Embed Size (px)
Citation preview
Basal ganglia
Sujata Sofat, class of 2009
Basal gangliaLearning Objectives
• Describe the function of the Basal Ganglia in movement
• Define the BG components and their locations
• Describe the motor loop of the BG
• Describe the direct motor circuit of the BG and how it functions
• Describe how the indirect motor circuit influences BG function
• Describe how the substantia nigra influences BG circuits
• Describe the symptoms of BG diseases and explain the vocabulary of movement disorders
• Describe the types of BG diseases, nuclei involved, and current treatments for Parkinson’s Dis.
http://nba.uth.tmc.edu/neuroscience/s3/chapter04.html
Overview
1. UMN activity in cortical motor areas is not great enough by itself to cause movement. So, it must get a boost – by the Basal Ganglia.
2. Basal Ganglia - 5 nuclei in cerebral hemispheres and brainstem.
Chris Cohan, Ph.D.Dept. of Pathology/Anat SciJacobs School of Medicine
Overview3. Basal Ganglia interconnected by excitatory and inhibitory
synapses. • increase precision of circuit• makes them difficult to analyze
4. Basal Ganglia diseases upset the balance of excitation and inhibition, leading to 2 paradoxical symptoms:
• Difficulty starting movements• Spontaneous movements at rest
Consequences of UMN needing a boost!
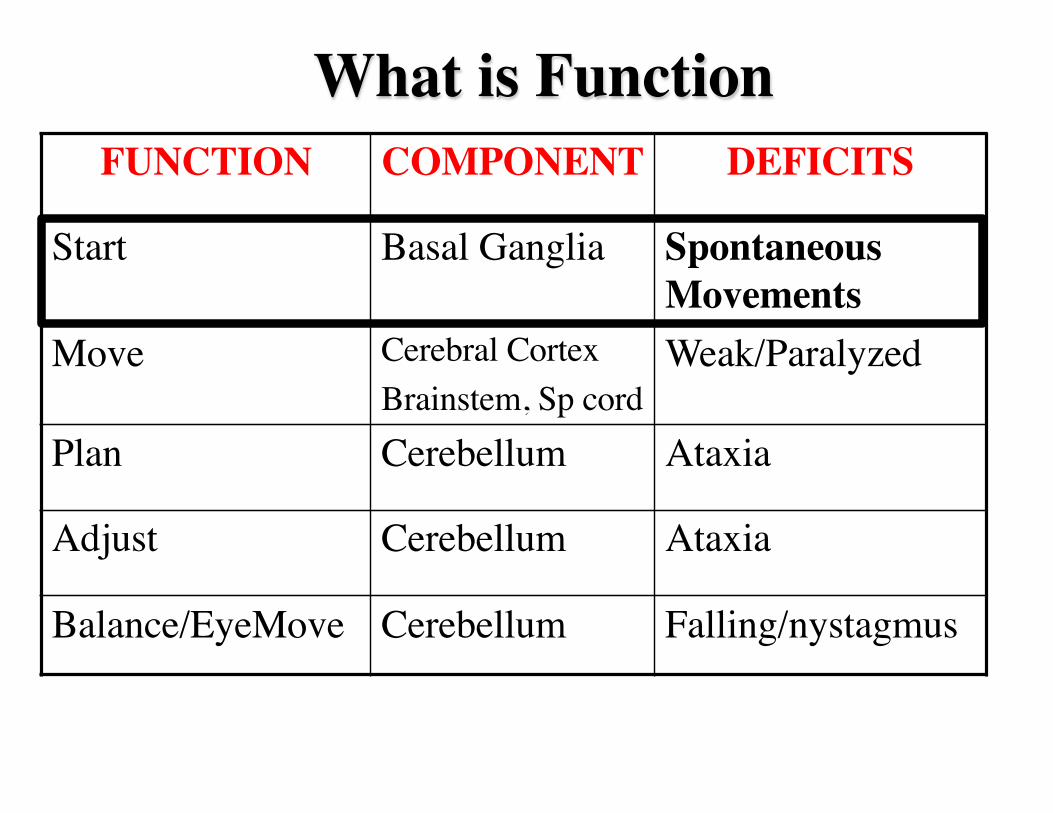
What is Function
• Start• Move• Coordinate• Adjust• Maintain balance and posture
FUNCTION COMPONENT DEFICITS
Start Basal Ganglia Spontaneous Movements
Move Cerebral CortexBrainstem, Sp cord
Weak/Paralyzed
Plan Cerebellum Ataxia
Adjust Cerebellum Ataxia
Balance/EyeMove Cerebellum Falling/nystagmus


Basal Ganglia- How it WorksUMN
Cerebral Cortex
Basal Ganglia
Cerebellum
Brainstem
Spinal Cord
Thalamus
head muscles
body muscles
Booster
The Basal Ganglia FACILITATE
movement
Terminology• Extrapyramidal (ie not the pyramidal system)
• Basal Ganglia are NUCLEI
• Basal Ganglia diseases are called MOVEMENT DISORDERS
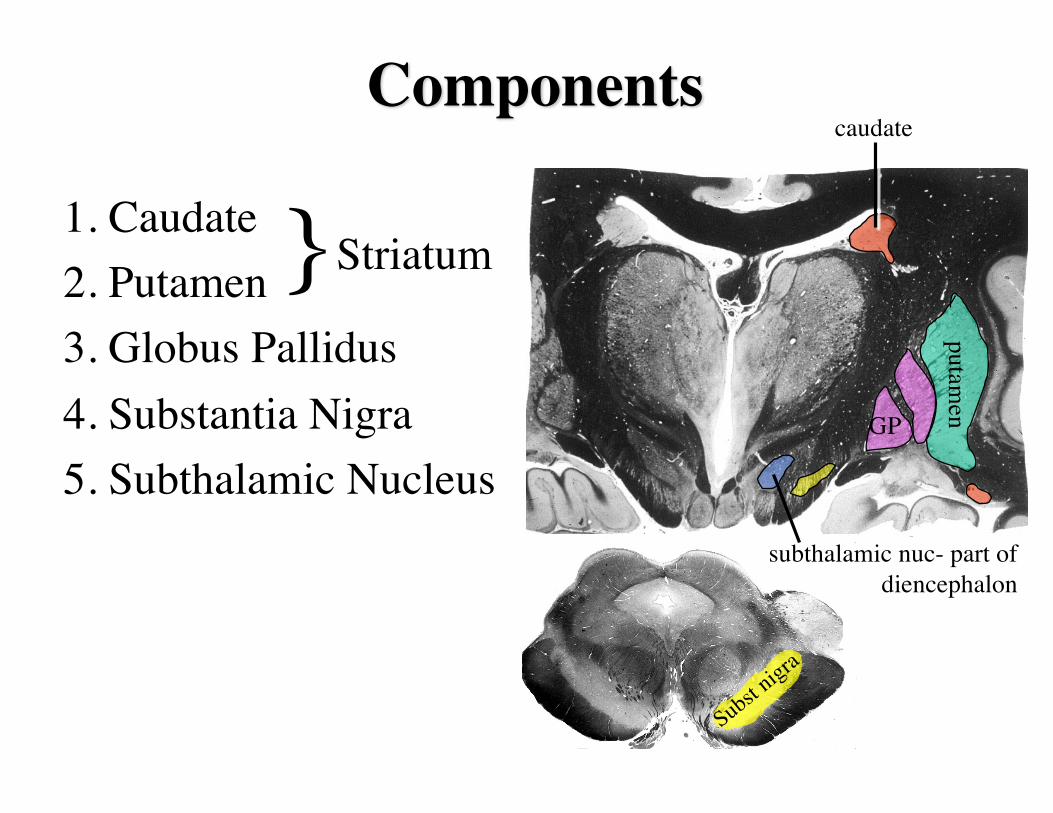
Components
1. Caudate2. Putamen3. Globus Pallidus4. Substantia Nigra5. Subthalamic Nucleus
}Striatum
caudate
Subst nigra
GP
putamen
subthalamic nuc- part of diencephalon
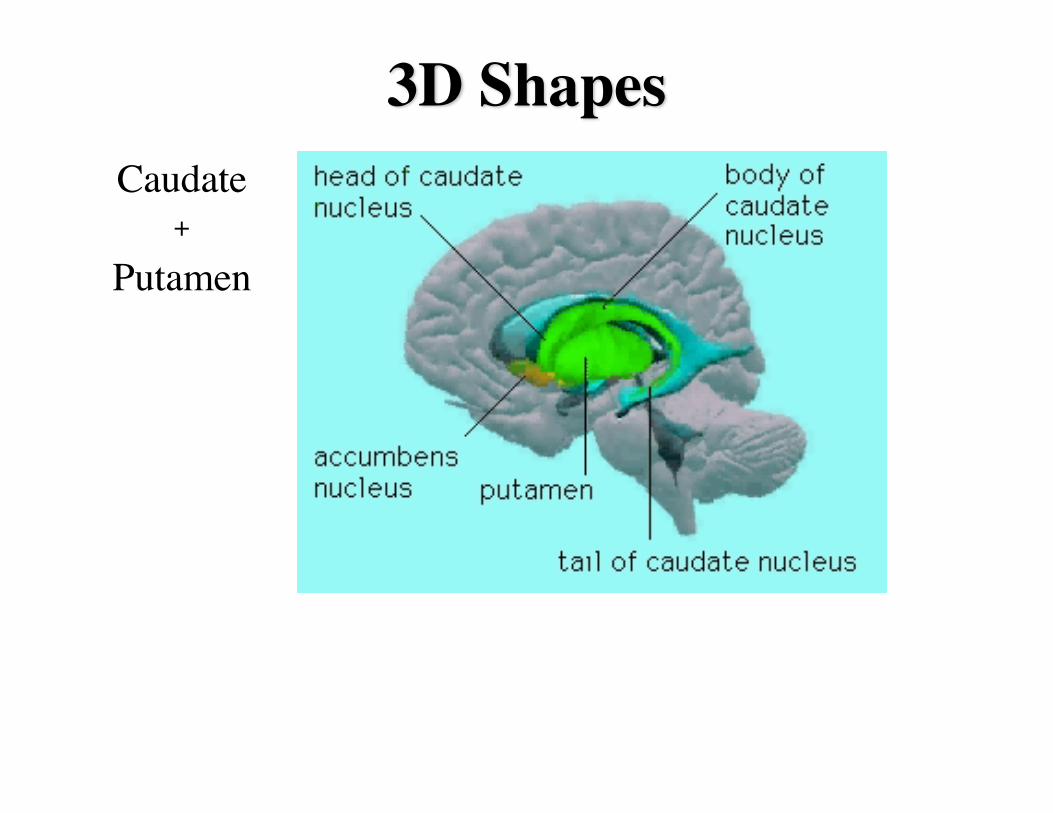
3D ShapesCaudate
+
Putamen
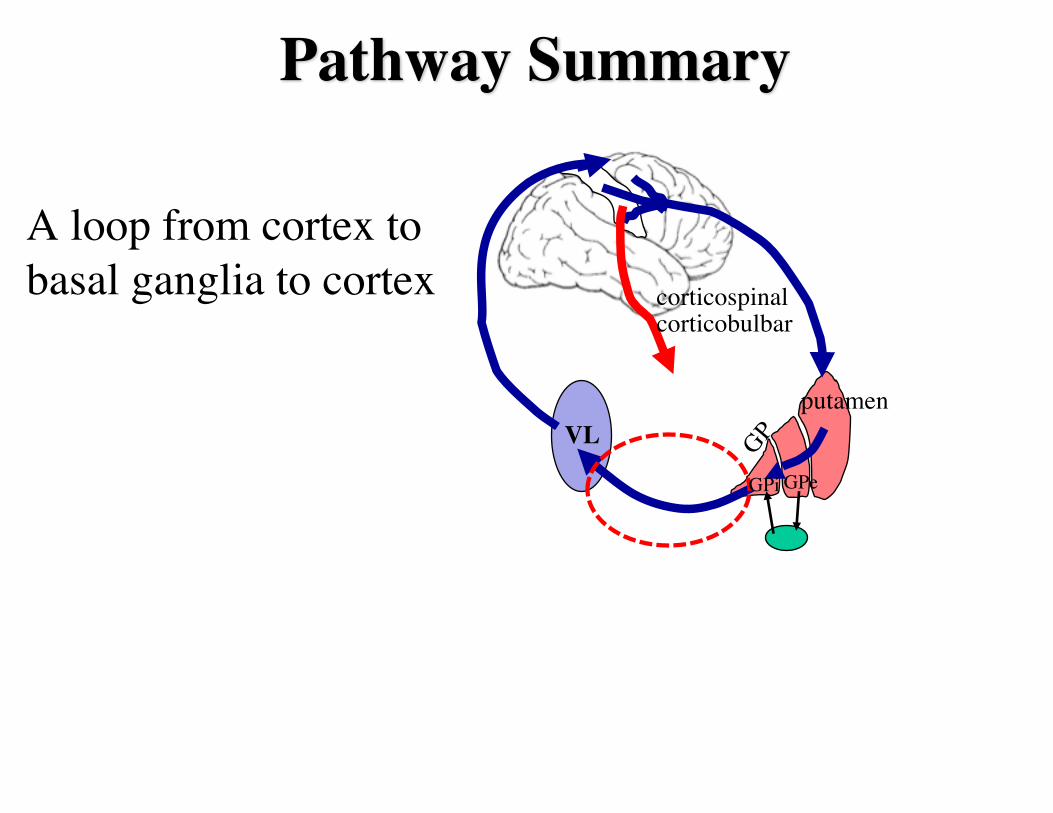
Pathway Summary
A loop from cortex to basal ganglia to cortex
VL
corticospinal corticobulbar
putamen
GP
GPeGPi
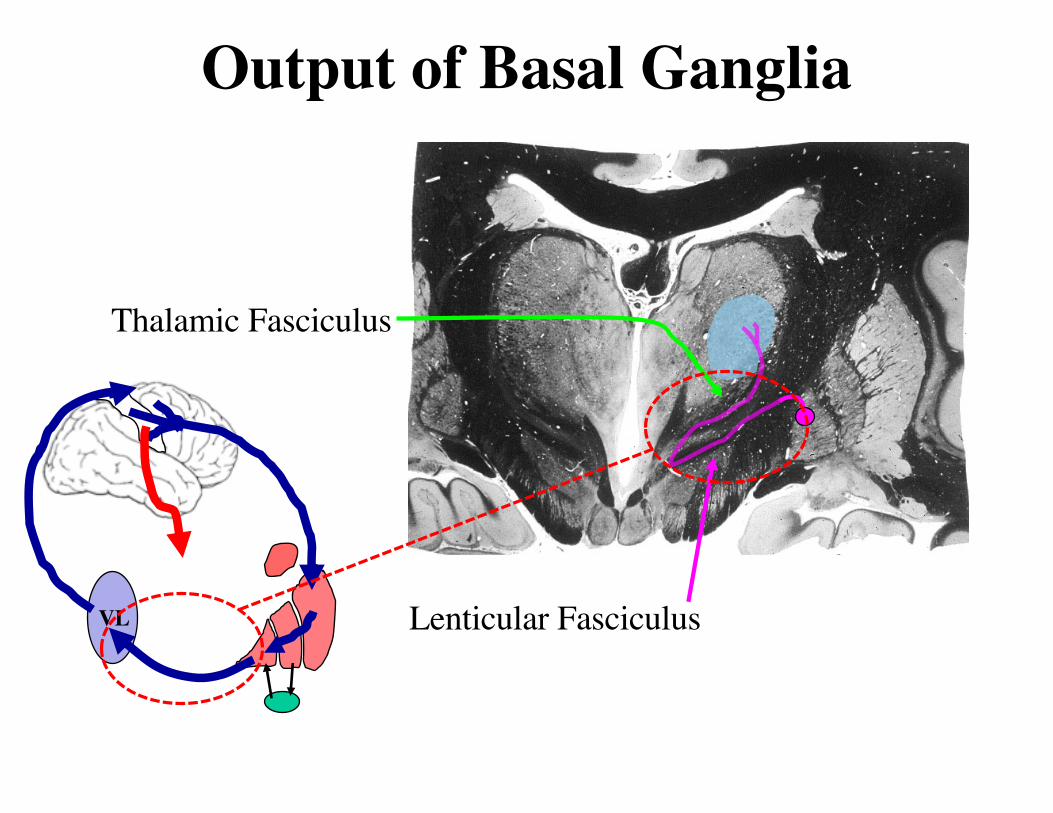
Output of Basal Ganglia
Lenticular Fasciculus
Thalamic Fasciculus
VL
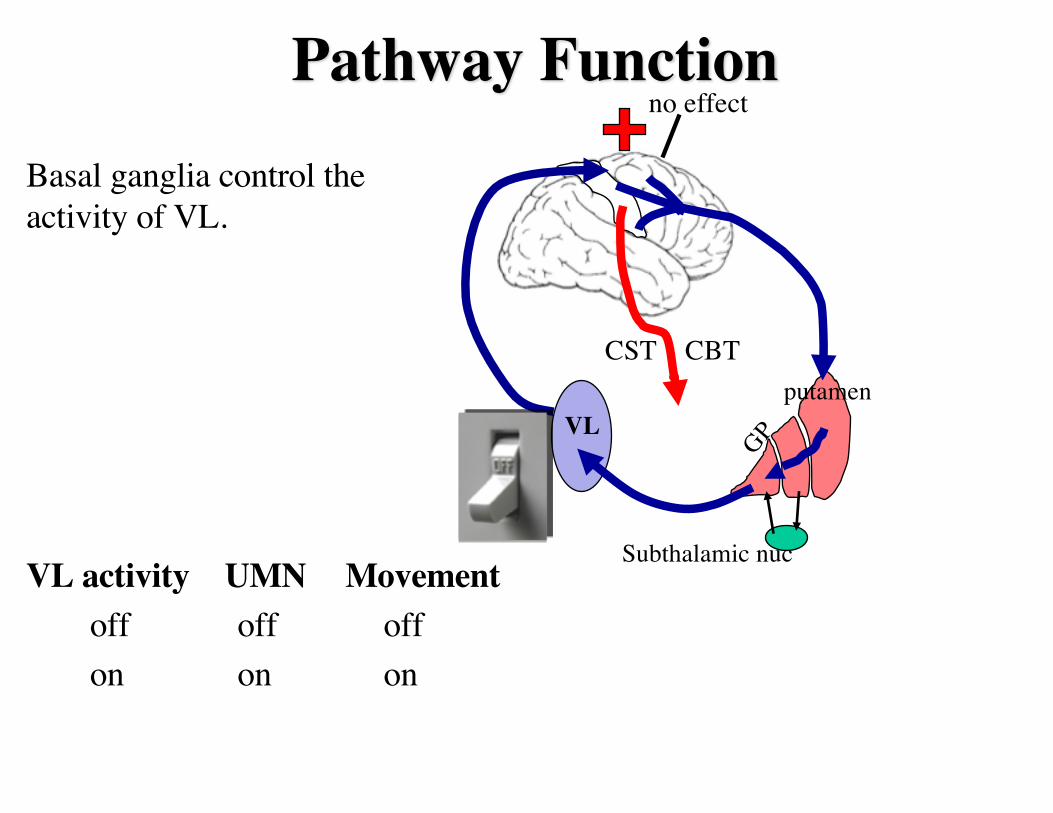
Pathway Function
VL
CST CBT
VL activity UMN Movementoff off offon on on
putamen
GP
Subthalamic nuc
on
Basal ganglia control the activity of VL.
no effect
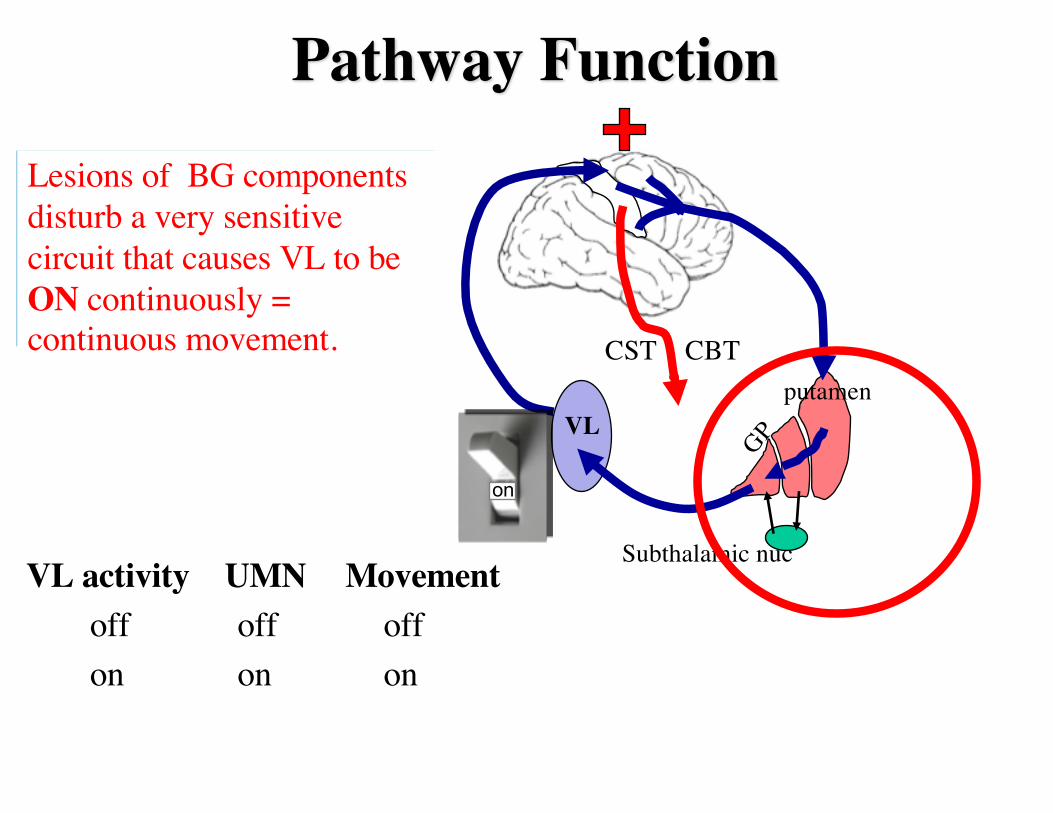
Pathway Function
VL
CST CBT
VL activity UMN Movementoff off offon on on
putamen
GP
Subthalamic nuc
What if there was a lesion in the BG that resulted in the switch being permanently turned on!
Lesions of BG components disturb a very sensitive circuit that causes VL to be ON continuously = continuous movement.
on
Direct and Indirect Circuits
VL
STN
indirect circuit
direct circuit
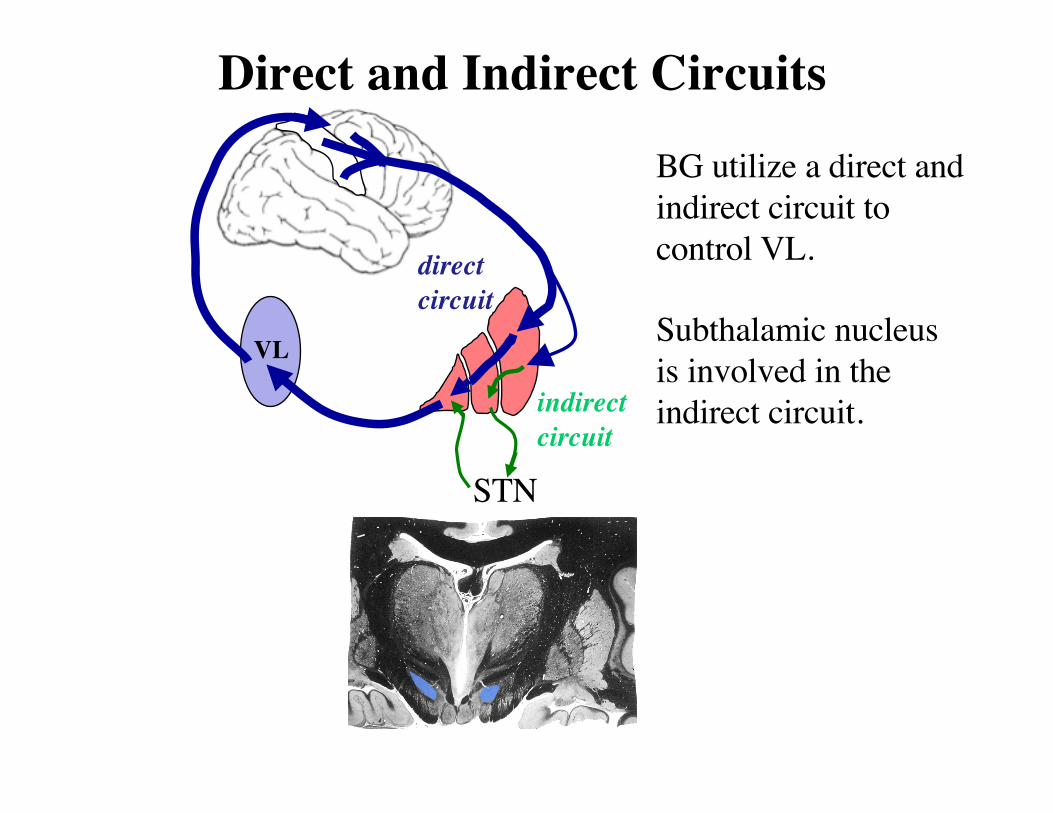
BG utilize a direct and indirect circuit to control VL.
Subthalamic nucleus is involved in the indirect circuit.
Direct and Indirect Circuits
VL
STN
indirect circuit
direct circuit
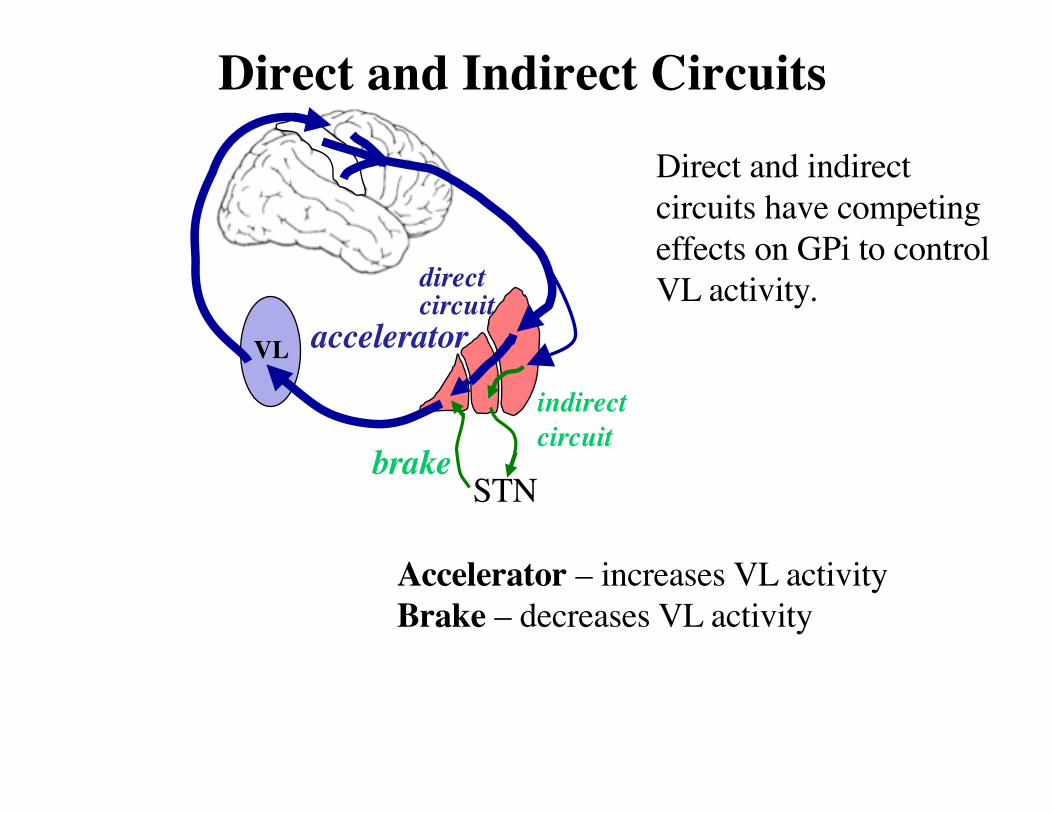
Direct and indirect circuits have competing effects on GPi to control VL activity.
accelerator
brake
Accelerator – increases VL activityBrake – decreases VL activity
Direct and Indirect Circuits
VL
STN
indirect circuit
direct circuit
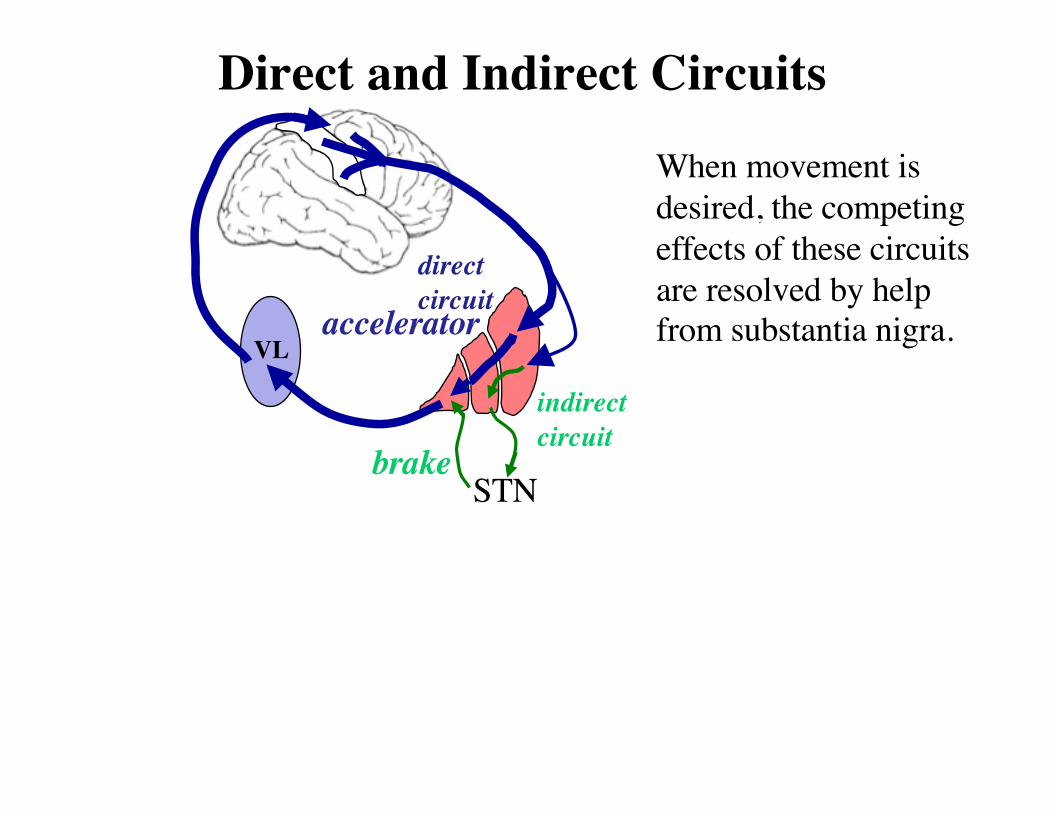
When movement is desired, the competing effects of these circuits are resolved by help from substantia nigra. accelerator
brake
Role of Substantia Nigra
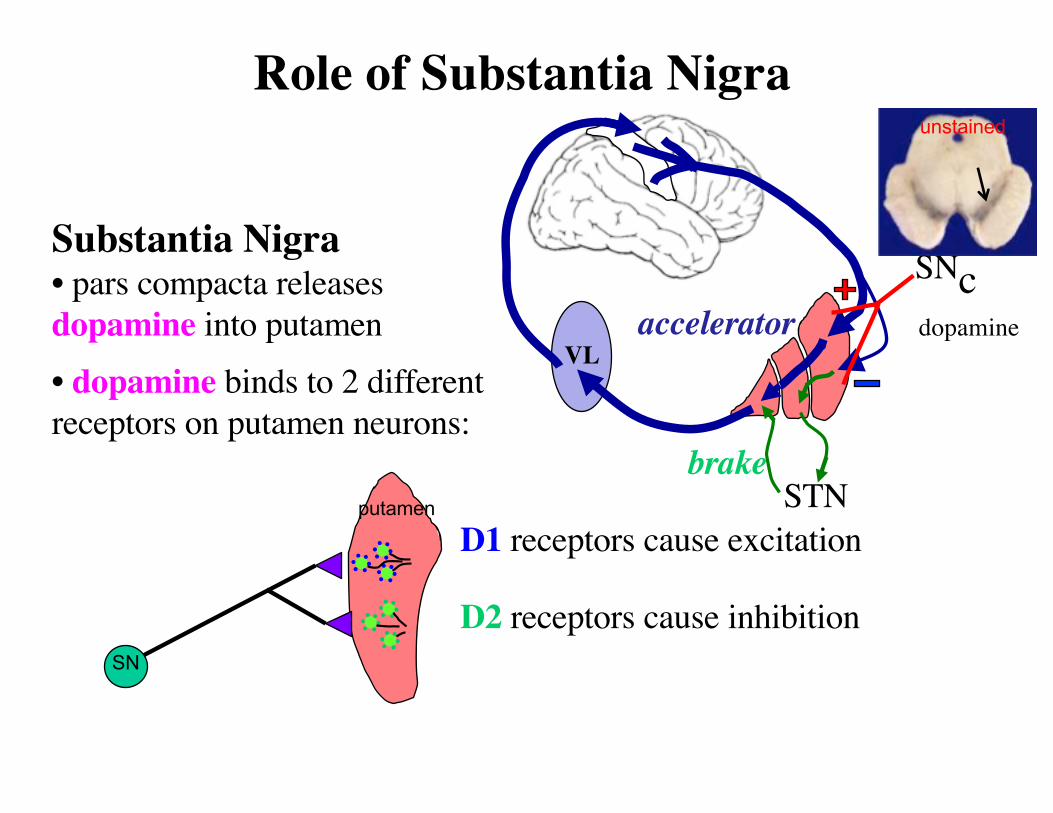
Substantia Nigra• pars compacta releases dopamine into putamen• dopamine binds to 2 different receptors on putamen neurons:
SNcdopamine
unstained
SN
putamen
D2 receptors cause inhibition
D1 receptors cause excitation
VL
STN
accelerator
brake
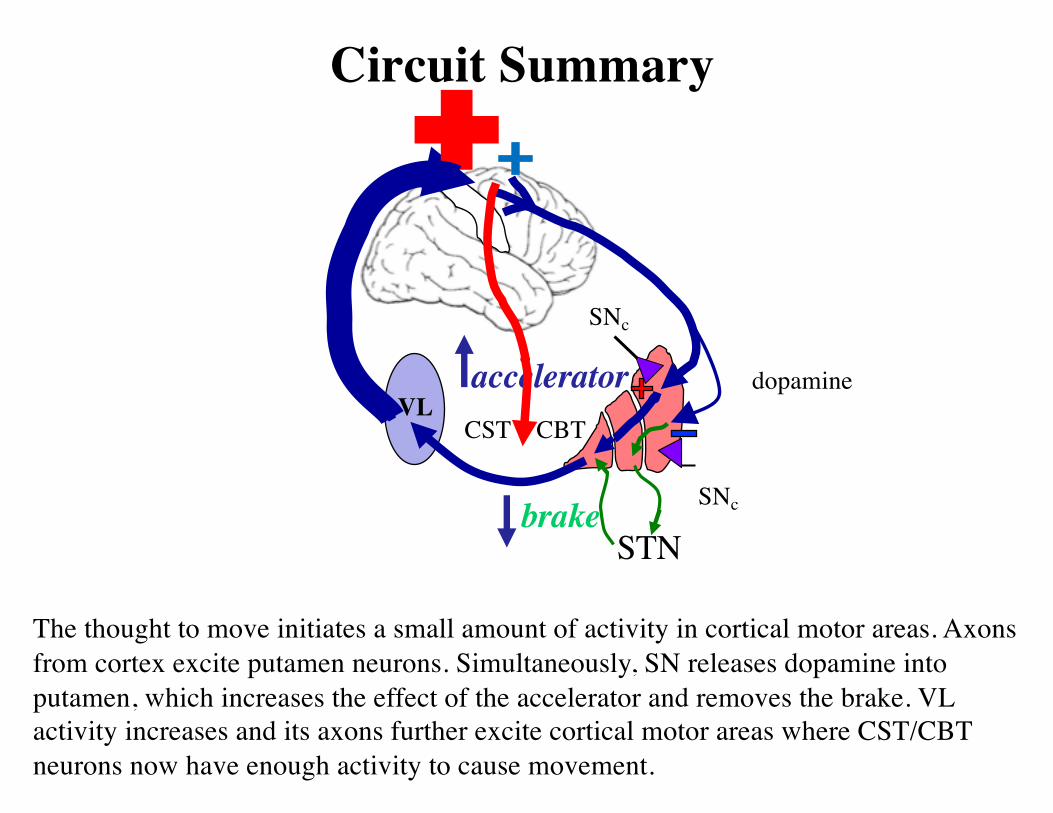
Circuit Summary
The thought to move initiates a small amount of activity in cortical motor areas. Axons from cortex excite putamen neurons. Simultaneously, SN releases dopamine into putamen, which increases the effect of the accelerator and removes the brake. VL activity increases and its axons further excite cortical motor areas where CST/CBT neurons now have enough activity to cause movement.
SNc
dopamineVL
STN
accelerator
brake
CST CBT
SNc
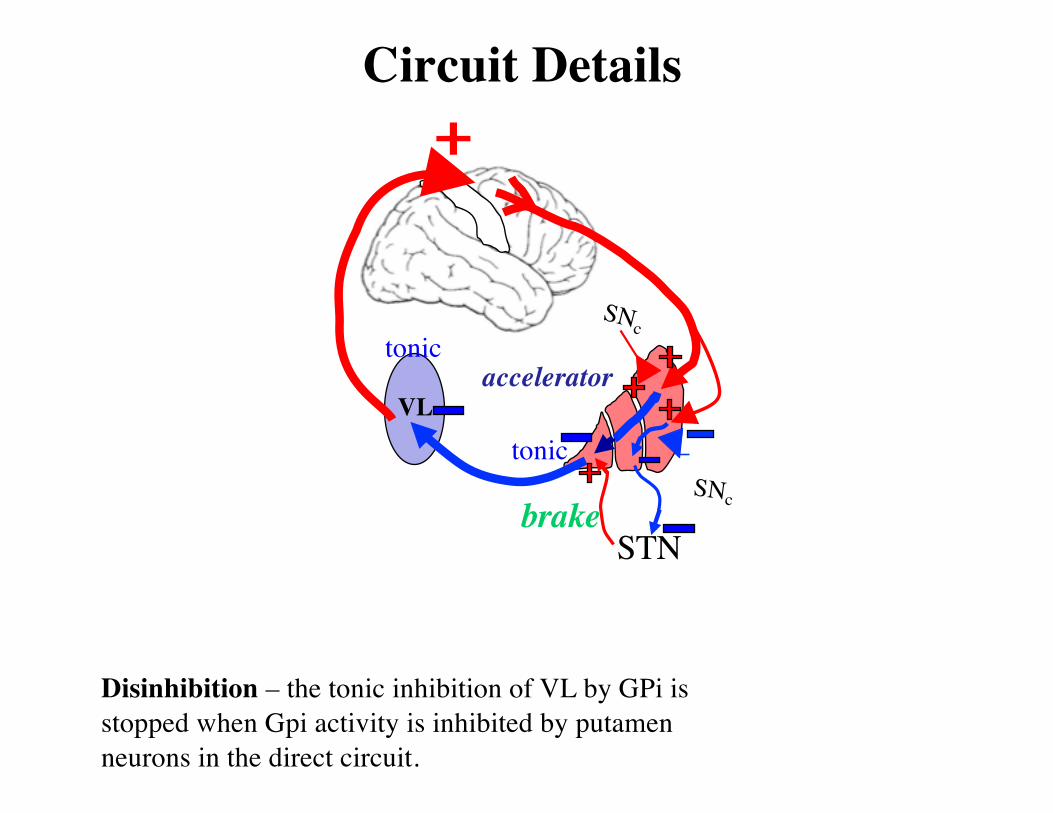
Circuit Details
VL
STN
accelerator
brake
Disinhibition – the tonic inhibition of VL by GPi is stopped when Gpi activity is inhibited by putamen neurons in the direct circuit.
tonic
tonicSNc
SNc
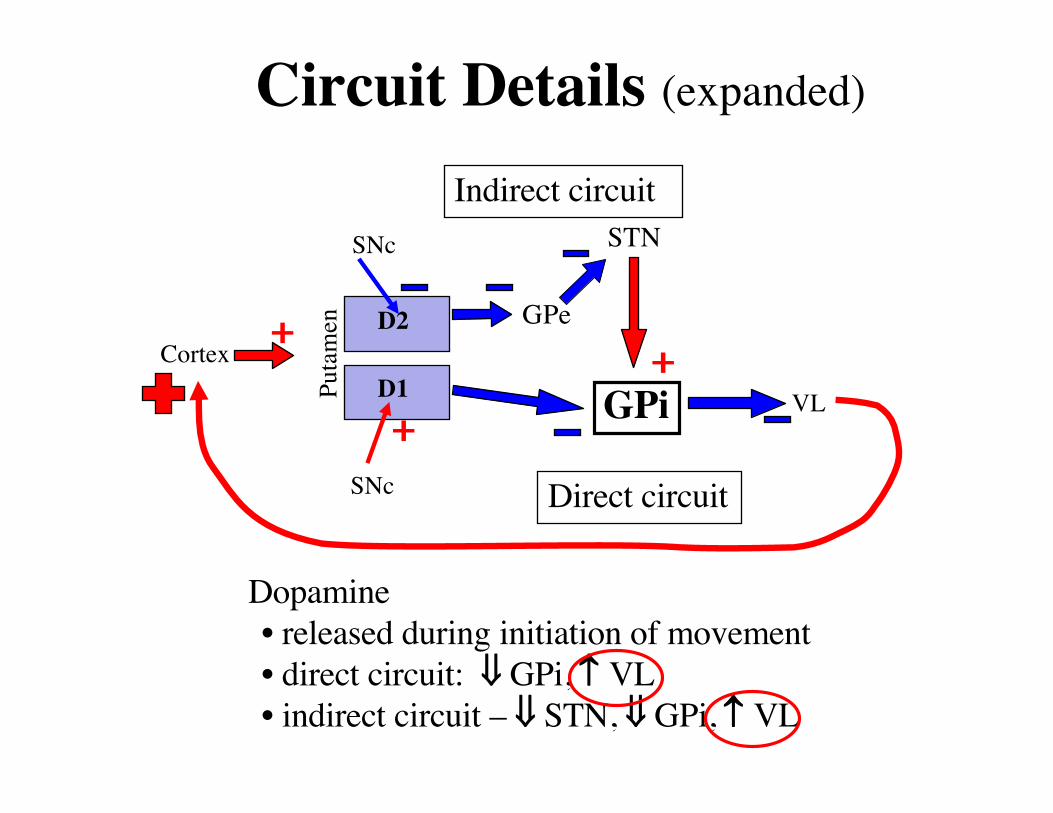
Circuit Details (expanded)
Cortex
VLPutamen
SNc
SNc
GPiD1
D2
STN
GPe
Direct circuit
Indirect circuit
Dopamine • released during initiation of movement• direct circuit: ß GPi, VL • indirect circuit – ß STN, ß GPi, VL
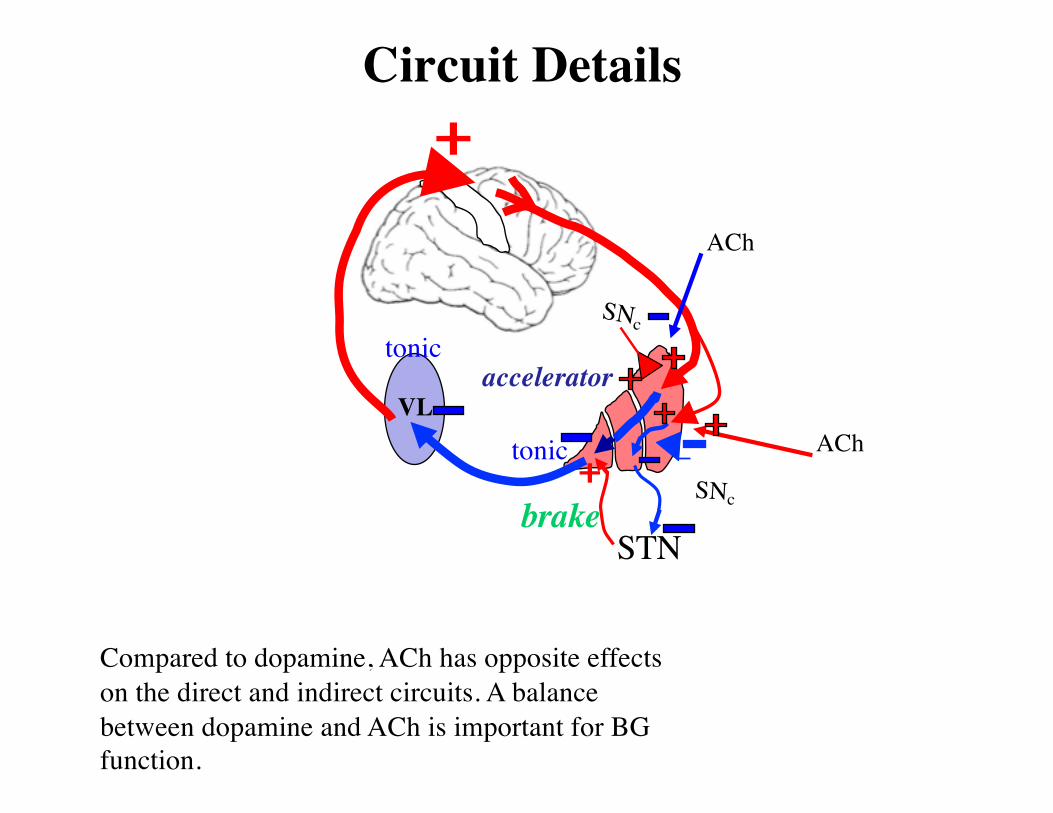
Circuit Details
VL
STN
accelerator
brake
Compared to dopamine, ACh has opposite effects on the direct and indirect circuits. A balance between dopamine and ACh is important for BG function.
tonic
tonicSNc
SNc
ACh
ACh
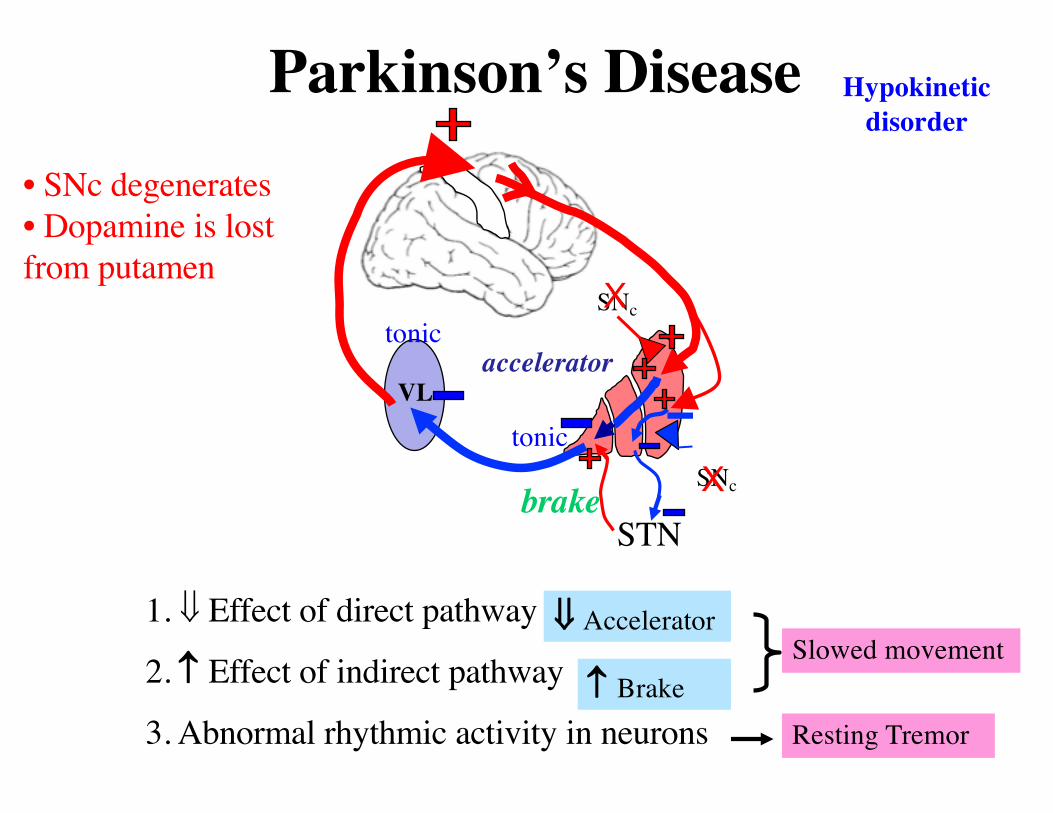
1. ß Effect of direct pathway
2. Effect of indirect pathway
3. Abnormal rhythmic activity in neurons
Parkinson’s Disease
Slowed movement
Resting Tremor
ß Accelerator
Brake
Hypokinetic disorder
VL
STN
accelerator
brake
tonic
tonicSNc
SNc
• SNc degenerates• Dopamine is lost from putamen
X
X
VL
STN
accelerator
brake
tonic
tonicSNc
SNc
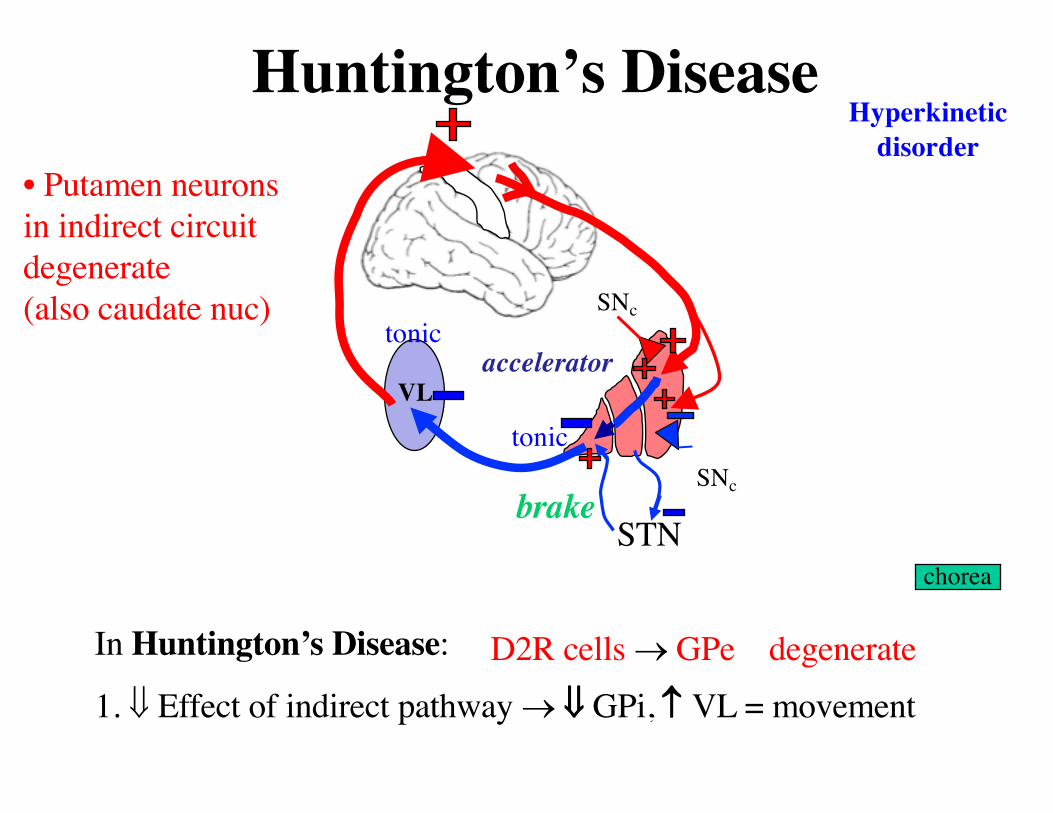
• Putamen neurons in indirect circuit degenerate(also caudate nuc)
Huntington’s Disease
chorea
In Huntington’s Disease:
1. ß Effect of indirect pathway ® ß GPi, VL = movementD2R cells ® GPe degenerate
Hyperkinetic disorder
VLaccelerator
brake
tonic
tonic
STN
SNc
SNc
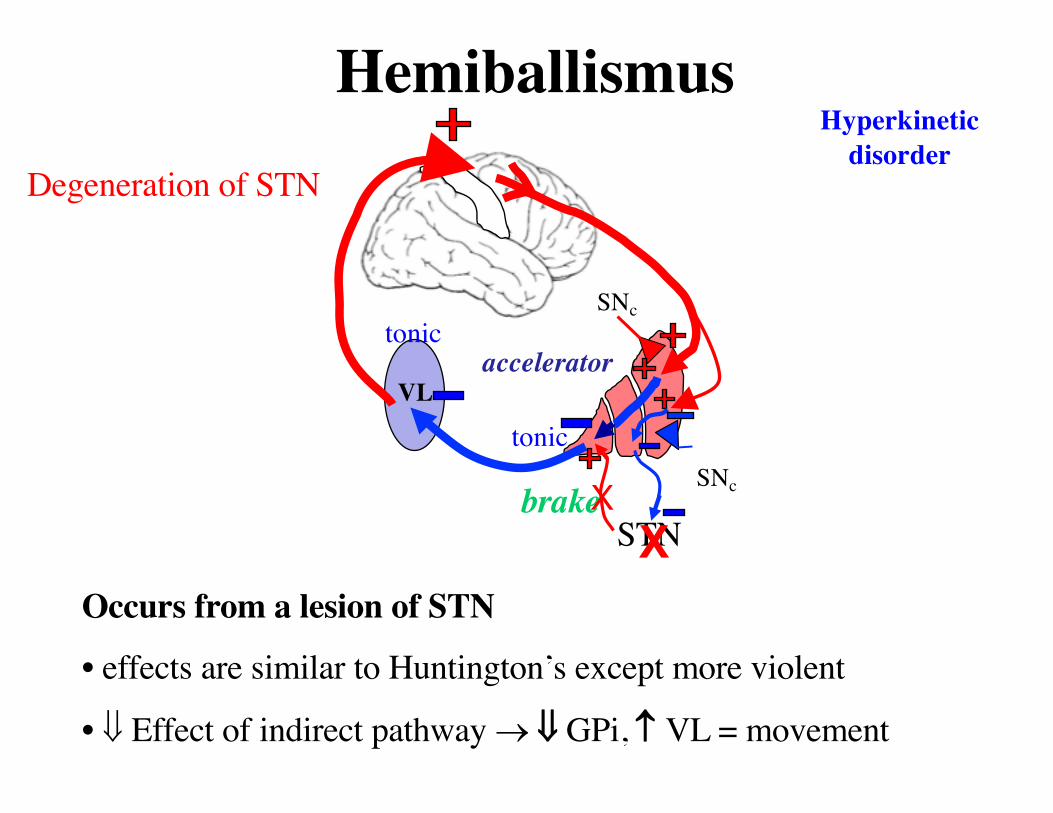
Degeneration of STN
Hemiballismus
Occurs from a lesion of STN
• effects are similar to Huntington’s except more violent
• ß Effect of indirect pathway ® ß GPi, VL = movement
Hyperkinetic disorder
XX
VLaccelerator
brake
tonic
tonic
STN
SNc
SNc
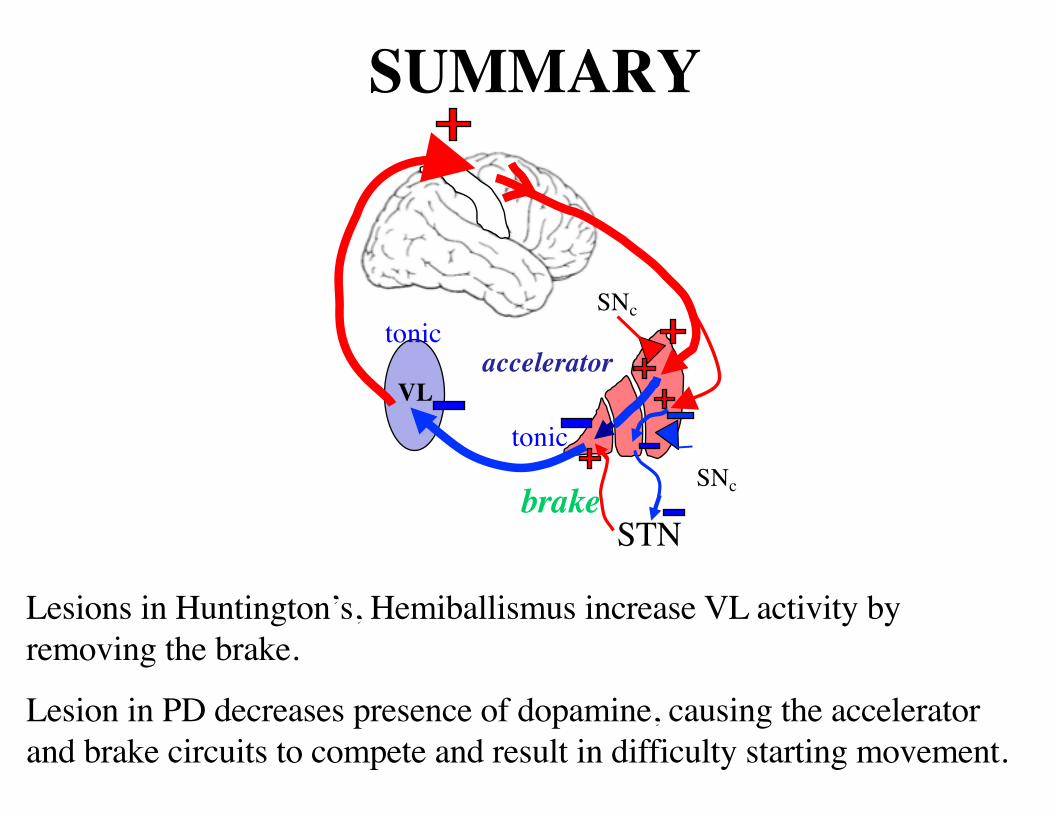
SUMMARY
Lesions in Huntington’s, Hemiballismus increase VL activity by removing the brake.
Lesion in PD decreases presence of dopamine, causing the accelerator and brake circuits to compete and result in difficulty starting movement.
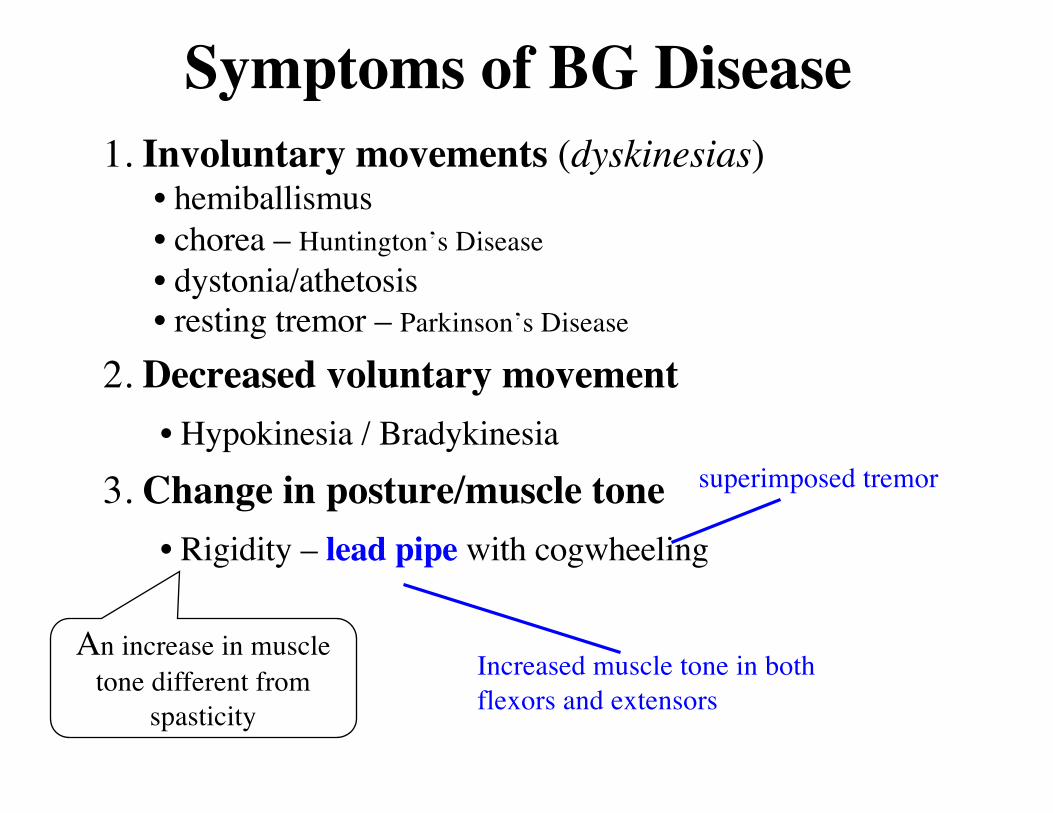
Symptoms of BG Disease1. Involuntary movements (dyskinesias)
• hemiballismus• chorea – Huntington’s Disease• dystonia/athetosis• resting tremor – Parkinson’s Disease
2. Decreased voluntary movement• Hypokinesia / Bradykinesia
3. Change in posture/muscle tone• Rigidity – lead pipe with cogwheeling
An increase in muscletone different from
spasticity
Increased muscle tone in both flexors and extensors
superimposed tremor
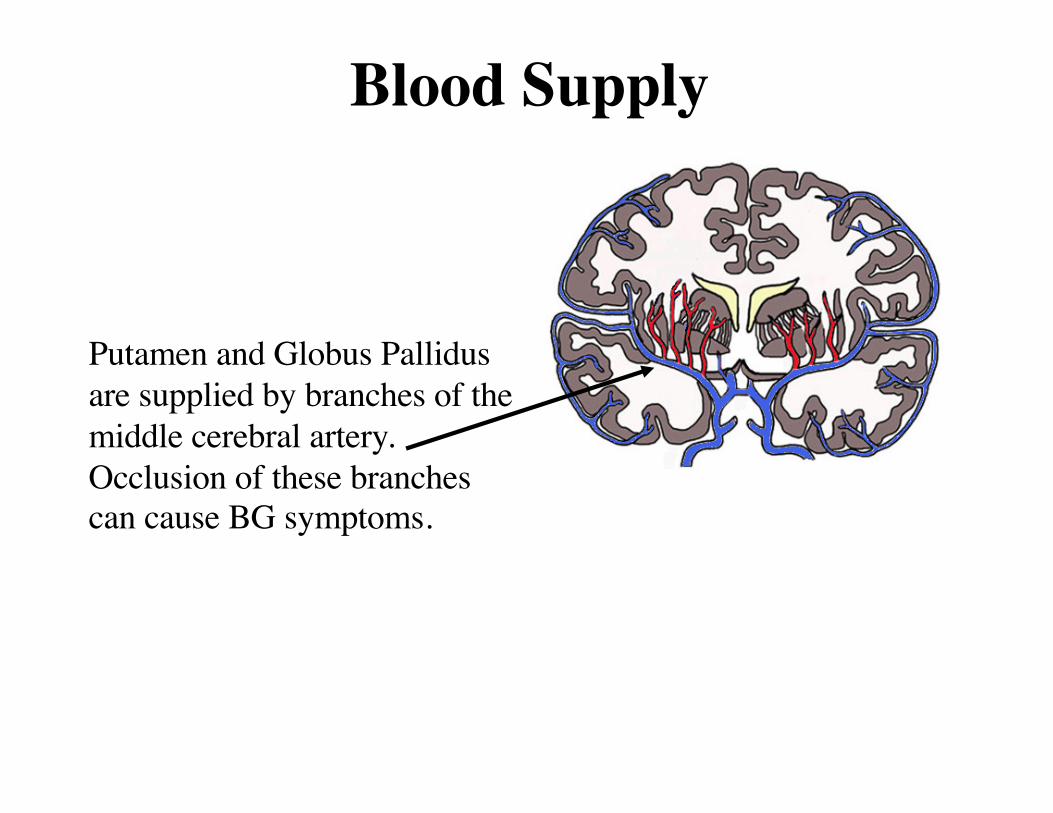
Blood Supply
Putamen and Globus Pallidus are supplied by branches of the middle cerebral artery. Occlusion of these branches can cause BG symptoms.

Basal Ganglia Diseases (movement disorders)Disease Lesion Site Symptoms
Ballism STN Wild,flailing movements
Parkinson’smost common movement disorder
SNc Resting tremor, ßmovement, rigidity, altered gait/posture
Huntington’s• autosomal dominant• adult onset
Putamen D2R neurons/Caudate
Chorea; caudate damage causes personality changes and dementia
Tardive dyskinesia Drug-induced block of D2 and other receptors
(eg antipsychotics)
Facial chorea/athetosis
Tourettes’s unknown Motor and verbal tics
.
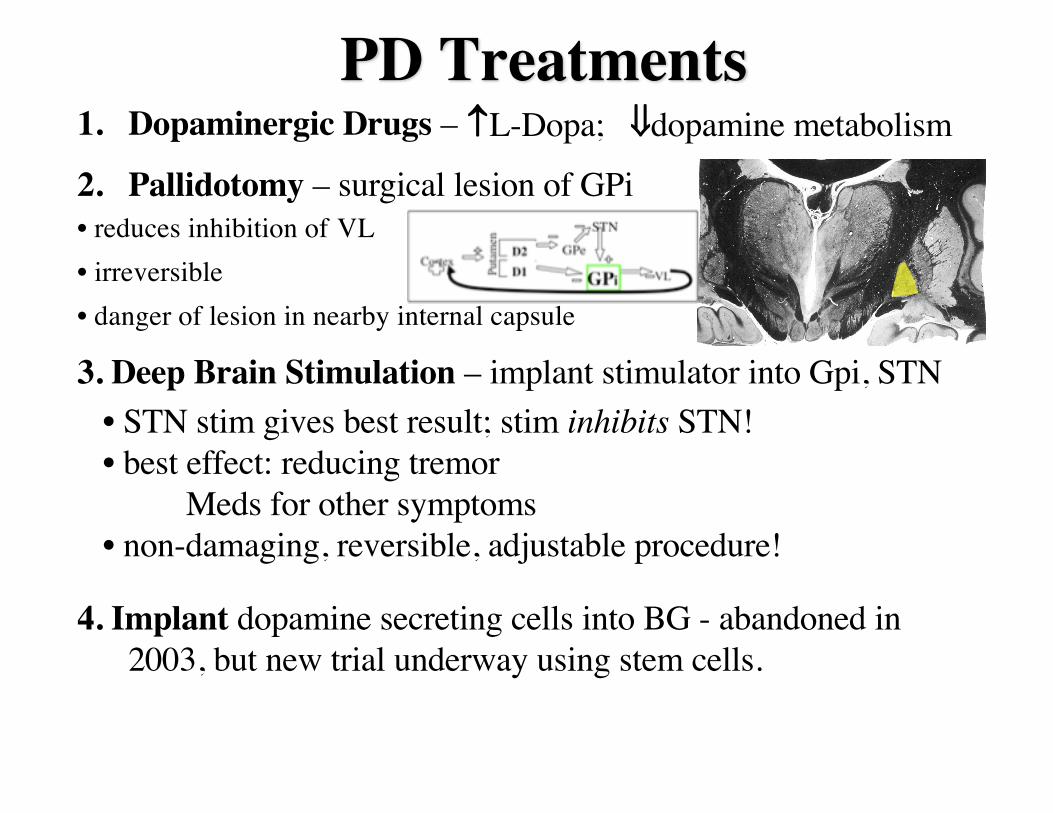
PD Treatments1. Dopaminergic Drugs –
2. Pallidotomy – surgical lesion of GPi• reduces inhibition of VL• irreversible• danger of lesion in nearby internal capsule
3. Deep Brain Stimulation – implant stimulator into Gpi, STN
4. Implant dopamine secreting cells into BG - abandoned in 2003, but new trial underway using stem cells.
L-Dopa; ßdopamine metabolism
• STN stim gives best result; stim inhibits STN!• best effect: reducing tremor
Meds for other symptoms• non-damaging, reversible, adjustable procedure!
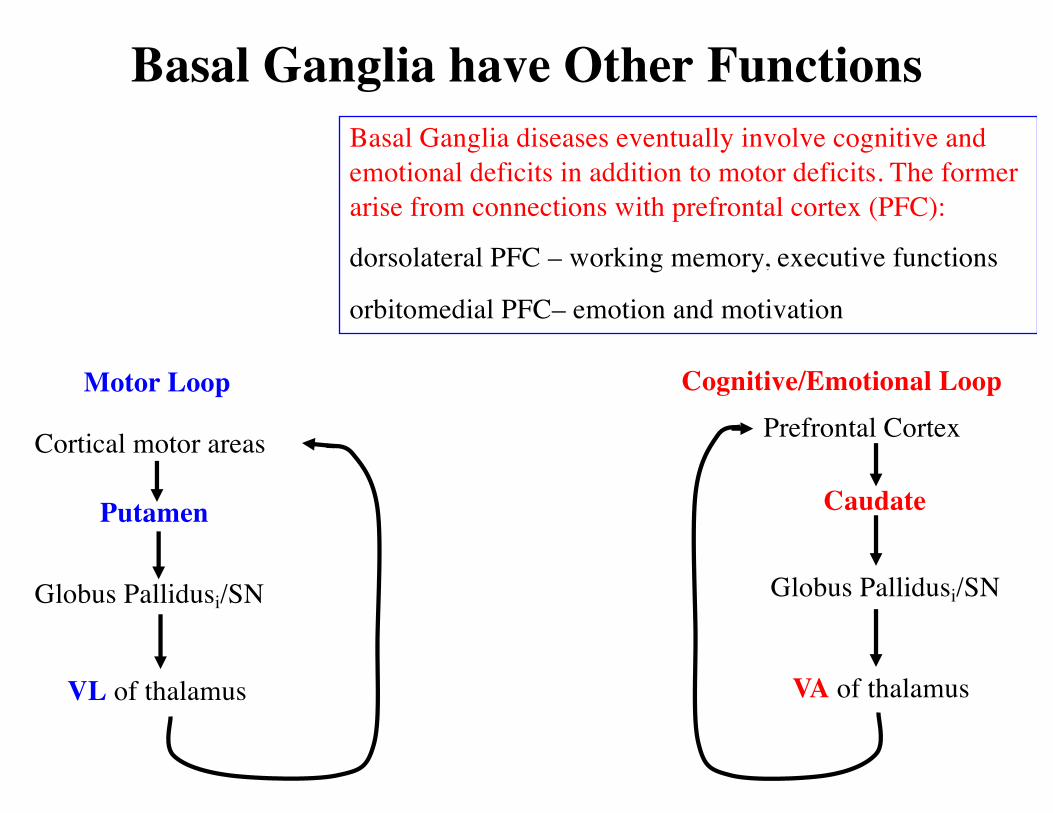
Motor Loop
Cortical motor areas
Globus Pallidusi/SN
VL of thalamus
Putamen
Basal Ganglia have Other Functions
Cognitive/Emotional LoopPrefrontal Cortex
VA of thalamus
Globus Pallidusi/SN
Caudate
Basal Ganglia diseases eventually involve cognitive and emotional deficits in addition to motor deficits. The former arise from connections with prefrontal cortex (PFC):
dorsolateral PFC – working memory, executive functions
orbitomedial PFC– emotion and motivation
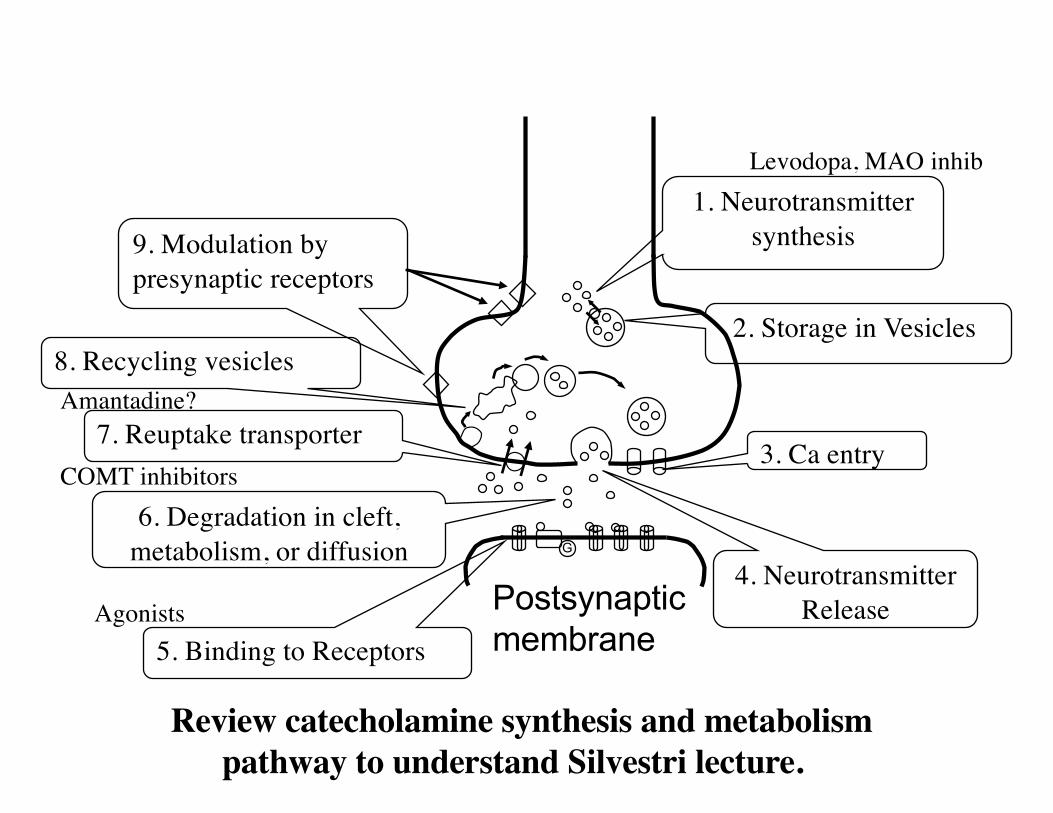
1. Neurotransmitter synthesis
2. Storage in Vesicles
4. Neurotransmitter Release
3. Ca entry
5. Binding to Receptors
6. Degradation in cleft, metabolism, or diffusion
7. Reuptake transporter
9. Modulation by presynaptic receptors
Postsynaptic membrane
G
8. Recycling vesicles
Review catecholamine synthesis and metabolism pathway to understand Silvestri lecture.
Levodopa, MAO inhib
Agonists
COMT inhibitors
Amantadine?