Embed Size (px)
Citation preview

Basal and stimulated gonadotropin levels in the perimenopause
Peter J. Schmidt, MD,a Paul R. Gindoff, MD,b David A. Baron, DO, a and David R. Rubinow, MDb
Bethesda, Maryland, and Washington, D.C.
OBJECTIVE: We investigated whether perimenopausal menstrual cycle irregularity is associated withincreased gonadotropin immunoactivity, bioactivity, or the bioactivity/immunoactivity ratio at baseline andafter short-term stimulation with gonadotropin-releasing hormone.STUDY DESIGN: Subjects consisted of four groups: (1) young regular cycling women (<35 years old),older women (>35 years) with (2) regular or (3) irregular menstrual cycles, and (4) postmenopausalwomen. Gonadotropin-releasing hormone stimulation tests (100 jIg intravenous gonadotropin-releasinghormone) were performed in the National Institute of Mental Health outpatient clinic during the follicularphase of the menstrual cycle or randomly in postmenopausal women.RESULTS: Perimenopausal women had baseline follicle-stimulating hormone and luteinizing hormonelevels and stimulated follicle-stimulating hormone levels (area under the curve) that were similar to thoseof postmenopausal women and significantly greater than those of control (younger and older) women.Postmenopausal women had significantly greater baseline levels of luteinizing hormone bioactivity thandid the other three groups. The bioactivity/immunoactivity ratio in the postmenopausal women wassignificantly greater than those in the perimenopausal and older cycling women, which were similar. Nochange in the bioactivity/immunoactivity ratio was seen after gonadotropin-releasing hormone stimulationin any group.CONCLUSIONS: Although the perimenopause is associated with increases in baseline and stimulatedgonadotropin levels similar to those seen after the menopause, significantly increased baseline luteinizinghormone bioactivity and the bioactivity/immunoactivity ratio are seen only after the menopause. (Am JObstet Gynecol 1996;175:643-50.)
Key words: Perimenopause, gonadotropins, bioactivity
The effects of aging on the hypothalamic-pituitary-ovarian axis include declining reproductive potential,increasing variability of the intermenses interval, decreas-ing ovarian responsivity to stimulation by the gonadotro-pins, and changes in both the quantity and quality ofbasal gonadotropin (follicle-stimulating hormone [FSH]and luteinizing hormone [LH]) secretion.' Decreases infertility appear before any demonstrated abnormality inreproductive endocrine function." 4 Thus, as suggested bySoules et al. (personal communication), reproductive ag-ing may occur in stages characterized initially by subtlechanges in components of the reproductive axis. Theperimenopause is defined as the transition between nor-mal reproductive life and the menopause and has beencharacterized by increases compared with youngerwomen in basal plasma FSH concentrations.4 Increasedbasal FSH levels in the perimenopause are most markedduring the early follicular phase but also appear during
From the Section on Behavioral Endocrinology, Biological PsychiatryBranch, National Institute of Mental Health,' and the Department ofObstetrics and Gynecology, George Washington University.!Received for publication January 30, 1995; revised March 17, 1996;accepted April 17, 1996.Reprint requests: Peter J. Schmidt, MD, National Institute of MentalHealth, Bldg. 10, Room 3N238, 10 Center Dr, MSC 1276, Bethesda,MD 20892-1276.6/1/74255
the midcycle gonadotropin surge and the luteal phase.Increased basal levels of immunoactive LH are less con-
sistently observed during the perimenopause. The in-creases in basal gonadotropin secretion frequently occurin association with ovulatory menstrual cycles; they there-fore do not predict anovulatory menstrual cycles,' nor doanovulatory menstrual cycles exclusively appear duringthe perimenopause.
Qualitative changes in the gonadotropins or changesin the ovarian response to gonadotropin may better re-flect ovarian senescence and the perimenopause than doelevated basal plasma levels of the gonadotropins. In-creases in bioactive LH relative to immunoactive LH havebeen observed consistently during chronic gonadotro-pin-releasing hormone (GnRH) stimulation such as oc-curs after natural or surgically induced menopause. Ad-ditionally, some,6 but not all,7 investigators have observedan increased LH bioactivity/immunoactivity ratio in cy-cling women and in normal males' after short-termGnRH stimulation.
The purpose of this study was to investigate whetherperimenopausal women could be distinguished fromnormal cycling women of comparable age and frommenopausal women on the basis of one or several mea-sures of hypothalamic-pituitary-ovarian axis activity. Spe-cifically, we addressed the following questions. (1) Does
643

September 1996AmJ Obstet Gynecol
bioactive LH increase during the perimenopausal transi-tion? (2) Does stimulated immunoactive LH or bioactiveLH increase during the perimenopausal transition? (3)Are changes in basal or stimulated gonadotropin levelsrelated to age or to menstrual cycle irregularity? We ex-amined plasma levels of the immunoactive gonadotro-pins (FSH and LH) and bioactive LH both at baseline andafter short-term GnRH stimulation in four groups ofwomen as follows: (1) women <35 years old with regularmenstrual cycles, (2) women >35 years old with regularmenstrual cycles, (3) women >35 years old with irregularmenstrual cycles, and (4) menopausal women.
Material and methods
Subject selection. The subjects of this study were 34women who responded to advertisements in the localnewspapers and a hospital newsletter. Normal cyclingyoung women (n= 6) reported regular menstrual cyclefunction of between 25 and 35 days and were <35 yearsold; normal cycling older women (n = 11) reported regu-lar menstrual cycles but were >35 years old; perimeno-pausal women (n =11) reported irregular menstrualcycles of either <21 days or >35 days for the previous 6months to 1 year and were >35 years old; postmenopausalwomen (n= 6) reported the absence of menses for >6months and had serial plasma FSH levels >40 IU/L. Men-strual cycle histories in all groups were confirmed bymenstrual cycle diaries for 2 months. None of thewomen were taking psychotropic medications, oral con-traceptives, or any other form of hormonal therapy. Nonehad any current medical illness, including thyroid dys-function, or illness within the previous year or any axis Ipsychiatric illness within the previous 2 years, as deter-mined by the administration of a semistructured diagnos-tic interview, the Modified Schedule for Affective Disor-ders and Schizophrenia-Lifetime. 9
The protocol was approved by both the National Insti-tute of Mental Health and George Washington UniversityResearch Review Subpanels. Before the study, written in-formed consent was obtained from all subjects for theirparticipation in a study investigating changes in ovarianfunction during the perimenopause. All subjects werepaid for their participation in this protocol.
Protocol. GnRH stimulation tests were performed dur-ing the follicular phase of the menstrual cycle (days 4 to8) or randomly in the postmenopausal women. TheGnRH stimulation test was performed as follows. Subjectswere admitted to the National Institute of Mental Healthoutpatient clinic. After venipuncture and a 20-minuteperiod of bed rest, two baseline blood samples weredrawn 15 minutes apart. A 100 pg bolus of syntheticGnRH (gonadorelin) (Factrel, Wyeth-Ayerst, Philadel-phia) was administered intravenously over 30 to 45 sec-onds. Blood samples were obtained at 15-minute intervalsfor 1 hour and at 90 minutes after GnRH. Blood samples
for radioimmunoassay were collected in heparinized glasstubes, and samples for bioassay were collected in additive-free glass tubes. All samples were placed on ice immedi-ately, allowed to congeal, and centrifuged at -40 C; ali-quots were then frozen at -70 ° C until assay.
Assays. Immunoactive FSH and LH were analyzed withspecific double-antibody radioimmunoassays for humanFSH and LH by use of antiserum prepared in rabbitagainst highly purified human FSH or human chorionicgonadotropin and iodine 125-labeled FSH or LH radio-ligands, respectively.10' 1 All samples were analyzed induplicate. The intraassay coefficients of variation for thehigh and low regions of the standard curve for immuno-active FSH were 2.7% and 4.9%, respectively, and forimmunoactive LH 1.4% and 2.6%, respectively.
The interassay coefficients of variation for the high andlow regions of the standard curve for immunoactive FSHwere 4.0% and 5.5%, respectively, and for immunoactiveLH were 5.3% and 5.6%, respectively. Cross-reactivitywith the free c subunit of human chorionic gonadotro-pin was approximately 0.8%. All measures of immunoac-tive LH were quantitated relative to the first internationalreference preparation.
Serum bioactive LH was analyzed by the rat interstitialcell testosterone bioassay as described previously.l2 Threedilutions were prepared for each sample, and all testos-terone samples were run in duplicate. Measures of bioac-tive LH were calculated relative to the second interna-tional reference preparation. One milligram of LER 907was equivalent to 99 IUs. To make measures of immuno-reactive and bioactive LH compatible, the values ob-tained for bioactive LH were divided by a conversionfactor of 2.5 that adjusted for differences in referencepreparation. (The first international reference prepara-tion is 2.5 times more potent than the second; thus mea-sures of bioactive LH were expressed relative to the firstinternational reference preparation.) The slopes of thestandard displacement curves were similar, and thereforethe conversion factor was consistent over the range of thestandard curve used in this study. The intraassay coeffi-cient of variation was 16% ± 8.6%. Duplicate samplesshowing >20% coefficient of variation were repeated.
Single baseline (time -20 minutes) measures of estra-diol, dehydroepiandrosterone (DHEA), and testosteronewere measured by radioimmunoassay as described previ-ously. s 6 The intraassay coefficients of variation for thehigh and low regions of the standard curve were asfollows: estradiol 6.1% and 7.2%, respectively; DHEA7.4% and 9.3%, respectively; and testosterone 8.9% and6.6%, respectively. The interassay coefficients of variationfor the high and low regions of the standard curve werewas as follows: estradiol 8.1% and 13.5%, respectively;DHEA 14% and 15%, respectively; and testosterone16.6% and 15.0%, respectively.
Statistical analysis. Basal levels of immunoactive FSH
644 Schmidt et al.

Schmidt et al. 645Volume 175, Number 3, Part 1AmJ Obstet Gynecol
and LH, bioactive LH and the bioactive LH to immuno-
active LH ratio at baseline were compared by analysis ofvariance with group as the independent variable. Areasunder the curve for immunoactive FSH and LH and
bioactive LH were time integrated and normalized forbaseline values (trapezoidal integration method) andcompared by analysis of variance with group as the inde-
pendent variable. The LH bioactive/immunoactive ratioafter GnRH stimulation was analyzed by analysis of vari-ance with repeated measures with group as the between-subjects factor and time as the within-subjects factor. Posthoc comparisons between groups were performed withthe Bonferroni t test.
Levels of bioactive LH and the LH bioactive/immuno-active ratio after GnRH stimulation were correlated withbaseline levels of estradiol, DHEA, and testosterone byPearson product-moment correlations.
Normal cycling women and postmenopausal womenhad immunoactive and bioactive LH levels that were not
normally distributed, and the area under the curve datawere therefore log transformed for both immunoactiveand bioactive LH and reanalyzed by analysis of variancewith group as the independent variable.
One postmenopausal subject had LH levels that wereinconsistent with the menopause (i.e., levels <30 IU/L),and the analysis was repeated with this subject excluded.
Results
Subject characteristics. The mean (SD) ages for thesubjects were as follows: normal cycling young women28 + 3 years (range 25 to 32 years), normal cycling olderwomen 41 + 4 years (range 36 to 48 years), perimeno-pausal women 46 4 years (range 37 to 52 years), andpostmenopausal women 52 + 2 years (range 49 to 55
years). The GnRH stimulation test was performed duringthe early to midfollicular phase in menstruating women
(young, older, perimenopausal) (mean menstrual cycleday of testing 6 + 1, day 6 + 1, day 5 ± 1, respectively) andrandomly in the postmenopausal women. Self-reports ofmenstrual cycle lengths ranged in subjects as follows:normal cycling young 27 to 30 days, normal cycling older
25 to 30 days, and perimenopausal 10 to 90 days. Allpostmenopausal women reported a period of amenor-rhea 6 months and ranged between subjects from 6months to 3 years. Four of the six normal cycling youngwomen had never been pregnant compared with threenormal cycling older women, two perimenopausalwomen, and none of the postmenopausal women. Persis-tent hot flushes were reported by none of the normalcycling young women, one normal cycling older woman,four perimenopausal women, and two postmenopausalwomen.
Hormone measures. None of the normal cyclingwomen (young or older) had baseline immunoactive FSHlevels >20 IU/L, whereas nine of the perimenopausal
women and all the postmenopausal women (by defini-
tion) had baseline FSH levels >20 IU/L. ImmunoactiveFSH levels were maximal at 45 minutes after GnRH infu-sion and were <40 in all normal cycling women (youngand older) and one perimenopausal woman, who alsohad basal immunoactive FSH levels <20 IU/L. The otherperimenopausal woman with baseline FSH levels <20
IU/L had a maximal immunoactive FSH level >40 IU/L,consistent with the other perimenopausal and postmeno-pausal women.
Analysis of variance demonstrated a significant effect ofgroup on baseline, area under the curve, maximumstimulated value, and the maximum stimulated value cor-rected for baseline (A max) for measures of immunoac-tive FSH and LH and bioactive LH. Additionally, analysis
of variance showed a significant effect of group in thecomparisons of the log-transformed area under the curvevalues for immunoactive and bioactive LH. There was nosignificant effect for the time taken to achieve the maxi-mum stimulated value after GnRH infusion in immuno-active FSH and LH and bioactive LH. Post hoc compari-sons of the significant between-group effects demon-strated the following results (Table I).
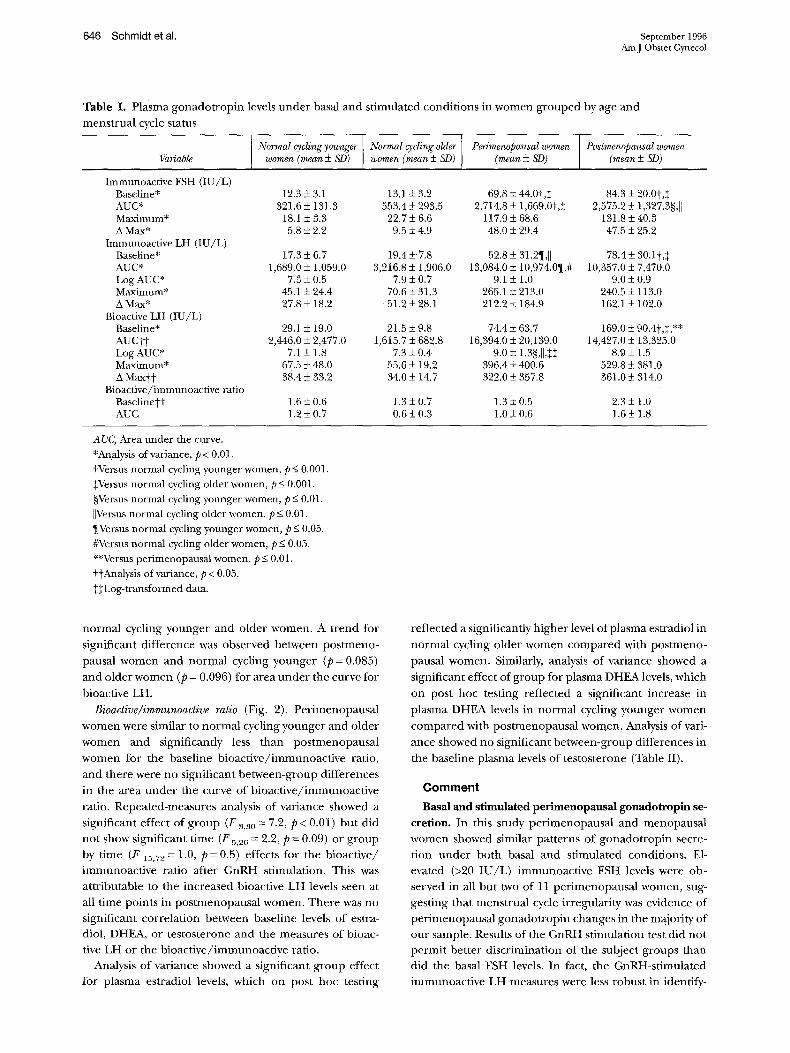
Immunoactive FSH (Fig. 1, Table I). Postmenopausalwomen were similar to perimenopausal women and both
were significantly greater than normal cycling youngwomen and normal cycling older women for baselineFSH and area under the FSH curve.
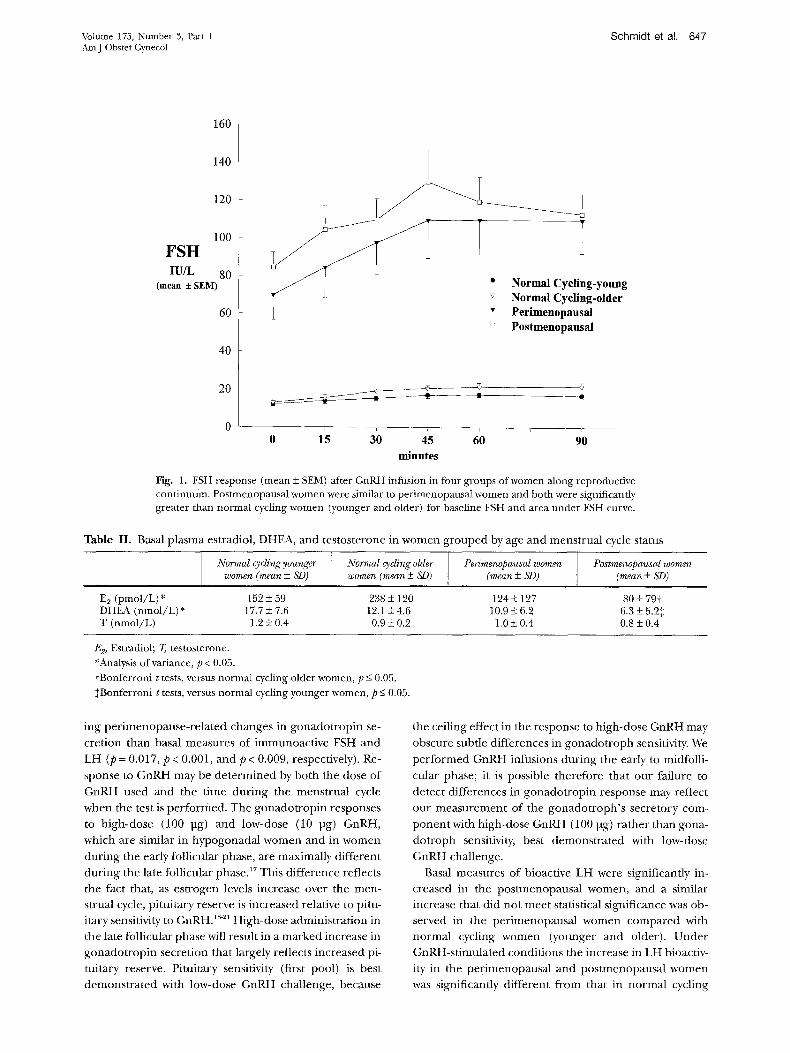
Immunoactive LH (Fig. 2, Table I). Postmenopausalwomen were similar to perimenopausal women and bothwere significantly greater than normal cycling youngwomen and normal cycling older women for baselineimmunoactive LH. Perimenopausal women were signifi-cantly greater than normal cycling young women andnormal cycling older women for area under the curve forimmunoactive LH; postmenopausal women did not differfrom normal cycling women (younger and older) or peri-menopausal women. Log transformation of the nonnor-mally distributed area under the curve immunoactive LHdata again showed perimenopausal women greater thannormal cycling women (younger and older); postmeno-pausal women were significantly greater than normal cy-cling younger women with a trend to be significantlygreater than normal cycling older women (p = 0.08).
Bioactive LH (Fig. 2, Table I). Postmenopausal womenwere significantly greater than the other three groups(younger, older, perimenopausal) for baseline bioactiveLH. Analysis of variance showed a significant group effectfor area under the curve for bioactive LH that on posthoc testing reflected a trend (p = 0.07) for an increasedresponse in perimenopausal women compared with nor-mal cycling older women. Log transformation of the non-normally distributed area under the curve bioactive LHdata showed perimenopausal women to be similar topostmenopausal women and significantly greater than
646 Schmidt et al. September 1996AmJ Obstet Gynecol
Table I. Plasma gonadotropin levels under basal and stimulated conditions in women grouped by age andmenstrual cycle status
Normal cyclingyounger Normal cyclingolder Penmenopausal women Postmenopausal womenVariable women (mean ± SD) women (mean + SD) (mean ± SD) (mean ± SD)
Immunoactive FSH (IU/L)Baseline* 12.3 ± 3.1 13.1 ± 3.2 69.8 ± 44.0t,1+ 84.3 ± 20.0t,+AUC* 321.6 ± 131.3 553.4 + 293.5 2,714.8 ± 1,669.0t,+ 2,575.2 ± 1,327.3§,|lMaximum* 18.1 ± 3.3 22.7 ± 6.6 117.9 ± 68.6 131.8 ± 40.3A Max* 5.8 ± 2.2 9.5 ± 4.9 48.0 ± 29.4 47.5 ± 25.2
Immunoactive LH (IU/L)Baseline* 17.3 ± 6.7 19.4 ±+7.8 52.8 ± 31.21,,l 78.4 ± 30.1t,TAUC* 1,689.0 + 1,059.0 3,216.8 ± 1,906.0 13,084.0 + 10,974.0¶,# 10,357.0 + 7,470.0Log AUC* 7.3 + 0.5 7.9 ± 0.7 9.1 ± 1.0 9.0 ± 0.9Maximum* 45.1 ± 24.4 70.6 ± 31.3 265.1 ± 213.0 240.5 ± 113.0A Max* 27.8 ± 18.2 51.2 ± 28.1 212.2 + 184.9 162.1 ± 102.0
Bioactive LH (IU/L)Baseline* 29.1 ± 19.0 21.5 ± 9.8 74.4 ± 63.7 169.0 ± 90.4t,+,**AUCti 2,446.0 ± 2,477.0 1,615.7 ± 682.8 16,394.0 + 20,139.0 14,427.0 ± 13,325.0Log AUC* 7.1 ± 1.8 7.3 ± 0.4 9.0 ± 1.3§,I ,++ 8.9 + 1.5Maximum* 67.5 ± 48.0 55.6 ± 19.2 396.4 ± 400.6 529.8 ± 381.0A Maxtt 38.4 ± 33.2 34.0 ± 14.7 322.0 ± 357.8 361.0 ± 314.0
Bioactive/immunoactive ratioBaselinett 1.6 ± 0.6 1.3 ± 0.7 1.3 ± 0.5 2.3 ± 1.0AUC 1.2 ± 0.7 0.6 ± 0.3 1.0 ± 0.6 1.6 +± 1.8
AUC, Area under the curve.
*Analysis of variance, p < 0.01.
tVersus normal cycling younger women, p < 0.001.+Versus normal cycling older women, p < 0.001.§Versus normal cycling younger women, p < 0.01.
IlVersus normal cycling older women, p < 0.01.[Versus normal cycling younger women, p < 0.05.
#Versus normal cycling older women, p < 0.05.**Versus perimenopausal women, p 0.01.ttAnalysis of variance, p < 0.05.+Log-transformed data.
normal cycling younger and older women. A trend forsignificant difference was observed between postmeno-pausal women and normal cycling younger (p = 0.085)and older women (p = 0.096) for area under the curve forbioactive LH.
Bioactive/immunoactive ratio (Fig. 2). Perimenopausal
women were similar to normal cycling younger and olderwomen and significantly less than postmenopausalwomen for the baseline bioactive/immunoactive ratio,and there were no significant between-group differencesin the area under the curve of bioactive/immunoactiveratio. Repeated-measures analysis of variance showed asignificant effect of group (F 3,30
= 7.2, p < 0.01) but didnot show significant time (F 5,26 = 2.2, p = 0.09) or groupby time (F 15,72 = 1.0, p= 0.5) effects for the bioactive/immunoactive ratio after GnRH stimulation. This wasattributable to the increased bioactive LH levels seen atall time points in postmenopausal women. There was nosignificant correlation between baseline levels of estra-diol, DHEA, or testosterone and the measures of bioac-tive LH or the bioactive/immunoactive ratio.
Analysis of variance showed a significant group effectfor plasma estradiol levels, which on post hoc testing
reflected a significantly higher level of plasma estradiol innormal cycling older women compared with postmeno-pausal women. Similarly, analysis of variance showed asignificant effect of group for plasma DHEA levels, whichon post hoc testing reflected a significant increase inplasma DHEA levels in normal cycling younger womencompared with postmenopausal women. Analysis of vari-ance showed no significant between-group differences inthe baseline plasma levels of testosterone (Table II).
Comment
Basal and stimulated perimenopausal gonadotropin se-cretion. In this study perimenopausal and menopausalwomen showed similar patterns of gonadotropin secre-tion under both basal and stimulated conditions. El-evated (>20 IU/L) immunoactive FSH levels were ob-served in all but two of 11 perimenopausal women, sug-gesting that menstrual cycle irregularity was evidence ofperimenopausal gonadotropin changes in the majority ofour sample. Results of the GnRH stimulation test did notpermit better discrimination of the subject groups thandid the basal FSH levels. In fact, the GnRH-stimulatedimmunoactive LH measures were less robust in identify-
Volume 175, Number 3, Part 1AmJ Obstet Gynecol
160
140
120
100FSHIU/L 80
(mean ±+ SEM)
60
40
20
0
Schmidt et al. 647
Ig-youngig-olderal
: Postmenopausal
p_ pI
0 15 30 45minutes
60 90
Fig. 1. FSH response (mean ± SEM) after GnRH infusion in four groups of women along reproductivecontinuum. Postmenopausal women were similar to perimenopausal women and both were significantlygreater than normal cycling women (younger and older) for baseline FSH and area under FSH curve.
Table II. Basal plasma estradiol, DHEA, and testosterone in women grouped by age and menstrual cycle status
Normal cycling younger Normal cycling older Perimenopausal women Postmenopausal womenwomen (mean ± SD) women (mean ± SD) (mean + SD) (mean + SD)
E2 (pmol/L)* 152 + 59 238 + 120 124 + 127 80 + 79tDHEA (nmol/L)* 17.7 ± 7.6 12.1 ± 4.6 10.9 ± 6.2 6.3 ± 5.2+T (nmol/L) 1.2 ± 0.4 0.9 + 0.2 1.0 ±+ 0.4 0.8 + 0.4
E2, Estradiol; T testosterone.*Analysis of variance, p < 0.05.tBonferroni t tests, versus normal cycling older women, p < 0.05.+Bonferroni t tests, versus normal cycling younger women, p < 0.05.
ing perimenopause-related changes in gonadotropin se-cretion than basal measures of immunoactive FSH andLH (p = 0.017, p < 0.001, and p < 0.009, respectively). Re-sponse to GnRH may be determined by both the dose ofGnRH used and the time during the menstrual cyclewhen the test is performed. The gonadotropin responsesto high-dose (100 pg) and low-dose (10 pg) GnRH,which are similar in hypogonadal women and in womenduring the early follicular phase, are maximally differentduring the late follicular phase."7 This difference reflectsthe fact that, as estrogen levels increase over the men-strual cycle, pituitary reserve is increased relative to pitu-itary sensitivity to GnRH. 8- 2' High-dose administration inthe late follicular phase will result in a marked increase ingonadotropin secretion that largely reflects increased pi-tuitary reserve. Pituitary sensitivity (first pool) is bestdemonstrated with low-dose GnRH challenge, because
the ceiling effect in the response to high-dose GnRH mayobscure subtle differences in gonadotroph sensitivity. Weperformed GnRH infusions during the early to midfolli-cular phase; it is possible therefore that our failure todetect differences in gonadotropin response may reflectour measurement of the gonadotroph's secretory com-ponent with high-dose GnRH (100 pg) rather than gona-dotroph sensitivity, best demonstrated with low-doseGnRH challenge.
Basal measures of bioactive LH were significantly in-creased in the postmenopausal women, and a similarincrease that did not meet statistical significance was ob-served in the perimenopausal women compared withnormal cycling women (younger and older). UnderGnRH-stimulated conditions the increase in LH bioactiv-ity in the perimenopausal and postmenopausal womenwas significantly different from that in normal cycling
T .,
648 Schmidt et al.
6UU
500
400
LH-BIOACIIVEI/L 300
(mean ± SEM)200
100
0
September 1996AmJ Obstet Gynecol
* Normal Cycling-youngV Normal Cyclin-older
3uU
250
200
Lfl-IMMUNOACTIVEIUL 150
(mean SEM)100
50
03.0
2.5
2.0LH B:I Ratio
1.5(mean SEM)
1.0
0.5
0.0
0 15 30 45 60 90
minutes * Normal Cvelin-voun
0 15 30 45
minutes
60
der
90
Fig. 2. Response (mean ± SEM) of immunoactive and bioactive LH and LH bioactive/immunoactiveratio to GnRH infusion in four groups of women along reproductive continuum. Immunoactive LH:Postmenopausal women were similar to perimenopausal women and both were significantly greater thannormal cycling women (younger and older) for baseline immunoactive LH. Perimenopausal womenwere significantly greater than normal cycling women (younger and older) for area under curve ofimmunoactive LH. Bioactive LH: Postmenopausal women were significantly greater than other women(younger, older, perimenopausal) for baseline bioactive LH. Bioactive/immunoactive ratio: Perimeno-pausal women were similar to normal cycling women (younger and older) and significantly less thanpostmenopausal women for baseline bioactive/immunoactive ratio. Repeated-measures analysis of vari-ance showed a significant effect of group that reflected increased bioactive LH levels seen at all timepoints in postmenopausal women. There were no significant time or group by time effects for bioac-tive/immunoactive ratio after short-term GnRH stimulation.
women (younger and older). The area under the bioac-tive LH curve was significantly greater in perimenopausalwomen compared with normal cycling women (younger
and older); however, postmenopausal women were notfound to be statistically different from normal cycling
women because of the presence of outlier values of bio-active LH secretion in both groups (younger and post-menopausal).
Thus, during the selection of subjects for studies on theperimenopause, hormonal measures such as plasma FSHlevels >20 IU/L may permit the selection of endocrino-logically homogeneous groups. However, in some womenwith menstrual cycle irregularity who have FSH levels <20
IU/L, our data suggest that GnRH-stimulated levels ofFSH and bioactive LH may be increased to levels seen inperimenopausal women with elevated baseline gonado-tropins.
Differences in bioactive/immunoactive ratio. Previousstudies have identified an increase in bioactive LH22 andthe LH bioactive/immunoactive ratio in menopausalwomen,6 , 12 men, 6 8, 12 and women with polycystic ovarysyndrome7 relative to normal cycling women. Addition-ally, some6 but not all studies7 have observed increases inthe bioactive/immunoactive ratio after short-term GnRHstimulation in regularly cycling women during the latefollicular phase of the menstrual cycle. The bioac-
l l l
I
---r
_
---
L

Schmidt et al. 649Volume 175, Number 3, Part 1AmJ Obstet Gynecol
tive/immunoactive ratio did not increase significantly inany of our four groups after short-term GnRH stimula-
tion. This finding is consistent with studies by Dufau etal.,6, 12 who also observed the lack of an increase in the
bioactive/immunoactive ratio after short-term GnRHstimulation in women during the early follicular phase orin postmenopausal women. In fact, we observed a nonsig-nificant decrease in the ratio from baseline to the +15-minute time point, reflecting a relatively greater increasein the secretion of immunoactive LH compared withbioactive LH after GnRH stimulation. Thus our data sug-gest that the LH bioactive/immunoactive ratio is in-creased only under conditions of long-term GnRH stimu-lation, such as during the postmenopause. The basal andstimulated LH bioactive/immunoactive ratios were notsignificantly increased during the perimenopause butwere significantly elevated in the postmenopausal womencompared with the other three groups. Nevertheless,stimulated bioactive LH secretion was identified to beincreased during the perimenopause, but it was propor-tionate to increases in immunoactive LH; the overallstimulated bioactive/immunoactive ratio of LH wastherefore unchanged. Thus the increased secretion ofbioactive LH was not reflective of a selective physiologicchange, as has been identified in postmenopausalwomen.
Several explanations have been proposed to explainthe relative increase of bioactive LH secretion23: (1)Changes in gonadal steroid levels may alter the produc-tion rates of bioactive LH compared with immunoactiveLH; (2) the clearance rates of bioactive or immunoactiveLH may be altered in postmenopausal women. In spite ofthe significantly increased bioactive/immunoactive ratioin postmenopausal women compared with all three othergroups, significantly lower baseline hormone levels wereseen in the postmenopausal group in only twocomparisons: lower estrogen levels than in older normalcycling women and lower DHEA levels than in youngernormal cycling women. Further, we observed no signifi-cant correlation between baseline levels of estradiol,DHEA, or testosterone and the measures of bioactive LHor the bioactive/immunoactive ratio. Consistent withother reports,2 4 therefore differences in basal estradiol,DHEA, and testosterone levels do not appear sufficient toexplain the observed increase in the LH bioactive/immu-noactive ratio in postmenopausal women.
Our definition of postmenopausal women (i.e., >6months of amenorrhea) entails the risk of misidentifyinga perimenopausal women as postmenopausal, thus po-tentially obscuring between-group differences. However,even a definition of >1 year of amenorrhea does notimmunize against this possibility, because the one post-menopausal women with LH levels inconsistent with themenopause had a history of >1 year of amenorrhea.Given our relatively small sample size, we additionallycannot rule out a type II error and the possible demon-stration of other group discriminators with a larger
sample. Nonetheless, our data do suggest that for identi-fying perimenopausal women for study, basal FSH dis-criminates perimenopausal from preperimenopausalwomen better than any other basal or stimulated mea-sure, with GnRH stimulation possibly permitting furtherdiscriminating power in older subjects with irregularmenses but basal FSH levels within the normal range.
REFERENCES
1. Gindoff PR, Jewelewicz R. Reproductive potential in theolder woman. Fertil Steril 1986;46:989-1001.
2. Cecos Federation, Schwartz D, Mayaux MJ. Female fecundityas a function of age: results of artificial insemination in 2193nulliparous women with azoospermic husbands. N Engl JMed 1982;306:404-6.
3. Romeu A, Muasher SJ, Acosta AA, Veeck LL, Diaz J, JonesGS, et al. Results of in vitro fertilization attempts in women40 years of age and older: the Norfolk experience. FertilSteril 1987;47:130-6.
4. Burger HG, Dudley EC, Hopper JL, Shelley JM, Green A,Smith A, et al. The endocrinology of the menopausaltransition: a cross-sectional study of a population-basedsample.J Clin Endocrinol Metab 1995;80:3537-45.
5. Reyes FI, WinterJSD, Faiman C. Pituitary-ovarian relation-ships preceding the menopause. AmJ Obstet Gynecol 1977;129:557-64.
6. Dufau ML, Beitins IZ, McArthur JW, Catt KJ. Effects ofluteinizing hormone releasing hormone (LHRH) upon bio-active and immunoreactive serum LH levels in normal sub-jects. J Clin Endocrinol Metab 1976;43:658-67.
7. Ding Y, Anttila L, Ruutiainen K, Erkkola R, Irjala K, Huht-aniemi I. Neither exogenous nor endogenous GnRH stimu-lation alters the bio/immuno ratio of serum LH in healthywomen and in polycystic ovarian disease. Acta Obstet Gy-necol Scand 1991;70:211-7.
8. VeldhuisJD,Johnson ML, Dufau ML. Preferential release ofbioactive luteinizing hormone in response to endogenousand low dose exogenous gonadotropin-releasing hormonepulses in man.J Clin Endocrinol Metab 1987;64:1275-82.
9. Spitzer RL, EndicottJ. Schedule for affective disorders andschizophrenia-lifetime version. New York: Biometrics Re-search Department, New York State Psychiatric Institute,1975.
10. Odell WD, Rayford PL, Ross GT. Simple partially automatedmethod for radioimmunoassay of human thyroid stimulat-ing, growth, luteinizing and follicle stimulating hormone.J Lab Clin Med 1967;70:973-80.
11. Odell WD, Ross GT, Rayford PL. Radioimmunoassay of hu-man luteinizing hormone. Metab Clin Exp 1966;15:287-9.
12. Dufau ML, Pock R, Newbaner A, Catt KJ. In vitro bioassay ofLH in human serum: the rat interstitial cell testosterone(RICT) assay. J Clin Endocrinol Metab 1976;42:958-69.
13. Abraham GE, Buster JD, Lucas LA, Corrales PC, Teller RC.Chromatographic separation of steroid hormones for use inradioimmunoassay. Anal Lett 1972;5:509-17.
14. Jiang N, Ryan PJ. Radioimmunoassay for estrogens: a pre-liminary communication. Mayo Clin Proc 1969;44:461-5.
15. BusterJE, Abraham GE. Radioimmunoassay of plasma dehy-droepiandrosterone. Anal Lett 1972;5:203-15.
16. Abraham GE. Radioimmunoassay of plasma steroid hor-mones. In: Heftman E, editor. Modern methods of steroidanalysis. New York: Academic Press, 1973:451-70.
17. Wang CF, Lasley BL, Yen SSC. Gonadotropin secretion inresponse to low and high doses of LRF in normal and hy-pogonadal women (functional disparity of the gonado-trophs).J Clin Endocrinol Metab 1976;42:42'7-31.
18. Lasley BL, Wang CF, Yen SSC. The effects of estrogen andprogesterone on the functional capacity of the gonado-trophs. J Clin Endocrinol Metab 1975;41:820-6.
19. Wang CF, Lasley BL, Lein A, Yen SSC. The functionalchanges of the pituitary gonadotrophs during the menstrualcycle. J Clin Endocrinol Metab 1976;42:718-28.

650 Schmidt et al. September 1996AmJ Obstet Gynecol
20. HoffJD, Lasley BL, Wang CF, Yen SSC. The two pools ofpituitary gonadotropin: regulation during the menstrualcycle. J Clin Endocrinol Metab 1977;44:302-12.
21. HoffJD, Lasley BL, Yen SSC. The functional relationshipbetween priming and releasing actions of luteinizing hor-mone-releasing hormone. J Clin Endocrinol Metab 1979;49:8-11.
22. Strollo F, Harlin J, Hernandez-Montes H, Roberston DM,Zaidi AA, Diczfalusy E. Qualitative and quantitative differ-ences in the isoelectrofocusing profile of biologically active
lutropin in the blood of normally menstruating and post-menopausal women. Acta Endocrinol 1981;97:166-75.
23. Dufau ML, VeldhuisJD. Pathophysiological relationships be-tween the biological and immunological activities of lutein-izing hormone. Baillieres Clin Endocrinol Metab 1987;1:153-76.
24. Urban RJ, Veldhuis JD, Dufau ML. Estrogen regulates thegonadotropin-releasing hormone-stimulated secretion ofbiologically active luteinizing hormone. J Clin EndocrinolMetab 1991;72:660-8.