Embed Size (px)
Citation preview

Basic Epidemiology for Community Health
Assessment
Nelson Adekoya, DrPHCenters for Disease Control and Prevention

Outline
DefinitionsFundamentals of EpidemiologyData Death Certificate
Determine the Leading Causes of DeathData Presentation Tips
Questions & Self Quiz
2

Define Health Define Public Health Define Epidemiology What are the goals of Public Health?
3

Public health is the science of preventing diseases, prolonging life, and promoting health thru organized community effort
4

5
Goals of Public Health?
Prevent or control disease, disability and injury
Improve quality of life for residents of state or community

Define Epidemiology (write down your definition, check
against definition in Part 2)
6

7
Epidemiology and Data are inseparable. So, why do we need data?
..…write down your answers
Part I

8
Why are Data Needed?
to determine major health problems (needs assessment, program development)
to identify where to focus efforts and resources (asset mapping)
to determine progress in solving health problems (measuring health indicators, outcomes, or Healthy People Objectives)
to conduct research and grant applications

9
Succinctly, data are needed
► to assess the health of a community or population;
► to search for causes of disease, injury and disability;
► to plan programs to meet community needs; and
► to measure progress in prevention and control efforts.

According to the National Center of Vital Health Statistics:
Data is required for “a process that involves the community in identifying problems, setting priorities, developing an action plan, measuring progress, deciding whether the actions are effective, modifying the actions if necessary, and reevaluating the community's problems and priorities”.
10

Types of Data Needed
Depend on:
• What is the program of interest?
• What is the focus of the program?
• What is the purpose of the program?
11

Primary data (data collected directly by the organization).
Secondary data (data collected by someone outside their own program or agency, to measure the outcomes of interest).
12

Locating and Accessing Secondary Data
Online Secondary Data access available by such links from the New Hampshire Health Data Inventory (HDI) at www.nhhealthdata.org
Some web sites provide data tables that can be used to perform calculations or create charts.
Other web sites allow users to obtain raw data files, which can be used to create aggregate tables, generate statistics, and perform calculations.
13

Web Sites for Secondary Data Sources
• CDC WONDER (http://wonder.cdc.gov/) has access to a variety of public health information, including links to environmental and disease-specific data.
• CDC WISQARS™ (http://www.cdc.gov/ncipc/wisqars/default.htm): “WISQARSTM (Web-based Injury Statistics Query and Reporting System) is an interactive database system that provides customized reports of injury-related data.”
• US Census (www.census.gov) makes some of its data about the US population available for download.
14

What is NM website address to access health data?
15

Relevance Accuracy Timeliness Accessibility Interpretability Coherence
Importance of Data Quality
16

The relevance of statistical information reflects the degree to which it meets the real needs of clients.
Relevance
17

The accuracy of statistical information is the degree to which the information correctly describes the phenomena it was designed to measure.
It may also be described in terms of the major sources of error that potentially cause inaccuracy (e.g., coverage, sampling, non-response, response).
Accuracy
18

The timeliness of statistical information refers to the delay between the reference point (or the end of the reference period) to which the information pertains, and the date on which the information becomes available.
Timeliness
19

The accessibility of statistical information refers to the ease with which it can be obtained from the Agency.
Accessibility
20

The interpretability of statistical information reflects the availability of the supplementary information and metadata necessary to interpret and use it appropriately. This information normally includes the methodology of data collection and processing, and indications or measures of the accuracy of the statistical information.
Interpretability
21

The coherence of statistical information reflects the degree to which it can be successfully brought together with other statistical information within a broad analytic framework and over time.
Coherence
22

Other aspects of data quality to consider
• Able to drive decision-making and behavior
• Can the outcome be monitored over time?
23

Fundamentals of Epidemiology
24
Part I1

25
Definition of Epidemiology
The study of the distribution and determinants of health-related states or events in specified populations in a specified time period, and the application of findings to control of health problems.

26
Purpose of Epidemiology
► To provide a basis for developing disease control and prevention measures for groups at risk.

27
Descriptive Epidemiology
Examine the distribution of disease in a population and observe the basic features of its distribution.
Answer questions about what, who, when and where people get ill, injured, or disabled.

28
Analytic Epidemiology
Test a hypothesis about the cause of disease by studying how exposures relate to the disease.
Answer questions about how and why people get ill, injured, or disabled.

29
Uses of Epidemiology
Determine the primary agent or causative factors Determine the characteristics of the agent Define the mode of transmission, and contributing factors Identify geographic patterns Describe the natural course of disease, disability, injury and death Help planning and developing health services and programs Provide administrative and planning data

30
Epidemiologists lookFor……
◈ Person ◈ Time ◈ Place
To answer questions about what, who, when and where, how and why people get ill, injured, or disabled.

31
Person
Age, gender, ethnicity Genetic predisposition Concurrent disease Diet, exercise, smoking Risk taking behavior SES, education, occupation

32
Place
Geographic placeUrban, suburban, ruralClimateGeologyPopulation densityEconomic developmentCultural normMedical practiceNutritional practices

34
Time
Calendar Time Time since an event Physiologic cycles Age (time since birth) Seasonality Temporal trends

35
Topics of Interest in Epidemiology
MortalityHospitalizationDisabilityDisease
InjurySafetyMental HealthQuality of Life

36
Epidemiology
Epidemiology weighs and balances Epidemiology contrasts and compares Epidemiologists use RATES
events/population at risk

37
Counting in Epidemiology
Numerator the number of people to whom something happened (i.e. they got sick, died, etc.)
Denominator the population at risk -- all the people at risk for the event

DATA
38
Part III

39
►Quantitative Data
►Qualitative Data

40
Quantitative Health DATA can focus on:
individuals, or entire populations.

41
Population-based Data versus Individualized Data
►Example of individualized data is a patient’s medical record.
►Each record is devoted exclusively to one person and contains information about his or her unique illnesses, injuries, behaviors, etc.
►The data are used primarily to improve the health of that one individual.

42
Population-based Data versus Individualized Data (cont)
►In public health, our focus is primarily on populations (e.g. communities, cities, counties, states).
►Population-based data tells us about the overall “health” of that population.

43
Major Types of Health Data available for analysis
Health outcome / Health Status Data Risk factor Data Resource Data Demographic Data

44
Quantitative DATA
► Measurable and tangible;
► Provides answer regarding what, who, when, and where of health-related events.

45
Simply, what we are doing in Quantitative DATA are:
► Counting of people, behaviors, conditions, or other discrete events;
► Classifying those events into categories;
► Using math and statistics to answer questions.

46
Quantitative DATA Examples (cont)
►Using numbers of deaths to identify leading causes of death (What);
►Using numbers of smokers and nonsmokers by gender to determine whether men are more likely to smoke than women (Who);
►Keeping track of the number of people with flu can identify the beginning of the flu season (When);

47
Quantitative DATA Example (cont)
►Comparing the proportion of women who began prenatal care after the first trimester in various counties will provide an indication of where access to prenatal services may be a problem.

47
Qualitative DATA
►Qualitative data can be used to explain the why and the how of health-related events.
►Qualitative data involve observing people in selected places and listening to discover how they feel and why they might feel that way.

48
Examples of Qualitative DATA
► A focus group of teenage girls could provide valuable insights concerning why they do or don’t use contraceptives.
► A visit to a local clinic might indicate how people might feel as they enter the waiting area.

What Analysis to Request for Quantitative Data?
Measures of central tendency:
● Mean is the arithmetic average of the values in the data
● Median is the middle value
● Mode is the most commonly occurring value
49

•Any Questions???
50

Death Certificate Data
51
Part IV

Introduction to Death Certificate Data
52
Part IV: Section One

53
Primary Source of Death / Mortality DATA
Death / mortality is one of the primary measures of a population’s health.
Death certificate is the primary source of death or mortality.

54
What data are on a typical death certificate?
Information about the characteristics of the decedent,
Information about the circumstances of death (e.g. time, date, and place), and
Specifics about the causes of death.

55
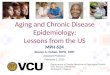
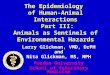
What a typical death certificate
looks like (Figure 1 & 2)

56
Information about the decedent includes:
►Sex (2), Age (5a) ►Birthplace (7) ►Marital Status (10) ►Residence (13 a-f) ►Hispanic Origin (14) and Race (15) ►Occupation (12a) and Education (16).

57
Information about the cause of death includes :
► Date of Death (3)
► Place of Death (9a)
► Immediate Cause and Underlying Cause of Death (27, Part I) and Other Significant Conditions (27, Part II)
► Manner of Death (29) and additional details for deaths due to accidents, suicide, or homicide (30 a-f).

58
At the state vital statistics office, information from death certificates is entered into electronic records.
All of the diseases and conditions reported on the death certificate are translated from text into medical codes using the International Classification of Diseases (ICD)
ICD and Diseases / Conditions

59
What are ICD codes ?
The International Classification of Diseases (ICD), published by the World Health Organization (WHO), establishes a structure for translating the entries on the death certificate into a statistical classification.
From 1979 to 1998, death certificates were codedaccording to ICD-9. Beginning in 1999, death certificates are being coded according to the Tenth Revision (ICD-10) .

60
How to Determine the Leading Causes of
Death by analyzing death data from a death
certificate
Part IV: Section Two

61
Death Data / Mortality DATA
Outline:
► Death certificate (Figure 1 )
► Data collection based on a death certificate
► Discuss limitations of those data

62
USES of Deaths Data / Mortality Data
► Calculate general death rates► Age-specific death rates ► Cause-specific death rates► Sex-specific death rates► Describe the difference between death counts and death rates► Identify leading causes of death

63
USES of Deaths Data / Mortality Data (cont)
► Use rates to examine differences in causes of death by sex
► Analyze trends in rates and changes in underlying causes over time
► Determine effective ways to present data

64
STANDARD MORTALITY MEASURES
What is a count?
the most basic unit of data.
the number of hospital visits, the number of injuries, the number of live-born twins, the number of mothers who deliver twins, the number of deaths, and the number of deaths due to AIDS, etc.
Counts are also useful when comparing numbers for the same population group.

65
What are leading causes of death?
Leading causes of death are diseases identified as being of public health importance based upon the burden of the disease within a population.
The importance of each disease is ranked relative to other important diseases.
A standard procedure for ranking leading causes of death was adopted by the National Center for Health Statistics decades ago in which eligible causes are ranked according to the number of deaths (not rates).

66
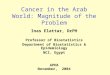
The eligible causes include the 37 rankable causes from the List of 72 Selected Causes of Death (those causes marked by an asterisk on Figure 6), along with HIV infection (added with 1987 data) and Alzheimer’s Disease (added with 1994 data).
Link to ICD-10 is provided below for revised ranking http://www.cdc.gov/nchs/datawh/nchsdefs/codrank.htm
Eligible Causes (ICD-9)

67
Counts are used to identify leading causes of death.
The leading cause of death is the cause with the greatest number of deaths.
Counts can be used to identify the leading causes of death in a single population, their value is limited.
Counts do not help you compare the risk of death in one population with the risk in another population.
Counts and Leading CausesOf Death

68
Rate
A rate is the most common way to measure the occurrence of an event in a population.
The general formula for a rate:
Number of events occurring during a given period x 100000Rate = Population at risk during the same time period

69
Three Consistent Characteristics of a RATE
The counts in the numerator and denominator should cover the same time period.
The persons who experienced the events in the numerator should all be included in the denominator.
The persons in the denominator should be at “risk” for the event in the numerator. In other words, it should be possible for them to experience the event.

Proportion
The number of observations with a given characteristic (a) divided by the total number of observations in a given group (a + b) 26. That is, proportion = a/(a+b).
70

Ratio
Ratio simply relates a figure to another. For example, there are 36 females and 18 males in a restaurant. The ratio of females to males is 36:18 or 36/18=2.
71

Adjusted Rate
An expression of the predicted number of health events within a standard population defined by one or more variables not under study and used to control for effects medicated by such variables.
72

Specific Rate
An expression of the observed number of health events within a defined subgroup or stratum of the population at risk within a predefined time period (e.g., age-specific death rate of 1.2 deaths per 1,000 persons aged 10 to 19).
73

Crude Rate
An expression of the observed number of health events per unit of the population at
risk in a defined time period (e.g., crude mortality rate of 5.7 deaths per 100,000
persons in 1985).
74

75
What is a death rate?
Number of deaths during a given time period Death rate = x 1,000,000
Number of people in the population in which the deaths occurred
A death rate is a measure of the occurrence of death in a defined population during a specified time interval.

76
What are some specific types of death rates?
The death rate discussed above is often called the crude death rate.
It measures the frequency of deaths from all causes in an entire population.

77
What are some specific types of death rates?
Example: Crude Death Rate
The crude death rate for the United States in 1990 would be:
Number of deaths in the U.S. in 1990 x 100,000 U.S. population in 1990

78
Example: Age-specific Death Rate
The death rate for a particular age group.
The death rate for older adults, age 65-80, in NM in 1983 would be:
Number of deaths among 65-80 year olds in NM in 1983 x 100,000 Number of 65-80 year olds in NM, 1983

79
Sex-specific death rate
The death rate for a particular sex, either males or females.
Formula: Number of deaths among males (or females) during a given time period x 100,000 Population of males (or females) during the time period

80
Example: Sex-specific Death Rate
The death rate for females in NM in 1991 would be:
Number of deaths among females in NM in 1991 x 100,000 Number of females in NM, 1991

81
Cause-specific death rate
The death rate from a specific cause for a population.
The sum of all cause specific mortality rates for a population equals the total mortality rate for that population.
Formula: Number of deaths from a specific cause during a given time period
x 100,000 Population during the time period

82
Example: Cause-specific Death Rate
The death rate from homicides in NM, 1990-1994 would be:
Number of deaths from homicide in NM, 1990-1994 x 100,000 Population in NM, 1990-1994

83
Example: Age-sex-cause-specific Death Rate
The death rate from homicides for 65-80 year old females in NM, 1990-1994 would be:
Number of deaths from homicide among 65-80
year old females in NM, 1990-1994 x 100,000 Number of 65-80 year old females in NM, 1990-1994

84
What happens when the numbers are small?
Occasionally, your numerators will be so small that the resulting rates become unstable or unreliable.
One rule of thumb is to have at least 20 deaths in each cause category that you are analyzing. You can accomplish this by combining several years of data.

85
How are rates used to make comparisons?
The real value of death (mortality) rates is that they enable us to compare the risk of death between different causes, different age/sex groups, different time periods, etc.

86
How are rates used to make comparisons?
Quite often, these comparisons are expressed in terms of a rate ratio.
The formula for calculating a rate ratio:
X ÷ Y or X/Y
where: X = death rate in one population Y = death rate in another population

87
Example: Comparing Death Rates
Suppose that in 1993 the overall death rate for males, ages 15-24 years, had been 141.8 per 100,000.
Further suppose that the death rate for males, ages 25-44, that same year had been 258.3 per 100,000.
Then the ratio of the death rate for younger males to the death rate for older males would be:
141.8 ÷ 258.3 = 0.55
This means that the death rate for younger males is half the death rate for older males.

88
What are some common mistakes in calculating rates?
When calculating a rate, always use the same time period in the numerator and denominator.
When the numerator includes deaths for more than one year, the denominator must include the population for the same years.
If the deaths in the numerator are added together for 5 years, the population in the denominator must also be added together for the same 5 years.

89
What are some common mistakes in calculating rates (cont)?
Be sure to use the same population, age group, and/or sex in both the numerator and denominator.
When calculating cause-specific rates, the denominator should include the entire population while the numerator should include only deaths due to one specific cause.
Be sure to indicate what scale was used — usually results are per 1,000 or per 100,000.

90
How are percents helpful?
Use a percent (%) to describe the proportion of deaths due to a specific cause (that is, those deaths assigned a specific ICD code).
The formula for calculating this percent is:
Number of deaths from a specific cause during a given time period x 100 Number of deaths due to all causes during the time period

91
Example: Using Percents
Suppose that in a certain population from 1992 to 1996, the number of deaths from suicide was 525, and the total number of deaths was 2,625.
The percent of deaths due to suicide would be calculated using the formula: 525 ÷ 2,625 = 0.20
This means that 20% of the deaths from 1992 to 1996 were due to suicide.

92
Deciding which results are most important to present;
Choosing the most appropriate format for presenting those results.
How Should These Data Best be Presented?

93
The results you present should answer:
► What are the leading causes of death?
► Do the causes differ by age group? By sex? By race or ethnic group?
► Are there any significant trends over time?
► What can be learned from comparisons with other states or with the United States as a whole?
A Presentation on the Leading Causes of Death

94
What are some tips for presenting quantitative data? (1/2)
Develop clear messages.
Limit your data points to those that are most important.
Display data in colorful, interesting graphics.
Make all of the graphics relate to the message.

95
What are some tips for presenting quantitative data? (2/2)
Avoid too much data on one graph.
Intersperse data with the “human” element to personalize the statistics.
Keep the “so what?” in mind to relate all data to your main points.

96
Are there any special rules for preparing tables? (1/3)
Effective tables have the following characteristics:
as simple as possible.
self-explanatory.
use a clear and concise title.

97
Are there any special rules for preparing tables? (2/3)
Effective tables have the following characteristics:
have clear and concise labels for each row and column, and include the unit of measurement for the data (e.g., years, rate per 100,000).

98
Are there any special rules for preparing tables? (3/3)
Effective tables have the following characteristics:
show totals for rows and columns.
explain any codes, abbreviations, or symbols in a footnote.
note the source of data in a footnote (if not original data).

99
What about charts? (1/2)
Arrange the categories that define the bars in a natural order, such as alphabetically or by increasing age, or in an order that will produce increasing or decreasing bar lengths.
Position the bars either vertically or horizontally as you prefer.
Make all the bars the same width.

100
What about charts? (2/2)
Make the length of bars proportional to the frequency of the event.
Leave a space between adjacent bars, to make the bar chart easier to read.
Code different variables by differences in bar color, shading, cross-hatching, etc., and include a legend that interprets your code

101

102

103

104

105

Summary
106

Framing epidemiologic questions?
Know the elements of question
107

Elements of the question
Who: what are the characteristics of the population you want to know about?
• Age
• Gender
• Race/ethnicity
108

Elements of the question (cont.)
What: About what indicator or outcome are you seeking information?• Behavior• Health/illness - particular ICD-10 codes can be found at:http://www3.who.int/icd/vol1htm2003/fr-icd.htm • ICD-9-CM codes can be found at:
http://www.cdc.gov/nchs/icd9.htm#RTF• Injuries• Chronic diseases
109

Elements of the question (cont.)
Where: What areas are you interested in learning about?
• Geographic area (e.g. HSA, SAU, county)
• Know the town, or group of towns in the
geographic area
• Residents v. occurrences
110

Elements of the question (cont.)
When: What time period are you considering?
• Trends over time
• Is a certain time frame necessary (is the
indicator changing)?
111

Examples of Questions
• What is the rate of cardiovascular disease in New Mexico for the most recent year for
which data is available? Five years ago? Ten years ago? For ages 65+?
• What is the prevalence of diabetes in New Mexico for different age groups?
112

Release of PublicHealth Data
• Confidentiality
• Stability and
• Reliability
113

137
End !