-
7/21/2019 Battista Grossi G. 2007.pdf
1/17
J Oral Maxillofac Surg65:901-917, 2007
Assessing Postoperative Discomfort After
Third Molar Surgery: A Prospective Study
Giovanni Battista Grossi, MD, DMD, DDS,*
Carlo Maiorana, MD, DDS,
Rocco Alberto Garramone, MD, DDS,
Andrea Borgonovo, DMD, MD, Luca Creminelli, DDS,
and Franco Santoro, MD, DDS
Purpose: The purpose of this study was to identify the risk
factors for severe discomfort aftermandibular third molar surgery
and to assess the validity of the Postoperative Symptom Severity
(PoSSe)scale.
Patients and Methods: In a 2-year prospective study, a total of
255 unilateral impacted mandibularthird molar teeth were surgically
removed under local anesthesia by 3 surgeons. Standardized
surgical
and analgesic protocols were followed. At the review
appointment, 1 week after surgery, all patients
returned a completed follow-up questionnaire (PoSSe scale) and
were evaluated clinically for postoper-ative pain (number of
painkillers taken) and trismus (differences in mouth opening).
Sixteen predictive
variables were evaluated using stepwise logistic regression
analysis to identify the risk factors associatedwith severe
discomfort.
Results: Severe postoperative discomfort was predicted by these
independent variables: gender,tobacco use, ramus relationship/space
available, and antibiotic prophylaxis. Oral contraceptive use
andoperation time were not identified as risk factors. The patients
perceptions of the severity of symptoms(PoSSe scale score) was
strongly correlated with clinical assessment of trismus (r 0.54)
and pain (r0.42).
Conclusion: The PoSSe scale resulted in a valid and responsive
measure of the severity of symptomsafter surgical extraction of
lower third molars and reflected the clinical severity of the
postoperativediscomfort. From a patients perspective, operative
factors had little bearing on the quality of life after
removal of mandibular third molars.2007 American Association of
Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 65:901-917, 2007
The surgical removal of impacted mandibular third
molars is one of the most commonly performed
dentoalveolar procedures in oral and maxillofacial
surgery and is associated with various postopera-
tive sequelae. Permanent nerve damage and seriousinfections are
the most severe complications fol-lowing third molar extractions,
but the rate of suchcomplications is low.1-4 Pain, trismus, and
swellingare the most common postoperative complaintsand influence
the patients quality of life in the daysfollowing surgery.5,6
Moreover, removal of third
molar is so common that the population morbidityof such minor
complications may be significant.
Surgeons perceptions of the consequences of thirdmolar surgery
on their patients quality of lifeshowsignificant differences from
those of patients.7 Overthe past 3 decades, the use of
patient-centeredoutcome scales in general medicine and surgery
hasincreased substantially, but has only recently beenused in oral
surgery.8,9 To date, there has been littlepublished on patients
perceptions on quality of lifeand risk factors for severe
discomfort after removal
of a third molar.5-7,9-13
Received from the Department of Oral Surgery, School of
Dentistry,
University of Milan, Milan, Italy.
*Clinical Assistant Profesor.
Associate Professor.
Resident.
Resident.
Clinical Assistant Professor.
Department Head.
Address correspondence and reprint requests to Dr Grossi:
Oral
Surgery, School of Dentistry, Istituti Clinici di
Perfezionamento, Via
Commenda n10, 20122 Milano, Italy; e-mail: Giovanni.Grossi@
unimi.it or [email protected]
2007 American Association of Oral and Maxillofacial Surgeons
0278-2391/07/6505-0013$32.00/0
doi:10.1016/j.joms.2005.12.046
901
-
7/21/2019 Battista Grossi G. 2007.pdf
2/17
The aim of this study was:
1) To measure patients perceptions of changes intheir quality of
life after mandibular third molarsurgery with a specific
questionnaire (PoSSescale).13
2) To measure the clinical severity of trismus and
pain (differences in mouth opening and totalanalgesic
consumption).
3) To identify preoperative and intraoperative risk
factors for severe postoperative discomfort.4) To assess the
clinical validity of the PoSSe scale.
Patients and Methods
Between September 2002 and September 2004,at the Oral Surgery
Department, I.C.P. Hospital,University of Milan (Italy), 213
consecutive patients
who had 266 extractions of mandibular third mo-
lars were prospectively studied. Fifty-three patientswho needed
bilateral extractions had their teethremoved on separate occasions
with at least 1month between them. Only 1 lower third molar
was removed at each operation and all teeth werepartially or
completely covered by mucosa. Oneinclusion criterion for this study
was that a muco-periosteal flap was to be raised during the
opera-tion, so 11 molars were excluded from analysis and
a total of 255 mandibular third molars were there-fore available
for analysis.
Participants were healthy individuals with no sys-
temic diseases or history of treatment for psychiat-ric
problems. The patients were not taking anymedications, except for
females who regularly tookoral contraceptives. Exclusion criteria
included pa-tients who were pregnant or lactating. All patients
were free of caries, extensive periodontal disease,
pain, or other inflammatory symptoms at the timeof operation.
Patients who were already taking an-timicrobials or had done so up
to 2 weeks prior
were excluded. Informed written consent was ob-tained from all
patients before they were includedin this study.
DATA COLLECTION
At the initial visit and at the follow-up on the sev-enth
postoperative day, the information was recordedby a single clinical
examiner: the surgeons that hadoperated on the patients were never
involved in thepreoperative or postoperative assessment.
Preoperative Assessment
After consenting to participate in the study, thefollowing data
were recorded: name, age, gender, siteof surgery, current tobacco
and oral contraceptives
use, reasons for seeking third molar removal, and
maximum interincisal distance. Third molar position
was evaluated on the presurgical panoramic radio-graph using
Winters and Pell and Gregory classifica-tion (Table 1).
Patients were scheduled for operation with no cor-relation
between patient and surgeon, so that a ran-dom surgeon operated on
the patient.
Medications
Patients were randomly allocated into 2 groups. Inthe first
group (n 119), prophylactic preoperativeoral antibiotic was
administered with 2 g amoxicillin/clavulanic acid 1 hour before
surgery (Augmentin;GlaxoSmithKline, Verona, Italy). The second
group(n 136) received no antibiotic medication and
served as the control. The surgeons were unawarewhether the
prophylaxis was given or not.
A mouth rinse with 15 mL of 0.2% chlorhexidinesolution
(Dentosan; Pfizer Consumer Healthcare,Rome, Italy) for 1 minute was
used before surgery andimmediately after the operation. The day
after sur-gery, patients began home use of the
chlorhexidinesolution twice a day for 1 week.
Table 1. DESCRIPTIVE STATISTICS FORPREOPERATIVE VARIABLES
Preoperative Variables Category n %
Age (yrs) 22 63 24.7Average (27.04) 2329 117 45.9Range (1467) 29
75 29.4
Gender M 120 47.1
F 135 52.9Tobacco use Yes 76 29.8
No 179 70.2Oral contraceptive
useYes 45 33.3No 90 66.7
Antibiotic prophylaxis Yes 119 46.7No 136 53.3
Indication for removal Infection 79 31.0Periodontal disease 19
7.4Prophylactic removal 80 31.4Orthodontic reason 13 5.1Caries 37
14.5Atypical facial pain 27 10.6
Radiographic findingsNo. of roots Multiple 161 63.1
Singular 90 35.3Incomplete 4 1.6
Spatial relationship Distoangular 52 20.4Horizontal 59
23.2Vertical 72 28.2Mesioangular 72 28.2
Depth Level A (high) 43 16.9Level B (medium) 166 65.1Level C
(deep) 46 18.0
Ramus relationship/space available
Class I (sufficient) 9 3.5Class II (reduced) 217 85.1Class III
(none) 29 11.4
Grossi et al. Assessing Discomfort After Third Molar Surgery.J
Oral Maxillofac Surg 2007.
902 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
3/17
Oral Coefferalgan (paracetamol 500 mg with co-deine 30 mg;
Bristol-Myers Squibb, Sermoneta, Italy)
was immediately given after the surgery and was pre-scribed to
be taken as required for pain relief (maxi-mum, 6 tablets daily).
Patients were instructed not totake any drugs other than those
prescribed and not to
seek medical help elsewhere for postoperative prob-lems.
Surgery
A total of 3 surgeons with more than 5 yearsdentoalveolar
training, assisted by training house sur-geons, performed the
surgeries. Each patient had sim-
ilar surgical procedures, in the same operating roomand under
similar conditions, using mepivacaine 2%
with epinephrine 1:100.000 as local anesthetic (2%Carbocaine;
AstraZeneca, Milan, Italy). No concomi-
tant medication was used during surgery other thanthe local
anesthetic. Access to the third molar wasachieved from the buccal
aspect and bone was re-moved with a round bur in a straight
handpiece under
continuous irrigation with sterile saline solution. Ifnecessary,
sectioning of crown and roots was per-formed with a fissure bur.
After tooth extraction, thealveolus was inspected, curetted for
granulation tis-sue removal, and irrigated with sterile saline
solution.
A 4/0 silk suture was used to close the wound without
tension. An ice pack was then applied to the patientsface for 20
minutes.
Immediately after the operation, details of the pro-cedure were
recorded, including the duration of sur-gery in minutes (from the
first incision to insertion ofthe last suture) (Table 2).
Patients were given the usual postoperative instruc-
tions and received 2 questionnaires, after being in-
structed in their use: the PoSSe scale13 and a 9-point
scale to record pain levels.14
Postoperative Assessment
All patients returned 1 week after the operation to
have their sutures removed: the examiner was the
same as the one who assessed them preoperatively.Trismus was
assessed by measuring the differences
in mouth opening (interincisal distance preopera-
tively and on postsurgery day 7).
The patients pain level were assessed with a
9-point visual analog scale anchored by the verbal
descriptors no pain (point 0) and very severe pain
(point 8).14 Patients were advised to take the analge-
sic tablet as soon as their pain reached a moderate
level. They were asked to enter their pain level and
the time at which the analgesic was taken, and then
make no further recordings.
The PoSSe scale13
was designed to assess the pa-tients perception of adverse
effects in 7 subscales:
eating, speech, sensation, appearance, pain, sickness,
and interference with daily activities. A score was
assigned to the possible responses to each forced
question. The scores of the responses to each ques-
tion were summed. These scores represent a percent-
age, so that a patient completing the questionnaire
and ticking the most severe response category for
each question would score 100%. A patient ticking
the least severe response category for each question
would score 0%.
Table 2. DESCRIPTIVE STATISTICS FOR OPERATIVE VARIABLES
Operative Variables Category n %
Surgeon 1 50 19.62 124 48.63 81 31.8
Assistant surgeon Clinical dental student 133 52.2
Resident 78 30.6Specialist training 44 17.2
Flap design Envelope flap 59 23.1Vestibular triangular flap 48
18.9Vestibular trapezoidal flap 148 58.0
Bone removal Yes 200 78.4No 55 21.6
Extraction difficulty Elevator/forceps alone 49 19.2Bone
removal/tooth sectioning 46 18.0Bone removal tooth/root sectioning
129 50.6Extremely difficult 31 12.2
Operation time (min) 10 49 19.21120 83 32.52130 69 27.130 54
21.2
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
GROSSI ET AL 903
-
7/21/2019 Battista Grossi G. 2007.pdf
4/17
Table 3. DESCRIPTIVE STATISTICS AND ANALYSIS OF VARIANCE (1-WAY
ANOVA) OF INDEPENDENT VARIABLESVERSUS FULL POSSESCALE
Independent Variables (Preoperative andOperative)
Dependent Variable Full PoSSe Scale
PValueRange (min) Range (max) Mean Median
Age (yrs)22 7.13 61.88 32.70 33.38 .092329 5.11 81.65 36.12
34.4829 5.38 67.93 37.64 35.83
GenderM 7.13 67.89 33.62 33.09 .01F 5.11 81.65 37.59 37.09
Tobacco useYes 9.91 67.89 37.76 36.35 .11No 5.11 81.65 34.85
33.62
Oral contraceptive useYes 5.11 60.88 34.88 36.01 .11No 5.38
81.65 38.95 37.60
Antibiotic prophylaxisYes 5.38 62.64 32.89 31.61 .001No 5.11
81.65 38.20 37.01
Indication for removalInfection 11.21 81.65 36.16 35.09
.78Periodontal disease 15.74 62.64 35.70 32.27Prophylactic removal
5.11 66.28 35.97 35.78Orthodontics reason 20.49 67.93 38.62
38.59Caries 5.38 60.88 32.83 32.16Atypical facial pain 14.81 60.64
36.27 33.46
Number of rootsMultiple 5.11 67.93 35.34 34.46 .75Singular 7.13
81.65 36.51 35.75Incomplete 20.49 44.79 33.23 33.82
Spatial relationshipDistoangular 14.97 81.65 38.28 36.34
.44Horizontal 5.38 64.16 34.22 33.62Vertical 5.11 67.89 35.61
34.60
Mesioangular 7.13 61.88 35.21 34.07DepthLevel A (high) 11.21
55.04 32.72 30.99 .27Level B (medium) 5.11 81.65 36.46 35.59Level C
(deep) 7.13 62.64 35.84 35.94
Ramus relationship/space availableClass I (sufficient) 17.87
41.13 31.22 33.46 .002Class II (reduced) 5.11 81.65 34.85
33.62Class III (none) 25.59 67.93 43.60 43.52
Surgeon1 7.13 62.64 32.56 31.35 .062 8.01 81.65 37.62 35.783
5.11 67.93 34.76 33.83
Assistant surgeonClinical dental student 7.13 81.65 35.70 34.43
.70
Resident 8.01 67.89 36.51 35.40Specialist training 5.11 67.93
34.38 33.49
Flap designEnvelope flap 5.11 56.46 32.07 31.41 .06Vestibular
triangular flap 9.01 67.93 36.80 35.77Vestibular trapezoidal flap
5.38 81.65 36.82 34.56
Bone removalYes 5.38 81.65 36.80 34.68 .01No 5.11 56.46 31.78
32.02
Extraction difficultyElevator/forceps alone 5.11 56.46 31.97
32.02 .11Bone removal/tooth sectioning 10.27 81.65 38.29 35.70Bone
removal tooth/root sectioning 5.38 67.93 35.79 34.43Extremely
difficult 7.13 62.64 37.55 36.01
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
904 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
5/17
Study Variables, Data Management,
and Analysis
The set of predictor variables was divided into 2groups:
preoperative and operative variables (Tables1and 2).
The outcome variables were:
1) PoSSe score (derived from the PoSSe scale byadding the
responses to each of the individualquestions).
2) Trismus (range of opening measured preopera-tively and on
postsurgery day 7).
3) Pain (total analgesic consumption).
Data were entered into a spreadsheet (Excel; Mi-
crosoft, Inc, Redmond, WA) over the course of thestudy. With use
of a statistical software package (SPSSfor Windows, version 12.0;
SPSS Inc, Chicago, IL,
2003), descriptive statistics were computed for all ofthe study
variables.All pertinent data were subsequently analyzed with
the 1-sample Kolmogorov-Smirnov test with respectto
normality.
According to normality, initial statistical analyses
used parametric (1-way ANOVA) or nonparametrictest
(Mann-WhitneyUtest or Kruskal-Wallis rank test)to measure the
association between each predictor
variable (preoperative and operative) and outcomevariables (full
PoSSe score, single PoSSe subscales,Trismus, and Pain). To measure
the association be-tween the predictor and outcome variables while
con-
trolling for confounders, a logistic regression modelwas used.
Biologically relevant variables (age and gen-
der) and variables that had P .20 in the initialanalyses were
entered into logistic regression modelas independent variables. All
parameters used as out-come variables were dichotomized before
enteringthe logistic regression: scores with a value of themedian
value were recorded as 0, those of themedian value were recorded as
1. The data wereallowed to enter the model using backward
selection
with the significance level to remove set at 0.1. Pear-
son 2 test was performed to test the goodness of fit
of the final model. Spearmans rank correlation coef-ficient was
used to assess the correlation between theoutcome variables.
A value of P .05 was accepted as statisticallysignificant.
Results
Two hundred fifty-five patients (135 females, 120males) aged 14
to 67 years (average, 27.04 years)representing 255 extraction sites
of mandibular thirdmolars were entered into this study. The
descriptivestatistics for the sample are summarized in Tables
1and2.
RISK FACTORS FOR SEVERE DISCOMFORT
(MEASURED WITH THE POSSESCALE)
The mean PoSSe score (SD) was 35.72 13.54
(range, 5.1181.65). The results of descriptive statis-tics and
of analysis of variance are shown in Table 3.The logistic
regression analysis revealed risk factors
for severe discomfort (Table 4). Only 4 out of 16independent
variables, all preoperative, were signifi-cant indicators for
severe discomfort: gender, tobacco
use, antibiotic prophylaxis, and ramus relationship/space
available.
Females had twice the odds of males of severediscomfort (odds
ratio [OR] 2.07; P .01). Espe-cially, females were found to be at 6
times higherrisk of feeling sickness (OR 6.20; P .000) thanmales,
and had a 2 to 2.5 times higher risk of
experiencing interference with daily activities,problems in
eating and speaking, and changes of
appearance (Table 5).Smokers were found to have a higher risk
for re-
porting more severe discomfort (OR 1.86; P .04),Patients who did
not receive prophylactic antibioticsalso reported more discomfort
(OR 2.05; P .007).
Finally, when evaluating the radiographic findings,the ramus
relationship/space available was the only
variable found to increase the risk of severe discom-fort. If
the third molar had insufficient space available
in relation to the ramus it was more likely that the
Table 3. (Contd)
Independent Variables (Preoperative andOperative)
Dependent Variable Full PoSSe Scale
PValueRange (min) Range (max) Mean Median
Operation time (min)10 5.11 81.65 33.05 32.76 .491120 5.38 67.93
36.08 34.432130 9.91 60.88 36.44 35.5630 7.13 62.64 36.67 34.45
Total 5.11 81.65 35.72 34.46
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
GROSSI ET AL 905
-
7/21/2019 Battista Grossi G. 2007.pdf
6/17
patient scored high on the PoSSe scale than if thethird molar
had sufficient space available (Class III,
OR 6.24, P .04; Class II, OR 2.18, P .34).
RISK FACTORS FOR TRISMUS
The mean difference of mouth opening (SD) was8.9 mm 8.2 (range,
0.036.0). Details of descriptivestatistics and nonparametric tests
are shown inTable 6.
Like that found in the precedent logistic regressionmodel,
gender, antibiotic prophylaxis, smoking hab-its, and ramus
relationship/space available werestatistically significant
predictors of severe trismus(Table 7). Moreover, in this model
there was a higherrisk of trismus if the molar was deeply impacted
orthe patients were over 23 years of age.
Finally, 2 operative variables were found to bestatistically
significant predictors of the occurrence of
severe trismus: bone removal and surgeon.
RISK FACTORS FOR PAIN
The mean number of analgesic tablets taken post-
operatively (SD) was 5.2 4.3 (range, 0.021.0).Details of
descriptive statistics and nonparametric
tests are shown inTable 8.
The only significant preoperative indicator for se-
vere postoperative pain was antibiotic prophylaxis
(Table 9): patients who received no antibiotic medi-
cation were found to have a higher risk for analgesic
consumption than those who received prophylaxis
(OR 2.20; P .005).
Two operative variables were found to be an
indicator for postoperative pain. When surgery was
perceived as being extremely difficult and a trape-
zoidal flap was raised, the patients had approxi-mately 3 times
the odds of feeling severe postoper-
ative pain.
Table 4. RISK FACTORS FOR SEVERE DISCOMFORT (INDEPENDENT
VARIABLES VERSUS FULL P OSSESCALE)
Independent Variables CategoryTotalNo.
PoSSe 0No.
PoSSe 1No. Odds Ratio CI 95% PValue
Gender M 120 73 47 1.00 1.183.60 .01F 135 65 70 2.07
Tobacco use No 179 102 77 1.00 1.023.40 .04
Yes 76 36 40 1.86Antibiotic prophylaxis Yes 119 75 44 1.00
1.213.45 .007
No 136 63 73 2.05Ramus relationship/
space availableClass I (sufficient) 9 7 2 1.00 0.4211.19
.34Class II (reduced) 217 121 96 2.18 1.0437.47 .04Class III (none)
29 10 19 6.24
NOTE. Logistic regression analysis: backward selection
(P-to-remove: 0.1); goodness of fit: Pearson 2 test 186.50 (P .28).
Odds ratio, 95%confidence intervals (CI) and Pvalues.
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
Table 5. RISK FACTORS FOR SEVERE DISCOMFORT (INDEPENDENT
VARIABLES VS EACH P OSSESUBSCALE-GENDER)
PoSSe Subscales Category TotalNo.
PoSSe 0No.
PoSSe 1No. Odds Ratio CI 95% PValue
Eating M 120 71 49 1.00F 135 63 72 2.40 1.374.20 .002
Speech M 120 74 46 1.00
F 135 66 69 2.02 1.183.45 .01Sensation M 120 85 35 NSF 135 93
42
Appearance M 120 65 55 1.00F 135 60 75 2.52 1.404.55 .002
Pain M 120 63 57 NSF 135 65 70
Sickness M 120 109 11 1.00F 135 83 52 6.20 3.0512.63 .000
Interference with daily activities M 120 68 52 1.00F 135 52 83
2.08 1.263.44 .004
NOTE. The table shows the gender-related odds
ratio.Abbreviation: NS, the independent variable was not a
statistically significant predictor of severe discomfort.
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
906 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
7/17
Table 6. DESCRIPTIVE STATISTICS AND LEVELS OF SIGNIFICANCE
(INDEPENDENT VARIABLES VS TRISMUS)
Independent Variables (Preoperative andOperative)
Dependent Variable Trismus (Differencein Mouth Opening in
mm)
Kruskal-WallisRank Test
Mann-WhitneyUTest
Range (min) Range (max) Mean Median PValue PValue
Age (yrs)22 0.0 35.0 6.5 5.0 .0022329 0.0 35.0 9.0 7.029 0.0
36.0 10.6 8.0
GenderM 0.0 36.0 8.8 5.5 .40F 0.0 31.0 8.9 7.0
Tobacco useYes 0.0 35.0 10.2 8.0 .18No 0.0 36.0 8.3 6.0
Oral contraceptive useYes 0.0 30.0 7.3 5.0 .02No 0.0 31.0 9.8
8.0
Antibiotic prophylaxisYes 0.0 25.0 6.8 5.0 .001No 0.0 36.0 10.8
8.0
Indication for removalInfection 0.0 31.0 9.1 7.0 .36Periodontal
disease 0.0 36.0 9.3 6.0Prophylactic removal 0.0 35.0 9.4
7.0Orthodontics reason 0.0 25.0 11.6 11.0Caries 0.0 33.0 6.4
5.0Atypical facial pain 0.0 30.0 8.6 6.0
Number of rootsMultiple 0.0 36.0 9.3 7.0 .53Singular 0.0 31.0
8.1 6.0Incomplete 0.0 24.0 10.7 9.5
Spatial relationshipDistoangular 0.0 35.0 10.1 7.5 .70Horizontal
0.0 33.0 9.0 7.0Vertical 0.0 31.0 8.1 5.5
Mesioangular 0.0 36.0 8.7 6.0Depth
Level A (high) 0.0 25.0 5.9 5.0 .02Level B (medium) 0.0 36.0 9.7
7.0Level C (deep) 0.0 30.0 8.7 7.0
Ramus relationship/space availableClass I (sufficient) 0.0 13.0
4.5 5.0 .0008Class II (reduced) 0.0 35.0 8.5 6.0Class III (none)
2.0 36.0 13.1 12.0
Surgeon1 0.0 36.0 6.7 4.5 .042 0.0 35.0 9.4 7.03 0.0 35.0 9.4
7.0
Assistant surgeonClinical dental student 0.0 33.0 7.6 6.0
.04
Resident 0.0 36.0 11.1 7.5Specialist training 0.0 35.0 8.8
5.5
Flap designEnvelope flap 0.0 26.0 6.3 5.0 .009Vestibular
triangular flap 0.0 35.0 10.6 6.5Vestibular trapezoidal flap 0.0
36.0 9.3 7.0
Bone removalYes 0.0 36.0 9.8 7.0 .0001No 0.0 26.0 5.5 3.0
Extraction difficultyElevator/forceps alone 0.0 26.0 5.9 5.0
.01Bone removal/tooth sectioning 0.0 31.0 9.0 6.0Bone removal
tooth/root sectioning 0.0 36.0 9.5 7.0Extremely difficult 0.0 35.0
10.7 8.0
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
GROSSI ET AL 907
-
7/21/2019 Battista Grossi G. 2007.pdf
8/17
VALIDATION OF THE POSSESCALE
The patients score on the PoSSe scale had signif-icant positive
correlations with both differences inmouth opening (r 0.54) and
total analgesic con-sumption (r 0.41) (Table 10). Correlations
be-
tween the 7 PoSSe subscales and the 2 clinical
dependent variables are shown in Table 10. Thetotal analgesic
consumption consistently gavestronger correlations with the pain
subscale thanthe other (r 0.60). Similarly, differences in
mouthopening strongly correlated with the eating sub-scale (r
0.53). Table 11 shows the correlationsbetween the subscale scores
and the overall PoSSescore.
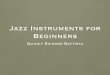
Figures 1through4 show the impact of gender onoutcome variables
when such independent variablesinteract with other risk
factors.
Table 12provides an overview of the risk factors fora severe
discomfort found in this study. The antibioticprophylaxis was the
only variable found statistically sig-nificant in all 3 regression
logistic models of this study.
DiscussionMuch has been written about the relationships be-
tween the postoperative morbidity after surgical re-moval of
lower third molars and preoperative riskfactors. However, little
has been published on thepatients perceptions on quality of life
after this op-eration. Moreover, most of these studies have
testedthe individual variables isolated without adjusting for
the other potential risk indicators, several reportingonly
descriptive data, making interpretation difficultbecause of
inadequate analyses.
Table 6. (Contd)
Independent Variables (Preoperative andOperative)
Dependent Variable Trismus (Differencein Mouth Opening in
mm)
Kruskal-WallisRank Test
Mann-WhitneyUTest
Range (min) Range (max) Mean Median PValue PValue
Operation time (min)10 0.0 31.0 6.7 5.0 .071120 0.0 35.0 9.0
5.02130 0.0 31.0 9.0 7.030 0.0 36.0 10.6 8.5
Total 0.0 36.0 8.9 6.0
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
Table 7. RISK FACTORS FOR SEVERE TRISMUS
Independent Variables CategoryTotalNo.
PoSSe 0No.
PoSSe 1No. Odds Ratio CI 95% PValue
Age (yrs) 22 63 47 16 1.002329 117 70 47 2.93 1.316.56 .00929 75
39 36 3.23 1.387.58 .007
Gender M 120 79 41 1.00F 135 77 58 3.04 1.555.96 .001
Tobacco use No 179 115 64 1.00Yes 76 41 35 2.14 1.094.22 .02
Antibiotic prophylaxis Yes 119 85 34 1.00No 136 71 65 3.11
1.675.78 .000
Depth Level A (high) 43 35 8 1.00Level B (medium) 166 93 73 3.15
1.228.14 .01Level C (deep) 46 28 18 2.45 0.787.64 .12
Ramus relationship/spaceavailable
Class I (sufficient) 9 8 1 1.00Class II (reduced) 217 138 79
1.48 0.1514.04 .72Class III (none) 29 10 19 6.52 0.5971.88 .12
Surgeon 1 50 39 11 1.002 124 71 53 3.53 1.468.51 .0053 81 46 35
3.77 1.489.61 .005
Bone removal No 55 45 10 1.00Yes 200 111 89 3.95 1.669.41
.002
NOTE. Logistic regression analysis: backward selection
(P-to-remove: 0.1); goodness of fit: Pearson 2 test 234.07 (P .32).
Odds ratio, 95%confidence intervals (CI) and Pvalues.
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
908 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
http://-/?-http://-/?-
-
7/21/2019 Battista Grossi G. 2007.pdf
9/17
Table 8. DESCRIPTIVE STATISTICS AND LEVELS OF SIGNIFICANCE
(INDEPENDENT VARIABLES VS PAIN)
Independent Variables (Preoperative andOperative)
Dependent Variable-Pain (No. ofPainkillers Taken)
Kruskal-WallisRank Test
Mann-WhitneyUTest
Range (min) Range ( max) Mean Median PValue PValue
Age (yrs)22 0.0 21.0 4.0 2.0 .012329 0.0 18.0 5.5 4.029 0.0 17.0
5.7 5.0
GenderM 0.0 21.0 5.5 4.0 .21F 0.0 17.0 4.9 4.0
Tobacco useYes 0.0 21.0 6.2 5.0 .002No 0.0 18.0 4.8 3.0
Oral contraceptive useYes 0.0 17.0 5.3 4.0 .41No 0.0 16.0 4.7
3.0
Antibiotic prophylaxisYes 0.0 18.0 4.7 4.0 .20No 0.0 21.0 5.6
4.5
Indication for removalInfection 0.0 16.0 4.8 4.0 .77Periodontal
disease 0.0 12.0 4.4 3.0Prophylactic removal 0.0 21.0 6.0
5.0Orthodontics reason 1.0 11.0 5.4 5.0Caries 0.0 14.0 5.1
3.0Atypical facial pain 0.0 17.0 4.8 3.0
No. of rootsMultiple 0.0 21.0 5.2 4.0 .55Singular 0.0 16.0 5.1
3.0Incomplete 2.0 9.0 6.5 7.5
Spatial relationshipDistoangular 0.0 16.0 6.6 6.0 .04Horizontal
0.0 14.0 4.7 4.0Vertical 0.0 14.0 4.4 3.5
Mesioangular 0.0 21.0 5.4 3.5Depth
Level A (high) 0.0 13.0 4.6 3.0 .75Level B (medium) 0.0 21.0 5.3
4.0Level C (deep) 0.0 18.0 5.4 4.0
Ramus relationship/space availableClass I (sufficient) 0.0 9.0
3.3 3.0 .07Class II (reduced) 0.0 21.0 5.1 4.0Class III (none) 1.0
18.0 6.5 6.0
Surgeon1 0.0 11.0 3.9 3.0 .0022 0.0 21.0 6.1 5.03 0.0 14.0 4.6
3.0
Assistant surgeonClinical dental student 0.0 18.0 5.3 4.0
.78
Resident 0.0 21.0 5.1 4.0Specialist training 0.0 14.0 5.0
4.0
Flap designEnvelope flap 0.0 14.0 4.9 3.0 .009Vestibular
triangular flap 0.0 14.0 4.2 3.0Vestibular trapezoidal flap 0.0
21.0 5.6 4.0
Bone removalYes 0.0 21.0 5.2 4.0 .91No 0.0 14.0 5.2 4.0
Extraction difficultyElevator/forceps alone 0.0 14.0 5.3 4.0
.10Bone removal/tooth sectioning 0.0 12.0 4.1 3.0Bone removal
tooth/root sectioning 0.0 17.0 5.1 4.0Extremely difficult 0.0 21.0
6.9 6.0
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
GROSSI ET AL 909
-
7/21/2019 Battista Grossi G. 2007.pdf
10/17
The following describes the outcomes of the studyand how our
findings might influence the outcome ofpreviously published studies
on risk factors for com-plications after third molar surgery.
PREOPERATIVE RISK FACTORS
Age
Removal of impacted third molar should not be
considered the best model for studying the age-re-lated
differences because such operation is usuallycarried out on
teenagers and young adults. However,it is commonly thought that
older patients are atgreater risk for complications after third
molar sur-gery.3,15,16
In our study, the patients age was found to be arisk factor only
for severe trismus; that is, patientsaged 22.0 years were found to
have a lower risk
than older patients.
Recently, Benediktsdttir et al17 studied the riskindicators for
postoperative complications after re-moval of 388 mandibular third
molars: older age (23
years) was found to increase the risk of an extendedoperation
time (10 minutes), but operation time
itself was not found to be a risk indicator for postop-
erative complications. In the present study, after ad-
justment for other risk factors, no significant associa-
tion was found between age and the PoSSe score or
total painkillers consumption. This means that older
patients are at greater risk of severe trismus after third
molar surgery, but younger patients have the same
odds of perceiving severe discomfort and pain. If
other similar studies confirm these data, it will likely
be wrong to advocate the early prophylactic removal
of the lower third molar claiming lower risk of post-
operative discomfort.
Gender
There is general agreement that women and men
perceive and respond differently to pain stimuli.18-20
Moreover, biologic differences exist between men
and women that can result in differences in responses
to drugs.21-26
The most common finding after removal of third
molar is that women reported more postsurgical pain
that men.11,12,14,17 In contrast, Capuzzi et al,27 in 146
patients having third molar surgery, reported that
Table 8. (Contd)
Independent Variables (Preoperative andOperative)
Dependent Variable-Pain (No. ofPainkillers Taken)
Kruskal-WallisRank Test
Mann-WhitneyUTest
Range (min) Range ( max) Mean Median PValue PValue
Operation time (min)10 0.0 12.0 5.0 4.0 .731120 0.0 17.0 5.0
3.02130 0.0 16.0 4.9 4.030 0.0 21.0 6.0 4.5
Total 0.0 21.0 5.2 4.0
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
Table 9. RISK FACTORS FOR SEVERE PAIN (NUMBER OF PAINKILLERS
TAKEN)
Independent Variables Category
Pain (No. of PainkillersTaken)
Odds Ratio CI 95% PValueTotal
No.
PoSSe 0
No.
PoSSe 1
No.
Antibiotic prophylaxis Yes 119 80 39 1.00No 136 74 62 2.20
1.273.81 .005
Flap design Envelope flap 59 35 24 1.87 0.695.09 .21Vestibular
triangular flap 48 35 13 1.00Vestibular trapezoidal flap 148 84 64
2.87 1.326.24 .007
Extraction difficulty Elevator/forceps alone 49 27 22 2.42
0.866.82 .09Bone removal/tooth sectioning 46 32 14 1.00Bone removal
tooth/root
sectioning129 82 47 1.34 0.632.85 .44
Extremely difficult 31 13 18 3.32 1.248.91 .01
NOTE. Logistic regression analysis: backward selection
(P-to-remove: 0.1); goodness of fit: Pearson 2 test 235.45 (P .20).
Odds ratio, 95%confidence intervals (CI) and Pvalues.
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
910 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
11/17
there was no gender-related differences in regard tothe number
of analgesic tablets taken.
In the present study, gender was not found to be arisk factor
for objectively measured pain (total pain-killer consumption), or
for subjectively measured
pain (pain subscale score).On the other hand, among our cohort
of patients,
females had more than 3 times higher risk for severe
trismus compared with males, and thesefindings arein agreement
with previous studies.11,12
For gender differences in symptom reporting, thedata show that
females had twice the odds of males ofperceiving a severe
postoperative discomfort (fullPoSSe score). Especially, except
forpain and sensa-tion subscales that have not shown differences to
begender-related, females were found to complain morethan males
about sickness (OR 6.2; P .000),appearance (OR 2.52; P .002),
eating (OR 2.40; P 0.002), speech (OR 2.0; P .01) andinterference
with daily activities (OR 2.0; P .004) (Table 5).
It can be proposed that the strong gender-relateddifference
found for sicknessmay be attributable to
the type of painkiller prescribed in our study,
acodeine-combined drug. In fact, it was shown that
women had 60% higher risk of nausea and vomitingthan men when
taking opioid agonists, althoughefficacy did not differ between the
2 groups.28
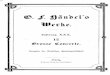
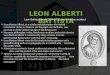
Finally, it seems that some risk factors increasegender
differences. Smoking appears to increasethe PoSSe score and the
total painkiller consump-tion in females much more than in males
(Figs 1and
4). Women are less likely than men to benefit from
antibiotic prophylaxis (Fig 2), and are more likely
than men to perceive severe discomfort when athird molar with no
space available was removed(Fig 3).
It is commonly believed that situational and psy-chological
factors can play a major role in symptomperception and that the
gender differences cannot
simply be attributed to a greater physical morbidityin women.
Contrary to popular belief, recent studiesindicate that when an
actual illness or disease is present,
however minor and transient, men and women areeither equally
likely to report related symptoms, ormen report more severe
symptoms.29
However, being male or female is an importantfundamental
variable that should be considered whendesigning and analyzing the
results of studies in allareas and at all levels of biomedical and
health-relatedresearch. Therefore, subjects who have lower
thirdmolars extracted should not be viewed as a uniform
population when postoperative discomfort is evalu-ated, but
should be stratified by gender.
Such data in relation to gender differences mayhelp surgeons to
counsel female patients about recov-ery after third molar surgery
and will enhance theinformed consent procedures.
Tobacco Use
Smoking has been shown to have a deleteriouseffect on the oral
cavity and has been associated withpostoperative complications
after oral surgery.30-35
In the present study, patients who smoke werefound to have a
higher risk for perceiving more severe
postoperative discomfort (OR 1.86; P .04) andtrismus (OR 2.14; P
.02).
It was shown that women who smoke are morelikely to develop
diseases than men.36 This is consis-tent with our finding that
smoking appears to en-hance gender differences in PoSSe score (Fig
1).
Interestingly, it has been reported that nicotineincreases the
pain threshold and tolerance rating of
Table 11. SPEARMANS CORRELATION COEFFICIENTTO ASSESS CORRELATION
BETWEEN THE POSSE
SCALE AND SUBSCALES
Subscale Full PoSSe
Eating 0.83*Speech 0.65*Sensation 0.37*Appearance 0.54*Pain
0.67*Sickness 0.35*Interference with daily activities 0.71*
*P .01.
Grossi et al. Assessing Discomfort After Third Molar Surgery.J
Oral Maxillofac Surg 2007.
Table 10. VALIDITY TESTING, SPEARMANSCORRELATION COEFFICIENT TO
ASSESSCORRELATION BETWEEN THE POSSESCALE, POSSESUBSCALES, AND THE
TWO CLINICAL DEPENDENTVARIABLES (TRISMUS AND PAIN)
Subjective DependentVariable
Objective DependentVariable
Pain (No. of Painkillers
Taken) Trismus
Full PoSSe 0.41** 0.54**Eating 0.26** 0.53**Speech 0.21**
0.34**Sensation 0.11 0.10Appearance 0.13* 0.41**Pain 0.60**
0.30**Sickness 0.05 0.18**Interference with daily
activities 0.29** 0.38**
*P .05.**P .01.
Grossi et al. Assessing Discomfort After Third Molar Surgery.J
Oral Maxillofac Surg 2007.
GROSSI ET AL 911
-
7/21/2019 Battista Grossi G. 2007.pdf
12/17
men, but has no effect on the pain rating of women.37
These findings can be an explanation of why smokersas a whole in
this study were not found at higher riskfor pain and why female
smokers consumed morepainkillers than male smokers (Fig 4).
Oral Contraceptive Use
Numerous studies reported increased complica-tions among females
associated with oral contracep-tive use.35,38-41 However, most of
these studies have
not been optimally designed or analyzed to removethe effects of
various known confounders. This study
fails to confirm the hypothesis that oral contraceptiveuse is a
risk factor for severe postoperative discom-fort, which is
consistent with other studies.16,33,42
However, data on the menstrual cycle of the womenwere not
gathered. Therefore, these findings shouldbe interpreted with
caution and further studies areneeded to consider the endocrine
status of subjects inanalyses.
Antibiotic Prophylaxis
The routine use of systemic preoperative and/orpostoperative
antibacterial given prophylactically is
FIGURE 1. Relationship between gender*tobacco use versus full
PoSSe score.
Grossi et al. Assessing Discomfort AfterThird Molar Surgery. J
Oral Maxillofac Surg2007.
FIGURE 2. Relationship between gender*antibiotic prophylaxis
versus full PoSSe score.
Grossi et al. Assessing Discomfort AfterThird Molar Surgery. J
Oral Maxillofac Surg2007.
912 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
13/17
highly disputed and by many considered to be con-troversial
because of the development of resistant
bacterial strains and possible systemic side effects,such as
hypersensitivity and unnecessary destructionof host flora.43-45
Several studies have shown that postoperative oralprophylactic
antibiotic treatment after the removal oflower third molars does
not contribute to a better
wound healing, less pain, or increased mouth open-
ing.27,46,47 In contrast, Delilbasi et al48 reported
someevidence of the benefit of postoperative antibiotic for
the prevention of alveolar osteitis. However, surgicalprinciples
dictate that if preventive antibiotics are
given to improve recovery, the drug should be admin-istered just
before surgery at a sufficient dosage toensure adequate blood and
tissue levels, and discontin-ued after surgery.44,49,50
Nevertheless, Sekhar et al51
failed to show any advantage in the routine preoper-ative or
postoperative use of metronidazole duringremoval of third
molars.
In this study, preoperative antibiotic prophylaxiswas found to
be the only independent variable statis-
FIGURE 3. Relationship between gender*ramus relationship/space
available versus fullPoSSe score.
Grossi et al. Assessing Discomfort AfterThird Molar Surgery. J
Oral Maxillofac Surg2007.
FIGURE 4. Relationship between gender*tobacco use versus number
of painkillers taken.
Grossi et al. Assessing Discomfort AfterThird Molar Surgery. J
Oral Maxillofac Surg2007.
GROSSI ET AL 913
-
7/21/2019 Battista Grossi G. 2007.pdf
14/17
tically significant (P .01) versus all outcome vari-ables
studied (Table 12).
Of note, women looked less likely than men tobenefit from
antibiotic prophylaxis (Fig 2). This find-ing could be explained by
the gender differences inpharmacokinetics and pharmacodynamics.52
Aboveall, gender differences in hepatic enzymes seem toplay a major
role in determining pharmacokinetic
variability by gender.22,52,53 Amoxicillin/clavulanicacid was
used as a prophylactic antibiotic treatment.
It was reported that erythromycin is cleared morerapidly in
women than men,52 and there may be a
common metabolic pathway forboth amoxicillin/cla-vulanic acid
and erythromycin.54 Moreover, it wasshown that men are much more
frequently affectedby amoxicillin/clavulanic acid-induced hepatitis
than
women (male to female ratio, 4:1) and it is likely
thatclavulanic acid is responsible for the hepatotoxicity.54
It can be hypothesized that when clavulanic acid was
given to females, because of the faster hepatic metabo-lism, it
cannot provide enough anti--lactamase activitycapable to enhance
the activity of amoxicillin. However,these findings have not been
confirmed in the literatureand further studies are needed.
Indication for RemovalIt has been suggested that the presence of
symp-
toms at the time of mandibular third molar removalmust be
consideredto be a risk factor for postopera-tive complications55 or
delay of wound healing.12 Inthe present study, we fail to confirm
this hypothesis,perhaps because all patients in this study were
free ofcaries, extensive periodontal disease, pain, or other
inflammatory symptoms at the time of operation.
Radiographic Findings
Classically, the assessment of difficulty of extrac-tion has
been based on angulation, depth of impac-
tion, ramus, and occlusal positions. Bui et al16
re-ported that mesioangular impactions were associated
with a higher risk forpostoperative complications;whereas Yuasa
et al56 found that depth and ramusrelationship/space available were
associated with dif-ficulty in extraction. We found that deeply
impactedmolar and insufficient space available in relation tothe
ramus were risk factors for severe postoperativediscomfort.
Different than operative variables (ie, operative
time and extraction difficulty), information gatheredfrom a
panoramic radiograph can help the surgeon
plan the surgery and inform the patient of the likeli-hood of
postoperative complications.
Operative Risk Factors
Many studies have emphasized that operative fac-tors were strong
indicators for postoperative compli-cations.
From the patients perspective, in this study noneof the
operative variables were found to be risk fac-tors for severe
discomfort (PoSSe score). If these dataare confirmed, the clinician
could counsel a patientbefore surgery about their outcome, with
only a slight
chance that an event at surgery would drastically alter
what was advised presurgically.Flap Design
There are very few specific data available from the
literature regarding postoperative flap-related discom-fort. In
this study, the triangular flap design was asso-ciated with those
consuming the least painkillers.
When a trapezoidal flap was raised the patients hadapproximately
3 times the odds of taking an above-average number of painkillers.
Of note, although sur-geons in this study used an envelope flap
technique
when the lower third molar surgery was expected tobe easy, when
access was achieved with such a flap
Table 12. OVERVIEW OF POSSIBLE RISK FACTORS
Dependent Variable
Preoperative Independent Variable Operative Independent
Variable
AGE
GENDER
TOBACCO
USE
ORALCONTRA
CEPTIVEUSE
ANTIBIOTICPROPHYLAXIS
INDICATIONF
ORREMOVAL
NUMBEROFR
OOTS
SPATIALRELATIONSHIP
DEPTH
RAMUSRELATIONSHIP
SURGEON
ASSISTANTSURGEON
FLAPDESIGN
BONEREMOVAL
EXTRACTION
DIFFICULTY
OPERATIONTIME
Trismus No. of painkillers taken Full PoSSe score
, Statistically significant predictor.
Grossi et al. Assessing Discomfort After Third Molar Surgery. J
Oral Maxillofac Surg 2007.
914 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
15/17
patients had almost twice the odds of consuming
more painkillers than when a triangular flap was used.These
findings are consistent with those from Jakseet al,57 who stated
that the envelope flap has a nearly6 times higher risk of
dehiscence during primary
wound healing than the triangular flap. These
authorshypothesized that soft tissue tensions resulting from
postoperative hematoma and masticatory movementsmay induce a
rupture of the wound margin during thefirst few postoperative days.
This would be more
likely when envelope flap is raised because it is
fixedanteriorly with intersulcular sutures.
Extraction Difficulty
It is commonly thought that there is a relationshipbetween
operative trauma and the magnitude of post-operative pain, and that
the amount of mucoperios-teum that has to be reflected and of bone
that has tobe removed affect the severity of postoperative pain
and swelling.
55
Evaluating the odds of consumingpainkillers, data from the
present study confirm thishypothesis (except for removal with
elevator/forcepsalone, which had higher odds for severe pain
than
bone removal/tooth root sectioning). It may be sug-gested that
sometimes raising a small flap withoutbone removal and/or
tooth/root sectioning is not agood idea, causing patients to suffer
more severe painpresumably because of the excessive soft tissue
dam-age and delayed wound healing.
However, extraction difficulty was not found statis-tically
significant versus patients perceptions of dis-comfort (PoSSe
score). It is possible that patients
assessed postoperative third molar pain as better or asexpected.
Another explanation may be that pain was
well controlled by painkillers.
Surgeon
It has been previously suggested that surgical ex-perience is
closelyrelated to the postoperative com-plication rate,27,55
although other studies have failedto show any relationship.17,58
The skill of the surgeonhas been identified as a risk factor for
severe trismusbut not for severe pain or for higher PoSSe score.
Apossible explanation for these findings could be that
all surgeons in this study had more than 5 yearsdentoalveolar
training and used the same surgical ap-proach, in the same
operating room, and under sim-ilar conditions.
Operation Time
Several studies have stated that the length of theoperation
could be used as a proxy variable for ex-traction difficulty.59-61
Other studies reported that pa-tients whose surgery time was 30
minutes or longerhad a prolonged recovery.11,12 Consistent with
previ-ous studies, our results fail to confirm the hypothesis
that operation time is a risk factor for severe postop-
erative discomfort.17,46 These findings may be attrib-
utable to the fact that the variation was not large in
thisstudy, that is, the mean operating time was 24.4 15.9minutes.
Interestingly, the surgeon whose patientshad less postoperative
discomfort spent more time inperforming the operations (mean
operating time 30.7 vs 23.6 and 21.8 minutes).
It could be wrong to assume that operating time iscorrelated
with postoperative discomfort, transpos-ing such concept from
general surgery to minor oral
surgery, where operating time is rarely longer than 1hour.
Validation of the PoSSe Scale
In a recent study, Ruta et al13 developed a postop-erative
symptom severity (PoSSe) scale specific toextractions of third
molars and assessed its validity tomeasure the impact of those
symptoms on patientsperceived quality of life. In our study, the
clinical
validity of the PoSSe scale was provided by its ability
to discriminate between different groups of patientsand to
correlate with trismus and pain objectivelymeasured. The pilot
study of Ruta et al13 showed ahighly significant association
between the number ofpainkiller tablets taken and the PoSSe score.
In thisstudy, we found that the PoSSe score was stronglycorrelated
with both trismus (r 0.54) and numberof painkillers taken (r 0.41).
Consistently, trismusgave higher correlations with
theeatingsubscale (r
0.53) and the number of painkillers taken withpainsubscale (r
0.60). Finally, eating (r 0.83) andinterference with daily
activities(r 0.71) subscales
gave higher correlations with the full PoSSe score.According to
Ogden et al,7 patients participating inthis study felt that surgery
exerted its impact on theirquality of life primarily by reducing
their ability to eatand interference with daily life. These
findings couldhave important implications for the surgeon when
attending to postoperative problems and when ob-taining informed
consent.
Acknowledgment
The authors thank Dr Dario Consonni for his advice and
assis-tance regarding the statistical analyses.
References1. Valmaseda-Castelln E, Berini-Ayts L, Gay-Escoda C:
Inferior
alveolar nerve damage after lower third molar surgical
extrac-tion: A prospective study of 1117 surgical extractions.
OralSurg Oral Med Oral Pathol Oral Radiol Endod 92:377, 2001
2. Renton T, McGurk M: Evaluation of factors predictive of
lingualnerve injury in third molar surgery. Br J Oral Maxillofac
Surg39:423, 2001
3. Goldberg MH, Nemarich AN, Marco WP: Complications
aftermandibular third molar surgery: A statistical analysis of
500consecutive procedures in private practice. J Am Dent
Assoc111:277, 1985
4. Indresano AT, Haug RH, Hoffman MJ: The third molar as acause
of deep space infections. J Oral Maxillofac Surg 50:33,1992
GROSSI ET AL 915
-
7/21/2019 Battista Grossi G. 2007.pdf
16/17
5. Savin J, Ogden GR: Third molar surgeryA preliminary reporton
aspects affecting quality of life in the early postoperativeperiod.
Br J Oral Maxillofac Surg 35:246, 1997
6. McGrath C, Comfort MB, Lo EC, et al: Changes in life
qualityfollowing third molar surgeryThe immediate
postoperativeperiod. Br Dent J 194:265, 2003
7. Ogden GR, Bissias E, Ruta DA, et al: Quality of life
followingthird molar removal: A patient versus professional
perspective.Br Dent J 185:407, 1998
8. Cunningham SJ, Hunt NP, Feinmann C: Perceptions of out-come
following orthognathic surgery. Br J Oral Maxillofac Surg34:210,
1996
9. McGrath C, Comfort MB, Lo EC, et al: Patient-centered
out-come measures in oral surgery: validity and sensitivity. Br J
OralMaxillofac Surg 21:43, 2003
10. Shugars DA, Benson K, White RP Jr, et al: Developing a
mea-sure of patient perceptions of short-term outcomes of
thirdmolar surgery. J Oral Maxillofac Surg 54:1402, 1996
11. Conrad SM, Blakey GH, Shugars DA, et al: Patients
perceptionof recovery after third molar surgery. J Oral Maxillofac
Surg57:1288, 1999
12. Phillips C, White RP, Shugars DA, et al: Risk factors
associatedwith prolonged recovery and delayed healing after third
molarsurgery. J Oral Maxillofac Surg 61:1436, 2003
13. Ruta DA, Bissias E, Ogston S, et al: Assessing health
outcomesafter extraction of third molars: The postoperative
symptomseverity (PoSSe) scale. Br J Oral Maxillofac Surg 38:480,
2000
14. Fisher SE, Frame JW, Route PGJ: Factors affecting the onset
andseverity of pain following the surgical removal of
unilateralimpacted mandibular third molar teeth. Br Dent J
164:351,1988
15. Bruce RA, Frederickson GC, Small G: Age of patients
andmorbidity associated with mandibular third molar surgery.
J Am Dent Assoc 101:240, 198016. Bui CH, Seldin EB, Dodson B:
Types, frequencies, and risk
factors for complications after third molar extraction. J
OralMaxillofac Surg 61:1379, 2003
17. Benediktsdttir IS, Wenzel A, Petersen JK et al:
Mandibularthird molar removal: Risk indicators for extended
operationtime, postoperative pain, and complications. Oral Surg
OralMed Oral Pathol Oral Radiol Oral Endod 97:438, 2004
18. Feine JS, Bushnell MC, Miron D, et al: Sex differences in
theperception of noxious heat stimuli. Pain 44:255, 1991
19. Berkley KJ: Sex differences in pain. Behav Brain Sci
20:371,1997
20. Wizeman TM, Pardue ML: Exploring the Biological
Contribu-tions to Human Health: Does Sex Matter? Washington,
DC,National Academy Press, 2001
21. Walker JS, Carmody JJ: Experimental pain in healthy
humansubjects: Gender differences in nociception and in response
toibuprofen. Anesth Analg 86:1257, 1998
22. Harris RZ, Benet LZ, Schwartz JB: Gender effects in
pharmaco-kinetics and pharmacodynamics. Drugs 50:222, 1995
23. Tanaka E: Gender-related differences in pharmacokinetics
andtheir clinical significance. J Clin Pharm Ther 24:339, 1999
24. Ingelman-Sundberg M, Oscarson M, McLellan RA: Polymor-
phisms human cytochrome P450 enzymes: An opportunity
forindividualized drug treatment. Trends Pharmacol Sci
20:342,1999
25. Craft RM: Sex differences in opioid analgesia: From mouse
toman. Clin J Pain 19:175, 2003
26. Bock K, Schrenk D, Forster A, et al: The influence of
environ-mental and genetic factors on CYP2D6, CYP1A2 and
UDP-glucuronosyltransferases in man using sparteine, caffeine,
andparacetamol as probes. Pharmacogenetics 4:209, 1994
27. Capuzzi P, Montebugnoli L, Vaccaro MA: Extraction of
im-pacted third molars. A longitudinal prospective study on
fac-tors that affect postoperative recovery. Oral Surg Oral Med
OralPathol 77:341, 1994
28. Cepeda MS, Farrar JT, Baumgarten M, et al: Side effects
ofopioids during short-term administration: Effect of age,
gender,and race. Clin Pharmacol Ther 74:102, 2003
29. Gijsbers van Wijk CMT, Kolk AM: Sex differences in
physicalsymptoms: The contribution of symptom perception theory.Soc
Sci Med 45:231, 1997
30. Bergstrom J, Preber H: Tobacco use as a risk factor. J
Periodon-tol 65:545, 1994
31. Jones JK, Triplett RG: The relationship of cigarette smoking
toimpaired intraoral wound healing: A review of evidence
andimplications for patient care. J Oral Maxillofac Surg 50:237,
1992
32. Grossi SG, Zambon J, Machtei EE, et al: Effects of smoking
and
smoking cessation on healing after mechanical
periodontaltherapy. J Am Dent Assoc 128:599, 1997
33. Larsen PE: Alveolar osteitis after surgical removal of
impactedmandibular third molars. Identification of the patient at
risk.Oral Surg Oral Med Oral Pathol 73:393, 1992
34. Al-Belasy FA: The relationship of Shisha (water pipe)
smokingto postextraction dry socket. J Oral Maxillofac Surg 62:10,
2004
35. Sweet JB, Butler DP: Increased incidence of
postoperativelocalized osteitis in mandibular third molar surgery
associated
with patients using oral contraceptives. Am J Obstet
Gynecol127:518, 1977
36. Bolego C, Poli A, Paoletti R: Smoking and gender.
CardiovascRes 53:568, 2002
37. Jamner LD, Girdler SS, Shapiro D, et al: Pain inhibition,
nico-tine, and gender. Exp Clin Psychopharmacol 6:96, 1998
38. Garcia AG, Grana PM, Sampedro FG, et al: Oral contraceptive
and
complication in third molar surgery. Br Dent J 194:453, 200339.
Chapnick P, Diamond L: A review of dry socket: a double-blindstudy
on the effectiveness of clindamycin in reducing theincidence of dry
socket. J Can Dent Assoc 58:43, 1992
40. Cohen ME, Simecek JW: Effects of gender-related factors on
theincidence of localized alveolar osteitis. Oral Med Oral
PatholOral Radiol Endod 79:416, 1995
41. Catellani JE, Harvey S, Erickson SH, et al: Effect of oral
contra-ceptive cycle on dry socket (localized alveolar osteitis). J
AmDent Assoc 101:777, 1980
42. Heasman PA, Jacobs DJ: A clinical investigation into the
inci-dence of dry socket. Br J Oral Maxillofac Surg 22:115,
1984
43. Zeitler DL: Prophylactic antibiotics for third molar
surgery: Adissenting opinion. J Oral Maxillofac Surg 53:61,
1995
44. Piecuch JF, Arzadon J, Lieblich SE: Prophylactic antibiotics
forthird molar surgery: A supportive opinion. J Oral MaxillofacSurg
53:53, 1995
45. Worrall SF: Antibiotic prescribing in third molar surgery
[let-ter]. Br J Oral Maxillofac Surg 36:74, 1998
46. Monaco G, Staffolani C, Gatto MR, et al: Antibiotic therapy
inimpacted third molar surgery. Eur J Sci 107:437, 1999
47. Poeschl PW, Eckel D, Poeschl E: Postoperative
prophylacticantibiotic treatment in third molar surgeryA necessity?
J OralMaxillofac Surg 62:3, 2004
48. Delilbasi C, Saracoglu U, Keskin A: Effects of 0.2%
chlorhexi-dine gluconate and amoxicillin plus clavulanic acid on
theprevention of alveolar osteitis following mandibular third
mo-lar extractions. Oral Surg Oral Med Oral Pathol Oral RadiolEndod
94:301, 2002
49. Stone HH, Hooper CA, Kolb LD, et al: Antibiotic prophylaxis
ingastric, biliary and colonic surgery. Ann Surg 184:443, 1976
50. Classen DC, Evans RS, Pestotnik SL, et al: The timing of
pro-phylactic administration of antibiotics and the risk of
surgical
wound-infection. N Engl J Med 326:281, 199251. Sekhar CH,
Narayanan V, Baig MF: Role of antimicrobials in
third molar surgery: Prospective, double blind,
randomized,placebo-controlled clinical study. Br J Oral Maxillofac
Surg39:134, 2001
52. Gandhi M, Aweeka F, Greenblatt RM, et al: Sex differences
inpharmacokinetics and pharmacodynamics. Annu Rev PharmacolToxicol
44:499, 2004
53. Hersh EV, Moore PA: Drug interactions in dentistry. The
impor-tance of knowing your CYPs. J Am Dent Assoc 135:298, 2004
54. Gresser U: Amoxicillin-clavulanic acid therapy may be
associ-ated with severe side effects-review of the literature. Eur
J MedRes 6:139, 2001
55. De Boer MPJ, Raghoebar GM, Stegenga B, et al:
Complicationafter mandibular third molar extraction. Quintessence
Int 26:779, 1995
916 ASSESSING DISCOMFORT AFTER THIRD MOLAR SURGERY
-
7/21/2019 Battista Grossi G. 2007.pdf
17/17
56. Yuasa H, Kawai T, Sugiura M: Classification of surgical
difficultyin extracting third molars. Br J Oral Maxillofac Surg
40:26, 2002
57. Jakse N, Bankaoglu V, Wimmer G, et al: Primary wound
healingafter lower third molar surgery: Evaluation of 2 different
flapdesigns. Oral Surg Oral Med Oral Pathol 93:7, 2002
58. Oginni FO, Fatusi OA, Alagbe AO: A clinical evaluation of
drysocket in a Nigerian teaching hospital. J Oral Maxillofac
Surg61:871, 2003
59. Susarla SM, Dodson TB: Risk factors for third molar
extractiondifficulty. J Oral Maxillofac Surg 62:1363, 2004
60. Santamaria J, Arteagoitia I: Radiologic variables of
clinical sig-nificance in the extraction of impacted mandibular
third mo-lars. Oral Surg Oral Med Oral Pathol 84:469, 1997
61. Renton T, Smeeton N, McGurk M: Factors predictive of
diffi-culty of mandibular third molar surgery. Br J Oral
MaxillofacSurg 190:607:10, 2001
GROSSI ET AL 917