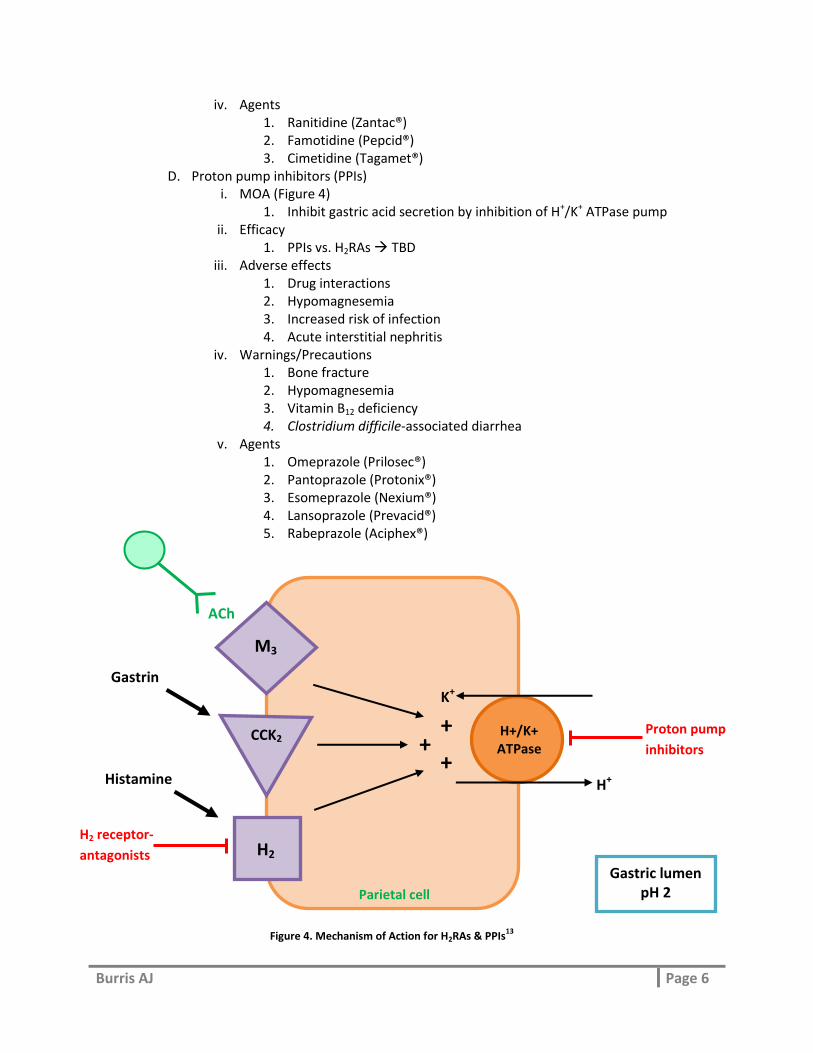
C. Histamine2-receptor antagonists (H2RAs) i. MOA (Figure 4)
1. Inhibit histamine-stimulated acid secretion by blocking H2-receptor 2. Highly selective with little or no effect on other histamine receptors
ii. Efficacy 1. H2RAs are significantly better than placebo, antacids and sucralfate9 2. Proton pump inhibitors vs. H2RAs to be determined (TBD)
iii. Adverse effects 1. Tolerance 2. Drug Interactions
a. Cimetidine = primary offender b. Inhibition of cytochrome P450s
3. Thrombocytopenia 4. Renal dysfunction requires dose adjustment
Burris AJ Page 6
iv. Agents 1. Ranitidine (Zantac®) 2. Famotidine (Pepcid®) 3. Cimetidine (Tagamet®)
D. Proton pump inhibitors (PPIs) i. MOA (Figure 4)
1. Inhibit gastric acid secretion by inhibition of H+/K+ ATPase pump ii. Efficacy
1. PPIs vs. H2RAs TBD iii. Adverse effects
1. Drug interactions 2. Hypomagnesemia 3. Increased risk of infection 4. Acute interstitial nephritis
iv. Warnings/Precautions 1. Bone fracture 2. Hypomagnesemia 3. Vitamin B12 deficiency 4. Clostridium difficile-associated diarrhea
v. Agents 1. Omeprazole (Prilosec®) 2. Pantoprazole (Protonix®) 3. Esomeprazole (Nexium®) 4. Lansoprazole (Prevacid®) 5. Rabeprazole (Aciphex®)
Histamine
H2 receptor-
antagonists
Proton pump
inhibitors
ACh
H+
Parietal cell
K+
H2
H+/K+ ATPase
M3
+
+ + CCK2
Gastrin
Gastric lumen pH 2
Figure 4. Mechanism of Action for H2RAs & PPIs13
Burris AJ Page 7
Discontinuation of Stress Ulcer Prophylaxis
I. Is SUP used appropriately in the inpatient setting?1
A. Patients who are critically-ill with zero risk factors 70% receive SUP B. Original risk factors resolve SUP is continued after ICU downgrade C. SUP often used in medicine patients and continued on hospital discharge
II. What is the economic impact of the inappropriate use of SUP?1
A. Substantial economic impact on the overuse of SUP i. Heidelbaugh et al.14 (n=1,769 general medicine patients)
1. Inappropriate SUP use increased annual inpatient and outpatient costs $111,791
ii. Managed care organization15 1. 20,000 patients prescribed PPI inappropriately at hospital discharge 2. Inappropriate continuation for 30 days associated with cost of US $3
million over four years iii. Neither study accounted for costs incurred from complications of SUP
III. What strategies can reduce the overuse of SUP?1
A. Few studies have explored potential solutions B. Interventions that improve prescribing patterns
i. Educational materials ii. Daily medication reconciliation
iii. Pharmacist participation on rounds C. Additional strategies
i. Reevaluate use of H2RAs and PPIs on standardized order sets ii. Integrate decision-making prompts into the electronic medical record
D. Quality improvement studies are needed
Burris AJ Page 8
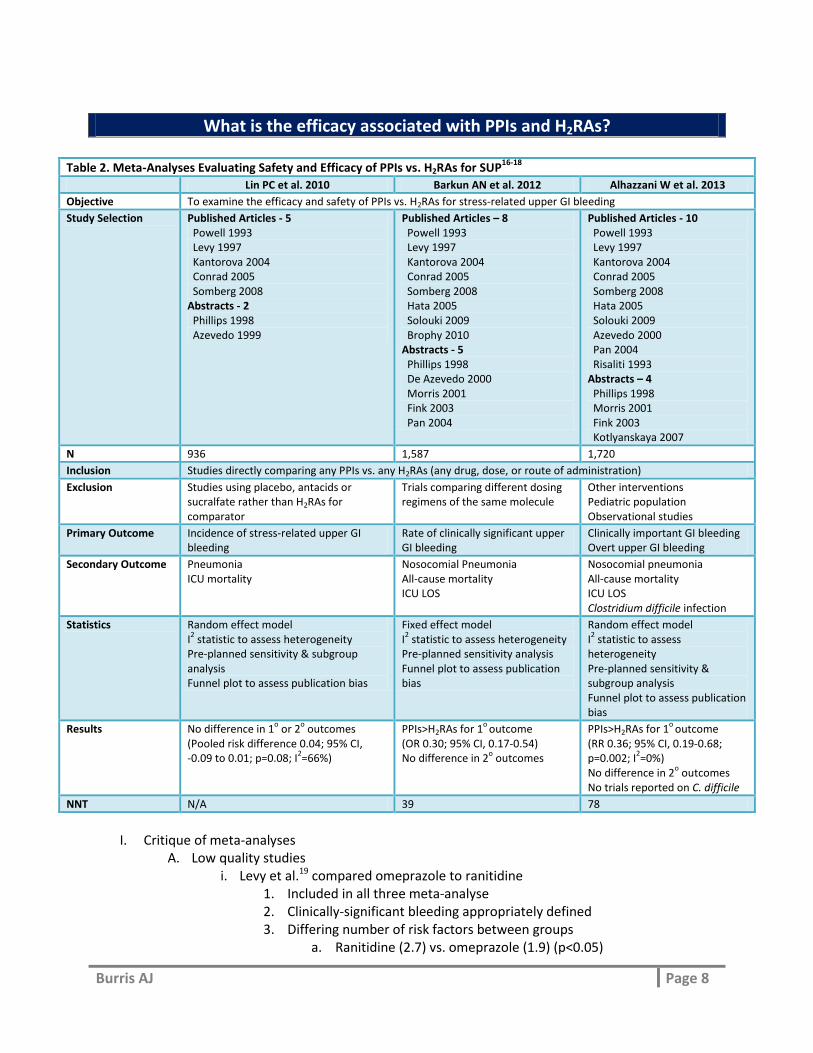
What is the efficacy associated with PPIs and H2RAs?
I. Critique of meta-analyses
A. Low quality studies i. Levy et al.19 compared omeprazole to ranitidine
1. Included in all three meta-analyse 2. Clinically-significant bleeding appropriately defined 3. Differing number of risk factors between groups
a. Ranitidine (2.7) vs. omeprazole (1.9) (p<0.05)
Table 2. Meta-Analyses Evaluating Safety and Efficacy of PPIs vs. H2RAs for SUP16-18
Lin PC et al. 2010 Barkun AN et al. 2012 Alhazzani W et al. 2013
Objective To examine the efficacy and safety of PPIs vs. H2RAs for stress-related upper GI bleeding
Study Selection Published Articles - 5 Powell 1993 Levy 1997 Kantorova 2004 Conrad 2005 Somberg 2008 Abstracts - 2 Phillips 1998 Azevedo 1999
Published Articles – 8 Powell 1993 Levy 1997 Kantorova 2004 Conrad 2005 Somberg 2008 Hata 2005 Solouki 2009 Brophy 2010 Abstracts - 5 Phillips 1998 De Azevedo 2000 Morris 2001 Fink 2003 Pan 2004
Published Articles - 10 Powell 1993 Levy 1997 Kantorova 2004 Conrad 2005 Somberg 2008 Hata 2005 Solouki 2009 Azevedo 2000 Pan 2004 Risaliti 1993 Abstracts – 4 Phillips 1998 Morris 2001 Fink 2003 Kotlyanskaya 2007
N 936 1,587 1,720
Inclusion Studies directly comparing any PPIs vs. any H2RAs (any drug, dose, or route of administration)
Exclusion Studies using placebo, antacids or sucralfate rather than H2RAs for comparator
Trials comparing different dosing regimens of the same molecule
Other interventions Pediatric population Observational studies
Primary Outcome Incidence of stress-related upper GI bleeding
Rate of clinically significant upper GI bleeding
Clinically important GI bleeding Overt upper GI bleeding
Secondary Outcome Pneumonia ICU mortality
Nosocomial Pneumonia All-cause mortality ICU LOS
Nosocomial pneumonia All-cause mortality ICU LOS Clostridium difficile infection
Statistics Random effect model I2 statistic to assess heterogeneity
Pre-planned sensitivity & subgroup analysis Funnel plot to assess publication bias
Fixed effect model I2 statistic to assess heterogeneity
Pre-planned sensitivity analysis Funnel plot to assess publication bias
Random effect model I2 statistic to assess
heterogeneity Pre-planned sensitivity & subgroup analysis Funnel plot to assess publication bias
Results No difference in 1o or 2
o outcomes
(Pooled risk difference 0.04; 95% CI, -0.09 to 0.01; p=0.08; I
2=66%)
PPIs>H2RAs for 1o
outcome (OR 0.30; 95% CI, 0.17-0.54) No difference in 2
o outcomes
PPIs>H2RAs for 1o
outcome (RR 0.36; 95% CI, 0.19-0.68; p=0.002; I
2=0%)
No difference in 2o outcomes
No trials reported on C. difficile
NNT N/A 39 78
Burris AJ Page 9
4. High incidence of bleeding a. Ranitidine (31%) vs. omeprazole (6%) (p<0.05) b. Higher than reported rate (0-16%) from other studies c. Barkun et al. reported overall incidence of 1.3%
5. Study accounted for 20% of weight ii. Brophy et al.20 compared lansoprazole to famotidine
1. Only included in meta-analysis by Barkun et al. 2. Clinically-significant bleeding appropriately defined
a. Only overt bleeding reported 3. Clinically-significant bleeding is secondary outcome
a. Study not powered for outcome B. Definitions of bleeding
i. Variable from study to study ii. Few studies appropriately define clinically-significant bleeding
iii. In Barkun et al.17 7 studies have no definition C. Data quality
i. Positives 1. Funnel plot performed 2. All assessed heterogeneity 3. Sensitivity and subgroup analysis preformed 4. Trial quality assessed
a. Higher quality studies showed smaller treatment effect ii. Negatives
1. Heterogeneity seen in Lin et al. a. No heterogeneity seen in Barkun et al.17 and Alhazzani et al.18 b. Five studies and one abstract included in all three meta-analysis
2. 40% of patients included low risk of clinically significant bleeding 3. Publication/language bias seen via funnel plots
II. Take home points
A. Majority of studies included in meta-analyses did not appropriately define clinically-significant bleeding
B. Significant heterogeneity among studies with regard to risk difference C. Superior efficacy of PPIs compared to H2RAs is difficult to support with current available
evidence
What are the risks associated with PPIs and H2RAs?
I. PPIs are one of the most commonly prescribed classes of drugs worldwide21 A. Sales totaling US $26.9 billion dollars in 200522 B. Experts generally view PPIs as safe C. Potential complications (↑ risk of infection) have caused concern
II. Community-acquired pneumonia (CAP)22
A. Proposed mechanisms i. Increase in gastric pH bacterial overgrowth and colonization
1. Subsequent translocation to lungs by aspiration
Burris AJ Page 10
ii. H+/K+ ATPase also present in the respiratory tract 1. PPIs may alter pH of seromucinous secretions bacterial growth
iii. Acid-suppressive drugs may impair function of neutrophils and natural killer cells23
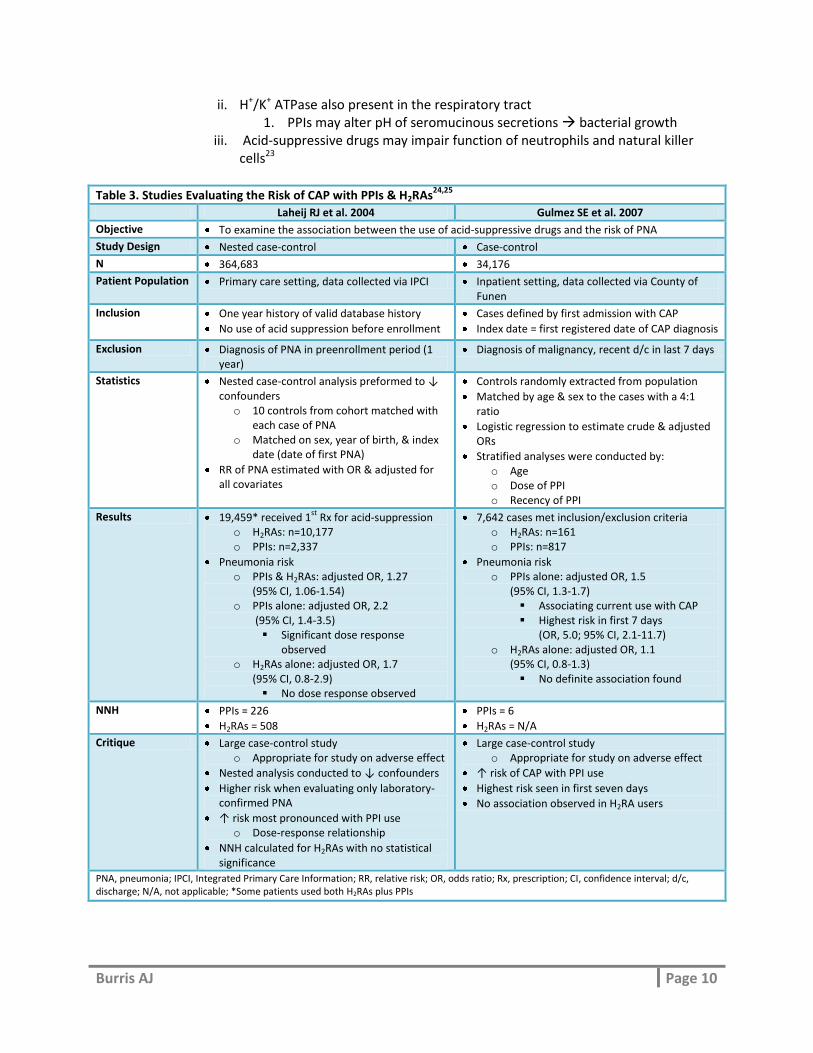
Table 3. Studies Evaluating the Risk of CAP with PPIs & H2RAs24,25
Laheij RJ et al. 2004 Gulmez SE et al. 2007
Objective To examine the association between the use of acid-suppressive drugs and the risk of PNA
Study Design Nested case-control Case-control
N 364,683 34,176
Patient Population Primary care setting, data collected via IPCI Inpatient setting, data collected via County of Funen
Inclusion One year history of valid database history
No use of acid suppression before enrollment
Cases defined by first admission with CAP
Index date = first registered date of CAP diagnosis
Exclusion Diagnosis of PNA in preenrollment period (1 year)
Diagnosis of malignancy, recent d/c in last 7 days
Statistics Nested case-control analysis preformed to ↓ confounders o 10 controls from cohort matched with
each case of PNA o Matched on sex, year of birth, & index
date (date of first PNA)
RR of PNA estimated with OR & adjusted for all covariates
Controls randomly extracted from population
Matched by age & sex to the cases with a 4:1 ratio
Logistic regression to estimate crude & adjusted ORs
Stratified analyses were conducted by: o Age o Dose of PPI o Recency of PPI
Results 19,459* received 1st
Rx for acid-suppression o H2RAs: n=10,177 o PPIs: n=2,337
Pneumonia risk o PPIs & H2RAs: adjusted OR, 1.27
(95% CI, 1.06-1.54) o PPIs alone: adjusted OR, 2.2
(95% CI, 1.4-3.5) Significant dose response
observed o H2RAs alone: adjusted OR, 1.7
(95% CI, 0.8-2.9) No dose response observed
7,642 cases met inclusion/exclusion criteria o H2RAs: n=161 o PPIs: n=817
Pneumonia risk o PPIs alone: adjusted OR, 1.5
(95% CI, 1.3-1.7) Associating current use with CAP Highest risk in first 7 days
(OR, 5.0; 95% CI, 2.1-11.7) o H2RAs alone: adjusted OR, 1.1
(95% CI, 0.8-1.3) No definite association found
NNH PPIs = 226
H2RAs = 508
PPIs = 6
H2RAs = N/A
Critique Large case-control study o Appropriate for study on adverse effect
Nested analysis conducted to ↓ confounders
Higher risk when evaluating only laboratory-confirmed PNA
↑ risk most pronounced with PPI use o Dose-response relationship
NNH calculated for H2RAs with no statistical significance
Large case-control study o Appropriate for study on adverse effect
↑ risk of CAP with PPI use
Highest risk seen in first seven days
No association observed in H2RA users
PNA, pneumonia; IPCI, Integrated Primary Care Information; RR, relative risk; OR, odds ratio; Rx, prescription; CI, confidence interval; d/c, discharge; N/A, not applicable; *Some patients used both H2RAs plus PPIs
Burris AJ Page 11
B. Take home points i. Increased risk of CAP observed with PPI use and no risk observed in H2RA users
ii. Most pronounced risk seen in current users of PPIs and higher doses iii. Case-control study and meta-analysis report consistent results26,27
III. Nosocomial pneumonia (PNA)
A. Proposed mechanisms i. Same proposed mechanisms as CAP
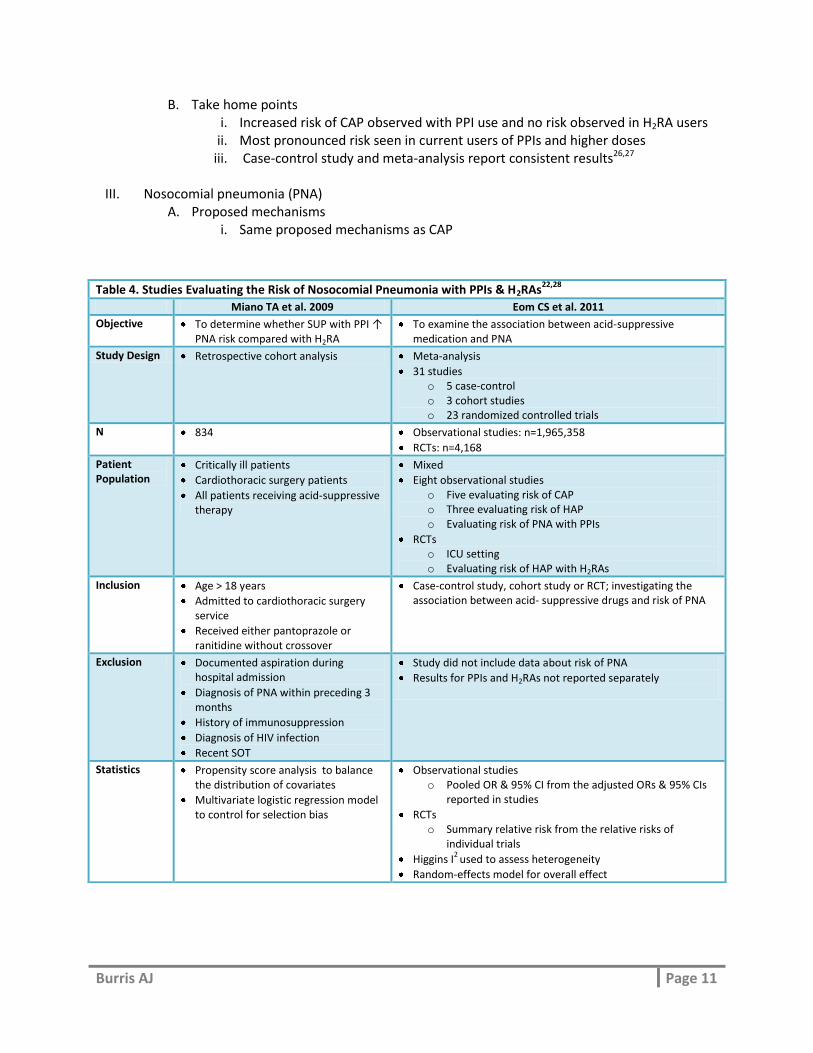
Table 4. Studies Evaluating the Risk of Nosocomial Pneumonia with PPIs & H2RAs22,28
Miano TA et al. 2009 Eom CS et al. 2011
Objective To determine whether SUP with PPI ↑ PNA risk compared with H2RA
To examine the association between acid-suppressive medication and PNA
Study Design Retrospective cohort analysis Meta-analysis
31 studies o 5 case-control o 3 cohort studies o 23 randomized controlled trials
N 834 Observational studies: n=1,965,358
RCTs: n=4,168
Patient Population
Critically ill patients
Cardiothoracic surgery patients
All patients receiving acid-suppressive therapy
Mixed
Eight observational studies o Five evaluating risk of CAP o Three evaluating risk of HAP o Evaluating risk of PNA with PPIs
RCTs o ICU setting o Evaluating risk of HAP with H2RAs
Inclusion Age > 18 years
Admitted to cardiothoracic surgery service
Received either pantoprazole or ranitidine without crossover
Case-control study, cohort study or RCT; investigating the association between acid- suppressive drugs and risk of PNA
Exclusion Documented aspiration during hospital admission
Diagnosis of PNA within preceding 3 months
History of immunosuppression
Diagnosis of HIV infection
Recent SOT
Study did not include data about risk of PNA
Results for PPIs and H2RAs not reported separately
Statistics Propensity score analysis to balance the distribution of covariates
Multivariate logistic regression model to control for selection bias
Observational studies o Pooled OR & 95% CI from the adjusted ORs & 95% CIs
reported in studies
RCTs o Summary relative risk from the relative risks of
individual trials
Higgins I2
used to assess heterogeneity
Random-effects model for overall effect
Burris AJ Page 12
B. Take home points
i. PPI use associated with increased risk of nosocomial PNA in ICU setting ii. Results echo CAP studies with highest risk in recent users and higher doses
iii. Results of high-quality RCTs did not find an increased risk of PNA with H2RAs
IV. Clostridium difficile infection (CDI)21 A. Proposed mechanism
i. ↑ gastric pH > 4 allows ≥50% of ingested bacteria to escape acid barrier ii. Disruption in natural gut bacteria
1. Lack of destruction of ingested microorganism 2. ↑ ascending bacterial colonization from the intestine
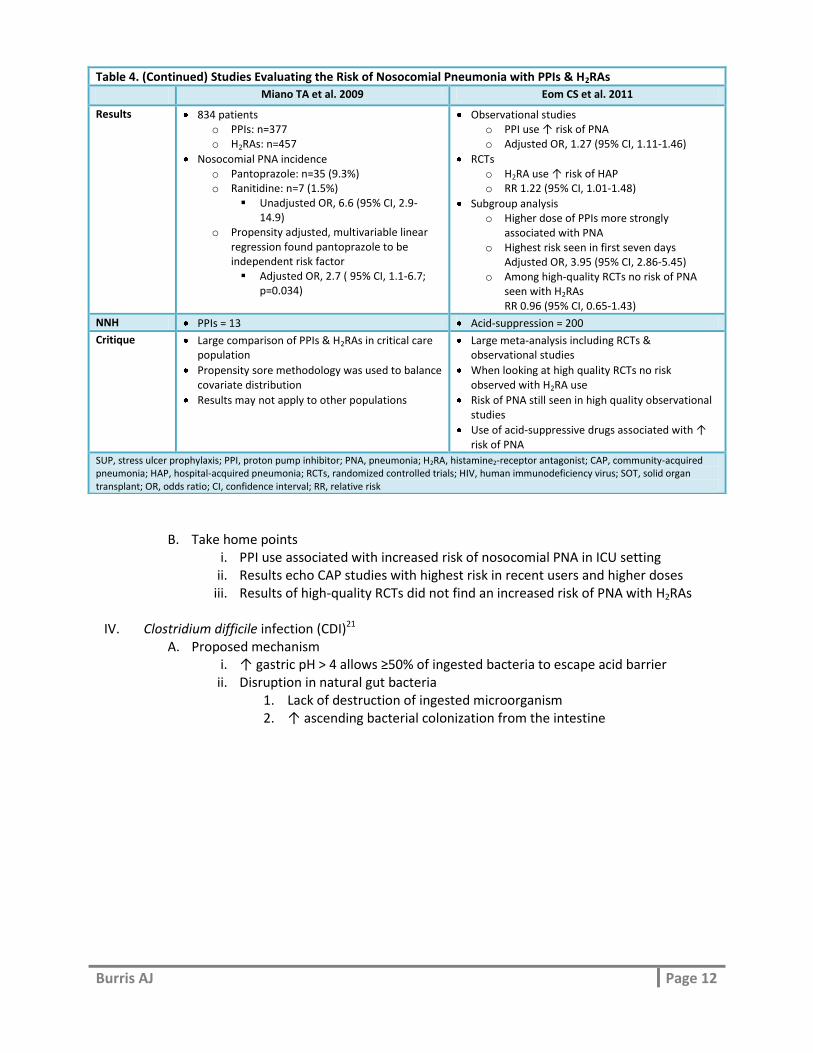
Table 4. (Continued) Studies Evaluating the Risk of Nosocomial Pneumonia with PPIs & H2RAs
Miano TA et al. 2009 Eom CS et al. 2011
Results 834 patients o PPIs: n=377 o H2RAs: n=457
Nosocomial PNA incidence o Pantoprazole: n=35 (9.3%) o Ranitidine: n=7 (1.5%)
Unadjusted OR, 6.6 (95% CI, 2.9-14.9)
o Propensity adjusted, multivariable linear regression found pantoprazole to be independent risk factor Adjusted OR, 2.7 ( 95% CI, 1.1-6.7;
p=0.034)
Observational studies o PPI use ↑ risk of PNA o Adjusted OR, 1.27 (95% CI, 1.11-1.46)
RCTs o H2RA use ↑ risk of HAP o RR 1.22 (95% CI, 1.01-1.48)
Subgroup analysis o Higher dose of PPIs more strongly
associated with PNA o Highest risk seen in first seven days
Adjusted OR, 3.95 (95% CI, 2.86-5.45) o Among high-quality RCTs no risk of PNA
seen with H2RAs RR 0.96 (95% CI, 0.65-1.43)
NNH PPIs = 13 Acid-suppression = 200
Critique Large comparison of PPIs & H2RAs in critical care population
Propensity sore methodology was used to balance covariate distribution
Results may not apply to other populations
Large meta-analysis including RCTs & observational studies
When looking at high quality RCTs no risk observed with H2RA use
Risk of PNA still seen in high quality observational studies
Use of acid-suppressive drugs associated with ↑ risk of PNA
SUP, stress ulcer prophylaxis; PPI, proton pump inhibitor; PNA, pneumonia; H2RA, histamine2-receptor antagonist; CAP, community-acquired pneumonia; HAP, hospital-acquired pneumonia; RCTs, randomized controlled trials; HIV, human immunodeficiency virus; SOT, solid organ transplant; OR, odds ratio; CI, confidence interval; RR, relative risk
Burris AJ Page 13
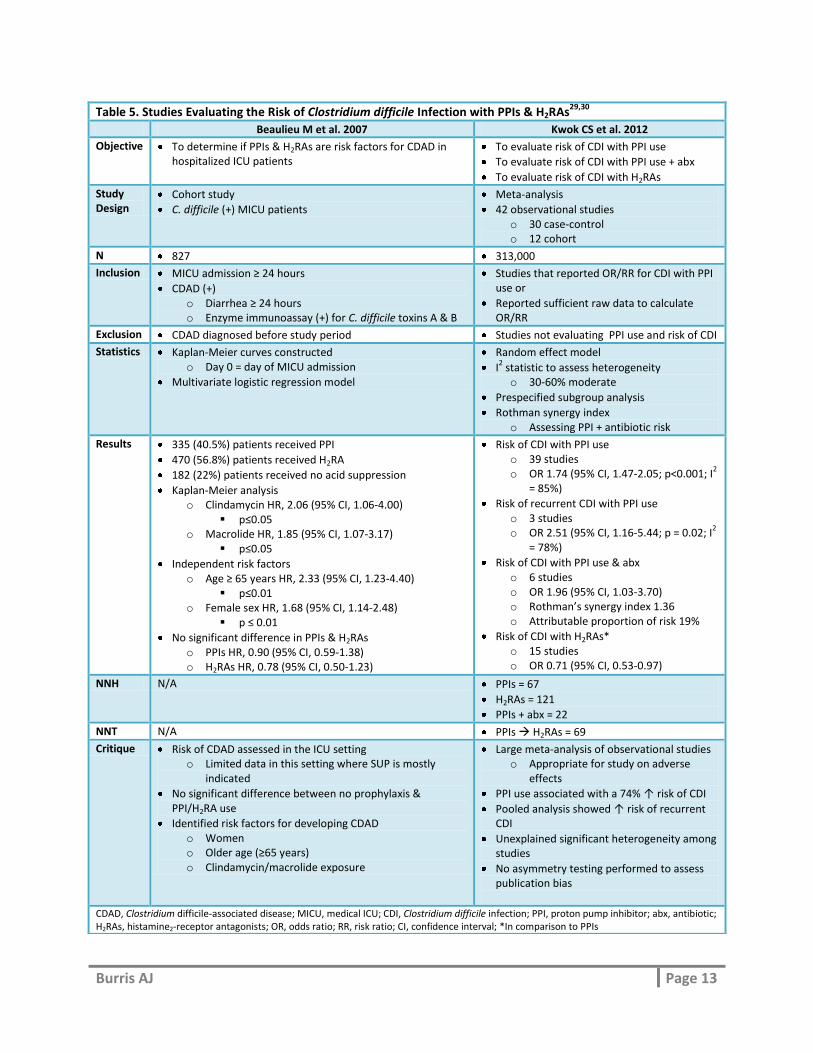
Table 5. Studies Evaluating the Risk of Clostridium difficile Infection with PPIs & H2RAs29,30
Beaulieu M et al. 2007 Kwok CS et al. 2012
Objective To determine if PPIs & H2RAs are risk factors for CDAD in hospitalized ICU patients
To evaluate risk of CDI with PPI use
To evaluate risk of CDI with PPI use + abx
To evaluate risk of CDI with H2RAs
Study Design
Cohort study
C. difficile (+) MICU patients
Meta-analysis
42 observational studies o 30 case-control o 12 cohort
N 827 313,000
Inclusion MICU admission ≥ 24 hours
CDAD (+) o Diarrhea ≥ 24 hours o Enzyme immunoassay (+) for C. difficile toxins A & B
Studies that reported OR/RR for CDI with PPI use or
Reported sufficient raw data to calculate OR/RR
Exclusion CDAD diagnosed before study period Studies not evaluating PPI use and risk of CDI
Statistics Kaplan-Meier curves constructed o Day 0 = day of MICU admission
Multivariate logistic regression model
Random effect model
I2 statistic to assess heterogeneity o 30-60% moderate
Prespecified subgroup analysis
Rothman synergy index o Assessing PPI + antibiotic risk
Results 335 (40.5%) patients received PPI
470 (56.8%) patients received H2RA
182 (22%) patients received no acid suppression
Kaplan-Meier analysis o Clindamycin HR, 2.06 (95% CI, 1.06-4.00)
p≤0.05 o Macrolide HR, 1.85 (95% CI, 1.07-3.17)
p≤0.05
Independent risk factors o Age ≥ 65 years HR, 2.33 (95% CI, 1.23-4.40)
p≤0.01 o Female sex HR, 1.68 (95% CI, 1.14-2.48)
p ≤ 0.01
No significant difference in PPIs & H2RAs o PPIs HR, 0.90 (95% CI, 0.59-1.38) o H2RAs HR, 0.78 (95% CI, 0.50-1.23)
Risk of CDI with PPI use o 39 studies o OR 1.74 (95% CI, 1.47-2.05; p<0.001; I
2
= 85%)
Risk of recurrent CDI with PPI use o 3 studies o OR 2.51 (95% CI, 1.16-5.44; p = 0.02; I
2
= 78%)
Risk of CDI with PPI use & abx o 6 studies o OR 1.96 (95% CI, 1.03-3.70) o Rothman’s synergy index 1.36 o Attributable proportion of risk 19%
Risk of CDI with H2RAs* o 15 studies o OR 0.71 (95% CI, 0.53-0.97)
NNH N/A PPIs = 67
H2RAs = 121
PPIs + abx = 22
NNT N/A PPIs H2RAs = 69
Critique Risk of CDAD assessed in the ICU setting o Limited data in this setting where SUP is mostly
indicated
No significant difference between no prophylaxis & PPI/H2RA use
Identified risk factors for developing CDAD o Women o Older age (≥65 years) o Clindamycin/macrolide exposure
Large meta-analysis of observational studies o Appropriate for study on adverse
effects
PPI use associated with a 74% ↑ risk of CDI
Pooled analysis showed ↑ risk of recurrent CDI
Unexplained significant heterogeneity among studies
No asymmetry testing performed to assess publication bias
CDAD, Clostridium difficile-associated disease; MICU, medical ICU; CDI, Clostridium difficile infection; PPI, proton pump inhibitor; abx, antibiotic; H2RAs, histamine2-receptor antagonists; OR, odds ratio; RR, risk ratio; CI, confidence interval; *In comparison to PPIs
Burris AJ Page 14
B. Take home points i. Conflicting results
ii. Significant unexplained heterogeneity also observed in Janarthanan et al.31 1. Janarthanan et al.31 conducted a meta-analysis (n=288,620) to
summarize the association between CDAD and PPIs 2. Included similar studies as Kwok et al.30 and heterogeneity unexplained
by subgroup analysis 3. Results showed a 65% increase in incidence of CDAD among PPI users
iii. PPI use may be associated with an increase risk of CDI and recurrent CDI 1. Quality of evidence is low interpret cautiously
V. Summary of risks
A. Studies have demonstrated association but not causality B. All associated risks were greater with PPIs as compared to H2RAs C. PPIs have also been linked to potential long-term side effects or complications21
i. Fracture risk ii. Iron deficiency
iii. Hypomagnesaemia iv. Vitamin B12 deficiency
D. Many evaluations did not find a risk with H2RAs
Summary and Recommendations
I. Summary A. SUP is important in preventing clinically significant bleeding B. Acid suppressive therapy is not indicated in everyone C. Discontinuation of SUP is warranted when original risk factors resolve D. Limitations of current available evidence make it difficult to claim PPIs as the superior
agent E. Increases in gastric pH are associated with an increase risk of infection
i. CAP32 1. Management of an uncomplicated case of PNA costs approximately US
$7,000 dollars 2. 40% attributable mortality in patients requiring admission to an ICU
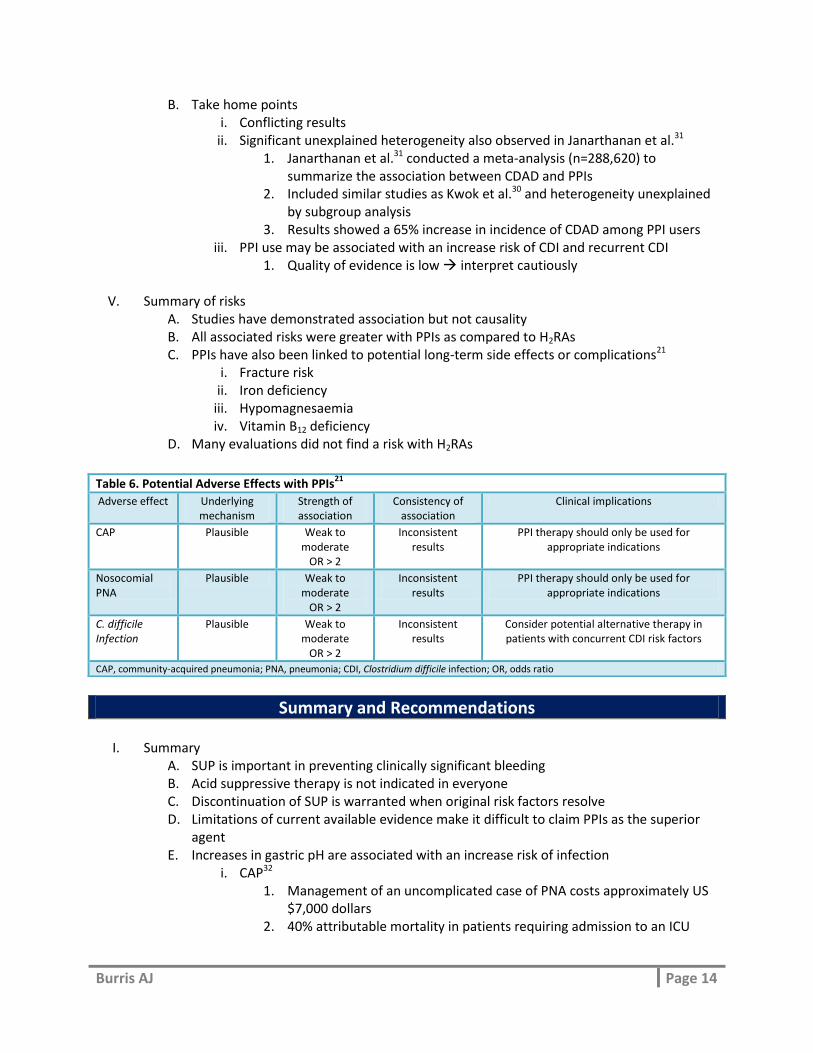
Table 6. Potential Adverse Effects with PPIs21
Adverse effect Underlying mechanism
Strength of association
Consistency of association
Clinical implications
CAP Plausible Weak to moderate
OR > 2
Inconsistent results
PPI therapy should only be used for appropriate indications
Nosocomial PNA
Plausible Weak to moderate
OR > 2
Inconsistent results
PPI therapy should only be used for appropriate indications
C. difficile Infection
Plausible Weak to moderate
OR > 2
Inconsistent results
Consider potential alternative therapy in patients with concurrent CDI risk factors
CAP, community-acquired pneumonia; PNA, pneumonia; CDI, Clostridium difficile infection; OR, odds ratio
Burris AJ Page 15
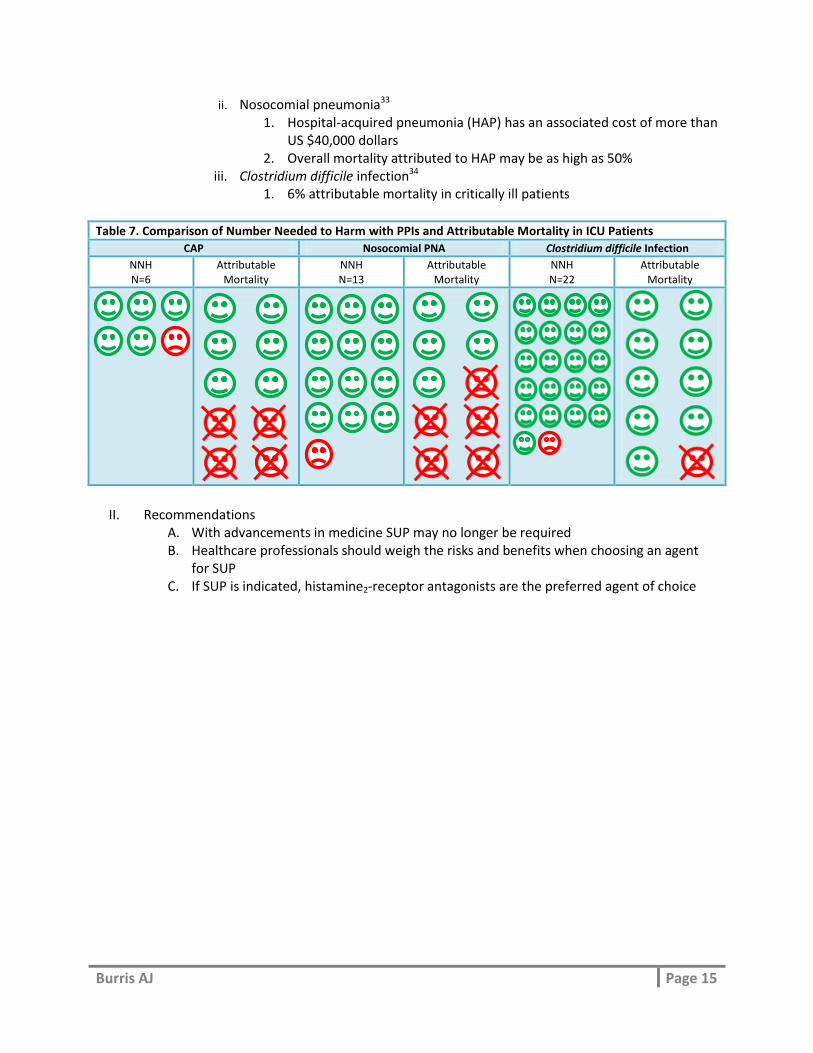
ii. Nosocomial pneumonia33
1. Hospital-acquired pneumonia (HAP) has an associated cost of more than US $40,000 dollars
2. Overall mortality attributed to HAP may be as high as 50% iii. Clostridium difficile infection34
1. 6% attributable mortality in critically ill patients
Table 7. Comparison of Number Needed to Harm with PPIs and Attributable Mortality in ICU Patients
CAP Nosocomial PNA Clostridium difficile Infection
NNH N=6
Attributable Mortality
NNH N=13
Attributable Mortality
NNH N=22
Attributable Mortality
II. Recommendations
A. With advancements in medicine SUP may no longer be required B. Healthcare professionals should weigh the risks and benefits when choosing an agent
for SUP C. If SUP is indicated, histamine2-receptor antagonists are the preferred agent of choice
Burris AJ Page 16
References
1. Anderson ME. Stress Ulcer Prophylaxis in Hospitalized Patients. Hosp Med Clin. 2013;2:e32-e44. 2. Spirt MJ. Stress-related mucosal disease: risk factors and prophylactic therapy. Clin Ther.
2004;26:197-213. 3. Stollman N, Metz DC. Pathophysiology and prophylaxis of stress ulcer in intensive care unit
patients. J Crit Care. 2005;20:35-45. 4. Laine L. Chapter 41. Gastrointestinal Bleeding. In: Longo DL, Fauci AS, Kasper DL, Hauser SL,
Jameson J, Loscalzo J. eds. Harrison's Principles of Internal Medicine, 18e. New York: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.libproxy.uthscsa.edu/content.aspx?bookid=331&Sectionid=40726761. Accessed January 03, 2014.
5. Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group. N Engl J Med. 1994;330:377-81.
6. Mutlu GM, Mutlu EA, Factor P. GI complications in patients receiving mechanical ventilation. Chest. 2001;119:1222-41.
7. Grube RR, May DB. Stress ulcer prophylaxis in hospitalized patients not in intensive care units. Am J Health-Syst Pharm. 2007;64:1396-400.
8. Hastings PR, Skillman JJ, Bushnell LS, Silen W. Antacid titration in the prevention of acute gastrointestinal bleeding: a controlled, randomized trial in 100 critically ill patients. N Engl J Med. 1978;298:1041-5.
9. Qadeer MA, Richter JE, Brotman DJ. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1:13-20.
10. ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998. Am J Health-Syst Pharm. 1999;56:347-79.
11. Lucas CE, Sugawa C, Riddle J, Rector F, Rosenberg B, Walt AJ. Natural history and surgical dilemma of "stress" gastric bleeding. Arch Surg. 1971;102:266-73.
12. Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338:791-7.
13. Wallace JL, Sharkey KA. Chapter 45. Pharmacotherapy of Gastric Acidity, Peptic Ulcers, and Gastroesophageal Reflux Disease. In: Brunton LL, Chabner BA, Knollmann BC. eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics, 12e. New York: McGraw-Hill; 2011. http://accessmedicine.mhmedical.com.libproxy.uthscsa.edu/content.aspx?bookid=374&Sectionid=41266255. Accessed January 30, 2014.
14. Heidelbaugh JJ, Inadomi JM. Magnitude and economic impact of inappropriate use of stress ulcer prophylaxis in non-ICU hospitalized patients. Am J Gastroenterol. 2006;101:2200-5.
15. Thomas L, Culley EJ, Gladowski P. Longitudinal analysis of the costs associated with inpatient initiation and susbsequent outpatient continuation of proton pump inhibitor therapy for stress ulcer prophylaxis in a large managed care organization. J Manag Care Pharm. 2010;16:122-9.
16. Lin PC, Chang CH, Hsu PI, Tseng PL, Huang YB. The efficacy and safety of proton pump inhibitors vs histamine-2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: a meta-analysis. Crit Care Med. 2010;38:1197-205.
Burris AJ Page 17
17. Barkun AN, Bardou M, Pham CQ, Martel M. Proton pump inhibitors vs. histamine 2 receptor antagonists for stress-related mucosal bleeding prophylaxis in critically ill patients: a meta-analysis. Am J Gastroenterol. 2012;107:507-20; quiz 21.
18. Alhazzani W, Alenezi F, Jaeschke RZ, Moayyedi P, Cook DJ. Proton pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in critically ill patients: a systematic review and meta-analysis. Crit Care Med. 2013;41:693-705.
19. Levy MJ, Seelig CB, Robinson NJ, Ranney JE. Comparison of omeprazole and ranitidine for stress ulcer prophylaxis. Dig Dis Sci. 1997;42:1255-9.
20. Brophy GM, Brackbill ML, Bidwell KL, Brophy DF. Prospective, randomized comparison of lansoprazole suspension, and intermittent intravenous famotidine on gastric pH and acid production in critically ill neurosurgical patients. Neurocrit Care. 2010;13:176-81.
21. Reimer C. Safety of long-term PPI therapy. Best Pract Res Clin Gastroenterol. 2013;27:443-54. 22. Eom CS, Jeon CY, Lim JW, Cho EG, Park SM, Lee KS. Use of acid-suppressive drugs and risk of
pneumonia: a systematic review and meta-analysis. CMAJ. 2011;183:310-9. 23. Zedtwitz-Liebenstein K, Wenisch C, Patruta S, Parschalk B, Daxbock F, Graninger W. Omeprazole
treatment diminishes intra- and extracellular neutrophil reactive oxygen production and bactericidal activity. Crit Care Med. 2002;30:1118-22.
24. Laheij RJ, Sturkenboom MC, Hassing RJ, Dieleman J, Stricker BH, Jansen JB. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA. 2004;292:1955-60.
25. Gulmez SE, Holm A, Frederiksen H, Jensen TG, Pedersen C, Hallas J. Use of proton pump inhibitors and the risk of community-acquired pneumonia: a population-based case-control study. Arch Intern Med. 2007;167:950-5.
26. Sarkar M, Hennessy S, Yang YX. Proton-pump inhibitor use and the risk for community-acquired pneumonia. Ann Intern Med. 2008;149:391-8.
27. Johnstone J, Nerenberg K, Loeb M. Meta-analysis: proton pump inhibitor use and the risk of community-acquired pneumonia. Aliment Pharmacol Ther. 2010;31:1165-77.
28. Miano TA, Reichert MG, Houle TT, MacGregor DA, Kincaid EH, Bowton DL. Nosocomial pneumonia risk and stress ulcer prophylaxis: a comparison of pantoprazole vs ranitidine in cardiothoracic surgery patients. Chest. 2009;136:440-7.
29. Beaulieu M, Williamson D, Pichette G, Lachaine J. Risk of Clostridium difficile-associated disease among patients receiving proton-pump inhibitors in a Quebec medical intensive care unit. Infect Control Hosp Epidemiol. 2007;28:1305-7.
30. Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R, Loke YK. Risk of Clostridium difficile infection with acid suppressing drugs and antibiotics: meta-analysis. Am J Gastroenterol. 2012;107:1011-9.
31. Janarthanan S, Ditah I, Adler DG, Ehrinpreis MN. Clostridium difficile-associated diarrhea and proton pump inhibitor therapy: a meta-analysis. Am J Gastroenterol. 2012;107:1001-10.
32. Tejerina E, Frutos-Vivar F, Restrepo MI, et al. Prognosis factors and outcome of community-acquired pneumonia needing mechanical ventilation. J Crit Care. 2005;20:230-8.
33. American Thoracic S, Infectious Diseases Society of A. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388-416.
34. Kenneally C, Rosini JM, Skrupky LP, et al. Analysis of 30-day mortality for clostridium difficile-associated disease in the ICU setting.[Erratum appears in Chest. 2007 Nov;132(5):1721 Note: McKenzie, Wendi [corrected to McKinzie, Wendi E]]. Chest. 2007;132:418-24.
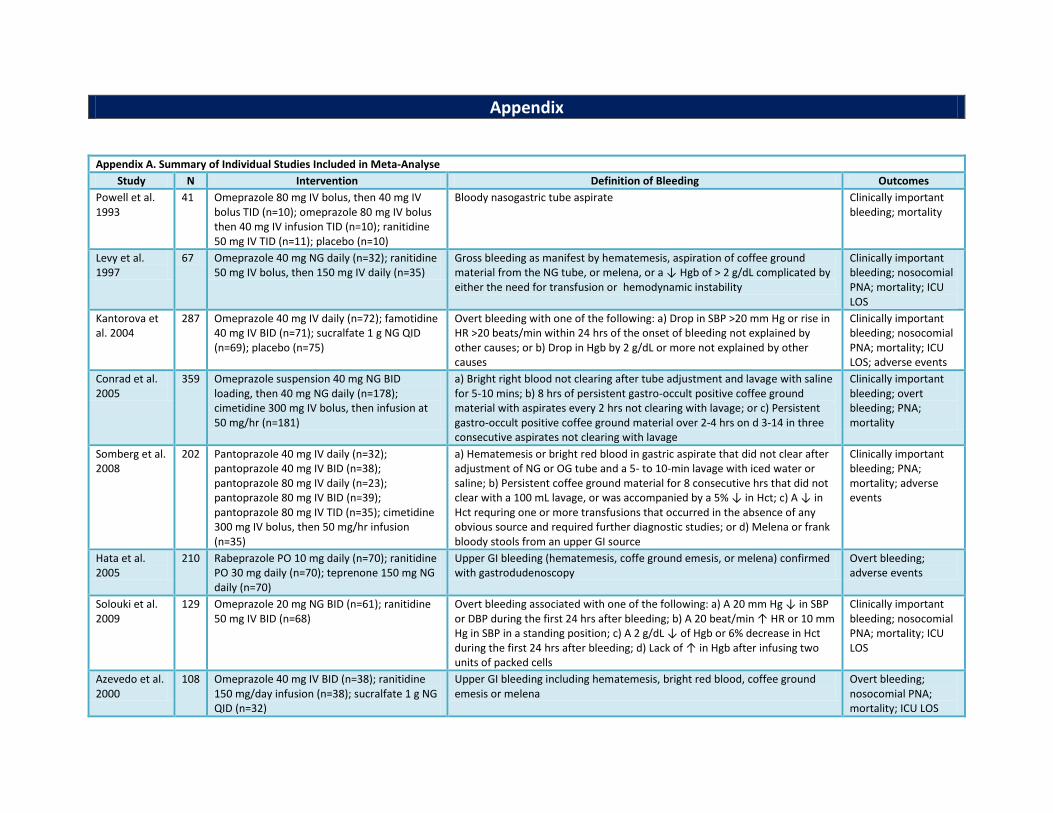
Appendix Appendix A. Summary of Individual Studies Included in Meta-Analyse
Study N Intervention Definition of Bleeding Outcomes
Powell et al. 1993
41 Omeprazole 80 mg IV bolus, then 40 mg IV bolus TID (n=10); omeprazole 80 mg IV bolus then 40 mg IV infusion TID (n=10); ranitidine 50 mg IV TID (n=11); placebo (n=10)
Bloody nasogastric tube aspirate Clinically important bleeding; mortality
Levy et al. 1997
67 Omeprazole 40 mg NG daily (n=32); ranitidine 50 mg IV bolus, then 150 mg IV daily (n=35)
Gross bleeding as manifest by hematemesis, aspiration of coffee ground material from the NG tube, or melena, or a ↓ Hgb of > 2 g/dL complicated by either the need for transfusion or hemodynamic instability
Clinically important bleeding; nosocomial PNA; mortality; ICU LOS
Kantorova et al. 2004
287 Omeprazole 40 mg IV daily (n=72); famotidine 40 mg IV BID (n=71); sucralfate 1 g NG QID (n=69); placebo (n=75)
Overt bleeding with one of the following: a) Drop in SBP >20 mm Hg or rise in HR >20 beats/min within 24 hrs of the onset of bleeding not explained by other causes; or b) Drop in Hgb by 2 g/dL or more not explained by other causes
Clinically important bleeding; nosocomial PNA; mortality; ICU LOS; adverse events
Conrad et al. 2005
359 Omeprazole suspension 40 mg NG BID loading, then 40 mg NG daily (n=178); cimetidine 300 mg IV bolus, then infusion at 50 mg/hr (n=181)
a) Bright right blood not clearing after tube adjustment and lavage with saline for 5-10 mins; b) 8 hrs of persistent gastro-occult positive coffee ground material with aspirates every 2 hrs not clearing with lavage; or c) Persistent gastro-occult positive coffee ground material over 2-4 hrs on d 3-14 in three consecutive aspirates not clearing with lavage
Clinically important bleeding; overt bleeding; PNA; mortality
Somberg et al. 2008
202 Pantoprazole 40 mg IV daily (n=32); pantoprazole 40 mg IV BID (n=38); pantoprazole 80 mg IV daily (n=23); pantoprazole 80 mg IV BID (n=39); pantoprazole 80 mg IV TID (n=35); cimetidine 300 mg IV bolus, then 50 mg/hr infusion (n=35)
a) Hematemesis or bright red blood in gastric aspirate that did not clear after adjustment of NG or OG tube and a 5- to 10-min lavage with iced water or saline; b) Persistent coffee ground material for 8 consecutive hrs that did not clear with a 100 mL lavage, or was accompanied by a 5% ↓ in Hct; c) A ↓ in Hct requring one or more transfusions that occurred in the absence of any obvious source and required further diagnostic studies; or d) Melena or frank bloody stools from an upper GI source
Clinically important bleeding; PNA; mortality; adverse events
Hata et al. 2005
210 Rabeprazole PO 10 mg daily (n=70); ranitidine PO 30 mg daily (n=70); teprenone 150 mg NG daily (n=70)
Upper GI bleeding (hematemesis, coffe ground emesis, or melena) confirmed with gastrodudenoscopy
Overt bleeding; adverse events
Solouki et al. 2009
129 Omeprazole 20 mg NG BID (n=61); ranitidine 50 mg IV BID (n=68)
Overt bleeding associated with one of the following: a) A 20 mm Hg ↓ in SBP or DBP during the first 24 hrs after bleeding; b) A 20 beat/min ↑ HR or 10 mm Hg in SBP in a standing position; c) A 2 g/dL ↓ of Hgb or 6% decrease in Hct during the first 24 hrs after bleeding; d) Lack of ↑ in Hgb after infusing two units of packed cells
Clinically important bleeding; nosocomial PNA; mortality; ICU LOS
Azevedo et al. 2000
108 Omeprazole 40 mg IV BID (n=38); ranitidine 150 mg/day infusion (n=38); sucralfate 1 g NG QID (n=32)
Upper GI bleeding including hematemesis, bright red blood, coffee ground emesis or melena
Overt bleeding; nosocomial PNA; mortality; ICU LOS
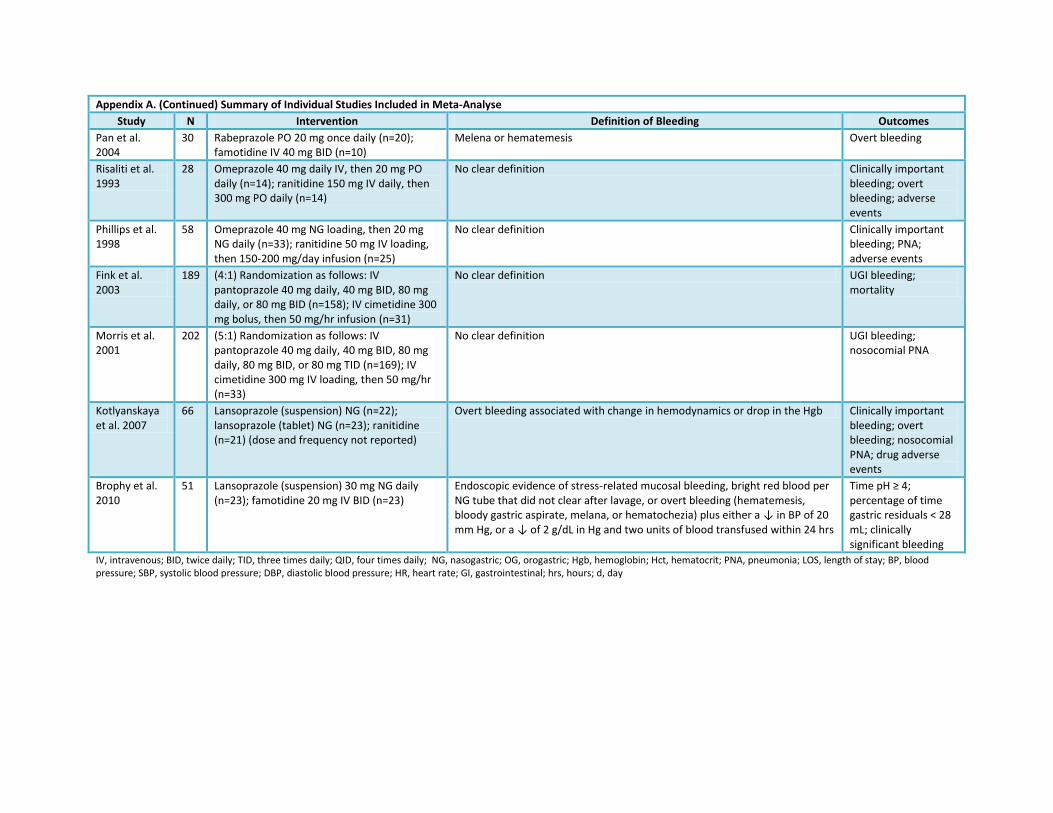
Appendix A. (Continued) Summary of Individual Studies Included in Meta-Analyse
Study N Intervention Definition of Bleeding Outcomes
Pan et al. 2004
30 Rabeprazole PO 20 mg once daily (n=20); famotidine IV 40 mg BID (n=10)
Melena or hematemesis Overt bleeding
Risaliti et al. 1993
28 Omeprazole 40 mg daily IV, then 20 mg PO daily (n=14); ranitidine 150 mg IV daily, then 300 mg PO daily (n=14)
No clear definition Clinically important bleeding; overt bleeding; adverse events
Phillips et al. 1998
58 Omeprazole 40 mg NG loading, then 20 mg NG daily (n=33); ranitidine 50 mg IV loading, then 150-200 mg/day infusion (n=25)
No clear definition Clinically important bleeding; PNA; adverse events
Fink et al. 2003
189 (4:1) Randomization as follows: IV pantoprazole 40 mg daily, 40 mg BID, 80 mg daily, or 80 mg BID (n=158); IV cimetidine 300 mg bolus, then 50 mg/hr infusion (n=31)
No clear definition UGI bleeding; mortality
Morris et al. 2001
202 (5:1) Randomization as follows: IV pantoprazole 40 mg daily, 40 mg BID, 80 mg daily, 80 mg BID, or 80 mg TID (n=169); IV cimetidine 300 mg IV loading, then 50 mg/hr (n=33)
No clear definition UGI bleeding; nosocomial PNA
Kotlyanskaya et al. 2007
66 Lansoprazole (suspension) NG (n=22); lansoprazole (tablet) NG (n=23); ranitidine (n=21) (dose and frequency not reported)
Overt bleeding associated with change in hemodynamics or drop in the Hgb Clinically important bleeding; overt bleeding; nosocomial PNA; drug adverse events
Brophy et al. 2010
51 Lansoprazole (suspension) 30 mg NG daily (n=23); famotidine 20 mg IV BID (n=23)
Endoscopic evidence of stress-related mucosal bleeding, bright red blood per NG tube that did not clear after lavage, or overt bleeding (hematemesis, bloody gastric aspirate, melana, or hematochezia) plus either a ↓ in BP of 20 mm Hg, or a ↓ of 2 g/dL in Hg and two units of blood transfused within 24 hrs
Time pH ≥ 4; percentage of time gastric residuals < 28 mL; clinically significant bleeding
IV, intravenous; BID, twice daily; TID, three times daily; QID, four times daily; NG, nasogastric; OG, orogastric; Hgb, hemoglobin; Hct, hematocrit; PNA, pneumonia; LOS, length of stay; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; GI, gastrointestinal; hrs, hours; d, day