Embed Size (px)
Citation preview

WHO Collaborating Centre for Oral Health Care Planning and Future ScenariosCollege of Dental Science University of Nijmegen, The Netherlands
Basic Package of Oral Care

Basic Package of Oral Care
Jo E. FrenckenChristopher J. HolmgrenWim H. van Palenstein Helderman

Acknowledgments
We kindly acknowledge with sincere appreciationthe contribution made by Dr. R. Duckworth(England) and Dr. G.J. van Rhenen (theNetherlands) in writing part of this monograph.
During the writing, the authors consulted manyauthorities around the world, who gave freely oftheir time and advice. In particular, the authorswish to express their sincere gratitude to the fol-lowing who reviewed and contributed to the con-tent of the monograph: Dr. B. Mouatt (England),Prof. Dr. S. Poulsen (Denmark), Dr. D. Purdell-Lewis (England), Prof. Dr. A. Sheiham (England).
Special thanks must also be given to those whoassisted in the production of this monograph.These include Margaret Kavanagh, who correctedall the spelling and grammatical errors, and KeesHakvoort, who skillfully designed the layout.
We would like to thank the Government of theNetherlands, through its Ministry of DevelopmentCooperation, for demonstrating its trust in theWHO Collaborating Centre for Oral Health CarePlanning and Future Scenarios in Nijmegen and inthe Basic Package of Oral Care by financing theproduction cost of this monograph.

Contents
Acknowledgments 2
Preamble 4
Foreword 6
Oral Health Priorities for the Disadvantaged 7
Oral Urgent Treatment (OUT) for the emergency management of oral pain, infection and trauma 15
Preventing dental caries through Affordable FluorideToothpaste (AFT) 21
Managing dental caries through the AtraumaticRestorative Treatment (ART) approach 29
Personnel and equipment for OUT and ART 39
Recommendations for establishing and evaluatingBPOC demonstration programs 45
References 50

4
Preamble
Oral health remains a luxury for most of theworld’s population. This is especially true forthe disadvantaged irrespective of whetherthey live in some of the world’s most wealthyor the world’s poorest countries. Oral healthproblems remain a global problem and there-fore must be a global concern.
The Basic Package of Oral Health Care(BPOC), as presented in this report, repre-sents a fusion of concepts and approachesthat have developed over the last decade. Inpresenting this package, great emphasis hasbeen placed on approaches with proveneffectiveness and that are acceptable, feasi-ble and affordable for most disadvantagedcommunities.
The BPOC is regarded as an essential foun-dation to any oral health care provision in acountry or community. Only once the founda-tions are well established should other oralhealth provisions be considered. Regrettably,this is often not the case, and as a resultlarge sums of public money are spent oninappropriate and often ineffective facilities.
The essential components of the BPOC:Oral Urgent Treatment (OUT), AffordableFluoride Toothpastes (AFT), and AtraumaticRestorative Treatment (ART), are componentsthat the Oral Health Unit of the World HealthOrganization has developed and promotedthrough partnership with non-governmentalorganizations, academia and industry. It is aperfect example of how different partnersworking together for a common goal canadvance the boundaries of oral health care.

5
As an example, the dramatic decline in thelevel of caries in many Western Countriesover the past two decades was first recog-nized through an analysis of data in the WHOGlobal Oral Data Bank. This decline isbelieved to be largely the result of theincreased use of fluoridated toothpastes insuch countries. Since poorer segments of theworld’s population are unable to affordtoothpastes, WHO collaborated with industryto produce an effective and affordable fluo-ride toothpaste. After successful field trialsin Indonesia, affordable fluoride toothpastesare now available to many more of theworld’s population than ever before.
Another example is Atraumatic RestorativeTreatment. The Oral Health Unit of the WorldHealth Organization was one of the first torecognize the huge potential that the ARTapproach could offer for community-basedoral care around the world. For this reasonART was presented at headquarters of theWHO in Geneva on World Health Day in 1994to mark the beginning of the Year of OralHealth 1994/95. The WHO has continued tosupport ART in the form of the WHO ARTGlobal Initiative 1998-2000. This has seenthe global promotion of ART through educa-tion in the form of training packages and ARTmaster classes, community demonstrationprojects and technical assistance.
Now the essential components of basicoral care have been combined into a well-defined package, the next and crucial step isto evaluate the package as a whole in differ-ent settings around the world. To make thispossible WHO once again calls for partner-ship between governmental and non-govern-mental organizations, the health profession,the academic community and industry.
It is also inevitable that as technologies andapproaches develop the package will evolveto adopt those that are appropriate, afford-able and scientifically proven to be effective.For this reason, there is a continued andessential need to continue research intoareas that show potential.
This report would not have been possiblewithout the continued support of manyaround the world, in particular members ofthe WHO Collaborating Center for Oral HealthCare Planning and Future Scenarios, Collegeof Dental Science, University of Nijmegen,the Netherlands.
Lastly I would like to acknowledge thecontribution of my predecessors, Dr. GennadyPakhomov and the late Dr. David Barmes,who had both the imagination and courageto foster and support fledgling concepts andapproaches. Their farsightedness has maturedinto the BPOC - an essential step for theimprovement in oral health globally.
Prof. Dr. P.E. PetersenOral Health Unit, WHOGeneva

6
Foreword
Oral health is recognized as a fundamentalcontributor to general health. Oral healthproblems continue to affect people through-out the world. Although seldom life threaten-ing, these problems adversely affect people’swell being, quality of life and economic activ-ities. Governments allocate budgets for oralservices, but in many non-established marketeconomies (non-EME) the budgets are verylimited and the services are not alwaysdirected to those most in need. This leads tosituations in which large segments of thepopulation have limited or no access to oralhealth care, and hence continue to suffer.This situation calls for the establishment oforal health as a priority and for the imple-mentation of the essential components oforal health care that are affordable withinthe prevailing health infrastructures ofdeprived communities.
The Oral Health Unit of the World HealthOrganization charged the WHO CollaboratingCentre for Oral Health Care Planning andFuture Scenarios in Nijmegen, theNetherlands, with the task of compiling areport on the establishment of priorities inoral health care for deprived communitiesbased on proven and effective oral healthmeasures.

7
The philosophy of Primary Health Care (PHC),with its leading principle of basic oral carefor all and emphasis on prevention andaffordable and sustainable services, was aguideline in writing the report. The basicassumption was that the services offeredshould primarily meet people’s perceivedneeds and treatment demands. The secondassumption was that periodontal diseases arenot a major cause of tooth loss. Therefore,removing calculus by scaling tooth surfacesis not considered a priority. As the reportfocuses on oral health care within the con-text of PHC, the treatment of serious disor-ders, e.g., oral cancer, cleft lip and palatedisorders, are also not addressed.
The report outlines the basic premisebehind the three key components that con-stitute the Basic Package of Oral Care(BPOC). These are: Oral Urgent Treatment(OUT), Affordable Fluoride Toothpaste (AFT)and Atraumatic Restorative treatment (ART).
It argues for community-oriented promo-tion of oral health and affordable and effec-tive interventions. It suggests that the pack-age should be financed predominantly bypublic funding and implemented by compe-tently trained primary (oral) health careworkers.
This report is a policy document. It pres-ents the rationale that eventually leads topriorities in basic oral care. It is intended asa call to action for policy makers (ChiefDental Officers and advocates of oral healthcare at the Ministry of Health) and for part-ners in the development of oral health care(Non-Government Organizations (NGOs) andindustry).
The report does not provide an overview ofthe specific content of each proposed compo-nent. Neither does it outline the tasks of var-ious cadres of dental personnel nor does itpresent a strategy for implementation.Although of great importance, these ele-ments cannot be covered in one report. Eachlocal situation demands tailor-made solutionswith respect to the personnel involved, itscontent and extent of the service offered.
This report strongly recommends theimplementation of small-scale (demonstra-tion) projects to assess the effectiveness andsustainability of the basic package of oralcare under local conditions before introduc-ing the BPOC on a wider scale. In thisendeavor, NGOs and industry have an impor-tant role to play, particularly in the planningand evaluation stages. They should considerthemselves as partners to governments inworking toward improved oral health fordeprived communities.
Ass. Prof. Dr. FHM Mikx, Director WHO Collaborating Centre for OralHealth Care Planning and Future Scenarios


9
This chapter describes the prevailing
oral health problems among disadvan-
taged populations in both established
and non—established market econo-
mies. Untreated oral diseases, inequa-
lities in delivery systems and the
absence of adequate community—
oriented preventive services characte-
rize the current situation. There is an
urgent need for a change toward an
oral care system that meets the princi-
ples of primary health care (PHC).
A basic package of oral care (BPOC),
which is available to all, aims at
achieving the objectives of the PHC
approach. The three components of the
BPOC are 1) Oral Urgent Treatment
(OUT); 2) Affordable Fluoride
Toothpaste (AFT); and 3) Atraumatic
Restorative Treatment (ART). Oral
health promotion is considered an
integral part of BPOC. Each region and
country should develop its own BPOC
based on the perceived needs of the
local population and on existing sup-
porting environmental conditions.
Oral Health Priorities for the Disadvantaged 1

10
Introduction
Oral health problems exist for the disad-vantaged both in non-established marketeconomy (non-EME) and established marketeconomy (EME) countries. The difficulties areparticularly severe for many communities innon-EME countries, which often have little orno access to basic emergency treatment fororal pain and infections. In addition, thesecommunities usually have no organized sys-tem for the prevention of oral diseases.
In non-EME countries as well as in pocketsof deprivation in EME countries, the insuffi-ciency of resources for oral health and theshortage of dentists are commonly consid-ered the main barriers to future improve-ments. Increasing the number of dentists andstimulating individual-oriented oral healtheducation (OHE) provided by dental profes-sionals often are not feasible. An alternative,consisting of training primary health careworkers to undertake elements of basic oralcare and the integration of OHE into the pri-mary health care system, is rarely available.Although oral health is often a low priorityamong decision-makers, most non-EME coun-tries have public funds available for oralhealth care. The important question is howto utilize these funds appropriately to meetthe most urgent needs. Governments do notalways realize that there is a compelling needto develop basic oral health care systemsagainst the background of limited funding,existing infrastructures and perceived needsand treatment demands of the population.

11
The primary health care approach
Governments in many countries have adoptedthe primary health care (PHC) approach intheir national health care systems. PHCmeans redirecting the prevention and controlof common diseases away from hospital-based care. PHC aims to provide basic cura-tive and preventive care for all at a cost thatthe country and community can afford. Oraldiseases, particularly dental caries with itsearly onset, are among the most commondiseases. Therefore, oral care should be partof the PHC system. Unfortunately, oral care isinadequately integrated into the PHC systemsin many countries.
There is currently no sustainable basic oralcare service in PHC that can be univer-
sally adopted. Two main barriers pro-hibit proper inclusion of oral healthcare into the PHC system: den-tistry's traditional orientationtoward individual care rather than
a community approach, and itsinherent technical - rather than
social and behavioral - character. Thephilosophy of conventional dentistry mustchange to one of low-technology treatment,control and prevention to meet the perceivedoral health needs and treatment demands ofthe community. National epidemiological data on the preva-lence and severity of oral diseases are of lim-ited use in planning for basic oral healthcare. The emphasis on professional normativeepidemiological data on oral diseases andtreatment needs has seriously distorted peo-ple’s views on oral health and on determin-ing priorities for establishing needed servic-es. More meaningful indicators for the plan-ning of basic oral care include informationon the community characteristics, people'shabits and perceived oral health problemsand needs as well as the existing infrastruc-tures.
The emphasis on these indicators of need iscrucial. In addition to the needs observed bythe professional, it should reflect the per-ceived needs and wants of the consumer. Thiscollaborative approach has a better chance ofbeing integrated into the existing communityhealth care structures. However, since manynon-EME countries have insufficientresources to run even a rudimentary PHC sys-tem, proposals for a new oral health carestrategy must be viewed in the wider contextof the available PHC services.

12
The prevailing oral health situation
In many non-EME countries, the majority of12-year-old children have untreated dentalcaries, with risk of pain, disfigurement andspreading infections. This condition canresult in tooth loss at a relatively young age.Relief of pain is the predominant treatmentdemand of disadvantaged populations. Painis mainly caused by oral infections, which insome cases can be life-threatening. Peoplefrom disadvantaged communities do not visitclinics for preventive intervention or forrestorative treatment to prevent loss ofteeth. The standard of oral hygiene is usually
low and knowledge and habits relating tooral health are often poor.
Changes in attitude, leading todemands for more preven-tion-oriented treatment andchanges in lifestyle con-ducive to good oral health,will take time. In such cir-
cumstances, oral health pro-motion (OHP) is the corner-
stone of oral health self care. Itis vital to the control and preven-
tion of oral diseases in the future.Unfortunately, most populations in non-EMEcountries are not exposed to community-ori-ented OHP.
Oral health care in most rural and someurban areas in non-EME countries is difficultto obtain. If available, tooth extraction is thepredominant mode of treatment. Oral care isusually conventional in nature with theemphasis on technical and curative solutions,which are expensive and an option only forthe affluent sector of the population. Thistype of traditional dentistry overlooks theimportance of community-oriented preven-tion, exemplified by the improvement in oralhealth in EME countries. The history of den-tistry in EME countries demonstrates thatmerely increasing the numberof dentists does not con-trol dental caries. Itwas not until theacceptance of OHPand the introduc-tion of mass pre-ventive measures,particularly the pro-vision of fluoridatedtoothpaste, that theincidence of caries andgingivitis started to decline.Toothpaste, including fluoridated toothpaste,is available in most countries. However, inmany cases, the price is too high. Thus, situ-ations may occur in which people want to usetoothpaste (and toothbrushes), but cannotafford to do so.
Despite the general improvements in oralhealth achieved in EME countries, there aremany people who have not benefited suffi-ciently from effective preventive and curativeoral health services that are available. This isapparent in the excessive level of caries andthe disproportionate treatment needs of theyoung, deprived and socially disadvantagedgroups. This unfavorable situation is also seenin immigrant groups in many EME countries.
Oral health care inmost rural and someurban areas in non-
EME countries is difficult to obtain.
The history of dentistry in EME coun-
tries demonstratesthat merely increasingthe number of dentistsdoes not control dental
caries.

13
Rationale for the Basic Package for OralCare (BPOC)
The situation in most non-EME countries andin disadvantaged communities in EME coun-tries calls for a change in approach.Traditional western oral health care shouldbe replaced by a service that follows theprinciples of PHC. This implies that moreemphasis should be given to community-ori-ented promotion of oral health. Treatmentthat is affordable for governments and indi-viduals should also receive more attention.Using this approach, the level of untreateddental disease will become manageable. Abasic package of oral care (BPOC) aims toreach all people at a much lower cost thantraditional oral health services. The threecomponents of BPOC are:• Oral Urgent Treatment (OUT)• Affordable Fluoride Toothpaste (AFT)• Atraumatic Restorative Treatment (ART)
Oral health promotion forms an integral com-ponent of BPOC to heighten awareness ofwhat is possible. The successful introductionof BPOC in a community relies to a largeextent on good communication among allparties involved. There is no single modelsuitable for universal application. Eachregion or country should develop its ownBPOC based on the perceived needs of itspopulation and on the utilization of existinghealth care structures. The latter point is cru-cial. Too many oral health programs havefailed as a result of management, logisticaland financial problems because they wereorganized apart from the existing PHC. Thefollowing chapters highlight the general principles behind the three compo-nents of BPOC and provide evidence of theireffectiveness.
Each region or country should developits own BPOC based on
the perceived needs of itspopulation and on theutilization of existinghealth care structures.

Oral Urgent Treatment (OUT) for the emergency

15
Chapter 2
This chapter discusses services targeted
at the emergency relief of oral pain,
management of oral infection and
dental trauma through Oral Urgent
Treatment (OUT). Access to this
component of basic oral care is a
fundamental right for everyone.
Therefore, governments must take the
responsibility to establish and main-
tain a functional OUT service that is
accessible and acceptable to the entire
population.
management of oral pain, infection and trauma 2

16
What is OUT?
Oral Urgent Treatment (OUT) is an on-demand service providing basic emergencyoral care. An OUT service must be tailored tothe perceived needs and treatment demandsof the local population. Thus the precise con-tent of an OUT service will differ from coun-try to country and possibly from district todistrict within the same country.
The three fundamental elements of OUT com-prise:• Relief of oral pain• First aid for oral infections and dento-alveolar trauma• Referral of complicated cases.
It is anticipated that an OUT service would beable to manage the majority of cases requir-ing basic emergency oral care. The maintreatment modalities would include: • Extraction of badly decayed and severely periodontally involved teeth under local anesthesia• Treatment of post-extraction complicationssuch as dry sockets and bleeding; • Drainage of localized oral abscesses• Palliative drug therapy for acute oral infections• First aid for dento-alveolar trauma• Referring complicated cases to the nearest hospital.
Why is there a need for OUT?
Although most oral diseases are not life-threatening, they constitute an importantpublic health problem. Their high prevalence,public demand for treatment, and theirimpact on the individual and society in termsof pain, discomfort, functional limitation andhandicap affect the quality of life. In addi-tion, the social and financial impact of oraldiseases on the individual and communitycan be very high.

17
Pain relief
In non-EME countries, the most common oralhealth problems and the use of oral healthservices are strongly related to pain and dis-comfort. The relief of pain is considered thepredominant treatment demand in many pop-ulation groups. Dental decay is the maincause of toothache. In these circumstancespain relief is achieved through extractingbadly decayed teeth. Despite treatment ofdental decay through tooth extraction, ahigh percentage (>90 %) of decayed teethare left untreated in many countries.In order to stop oral pain, people usuallyresort to medicines. Large sums ofmoney are spent on pharma-ceutical painkillers, antibi-otics and traditional medi-cines. Often the use ofmedicines is not followedup by treatment of thesource of the pain. Thecombination of palliativedrug therapy and operativetreatment should be empha-sized in a proper OUT situation.It is important to note that theinappropriate use of antibiotics for oralinfections, such as localized abscesses, car-ries the risk of seriously affecting the effica-cy of these medicines when used in life-threatening conditions. A report entitled‘Antibiotic use in Dentistry’, from theAmerican Dental Association (1997), pointedto the alarming increase in microbial resist-ance to antibiotics. It cautioned dental pro-fessionals against the overuse of antibiotics.A number of studies carried out in variouscountries on antibiotic use in dentistry deter-mined that antibiotics were prescribedunnecessarily in 22 to 74 percent of cases.
The inappropriate use of antibiotics for oral
infections, such as local-ized abscesses, carries
the risk of seriouslyaffecting the efficacy ofthese medicines when
used in life-threateningconditions.

18
First aid for oral infections and dento-alveolar trauma
Oral InfectionsThe most common oral infection that requiresassistance in an OUT situation is the local-ized dental abscess. This condition usuallyresults from untreated dental decay and/orperiodontal disease. Health personnel shouldbe able to provide first aid to people withoral infections.
Dento-alveolar traumaThe second most common reason for childrento visit the dental clinic for emergency careis the management of dental trauma. Themost frequent types of dental trauma includeenamel and enamel-dentine fractures.Studies investigating the prevalence ofuntreated dental trauma among children upto age 15 ranged from 7 to 50 percent,depending on age and location. These datashow that there is a need for organized careto manage dental trauma within the govern-ment medical health services. It is knownthat late complications of dental injuries maylead to pulp death, root resorption and lossof alveolar bone.
Until recently traffic accidents were themost frequent cause of dental and facialtrauma in EME countries. Currently (domes-tic) violence and sports accidents are theleading cause. However, in most non-EMEcountries traffic accidents remain the majorreason for dental and facial trauma.Reduction in dental and facial trauma isattributed to stronger legislation on alcoholrestrictions for drivers, the compulsory wear-ing of seatbelts, safety requirements for vehi-cles and better road conditions.
Referral of complicated cases
In line with the referral system in use in acountry’s health infrastructure, complicatedcases require referral to specialists. OUT per-sonnel should be adequately trained on thecircumstances that require referral to an oralhealth professional.
Conclusion
Emergency oral care that is easily accessiblefor all should be the first priority in any oralhealth program. OUT should be integratedinto the PHC system at a sub-district leveland should make use of PHC facilities in bothurban and rural areas.

19
Bijschrift BijschriftBijschrift
Bijschrif Bijschrift Bijschrift
Bijschrift Bijschrift
Bijschrift Bijschrift Bijschrift

Preventing Dental Caries

21
Chapter 3
The use of fluoride toothpaste is con-
sidered to be the most efficient means
of controlling dental caries. However,
for it to be effective, the fluoride in
the toothpaste needs to be bio-
available at a sufficient concentration
at the tooth surface. This chapter dis-
cusses these aspects and ways in which
governments and industry can ensure
the availability of effective fluoride
toothpaste at an affordable cost to
consumers.
through Affordable Fluoride Toothpaste (AFT) 3

22
Fluoride for the control of caries
Exposure to the correct amount of fluoride isconsidered by the World Health Organizationto be the most effective preventive measureagainst caries. Unfortunately, in most non-EME countries the recommended fluoridationof water and salt may not be easily attain-able, since they lack the required infrastruc-ture, technology and resources, particularlyin rural areas. A report of an internationalworkshop on fluoride states unequivocallythat fluoride toothpaste is one of the mostimportant delivery systems for fluoride. Thecaries-reducing effect of fluoride is almostexclusively topical, which explains the anti-caries efficacy of fluoride toothpaste.
Why fluoride toothpaste?
The anti-caries efficacy of fluoride tooth-paste has been proven in an extensive seriesof well-documented clinical trials. Thesestudies have involved different sources of flu-oride (sodium fluoride, sodium monofluo-rophosphate, etc.), different levels of fluo-ride (mainly 1,000 and 1,500 ppm F_) anddifferent abrasive systems (for example, sili-ca, chalk, alumina, etc.).
In many EME countries, there have beensubstantial reductions in dental caries overthe past few decades. The number of teethaffected by caries (DMFT)decreased from about8 to about 1.5 for12-year-oldsMost scientistsagree that thedecline indental cariesin EME coun-tries can beattributedmainly to thewidespread use offluoride toothpaste,particularly through twice-dailytoothbrushing with fluoride toothpaste.
Variations in the level of dental caries,both within and between non-EME countries,have been reported, so it is difficult to drawstrong conclusions regarding the trend indental caries in these countries. In areaswith ongoing traditional lifestyles, the preva-lence of dental caries may remain fairly sta-ble. In some urban areas, the level of dentalcaries may increase. This assumption is basedon changing dietary patterns and increasedsugar consumption. In general, it can beconcluded that there are contrasting trendsin caries prevalence in children in EME com-pared to non-EME countries: EME countrieshave a decreasing trend while non-EME coun-tries with improving economies show anincreasing trend.
Widespread and regularuse of fluoride tooth-
paste in non-EME coun-tries would have an enor-mous beneficial effect on
the incidence of dentalcaries and periodontal
disease.

23
The interesting phenomenon in EME coun-tries is that the incidence of caries hasdeclined tremendously, although the totalamount of sucrose consumption per capitahas hardly changed. Where oral hygiene withfluoride toothpaste is adequate, diet hasbecome a less significant factor in caries pre-vention. Hence, promotion of the exposureto fluoride through twice-daily toothbrushingwith fluoride toothpaste is the first step inthe prevention of caries. More than one bil-lion people in EME countries use fluoridetoothpaste for toothbrushing. This provenoral hygiene adjunct is the best cariesreduc-ing measure. Therefore, widespread and regular use of fluoride toothpaste in non-EMEcountries would have an enormous beneficialeffect on the incidence of dental caries andperiodontal disease. Nevertheless, in non-EME countries, widespread and regular use offluoride toothpaste is uncommon. In additionto the benefits for preventing caries, tooth-brushing has a favorable impact on the con-dition of periodontal tissues.
Bijschrift BijschriftBijschrift
Bijschrif Bijschrift Bijschrift
Bijschrift Bijschrift
Bijschrift Bijschrift Bijschrift

24
Developing an effective, low-cost fluoridetoothpaste
The price of toothpaste is often too high innon-EME countries. Therefore many peoplecannot afford to use it regularly.Collaboration between the WHO Oral HealthProgram and industry resulted in the devel-opment of a new, low-cost fluoride tooth-paste (SMFP), which proved to have anti-caries efficacy in a school-based oral healthprogram in Indonesia.
Supervised daily toothbrushing with SMFPtoothpaste (1,000 ppm F_) in a Chinesekindergarten, under conditions prevailing ina rural county in China and with minimalinvolvement of oral health personnel, alsodemonstrated the effectiveness of this pre-ventive approach. After three years of study,a 43 percent reduction in caries was foundamong children who performed daily super-vised toothbrushing with fluoride toothpasteand who received oral health education ascompared to control children. In each ofthese studies, cooperation among dentalacademia, local government authorities andindustry was the key to success.
Access and promotion
Promotion campaigns are required to attainwidespread and regular use of fluoride tooth-paste by people in non-EME countries. Animportant aspect in the outcome of suchactivities is the cost of the promoted tooth-paste. All parties involved, i.e. governments,toothpaste manufacturers, the dental profes-sion, and most important, the general popu-lation, would benefit if twice-daily tooth-brushing with a pea-sized quantity of fluo-ride toothpaste were to become a widespreadhabit. Therefore, these parties should com-bine their efforts to reduce theprice and to stimulate theuse of fluoride tooth-paste with anti-cariesefficacy.
Governments should recognize the enormous
benefits of fluoridetoothpaste to oral health
and should take theresponsibility to reduce
or eliminate the tax bur-den on this product.

25
Toothpaste is often regarded by governmentsas a cosmetic product and is, therefore, sub-ject to a higher level of taxation. This, inturn, makes toothpaste less affordable.Governments should recognize the enormousbenefits of fluoride toothpaste to oral healthand should take the responsibility to reduceor eliminate the tax burden on this product.Preferential tax consideration for toothpasteshould be considered only when the tooth-paste has been shown to have not simplyappealing claims but proven anti-caries effi-cacy as well. The highest priority for toothpastemanufacturers should be to producetoothpaste with anti-caries efficacy,which people will buy and use. Anaffordable fluoride toothpaste thatis “low cost” should not imply “lowquality”. Efficacy should be thehighest priority. Fortunately, fluo-ride is a comparatively inexpensiveingredient. In contrast, such cos-metic components as flavor andpackaging, which contribute to theintrinsic consumer appeal of tooth-paste, are relatively expensive.Manufacturers are striving to produce lower-cost packaging for toothpaste. For example,sachets, rather than tubes, have been triedand have not detracted from consumerappeal. Moreover, producing paste in smallercontainers lowers the unit cost to the con-sumer, which can also influence the decisionto buy.
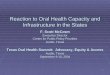
Fig 3.1 Supervised tooth-
brushing by school children
in different countries

26
With economic growth, lifestyle changesoften follow. People start to change theirdiets, pay more attention to their appearanceand buy products, such as carbonated softdrinks, snacks and cosmetics, associated withthese changes. However, it remains uncertainhow people will decide which items get prior-ity. The consumer may regard toothpaste pri-marily as a cosmetic that helps improve hisor her looks and the way his or her mouthfeels. Hence, the use of toothpaste may wellfit into the new lifestyle. Advertisements fortoothpaste should appeal to public senti-ments of changing lifestyle and awareness ofgood oral health. This requires cooperationamong government, toothpaste manufactur-ers and the health care profession in nationaladvertisement campaigns. These campaignsshould be combined with long-term rein-forcement programs of oral health educationstressing the use of oral hygiene with fluo-ride toothpaste at an early age.
Using fluoride toothpaste effectively
Oral hygiene education should include adviceon toothcleaning habits. Research has shownimportant links between the anti-caries effi-cacy of fluoride toothpaste and the way inwhich it is used. The two most important fac-tors are brushing frequency and rinsinghabits. Twice-daily brushing is recommendedbecause it improves anti-caries efficacy com-pared to brushingonce a day.Thorough rinsingafter brushingreduces theefficacybecause itreduces fluoridein the mouth tosub-optimal concen-trations. Therefore, no rinsing or rinsingonly once after brushing, followed byexpectoration of the remaining tooth-paste, is recommended
Education should also be targeted at theamount of toothpaste used. It is nowrecommended that only a ‘pea-sized’ amountof toothpaste, about 0.5 g, be used.Toothpaste can be used with a toothbrush orchewing stick if that is the cultural norm.This small amount of fluoride toothpastedoes not appear to reduce the effectivenessof the toothpaste. Besides, by using a small-er amount of toothpaste per brushing, thetoothpaste will last longer, thereby making itmore affordable. The main reason for recom-mending a pea-sized amount of toothpaste isthe concern for young children who are lessable to expectorate and who may ingest toomuch toothpaste, which might lead to dentalfluorosis. To prevent dental fluorosis, it isalso recommended that an adult supervisetoothbrushing of children younger than sixyears of age. Clear instructions on the effi-cient use of the toothpaste, including theoptimum amount of toothpaste to use, cor-rect rinsing methods, and advice on supervis-ing young children, should be printed on thetoothpaste package.

27
Ensuring the efficacy of fluoride toothpaste
Recent analyses of toothpaste in several non-EME countries have shown that not all fluo-ride toothpaste on the market contains suffi-cient amounts of free ionized fluoride (NaF)or ionizable fluoride (SMFP). The efficacy offluoride toothpaste depends on the amountof free ionized or ionizable fluoride. Mostfluoride toothpastes, particularly privatebrands, are categorized as cosmetic products.They do not require approval from any regu-latory body and therefore need not demon-strate proven anti-caries efficacy. Besides,many non-EME countries do not have ade-quate control mechanisms. Analyses areneeded in non-EME countries to monitorlocally available fluoride toothpastes fortheir anti-caries efficacy. The WHOCollaborating Centre in Nijmegen, theNetherlands, can act as an independent insti-tute for monitoring the amount of free ion-ized or ionizable fluoride in locally producedtoothpastes.The fluoride toothpastes on the market havevarying concentrations of fluoride. The bestchoice might be toothpaste with between1,000 and 1,500 ppm fluoride, since it seemsthat 1,000 ppm fluoride in toothpaste ismore effective than lower concentrations offluoride. A higher concentration of fluoride(>1,500 ppm F_) in toothpaste has the inher-ent risk of causing dental fluorosis whenused by young children.
Recommendations
1. Affordable fluoride toothpaste with anti-caries efficacy should be made available to all to ensure that all populations are exposed to adequate levels of fluoride by the most appropriate, cost-effective and equitable means2. The packaging of the fluoride toothpastes should be clearly labeled with:• The fluoride concentration and the descriptive name of the fluoride compound• Descriptive names of other ingredients, such as abrasives• Production and expiration date• Instructions for using a pea-sized amount of paste• Directions for proper rinsing after brushing• Advice for adult supervision of toothbrushing by young children. 3. The method of dispersal of toothpaste should facilitate the use of small amounts of the paste.4. An independent laboratory should moni-tor the fluoride content of toothpaste.5. Fluoride toothpaste that meets recommended standards for efficacy should be tax-free and classified by governments as a therapeutic agent rather than a cosmetic.

Managing dental caries through the

29
Chapter 4
Atraumatic Restorative Treatment
(ART) is an appropriate approach to
the treatment of dental caries because
it is not limited to the confines of a
dental clinic. ART thus increases
affordability, availability and accessi-
bility of dental treatment. ART has
been demonstrated to be effective for
the management of single-surface
cavities and for fissure sealants. It is
acceptable to patients. As such the
approach complements primary caries
preventive methods as part of a basic
package of oral care.
Atraumatic Restorative Treatment (ART) approach 4

30
Introduction
While preventive methods, such as affordablefluoride toothpaste, continue to make a largeimpact on the level of caries, some cariouslesions inevitably progress to cavitation. Inthe absence of restorative treatment, thisleads to pain, infection and ultimate loss ofthe tooth.
Conventional restorative treatmentapproaches rely heavily on electrically drivenequipment that is expensive and difficult tomaintain. Moreover, the complexity of theequipment required usually restricts thetreatment setting to a dental clinic. Thus,conventional restorative treatment for manynon-EME countries and communities hasbeen shown to be impractical on the groundsof cost, availability and accessibility.
Atraumatic Restorative Treatment (ART) is anovel approach to the management of dentalcaries that involves no dental drill, plumbedwater or electricity. The approach consists ofmanually cleaning dental cavities using handinstruments. The cavities and adjacent fis-sures are filled with an adhesive, fluoride-releasing restorative material. An ART sealantcan be applied in pits and fissures with evi-dence of enamel caries but without cavita-tion. The ART approach is entirely consistentwith modern concepts of preventive andrestorative oral care, whichstress maximum effort inprevention and minimalinvasiveness of oraltissues. Moreover,since all soundtooth tissue isretained during thecleaning of the cav-ity, pain and dis-comfort are rare dur-ing treatment, virtuallyeliminating the need foran anesthetic. The elimina-tion of the need for a dental drill or localanesthesia with ART means the approach isextremely well accepted even by young chil-dren who have never had dental treatmentbefore.
Appropriately trained dental auxiliaries,such as dental therapists, can perform ART atthe lower level of the health care pyramidsuch as in health centers and in schools. Thismakes restorative treatment more affordable,while simultaneously making it more avail-able and accessible. ART, therefore, meetsthe principles of PHC: prevention (throughsecondary prevention), appropriate technolo-gy, affordable treatment and equitable distri-bution of services. A textbook on ART, byFrencken and Holmgren, provides a detailed,step-by-step description of the ARTapproach.
Atraumatic RestorativeTreatment (ART) is anovel approach to themanagement of dentalcaries that involves nodental drill, plumbedwater or electricity.

31
Effectiveness of the ART approach
The effectiveness of hand instruments foropening tooth cavities has been studied. InZimbabwe adolescents belonging to a low-caries risk group, it was possible to gainaccess to tooth cavities with a dental hatchetin 84 percent of the dentinal lesions judgedto be in need of treatment. Dentinal lesionsin approximal surfaces of anterior teeth,however, were judged to be difficult to treatusing ART.
In Syria, in a younger age group (6-8-yearolds) with high-caries risk, it was possible totreat at least 90 percent of the dentinallesions in the primary dentitions. The compa-rable figure in the permanent dentition inthis age group was 54 percent.
The use of excavators for removing infect-ed carious dentine was in use long before theadvent of rotary instruments and their effec-tiveness has been clearly demonstrated.
Survival of ART restorations
Current research on the ART approach hasmainly investigated the approach in single-surface carious cavities using glass ionomeras a restorative material. In earlier ART stud-ies a low-stress bearing glass ionomer(ChemFil, ChemFil Superior, Fuji II) was used.More recent studies have used a medium-stress bearing glass ionomer specifically
developed for the ART approach (Fuji IX,KetacMolar, ChemFlex).
The use of the ARTapproach for the restoration of
multiple-surface carious cavi-ties using glass ionomershould be carefully consid-ered. Studies evaluatingmultiple-surface ARTrestorations are currently
being carried out. As evalua-tion results are not yet avail-
able, the indication for the useof ART is currently limited to sin-
gle-surface carious cavities. Therefore,in order to ensure consistent and reliableresults with ART, careful selection of casesand restorative materials is required.
How good are ART restorations in the per-manent dentition?
The majority of studies evaluating ARTrestorations have been made in the perma-nent teeth of adolescents. At this age, den-tine caries are most common in pits and fis-sures. Hence the studies that are presentedin Figure 4.1 refer only to single-surface ARTrestorations of longer than one year.
With the exception of the earlier studies,when the ART approach was still being devel-oped, it can be concluded that the one-yearsurvival rate of single-surface ART restora-tions used in permanent dentition liesbetween 95 and 100 percent and that thetwo- and three-year survival rates liebetween 92 and 94 percent and 85 and 89percent, respectively. When ART restorationsfrom the 1996-1999 China study were classi-fied into “small” restorations (less than halfthe occlusal width) and “large” restorations(greater than half the occlusal width), thethree-year survival percentages were 92 per-cent and 77 percent, respectively. The overallresults suggest that the average annual fail-ure rate for ART restorations is about 4-5percent for the first three years.
The one-year survivalrate of single-surfaceART restorations used
in permanent dentitionlies between 95 and100%; the two- andthree-year survival
rates lie between 92and 94% and 85 and89%, respectively.

32
Figure 4.1 Overview of sur-
vival of single-surface ART
restorations in permanent
dentition longer than 1 year
100%
90%
80%
70%
60%
50%
40%
1 year 2 year 3 year
China (1996-1999)
China (1997-1999)
Hong Kong (1995-1997)
Pakistan (1995-1997)
Syria (1998-2001)
Tanzania (1992-1994)
Thailand (1991-1994)
Zimbabwe (1993-1996)
Zimbabwe (1994-1997)
Figure 4.2 Overview of sur-
vival of single-surface ART
restorations in the primary
dentition longer than 1 year
100%
90%
80%
70%
60%
50%
40%
1 year 2 year 3 year
China (1996-1998)
China (1997-1999)
China (1997-1999)
Syria (1997-2000)
Thailand (1991-1994)

33
Figure 4.3 Survival results
of restorations prepared
with hand instruments and
filled with glass-ionomers
(ART) compared to restora-
tions produced using rotary
instruments and amalgam
100%
80%
60%
40%
20%
0%
1 year 2 year 3 year
Mal
awi
Paki
stan
Tanz
ania
Syri
a
Thai
land
ART
MTA
1year study:
Malawi (1990)
2 year study:
Pakistan (1995-1997)
Tanzania (1992-1994)
3 year study:
Syria (1998-2001)
Thailand (1991-1994)

34
ART restorations vs. conventional restorations
Permanent dentitionAs with all restorative procedures, survival isinfluenced by many factors. These includethe caries risk profile of the population, thepractice environment, the operator and thematerials used. Numerous studies haveassessed the quality of amalgam and compos-ite resin restorations. Comparisons betweenstudies are difficult because of diverse studydesigns, evaluators and evaluation criteria.Therefore, only estimates can be made aboutthe average life span of an amalgam andcomposite resin restoration in general dentalpractice. Survival of these types of restora-tion varies considerably and ranges from fiveto more than 20 years. The outcomes fromconventional restorations are considered thereference point to which the ART restorationsshould be compared. A few studies have com-pared restoration survival of ART to thatusing the conventional approach. The studieswere conducted among school children inMalawi, Tanzania, Pakistan and Syria andamong school children and adults inThailand. The results of these studies are pre-sented in Figure 4.2.
There was no statistically significant differ-ence reported between the survival of con-ventionally placed amalgam and ART restora-tions using glass ionomers in single-surfacesafter one year in Malawi and two years inPakistan and Tanzania. Only in the earlierThailand study was a statistically significantdifference reported between the survival ofconventionally placed amalgam and ARTrestorations in single-surfaces after threeyears. The amalgam restorations performedbetter. However, recent results from Syriashowed no statistically significantdifference between single-surface ART and amal-gam restorations afterthree years. Thesefindings indicatethat ART restora-tions in single-sur-faces in permanentteeth perform aswell as conventionalamalgam restorations.However, these short-term findings should be con-firmed in longer-term comparativestudies.
Deciduous teethOnly one study has investigated the differ-ence between ART restorations using a medi-um-stress bearing glass ionomer and conven-tional amalgam restorations in the deciduousdentition. The three-year survival of single-surface ART and amalgam restorations inSyrian school children were 86 percent and80 percent, respectively. This difference wasstatistically significant in favor of ART. Thesurvival outcomes for single-surface ARTrestorations in primary teeth longer than oneyear are shown in Figure 4.3.
Results indicate that ART restorations in
single-surfaces in perma-nent teeth perform aswell as conventional
amalgam restorations.

35
The three China studies show differences inresults over two years, although the newerimproved glass ionomers were used in allthree studies. In the first two studies inChina, where lower survival rates wereobserved, the restorations were placed underfield conditions in very young children bydental therapists and dental students. In thethird study in China, where higher survivalrates were reported, an experienced dentistplaced the restorations in older children. It islikely that the differences were largely due tooperator performance. In Syria, an operatoreffect was observed among the eight dentistswho placed the ART restorations. Thus, itseems that when experienced operators placesingle-surface ART restorations in primaryteeth, the survival rates approach those seenfor ART restorations in permanent teeth.While ART has the potential to be particularlyuseful in providing care for the young child,the results of studies thus far need to beconfirmed by other investigations.
ART related sealants
The success of sealants must be considered intwo ways. While retention rate has routinelybeen used as a criterion for success, the ulti-mate success of a sealant should beexpressed in terms of its ability to preventcaries, which is the primary purpose ofsealants. Thus, biological outcomes shouldtake precedence over mechanical outcomes.
Sealing surfaces with glass ionomer aspart of the ART approach seems to be benefi-cial. In Zimbabwe, after three years, compa-rable surfaces that were not sealed had afour times higher chance of developing adentinal lesion than those that were sealed.Despite the somewhat lower retention rateobtained with glass ionomer compared tocomposite resin sealants, its caries- preven-tive effect is still very acceptable. In thestudies in Zimbabwe and China, caries pro-gressed in 2 to 4 percent of the surfaces thathad been sealed after three years and thenonly in those teeth that had lost the sealant.
More recent studies of ART sealants haveused both improved materials and methodsof placement and careful selection of sur-faces in high-risk individuals with earlyenamel lesions and with deep fissures. Thethree-year survival of 71-72 percent for par-tially and fully retained glass ionomersealants is extremely encouraging consi-dering they were placed under field condi-tions.

36
The acceptability of ART
Discomfort during treatmentIn Pakistan, patient discomfort was com-
pared for restorations placed using ART withthose placed using conventional procedures,i.e. rotary drill and amalgam, in patientsaged 6-16 years. Discomfort was reported infewer restorations placed with ART (19%)than in those placed using the drill andamalgam (36%). Similarly, in Indonesianchildren, discomfort as assessed using bothphysiological and behavioral methods, wasless with the ART approach than with conven-tional procedures. In Chinese pre-school chil-dren, discomfort was experienced by only 7percent of those receiving an ART restora-tion.
Post-operative sensitivityIn Zimbabwean teenagers, patients were
asked about post-operative sensitivity two tofour weeks after restoration placement. Post-operative sensitivity had been experienced in6 percent of the ART restorations placed, butby the time of the evaluation sensitivity haddisappeared from all but one restoration.Similar results were reported in Chinese ado-lescents, with only 5 percent reported havingsome post-operative sensitivity.
Acceptance by patients95 percent and 91 percent of secondary
school students in Zimbabwe and China,respectively, expressed satisfaction with theART procedure and with the resulting restora-tion(s). The same percentages of studentsreported that they would not hesitate toundergo the same treatment again if neededand would recommend it to their best friend.
ART in the health sector
In many countries there is already some pro-vision for dental care in schools. This is oftendelivered through the use of mini-clinics ormobile dental units where traditional dentalcare is provided. The advantage of the use ofART in a mobile setting has been shown inSouth Africa. For years a well-equippedmobile dental unit with three dental chairswas in operation in rural primary schools.However, it was reported that staff membershad difficulties in treating these childrenbecause many of them were afraid of thedental treatment delivered through this sys-tem. It was decided to introduce ART into thecare delivery system. A yearafter the introduction ofART, the percentage ofextractions was reducedby 17 percent for per-manent teeth and by36 percent for primaryposterior teeth com-pared to the year prior toART. In addition, the per-centage of amalgam restorationswas reduced by 16 percent in permanentteeth and 1 percent in primary teeth.Conversely, restorative care increased by 33percent in permanent teeth and 37 percentin primary posterior teeth. This positivechange was ascribed to the patient-friendlynature of ART. It had reduced fear, mainlybecause of the absence of injections, andconsequently had increased children’sacceptance of restorative care. Anotheradvantage was the simplified cross-infectioncontrol, particularly in an area with a highincidence of people with HIV and hepatitis.

37
Cost of ART restoration and ART sealant
The implementation phase of a cost-effec-tiveness study, comparing ART restorationsusing glass ionomer with amalgam restora-tions, started in Ecuador, Panama andUruguay in May 2002. It will take more thanthree years before the results are published.Less complete data come from the ART studyin Zimbabwe. When the cost of all consum-able materials such as filling material, gauze,cotton wool, mouth masks, gloves etc. wastaken into account, it was estimated that anART restoration or ART sealant cost US$ 0.47in 1993 and US$ 0.51 in 1996, excluding per-sonnel salaries. These estimates are muchlower than recently published estimates fortraditional amalgam restorations in non-EMEcountries. A BPOC demonstration project willinclude costing of the package.
Conclusion
• A large proportion of dentine lesions can be treated using the ART approach.• The placement of restorations using the ART approach seems to cause less discomfort than conventionally placed amalgams.• The survival rate of single-surface ART restorations using glass ionomers in the permanent dentition is higher in more recent studies compared to earlier studies. • The average annual failure rate for ART restorations using glass ionomers in single-surfaces in the permanent dentition is about 4-5 percent for the first three years.• The short-term survival of single-surface ART restorations using glass ionomers in the permanent dentition is comparable to amalgam restorations using conventional methods.• The caries-preventive effect of ART relatedglass ionomer sealants is 96 to 98 percent after three years.• The three-year survival of 71-72 percent for partially and fully retained glass ionomer sealants is extremely encouraging considering they were placed under field conditions. • To ensure optimal results from the ART approach, educational courses for operators new to the techniques need to be organized prior to applying the approach in the field and clinic.


39
Chapter 5
The training and job description of oral
health personnel will differ from coun-
try to country and are regulated by the
country’s legislative system. This chap-
ter provides information about the var-
ious types of oral health personnel
suitable to provide OUT and ART servic-
es at the lower level of the PHC pyra-
mid. Affordable fluoride toothpaste is
considered an element of health pro-
motion and no attempt is made to dis-
cuss the types of personnel required to
be involved in this promotion.
Furthermore, an attempt is made to
list the basic requirements in terms of
equipment and instruments to perform
OUT and ART.
Personnel and equipment for OUT and ART 5

40
Personnel requirements for OUT
The precise type of personnel required forOUT services largely depends on local condi-tions, national health personnel infrastruc-ture, and health strategies. The differencesin types of health care personnel for OUT areshown in the three examples presented here.In Cambodia, primary health care nursesimplement the Basic Package of Oral Care(BPOC). These nurses undergo a five-monthdental training program. They are consideredproficient in the skills required to render allservices included in the BPOC. The require-
ments for enrolling in the dentalupgrading course include the fol-
lowing: one year of basichealth training; at least one
year employed as a pri-mary health care nurse ata district referral orhealth center; and asigned agreement toreturn to the district
referral or health centerafter the dental training has
been completed. Tanzania is the next exam-
ple. There, rural medical aids provide painrelief through tooth extraction supported bydrug therapy at rural health centers or dis-pensaries. The basic training for rural med-ical aids lasts three years. The dental upgrad-ing training is accomplished through a shortin-service training course. The rural medicalaid is then considered proficient in the skillsrequired to render OUT services. Both patientsatisfaction with the pain relief service andjob satisfaction among rural medical aidswere reported to be high.
In Nepal, health assistants with extendedduties that include oral health education,tooth extraction and first aid for maxillo-facial trauma, have been trained in a coupleof months. In other countries, such as Kenya,Malawi, Vietnam and Zimbabwe, OUT servicesmay be provided by dentally trained person-nel such as dental therapists.
The precise type of per-sonnel required for OUTand ART services largelydepends on local condi-tions, national health
personnel infrastructure,and health strategies.

41
Personnel requirements for ART
Different types of dental personnel have par-ticipated in ART studies. They vary from finalyear dental therapy students to dentists.Data analyses have shown the following find-ings.• There was a statistically significant differ-ence in survival of ART restorations betweendentists (Pakistan, Syria) and between seniordentists and junior dental therapists, withthe former performing better (Zimbabwe),but not between senior dentists and seniordental therapists (Thailand).• The survival of ART restorations placed bydental therapists (China and Tanzania) wascomparable to those placed by dentists(Pakistan and Syria).• The survival of ART restorations placed byfinal year dental therapy students was belowaverage (Cambodia).
Restoring decayed teeth through ARTrequires knowledge and skills about themaintenance and functioning of the dentitionin total. Therefore, short training courses, ashave been conducted for OUT personnel inNepal and Tanzania, are inappropriate. Itseems that the dental therapist is a suitabletype of dental personnel to carry out the ARTapproach. However, local circumstances maylead to specific training courses on ART thatexclude elements that make up the dentaltherapy training. Such a training coursewould then be shorter than the usual threeyears needed for the dental therapy training.It is up to each government to decide what isbest under the prevailing circumstances.
Conclusion
While auxiliary medical and dental personnelwill provide most of the OUT service at thelower level of the PHC pyramid, dentists playan important role in the overall structure.Dentists interested in community dentistrymay be useful as teachers and instructors inthe competency-based training of providingOUT and ART personnel. Furthermore, den-tists in government service, preferably withsome training in public health, are requiredto supervise and monitor the oral healthservices in regions or districts. These govern-ment dental officers are also responsible forthe training and upgrading/refresher coursesfor dental and medical auxiliaries.
Equipment, instruments and materialsrequired for OUT
The equipment may include the following:• A chair or bed/couch with head support• A stool for the dental health worker and assistant• A table for instruments and medicines• A light source, which ideally does not rely totally on electricity supply• A wash basin• A system of water storage if running wateris not available• A pressure cooker and heat source for sterilizing the instruments.
A basic set of dental instruments and materi-als should be compiled. This should be con-sidered the minimum required for the provi-sion of OUT services. There are numeroustypes of extraction forceps and they areexpensive. Decisions must be made regardingthe number and type of forceps required. Alimited set of two to four different types offorceps and one or two dental elevators willsuffice for the extraction of all types ofteeth. The expected number of patients perday and the time needed for sterilizing theinstruments determine the number of sets ofinstruments required. This will differ fromcountry to country and from community tocommunity.

42
Equipment, instruments and materialsrequired for ART
The equipment and material requirements forART have been reduced to a minimum. Thislowers initial set up and maintenance costsand allows treatment to be provided in virtu-ally any environment. All that is required areappropriate supports for the patient andoperator, dental hand instruments, an adhe-sive restorative material, relevant consum-able materials and a source of lighting. The hand instruments used in the ARTapproach have been carefully selected andare based on the steps involved in placing anART restoration. Only those instruments thatare essential are included. Almost all theinstruments used are those commonly foundin dental clinics and are readily availablefrom dental instrument suppliers (fig. 5.1).The instruments used are mouth mirror,explorer or probe, tweezers, excavators, den-tal hatchet and an applier/carver. A newinstrument for opening tooth cavities hasbeen developed recently (fig 5.2).
The consumable materials required includecotton wool rolls, cotton wool pellets, petro-leum jelly, tumbler/cup, wooden wedges,matrix band and plastic strip. Until now glassionomers have been used as the restorativematerial. However, if ART is to be undertakenin a well-equipped dental clinic, either in adistrict or provincial hospital or privately,then resin-based composite materials mightbe considered.
Conclusion
The type of dental personnel needed to per-form OUT requires a shorter training periodthan those performing ART. The nationalhealth and legal structures will have to befollowed when intro-ducing the BPOC. The equipment, materialsand instruments required to do OUT and ARTare not electricity-dependent, much cheaperto purchase and to maintain than thatrequired for traditional western dental treat-ment and, therefore, permit the BPOC to beundertaken almost anywhere.
All that is required areappropriate supports forthe patient and operator,dental hand instruments,an adhesive restorativematerial, relevant con-
sumable materials and asource of lighting.

43
Figure 5.1 A set of instruments
and materials required for pro-
ducing an ART restoration.
(Reprinted with permission
from Drs. J.E. Frencken and C.J.
Holmgren)
Figure 5.2 The new ART instru-
ment for opening tooth cavi-
ties. It is placed in the
entrance of a cavity. The soft
carious tooth material and
biofilm are seen alongside the
instrument. (Reprinted with
permission from Dr. D. Taifour)

Recommendations for establishing and

45
Chapter 6
The need for and effectiveness of each
of the individual components that con-
stitute the Basic Package of Oral Care
(BPOC) have been discussed in pre-
vious chapters. The next step is to
demonstrate the effectiveness,
efficiency, acceptability and sustain-
ability of the BPOC as a means of
improving oral health within the coun-
try or community for which it is
intended.
evaluating BPOC demonstration programs 6

46
Introduction
Implementation of the BPOC depends on pre-vailing local factors, including availablehuman and financial resources and existinginfrastructures, local perceived needs, andtreatment demands of the community andthat of its leaders. The conditions in eachcountry or community will not only influencethe content of BPOC and the method bywhich it is applied, but also its success. Inorder to investigate this, demonstration proj-ects on BPOC are recommended in differentcountries.
The guidelines presented below assumecollaboration among local partners, localgovernment, industry and organizations(including NGOs) providing oral healthexperts. It aims at highlighting aspects ofpreparation, planning, implementation andevaluation of demonstration projects. A sum-mary of the essential steps to be taken in ademonstration project is given in Table 6.1.
The conditions in eachcountry or community willnot only influence the con-
tent of BPOC and themethod by which it isapplied, but also its
success. In order to investi-gate this, demonstrationprojects on BPOC are rec-ommended in different
countries.

47
Factors to consider before starting the program
Identifying a local partner The local partner should be willing to acceptjoint responsibility for the planning and imple-mentation of the program with the ultimateobjective of taking on the ownership of theongoing activities in a later phase. The settingup of a working group to initiate the programand to oversee its implementation is desirable.
Obtaining approval from decision makersApproval for the program implies consulta-tion with the authorities as early as possible.It is essential to obtain their consent for theplanning of the demonstration program andfor its implementation. In this context it isessential to have briefing at ministry level,since the Ministry of Health is a fundamentalplayer in developing (oral) health services.
Probing the interest of possible parties involved
Local political, religious and community lead-ers, as well as the heads of medical and edu-cational systems and other possible serviceproviders, e.g. traditional healers, should beconsulted to probe their views and interest inthe BPOC program. If their interest is low andtheir willingness to support the program isnil, then it might be necessary to abandonthe idea of starting a program for that par-ticular community.
Understanding the local situationThe success of any oral health program,including oral health services research proj-ects, depends on how well it meets the wish-es and expectations of the community. If theprogram fails to meet these, then there islikely to be a problem with both acceptanceand sustainability. In designing the program,many factors should be taken into considera-tion, including epidemiological data on thecommunity‘s oral health status and norma-tive needs, the people’s perceived needs(wishes) and treatment demands, theirknowledge and habits related to oral health,existing health and educational structures,and available human and financial resources.
The process of planning
Formulating measurable objectivesThe collected information on the local pre-vailing conditions provides a basis for devel-oping the program proposal. The next step isthe formulation of appropriate objectives forthe program that are consistent with thewishes and expectations of the communityand its leaders. The objectives must bedefined in such a way that allows for mean-ingful evaluation. Objectives that cannot beachieved or cannot be properly evaluated willfrustrate both the providers and consumers,which could hinder continuation of the pro-gram.
Consultation among all parties involvedWhen the program proposal has been formu-lated it should be presented to all partiesinvolved. This consultation is important todetermine whether the objectives and thechosen strategy meet their wishes and expec-tations. It is probable that in the light ofconsultation, minor modifications will berequired. It is essential that all partiesinvolved agree on the final draft of the pro-gram proposal. When the proposal has beenaccepted by those responsible, a protocolshould be devised, which highlights thedetails of all parts of the program, the indi-viduals responsible for each activity and thetime frame.

48
Implementation, process monitoring andevaluation
Monitoring activities, maintaining communication, tackling problems
Continuous monitoring of all activities isrequired during implementation. Maintainingcommunication with all parties involved is aprerequisite to identifying small problems,which if not resolved can seriously threatenthe success of the program. Unforeseen moreserious problems may emerge that requiremodifications of the original proposal or mayforce the discontinuation of the program.Moreover, the monitoring process reduces therisk of drawing faulty conclusions from theresults of the outcome evaluation. Forinstance, the conclusion that the programwas ineffective when in reality the programwas not carried out as designed.
Assessing the outcomesThe rationale for setting up a demonstrationprogram (community trial) is to determinethe feasibility, effectiveness, efficiency,social acceptability and sustainability of theBPOC under local conditions. This impliesthat the results of the outcome evaluationmust be determined to assess whether theobjectives have been met. Depending on theformulated objectives, achievements can beevaluated by assessing the concomitant out-come effects, for example:• A reduction in the number of people withtoothache • Utilization patterns of offered services,such as an increase in people seeking regularcheck-ups and in those coming to havedecayed teeth filled. The utilization patternof toothpaste and tooth-cleaning devicesshould also be determined• Oral health status, e.g., number of teethdecayed, filled or sealed• Consumer’s satisfaction with treatmentreceived• Job satisfaction of providers• Generated resources • Sales figures of toothpaste or price fluctu-ation of toothpaste by year.
The length of the demonstration programdepends on the type of outcome effect to beassessed. Studies with the objective of con-trolling or reducing the level of dental cariesmight need to run for two to four yearsbefore results can be assessed. Ideally,process evaluation should have revealedwhether the program is likely to be sustain-able before a final assessment has been car-ried out.
Reporting the findingsThe results of the evaluation process, includ-ing conclusions and recommendations, mustbe reported to all parties at regular intervalsfor subsequent discussion. The final outcomeof the program should also be reported to allparties. In addition, outcomes, whether suc-cessful or unsuccessful, should be reported inthe scientific literature. This will guide othercountries or communities that might considercommencing a BPOC program.

Before starting•Identify local partner
•Obtain approval from decision-makers•Consider the interests of all parties
•Understand the local situation
The process of planning•Write project protocol
•Formulate measurable objectives •Design evaluation
•Consult all parties involved
Implementation, process monitoring and evaluation
•Monitor activities, maintain communication and tackle problems
•Assess the outcomes•Report the findings
Future options after evaluation•Abandon the program•Modify the program
•Continue and expand
49
Future options after evaluating a BPOC program
Abandon the programThe option of abandoning the programshould be considered if it is found to be inef-fective, unacceptable or unaffordable.Without adequate support from the commu-nity or government, an oral health servicesprogram cannot become sustainable. There isno reason to continue the program withexternal funding if all signs indicate that nei-ther the government nor the community iswilling to support the program with localresources.
Modify the program and run another demonstration project
Another option might be to modify the pro-gram in order to solve problems identifiedduring the evaluation. For example, a reori-entation of the program might be required toaddress the wishes of the parties involved,which emerged during the course of imple-mentation. Initiation of a modified programmay be considered in another demonstrationprogram.
Continuation and expansion of the programAgreements on ownership must be made atan early stage of the demonstration program.The responsibilities regarding continuationshould be formalized with the authorities atthe end of the demonstration program. Thedecision to expand the program on a largerscale belongs to the authorities and the com-munity. All efforts related to the implemen-tation of the demonstration program on alarger scale must be based on self-supportingactivities, which implies that no externalfunding should be considered.
Table 1 Flow chart of
activities in an oral health
demonstration study

50
References
Chapter 1Bedi R, Sardo Infirri J. Oral health care in
disadvantaged communities. The root cause: A proposal for action. FDI World Dental Press 1999.
Bedi R. Ethnic indicators of dental health for young Asian schoolchildren resident in areas of multiple deprivation. Brit Dent J 1989; 166: 331-334.
Brindle R, Wilkinson D, Harrison A, Connolly C. Oral health in Hlabisa, Kwazulu/Natal –a rural school and community based survey. Int Dent J 2000; 50: 13-20.
Hobdell MH, Myburgh NG, Kelman M, Hausen H. Setting global goals for oral health for the year 2010. Int Dent J 2000; 50: 245-249.
Kikwilu EN, Hiza JFR. Oral health knowledge and attitude among public health nurse school, Tanzania. Odontostomatol Trop 1994; 17: 20-24.
Lin HC, Wong MCM, Wang ZJ, Lo ECM. Oral health knowledge, attitudes, and practicesof Chinese adults. J Dent Res 2001; 80: 1466-1470.
Mausch W, Sheiham A. Promoting oral health in depressed communities. German Foundation for International Develop-ment. 1995.
Pakhomov GN. Future trends in oral health and disease. Int Dent J 1999; 49: 27-32.
Petersen PE, Hadi R, Al-Zaabi FS, Hussein JM,Behbehani JM, Skougaard MR, Vigild M. Dental knowledge, attitudes and behavior among Kuwaiti mothers and schoolteach-ers. J Pedodontics 1990; 14: 158-164.
Sheiham A, Plamping D. Strategies for improving oral health and reforming oral health care systems. Afr Dent J 1988; 2: 2-7.
Ture TE. Dental survey: patients’ attitudes in Oman. Int Dent J 1993; 43: 585-590.
Todd R, Durward CS. Utilisation of dental services in Cambodia and the role of tradi-tional dentists. Community Dent Health 1994; 11: 34-37.
van Palenstein Helderman WH, Nathoo ZAW. Dental treatment demands among patientsin Tanzania. Community Dent Oral Epidemiol 1990; 18: 85-87.

51
van Palenstein Helderman WH, Begum A, Kalam Joarder MA. Awareness, knowledge and behaviour pertaining to oral health ofa rural population in Sreepur. J Oral Health Bangladesh 1998; 4: 4-7.
Verrips GH, Frencken JE, Kalsbeek H, Kok-Weimar TLF. Oral health and dental beha-viour in 11year-old children of different ethnic groups. Community Dent Health 1992; 10: 41-48.
Warnakulasuriya S. Demand for dental care inSri Lanka. Community Dent Oral Epidemiol 1985; 13: 68-69.
World Health Organization. Primary health care, Alma Ata,1978. in: Health for all series no.1. WHO Geneva.1978.
World Health Organization. DMFT data. Geneva, WHO Global Data Bank 1999.
Chapter 2American Dental Association: Special report
on antibiotics use in dentistry. J Amer Dent Assoc 1997;128: 648.
Çaliskan MK, Türkün M. Clinical investigationsof traumatic injuries of permanent incisorsin Izmir, Turkey. Endod Dent Traumatol 1995; 11: 210-213.
Frencken JE, Sithole WD, Mwaenga R, Htoon HM, Simon E. National oral health survey Zimbabwe 1995: Dental caries situation. Int Dent J 1999; 49: 3-9.
Hargreaves JA, Cleaton-Jones PE, Roberts GJ,Williams S, Matejka JM. Trauma to primaryteeth of South African preschool children. Endod Dent Traumatol 1999; 15: 73-76.
Kahabuka FK, Mwangosi IE. Emergency visits at a paedodontic clinic in Tanzania. Tanz Dent J 1997; 8: 21-23.
Kahabuka FK, Plasschaert A, van ‘t Hof MA. Prevalence of teeth with untreated dental trauma among nursery and primary schoolpupils in Dar es Salaam, Tanzania. Dent Traumatol 2001; 17: 109-113.
Kandemir S, Ergul N. Grievances in cases using antibiotics due to oro-dental problems and assessment of need for anti-biotics. Int Dent J 2000; 50: 73-77.
Majewski RF, Snyder CW, Bernat JE. Dental emergencies presenting to a children’s hospital. J Dent Child 1988; 55: 339-342.
Marcenes W, Al Beiruti N, Taifour D, Issa S.
Epidemiology of traumatic injuries to the permanent incisors of 9-12 year-old schoolchildren in Damascus, Syria. Endod Dent Traumatol 1999; 15: 117-123.
Mautsch W, Sheiham A. Promoting oral healthin deprived communities. German Foundation for International Development. 1995.
Mestrinho HD, Bezerra ACB, Carvalho JC. Traumatic dental injuries in Brazilian pre-school children. Braz Dent J 1998; 9: 101-104.
Mosha HJ, Scheutz F. Perceived need and use of oral health services among adolescents and adults in Tanzania. Community Dent Oral Epidemiol 1993; 21: 129-132.
Ntabaye MK, Scheutz, F, Poulsen S. Patient satisfaction with emergency oral health care in rural Tanzania. Community Dent Oral Epidemiol 1998; 26: 289-285.
Petersen PE, Hadi R, Al-Zaabi FS, Hussein JM,Behbehani JM, Skougaard MR, Vigild M. Dental knowledge, attitudes and behavior among Kuwaiti mothers and school teach-ers. J Pedodontics 1990; 14: 158-164.
Razak IA, Jaafar N. Dental needs, demands and patterns of service utilization in a selected Malaysian urban population. Community Dent Oral Epidemiol 1987; 15: 188-191.
Vincent-Townend JL, Shepherd JP: Appendix. In: Rowe NL, Williams JL (eds): Maxillofacial injuries, pp 1053-1067 Edinburgh, Churchill Livingstone 1994.
The Oral Health Alliance. The Berlin Declaration 1992 on oral health services in deprived communities. In: Promoting oral health in deprived communities. Eds: W. Mautsch, A. Sheiham. German Foundation for International Development, Berlin, 1995.
Todd R, Durward CS. Utilisation of dental services in Cambodia and the role of tradi-tional dentists. Community Dent Health 1994; 11: 34-37.
Ture TE. Dental survey: patient attitudes in Oman. Int Dent J 1993; 43: 585-590.
Vanderas AP, Papagiannoulis L. Incidence of dento-facial injuries in children: a 2-year longitudinal study. Endod Dent Traumatol 1999; 15: 235-238.

52
van Palenstein Helderman WH, Nathoo ZAW. Dental treatment demands among patientsin Tanzania. Community Dent Oral Epidemiol 1990; 18: 85-87.
Warnakulasuriya S. Demand for dental care inSri Lanka. Community Dent Oral Epidemiol 1985; 13: 68-69.
World Health Organization. Primary health care, Alma Ata 1978. in: Health for all series no.1. WHO Geneva. 1978.
World Health Organization. DMFT data. WHO Global Data Bank. Geneva, 2000.
Zeng Y, Sheller B, Milgrom P. Epidemiology ofdental emergency visits to an urban chil-dren’s hospital. Pediat Dent 1994; 16: 419-423.
Chapter 3Adyatmaka A, Sutopo U, Carlsson P, Bratthall
D, Pakhomov GN. School-based primary preventive programme for children: afford-able toothpaste as a component in pri-mary oral health care: experiences from a field trial in Kalimantan Barat. WHO Geneva.1998.
Ashley PF, Attrill DC, Ellwood RP, WorthingtonHV, Davies RM. Toothbrushing habits and caries experience. Caries Res 1999; 33: 401-402.
Bratthall D, Hänsel Petersson G, Sundberg H.Reason for the caries decline: what do theexperts believe? Eur J Oral Sci 1996; 104: 416-422.
Burt BA. Trends in caries prevalence in North American children. Int Dent J 1994; 44: 403-413.
Chesters RK, Huntington E, Burchell CK, Stephen KW. Effect of oral care habits on caries in adolescents. Caries Res 1992; 26:299-304.
Chestnutt IG, Schafer F, Jacobson APM, Stephen KW. The influence of toothbrush-ing frequency and post-brushing rinsing on caries experience in a caries clinical trial. Community Dent Oral Epidemiol 1998; 26: 406-411.
Clarkson JJ, Hardwick K, Barmes D, Richardson LM. International collaborativeresearch on fluoride. J Dent Res 2000; 79:893-904.
Davies RM, Holloway PJ, Ellwood RP. The role
of fluoride dentifrices in a national strate-gy for the oral health of children. British Dent J 1995; 172: 84-87.
Duckworth RM, Knoop DTM, Stephen KW. Effect of mouthrinsing after toothbrushingwith a fluoride dentifrice on human salivary fluoride levels. Caries Res 1991; 25: 287-291.
Hugoson A, Norderyd O, Thorstensson H. Distribution of periodontal disease in Swedish adult population 1973, 1983 and 1993. J Clin Periodontol 1998; 25: 542-548.
Ismail AI, Tanzer JM, Dingle JL. Current trends of sugar consumption in developingsocieties. Community Dent Oral Epidemiol 1997; 25: 438-443.
Kalsbeek H, Truin GJ, Poorterman JHG, van Rossum GMJM, van Rijkom HM, Verrips GHW. Trends in periodontal status and oralhygiene habits in Dutch adults between 1983 and 1995. Community Dent Oral Epidemiol 2000; 28: 112-118.
Leous P, Pakhomov G, Ramanathan J. Community based primary preventive pro-gramme for young adults. WHO Geneva. 1995.
Marthaler TM, O’Mullane D, Vrbic V. The prevalence of dental caries in Europe 1990-95. Caries Res 1996; 30: 237-255.
Pakhomov GN. Future trends in oral health and disease. Int Dent J 1999; 49: 27-32.
Rojas-Sanchez F, Kelly SA, Drake KM, Eckert GJ, Stookey GK, Dunipace AJ. Fluoride intake from foods, beverages and denti-frice by young children in communities with negligibly and optimally fluoridated water: a pilot study. Community Dent Oral Epidemiology 1999; 27: 288-97.
Pine CM, McGoldrick PM, Burnside G, Cursow MM, Chesters RK, Nicholson J, Huntington E. An intervention programme to establishregular toothbrushing: understanding pa-rents’ beliefs and motivating children. Int Dent J 2000; 50: 312-323.
Schwarz E, Lo ECM, Wong MCM. Prevention ofearly childhood caries – results of a fluo-ride toothpaste demonstration trial on Chinese preschool children after three years. J Public Health Dent 1998; 58: 12-18.

53
Sjogren K, Birkhed D, Rangmar B. Effect of a modified toothpaste technique on ap-proximal caries in preschool children. Caries Res 1995; 29: 435-441.
van Loveren C, Duggal MS. The role of diet in caries prevention. Int Dent J 2001; 51: 399-406.
van Loveren C, Moorer WR, Buis MJ, van Palenstein Helderman WH. Total and free fluoride in toothpaste from non-EME countries. WHOCC Nijmegen, The Netherlands. 2002.
World Health Organization. Technical Report Series No.726. Recent advances in oral health. WHO Geneva. 1992.
World Health Organization. Technical Report Series No.846. Fluorides and oral health. WHO Geneva. 1994.
World Health Organization. DMFT data. WHO Global Data Bank. Geneva. 2000.
Chapter 4Banerjee A, Kidd EAM, Watson TF. In vitro
evaluation of five alternative methods of carious dentine excavation. Caries Res 2000; 34: 144-150.
Downer MC, Azli NA, Bedi R, Moles DR, Setchell DJ. How long do routine dental restorations last? A systematic review. BritDent J 1999; 187: 432-439.
Frencken JE, Makoni F, Sithole WD. Atraumatic Restorative Treatment and glass ionomer sealants in a school oral health programme in Zimbabwe: Evaluation after 1 year. Caries Res 1996; 30: 428-433.
Frencken JE, Makoni F, Sithole WD.Oral health services and promotion at secon-dary schools in Greater Harare area. Harare: Ministry of Health, Government of Zimbabwe, 1997.
Frencken JE, Makoni F, Sithole WD, HackenitzE. Three year survival of one-surface ART restorations and glass-ionomer sealants ina school oral health programme in Zimbabwe. Caries Res 1998; 32: 119-126.
Frencken JE, Makoni F, Sithole WD. ART restorations and glass-ionomer sealants inZimbabwe: survival after 3 years. Community Dent Oral Epidemiol 1998; 26: 372-381.
Frencken JE, Holmgren CJ. Atraumatic Restorative Treatment for dental caries. Nijmegen. STIbook. 1999.
Ho TFT, Smales RJ, Fang DTS. A 2-year clinicalstudy of two glass ionomer cements used in the atraumatic restorative treatment (ART) technique. Community Dent Oral Epidemiol 1999; 27: 195-201.
Holmgren CJ, Lo ECM, Hu DY, Wan HC. ART restorations and sealants placed in Chinese school children – results after three years. Community Dent Oral Epidemiol 2000; 28: 314-320.
Lo ECM, Holmgren CJ. Provision of AtraumaticRestorative Treatment (ART) restorations in Chinese pre-school children – a 30-month evaluation. Int J Paed Dent. 2001; 11: 3-10.
Lo ECM, Luo Y, Fan MW, Wei SHY. Clinical investigation of two glass-ionomer restoratives used with the ART approach inChina: Two-year results. Caries Res 2001; 35: 458-463.
Luo Y, Wei SHY, Lo ECM. Clinical investigationof a high-strength glass ionomer restora-tive used with the ART technique in Wuhan, China: one-year results. Chinese J Dent Res 1999; 2: 73-78.
Makoni F, Frencken JE, Sithole WD. Oral health status among secondary school students in Harare, Zimbabwe. J South AfrDent Ass 1997; 52: 491-94.
Mandari GJ, Truin GJ, van ‘t Hof MA, FrenckenJE. Effectiveness of three minimal inter-vention approaches for managing dental caries: Survival of restorations after 2 years. Caries Res 2001; 35: 90-94.
Mickenautsch S, Rudolph MJ, Ogunbodede EO, Frencken JE. The impact of the ART approach on the dental treatment profile in a mobile dental system (MDS) in South Africa. Int Dent J 1999; 49: 132-138.
Nadanovsky P, Cohen Carneiro F, Souza de Mello F. Removal of caries using only handinstruments: A comparison of mechanical and chemomechanical methods. Caries Res2001; 35: 384-389.
Phantumvanit P, Songpaisan Y, Pilot T, Frencken JE. Atraumatic Restorative Treatment (ART): A three-year community field trial in Thailand - survival of one-sur-

54
face restorations in the permanent denti-tion. J Publ Health Dent 1996; 56: 141-145.
Rahimtoola, S, van Amerongen WE. Comparison of two toothsaving prepara-tion techniques for onesurface cavities. J Dent Child 2002; in print.
Schriks MCM, van Amerongen WE, Bezemer PD. Atraumatic perspectives of ART. Psychological and physiological aspects of treatment with and without rotating instruments. Community Dent Oral Epidemiol 2001; submitted.
Smith AJE, Chimimba PD, Kalf-Scholte S, Bouma J. Clinical pilot study on new den-tal filling materials and preparation proce-dures in developing countries. Community Dent Oral Epidemiol 1990; 18: 309-312.
Taifour D, Frencken JE, Beiruti N, van ‘t Hof MA, Truin GJ. Prevalence of caries and prevalence of dentinal lesions treatable through the ART approach in caries high-risk school children in Damascus, Syria. Medical Principles and Practice 2002; sub-mitted.
Taifour D, Frencken JE, Beiruti N, van ‘t Hof MA, Truin GJ. Effectiveness of glass ionomer (ART) and amalgam restorations in the deciduous dentition – results after 3 years. Caries Res 2002; accepted.
Taifour D, Frencken JE, Beiruti N, van ‘t Hof MA, Truin GJ, van Palenstein Helderman WH. Comparison between restorations in thepermanent dentition produced by hand and rotary instrumentation - survival after3 years. Community Dent Oral Epidemiol 2002; in print.
Yee R, Sheiham A. The burden of restorative dental treatment for children in Third World countries. Int Dent J 2002; 52:1-9.
Chapter 5Frencken JE, Makoni F, Sithole WD, Hackenitz
E. Three year survival of one- surface ART restorations and glass-ionomer sealants ina school oral health programme in Zimbabwe. Caries Res 1998; 32: 119-126.
Frencken JE, Makoni F, Sithole WD. ART restorations and glass-ionomer sealants in Zimbabwe: survival after 3 years. Community Dent Oral Epidemiol 1998; 26:
372-381.Holmgren CJ, Lo ECM, Hu DY, Wan HC. ART
restorations and sealants placed in Chinese school children – results after three years. Community Dent Oral Epidemiol 2000; 28: 314-320.
Mallow PK, Klaipo M, Durward CS. Dental nurse training in Cambodia – a new approach. Int Dent J 1997; 47: 148-156.
Mallow PK, Durward CS, Klaipo M. Restorationof permanent teeth in young rural chil-dren in Cambodia using atraumatic restorative treatment (ART) technique andFuji II glass ionomercement. Int J Paediat Dent 1998; 8: 35-40.
Mandari GJ, Truin GJ, van ‘t Hof MA, FrenckenJE. Effectiveness of three minimal inter-vention approaches for managing dental caries: Survival of restorations after 2 years. Caries Res 2001; 35: 90-94.
Ministry of Health. Oral health project. Trainer’s handbook. Kathmandu, Nepal 1996.
Ntabaye MK, Scheutz F, Poulsen S. Job satis-faction amongst rural medical aids provi-ding emergency oral health care in rural Tanzania. Community Dent Health 1999; 16: 40-44.
Phantumvanit P, Songpaisan Y, Pilot T, Frencken JE. Atraumatic Restorative Treatment (ART): A three-year community field trial in Thailand - Survival of one-surface restorations in the permanent dentition. J Publ Health Dent 1996; 56: 141-145.
Rahimtoola, S, van Amerongen WE. Comparison of two tooth saving prepara-tion techniques for one surface cavities. J Dent Child 2002; in print.
Taifour D, Frencken JE, Beiruti N, van ‘t Hof MA, Truin GJ. Effectiveness of glass-ionomer (ART) and amalgam restorations in the deciduous dentition - results after 3years. Caries Res 2002; accepted.
Taifour D, Frencken JE, Beiruti N, van ‘t Hof MA, Truin GJ, van Palenstein Helderman WH. Comparison between restorations in thepermanent dentition produced by hand and rotary instrumentation - survival after3 years. Community Dent Oral Epidemiol 2002; in print.

55
van Palenstein Helderman W, Mikx F, Begum A, Adyatmaka A, Bajracharya M, Kikwilu E,Rugarabamu P. Integrating oral health into primary health care - experiences in Bangladesh, Indonesia, Nepal and Tanzania. Int Dent J 1999; 49: 240-248.
van Palenstein Helderman WH, Mikx F, Truin GJ, Hung HT, Luc PH. Workforce require-ments for a primary oral health care sys-tem. Int Dent J 2000; 50: 371-377.

56