Embed Size (px)
DESCRIPTION
John R. Guyton, M.D. Associate Professor of Medicine Duke University Durham, NC. Basics of Lipid and Lipoprotein Metabolism. Lipid Structure. Cholesterol. HO. Fatty Acids. Triglycerides. COOH. COO. COOH. COO. COOH. COO. HO. Phospholipid: Lecithin. +. Glycerol. COO. HO. COO. - PowerPoint PPT Presentation
Citation preview

Basics of Lipid andLipoprotein Metabolism
John R. Guyton, M.D.Associate Professor of Medicine
Duke UniversityDurham, NC

Lipid Structure
HO
Cholesterol
COOH
COOH
COOH
HO
HO
HO
+
Fatty Acids
Glycerol
COO
COO
COO
Triglycerides
COO
COO
OPOON
Phospholipid: Lecithin
+

HMG CoA Reductase(More Than Cholesterol Synthesis)
Acetyl CoA
HMG CoA
Mevalonate
Farnesyl Pyrophosphate
Cholesterol
HMG CoA ReductaseIsopentenyl
adenine(transfer RNA)
Prenylation ofsignalling peptides(ras, rho, etc.)
Ubiquinones(CoQ-10, etc.)Dolichols
Inhibition of other key products of mevalonate may relate tononlipid effects & rare side effects of statins.

NORMAL CHOLESTEROL METABOLISM
Tissuepools70G
0.8 GSYN CHOL*
*SYN CHOL = CHOLESTEROL SYNTHESIS
0.4 G CHOL

NORMAL CHOLESTEROL METABOLISM
Tissuepools70G
.65 G
.20 G
.20 G CHOL 0.65 G CHOL
0.85 GABS CHOL
50%
0.4 G CHOL
0.8 GSYN CHOL*
*SYN CHOL = CHOLESTEROL SYNTHESIS
1.3 GCHOL

Key concepts: synthesis– Primary synthetic sites are extrahepatic, but liver
is key regulator of homeostasis
Key concepts: absorption– Largest source is biliary secretion, not diet.– Normal absorption: 50%– For cholesterol to be absorbed it must:
• undergo hydrolysis (de-esterification by esterases)
• be incorporated into micelles
• be taken up by cholesterol transporter
• be re-esterified and incorporated into chylomicrons
NORMAL CHOLESTEROL METABOLISM

400 mg/day
1,300 mg/day
NORMAL CHOLESTEROL ABSORPTION
Oil phase

400 mg/day
1,300 mg/day
17,400 mg/day
NORMAL CHOLESTEROL ABSORPTION
Plant sterols competeFor cholesterol here
Oil phase

STRUCTURE OF PLANT STEROL ESTERS
HO
Cholesterol
Sitosterol
HO
O
C - O
Sitosterol Ester

400 mg/day
1,300 mg/day
17,400 mg/day
850 mg/day
NORMAL CHOLESTEROL ABSORPTION
Ezetimibe competesFor cholesterol here
Oil phase

400 mg/day
1,300 mg/day
17,400 mg/day
850 mg/day
NORMAL CHOLESTEROL ABSORPTION
Defect in ABCG5/G8transporter causesphytosterolemia
Oil phase

Role of Bile Salts, cholesterol, phospholipids in gall stone formation.
Importance of Bile Salts for cholesterol absorption
NORMAL CHOLESTEROL METABOLISM
Key concepts: bile salt absorption inhibitors– Bile acid binding compounds:
• Welchol
• Cholestyramine
• Colestipol
• Fiber
– Surgery: Partial ileal bypass.

Bile Acid Synthesis
HO
Cholesterol
OH
OH
OH
COOH
OH OH
COOH
OH
COOH
OH
OH
COOH
ChenodeoxycholicAcid
LithocholicAcid
CholicAcid
DeoxycholicAcid

NORMAL CHOLESTEROL METABOLISM
Tissuepools70G
0.8 GSYN CHOL
.65 G
.20 G
0.85 GABS CHOL
50%
0.4 G CHOL
1.3 GCHOL
.20 G CHOL 0.65 G CHOL

17 GBA*
NORMAL CHOLESTEROL METABOLISM
Tissuepools70G
0.8 GSYN CHOL
17.35 GBA*
0.85 GABS CHOL
0.35 G BA*
.35 G
.65 G
.20 G
1.20 GCHOL + BA
50% 95%
0.4 G CHOL
1.3 GCHOL
* BA = BILE ACIDS
.20 G CHOL 0.65 G CHOL

Key concepts: absorption– Triglyceride (i.e. energy) assimilation is key to
the survival of the organism.– Dietary triglyceride must be hydrolyzed to fatty
acids, mono-glycerides and glycerol prior to absorption.
– Fatty acids must partition to micellar phase for absorption.
– For transport, triglyceride must be reconstituted from glycerol and fatty acid and incorporated into chylomicrons.
NORMAL TRIGLYCERIDE METABOLISM

Structures of Fatty Acids
CHO
O
CHO
O
CHO
O
CHO
O
CHO
O
18:0
cis-18:1 -6
trans-18:1 -6
18:2 -6
18:3 -3

Structures of Fatty Acids
CHO
O
CHO
O
CHO
O
CHO
O
CHO
O
16:0 (palmitic)
cis-18:1 -6 (oleic)
trans-18:1 -6 (elaidic)
18:2 -6 (linoleic)
18:3 -3(alpha linolenic)
CHO
O 20:5 -3 (EPA)


FATTYACIDS
(ALBUMIN)
TG (VLDL)
TG (CHYLO-MICRONS)
LIPO-PROTEINLIPASE
Fatty Acid and Triglyceride Flux

PlasmaTriglyceride
(VLDL)
Dietary Carbohydrate Increases VLDL Production
DietaryCarbohydrate

Effect of Carbohydrate Restriction on Carbohydrate-induced Hypertriglyceridemia
0
500
1000
1500
2000
2500
3000
Initial Level End of Fast Inpatient LowCHO Diet
OutpatientLow CHO Diet
Reisell et al., Am J Clin Nutr 1966;19:84
Treatment: Fast for average 5 days, then consume low CHO diet.
Compositionof diet:
7-15% CHO25-30% Prot60-65% Fat

Lipoprotein Metabolism

Cholesterol Ester Synthesis
HO
Cholesterol
COOH
COO
COO
OPOON+
CholesterolEster
COO
COO
COO
OPOON+
Lysolecithin
Lecithin-Cholesterol Acyl Transferase (LCAT)
Acyl-Cholesterol Acyl Transferase (ACAT)





Lipoproteins:Separation by –
Electrophoresis
Density
Size by Electron Microscopy



Pancreatic Lipase Movement
Most pancreatic lipase is secreted into the pancreatic duct, but some moves back into capillaries.
Most pancreatic lipase is secreted into the pancreatic duct, but some moves back into capillaries.

Chylomicron Role in Pancreatitis
Pancreatic lipase actson chylomicrons adherent to capillaryendothelium, producingfatty acid anions, or soaps. By detergentaction, cell membranesare disrupted, releasingmore lipase, and additional fatty acidanions are produced ina vicious cycle.
Pancreatic lipase actson chylomicrons adherent to capillaryendothelium, producingfatty acid anions, or soaps. By detergentaction, cell membranesare disrupted, releasingmore lipase, and additional fatty acidanions are produced ina vicious cycle.





Apolipoproteins
B/E receptor ligand *E2:IDL; *E4: Diet ResponsivityapoE
LpL inhibitor; antagonizes apoEapoC-III
LpL activatorapoC-II
Inhibit Lp binding to LDL R; LCAT activatorapoC-I
apoB-48
Structural protein of all LP except HDL
Binding to LDL receptor
apoB-100
Tg metabolism; LCAT activator; diet responseapoA-IV
HL activationapoA-II
HDL structural protein; LCAT activator;RCTapoA-I

Metabolic RelationshipsAmong Lipoproteins
LDL
1.
3.2.
LipoproteinLipase`
TG
HDL
VLDL

TRIGLYCERIDES
HDLSMALL
DENSE LDL

Role of CETP in Triglyceride/Cholesteryl Ester Exchange
VLDL CETP HDL
TG
CE
LDLCETPHDL
TG
CE

Role of Triglycerides in Producing Small Dense LDL or HDL
TGTG TG
CE CE CECETP Lipase
1. CE exchanged for TG 2. TG removed

FREE FATTYACIDS
Dyslipidemia of Metabolic Syndrome
VLDL CETP
TG
CE
HDL LDLCETP
TG
CE
LIPASEsdLDL
FATTY ACIDSGLYCEROL
HDL CATABOLISM
UNINHIBITEDLYPOLYSIS

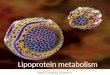
Distribution of LDL Size Phenotypes According to Triglyceride Levels
01020304050
60708090
100
0 50 100 150 200 250 300
Phenotype A(light fluffy LDL)
Phenotype B(small dense LDL)
Cum
ulat
ive
perc
ent o
f ca
ses
Triglyceride (mg/dl)
Austin et al, Circulation 1990; 82:495

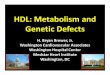
Peroxisome Proliferator-Activated Receptor:
A Nuclear Receptor for Metabolic Genes
a, Basic mechanism of action of nuclear hormone receptors: bind to a specific sequence in the promoter of target genes (called hormone response elements), and activate transcription upon binding of ligand. Several nuclear hormone receptors, includingthe retinoic acid receptor, the vitamin D receptor and PPAR, can bind to DNA only as a heterodimer with the retinoid X receptor, RXR, as shown. b, some PPAR and PPAR ligands.
Kersten et al. Roles of PPARs in health and disease. Nature 2000; 405: 421-424

Role of PPAR* and in VLDL, LDL
and HDL metabolism
* Peroxisome Proliferator Activated Receptor
PPAR Tissues: Liver, kidney, heart,muscle.Ligands: fatty acids, fibrates
Actions: Stimulate productionof apo A I, lipoprotein lipase,increase expression of ABC A-1, increase FFA uptake andcatabolism, decrease FFAand VLDL synthesis.
PPAR Tissues: Adipose tissue andintestine.Ligands: arachidonic acid, GlitazonesActions: increase expression ofABC A-1, increase FFA synthesisand uptake by adipocytes, increaseinsulin sensitivity (?)

HDL and Reverse Cholesterol Transport

HDL and Reverse Cholesterol Transport
Tangier DiseaseTangier Disease

HDL and Reverse Cholesterol Transport

HDL and Reverse Cholesterol Transport

HDL and Reverse Cholesterol Transport

LDL-R
HDL and Reverse Cholesterol Transport

LDL-R
50% of HDL C mayReturn to the liverOn LDL via CETP
HDL and Reverse Cholesterol Transport

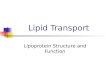
• An atherogenic lipoproteincontaining apo(a) and apoB.
• 20-30% of people have levelssuggesting C-V risk.
• Black subjects have Lp(a)normal range twice as highas white and Asiatic subjects.
• Apo(a) sequence similar to plasminogen, and Lp(a)interferes with spontaneous thrombolysis.
• Lp(a) levels highly genetic, resistant to diet and drugtherapy, although niacin may help.
““LDL”LDL”
Apo(a)Apo(a)
-S-S--S-S-
Lipoprotein(a), or Lp(a)



Summary – Lipid and Lipoprotein Metabolism
• Cholesterol absorption, synthesis, and disposition
• Triglyceride/fatty acid transformations and energy metabolism
• Lipoprotein core and surface components• Lipoprotein origins and destinations governed
by apo’s• Derangement in the metabolic syndrome• Reverse cholesterol transport – the dominant
direction• Lipoprotein(a)• Lipoproteins in the arterial wall