Embed Size (px)
Citation preview
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 1/24

8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 2/24
Copyright © 2009 The SEEP Network
Sections o this publication may be copied or adapted to meet local needs without thepermission rom The SEEP Network, provided that the parts copied are distributed
or ree or at cost—not or prot. Please credit the “Practitioner Learning Program inBuilding Alliances to Serve HIV/AIDS-Impacted Communities in Sub-Saharan Arica”
and The SEEP Network or those sections excerpted.
SEEP would like to thank Kristen Eckert and Jared Penner, SEEP’s HAMED WorkingGroup Facilitators, or reviewing this document.
This study is made possible by the generous support o the American people throughthe United States Agency or International Development (USAID). The contents are theresponsibility o The SEEP Network and do not necessarily refect the views o USAID
or the United States Government.
This initiative is carried out as part o the AED FIELD-Support mechanism. For moreinormation, please visit www.microlinks.org/eld.
For any commercial reproduction, please obtain permission rom
The SEEP Network1875 Connecticut Avenue NW, Suite 414
Washington, DC 20009-5721Tel.: 202-534-1400 Fax: 202-534-1433
E-mail: [email protected]: www.seepnetwork.org
Printed in the United States o America.
To access this publication online, visit http://hamed.seepnetwork.org.

8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 3/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • iii
Abstract
Tis technical note explores the models o partnership that can promote economic strengthening in communities a-ected by HIV and AIDS through microenterprise development—both micronance and enterprise development. Teinormation is based on the experiences and lessons learned o the participants o Te SEEP Network PractitionerLearning Program (PLP) on Building Alliances to Serve HIV and AIDS-Impacted Communities in sub-Saharan
Arica (BASICS).
In this technical note, our case studies analyze the characteristics, lessons learned, challenges, and recommendationsaround our types o partnerships. Te institutional partnership model is based on a long-term relationship between twoorganizations. Te targeted partnership model is a collaboration that ocuses on ullling specic technical or programneeds, and may be short-term or long-term. An intermediary partnership typically involves a local or national NGOas the connection between an international organization and community-level organizations. Te commercial partner-ship model develops a relationship between a business and producer groups with a acilitating partner that brokers therelationship.
By the end o this document, readers will be able to understand these our types o partnerships and the specicstrengths and challenges o each, and will have gained lessons and recommendations to apply to their own partnerships.
Tis document is also published as an addendum to Te SEEP Network Guidelines for Microenterprise Development inHIV and AIDS-Impacted Communities at http://hamed.seepnetwork.org .

8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 4/24
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 5/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • v
Table o Contents
Abstract iiiList o Acronyms viAbout The SEEP Network 1About the Practitioner Learning Program 1
Introduction 1
Case Study 1: Institutional Partnership Model 3The Context 3The Partners 4Partnership Objectives 4Partnership Activities and Results 5Lessons Learned 6
Case Study 2: Targeted Partnership Model 6The Context 6
The Partners 7Partnership Objectives 7Partnership Activities and Results 7Lessons Learned 8
Case Study 3: Intermediary Partnership Model 9The Context 9The Partners 9Partnership Objectives 10Partnership Activities and Results 10Lessons Learned 11
Case Study 4: Commercial Partnership Model 12The Context 12The Partners 12Partnership Objectives 13Partnership Activities and Results 13Lessons Learned 13
Conclusions and Recommendations 14Bibliography 18
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 6/24
vi • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
List o Acronyms
ART anti-retroviral therapy
CBO community-based organization
COPE Community-Based Orphan Care, Protection, and Empowerment project
CRS Catholic Relie Services
EASSI Economic Awareness Sel Sustenance Initiative
EMG Emerging Markets Group, Ltd.
ICAP International Center or AIDS Care and Treatment Program(Columbia University)
MDGs Millennium Development Goals
MED micronance and enterprise development
MFI micronance institution
MOU memorandum o understanding
NGO non-governmental organization
OVC orphans and vulnerable children
PEPFAR US President’s Emergency Plan or AIDS Relie
PLP Practitioner Learning Program
PLWHA people living with HIV and AIDS
PMTCT prevention o mother to child transmission
PPAG Planned Parenthood Association o GhanaSAT Sinapi Aba Trust
SILC savings and internal lending communities
USAID United States Agency or International Development
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 7/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 1
About The SEEP Network
Te SEEP Network, ounded in 1985 and headquartered in Washington, DC, is an association o more than 70 inter-national NGOs that support micro- and small-enterprise development programs around the world. SEEP’s missionis to connect microenterprise practitioners in a global learning community. As such, SEEP brings members and otherpractitioners together in a peer-learning environment to produce practical, innovative solutions to key challenges in theindustry. SEEP then disseminates these solutions through training, publications, proessional development, and techni-
cal assistance.
About the Practitioner Learning Program
Te Practitioner Learning Program (PLP) methodology was developed by SEEP as a way to engage microenterprisepractitioners in a collaborative learning process to document and share ndings and to identiy eective and replicablepractices and innovations to benet the industry as a whole. Te PLP combines a small grant program with an inten-sive small-group acilitated-learning process, usually over a period o one or more years, and utilizes workshops, emaillistservs, conerence calls, and distance learning. Practitioner Learning Programs ocus on learning at three levels: theindividual organization, the PLP group, and the industry at large.
Te objectives o the BASICS PLP are to empower micronance and enterprise development practitioners throughpeer learning to build and strengthen strategic alliances with partner organizations and to document and disseminatethe most eective models or developing these alliances or maximizing impact.
For more inormation on partnerships or microenterprise development in HIV and AIDS impacted communities,please visit http://hamed.seepnetwork.org to view the other learning products in this series:
Partnering to Achieve Economic Impact in HIV and AIDS Impacted Communities: A Partnership oolkit or•
Microenterprise DevelopmentEnhanced Service Provision or Economic Strengthening in HIV and AIDS Impacted Communities•
Partner Capacity Building or Economic Strengthening in HIV and AIDS Impacted Communities•
Introduction
Development organizations working in micronance or enterprise programming oten work with and through localpartners. Tis is especially common or organizations trying to serve HIV and AIDS-aected clients and communities,particularly when attempting to deliver or provide access to holistic services and integrated programming.1
Te SEEP Guidelines for Microenterprise Development in HIV and AIDS-Impacted Communities states that “microenter-prise development is a crucial element o a holistic approach to HIV and AIDS prevention and mitigation.” It ac-knowledges, however, that “implementing integrated programming is challenging. It requires bringing together diversetechnical approaches, dierent program priorities, and—sometimes—competing institutional and proessional interests.
Te key to addressing these challenges is acilitating eective cross-sector partnerships among public health and MED(microenterprise development) proessionals and organizations.”2
1. For more inormation on the importance o partnerships, see C. Green, “Micronance and HIV/AIDS: Strategic Partnerships,”AMAP Micronance and HIV/AIDS Note 2, prepared or USAID by DAI (Washington, DC: USAID). http://www.microlinks.org/ ev.php?ID=22387_201&ID2=DO_TOPIC.
2. The SEEP Network, 2008, online document. “What Kind o Microenterprise Development Strategies Work or HIV and AIDS-Impacted Communities?” section 2.3, and “How Can We Facilitate a Cross-Sector Partnership?” section 2.5, in Guidelines for Mi-
croenterprise Development in HIV and AIDS-Impacted Communities, Book 2, For Microenterprise Development Practitioners, http://
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 8/24
2 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
Section 2.5 o the Guidelines sets orth guiding principles or integrated programming and discusses institutional andtechnical challenges to delivering integrated programming through partnerships. Te major institutional challenges andstrategies identied are:
adoption o broader goals—and indicators—that provide stronger incentives or joint programming;•
unding streams with joint goals that require collaboration;•
incentives or institutional collaboration built into programs at all relevant levels;•
adoption o eective institutional models or implementation; and•
support or ongoing research, active communities o practice, and leadership opportunities or proessionals who•
advance practice in integrated programming.
Te major technical challenges identied are:
dierent targeting strategies (between MED programs and other organizations);•
dierent terminology;•
risk to MED program perormance;•
need or ocus and technical specialization to achieve good practices and results; and•
the small scale o some MED initiatives.•3
Tis document urthers the dialogue by comparing and contrasting our specic partnerships (each representing adierent model) their role in serving people living with HIV and AIDS, and their individual successes and challengesstemming rom that partnership. Many o these challenges reect the challenges identied in the Guidelines above; oth-ers are more specic to certain types o partnerships.
Te document presents our cases:
Te1. institutional partnership model represents a long-term collaboration between two organizations. Te casedescribed here is based on an ongoing relationship between an international non-governmental organization(NGO) and a national implementing NGO partner. Te international NGO provides technical support andunding, while the national NGO is the implementer o the program at the community level.
Te2. targeted partnership model ocuses on ullling specic technical or program needs, and may be long term
or short term, depending upon the objectives o the partnership. In this technical note, one national NGOsubcontracts another national NGO to pilot the delivery o supplementary services.
Te3. intermediary partnership model typically involves an international NGO, a local (national or regional)NGO, and community-based organizations (CBO). Te international NGO relies on the local NGO toimplement an overall program, while the local NGO works with CBOs, ranging rom sel-help groups tosmall NGOs, to implement specic services needed by their clients.
Te4. commercial partnership model develops a relationship between a business (lead rm) and producer groups. A acilitating partner brokers the relationship and organizes and builds capacity o producer groups. In thiscase, the producer groups are clusters o caregivers who benet rom expanded products and market access.
communities.seepnetwork.org/hamed/node/38 and http://communities.seepnetwork.org/hamed/node/40, respectively. Section 2.5contains guiding principles or integrated programming.
3. For a ull discussion o these challenges, see SEEP, 2008, Guidelines, “Structural (Institutional) Challenges and Strategies orCross-Sector Collaboration,” section 2.5.2 (http://communities.seepnetwork.org/hamed/node/777) and “Technical Challenges andStrategies or Cross-Sector Collaboration,” section 2.5.3 (http://communities.seepnetwork.org/hamed/node/778).
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 9/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 3
PLP Participant Case Studies and Models
Institutional partnership model: Catholic Relie Services (CRS) is a large, multisectoral international NGO operating in over 100countries. This case study examines the Lieline project, which assists HIV and AIDS-aected households in Rwanda in devel-oping community-managed savings and lending groups. The delivery o the service is managed by CRS’ implementing partnerCaritas Rwanda, which coordinates an extensive network o diocese, parish, and sub-parish structures at the community levelthroughout the country. The activities o the Lieline project are integrated into virtually all CRS’ HIV and AIDS programsunded through PEPFAR.1
Targeted partnership model: Sinapi Aba Trust (SAT) and Planned Parenthood Association o Ghana (PPAG) are national NGOswith extensive experience in their respective elds. SAT is a micronance institution (MFI) and part o the Opportunity Inter-national Network, and PPAG is an autonomous national body o the Planned Parenthood Network. SAT and PPAG ormed analliance under the SEEP PLP to pilot the delivery o health services—HIV and AIDS awareness raising, voluntary testing, andhealth reerrals and support—to MF clients, while maintaining the privacy o clients with regard to the lending institution, loanocers and borrower groups.
Intermediary partnership model: Fantsuam Foundation is a holistic, multisectoral NGO operating in Kaduna State in north centralNigeria. Fantsuam works with a large number o partners, including international and local NGOs, community developmentcouncils, and sel-help groups. Through its partners, Fantsuam provides micronance, livelihoods development, and health ser-vices to their target populations, which include rural women, people living with HIV and AIDS (PLWHA), children, and youth.Fantsuam requently acts as the intermediary and implementing partner between international NGO donors and community-based organizations.
Commercial partnership model: Emerging Markets Group (EMG) is an international development consulting rm engaged inagribusiness and rural livelihoods, nancial services, health care, private sector development, public sector and businessenvironment reorm, and tourism. EMG works on the COPE project (Children-Community-Based Orphan Care, Protection, andEmpowerment) ocused on orphans and vulnerable children in Tanzania, Uganda, Rwanda and Mozambique (unded by USAIDthrough PEPFAR). EMG partners with community-based caregiver associations and private-sector rms to help caregivers ac-cess better markets, resources, and skills training. The case presented in this technical note describes the relationship with theprocessing and marketing rm Fruits o the Nile.
1. The US President’s Emergency Plan or AIDS Relie.
Case Study 1: Institutional Partnership Model
The Context
Rwanda is among the least developed countries in the world, ranking 165 o 179 countries in the UNDP HumanDevelopment Index.4 Rwanda’s 9-million people inhabit the most densely populated country in Arica, with approxi-mately 310 inhabitants per square kilometer. Te estimated adult HIV prevalence rate is 2.8 percent. In 2007, UNAIDSreported 150,000 people living with HIV and 220,000 children orphaned by AIDS.5 Chronic and acute ood insecurity has only compounded the problem as people living with HIV and AIDS and orphans and vulnerable children (OVC)have been most aected.
4. UN Development Programme (UNDP), 2008, website, Human Development Reports, Update 2008, Country Fact Sheets, “2008Statistical Update: Rwanda—Human Development Index, Going beyond Income,” http://hdrstats.undp.org/2008/countries/coun-try_act_sheets/cty_s_RWA.html.
5. UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance, 2009, “Epidemiological Fact Sheet on HIV and AIDS—Core Data on Epidemiology and Response: Rwanda 2008 Update” (Geneva: UNAIDS and WHO) 5, 7. http://apps.who.int/globalatlas/ predenedReports/EFS2008/ull/EFS2008_RW.pd.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 10/24
4 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
Te population o Rwanda is overwhelmingly rural; 90 percent o the country depends on agriculture. Poor soil ertility and climatic shocks contribute to chronic and acute ood insecurity and aect a signicant portion o the population.6 Studies have shown that Rwandan households that care or sick individuals spend less time on agricultural activities,leading to neglect o elds, a decrease in area planted, and shits to less labor-intensive crops.7 Some are also orced tosell their land and livestock, decreasing their productive assets.8
The Partners
Founded in 1943, Catholic Relie Services has technical-development programming experience in more than 100dierent countries across the globe. CRS has worked in Rwanda since 1963, managing projects that encourage localcommunities to participate in identiying and resolving development issues. CRS was directly involved in emergency programs ater the outbreak o civil conict in 1990, but has now transitioned back to development activities. CRS’sprograms in Rwanda ocus on agriculture, micronance, peace building, and ood assistance to vulnerable populations.
Caritas Rwanda is a local, aith-based community organization oering social, health, and development activitiesthrough a comprehensive network o dioceses, parishes, and more than 10,000 small Christian communities throughoutthe country. Te primary goal o Caritas Rwanda is to empower society’s most disadvantaged groups and restore humandignity to those who have been threatened by social marginalization, ethnic divisions, and injustice.
Partnership Objectives
CRS has partnered with Caritas in Rwanda since 1963. Caritas Rwanda shares a similar mission as CRS, and alsoimplements a variety o social, medical, and spiritual services through a vast network o community structures and localhealth centers. Caritas also possesses the drive, the means, and the credibility needed to help the poorest o the pooraccess essential services. CRS’s primary role in this partnership is to support Caritas with programming, administrative,and technical expertise. Te goal is to build up Caritas’ capacity in these areas until Caritas is able to implement high-quality programs and access external donor unding independently.
o address issues o chronic ood insecurity and economic vulnerability among amilies and households aected by HIV and AIDS, CRS in collaboration with Caritas Rwanda introduced the Savings and Internal Lending Communities
(SILC) methodology. SILC is a group-managed, savings-led approach that allows communities to better manage theirown resources or investing in opportunities and cushioning against shocks.
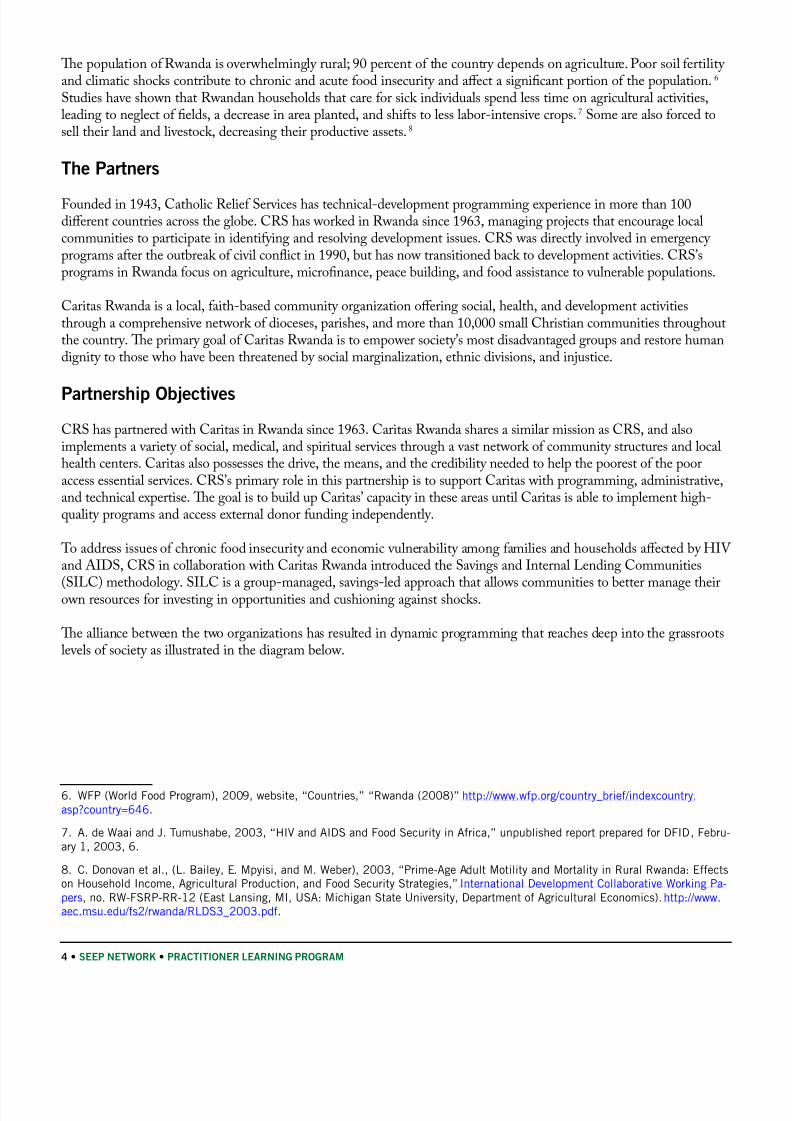
Te alliance between the two organizations has resulted in dynamic programming that reaches deep into the grassrootslevels o society as illustrated in the diagram below.
6. WFP (World Food Program), 2009, website, “Countries,” “Rwanda (2008)” http://www.wp.org/country_brie/indexcountry.asp?country=646.
7. A. de Waai and J. Tumushabe, 2003, “HIV and AIDS and Food Security in Arica,” unpublished report prepared or DFID, Febru-ary 1, 2003, 6.
8. C. Donovan et al., (L. Bailey, E. Mpyisi, and M. Weber), 2003, “Prime-Age Adult Motility and Mortality in Rural Rwanda: Eectson Household Income, Agricultural Production, and Food Security Strategies,” International Development Collaborative Working Pa-pers, no. RW-FSRP-RR-12 (East Lansing, MI, USA: Michigan State University, Department o Agricultural Economics). http://www.aec.msu.edu/s2/rwanda/RLDS3_2003.pd.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 11/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 5
CRS Rwanda
Lifeline project manager
Diocese
Caritas Lifeline Supervisor
Diocese
Caritas Lifeline Supervisor
Parish
Caritas Lifeline Field Agents
Parish Parish Parish
SILC group SILC group SILC group SILC group
SILC group SILC group SILC group
Partnership Activities and Results
In 2006, CRS and Caritas initiated the Lieline Project in Rwanda to scale up micronance services oered to HIV and AIDS-aected households. Te CRS Lieline project manager provides training, technical assistance, monitoring, andcapacity building to Caritas partners in the dioceses. Caritas employs one SILC supervisor in each diocese and seveneld agents per diocese. Te eld agents operate at the parish level to raise awareness about SILC and encourage theormation o SILC groups. Once ormed, the eld agents train these groups in the SILC methodology and providethem with technical assistance and supervision. Each parish eld agent supports a maximum o ten SILC groups, with
approximately 20–25 members per group.
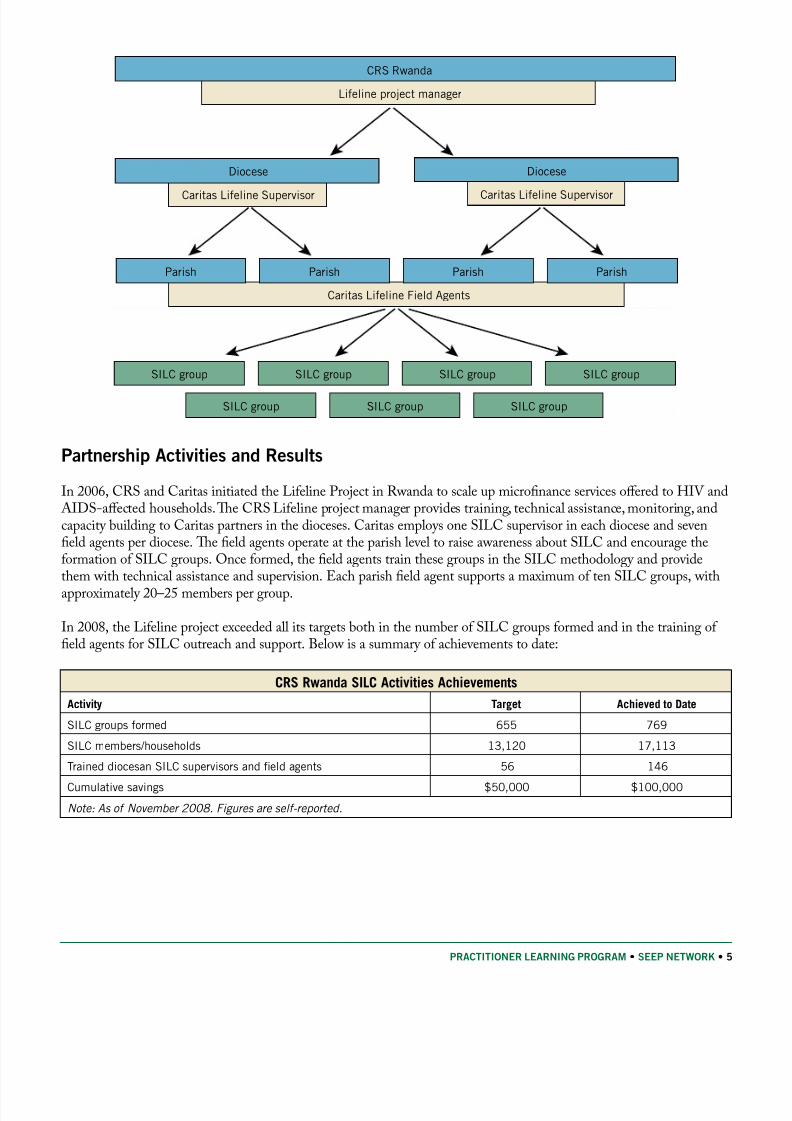
In 2008, the Lieline project exceeded all its targets both in the number o SILC groups ormed and in the training o eld agents or SILC outreach and support. Below is a summary o achievements to date:
CRS Rwanda SILC Activities Achievements
Activity Target Achieved to Date
SILC groups ormed 655 769
SILC members/households 13,120 17,113
Trained diocesan SILC supervisors and eld agents 56 146
Cumulative savings $50,000 $100,000
Note: As of November 2008. Figures are self-reported.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 12/24
6 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
Lessons Learned
Successes
Shared goals and values have increased the strength o the partnership.1. CRS and Caritas Rwanda arelong-time collaborators. Te Lieline Project supports the CRS goal o promoting social justice and reachingthe poorest o the poor with high-quality services. Te project also supports the National Caritas 2005–2007Strategic Plan objective to increase nancial revenues and two o its “intermediate results” to improve access
to capital and strengthen entrepreneurial spirit among beneciaries.Beneciary communities are actively engaged through the partner.2. At the community level, SILC parisheld agents are recruited rom already-existing SILC groups. Tese community members go through intensetraining and supervision rom Caritas to expand their knowledge and capacity. Ater two years, new SILCgroups will be able to pay a small ee to the parish eld agents or their technical assistance. (Parish eldagents receive only a small stipend and a bicycle.)
CBO-capacity building activities enable longer-lasting program results or beneciaries.3. Te CRS pro-gram manager oers a training o trainers program to diocesan supervisors. Trough CRS technical assistanceand monitoring, the supervisors then progressively increase their ability to independently manage and pro-mote SILC activities. Tey also provide eedback and advice to CRS on the progress o implementation o activities.
Challenges
Inconsistent policies are disruptive to institutional collaboration.1. CRS and Caritas, as institutional part-ners, cooperate on many projects; however, each project comes with its own budget and structure. As a result,this can lead to inconsistencies within both organizations and aect the quality o services oered to clients.For example, Caritas ofces at the diocesan level do not always have a pre-determined salary scale, so sta members with the same level o responsibility might be oered dierent salaries, depending on the proj-ect. Te same is true or incentives oered to volunteers: projects with bigger budgets can aord to provide
volunteers with bicycles, radios, mobile phones, and access to health care, whereas others can provide only tee-shirts. As a result, volunteers oten abandon one project in avor or another that provides better incen-tives, helping some joint projects and hurting others.
A two-tier administrative system can delay implementation.2. Caritas serves as a sub-grantee o CRS donorunding and, as such, Caritas relies on CRS or the bulk o the programs’ nancial management. Missingreceipts rom Caritas or delayed advances by CRS can hold up the implementation o project activities andengender eelings o rustration on the part o project sta rom both organizations.
Case Study 2: Targeted Partnership Model
The Context
Ghana, on the west coast o Arica, is home to an estimated population o about 19 million that has been growing at 2.7percent annually. Ghana’s human development ranking is 135 o 177 countries, putting it at the top o the rankings in A-rica.9 As Ghana seeks to achieve the Millennium Development Goals (MDGs) and reach middle-income status by 2015,it has sustained a period o economic stability, with income poverty levels declining rom 39.5 per cent in 1999 to around
9. UNDP, 2008, website, Human Development Reports, Update 2008, Country Fact Sheets, “2008 Statistical Update: Ghana—Human Development Index, Going beyond Income,” http://hdrstats.undp.org/en/2008/countries/country_act_sheets/cty_s_GHA.html.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 13/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 7
28.5 per cent in 2006.10 However, while there has been steady progress in some areas, they are still acing challenges in theareas o child health/child mortality, maternal mortality, gender equality and worsening income inequalities.11
Te national HIV prevalence o Ghana is relatively low, at just under 2 percent in 2007. However, only 1 percent o households with orphans and vulnerable children receive basic external aid, and only 15 percent o advanced HIV pa-basic external aid, and only 15 percent o advanced HIV pa-percent o advanced HIV pa-o advanced HIV pa-tients receive anti-retroviral therapy (AR).12
The Partners
Sinapi Aba rust (SA), one o the largest micronance institutions in Ghana, is a Christian NGO established in 1994and headquartered in �umasi, the capital o the Ashanti region. SA operates in all 10 regions o Ghana with 39 branch-in �umasi, the capital o the Ashanti region. SA operates in all 10 regions o Ghana with 39 branch-es, serving approximately 80,000 clients, 95 percent o whom are women. SA, as a member o the Opportunity Interna-tional Network, seeks to transorm the lives o their clients holistically through microenterprise development and train-ing, business advisory services, HIV and AIDS awareness programs, community development, and youth development.
Te Planned Parenthood Association o Ghana (PPAG) was established in Ghana in 1967 and is a member o theInternational Planned Parenthood Federation. Its activities include amily planning and sexual and reproductive healthissues, including HIV and AIDS. Like SA, PPAG is also a nationwide organization with regional ofces throughoutGhana. PPAG’s mission is to “provide youth with the knowledge and means to exercise their basic right to decide reely
and responsibly about their sexual and reproductive health as a means o improving quality o lie.”13
Partnership Objectives
SA recognized the seriousness o the HIV and AIDS pandemic and the associated tragic consequences or clients,their businesses, and their communities, as well as potential consequences or SA sta. Tey reached out to and ormedan alliance with PPAG, with the goal o improving clients’ well being through quality health services related to HIV and AIDS, along with micronance services.
Specic objectives included:
intensiying education and awareness eorts or SA clients;•
oering voluntary counseling and testing or HIV and AIDS;•
educating clients on stigmatization and discrimination against people living with HIV and AIDS;•
provide care and support or HIV and AIDS aected people; and•
playing a leading role in advocacy in various dimensions to support people living with HIV and AIDS.•
Partnership Activities and Results
Under the BASICS PLP, SA and PPAG conducted a range o activities to serve the clients o both organizations. Tese included a three-day capacity building workshop on education and prevention, voluntary counseling, and test-ing in our SA branches, ongoing support or inected persons, reerrals to clinics or treatment, and the creation o anHIV-positive client support group. Te training included discussions on sexually transmitted inections and associated
10. “MDG Prole: Ghana,” MDG Monitor website, available rom http://www.mdgmonitor.org/actsheets_00.cm?c=GHA. Accessedon August 27, 2009.
11. Ibid.
12. UNAIDS, 2008, 2008 Report on the global AIDS epidemic. (Geneva: Joint United Nations Programme on HIV/AIDS). http:// viewer.zmags.com/publication/ad3eab7c#/ad3eab7c/1. 214,268, 293.
13. Planned Parenthood Association o Ghana. http://www.ppag-gh.org/vision.asp.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 14/24
8 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
risk, protection against inection; relationships and HIV risk; needs o people living with HIV and AIDS, eects o AR, stigma and discrimination, and whether to undergo testing.
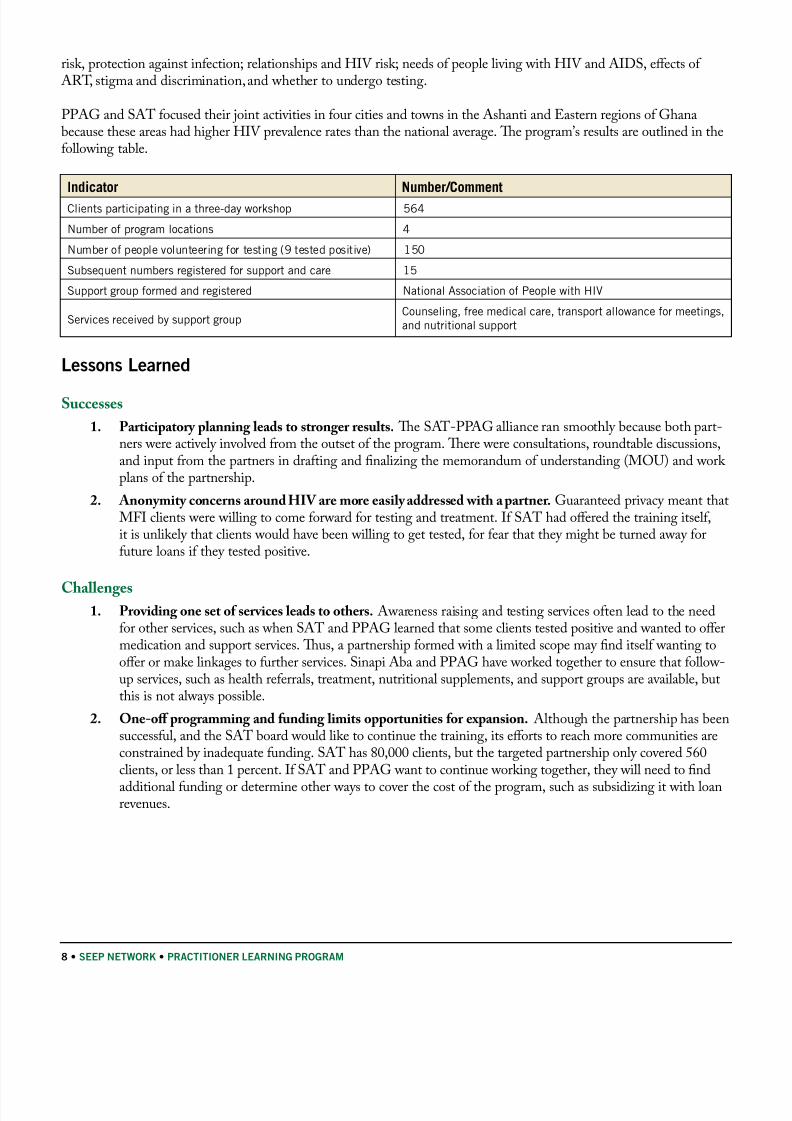
PPAG and SA ocused their joint activities in our cities and towns in the Ashanti and Eastern regions o Ghanabecause these areas had higher HIV prevalence rates than the national average. Te program’s results are outlined in theollowing table.
Indicator Number/Comment
Clients participating in a three-day workshop 564
Number o program locations 4
Number o people volunteering or testing (9 tested positive) 150
Subsequent numbers registered or support and care 15
Support group ormed and registered National Association o People with HIV
Services received by support groupCounseling, ree medical care, transport allowance or meetings,and nutritional support
Lessons Learned
Successes
Participatory planning leads to stronger results.1. Te SA-PPAG alliance ran smoothly because both part-ners were actively involved rom the outset o the program. Tere were consultations, roundtable discussions,and input rom the partners in drating and nalizing the memorandum o understanding (MOU) and work plans o the partnership.
Anonymity concerns around HIV are more easily addressed with a partner.2. Guaranteed privacy meant thatMFI clients were willing to come orward or testing and treatment. I SA had oered the training itsel,it is unlikely that clients would have been willing to get tested, or ear that they might be turned away oruture loans i they tested positive.
ChallengesProviding one set o services leads to others.1. Awareness raising and testing services oten lead to the needor other services, such as when SA and PPAG learned that some clients tested positive and wanted to oermedication and support services. Tus, a partnership ormed with a limited scope may nd itsel wanting tooer or make linkages to urther services. Sinapi Aba and PPAG have worked together to ensure that ollow-up services, such as health reerrals, treatment, nutritional supplements, and support groups are available, butthis is not always possible.
One-o programming and unding limits opportunities or expansion.2. Although the partnership has beensuccessul, and the SA board would like to continue the training, its eorts to reach more communities areconstrained by inadequate unding. SA has 80,000 clients, but the targeted partnership only covered 560clients, or less than 1 percent. I SA and PPAG want to continue working together, they will need to nd
additional unding or determine other ways to cover the cost o the program, such as subsidizing it with loanrevenues.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 15/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 9
Case Study 3: Intermediary Partnership Model
The Context
Nigeria is Arica’s most populous country, with a population o over 140 million and more than 373 ethnic groups.It ranks 158 o 177 countries in human development14, and the prevalence o HIV has decreased rom a high o 5.8percent in 2001 to 3.1 percent in 2007.15 Although these prevalence rates appear low, Nigeria ranks third in terms o theactual number o people inected with HIV. Furthermore, less than 10 percent o orphans and vulnerable children under17 receive basic external support, and less than 17 percent o adults and children with advanced HIV inection have ac-cess to AR.16
Fantsuam operates within �aduna State, which suers rom a lack o jobs and inrastructure, including sae housing.Many residents do not have access to aordable, quality health-care services. Economic activity is predominantly subsis-tence and agricultural, with extremely limited opportunities or employment. A rural-urban migration has led to a “braindrain” o many proessionals moving to the cities to seek employment, urther weakening the area’s economic oundation.
The Partners
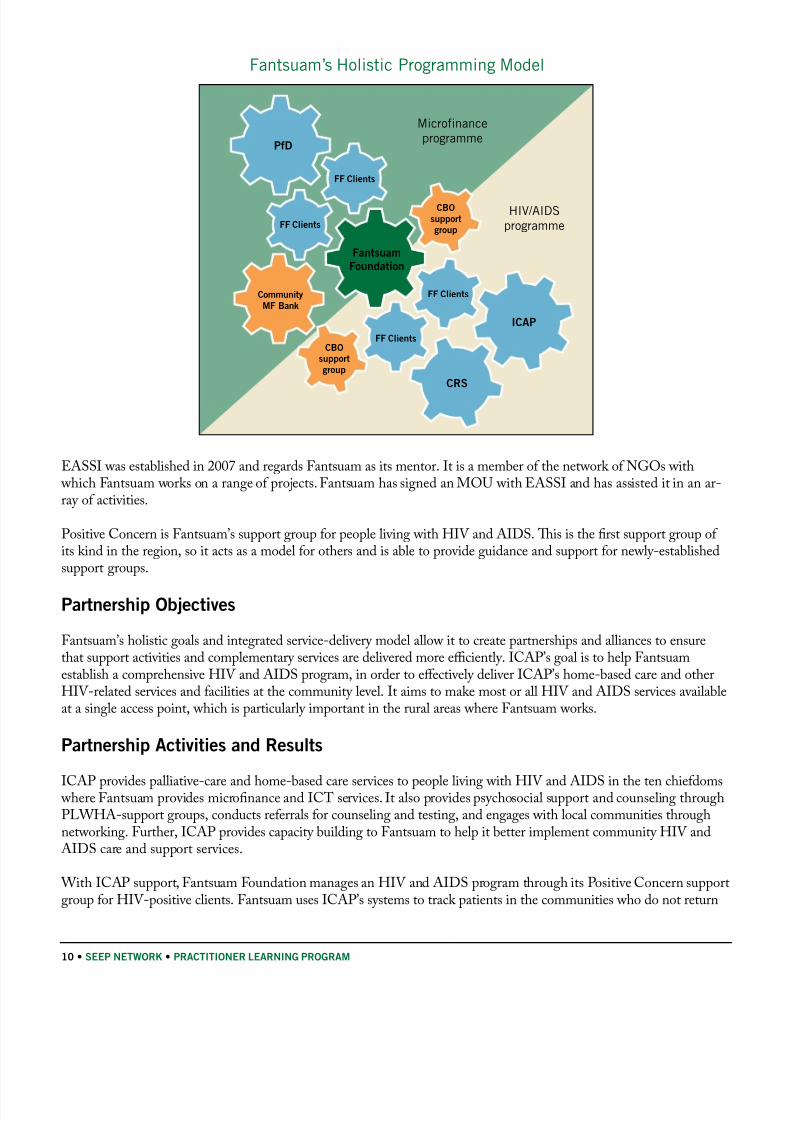
Fantsuam Foundation is a regionally-based NGO committed to making �aduna State a successul and replicable modelo integrated rural development in Nigeria. Fantsuam’s unique, integrated services approach includes micronance,health (including HIV and AIDS programs), inormation and communications technology (IC) training and serviceprovision. Tis model requires Fantsuam to actively engage with and coordinate the activities o both international andnational partners, NGOs, and CBOs in dierent elds, in pursuit o its objective.
Fantsuam Foundation works with several international partners, including Columbia University’s International Center or AIDS Care and reatment Program (ICAP) and Partners or Development. In turn, all three organizations have extensivepartnerships with CBOs, recognizing the important roles they play in mobilizing communities, reaching the most vulner-able, raising awareness, and reducing stigma. Tis case study ocuses on one international partner, ICAP; one community-level NGO, EASSI (Economic Awareness Sel-Sustenance Initiative); and selected community sel-help groups.
In partnership with the Nigerian government, ICAP provides a range o HIV and AIDS services in �aduna State andelsewhere: technical and nancial assistance to scale up comprehensive HIV and AIDS prevention, care, and treatmentservices, including AR. ICAP provides unding to Fantsuam under the Multi-Country Columbia Anti-retroviral Pro-gram cooperative agreement between ICAP and the U.S. Centers or Disease Control and Prevention. Fantsuam, or itspart, provides palliative care and reerral linkages between the community and ICAP-supported acilities.
14. UNDP, 2008, website, Human Development Reports, Update 2008, Country Fact Sheets, “2008 Statistical Update: Nigeria—Human Development Index, Going beyond Income,” http://hdrstats.undp.org/en/2008/countries/country_act_sheets/cty_s_NGA.html.
15. UNAIDS, 2008, 2008 Report on the global AIDS epidemic. (Geneva: Joint United Nations Programme on HIV/AIDS). http:// viewer.zmags.com/publication/ad3eab7c#/ad3eab7c/1. 214.
16. UNAIDS, 2008, 2008 Report on the global AIDS epidemic. (Geneva: Joint United Nations Programme on HIV/AIDS). http:// viewer.zmags.com/publication/ad3eab7c#/ad3eab7c/1. 270.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 16/24
10 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
Fantsuam’s Holistic Programming Model
PfD
FF Clients
FF Clients
FF Clients
FF Clients
Fantsuam
Foundation
ICAP
CBO
support
group
Community
MF Bank
CBO
support
group
CRS
Microfinance
programme
HIV/AIDS
programme
EASSI was established in 2007 and regards Fantsuam as its mentor. It is a member o the network o NGOs with which Fantsuam works on a range o projects. Fantsuam has signed an MOU with EASSI and has assisted it in an ar-ray o activities.
Positive Concern is Fantsuam’s support group or people living with HIV and AIDS. Tis is the rst support group o its kind in the region, so it acts as a model or others and is able to provide guidance and support or newly-establishedsupport groups.
Partnership Objectives
Fantsuam’s holistic goals and integrated service-delivery model allow it to create partnerships and alliances to ensurethat support activities and complementary services are delivered more efciently. ICAP’s goal is to help Fantsuamestablish a comprehensive HIV and AIDS program, in order to eectively deliver ICAP’s home-based care and otherHIV-related services and acilities at the community level. It aims to make most or all HIV and AIDS services availableat a single access point, which is particularly important in the rural areas where Fantsuam works.
Partnership Activities and Results
ICAP provides palliative-care and home-based care services to people living with HIV and AIDS in the ten chiedoms where Fantsuam provides micronance and IC services. It also provides psychosocial support and counseling throughPLWHA-support groups, conducts reerrals or counseling and testing, and engages with local communities throughnetworking. Further, ICAP provides capacity building to Fantsuam to help it better implement community HIV and
AIDS care and support services.
With ICAP support, Fantsuam Foundation manages an HIV and AIDS program through its Positive Concern supportgroup or HIV-positive clients. Fantsuam uses ICAP’s systems to track patients in the communities who do not return
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 17/24

8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 18/24
12 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
Case Study 4: Commercial Partnership Model
The Context
Children who have lost a parent to AIDS are at higher risk o HIV inection, poverty, illiteracy, homelessness, anddiscrimination.17 In sub-Saharan Arica, it is common practice or children orphaned by AIDS to be cared or by amily members, riends, or others in the community, which may cause nancial constraints and additional burdens o poverty.
wo million o Uganda’s 31.4 million people are estimated to be orphans, 50 percent due to AIDS.
Te Community-Based Orphan Care, Protection and Empowerment project, or COPE, is being implemented inthe three counties o Ntungamo District, where its implementing partners have a long history o addressing the HIV and AIDS pandemic in collaboration with both public and private sectors. Te income-generation component targetscaregivers o orphans and vulnerable children. Tese caregivers live in rural areas and grow bananas and pineapples,
which are particularly perishable during the harvest season. In the past, the caregivers had no connection to any externalmarkets and reported being cheated by middlemen. o provide clusters o clients with access to more-promising marketopportunities, Emerging Markets Group (EMG), under a subcontract with Aricare, works to link clients to rms inthe value chain, such as ood processors and exporters working in industries with high-growth potential. Matchingclients to well-established, stable rms in these industries aords them opportunities to sell their goods and services at
air-market values. Over ve years, COPE aims to target 20,000 orphans and vulnerable children and their caregivers,both directly and indirectly.
The Partners
EMG, based in Brussels, London, and Washington, DC, is an international consulting rm that serves donor agencies,governments, and private clients. For the past 25 years, EMG has applied business expertise to improving communi-ties’ economic, social, and physical inrastructures. In 2007, EMG became a wholly-owned subsidiary o the Australianbased-rm Cardno.
In Uganda, anzania, Mozambique, and Rwanda, EMG implements economic empowerment activities under COPE.18 EMG’s ocus in the program has been to develop a successul and sustainable approach to build up the economic capac-ity o orphans and vulnerable children and their caregivers, eectively increasing uture prospects or these children.Other services oered to caregivers by COPE through Aricare include community capacity building, access to health-care, lie skills training, and educational support. Tis case ocuses on a specic partnership in rural Uganda to oerinsights into good practices in market-driven approaches.
In Uganda, EMG partners with clusters o OVC caregivers on economic empowerment programs. Each caregiver clus-ter is composed o 10 groups consisting o 5–8 caregivers, each caring or an average o ve orphans. Tese clusters arethe COPE project’s primary entry point or training, enterprise development, and other services.
Fruits o the Nile is a Ugandan business that processes and exports dried ruit to markets in the U�. Fruits o the Nile was set up in the early 1990s as a way or Ugandan armers to avoid wasting resh ruit and to process and market their
resh ruits and vegetables using aordable, easy-to-construct, and environmentally riendly materials. Fruits o the Nilebuys sun-dried produce at air prices, as well as organizing training and maintenance services or operators o solar dry-ers, acilitating access to nance when possible.
17. UNAIDS, UNICEF, and WHO, 2007, “Children and AIDS: A Stocktaking Report, 2007,” Report o the “Unite or Children,Unite against AIDS” program (New York: UNICEF).
18. The Community-Based Orphan Protection and Empowerment (COPE) project is unded by PEPFAR and implemented throughUSAID. Aricare is the primary grantee, with EMG as its subcontractor.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 19/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 13
Following a market analysis and identication o caregiver needs and market opportunities, EMG brought togethercaregivers to build a partnership with the Fruits o the Nile. Caregivers are organized into clusters, given appropriatetraining, and linked into a business relationship with the export company. In addition, the caregivers are required toparticipate in a group savings program (similar to a village savings and loan association), a practice that creates urtherbuy-in and signies a commitment rom the group members.
Partnership Objectives
Te objectives o the partnership are to reach export markets with dried ruits, bring economic benet to the caregiverclusters, and to realize a prot or the private-sector partner. EMG acilitates the relationship and development o thechain as its contribution to achieving these goals.
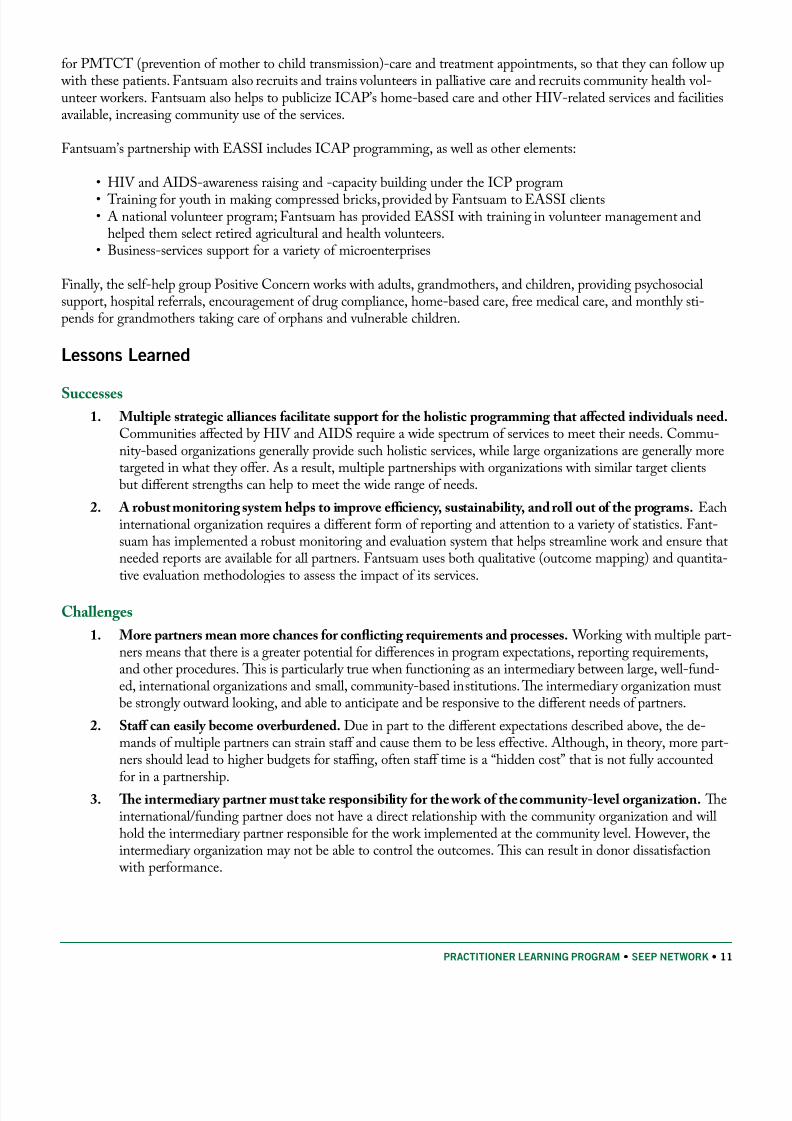
Each partner in the alliance plays a specic role according to its capacity: EMG develops caregivers’ skills and operatesas a acilitator, the caregivers produce the dried ruit and supply the buyer, and Fruits o the Nile buys the product romthe clusters. Te ollowing diagram illustrates the partner approach to achieve these objectives:
• Business Relationships
Formed
• Producers inserted in
Value Chain
EMG Input:
Entrepreneurial Training
EMG Input: Training
and Development
EMG SupportPhases Out
EMG Input: FacilitatedBusiness Linkages
• Group Formation
• Product Value
Increased
• Producers Prepared
for Value Chain
• Product Value
Increased Again
• Producers Move Up in
Value Chain
Partnership Activities and Results
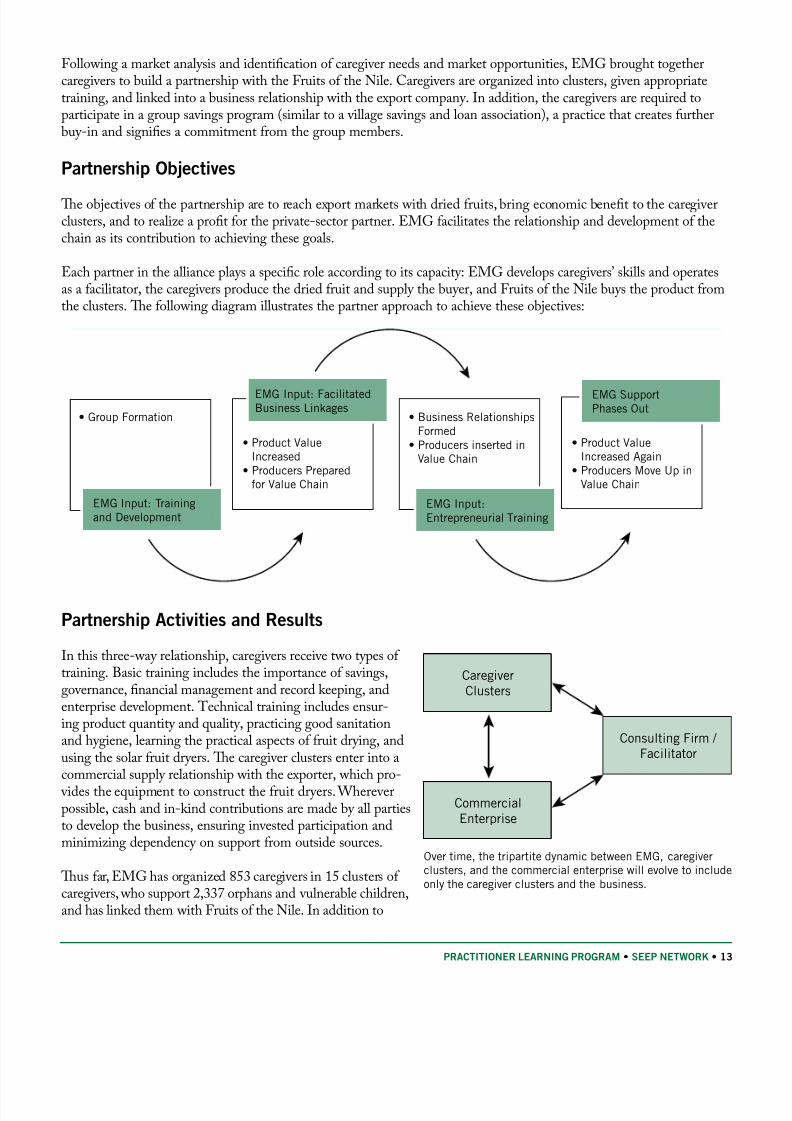
In this three-way relationship, caregivers receive two types o training. Basic training includes the importance o savings,governance, nancial management and record keeping, andenterprise development. echnical training includes ensur-ing product quantity and quality, practicing good sanitationand hygiene, learning the practical aspects o ruit drying, andusing the solar ruit dryers. Te caregiver clusters enter into acommercial supply relationship with the exporter, which pro-
vides the equipment to construct the ruit dryers. Whereverpossible, cash and in-kind contributions are made by all partiesto develop the business, ensuring invested participation andminimizing dependency on support rom outside sources.
Tus ar, EMG has organized 853 caregivers in 15 clusters o caregivers, who support 2,337 orphans and vulnerable children,and has linked them with Fruits o the Nile. In addition to
Consulting Firm /
Facilitator
Caregiver
Clusters
Commercial
Enterprise
Over time, the tripartite dynamic between EMG, caregiverclusters, and the commercial enterprise will evolve to includeonly the caregiver clusters and the business.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 20/24
14 • SEEP NETWORK • PRACTITIONER LEARNING PROGRAM
their sales o resh ruit in the local market, ruit drying has become a supplemental source o income or the caregiverclusters. Caregivers have seen a steady increase in the volume o their dried ruit sales to the company over the past yearand have earned a total o $8,128 in supplemental income. Tey have used this income to support the children in theircare with essential basic needs and even larger purchases, as well as reinvesting a portion o proceeds into their businesses.
Te commercial partnership model diers rom conventional income-generating interventions, in that EMG plays a a-cilitating role and phases out its involvement. Te project’s exit strategy includes a number o steps designed to increasethe sustainability o economic activities beyond the lie o the project. First, clusters are encouraged to work directly with
Fruits o the Nile, or example, by attending company trainings and meetings. COPE also helps the clusters register aslegal entities, making it easier to orm commercial relationships with buyers. In addition, the clusters have developed aFruit Dryers Association, made up o cluster representatives. COPE plans to build the association’s capacity or collec-tive negotiation and administration. In the uture, the association will take up EMG’s broker/acilitator role. Eventually,COPE’s MOU with Fruits o the Nile will be replaced with a ormal commercial agreement (and relationship) betweenthe association and Fruits o the Nile. Tis document would include guiding principles, as well as specic inormationabout price, quantity, and quality expectations.
Because the new relationship will be purely commercial, EMG’s phase-out plan includes identiying ways to reduce the vulnerability o caregivers, orphans, and other aected children to downward swings in the market. Tis might include,or example, encouraging caregivers groups to save additional money or investment or emergencies, and perhaps adding
matching savings rom the project.
Lessons Learned
Successes
Partnerships can bridge the gap between aected communities’ needs and economically-oriented market 1.actors. EMG’s acilitating role was to bring economic benets to the caregivers in a way that t their needsand constraints and that also met the buyer’s economic motivation. EMG understood both sides’ perspectivesand thus was well positioned to make this link.
Having a businesslike relationship with the commercial partner strengthened the partnership.2. Wheninitially approaching Fruits o the Nile, EMG ocused on the business case or engaging the producer groups.
It was clear that the company’s interest was in obtaining a reliable source or dried ruit at a air price. Tere-ore, negotiations ocused on this aspect o the relationship, rather than on charitable motivations or helping
vulnerable populations.
Planning an exit strategy or phase-out rom the outset is critical.3. All three parties in the partnership play vital roles and will be needed or some time. Eventually, however, it is important that the relationship becomea direct two-way relationship. As can be seen rom the case here, phase-out may be a lengthy process. Itshould happen gradually, to allow time or capacity building as needed and to gure out who will provide any key services that the existing acilitating partner used to provide.
Challenges
Market dynamics can aect the stability o commercial partnerships.1. Tis can cause particular challengesin partnerships between community organizations and businesses, as the community partner may not be ully aware o market dynamics and the eect these have on the partnership.
Commercial enterprises and subsidies can mix—i it is done right.2. Te costs o transport, storage, certica-tions, and other issues can eat away at businesses’ already-thin prot margins. However, a completely unsub-sidized approach is highly challenging in a setting with abundant charitable programs. One-time subsidies,such as building a small storage acility to serve as a demonstration model, motivated clusters to adopt thenew technology without running up high costs or the project or the buyer.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 21/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 15
Support services are critical to HIV and AIDS-aected community enterprises.3. However, receiving reeservices (uniorms, nutrition support, or health care) does not encourage a market mindset regarding theenterprise-development component o a project. Further, such services are not sustainable over the long run.
Te acilitating organization must work hard to mitigate the mixed message and reinorce a condent, sel-reliant attitude in their dealings with a commercial business. Promotion o savings clusters can do a great dealor sel-sufciency.
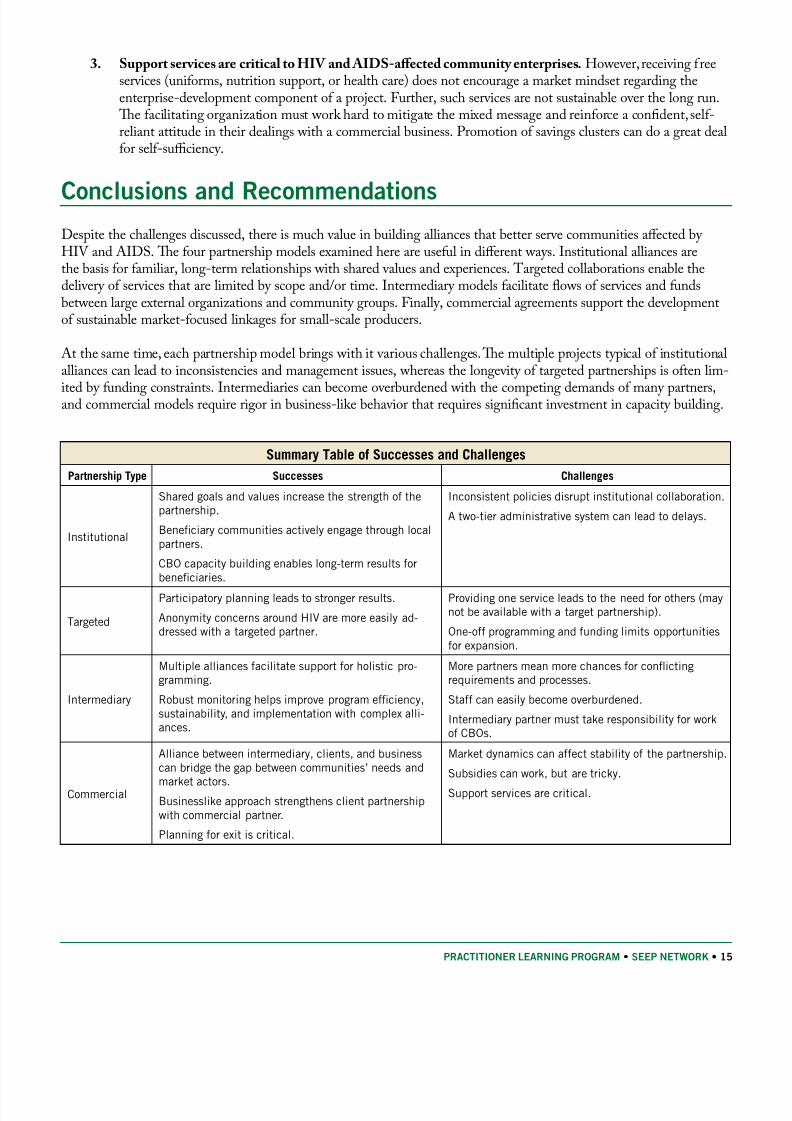
Conclusions and RecommendationsDespite the challenges discussed, there is much value in building alliances that better serve communities aected by HIV and AIDS. Te our partnership models examined here are useul in dierent ways. Institutional alliances arethe basis or amiliar, long-term relationships with shared values and experiences. argeted collaborations enable thedelivery o services that are limited by scope and/or time. Intermediary models acilitate ows o services and undsbetween large external organizations and community groups. Finally, commercial agreements support the developmento sustainable market-ocused linkages or small-scale producers.
At the same time, each partnership model brings with it various challenges. Te multiple projects typical o institutionalalliances can lead to inconsistencies and management issues, whereas the longevity o targeted partnerships is oten lim-
ited by unding constraints. Intermediaries can become overburdened with the competing demands o many partners,and commercial models require rigor in business-like behavior that requires signicant investment in capacity building.
Summary Table of Successes and Challenges
Partnership Type Successes Challenges
Institutional
Shared goals and values increase the strength o thepartnership.
Beneciary communities actively engage through localpartners.
CBO capacity building enables long-term results orbeneciaries.
Inconsistent policies disrupt institutional collaboration.
A two-tier administrative system can lead to delays.
Targeted
Participatory planning leads to stronger results.
Anonymity concerns around HIV are more easily ad-dressed with a targeted partner.
Providing one service leads to the need or others (maynot be available with a target partnership).
One-o programming and unding limits opportunitiesor expansion.
Intermediary
Multiple alliances acilitate support or holistic pro-gramming.
Robust monitoring helps improve program eciency,sustainability, and implementation with complex alli-ances.
More partners mean more chances or confictingrequirements and processes.
Sta can easily become overburdened.
Intermediary partner must take responsibility or worko CBOs.
Commercial
Alliance between intermediary, clients, and businesscan bridge the gap between communities’ needs and
market actors.Businesslike approach strengthens client partnershipwith commercial partner.
Planning or exit is critical.
Market dynamics can aect stability o the partnership.
Subsidies can work, but are tricky.
Support services are critical.
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 22/24
8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 23/24
PRACTITIONER LEARNING PROGRAM • SEEP NETWORK • 17
When constructing the dryers, the Fruits o the Nile company provided materials, EMG oered training, and caregivers contrib-uted room and board or the carpenters. In this way, each party had a stake in the success o the activity. All parties also areclear on who is paying or what, minimizing conusion.
Involve clients in the partnership.
Clients receive the most benet when they are active contributors to the partnership and its objectives. Tis may meanthat they participate in the ormation o the partnership, the design o the project, and/or project implementation.Sometimes, as with the EMG case, they are ormal partners and signatories to legal agreements. Te participatory pro-cess can build clients’ skills, increase understanding, and reduce the risk o conict or disappointment.
Defne sustainability strategies, including impact goals, up ront.In order to achieve successul outcomes, it is crucial or partners to share a long-term vision regarding the impact o theshared initiative and how this impact will be sustained. Planning or this vision, with a predened exit strategy, needsto happen up ront as part o the overall planning process. Using such tools as causal chains can assist in moving romproject activities to nal and lasting impact.
A long-term partnership makes it easier to measure long-term program impact. For example, several SILC groups started smallincome generating projects without any assistance rom Lieline. CRS Rwanda and the Caritas diocesan partners would like toharness this spirit and direct it into viable businesses. Given their ongoing collaboration, Caritas can readily keep CRS inormedo such developments.
Identiy sta dedicated to partnership management.
A project management team in which both partners participate acilitates smoother implementation and communica-tion. Institutional partnerships in particular have beneted rom the presence o a sta person solely responsible ormanaging the relationship between both organizations. He/she serves as a neutral conduit that can help tackle the
misunderstandings and unmet expectations that are bound to arise at some point in long-term relationships.
Ensure that policies and procedures are consistent and standardized.
Institutional partnerships by denition involve the joint implementation o several projects. Tere is, thereore, a needto create nancial, administrative, and program policies that are transparent and consistent across all projects sharedby partners to avoid eelings o rustration or unmet expectations on the part o partner sta and clients. When this isimpossible (e.g. due to donor regulations), partners should spend extra time making sure all understand the new or di-erent policies.
For more recommendations, readers are invited to read other publications rom this PLP and SEEP, particularly “Part-
nering to Achieve Economic Impact in HIV and AIDS Impacted Communities: A Partnership oolkit or Microen-terprise Development.”

8/8/2019 Basics Plp Technote Models
http://slidepdf.com/reader/full/basics-plp-technote-models 24/24
Bibliography
de Waai, A., and J. umushabe. 2003. “HIV and AIDS and Food Security in Arica.” Unpublished report prepared orDFID, February 1, 2003, 6.
Donovan, C., L. Bailey, E. Mpyisi, and M. Weber. 2003. “Prime-Age Adult Motility and Mortality in Rural Rwanda:Eects on Household Income, Agricultural Production, and Food Security Strategies.”International Development
Collaborative Working Papers, no. RW-FSRP-RR-12. East Lansing, MI, USA: Michigan State University, Depart-ment o Agricultural Economics. http://www.aec.msu.edu/s2/rwanda/RLDS3_2003.pd. Accessed August 2009.
Green, C. 2008. “Micronance and HIV/AIDS: Strategic Partnerships,” AMAP Micronance and HIV/ AIDS Note 2. Prepared or USAID by DAI. Washington, DC: USAID.http://www.microlinks.org/ ev.php?ID=22387_201&ID2=DO_TOPIC . Accessed August 2009.
MDG Monitor. Website. “MDG Prole: Ghana.” http://www.mdgmonitor.org/actsheets_00.cm?c=GHA . Accessed August 2009.
Planned Parenthood Association o Ghana. Website. http://www.ppag-gh.org/vision.asp . Accessed August 2009.
Te SEEP Network. 2008. Online document. In Guidelines for Microenterprise Development in HIV and AIDS-Impacted Communities. Book 2, For Microenterprise Development Practitioners . http://communities.seepnetwork.org/hamed/ node/27
. Accessed August 2009.———. “What �ind o Microenterprise Development Strategies Work or HIV and AIDS-Impacted
Communities?”section 2.3, (http://communities.seepnetwork.org/hamed/node/38 )
———. “How Can We Facilitate a Cross-Sector Partnership?” section 2.5. (http://communities.seepnetwork.org/ hamed/node/40, respectively. Accessed August 2009.
———. “Structural (Institutional) Challenges and Strategies or Cross-Sector Collaboration,” section 2.5.2 (http:// communities.seepnetwork.org/hamed/node/777 )
———. “echnical Challenges and Strategies or Cross-Sector Collaboration,” section 2.5.3 (http://communities.seepnetwork.org/hamed/node/778 ).
UNAIDS. 2008. “Report on the Global AIDS Epidemic.” (Geneva: Joint United Nations Programme on HIV/AIDS).
http://viewer.zmags.com/publication/ad3eab7c#/ad3eab7c/1 . Accessed August 2009.UNAIDS/WHO Working Group on Global HIV/AIDS and SI Surveillance. 2009. “Epidemiological Fact Sheet
on HIV and AIDS—Core Data on Epidemiology and Response: Rwanda 2008 Update.” Geneva: UNAIDS and WHO. 4, 7. http://apps.who.int/globalatlas/predenedReports/EFS2008/ull/EFS2008_RW.pd . Accessed August 2009.
UNAIDS, UNICEF, and WHO, 2007, “Children and AIDS: A Stocktaking Report, 2007,” Report o the “Unite orChildren, Unite against AIDS” program (New York: UNICEF).
UN Development Programme (UNDP). 2008. Website. Human Development Reports, Update 2008, Country FactSheets. “2008 Statistical Update: Rwanda—Human Development Index, Going beyond Income.” http://hdrstats.undp.org/2008/countries/country_act_sheets/cty_s_RWA.html . Accessed August 2009.
———. 2008. Website. Human Development Reports, Update 2008, Country Fact Sheets, “2008 Statistical Update:Ghana—Human Development Index, Going beyond Income,”http://hdrstats.undp.org/en/2008/countries/ country_act_sheets/cty_s_GHA.html . Accessed August 2009.
World Food Program (WFP). 2009. Website. Countries, “Rwanda (2008).”http://www.wp.org/country_brie/index-country.asp?country=646. Accessed August 2009.





























