Embed Size (px)
Citation preview

Barts Cancer InstituteRebecca Auer
www.cancer.qmul.ac.uk
Waldenstrom’s: The Future

WM treatment
• WM1 recently closed
• No other UK trials
• No standard treatment
• Difficult to achieve CR
• New agents

Development pathway

Novel strategies
• Combinations including rituximab and/or bortezomib
• Novel anti-CD20 Abs / proteasome inhibitors• Bendamustine• Novel signal inhibitors Everolimus
Perifosine• Epigenetic modifiers Panobinostat• Immunomodulators IMiDs• Stem cell transplantation

The BCR study

Waldenstrom’s macroglobulinemia is somewhat similar to two other types of cancer, multiple myeloma (plasma cell cancer) and non-Hodgkin's lymphoma (a group of cancers of lymphocytes).

Bortezomib
plasma cells
Rituximab
B cells

Bortezomib in WM
• Predominantly in phase II trials in the relapsed or refractory setting
• Alone or in combination• Rapid responses• As a salvage treatment option - Fourth
International Workshop on WM treatment recommendations

Rituximab
• Minimal myelosuppression
• Single agent RR 40-50%
• Combination – chemotherapy– IMiDs

Bortezomib & Rituximab in WM
• Barts study in relapsed lymphoma– 9 of 10 patients with WM responded
• 2 studies in USA in untreated WM – BDR twice a week 83% responded– BR once a week 65% responded
Complete response/near-complete response = 22%

A phase II trial of bortezomib, rituximab and cyclophosphamide in patients with symptomatic, untreated Waldenstrom macroglobulinemia
• To determine the efficacy and safety of bortezomib, rituximab and cyclophosphamide
• Symptomatic untreated WM
• IV Bortezomib 1.6 mg/m2 on days 1, 8, 15• Oral Cyclophosphamide 250 mg/m2 on days 1, 8, 15• IV Rituximab 375 mg/m2 d1, 8, 15, 22 of cycles 2 and 4
– this will be repeated every 28 days for 6 cycles in responding patients.
• 1° endpoint: Response rate• 2° endpoint: Toxicity, complete response rate, duration of response,
speed of response, time to next treatment, progression free survival

Study design
• Run in phase 6 patients
• Multicentre phase 33 patients
• Recruit over 2 years
• 6 centres– Barts, Leeds, Mid-Yorkshire, Heartlands,
King’s, UCH, Plymouth
• Plan to follow on with a phase III– BCR versus FCR

Randomised phase II
FCRBCR v or
DCR
Possibility of s/c bortezomib

Side effects
• Bortezomib neurological
• Rituximab allergic / infections
• Cyclophosphamide low blood counts

Assessments
• Blood tests every cycle• Bone marrow and CT scans at start, midway, at completion
• Blood and BM assays to look for better markers of response
• Research samples to look at some of the genetic & protein changes in WM

Timelines
• Application to CRUK Aug 2010 April 2011
• Decision by CRUK Nov 2010 July 2011• Expectation open May 2011 Jan 2012• Duration recruitment 2 years 2 years• Duration follow up 5 years 5 years

New proteasome inhibitors
• s/c Bortezomib– less neurotoxicity but as active
• Carfilzomib– phase I data– no grade 3/4 neuropathy– activity
• Marizomib– phase I studies recruiting

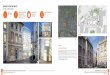
Copyright ©2004 American Society of Hematology. Copyright restrictions may apply.
Cartron, G. et al. Blood 2004;104:2635-2642
Main mechanisms of action of rituximab and ways to increase its clinical efficacy

Novel anti-CD20 Abs
• GA101
• Ofatumumab
And other Abs to other proteins eg. Belimumab

Bendamustine

StiL Group - Rummel
• BR versus R-CHOP first line n=549
– WM n=42– ORR similar BUT CR, PFS, TTNT all
significantly better with BR– Progressive disease in 2/23 BR versus 7/17
R-CHOP– Less grade 3/4 neutropenia with BR

StiL Group - Rummel
• BR versus FR relapse n=219 – BR higher ORR 83.5% v 52.5%
CR 38.5% v 16.2%– grade 3/4 neutropenia similar

Overactive in WM cells
EverolimusPerifosine
PI3K/Akt/mTOR cell signalling pathway

Everolimus
• Oral
• ORR – 70%– PR 42% MR 28%
• Median PFS and duration response not reached
• Toxicities– Grade 3 or higher in 56%– Lung toxicity in 10%

Perifosine
• Oral
• ORR - 35%
• Median PFS 12.6 months
• Toxicities– cytopenias– GI– Arthritis flare

IMiDs

IMiDs
• Thalidomide + rituximab– dose reductions required in all patients – neuropathy
• Lenalidomide + rituximab– study discontinued due to unexpected
clinically significant anaemia
• Pomolidomide

HDACIEg. Panobinostat

Open studies
Ofatumumab anti-CD20 monoclonal Ab
Panobinostat epigenetic - HDACI
Everolimus + BR mTOR inhibitor
Belimumab monoclonal Ab
Pomolidomide ImiD

Chemotherapy
Biologic agent
Monoclonal Ab
Waldenstrom’s: The Future