Embed Size (px)
Citation preview

2012/03/28
1
15/03/2012
CDC TB workshop, East London
Basic microbiology of TB & “traditional” diagnosis of TB
Dr Natalie Bey lisNHLS My cobacterial Ref erral Laboratory Johannesburg011 489 9182 / 9262natalie.bey [email protected]
MYCOBACTERIA
Mycobacterium tuberculosiscomplex
Mycobacterium otherthan M.tuberculosis
complex: NTM / MOTT
Mycobacterium leprae
M.tuberculosis
M.bov is
M.bovis BCG
5 others
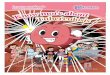
exposed not infected
infected
Immune response
Active diseaseContain disease
Latent infxn
10%90%
2-23% lifetime risk10% / y with HIV infection
Cell wall richin fatty acids (mycolic acids)
Contents of cell includinggenes (DNA)
• Slow growing bacteria• Special stains needed for visualization of bacteria in specimens• Require special conditions for optimal growth• Damaged by heat – refrigerate specimens if delays expected
WHO IS MYCOBACTERIUM TUBERCULOSIS ?
Latent tuberculosisActive tuberculosis
The TB diagnostic pipeline

2012/03/28
2
Primary stain binds to mycolic acids
virulence
factor
Prevents osmotic lys is
60% of cell wall
Virulence factor:
prevents attack in phagocytic vacuoles
1. Young HIV infected women has been losing weight, is lethargic and coughs
occasionally.What would you do?
a) This patient probably does not have TB
b) This patient may have TB. I will send another sputum sample for mycobacterial culture
c) This patient may have TB. I will send another sputum sample for microscopy for acid-fast bacilli (AFB)
Sputum microscopy
• Detects most infectious cases
• Used for monitoring
• Cheap, available
• LIMITATION– Low sensitivity : 25-65%
– Lower in HIV+, children, paucibacillary disease, extrapulmonary disease
• Auramine (fluorescent) 10% more sensitive than ZN
The delayed TB diagnosis
Sl ide courtesy of FIND: Foundation for Innovative New Diagnostics
Reminder: sensitivity & specificity
Sensitivity = true pos / (true pos + false neg)
Specificity = true neg / (true neg + false pos)

2012/03/28
3
MICROSCOPY CULTURESENSITIVITY 25-65%
(5000 – 10 000 bacilli / ml)
ie many f alse negativ es
80-85%(10 bacilli / ml)
ie f ew f alse negativ es
Diagnosis of Tuberculosis Factors that contribute to improved sensitivity of both microscopy and
culture?
• Adequate specimen collection
• No. of specimens
• Optimal specimen transport
• Optimal specimen processing
• Certain clinical scenarios are less likely to yield positive smear and culture results
SPECIMEN COLLECTION
• Clean, sterile containers • Request forms completed• Safe packaging materials to
minimize risk of leakage / contamination
• Transport rapidly to laboratory – Infrastructure of nationwide
transport networks• Refrigerate if cannot be
processed immediately – Prevents overgrowth by
other bacteria• Collect before chemotherapy
started
2. A young HIV infected women who has been losing weight, is lethargic and coughs
occasionally.
What would you do?
a) Treat the patient for tuberculosis
b) Send another sputum for microscopy for AFBs
c) Send another sputum for mycobacterial culture
“A case of pulmonary TB is considered to be smear-positive if one or more sputum smear specimens at the start of treatment are positive for AFB (provided that there is a functional EQA system with blind rechecking1).
The definition of a new sputum smear-positive pulmonary TB case is based on the presence of at least one acid fast bacillus (AFB+) in at least one sputum sample in countries with a well functioning EQA system. (See www.who.int/tb /dots/laboratory/policy/en/index1.html.)”

2012/03/28
4
3. What would you do?
a. Phone the laboratory in frustration
b. Remain calm knowing that a certain amount of contaminated cultures is expected from the laboratory
c. Phone the laboratory and ask them to identify the contaminant as this is likely the cause of the lower respiratory tract infection and will assist with treatment choice
Culture of M.tuberculosis Fluorescence
indicates utilization of O2 by bacilli
320 specimens per drawer
Culture of mycobacteria
• Advantages: – Much more sensitive than microscopy
• 80 - 85% • LOW limit of detection: able to detect as few as
10 bacteria /ml– Allows
• Precise species identification• Drug susceptibility testing (DST) • Genotyping - identify epidemiological links
between patients
• Only definitive diagnosis and considered the “Gold Standard” microbiological test for TB

2012/03/28
5
4. What do you do now?
a.Start TB treatment
b.Do not start TB treatment; wait for final identification
c.Assess clinically & Rx for TB if indicated
d. Withhold TB treatment pending identification of AFB even if patient is ill
e. Assess clinically; if patient is stable & asymptomatic withhold Rx until identification is available
5. If you chose option a for Q4, what do you do now?
a.Stop TB treatment as this patient does not have TB
b. Continue TB treatment & send another specimen
c. Stop TB Rx & send another specimen
d. Assess clinically, send another specimen & start empiric TB Rx if indicated
e. Request a GeneXpert on another specimen
6. What does this result mean?
a. Laboratory reporting error
b.The lab failed to detect M.tb
c.The AFBs in this culture are non tuberculous mycobacteria (NTM)
d.This represents contamination of the specimen
e.The patient does not have TB