Embed Size (px)
Citation preview
ORIGINAL REPORTS
Basic Aseptic Technique for Medical Students:Identifying Essential Entry-level Competencies
Kristine Leeper, MSE,* M. Scott Stegall, PhD,† and MeriBeth H. Stegall, PhD†
*Department of Surgery, Des Moines University-Osteopathic Medical Center, Des Moines, Iowa, and†Department of Health Sciences–Health Care Administration and Informatics Program, University ofWisconsin–Milwaukee
PURPOSE: Medical students must be competent in basicaseptic technique (BAT) to function effectively in the operatingroom. However, a comprehensive literature review revealed adeficit of research in standardized BAT training for the operat-ing room in medical school curricula.
METHODS: A modified reactive Delphi technique was usedto survey an expert panel of 100 surgical educators. A focusgroup provided initial responses to key questions, and the panelcompleted 2 surveys. In the first survey, the panel identifiedelements for a BAT curriculum for the operating room. In thesecond survey, the panel received feedback from the first surveyand was asked to respond in light of those results.
RESULTS: An 81% response rate was obtained from the firstsurvey. A 74% response rate was obtained from the secondsurvey. Seven of the 18 essential entry-level competencies(EELCs) identified were ranked as the most important. The top5 instructional strategies and the top 3 methods for evaluationwere also selected. The panel identified the third-year curricu-lum as the preferred time of training and a nurse preceptor/educator as the preferred instructor.
CONCLUSIONS: These results provide a minimum set ofeducational objectives that can be used to develop a standard-ized curriculum in BAT for the operating room for medicalstudents. (Curr Surg 59:69–73. © 2002 by the Association ofProgram Directors in Surgery.)
KEY WORDS: Delphi, basic aseptic technique (BAT), steriletechnique, medical students, essential entry-level competencies(EELC)
INTRODUCTION
How prepared are third-year medical students who walk intothe surgical suite? Are they aware of where the sterile field begins
Correspondence: Inquiries to Kristine Leeper, MSE, Department of Surgery, Des MoinesUniversity-Osteopathic Medical Center, 3200 Grand Avenue, Des Moines, IA 50312; fax:(515) 271-1697; e-mail: [email protected].
CURRENT SURGERY • © 2002 by the Association of Program DirectorPublished by Elsevier Science Inc.
and ends? Have they had any formalized training regardingasepsis? To medical educators with a surgical conscience, theseare important questions. However, anecdotal evidence indi-cates that education in the basic principles of aseptic techniquehas not continually evolved in medical schools. Consequently,many new residents and interns, among others, have been char-acterized as not knowing the difference between a sterile fieldand a cow pasture.1
The purpose of this study was to identify essential entry-levelcompetencies (EELCs) in basic aseptic technique (BAT) that amedical student should demonstrate before first entering theoperating room. This information can then be used to aid in thedevelopment of a standardized BAT curriculum.
Several factors suggested the need for this study. First, areview of the medical education literature between 1970 and2000 revealed a void in studies that examine teaching principlesand standards of BAT to medical students.3-5 One study de-scribed 2 problems with technical skills instruction: a lack ofuniformity in skills that are taught and variability in teachingstrategies.6 In addition, Wells suggested that students need pos-itive role models to emulate acceptable behaviors, and manyrole models in the clinical setting support the concept that BATis not important.1 She further stated that BAT is not difficult toteach or learn, but that it is little valued by members of aca-demia.
A second factor indicating need is that problems exist regard-ing standards and recommended practices in BAT. A review ofthe standards and recommended practices from the Associationof Surgical Technologists, the Association of Operating RoomNurses (AORN), the American College of Surgeons, and theJoint Commission on Accreditation of Healthcare Organiza-tions showed that the standards for BAT for the operating roomenvironment were vague and inconsistent. For example,AORN states that recommended practices should be used asguidelines for the development of policies and procedureswithin the practice setting.7 However, if each practice settingdevelops policies and procedures for BAT in the operatingroom, standardization will not exist.
The third factor suggesting a need is the absence of criteria
s in Surgery 0149-7944/02/$22.00PII S0149-7944(01)00494-9
69

for designated personnel to evaluate performance. On-site re-views of various programs revealed a number of inconsistenciesamong medical student performance in the skills of sterile tech-nique for the operating room. Surgical educators can addressthe above needs by first assessing the current practices for steriletechnique training. Secondly, BAT must be defined in terms ofEELCs that medical students should be able to demonstratefirst, before entering the operating room.
METHODS
The Delphi technique has been successfully used in medicalschool curriculum development.8,9 In this study, data were col-lected using the modified reactive Delphi technique. The mod-ified reactive Delphi differs from the conventional Delphi inthat an expert panel is asked on the first, of 2 surveys, to analyzea previously prepared list of items rather than generate an orig-inal list of items.10 In this study, a list of competencies and otheressential elements for a BAT curriculum were first created by asmall focus group of surgical educators.
The expert panel consisted of a random sample of 50 clerk-ship directors from the Association for Surgical Education(ASE) and 50 perioperative nurse educators affiliated withAORN. The sample was selected from a published ASE mem-bership list of clerkship directors and a published AORN mem-bership list of perioperative nurse educators.
A questionnaire was mailed to the panel members for each ofthe 2 surveys. A letter of explanation was sent with the firstsurvey in which sample members were assured of the anonymityof responses. To enhance the return rate, reminder calls tononrespondents were made 2 weeks after each survey wasmailed.
In this study, the first survey asked the panel to react to theinformation obtained from the focus group in the followingmanner. Panel members were asked to rate the items in the listof EELCs in BAT and the list of instructional strategies gener-ated by the focus group as important or not important. Respon-dents were allowed multiple responses to the remaining 3 ques-tions regarding the curriculum year in which the EELCs shouldbe taught, the preferred instructor, and the optimum method(s)for evaluation of BAT competencies. Each question was open-ended; so those panel members could add other items that theyconsidered important.
The results of the first survey were examined and compiled,with duplicate or similar items from responses to the open-ended questions combined. These first round results were thenused as feedback to the panel in the second survey.
The second survey sought to clarify further the opinion of thepanel. Panel members were asked to review the results of thefirst survey, reconsider their original responses in light of thegroup response, and then indicate their final top rankings orchoices as required for each question. The panel was asked torank the top 8 EELCs, which represent less than one-half of the18 EELCs identified in the first survey. In multivoting, it is
70 CUR
common to reduce a large number of choices by approximatelyone-third to one-half plus 1.11,12
The rankings of the top 8 EELCs were used to prioritize skillsin the refined inventory. For analysis purposes, a panel mem-ber’s top-ranked competency received 8 votes, the second re-ceived 7 votes, the third received 6 votes, and so on, for a totalof 36 votes per panel member. Categories of skills not receivinga rank were assigned 0 votes. Cluster analysis was then used totest for statistically significant differences among the number ofvotes for the competencies.13 Competencies within a clustershould be considered “equal”; that is, the vote differences incompetencies within a cluster are not statistically significant.The vote differences in competencies between clusters, how-ever, are statistically significant.
The last 4 questions were scored as follows. Panel memberswere asked to indicate the most desirable year for teaching BATskills, to indicate (without ranking) the top 5 instructional strat-egies for teaching BAT skills, to select and rank order their top3 choices for instructor, and to select and rank order the top 3methods for evaluating student competencies in BAT skills.
RESULTS
Eighty-one of the 100 first surveys were returned, and 74 of the100 second surveys were returned. Responses were receivedfrom panel members in 33 states and 3 Canadian provinces.The study group had a mean of 21.3 years (S.D. � 10.0) ofclinical experience and a mean of 14.4 years (S.D. � 10.2) ofteaching experience. The study was completed during a6-month period.
Cluster analysis indicated that the 18 EELCs should be clas-sified into 6 clusters, with the 7 competencies that receivedmore than the “expected” 148 votes falling into the first 4clusters. Figure 1 shows the ranking of the 18 EELCs by thevotes received in the second survey. A competency could havereceived as many as 592 votes in the second survey if everyparticipant had ranked it as the most important competency tobe learned by medical students. If the rankings had been totallyrandom, each competency would have received 148 votes,which is 25% of 592. Seven competencies received more than148 votes, and the remaining competencies received less than148 votes. “Maintenance of the sterile field” received the mostvotes with 494 of 592 (83.4%) possible votes. The final 11competencies each received less than 16% of the possible voteand were split between the fifth and sixth clusters, respectively.
The third year appeared to be the curriculum year mostfavored for delivering BAT instruction, receiving 86.5% of thevote in the second survey. Most of the remaining votes cast werefor the second curriculum year.
The top 5 instructional strategies for teaching entry-levelBAT skills are shown in Table 1. Again, panel members were tosimply indicate their top 5 choices for this question. Therefore,percentages do not sum to 100. Panel members for this ques-tion performed no other ranking.
Results for ranking the top 3 choices for instructor indicated
RENT SURGERY • Volume 59/Number 1 • January/February 2002
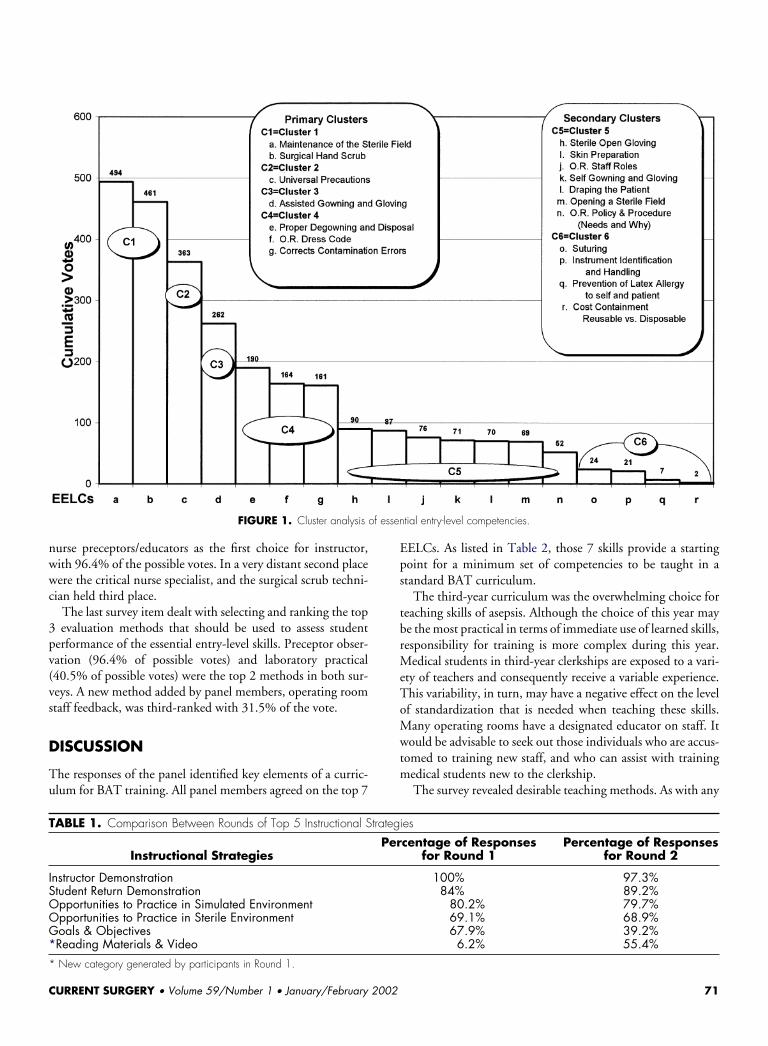
FIGURE 1. Cluster analysis of essential entry-level competencies.
nurse preceptors/educators as the first choice for instructor,with 96.4% of the possible votes. In a very distant second placewere the critical nurse specialist, and the surgical scrub techni-cian held third place.
The last survey item dealt with selecting and ranking the top3 evaluation methods that should be used to assess studentperformance of the essential entry-level skills. Preceptor obser-vation (96.4% of possible votes) and laboratory practical(40.5% of possible votes) were the top 2 methods in both sur-veys. A new method added by panel members, operating roomstaff feedback, was third-ranked with 31.5% of the vote.
DISCUSSION
The responses of the panel identified key elements of a curric-ulum for BAT training. All panel members agreed on the top 7
TABLE 1. Comparison Between Rounds of Top 5 Instructional Strate
Instructional StrategiesP
Instructor DemonstrationStudent Return DemonstrationOpportunities to Practice in Simulated EnvironmentOpportunities to Practice in Sterile EnvironmentGoals & Objectives*Reading Materials & Video * New category generated by participants in Round 1.
CURRENT SURGERY • Volume 59/Number 1 • January/February 200
EELCs. As listed in Table 2, those 7 skills provide a startingpoint for a minimum set of competencies to be taught in astandard BAT curriculum.
The third-year curriculum was the overwhelming choice forteaching skills of asepsis. Although the choice of this year maybe the most practical in terms of immediate use of learned skills,responsibility for training is more complex during this year.Medical students in third-year clerkships are exposed to a vari-ety of teachers and consequently receive a variable experience.This variability, in turn, may have a negative effect on the levelof standardization that is needed when teaching these skills.Many operating rooms have a designated educator on staff. Itwould be advisable to seek out those individuals who are accus-tomed to training new staff, and who can assist with trainingmedical students new to the clerkship.
The survey revealed desirable teaching methods. As with any
gies
ercentage of Responsesfor Round 1
Percentage of Responsesfor Round 2
100% 97.3%84% 89.2%
80.2% 79.7%69.1% 68.9%67.9% 39.2%
6.2% 55.4%
2 71

TABLE 2. Summary of Results for a BAT Curriculum
Top Seven Entry-Level CompetenciesMaintenance of a Sterile FieldSurgical Hand ScrubUniversal PrecautionsAssisted Gowning and GlovingProper Degowning and DisposalOperating Room Dress CodeCorrects Contamination Errors
Curriculum YearThird Curriculum Year
Instructional StrategiesInstructor DemonstrationStudent Return DemonstrationOpportunities to Practice in a Simulated EnvironmentOpportunities to Practice in a Sterile EnvironmentReading Materials and Video
Preferred InstructorNurse Preceptors/Educators
Evaluation MethodsPreceptor ObservationLaboratory PracticalOperating Room Staff Feedback
training of psychomotor skills, it is not surprising that instruc-tor demonstration followed by student return demonstrationand opportunities to practice were the most beneficial instruc-tional strategies. However, it was perplexing that the expertpanel preferred preceptor observation to that of a laboratorypractical for evaluating these skills. After all, the preceptorwould rarely witness these skills before the student entering theoperating room.
It is interesting to note that the panel identified nurse pre-ceptors/educators as the first choice of instructor to teach thesecompetencies to medical students. This finding may suggest thereason for the 30-year gap in the medical education literatureregarding BAT training. These skills may be taught by nursingstaff at medical institutions, but are not well documented in theliterature. Traditionally, nurses have published less in medicaleducation literature than have other medical school facultymembers. On the other hand, the gap in the literature mayrelate to the minor importance such training is given in medicalcurricula.
As previously indicated, the response rate was high for bothsurveys. This implies an exceptional interest in this educationalissue. Of course, the major drawback to providing comprehen-sive BAT training is the cost, both in terms of time and money.Although this study points toward the need to teach BAT com-petencies and assess student proficiency, each educational insti-tution must assess its priorities.
The major limitation of this study is sampling bias. Mem-bership in the organizations from which the sample of panelmembers was drawn is voluntary. The response of volunteermembers from these 2 organizations may differ in important
72 CUR
aspects from those who are nonmembers. One hypothesis theauthors suggest is that organizations focusing on educationalissues may inherently contribute to intended philosophies thatnonmembers may not have previously considered.
Various positive outcomes of BAT training include a reducedrisk of postoperative wound infection and efficiency in operat-ing room procedures, ostensibly leading to a decrease inmedico-legal concerns. In addition, BAT training can partiallyalleviate the intimidating environment of the operating roomfor medical students. Principles of aseptic technique are notcomplex. Knowledge of certain rules can alleviate undue stressfor a medical student working in the operating room; however,lack of instruction and repeated exposure to these practices inthe operating room minimizes the opportunity to develop astrong surgical conscience in the medical student.
This study represents a first step toward creating an opera-tional definition of BAT by determining competencies thatshould be taught to medical students before their first operatingroom experience. The identification of these competencies pro-vides a foundation for the development of a standardized cur-riculum in BAT.
In summary, the overall goal of this study was to identifyentry-level competencies in BAT. The survey results from thepanel of surgical educator experts suggest a list of prioritizedEELCs in BAT that should be taught in medical curricula.With such competencies identified, valid evaluation techniquescan be further developed to assess student proficiency. This typeof outcomes-based curriculum in BAT training for the operat-ing room should help to improve the overall surgical educa-tional experience for all medical students.
ACKNOWLEDGMENT
This research was completed as Ms. Leeper’s Surgical Educa-tion Research Fellowship offered through the Association forSurgical Education.
REFERENCES
1. Wells P. Teaching aseptic technique. Today’s OR Nurse.1983;5: 20-24.
2. Atkinson LJ, Kohn ML. Berry and Kohn’s Introduction toOperating Technique. 7th ed. New York: McGraw-Hill;1992.
3. Couves CM. A course in surgical technique for medicalstudents. Can J Surg. 1970;13:31-32.
4. Lazaro EJ, Rush BJ, Blackwood JM, Swaminathan AP.Assessment of student experiences in technical proceduresin surgical clerkship. Can J Surg. 1978;21:540-541.
5. Nakayama DK, Steiber A. Surgery interns’ experiencewith surgical procedures as medical students. Am J Surg.1990;159:341-343.
RENT SURGERY • Volume 59/Number 1 • January/February 2002
6. Lossing A, Groetzsch G. A prospective controlled trial ofteaching basic surgical skills with 4th year medical stu-dents. Med Teach. 1992;14(1):49-52.
7. Association of Operating Room Nurses. Standards andRecommended Practices for Perioperative Nurses. Denver:AORN Inc.; 1994.
8. Somers K, Baker G, Isbell C. How to use the Delphitechnique to forecast training needs. Performance Instruc-tion J. 1984;5:26-28.
9. Stritter F, Tresolini C, Reeb K. The Delphi technique incurriculum development. Teaching Learning Med. 1994;6:136-141.
CURRENT SURGERY • Volume 59/Number 1 • January/February 200
10. McKenna H. The Delphi technique: a worthwhile re-search approach for nursing. J Adv Nurs. 1994;19:1221-1225.
11. Scholtes PR. The Team Handbook. Joiner Associates Inc.;1988.
12. Brassard M, Ritter D. The Memory Jogger II. GOAL/QPC;1994.
13. Aldenerfer M, Blashfield R. Cluster Analysis. Sage Univer-sity Paper Series on Quantitative Applications in the So-cial Sciences, 07-001. Beverly Hills: Sage Publications;1984.
2 73