Embed Size (px)
Citation preview
Barry K Logan PhD, D-ABFT
Impact of Changing Marijuana Laws on Impaired Driving
Cannabis
•Most popular recreational drug in the US after alcohol and tobacco.
•#1 Drug in the DUI Drug Arrests and 6.8% of Friday and Saturday evening drivers test positive for use.
•Some 25 million Americans have smoked marijuana in the past year, and more than 14 million do so regularly.
•Possession and use illegal under federal law, but states have variable policies on enforcement and prosecution.
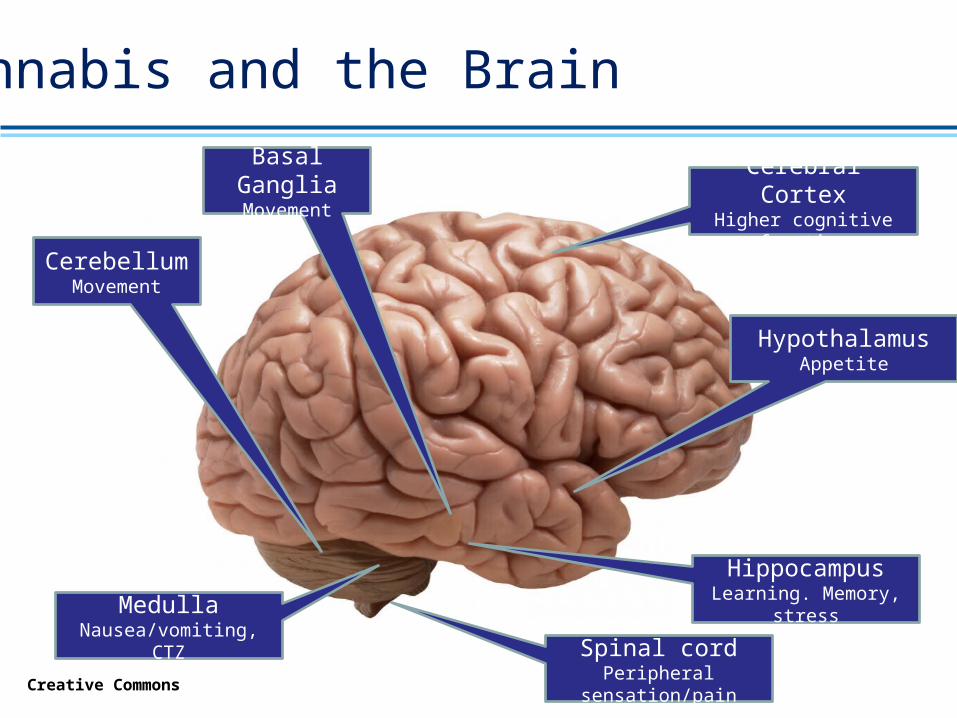
Cannabis and the Brain
Creative Commons
CerebellumMovement
Basal GangliaMovement
Cerebral CortexHigher cognitive
function
HippocampusLearning. Memory,
stress
Spinal cordPeripheral
sensation/pain
HypothalamusAppetite
MedullaNausea/vomiting, CTZ
Cannabis and Impairment
Well known Cognitive effects include:Concentration and sustained attention/vigilance.Fatigue, sleepiness, lethargy, memory problems.Reaction time Difficulty in thinking and
problem-solving. Difficulty in registering,
processing, and using information.
Cannabis and Impairment
Well Known Psychomotor Effects Include Decreased motor coordination Slurred speech Dizziness Impairment in reaction time
and tracking.
Cannabinoids and Driving
• Epidemiological Evidence• Several studies support increased crash and
culpability risk resulting from driving within two hours of smoking.
• More frequent cannabis exposure results in higher odds ratios for MVA’s of ~2.5 (i.e. 2.5 X more likely).
• Fatally injured cannabis positive drivers (other drugs may be present) had an adjusted OR of 8.6.
• Meta analysis of 16 published studies concluded an adjusted OR of between 2.66 and 1.92, in cannabis positive crash drivers.
Cannabinoids and Driving
• Experimental Evidence• THC’s impairing effects increase with task
complexity.• Unexpected circumstances and choice during
otherwise monotonous driving exhibit increased risk for errors over non cannabis using controls.
• Reaction time, road tracking, weaving, steering wheel variability, and brake latency all increase with recent cannabis exposure.
• THC effects on cognitive performance following smoking include immediate recall, executive functioning, working memory and attention.
Cannabinoids and Driving
• Experimental Evidence (cont’d.)• Complex tasks involving multiple
neurocognitive and neuromotor skills are particularly sensitive to THC.
• Driving simulator studies support dose dependant increases in weaving.
• Evidence of compensatory behavior in marijuana impaired drivers.
• There is evidence of tolerance to some acute effects in frequent users, however there is also evidence of long term reversible impairment in baseline performance in heavy chronic users following cessation.
Cannabinoids and Driving
• Experimental Evidence (cont’d.)• Standardized Field Sobriety Tests are
insensitive to THC in some cases where there is objective evidence of driving impairment.
• Cannabis use in conjunction with alcohol markedly increases the level of impairment.
Hartman RL, Huestis MA. Cannabis effects on driving skills. Clin Chem. 2013 Mar;59(3):478-92.
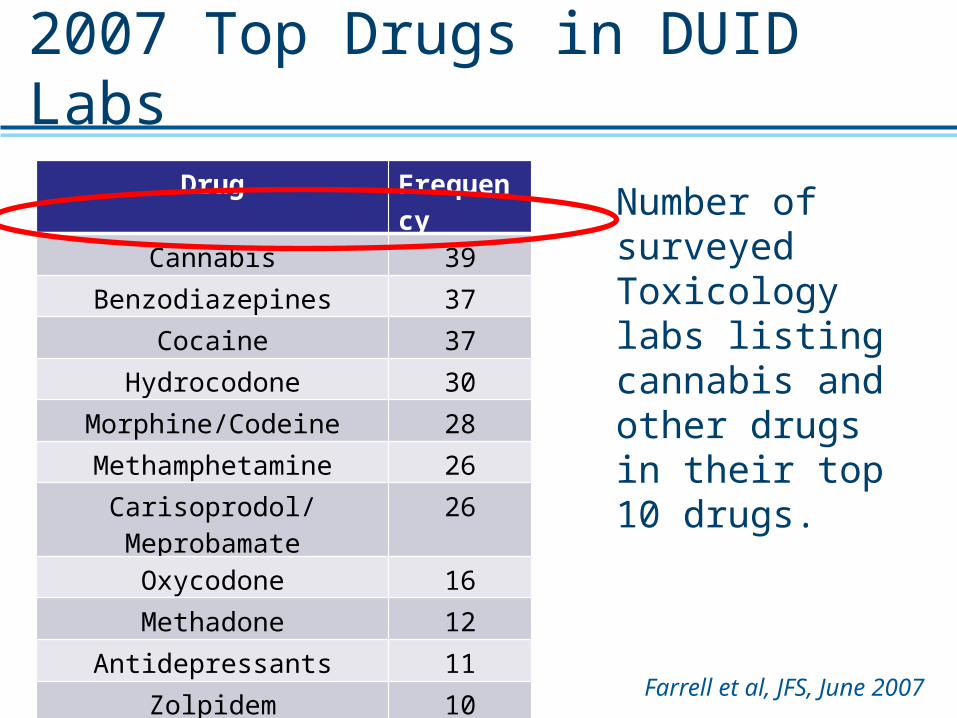
Farrell et al, JFS, June 2007
Drug Frequency
Cannabis 39
Benzodiazepines 37
Cocaine 37
Hydrocodone 30
Morphine/Codeine 28
Methamphetamine 26
Carisoprodol/Meprobamate 26
Oxycodone 16
Methadone 12
Antidepressants 11
Zolpidem 10
2007 Top Drugs in DUID Labs
Number of surveyed Toxicology labs listing cannabis and other drugs in their top 10 drugs.
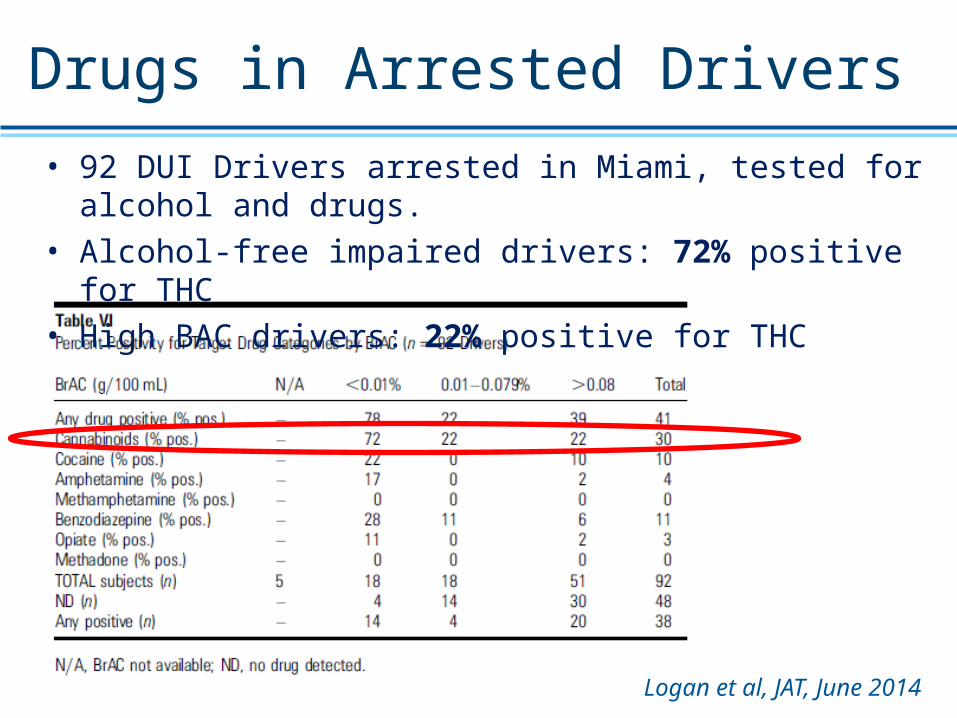
Drugs in Arrested Drivers• 92 DUI Drivers arrested in Miami, tested for alcohol and drugs.• Alcohol-free impaired drivers: 72% positive for THC• High BAC drivers: 22% positive for THC
Logan et al, JAT, June 2014
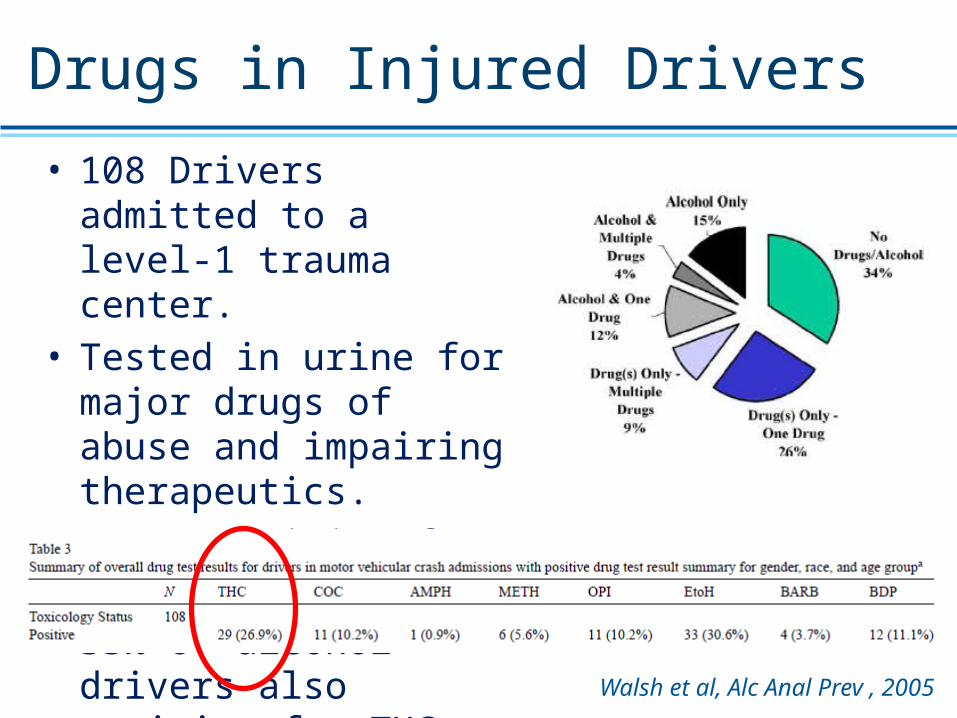
Drugs in Injured Drivers
• 108 Drivers admitted to a level-1 trauma center.
• Tested in urine for major drugs of abuse and impairing therapeutics.
• 26.9% positive for THC• 33% of alcohol drivers also
positive for THC
Walsh et al, Alc Anal Prev , 2005
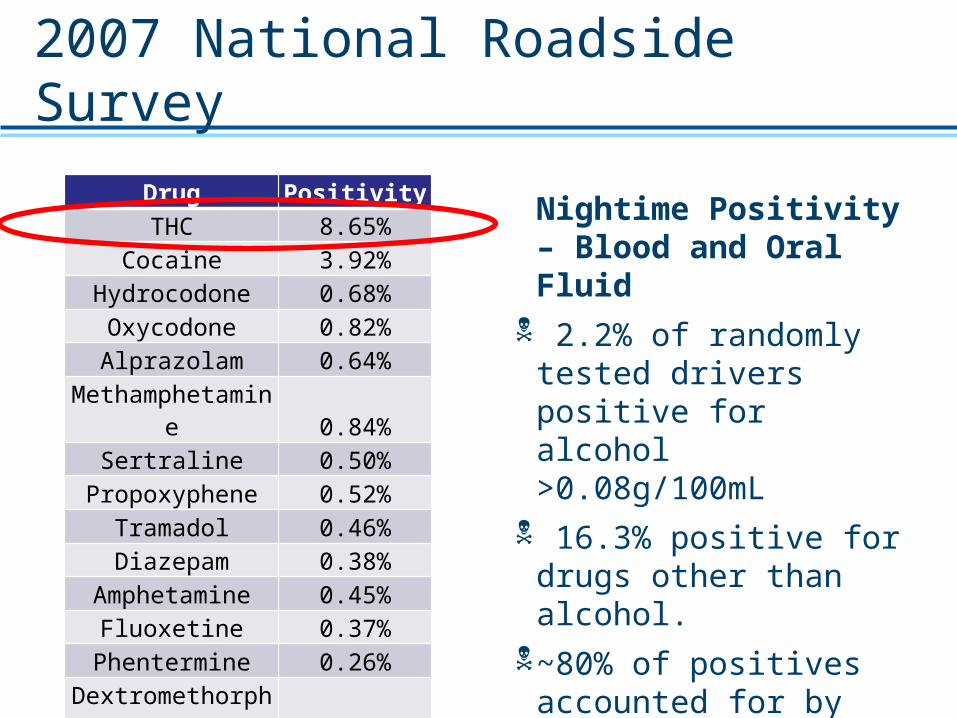
2007 National Roadside Survey
Drug PositivityTHC 8.65%
Cocaine 3.92%Hydrocodone 0.68%Oxycodone 0.82%Alprazolam 0.64%
Methamphetamine 0.84%
Sertraline 0.50%Propoxyphene 0.52%
Tramadol 0.46%Diazepam 0.38%
Amphetamine 0.45%Fluoxetine 0.37%
Phentermine 0.26%Dextromethorph
an 0.22%Methadone 0.19%
Nightime Positivity – Blood and Oral Fluid
2.2% of randomly tested drivers positive for alcohol >0.08g/100mL
16.3% positive for drugs other than alcohol.
~80% of positives accounted for by ~20% of the drugs.
Cannabis use #1 at 8.65%
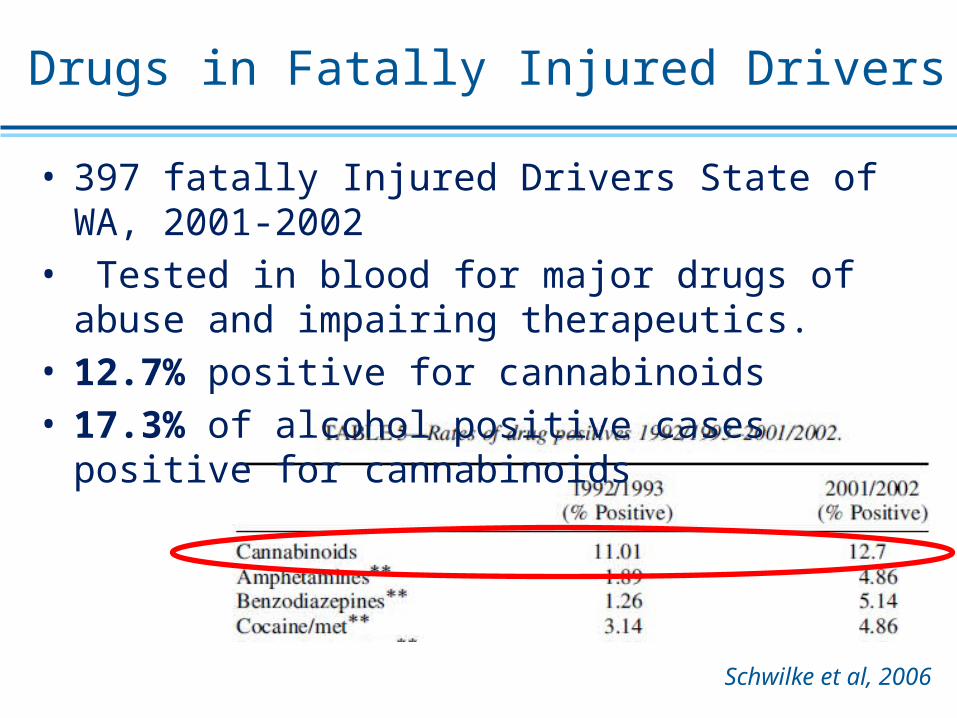
Drugs in Fatally Injured Drivers
• 397 fatally Injured Drivers State of WA, 2001-2002• Tested in blood for major drugs of abuse and impairing
therapeutics.• 12.7% positive for cannabinoids• 17.3% of alcohol positive cases positive for cannabinoids
Schwilke et al, 2006
Changing US Attitudes to MJ
• November 2012• WA State and CO legalize
possession by adults of 1oz of useable MJ for recreational use.
• Regulate and tax sale and distribution of marijuana.
• Focus enforcement on illegal marijuana trade, and DUID
• November 2014
• OR, AK, and Washington D.C. follow suit
Marijuana DUI post Legalization
• Colorado • The new law went into effect in January 2014.• The THC percent positivity rates for January-
February data were 21%, 38%, 45% and 48% in 2011, 2012, 2013 and 2014, respectively.
• The positive rate appears to be steadily increasing and the 2011-2012 increase was statistically significant.
• There was no significant difference between 2012 and 2013, 2012 and 2014 or 2013 and 2014 (Pearson's chi-squared test at a=0.05).
S. Urfer, J. Morton, V. Beall, J. Feldmann, and J. Gunesch, “Analysis of Δ9-tetrahydrocannabinol driving under the influence of drugs cases in Colorado from January 2011 to February 2014,” J. Anal. Tox., vol. 38, no. 8, pp. 575–581, Oct. 2014.
Marijuana DUI post Legalization
• Washington• The new law went into effect in January 2014*.• The percentage of tested impaired driving
cases which were positive for Delta-9 THC in whole blood at concentrations at or above 5 ng/mL were 18.6% and 24.9% in 2012 and 2013, respectively
• A significant increase (p=0.05) was noted between the pooled prevalence, pre-legislation and the post-legislation of confirmed positive THC cases, implying higher rates of use in the impaired driving population.
F. J. Couper and B. L. Peterson, “The prevalence of marijuana in suspected impaired driving cases in Washington state,” J. Anal. Toxicol., vol. 38, no. 8, pp. 569–574, Oct. 2014.
NMS Labs DUID Marijuana Data
• 36,037 cases drawn from DUID arrests.
• 17,612 (48.8%) cases between Aug 2009 and Oct 2014 presumptively positive for cannabinoids (ELISA, c/o 5ng/mL).
• 13,988 (79.4%) confirmed positive for one of THC (1ng/mL), THC-COOH, (5ng/mL), or THC-OH (5ng/mL).
• 7,448 cases were also screened for alcohol and other drugs: benzodiazepines, opiates, cocaine metabolite, amphetamines, methadone, phencyclidine, barbiturates, and propoxyphene.
• 6,877 cases had available gender, age, alcohol/other drug data:• 80.6% male; Mean/median age 29/25; Range, 15-75
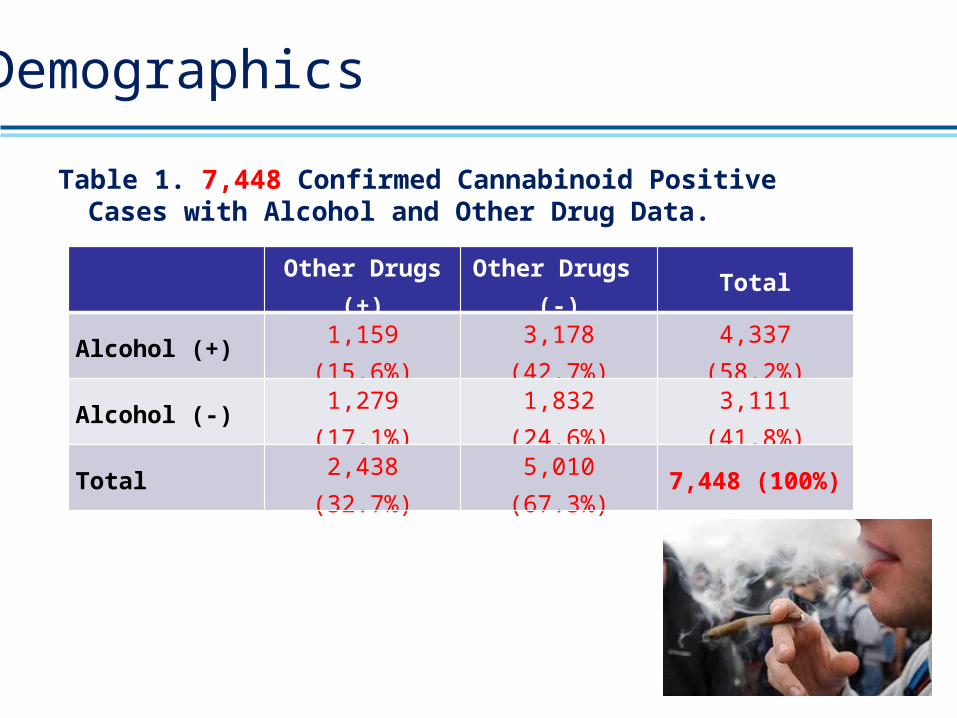
Demographics
Other Drugs (+) Other Drugs (-) Total
Alcohol (+) 1,159 (15.6%) 3,178 (42.7%) 4,337 (58.2%)
Alcohol (-) 1,279 (17.1%) 1,832 (24.6%) 3,111 (41.8%)
Total 2,438 (32.7%) 5,010 (67.3%) 7,448 (100%)
Table 1. 7,448 Confirmed Cannabinoid Positive Cases with Alcohol and Other Drug Data.
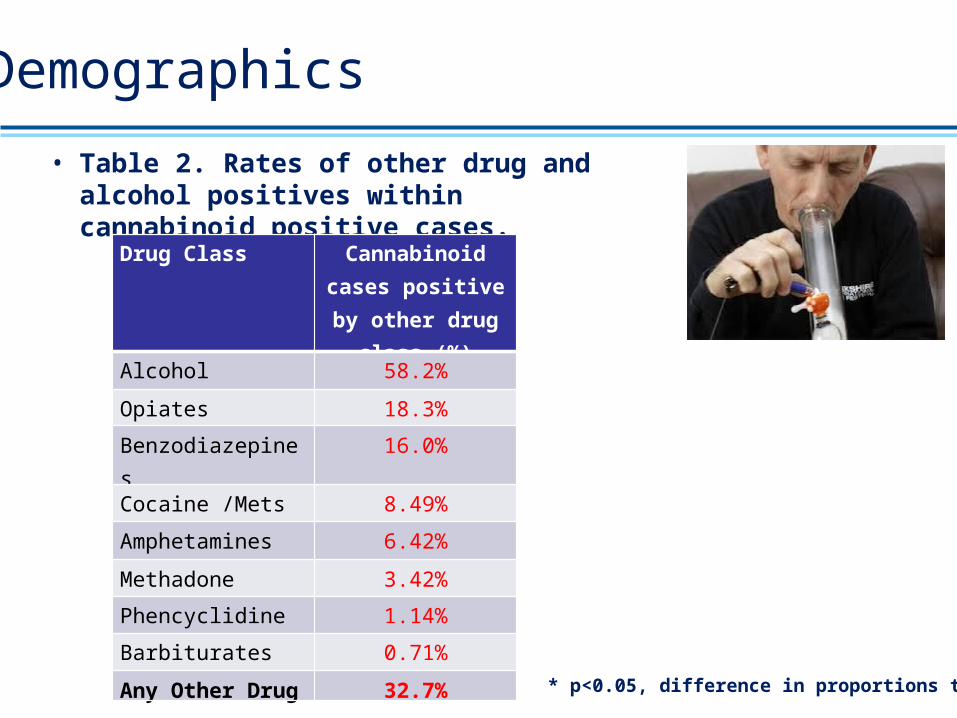
Demographics
• Table 2. Rates of other drug and alcohol positives within cannabinoid positive cases.
Drug Class Cannabinoid cases positive by other
drug class (%)
Alcohol 58.2%
Opiates 18.3%
Benzodiazepines 16.0%
Cocaine /Mets 8.49%
Amphetamines 6.42%
Methadone 3.42%
Phencyclidine 1.14%
Barbiturates 0.71%
Any Other Drug 32.7%
* p<0.05, difference in proportions test.
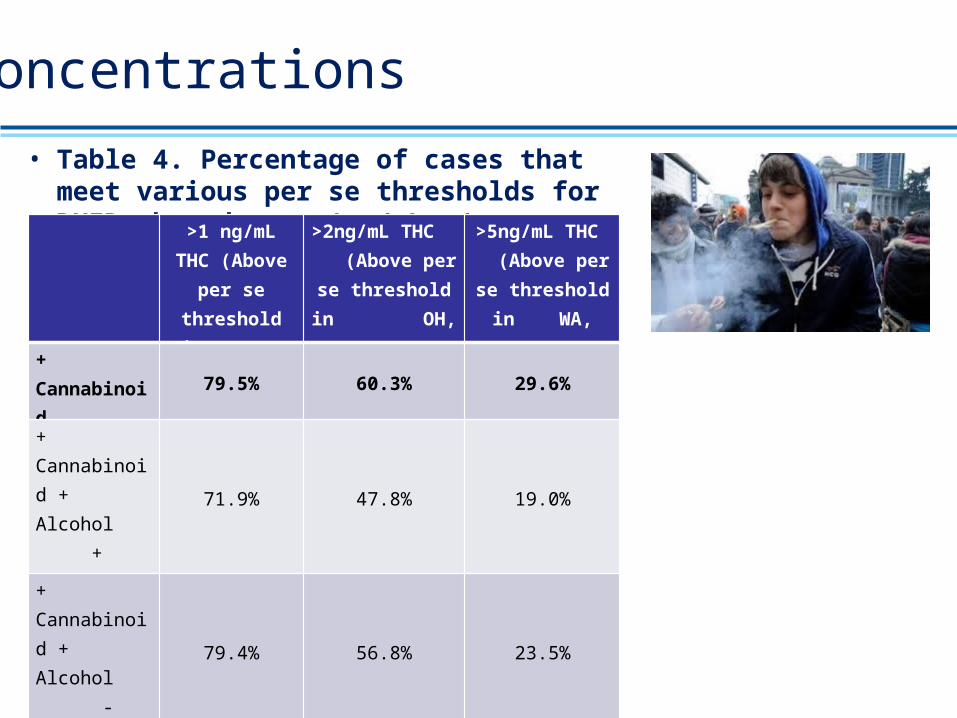
Concentrations• Table 4. Percentage of cases that meet various per
se thresholds for DUID, based on a 1ng/mL c/o
>1 ng/mL THC (Above per se threshold in
PA)
>2ng/mL THC (Above per se
threshold in OH, NV)
>5ng/mL THC (Above per se threshold in WA, CO, MT)
+ Cannabinoid 79.5% 60.3% 29.6%
+ Cannabinoid + Alcohol + Other Drug
71.9% 47.8% 19.0%
+ Cannabinoid + Alcohol - Other Drug
79.4% 56.8% 23.5%
+ Cannabinoid - Alcohol + Other Drug
74.6% 55.5% 28.6%
+ Cannabinoid - Alcohol - Other Drug
90.51% 78.9% 49.3%
Impact of 5ng/mL THC per se Law
0 2.0-2.9
3.0-3.9
4.0-4.9
5.0-5.9
5 7.0-7.9
8.0-8.9
9.0-9.9
10.0-10.9
10
12.0-12.9
13.0-13.9
14.0-14.9
15.0-15.9
15
17.0-17.9
18.0-18.9
19.0-19.9
20
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Relative Frequency %
[THC]blood, ng/mL
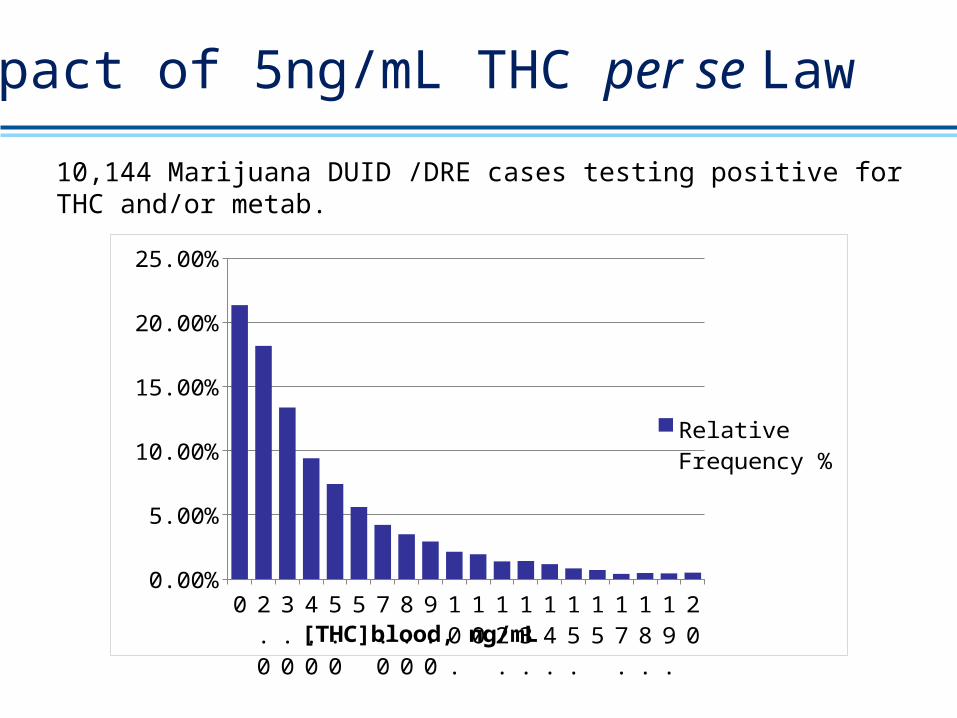
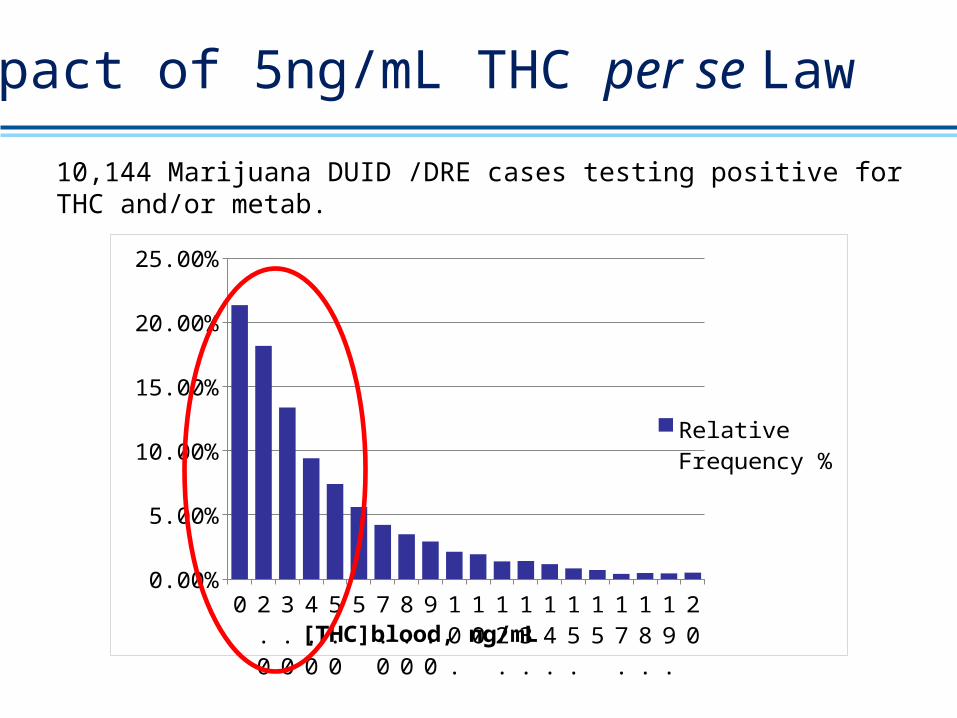
10,144 Marijuana DUID /DRE cases testing positive for THC and/or metab.
Impact of 5ng/mL THC per se Law
0 2.0-2.9
3.0-3.9
4.0-4.9
5.0-5.9
5 7.0-7.9
8.0-8.9
9.0-9.9
10.0-10.9
10
12.0-12.9
13.0-13.9
14.0-14.9
15.0-15.9
15
17.0-17.9
18.0-18.9
19.0-19.9
20
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Relative Frequency %
[THC]blood, ng/mL
10,144 Marijuana DUID /DRE cases testing positive for THC and/or metab.
Conclusions
• Cannabis use under typical conditions creates a high-risk of impairment for 2-4 hours after dosing.
• When used with alcohol, risk of impairment increases substantially.
• Cannabis use is the drug category most frequently detected in arrested, injured, and fatally injured drivers after alcohol.
• There is no basis for setting a 5ng/mL per se standard for THC at ~2 hours post-driving to reflect the level at the time of driving.
Conclusions
• 81% of all cannabinoid drivers are below 5ng/mL at the time of the test.
• 51% of drivers using only marijuana are below 5ng/mL at the time of the test.
• 76.8% of cannabinoid positive drivers are also positive for alcohol (60%), or other drugs (33%).
• Optimum solution is objective impairment assessment using tools like the DRE program, with toxicological confirmation of use at an analytically based cut-off of 1ng/mL.