Embed Size (px)
Citation preview
Basic and clinical aspects of selection and application of fiber posts
Simone Grandini
UNIVERSITY OF SIENA SCHOOL OF DENTAL MEDICINE
PHD PROGRAM:
“DENTAL MATERIALS AND CLINICAL APPLICATIONS”
PhD THESIS OF: Simone Grandini TITLE “Basic and clinical aspects of selection and application of fiber posts”
ACADEMIC YEAR 2003/2004 18 December 2004 Siena, Italy Committee: Promoter Prof. Marco Ferrari Co-Promoter Prof. Franklin R Tay Prof. Egidio Bertelli Prof. Carel L Davidson Prof. Manuel Toledano Prof. Michel Goldberg Prof. Piero Balleri
TITLE Basic and clinical aspects of selection and application of fiber posts CANDIDATE Simone Grandini
18 December 2004

CONTENTS
Chapter 1 General Introduction……………………………………..…….……...3
1.1 Differences between healthy and root canal treated teeth………………………….4
1.1.1 Changes in the physical and chemical properties of the tissue……….5
1.1.2 Changes in the morphology and in the biomechanical behavior of
teeth under stress…………………………………………………………………….6
1.1.3 Possible elevation of pain threshold and loss of pressoreceptors....…7
1.2 Relation between fracture resistance of the endodontically-treated teeth and
presence of posts………………..…………………...………………………………………8
Chapter 2 The use of fiber posts in dentistry…………………………………....16
2.1 The use of fiber posts………………………………………………………..…………16
2.2 Fabrication process and structure of fiber posts ………………………………16
2.3 Structure and mechanical properties of fibre posts ……………………………18
2.4 Metal posts versus fiber posts…………………………………………………..19
2.5 Role of the final restoration design (ferrule effect)………...………..……………20
Chapter 3 Preparation of root canal dentin to bonding………..………………26
3.1 Evaluation of Glyde File Prep in combination with sodium hypochlorite as root
canal irrigant: a scanning electron microscopic study……………………………...28
Chapter 4 Criteria for selecting fiber posts ……………………………………..41
4.1 Fatigue resistance and structural characteristics of fiber posts: three-point
bending test and SEM evaluation. …………………………………………………41
Chapter 5 Adjusting the length of a post………………………………….60
5.1 Scanning electron microscopic investigation of the surface of fibre posts after
cutting………………………………………………………………………………60
Chapter 6 Selection of clinical luting procedures ..............................................70
6.1 A one step procedure for luting glass fibre posts: an SEM evaluation…………71
Chapter 7 Anatomic Post: an innovative approach…………………………… 85
7.1 SEM evaluation of the cement layer thickness after the luting procedures of two
different posts……………………………………………………………………….85
7.2 Use of Anatomic Post’n Core for reconstructing an endodontically treated tooth:
a case report………………………………………………………………………...94
1

Chapter 8 Clinical aspects and future role of fiber posts in dentistry ……...113
8.1. Clinical evaluation of the use of fiber posts and direct resin restorations for
endodontically-treated teeth ………………………………………………………113
Chapter 9 Summary and conclusions …………………………………..129
Riassunto e conclusioni ………………………………………………………….135
Résumé et conclusions …………………………………………………………..142
Schlußfolgerung …………………………………………………………………149
Resumen y conclusiones .......................................................................................155
Sumário e conclusões ............................................................................................162
Complete list of references ……………………………………………………...169
Acknowledgements ……………………………………………………………...183
CURRICULUM VITAE ………………………………………………………...185
2

Chapter 1 General introduction
The restoration of the endodontically-treated teeth has always been a debated topic.
A tooth requires endodontic treatment as a result of caries, repeated restorative
procedures, or trauma. Many changes occur to a tooth after root canal treatment,
including the physical and chemical properties of dentin, its elasticity, resistance to
fatigue, changes in the morphology and biomechanical behaviour. As early as 1746,
Fauchard (Fauchard, 1746) proposed the insertion of wooden dowels (the first real
“fiber post”) in canals of teeth to give support to crown retention. Since then, many
different materials have been proposed for “reinforcement” and retention of the
restorative core.
This thesis contains a study on several different basic and clinical aspects related to
the selection and use of fiber posts.
Starting from the assessment of the differences between healthy and root canal
treated teeth, the next step was to analyse the relationship between the presence of a
post and root fracture. Fiber posts were the first true alternative to metal posts, and
they jeopardized in the dental market in the last 10 years; for this reason an
overview regarding the properties, advantages and disadvantages of fiber reinforced
materials is presented.
A clean and neat root canal is one of the goals pursued during endodontic treatment.
The first objective of this thesis was to evaluate different irrigating regimes to
achieve a clean root canal before guttapercha condensation procedures and
eventually the insertion of the post.
As actually many fiber posts are available on the market, it is important for the
clinician to know the properties of each fiber post available on the market, and to
consequently select the more appropriate. The second was indeed to conduct a study
to assess the fatigue resistance of different types of fiber posts, and to verify the
existence of a correlation between the fatigue resistance exhibited by the different
types of posts and their structural characteristics. These are also very important
when calibrating a post before or after the luting procedures. Another goal of this
thesis was in fact to evaluate if and how three cutting methods can affect integrity of
fibre posts, and analyse the differences in cutting procedures.
3

Bonding procedures are a prerequisite when using fiber posts. Another step of this
thesis was to evaluate the efficacy of a technique (“one-shot”) -alternative to the
well-established procedure- in forming resin tags, adhesive lateral branches and
RDIZ when luting translucent fibre posts into root canal preparations.
Fibre posts went through rapid developments in the last few years, in particular
when dealing with the shape of the post. Interestingly, starting from the double-
cylinder shape, endodontic shapes and then double tapered shapes were presented,
as the adhesive cementation now relies on formation of resin dentin interdiffusion
zone and resin tags (Ferrari et al 2002) even if the good fitting and mechanical
retention of the post inside the root canal contribute to sliding friction as for non
adhesive cements (Goracci et al 2004). As a matter of fact it is pretty common to
face root canals that are not perfectly round after endodontic instrumentation. A
study was conducted regarding the very last brand of fiber post available (Anatomic
Post’n Core, RTD, St Egrève, France), that is able to reduce the cement thickness
and to immediately restore the coronal portion in cases where the root canal is not
round and a huge loss of tooth structure is present.
Finally a possible future use of fiber posts in combination with a direct resin
restoration is examined for the restoration of root canal treated teeth, according to
the aim of the minimal intervention philosophy.
1.1 Differences between healthy and root canal treated teeth
There is substantial literature stating that endodontically-treated teeth differ from
teeth with a viable pulp (Ingle JA 1973, Walton R et al.,1996). As a matter of fact,
tooth fractures often result in severe damages to non-vital teeth (Angmar-Månsson
et al., 1969, Rud et al., 1970, Meister et al., 1980, Morfis, 1990, Testori et al., 1993,
Bergman et al., 1989, Torbjöner et al., 1995, Fuss et al., 1999), and mostl likely, the
only alternative therapy is extraction. Three main aspects can be analyzed regarding
these differences after root canal therapy: 1) changes in the physical properties and
in the chemical composition, 2) changes in the morphology and in the
biomechanical behavior of teeth under stress, 3) possible elevation of pain threshold
and loss of pressoreceptors.
4

1.1.1 Changes in the physical and chemical properties of the tissue
A vital tooth presents with a stiffer structure (enamel) and a more compliant support
underlying it (dentin). Notwithstanding a fracture that can always occur, teeth
usually exhibit microcracking of the enamel as a consequence of wear (tooth-to-
tooth and tooth-to-food wear). Type I mineralized collagen fibrils are abundant
within healthy dentin. Back in 1998, Nakabayashi and Pashley (Nakabayashi et al.,
1998) demonstrated that these fibrils are able to retard the growth of microcracks
(Sakaguchi et al., 1992), and that if they are removed after root canal treatment a
fracture is more likely to occur. The main physical properties of dentin that were
studied during the years were the modulus of elasticity, the tensile strength and the
compressive strength. Unfortunately results differ a lot from tooth to tooth and
within the same type of tooth (Peyton et al., 1952; Tyldesley 1959). The methods in
which elasticity or the dentin hardness were measured have changed through time.
Using a micro-indentation technique, Lewinstein et al. (1981) observed no
difference in the elasticity and dentin hardness between vital teeth and teeth that
were endodontically treated 5 or 10 years before (Lewinstein et al. 1981). Pashley et
al. (1985) showed that the micro-hardness of coronal dentin is higher in superficial
than in deep dentin. This decrease in hardness may be due to a decrease in the
stiffness of the intertubular matrix (Kinney et al., 1996). Many techniques were used
to measure the modulus of elasticity. Some studies reported values between 15 and
19 GPa (Sano et al., 1995; Van Meerbeek et al., 1993), while the ultimate
compressive strength was around 300 MPa. When the microtensile test was used to
measure the ultimate tensile strength of dentin, values around 100 MPa were
reported (Sano et al., 1994). Irrigating solutions that are used in endodontics have
been reported to have a negative effect on the physical properties of dentin. Micro-
hardness is significantly reduced in root canal dentin after the use of H2O2/NaOCl
and EDTA (Saleh et al., 1999). Different concentrations of NaOCl can also reduce
tooth surface strain, even if no difference was found in the strain recorded after
different irrigation regimes (Goldsmith et al., 2002). Chemical changes may also
occur when a tooth is endodontically treated. Healthy dentin can be described as a
“…biological composite of a collagen matrix filled with submicron to nanometer-
sized calcium deficient, carbonate-rich apatite crystallites dispersed between
5

micron–sized hyper-mineralised, collagen-poor hollow cylinders…” (Marshall et al.,
1997). Dentin is about 50% (vol.) mineral, 20% (vol.) water and 30% (vol.) organic
matrix (LeGeros 1991), but the composition may change with position of the tooth
and even within a tooth (Panighi et al., 1993). Age or disease can affect the
composition: coronal dentin has approximately twice the number of tubules of
radicular dentin and also less inorganic substrate and less intertubular dentin, while
radicular dentin contains less moisture. A 9% lower moisture content was found in
pulpless dog teeth when compared with vital dog teeth (Helfer et al., 1972). A later
study (Huang et al., 1992) showed that dehydration of human dentin increased its
Young’s modulus and that wet dentin specimens from treated pulpless teeth
generally showed lower elastic modulus and proportional limit in compression than
those of normal teeth. Using a method of collagen dissolution, Mason (2001)
demonstrated that the percentage of collagen present in crown and root dentin
decreases after the root canal treatment. The percentage of collagen in crown dentin
of healthy teeth is 21.7%. The value was reduced to 20.1% in teeth that had been
endodontically treated for 2 years, and was further reduced to 16.8% in teeth that
had been endodontically for 10 years. In root dentin the percentages are 25.5%,
23.5% and 19.3% respectively. Moreover, a degradation of resin composite and
depletion of collagen fibrils were observed in specimens that were aged in an oral
environment (Hashimoto et al., 2000). These findings were further confirmed in a
recent transmission electron microscopy study, showing a decrease in the
distribution of the collagen fibrils within root dentin 5 years after endodontic
treatment (Ferrari et al., 2004).
1.1.2 Changes in the morphology and in the biomechanical behavior of teeth under
stress
In 1976, Tidmarsh described the intact tooth as a “…hollow, laminated structure that
deforms under load; this structure may undergo permanent deformation following
excessive or sustained loads…”(Tidmarsh 1976) . In his PhD thesis at the University
of Otago, Grimaldi showed that there is a “…direct relationship between the amount
of central tooth structure lost in cavity preparation and the deformation under
load….after endodontic access preparation the tooth can deform to a greater extent
6

under applied load and thus be more susceptible to fracture. It might therefore be
expected that the removal of dental substance during access cavity preparation and
cleaning and shaping procedures would significantly weaken the tooth…” (Grimaldi
1971). On the other hand, in a study comparing MOD cavity preparation with simple
access opening and endodontic procedures in maxillary second premolars, the
reduction in tooth stiffness was 60% versus 5% (Reeh et al., 1989). The highlights
the importance of preserving the marginal crest as a structure that can compensate
for the stresses generated by the occlusal and chewing forces. Other structures, such
as the presence of intact roofs of pulp chambers, are also important in avoiding root
fractures in a healthy tooth (Fuzzi 1993). Usually, pulpless teeth have lost
substantial coronal and radicular tooth structure from pre-existing restorations,
dental caries, and access cavity preparations (Morgano et al., 1993). The endodontic
procedure in itself can also be an explanation for additional morphological changes.
Excessive flaring during endodontic treatment and poor gutta-percha condensation
procedures were considered as possible causes of root fracture (Trabert et al., 1978,
Milot et al., 1992). The introduction of NiTi rotary instruments has led to great
improvements in the effectiveness and speed of root canal instrumentation, and a
more conservative approach is universally adopted in order to reduce the amount of
tooth structure that has to be eliminated during the root canal treatment. These
instruments allow faster (Schafer et al., 2001, Gambill et al., 1996, Glosson et al.,
1995), more centered (Gambill et al., 1996, Glosson et al., 1995, Bertrand et al.,
2001), rounder (Gambill et al., 1996, Glosson et al., 1995) and more conservative
(Schafer et al., 2001, Gambill et al., 1996, Glosson et al., 1995) shapings of the root
canals than stainless steel instruments.
1.1.3 Possible elevation of pain threshold and loss of pressoreceptors.
Another possible cause of weakness of endodontically-treated teeth might be the
loss of pressoreceptors. There is no clear evidence about this topic. When pain
thresholds of vital and endodontically-treated teeth were analysed with a minimal
load (Lowenstein et al., 1955), it was found that the load thresholds were 57%
higher in endodontically-treated teeth compared to vital teeth. An autoradiographic
study of the sensory innervation of rats’ teeth (Pimenidis et al., 1977) showed the
7

presence of structures similar to corpuscular receptors in the pulp, thereby
suggesting that those tissues may be responsive to modalities other than pain, such
as pressure. Another study (Linden 1975) did not support this hypothesis. More
recent studies on the reflex control of human jaw-closing muscles suggested the role
of periodontal and gingival receptors as potential pressoreceptors (Louca et al.,
1996, 1998).
In conclusion, the general loss of tooth structure in the non-vital tooth, together with
the alterations in collagen distribution, may simultaneously contribute to the
increased susceptibility of endodontically-treated teeth to fracture under loading. A
further reduction in micro-hardness can be induced by the use of irrigating solutions
during endodontic treatment. The loss of water, the increase in deformation due to
the loss of load-supporting structure, and the generation of micro-fractures by gutta-
percha condensation procedures may also contribute to the weakness reported in
endodontically-treated teeth.
1.2 Relation between fracture resistance of the endodontically-treated teeth and
presence of posts
It is a common belief that the likelihood of survival of a pulpless tooth is directly
related to the quantity and quality of remaining tooth structure (Assif et al., 1994,
Guttman, 1992, Cohen et al., 1996). For many years, the concept of using a post for
the restoration of endodontically-treated teeth was based upon the philosophy that
the post would “reinforce” the tooth, and that additional retention was needed for the
core restoration. A post was generally placed in an attempt to strengthen the tooth.
However, as dentin has to be sacrified, especially when a metal post is utilized, and
in consideration of other aspect that will be analyzed later, a post does not
strengthen the root, but serves solely to improve retention of the core (Lloyd et al.,
1993, Sorensen et al., 1990, Morgano et al., 1996, Abou-Rass, 1992). Resistance to
fracture of the non-vital tooth is related with the thickness of remaining root dentin,
especially in the bucco-lingual direction (Guzy et al., 1979, Mattison, 1982, Tjan et
al., 1985). Several factors have been identified (Stockton, 1999, Morgano et al.,
8
1999), in both clinical or laboratory studies, to affect the fracture resistance and the
failure modes of post-core restorations.
An important factor is the type of tooth and its position in the dental arch. It was
found that half of the fractured post-retained teeth were maxillary second premolars
(27.2%) and mesial roots of the mandibular molars (24%). The susceptibility of
these teeth to root fracture increased when the residual sound tooth structure was
less than 1-2 mm (Pilo et al., 1998, 2000; Tamse et al., 1999). Moreover, oval-
shaped canals are more prone to root fracture, as there are more spaces that have to
be filled with luting cements. As the cement dissolves, spaces are inadvertently
created for the post to move inside the dowel space. These micro-movements may
eventually result in dislodging of the post, fatigue of the tooth and root fracture
(Chapman et al., 1985).
Post length is important as well. Many different recommendations have been given
to clinicians regarding this issue (one half, two thirds, three quarters of the root,
below the cemento-enamel junction, as long as possible…etc). Sorensen and
Martinhof (1984a, 1984b) reported a high risk of tooth fracture for teeth with short
posts, while other studies indicated that long posts can affect root resistance because
of the removal of tooth structure in the deepest part of the root itself (Guzy et al.,
1979).
Besides the length, the diameter of the post is also significant. This is related to the
remaining tooth structure. As an increase in post diameter did not provide in
increase in post retention, conservation of remaining tooth structure by avoiding the
use of posts with a large diameters have been recommended (Standlee et al., 1978;
Guzy et al., 1979; Standlee et al., 1980).
Three basic types of clinical study are able to provide information on the incidence
of root fracture in endodontically-treated teeth. They include surveys of root
fractured extracted teeth, retrospective studies on the fracture rate of endodontically-
treated restored teeth, and prospective studies on the fracture rate of certain types of
restorations of endodontically-treated teeth.
Initially, corrosion was cited as a cause of root fractures (Angmar-Månsson et al.,
1969; Rud et al., 1970). In these papers maxillary premolars accounted for 61.5% of
the total number of root fractures, the mandibular premolars accounted for 16.3%,
9

and the other tooth types ranged from 0.4% for mandibular incisors to 5.4% for the
first mandibular molars. These percentages may be partially caused by the
observation that some teeth are endodontically treated and restored with posts less
frequently than others, and by the fact that molars were more commonly extracted in
the era in which these studies were conducted. High percentages of endodontically-
treated fractured premolars, 56% and 52% respectively, were also found in two more
recent surveys of 36 (Testori et al., 1993) and of 92 vertically fractured teeth (Tamse
et al., 1999). The mesial roots of mandibular molars were also frequently extracted
because of root fractures (Tamse et al., 1999). Among all the surveys of tooth
extraction due to root fracture, only the study of Testori et al. (1993) included a
statistical analysis of the results. A significantly higher incidence of fractures in
premolars and molars was found. But the majority of studies available on the root
fractures of endodontically-treated teeth are retrospective in nature (Hansen et al.,
1990a, 1990b; Walton, 1997, 1999). The studies by Sorensen and Martinoff (1984 a,
1984b) are often cited when debating this topic. Their conclusions were that coronal
coverage did not significantly improve the rate of clinical success for anterior teeth
while it improved the rate of clinical success for premolars and molars. Among teeth
restored with posts, the parallel-sided serrated dowel with an amalgam or resin
composite core recorded the highest success rate. The tapered cast dowel and core
displayed a higher failure rate than teeth treated without intracoronal reinforcement.
The parallel-sided serrated dowel did not have failures caused by root fracture,
whereas root fractures caused extractions of teeth restored with tapered cast dowels
and cores. The success rate of teeth with a dowel length equal or greater than the
crown length exceeded 97%. One of the authors’ conclusions was that “…a post did
not significantly strengthen endodontically treated teeth…”. Unfortunately no
prospective studies are available to definitely validate all the aspects analyzed. More
prospective studies are required to evaluate post-core restorations in controlled
clinical situations.
10
References
Abou-Rass M. Post and core restoration of endodontically treated teeth. Curr Opin
Dent 1992;2: 99-107.
Angmar-Månsson B, Omnell K-Å, Rud J. Root fractures due to corrosion. I.
Metallurgical aspects. Odontol. Revy 1969;20: 244-65.
Assif D, Gorfil C. Biomechanical considerations in restoring endodontically treated
teeth. J Prosthet Dent 1994; 71:565-7.
Bergman B, Lunquist P, Sjögren U, Sundqvist G. Restorative and endodontic results
after treatment with cast posts and cores J Prosthet Dent 1989;61: 10-15.
Bertrand M-F, Lupi-Pegurier L, Medioni M, Muller M, Bolla M. Curved molar root
canal preparations using Hero 642 rotary nickel-titanium instruments. International
Endododontic Journal 2001;34, 631-36.
Chapman KW, Worley IL, Von Fraunhofer JA. Retention of prefabricated posts by
cements and resins. J Prosthet Dent 1985;54: 649-52.
Cohen BI, Pagnillo MK, Condos S, Deutsch AS. Four materials measured for
fracture strength in combination with five designs of endodontic posts. J Prosthet Dent 1996;
76:487-95.
Fauchard P. The surgeon dentist or treatise on the teeth, vol.2. Translated from the
2nd edition 1746 by L. Londsay, London, Butterworth and company LtD 1946.
Ferrari M, Mason PN, Goracci C, Pashley DH, Tay FR. Collagen degradation in
endodontically treated teeth after clinical function. J Dent Res. 2004 May;83(5):414-9.
Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted
endodontically treated teeth. Int Endod J 1999;32: 283-86.
Fuzzi M. The restoration of the endodontically treated tooth. From the text
“Endodontics”, Castellucci A, Ed Martina, Milano, 1993.
Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless
steel hand file instrumentation using computed tomography. J Endod 1996;22, 369-375.
Glosson CR, Haller RH, Brentdove S, del Rio CE. A comparison of root canal
preparations NiTi hand, NiTi engine-driven and K-Flex endodontic instruments. J Endod
1995;21, 146-151.
Goldsmith M, Gulabivala K, Knowles JC. The effect of sodium Hypochlorite
irrigant concentration on tooth surface strain. J Endod 2002;vol 28, n.8:575-9.
Goracci C, Fabianelli A, Sadek F, Papacchini F, Tay FR, Ferrari M. The
contribution of friction to the dislocation resistance of bonded fiber posts. J Endod 2004 in
press.
11
Grimaldi J. Measurement of the lateral deformation of the tooth crown under axial
compressive cuspal loading. 1971. Thesis University of Otago, Dunedin, New Zealand.
Gutman JL. The dentin-root complex: anatomic and biological considerations in
restoring endodontically treated teeth. J Prosthet Dent 1992; 67:458-67.
Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth
with and without endo-post reinforcement. J Prosthet Dent 1979;42: 39-44.
Hansen EK; Asmussen E. In vivo fractures of endodontically treated posterior teeth
restored with enamel bonded resin. Endod Dent Traumatol 1990;6: 218-25.
Hansen EK, Asmussen E, Christansen NC. In vivo fractures of endodontically
treated posterior teeth restored with amalgam. Endod Dent Traumatol 1990;6: 49-55.
Hashimoto M, Ohno H, Kaga M, et al. In vivo degradation of resin-dentin bonds in
humans over 1 to 3 years. J Dent Res 2000 Jun;79(6):1385-91.
Helfer AR, Melnick S, Schilder H. Determination of the moisture content of vital
and pulpless teeth. Oral Surg Oral Med Oral Pathol 1972;34: 661-70.
Huang T-JG, Shilder H, Nathanson D. Effects of moisture content and endodontic
treatment on some mechanical properties of human dentin. J Endod 1992;18: 209-15.
Ingle JA. Endodonzia. Piccin Editore, 1993, Padova, Italy 29-40.
Kinney JH, Balooch M, Marshall SJ, Marshall GW, Weihs TP. Atomic force
microscope measurements of the hardness and elasticity of peritubular and intertubular human
dentin. J Biomech Eng 1996;118: 133-35.
LeGeros RZ.Calcium phosphates in oral biology and medicine. In Meyers HM(ed)
Monographs in Oral Sciences. New-York Karger 1991;15:109-11.
Lewinstein I, Grajower R. Root dentin hardness of endodontically treated teeth. J
Endod 1981;7: 421-22.
Linden RW. Touch thresholds of vital and non vital human teeth. Exp Neurol
1975;48: 387-90.
Lloyd PM, Palik JF. The philosophies of dowel diameter preparation: a literature
review. J Prosthet Dent 1993; 69:32-6.
Louca C, Cadden SW, Linden RW. The roles of periodontal ligament
mechanoreceptors in the reflex control of human jaw-closing muscles. Brain Res 1996;731:
63-71.
Louca C, Vidgeon SD, Cadden SW, Linden RW. The role of gingival
mechanoreceptors in the reflex control of human jaw-closing muscles. Arch Oral Biol
1998;43: 55-63.
12
Lowenstein NR, Rathkamp R. A study on the pressoreceptive sensibility of the
tooth. J Dent Res 1955;34: 287-94.
Marshall GW, Marshall S, Kinney JH, Balooch M. The dentin substrate: structure
and properties related to bonding. J Dent 1997;25: 441-58.
Mason PN. Transactions of International ADM meeting, Siena 2001.
Mattison GD. Photoelastic stress analysis of cast-gold endodontic posts. J Prosthet
Dent 1982;48: 407-11.
Meister F, Lommel TJ, Gerstein H. Diagnosis and possible causes of vertical root
fractures. Oral Surg, Oral Med, Oral Pathol 1980;49: 243-53.
Milot P, Stein RS. Root fracture in endodontically treated teeth related to
post selection and crown design J Prosthet Dent 1992;68: 428-35.
Morfis AS. Vertical root fractures. Oral Surg, Oral Med, Oral Pathol 1990;69:631-5.
Morgano SM. Restoration of pulpless teeth: application of traditional principles in
present and future contexts J Prosthet Dent 1996;75: 375-80.
Morgano SM, Brackett SE. Foundation restorations in fixed prosthodontics: current
knowledge and future needs. J Prosthet Dent 1999;82: 643-57.
Morgano SM, Milot P. Clinical success of cast metal post and cores. J Prosthet Dent
1993; 70:11-6.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissues Berlin:
Quintessence Co. Publ. 1998.
Panighi M, G’Sell C. Effect of the tooth microstructure on the shear bond strength
of a dental composite. J Biomed Mater Res 1993;27: 975-81.
Pashley DH, Okabe A, Parham P. The relationship between dentin microhardness
and tubule density. Endod Dent Traumatol 1985;1: 176-79.
Peyton FA, Mahler DB, Hershenov MS. Physical properties of dentin. J Dent Res
1952;31: 366-70.
Pilo R, Corcino G, Tamse A. Residual dentin thickness in mandibular premolars
prepared with hand and rotatory instruments. J Endod 1998;24: 401-04.
Pilo R, Tamse A. Residual dentin thickness in mandibular premolars prepared with
gates glidden and ParaPost drills. J Prosthet Dent 2000;8: 617-23.
Pimenidis MZ, Hinds JW. An autoradiographic study of the sensory innervation of
teeth. Dental pulp and periodontium. J Dent Res 1977;56: 835-40.
Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of
endodontic and restorative procedures. J Endod 1989;15: 512-16.
13
Rud J, Omnell KÅ. Root fractures due to corrosion. Diagnostic aspects. Scand J
Dent Res. 1970;78: 397-403.
Saleh AA, Ettman WM Effect of endodontic irrigation solutions on microhardness
of root canal dentin. J Dent 1999;27: 43-6.
Sano H, Ciucchi B, Matthews WG, Pashley DH. Tensile properties of mineralized
and demineralized human and bovine dentin. J Dent Res 1994;73: 1205-11.
Sano H, Takatsu T, Ciucchi B, Russell CM, Pashley DH. Tensile properties of resin
infiltrated demineralized human dentin. J Dent Res 1995;74: 1093-1102.
Sakaguchi RL, Cross M, Douglas WH. A simple model of crack propagation in
dental restorations. Dent Mater. 1992 ;8(2):131-6.
Schafer E, Lohman D. Efficiency of rotary nickel-titanium Flex-Master instruments
compared with stainless steel hand K-Flexofile – Part 1. Shaping ability in simulated curved
canals. Int Endod J 2002;35, 502-13.
SorensenJA, Engelmen MJ. Effect of post adaptation on fracture resistance of
endodontically treated teeth. J Prosthet Dent 1990;64:419-24.
Sorensen JA, Martinoff JT. Clinically significant factors in dowel design. J Prosthet
Dent 1984a 52: 28-35.
Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a
study of endodontically treated teeth. J Prosthet Dent 1984b 51: 780-84.
Standlee JP, Caputo M, Hanson EC. Retention of endodontic dowels: effect of
cement, dowel length, diameter and design. J Prosthet Dent 1978;39: 400-5.
Standlee JP, Caputo AA, Holcomb JP, Trabert KC. The retentive and stress-
distributing properties of a threaded endodontic dowel. J Prosthet Dent 1980;44: 398-404.
Stockton LW. Factors affecting retention of post systems: a literature review. J
Prosthet Dent 1999;81: 380-85.
Tamse A, Fuss Z, Lustig J, Kaplavi J. An evaluation of endodontically treated
vertically fractured teeth. J Endod 1999;25: 506-8.
Testori T, Badino M, Castagnola M. Vertical root fractures in endodontically treated
teeth: a clinical survey of 36 cases. J Endod 1993;19: 87-91.
Tidmarsh BG. Restoration of endodontically treated posterior teeth. J Endod 1976, 2
:374-75.
Tjan AHL, Whang S. Resistance to root fracture of dowel channels with various
thicknesses of buccal dentin walls. J Prosth Dent 1985; 53: 496-500.
Torbjöner A, Karlsson S, Odman PA. Survival rate and failure characteristics for
two post designs. J Prosthet Dent 1995;73: 439-44.
14
Trabert KC, Caputo AA, Abou Rass M. Tooth fracture: a comparison of endodontic
and restorative treatments. J Endod 1978;4: 341-45.
Tyldesley WR. The mechanical properties of human enamel and dentine. Br Dent J
1959;106: 269-78.
Van Meerbeek B, Willems G, Celis JP, Roos JR, Braem M, Lambrechts P,
VanHerle G. Assessment by nano-indentation of the hardness and elasticity of the resin-
dentin-bonding area. J Dent Res 1993;72: 1434-42.
Walton TR. A 10-year longitudinal study of fixed prosthodontics.1 Protocol and
patient profile. Int J Prosthodont 1997;10: 325-31.
Walton TR. A 10-year longitudinal study of fixed prosthodontics: clinical
characteristics and outcome of single unit metal crowns. Int J Prosthodont 1999;12: 519-26.
Walton R, Torabinejad M. Principles and practice of endodontics, 2nd edition, W.B.
Saunders Co., 1996: 212-14.
15

Chapter 2 The use of fiber posts in dentistry
2.1 The use of fiber posts
The potential of fiber reinforced materials in restorative dentistry has been
appreciated for some time (Bradley et al., 1980). With the introduction of fiber posts
(Duret et al., 1990a; 1990b, 1992), a new trend has been established, in the
restoration of the endodontically-treated teeth. Fiber posts can be considered as
composite reinforced materials. A composite is “any material that is composed of
hard, peeble-like filler particles, surrounded by a hard matrix of a second material,
which binds the filler particles together” (Vichi A et al., 2002). The purpose of
making composite structures is to obtain better mechanical characteristics with the
final material when compared to the single components. As far as fiber posts are
concerned, fibers are embedded in a matrix of epoxy-resin, and an interfacial agent
such as silane is used to optimize the link between the two components.
2.2 Fabrication process and structure of fiber posts
To manufacture fiber-reinforced post, the first step is to produce cylindrical barrels
and then these barrels are machined into different shape and diameter. Pultrusion is
the name for this process, frequently it is a continuous and semi-automated process.
Resin-impregnated fibers are pulled through a series of forming dies. The final die is
heated to cure the resin, thereby producing a rigid composite section. The profile is
determined by the die cross-section which could be round, rectangular, square or a
variety of other shapes. The section produced can either be cut into dicrete lengths
after the puller system or wound onto a drum. The speed of travel through the die is
determined by the viscosity, thickness and curing of the resin. The process uses a
hardened (hard-chromed) steel die and a pultrusion machine (Fig 1).
16
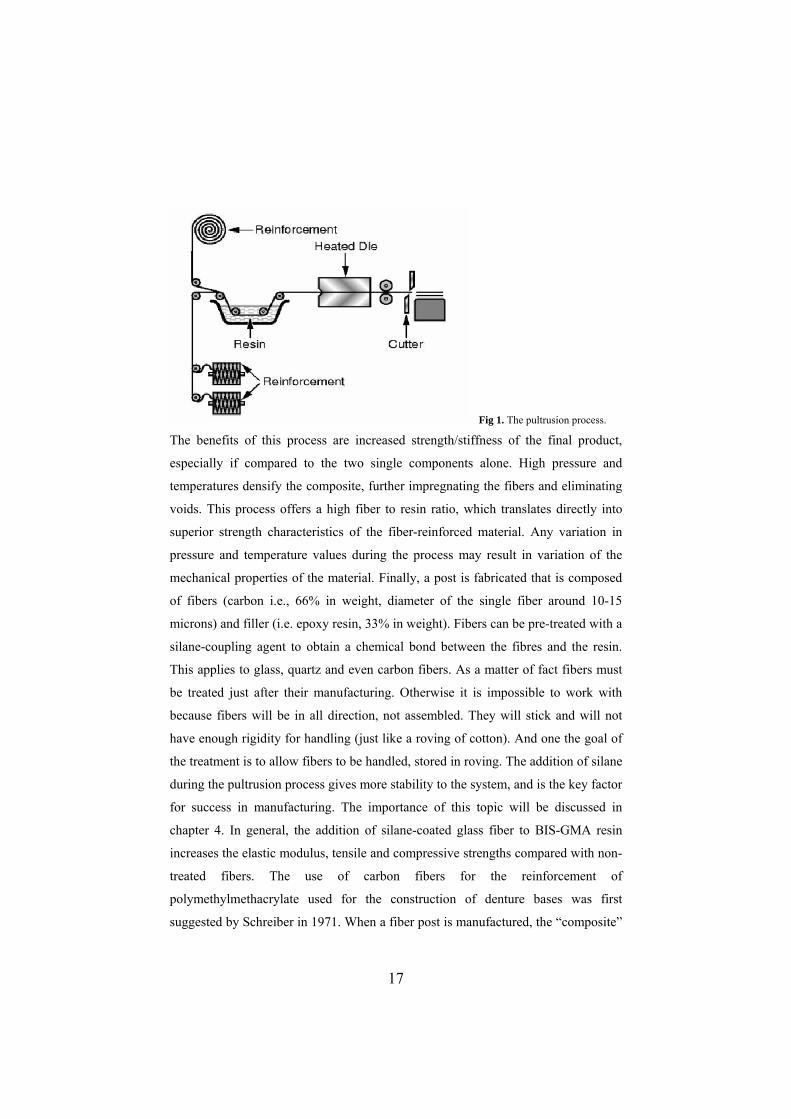
Fig 1. The pultrusion process.
The benefits of this process are increased strength/stiffness of the final product,
especially if compared to the two single components alone. High pressure and
temperatures densify the composite, further impregnating the fibers and eliminating
voids. This process offers a high fiber to resin ratio, which translates directly into
superior strength characteristics of the fiber-reinforced material. Any variation in
pressure and temperature values during the process may result in variation of the
mechanical properties of the material. Finally, a post is fabricated that is composed
of fibers (carbon i.e., 66% in weight, diameter of the single fiber around 10-15
microns) and filler (i.e. epoxy resin, 33% in weight). Fibers can be pre-treated with a
silane-coupling agent to obtain a chemical bond between the fibres and the resin.
This applies to glass, quartz and even carbon fibers. As a matter of fact fibers must
be treated just after their manufacturing. Otherwise it is impossible to work with
because fibers will be in all direction, not assembled. They will stick and will not
have enough rigidity for handling (just like a roving of cotton). And one the goal of
the treatment is to allow fibers to be handled, stored in roving. The addition of silane
during the pultrusion process gives more stability to the system, and is the key factor
for success in manufacturing. The importance of this topic will be discussed in
chapter 4. In general, the addition of silane-coated glass fiber to BIS-GMA resin
increases the elastic modulus, tensile and compressive strengths compared with non-
treated fibers. The use of carbon fibers for the reinforcement of
polymethylmethacrylate used for the construction of denture bases was first
suggested by Schreiber in 1971. When a fiber post is manufactured, the “composite”
17

that is formed is anisotropic: as a consequence mechanical properties differ
according to the direction of measurement.
2.3 Structure and mechanical properties of fibre posts
The Composipost (RTD, St Egrève, France) is the most studied carbon-fiber post. It
was described by its inventors as a post fabricated from continuous, unidirectional
high performance, pyrolytic carbon fibers, 8 µm in diameter uniformly embedded in
an epoxy-resin matrix (Duret et al., 1990a, 1990b). The fibers constitute 64% by
volume of the post. A coupling agent, that is usually called “silane”, is used to link
the fibers to the epoxy resin matrix. It is usually a mixture containg silane but not
only silane (with wetting agent, coupling amino agent for example). “Silane” is a
general word”. A silane is a chemical component with two extremities (at least), one
is really silane (OH) and the other is epoxy if the manufacturer wants to use it with
epoxy resin. But this extremity can be methacrylate when the resin matrix is
methacrylate. Definitely the “silane” must be selected to be suitable with the resin
matrix. This “silanisation” is made by the manufacturer at a temperature of 160-
180°C. There’s first a heat treatment and then a chemical treatment to fix coupling
agent (like silane). Manufacturers do not give much details but the first treatment is
a physical treatment to enhance the power of the silanisation.
The epoxy resin matrix is injected into the pre-tensioned fiber bundle. The original
Composipost was not radio-opaque; the radio-opacity was obtained in the second
generation of these posts (Composipost Radio-opaque, RTD) by the injection of a
high-molecular weight element powder into the un-polymerized post structure.
Many different types of carbon, quartz, silica-zirconium and glass fibers are now
available in the market: carbon was the first material used for manufacturing fiber
posts. These posts represented the first true alternative to cast post and cores, and to
pre-fabricated metal posts.
The following chart shows the mechanical properties of these kinds of posts. COMPOSIPOST No radiopaque TENSILE STRENGTH* 2900 MPa TENSILE MODULUS OF ELASTICITY* AT 30° 17-18 GPa FLEXURAL STRENGTH** 1900 MPa FLEXURAL MODULUS OF ELASTICITY** 135 GPa INTERLAMINATE SHEAR STRENGTH** 65-95 MPa * values determined by calculations. ** values determined by testing raw material
18

The use of glass and quartz fibers was initially proposed as an alternative to the dark
colour of carbon posts. Even though a ceramo-metal crown, and often even a full
ceramic crown is able to mask the dark colour of the post underlying the restoration
(Vichi et al., 2000), “esthetic” posts eventually gained popularity (Ferrari et al.,
2001). Moreover, during the preparation of the abutment (when a carbon fiber post
was selected), a dark powder was spread all around the mouth of the patients, who
sometimes complained because of this fact. As far as esthetics is concerned, several
brands of translucent glass fiber posts are available. They are better accepted than
carbon fiber posts, especially for anterior roots that provide support to all-ceramic
coronal restorations. The mechanical behaviours of these newer generations of posts
do not seem to differ from the first generation of fiber posts (Mannocci et al., 1999;
Grandini et al., 2004). By further adding a component usually in the resin matrix,
radiopaque posts can be obtained. Finally, translucent fiber posts are now available
to be used in combination with a dual curing resin cement and to take advantage of
light passing through the post for polymerization.
2.4 Metal posts versus fiber posts
The technique for the preparation of cast post and cores requires the clinician to
prepare the dowel space in order to finally have a length equal to two thirds of the
root, a width equal to one third of the root and 3-4 mm of root canal filling left at the
apex of the root (Shillimburg et al., 1982). In the last decades many opinion leaders
stressed the fact that a well-performed cast post and core could work for years
(Shillimburg et al., 1982). However, this kind of restoration has a failure rate
ranging from 6 to 10% in the literature (Morgano et al., 1993, Sorensen et al., 1984,
Torbjoner et al., 1995). Failure rate can even be worse as far as pre-fabricated metal
posts are analyzed (Tjan et al., 1985, Fuss et al., 1999). It was previously thought
that in order to achieve success with post-retained restorations, the post had to be as
strong, as long and as stiff as possible (Shillimburg et al., 1982, Sorensen et al.,
1984, Morgano et al., 1993, Torbjoner et al., 1995). However, metal posts can only
be successful if they do not overpass the elastic limit of the dentin (Desort et al.,
1983, Leary et al., 1987). As “…retention often requires the removal of tooth
structure…it is a procedure that may reduce the strength of the root…when placing a
19

post, the dentist must evaluate each tooth individually to determine the best
approach to obtaining the maximal fracture resistance…” (Stockton, 1999). In a
study comparing cast post and cores and carbon fiber posts, 200 patients were
examined. The failure rate for cast post and cores (Group 1, high modulus
restorations in terms of modulus of elasticity) and fiber posts (Group 2, low modulus
restorations) was totally different. Group 1 had 84% clinical success, 2% excluded
for non-compliance, and 9% root fracture (no need to inderline), 2% dislodgement
of crown, 3% endodontic failures. Conversely Group 2 had 95% clinical success,
3% excluded for non-compliance, 2% endodontic failures. The difference between
the two groups was highly statistically significant (Ferrari et al., 2000). For this
reason, clinical acceptance of fiber posts is now higher than it was before. The
advantage of having no root fracture is very important. Failure can occur as a
“debonding” of the post, especially at the time of removing the temporary
restoration, but this failure can easily be dealt with by repeating the adhesive
procedures. When fiber posts and a core and metal posts and a core were compared,
it became more and more obvious that the first ones functioned more satisfactorily.
As far as the mechanism of failure is concerned, metallic posts on failure tend to
produce an irreversible root fracture. Conversely, in the presence of a fiber post, root
fracture that occurs is usually located more coronally and is more easily retreatable
(Reagan et al., 1999, Ukon et al., 2000, Cornier et al., 2001). This type of failure
may be due to the wider amount of tooth structure must be sacrificed when a
metallic post is placed (Stankiewicz et al., 2002). Two recent papers underlined the
concept mentioned above: even if a crown is made, when a failure occurs, favorable
fractures are seen in teeth restored with fiber posts and resin cores, whereas
unfavorable fractures or failures are usually encountered with the use of a metal
post, or a fiber post of bad quality (Heydecke et al., 2002, Akkayan et al., 2002).
2.5 Role of the final restoration design (ferrule effect)
It is known that post luting in a way brings to the transportation of stresses in the
root canal and eventually to vertical root fractures (Guzy and Nicholls 1979).
Coronal coverage has always been considered a very important factor for preventing
root fractures in endodontically treated teeth (Frank 1959). Many years ago it was
20

suggested (Rosen 1961) that a sub-gingival collar might provide an extra-coronal
bracing able to prevent fractures of the root. The term “ferrule effect” was used for
the first time in 1987 by Eissman and Radke and it indicates a 360-degree ring of
cast metal that embraces the tooth.
A ferrule is defined as a metal ring or cap used to strengthen the end of a stick or
tube (Glossary of Prosthodontic terms). The effect of a metal collar on stress
distribution with cast post and cores was studied by using three-dimensional
photoelastic models of maxillary canine teeth of average dimensions. Standardized
parallel post and cores cemented into the models were used, with half of the samples
incorporating a 1.5 mm metal collar, and a 400 gm load was applied to the cingulum
of the cores. Stresses were then calculated and, on a point by point basis, a better
distribution was found in the collared specimens (Loney et al 1990). Another
simulation study was designed to compare the effect of different corono-radicular
reconstruction methods on stress transmission to dental tissues. Whatever the type of
stress (tensile or compressive), the greatest stress was observed in the cervical
region, regardless of the model. The absence of a cervical ferrule was found to be a
determining negative factor, giving rise to considerably higher stress levels.
Nevertheless, the peripheral ferrule seemed to cancel the mechanical effect of the
reconstruction material on the intensity of the stresses. Moreover, when a ferrule
effect was achieved, the choice of reconstruction material had no impact on the level
of cervical stress (Pierrisnard et al 2002). In another in vitro study it was
demonstrated that increasing the ferrule length of the endodontically treated teeth
from 1 mm to 1.5 mm in specimens restored with quartz-fiber and glass-fiber dowels
did not produce significant increases in the failure loads. No significant difference
was detected between glass-fiber and glass-fiber plus zirconia dowels with 1.5-mm
and 2.0-mm ferrules. However, fracture thresholds were higher for all 4 dowel
systems tested in the study when the specimens were prepared with a 2.0-mm ferrule
length (P<.001) (Akkayan 2004). Also among clinicians the ferrule effect was
perceived as an important factor; responses to a questionnaire sent to 1000 dentists
in Switzerland showed that most of the answering dentists strove to stabilize the
remaining tooth structure by circular enclosure of the tooth structure by the later
crown (ferrule effect) (Tinner et al 2001). In a recent literature review Stankiewicz
21

underlined that a ferrule effect occurs owing to the artificial crown bracing against
the dentine extending coronal to the crown margin. Overall, the author concluded
that a ferrule is desirable, but should not be provided at the expense of the remaining
tooth/root structure. (Stankiewicz et al 2002). Another important factor is the height
of the remaining tooth structure between the core and the crown margin: this is a
much more significant factor in determining the fracture resistance of teeth (Hunter
et al 1991). For this reason the crown lengthening surgical procedure has been taken
into account to obtain a consistent height of the remaining tooth structure and
eventually a desirable ferrule effect (Gegauff 2000).
In conclusion, a ferrule effect is desirable when restoring compromised
endodontically treated teeth. Crown lengthening can be considered as one of the
therapeutic options, and a positive crown/root ratio is an important factor for
predicting success of the treatment.
22
References
Akkayan B, Gulmez T. Resistance to fracture of endodontically treated teeth
restored with different post systems. J Prosthet Dent 2002; 87: 431-437.
Akkayan B. An in vitro study evaluating the effect of ferrule length on fracture
resistance of endodontically treated teeth restored with fiber-reinforced and zirconia dowel
systems. J Prosthet Dent. 2004 Aug;92(2):155-62.
Bradley JS, Hastings GW, Johnson-Nurse C. Carbon fibre reinforced epoxy as a
high strength, low modulus material for internal fixation plates. Biomaterials 1980;1, 38-40.
Cornier CJ, Burns DR, Moon P. In vitro comparison of the fracture resistance and
failure mode of fiber, ceramic and conventional post systems at variuos stages of restorations.
J Prosthodont 2001; 10: 26-36.
Desort KD. The prosthodontic use of endodontically treated teeth: theory and
biomechanics of post preparation. J Prosthet Dent 1983;49:203-6.
Duret B, Reynaud M, Duret F (1990 a) Un noveau concept de reconstitution
coronoradiculaire: le Composipost 1°. Le Chir Dent de France 540:131-41.
Duret B, Reynaud M, Duret F (1990 b) Un noveau concept de reconstitution
coronoradiculaire: le Composipost 2°. Le Chir Dent de France 542: 69-77.
Duret B, Reynaud M, Duret F (1992) Intérêt des materiaux á structure
unidirectionnelle dans les reconstitutions corono-radiculaires. Journal de Biomateriaux
Dentaires 7:45-57.
Eissman HF, Radke RA. Postendodontic restoration. In Cohen S, Burns RC, editors.
Pathways of the pulp 4th ed. St Louis CV Mosby 1987:640-43.
Ferrari M, Vichi A, Garcia Godoy F. A retrospective study of fiber-reinforced
epoxy resin posts vs. cast post and cores: a four year recall. Am J Dent 2000;13:9B-14B.
Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy of a self-curing adesive-resin
cement system on luting glass-fiber posts into root canals: an SEM investigation. Int J
Prosthod 2001;14:543-9.
Frank AL. Protective coverage of pulpless teeth. J Am Dent Assoc 1959;59: 895-
900.
Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted
endodontically treated teeth. Int Endod J 1999;32: 283-86.
Gegauff AG. Effect of crown lengthening and ferrule placement on static load
failure of cemented cast post-cores and crowns. J Prosthet Dent. 2000 Aug;84(2):169-79.
23
Grandini S, Goracci C, Monticelli F, Tay FR, Ferrari M. Fatigue resistance and
structural characteristics of fiber posts: three-point bending test and SEM evaluation. Dent
Mat 2004, in press.
Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth
with and without endo-post reinforcement. J Prosthet Dent 1979;42: 39-44.
Heydecke G, Butz F, Hussein A, Strub JR. Fracture strength after dynamic loading
of endodontically treated teeth restored with different post-and-core systems. J Prosthet Dent
2002; 87: 438-445.
Hunter AJ, Hunter AR. The treatment of endodontically treated teeth. Curr Opin
Dent. 1991 Apr;1(2):199-205.
Leary JM, Aquilino SA, Svare CW. An evaluation of post length within the elastic
limits of dentin. J Prosthet Dent 1987;57:277-81.
Loney RW, Kotowicz WE, McDowell GC. Three-dimensional photoelastic stress
analysis of the ferrule effect in cast post and cores. J Prosthet Dent. 1990 May;63(5):506-12.
Mannocci F, Ferrari M, Watson TF. Intermittent loading of teeth restored using
quartz fiber, carbon-quartz fiber, and zirconium dioxide ceramic root canal posts. J Adhes
Dent. 1999;1:153-8.
Morgano SM, Milot P. Clinical success of cast metal post and cores. J Prosthet Dent
1993; 70:11-6.
Pierrisnard L, Bohin F, Renault P, Barquins M. Corono-radicular reconstruction of
pulpless teeth: a mechanical study using finite element analysis. J Prosthet Dent 2002
Oct;88(4):442-8.
Reagan SE, Fruits TJ, Van Brunt CL, Ward CK. Effects of cycling loading on
selected post-and-core systems. Quintessence Int 1999; 30: 61-67.
Rosen H. Operative procedures in mutilated endodontically treated teeth. J Prosthet
Dent 1961;11: 973-86.
Schillimburg HT, Kessler JC. Restoration of endodontically treated teeth.
Quintessence Publishing Co Inc Chicago 1982.
Schreiber CK. Polymethylmetacrilate reinforced with carbon fibres. Br Dent J 1971;130: 29-
30.
Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a
study of endodontically treated teeth. J Prosthet Dent 1984;51: 780-84.
Stankiewicz NR, Wilson PR. The ferrule effect: a literature review. Int J Endod
2002; 35: 575-581.
24
Stockton LW. Factors affecting retention of post systems: A literature review. J
Prosthet Dent 1999; 81: 380-5.
Tinner D, Marinello C, Kerschbaum T. The preprosthetic preparation of the
endodontically treated abutment tooth. Post and core technique: a questionnaire analysis.
Schweiz Monatsschr Zahnmed 2001;111(4):402-9.
Tjan AHL, Whang S. Resistance to root fracture of dowel channels with various
thicknesses of buccal dentin walls. J Prosthet Dent 1985; 53: 496-500.
Torbjöner A, Karlsson S, Odman PA. Survival rate and failure characteristics for
two post designs. J Prosthet Dent 1995;73: 439-44.
Ukon S, Moroi H, Okimoto K. Influence of different elastic moduli of dowel and
core on stress distribution in root. Dent Mater 2000; 19: 50-64.
Vichi A. A study into application of fiber technology into fiber posts. PhD thesis,
Amsterdam 2002.
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on the
masking of various types of opaque posts. J Prosthet Dent 2000; 83: 412-7.
25

Chapter 3 Preparation of root canal dentin to bonding
Success in endodontic treatment is a key factor to allow success in the restoration of
root canal treated teeth. A well performed endodontic treatment is based on the
removal of debris and organic material inside the root canal (Castellucci 1993) and
on the mechanical preparation of the canal itself to receive an obturation material
(Ingle 1993). The importance of apical seal has been already underlined in the
literature (Walton et al 1996). More recently coronal seal has acquired the same
importance, and many authors concluded that exposure to the oral cavity of a well
performed endodontic treatment (not preventing from coronal leakage) inevitably
brings to a re-infection and in conclusion to a failure (Madison et al 1987 and 1988,
Swanson et al 1987). In 1985 Saunders evaluated the long-term coronal leakage in
root fillings achieved by 2 gutta-percha techniques using 2 calcium hydroxide-
containing sealers. Coronal leakage was then determined with an India ink tracer
and a clearing technique. The extent of coronal leakage was measured with a
magnification device and the authors concluded that all the techniques analyzed
were subjected to extended leakage (Saunders et al 1985). In another study three
common sealers were evaluated for coronal leakage using an animal model in vivo.
After 45 days exposure to the oral cavity, none of the sealers was capable of
preventing leakage and coronal dye penetration (Kopper et al 2003).
The detrimental effect of eugenol on adhesion of resinous cements has been taken
into consideration (Tjan et al 1992, Schwartz et al 1998). Resin composites
polymerise by the addition of free radicals; this process may be inhibited by
phenolic compounds, such as eugenol (2-methoxy-4-allyphenol) that is contained in
the vast majority of endodontic sealers and temporary filling materials, and can
penetrate into the root canal walls (Kielbassa et al 1997). The contact of eugenol
with the dentinal walls significantly altered the dentin penetration of dentin bonding
system (Mayer et al 1997). For these reasons the persistence of eugenol into the root
canal walls has been advocated as a cause of some inconsistent results of posts
cemented with adhesive resins. Unfortunately, the results of the studies about post
retention are not reliable because they were performed on root canals that were
different in shape and sizes. As a consequence it is not possible to establish whether
26

the force needed to remove the post was the result of adhesion of the cement to root
dentin or of the different degree of adaptation of the post to the varying
morphologies of the root canals of the teeth used. The adhesive strength of resin
composites to tooth structure may be simply influenced by the cleanliness of tooth
surface; in two recent investigations (Watanabe et al 1997) on temporary cement
remnants as adhesion inhibiting factors in the interface between resin cements and
bovine dentin, the temporary cement application significantly decreased the tensile
bond strength of all adhesive systems employed. The contamination with various
agents of enamel and dentin surface lowered the bond strength of resin composite
restorations performed with different bonding agents (Xie et al 1993). Both eugenol
containing and eugenol free temporary cements decreased the tensile bond strength
of resin luting cements to bovine teeth (Terata 1993). No difference was reported in
leakage of resin luted inlays when the cavity preparations were treated with either
eugenol-containing or eugenol-free temporary cements (Woody et al 1992).
Definitely, as the effect of eugenol is generally limited to superficial dentin, and as a
certain removal of tooth structure always happens during preparation for post
placement, it is likely to happen that the eventually inhibited layer is removed, and a
lack of adhesion can be explained differently. The preparation for post placement
can be performed in two ways: with hot pluggers and with burs (Ferrari et al 2003).
Burs are usually preferred as they are faster and allow a higher removal of debris,
leaving a cleaner dowel space where adhesive luting can be performed. Recently
Serafino evaluated the cleanness of root dentin walls after mechanical preparation
and etching procedure. All the tested procedures showed a clean walls’ surface.
Pieces of guttapercha remained along the canal walls where the drill shape did not
follow the root canal shape. Endodontic cement and small amount of guttapercha
were noted closing dentinal tubules in some areas of the root walls (Serafino et al
2004). It is obvious then that high accuracy has to be put when preparing the dowel
space, and that a rotating brush could improve the cleanness of the post space. But
the starting point is always that the endodontic procedure has to be well performed if
we look for success in restoring root canal treated teeth. The following SEM study
regards different irrigating regimes used during endodontic treatment to achieve a
clean root canal before guttapercha condensation procedures.
27

3.1 Evaluation of Glyde File Prep in combination with sodium hypochlorite as
root canal irrigant: a scanning electron microscopic study.
It is well known that the irrigation of the root canal plays a critic role in the
determination of success in the endodontic therapy (Walton et al 1996). Several
studies demonstrated that the quantity of debris found after the instrumentation is
higher in canals prepared without irrigating solutions than in cases where irrigating
solutions have been used (Goldman et al, 1981). Even in canals where a proper
preparation had been performed, Davids et al (1972) experimentally demonstrated
that there were not instrumented areas where organic and inorganic debris could be
found. On the other hand dentin instrumentation always causes the formation of a
thin smear layer which recovers the whole surface of the root canal. Ostby (1957)
was the first one to use EDTA as an irrigating solution, with a chelating action, to
remove the inorganic component. With the same purpose solutions of sodium
hypochlorite have been later proposed, varying the concentration from 2% to 5%
(Mc Comb et al 1975, Brannstrom et al 1974, Pashley et al 1981). So far EDTA was
considered the best irrigating for removing the inorganic component of the smear-
layer and, in association with sodium hypochlorite, showed the best results
(Goldman et al 1984, Aktener et al 1993).
Different morphological observations can be performed to evaluate smear layer and
remained debris after endodontic instrumentation and irrigation of the root canal
(Peters et al 2000). Barbakov et al (1998) proposed a quantitative evaluation of
smear layer and debris presence along root canal walls, based on serial
photomicrographs placed next to each other, forming a continuous horizontal
examination strip at three levels (2-, 6-, 10-mm from the apex) of the canal walls.
Recently a new chelating agent (Glyde File Prep, Dentsply-Maillefer, Ballaigues,
Switzerland) containing EDTA has been proposed.
The aim of the present study was to evaluate 1. the smear layer, debris and tubule
orifices of root canal walls after being instrumented and irrigated by Glyde File Prep
and 2. the null hypothesis that different irrigating techniques can not determine any
difference on amount of debris along root canal walls.
28

3.2 Materials and Methods
Forty mandibular anterior teeth (incisors and canines), stored in 0.1% thymol, were
randomly selected for this study from the department’s stock of extracted teeth.
Canal morphology was verified from radiographs (70 kV and 0.08 s) taken both
buccolingually and mesiodistally (Kodak, USA). The crowns were resected to
ensure good visibility of the canal and optimal access.
Final working lengths were set by deducting 1 mm from lengths recorded when tips
of size 10 or 15 K-files (Dentsply-Maillefer, Ballaigues, Switzerland) were visible at
the apical foramina. All working lengths were confirmed radiographically. The
coronal 3 to 4 mm of the canals were prepared with Gates-Glidden burs (sizes 2
through 4). The teeth of all groups were shaped with Ni-Ti (Profile 0.4-0.6 –
Maillefer) instruments. The instrumentation was performed exactly according to the
manufacturer’s instructions. ProFile (PF, Dentsply-Maillefer) instruments were used
in a modified crown-down approach after using Gates-Glidden burs and the step-
down technique. The coronal two-thirds were enlarged using PF sizes 5, 4 and 3,
sequentially. The size 2 instrument was used in most canals, but the size 1 PF was
not used at all. Apical preparations were then completed using nos. 3, 4, 5 and 6 PF
instruments. Finally, canals were stepped-back using PF instruments nos. 7, 8 and 9.
Each set of PF instruments was discarded after preparing 10 canals.
The specimens were randomly assigned to four equal groups of 10 each (Table 1).
Table1: Type of irrigant used in the different groups Group Irrigant
Group A Physiological solution
Group B NaOCl 2.5%
Group C NaOCl 2.5% and GFP
Group D NaOCl 2.5% and GFP (PP)
Legends: NaOCL= Sodium Hypochlorite, GFP= Glyde File Prep, PP= Paper points
All canals were flushed with 10 ml of the test irrigant using disposable syringes and
27-gauge needles. The total time of irrigation has been 30 minutes per canal. Group
A was irrigated with physiological solution; Group B with sodium hypochlorite
2.5%; Group C with sodium hypochlorite 2.5% and Glyde File Prep alternately.
Group D was irrigated with sodium hypochlorite 2.5% during the preparation, the
29

root canals were then dried and Glyde File Prep applied with sterile paper points
(Mynol) and left for five minutes. At the end a further irrigation with sodium
hypochlorite 2.5% was performed. It must be noticed that in Group C Glyde File
Prep has been used following manufacturer’s instructions, while in Group D a
modified technique has been performed. In Group C Glyde File Prep was used
alternating it as irrigant with sodium hypochlorite during the preparation. In Group
D, instead, only sodium hypochlorite was used during the preparation, and after that
Glyde File Prep was applied with a paper point and left for five minutes. At the end
a further irrigation with sodium hypochlorite was performed.
After preparing the canals, the teeth were sectioned along their buccal and lingual
surfaces, using a low speed diamond saw (Isomet, Buhler, Lake Bluff, NY, USA).
The root halves were coded and examined in a stereomicroscope (Nikon, Germany).
The coded, halved specimens were then dried, mounted on metallic stubs, gold-
sputtered (Balzers CSD 030, Balzers, Liechtenstein), and evaluated using a scanning
electron microscope (SEM) at low (x10 and x 15) and higher (x200 and x500)
magnifications (Philips, 515, Amsterdam, The Netherlands) at the apical, middle and
coronal levels. Serial SEM photomicrographs at x500 original magnification were
taken of the canal walls at the 2-, 6-, and 10-mm levels. The serial photomicrographs
were placed next to each other, forming a continuous horizontal examination strip at
three levels (Fig. 1). Irrespective of the number of photomicrographs needed to form
a complete strip, each strip was subdivided into eight “assessment units” (Barbakow
et al 1998).
The amounts of debris, smear layer and the visibility of open tubules were rated
using a 4-step scale method by the same person (M.F.) who was unaware of the
coding system to exclude observer bias. Evaluation was repeated twice for the first
20 specimens to ensure intraexaminer consistency. The amount of debris present at
x500 magnification was graded between 0 and 3 (Table 2a).
Table 2a : Debris scores Score 0 1 2 3
Description No debris Few debris particles,
with a diameter
< 20 microns
Many debris particles,
with a diameter
< 20 microns
Many debris particles,
with a diameter
> 20 microns
30

A debris score of 0 was assigned when no debris was present. A score of 1 was
assigned when few debris particles were present, whose largest diameter was less
than 20 microns. A score of 2 was recorded when large quantities of debris particles
were present, whose diameter was less than 20 microns. A score of 3 was assigned
when large amounts of debris particles were present, whose diameters were greater
than 20 microns in any direction. The amount of smear layer and the opening of the
dentinal tubules were graded between 0 and 3 (Table 2b).
Table 2b: Smear layer and dentinal tubules scores Score 0 1 2 3
Description Open dentinal tubules.
No smear layer nor
calcospherites
Some open dentinal
tubules. A thin
smear layer is
present
All dentinal tubules
covered by a thin
smear layer
All dentinal tubules
closed by a thick
smear layer
A score of 0 was assigned when all dentinal tubules were open and no smear layer
was present or not instrumented calcospherites were noted. A score of 1 was
recorded when some dentinal tubules were open and a thin smear layer covered the
openings of the cut dentinal tubules. A score of 2 was recorded when all dentinal
tubules were covered by a thin smear layer. A score of 3 was assigned when all the
dentinal tubules were closed by a thick smear layer.
Mean debris, smear layer and open tubules scores were calculated for Groups A, B,
C and D and statistically evaluated using the Kruskal-Wallis and Mann-Whitney U
tests at p 0.001 level.
3.3 Results
The mean amounts of debris, smear layer and open tubules found at the 2-, 6- and
10-mm levels in the test groups are listed in Tables 3 and 4 respectively.
To indicate the distribution of the individual scores, medians are recorded for the
debris, smear layer and open tubules in Tables 3 and 4 respectively.
Mean debris scores for Group A and B were significantly higher than those found in
Groups C and D. Lower debris scores were recorded in Groups C and D, in those
Groups in which Glyde File Prep was used (Table 3).
31
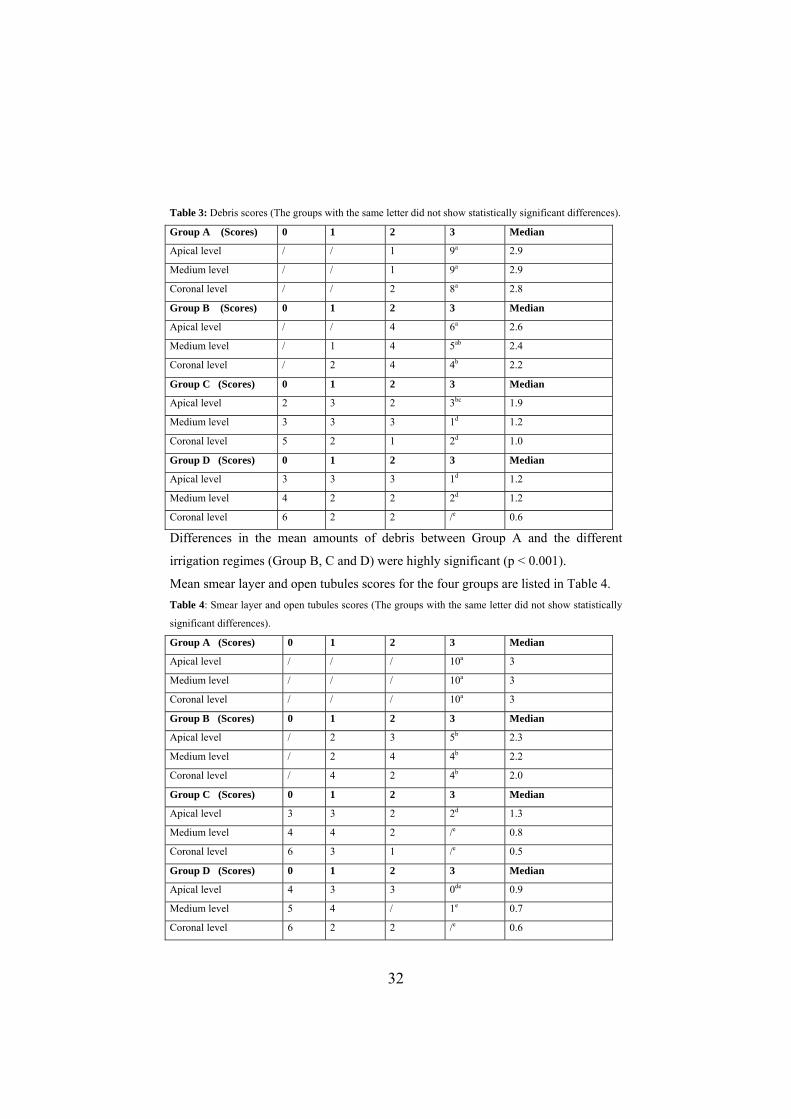
Table 3: Debris scores (The groups with the same letter did not show statistically significant differences).
Group A (Scores) 0 1 2 3 Median
Apical level / / 1 9a 2.9
Medium level / / 1 9a 2.9
Coronal level / / 2 8a 2.8
Group B (Scores) 0 1 2 3 Median
Apical level / / 4 6a 2.6
Medium level / 1 4 5ab 2.4
Coronal level / 2 4 4b 2.2
Group C (Scores) 0 1 2 3 Median
Apical level 2 3 2 3bc 1.9
Medium level 3 3 3 1d 1.2
Coronal level 5 2 1 2d 1.0
Group D (Scores) 0 1 2 3 Median
Apical level 3 3 3 1d 1.2
Medium level 4 2 2 2d 1.2
Coronal level 6 2 2 /e 0.6
Differences in the mean amounts of debris between Group A and the different
irrigation regimes (Group B, C and D) were highly significant (p < 0.001).
Mean smear layer and open tubules scores for the four groups are listed in Table 4. Table 4: Smear layer and open tubules scores (The groups with the same letter did not show statistically
significant differences).
Group A (Scores) 0 1 2 3 Median
Apical level / / / 10a 3
Medium level / / / 10a 3
Coronal level / / / 10a 3
Group B (Scores) 0 1 2 3 Median
Apical level / 2 3 5b 2.3
Medium level / 2 4 4b 2.2
Coronal level / 4 2 4b 2.0
Group C (Scores) 0 1 2 3 Median
Apical level 3 3 2 2d 1.3
Medium level 4 4 2 /e 0.8
Coronal level 6 3 1 /e 0.5
Group D (Scores) 0 1 2 3 Median
Apical level 4 3 3 0de 0.9
Medium level 5 4 / 1e 0.7
Coronal level 6 2 2 /e 0.6
32

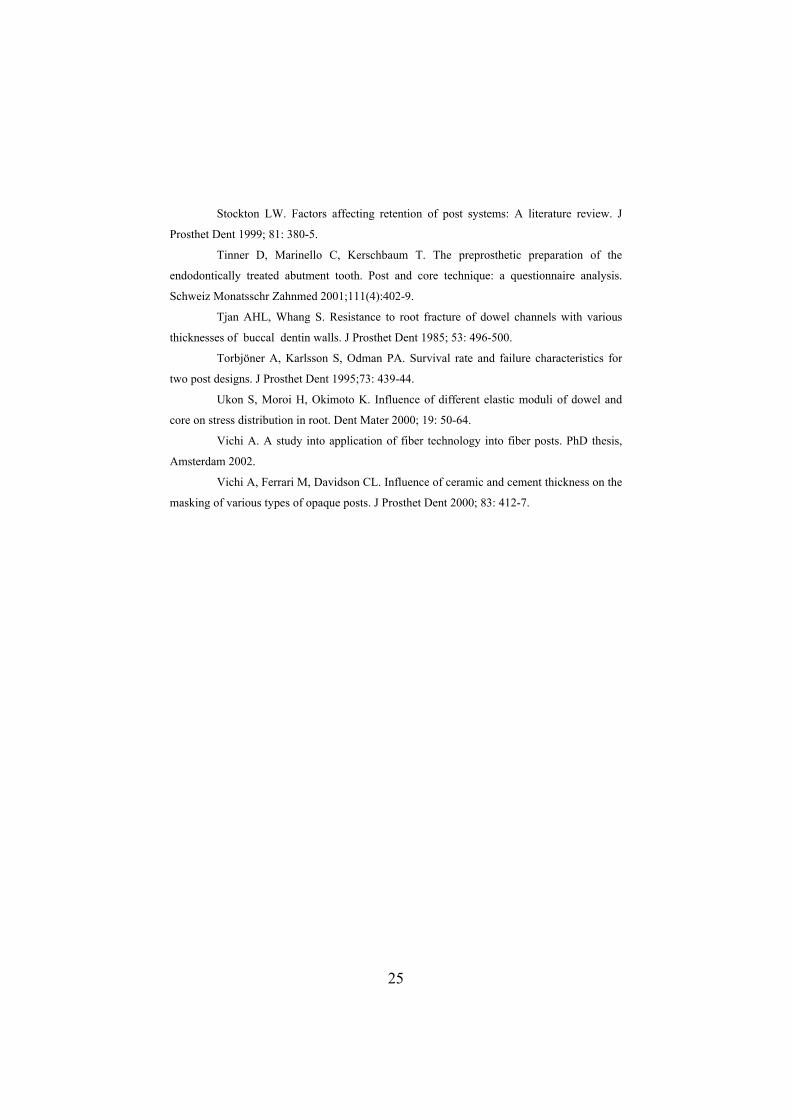
A high amount of smear layer and no visibility of tubules on the prepared canal
walls were found when physiological solution was used as the only irrigant (Group
A). Mean amounts of smear layer scores in Group A reached the maximum score of
3. When sodium hypochlorite 2.5% was used (Group B) as irrigant, the samples
showed less smear layer and more open tubules compared with Group A samples.
When Glyde File Prep was used, in both tested techniques, the lowest scores were
noted, and Group C and D had significantly less smear layer and more open tubules
on the canal walls at the apical, mid-third and coronal levels, respectively, compared
with Group A and B samples. Although there is not a statistically significant
difference between Group C and D, Group D showed better scores than Group C.
3.4 Discussion
Smear layer is produced every time a canal is instrumented. The smear layer,
which is mainly inorganic, is also made up by a slight organic component (proteinic
agglomerates, vital or non-vital pulp tissue, odontoblastic processes, bacteria and
blood cells) (2,5). The thickness and composition of smear layer can vary depending
on the kind of dentin and the instruments used (Mader et al 1984, Davis et al 1972,
Mc Comb et al 1975). The smear layer can be organized in two layers: superficial
smear-layer, made up by a 1-2 microns layer above the intertubular dentin, adhering
on it and becoming indistinguishable from it, and smear-plugs within dentinal
tubules, deepening for about 2-40 microns with a fingerlike or small-tube segments
aspect (Mader et al 1984).
There is a rich but conflicting scientific data regarding the choice between
removing or leaving the smear-layer from the dentinal wall. Some authors reported
that the smear layer remaining on the canal walls should have two positive effects:
to reduce the dentin permeability (about 40%) and to block the way through the
tubules for bacteria and endotoxins in a mechanical way (13,14). Other authors
emphasize the need of creating smear free canalar surfaces. Brannstrom e Nyborg
(1974) demonstrated that the smear-layer can give shelter to anaerobic
microorganisms, thus creating a chronic focus of irritating substances. In 1982
Akpata and Blechman (1982) confirmed the smear layer permeability to
streptococcus. Moreover Williams and Goldman (1985) demonstrated that the
33

smear-layer can slow, but not block the way of microorganisms through the dentinal
tubules. In 1993 Nissan et al. (1993) noticed that bacterial products, such as
polysaccharidic endotoxin, can easily permeate human dentin, even when smear-
layer was present. Besides it is known that the smear-layer negatively affects the
adaptation of the materials used to fill the canal, and reduces the diffusion through
the tubules, and as a consequence the efficacy, of many intracanalar medicaments.
Nevertheless smear-layer has the potential to harbor microorganisms: the choice of
eliminating the smear-layer is essentially derived from the need of sealing the open
dentinal tubules.(Behrend et al 1996, Goldman et al 1984).
Usually microscopic investigations are performed under laboratory conditions in
order to predict the clinical behavior of new irrigating solutions. Unfortunately,
SEM evaluation do not permit numeric data collection and consequently statistical
analysis. Only a few studies have reported on quantitative evaluation of
morphological observations of root canals (Peters et al 2000, barbakow et al 1998).
In this way, a repeatable method was introduced.
The results of this study confirm that the irrigation with sodium hypochlorite alone
is not able to totally remove the smear-layer, as its action is mainly directed to the
organic debris. In order to obtain the total removal of the smear-layer, both organic
and inorganic components, the combined use of sodium hypochlorite and EDTA is
recommended (Group C and D) (Aktener et al 1993, Dippel et al 1984). The
chelating agent somehow “prepares” the canal walls surfaces so that irrigants and
medicaments are really effective with their anti-bacterial action.
The role of EDTA during the instrumentation is mainly directed to the creation of
smear free canalar surfaces. Glyde File Prep contains EDTA. Because of its acidity,
no matter how EDTA is used as irrigant, it needs a last flush with hypochlorite in
order to neutralize its acid effect. The technique used for teeth in Group D probably
lets EDTA act in the deepest part of the canal, and this may explain why in the
apical portion the best results were obtained by this Group.
Other substances have been used to remove the smear-layer, such as 20%
polyacrylic acid, 10% citric acid, ortophosphoric and maleic acid (Goldman et al
1981, Wayman et al 1979, Takeda et al 1999). However this acid substances are
clinically not easy to handle, as the effect varies according to the kind of acid used,
34

the concentration and the time of application; besides the low pH (1,5) could have a
harmful effect on the periapical tissues (Takeda et al 1999, Garberoglio et al 1994).
As alternative to irrigant solutions, Laser (CO2 and Er:YAG) has also been
successfully proposed to remove the smear-layer; however further studies are
needed about the thermal effects before the clinical use of lasers can be
recommended (Takeda et al 1999).
In conclusion, none of the techniques used in this study showed a perfect removal of
smear layer and debris. The significantly lower debris and smear layer scores in
Group C and D is probably due to the better effect, as irrigant, of Glyde File Prep
combined with sodium hypochlorite 2.5%.
The null hypothesis tested in this study was not confirmed: differences in the
amount of debris along root canal walls after different irrigation regimes were noted.
35
Fig. 1: Composite picture showing a horizontal examination strip at the coronal level of a
Group A sample.
Fig. 2: Tooth irrigated with physiological solution (Group A, apical portion) (x 500). An
amorphous layer with debris can be noted on the canal wall. No tubule openings are visible.
Fig. 3: Tooth irrigated with NaOCl (Group B, apical portion) (x 500). Smear layer can be
noted, with less amount of debris than in Fig. 2. No openings of dental tubule are visible.
36
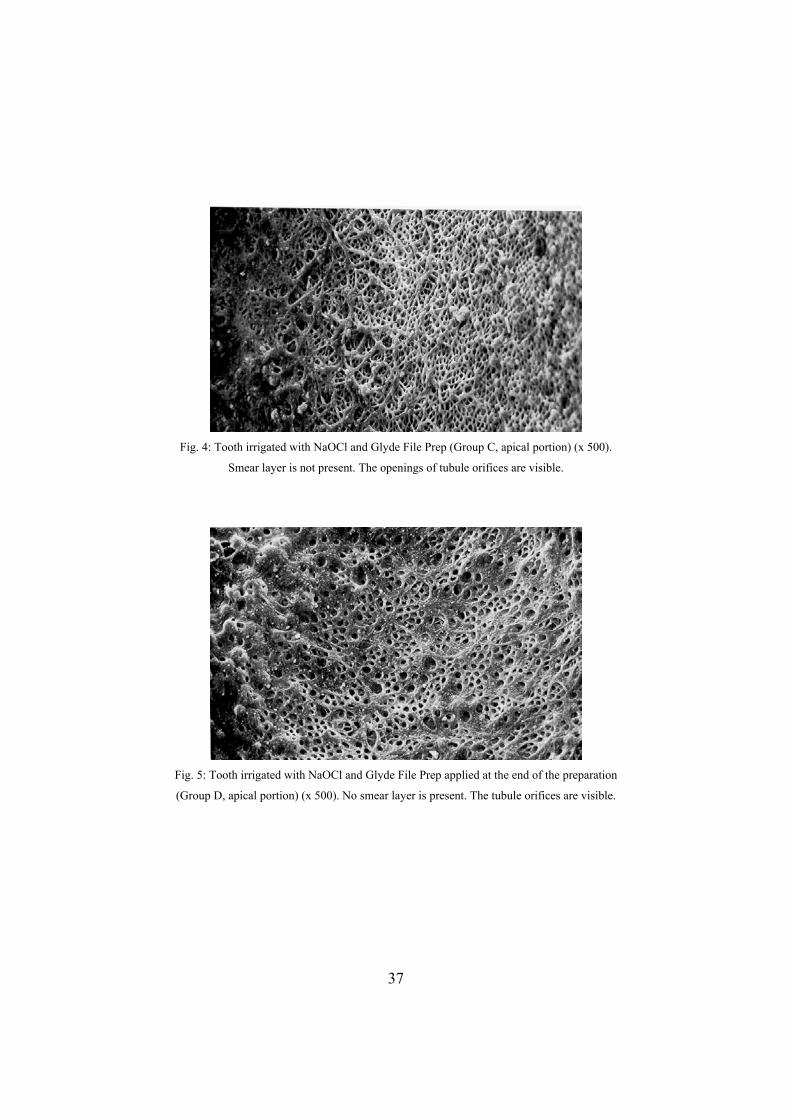
Fig. 4: Tooth irrigated with NaOCl and Glyde File Prep (Group C, apical portion) (x 500).
Smear layer is not present. The openings of tubule orifices are visible.
Fig. 5: Tooth irrigated with NaOCl and Glyde File Prep applied at the end of the preparation
(Group D, apical portion) (x 500). No smear layer is present. The tubule orifices are visible.
37
References
Akpata ES, Blechman H. Bacterial invasion of pulpar dentin wall in vitro. J Dent
Res 1982; 61: 435-8.
Aktener BO, Bikay U. Smear layer removal with different concentrations of EDTA
mixtures. J Endod 1993; 19: 228-31.
Barbakov F, Peters O, Havranek L. Effects of Nd:YAG lasers on root canal walls: a
light and scanning electron microscopic study. Quint Int 1998: 837-45.
Behrend GD, Cutler CW, Gutmann JL. An in-vitro study of smear layer removal
and microbial leakage along root canal fillings. Int End J 1996; 29(2): 99-107.
Brannstrom M, Nyborg H. Bacterial growth and pulpar changes under inlays
cemented with zinc phosphate and epoxylate CBA 9080. J Prosth Dent 1974; 31: 556-65.
Castellucci A. Endodontics, Ed Martina, Milano, 1993.
Davis SR, Brayton SM, Goldman M. The morphology of the prepared root canal: a
study utilizing injectable silicone. Oral Surg 1972; 34: 642-8.
Dippel H, Borggreven J, Hoppenbrouvers PMM. Morphology and permeability of
the dentin smear layer. J Prosthet Dent 1984; 52: 657-62.
Ferrari M, Scotti R. Fiber posts: clinical and research aspects. Masson Ed, Milano
2002.
Garberoglio R, Becce C. Smear layer removal by root canal irrigants. Oral Surg
Oral Med Oral Pathol 1994; 78: 358-66.
Goldman M, Devitre R, Pier M. Effect of the dentin smeared layer on tensile
strength of cemented post. J Prosthet Dent 1984; 52: 485-8.
Goldman M, Goldman LB, Kronman JH, Lin PS. The efficacy of several irrigating
solutions for endodontics: a scanning electron microscopic study. Oral Surg 1981; 52: 197-
204.
Ingle JA. Endodonzia. Piccin Editore, 1993, Padova, Italy 29-40.
Kielbassa AM, Attin T, Hellwigg E. Diffusion behaviour of eugenol from zinc
oxide eugenol mixtures through human and bovine dentin in vitro. Oper Dent 1997;22: 15-20.
Kopper PM, Figueiredo JA, Della Bona A, Vanni JR, Bier CA, Bopp S.
Comparative in vivo analysis of the sealing ability of three endodontic sealers in post-
prepared root canals. Int Endod J 2003 Dec;36(12):857-63.
Madison S, Wilcox LR. An evaluation of coronal microleakage in endodontically
treated teeth. Part III. In vivo study. J Endod. 1988 Sep;14(9):455-8.
Madison S, Swanson K, Chiles SA.An evaluation of coronal microleakage in
endodontically treated teeth. Part II. Sealer types. J Endod. 1987 Mar;13(3):109-12.
38
Mader LL, Baumgarter JC, Peters DD. A scanning electron microscopic
investigation of the smear layer on root canal walls. J Endod 1984; 10: 477-83.
Mayer T, Pioch T, Duschner H, Stahele HJ. Dentinal adhesion and histomorphology
of two dentinal bonding agents under the influence of eugenol. Quintess Int 1997;28: 57-62.
Mc Comb D, Smith DC. A preliminary scanning electron microscope study of root
canals after endodontic procedures. J Endod 1975; 1: 238-42.
Nissan R, Sehal H, Pashley DH, Trowbridge H. Ability of bacterial endotoxin to
permeate human dentin. J Dent Res 1993; 92: 127.
Otsby BN. Chelation in root canal therapy. EDTA for cleaning and widening of root
canals. Odontal. Tidskz. 1957; 65: 3-11.
Pashley DH, Michelich V, Kehl T. Dentin permeability: effect of smear layer
removal. J Prosthet Dent 1981; 46: 531-7.
Peters O, Barbakov F. Effects of irrigation on debris and smear layer on canal walls
prepared by two rotary techniques: a scanning electron microscopic study. J Endod 2000; 1:
6-10.
Saunders EM, Saunders WP. Long-term coronal leakage of JS Quickfill root fillings
with Sealapex and Apexit sealers. Endod Dent Traumatol. 1995 Aug;11(4):181-5.
Schwartz RS, Murchison DF, Walker WA 3rd. Effects of eugenol and non eugenol
endodontic sealer cements on post retention. J Endod 1998;24:564-67.
Serafino C, Gallina G, Cumbo E, Ferrari M. Surface debris of canal walls after post
space preparation in endodontically treated teeth: a scanning electron microscopic study. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod. 2004 Mar;97(3):381-7.
Swanson K, Madison S.An evaluation of coronal microleakage in endodontically
treated teeth. Part I. Time periods. J Endod. 1987 Feb;13(2):56-9.
Takeda FH, Harashima T, Kimura Y, Matsumoto K. A comparative study of smear
layer by three endodontic irrigants and two types of laser. Int End J 1999; 32: 32-9.
Terata R. Characterization of enamel and dentin surfaces after removal of temporary
cement. Dent Mater J 1993:12:18-28.
Tjan AHL, Nemetz H. Effect of eugenol-containing endodontic sealer on the
retention of prefabricated posts luted with an adhesive composite luting cement. Quintessence
Int 1992;23:839-44.
Walton R, Torabinejad M. Principles and practice of endodontics, 2nd edition, W.B.
Saunders Co., 1996.
39

Watanabe EK, Yamashita A, Imai M, Suzuki K. Temporary cements remnants as an
adhesion inhibiting factor in the interface between resin cements and bovine dentin. Int J
Prosthodont 1997;10: 440-52.
Wayman BE, Kopp WM, Pinero GJ, Lazzari EP. Citric and lactic acids as root canal
irrigants in vitro. J Endod 1979; 5: 258-60.
Williams S, Goldman M. Penetrability of the smeared layer by strain of proteus
vulgaris. J Endod 1985; 11: 385-8.
Woody TL, Davis RD. The effect of eugenol-containing and eugenol free temporary
cements on microleakage in resin bonded restorations. Oper Dent 1992;17: 175-80.
Xie J, Powers JM, Mc Guckin RS. In vitro bond strength of two adhesives to
enamel and dentin under normal and contaminated conditions. Dent Mater 1993;9: 295-99.
40

Chapter 4 Criteria for selecting fiber posts
Actually many fiber posts are available on the market. Their huge success among
clinician brought many manufacturers to produce their own fiber post. For this
reason it is important for the clinician to know the properties of each fiber post
available on the market, and to consequently select the more appropriate.
Composition and shape of the post are usually the first criteria. Carbon, glass or
quartz fibers are available, and after the first double cylinder shape endodontic and
double tapered shape became available. Depending on the type of root canal and of
tooth the clinician can decide which one can be more appropriate. Also the
combination with an appropriate bonding system acquires high importance: it is
known that materials give better results if they are employed following
manufacturer’s instructions and if proprietary resin cement and adhesives are used
(Ferrari et al 2002). Also the cost can be a factor: some of the posts available on the
market are cheaper than others, but we have to keep in mind that a cost/benefit ratio
should be taken into account when deciding what kind of material we should employ
(Monticelli et al 2003). Probably the most important factor to take into account is
the experimental and clinical evaluation of the behaviour of fiber post/adhesive
material/resin cement/core material used (Monticelli et al 2003, Ferrari et al 2002,
Vichi et al 2001 and 2002). The following study regards a comparison among some
post actually available on the market when resistance to fatigue is considered.
4.1 Fatigue resistance and structural characteristics of fiber posts: three-point
bending test and SEM evaluation.
Over the recent years a rapid development has occurred in the area of fiber posts.
The introduction of carbon fiber posts in 1990 (Duret et al 1990) provided the dental
profession with the first true alternative to cast or prefabricated metal posts. The
elastic moduli of fiber posts are closer to dentin than that of any metal post
(Asmussen et al 1999), and their clinical trials yielded convincing results
(Fredriksson et al 1998, Ferrari et al 2000b, Ferrari et al 2000a, Malferrari et al
2002, Scotti et al 2002, Dallari et al 1998). However, the earlier generations of fiber
posts had some limitations to their universal use, as they were radiolucent and
41

difficult to mask under all-ceramic or composite restorations (Vichi et al 2000).
Later, radiopaque fiber posts, and more esthetic posts were made. These
improvements brought about a drastic change in the acceptance of fiber posts by the
dental profession. As a consequence of practitioners finding esthetic fiber posts a
viable alternative to metal posts (Drummond et al 1999), a number of different fiber
posts were quickly introduced into the market. Many studies are available on the
adhesion of fiber posts to root canal substrates (Nakabayashi et al 1998, Chappel et
al 1994, Mjor et al 1996), on the different luting procedures (Ferrari et al 2000c,
Vichi et al 2002) and the abutment build-up (Gateau et al 1999 ,Cohen et al 1996,
Freedman et al 2001), and all of them demonstrate the quality performances of fiber
posts (Dietschi et al 1996 and 1997). The rapid influx of these new esthetic fiber
posts has imposed the need for a systematic evaluation of their mechanical
properties and clinical performances. For that purpose, scanning electron
microscopy (SEM) and fatigue test can provide an indication of what type of post
would perform better under clinical conditions. Also, SEM observations can be
useful to assess the fiber/resin matrix ratio, as well as the fiber diameter and the
global integrity of the posts. Fatigue is considered as one of the main causes of
structural failure in restorative dentistry (Hsu et al 2002, Baran et al 2001, Fan et al
1995, Yamamoto et al 1995). It has been reported that dental restorations fail much
more frequently under cyclic loading that are well below the ultimate flexural
strength of these materials, than under application of a single, relatively high force
(Kahn et al 1996). Fatigue tests can reveal the resistance level of each type of post
under cyclic loading that simulates the normal occlusal and masticatory function
(Gateau et al 1999, Cohen et al 1997, Reagan et al 1999). Since fiber posts are in
essence composite materials, it seems logical to expect that their mechanical
properties would increase as a result of an increase in fiber content. The objectives
of the present study were to assess the fatigue resistance of different types of fiber
posts, and to verify the existence of a correlation between the fatigue resistance
exhibited by the different types of posts and their structural characteristics. The null
hypotheses tested were: 1. there is no difference in the structural characteristics and
in the fiber/resin ratio of the posts, 2. there is no difference in the fatigue resistance
among different kinds of fiber posts.
42

4.2 Materials and Methods
Eight types of esthetic posts were selected for this study (Table I). Table I.. This table shows the structural characteristics of the eight groups of tested posts
Group
number
Type of post Post
diameter
(mm)
Fiber
diameter
(µm)
Fiber
density
(number
of fibers
per mm2)
Surface
occupied by
fibers per
mm2 of post
surface (%)
Group 1 Easypost 1.6 12 29 34.8
Group 2 Para Post Fiber White 1.5 6 18 10.8
Group 3 FibreKor 1.5 18 28 50.4
Group 4 Ghimas White 1.8 12 30 36.0
Group 5 DT Light-post radiopaque 2.0 12 32 38.4
Group 6 FRC Postec 2.0 12 25 30.0
Group 7 Luscent Anchors 1.7 15 29 43.5
Group 8 Snowpost 1.6 7 36 25.2
They were Easypost (Krugg, Milano, Italy; Group 1, carbon fibers), Para Post Fiber
White (Coltene/Whaledent, Mawhaw, NJ, USA; Group 2, glass fibers), FibreKor
(Jeneric/Pentron, Wallingsford, CT, USA; Group 3, glass fibers), Ghimas White
(Ghimas, Casalecchio di Reno, Bologna, Italy: Group 4, glass fibers), DT Light-Post
radiopaque (RTD, Grenoble, France; Group 5, pre-tensioned glass fibers), FRC
Postec (Ivoclar-Vivadent, Schaan, Liechtenstein; Group 6, glass fibers), Luscent
Anchors (Dentatus, New York, NY, USA; Group 7, glass fibers), Snowpost
(Carbotech, Ganges, France, Group 8, silica fibers). From each group fifteen posts
of the largest available size (Table I) were collected. The size of the post in the
different groups varied from 1.5 mm to 2.0 mm. Ten of them, randomly chosen,
were used for fatigue test, whereas the other five were processed for microscopic
evaluation.
4.2.1 Fatigue test
Ten posts from each group were tested in a fatigue machine (Procyon systemes,
France). This device has a counter that measures the number of cycles and stops
when the specimen breaks (Fig. 1). The three-point bending method of loading was
43

applied, with a loading angle of 90° at a frequency of 3Hz. As the posts in the eight
groups had different diameters, a calculation was done to establish the load to be
applied on the different posts, according to the diameter itself.
( )( )
( )( )
δπ
δ
=××
×
= =
=
=
=
83
F Id
stress N mm MPaF load or force NewtonI span mmd diameter mm
/ ²
The load was applied according to the diameter of post
IdF
3
8×
××
=πδ
The two supports and the punch had a 3-mm diameter, and the distance between the
two supports was 9 mm. All the tests were carried out at a room temperature of
approximately 22°C. The machine was set to carry out 2,000,000 cycles, the
assumption being that, as teeth normally come into contact once a minute, this
number of cycles would simulate about four years of physiologic occlusal and
masticatory activity (Ferrari et al 2000b, Scotti et al 2002).
For those fiber posts that failed prior to reaching the projected cycle count, the
actual number of resisted cycles as counted by the fatigue machine was recorded.
The differences among the tested posts in the number of resisted cycles were tested
for statistical significance with the One-Way ANOVA, followed by the Bonferroni
test for multiple comparisons. The level of significance was set at p<0.05.
At the completion of the fatigue test, the posts were processed for a SEM evaluation,
which was aimed at verifying whether any changes had occurred in the structure of
the post as a result of loading. The detected modifications were documented through
microphotographs.
4.2.2 SEM evaluation
Each post was cross-sectioned into two halves using a diamond saw (Isomet,
Buehler, Lake Bluff, NY). One half was used for the observation of the surface
44

exposed by the cross-sectional cut, whereas the other half was again sectioned
longitudinally (with the same diamond saw described above), in order to examine
the fibers along their longitudinal axes. The external surface of this half of each
sectioned fiber post was also examined. The specimens were mounted on metallic
stubs, and sputtered with gold in an ion-sputtering device (Balzers Ltd., London,
Great Britain). Then the specimens were analyzed under a scanning electron
microscope (Philips 505, Eindoven, The Netherlands), and microphotographs were
taken for documenting the morphologic characteristics of posts. The diameter of the
fibers, the number of fibers per mm2, and the surface occupied by fibers per square
millimeter of post surface were measured. Three micrographs were taken for
evaluating each post, and the result was obtained calculating the mean of the score
assigned to the three single micrographs. Also, the presence of voids/bubbles within
the post and on its outer surface was assessed and expressed through a three-step
scoring system, which was defined as: 0 = no voids or bubbles visible; 1 = micro
voids or bubbles can be detected (diameter < 20 microns); 2 = voids or bubbles
(diameter > 20 microns) are evident and/or fiber detachments due to a loose bond
within the resin matrix. The scoring method allowed for a quantitative evaluation of
the structural integrity of the posts, as well as for a statistical evaluation of the
differences among the various types of post. SEM scores were assigned by two
different operators, who separately examined the micrographs taken from the
specimens. In case of disagreement between the two investigators on the score
assigned to a specimen, the worse score was chosen for the statistical analysis. The
observations were repeated twice to verify the inter-examiner reliability. The
differences in the scores recorded for the eight groups of posts were tested for
statistical significance with the Kruskal Wallis ANOVA on ranks, followed by the
Mann-Whitney U test for multiple comparisons. The level of statistical significance
was set at p<0.05.
4.2.3 Correlation analyses
A further objective of the investigation was to verify the existence of a correlation
between the fatigue resistance exhibited by the different types of posts and their
structural characteristics, namely fiber diameter, fiber density, and the surface
occupied by fibers per square millimetre of post surface. For that purpose, the
45

strength of the correlation between the number of resisted cycles and each one of the
mentioned structural variables of the posts was measured by calculating the
Pearson’s correlation coefficients. The statistical significance of the correlations was
also assessed (p<0.05).
4.3. Results
4.3.1 Fatigue tests
Table II reports the means and standard deviations of the number of cycles that the
different types of posts were able to withstand before breaking. Table II. Mean and standard deviation of the number of cycles that each type of post proved able to
withstand before breaking.
Group
number
Type of post Mean number of resisted cycles Standard
deviation
Group 1 Easypost 931750.2 829005.8
Group 2 Para Post Fiber White 84915.7 106039.0
Group 3 FibreKor 29687.8 24327.5
Group 4 Ghimas White 440952.9 160671.8
Group 5 DT Light-post radiopaque 2000000 0
Group 6 FRC Postec 1837138.7 371387
Group 7 Luscent Anchors 807242.9 2008
Group 8 Snowpost 6763.1 780
The results of the statistical analysis performed on these data are summarized in
Figure 2.
The highest resistance to cyclic loads was exhibited by the DT Light-post group
(Group 5), followed by the FRC Postec group (Group 6). None of the specimens
from the DT Light-Post group was broken after two million cycles, whereas among
the FRC Postec posts only one failure occurred. From a statistical standpoint the
results given by these two groups were similar (Fig. 2). Conversely, Snowpost,
FibreKor, and Para Post (Groups 8, 3, and 2) showed fatigue resistance that were
significantly lower than that of any other post tested (Fig. 2).
4.3.2 Structural integrity
The scores assigned to the different types of posts in order to quantify their
structural integrity, as revealed by SEM observations, are summarized in Table III.
46

Table III. Median values of the scores assigned to the different types of posts, providing an estimate of
posts’ structural integrity, as shown by scanning electron microscopy.
Group number Scores
Type of post
Cross
section of
the post
Longitudinal
section of
the post
External surface of
the post
Group 1 Easypost 2 2 2
Group 2 Para Post Fiber White 2 2 1
Group 3 FibreKor 0 1 1
Group 4 Ghimas White 0 0 0
Group 5 DT Light-post radiopaque 0 0 0
Group 6 FRC Postec 0 0 0
Group 7 Luscent Anchors 1 2 1
Group 8 Snowpost 0 1 0
The specimens from the Easypost, Para Post, and Luscent groups (Groups 1, 2, and
7) exhibited voids and/or bubbles within the post structure on both the cross and the
longitudinal sections. The specimens from the Easypost group (Group 1) also
showed gaps between the fibers and the resin matrix, in particular in the peripheral
area and on the external surface of the post. The Easypost and Para Post groups
recorded scores that were significantly higher than those of any other type of post
(p<0.05; Fig. 3). Only on the specimens from DT Light-post (Group 5), FRC Postec
(Group 6), and Ghimas White (Group 4) were no structural defects visible either on
the cross and longitudinal sections or on the outer surface of the post. The scores
assigned to these three types of posts were significantly lower than those of any
other group (p<0.05; Fig. 3).
When the posts that were fractured after load cycling were observed under the SEM,
their loss of structural integrity was evident (Fig 4). On the other hand, the DT
Light-post and the FRC Postec posts, which were able to withstand the fatigue test,
exhibited only a small circumferential depression in the area of contact of the
loading punch (Fig 5).
47

4.3.3 Correlation analyses
The data expressing the strength of the correlation between fatigue resistance and
structural characteristics of the posts are summarized in Table IV. No correlation
was found to be statistically significant (p>0.05). Table IV. Strength and statistical significance of the correlation between fatigue resistance of the posts
and their structural characteristics.
Variable Variable
Fibers diameter Fibers density Surface occupied by fibers per
square millimeter of post
surface
Pearson’s
correlation
coefficient
r = 0.167 r = 0.069 r = 0.171
Mean
number of
resisted cycles
Statistical
significance
p = 0.693 p = 0.871 p = 0.685
4.4 Discussion
As fiber-reinforced composite materials, fiber posts owe their mechanical properties
not only to the characteristics of fibers and matrix, but also to the strength of the
bond at the interface between these components and to the geometry of
reinforcement, such as fiber length, orientation and concentration (Callister et al
1997). The addition of fibers to a polymer matrix leads to a significant increment in
fracture toughness, stiffness, and fatigue resistance of the material. Since fibers
represent the stiffer component in a post, as compared with the resin matrix, the
posts that exhibit a higher fiber density (Figure 4) would be expected to yield a
greater fracture resistance than those with lower fiber densities (Figure 5) (Callister
et al 1997). Any fiber direction diverging from the longitudinal axis of the post
results in a stress transmission to the matrix. For this reason, posts with parallel
fibers should, at least theoretically, withstand loads more efficiently than posts
containing obliquely-oriented fibers (Callister et al 1997).
In the fabrication of endodontic posts, glass, quartz, carbon, and ceramic fibers have
been used (Drummond et al 1999, Asmussen et al 1999). The posts produced by
RTD and Ivoclar-Vivadent contain silanized glass fibers and an epoxy resin. During
48

the manufacturing process of RTD posts, the fibers are pre-stressed in tension and
then soaked in resin, which is finally polymerized. On the final cure of the resin, the
tension in the fibers is released and, as a result, the resin surface is placed under
compression. For this reason, when the post is subjected to a flexural force, the
tensile stresses which are introduced can easily be absorbed. For the Ivoclar-
Vivadent posts, they are made following the Vectris technology (Vichi et al 2001).
The methods of fabrication of DT Light-post and FRC Postec can provide an
explanation for the significantly higher resistance to fracture under cyclic bending
forces. Unfortunately manufacturers do not declare the modulus of elasticity of the
resin employed as the resin matrices of these posts: it could eventually play an
important role in the determination of the fatigue resistance of the post. Another
important factor is whether the fibers are silanized prior to embedding in the resin
matrices: in particular, it can affect both the resistance of these fiber posts to the
fatigue tests as well as the structural integrity of these posts. Good interfacial
bonding ensures load transfer from the matrix to the reinforcement, and is a primary
requirement for effective use of reinforcement properties (Gu 1997).
During normal occlusal and masticatory function, both the natural and the restored
teeth are subjected to cyclic loading. Thus, failure due to fatigue stress is a
phenomenon of paramount importance from a clinical standpoint (Dietschi et al
1996 and 1997, Hsu et al 2002), as failure commences from a small structural defect
such as a void or microcrack within the material. From this area of weakness a crack
front can gradually propagate through the material, finally resulting in catastrophic
failure (Griffith et al 1920). Potential areas of weakness in a fiber-reinforced post
can be seen in the voids present within the resin or in the discontinuities along the
interfaces between fibers and matrix. Thus, a solid void-free post with evenly
distributed and parallel-oriented fibers seems to be critical for their clinical success.
Areas of potential weakness may also be found in regions where the section of the
post has an abrupt change (Baran et al 2001). For this reason, the addition of a notch
on the post for the purpose of retention does not seem to benefit the post’s fatigue
resistance. The SEM observation of posts that fractured under load showed how
their structure was altered by the fatigue stress.
49

In the fatigue test, as in a repeated masticatory action, the load varies between a
minimum (Kmin) and a maximum (Kmax). Theoretically the moment in which a
rapid fracture occurs has to be related to the Kmax value. On the other hand, the
difference between the maximum and the minimum values (K) corresponds to the
cyclic dissipation of stress energy. The two different values (Kmax and K)
combined provide important information, and are likely to be simulating what really
happens in the mouth (Wiskott et al 1997).
In the present study a load ranging from 20 to 100 N was applied at a frequency of
3 Hz. With the 20-N force, the loading unit was kept in stable contact with the
specimen. In fatigue tests, Kmax does not usually exceed 50% of the ultimate
strength of the material (Cohen et al 1996). This criterion was applied also in the
present study, and the results showed that specimen failure could occur when a
cyclic force as low as one half of the material’s ultimate strength was exerted.
The stress acts on the matrix particularly when a compressive force is exerted on the
post or when the forces are directed obliquely or diagonally to the post’s
longitudinal axis. The high stresses on the fiber/resin interface are responsible for a
gradual inelastic behaviour, which occurs as a consequence of interface detachment
between the fibers and the matrix. Also plastic deformation of the matrix and resin
microcracking occur. Such stresses are minimum in the equidistant areas of the
fibers, and maximum immediately next to the same fibers (Grandini et al 2002a).
Regarding the fracture mode of the post, it is speculated that when failure
commences under compression the more brittle fibers break due to variability in
individual fiber surface defects. This leads to interfacial slip between the broken
fiber and the matrix, and consequently stress magnification in the adjacent fibers.
As the interfacial bond is probably still effective, tensile stress in the broken fiber
along the bond transfer length will gradually build-up. If the bond strength is
exceeded, delamination of the fiber from the matrix will commence and propagate
(Grandini et al 2002a). With interfacial bond lost progressive fiber fracture will
occur leading to overall catastrophic failure. Further detailed fractographic analysis
should be performed to validate the results of this study.
The overall results of this study require rejection of both null hypotheses.
Differences exist among different brands of fiber posts in terms of their structural
50

characteristics and fatigue resistance, although little correlation was observed
between these two attributes. DT Light-post and FRC Postec can be expected to
function efficiently in their ability to resist fatigue stresses. This factor adds to the
reliability of these materials when used clinically for the restoration of
endodontically treated teeth.
In conclusion, the overall results of this study require rejection of both null
hypotheses. Differences exist among different brands of fiber posts in terms of their
structural characteristics and fatigue resistance, although little correlation was
observed between these two attributes. Wiskott et al. (1997) indicated that the
number of cycles in fatigue testing should be at least one million cycles. In the
present study, a maximum of two millions cycles was applied, with the intention of
simulating about four years of normal occlusal and masticatory activity (Ferrari et al
2000b, Scotti et al 2002). It should be pointed out that the cyclic fatigue test
performed in this study most likely exposed the specimens to higher tensile stresses
than those that would have actually been transmitted to an endodontic post cemented
inside a root, as failure of the bonding cement could have occurred prior to post
fracture. For this reason, in order to have a fatigue resistance appraisal that is closer
to clinical reality, the same study should be repeated on roots with cemented posts
instead of just posts. This requires a completely different study design that does not
involve three-point bending test.
51
Fig. 1. The post ready to be tested.
52
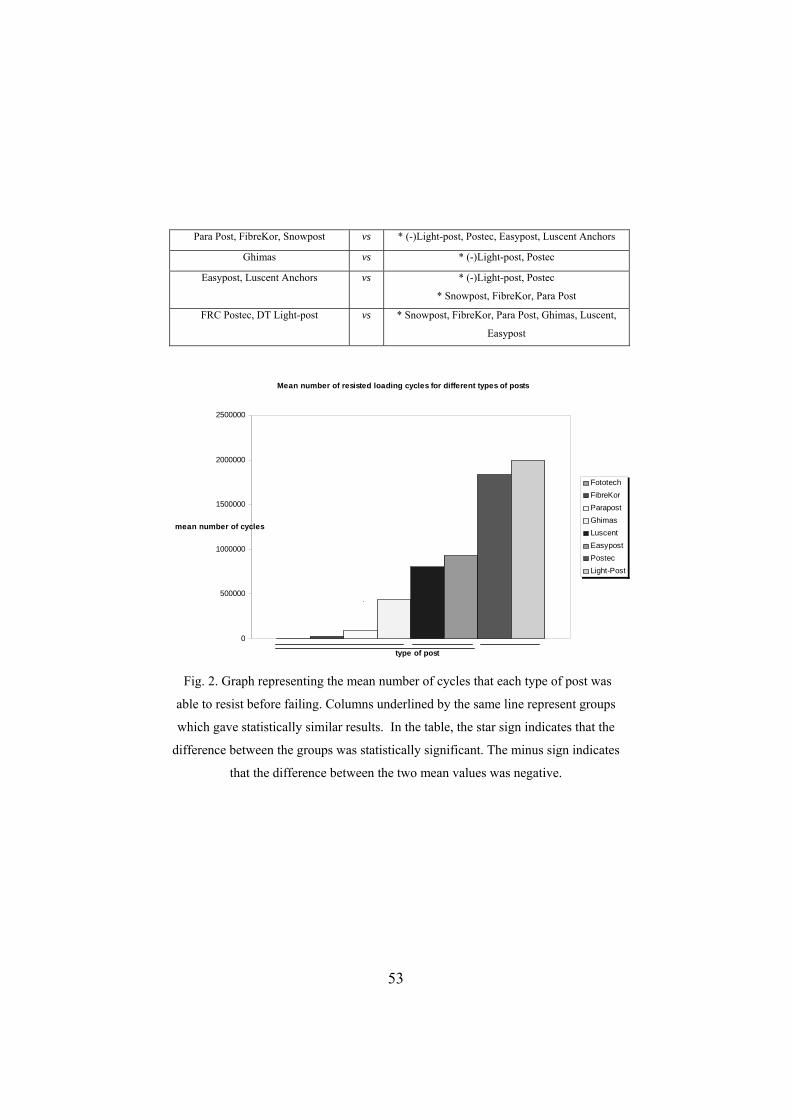
Para Post, FibreKor, Snowpost vs * (-)Light-post, Postec, Easypost, Luscent Anchors
Ghimas vs * (-)Light-post, Postec
Easypost, Luscent Anchors vs * (-)Light-post, Postec
* Snowpost, FibreKor, Para Post
FRC Postec, DT Light-post vs * Snowpost, FibreKor, Para Post, Ghimas, Luscent,
Easypost
Mean number of resisted loading cycles for different types of posts
0
500000
1000000
1500000
2000000
2500000
type of post
mean number of cycles
FototechFibreKorParapostGhimasLuscentEasypostPostecLight-Post
Fig. 2. Graph representing the mean number of cycles that each type of post was
able to resist before failing. Columns underlined by the same line represent groups
which gave statistically similar results. In the table, the star sign indicates that the
difference between the groups was statistically significant. The minus sign indicates
that the difference between the two mean values was negative.
53
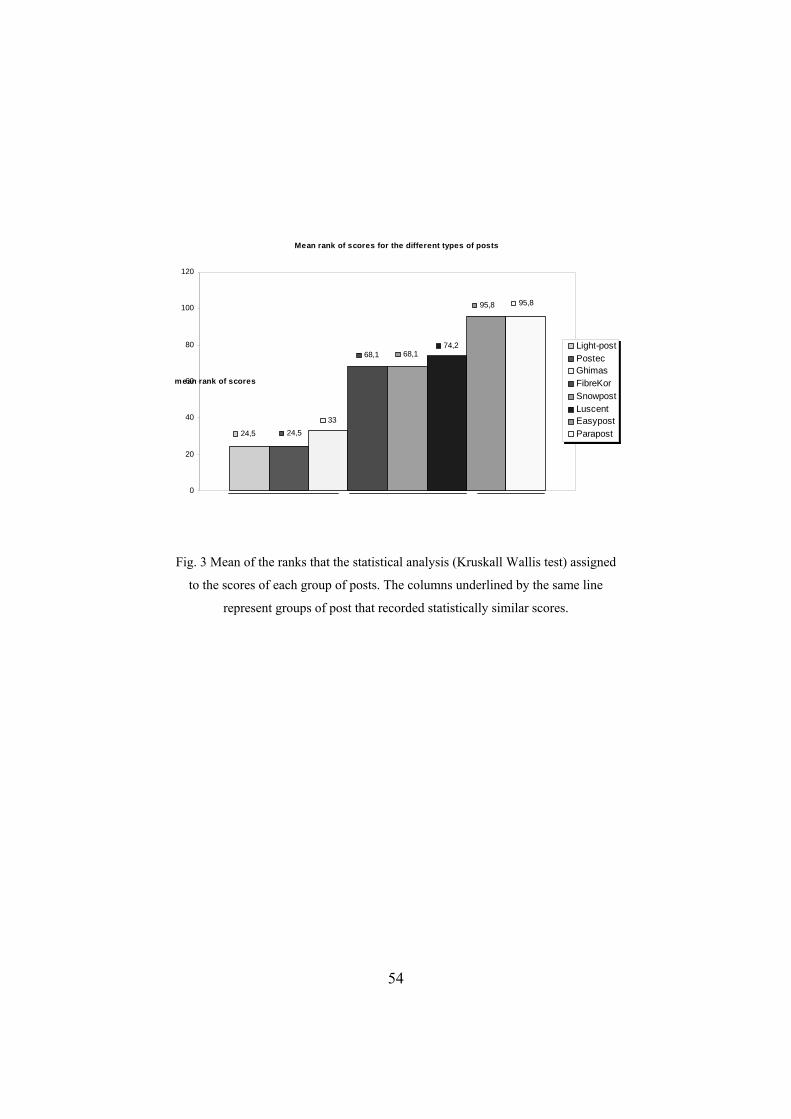
Mean rank of scores for the different types of posts
24,5 24,533
68,1 68,174,2
95,8 95,8
0
20
40
60
80
100
120
mean rank of scores
Light-postPostecGhimasFibreKorSnowpostLuscent EasypostParapost
Fig. 3 Mean of the ranks that the statistical analysis (Kruskall Wallis test) assigned
to the scores of each group of posts. The columns underlined by the same line
represent groups of post that recorded statistically similar scores.
54

Fig. 4 A sample from group 7. The fatigue test caused the breaking of the post.
55

Fig. 5 Group 5 sample. After 2.000.000 cycles the post is still unbroken. The point
where the loading punch worked is evident.
56
References
Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
newer types of endodontics posts. J Dent 1999;27:275-278.
Baran G, Boberick K, McCool J. Fatigue of restorative materials. Crit Rev Oral Biol
Med 2001;12:350-356.
Callister WD Jr. Materials Science and engineering. An introduction. 3rd Edition.
Chapter 17. Composites. Wiley: New York; 1997; 513-541.Chappel RP, Cobb CM, Spencer
P. Dentinal tubule anastomosis: A potential factor in adhesive bonding? J Prosthet Dent 1994;
72: 183-188.
Cohen BI, Pagnillo MK, Condos S, Deutsch AS. Four different core materials
measured for fracture strength in combination with five different designs of endodontic posts.
J Prosthet Dent 1996;76:487-495.
Cohen BI, Pagnillo MK, Newman I, Musikant BL, Deutsch AS. Cyclic fatigue
testing of five endodontic post designs supported by four core materials. J Prosthet Dent
1997;78:458-464.
Dallari A, Rovatti L. Six years of in vitro/in vivo experience with Composipost.
Compendium 1998;20:S57-S63.
Dietschi D, Romelli M, Goretti A. Evaluation of post and cores in the laboratory:
rationale for developing a fatigue test and preliminary results. Compend Contin Educ Dent
Suppl 1996;20:S65-S73.
Dietschi D, Romelli M, Goretti A. Adaptation of adhesive posts and cores to dentin
after fatigue testing. Int J Prosthodont 1997;10:498-507.Drummond JL, Toepke RS, King TJ.
Thermal and cycling loading of endodontic posts. Eur J Oral Sci 1999;107:220-224.
Duret B, Reynaud M, Duret F. Un nouveau concept de reconstitution corono-
radiculaire: le composiposte (1). Chir Dent France 1990;540:131-141.
Fan P, Nicholls JI, Kois JC. Load fatigue of five restoration modalities in
structurally compromised premolars. Int J Prosthodont 1995;8:213-220.
Ferrari M, Scotti R. Fiber posts: clinical and research aspects. Masson Ed, Milano
2002.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of clinical
performance of fiber posts. Am J Dent 2000a;13:9B-14B.
Ferrari M, Vichi A, García-Godoy F. A retrospective study of fiber-reinforced
epoxy resin posts vs. cast posts and cores: a four year recall. Am J Dent 2000b;13:B9-B14.
Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjör IA. Bonding to root canal:
Structural characteristics of the substrate. Am J Dent 2000c;13:380-386.
57
Fredriksson M, Astback J, Pamenius M, et al. A retrospective study on 236 patients
with teeth restored by carbon fiber-reinforced epoxy resin posts. J Prosthet Dent 1998;80:151-
7.
Freedman GA. Esthetic post and core treatment. Dent Clin North Am
2001;45:1:103-116.
Gateau P, Sabek M, Dailey B. Fatigue testing and microscopic evaluation of post
and core restorations under artificial crowns. J Prosthet Dent 1999;82:341-347.
Grandini S, Balleri P, Ferrari M. Scanning electron microscopic investigation of the
surface of fiber posts after cutting. J Endod. 2002; 28:610-612.
Griffith AA. The phenomena of rupture and flow in solids. Philosophical
Transactions of the Royal Society of London (Series A) 1920; A221: 168-198.
Hsu YB, Nicholls JI, Phillips KM, Libman WJ. Effect of core bonding on fatigue
failure of compromised teeth. Int J Prosthodont 2002;15:175-178.
Gu W. Interfacial Adhesion Evaluation of Uniaxial Fiber-Reinforced-Polymer
Composites by Vibration Damping of Cantilever Beam. PhD thesis at Virginia Polytechnic
Institute and State University. 1997; 11-13.
Kahn FH, Rosenberg PA, Schulman A, Pines M. Comparison of fatigue for three
prefabricated threaded post systems. J Prosthet Dent 1996;75:148-153.
Malferrari S, Baldissara P, Arcidiacono A. Translucent quartz fiber posts: a 20
months in vivo study. IADR 80th General Session, S.Diego, 2002, abstract n° 2656.
Monticelli F, Grandini S, Goracci C, Ferrari M. Clinical behaviour of translucent
fiber posts and luting and restorative materials: a 2-year report. Int J Prosthod
2003;16,(6):593-6.
Mjör IA, Nordhal I. The density and branching of dentinal tubules in human teeth.
Archs Oral Biol 1996; 41: 401-412.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissue. Berlin:
Quintessence Co. Publ., 1998.
Reagan SE, Fruits TJ, Van Brunt CL, Ward CK. Effects of cyclic loading on
selected post-and-core systems. Quintessence Int 1999; 30:61-67.
Scotti S, Malferrari S, Monaco C. Clinical evaluation of quartz fiber posts: a 30
months results. IADR 80th General Session, S.Diego, 2002, abstract n° 2657.
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on the
masking of various types of opaque posts. J Prosthet Dent. 2000;83:412-7.
Vichi A, Grandini S, Ferrari M, Clinical procedure for luting Vectris fiber posts. J
Adhes Dent 2001; 3: 353-359.
58

Vichi A Grandini S, Ferrari M. Comparison between two clinical procedures for
bonding fiber posts into a root canal: a microscopic investigation. J. Endod 2002;28:355-360.
Wiskott HW, Nicholls JI, Belser UC. The effect of tooth preparation height and
diameter on the resistance of complete crowns to fatigue loading. Int J Prosthodont
1997;10:207-215.
Yamamoto M, Takahashi H. Tensile fatigue strength of light cure composite resins
for posterior teeth. Dent Mater J 1995 ;14:175-184.
59

Chapter 5 Adjusting the length of a post
As the wear properties of fiber posts are inferior if compared to resin composite
materials, it is not safe to have them exposed to the tooth to tooth and tooth to food
wear. If a crown is placed, the exposed fiber post is protected by the crown itself. If
a direct restoration is made, it is convenient to cut the post before the luting
procedures of the post itself (Ferrari et al 2002). As a matter of fact fiber posts are
pre-fabricated, so they have to be adapted to the root and to the crown length. The
following study regards a comparison between different techniques for cutting fiber
posts.
5.1 Scanning electron microscopic investigation of the surface of fibre posts
after cutting
At the beginning of 1990 carbon fibre posts were proposed as alternative to metallic
posts (Duret et al 1990). In the last 10 years, different types of fiber posts were
proposed to improve mechanical and esthetic properties of fibre posts (Fredrikson et
al 1998, Dallari et al 1998, Ferrari et al 2000a). Initially hybrid posts and almost
simultaneously white quartz posts were proposed (Scotti et al 2000, Ferrari et al
2000b). More recently, translucent posts became available. As the development of
fibre posts was very quick, all these types of posts are still in the market and are
routinely used by practitioners. Recently, clinical efficacy and performances of 3
different types of fibre posts were documented (Fredrikson et al 1998, Dallari et al
1998, Ferrari et al 2000a, Scotti et al 2000, Ferrari et al 2000b). All different types
of fibre posts have a similar strength and stiffness (Asmussen et al 1999). The
stiffness (or modulus of elasticity) of the posts is similar to that of dentin and, for
that, the risk of root fracture became much lower than that noted when metallic posts
were used (Ferrari et al 2000a). In addition, bonding between different types of posts
and resin cements has been demonstrated (Mannocci et al 1999, Ferrari et al 2001,
Vichi et al 2002).
Fibre posts are made in a standardised length in order to be adapted to the length of
different roots. Each post must be tried in and then cut at the most convenient length
in order to avoid exposition of the post along the surface of the abutment/restoration.
60

This is due to the fact that the exposition of the post in to the oral environment might
determine degradation of the resin with a consequent loss of its mechanical
properties during clinical service. However, in order to have a sufficient rigidity of
the abutment at the coronal level, the post must keep its integrity and mechanical
properties after being cut.
In clinical practice, three different methods for cutting fibre posts might be used: 1.
Diamond bur mounted in a turbine handpiece, 2. Carborundum disc mounted in a
handpiece and 3. Scissors.
The aim of this study was to evaluate 1. if and how three cutting methods can affect
integrity of fibre posts and 2. to test the null hypothesis that the type of cutting
procedure can not affect the integrity of post’s surface.
5.2 Materials and Methods
Among those available in the market, six types of fibre posts were selected for this
study: Caron Fibre Posts (RTD, St Egreve, France) as control, Quartz Fibre Posts
(RTD), Aesthetic Posts (RTD), Aesthetic Plus Posts (RTD), Translucent Posts
(Dentatus, Zurich, Switzerland), FRC Postec Posts
(Ivoclar-Vivadent, Schaan, Liecthenstein). Fifteen posts of each type were used. A
total of 90 posts were evaluated.
All fiber posts had a diameter between 1.2 and 1.4 mm and a standardised length
(between 14-16 mm). Each group was divided into three subgroups, according to the
cutting method: a. Diamond bur, b. Carborundum disk and c. Scissors (Fig 1).
5.2.1 Subgroup a (diamond bur): Five samples of all six groups were cut
approximately between medium and coronal third using a diamond bur (2979,
Komet, Zurich, Switzerland) mounted in a turbine handpiece under water spray.
Both sections of each sample were collected and then mounted in a metallic stub to
observe the cut surfaces. Then, the samples were gold-coated (Edwards Co, London,
GB), evaluated using a scanning electron microscope (Philips 515, Amsterdam, The
Netherlands) and microphotographs were taken at different magnifications (x36,
200, 500, 1010) in order to properly document their cut surfaces.
5.2.2 Subgroup b (carborundum disc): Other five samples of each group were used.
The posts were cut using a carborundum disk mounted in a handpiece (L.I.M.A.,
61

Torino, Italy). Then the samples were processed microscopically (for SEM
observations) as described for Subgroup a.
5.2.3 Subgroup c (scissors): The last five samples of each group were cut using
scissors (Dentronix Inc., New York, NY, USA). Then, both halves of each post were
processed as described above for subgroup a and b.
5.3 Results
Analysis of the fibre posts after being cut showed different features mainly due to
the cutting procedures. Uniform results were found according to the type of cutting
procedure.
At low magnifications, no microscopic differences were found among the samples
of group 1-4 and 6. Only samples of group 5 showed more irregular surfaces after
being cut with the two procedures providing rotary instruments (subgroup a and b).
All groups showed evident differences between cut surface of subgroup c samples
and those of group a and b.
In subgroup a, posts showed regular surfaces after cutting with diamond bur (Fig. 2).
Cutting with a carborundum disc (subgroup b) brought to an almost regular surface,
but in all groups with some burs and sometime ‘burns’ close to the surface borders.
In subgroup c, in which the posts were cut using scissors, the cut surfaces of all
samples showed two plane and convergent flanges (Fig. 3); also due to formation of
fracture lines, these posts loose their integrity not only at the cutting surface but also
along their length.
At higher magnifications, the structure of all type of posts, based on fibres
embedded in a resin matrix, was observed. Also, in subgroup a and b samples the
cutting procedure produced a smear layer mainly covering the cut post surface.
5.4 Discussion
Cutting fibre post procedure is commonly performed before luting procedures
or/and during build- up and final preparation of the abutment. During this clinical
step, a good adaptation of the post at the coronal third of the root canal preparation
and a proper adhesion to the resin cement and composite material used for build up
of the tooth at the coronal level is desirable.
62

The findings of this study revealed significant differences in post surfaces after
cutting, similarly to those already described for guttapercha cones (Lopes et al
2000).
The loss of integrity of the posts noted after having been cut with scissors might
negatively affect the adaptation of the post to apical and medium thirds of the root
preparation and to the resin composite used for the coronal build-up. Also, the loss
of integrity of the posts after cutting using scissors can probably reduce their
mechanical properties (Fig 4).
In Subgroup a, samples of groups 1-4 and 6 showed regular cut surfaces. The cut
using diamond bur creates shear stress in the cross-section of the post, but the speed
of the handpiece reduces the plastic deformation of the post. Therefore the stress
tensions induced by the diamond bur allow the development of an almost plane cut
surface, which is perpendicular to the direction of displacement of the cut
instrument. In Subgroup b, posts of groups 1-4 and 6 also showed a regular cut
surfaces. The tips of the posts were irregular and some burs were observed close to
the surface boarders. These probably occurred because the posts were not cut against
a surface, which could create a mechanical resistance load opposed to the cut
direction. In Group 5 a less regular cut surface was noted for the two procedures
based on high speed cutting (subgroup a and b). This can be due to the different
stiffness of the posts and their fibre disposition. As a matter of fact, in group 5
samples, the density of the fibres might be less uniform than that of the other groups
and this fact can determine a different plasticity of the post and consequently the
irregular cut. When subgroup a and b were compared, a more regular cut surface
was observed in subgroup a. This difference might be due to the fact that water
cooling was only used in combination with turbine handpiece, and also to the higher
speed of this cutting procedure. In Subgroup c, in which the posts were cut using
scissors, the cut surfaces of the samples of all groups showed two plane and
convergent flangers. The magnitude of the post deformation after cutting depends on
both scissors shape and post plasticity. Also, the posts showed an area of cut
surfaces where fibres were irregularly cut at different lengths and a deattachment
between fibres and resin matrix was evident along their length.
63

Fig. 12 shows the kind of loading applied on the post during cutting with scissors.
At point P and P’, plastic deformation of the posts occurs. As the load increases, the
post is moved through the two blade surfaces of the scissors, producing two different
inclined planes. Other studies have reported similar results when guttapercha cones
were cut (Lopes at al 2000).
However, every time a fibre post is cut, the cut of the post occurs by the application
of a shear stress in the transverse section of the post. The cutting procedure induces
an elastic compression/deformation of the material. Close to the cut surface, post
fibres bend in a direction that is similar to the movement applied by the cutting
instrument. When the applied pressure overcomes the elastic resistance of the
material, the fibre post is separated.
As the cutting with the carborundum disk (subgroup b) might be associated with
irregularities in the cut post surface, a second cut might be desirable to repair the
defects. Thus, whereas the first cut allowed the calibration of the post, the second
cut can regularise the post surface (Fig 5).
Probably the speed of bur/disc mounted on the handpiece played a role such as also
the stiffness of the posts. It may happen that a “burn out” phenomenon takes place if
excessive heating is applied (Fig 6). The posts of group 1-4 are made by the same
company following the same procedure: for that the similar behaviour during cutting
posts of Group 1-4 can be related to their structure and stiffness. Posts of group 6
have similar stiffness (modulus of elasticity) than that of RTD posts (group 1-4) and
because of that they might show similar cut surface.
Also, when different posts have similar stiffness, the speed of the bur/disc played a
key role in subgroups a and b to obtain better results.
Cutting procedures can have clinical implications. After the coronal build-up, the
abutment can be prepared in order to finalise its shape to receive a crown or to refine
the anatomy of the coronal portion of the tooth. In these clinical steps the quality of
bonding between the post and the resin composite used for building it up is critical:
it must be without discontinuity between the two portions and the length of the post
at the coronal level must be sufficient to held occlusal stress. If the post presents a
superficial and internal loss of its integrity due to the cutting procedure, the bonding
between the post and the resin composite is less uniform, discontinuity might be
64

easily present in between, and the possibility of a fracture of the abutment highly
increases.
The cutting procedure using scissors must be avoided. It must be considered that
cutting the post is usually performed after trying-in into the root canal space and
before luting it. If the cutting procedure is performed at this clinical step, the rotary
cutting procedures tested in subgroups a and b might be used. If the cutting
procedure is performed after luting the post, it is strongly suggested to reduce the
length of the post with a diamond bur (as tested in subgroup a) after building-up the
abutment and during its final preparation.
The results of this study indicated that fibre posts can be regularly cut off using a
diamond bur mounted in a handpiece under copious water cooling. Although
carborundum disc cutting procedure (subgroup b) showed a less regular post surface,
it can be speculated that it might be clinically acceptable. The results of this study
might be extrapolated to other fibre posts with similar properties already available in
the market.
The null hypothesis tested in this study was not confirmed, because post surface
morphology was related to the type of cutting procedure.
65
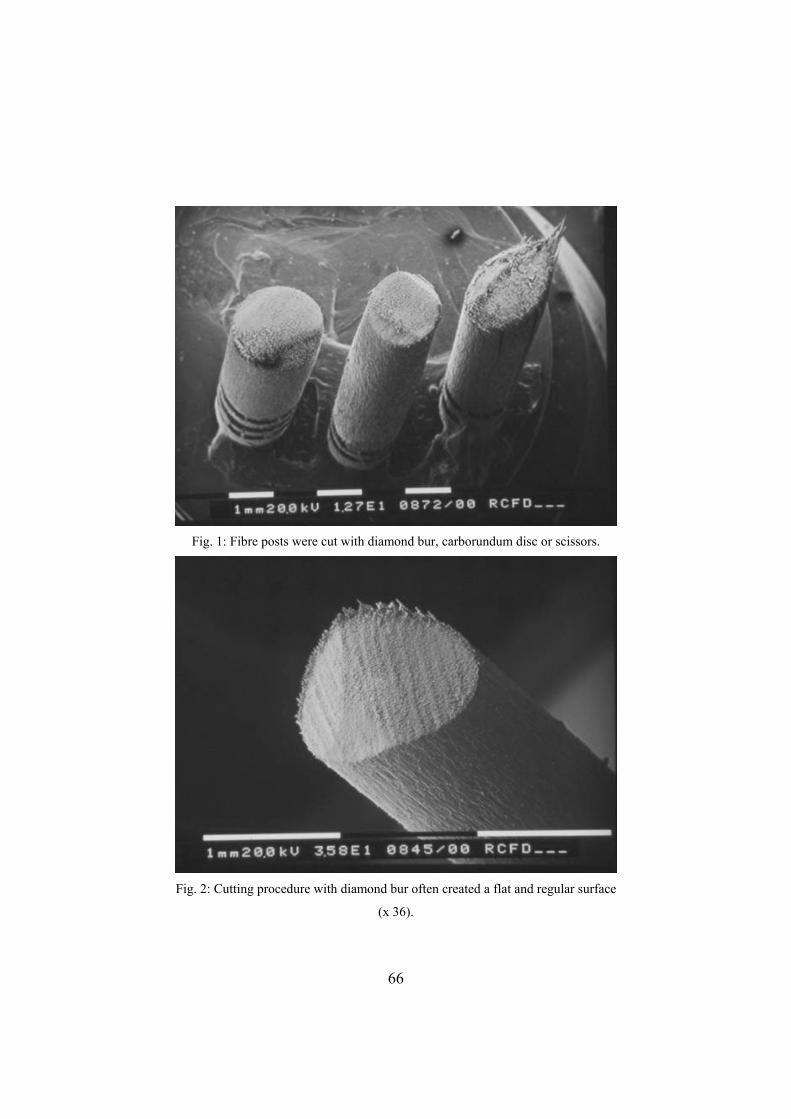
Fig. 1: Fibre posts were cut with diamond bur, carborundum disc or scissors.
Fig. 2: Cutting procedure with diamond bur often created a flat and regular surface
(x 36).
66
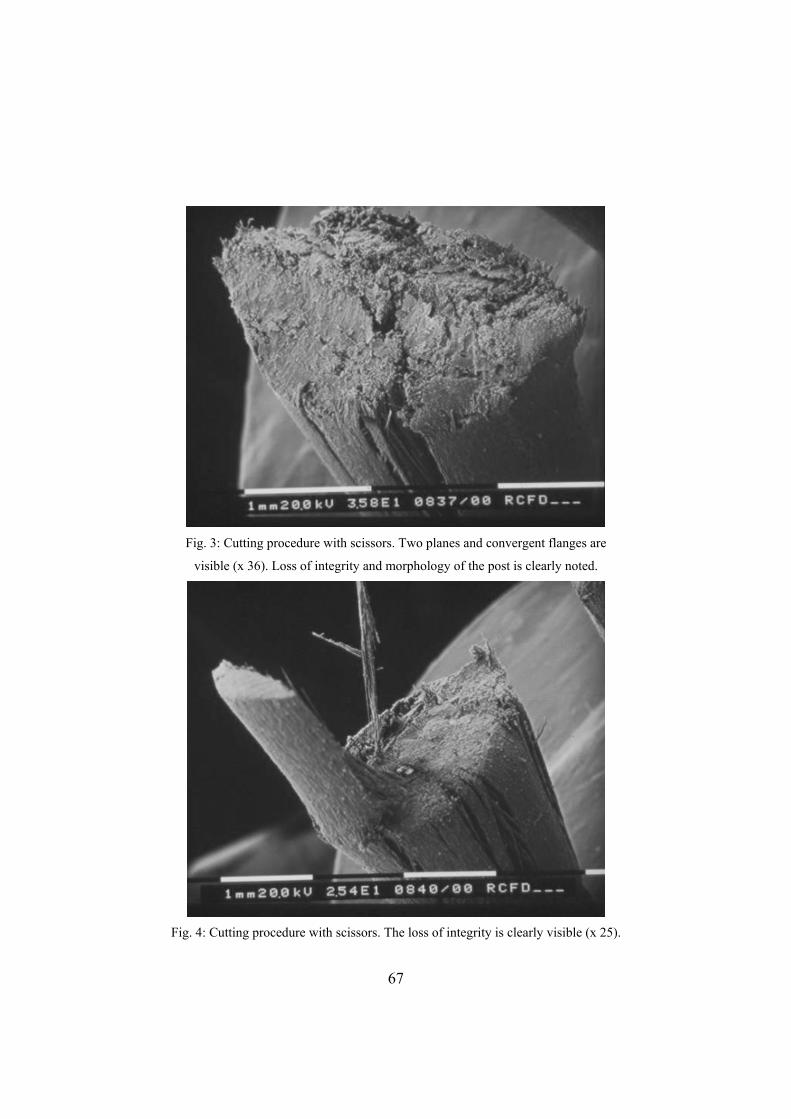
Fig. 3: Cutting procedure with scissors. Two planes and convergent flanges are
visible (x 36). Loss of integrity and morphology of the post is clearly noted.
Fig. 4: Cutting procedure with scissors. The loss of integrity is clearly visible (x 25).
67

Fig. 5: A second cut can help making more regular the cut end (x 36)
Fig. 6: Excessive heating of the post (x 36)
68
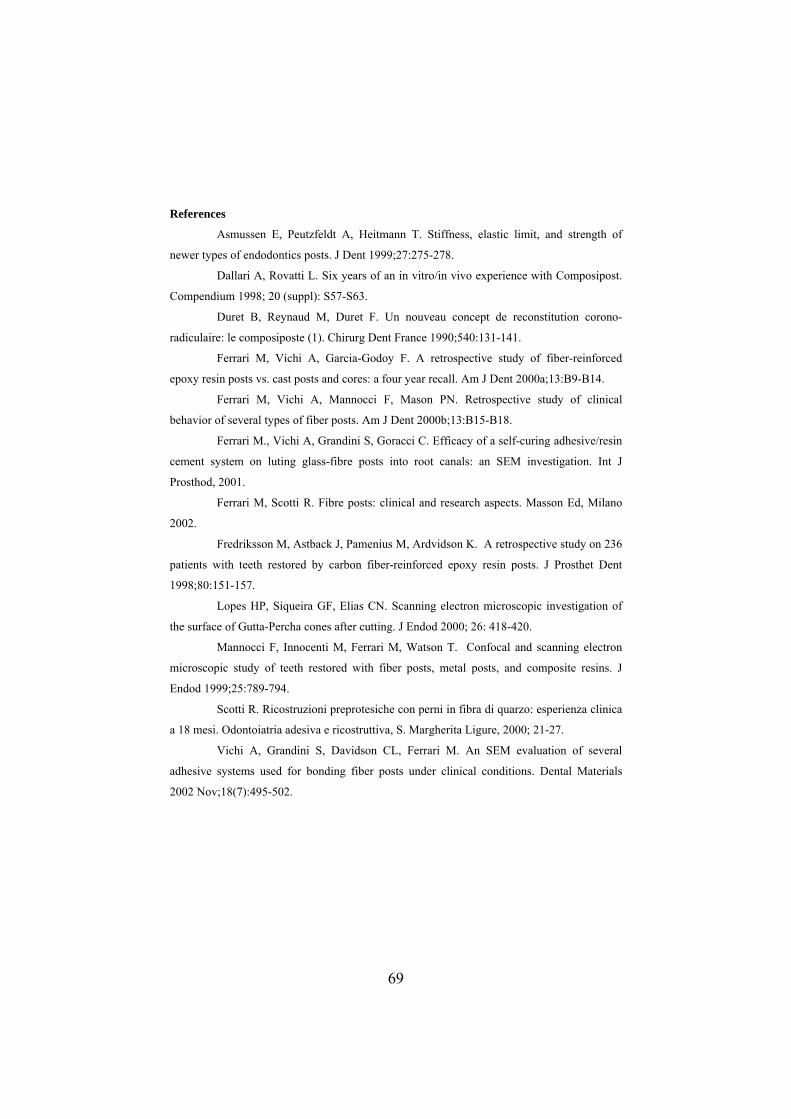
References
Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
newer types of endodontics posts. J Dent 1999;27:275-278.
Dallari A, Rovatti L. Six years of an in vitro/in vivo experience with Composipost.
Compendium 1998; 20 (suppl): S57-S63.
Duret B, Reynaud M, Duret F. Un nouveau concept de reconstitution corono-
radiculaire: le composiposte (1). Chirurg Dent France 1990;540:131-141.
Ferrari M, Vichi A, Garcia-Godoy F. A retrospective study of fiber-reinforced
epoxy resin posts vs. cast posts and cores: a four year recall. Am J Dent 2000a;13:B9-B14.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of clinical
behavior of several types of fiber posts. Am J Dent 2000b;13:B15-B18.
Ferrari M., Vichi A, Grandini S, Goracci C. Efficacy of a self-curing adhesive/resin
cement system on luting glass-fibre posts into root canals: an SEM investigation. Int J
Prosthod, 2001.
Ferrari M, Scotti R. Fibre posts: clinical and research aspects. Masson Ed, Milano
2002.
Fredriksson M, Astback J, Pamenius M, Ardvidson K. A retrospective study on 236
patients with teeth restored by carbon fiber-reinforced epoxy resin posts. J Prosthet Dent
1998;80:151-157.
Lopes HP, Siqueira GF, Elias CN. Scanning electron microscopic investigation of
the surface of Gutta-Percha cones after cutting. J Endod 2000; 26: 418-420.
Mannocci F, Innocenti M, Ferrari M, Watson T. Confocal and scanning electron
microscopic study of teeth restored with fiber posts, metal posts, and composite resins. J
Endod 1999;25:789-794.
Scotti R. Ricostruzioni preprotesiche con perni in fibra di quarzo: esperienza clinica
a 18 mesi. Odontoiatria adesiva e ricostruttiva, S. Margherita Ligure, 2000; 21-27.
Vichi A, Grandini S, Davidson CL, Ferrari M. An SEM evaluation of several
adhesive systems used for bonding fiber posts under clinical conditions. Dental Materials
2002 Nov;18(7):495-502.
69

Chapter 6 Selection of clinical luting procedures
When fiber posts are employed proper luting is a prerequisite. Depending on what
type of fibers are involved, different options can be taken into account. The first step
is the removal of the guttapercha and the preparation of the dowel space, usually
enlarged with a low-speed bur provided by the manufacturer. The depth of the post
space preparation is around 9-10 mm. Then the post has to be tried into the canal, so
to avoid imperfect fitting and excess of cement at the tip end of the post; if this
happens the post cannot be seated in the correct position. The root canal walls are
etched with phosphoric acid (usually 37%) for 15 (or 30) seconds, washed with
water spray and then gently air-dried. The excess water is removed from the post
space using paper points. Subsequently, adhesive is applied with a microbrush,
gently air-dried and the pooled adhesive left in the post space removed using a paper
point before light curing for 20 seconds. Then a dual-cure resin cement (for
translucent posts) or a self-curing resin cement (for non-translucent posts) is used to
complete the luting procedure. According to the diameter and the shape of the canal,
different brands and sizes can be utilized. The cement is applied with a lentulo spiral
into the post space, and the post inserted into the canal. Resin cement excess is
removed with a clean microbrush and then the cement light-cured for 40 seconds
(Monticelli et al 2003, Vichi et al 2002a and 2002b, Ferrari et al 2002). Some
clinicians suggest to use the same material for the cementation of the post and the
build up of the abutment: it is actually difficult to obtain a material that is hard
enough to be used as a core and that at the same time can flow in the canal like a
cement. Recently new simplified materials appeared on the market (RelyX Unicem,
3M Espe, St Paul, MN, USA) that have also been proposed for bonding fiber posts
into root canals. The bonding mechanism of this self – adhesive resin cement is still
debated, but it has been recently proven that if the substrate is non etched dentin and
if a certain pressure is applied during the luting procedures (the situation we find in
the root canal) there are encouraging results (De Munck et al 2004).
In this chapter an alternative to the well established procedure described above is
discussed.
70

6.1 A one step procedure for luting glass fibre posts: an SEM evaluation
The potential of fibre reinforced materials in restorative dentistry has been
appreciated for some time (Bradley et al. 1980). However, the concept of carbon
fibre posts as a method for reconstructing root filled teeth was not described until
later (Duret et al. 1990). Subsequent research confirmed the retention potential of
carbon fibre posts (Drummond et al. 1999, Asmussen et al. 1999), the low stressing
behaviour of the fibre post-resin cement complex, and its good clinical performance
(Fredrikson et al. 1998, Ferrari et al. 2000a, Malferrari et al. 2002, Scotti et al.
2002).
Various changes have been made to fibre post composition, radiopacity, and shape
(Love & Purton 1996, Asmussen et al. 1999, Vichi et al. 2002a). For example,
carbon has been replaced by quartz in the fibre composition, and then by glass. The
manufacturers have recently developed posts that are radiopaque, allowing the
clinician them to be seen on radiography. Several modifications have been made to
post configuration, with the aim of achieving better adaptation to root canal shape.
It is possible to transmit light through a glass fibre post that is translucent. Light
transmission through the post might permit a bonding procedure, in combination
with an acid-etching technique, based on a light curing adhesive system (as for the
other posts) and a dual curing resin cement (Vichi et al. 2002a). The translucent
fibre post has a modulus of elasticity similar to that of the other fibre posts and of
dentin, and offers adequate mechanical properties (Dietschi et al. 1997, Asmussen et
al. 1999). Transmission of light through the post also makes it possible to light-cure
the resin cement and the bonding system in only one clinical step (“one-shot”), thus
simplifying and shortening the clinical procedure (Lui 1994).
Evaluation of the efficacy of an adhesive system can be performed by observing the
uniformity of the resin dentin interdiffusion zone (RDIZ), resin tags, and adhesive
lateral branches (Nakabayashi & Pashley 1998), and by recording the presence of
voids/bubbles within the luting material or at the interface between the cavity wall
and the post (Ferrari et al. 2001a). An evaluation of the quality of the RDIZ is not
possible using scanning electron microscopy (SEM), rather TEM is the appropriate
way to assess it (Tay et al. 1995).
71

Recently, the so called ‘one bottle’ adhesive systems have been proposed for
bonding a fibre post into a root canal (Ferrari et al. 2001b). In order to perform
reproducible studies and to apply a statistical analysis, a method for scoring resin
tags, adhesive lateral branches, and RDIZ into root canal etched dentin has been
proposed (Ferrari et al. 2001a).
The aim of this study was to evaluate the efficacy of a one-step technique (“one-
shot”) in forming resin tags, adhesive lateral branches and RDIZ when luting
translucent fibre posts into root canal preparations. The null hypothesis that the one-
step technique creates the same bonding mechanism into root canal dentin than the
more traditional two-step luting procedure was tested.
6.2 Materials and Methods
Forty mandibular anterior teeth (incisors and canines), stored in a 0.1% thymol
solution, were randomly selected for the study from the department’s stock of
extracted teeth. Canal morphology was verified from radiographs (Kodak,
Rochester, NY, USA) (70 KV and 0.08 s), taken both buccolingually and
mesiodistally. The pulp chambers were opened and canal preparation at a working
length 1 mm from the apex was completed to a 35 size master apical file. A step-
back technique was used with stainless-steel K-files (Union Broach, New York, NY,
USA), Gates Glidden drills size 2 to 4 (Union Broach). Irrigation was performed
using 2.5% sodium hypochlorite and EDTA (Glyde File Prep, Dentsply Maillefer,
Ballaigues, Switzerland). The prepared teeth were obturated with thermoplasticized,
injectable gutta-percha (Obtura, Texceed Corp., Costa Mesa, CA, USA), and resin
sealer (AH-26, DeTrey, Zurich, Switzerland).
The root canal walls of each sample were enlarged and the gutta-percha removed
with the low-speed drills provided by the manufacturer (RTD, St. Egrève, France),
to a depth of 9 mm from the cementum-enamel junction. The samples were
randomly divided into four groups of ten specimens each (Table 1).
72

Table 1: Bonding-luting procedures
Group 1 - OS (control): The bonding system was light cured separately for 20 seconds.
Group 2 – OS 30: The bonding system was light cured together with the resin cement through the
translucent post for 30 seconds.
Group 3 – OS 60: The bonding system was light cured together with the resin cement through the
translucent post for 60 seconds.
Group 4 – OS 90: The bonding system was light cured together with the resin cement through the
translucent post for 90 seconds.
Group Bonding system Clinical steps Resin cement Clinical steps
1. OS a,b,c, Duo-Link d,e,f,g,h
2. OS - 30 a,b, Duo-Link d,e,f,g,h
3. OS - 60 a,b, Duo-Link d,e,f,g,h
4. OS – 90 a,b, Duo-Link d,e,f,g,h
a. Dentin conditioning with phosphoric acid b. Primer application with microbrush c. Light-curing d. Post treated with the Primer-adhesive solution e. Mixing resin cement f. Cement application into the root canal with a lentulo drill g. Removing resin excess h. Light-curing through the translucent fibre post
OS: One-Step (Bisco, Schaumburg, Il); Duo-Link (Bisco)
Group 1: The first ten specimens were treated with One Step bonding system (Bisco,
Schaumburg, IL, USA), following the manufacturer’s instructions (Ferrari et al
2000b). The root canal walls were etched with 32% phosphoric acid (Bisco) for 15 s,
washed with water by means of a syringe with a small endodontic needle, in order to
completely remove the acid, and then gently air-dried. Excess water was removed
from the post space using paper points. Four coats of primer-adhesive material were
placed in the root canals with a thin microbrush Plus (Microbrush Co., Greyton, WI,
USA) (Ferrari et al 2001b). The excess primer-adhesive solution was removed with
a paper point, gently air-dried, and then cured by applying the light tip at the canal
orifice, parallel to the long axis of the root for 20 s. For curing purposes, a VIP
curing device (Bisco) was used, with a light intensity of 600 mW/cm2. Duo-Link
(Bisco) resin cement, a dual cure resin cement, catalyst and base were mixed and
used following the manufacturer’s instructions. The resin cement was applied into
73

the root canal space with a lentulo drill, the fibre post was seated, and the excess
resin removed and each specimen light-cured for 20 s through the post.
Group 2: Ten root specimens were treated as Group 1 samples. The only difference
was that the primer/adhesive solution One Step (Bisco) was not cured immediately.
Rather, the dual-cure resin cement was applied with a lentulo drill, the post was
placed in the root canal preparation, and only at this time were the adhesive material
and the cement light-cured simultaneously through the post for 30 s.
Group 3: These roots were treated as described in Group 2. The simultaneous light-
curing was performed for 60 s
Group 4: These samples were treated as described in Group 2. The simultaneous
light-curing was performed for 90 s.
DT light posts (RTD, St Egrève, France) were used in the 40 samples (Boudrias et
al. 2001). Depending on the size and the shape of the root specimens, number 1 (tip
diameter = 90, taper 06) and 2 (tip diameter = 100, taper 08) DT posts were used.
The length of each post was controlled before the luting procedure, and the post was
sectioned to match the length to the root canal preparation.
After complete setting of the cement, crown build-ups were performed with the
proprietary resin composite (Biscore, Bisco) to eliminate the chance of
incompatibility between the luting cement and the core material.
The teeth were stored in water at room temperature for 1 week. The roots were then
sectioned parallel to the long axis of the tooth using a diamond saw (Isomet,
Buehler, Lake Bluff, NY, USA), at slow speed under water.
6.2.1 RDIZ observations
One section of each root was gently decalcified (32% phosphoric acid was applied
for 30 s; the sample was then washed and gently air-dried) and deproteinized (the
sample was immersed in a 2% sodium hypochlorite solution for 120 s), in order to
evaluate RDIZ formation.
After being extensively rinsed with water, the specimens were gently air-dried and
dehydrated with alcohol, sputter-coated with gold (Edwards Ltd, London, UK) and
observed under a scanning electron microscope (Philips 515, Philips Co.,
Amsterdam, The Netherlands) at x1010 magnification. The observations were made
74

by two operators, and repeated twice in order to ensure intra examiner consistency.
When a different score was given, the lower score was taken into account.
The following aspects were evaluated by scanning electron microscope:
1. The continuity of the RDIZ: this variable was assessed as the percentage ratio
between the length of the RDIZ and the total length of the adhesive interface using a
visual and computer aided examination and calculation. The differences among the
average ratios calculated for the four groups were tested for statistical significance.
The One-Way ANOVA and Newman-Keuls Multiple Comparisons Test were
applied, setting the level of significance at p=0.05.
2. The presence or absence of gaps: a. Inside the adhesive layer, b. Between the
adhesive and the resin cement layer, c. Inside the resin cement layer, d. Between the
adhesive and the post.
6.2.2 Evaluation of resin tag formation
The other section of each sample was stored in 30% HCl for 24 h and in 2% sodium
hypochlorite solution for 10 min, in order to completely dissolve the dental substrate
and to detect resin tags and adhesive lateral branch formation. The samples were
then processed for SEM observation as already described.
Serial SEM photomicrographs at x500 original magnification were taken of the
canal walls at the 1, 4.5 and 8 mm levels from the end of the post. The serial
photomicrographs were aligned to form a continuous horizontal examination strip at
the 3 levels. Irrespective of the number of photomicrographs needed to form a
complete strip, each strip was subdivided into eight “assessment units”. The density
and morphology of the resin tags were then assessed.
The density and morphology of resin tags present at x500 magnifications were
graded between 0 and 3. A score of 0 was assigned where resin tags were not
detectable, a score of 1 was recorded when few, short resin tags (resin plugs) were
visible. A score of 2 was recorded when uniform resin tags formation was seen but
with a few lateral branches. A score of 3 was recorded when long resin tags with
lateral branches were uniformly evident.
Higher standardized magnifications were taken in order to document resin tags and
adhesive lateral branches morphology.
75

The scores assigned to resin tags seen at the 1, 4.5, and 8 mm levels were analyzed
with the Kruskal Wallis test, in order to check for statistical significance of the
differences both within and among the groups. The level of significance was set at
p=0.05 level.
6.3 Results
The number of samples showing voids/bubbles within the resin cement or/and at the
interface between resin cement and root walls are summarized in Table 2. Table 2: Number of specimens in which the presence of gaps/voids/bubbles within resin
cements was noted.
Within resin cement Post/cement Adhesive/cement
Group 1 1 1 /
Group 2 2 1 5
Group 3 3 2 3
Group 4 2 2 2
Voids were present in the composite cement layers of all groups. The cement layer
was substantially similar in all groups. Between 10% (Group 1) and 30% (Group 3)
of samples showed bubbles/voids within the cement. The adhesive-composite
cement and composite cement-fibre post interfaces were substantially free of voids.
Half of the samples in Group 2 showed voids/bubbles in the adhesive/cement layer.
All groups with simultaneous curing of the adhesive and of the cement (Group 2, 3
and 4) showed a high number of voids in post/cement and adhesive/cement
interfaces.
6.3.1 RDIZ observations
The results obtained regarding the presence of RDIZ in the various groups under the
SEM microscope are shown in Table 3.
76

Table 3: Scanning electron microscope evaluation of the resin dentin interdiffusion zone (RDIZ). Groups
labelled with the same letter did not show any statistically significant difference.
Group Overall length of observed
interface (in mm)
Length of interface with RDIZ (in mm)
1 OS 25.5 22.7 (89%)a
2 OS 30 26.5 18.5 (60%)b
3 OS 60 27.0 18.5 (65%)b
4 OS 90 26.0 18.2 (70%)b
Group 1 - OS (control): The bonding system was light cured separately for 20 seconds. Group 2 – OS 30: The bonding system was light cured together with the resin cement through the translucent post for 30 seconds. Group 3 – OS 60: The bonding system was light cured together with the resin cement through the translucent post for 60 seconds. Group 4 – OS 90: The bonding system was light cured together with the resin cement through the translucent post for 90 seconds.
The ratio between the length of the RDIZ and the total length of the interface was
significantly higher in Group 1 than in the other two Groups (p<0.05). Group 1
samples had uniform RDIZ formation, while in the other groups RDIZ was less
represented, especially at the apical level. In some samples of Group 2, 3, and 4, a
discontinuous gap between the RDIZ and resin cement was observed. The RDIZ
formation of Group 1 samples was significantly more evident than in the other three
Groups (Group 2, 3 and 4). Group 4 showed a higher ratio than Group 3, which in
turn presented a higher ratio than Group 2, but no statistically significant differences
were found among these three Groups (p>0.05).
6.3.2 Evaluation of resin tag formation
The results obtained regarding morphology and density of resin tags are
summarized in Table 4.
In Group 1 resin tags and lateral branches formation was more uniform than in the
other Groups. Although the length of resin tags was more evident at the coronal
third, the morphology of the resin tags was similar in all three thirds. The surface of
resin tags reproducing de-mineralized tubular dentin was rough and depicted the
appearance of tubular dentin dissolved by the acid. In the apical third resin tags were
all approximately the same length, which was shorter than that seen in the coronal
and middle third.
77

Table 4: Median values of the resin tags formation scores recorded at 1-, 4.5-, and 8 mm
levels. (Groups labelled with the same letter did not show any statistically significant
difference).
Group 1mm level
(Coronal third)
4.5 mm level
(Middle third)
8 mm level
(Apical third)
1. OS 2.9a 2.9a 2.5a,b
2.OS 30 2.6a,b 2.4b 1.1d
3.OS 60 2.6a,b 2.5b 1.3c,d
4.OS 90 2.7a 2.5a,b 1.7c
Group 2, 3 and 4: The resin tags formed in the coronal and/or middle areas of the
roots were much longer than those in the apical areas. Also, the density of resin tags
was higher in the coronal and middle areas than in the apical areas. In the coronal
two thirds of the roots adhesive lateral branch formation was also observed. In the
coronal and middle third the resin tags had a characteristic reverse-cone shape, while
in the apical third this morphology could only occasionally be seen. In the apical
third resin tags were often seen to only plug the tubules or were completely absent.
In Group 2, 3, and 4, some ‘globuli’ were observed (Figs. 1-2). Resin tag formation
was statistically significant different (p<0.05) between Group 1 and the other three
groups.
6.4 Discussion
Recently, several studies have reported the quantitative evaluation of morphological
observations of root canals (Ferrari et al 2001a, Ferrari et al 2001b). In this study,
RDIZ formation was evaluated calculating the entire length of RDIZ formed along
the interface between conditioned dentin and adhesive resin. Also the incidence of
resin tags was recorded from horizontal bands around the post, 1-, 4.5- and 8- mm
from the apices of the root canal preparations. In this way it was possible to
statistically analyze the data obtained from SEM observations of the four different
groups. This evaluation was performed because formation of both resin tags and
RDIZ contribute to the mechanical bonding process to the etched dentin and
consequently to the sealing process (Nakabayashi & Pashley 1998, Vichi et al.
78
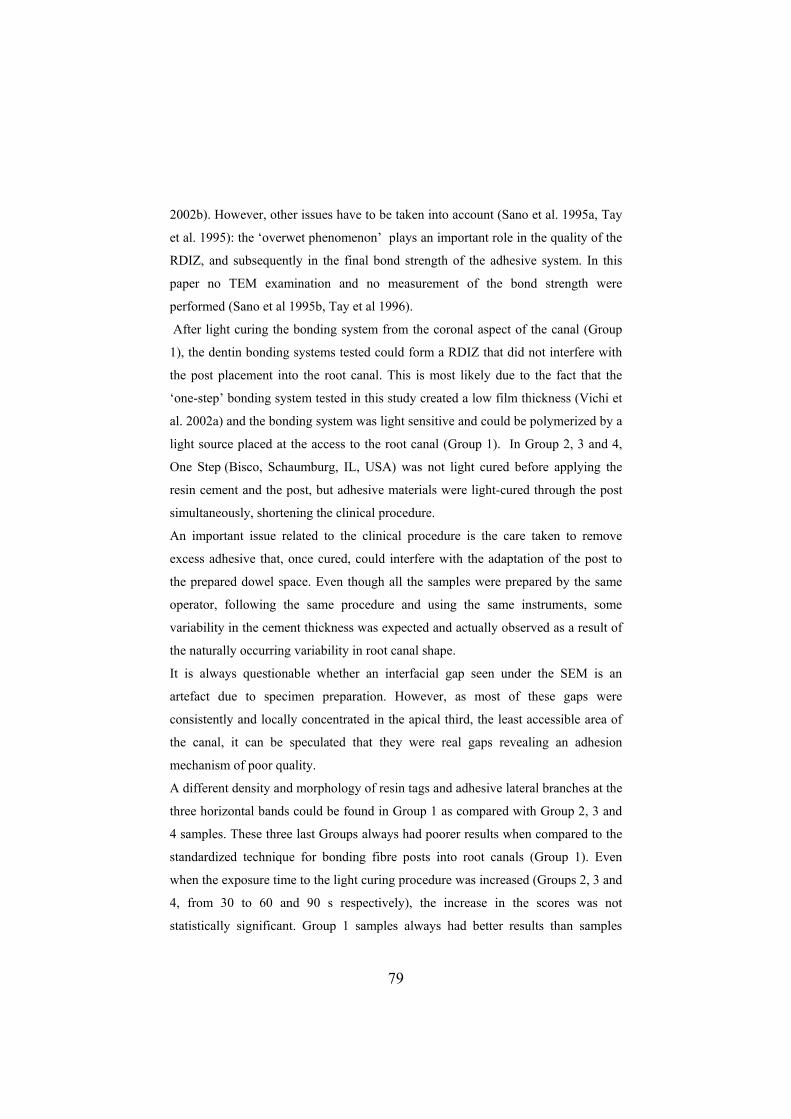
2002b). However, other issues have to be taken into account (Sano et al. 1995a, Tay
et al. 1995): the ‘overwet phenomenon’ plays an important role in the quality of the
RDIZ, and subsequently in the final bond strength of the adhesive system. In this
paper no TEM examination and no measurement of the bond strength were
performed (Sano et al 1995b, Tay et al 1996).
After light curing the bonding system from the coronal aspect of the canal (Group
1), the dentin bonding systems tested could form a RDIZ that did not interfere with
the post placement into the root canal. This is most likely due to the fact that the
‘one-step’ bonding system tested in this study created a low film thickness (Vichi et
al. 2002a) and the bonding system was light sensitive and could be polymerized by a
light source placed at the access to the root canal (Group 1). In Group 2, 3 and 4,
One Step (Bisco, Schaumburg, IL, USA) was not light cured before applying the
resin cement and the post, but adhesive materials were light-cured through the post
simultaneously, shortening the clinical procedure.
An important issue related to the clinical procedure is the care taken to remove
excess adhesive that, once cured, could interfere with the adaptation of the post to
the prepared dowel space. Even though all the samples were prepared by the same
operator, following the same procedure and using the same instruments, some
variability in the cement thickness was expected and actually observed as a result of
the naturally occurring variability in root canal shape.
It is always questionable whether an interfacial gap seen under the SEM is an
artefact due to specimen preparation. However, as most of these gaps were
consistently and locally concentrated in the apical third, the least accessible area of
the canal, it can be speculated that they were real gaps revealing an adhesion
mechanism of poor quality.
A different density and morphology of resin tags and adhesive lateral branches at the
three horizontal bands could be found in Group 1 as compared with Group 2, 3 and
4 samples. These three last Groups always had poorer results when compared to the
standardized technique for bonding fibre posts into root canals (Group 1). Even
when the exposure time to the light curing procedure was increased (Groups 2, 3 and
4, from 30 to 60 and 90 s respectively), the increase in the scores was not
statistically significant. Group 1 samples always had better results than samples
79

from the other three Groups. This may be due to a difference in the procedure, for
example, although it has been demonstrated that a proper light curing of resin
cement can be obtained in an experimental model (Boschian et al. 2001), it is
possible that light transmission through the post might not be sufficient to light-cure
the cement and the adhesive in the same step. The adhesive may be subjected to an
inadequate intensity of light and thus not be completely cured, thus leaving
‘unpolymerized’ adhesive resin. Even when increasing the light-exposure time, from
30 s (Group 2) to 60 s (Group 3) and to 90 s (group 4), uncured resin globuli were
still present. This could account for a reduction in resin tag formation and the poor
results presented in Table 4. This problem is supported by the finding of other
studies (Tay et al 1995).
Another factor affecting RDIZ and resin tag formation can be the viscosity of the
cement and its adaptation to prepared canal space. If the adhesive solution is not
light-cured before the application of the cement, a good adaptation to the root canal
walls is not achieved, and the RDIZ is not established adequately. Under these
conditions, when the cement is placed together with the post, the cement itself may
wash out the adhesive.
In all the four Groups a microbrush was used. The importance of this device in
reaching the narrowest and deepest portions of the root canal preparations has been
showed by recent findings (Ferrari et al 2001b, Vichi et al 2002b). The microbrush
is able to reach all the prepared root canal dentin, and to apply a certain pressure on
the adhesive solution, so as to maximize its penetration into the etched substrate.
This results in a deep diffusion of resin into the tubules and in the formation of
lateral branches (Chappel et al. 1994, Mjor & Nordhal 1996).
The absence of voids/bubbles at fibre post/resin cement interface could be related to
the good bond between the resin matrix of the post and that of the resin cement,
whereas the presence of voids/bubbles within the resin cement might be mainly due
to the viscosity of the resin cement and to the anatomy of the root samples. In fact,
anatomical variations of roots, the consequent variable amount of resin cement, and
its distribution into a prepared canal space could be other possible causes of void
formation. Discrepancies between root anatomy and post shape might account for
the clinical finding that the weakest point of fibre post/resin cement/adhesive
80

material/etched dentin system is the link between resin cement and the post (Ferrari
& Scotti 2002). The high percentage of voids/bubbles found in Group 2, 3 and 4
shows that several factors (light intensity, cement viscosity etc.) interfere with the
complete setting of the materials used, as compared with Group 1, where a
traditional technique was used and a lower number of voids were detected. No data
are available regarding a calculation of the percentage of light passing through the
post and reaching the apical area. However in order to improve the predictability of
the one-step technique, it would be desirable for the manufacturers to provide
translucent posts able to transmit a high intensity of light from coronal to apical
areas. Of course, the amount of light emitted by the light source is important, ideally
the light transmitted to the post should be such as to ensure an adequate degree of
polymerisation in the apical third, without resulting in an augmented polymerisation
shrinkage in the presence of unfavourable configuration factor that occurs in the root
canal (Feilzer 1987).
The microscopic observations in this study and their quantitative evaluations does
not provide information on the quality of RDIZ. It has been shown recently (Mason
2001) that collagen fibres can be denaturated in direct correlation with the time
passed after root canal treatment. In recently treated teeth a wide and dense collagen
fibre network could be noted. On the contrary, when the treatment had been
performed more than 5 years previously, the collagen fibres appeared shorter, and
their organization and uniformity was lost. This denaturation of collagen fibres can
be related to the loss of organic tissue turnover after root canal treatment.
6.5 Conclusions
The null-hypothesis tested in this study was not confirmed. The one-step (‘one-
shot’) technique, used for luting translucent fibre posts into root canal preparations
proved to be less effective than the traditional technique in forming resin tags,
adhesive lateral branches and RDIZ.
81
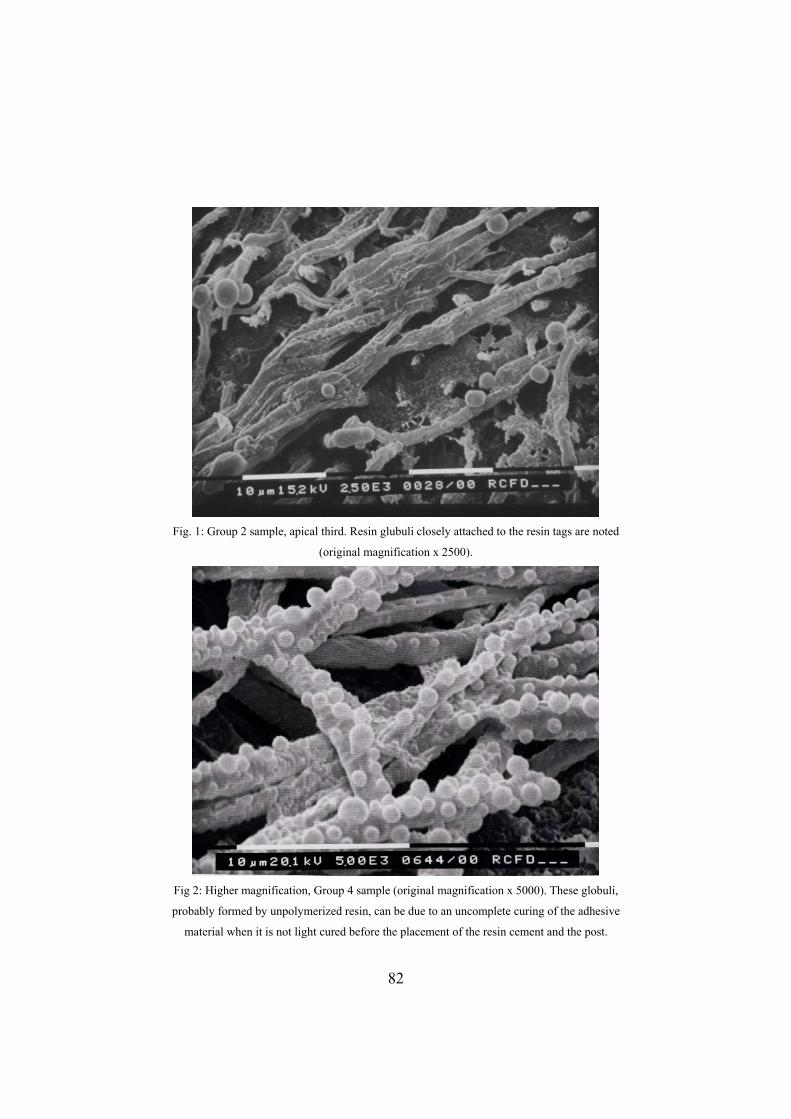
Fig. 1: Group 2 sample, apical third. Resin glubuli closely attached to the resin tags are noted
(original magnification x 2500).
Fig 2: Higher magnification, Group 4 sample (original magnification x 5000). These globuli,
probably formed by unpolymerized resin, can be due to an uncomplete curing of the adhesive
material when it is not light cured before the placement of the resin cement and the post.
82
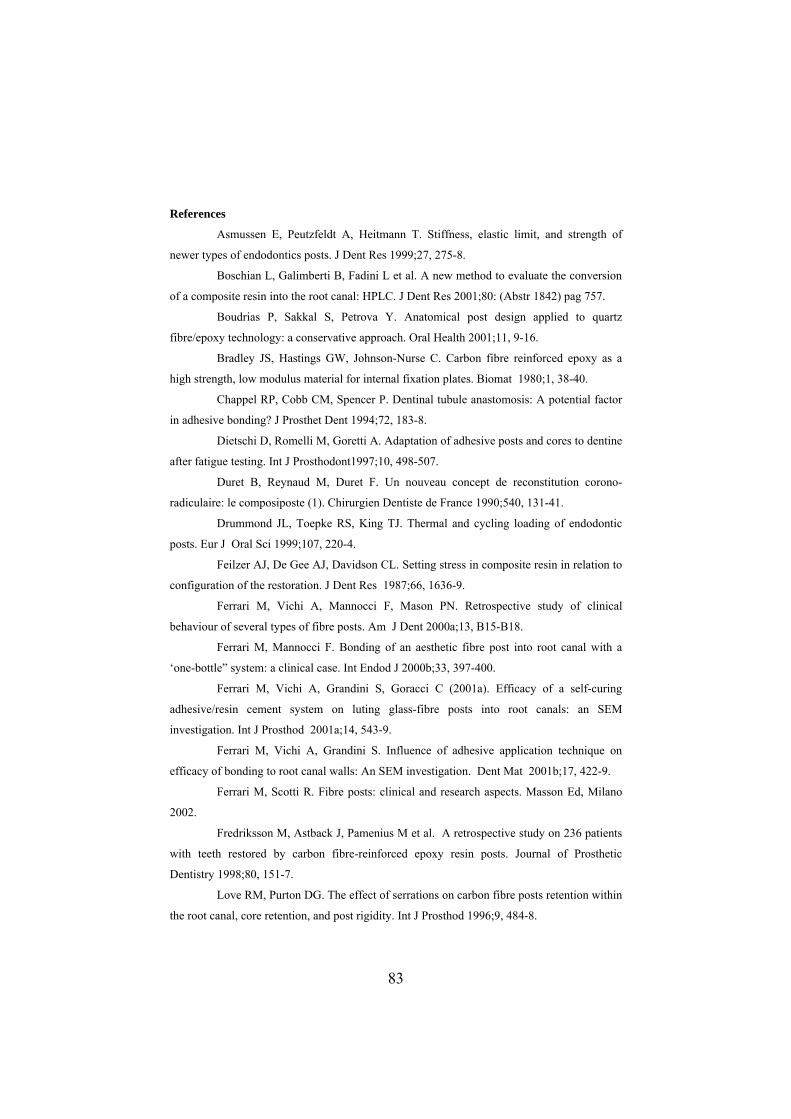
References
Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
wer types of endodontics posts. J Dent Res 1999;27, 275-8. ne
schian L, Galimberti B, Fadini L et al. A new method to evaluate the conversion
of a comp
ost design applied to quartz
bre/epo
a
potential factor
adhesiv
ntine
ter fatig
au concept de reconstitution corono-
diculair
l and cycling loading of endodontic
sts. Eu
relation to
cci F, Mason PN. Retrospective study of clinical
ehaviou
to root canal with a
y of a self-curing
hesive/
ical and research aspects. Masson Ed, Milano
02.
ry 1998;80, 151-7.
Love RM, Purton DG. The effect of serrations on carbon fibre posts retention within
the root canal, core retention, and post rigidity. Int J Prosthod 1996;9, 484-8.
Bo
osite resin into the root canal: HPLC. J Dent Res 2001;80: (Abstr 1842) pag 757.
Boudrias P, Sakkal S, Petrova Y. Anatomical p
fi xy technology: a conservative approach. Oral Health 2001;11, 9-16.
Bradley JS, Hastings GW, Johnson-Nurse C. Carbon fibre reinforced epoxy as
high strength, low modulus material for internal fixation plates. Biomat 1980;1, 38-40.
Chappel RP, Cobb CM, Spencer P. Dentinal tubule anastomosis: A
in e bonding? J Prosthet Dent 1994;72, 183-8.
Dietschi D, Romelli M, Goretti A. Adaptation of adhesive posts and cores to de
af ue testing. Int J Prosthodont1997;10, 498-507.
Duret B, Reynaud M, Duret F. Un nouve
ra e: le composiposte (1). Chirurgien Dentiste de France 1990;540, 131-41.
Drummond JL, Toepke RS, King TJ. Therma
po r J Oral Sci 1999;107, 220-4.
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in
configuration of the restoration. J Dent Res 1987;66, 1636-9.
Ferrari M, Vichi A, Manno
b r of several types of fibre posts. Am J Dent 2000a;13, B15-B18.
Ferrari M, Mannocci F. Bonding of an aesthetic fibre post in
‘one-bottle” system: a clinical case. Int Endod J 2000b;33, 397-400.
Ferrari M, Vichi A, Grandini S, Goracci C (2001a). Efficac
ad resin cement system on luting glass-fibre posts into root canals: an SEM
investigation. Int J Prosthod 2001a;14, 543-9.
Ferrari M, Vichi A, Grandini S. Influence of adhesive application technique on
efficacy of bonding to root canal walls: An SEM investigation. Dent Mat 2001b;17, 422-9.
Ferrari M, Scotti R. Fibre posts: clin
20
Fredriksson M, Astback J, Pamenius M et al. A retrospective study on 236 patients
with teeth restored by carbon fibre-reinforced epoxy resin posts. Journal of Prosthetic
Dentist
83
Lui JL. Composite resin reinforcement of flared canals using light-transmitting
posts. Quint Int 1994;25, 313-9.
Malferrari S, Baldissara P, Arcidiacono A. Translucent quartz fibre posts: a 20
emy of Dental
96). The density and branching of dentinal tubules in human
nslucent
ber po
95a;20, 160-7.
leakage within the hybrid layer. Oper Dent 1995b;20, 18-25.
ng KM, Wei SHY. Micromorphologic relationship of the
tine interface.
fibre posts under clinical conditions. Dent Mat 2002a;18,
-502.
root canal: a microscopic investigation. J Endod 2002b;28, 355-60.
months in vivo study. J Dent Res 2002;81. Special issue A, pag A-333 (Abstr 2656).
Mason PN. Bonding to root canal dentine. Transactions of Acad
Materials Meeting, Siena, 2001, pp. 65-9.
Mjor IA, Nordhal I (19
teeth. Arch Or Biol 41, 401-2.
Monticelli F, Grandini S, Goracci C, Ferrari M. Clinical behaviour of tra
fi sts and luting and restorative materials: a 2-year report. Int J Prosthod
2003;16,(6):593-6.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissue. Berlin: Quint Co.
Pubbl 1998.
Sano H, Yoshiyama M, Ebisu S, Burrow MF, Takatsu T, Ciucchi B, Carvalho R,
Pashley DH. Comparative SEM and TEM observations of nanoleakage within the hybrid
layer. Oper Dent 19
Sano H, Takatsu T, Ciucchi B, Horner JA, Matthews WG, Pashley DH (1995b).
Nanoleakage:
Scotti S, Malferrari S, Monaco C. Clinical evaluation of quartz fibre posts: a 30
months results. J Dent Res 2002;81. Special issue A, pag A-333 (Abstr 2657).
Tay FR, Gwinnett AJ, Pa
resin-dentine interface following a total-etch technique in vivo using a dentinal bonding
system. Quint Int 1995;26, 63-70.
Tay FR, Gwinnett AJ, Wei SH. The overwet phenomenon: an optical,
micromorphological study of surface moisture in the acid-conditioned, resin-den
Am J Dent 1996;9, 43-8.
Vichi A, Grandini S, Davidson CL, Ferrari M. An SEM evaluation of several
adhesive systems used for bonding
495
Vichi A, Grandini S, Ferrari M. Comparison between two clinical procedures for
bonding fibre posts into a
84

C 7 Anatomic Post: an innovative approach
hapter
hrough rapid developments in the last few years. These changes
regarded essentially three main issues: materials, radiopacity and shape. Starting
from carbon fibers, glass and quartz fiber are now widely used, and the addition of
strontium to the resin components radiopaque fiber posts are now available. The
optical property of translucency has also been appreciated by clinicians, allowing the
use of dual-curing resin cements for luting purposes. Interestingly, starting from the
double-cylinder shape, endodontic shapes and then double tapered shapes were
presented, as the adhesive cementation now relies more on formation of resin dentin
interdiffusion zone and resin tags rather than on the good fitting and mechanical
retention of the post inside the root canal (Ferrari et al 2002). It is a clinical evidence
to encounter debondings, of the post or of the core, during temporary phase (Ferrari
et al 2000). An excess thickness of the cement, especially at the coronal level, can
generally be regarded as the main cause. As a matter of fact it is pretty common to
face root canals that are not perfectly round after endodontic instrumentation. This
chapter presents an in vitro and an in vivo study regarding the very last brand of
fiber post available (Anatomic Post’n Core, RTD, St Egrève, France), that is able to
reduce the cement thickness and to immediately restore the coronal portion in cases
where the root canal is not round and a huge loss of tooth structure is present.
7.1 SEM evaluation of the cement layer thickness after the luting procedures of
two different posts
The increasing popularity and wide-spreading use of fiber posts is inevitably
changing the procedure of reconstructing endodontically treated teeth. Since fiber
posts introduction in 1990 (Duret et al 1990), many investigations have confirmed
the good clinical performance of the system adhesive- resin cement- fiber post
(Ferrari et al 2000a, fredriksson et al 1998) due to its good retention value Asmussen
et al 1999, Drummond et al 1999) and low stressing behaviour (Rengo et al 1999).
The evolution of fiber posts has received an acceleration since Carbon and quartz
fiber posts have been replaced by glass fiber posts that are translucent and often
radiopaque. Also the shape of these posts have changed: from a double-cylinder,
Fibre posts went t
85

thus designed for retention purposes, cylindrical (Endopost) and conic profiles (DT
osts) have been developed, based on the good performances of the new bonding
is
asier than that of any kind of metallic posts (de Rijk et al 2000), thus offering the
ule effect’, or in the presence of a too thick layer of cement
p
p
procedures (Kurtz et al 2002).
The property of translucency reveals favourable for luting purposes, as the
transmission of light through the post allows the clinician to use also dual-cure
cements (Grandini et al 2003, Sawada et al 2002). Moreover, the wider choice of
available shapes permits to limit the amount of residual dentin that has to be
removed in order to achieve a satisfactory post adaptation.
Furthermore, the translucent fiber post has a modulus of elasticity similar to that of
dentin and of the other posts, and has indeed given proof of adequate mechanical
properties (Drummond et al 1999). The use of ‘one-bottle’ adhesive systems has
greatly simplified the procedure of bonding also into root canals, and has proved to
be clinically adequate (Ferrari et al 2001a and 2001b), especially when a
microbrush, in the place of a regular brush, is employed as a carrier of the adhesive
and the resin cement inside the root canal (Ferrari et al 2001b).
Clinical studies (Fredriksson et al 1998, Malferrari et al 2002, Scotti et al 2002) have
revealed that when using fiber posts, the most common cause of failure is not root
fracture, as it happens with metallic or cast posts, but debonding. Also endodontic
failure is an important issue (Tronstad et al 2000), and a reliable predictor of the
success rate of many kind of reconstructions; although the removal of a fiber post
e
clinician a chance of retreatment. Debonding is more likely to occur in the absence
of the desirable ‘fer
(Ferrari et al 2000a). In particular, if the post is not well fitting, especially at the
coronal level, the cement layer ends up being too thick, and bubbles are likely to be
present within it, all this predisposing to a debonding.
Clinically, when debonding occurs, the post often appears lined by cement still
adhering to it. In this case it is possible to lute again this cement-relined post, which
is now “anatomic”. This individual post, shaped to the root canal space ends u
having a better fit than any other prefabricated post (Ferrari et al 2000a).
This opportunity is particularly appreciated when dealing with root canals which
have an elliptic shape, such as canines, lower premolars etc. In these cases the
86

clinician is forced to adapt the residual root structure to the post shape, through the
removal of a further amount of dentin. On the contrary, it would be desirable that the
post adapt to the root canal anatomy as produced by the endodontic treatment. This
ini et al 2003). This way
ricated them with a
nesses were present when
analyzed
is indeed the rationale for the creation of an anatomic post (Boudrias et al 2001a and
2001b).
It goes back to two years ago the first documented attempt to make anatomic posts
by relining a quartz post with self-curing resin and a translucent post with light-
curing resin (Boudrias et al 2001a, Ferrari et al 2002, Grand
the authors were able to achieve a better adaptation of the post to the residual root
canal anatomy. Recently the Anatomic Post’n Core (RTD, St Egrève, France) has
been introduced (Ferrari et al 2002) . This new post is made by a DT post n. 1a that
is covered by a light-curing resin (Lumiglass, RTD, St Egrève, France).
The clinical procedure for the use of this post starts with the fitting of the Anatomic
post (post plus resin) into the root canal, after having eliminated with a drill all the
possibly present undercuts from the canal walls, and having lub
glycerine gel. When the anatomic post is introduced into the root canal, the resin
surrounding the post is able to reline the post itself, thus creating a new post whose
adaptation is expected to be better than that of any prefabricated post. A twenty-
second light-curing through the post allows the resin surrounding the post to set,
then the Anatomic post is removed and fully light cured for other twenty seconds.
Now the post has to be tried in, to make sure that no interference exists to its easy
placement. At this point the usual procedure for luting a translucent post can be
followed.
Aim of this study was indeed to evaluate the resin cement thickness after luting
anatomic posts and standardized fiber posts into root canal preparations.
The null hypothesis that similar resin cement thick
anatomic or standardized posts were used was evaluated.
In addition, the presence of voids and/or bubbles within the luting material or at the
interface between the cavity walls and the post was verified, and the uniformity and
morphologic characteristics of the resin-dentin interdiffusion zone were
under a scanning electron microscope, as parameters usually assessed when judging
87

the quality of the adhesion of the post inside the canal (Chappel et al 1994, Ferrari et
al 2001b, Mason et al 2001, Mjor et al 1996, Nakabayashi et al 1998).
7.1.1 Materials and Methods
Twenty upper anterior teeth, extracted for periodontal problems, were selected for
cturer. Excess primer-adhesive solution was removed with a paper point,
was used.
d into the root canal space
diameter, 08 % conicity; DT3, 90 tip diameter, 06 % conicity). The choice between
this study. The teeth were endodontically instrumented at a working length of 1 mm
from the apex to a #35 master apical file. A step-back technique was used with
stainless-steel K-files (Union Broach, New York, NY, USA), gates Glidden drills #2
to #4 (Union Broach, New York, NY, USA), and a 2.5% sodium hypochlorite
irrigation. The prepared teeth were obturated with thermoplasticized, injectable
gutta-percha (Obtura, Texceed Corp., Costa Mesa, CA, USA) and a resin sealer
(AH-26, DeTrey, Zurich, Switzerland).
The root canal walls of each specimen were enlarged with low-speed drills provided
by the manufacturer (RTD, St Egrève, France), and the depth of the post space
preparation was 9 mm from the cementum-enamel junction. The sample was
randomly divided into two groups of ten specimens each.
Group 1: The first ten specimens were treated with the One Step bonding system
(Bisco, Shaumburg, Il, USA), following manufacturer’s instructions. The root canal
walls were etched with 32% phosphoric acid (Bisco, Shaumburg, Il, USA) for 15
seconds, washed with a water syringe, and then gently air-dried. Excess water was
removed from the post space using paper points. Four to five coats of primer-
adhesive material were applied into the root canals with a microbrush provided by
the manufa
the remaining material was gently air-dried, and then light-cured for 20 seconds.
Duo-Link (Bisco, Shaumburg, Il, USA), a new dual-cure resin cement
The catalyst and base components of the material were mixed according to the
manufacturer’s instructions. The resin cement was applie
with a lentulo drill, and the fiber post was seated. The excess resin was removed and
the remaining material light-cured for 20 seconds through the post.
The DT translucent fiber posts (RTD, St Egrève, France) were used. They were
available in three different sizes (DT1, 120 tip diameter, 10% conicity; DT2, 100 tip
88

them was dictated by the size and the shape of the roots, the objective being the
achievement of a good fit of the post at the apical portion of the canal. The length of
ach post was controlled and the post was properly cut before luting.
ens were used for testing ‘experimental anatomic
h involved phosphoric acid etching of root
of the tooth, by means of
were aligned to
e
Group 2: The other ten specim
posts (RTD, St Egrève, France)’, following manufacturer’s instructions (Fig 1).
After lubricating the canal walls with a glycerin gel, the anatomic post was fitted
into the root preparation, and irradiated by the curing light for 20 seconds. Then the
post was removed and fully light-cured for other 20 seconds. The post was tried in
the root canal again, in order to check for its easy insertion, without any
interference. An abundant rinsing was performed to remove the excess of the
lubricant gel. Finally, the post was luted following the same technique already
described for Group 1 specimens, whic
canals, followed by the application of the One-Step adhesive system, and of the
Duo-Link resin cement.
The sample teeth were stored in a water solution at room temperature. A week later,
the root specimens were sectioned parallel to the long axis
a diamond saw (Isomet, Buhler, Lake Bluff, NY, USA).
7.1.1.1 Resin cement thickness
The sections were gently decalcified (32% phosphoric acid was applied for 30
seconds, then the sample was washed and gently air-dried) and deproteinized (the
sample was immersed in a 2% sodium hypochlorite solution for 120 seconds), in
order to clean the surface from any debris.
Specimens were at this point dehydrated with alcohol, sputter-coated with gold
(Edwards Ltd., London, UK), and observed under a scanning electron microscope
(Philips 515, Philips Co., Amsterdam, The Netherlands) at different standardized
magnifications (x250, x500, x2300 and x4580 for resin tags; x625 and x1310 for
resin dentin interdiffusion zone).
Serial SEM photomicrographs of the canal walls were taken at the 1-, 4.5- and 8-
mm levels (x500 magnification) (Fig. 2). The photomicrographs
form a continuous horizontal examination strip at the three levels. Irrespective of the
number of photomicrographs needed to form a complete strip, each strip was
89

subdivided into eight “assessment units”. In each assessment unit two distinct
operators in double blind evaluated the following aspects:
1. Resin cement thickness at the three different levels.
2. Presence or absence of gaps: a. Inside the resin cement, b. Between the dentinal
walls and resin cement, c. Between the resin cement and the post.
The differences in the cement layer thickness surrounding the two types of posts at
each of the three root canal levels were tested for statistical significance (t-Test,
p=0.05). Also, within the same group of samples and therefore for each type of post,
the differences among the cement layer thicknesses measured at the three checked
levels of the root canal were evaluated statistically (One-Way ANOVA, p=0.05).
Additionally, the Fisher’s Exact test was applied to check for statistical significance
of the differences in frequency of defects between the two experimental groups
(p>0.05).
7.1.2 Results
The cement thickness measured in microns in the two groups of specimens is
reported in Table I. Table I: Mean and standard deviation values of resin cement thickness (in µm) recorded at 1-,
4.5-, and 8 mm levels. The values labeled by the same letter were not significantly different.
Group 1mm level
(Coronal third)
4.5mm level
(Middle third)
8mm level
(Apical third)
1. control 610±67d 240±2 c b1.6 130±10.4
2. anatomic posts 20±2a 40±3.6a 100±8.2b
It can be noted that the resin cement thickness decreases from the apical to the
coronal level in the anatomic samples, while the opposite happens in the control
group (Figs. 3 and 4).
In Group 2 the highest thickness of cement (around 100 microns) was seen at the
margin between the coronal portion of the anatomic post and the resin composite
abutment (Fig. 5).
90

Statistically significant differences in cement thickness were found between the two
groups of specimens at the coronal and the middle level of the canal (p<0.05). Also,
the three different levels
t the coronal and
long the root canal preparation
Within resin cement Post/resin material Dentinal walls/cement
within the same group of specimens, cement thicknesses at
of observation were significantly different (p<0.05). Only in the presence of
anatomic posts, were similar thicknesses of cement measured a
middle third of the canal (Fig. 6) (Table I).
A good adaptation of the fiber post, relining material, luting material and residual
dentin could be noted (Fig. 7).
Often voids and bubbles were detected within the resin cement (Table II), as well as
within the abutment in both groups of specimens (Table III). Also, voids and
bubbles were noted between the fiber post and the resin material. Table II: Number of samples in which presence of gaps/voids/bubbles within resin cements
was noted a
Group 1 5 / 3
Group 2 1 1 /
Table III: Number of samples in which presence of gaps/voids/bubbles within the abutment
ed.
mate mater
was not
Within resin rial Post/resin ial
Group 1 8 3
Group 2 9 2
Occasionally, gaps of different extension were observed between the resin
composite relining material and the fiber post (Table II).
The differences in frequency of defects between the two experimental groups were
not statistically significant (p>0.05).
91

7.1.3 Discussion
SEM observations allow for a high resolution assessment of the conditions of
adhesion. The morphologic characteristics of the adhesive interface, as revealed by
scanning electron microscopy, can be evaluated through either a qualitative or a
quantitative analysis. The latter is usually preferable, as it provides a repeatable
method. For this reason, in the present study it was chosen to follow a recently
quency of structural discontinuities in the adhesive
i et al 1998, Vichi
dentin interdiffusion zone (Sano et al 1995,
Tay et al 1995). H S R y
to the qu ty of the adhesion, it eventually gives q ntitative information
on its uniform formation.
Th l steps eeded to create the anatomic post hav n described. The
que is relatively easy, and adding only few more actions to those required to
to considerably reduce the thickness of the cement layer, within which
the development of vo l
The expected advantages of this technique c be listed as follows: as a result of the
relining, the thickness of the cement layer is lower and constant; the formation of
bu oids, repr ing areas of weak ss within the material, is less likely in
thin and uniform layer of cement; the polymerization stress that develops within a
ent, being conic-shaped or
ing to adapt the root canal to the standardized
ost (Grandini et al 2003). Of course these advantages must be verified by further
udies as no statistically significant differences were evident between the two
roups.
proposed quantitative analysis (Ferrari et al 2001b), for the evaluation of cement
thickness, as well as of the fre
interface, such as bubbles, voids or gaps. This evaluation was performed because
formation of both resin tags and RDIZ contribute to creating a proper mechanical
bonding to etched dentin and consequently sealing it (Nakabayash
et al 2002a). TEM examination and measurement of the bond strength are the best
way to assess the quality of the resin-
owever, even if the EM evaluation of DIZ is not the best wa
measure ali ua
e clinica n e bee
techni
bond a regular translucent fiber post, allows to achieve a superior quality of the
fitting, and
ids or bubbles is less ikely.
an
bbles or v esent ne
a
low-thickness film of cement is minimal; furthermore, from a clinical point of view,
in a root canal that ends up, after the endodontic treatm
not perfectly round, the possibility of relining the Anatomic post is appreciated: the
post adapts to the canal instead of try
p
st
g
92
In comparison with metallic posts, the anatomic post offers the same advantages as
ity sufficient to induce polymerization (Boschian et al
ntific data that will answer the
all of the other fiber posts, including the fact that, in case endodontic retreatment is
needed, a fiber post is more quickly and easily removed than a metallic post
(Tronstad et al 2000). Also the considerations regarding chair-time and costs
required by the two compared procedures for restoring endodontically treated teeth
tend to tip the balance in favor of fiber posts, as the use of these, differently from
cast posts, allow to bond the post and build the core in only one visit, without any
laboratory phase and fee.
Whether a light-curing cement can be adequate for luting fiber posts or it is safer to
resort to a dual-cure material is still debated in the literature, the heart of the issue
being light transmission through the post. In other words, according to some Authors
the amount of light that, passing through the post, gets to the apical portion of the
post is not enough to adequately cure a light-activated resin cement (Rovatti et al
2001). Some other researchers, on the other hand, state that transmission through a
translucent post is efficient enough to allow also the apical portion of the post to be
reached by a light intens
2001).
As far as the anatomic post is concerned, the issue of light transmission through its
relining resin has still to be investigated. The question whether light absorption
through the relining resin may negatively affect the polymerization process of the
cement can in fact be raised. In the wait for scie
question, it remains safer and advisable to use a dual-curing resin cement for luting
anatomic posts.
Just like all of the resin-based materials, also the relining resin surrounding the
anatomic post shrinks as it cures. Although this aspect needs further evaluation,
however, it logically seems that the shrinkage should favor the extrusion of the
anatomic post from the canal after its relining.
The quality of the adhesion between the post and the relining resin appeared good in
all of the SEM views. This may be due to the compatibility between the two
materials, which have the same matrix components, as well as to the addition of a
coupling agent (silane) at the interface between the post and the relining resin.
93

Regarding the wider thickness of the resin cement layer found with the standardized
post, the references from the literature do not give a certain answer. Some clinical
works, perspective or retrospective studies (Ferrari et al 2000a, Fredriksson et al
1998, Malferrari et al 2002, Scotti et al 2002), show that debonding occurs when a
thicker cement layer is present. In this sense it can be assumed that a more precise
fitting obtained with the anatomic post can improve this aspect, even if a further
clinical control study is needed to confirm this aspect.
The null-hypothesis tested in the study was not confirmed. The resin cement
pe of fibers (from carbon to quartz, to glass), as well as the shape of
at variety of shapes (Asmussen et al
thickness was significantly lower in the ‘anatomic post’ group than in the control
group (standardized posts), except at the apical third of the canal, where there was
no statistically significant difference. Although there is no scientific evidence that a
thinner layer of cement can improve the quality of the luting procedure, a good
adaptation of anatomic posts was evident in all of the specimens, allowing the post
to stand still during the luting procedures .
The clinical procedure to make an anatomic post was effective and easy to perform.
7.2 Use of Anatomic Post’n Core for reconstructing an endodontically treated
tooth: a case report.
The introduction of fiber posts has had a great impact on the clinical procedures to
restore endodontically treated teeth. Since their début at the beginning of the 90’s
(Duret et al 1990), the research behind these products has continuously worked on
modifying the ty
the posts. The evolution in the technology has enabled the manufacturers to provide
today fiber posts that, beside offering superior esthetic and mechanical properties,
which had been the first qualities to be appreciated in comparison with metal or cast
posts, are also radiopaque and available in a gre
1999, Asmussen et al 1999, Fredriksson et al 1998). The growing popularity of fiber
posts witnesses their clinical success, and the results of longitudinal trials (Ferrari et
al 2000, Malferrari et al 2002, Scotti et al 2002, Fredriksson et al 1998) confirm
their reliability.
94

As regards in particular the shape of the posts, the evolution has gone from the
double-cylinder of the carbon posts, thus designed for retention purposes, to the
cylindrical or the conic profile of the Endoposts and DT posts respectively. These
latter designs are meant for a better adaptation of the post to the canal anatomy, thus
minimizing the amount of residual root structure that has to be sacrificed in order to
get the post to fit. Obviously, this trend toward more and more conservative root
preparations for post adaptation has been possible only thanks to the contemporary
ugh its insertion into the canal, with the
t al 2000, Ferrari et al 2002a). As a result of its precise adaptation to the root canal
ace, the relined post is going to be surrounded by a thin and uniform layer of resin
ividualizing’ the post through its relining, although advisable
n fracture with extensive pulp exposure on teeth 1.1 and 2.1, and
an enamel-dentinal fracture without pulp exposure on tooth 2.2. After clinical and
progress in the field of materials and techniques for bonding, that has made adhesion
to root canal walls safer and more predictable (Ferrari et al 2001a, 2001b and 2002b,
Mason 2001, Mjor et al 1996).
It is likely that a further significant improvement in fiber posts adaptation and
retention will be achieved with the so-called ‘anatomic post’. This is a translucent
fiber post covered by a layer of light-curing resin (Anatomic Post’n Core. RTD),
which allows for a relining of the post thro
aim of achieving a better fit than that possible with any prefabricated post (Grandini
e
sp
cement, which creates ideal conditions for post retention (Boudrias et al 2001).
The procedure of ‘ind
in all cases, appears to be particularly effective for the purpose of improving post
retention when dealing with canals of elliptic shape, or exhibiting a reduced amount
of residual root structure after endodontic treatment; this latter situation obviously
contraindicates a further removal of dentin to make the canal shape match the post
shape. The creation of an ‘anatomic post’, involving the opposite adaptation, that is
shaping the post to the root anatomy, is the procedure of choice in these clinical
situations, of which the described case is an example.
7.2.1 Case report
A nine-year old patient comes to the office two days after having hit his front teeth
as a result of falling down while playing in the school gym. The trauma caused a
complicated crow
95

x-ray examination, it was decided to endodontically treat teeth 1.1 and 2.1, and to
restore all the teeth with resin composites, waiting for the adequate time to perform
a prosthetic treatment. The root canal treatments were done, and tooth 1.1 was
restored with a direct resin composite restoration (Figs. 8 and 9). On tooth 2.1, the
root canal anatomy after endodontic treatment was such that no prefabricated post
could satisfactorily adapt to it (Fig. 10); on the other hand, the amount of residual
dentin on the canal walls was such as to contraindicate the further removal of tissue,
to make the canal shape adapt to that of the post. It was then decided to use for tooth
2.1 an ‘anatomic post’. The procedure started with removing by means of a drill any
undercut still possibly present on the canal walls, which were then lubricated with
was
ss of material removed before
ght-curing for 40 seconds through the post (Fig 14). Due to the young age of the
ded to avoid the immediate preparation for a prosthetic crown.
glycerine. At this point the anatomic post’n core was inserted (Fig 11) and light
cured for 20 seconds (Fig 12). Then the anatomic post was gently pulled out of the
canal, and an additional 20-second light curing was performed in order to
completely polymerize the relining resin (Fig 13). The anatomic post was tried in
again, in order to check for its easy insertion, without any interference. At this point
a luting procedure was performed similar to that recommended for a regular
translucent post. The root canal walls were etched with 32% phosphoric acid (Bisco)
for 15 seconds, washed with a water syringe and gently air-dried. Excess water
removed from the post space using paper points (Mynol). Four to five coats of the
One Step bonding system (Bisco) were applied into the root canals with a
microbrush provided by the manufacturer. The excess primer-adhesive solution was
removed with a paper point (Mynol), gently air-dried, and then light-cured for 20
seconds. Dual Link (Bisco), a new dual-cure resin cement was used for luting. The
catalyst and base components of the material were mixed and applied following
manufacturer’s instructions. The resin cement was carried into the root canal space
with a lentulo drill, the post was seated, and the exce
li
patient, it was deci
The anatomic post was therefore simply used as a base for a direct composite
restoration (Fig. 15). The prepared tooth was etched with 32 % phosphoric acid
(Bisco) (Fig. 16); then, the One step adhesive system (Bisco) was applied as
96

recommended by the manufacturer (Fig 17), and the restoration was completed with
a microhybrid resin composite material (Micronew, Bisco) (Figs. 18, 19 and 20).
7.2.2 Discussion
The observation of a residual root canal shape after endodontic treatment which is
not perfectly round is not so uncommon (Davis et al 1972, Walton et al 1996). This
case is a suitable situation for using the Anatomic post. In fact, in the attempt to
place a regular fiber post in a thus shaped canal, one would be forced to round up the
canal walls with burs, thus sacrificing a conspicuous amount of the residual tissue,
or would end up applying a thick layer of cement, to fill up the spaces between the
loosely fitting post and the canal walls. The latter is a predisposing situation to
failure of the adhesion and debonding of the post (Ferrari et al 2000). On the other
hand, a post relined to closely match the shape of the canal will be surrounded by a
thin and uniform film of cement, which represents an ideal situation for retention
purposes.
In addition, the technique of the anatomic post allows to perform a direct restoration
on an ‘individual’ post in only one visit and without the laboratory involvement,
whereas the classic post and core system, direct or indirect, requires at least two
visits and a laboratory phase. This opportunity is particularly appreciated in a case
like the one described, where the young age of the patient calls for a treatment to be
completed in few visits, each one as quick and easy as possible.
On the other hand, if a prosthetic restoration is planned for the endodontically
treated tooth, it is possible to immediately build up on the anatomic post a resin
composite core, which in the same visit can be prepared for prosthetic purposes.
From a clinical point of view, it appears that the step of creating an individual post
by letting the surrounding resin reline it according to the canal shape, adding only
five minutes of chair-time to the standard procedure for luting a translucent post, can
greatly improve post adaptation and retention. A study involving both an in vivo trial
and a SEM evaluation of the quality of adhesion is already available (Grandini et al
2004), with the aim of providing some more scientific support to the positive clinical
impression.
97

7.2.3 Conclusions
The clinical procedure of the Anatomic post can be used for reconstructing an
ndodontically treated tooth when the resulting anatomy of the root canal walls is
, and when there’s an important loss of substance at the coronal
e
not perfectly round
level. This way it is possible to obtain a superior fitting of the individual anatomic
post, as compared with any other prefabricated fiber post.
98
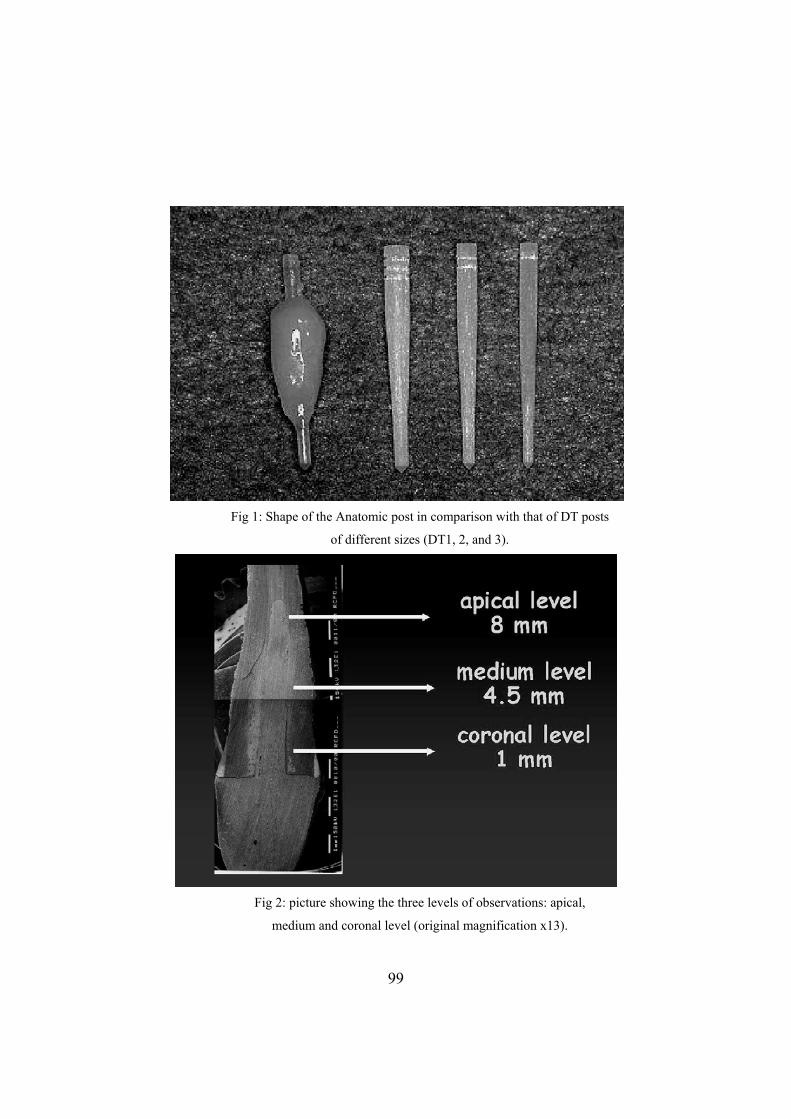
Fig 1: Shape of the Anatomic post in comparison with that of DT posts
of different sizes (DT1, 2, and 3).
Fig 2: picture showing the three levels of observations: apical,
medium and coronal level (original magnification x13).
99
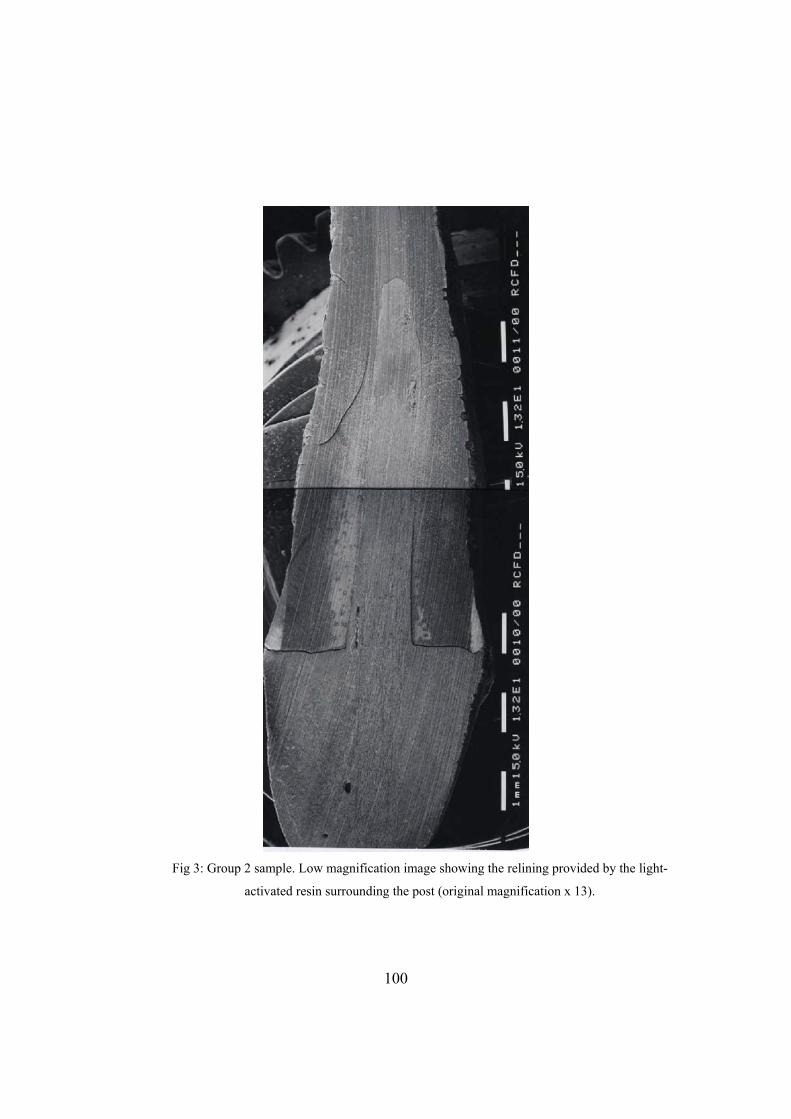
Fig 3: Group 2 sample. Low magnification image showing the relining provided by the light-
activated resin surrounding the post (original magnification x 13).
100
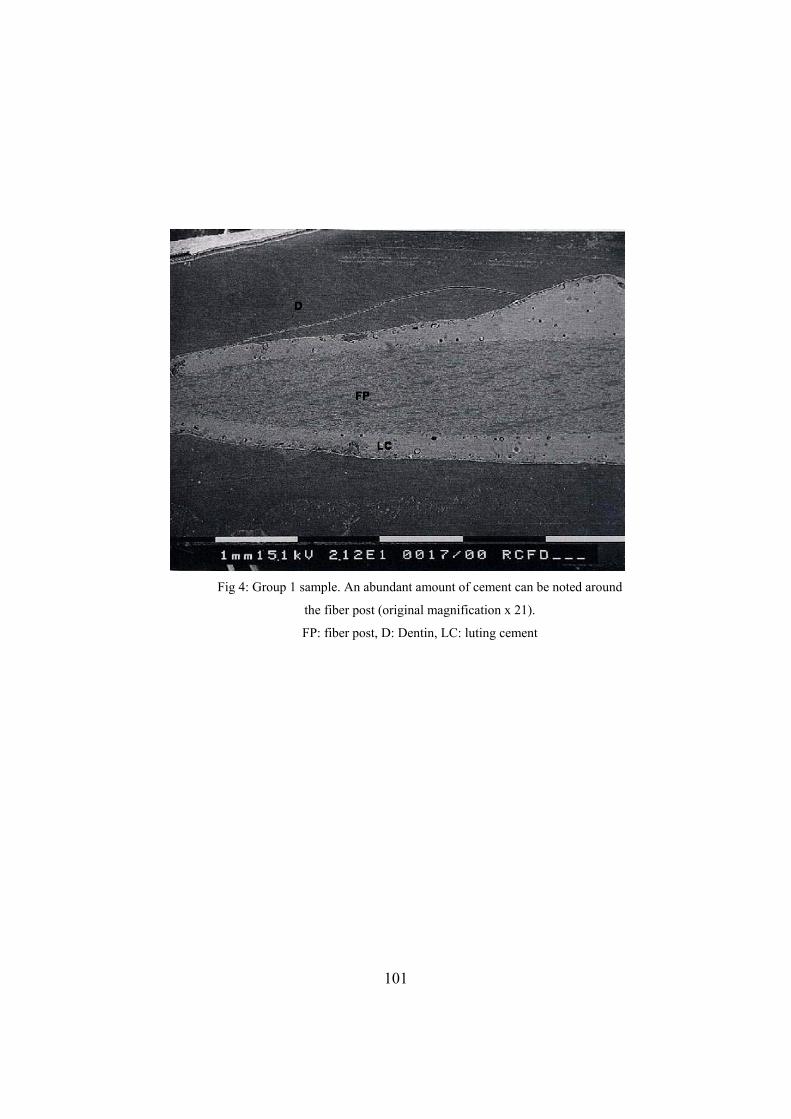
Fig 4: Group 1 sample. An abundant amount of cement can be noted around
the fiber post (original magnification x 21).
FP: fiber post, D: Dentin, LC: luting cement
101
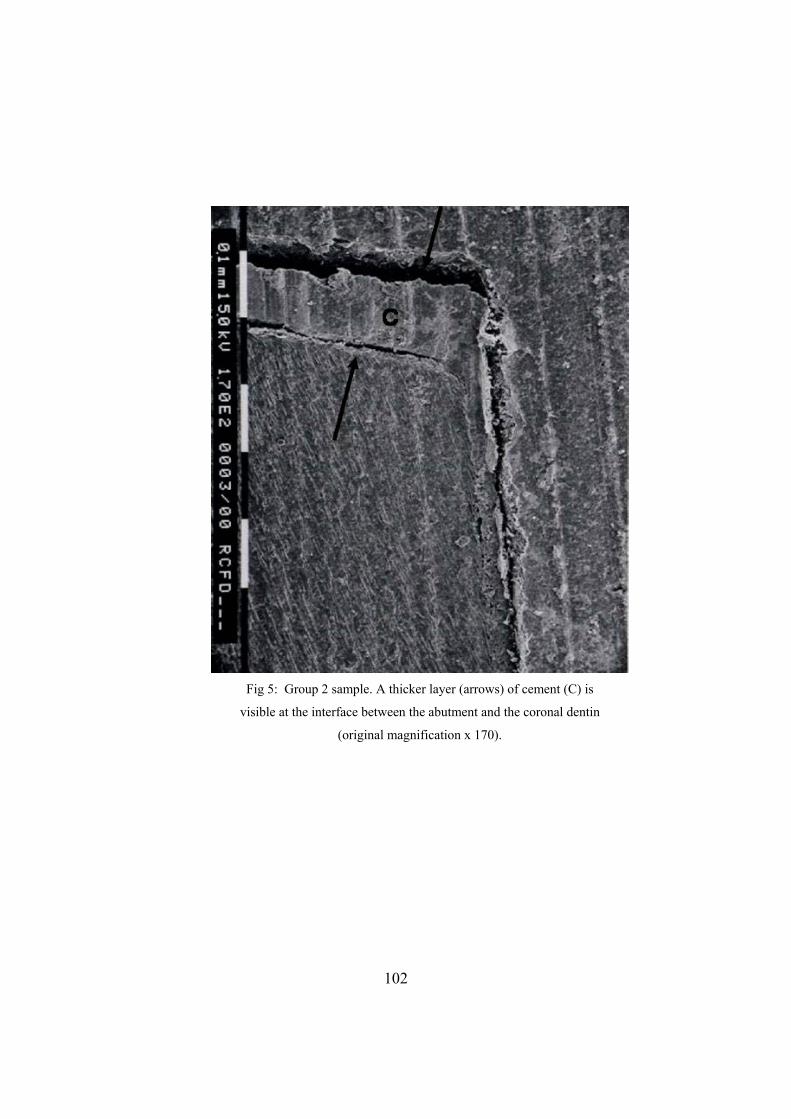
Fig 5: Group 2 sample. A thicker layer (arrows) of cement (C) is
visible at the interface between the abutment and the coronal dentin
(original magnification x 170).
102
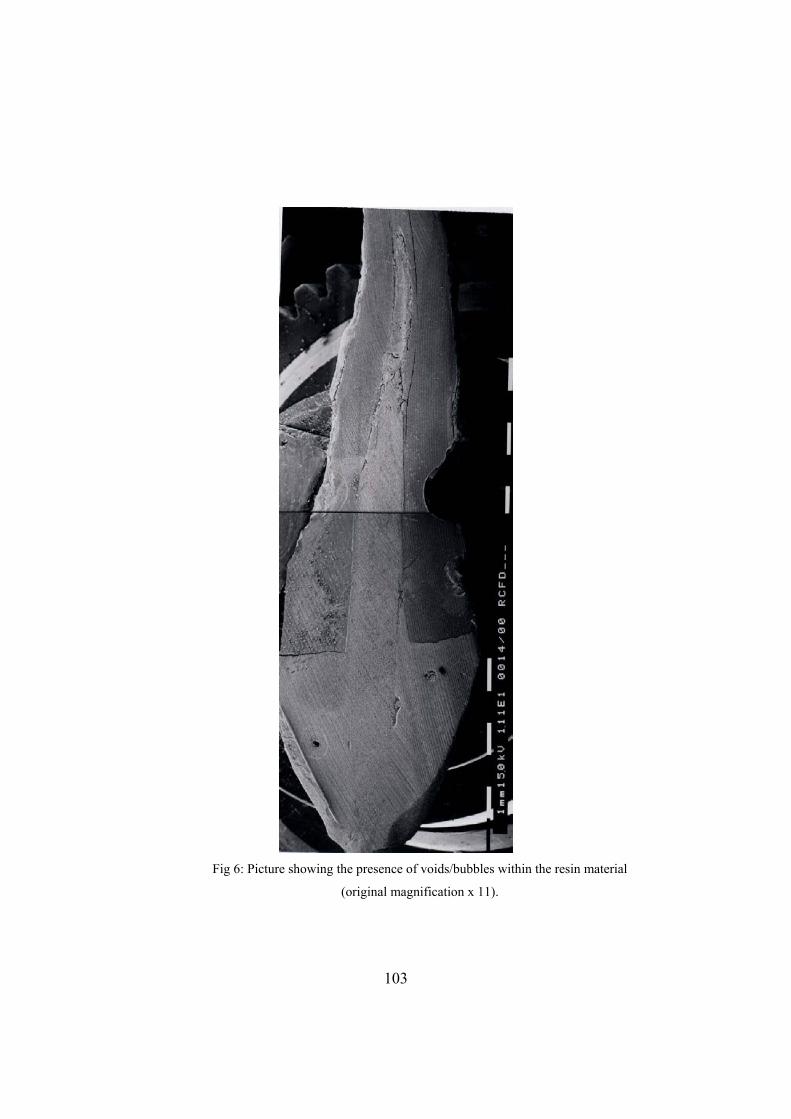
Fig 6: Picture showing the presence of voids/bubbles within the resin material
(original magnification x 11).
103

Fig 7: High magnification picture showing the good quality of the adhesion
between relining material (RM), luting material (between arrows) and root canal
dentin (D) (original magnification x 356).
104
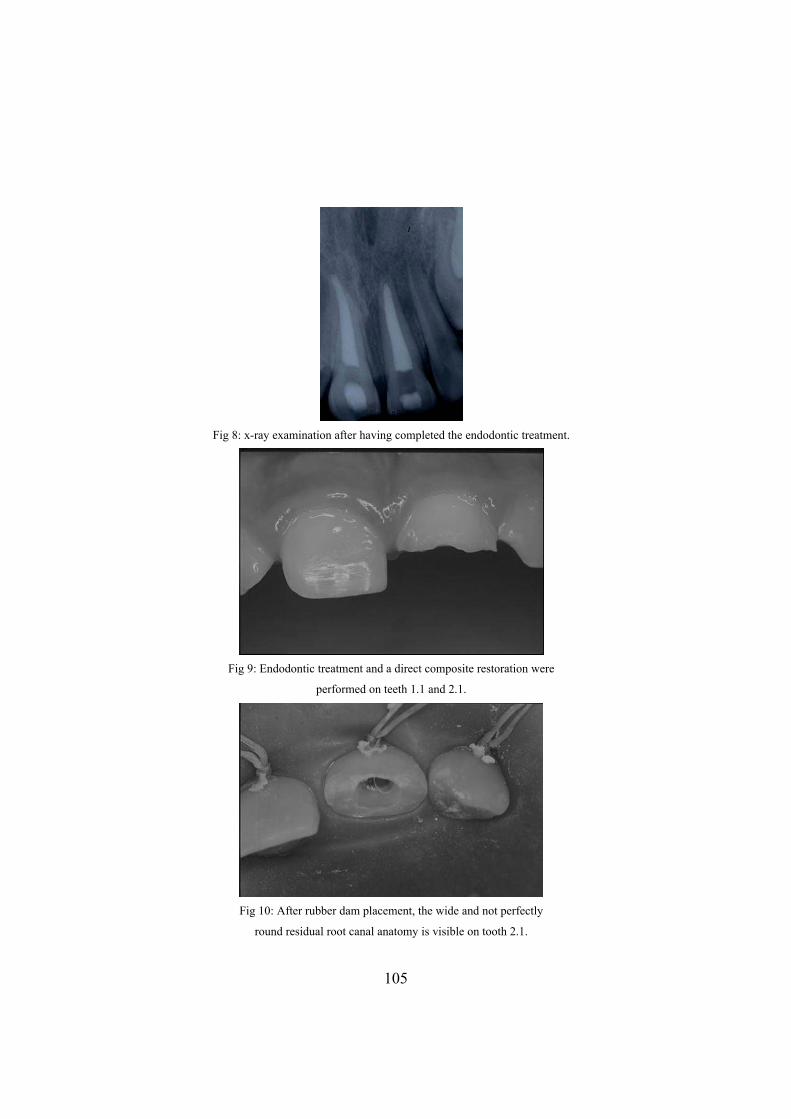
Fig 8: x-ray examination after having completed the endodontic treatment.
Fig 9: Endodontic treatment and a direct composite restoration were
performed on teeth 1.1 and 2.1.
Fig 10: After rubber dam placement, the wide and not perfectly
round residual root canal anatomy is visible on tooth 2.1.
105
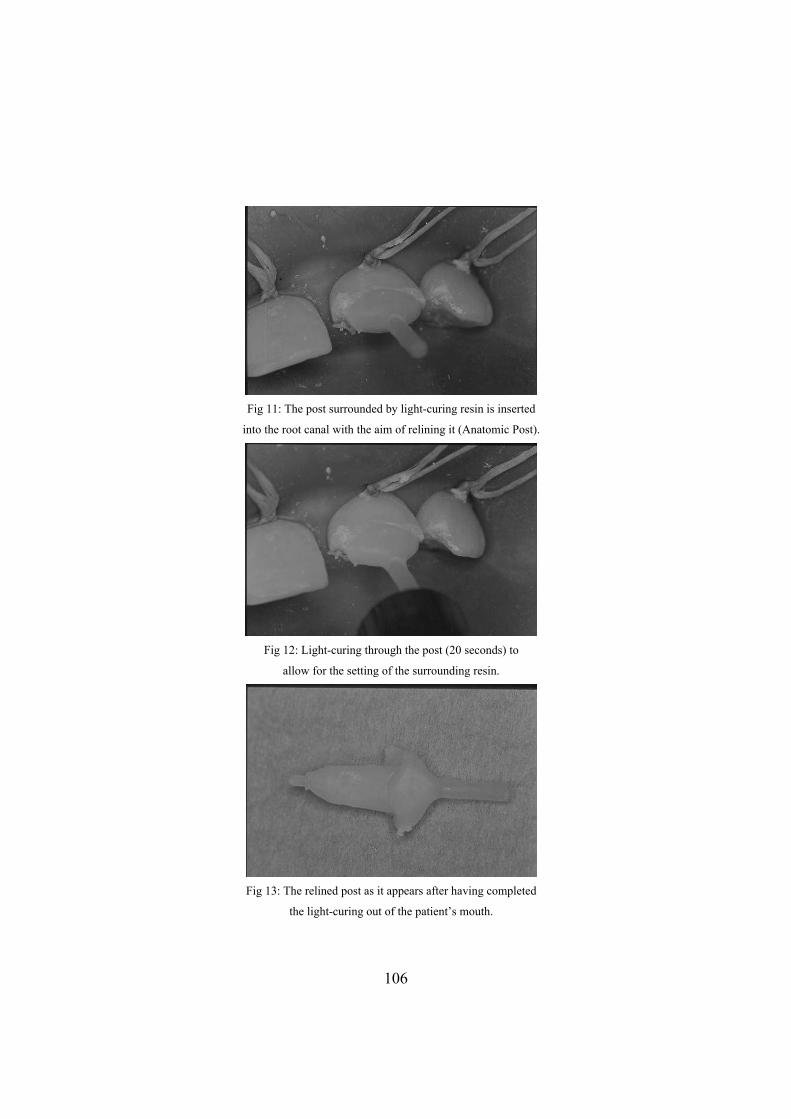
Fig 11: The post surrounded by light-curing resin is inserted
into the root canal with the aim of relining it (Anatomic Post).
Fig 12: Light-curing through the post (20 seconds) to
allow for the setting of the surrounding resin.
Fig 13: The relined post as it appears after having completed
the light-curing out of the patient’s mouth.
106
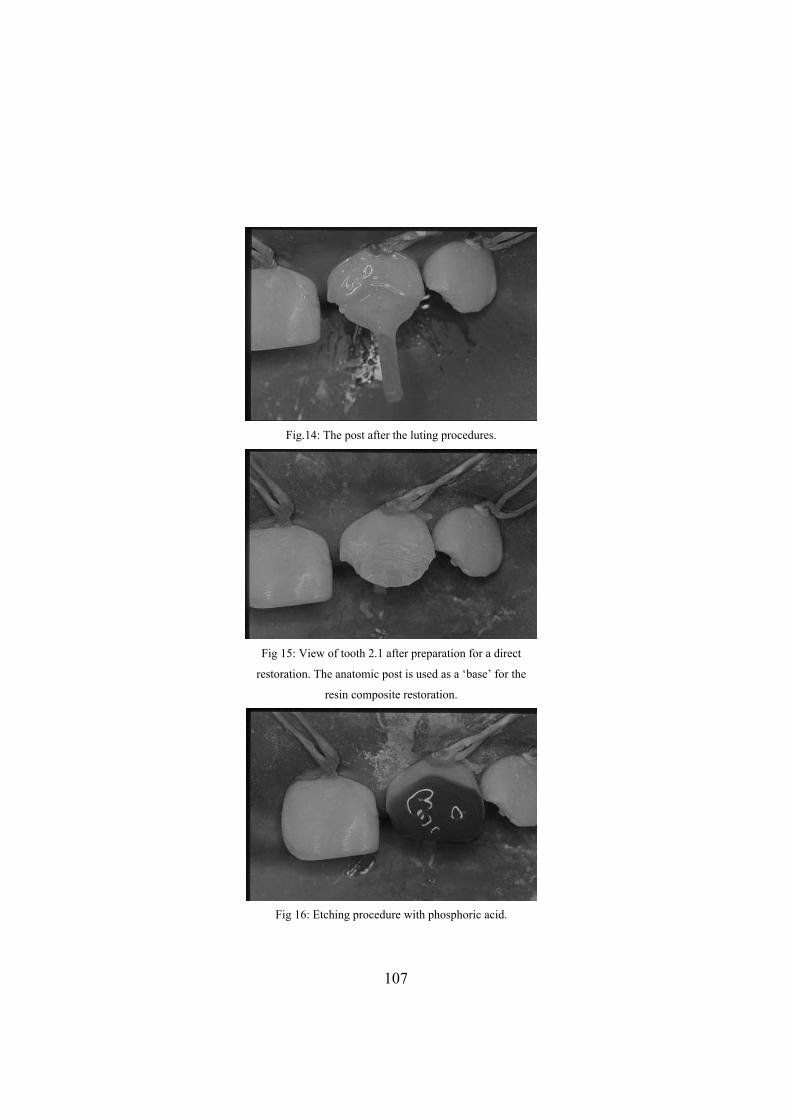
Fig.14: The post after the luting procedures.
Fig 15: View of tooth 2.1 after preparation for a direct
resto r the
resin composite restoration.
ration. The anatomic post is used as a ‘base’ fo
Fi d. g 16: Etching procedure with phosphoric aci
107
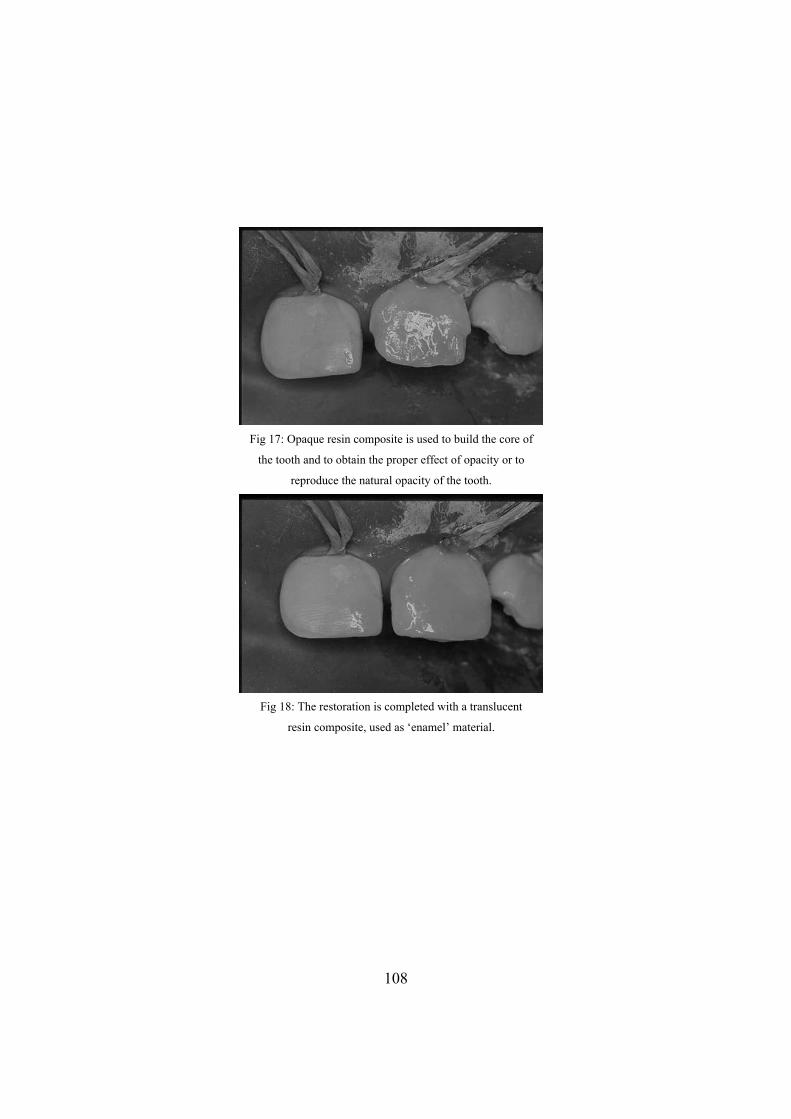
Fig 17 ore of
the tooth and to obtain the proper effect of opacity or to
reproduce the natural opacity of the tooth.
: Opaque resin composite is used to build the c
Fig 18: The restoration is completed with a translucent
resin composite, used as ‘enamel’ material.
108
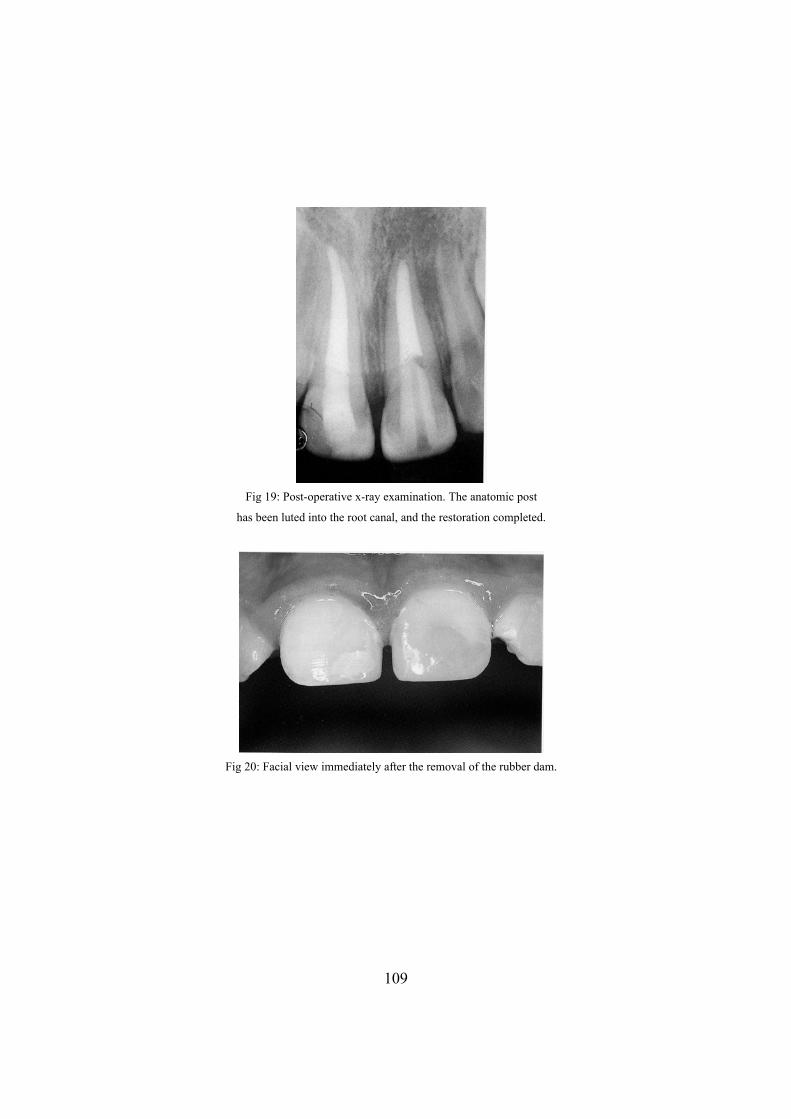
Fig 19: Post-operative x-ray examination. The anatomic post
has been luted into the root canal, and the restoration completed.
Fig 20: Facial view immediately after the removal of the rubber dam.
109
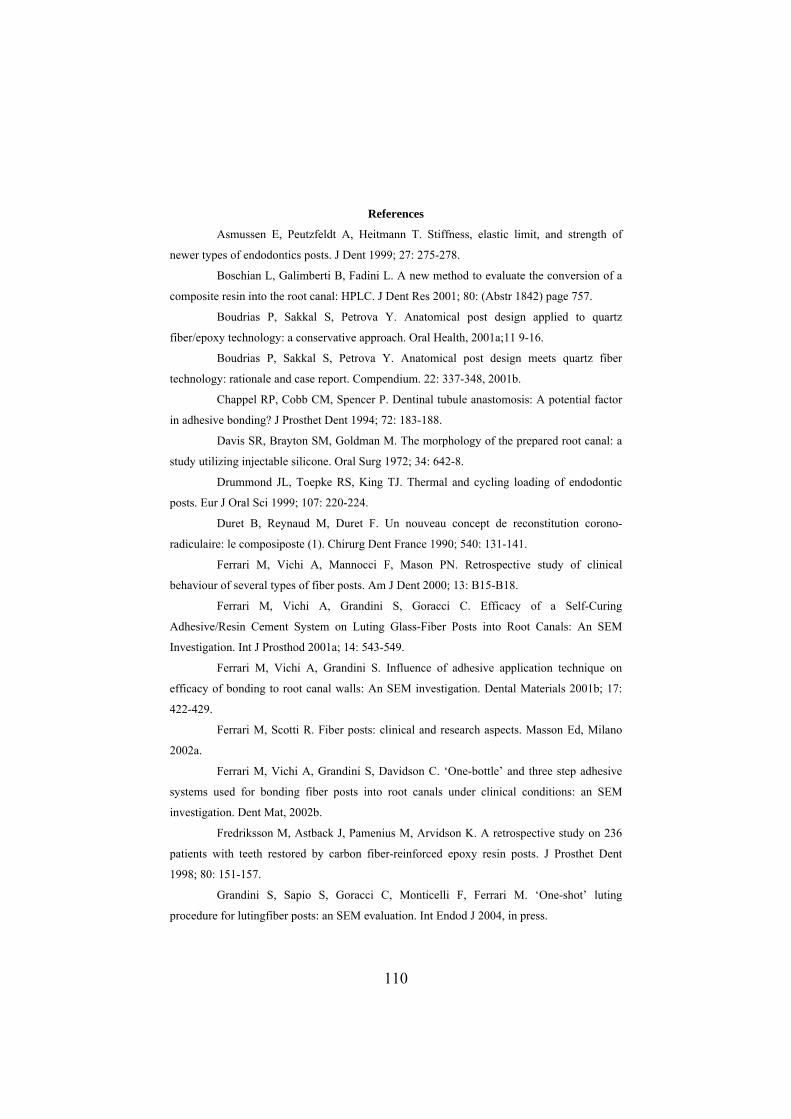
References
Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
newer types of endodontics posts. J Dent 1999; 27: 275-278.
Boschian L, Galimberti B, Fadini L. A new method to evaluate the conversion of a
composite resin into the root canal: HPLC. J Dent Res 2001; 80: (Abstr 1842) page 757.
Boudrias P, Sakkal S, Petrova Y. Anatomical post design applied to quartz
fiber/epoxy technology: a conservative approach. Oral Health, 2001a;11 9-16.
Boudrias P, Sakkal S, Petrova Y. Anatomical post design meets quartz fiber
technology: rationale and case report. Compendium. 22: 337-348, 2001b.
Chappel RP, Cobb CM, Spencer P. Dentinal tubule anastomosis: A potential factor
in adhesive bonding? J Prosthet Dent 1994; 72: 183-188.
Davis SR, Brayton SM, Goldman M. The morphology of the prepared root canal: a
study utilizing injectable silicone. Oral Surg 1972; 34: 642-8.
Drummond JL, Toepke RS, King TJ. Thermal and cy ing loading of endodontic
posts. Eur J Or
Du tution corono-
radiculaire: le composiposte (1). Chirurg Dent France 1990; 540: 131-141.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of clinical
behaviour of several types of fiber posts. Am J Dent 2000; 13: B15-B18.
Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy of a Self-Curing
Adhesive/Resin Cement System on Luting Glass-Fiber Posts into Root Canals: An SEM
Investigation. Int J Prosthod 2001a; 14: 543-549.
Ferrari M, Vichi A, Grandini S. Influence of adhesive application technique on
efficacy of bonding to root canal walls: An SEM investigation. Dental Materials 2001b; 17:
422-429.
Ferrari M, Scotti R. Fiber posts: clinical and research aspects. Masson Ed, Milano
2002a.
F ep adhesive
systems used for bonding fiber posts into root canals under clinical conditions: an SEM
investigation. Dent Mat, 2002b.
Fredriksson M, Astback J, Pamenius M, Arvidson K. A retrospective study on 236
patients with teeth restored by carbon fiber-reinforced epoxy resin posts. J Prosthet Dent
1998; 80: 151-157.
Grandini S, Sapio S, Goracci C, Monticelli F, Ferrari M. ‘One-shot’ luting
procedure for lutingfiber posts: an SEM evaluation. Int Endod J 2004, in press.
cl
al Sci 1999; 107: 220-224.
ret B, Reynaud M, Duret F. Un nouveau concept de reconsti
errari M, Vichi A, Grandini S, Davidson C. ‘One-bottle’ and three st
110
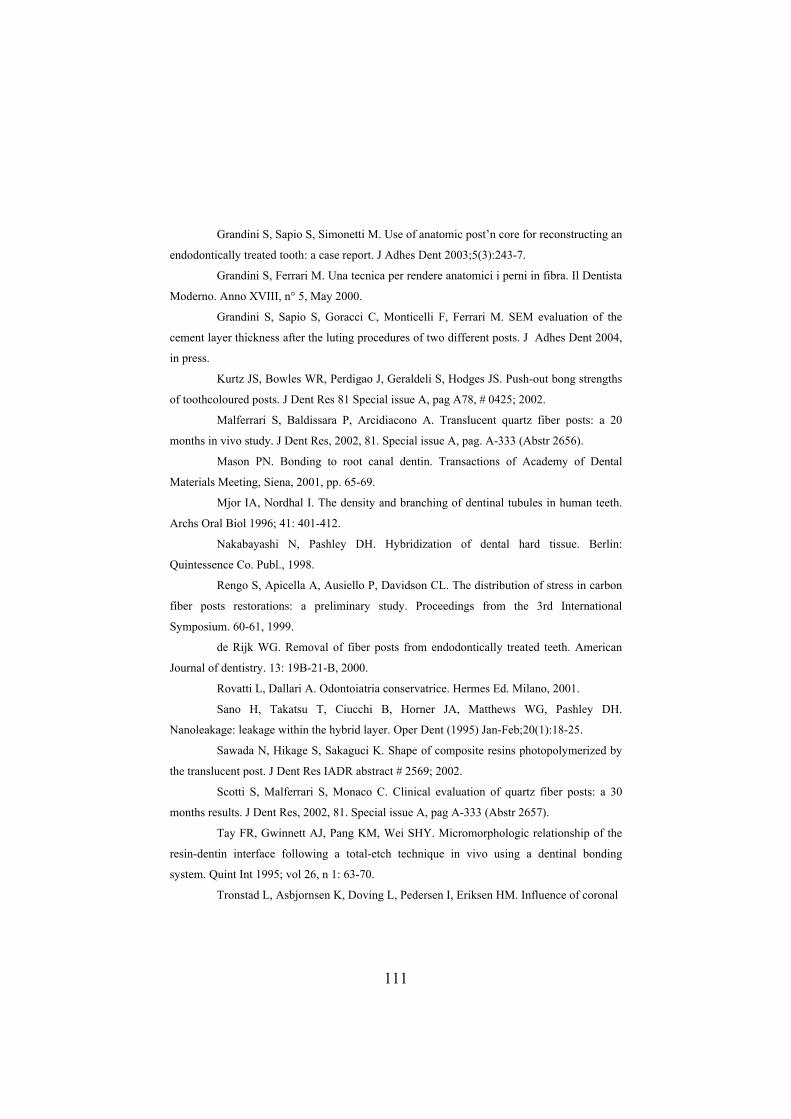
;5(3):243-7.
hes Dent 2004,
in press.
-out bong strengths
of toothco
ranslucent quartz fiber posts: a 20
ions of Academy of Dental
and branching of dentinal tubules in human teeth.
erlin:
n of stress in carbon
er pos
om endodontically treated teeth. American
ano H, Takatsu T, Ciucchi B, Horner JA, Matthews WG, Pashley DH.
anoleak
Sawada N, Hikage S, Sakaguci K. Shape of composite resins photopolymerized by
e transl
Special issue A, pag A-333 (Abstr 2657).
95; vol 26, n 1: 63-70.
Grandini S, Sapio S, Simonetti M. Use of anatomic post’n core for reconstructing an
endodontically treated tooth: a case report. J Adhes Dent 2003
Grandini S, Ferrari M. Una tecnica per rendere anatomici i perni in fibra. Il Dentista
Moderno. Anno XVIII, n° 5, May 2000.
Grandini S, Sapio S, Goracci C, Monticelli F, Ferrari M. SEM evaluation of the
cement layer thickness after the luting procedures of two different posts. J Ad
Kurtz JS, Bowles WR, Perdigao J, Geraldeli S, Hodges JS. Push
loured posts. J Dent Res 81 Special issue A, pag A78, # 0425; 2002.
Malferrari S, Baldissara P, Arcidiacono A. T
months in vivo study. J Dent Res, 2002, 81. Special issue A, pag. A-333 (Abstr 2656).
Mason PN. Bonding to root canal dentin. Transact
Materials Meeting, Siena, 2001, pp. 65-69.
Mjor IA, Nordhal I. The density
Archs Oral Biol 1996; 41: 401-412.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissue. B
Quintessence Co. Publ., 1998.
Rengo S, Apicella A, Ausiello P, Davidson CL. The distributio
fib ts restorations: a preliminary study. Proceedings from the 3rd International
Symposium. 60-61, 1999.
de Rijk WG. Removal of fiber posts fr
Journal of dentistry. 13: 19B-21-B, 2000.
Rovatti L, Dallari A. Odontoiatria conservatrice. Hermes Ed. Milano, 2001.
S
N age: leakage within the hybrid layer. Oper Dent (1995) Jan-Feb;20(1):18-25.
th ucent post. J Dent Res IADR abstract # 2569; 2002.
Scotti S, Malferrari S, Monaco C. Clinical evaluation of quartz fiber posts: a 30
months results. J Dent Res, 2002, 81.
Tay FR, Gwinnett AJ, Pang KM, Wei SHY. Micromorphologic relationship of the
resin-dentin interface following a total-etch technique in vivo using a dentinal bonding
system. Quint Int 19
Tronstad L, Asbjornsen K, Doving L, Pedersen I, Eriksen HM. Influence of coronal
111

restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol
2000 Oct
several
;16(5): 218-221.
Vichi A, Grandini S, Davidson CL, Ferrari M. An SEM evaluation of
adhesive systems used for bonding fiber posts under clinical conditions. Dent Mater. (2002)
Nov;18(7):495-502.
Walton R, Torabinejad M. Principles and practice of endodontics, 2nd edition, W.B.
Saunders Co., 1996: 212-14.
112

Chapter 8 Clinical aspects and future role of fiber posts in dentistry
In st 10 years the use of fiber posts for restoring root canal treated teeth has
increased in popularity. The major advantage is their similar elastic modulus to
entin, produ
the la
ions at the post-dentin interface (Pegoretti et al 2002).
ze this fact by calling “low modulus” restorations those made
with a fiber post, and “high modulus” those made with rigid posts (metal, alloys,
zirconium etc.) (Ferrari et al 2002). It has also been reported that using a “low
modulus” restoration could reduce the risk of root fractures (Isidor et al 1996,
Akkayan et al 2002). Clinical studies have also demonstrated high success rates
without the occurrence of root fractures (Ferrari et al 2000a and 2000b). Many
clinical studies are available regarding the use of fiber posts, a resin core and a
crown (Scotti et al 2002, Malferrari et al 2002, Ferrari et al 2000a and 2000b, Dallari
et al 1998, Monticelli et al 2002).
With the use of contemporary restorative techniques, it is possible to restore teeth
with direct composite procedures, with good functional and esthetic outcomes, and
in a way to save tooth structure. Indications for their use have expanded enormously
in recent years, and now include restoration of tooth structure and contour, changes
to tooth form and enhancement of esthetics, combination restorations (Hickel et al
2004).
This chapter analyzes a possible future use of fiber posts in combination with a
direct resin crown for the restoration of root canal treated teeth, according to the aim
of the minimal intervention philosophy (Mjor et al 2002).
8.1. Clinical evaluation of the use of fiber posts and direct resin restorations for
endodontically-treated teeth
The potential of utilizing fiber-reinforced materials in restorative dentistry has been
appreciated for some time (Bradley et al 1980). The introduction of carbon fiber
posts in 1990 (Duret et al 1990) provided the dental profession with an alternative to
cast or prefabricated metal posts for the restoration of endodontically-treated teeth,
as the elastic moduli of these fiber posts are closer to that of dentin when compared
d cing a stress field similar to that of natural teeth, whereas metal posts
exhibit high stress concentrat
Some authors emphasi
113

with the metal posts (Asmussen et al 1999). Although these earlier generations of
ber posts yielded promising results in clinical trials (Fredriksson et al 1998, Ferrari
ure when fiber posts are used for restoration of
overage has always been highly recommended (Fuss et al 2001). An
e or deflection of bonded
ber-reinforced composite posts demonstrated that they are protective of the
). Although retrospective studies reported good
fi
et al 2000a and 2000b), they suffered from the limitations of being radiolucent and
difficult to mask under all-ceramic or resin composite restorations (Vichi et al
2000).
Over the years, there has been a rapid development in fiber post technology. With
the more recent introduction of radiopaque and more aesthetic quartz and glass fiber
post systems, there is a continuing improvement in the acceptance of fiber posts by
the dental profession (Ferrari et al 2000a, Drummond et al 1999). Studies on the
adhesion of fiber posts to root dentin Nakabayashi et al 1998, Chappel et al 1994,
Mjor et al 1996), the different luting procedures (Ferrari et al 2000c, Vichi et al
2002) and the abutment build-up (Gateau et al 1999, Cohen et al 1996, Freedman
2001) demonstrated the quality performance of the new generations of fiber posts
(Dietschi et al 1997). These favorable results are also supported by clinical trials
showing the absence of tooth fract
endodontically-treated teeth (Monticelli et al 2003, Ferrari et al 2000a and 2000b).
The need for crown coverage after root canal treatment is still conjectural, and no
recent clinical study is available to confirm the indications given in the literature
(Sorensen et al 1984, Paul et al 1998). Post placement and root canal treatment are
usually considered the major etiological factors for root fractures. For this reason
crown c
association between crown placement and the survival of endodontically-treated
teeth was observed when the loss of tooth structure was remarkable (Aquilino et al
2002, Newman et al 2003). However, the mode of failur
fi
remaining tooth structures, and fracture usually comes about at loads that rarely
occur clinically (Paul et al 2001
clinical performances when a crown was used after tooth build-up (Monticelli et al
2003, Ferrari et al 2000a and 2000b), no clinical study was available to confirm the
performances of fiber posts when they are used in conjunction with direct resin
restorations. Thus, the aim of this study was to evaluate the results of a clinical
114

evaluation on root-treated teeth that were restored using fiber posts and direct resin
restorations without additional crown coverage.
8.2 Materials and Methods
Eighty-one patients who required endodontic treatment and restorations on 38
anterior teeth and 62 posterior teeth (33 premolars and 29 molars) were recruited for
s
walls were enlarged with a low-speed bur provided by the manufacturer. The depth
this study. Clinical and radiographic examination demonstrated the need for root
canal treatment in these 100 teeth. The treatment and recall protocol was approved
by the ethical committee from the University of Siena, Italy, and the patients’
informed consent was obtained before enrolment in the clinical evaluation. The
endodontic procedure was performed using a crown-down technique. A portable E-
Master (VDW GmbH, Munich , Germany) endodontic motor was used and speed
rotation and torque were adjusted according to manufacturer’s indications. A
chelating agent (FileCare EDTA, VDW GmbH) and 2.5% sodium hypochlorite
(NaOCl) were used to clean the pulp chamber at the beginning of the
instrumentation. In addition, 2 ml of NaOCl were delivered to the pulp chamber
after the use of each file. All teeth were instrumented with Flexmaster instrument
(VDW, Germany). These instruments’ philosophy is based on the crown down
approach, and they include an “introfile” for the enlargement of the coronal end, a
35.02 file and three different tapers (0.6, 0.4, 0.2) for 30, 25 and 20 files. The
working sequence, proposed by the manufacturer, is based on the degree of the
curvature: canals are divided in wide, medium and narrow canals. For all of them, a
guiding path for the insertion of a size 10 manual file to the working length was
created. Then the sequence was changed depending on the size of the canals.
- wide canals: intro file, 30.06, 25.06, 20.06, 30.04.
- medium canals: intro file, 25.06, 20.06, 30.04, 25,04 (then 25.02, 30.02 and
35.02 if needed).
- narrow canals: intro file, 20.06, 30.04, 25.04, 20.04 (then 20.02, 25.02, 30.02,
35.02 if needed).
The prepared canals were obturated with gutta-percha points (Mynol, Block Co,
Jersey City, NJ, USA) and an epoxy resin sealer (Pulp Canal Sealer, Kerr, Romulus,
Michigan, USA) using a warm vertical compaction technique. Then the root canal
115

of the post space preparation was 9-10 mm. The root canal walls were etched with
37% phosphoric acid (Bisco Inc., Schaumburg, Illinois, USA) for 15 seconds,
then gently air-dried. The excess water was removed
s were
ts were recalled before the
bruary 2004 for the third evaluation and before August 2004 to
vity of the restorations was performed with the following criteria:
washed with water spray and
from the post space using paper points (Mynol). Subsequently, One-Step (Bisco)
adhesive was applied with a microbrush in two consecutive coats, gently air-dried
and the pooled adhesive left in the post space was removed using a paper point
before light curing for 20 seconds. Then a dual-cure resin cement (DuoLink, Bisco)
was used to perform the luting procedure with translucent glass fiber posts (DT post,
RTD, St Egrève, Grenoble, France). According to the diameter of the canal, either
DT size 1, 2 or 3 was used. The cement was applied with a lentulo spiral into the
post space, and the post was inserted into the canal. Resin cement excess was
removed with a clean microbrush and then the cement was light-cured for 40
seconds. The restorative procedure was completed by building up the tooth with a
direct composite restoration (Gradia Direct, GC Corp., Tokyo, Japan) using the
appropriate shades. As far as anterior teeth were concerned, both opaque dentin,
enamel and translucent enamel shades were used with a layering technique in order
to achieve the aesthetic results of the restorations. Regarding posterior teeth, they
were included in the study when showing 2 or 3 remaining coronal walls. The
restorative procedure was carried out using a centripetal technique (Hassan et al
1987, Bichacho 1994), and layering procedure also included opaque dentin and
enamel shades.
The patients were recalled at 6, 12, 24 and 30 months for clinical and radiographic
evaluation of the endodontically-treated and restored teeth. All restoration
placed between January and February 2002. The patien
end of July 2002 for first evaluation, before February 2003 for the second
evaluation, before Fe
complete the final evaluation. During the recall appointments, an assessment of the
stability and longe
1. The presence or absence of periapical lesions; 2. Marginal leakage and integrity;
3. Color stability; 4. Surface staining; 5. Loss of retention due to fracture of the post
or fracture of the composite build-up material. The restorations were evaluated by
116
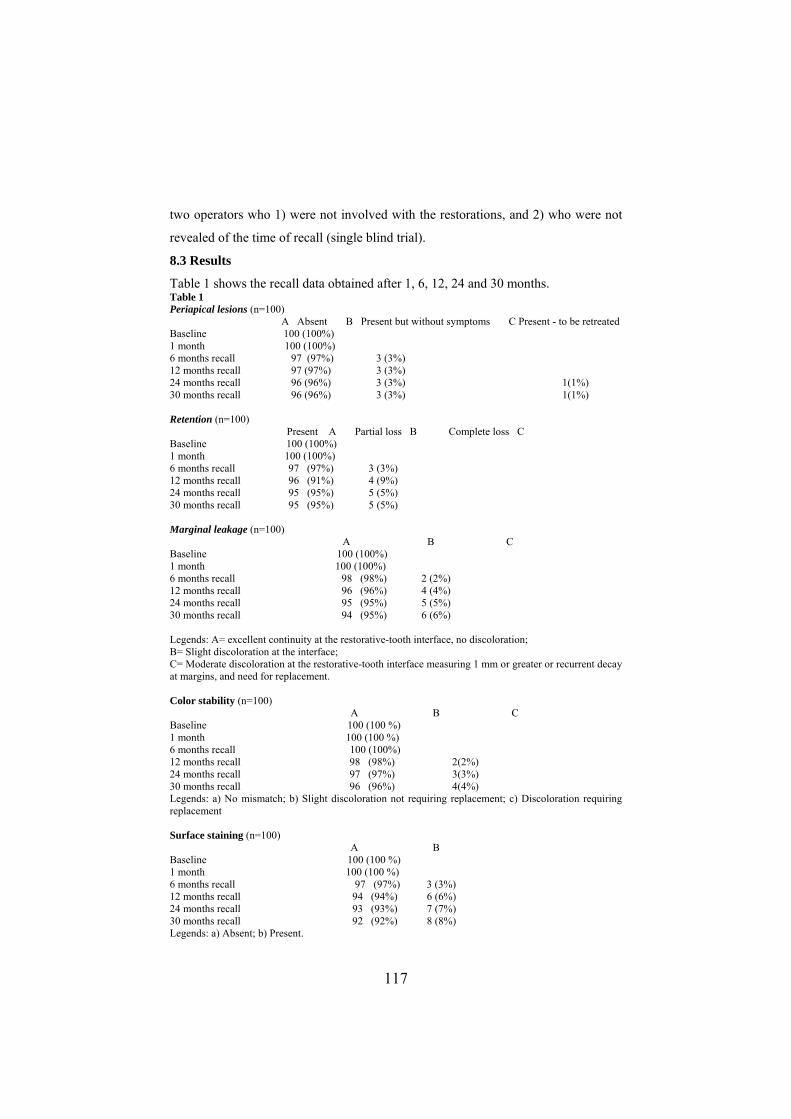
two operators who 1) were not involved with the restorations, and 2) who were not
revealed of the time of recall (single blind trial).
8.3 Results
Table 1 shows the recall data obtained after 1, 6, 12, 24 and 30 months. Table 1 Periapical lesions (n=100) A Absent B Present but without symptoms C Present - to be retreated Baseline 100 (100%) 1 month 100 (100%) 6 months recall 97 (97%) 3 (3%) 12 months recall 97 (97%) 3 (3%) 24 months recall 96 (96%) 3 (3%) 1(1%) 30 months recall 96 (96%) 3 (3%) 1(1%) Retention (n=100) Present A Partial loss B Complete loss C Baseline 100 (100%) 1 month 100 (100%) 6 months recall 97 (97%) 3 (3%) 12 months recall 96 (91%) 4 (9%) 24 months recall 95 (95%) 5 (5%) 30 months recall 95 (95%) 5 (5%) Marginal leakage (n=100) A B C Baseline 100 (100%) 1 month 100 (100%) 6 months recall 98 (98%) 2 (2%) 12 months recall 96 (96%) 4 (4%) 24 months recall 95 (95%) 5 (5%) 30 months recall 94 (95%) 6 (6%) Legends: A= excellent continuity at the restorative-tooth interface, no discoloration; B= Slight discoloration at the interface; C= Moderate discoloration at the at margins, and need
restorative-tooth interface measuring 1 mm or greater or recurrent decay for replacement.
30 months recall 92 (92%) 8 (8%) Legends: a) Absent; b) Present.
Color stability (n=100) A B C Baseline 100 (100 %) 1 month 100 (100 %) 6 months recall 100 (100%) 12 months recall 98 (98%) 2(2%) 24 months recall 97 (97%) 3(3%) 30 months recall 96 (96%) 4(4%) Legends: a) No mismatch; b) Slight discoloration not requiring replacement; c) Discoloration requiring replacement Surface staining (n=100) A B Baseline 100 (100 %) 1 month 100 (100 %) 6 months recall 97 (97%) 3 (3%) 12 months recall 94 (94%) 6 (6%) 24 months recall 93 (93%) 7 (7%)
117

At 1- or 2-year recall, endodontic retreatment was performed on those patients with
persisting periapical lesions, and/or clinical symptoms. Only 4 teeth exhibited
sions after 30 months of clinical service, and in one case retreatment
5 out of 100
loss of the restoration. This was manifested as “chipping” of
the hundred teeth examined exhibited
ssfully refurbished using the same
of clinical servic
t discoloration, not requiring replacement. Surface staining was
fter 2 years of clinical service. These teeth were
nst the following two clinical cases:
car accident (fig
m the enamel and dentin fracture, and was
tral incisor (tooth 11) had an
d. After root canal treatment, a
ber post was inserted (fig 1b). Then the restoration was completed with the same
to restore tooth 11 (fig 1c). During the recall
. The restorations were reburished with BisCover (Bisco), a
lt after 30 months
ed fo cute pain regarding tooth
molar was subsequently endodontically-treated (fig2a), and a direct resin
was placed after the bonding of a fiber post to the root-treated
as a treatment alternative to
tient decided to postpone the
aphic results of the
periapical le
was performed without replacing the direct restoration. After 30 months
teeth showed a partial
the resin composite. The restorations were repaired using the same resin composite
used for the initial restoration. Six out of
slight marginal staining. They were also succe
material used for the initial restoration. After 2 years e, only 4 teeth
showed a sligh
present in 8 out of 100 teeth a
finished and polished.
Representative results are demo rated with
CLINICAL CASE #1
This 21 years old patient was treated as an emergency case after a
1a). Tooth 11 was asymptomatic apart fro
restored with a direct resin restoration. The left cen
irreversible pulp injury and was endodontically-treate
fi
resin composite material used
appointment, the patient did not want to prepare tooth 11 for a full ceramic crown
for economic reason
composite surface sealant and the clinical and radiographic resu
are illustrated in fig. 1d and 1e.
CLINICAL CASE #2
This 53 years old patient was initially examin r an a
44. The pre
composite restoration
tooth (figs 2b,2c). An all ceramic crown was suggested
the patient. However, for economic reasons, the pa
indirect restoration. Figs 2d and 2e show the clinical and radiogr
composite restoration after 30 months.
118

8.4 Discussion
In the last decade, metallic posts have been widely used for restoring
endodontically-treated teeth. Metal posts (i.e., alloys or titanium) were most
commonly used because of their physical properties (Sorensen et al 1984): their high
stiffness and rigidity were highly appreciated. Because of their color, they cannot
meet the aesthetic demands of contemporary direct resin composite restorations. The
aesthetic requirements for posts and cores became even more demanding following
the introduction of more translucent, enamel-like all-porcelain restorations.
Some authors have emphasized the need to use endodontic posts made with
biomechanical properties similar to those of dentin. Fiber posts are the only
available materials that have this property (Ferrari et al 2002). This is because the
stresses that were distributed to the residual tooth structure by the presence of a
1997,
he important difference between using "stiff" metal posts and
d for bonding of fiber posts may be performed by
y of the resin-dentin interdiffusion zone (RDIZ), resin tags,
i et al 2002). The microbrush is also able to
metal post were much higher than when a fiber-post was used (Ausiello et al
Yamada et al 2004). T
flexible resin based posts is in the transfer of stress (energy) from restoration to
tooth. With flexible posts all stress is located at the top of the root (the root-crown
border area) while the stiff post can transfer stress down in the root canal.
The rapid influx of these new aesthetic fiber posts has imposed the need for a
systematic evaluation of their mechanical properties and clinical performances. For
that purpose, scanning electron microscopy (SEM) –with or without the use of a
tracer- (Ferrari et al 2001a, Tay et al 1995)), transmission electron microscopy
(TEM) and fatigue test (Baran et al 2001) can provide an indication of the type of
post that would perform better under clinical conditions. The evaluation of the
efficacy of adhesive systems use
observing the uniformit
and adhesive lateral branches (Drummond et al 1999), and by recording the presence
of voids/bubbles within the luting material or at the interface between the cavity
wall and the post (Ferrari et al 2001b).
In this clinical trial, microbrushes were used to carry the “one-bottle” adhesive
system inside the root canal. The importance of the microbrush in reaching the
narrowest and deepest portions of the root canal preparations has been shown by
recent findings (Ferrari et al 2001b, Vich
119

reach all the prepared root canal dentin, resulting in a deep diffusion of resin into the
ost and
omposites
of the resin material sometimes occurred,
tubules and in the formation of lateral branches (Nakabayashi et al 1998, Chappel et
al 1994).
The results of this clinical trial can be important in that direct resin restorations were
performed, whereas previous prospective and retrospectives studies evaluated fiber
post/resin restorations that were covered with either full porcelain or metal-ceramic
crowns (Fredriksson et al 1998, Ferrari et al 2000a and 2000b, Monticelli et al
2003). Thus, we were able to analyze the clinical performances of fiber p
resin restoration alone. Moreover, the preservation of tooth structure is regarded as
the most important aspect in increasing the survival rate of endodontically-treated
teeth (Lodval et al 1977, Trabert et al 1978, Sorensen 1988). When only adhesive
procedures and direct resin composites are used, all the tooth structure remaining
after caries removal and the root canal treatment is preserved. On the contrary, tooth
preparation for an indirect restoration would eliminate a substantial amount of sound
tooth structure. A 2.5 years period of observation is short, for this reason the
evaluation is being continued to have more significant clinical results.
After 30 months, good coronal seals were achieved with the direct resin c
and fiber post restorations, as the incidence of persistent periapical lesions did not
differ from those provided by other studies (Fredriksson et al 1998, Ferrari et al
2000a and 2000b, Monticelli et al 2003). In the only case that was endodontically
retreated, the procedure was performed without removing the direct restoration. The
composite material was partially removed until the fiber post was visible. Then the
removal of the post was performed using a “removal kit” provided by the
manufacturer (Removal Kit, RTD, France). After the completion of the new
endodontic procedure, a new post was inserted and the restoration completed with
resin composite. The whole procedure of the endodontic retreatment was easily
performed, according to recent data available in the literature (Gesi et al 2003).
Marginal discoloration, and “chipping”
and their repair with the same type of composite achieved acceptable clinical results
(Frankemberger et al 2003, Saunders 1990). In 8 out of 100 cases, slight
discoloration of the restorations were present after 30 months. Refurbishing and
polishing were performed, and these procedures appeared to have prevented further
120

discoloration or color mismatch problems. Undoubtedly, the resin composite
employed is inferior in terms of wear resistance (Yip et al 2004), when compared to
full ceramic or ceramometal crowns (Derand et al 1999). On the other hand,
mechanical
porcelain are susceptible to brittle failure, while ductile materials utilize their
plasticity to reduce stress concentrations along the crack tip (Derand et al 1999). The
use of a direct resin restoration is also more economical from the patient’s point of
view, as these restorations are much cheaper than any other indirect restorations.
The use of direct composite restorations also minimizes the amount of residual tooth
structure that has to be sacrificed for full crown coverage. They are also less time
consuming in their fabrication and no additional laboratory costs are required. The
ability to refurbish these fiber post-direct composite restorations is thus an important
alternative with the potential to save tooth structure and increase the longevity of
restorations at a lower cost (Hickel et al 2004, Mjor et al 2002) In cases with
questionable prognosis, it is also desirable to wait for a period of time before making
definitive indirect restorations.
It has recently been shown that if a quality fiber post with good
properties is used, it can resist up to two million cycles in fatigue testing (Grandini
S, Goracci C, Monticelli F, Tay FR, Ferrari M. Fatigue resistance and structural
characteristics of fiber posts: three-point bending test and SEM evaluation. Dent
Mater-in press). It is encouraging to observe that no post or root fracture occurred
after 30 months of clinical service, confirming the results of previous studies
(Fredriksson et al 1998, Ferrari et al 2000a and 2000b). Longer clinical trials should
be performed to validate the use of fiber posts and direct resin composites as a
simplified conservative approach to the rehabilitation of endodontically-treated
teeth.
8.5 Conclusions
After 30 months of clinical service, the root canal treated teeth restored with fiber
posts and direct resin composite restorations exhibited favourable clinical results.
121
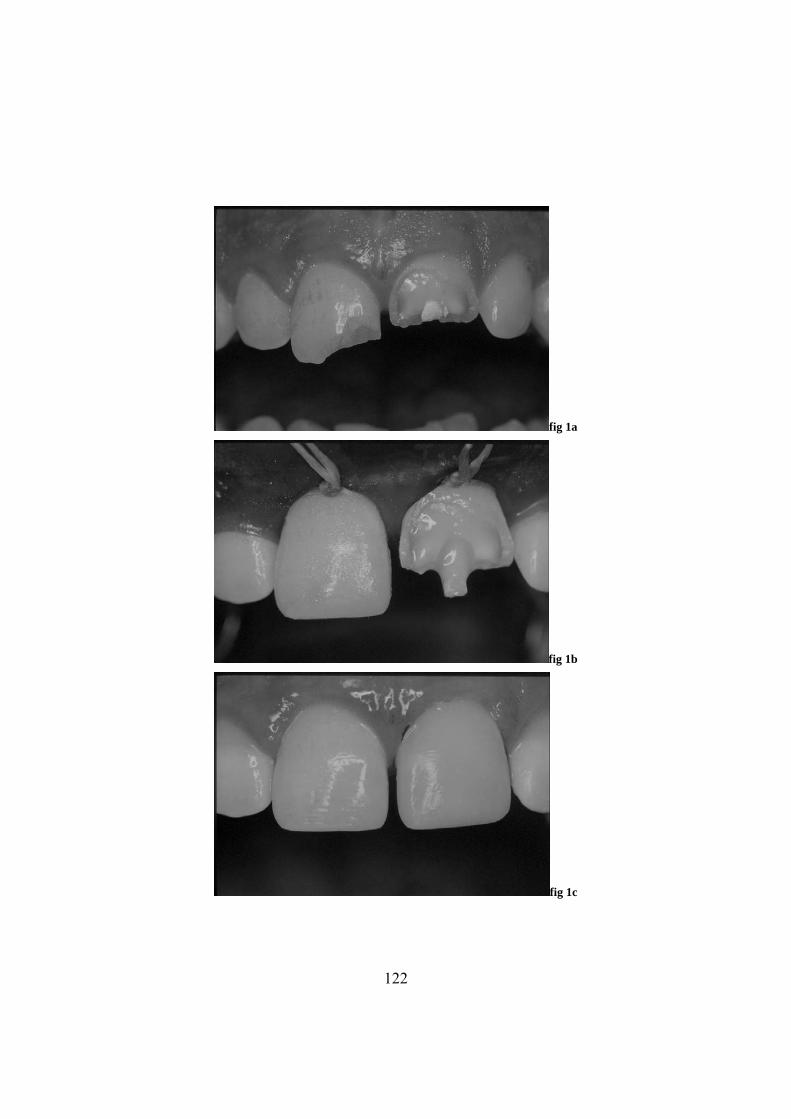
fig 1a
fig 1b
fig 1c
122
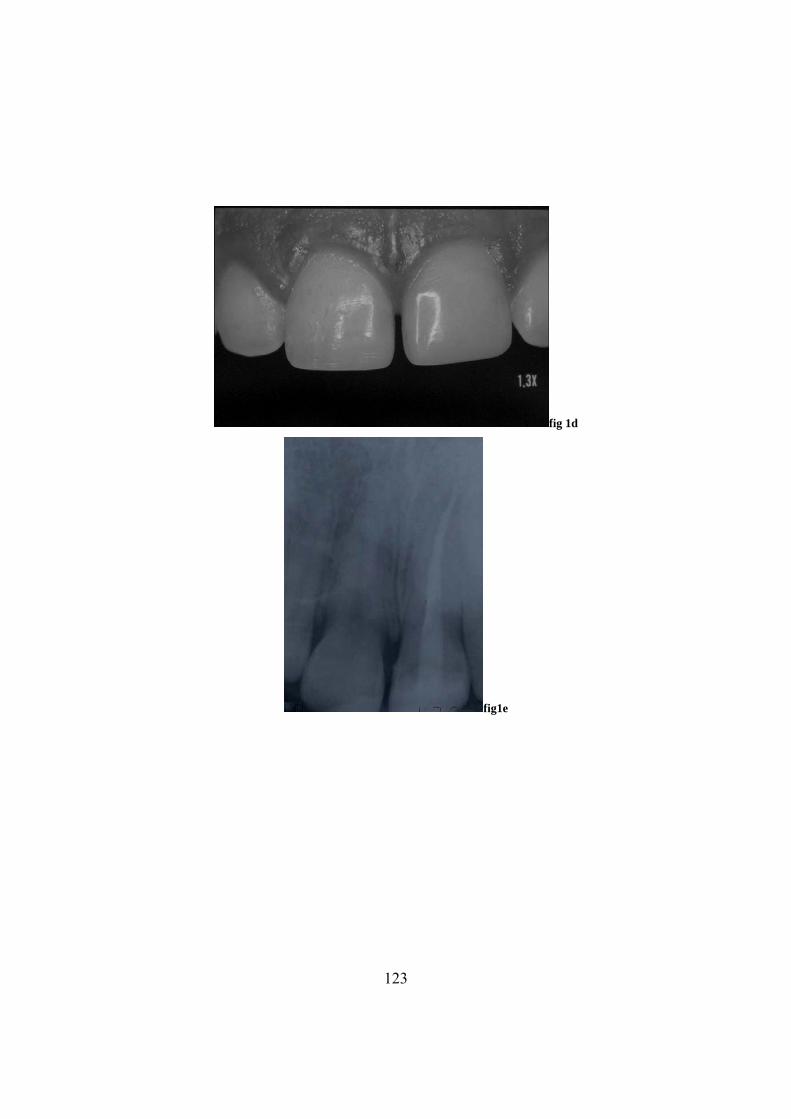
fig 1d
fig1e
123
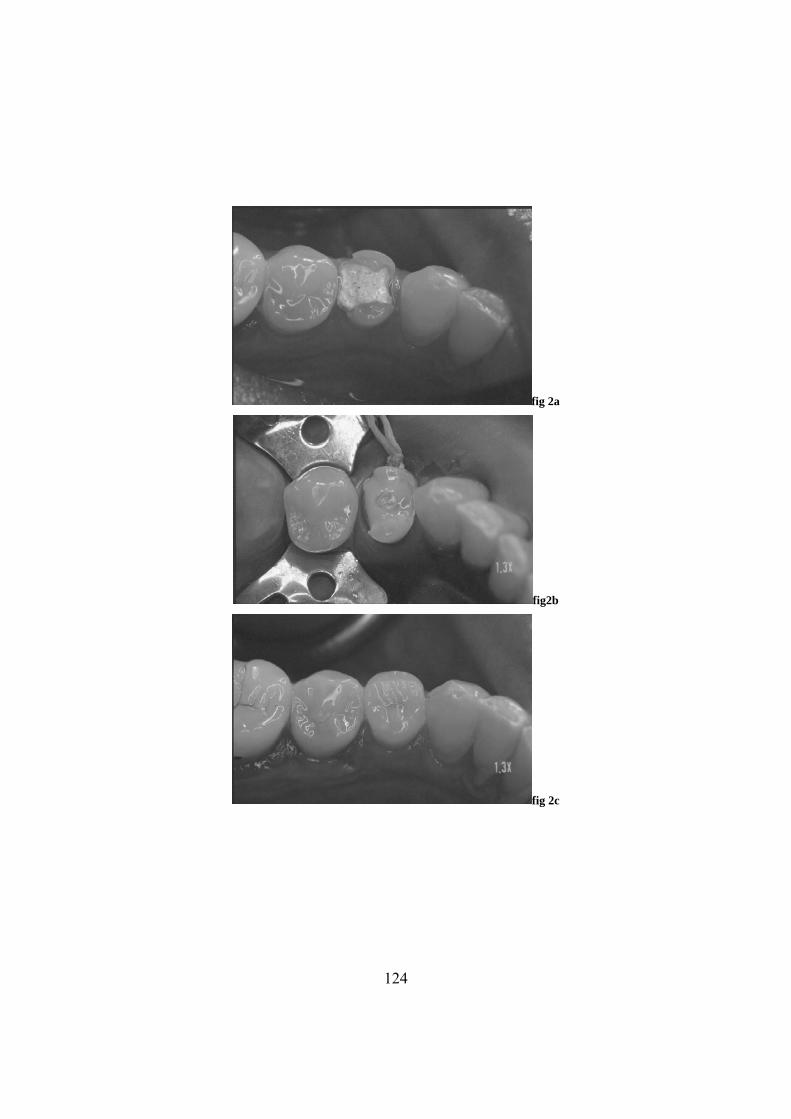
fig 2a
fig2b
fig 2c
124
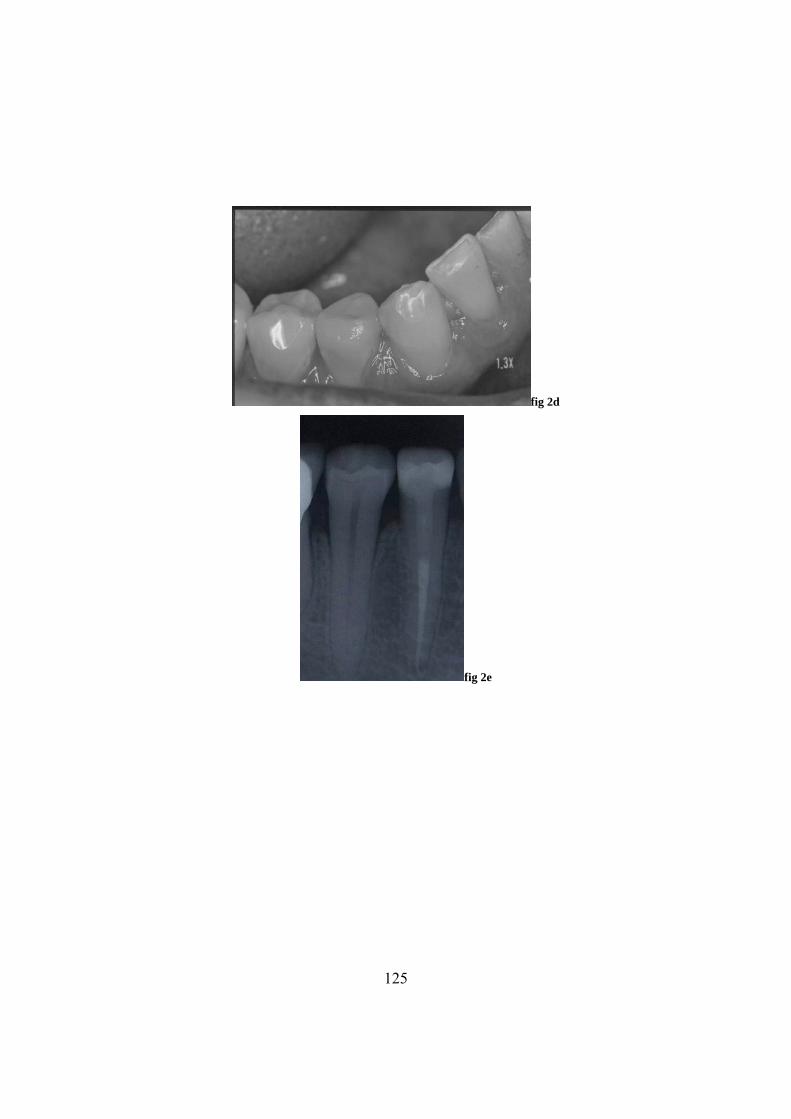
fig 2d
fig 2e
125
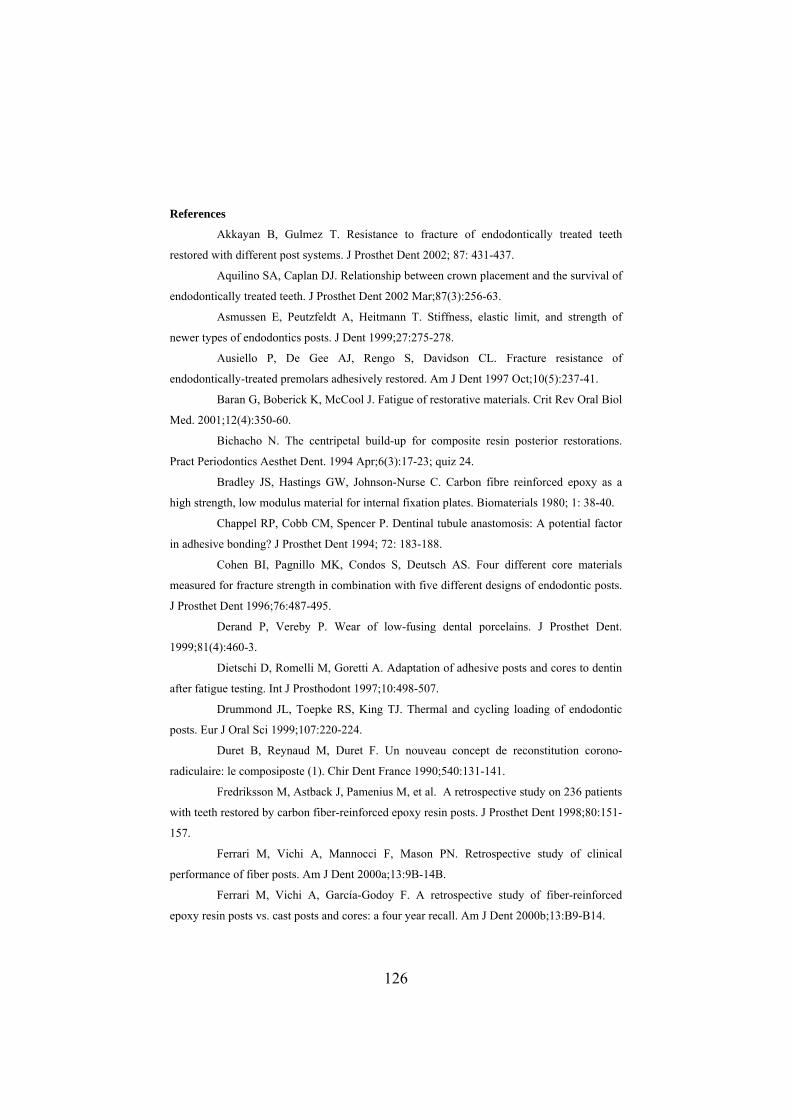
References
Akkayan B, Gulmez T. Resistance to fracture of endodontically treated teeth
restored with different post systems. J Prosthet Dent 2002; 87: 431-437.
Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of
endodontically treated teeth. J Prosthet Dent 2002 Mar;87(3):256-63.
Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
newer types of endodontics posts. J Dent 1999;27:275-278.
Ausiello P, De Gee AJ, Rengo S, Davidson CL. Fracture resistance of
endodontically-treated premolars adhesively restored. Am J Dent 1997 Oct;10(5):237-41.
Baran G, Boberick K, McCool J. Fatigue of restorative materials. v Oral Biol
Med. 2001;12(4):350-60.
Bichacho N. The centripetal build-up for composite resin posterior restorations.
Pract Periodontics Aesthet Dent. 1994 Apr;6(3):17-23; quiz 24.
Bradley JS, Hastings GW, Johnson-Nurse C. Carbon fibre reinforced epoxy as a
high strength, low modulus material for internal fixation plates. Biomaterials 1980; 1: 38-40.
Chappel RP, Cobb CM, Spencer P. Dentinal tubule anastomosis: A potential factor
in adhesive bonding? J Prosthet Dent 1994; 72: 183-188.
Cohen BI, Pagnillo MK, Condos S, Deutsch AS. Four different core materials
measured for fracture strength in combination with five different designs of endodontic posts.
J Prosthet Dent 1996;76:487-495.
Derand P, Vereby P. Wear of low-fusing dental porcelains. J Prosthet Dent.
1999;81(4):460-3.
Dietschi D, Romelli M, Goretti A. Adaptation of adh and cores to dentin
after fatigue testing. Int J Prosthodont 1997;10:498-507.
Drummond JL, Toepke RS, King TJ. Thermal and cycling loading of endodontic
posts. Eur J Oral Sci 1999;107:220-224.
Duret B, Reynaud M, Duret F. Un nouveau concept de reconstitution corono-
radiculaire: le composiposte (1). Chir Dent France 1990;540:131-141.
Fredriksson M, Astback J, Pamenius M, et al. A retrospective study on 236 patients
with teeth restored by carbon fiber-reinforced epoxy resin posts. J Prosthet Dent 1998;80:151-
157.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of clinical
performance of fiber posts. Am J Dent 2000a;13:9B-14B.
Ferrari M, Vichi A, García-Godoy F. A retrospective study of fiber-reinforced
epoxy resin posts vs. cast posts and cores: a four year recall. Am J Dent 2000b;13:B9-B14.
Crit Re
esive posts
126
Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjör IA. Bonding to root canal:
of a Self-Curing
ion. Dent Mater 2001b;17:422-
9.
ano
002.
, Kramer N, Ebert J, Lohbauer U, Kappel S, ten Weges S, Petschelt
. Fatigu
od 2001 Jan;27(1):46-8.
oracci C, Ferrari M. Comparison of two techniques for
S, Goracci C, Monticelli F, Tay FR, Ferrari M. Fatigue resistance and
structural
t Dent. 1987 Aug;58(2):153-6.
al Investig 2004; 8:43-
4.
rbon fiber posts. Int J Prosthod 1996;9:131-6.
Structural characteristics of the substrate. Am J Dent 2000c;13:380-386.
Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy
Adhesive/Resin Cement System on Luting Glass-Fibre Posts into Root Canals: An SEM
Investigation. Int J Prosthodont 2001a;14:543-549.
Ferrari M, Vichi A, Grandini S. Influence of adhesive application technique on
efficacy of bonding to root canal walls: An SEM investigat
42
Ferrari M, Scotti R. Fibre posts: clinical and research aspects. Masson Ed, Mil
2
Frankenberger R
A e behavior of the resin-resin bond of partially replaced resin-based composite
restoration. Am J Dent 2003; 16: 17-22.
Freedman GA. Esthetic post and core treatment. Dent Clin North Am
2001;45:1:103-116.
Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical
root fractured teeth: impact of operative procedures. J End
Gateau P, Sabek M, Dailey B. Fatigue testing and microscopic evaluation of post
and core restorations under artificial crowns. J Prosthet Dent 1999;82:341-347.
Gesi A, Magnolfi S, G
removing fiber posts. J Endod. 2003;29(9):580-2.
Grandini
characteristics of fiber posts: three-point bending test and SEM evaluation. Dent
Mater 2004 (in press).
Hassan K, Mante F, List G, Dhuru V. A modified incremental filling technique for
Class II composite restorations. J Prosthe
Hickel R, Heidemann D, Staehle HJ, Minnig P, Wilson NH. Direct composite
restorations: extended use in anterior and posterior situations. Clin Or
4
Isidor F, Odman P, Brondum K. Intermittent loading of teeth restored using
prefabricated ca
Lodvahl PE, Nicholls JI. Pin retained amalgam cores vs. cast gold dowel cores. J
Prosthet Dent 1977, 38:507-14.
Mjör IA, Nordhal I. The density and branching of dentinal tubules in human teeth.
Archs Oral Biol 1996; 41: 401-412.
127
Mjör IA, Gordan VV. Failure, repair, refurbishing and longevity of restorations.
Oper Dent 2002;27(5):528-34.
Monticelli F, Grandini S, Goracci C, Ferrari M. Clinical behavior of translucent-
fiber posts: a 2-year prospective study. Int J Prosthodont 2003 Nov-Dec;16(6):593-6.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissue. Berlin:
ontically treated teeth restored with composite posts. J Prosthet Dent 2003
Paul S, Scharer P. Post and core reconstruction for fixed prosthodontic restoration.
ract Per
st. Biomat 2002;23:2667-82.
ent 1990; 18: 158-162.
onship of the
ari M, Davidson CL. Influence of ceramic and cement thickness on the
cal procedures for
tance of endodontically treated maxillary premolars. Int J Prosthodont 2004; 17:94-98.
-356.
Quintessence Co. Publ., 1998.
Newman MP, Yaman P, Dennison J, Rafter M, Billy E. Fracture resistance of
endod
Apr;89(4):360-7.
P iod Aesthet Dent 1998;5:513-20.
Pegoretti A, Fambri L, Zappini G, Bianchetti M. Finite element analysis of a glass
fibre reinforced composite endodontic po
Saunders WP. Effect of fatigue upon the interfacial bond strength of repaired
composite resin. J D
Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a
study of endodontically treated teeth. J Prosthet Dent 1984 Jun;51(6):780-4.
Sorensen JA. Preservation of tooth structure. J Calif Dent Assoc 1988, 16:15-22.
Tay FR, Gwinnett AJ, Pang KM, Wei SHY. Micromorphologic relati
resin-dentine interface following a total-etch technique in vivo using a dentinal bonding
system. Quintessence Int 1995;26,1:63-70.
Trabert KC, Caputo AA, Abou Rass M. Tooth fracture: a comparison of endodontic
and restorative treatments. J Endod 1978, 4:341-45.
Vichi A, Ferr
masking of various types of opaque posts. J Prosthet Dent. 2000;83:412-7.
Vichi A Grandini S, Ferrari M. Comparison between two clini
bonding fiber posts into a root canal: a microscopic investigation. J Endod 2002;28:355-360.
Yamada Y, Tsubota Y, Fukushima S. Effect of restoration method on fracture
resis
Yip KH, Smales RJ, Kaidonis JA. Differential wear of teeth and restorative
materials: clinical implications. Int J Prosthodont. 2004; 17(3):350
128

C 9 Summary and conclusions
hapter
has al
s. This
e select
reated tooth. Many changes can occur after root canal treatment in
rms of
vior. A vital tooth presents with a stiffer
ructure
hat can reduce tooth
04). Moreover,
th
nder str
ure incidence documented in maxillary
remola
ures, are responsible for a reduction
the fr
the qu
re and
7), as they
ficantly strengthen endodontically-treated teeth…” (Sorensen
1984a). The progress made in the technology of fiber-reinforced materials have
improved the structure, shape, and optical properties of contemporary fiber-
reinforced resin posts. This led to the development of materials which have
It ways been a big challenge for clinicians to restore endodontically-treated
teeth. Fiber posts acquired high importance in this field in the last 15 year
thesis contains a study about several different basic and clinical aspects related to
th ion and use of fiber posts.
There is scientific evidence showing that a healthy tooth is different from an
endodontically-t
te the physical, chemical and elastic properties of dentin, resistance to fatigue,
morphology and biomechanical beha
st (enamel) and a more compliant support underlying it (dentin). Caries and
tooth preparation for endodontic treatment are the first factors t
resistance. There is a decrease in moisture content (Helfer et al. 1972), an increased
ung’s mYo odulus (Huang et al. 1992), and a reduction in the percentage of collagen
fibrils in dentin (Mason 2001, Hashimoto et al. 2000, Ferrari et al. 20
changes also occur in the morphology and in the biomechanical behavior of tee
u ess (Grimaldi 1971, Tidmarsh 1976). The access preparation for endodontic
treatment causes the loss of both the roof of the pulp chamber and the marginal
ridges, influencing the relatively high fract
p rs (Ross et al. 1980, Salis et al. 1987). In general, removal of the roof of the
pulp chamber, together with endodontic proced
in acture resistance (Fuzzi 1993, Morgano et al. 1993, Trabert et al. 1978,
t et al. 199Milo 2).
It is also known that the likelihood of survival of a pulpless tooth is directly related
to antity and quality of remaining tooth structure (Assif et al. 1994, Guttman
1992, Cohen et al. 1996). Traditionally, a post was inserted to ensure retention of the
co to “reinforce” the tooth. To date, the eventual reinforcement provided by
metal posts is no longer considered as possible (Shillimburg HT 199
“…do not signi
129

overcome so of the limitations of metallic me posts (platinum, alloys or titanium),
oncerning esthetic appearance, mode of failure, and clinical performance. In terms
ts are concerned, it has been shown that metallic
number of residual walls, that were restored using resin
c
of esthetics, translucent fiber posts were introduced commercially to support anterior
restorations (Vichi et al. 2000a and 2000b, Ferrari et al. 2001a and 2001b, Ferrari et
al. 2002, Paul et al. 1998, Heydecke et al. 2002). As far as the mechanical behavior
and failure mechanisms of fiber pos
posts on failure tend to produce irreversible root fractures. Conversely, root fracture
that occur with the use of fiber posts are usually located more coronally and are
more easily retreatable (Akkayan et al. 2002, Cornier et al. 2001, Reagan et al. 1999,
Newman et al. 2003). This type of failure may be due to the greater amount of tooth
structure that must be removed when a metallic post is placed (Stankiewitz et al.
2002). In the event that endodontic re-treatment is necessary, fiber posts are more
easily removed than either metallic or ceramic ones (Gesi et al. 2003, Hauman et al.
2003). In conclusion, fiber posts function well as retention for resin composite cores.
When compared to metal or zirconia posts, they are able to preserve residual tooth
structure due to their mechanical behavior and the accompanying luting procedures.
Techniques has been described for restoring endodontically-treated teeth with the
use of resin composites to replace lost root dentin, with the possibility of
strengthening the root. Unfortunately these reports were published in non peer-
reviewed publications (Freedman et al. 1994, Godder et al. 1994, Martelli 2000,
Castellucci 2004). A recent study was performed comparing the fracture resistance
and failure patterns of endodontically-treated maxillary premolars with a
progressively reduced
composite materials with or without translucent glass fiber posts (Sorrentino et al.
2004). This study showed that the number of residual dental walls influenced the
mechanical resistance of endodontically-treated maxillary premolars. In specimens
with the same number of residual dental walls, higher fracture loads were recorded
in teeth restored with fiber posts. Moreover, restorable fractures were observed in
the specimens restored with fiber posts. If these data can be subsequently validated
with clinical studies, the concept of reinforcing root structures with the bonding of
fiber posts to root canals will be more firmly established.
130

A successful endodontic procedure is a key factor to ensure success in the
restoration of root-treated teeth. A well performed endodontic treatment is based on
the removal of debris and organic material inside the root canal (Castellucci 1993)
and on the mechanical preparation of the canal itself to receive an obturation
material (Ingle 1993). The influence of cements and irrigating solutions has been
extensively discussed in the literature. When evaluating the effect of different
irrigating regimes on the cleanliness of the root canals achieved after endodontic
treatment (Grandini et al. 2002b), it was found that none of the techniques used in
that study showed a perfect removal of the smear layer and debris. However, it was
noted that a combination of sodium hypochlorite and a chelating agent can help
reduce the amount of debris along root canal walls. The functions of root canal
filling are essentially to seal the root canal and to prevent further microleakage. In
this sense, post fabrication and placement can be considered as part of the
endodontic treatment if they contribute to the filling and sealing of the root canal
space (Trope 2004). Unfortunately, due to the high C-factors encountered in post
spaces (Morris et al., 2002; Bouillaguet et al., 2003; Goracci et al., 2004), substantial
difficulty was experienced with the luting of fiber posts to intraradicular dentin with
resin cements. It has been suggested that similar to the use of non-bonding cements,
a substantial part of the dislocation resistance of bonded fiber posts to root canals is
contributed by sliding friction (Goracci et al., 2005).
The popularity with the use of fiber posts for restoration of the endodontically-
treated teeth has imposed the need for a systematic evaluation of the different brands
and types of fiber posts available commercially. Some criteria are usually employed,
such as the composition and shape of the post, cost and luting procedures, based on
basic and experimental evaluations. A study comparing the fatigue resistance and
the structural characteristics of different types of fiber posts has been described
(Grandini et al. 2004a). Some brands of fiber posts can resist up to 2.000.000 cycles
of fatigue testing without affecting their general quality. In particular the quality of
the bonding between the two components of a fiber post (the fibers and the epoxy
resin matrix) can influence the quality of the post itself. As a matter of fact, static
impact and fatigue properties are proportional to the strength of the filler/resin
interface in fiber-reinforced composite systems (Zhao et al. 2000, Kessler et al.
131

2000, Keusch et al. 1999). A recent study confirmed that increasing the strength of
the bond between the fillers and matrix will result in improvements in the
mechanical properties of fiber-reinforced composites (Debnath et al. 2004).
Luting procedures are extremely important as far as fiber posts are concerned. The
recommended procedure has already been described in the literature (Ferrari et al.
2001a and 2001b, Vichi et al. 2002a). Acid etching, the use of a fourth or fifth
generation adhesive, and of a dual-curing resin cement provides the best clinical
results. Leaving the adhesive solution unpolymerized before placing the cement
(one-step procedure), in order to reduce the time for the cementation procedure,
produces unfavourable results both from the clinical and experimental standpoint
(Grandini et al. 2004b). If a crown is placed, the post can be adjusted after the core
restoration. In case a direct restoration is placed, it is better to adjust the length of
the post before the luting procedures. The adjustment should be performed with a
carborundum disk or a diamond bur (Grandini et al. 2002a). This way, it is possible
to cover the cut end of the post with resin composite, a material much more able
than a fiber post to resist tooth-to-tooth and tooth-to-food wear. If a post is good
enough, cutting procedures will not affect its structural integrity.
Much development occurred concerning the materials used for the fabrication of
posts: carbon was the first material employed; glass, quartz and silica have
subsequently been used, taking advantage of their translucent optical properties.
Interesting development was also seen in the modification of the design of these
posts, from the original double-cylinder, endodontic shapes, to the more recently
introduced double-tapered shapes, as adhesive cementation now relies more on the
formation of the resin-dentin interdiffusion zone and resin tags rather than on the
good fitting and mechanical retention of the post inside the root canal (Ferrari et al.
2002). Moreover, a wider selection of sizes permits conservation of the amount of
residual dentin that has to be removed in order to achieve a satisfactory post
adaptation. Debonding is more likely to occur in the absence of the desirable ‘ferrule
effect’, or in the presence of an overly thick layer of cement wherein the entrapment
of bubbles is conducive to debonding (Ferrari et al. 2000a). The idea of having a
custom-fabricated post that fits individual post space is appealing, especially when
dealing with root canals that have elliptical shapes, such as those observed in
132
canines and lower premolars. In these cases, the clinician is forced to adapt the
residual root structure to the post shape, through the removal of a further amount of
dentin. On the contrary, it would be desirable that the post adapt to the root canal
ct resin composite
anatomy as produced by the endodontic treatment. This is indeed the rationale for
the creation of an anatomic post (Grandini et al 2000, Boudrias et al. 2001a and
2001b). Recently the Anatomic Post’n Core (RTD, St Egrève, France) has been
introduced (Ferrari et al. 2002). This new post is made by a DT post n. 1 that is
covered by a light-curing resin (Lumiglass, RTD, St Egrève, France). The relining
resin is able, once introduced in the root canal, to produce a good fitting thus
reducing the amount of cement to be used and stabilizing the post during the luting
procedures.
The final test for a clinical procedure is always the clinical evaluation. Many studies
reported on the use of fiber post to restore endodontically-treated teeth (Malferrari et
al. 2003, Ferrari et al. 2000a and 2000b, Fredriksson et al. 1998, Monticelli et al.
2003, Dallari et al. 1998, Scotti et al. 2002). The majority of them combines the use
of fiber post restorations with ceramic or ceramometal crowns. The last few years
have seen an enormous expansion in the indications for dire
restorations (Hickel et al. 2004). Thus, it is interesting to evaluate the performances
of fiber posts when they were used in conjunction with direct resin restorations,
without additional crown coverage. After 30 months of clinical service, root-treated
teeth restored with fiber posts and direct resin composite restorations exhibited no
root fractures and favourable clinical results.
Conclusions and recommendations
The following conclusions and recommendations may be drawn from our basic and
clinical evaluations on the use of fiber posts in dentistry:
1) Fiber posts exhibit good overall mechanical properties and the related failure
modes are usually more conservative and favorable when compared to metallic
posts.
2) Endodontic procedures can influence the final result of the post restoration. Great
attention should be placed in the removal of bacteria, debris and other materials
inside the root canal before the filling is completed.
133

3) Fiber posts contribute to the filling sealing of the root canal space with the help of
adhesive cementation. For this reason they can be considered as part of the
endodontic treatment.
4) There are several brands of fiber posts. The quality of the bonding between the
fibers and the resin may influence the final quality of the whole post, and this should
be taken into account when selecting a fiber post together with composition, desired
shape, basic and experimental evaluation.
5) As far as luting procedures are concerned, a reliable bonding between the fiber
post-resin cement unit and the root canal can be reasonably well achieved with the
use of acid etching, that has to removed meticulously from the root canal with a
syringe and an endodontic needle.
6) A fourth or fifth generation adhesive system, inserted in the canal with the help of
a microbrush, and a dual-curing resin cement can be recommended when using
translucent fiber posts.
7) An individual post (Anatomic Post’n Core) can be of great help in a clinical
situation where there is a great loss of coronal structure and root canals after
endodontic treatment end up in a non-rounded shape.
8) Fiber posts can be safely used in combination with ceramic or ceramo-metal
crowns. Indications for their use are rapidly expanding, and recent clinical studies
indicated that they can be safely used as a foundation for direct resin composite
crowns. With the use of this technique, the restoration of the endodontically treated
teeth can be easier and less costly.
134

Riassunto e conclusioni
Il restauro del dente trattato endodonticamente ha da sempre rappresentato una
te trattato endodonticamente differisce da
più cedevole all’interno (la dentina). La carie e la
72), un aumento del modulo di Young (Huang et al. 1992),
io-meccanico del dente sotto
generale, la rimozione del tetto della camera
ulpare, insieme alle procedure endodontiche, è responsabile di una riduzione
complessiva della resistenza alla frattura (Fuzzi 1993, Morgano et al. 1993, Trabert
et al. 1978, Milot et al. 1992).
La possibilità di sopravvivenza nel cavo orale di un dente trattato endodonticamente
è direttamente proporzionale alla qualità ed alla quantità della struttura dentale
residua (Assif et al. 1994, Guttman 1992, Cohen et al. 1996). Tradizionalmente,
veniva inserito un perno per assicurare ritenzione alla ricostruzione coronale e per
“rinforzare” il dente. Attualmente, l’eventuale rinforzo determinato da un perno
metallico non può più essere considerato possibile (Shillimburg HT 1997), poichè
esso “…non rinforza significativamente il dente trattato endodonticamente…”
grossa sfida, e negli ultimi 15 anni i perni in fibra hanno acquisito una grossa
importanza in questo campo. Questa tesi contiene uno studio riguardante diversi
aspetti scientifici di base e clinici in relazione all’uso dei perni in fibra.
La letteratura scientifica mostra che un den
un dente sano. Molti cambiamenti avvengono in termini di proprietà chimiche,
fisiche ed elastiche della dentina, di resistenza alla fatica, morfologia e
comportamento bio-meccanico. Un dente vitale presenta una struttura più rigida (lo
smalto) all’esterno ed un supporto
preparazione per il trattamento endodontico sono i primi fattori che possono ridurre
la resistenza complessiva del dente. Vi è inoltre un decremento nel contenuto di
umidità (Helfer et al. 19
ed una riduzione nella percentuale di fibrille collageniche nella dentina (Mason
2001, Hashimoto et al. 2000, Ferrari et al. 2004). Altri cambiamenti avvengono
anche riguardo la morfologia ed il comportamento b
stress (Grimaldi 1971, Tidmarsh 1976). La preparazione della cavità di accesso per
il trattamento endodontico provoca la perdita sia del tetto della camera pulpare che
del collegamento fra le creste marginali, ed è considerata una delle possibili cause
che portano all’elevata incidenza di fratture documentata nei premolari superiori
(Ross et al. 1980, Salis et al. 1987). In
p
135

(Sorensen 1984a). I progressi fatti nel campo della tecnologia dei materiali rinforzati
on fibra hanno migliorato la struttura, le proprietà di trasmissione della luce e la
ti sono stati
unatamente questi reports sono stati pubblicati su
c
forma dei perni in fibra attualmente disponibili sul mercato. Questo ha portato allo
sviluppo di materiali che hanno superato alcune delle limitazioni dei perni metallici
(platino, leghe o titanio) riguardanti le proprietà estetiche, la modalità di fallimento
ed i risultati clinici. In termini di estetica, i perni in fibra translucen
introdotti in commercio per supportare restauri anteriori estetici (Vichi et al. 2000a
and 2000b, Ferrari et al. 2001a and 2001b, Ferrari et al. 2002, Paul et al. 1998,
Heydecke et al. 2002). Per quanto riguarda il comportamento bio-meccanico e la
modalità di fallimento, è stato dimostrato che i perni metallici tendono a produrre
fratture irreversibili. All’opposto, le fratture che avvengono con i perni in fibra sono
generalmente posizionate più coronalmente e sono più facili da ritrattare (Akkayan
et al. 2002, Cornier et al. 2001, Reagan et al. 1999, Newman et al. 2003). Questo
tipo di fallimento può essere dovuto alla maggior quantità di struttura dentale che
deve essere rimossa per il posizionamento di un perno metallico (Stankiewitz et al.
2002). Nel caso in cui sia necessario eseguire un ritrattamento endodontico, i perni
in fibra possono essere rimossi più facilmente dei perni metallici e dei perni
ceramici (Gesi et al. 2003, Hauman et al. 2003). In conclusione, i perni in fibra
possono essere adoperati allo scopo di ritenere i restauri coronali in denti trattati
endodonticamente; se comparati ai perni metallici o in zirconio sono in grado di
preservare una maggiore quantità di struttura dentale residua grazie al loro
comportamento bio-meccanico ed alle relative procedure di cementazione.
Sono state riportate tecniche cliniche per il restauro del dente trattato
endodonticamente con resine composite per ripristinare la struttura dentale residua e
per rinforzare la radice. Sfort
riviste prive di revisione da parte di esperti (Freedman et al. 1994, Godder et al.
1994, Martelli 2000, Castellucci 2004).
Uno studio recente ha comparato la resistenza alla frattura e le modalità di
fallimento di premolari superiori trattati endodonticamente con un numero
progressivo sempre minore di pareti residue, che sono state ricostruite usando resine
composite con o senza perni in fibra translucenti (Sorrentino et al. 2004). Questo
modello di studio ha mostrato che il numero di pareti residue influenza la resistenza
136

meccanica dei denti sottoposti a carico: in campioni con lo stesso numero di pareti
residue sono state registrati valori più elevati di resistenza alla frattura nei denti
“rinforzati” con perni in fibra. Inoltre, nei campioni ricostruiti con i perni in fibra le
fratture osservate erano “favorevoli”, quindi fratture facilmente riparabili in quanto
avvenute al di sopra della cresta ossea. Se questi dati dovessero essere confermati da
studi clinici, il concetto di “rinforzare” le strutture radicolari con l’adesione al canale
di perni in fibra sarà indiscutibilmente rafforzato.
Un trattamento endodontico efficace risulta essere un fattore chiave nell’ambito del
restauro del dente trattato endodonticamente. Di basilare importanza risultano la
rimozione di detriti e materiale organico dall’interno del canale (Castellucci 1993) e
la preparazione meccanica del canale stesso per ricevere un materiale da otturazione
(Ingle 1993). L’influenza dei cementi e delle soluzioni irriganti è stata discussa
ampiamente in letteratura. Valutando l’effetto di diverse soluzioni irriganti
nell’ottenere un canale libero da impurità dopo il trattamento endodontico (Grandini
et al. 2002b), si è verificato che nessuna delle tecniche usate nello studio in oggetto
si è dimostrata perfettamente efficace nel rimuovere completamente fango dentinale
e detriti. Ad ogni modo, una combinazione di ipoclorito di sodio e di un agente
chelante possono efficacemente rimuovere gran parte dei detriti dal canale. Gli scopi
dell’otturazione canalare sono essenzialmente quelli di sigillare il canale radicolare e
prevenire l’ulteriore eventuale microinfiltrazione. In questo senso, il posizionamento
di un perno in fibra può aiutare a fornire un sigillo efficace contro l’infiltrazione
batterica coronale (Trope 2004). Sfortunatamente, a causa dell’elevato fattore C
desivamente sia data dal contributo della
presente nei canali radicolari (Morris et al., 2002; Bouillaguet et al., 2003; Goracci
et al., 2004), sono state registrate difficoltà nella cementazione dei perni in fibra alla
dentina intra-radicolare con i cementi resinosi. Si è speculato che, come per l’uso di
cementi non adesivi, una elevata quota parte della resistenza alla dislocazione
incontrata nei perni in fibra cementati a
frizione da contatto del perno stesso e del cemento resinoso all’interno del canale
radicolare (Goracci et al., 2005).
La sempre maggiore popolarità incontrata dai restauri con perni in fibra ha imposto
la necessità di una valutazione sistematica dei diversi tipi e qualità dei perni in fibra
ad oggi presenti sul mercato. I criteri di scelta sono generalmente basati sulla
137

composizione e forma dei perni, costo, procedure di cementazioni adesive,
valutazioni sperimentali in vivo e in vitro. Uno studio ha comparato la resistenza alla
fatica e le caratteristiche strutturali di diversi tipi di perni in fibra (Grandini et al.
2004a). Alcuni tipi di perni in fibra possono facilmente resistere fino a 2.000.000 di
cicli di fatica senza cambiamenti alla loro struttura. In particolare, la qualità
dell’adesione e del legame fra le due componenti del perno in fibra (le fibre e la
matrice di resina epossidica) può influenzare la qualità del perno stesso. Infatti,
perno con resina composita, un materiale cioè
l’impatto statico e la resistenza alla fatica sono proporzionali alla forza di adesione
dell’interfaccia riempitivo/resina nei sistemi compositi rinforzati con fibre (Zhao et
al. 2000, Kessler et al. 2000, Keusch et al. 1999). Uno studio recente ha confermato
che all’aumentare della forza di adesione tra il riempitivo e la matrice si ottiene un
incremento delle proprietà meccaniche dei compositi rinforzati con fibre (Debnath et
al. 2004).
Le procedure di cementazione sono un fattore estremamente importante nell’ambito
del restauro con perni in fibra, e sono da tempo state descritte nella letteratura
internazionale (Ferrari et al. 2001a and 2001b, Vichi et al. 2002a). La mordenzatura
acida, l’uso di adesivi di quarta o quinta generazione, e di un cemento resinoso duale
porta a risultati clinici ottimali. Il fatto di lasciare la soluzione adesiva non
polimerizzata prima del posizionamento del cemento (one-step procedure), allo
scopo di ridurre il tempo necessario per la cementazione, produce risultati clinici
sfavorevoli sia dal punto di vista clinico che sperimentale (Grandini et al. 2004b).
Nel caso si scelga di eseguire una corona dopo il posizionamento del perno in fibra,
il perno stesso può essere aggiustato in lunghezza dopo il restauro del core. Invece,
nel caso in cui si scelga un restauro conservativo, è preferibile aggiustare la
lunghezza del perno prima di procedere alla cementazione, in modo da poter
eseguire al contempo cementazione del perno e ricostruzione adesiva avvalendosi di
un’unica fase di mordenzatura ed adesione. Il taglio del perno può avvenire con un
disco di carborundum o con una fresa diamantata (Grandini et al. 2002a). In questo
modo è possibile ricoprire la testa del
maggiormente capace di resistere alle sollecitazioni dell’usura dente contro dente e
dente contro cibo. Se siamo di fronte ad un perno di buona qualità, la procedura di
taglio non modificherà l’integrità strutturale del perno stesso.
138

Negli anni molti cambiamenti hanno riguardato i materiali impiegati per la
fabbricazione dei perni in fibra: il carbonio è stato il primo materiale impiegato;
quindi il vetro, il quarzo e la silice, con particolare riguardo alle capacità di
trasmissione della luce. Interessanti sviluppi hanno inoltre riguardato la forma dei
perni stessi, partendo dal doppio cilindro originale, fino alle forme endodontiche ed
ai più recenti perni a doppia conicità. Infatti la cementazione adesiva permette di
affidarsi alla formazione di zaffi resinosi e strato ibrido piuttosto che alla forma
ritentiva, alla ritenzione meccanica ed al perfetto adattamento del perno all’interno
delle pareti canalari (Ferrari et al. 2002). Inoltre, nel conseguire l’adattamento del
perno, una maggiore varietà di perni disponibili sul mercato permette all’operatore
di selezionare quello più appropriato allo scopo di risparmiare la maggior quantità di
struttura dentale residua. La decementazione avviene più facilmente in assenza
dell’auspicabile “effetto ferula”, o in presenza di un elevato spessore di cemento nel
a
n fibra per il restauro
quale è più verosimile che si verifichi l’intrappolamento di bolle d’aria che può
portare appunto alla decementazione (Ferrari et al. 2000a). L’idea di avere un perno
individuale, che si adatti perfettamente al singolo spazio canalare è decisamente
attraente per l’operatore, specialmente quando si tratti di canali con forma ellittica
così come i canini ed i premolari. In questi casi il clinico è costretto ad adattare la
struttura dentale residua al perno attraverso la rimozione di un’ulteriore quantità di
dentina, o a cementare un perno affidandosi ad una maggiore quantità e spessore di
cemento. Al contrario, sarebbe desiderabile che il perno si adattasse all’anatomi
canalare prodotta dal trattamento endodontico. Questo è infatti il fondamento logico
alla base della creazione del perno anatomico (Grandini et al 2000, Boudrias et al.
2001a and 2001b). Recentemente è stato introdotto l’ Anatomic Post’n Core (RTD,
St Egrève, France) (Ferrari et al. 2002). Questo nuovo perno è composto da un perno
a doppia conicità (DT) numero 1, ricoperto da una resina foto-polimerizzabile
(Lumiglass, RTD, St Egrève, France). La resina ribasante è in grado, una volta
introdotta nel canale, di produrre un buon fitting fra perno ribassato e pareti canalari,
riducendo la quantità di cemento e stabilizzando il perno durante le procedure di
cementazione.
Ma il test decisivo e finale per una procedura è sempre la valutazione clinica. Molti
studi presenti in letteratura hanno riguardato l’uso dei perni i
139

del dente trattato endodonticamente (Malferrari et al. 2003, Ferrari et al. 2000a and
2000b, Fredriksson et al. 1998, Monticelli et al. 2003, Dallari et al. 1998, Scotti et
al. 2002). La maggior parte di essi combina l’uso di restauri con perni in fibra e
corone in ceramica o metallo-ceramica. Negli ultimi anni abbiamo assistito ad una
enorme espansione delle indicazioni per i restauri diretti in resina composita (Hickel
et al. 2004). Perciò è interessante valutare i risultati dei perni in fibra in
combinazione con restauri diretti in resina composita, senza copertura protesica.
Dopo 30 mesi di servizio clinico, i denti trattati endodonticamente ricostruiti con
perni in fibra e restauri diretti in resina composita hanno mostrato risultati clinici
favorevoli senza fratture radicolari.
Conclusioni e raccomandazioni
Sulla base delle valutazioni cliniche e sperimentali possiamo trarre le seguenti
conclusioni e raccomandazioni riguardo l’uso dei perni in fibra in odontoiatria.
1) I perni in fibra hanno mostrato buone proprietà meccaniche ed il relativo modo di
fallimento è generalmente più conservativo e favorevole di quello mostrato dai perni
metallici.
2) Le procedure endodontiche possono influenzare il risultato finale del restauro con
perno. Deve essere posta grande attenzione nella rimozione di batteri, detriti ed altri
materiali dall’interno del canale prima di procedere all’otturazione canalare.
3) I perni in fibra possono contribuire al sigillo dello spazio canalare con l’aiuto
della cementazione adesiva. Per questa ragione possono essere considerati come
parte del trattamento endodontico.
4) Ci sono diversi tipi di perni in fibra. La qualità del legame tra le fibre e la matrice
può influenzare la qualità globale del perno, e questo dovrebbe essere preso in
considerazione al momento della scelta del perno, insieme alla composizione, alla
forma, ed alla valutazione di base e clinica.
5) Per quanto riguarda le procedure di cementazione, un legame affidabile fra perno
in fibra, cemento, sistema adesivo e canale radicolare può essere raggiunto con la
mordenzatura acida. Il mordenzante deve essere accuratamente rimosso dal canale
radicolare con una siringa contenente acqua ed un ago endodontico.
140

6) Un sistema adesivo di quarta o di quinta generazione, veicolato nel canale con
l’aiuto di un microbrush, ed un cemento resinoso duale possono essere adoperati con
i perni in fibra translucenti.
7) Un perno individuale (Anatomic Post’n Core) può essere di grande aiuto in
situazioni cliniche dove si abbia grossa perdita di struttura coronale ed un canale che
risulta non circolare dopo il trattamento endodontico.
8) I perni in fibra possono essere adoperati con sicurezza in combinazione con
restauri protesici in ceramica o in metallo-ceramica. Le indicazioni per il loro uso
sono in rapida espansione, e studi clinici recenti indicano che possono essere
adoperati anche come base per un restauro diretto in resina composita. Con questa
cnica, il restauro del dente trattato endodonticamente può essere più semplice e più te
economico.
141

Résumé et conclusions
Depuis longtemps la restauration de la dent traitée endodontiquement représente un
ploi des tenons en fibres.
réparation pour le traitement endodontique sont les premiers facteurs
ui peuvent réduire la résistance globale de la dent. Il y a aussi une diminution de
umidité contenue dans la dentine (Helfer et al. 1972), une augmentation du module
e Young (Huang et al. 1992), et une réduction du pourcentage de fibrilles de
collagène dans la dentine (Mason 2001, Hashimoto et al. 2000, Ferrari et al. 2004).
D’autres changements surviennent aussi dans la morphologie et le comportement
biomécanique de la dente soumise à des contraintes (Grimaldi 1971, Tidmarsh
1976). La préparation de la cavité d’accès pour le traitement endodontique provoque
la perte du toit de la chambre pulpaire et aussi de la liaison entre les crêtes
marginales, et elle est considérée comme une des causes possibles entraînant le taux
important de fractures que l’on rencontre dans les prémolaires supérieures (Ross et
al. 1980, Salis et al. 1987). En général, le déplacement du toit de la chambre
pulpaire, avec les procédures endodontiques, est responsable d’une réduction
globale de la résistance à la fracture (Fuzzi 1993, Morgano et al. 1993, Trabert et al.
1978, Milot et al. 1992).
La possibilité de survie dans la cavité orale d’une dent traitée endodontiquement est
directement proportionnelle à la qualité et à la quantité de la structure dentaire
restante (Assif et al. 1994, Guttman 1992, Cohen et al. 1996). Traditionnellement,
un tenon était mis en place pour assurer la rétention à la reconstruction coronaire et
pour renforcer la dent. Actuellement, l’éventuelle consolidation déterminée par un
tenon métallique ne peut plus être considérée possible (Shillimburg HT 1997),
grand défi, et durant les 15 dernières années les tenons en fibre ont acquis une
énorme importance dans ce domaine. Cette thèse est une étude sur les différents
aspects scientifiques de base et cliniques relatifs à l’em
La littérature scientifique démontre qu’une dent traitée diffère d’une dente saine.
Plusieurs changements se produisent en termes de propriétés chimiques, physiques
et élastiques de la dentine, de résistance à la fatigue, de la morphologie et du
comportement biomécanique. Une dente vital présente une structure plus rigide
(l’email) à l’extérieur et un support plus malléable à l’intérieure (la dentine). Les
caries et la p
q
h
d
142

puisqu’il “…ne fortifie pas de façon significative la dent traitée
ndodontiquement… ” (Sorensen 1984a). Les progrès faits dans le domaine de la
ont
s résines composites au fin de rétablir la structure dentaire
e
technologie des matériaux renforcés avec de la fibre ont amélioré la structure du
tenon, la propriété de transmission de la lumière et la forme des tenons en fibres
actuellement disponible sur le marché. Ces progrès concernant les propriétés
esthétiques, les modalités d’échec et les résultats cliniques des tenons fibrés
permis de dépasser quelques unes des limitations des tenons métalliques (platine,
titane ou alliages). En termes d’esthétique, les tenons fibrés translucides ont été
introduits sur le marché pour soutenir les restaurations antérieures esthétiques (Vichi
et al. 2000a and 2000b, Ferrari et al. 2001a and 2001b, Ferrari et al. 2002, Paul et al.
1998, Heydecke et al. 2002). En ce qui concerne le comportement biomécanique et
le mode d’échec, il a été démontré que les tenons métalliques tendent à produire des
fractures irréversibles. A l’inverse, les fractures qui se produisent avec les tenons en
fibres sont en général en position plus coronaire et sont plus faciles à retraiter
(Akkayan et al. 2002, Cornier et al. 2001, Reagan et al. 1999, Newman et al. 2003).
Ce type d’échec peut être dû à la plus grande quantité de structure dentaire qui doit
être déplacée pour placer les tenons métalliques (Stankiewitz et al. 2002). Au cas où
il serait nécessaire d’effectuer le retraitement endodontique, les tenons en fibres sont
plus faciles à déposer que les tenons métalliques et les tenons céramiques (Gesi et al.
2003, Hauman et al. 2003). En conclusion, les tenons en fibres peuvent être
employés dans le but de retenir les restaurations coronaires dans les dents traitées
endodontiquement ; si on les compare aux tenons métalliques ou en zirconium, ils
sont à même de préserver une plus grande quantité de structure dentaire restante
grâce à leur comportement biomécanique et aux procédures associées de scellement.
La littérature décrit des techniques cliniques pour la restauration de la dent traitée
endodontiquement avec de
restante et pour renforcer la racine. Malheureusement ces rapports ont été publiés sur
des revues sans aucune révision des experts (Freedman et al. 1994, Godder et al.
1994, Martelli 2000, Castellucci 2004).
Une étude récente a comparé la résistance à la fracture et les modalités de faillite de
prémolaires supérieures traitées endodontiquement avec un nombre progressif
toujours plus petite de parois restantes, qui ont été reconstruites avec des résines
143

composites avec ou sans tenons en fibres translucides (Sorrentino et al. 2004). Ce
modèle d’étude a démontré que le nombre de parois restantes influence directement
la résistance mécaniques des dents soumises à une charge. Des échantillons avec le
même nombre de parois restantes ont permis d’enregistrer des valeurs plus élevées
de résistance à la fracture dans les dents « renforcées » avec des tenons en fibres. De
plus, dans les échantillons reconstruits avec les tenons en fibres, les fractures
observées étaient « favorables », c'est-à-dire des fractures facilement réparables car
elles s’étaient produites au dessus de la crête osseuse. Si ces données peuvent être
confirmées par des études cliniques, l’idée de « renforcer » les structures radiculaires
avec le collage canalaire des tenons en fibres sera sans aucun doute renforcé.
Un traitement endodontique efficace se révèle être un facteur clef dans les limites de
la restauration de la dent traitée endodontiquement. Un traitement performant est
basé sur l’enlèvement de débris et de matière organique de l’intérieure du canal
(Castellucci 1993) et la préparation mécanique de ce canal pour recevoir un matériau
d’obturation (Ingle 1993). L’influence des ciments et des solutions irrigantes a été
amplement discutée en littérature. D’après l’évaluation de l’effet de différentes
solutions irrigantes dans le but d’obtenir un canal exempt d’impuretés après le
traitement endodontique (Grandini et al. 2002b), il a été vérifié qu’aucune des
techniques employées dans l’étude ne s’est montrée parfaitement efficace pour
enlever complètement la boue et les détritus. Cependant, une combinaison
d’hypochlorite de sodium et d’un agent chélatant peut efficacement enlever une
grande partie des détritus du canal. Les fonctions de l’obturation canalaire sont
essentiellement de sceller le canal radiculaire et de prévenir une éventuelle micro
infiltration ultérieure. Dans ce sens, le placement d’un tenon en fibres peut aider à
fournir un sceau efficace contre l’infiltration bactérienne coronaire (Trope 2004).
Malheureusement, à cause de « facteur C » élevé présente dans les canaux
radiculaires (Morris et al., 2002; Bouillaguet et al., 2003; Goracci et al., 2004), on a
enregistré des difficultés dans le scellement des tenons en fibres à la dentine intra
radiculaire avec les ciments résineux. On croit que, comme pour l’emploi de ciments
non adhésifs, une résistance au dé-scellement rencontré dans les tenons en fibres
cimentés adhésivement est donnée par la friction du contact tenon-ciment résineux à
l’intérieur du canal radiculaire (Goracci et al., 2005).
144

La popularité toujours croissante rencontrée par les restaurations avec les tenons en
fibres a imposé la nécessité d’une évaluation systématique des différents types et de
la qualité des tenons en fibre aujourd’hui présents sur le marché. Les critères de
choix en général sont fondés sur la composition et la forme des tenons, les coûts, sur
les procédures de scellement adhésif, les évaluations expérimentales in vivo et in
vitro. Une étude a comparé la résistance à la fatigue et les caractéristiques
structurales de différents types de tenons en fibre (Grandini et al. 2004a). Quelques
types de tenons en fibres peuvent facilement résister jusqu’à 2.000.000 de cycles de
fatigue sans aucune conséquence à leur qualité générale. En particulier, la qualité de
l’adhésion et du lien entre les deux composants du tenon en fibre (les fibres et la
n adhésive en se servant d’une
matrice de résine époxydique) peut influencer la qualité du tenon lui-même. En
effet, la résistance à la charge statique et la résistance à la fatigue, sont
proportionnelles à la force d’adhésion de l’interface charges-résine, dans les
systèmes composites renforcés avec des fibres (Zhao et al. 2000, Kessler et al. 2000,
Keusch et al. 1999). Une étude récente a confirmé que l’augmentation de la force de
adhésion entre les charges (fibres) et la matrice conduit à un accroissement des
propriétés mécaniques des composites renforcés avec des fibres (Debnath et al.
2004).
Les procédures de collage/scellement sont un facteur extrêmement important dans le
domaine de la restauration avec des tenons en fibres, et elles ont été depuis
longtemps décrites dans la littérature internationale (Ferrari et al. 2001a and 2001b,
Vichi et al. 2002a). Le mordançage acide, l’emploi d’ adhésifs de quatrième ou
cinquième génération et d’un ciment résineux dual conduit à des résultats cliniques
optimales. Le fait de laisser la solution adhésive non polymérisée avant le placement
du ciment (« One-Step procédure ») afin de réduire le temps nécessaire pour le
scellement, conduit à des résultats cliniques défavorables tant du point de vue
clinique qu’expérimental (Grandini et al. 2004b).
Le tenon peut être ajusté à la longueur adéquate après la restauration du faux-
moignon dans le cas où une couronne recouvre l’ensemble. Dans le cas contraire, au
cas où l’on choisit une restauration conservative, il est préférable d’ajuster la
longueur du tenon avant de procéder au scellement de manière à pouvoir exécuter en
même temps le scellement du tenon et la reconstructio
145

phase unique de mordançage et de collage. La section tenon peut s’effectuer à l’aide
d’un disque de carborundum ou une fraise diamantée (Grandini et al. 2002a). De
cette façon il est possible de recouvrir la tête du tenon avec de la résine composite,
c'est-à-dire un matériau capable de supporter les contraintes dent contre dent ou des
contraintes masticatoires. Si l’on est en face d’un tenon de bonne qualité, la
procédure de coupure ne modifiera pas l’intégrité de la structure du tenon.
Pendant des années beaucoup de changements ont concerné les matériaux employés
pour la fabrication des tenons en fibres : les fibres de carbone ont été la première
fibre employée ; après la fibre de verre, de quartz et de silice, avec une attention
particulière aux capacités de transmission de la lumière. Des développements
intéressants ont eu lieu sur la forme des tenons, partant du double cylindre original,
jusqu’aux formes endodontiques et aux plus récents tenons à double conicité. En
effet la cimentation adhésive permet de se confier à la formation de « resin tags » et
à la couche hybride plutôt qu’à la rétention mécanique et à la parfait ajustement du
tenon (Ferrari et al. 2002). De plus, pour obtenir l’adaptation du tenon, une plus
grande variété de tenons disponibles sur le marché permet au clinicien de
sélectionner le tenon le plus approprié afin d’économiser la plus grande quantité de
structure dentaire restante. Le descellement survient plus facilement en l’absence du
le que le tenon s’adapte à
souhaitable « Ferrule effect» ou en présence d’une épaisseur élevée de ciment dans
laquelle vraisemblablement des bulles d’air se sont formées conduisant au
descellement (Ferrari et al. 2000a). L’idée d’avoir un tenon sur-mesure, qui s’ajuste
parfaitement à chaque espace du canal est décidément attrayant pour le praticien,
surtout quand il s’agit de canaux à forme elliptique telle que les dents canines et les
prémolaires. Dans ces cas le clinicien est obligé d’adapter la structure dentaire
restante au tenon à travers l’enlèvement d’une quantité ultérieure de dentine, ou à
sceller un tenon plus petit, par conséquent d’avoir une plus grande épaisseur de
ciment. Dans le cas contraire , il serait souhaitab
l’anatomie du canal produite par le traitement endodontique. En effet c’est le
fondement logique à la création du tenon anatomique (Grandini et al 2000, Boudrias
et al. 2001a and 2001b). Récemment le tenon Anatomic Post’n Core (RTD, St
Egrève, France) (Ferrari et al. 2002) a été introduit. Ce nouveau tenon est composé
d’un tenon à double conicité (DT) numéro 1 recouvert par un résine photo-
146

polymérisable (Lumiglass, RTD, St Egrève, France). La résine qui environne le
tenon est à même, une fois introduite dans le canal, de produire un bon ajustement
entre le tenon et le parois du canal, en réduisant la quantité de ciment et en
stabilisant le tenon pendant les procédures de scellement.
De toute façon le test décisif pour une procédure clinique est toujours l’évaluation
clinique. Beaucoup d’études publiées se sont concentrées sur l’emploi des tenons
fibrés pour la restauration de la dent traitée endodontiquement (Malferrari et al.
2003, Ferrari et al. 2000a and 2000b, Fredriksson et al. 1998, Monticelli et al. 2003,
Dallari et al. 1998, Scotti et al. 2002). La plus grande partie d’entre eux combine
l’emploi des restaurations avec des tenons fibrés et des couronnes en céramique ou
métallo-céramique. Une énorme expansion des indications pour les restaurations
directes en résine composite s’est produite pendant ces dernières années(Hickel et al.
2004). Pour cela il est intéressant d’évaluer les performances des tenons fibrés en
combinaison avec des restaurations directes en résine composite, sans être
recouverts par une prothèse dentaire. Après 30 mois de service clinique, les dents
traitées endodontiquement reconstruites avec des tenons en fibres et des
restaurations directes en résine composite ont démontré des résultats cliniques
favorables sans fractures radiculaires.
Conclusions et recommandations
En ce qui concerne l’emploi des tenons en fibres en dentisterie, selon les résultats
issus de nos évaluations cliniques et expérimentales, les conclusions et
recommandations suivantes peuvent être comme suit :
1) Les tenons fibrés ont montré de bonnes propriétés mécaniques et le mode d’échec
est en général plus favorable et conservateur que celui des tenons métalliques.
2) Les procédures endodontiques peuvent influencer le résultat final de la
restauration avec le tenon. Une grande attention doit être portée à l’enlèvement de
bactéries, de débris et d’autres matériaux à l’intérieur du canal avant d’obturer le
canal.
3) Les tenons en fibres peuvent contribuer au seau de l’espace canalaire avec l’aide
du scellement adhésif Pour cela ils peuvent être considérées comme une partie
intégrante du traitement endodontique.
147
4) Plusieurs marques de tenons existent. La qualité de la liaison entre les fibres et la
matrice peut influencer sur la qualité finale du tenon, et ceci devrait être pris en
considération au moment du choix du tenon, en même temps que la composition, la
forme, et l’évaluation de base et clinique.
5) En ce qui concerne les procédures de scellement, un lien fiable entre tenon fibré,
le système adhésif et le canal radiculaire peut être atteint avec l’emploi du
mordançage acide. L’acide de mordançage doit être enlevé soigneusement avec une
seringue et une aiguille endodontique.
6) Un système adhésif de quatrième ou de cinquième génération, inséré dans le canal
à l’aide d’un applicateur Microbrush®, et un ciment résineux duale peuvent être
employé avec les tenons en fibre translucides.
7) Un tenons sur-mesure (Anatomic Post’n Core®) peut être d’une grande aide dans
une situation clinique où une perte importante de substance coronaire et canalaire a
conduit à une forme non circulaire après le traitement endodontique.
8) Les tenons en fibre peuvent être employés en toute sécurité en combinaison avec
des restaurations prothétiques en céramique ou métallo-céramique. Les indications
pour leur usage sont en constante progression, et des études cliniques récentes ont
démontré qu’ils peuvent être employées aussi comme élément de base pour une
stauration directe en résine composite. Avec cette technique, la restauration de la
tre plus simple et plus économique.
re
dent traitée endodontiquement peut ê
148
Schlußfolgerung
Schon immer war die Restauration endodontisch behandelter Zähne eine
Herausforderung für den Zahnarzt. Im Laufe der letzten 15 Jahre haben Faserstifte
einer Wurzelkanalbehandlung können viele
ail) und eine darunter liegende
odulus erhöht
ßt, die in
berkiefer-Prämolaren angetroffen werden (Ross et al. 1980, Salis et al. 1987). Im
Allgemeinen ist die Entfernung der Pulpakammerdecke, zusammen mit der
endodontischen Behandlung verantwortlich für eine Verringerung der
Frakturresistenz (Fuzzi 1993, Morgano et al. 1993, Trabert et al. 1978 , Milot et al.
1992)
Bekanntlich hängt das Überleben von pulpalosen Zähnen direkt von Menge und
Qualität der verbliebenen Zahnstruktur ab (Assif et al. 1994, Guttman 1992, Cohen
et al. 1996).
Bisher wurde ein Stift eingesetzt, um den Kern zu befestigen und den Zahn zu
“verstärken”. Heute ist die Verstärkung der Zahnwurzelstruktur durch Metallstifte
widerlegt (Shillimburg HT 199), denn sie „...verstärken endodontisch behandelte
Zähne nicht signifikant..“ (Sorensen 1984a). Im Zuge des technischen Fortschritts in
an Bedeutung gewonnen. Die vorliegende Arbeit untersucht mehrere grundsätzliche
und klinische Aspekte zu Wahl und Anwendung von Faserstiften. Es ist
wissenschaftlich bewiesen, dass sich ein gesunder Zahn von einem endodontisch
behandelten Zahn unterscheidet. Nach
Veränderungen auftreten bezüglich physischer, chemischer und elastischer
Eigenschaften, Ermüdungsresistenz, Morphologie und biomechanischem Verhalten.
Ein vitaler Zahn hat eine steifere Struktur (Em
nachgiebige und unterstützende Schicht (Dentin). Karies und endodontische
Zahnaufbereitung sind die ersten Faktoren, die den Zahn schwächen können. Der
Feuchtigkeitsgehalt verringert sich (Helfer et al. 1972), Young’s M
sich (Huang et al. 1992), die Anzahl der Kollagenfibrillen im Dentin nimmt ab
(Mason 2001, Hashimoto et al. 2000, Ferrari et al. 2004). Weiterhin können sich
unter Stress Veränderungen in der Morphologie und im biomechanischen Verhalten
der Zähne ergeben (Grimaldi 1971, Tidmarsh 1976). Die Zugangsaufbereitung für
eine endodontische Behandlung führt zum Verlust der Pulpakammerdecke und der
Randleisten, was die relativ hohe Anzahl von Frakturen beeinflu
O
149

faserverstärkten Materialien wurden Struktur, Form und optische Eigenschaften
serverstärkter Harzstifte verbessert, und trugen zur Entwicklung von Materialien
Frakturwiderstand und Fehlermuster endodontisch behandelter Oberkiefer-
al. 2004). Diese Studie zeigt, dass die Menge der Kanalwandreste den
fa
bei, die über die Grenzen der Metallstifte (Platin, Legierungen oder Titan)
hinausgehen, insbesondere in Bezug auf ihre ästhetische Erscheinung, ihre
Fehlermechanismen und klinische Leistung. Wegen der Ästhetik und zur
Unterstützung bei Frontzahn-Revisionen wurden transluzente Faserstifte eingeführt
(Vichi et al. 2000a und 2000b, Ferrari et al. 20002, Paul et al. 1998, Heydecke et al.
2002). Was das mechanische Verhalten und die Fehlermechanismen der Faserstifte
angeht, wurde festgestellt, dass Versagen von Metallstiften zu irreversiblen
Wurzelfrakturen tendieren. Jedoch entstehen Wurzelfrakturen bei Faserstiften eher
im koronaren Bereich, und sie sind leichter zu behandeln (Akkayan et al. 2002,
Cornier et al. 2001, Reagan et al. 1999, Newman et al. 2003). Der Grund für das
Versagen könnte darin liegen, dass für einen Metallstift eine größere Menge
Zahnstruktur entfernt werden muss (Staniewitz et al. 2002). Im Fall einer
endodontischen Revision, können Faserstifte leichter als Metall- oder Keramikstifte
entfernt werden (Geisi et al. 2003, Hauman et al. 2003). Abschließend: Faserstifte
eignen sich gut für die Retention von Harz-Komposit-Kernen. Im Vergleich zu
Metall- oder Zirkonstiften, sind sie dank ihres mechanischen Verhaltens und der
Zementierungstechniken, fähig, die verbleibende Wurzelstruktur zu bewahren.
Einige Restaurationstechniken endodontisch behandelter Zähne mit Harz-
Kompositen, die verloren gegangenes Wurzeldentin ersetzen und möglicherweise
die Wurzel stärken sollten, wurden beschrieben. Leider wurden diese Berichte ohne
wissenschaftliche Überprüfung veröffentlicht (Freedman et al. 1994, Godder et al.
1994, Martelli 2000, Castellucci 2004). In einer kürzlich durchgeführten Studie
wurden
Prämolaren mit zunehmend reduzierten Kanalwandresten untersucht, die mit Harz-
Komposit und mit oder ohne durchsichtige Glasfaserstifte restauriert wurden
(Sorrentino et
mechanischen Widerstand endodontisch behandelter Oberkiefer-Prämolaren
beeinflusst. Die mit Fasterstiften versorgten Exemplare zeigten, bei gleicher
Restwandmenge, höhere Bruchbelastungsgrenzen auf. Weiterhin wurden
restaurierbare Frakturen in mit Faserstiften restaurierten Exemplaren beobachtet.
150

Wenn diese Daten durch klinische Studien überprüft würden, könnte die Annahme
bestätigt werden, dass Wurzelkanalwände durch den Verbund mit Faserstiften
verstärkt werden.
Schlüsselfaktor für eine gelungene Restauration ist eine erfolgreiche endodontische
Aufbereitung. Für eine gut ausgeführte endodontische Behandlung müssen Debris
und organisches Material aus dem Wurzelkanal entfernt (Castellucci 1993), und der
Kanal zur Aufnahme des Obturationsmaterials mechanisch aufbereitet sein (Ingle
1993). Der Einfluss von Zementen und Irrigationslösungen wurde in der Literatur
ausführlich diskutiert. In einer Untersuchung über die Wirkung verschiedener
Irrigationsmethoden auf die Sauberkeit des Wurzelkanals nach endodontischer
Behandlung (Grandini et al. 2002b), wurde festgestellt, dass keine der in der Studie
benutzten Techniken einwandfreie Entfernung von Smear Layer und Debris
erreichte. Jedoch, wurde ebenfalls festgestellt, dass die Kombination von Natrium
Hypochlorit und einem Chelator helfen kann, die Debrismenge an den
Wurzelkanalwänden zu verringern. Die Hauptaufgabe der Wurzelkanalfüllung ist es,
den Wurzelkanal abzudichten und Undichtigkeit; Microleakage, zu verhindern. In
diesem Sinne kann die Herstellung und das Setzen eines Stiftes, wenn sie dazu
beitragen, den Raum im Wurzelkanal zu füllen und abzudichten, als Teil der
endodontischen Behandlung angesehen werden (Trope 2004). Wegen des hohen C-
Faktors, in den Stiftzwischenräumen (Morris et al., 2002, Bouillaguet et al., 2003,
Goracci et al., 2004), treten große Adhäsionsprobleme zwischen intra-radikularem
Dentin und Faserstift mit Hrz-Zementen auf. Man nimmt an, dass, ähnlich wie bei
nicht bindenden Zementen, auch bei den Faserstiften die Gleitfriktion im
Wurzelkanal zum großen Teil dazu führt, dass der Stift sich nicht löst (Goracci et
al., 2005). Da Restaurationen mit Faserstiften große Nachfrage finden, ist es
notwendig, die verschiedenen Marken und Typen auf dem Markt systematisch zu
untersuchen. Hierfür werden üblicherweise einige auf grundlegenden und
experimentellen Untersuchungen basierende Kriterien angewandt, wie z.B.
Komposition und Form des Stiftes, Kosten und Zementierungstechnik. Es gibt eine
Studie die Ermüdungswiderstand und Struktureigenschaften verschiedener
Faserstifte vergleicht (Grandine et al. 2004a). Einige Faserstiftmarken widerstehen
ohne Qualitätsbeeinträchtigung bis zu 2.000.000 Ermüdungs-Test-Zyklen.
151
Insbesondere die Verbundqualität zwischen zwei Komponenten eines Faserstiftes
(die Faser und die Harz Matrix) können die Qualität des Stiftes beeinflussen. In
faserverstärkten Komposit-Systemen verhalten sich statischer Druck und
Ermüdungseigenschaft proportional zur Stärke der Kontaktstelle von Füllung und
Harz (Zhao et al. 2000, Kessler et al. 2000, Keusch et al. 1999). Eine kürzlich
erschienene Studie bestätigt, dass die Anhebung der Verbundstärke zwischen
Füllmaterial und Matrix zur Verbesserung der mechanischen Eigenschaften
faserverstärkter Komposite führt (Debnath et al. 2004).
Bei Faserstiften sind die Verbundprozesse von großer Bedeutung. Die Technik
wurde bereits in der Literatur behandelt (Ferrari et al. 2001a und 2001b, Vichi et al.
2002a). Das Ätzen sowie die Verwendung von Adhäsiven der 4. und 5. Generation
und eines dual härtenden Zement-Harzes erzielen die besten klinischen Resultate.
Wenn die Adhäsiv-Lösung vor Anwendung des Zements nicht polymerisiert wird
(Einstufen-Prozedur), um die Zeit für die Zementierung zu verringern, ergibt das
ungünstige Resultate vom klinischen sowie experimentellen Standpunkt (Grandinie
et al. 2004b). Wenn eine Krone gesetzt wird, kann der Stift nach Restauration des
Kerns angepasst werden. Handelt es sich um eine direkte Restauration, wird
empfohlen, die Länge des Stiftes vor dem Verkleben anzupassen. Der Stift sollte mit
einer Korundscheibe oder einem Diamantbohrer geschnitten werden (Grandini et al.
2002a). So kann das abgeschnittene Stiftende mit Epoxyd-Komposit beschichtet
werden, ein Material, das fähiger als Faserstifte ist, der Zahn zu Zahn und Zahn zu
Essen Abnutzung zu widerstehen. Ein Stift von guter Qualität wird seine strukturelle
Integrität durch das Abschneiden nicht verändern.
Was das Material der Stifte betrifft, gibt es viele Neuentwicklungen: Karbon wurde
als erstes als Stiftmaterial verwendet, dann kamen Stifte aus Glas, Quarz und
Silizium wegen ihrer transluzenten Eigenschaften. Im Design gab es ebenfalls
interessante Entwicklungen, vom Original-Doppel-Zylinder, über endodontische
Formen bis hin zu den jüngeren Double-Taper-Stiften. Hier beruht die Adhäsiv-
Zementierung mehr auf die Verbindung der Harz-Marker mit dem Dentins als auf
gute Passform und mechanische Verankerung des Stiftes im Kanal (Ferrari et al.
2002). Weiterhin wird durch eine erweiterte Größenauswahl der Stifte mehr
Zahnsubstanz bewahrt, die für eine zufrieden stellende Stiftanpassung abgetragen
152

werden muss. Der Stift wird sich eher lösen, wenn der gewünschte „ferrule-effect“
nicht vorhanden ist, oder wenn eine zu dicke Zementschicht mit Blasenbildung
vorliegt (Ferrari et al. 2000a). Die Idee, individuell geformte, dem Kanal angepasste
Stifte, herzustellen, besonders bei elliptisch geformten Wurzelkanälen, die in
Eckzähnen und unteren Prämolaren vorkommen, ist interessant. In diesen Fällen
muss der Zahnarzt die Wurzelstruktur durch Entfernung von noch mehr Dentin an
die Stiftform anpassen. Jedoch wäre es wünschenswert, dass sich der Stift an die
Anatomie des Wurzelkanals nach erfolgter endodontischer Behandlung anpasst. Das
interessant, die Leistungen der
ist die Grundlage für die Entwickluung eines anatomischen Stiftes (Grandini et al.
2000, Boudrias et al. 2001a und 2001b). Kürzlich wurde der Anatomic Post’n Core
eingeführt (RTD, St. Egrève, Frankreich), (Ferrari et al. 2002). Dieser neue Stift
wird aus einem DT Post Nr.1 mit lichthärtendem Harz (Lumoglass, RTD, St.
Egrève, Frankreich) hergestellt. Dieser (relining) Harzbelag stellt, nach Einführung
in den Wurzelkanal, eine gute Passform her, und erlaubt es, die Zementmenge zu
reduzieren, die zum Stabilisieren des Stiftes während des Verbunds nötig ist.
Der endgültige Test eines Verfahrens besteht immer aus seiner klinischen
Beurteilung. Viele Studien berichten über die Anwendung von Faserstiften für die
Restauration von endodontisch behandelten Zähnen (Malferrari et al. 2003, Ferrari
et al. 2000a und 2000b, Fredriksson et al. 1998, Monticelli et al. 2003, Dallari et al.
1998, Scotti et al. 2002). Die meisten Studien verbinden die Anwendung von
Faserstift-Restaurationen mit Kronen aus Keramik- oder Keramo-Metall. Während
der letzten Jahre haben Direkt-Restaurationen mit Harz-Kompositen zugenommen
(Hickel et al. 2004). Aus diesem Grund ist es
Faserstifte im Zusammenhang mit Direkt-Restaurationen aus Harz-Kompositen
ohne Kronenabeckung zu untersuchen. Nach 30 Monaten klinischen Einsatz
wurzelbehandelter Zähne gab es keine Wurzelfrakturen. (und zeigten positive
Ergebnisse.)
Fazit und Empfehlungen
Aufgrund unserer grundlegenden und klinischen Untersuchungen über die
Anwendung von Faserstiften in der Zahnheilkunde können wir folgende
Schlussbetrachtungen und Empfehlungen geben:
153

1) Im Vergleich zu Metallstiften zeigen Faserstifte allgemein positive mechanische
Eigenschaften und besseres Fehlerverhalten.
2) Vorangegangene endodontische Behandlungen können das Endresultat einer
Stiftrestauration beeinflussen. Vor Abschluss der Füllung muss der Entfernung von
Bakterien, Debris und anderen Materialien aus dem Wurzelkanal größte Beachtung
beigemessen werden.
3) Die Adhäsivtechnik mit Faserstiften verhilft zur kompletten Füllung und
Abdichtung des Wurzelkanals. Aus diesem Grund kann sie durchaus als Teil der
endodontischen Behandlung angesehen werden.
4) Es gibt mehrere Faserstiftmarken. Die Verbundqualität zwischen Faser und Harz
kann die endgültige Qualität des Stiftes beeinflussen. Dies sollte, ebenso wie die
Zusammensetzung, die gewünschte Form, und die grundlegenden Überlegungen bei
der Wahl des Faserstiftes beachtet werden.
5) Ein zuverlässiger Verbund zwischen Faserstift-Harz-Zement und dem
Wurzelkanal kann relativ leicht mit einem Ätzmittel erreicht werden, wenn dieses
nen verwendet werden können. Durch diese Technik wird die
estauration von endodontisch behandelten Zähnen leichter und kostengünstiger.
mit Hilfe einer Spritze und einem Wurzelkanalinstrument gründlich aus dem
Wurzelkanal entfernt wird.
6) Für transluzente Stifte wird empfohlen, den Kanal mit einem Adhäsiv-System der
4. oder 5. Generation, zusammen mit einem dual-härtenden Harz-Zement und mit
Hilfe einer Microbrush zu beschicken.
7) Ein individueller Stift (Anatomic Post’n Core) kann sehr hilfreich sein, wenn ein
großer Verlust koronaler Struktur vorliegt, und wenn der Wurzelkanal nach
endodontischer Behandlung eine nicht-runde Form aufweist.
8) Faserstifte können zusammen mit Keramik oder Keramo-Metall-Kronen
eingesetzt werden. Ihre Verbreitung nimmt schnell zu, und neue klinische Studien
zeigen, dass sie ohne Risiko als Grundlage für Direkt-Restaurationen mit Harz-
Komposit-Kro
R
154
Resumen y conclusiones
Siempre ha sido un desafío grande para los clínicos el restaurar dientes
endodonticamente tratados. Los postes de fibra han adquierido una importancia en
este campo en los últimos 15 años. Esta tesis contiene un estudio acerca de varios
aspectos diferentes, básicos y clínicos relacionando la selección y el uso de postes de
físicos, químicos morfologicos y
eros factores que pueden reducir la
ri et al. 2004). Además, los cambios ocurren también en
lpa y las aristas marginales, influyendo en la
, son responsables de
un
poste se introducia para asegurar la retención a la recostrución y para “reforzar” el
diente. Hoy en día el refuerzo determinado por postes de metal no se puede
considerar posible (Shillimburg HT 1997) porque “…no refuerza apreciablemente
dientes tratados endodonticamente…” (Sorensen 1984a). El progreso hecho en la
fibra. Existe la evidencia cientifica de que la actuacion de un diente sano es diferente
a la de un diente endodonticamente tratado. Muchos cambios pueden ocurrir después
del tratamiento del canal de la raíz en términos
bioquímico y de las propiedades elásticas de la dentina, la resistencia para la fatiga,.
Un diente vital presenta una estructura (esmalte) más rigida y un apoyo
fundamentalmente más blando (dentina). La caries y la preparación del diente para
el tratamiento endodóntico son los prim
resistencia de un diente. Hay una disminución en el contenido de la humedad (Helfer
et al. 1972), un incremento del modulo de Young (Huang et al. 1992), y una
reducción en el porcentaje de fibras de colágeno en la dentina (Mason 2001,
Hashimoto et al. 2000, Ferra
la morfología y en la conducta biomecanica de dientes bajo el estrés (Grimaldi 1971,
Tidmarsh 1976). La preparación del acceso para el tratamiento endodóntico causa la
pérdida del techo de la cámara de la pu
incidencia relativamente alta de fracturas documentadas en premolares maxilares
(Ross et al. 1980, Salis et al. 1987). En general, la eliminación del techo de la
cámara de la pulpa, juntos con procedimientos endodónticos
una reducción en la resistencia a la fractura (Fuzzi 1993, Morgano et al. 1993,
Trabert et al. 1978, Milot et al. 1992).
También es sabido que la probabilidad de sobrevivencia de un diente sin pulpa es
relacionada directamente con la cantidad y la calidad de la estructura restante del
diente (Assif et al. 1994, Guttman 1992, Cohen et al. 1996). Tradicionalmente,
155

tecnología de materiales de fibra-reforzada ha mejorado la estructura, la forma, y las
ropiedades ópticas de postes de fibra-reforzados de resina. Esto llevó al desarrollo
ara expertos (Freedman et al. 1994, Godder et
p
de materiales que vencen algunas de las limitaciones de postes metálicos (platino,
aleaciones o titanio), con respecto a la apariencia estética, el modo del fracaso y el
desempeño clínico. En términos de la estética, los postes translúcidos de fibra se
introdujeron para sostener comercialmente las restauraciones anteriores (Vichi et al.
2000a y 2000b, Ferrari et al. 2001a y 2001b, Ferrari et al. 2002, Paul et al. 1998,
Heydecke et al. 2002). Por lo que concierne a el comportamiento bio-mecánicos y el
fracaso, se ha demostrado que los postes metálicos tienden a producir fracturas
irrevocables de la raíz. Opuestamente, una fractura de la raíz que ocurre con el uso
de postes de fibra se localiza generalmente más coronalmente y es más fácilmente
retratable (Akkayan et al. 2002, Cornier et al. 2001, Reagan et al. 1999, Newman et
al. 2003). Este tipo de fracaso puede estar debido a la mayor cantidad de estructura
del diente que se debe quitar cuando se coloca un poste metálico (Stankiewitz et al.
2002). En el caso en que sea necesario un re-tratamiento endodóntico, los postes de
fibra son más fácilmente removibles de los metálico o los cerámicos (Gesi et al.
2003, Hauman et al. 2003). En conclusion, los postes de fibra funcionan bien como
retenciones para los cementos de resinas compuestas en dientes tratados
endodonticamente. Cuando se compararon con postes de metal o circonios, ellos son
capaces de preservar la estructura residual del diente gracias a su conducta mecánica
y a los procedimientos de cementación que los acompañan.
Se han descrito técnicas para restaurar dientes endodonticamente tratados con el uso
de resinas compuestas para remplazar la dentina perdida de la raiz, con la
posibilidad del refuerzo de esta. Desgraciadamente, estos informes se publicaron en
publicaciones que no estan revisadas p
al. 1994, Martelli 2000, Castellucci 2004). Recientemente se realizó un estudio
comparando la resistencia de fractura y las pautas de fracaso de premolares
maxilares endodonticamente tratados con un número progresivamente reducido de
paredes residuales, estos se restauraron utilizando un material de resinas compuestas
con o sin postes traslúcidos de fibra de vidrio (Sorrentino et al. 2004). Este estudio
mostró que el número de paredes dentales residuales influyó en la resistencia
mecánica de los premolares maxilares endodonticamente tratados. En especímenes
156
con el mismo número de paredes dentales residuales, las cargas más altas de fractura
se registraron en dientes restaurados con postes de fibra. Además, en los
especímenes restaurados con postes de fibra se observaron fracturas sencillamente
restaurables. Si estos datos se pueden validar con estudios clínicos, el concepto de
reforzar las estructuras radiculares con el cementado de postes de fibra se
establecerá más firmemente.
Un exitoso procedimiento endodóntico es un factor clave de asegurar el éxito en la
restauración de dientes con las raices tratadas. Un tratamiento endodóntico bien
realizado se basa en la eliminación de detritus y material orgánico que hay dentro
del canal de la raíz (Castellucci 1993) y en la preparación mecánica del canal para
recibir un material de obturación (Ingle 1993). La influencia de cementos y de las
soluciones irrigadoras se han discutido extensamente en la literatura. Cuando se
evaluó el efecto de diferentes regímenes de irrigación en la limpieza de los canales
de la raíz que se lograron después del tratamiento endodóntico (Grandini et al.
2002b), se encontró que ninguna de las técnicas utilizadas en ese estudio mostró una
eliminación perfecta de la capa de barrillo dentinario y de los detritus. Sin embargo,
se notó que una combinación de hipoclorito sódico y un agente quelante puede
ayudar a reducir la cantidad de detritus por las paredes del canal. Las funciones de
relleno del canal de la raíz deberán sellar esencialmente el canal y prevenir futuras
microfiltraciones. En este sentido, la fabricación del poste y su colocación se pueden
considerar como partes del tratamiento endodóntico si ellos contribuyen al relleno y
al sellado del espacio de canal (Trope 2004). Desgraciadamente, debido a los
factores-C altos que hay en los canales radiculares (Morris et al., 2002; Bouillaguet
et al., 2003; Goracci et al., 2004), se encontraron dificultades en la cementacion de
postes de fibra a la dentina intraradicular con cementos de resina. Se ha sugerido que
semejante al uso de cementos no-adhesivos, la fricción de deslizamiento contribuje
por una parte substancial a la resistencia a la dislocación de postes cementados en
los canales radiculares (Goracci et al., 2005).
La popularidad siempre mas grande que tiene el uso de postes de fibra para la
restauración de los dientes endodonticamente tratados ha impuesto la necesidad de
una evaluación sistemática de las marcas y tipos diferentes de postes de fibra
disponibles comercialmente. Algunos criterios se emplean generalmente, tal como la
157
composición y la forma del poste, el costo y los procedimientos de cementacion,
basado en evaluaciones básicas y experimentales. Un estudio ha comparado la
resistencia a la fatiga y las características estructurales de tipos diferentes de postes
de fibra (Grandini et al. 2004a). Algunas marcas de postes de fibra pueden resistir
hasta 2.000.000 de ciclos de fatiga sin afectar su calidad general. En particular la
calidad de la adhesión entre los dos componentes de un poste de fibra (las fibras y la
rocedimientos de corte no afectarán a
matriz de resina de epoxi) puede influir en la calidad del poste mismo. De hecho, las
propiedades de fatiga y los impactos estaticos son proporcionales a la fuerza de la
interfase relleno/resina en sistemas de composite reforzados con fibra (Zhao et al.
2000, Kessler et al. 2000, Keusch et al. 1999). Un reciente estudio confirmó que
aumentando la fuerza de adhesion entre el relleno y la matriz se obtiene como
resultado un aumento de las propiedades mecánicas de composites reforzados con
fibras (Debnath et al. 2004).
Los procedimientos de cementado son muy importantes en las restauraciones con
postes de fibra. El procedimiento recomendado ya se ha descrito en la literatura
(Ferrari et al. 2001a y 2001b, Vichi et al. 2002a). El grabado ácido, el uso de un
adhesivo de cuarta o quinta generación, y el uso de un cemento de resina de doble-
curado proporciona los mejores resultados clínicos. Dejando la solución adhesiva
no-polimerizada antes de colocar el cemento (one step procedure), para reducir el
tiempo del procedimiento de cementación, se producen resultados desfavorables
desde el punto de vista clínico y experimental (Grandini et al. 2004b). Si se coloca
una corona, el poste se puede cortar después de la restauración del “core” (muñon).
En caso de que se haga una restauración conservadora es preferible ajustar la
longitud del poste antes del cementado. El ajuste se debe realizar con un disco de
carborundum o una fresa de diamante (Grandini et al. 2002a).De esta manera, es
posible cubrir el fin del corte del poste con composite de resina, un material más
capaz de resistir que un poste de fibra a el desgasto diente-diente y diente-alimento.
Si un poste es lo suficientemente bueno, los p
su integridad estructural.
Un gran desarrollo ocurrió con respecto a los materiales utilizados para la
fabricación de postes: el carbono era la primera materia empleada; vidrio, cuarzo y
sílice se han utilizado despues, aprovechándose de sus propiedades ópticas
158
traslúcidas. Un desarrollo interesante fue también la modificación del diseño de
estos postes, desde el doble-cilíndro original, a las formas “endodontica”, y por fin a
las formas más recientemente introducidas de la doble-conicidad. De echo la
cementación adhesiva ahora confía más en la formación de la zona de interdifusión
de resina-dentina y tags de resina que en la retención mecánica del poste dentro del
canal (Ferrari et al. 2002). Además, un amplio surtido de tamaños permite la
conservación de la dentina residual que se tiene que quitar para lograr una
adaptación satisfactoria del poste. El despegamiento es más probable que ocurra en
ausencia del deseable ‘ferrule effect’, o a la presencia de una capa excesivamente
gruesa de cemento en donde la incitación de burbujas conduce al despegamiento
(Ferrari et al. 2000a). La idea de tener un poste anatomico que quede bien en el
espacio individual del canal, especialmente con canales de raíz tratados que tienen
las formas elípticas, tal como fueron observados en caninos y premolares, seria una
onticelli et al. 2003, Dallari et al. 1998, Scotti et al. 2002).
situacion muy agradable por el clinico. En estos casos, el clínico es forzado a
adaptar la estructura dental residua a la forma del poste, mediante la eliminación de
una cantidad adicional de dentina o mediante una major cantidad y grosor de la capa
de cemento. Al contrario, sería deseable que el poste se adaptese a la anatomía del
canal de la raíz producida por el tratamiento endodóntico. Esto es verdaderamente
la base para la creación de un poste anatómico (Grandini et al 2000, Boudrias et al.
2001a y 2001b). Recientemente el Poste anatómico cementado (RTD, San Egrève,
Francia) ha sido introducido (Ferrari et al. 2002). Este nuevo poste es hecho por un
poste de DT n.1 que es cubierto por una resina de fotocurado (Lumiglass, RTD, San
Egrève, Francia). La resina es capaz, una vez que es introducido en el canal de la
raíz, de producir un adecuada forma, reduciendo la cantidad de cemento que debe
ser utilizada y estabilizando el poste durante los procedimientos de cementado.
La prueba final para un procedimiento clínico es siempre la evaluación clínica.
Muchos estudios informaron sobre el uso del poste de fibra para restaurar dientes
endodónticamente tratados (Malferrari et al. 2003, Ferrari et al. 2000a y 2000b,
Fredriksson et al. 1998, M
La mayoría de ellos combinan el uso de restauraciones de poste de fibra con
cerámico o coronas de ceramometal. En los ultimos años se ha podido observar una
enorme expansión en las indicaciones para las restauraciones directas con resina
159
(Hickel et al. 2004). Así, es interesante evaluar la actuación de postes de fibra
cuando ellos fueron utilizados en conjunción con restauraciones directas de resina,
sin el cubrimiento adicional de corona. Después de 30 meses de servicio clínico,
dientes con raices tratadas con postes de fibra y restauraciones de composite de
resina directa exhibieron unos resultados clínicos favorables y no ocurriron fracturas
de raíces.
Conclusiones y recomendaciones
Las conclusiones y recomendaciones siguientes se pueden deducir de nuestras
evaluaciones básicas y clínicas en el uso de postes de fibra en odontología:
1) Los postes de fibra exhiben unas propiedades mecánicas generales buenas y los
tipos de fracaso son generalmente más conservadores y favorables que cuando son
comparado con postes metálicos.
2) Los procedimientos endodónticos pueden influir en el resultado final de la
restauración con el poste. Se debe prestar gran atención en la eliminación de
bacterias, detritus y otros materiales que queden dentro del canal de la raíz antes que
el relleno sea completado.
3) Los postes de fibra contribuyen al relleno que sella el espacio de canal de la raíz
con la ayuda de la cementación adhesiva. Es por esta razón que ellos se pueden
considerar como parte del tratamiento endodóntico.
4) Existen varias marcas de postes de fibra. La calidad de la adhesión entre las fibras
y la resina puede influir en la calidad final del poste entero, y esto debe ser tenido en
cuenta al escoger un poste de fibra junto con la evaluación de la composición, la
forma deseada, la evaluación básica y clínica.
5) Por lo que conciernan a los procedimientos de cementado, una adhesión segura
entre la unitad cemento-poste de fibra y el canal de la raíz puede ser razonablemente
conseguido con el uso del grabado ácido, que ha sido meticulosamente removido del
canal de la raíz con una jeringa y un aguja endodóntica.
6) Un adhesivo de cuarta o quinta generación, metido en el canal con la ayuda de un
micropincel, y de un cemento de resina de doble-curado puede ser recomendado
cuando se utilizan postes de fibra traslúcidas.
160

7) Un poste individual (Anatomic Post’n Core) puede ser de gran ayuda en una
situación clínica donde hay una falta de estructura coronal y canales de raíz en una
forma no-redondeado despues el tratamiento endodontico.
8) Los postes de fibra se pueden utilizar con seguridad en combinación con cerámica
o coronas de ceramo-metal. Las indicaciones para su uso han sido rapidamente
extendidas, y los estudios clínicos recientes indicaron que ellos pueden ser utilizados
guramente como una base para las restauracion directa de resina. Con el uso de
e tratado endodónticamente puede ser más fácil
se
esta técnica, la restauración del dient
y meno costosa.
161
Sumário e conclusões
A restauração de dentes tratados endodonticamente permanence ainda como um
dente endodonticamente tratado. Diversas alterações podem
correr apόs o tratamento do complexo radicular no que concerne as propriedades
físicas, químicas e elásticas da dentina, além de alterações quanto a resistência a
fadiga, morfologia e comportamento biomecânico. Um dente vital, por sua vez,
apresenta uma estrutura mais rígida (esmalte) e um suporte com relativa
complascência abaixo (dentina). A presença de cáries e o preparo mecânico para o
tratamento endodôntico são os fatores iniciais que levam a uma queda da resistência
dental. Observa-se um decréscimo na umidade intrínseca da estrutura dental (Helfer
et al. 1972), um aumento do mόdulo de Young (Huang et al. 1992), e uma redução
na porcentagem de fibrilas colágenas na dentina (Mason 2001, Hashimoto et al.
2000, Ferrari et al. 2004). Além disso, alterações ocorrem também na morfologia e
no comportamento mecânico da estrutura dental mediante esforços (Grimaldi 1971,
Tidmarsh 1976). O acesso para o preparo endodôntico leva a perda de tanto o teto da
câmara pulpar quanto das cristas marginais, influenciando a incidência de fraturas
documentadas em pré-molares superiores (Ross et al. 1980, Salis et al. 1987). De
uma forma geral, a remoção do teto da câmara pulpar, aliado a terapia endodôntica,
são grandes responsáveis pela redução da resistência a fratura dental (Fuzzi 1993,
Morgano et al. 1993, Trabert et al. 1978, Milot et al. 1992).
Sabe-se também que a taxa de “sobrevivência” de um dente despolpado está
diretamente relacionado com a quantidade e a qualidade da estrutura dental
remanescente (Assif et al. 1994, Guttman 1992, Cohen et al. 1996).
Tradicionalmente, um pino era indicado para aumentar a retenção do material de
preenchimento, bem como “reforçar” o remanescente dental. Atualmente, o eventual
“reforço” promovido por pinos metálicos não é mais considerado possível
grande desafio para a grande maioria dos clínicos. Dentro deste campo da
Odontologia, os pinos de fibra de vidro ganharam muita importância nos últimos 15
anos. Esta tese contêm um estudo sobre diferentes aspectos básicos e clínicos
relacionados com a seleção e a utilização destes tipos de pinos.
Há evidências clínicas que mostram que um dente hígido apresenta características
diferentes de um
o
162

(Shillimburg HT 1997), uma vez que estes “…não reforçam significativamente os
entes tratados endodonticamente …” (Sorensen 1984a). O progresso tecnolόgico
estética, os pinos de
d
no campo de materiais reforçados por fibras melhoraram a estrutura, a forma, e as
propriedades όpticas dos pinos reforçados por fibra contemporâneos. Tal progresso
levou ao desenvolvimento de materiais que puderam se sobrepor às limitações dos
pinos metálicos (platina, ligas ou de titânio), no que diz respeito a sua aparência
estética, modo de fratura e performance clínica. Em termos de
fibra translúcidos foram introduzidos no mercado buscando dar maior suporte às
restaurações de dentes anteriores (Vichi et al. 2000a e 2000b, Ferrari et al. 2001a e
2001b, Ferrari et al. 2002, Paul et al. 1998, Heydecke et al. 2002). O conhecimento
do comportamento mecânico e o mecanismo de falha dos pinos de fibra é de suma
importância, e é demonstrado que os pinos metálicos, quando submetidos a testes de
fadiga, tendem a produzir fraturas radiculares irreversíveis. Adicionalmente, as
fraturas radiculares que ocorrem quando da utilização de pinos de fibra se localizam
em uma porção mais coronária da raiz, além de serem mais facilmente retratadas e
reparadas (Akkayan et al. 2002, Cornier et al. 2001, Reagan et al. 1999, Newman et
al. 2003). Tal tipo de fratura pode se dar em função da grande quantidade de
estrutura dental que deve ser removida quando da inserção de um pino metálico
(Stankiewitz et al. 2002). Em casos em que se faz necessário um retratamento
endodôntico, pinos de fibra são mais facilmente removidos, quando comparado com
pinos metálicos ou cerâmicos (Gesi et al. 2003, Hauman et al. 2003). Como
conclusão, pinos de fibra funcionam de maneira efetiva como “ancoragem” para
núcleos de resina composta. Quando comparados com pinos metálicos ou de
zircônia, pinos de fibra mostram-se capazes de preservar a estrutura dental
remanescente em função de seu comportamento mecânico, bem como em função de
seu método de cimentação adesivo.
Ultimamente, técnicas restauradoras com resinas compostas em dentes tratados
endodonticamente têm sido descritas, buscando repor a dentina perdida, e
possivelmente reforçar a estrutura radicular. Infelizmente, tais artigos foram
publicados em publicações que não são acuradamente revisadas (Freedman et al.
1994, Godder et al. 1994, Martelli 2000, Castellucci 2004). Um recente estudo
buscou comparar a resistência e o padrão de fratura de pré-molares superiores
163

tratados endodonticamente, com diferentes quantidades de paredes remanescentes,
que foram restaurados com compósitos; associados ou não a utilização de pinos de
fibra de vidro translúcidos (Sorrentino et al. 2004). Este estudo mostrou que o
número de paredes dentais remanescentes influenciou significativamente a
resistência mecânica de tais dentes tratados endodonticamente. Em dentes com o
mesmo número de paredes remanescentes, observou-se uma maior resistência a
fratura quando da utilização dos pinos de fibra de vidro. Adicionalmente, fraturas
com prognóstico mais favoráveis foram observadas nos dentes restaurados com
pinos de fibra. Se tais observações puderem ser validadas em estudos clínicos, o
conceito de reforço das estruturas radiculares através da adesão de pinos de fibra
estará definitivamente muito melhor embasada.
Um tratamento endodôntico bem realizado é um fator chave para se obter sucesso
longitudinal na restauração de dentes tratados endodonticamente. Um tratamento
endodôntico bem realizado está baseado na remoção total de debris e materiais
orgânicos internamente à porção radicular (Castellucci, 1993) bem como no preparo
mecânico propriamente dito, para que seja possível o perfeito acomodamento do
material obturador (Ingle 1993). A influência de cimentos e soluções irrigantes têm
sido extensivamente discutidas na literatura. Quando da avaliação de diferentes
soluções irrigantes na efetividade da limpeza das paredes radiculares após o
tratamento endodôntico (Grandini et al. 2002b), pode-se observar que nenhuma das
técnicas avaliadas em tal estudo mostrou uma remoção perfeita da camada de
“smear layer” e de debris. No entanto, notou-se que a combinação de hipoclorito de
sódio e um agente quelante reduz a quantidade de debris ao longo das paredes
radiculares. As funções primordiais de um material obturador são essencialmente
selar o canal radicular e prevenir uma futura microinfiltração. Neste sentido, a
confecção e a colocação de pinos intraradiculares podem ser consideradas parte do
tratamento endodôntico, uma vez que contribuem para o preenchimento e o
selamento do espaço radicular (Trope 2004). Infelizmente, em função de um alto
fator C encontrado nesta região (Morris et al., 2002; Bouillaguet et al., 2003;
Goracci et al., 2004), dificuldades substanciais são comumente encontradas quando
da cimentação de pinos de fibra à dentina intraradicular com o auxilio de cimentos
resinosos. Postula-se que similarmente aos cimentos não-adesivos, uma parte
164
substancial da resistência ao deslocamento de pinos de fibra aderidos às paredes
radiculares está ligada a forças friccionais (Goracci et al., 2005).
A popularização do uso de pinos de fibra para a restauração de dentes tratados
endodonticamente impuseram uma necessidade de avaliação sistemática dos mais
diferentes tipos de pinos disponíveis no mercado. Alguns critérios são usualmente
empregados, tais como a composição e o formato do pino, o custo e os
procedimentos de cimentação, sempre baseados em avaliações básicas e
experimentais. Um estudo comparando a resistência a fadiga e as características
estruturais dos mais diferentes tipos de pinos de fibra foi desenvolvido (Grandini et
al. 2004a). Algumas variedades de pinos de fibra podem resistir a mais de 2.000.000
ciclos de fadiga in vitro, sem que haja efeitos em sua integridade. Particularmente, a
qualidade adesiva entre os dois componentes inerentes a um pino de fibra (as fibras
e a matriz de resina epóxica) pode influenciar a qualidade do pino propriamente dita.
Como via de regra, as propriedades de impacto estático e de fadiga são
proporcionais a resistência da interface carga/resina nos sistemas de compósito
reforçado por fibras (Zhao et al. 2000, Kessler et al. 2000, Keusch et al. 1999). Um
recente estudo confirmou que aumentando a força de união entre as partículas de
carga e a matriz, obtêm-se melhoras significativas nas propriedades mecânicas dos
compósitos reforçados por fibras (Debnath et al. 2004).
Em se tratando de pinos de fibra, os procedimentos de cimentação apresentam
extrema importância. Os procedimentos recomendados encontram-se amplamente
descritos na literatura (Ferrari et al. 2001a e 2001b, Vichi et al. 2002a). As etapas de
condicionamento ácido, a utilização de um sistema adesivo de quarta ou quinta
geração, aliado a um cimento resinoso de polimerização dual, possibilitam os
melhores resultados clínicos. A tentativa de deixar o sistema adesivo sem ser
polimerizado antes da colocação do cimento (procedimento em passo único),
buscando reduzir o tempo clínico de cimentação, produz resultados desfavoráveis,
tanto do ponto de vista experimental quanto do ponto de vista clínico (Grandini et al.
2004b). Se uma coroa será posteriormente efetuada, o pino pode ser ajustado após a
confecção de um núcleo de preenchimento. Em casos de restaurações diretas, deve-
se ajustar o comprimento do pino anteriormente ao procedimento de cimentação. Tal
ajuste pode ser feito com um disco de carborundum ou com uma ponta diamantada
165

(Grandini et al. 2002a). Desta maneira, é possível recobrir a porção mais coronal do
pino com resina composta, um material que apresenta maior resistência ao desgaste
iva (Ferrari et al. 2000a). A
que os pinos de fibra de vidro. Partindo do principio que se está trabalhando em um
pino de boa qualidade, os procedimentos de corte não virão a afetar a sua integridade
estrutural.
Muitos avanços nos materiais utilizados para a fabricação de pinos foram obtidos
nos últimos tempos: o carbono foi o primeiro material utilizado; vidro, quartzo e
sílica foram em seguida aplicados, buscando tirar vantagem de suas propriedades
ópticas translucentes. Alterações interessantes foram também empreendidas no
“design” de tais pinos, o originalmente duplo cilíndro, com formato endodôntico,
para os mais recentes de “double-tapered”, ja que a cimentação adesiva esta
principalmente baseada na formaçao da zona de interdifusão resina-dentina e na
formação de “tags” de resina, em detrimento de uma maior adaptação e de retenção
mecânica do pino dentro do canal radicular (Ferrari et al. 2002). Além disso, a
variedade de tamanhos permite uma maior conservação da dentina radicular que
provavelmente teria que ser removida para buscar uma melhor adaptação do pino. A
quebra da adesão (debonding) esta mais propensa a acontecer na ausência de um
efeito férula, ou na presença de uma camada de cimento muito espessa, onde uma
maior quantidade bolhas incorporadas levam a falha ades
idéia de se ter um pino individualizado que se encaixa justamente no canal radicular
é extremamente interessante, especialmente quando lida-se com canais radiculares
que apresentam formato elíptico, comumente observados em caninos e pré-molares
inferiores. Nestes casos, o clínico é forçado a adaptar a estrutura radicular residual
ao formato do pino, através da remoção de uma determinada quantidade de dentina.
Contrariamente, o ideal seria que o pino se adaptasse à anatomia do canal radicular
produzida após o tratamento endodôntico. Sem dúvida, tal problemática levou ao
desenvolvimento de pinos anatômicos (Boudrias et al. 2001a e 2001b).
Recentemente, o sistema Anatomic Post’n Core (RTD, St Egrève, France) foi
introduzido no mercado (Ferrari et al. 2002). Este novo pino é feito por um DT n. 1
que em seguida é coberto por uma resina fotopolimerizável (Lumiglass, RTD, St
Egrève, France). Tal resina de reembasamento, uma vez introduzida no canal
radicular, permite uma boa adaptação às paredes radiculares, além de reduzir a
166
quantidade de cimento a ser utilizada e estabilizando melhor o pino durante os
procedimentos de cimentação.
O teste final para um procedimento clínico cai sempre em uma minuciosa avaliação
clínica. Muitos estudos relatam o uso de pinos de fibra de vidro para restaurar dentes
tratados endodonticamente (Malferrari et al. 2003, Ferrari et al. 2000a e 2000b,
Fredriksson et al. 1998, Monticelli et al. 2003, Dallari et al. 1998, Scotti et al. 2002).
A grande maioria deles associa o uso de pinos de fibra com a colocação de coroas
metaloceramicas ou em cerâmica pura. Nos últimos anos pode-se observar uma
enorme expansão na indicação de restaurações diretas em resina composta (Hickel et
al. 2004). Adicionalmente, é de grande relevância avaliar a performance de pinos de
fibra quando utilizados em conjunto com restaurações diretas em compósito, sem
cobertura adicional de próteses unitárias. Após 30 meses de avaliação clínica, dentes
tratados endodonticamente, que foram restaurados diretamente com pinos de fibra
de vidro e resina composta não exibiram fraturas radiculares, com resultados
clínicos bastante favoráveis.
Conclusões e recomendações
As seguintes conclusões e recomendações podem ser extraidas a partir de nossas
avaliações clínicas e laboratoriais, quanto a utilização de pinos de fibra em
Odontologia:
1) Pinos de fibra apresentam ótimas propriedades mecânicas, com padrões de fratura
mais conservadores e favoráveis, quando comparados com pinos metálicos.
2) Os procedimentos endodônticos podem influenciar o resultado final da
restauração com pinos. Extremo cuidado deve ser tomado quanto à remoção de
bactérias, debris e outros materiais dentro do canal radicular previamente ao
fechamento completo da estrutura.
3) Pinos de fibra contribuem para o selamento do espaço radicular adjuntamente
com a cimentação adesiva. Por tal razão, tal etapa operatória pode ser considerada
como parte do tratamento endodôntico.
4) Existem diversos tipos de pinos de fibra. A qualidade da adesão entre as fibras e a
resina influenciam a qualidade final de todo o pino, e tal fato deve ser levado em
167

conta quando da seleção de um pino de fibra, juntamente com a composição e o
formato, além das avaliações básicas e experimentais.
ica pura. Suas indicações estão se expandindo
pidamente, e estudos clínicos recentes indicam que podem ser utilizados como
s em resina composta. Através do uso desta técnica,
5) No que concerne aos procedimentos de cimentação, a obtenção de uma adesão
confiável entre o pino de fibra de vidro e o cimento resinoso pode ser conseguida
através da técnica do condicionamento ácido, que deve ser enxaguado com água do
canal radicular meticulosamente, com auxílio de uma agulha endodôntica.
6) Um sistema adesivo de quarta ou quinta geração, aplicado ao canal com auxílio
de um “microbrush”, e um cimento resinoso de polimerização dual são
recomendados quando da utilização de um pino de fibra translúcido.
7) Um pino indvidualizado (Anatomic Post’n Core) pode ser de grande valia em
situações clínicas de grande perda de estrutura coronária, bem como após
tratamentos endodônticos onde nao é possível obter os canais com formato
cilíndrico.
8) Pinos de fibra podem ser seguramente utilizados em conjunto com coroas
metalocerâmicas ou em cerâm
ra
alicerce para restaurações direta
a restauração de dentes tratados endodonticamente pode ser facilitada, e muito
menos custosa.
168
Complete list of references
Abou-Rass M. Post and core restoration of endodontically treated teeth. Curr Opin
rations of EDTA
mussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of
356.
Barbakov F, Peters O, Havranek L. Effects of Nd:YAG lasers on root canal walls: a
light and scanning electron microscopic study. Quint Int 1998: 837-45.
Behrend GD, Cutler CW, Gutmann JL. An in-vitro study of smear layer removal
and microbial leakage along root canal fillings. Int End J 1996; 29(2): 99-107.
Bergman B, Lunquist P, Sjögren U, Sundqvist G. Restorative and endodontic results
after treatment with cast posts and cores J Prosthet Dent 1989;61: 10-15.
Bertrand M-F, Lupi-Pegurier L, Medioni M, Muller M, Bolla M. Curved molar root
canal preparations using Hero 642 rotary nickel-titanium instruments. International
Endododontic Journal 2001;34, 631-36.
Boschian L, Galimberti B, Fadini L et al.. A new method to evaluate the conversion
of a composite resin into the root canal: HPLC. J Dent Res 2001;80: (Abstr 1842) pag 757.
Boudrias P, Sakkal S, Petrova Y. Anatomical post design applied to quartz
fibre/epoxy technology: a conservative approach. Oral Health 2001a;11, 9-16.
Dent 1992;2: 99-107.
Angmar-Månsson B, Omnell K-Å, Rud J. Root fractures due to corrosion. I.
Metallurgical aspects. Odontol. Revy 1969;20: 244-65.
Akkayan B, Gulmez T. Resistance to fracture of endodontically treated teeth
restored with different post systems. J Prosthet Dent 2002; 87: 431-437.
Akpata ES, Blechman H. Bacterial invasion of pulpar dentin wall in vitro. J Dent
Res 1982; 61: 435-8.
Aktener BO, Bikay U. Smear layer removal with different concent
mixtures. J Endod 1993; 19: 228-31.
Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of
endodontically treated teeth. J Prosthet Dent 2002 Mar;87(3):256-63.
As
newer types of endodontics posts. J Dent 1999;27:275-278.
Assif D, Gorfil C. Biomechanical considerations in restoring endodontically treated
teeth. J Prosthet Dent 1994; 71:565-7.
Ausiello P, De Gee AJ, Rengo S, Davidson CL. Fracture resistance of
endodontically-treated premolars adhesively restored. Am J Dent 1997 Oct;10(5):237-41.
Baran G, Boberick K, McCool J. Fatigue of restorative materials. Crit Rev Oral Biol
Med 2001;12:350-
169
Boudrias P, Sakkal S, Petrova Y. Anatomical post design meets quartz fiber
chnolog
S, Troesch S, Wataha JC, Krejci I, Meyer JM and Pashley DH.
980;1, 38-40.
osphate and epoxylate CBA 9080. J Prosth Dent 1974; 31: 556-65.
York; 1997; 513-541.
dei denti compromessi.
spetti b
anastomosis: A potential factor
adhesiv
n Fraunhofer JA. Retention of prefabricated posts by
acture s
rials. J Prosthet Dent
resistance and
ilure m
an M. The morphology of the prepared root canal: a
udy util
ce
n Meerbeek B.
Bonding of an auto-adhesive luting material to enamel and dentin. Dent Mat 2004, in press.
te y: rationale and case report. Compendium 2001b;22:337-48.
Bouillaguet
Microtensile bond strength between adhesive cements and root canal dentin. Dent Mater
2003;19:99-205.
Bradley JS, Hastings GW, Johnson-Nurse C. Carbon fibre reinforced epoxy as a
high strength, low modulus material for internal fixation plates. Biomat 1
Brannstrom M, Nyborg H. Bacterial growth and pulpar changes under inlays
cemented with zinc ph
Callister WD Jr. Materials Science and engineering. An introduction. 3rd Edition.
Chapter 17. Composites. Wiley: New
Castellucci A. Endodontics, Ed Martina, Milano, 1993.
Castellucci A, Becciani R. Ricostruzione postendodontica
A iomeccanici. Dental Cadmos 2004,2:2-21.
Chappel RP, Cobb CM, Spencer P. Dentinal tubule
in e bonding? J Prosthet Dent 1994;72, 183-8.
Chapman KW, Worley IL, Vo
cements and resins. J Prosthet Dent 1985;54: 649-52.
Cohen BI, Pagnillo MK, Condos S, Deutsch AS. Four materials measured for
fr trength in combination with five designs of endodontic posts. J Prosthet Dent 1996;
76:487-95.
Cohen BI, Pagnillo MK, Newman I, Musikant BL, Deutsch AS. Cyclic fatigue
testing of five endodontic post designs supported by four core mate
1997;78:458-64.
Cornier CJ, Burns DR, Moon P. In vitro comparison of the fracture
fa ode of fiber, ceramic and conventional post systems at variuos stages of restorations.
J Prosthodont 2001; 10: 26-36.
Dallari A, Rovatti L. Six years of in vitro/in vivo experience with Composipost.
Compendium 1998;20:S57-S63.
Davis SR, Brayton SM, Goldm
st izing injectable silicone. Oral Surg 1972; 34: 642-8.
Debnath S, Ranade R, Wunder SL, McCool j, Boberick K, Baran G. Interfa
effects on mechanical properties of particle-reinforced composites. Dent Mat 2004;20:677-86.
De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P, Va
170
Derand P, Vereby P. Wear of low-fusing dental porcelains. J Prosthet Dent.
1999;81(4):460-3.
Desort KD. The prosthodontic use of endodontically treated teeth: theory and
biomechanics of post preparation. J Prosthet Dent 1983;49:203-6.
Dietschi D, Romelli M, Goretti A. Evaluation of post and cores in the laboratory:
tionale
TJ.
Morphology and permeability of
e dentin
France 540:131-41.
France 542: 69-77.
:45-57.
d P. The surgeon dentist or treatise on the teeth, vol.2. Translated from the nd editio
J Dent Res 1987;66, 1636-9.
Dent 2000a;13:9B-14B.
m J Dent 2000b;13:B9-B14
ra for developing a fatigue test and preliminary results. Compend Contin Educ Dent
Suppl 1996;20:S65-S73.
Dietschi D, Romelli M, Goretti A. Adaptation of adhesive posts and cores to dentin
after fatigue testing. Int J Prosthodont 1997;10:498-507.Drummond JL, Toepke RS, King
Thermal and cycling loading of endodontic posts. Eur J Oral Sci 1999;107:220-224.
Dippel H, Borggreven J, Hoppenbrouvers PMM.
th smear layer. J Prosthet Dent 1984; 52: 657-62.
Drummond JL, Toepke RS, King TJ. Thermal and cycling loading of endodontic
posts. Eur J Oral Sci 1999;107, 220-4.
Duret B, Reynaud M, Duret F (1990 a) Un noveau concept de reconstitution
coronoradiculaire: le Composipost 1°. Le Chir Dent de
Duret B, Reynaud M, Duret F (1990 b) Un noveau concept de reconstitution
coronoradiculaire: le Composipost 2°. Le Chir Dent de
Duret B, Reynaud M, Duret F (1992) Intérêt des materiaux á structure
unidirectionnelle dans les reconstitutions corono-radiculaires. Journal de Biomateriaux
Dentaires 7
Fan P, Nicholls JI, Kois JC. Load fatigue of five restoration modalities in
structurally compromised premolars. Int J Prosthodont 1995;8:213-220.
Fauchar
2 n 1746 by L. Londsay, London, Butterworth and company LtD 1946.
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in relation to
configuration of the restoration.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of clinical
performance of fiber posts. Am J
Ferrari M, Vichi A, García-Godoy F. A retrospective study of fiber-reinforced
epoxy resin posts vs. cast posts and cores: a four year recall. A
Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjör IA. Bonding to root canal:
Structural characteristics of the substrate. Am J Dent 2000c;13:380-386.
171
Ferrari M, Vichi A, Grandini S, Goracci C (2001a). Efficacy of a self-curing
adhesive/resin cement system on luting glass-fibre posts into root canals: an SEM
application technique on
ficacy o
Petschelt
. Fatigu
fiber-reinforced epoxy resin posts. J Prosthet Dent
Clin North Am
ar rehabilitation: a
nical a
d teeth. Int Endod J 1999;32: 283-86.
ntics 1996;22,
69-75.
canal irrigants. Oral Surg
ral Med
nd microscopic evaluation of post
d core r
for
arison of root canal
preparations NiTi hand, NiTi engine-driven and K-Flex endodontic instruments. Journal of
Endodontics 1995;21, 146-51.
investigation. Int J Prosthod 2001a;14, 543-9.
Ferrari M, Vichi A, Grandini S. Influence of adhesive
ef f bonding to root canal walls: An SEM investigation. Dent Mat 2001b;17, 422-9
Ferrari M, Scotti R. Fiber posts: clinical and research aspects. Masson Ed, Milano
2002.
Ferrari M, Mason PN, Goracci C, Pashley DH, Tay FR. Collagen degradation in
endodontically treated teeth after clinical function. J Dent Res. 2004 May;83(5):414-9.
Frankenberger R, Kramer N, Ebert J, Lohbauer U, Kappel S, ten Weges S,
A e behavior of the resin-resin bond of partially replaced resin-based composite
restoration. Am J Dent 2003; 16: 17-22.
Fredriksson M, Astback J, Pamenius M, et al.. A retrospective study on 236
patients with teeth restored by carbon
1998;80:151-157.
Freedman GA. Esthetic post and core treatment. Dent
2001;45:1:103-116.
Freedman G, Nowak IM, Serota KS, Glassman GD. Intraradicul
cli pproach. Pract Period Aesth Dent 1994;6:33-9.
Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted
endodontically treate
Fuzzi M. The restoration of the endodontically treated tooth. From the text
“Endodontics”, Castellucci A, Ed Martina, Milano, 1993.
Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless
steel hand file instrumentation using computed tomography. Journal of Endodo
3
Garberoglio R, Becce C. Smear layer removal by root
O Oral Pathol 1994; 78: 358-66.
Gateau P, Sabek M, Dailey B. Fatigue testing a
an estorations under artificial crowns. J Prosthet Dent 1999;82:341-7.
Gesi A, Magnolfi S, Goracci C, Ferrari M. Comparison of two techniques
removing fiber posts. J Endod. 2003;29(9):580-2.
Glosson CR, Haller RH, Brentdove S, del Rio CE. A comp
172
Godder B, Zhukowsky L, Bivona PL, Epelboym D. Rehabilitation of thin-walled
roots with light-activated composite resin: a case report. Compend Contin Edu Dent
1994;15:52-7.
Goldman M, Devitre R, Pier M. Effect of the dentin smeared layer on tensile
strength of cemented post. J Prosthet Dent 1984; 52: 485-8.
Goldman M, Goldman LB, Kronman JH, Lin PS. The efficacy of several irrigating
solutions for endodontics: a scanning electron microscopic study. Oral Surg 1981; 52: 197-
4.
hlorite
rigant c
er posts and root canal walls: comparison between
tion to the dislocation resistance of bonded fiber posts. J Endod 2005, in
ss.
Balleri P, Ferrari M. Scanning electron microscopic investigation of the
yde File Prep in combination with
dium h
Fatigue resistance and
l
Grandini S, Ferrari M. Una tecnica per rendere anatomici i perni in fibra. Il Dentista
a of rupture and flow in solids. Philosophical
own under axial
mpress
n of Uniaxial Fiber-Reinforced-Polymer
20
Goldsmith M, Gulabivala K, Knowles JC. The effect of sodium Hypoc
ir oncentration on tooth surface strain. J Endod 2002;vol 28, n.8:575-9.
Goracci C, Tavares AU, Fabianelli A, Monticelli A, Raffaelli O, Cardoso PEC, Tay
FR, Ferrari M. The adhesion between fib
microtensile and push-out bond strength measurements. Eur J Oral Sci 2004;112:353-61.
Goracci C, Fabianelli A, Sadek F, Papacchini F, Tay FR, Ferrari M. The
contribution of fric
pre
Grandini S,
surface of fiber posts after cutting. J Endod 2002a; 28:610-612.
Grandini S, Balleri P, Ferrari M. Evaluation of Gl
so ypochlorite as a root canal irrigant. J Endod 2002b;28(4):300-3.
Grandini S, Goracci C, Monticelli F, Tay FR, Ferrari M.
structura characteristics of fiber posts: three-point bending test and SEM evaluation. Dent
Mat 2004a, in press.
Grandini S, Sapio S, Goracci C, Monticelli F, Ferrari M. A one step procedure for
luting glass fibre posts: an SEM evaluation. Int Endod J. 2004 Oct;37(10):679-86.
Moderno. Anno XVIII, n° 5, May 2000.
Griffith AA. The phenomen
Transactions of the Royal Society of London (Series A) 1920; A221: 168-98.
Grimaldi J. Measurement of the lateral deformation of the tooth cr
co ive cuspal loading. 1971. Thesis University of Otago, Dunedin, New Zealand.
Gu W. Interfacial Adhesion Evaluatio
Composites by Vibration Damping of Cantilever Beam. PhD thesis at Virginia Polytechnic
Institute and State University. 1997; 11-3.
173

Gutman JL. The dentin-root complex: anatomic and biological considerations in
restoring endodontically treated teeth. J Prosthet Dent 1992; 67:458-67.
Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth
ith and
dontically treated posterior teeth
d posterior teeth restored with amalgam. Endod Dent Traumatol 1990;6: 49-55.
ital
d pulpl
dontically treated teeth restored with different post-and-core systems. J Prosthet Dent
2002; 87:
ilson NH. Direct composite
, Shilder H, Nathanson D. Effects of moisture content and endodontic
sthod 1996;9:131-6.
ents.
sites. Composites A 1999;30:997-1002.
w without endo-post reinforcement. J Prosthet Dent 1979;42: 39-44.
Hansen EK; Asmussen E. In vivo fractures of endo
restored with enamel bonded resin. Endod Dent Traumatol 1990;6: 218-25.
Hansen EK, Asmussen E, Christansen NC. In vivo fractures of endodontically
treate
Hashimoto M, Ohno H, Kaga M, et al.. In vivo degradation of resin-dentin bonds in
humans over 1 to 3 years. J Dent Res 2000 Jun;79(6):1385-91.
Hauman CH, Chandler NP, Purton DG. Factors influencing the removal of posts. Int
Endod J 2003;36(10):697-90.
Helfer AR, Melnick S, Schilder H. Determination of the moisture content of v
an ess teeth. Oral Surg Oral Med Oral Pathol 1972;34: 661-70.
Heydecke G, Butz F, Hussein A, Strub JR. Fracture strength after dynamic loading
of endo
438-445.
Hickel R, Heidemann D, Staehle HJ, Minnig P, W
restorations: extended use in anterior and posterior situations. Clin Oral Investig 2004; 8:43-
44.
Hsu YB, Nicholls JI, Phillips KM, Libman WJ. Effect of core bonding on fatigue
failure of compromised teeth. Int J Prosthodont 2002;15:175-8.
Huang T-JG
treatment on some mechanical properties of human dentin. J Endod 1992;18: 209-15.
Ingle JA. Endodonzia. Piccin Editore, 1993, Padova, Italy 29-40.
Isidor F, Odman P, Brondum K. Intermittent loading of teeth restored using
prefabricated carbon fiber posts. Int J Pro
Kahn FH, Rosenberg PA, Schulman A, Pines M. Comparison of fatigue for three
prefabricated threaded post systems. J Prosthet Dent 1996;75:148-53.
Kessler A, Bleddzky A. Correlation between interphase-relevant tests and the
impact-damage resistance of glass/epoxy laminates with different fibre surface treatm
Compos Sci Technol 2000;60:125-30.
Keush S, Haessler R. Influence of surface treatments of glass fibres on the dynamic
mechanical properties of epoxy resin compo
174
97;22: 15-20.
tertubular human
dentin. J
S.
Compara
A78, # 0425.
t 1987;57:277-81.
. Touch thresholds of vital and non vital human teeth. Exp Neurol
w. J Prosthet Dent 1993; 69:32-6.
ontal ligament
scles. Arch Oral Biol
igidity. Int J Prosthod 1996;9, 484-8.
Kielbassa AM, Attin T, Hellwigg E. Diffusion behaviour of eugenol from zinc
oxide eugenol mixtures through human and bovine dentin in vitro. Oper Dent 19
Kinney JH, Balooch M, Marshall SJ, Marshall GW, Weihs TP. Atomic force
microscope measurements of the hardness and elasticity of peritubular and in
Biomech Eng 1996;118: 133-5.
Kopper PM, Figueiredo JA, Della Bona A, Vanni JR, Bier CA, Bopp
tive in vivo analysis of the sealing ability of three endodontic sealers in post-
prepared root canals. Int Endod J 2003 Dec;36(12):857-63.
Kurtz JS, Bowles WR, Perdigao J, Geraldeli S, Hodges JS. Push-out bong strengths
of toothcoloured posts. J Dent Res 2002, 81 Special issue A, pag
Leary JM, Aquilino SA, Svare CW. An evaluation of post length within the elastic
limits of dentin. J Prosthet Den
LeGeros RZ.Calcium phosphates in oral biology and medicine. In Meyers HM(ed)
Monographs in Oral Sciences. New-York Karger 1991;15:109-11.
Lewinstein I, Grajower R. Root dentin hardness of endodontically treated teeth. J
Endod 1981;7: 421-2.
Linden RW
1975;48: 387-90.
Lloyd PM, Palik JF. The philosophies of dowel diameter preparation: a literature
revie
Lodvahl PE, Nicholls JI. Pin retained amalgam cores vs. cast gold dowel cores. J
Prosthet Dent 1977, 38:507-14.
Lopes HP, Siqueira GF, Elias CN. Scanning electron microscopic investigation of
the surface of Gutta-Percha cones after cutting. J Endod 2000; 26: 418-20.
Louca C, Cadden SW, Linden RW. The roles of period
mechanoreceptors in the reflex control of human jaw-closing muscles. Brain Res 1996;731:
63-71.
Louca C, Vidgeon SD, Cadden SW, Linden RW. The role of gingival
mechanoreceptors in the reflex control of human jaw-closing mu
1998;43: 55-63.
Love RM, Purton DG. The effect of serrations on carbon fibre posts retention within
the root canal, core retention, and post r
Lowenstein NR, Rathkamp R. A study on the pressoreceptive sensibility of the
tooth. J Dent Res 1955;34: 287-94.
175
Lui JL. Composite resin reinforcement of flared canals using light-transmitting
posts. Quint Int 1994;25, 313-9.
Madison S, Wilcox LR. An evaluation of coronal microleakage in endodontically
treated teeth. Part III. In vivo study. J Endod. 1988 Sep;14(9):455-8.
Madison S, Swanson K, Chiles SA.An evaluation of coronal microleakage in
1984; 10: 477-83.
656.
4.
oot canal posts. J Adhes
nocenti M, Ferrari M, Watson T. Confocal and scanning electron
9-794.
t 1997;25: 441-58.
sthet Dent 2000;12:579-84.
c posts. J Prosthet
entinal bonding agents under the influence of eugenol. Quintessence Int 1997;28: 57-
62.
ures. J Endod 1975; 1: 238-42.
t Dent 1992;68: 428-35.
endodontically treated teeth. Part II. Sealer types. J Endod. 1987 Mar;13(3):109-12.
Mader LL, Baumgarter JC, Peters DD. A scanning electron microscopic
investigation of the smear layer on root canal walls. J Endod
Malferrari S, Baldissara P, Arcidiacono A. Translucent quartz fiber posts: a 20
months in vivo study. IADR 80th General Session, S.Diego, 2002, abstract n° 2
Malferrari S, Monaco C, Scotti R. Clinical evaluation of teeth restored with quartz-
fiber-reinforced epoxy resin posts. Int J Prosthod 2003;16(1):39-4
Mannocci F, Ferrari M, Watson TF. Intermittent loading of teeth restored using
quartz fiber, carbon-quartz fiber, and zirconium dioxide ceramic r
Dent. 1999 Summer;1(2):153-8.
Mannocci F, In
microscopic study of teeth restored with fiber posts, metal posts, and composite resins. J
Endod 1999;25:78
Marshall GW, Marshall S, Kinney JH, Balooch M. The dentin substrate: structure
and properties related to bonding. J Den
Martelli R. Fourth generation intraradicular posts for the aesthetic restoration of
anterior teeth. Pract Periodont Ae
Mason PN. Transactions of International ADM meeting, Siena 2001.
Mattison GD. Photoelastic stress analysis of cast-gold endodonti
Dent 1982;48: 407-11.
Mayer T, Pioch T, Duschner H, Stahele HJ. Dentinal adhesion and histomorphology
of two d
Mc Comb D, Smith DC. A preliminary scanning electron microscope study of root
canals after endodontic proced
Meister F, Lommel TJ, Gerstein H. Diagnosis and possible causes of vertical root
fractures. Oral Surg, Oral Med, Oral Pathol 1980;49: 243-53.
Milot P, Stein RS. Root fracture in endodontically treated teeth related to post
selection and crown design J Prosthe
176
Mjör IA, Nordhal I. The density and branching of dentinal tubules in human teeth.
Archs Oral Biol 1996; 41: 401-412.
Monticelli F, Grandini S, Goracci C, Ferrari M. Clinical behaviour of translucent
fiber posts and luting and restorative materials: a 2-year report. Int J Prosthod
2003;16,(6):593-6.
Morgano SM, Milot P. Clinical success of cast metal post and cores. J Prosthet Dent
1993; 70:11-6.
Morfis AS. Vertical root fractures. Oral Surg, Oral Med, Oral Pathol 1990;69: 631-
.
ciples in
resent an
d prosthodontics: current
osts. J Prosthet Dent 2003
J Dent Res 1993; 92: 127.
Panighi M, G’Sell C. Effect of the tooth microstructure on the shear bond strength
f a denta
between dentin microhardness
d tubul
eability: effect of smear layer
fixed prosthodontic restoration.
Pract Period Aesthet Dent 1998;5:513-20.
35
Morgano SM. Restoration of pulpless teeth: application of traditional prin
p d future contexts J Prosthet Dent 1996;75: 375-80.
Morgano SM, Brackett SE. Foundation restorations in fixe
knowledge and future needs. J Prosthet Dent 1999;82: 643-57.
Morgano SM, Milot P. Clinical success of cast metal post and cores. J Prosthet Dent
1993; 70:11-6.
Morris MD, Lee KW, Agee KA, Bouillaguet S, Pashley DH. Effects of sodium
hypochlorite and RC-prep on bond strengths of resin cement to endodontic surfaces. J Endod
2001;27:753-7.
Nakabayashi N, Pashley DH. Hybridization of dental hard tissues Berlin:
Quintessence Co. Publ. 1998.
Newman MP, Yaman P, Dennison J, Rafter M, Billy E. Fracture resistance of
endodontically treated teeth restored with composite p
Apr;89(4):360-7.
Nissan R, Sehal H, Pashley DH, Trowbridge H. Ability of bacterial endotoxin to
permeate human dentin.
Otsby BN. Chelation in root canal therapy. EDTA for cleaning and widening of root
canals. Odontal. Tidskz. 1957; 65: 3-11.
o l composite. J Biomed Mater Res 1993;27: 975-81.
Pashley DH, Okabe A, Parham P. The relationship
an e density. Endod Dent Traumatol 1985;1: 176-79.
Pashley DH, Michelich V, Kehl T. Dentin perm
removal. J Prosthet Dent 1981; 46: 531-7.
Paul S, Scharer P. Post and core reconstruction for
177
Pegoretti A, Fambri L, Zappini G, Bianchetti M. Finite element analysis of a glass
fibre reinforced composite endodontic post. Biomat 2002;23:2667-82.
.
ared with hand and rotatory instruments. J Endod 1998;24: 401-4.
-23.
0.
d-core systems. Quintessence Int 1999; 30: 61-7.
S, Apicella A, Ausiello P, Davidson CL. The distribution of stress in carbon
er pos
, Dallari A. Odontoiatria conservatrice. Hermes Ed. Milano, 2001.
987;3:10-4.
. J Dent Res 1994;73: 1205-11.
Peters O, Barbakov F. Effects of irrigation on debris and smear layer on canal walls
prepared by two rotary techniques: a scanning electron microscopic study. J Endod 2000; 1:
6-10.
Peyton FA, Mahler DB, Hershenov MS. Physical properties of dentin. J Dent Res
1952;31: 366-70
Pilo R, Corcino G, Tamse A. Residual dentin thickness in mandibular premolars
prep
Pilo R, Tamse A. Residual dentin thickness in mandibular premolars prepared with
gates glidden and ParaPost drills. J Prosthet Dent 2000;8: 617
Pimenidis MZ, Hinds JW. An autoradiographic study of the sensory innervation of
teeth. Dental pulp and periodontium. J Dent Res 1977;56: 835-4
Reagan SE, Fruits TJ, Van Brunt CL, Ward CK. Effects of cycling loading on
selected post-an
Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of
endodontic and restorative procedures. J Endod 1989;15: 512-6.
Rengo
fib ts restorations: a preliminary study. Proceedings from the 3rd International
Symposium. 60-61, 1999.
de Rijk WG. Removal of fiber posts from endodontically treated teeth. American
Journal of dentistry. 13: 19B-21-B, 2000.
Rovatti L
Ross IF. Fracture susceptibility of endodontically treated teeth. J Endod1980;6:560-
5.
Rud J, Omnell KÅ. Root fractures due to corrosion. Diagnostic aspects. Scand J
Dent Res. 1970;78: 397-403.
Saleh AA, Ettman WM Effect of endodontic irrigation solutions on microhardness
of root canal dentine. J Dent 1999;27: 43-6.
Salis SG, Hood JAA, Stokes ANS, Kirk EEJ. Patterns of indirect fracture in intact
and restored human premolar teeth. Endod Dent Traumatol 1
Sano H, Ciucchi B, Matthews WG, Pashley DH. Tensile properties of mineralized
and demineralized human and bovine dentin
178
Sano H, Yoshiyama M, Ebisu S, Burrow MF, Takatsu T, Ciucchi B, Carvalho R,
Pashley DH. Comparative SEM and TEM observations of nanoleakage within the hybrid
yer. Op
ed demineralized human dentin. J Dent Res 1995b;74: 1093-102.
. Dent Mater. 1992 Mar;8(2):131-6.
g;11(4):181-5.
ability in simulated curved
canals. In
of eugenol and non eugenol
e ricostruttiva, S. Margherita Ligure, 2000; 21-27.
, S.Diego, 2002, abstract n° 2657.
ter post
space pre
g Oral Med Oral Pathol Oral Radiol Endod. 2004 Mar;97(3):381-7.
arol Stream, IL: Quint Publ. Co., Inc 1997;194-7.
0;64:419-24.
Standlee JP, Caputo M, Hanson EC. Retention of endodontic dowels: effect of
cement, dowel length, diameter and design. J Prosthet Dent 1978;39: 400-5.
la er Dent 1995a;20, 160-7.
Sano H, Takatsu T, Ciucchi B, Russell CM, Pashley DH. Tensile properties of resin
infiltrat
Sakaguchi RL, Cross M, Douglas WH. A simple model of crack propagation in
dental restorations
Saunders WP. Effect of fatigue upon the interfacial bond strength of repaired
composite resin. J Dent 1990; 18: 158-62.
Saunders EM, Saunders WP. Long-term coronal leakage of JS Quickfill root fillings
with Sealapex and Apexit sealers. Endod Dent Traumatol. 1995 Au
Sawada N, Hikage S, Sakaguci K. Shape of composite resins photopolymerized by
the translucent post. J Dent Res IADR abstract # 2569; 2002.
Schafer E, Lohman D. Efficiency of rotary nickel-titanium Flex-Master instruments
compared with stainless steel hand K-Flexofile – Part 1. Shaping
ternational Endododontic Journal 2002;35, 502-13.
Schwartz RS, Murchison DF, Walker WA 3rd. Effects
endodontic sealer cements on post retention. J Endod 1998;24:564-67.
Scotti R. Ricostruzioni preprotesiche con perni in fibra di quarzo: esperienza clinica
a 18 mesi. Odontoiatria adesiva
Scotti S, Malferrari S, Monaco C. Clinical evaluation of quartz fiber posts: a 30
months results. IADR 80th General Session
Serafino C, Gallina G, Cumbo E, Ferrari M. Surface debris of canal walls af
paration in endodontically treated teeth: a scanning electron microscopic study. Oral
Sur
Shillimburg HT, Hobo S, Whitsett LD, Jakobi R, Bracket SE. Fundamentals of
fixed prosthodontics, 3rd ed. C
SorensenJA, Engelmen MJ. Effect of post adaptation on fracture resistance of
endodontically treated teeth. J Prosthet Dent 199
Sorensen JA, Martinoff JT. Clinically significant factors in dowel design. J Prosthet
Dent 1984a52: 28-35.
Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a
study of endodontically treated teeth. J Prosthet Dent 1984b51: 780-84.
179
Standlee JP, Caputo AA, Holcomb JP, Trabert KC. The retentive and stress-
distributing properties of a threaded endodontic dowel. J Prosthet Dent 1980;44: 398-404.
Stankiewicz NR, Wilson PR. The ferrule effect: a literature review. Int J Endod
literature review. J
ronal microleakage in endodontically
eated te
M. Effect of Post and Core Restorations and the
J 1999; 32: 32-9.
morphologic relationship of the
resin-den
interface.
al of temporary
6-500.
d posts luted with an adhesive composite luting cement. Quintessence
characteristics for
2002; 35: 575-581.
Stockton LW. Factors affecting retention of post systems: A
Prosth Dent 1999; 81: 380-5.
Swanson K, Madison S.An evaluation of co
tr eth. Part I. Time periods. J Endod. 1987 Feb;13(2):56-9.
Sorrentino R, Tanganelli E, Ferrari
Number of Residual Dental Walls on the Resistance to Fracture of Endodontically Treated
Maxillary Premolars. Submitted to Am J Dent 2004.
Takeda FH, Harashima T, Kimura Y, Matsumoto K. A comparative study of smear
layer by three endodontic irrigants and two types of laser. Int End
Tamse A, Fuss Z, Lustig J, Kaplavi J. An evaluation of endodontically treated
vertically fractured teeth. J Endod 1999;25: 506-08.
Tay FR, Gwinnett AJ, Pang KM, Wei SHY. Micro
tine interface following a total-etch technique in vivo using a dentinal bonding
system. Quint Int 1995;26, 63-70.
Tay FR, Gwinnett AJ, Wei SH. The overwet phenomenon: an optical,
micromorphological study of surface moisture in the acid-conditioned, resin-dentine
Am J Dent 1996;9, 43-8.
Terata R. Characterization of enamel and dentin surfaces after remov
cement. Dent Mater J 1993:12:18-28.
Testori T, Badino M, Castagnola M. Vertical root fractures in endodontically treated
teeth: a clinical survey of 36 cases. J Endod 1993;19: 87-91.
Tidmarsh BG. Restoration of endodontically treated posterior teeth. J Endod 1976,
2:374-5.
Tjan AHL, Whang S. Resistance to root fracture of dowel channels with various
thicknesses of buccal dentin walls. J Prosth Dent 1985; 53: 49
Tjan AHL, Nemetz H. Effect of eugenol-containing endodontic sealer on the
retention of prefabricate
Int 1992;23:839-44.
Torbjöner A, Karlsson S, Odman PA. Survival rate and failure
two post designs. J Prosthet Dent 1995;73: 439-44.
180
Trabert KC, Caputo AA, Abou Rass M. Tooth fracture: a comparison of endodontic
and restorative treatments. J Endod 1978;4: 341-5.
Tronstad L, Asbjornsen K, Doving L, Pedersen I, Eriksen HM. Influence of coronal
restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol
perts, by J. Swift. J Esth Rest Dent 2004;16(1):6.
oos JR, Braem M, Lambrechts P, Van
Dent. 2000;83:412-7.
ari M. Comparison between two clinical procedures for
re posts under clinical conditions. Dent Mat 2002a;18,
95-502.
een two clinical procedures for
Walton TR. A 10-year longitudinal study of fixed prosthodontics.1 Protocol and
rosthodontics: clinical
12-4.
olars. Int J Prosthodont 2004; 17:94-8.
2000,16(5): 218-21.
Trope M. Ask the ex
Tyldesley WR. The mechanical properties of human enamel and dentine. Br Dent J
1959;106: 269-78.
Ukon S, Moroi H, Okimoto K. Influence of different elastic moduli of dowel and
core on stress distribution in root. Dent Mater 2000; 19: 50-64.
Van Meerbeek B, Willems G, Celis JP, R
Herle G. Assessment by nano-indentation of the hardness and elasticity of the resin-dentin-
bonding area. J Dent Res 1993;72: 1434-42.
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on the
masking of various types of opaque posts. J Prosthet
Vichi A, Grandini S, Ferrari M, Clinical procedure for luting Vectris fiber posts. J
Adhes Dent 2001; 3: 353-359.
Vichi A Grandini S, Ferr
bonding fiber posts into a root canal: a microscopic investigation. J. Endod 2002;28:355-60.
Vichi A. A study into application of fiber technology into fiber posts. PhD thesis,
Amsterdam 2002.
Vichi A, Grandini S, Davidson CL, Ferrari M. An SEM evaluation of several
adhesive systems used for bonding fib
4
Vichi A, Grandini S, Ferrari M. Comparison betw
bonding fibre posts into a root canal: a microscopic investigation. J Endod 2002b;28, 355-60.
patient profile. Int J Prosthodont 1997;10: 325-31.
Walton TR. A 10-year longitudinal study of fixed p
characteristics and outcome of single unit metal crowns. Int J Prosthodont 1999;12: 519-26.
Walton R, Torabinejad M. Principles and practice of endodontics, 2nd edition, W.B.
Saunders Co., 1996: 2
Yamada Y, Tsubota Y, Fukushima S. Effect of restoration method on fracture
resistance of endodontically treated maxillary prem
181

Yamamoto M, Takahashi H. Tensile fatigue strength of light cure composite resins
for posterior teeth. Dent Mater J 1995 ;14:175-84.
Yip KH, Smales RJ, Kaidonis JA. Differential wear of teeth and restorative
materials: clinical implications. Int J Prosthodont. 2004; 17(3):350-6.
Zhao F, Takeda N. Effect of interfacial adhesion and statistical fiber strength on
ental Results. tensile strength of unidirectional glass fiber/epoxy composites. Part I. Experim
Composites A 2000;31:1203-14.
182
A ledgements
cknow
is the
, University of Siena,
nce, and to Prof Marco Ferrari, Pro-Rector for
international affairs and President of Dental School, University of Siena.
I want to express my heartfelt appreciation to Prof Bertelli. He gave me the
possibility to start my adventure in Siena, and always supported my uncertain steps
in my new University.
My sincere gratitude to my promoter Prof Marco Ferrari. He patiently and
continuously reviewed my work, and shared his knowledge with generosity. He has
been my promoter, my professor, my friend. “Give a man a fish, and he survives for
a day. Teach the man to fish, and he will feed himself for life”, he always say, and I
thank him for the fishes and for the fishing!
My deepest thanks to Prof Franklin Tay, my co-promoter. Not only he shared his
awareness with me, but he also “lighted the fire” of research! His knowledge and
friendship have been so precious to me. I find it hard to express my gratitude to him.
I would also like to express my sincere appreciation to the whole Committee, Prof
Carel Davidson, Prof Michel Goldberg, Prof Manuel Toledano, Prof Piero Balleri,
for spending time on reviewing this piece of work and for their precious suggestions,
stimulation and encouragement.
Let me also thank the friends who shared this challenge with me and helped me in so
many ways that they cannot even imagine. Dr Marco Simonetti, my very dear
friend; Dr PierFrancesco Porciani (the wizard of computers!) for unwearyingly
solving all the problems with my laptop, and listening to my other problems as a real
friend; Dr Cecilia Goracci (the queen of statistics!) and all the other PhD candidates
and PhD students that shared this way and worked with me during this period.
A great thank you to Dr Bianca Angelotti, for the secretarial support, and to the
people who helped me with the translation: my mother Vanda (french), Mrs Pamela
Marklew and Mrs Barbara Johnson (german), Dr Maria Carolina Erhardt
(portuguese), Mrs Ornella Raffaelli and Dr Alberto Albalalejo Martinez (spanish).
Th sis is respectfully submitted to Prof Piero Tosi, Rector of the University of
Siena, to Prof Alberto Auteri, Dean of the Faculty of Medicine
to Prof Egidio Bertelli, vice-Dean of the Faculty of Medicine and Director of the
Department of Dental Scie
183

Last but not least I would like to thank my family at large. They supported me
uring this busy period and had to bear my unpredictable humour in the house: I
y life. A
d
love them forever, and I am probably incapable to show how much. My father
Romano (The Professor!): I probably did all I did because I wanted to try to imitate
him, poor me, he is not imitable. He’s a superb clinician, a warm and generous
teacher in the University, and most important of all a respected and honest man. My
mother Vanda: she’s the best mum one could have, and a milestone in m
kiss to my sisters Ilaria and Valentina.
There are too many other people I’d like to thank, who will, I hope, understand my
forgetfulness.
184
CURRICULUM VITAE
Dr. Simone Grandini
Office Via Poliziano, 3
50127 Florence.
Home: Via Guelfa 86
Phones Tel: 055-472895 (office) Fax: 055-474520
055-489789 (home)
e-mail: [email protected]
Date and place of birth: Florence, Italy, 22 February 1970
Professional positions
Chair of Restorative Dentistry III, School of Dentistry, University of Siena.
Professional Organizations membership
2004- Academy of Dental Materials
2001 and 2003 International Association for Dental Research
1993- Società Italiana di Odontoiatria Conservatrice (Italian Society of
Restorative Dentistry)
1993- Società Italiana di Odontoiatria e Chirurgia Maxillo-Facciale (SIOCMF)
50129 Florence, Italy
185

List of papers part of this thesis
randini S, Balleri P, Ferrari M. valuation of Glyde File Prep in combination with sodium hypochlorite as root anal irrigant: a scanning electron microscopic study. ournal of Endodontics 2002 Apr;28(4):300-3.
n , Balleri P, Fe M. g lectron microscopic inve rface of post after cutting.
-2.
se of Anatomic post’n for dontically treated tooth: a ase report. ournal of Adhesive Dentistry 2003, vol 5, num. 3, pag. 243-247
cedures of two
randini S, Sapio S, Goracci C, Monticelli F, Ferrari M. l
Monticelli F, Tay F, Ferrari M. tructural characteristics of fiber posts: three-point bending
ental Materials 2004, in press.
, Grandini R, Ferrari M. posts and direct resin crowns for restoring
re
GEcJ Grandi i S rrariScannin e stigation of the suJournal of Endodontics 2002 Aug;28(8):610 Grandini S, Sapio S, Simonetti M. U core reconstructing an endocJ Grandini S, Sapio S, Goracci C, Monticelli F, Ferrari M. SEM evaluation of the cement layer thickness after the luting prodifferent posts. Journal of Adhesive Dentistry 2004, in press. GA one step procedure for uting glass fibre posts: an SEM evaluation International Endodontic Journal 2004, Oct;37(10):679-86. Grandini S, Goracci C, Fatigue resistance and stest and SEM evaluation. D Grandini S, Goracci C, Monticelli F, Tay FClinical evaluation of the use of fiber endodontically-treated teeth. International Journal of Prosthodontics, in press, 2004. Grandini S. The Anatomic post’n coFrom the book: “Fiber posts” Scotti R, Ferrari M. Masson Ed, Milano 2002
186

List of abstracts part of this thesis
F, Ferrari M.
randini S, Ferrari M, Goracci G, Bertelli E. morphology in root canals after shaping and
002, #52, pag B238
chi A.
resin cement. 2
Ferrari M.
any, June 5-8, 2003
ri M. Posts
, B-192
82 (Special Issue B) 2003, #2935, B-376
randini S, Vichi A, Borracchini A, Ferrari M.
Grandini S, Narducci P, Porciani PSEM investigation of the surface of fiber posts after cutting procedures. ADM transactions, 232, vol 15, 2001 GQuantitative evaluation of dentinirrigation of the endodontic space. Journal of Dental Research 81 (special issue B) 2 Grandini S, Ferrari M, Balleri P, ViClinical trial of fiber posts luted with self-curing Excite in combination with an experimentalJournal of Dental Research 81 (special issue A) 2002, #198, pag A5 Grandini S, Balleri P, Goracci C, Monticelli F, Bertelli E,Scanning Electron Microscopic Evaluation of two different techniques for luting glass fiber post Abstract from Conseuro meeting, Munich, Germ Grandini S, Borracchini A, Goracci C, Monticelli F, FerraSEM Study to Compare the Luting Procedures of Two Different FiberJournal of Dental Research 82 (Special Issue B) 2003, #1442 Grandini S, Goracci C, Monticelli F, Tay FR, Ferrari M.Fatigue Resistance of Different Kinds of Fiber Posts Journal of Dental Research GDirect resin restorations with a fiber post: a case report Accepted for IADR meeting, Istambul 2004
187

Complete list of papers Ferrari M, Grandini S. Use of enamel dentinal adhesives systems: clinical implications. (Les adhésifs
) ealités Cliniques 2000.; 11:419-429
iques on bonding to root canal walls: An SEM
ental Materials 2001 Sep;17(5):422-9.
glass-fiber posts.
an SEM investigation.
as root
ournal of Endodontics 2002 Apr;28(4):300-3.
sts into a root anal: a microscopic investigation.
reatment of crown fractures. (Traitement des fractures coronaires) Réalités Cliniques 2002, vol 13, n.1, 17-26. Grandini S, Balleri P, Ferrari M. Scanning electron microscopic investigation of the surface of post after cutting. Journal of Endodontics 2002 Aug;28(8):610-2. Ferrari M, Grandini S, Simonetti M, Monticelli F, Goracci C. Influence of a microbrush on bonding fiber posts into root canals under clinical conditions. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 2002; 94: 627-631.
amélo-dentinaires: implications pratiquesR Ferrari M, Vichi A, Grandini S. Efficacy of different adhesive technevaluation. D Vichi A, Grandini S, Ferrari M. Clinical procedure for luting Journal of Adhesive Dentistry 2001 Winter;3(4):353-9. Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy of a self-curing adhesive resin cement system on luting glass-fiber posts into root canals:International Journal of Prosthodontics 2001 Nov-Dec;14(6):543-9. Grandini S, Balleri P, Ferrari M. Evaluation of Glyde File Prep in combination with sodium hypochlorite canal irrigant: a scanning electron microscopic study. J Vichi A, Grandini S, Ferrari M. Comparison between two clinical procedures for bonding fiber pocJournal of Endodontics 2002 May;28(5):355-60. Grandini S, Sapio S, Ferrari M. T
188

Vichi A, Grandini S, Davidson CL, Ferrari M. n SEM evaluation of several adhesive systems used for bonding fiber posts under
i S. fluence of microbrush on efficacy of bonding into root canals
Aug;15(4):227-31.
Sapio S, Simonetti M. ucting an endodontically treated tooth: a
ase report. 3, vol 5, num. 3, pag. 243-247
linical behavior of translucent fiber posts and luting and restorative materials: a 2-
Six-Week Study to Evaluate the AnticalculusEfficacy of a Chewing Gum olyphosphate”
nticalculus Efficacy of a Chewing Gum with Polyphosphates in a Twelve-Week
rari M. EM evaluation of the cement layer thickness after the luting procedures of two
oracci C, Ferrari M, Grandini S, Monticelli F, Tay FR. ment to dental hard tissues
onticelli F, Goracci C, Grandini S, Garcìa-Godoy F, Ferrari M. re units built up with
publication in the American Journal of Dentistry 2003
Goracci C, Monticelli F, Ferrari M. one step procedure for luting glass fibre posts: an SEM evaluation ternational Endodontic Journal 2004, Oct;37(10):679-86.
Aclinical conditions. Dental Materials 2002 Nov;18(7):495-502. Ferrari M, Vichi A, Grandini S, GeppInAmerican Journal of Dentistry 2002 Grandini S, Use of Anatomic post’n core for reconstrcJournal of Adhesive Dentistry 200 Monticelli F, Grandini S, Goracci C, Ferrari M. Cyear report. International Journal of Prosthodontics 2003, volume 16, number 6, pag. 593-596 Porciani PF, Grandini S. AContaining Pyrophosphate and TripJournal of Clinical Dentistry 14:11-13, 2003 Porciani PF, Grandini S. ASingle-Blind Trial Journal of Clinical Dentistry 14: 2003 Grandini S, Sapio S, Goracci C, Monticelli F, FerSdifferent posts. Accepted in the Journal of Adhesive Dentistry 2003. GBonding of a self-adhesive resin ceAccepted in the Journal of Adhesive Dentistry 2003 MScanning electron microscopic evaluation of fiber post-resin codifferent resin composite materials Accepted for Grandini S, Sapio S, AIn
189

Grandini S, Goracci C, Monticelli F, Tay F, Ferrari M.
tion. 2004
C, Monticelli F, Yiu C, Huang C, Prati
ives ournal of Dental Research 2004; 83: 459-464.
Fatigue resistance and structural characteristics of fiber posts: three-point bending test and SEM evaluaAccepted for publication in Dental Materials Chersoni S, Suppa P, Grandini S, GoracciC, Breschi L, Ferrari M, Pashley DH, Tay FR. In vivo and in vitro permeability of 1-step self-etch adhesJ
190
Complete list of abstracts Grandini S, Magheri P, De Marco M.
EA. 3 endodontic world congress. Rome, 1995
central incisor. ental trauma. Florence, Italy, 1996.
ag 76 Porciani PF, Magheri P, Grandini S. Multidisciplinary approach to endodontic retreatments. Abstracts from 8th biennial congress european society of endodontology. Goteborg 1997 Porciani PF, Magheri P, Grandini S. Multi-disciplinary management of endodontic retreatments. Abstracts from IFEA fourth endodontic world congress. Jerusalem 1998, pag.1 Fabianelli A, Vichi A, Grandini S, Ferrari M, Davidson CL. Influence of self-etching priming bonding systems on sealing ability of class II restorations: leakage and SEM evaluation. Atti del congresso delle Società Europee di Conservativa (Conseuro 2000), pag 26 Ferrari M, Grandini S, Vichi A, Mannocci F, Lopes B, Fuzzi M. One-bottle and three steps adesive systems used for bonding fiber posts into root canals under clinical conditions: a SEM investigation. Atti del congresso delle Società Europee di Conservativa (Conseuro 2000), pag 27 Porciani PF, Grandini S. Clinical evaluation of a new endo-system: The A.E.T. IFEA, fifth endodontic world congress. Madrid 2001. Porciani PF, Grandini S. A new endodontic system: the A.E.T. A suggested flow chart. The 10th Biennial Congress of the European Society of Endodontology, 4-6 October 2001, Munich Fuzzi M, Grandini S. Clinical application of ceramic bonded restorations. ADM transactions, 51, vol 15, 2001 Lima Mourao R, Reis Hannas A, Grandini S, Ferrari M. Microleakage evaluation of the marginal adaptation of different restorative-adhesive combinations in class II composite restorations. ADM transactions. 167, vol. 15. 2001
The utilization of a new dental dam for endodontics. rdIF
Bertini F, Grandini S, Magheri P. Multidisciplinary aproach in a case of complicated fracture of aAbstract book. IADT. VIIth world congress on dP
191
Fabianelli A, Ferrari M, Dagostin A, Grandini S. perator variability influence on marginal seal of class II resin restorations.
EM investigation of the surface of fiber posts after cutting procedures.
tive evaluation of dentin morphology in root canals after shaping and rigation of the endodontic space.
issue B) 2002, #52, pag B238
study on the efficacy of a self-activating adhesive system used for bonding ber posts into root canal. Journal of Dental Research 81 (special issue B) 2002,
linical trial of Gradia indirect restorations. ag A333
elli E, Dolci G.
urnal of Dental Research 81 (special issue A) 2002, #3486, pag A429
ink luting materials.
Pyrophosphate: a six week
urnal of Dental Research 81 (special issue A) 2002, #2155, pag A276
sin cement. urnal of Dental Research 81 (special issue A) 2002, #198, pag A52
lli E, Ferrari M. of two different techniques for luting
lass fiber post June 2003
OADM transactions, 213, vol 15, 2001 Grandini S, Narducci P, Porciani PF, Ferrari M. SADM transactions, 232, vol 15, 2001 Grandini S, Ferrari M, Goracci G, Bertelli E. QuantitairJournal of Dental Research 81 (special Ferrari M, Grandini S, Fabianelli A, Vichi A. SEM fi#420, pag B282 Fabianelli A, Grandini S, Bertelli E, Ferrari M. CJournal of Dental Research 81 (special issue A) 2002, #2654, p Ferrari M, Cagidiaco MC, Grandini S, BertEffect of concentration on tooth whitening in a highly stained population. Jo Borracchini A, Fabianelli A, Grandini S, Ferrari M. Clinical trial of Empress II, selfcuring Excite and MultilJournal of Dental Research 81 (special issue A) 2002, #2634, pag A331 Porciani PF, Grandini S. Anticalculus efficacy of a chewing-gum containing study. Jo Grandini S, Ferrari M, Balleri P, Vichi A. Clinical trial of fiber posts luted with self-curing Excite in combination with an experimental reJo Grandini S, Balleri P, Goracci C, Monticelli F, BerteScanning Electron Microscopic Evaluation gProceedings of Conseuro meeting, Munich (Germany), 5-8
192
Monticelli F, Goracci C, Balleri P, Grandini S, Ferrari M. Clinical behavior of translucent fiber posts and luting restorative materials: a 2-year
port. ny), 5-8 June 2003
laque accumulation in One day with Four Chewing-gums in the absence of Oral
ransmission Electron Microscopic Evaluation of a Self-adhesive Material Luted to
racchini A, Goracci C, Monticelli F, Ferrari M. EM Study to Compare the Luting Procedures of Two Different Fiber Posts
003, #1442, B-192
ne-year Clinical Trial of Gradia Direct Class II Restorations , B-196
canning Electron Microscopic Evaluation of Fiber Post-Resin Core Unit , #1953, B-254 Journal of
randini S, Goracci C, Monticelli F, Tay FR, Ferrari M. rent Kinds of Fiber Posts
omposite inlays (Les inlays composites) e 169-171
errari M, Grandini S, Pashley DH, Prati C, Tay FR.
DR meeting, Honolulu 2004, Paper #46694
tric observations about the chromatic correspondence of some shade
ccepted for IADR meeting, Istambul 2004
reProceedings of Conseuro meeting, Munich (Germa Porciani PF, Grandini S, Sapio S. PHygiene Journal of Dental Research 82 (Special Issue B) 2003, #1056, B-144 Monticelli F, Grandini S, Goracci C. Ferrari M, Tay FR. TDifferent Dental Substrates. Journal of Dental Research 82 (Special Issue B) 2003, #1439, B-192 Grandini S, BorSJournal of Dental Research 82 (Special Issue B) 2 Fabianelli A, Grandini S, Goracci C, Ferrari M. OJournal of Dental Research 82 (Special Issue B) 2003, #1472 Monticelli F, Goracci C, Grandini S, Bertelli E, Balleri P, Ferrari M. SJournal of Dental Research 82 (Special Issue B) 2003dental Research 82 (Special Issue B) 2003, #1056, B-144 GFatigue Resistance of DiffeJournal of Dental Research 82 (Special Issue B) 2003, #2935, B-376 Ferrari M, Grandini S, Colon P. CAtti del Congresso ADF, Parigi, 2003. pagin Chersoni S, Acquaviva GL, FIn vivo fluid movement through adhesive in post space IA Borracchini A, Vichi A, Grandini S, Goracci C, Ferrari M. Spectrophotomeguides A
193

Goracci C, Sadek F, Grandini S, Vichi A, Borracchini A, Tay FR, Ferrari M.
d for IADR meeting, Istambul 2004
randini S, Vichi A, Borracchini A, Ferrari M. a case report
olor correspondence between Vita Shade guide and three different composite
Push-out bond strength and TEM evaluation of luted fiber posts Accepte GDirect resin restorations with a fiber post: Accepted for IADR meeting, Istambul 2004 Vichi A, Grandini S, Borracchini A, Ferrari M CAccepted for IADR meeting, Istambul 2004
194