Embed Size (px)
Citation preview
BARRIERS TO THE USE OF MAGNESBARRIERS TO THE USE OF MAGNESBARRIERS TO THE USE OF MAGNESBARRIERS TO THE USE OF MAGNESIUM SULPHATE IUM SULPHATE IUM SULPHATE IUM SULPHATE
IN PAKISTANIN PAKISTANIN PAKISTANIN PAKISTAN---- A STUDY TO DEVELOP INFORMED A STUDY TO DEVELOP INFORMED A STUDY TO DEVELOP INFORMED A STUDY TO DEVELOP INFORMED
POLICYPOLICYPOLICYPOLICY
Submitted by:
Dr Assad Hafeez
Professor Shamsa Rizwan
Table of Contents
1. Background ------------------------------------------------------------------------ 1
2. Methodology ---------------------------------------------------------------------- 3
2.1 Data collection ------------------------------------------------------------------------------- 4
2.1.1 Government/Regulatory Level ------------------------------------------------------- 4
2.1.2 Pharmaceutical Supply System ------------------------------------------------------- 4
2.1.3 Health Professionals --------------------------------------------------------------------- 4
2.1.4 Health Facilities --------------------------------------------------------------------------- 5
2.2 Data analysis --------------------------------------------------------------------------------- 5
3. Findings ---------------------------------------------------------------------------- 6
3.1 Policy, Guidelines and Registration ----------------------------------------------------- 6
3.2 Procurement and Distribution ------------------------------------------------------------ 6
3.3 Cost and Consumption ---------------------------------------------------------------------- 7
3.4 Dosage Regimens and Route ------------------------------------------------------------- 8
3.5 Availability ------------------------------------------------------------------------------------ 9
3.6 Training --------------------------------------------------------------------------------------- 10
3.7 Awareness and Practices of Health Professionals --------------------------------- 11
4. Discussion ----------------------------------------------------------------------- 15
5. Recommendations ------------------------------------------------------------ 17
ANNEXURES: -----------------------------------------------------------------------------------------------18-24
ANNEXURE – I: TOOLS
ANNEXURE – II: PARTICIPANTS OF THE FOCUS GROUP DISCUSSIONS
ANNEXURE – III: LIST OF HEALTH FACILITIES SURVEYED FOR THE STUDY
REFRENCES

Acronyms
AIDS Acquired Immunodeficiency Syndrome
AJK Azad Jammu & Kashmir
ARI Acute Respiratory Infections
CMW Community Midwife
CPR Contraceptive Prevalence Rate
DoH Department of Health
DOTS Directly Observed Short Course Treatment
DPIU District Program Implementation Unit
EDO Executive District Officer
EMoC Emergency Obstetric Care
EPI Extended Programme on Immunization
ESS-EMCH Essential Surgical skills and Emergency Maternal and child Health
ESPs Essential Services Packages
FANA Federally Administered Northern Areas
FATA Federally Administered Tribal Areas
FLCFs First Level Care Facilities
FP Family Planning
FP & PHC Family Planning & Primary Health Care
FPIU Federal Program Implementation Unit
FPO Field Program Officer
GDP Gross Domestic Product
HDI Human Development Index
HIV Human immunodeficiency virus
HMIS Health Management Information System
ICT Islamabad Capital Territory
IMR Infant Mortality Rate
LHS Lady Health Supervisor
LHV Lady Health Visitor
LHWP Lady Health Workers Programme
LHWs Lady Health Workers
MgSO4 Magnesium sulfate
MS DMedical Store Depot
MCH Maternal and Child Health
MDG Millennium Development Goals
MNCH Maternal, Newborn and Child Health
MIS Management Information System
MMR Maternal Mortality Rate
MoH Ministry of Health
NGOs Non Governmental Organizations
NHF National Health Facility
PDHS Pakistan Demographic Household Survey
PIU Program Information Unit
PPIU Provincial Program Implementation Unit
PSDP Public Sector Development Programme
PSLM Pakistan Survey of Living Standards
RH Reproductive Health
SBA Skilled Birth Attendants
STI Sexually Transmitted Infections
TT Tetanus Toxiod
UK United Kingdom
UNFPA United Nation Fund for Population
UNICEF United Nation Children Fund
WHO World Health Organization
1
1. Background
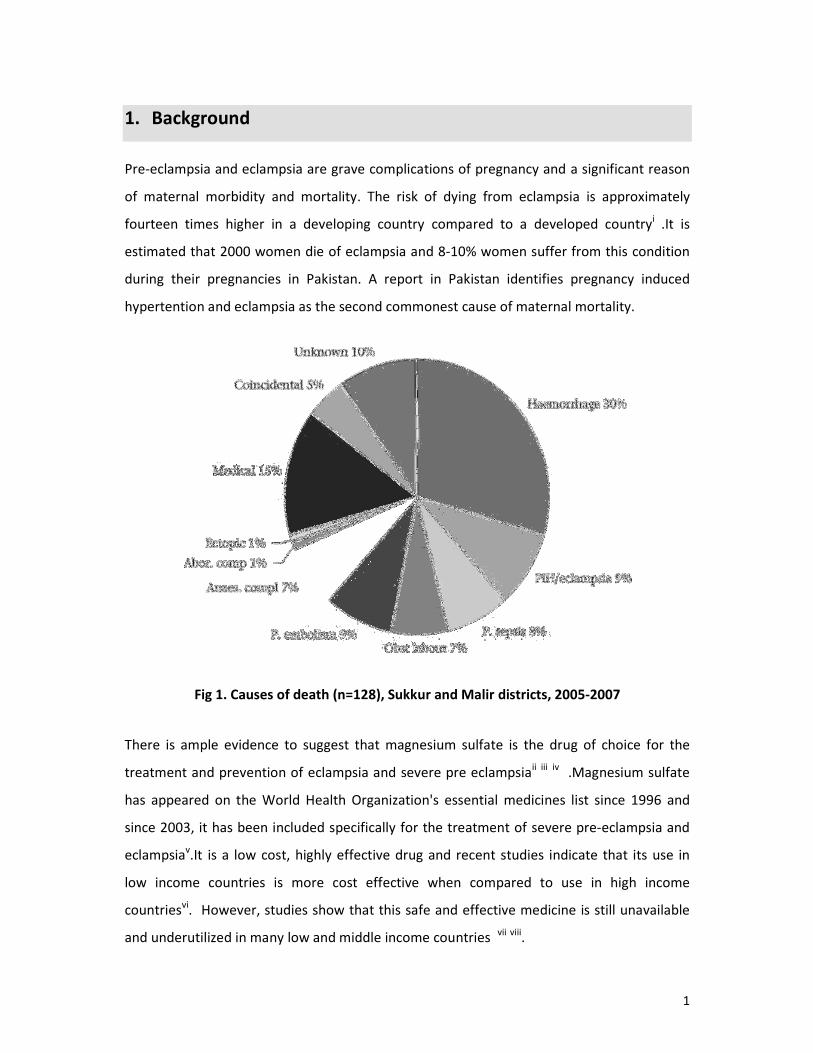
Pre-eclampsia and eclampsia are grave complications of pregnancy and a significant reason
of maternal morbidity and mortality. The risk of dying from eclampsia is approximately
fourteen times higher in a developing country compared to a developed countryi .It is
estimated that 2000 women die of eclampsia and 8-10% women suffer from this condition
during their pregnancies in Pakistan. A report in Pakistan identifies pregnancy induced
hypertention and eclampsia as the second commonest cause of maternal mortality.
Fig 1. Causes of death (n=128), Sukkur and Malir districts, 2005-2007
There is ample evidence to suggest that magnesium sulfate is the drug of choice for the
treatment and prevention of eclampsia and severe pre eclampsiaii iii
iv .Magnesium sulfate
has appeared on the World Health Organization's essential medicines list since 1996 and
since 2003, it has been included specifically for the treatment of severe pre-eclampsia and
eclampsiav.It is a low cost, highly effective drug and recent studies indicate that its use in
low income countries is more cost effective when compared to use in high income
countriesvi. However, studies show that this safe and effective medicine is still unavailable
and underutilized in many low and middle income countries vii
viii
.

2
If magnesium sulfate is used appropriately, 2000 maternal deaths could be prevented and
50,000 cases of eclampsia could be cured in a year in Pakistan, making a significant dent in
the overall mortality and morbidity figures. This would contribute positively to the national
efforts towards achieving Millennium Development Goals by 2015. The first step in
designing effective interventions to increase the use of MgSO4 is to identify barriers to use
and target the intervention accordinglyix.
If we consider the cost effectiveness of MgSO4 if only eclampsia were treated with
magnesium sulfate (and not preeclampsia) the use of magnesium sulfate would be an
extraordinarily cost effective intervention. Only two eclamptic women would need to be
treated to save one life because maternal deaths are almost halved with the use of
magnesium sulfate, whereas 36 women with signs of imminent eclampsia required
treatment to prevent one case of eclampsiax . Reasons for low usage in practice could have
a wide spectrum ranging from issues of production, pricing, availability, safety concerns,
attitudes of medical staff and other barriers. There is ample data from other developing
countries highlighting the issue of mgso4 use. A study in Mozambique and Zimbabwe, two
countries with high maternal mortality ratios, describes problems with the registration,
approval, acquisition, and distribution of magnesium sulphate, and hence its availability to
clinicians There is no published evidence from Pakistan that looks at the availability and
barriers in the use of magnesium sulphate. We aim to determine the barriers to the use of
magnesium sulphate and assess its availability in the public and private health facilities of
Pakistan with the ultimate goal of gathering context-specific evidence for formulation of
enabling policies at national and provincial level.

3
2. Methodology
We used a multipronged approach to assess the problem. A list of all the necessary
requirements for the rational use of the drug was formulated after literature search and
discussion (Fig 2). For each requirement listed, we identified the level in the health system
where the information could be gathered from.
Fig 2. Requirements for Rational MgSO4 use
The levels identified were
• Government/regulatory
• Pharmaceutical supply system
• Health facilities
• Health professionals.
We carried out quantitative and qualitative research and developed separate tools for the
health facility survey, in-depth interviews with pharmacists, government officials and key
Rational Use of
MgSO4
4
informants. Guidelines for the focus group discussion with the obstetricians and medical
officers were also developed. [Annex 1]
2.1 Data collection
Based on the requirements, we collected data for each level from all the four provinces of
Pakistan. Data collection took place between 20th
Nov and 31st
Dec 2010.
Different data collection approaches were used for different levels including in-depth, semi
structured qualitative interviews , informal discussions and quantitative questionnaires
covering the structure and process of policy for the management of eclampsia and pre-
eclampsia, factors affecting the implementation of policies ,individual's knowledge of
evidence , availability and use of Mg SO4.
Purposive sampling approach was used, based on the respondents' involvement in policy
making or procurement for magnesium sulphate for qualitative data and the type of facility.
The data collection procedure at different levels is given below.
2.1.1 Government/Regulatory Level
For government regulatory procedures desk review of available evidence from published
literature and national documents such as standard treatment guidelines, essential drug list,
other clinical guidelines and national policies was undertaken. Moreover in-depth interviews
with the Director General Health and MNCH program manager were carried out.
2.1.2 Pharmaceutical Supply System
Information about the procurement, supply and distribution of MgSO4 within the public
health system of Pakistan was obtained from Ministry of Health personnel responsible for
the procurement of medicines for the public sector, employees at the Central Medical Store
and pharmacy workers in the visited health facilities.
2.1.3 Health Professionals
Members from the Society of Gynaecologists and Obstetricians (SOGP) were interviewed,
and focus group discussions were carried out with Gynaecologists from all provinces as well
as women medical officers most likely to be managing patients with pre-eclampsia and
eclampsia[Annex 2].

5
2.1.4 Health Facilities
An observational exercise was undertaken at each sampled health facility to ascertain if the
facility had the necessary supplies and equipment to administer MgSO4 injection and
monitor a patient receiving MgSO4 treatment of severe pre-eclampsia or eclampsia. This
was to assess not only if MgSO4 was available on the day of the visit, but also if the facility
had sufficient quantity of MgSO4 to give the recommended treatment regimen to one
patient. Moreover which route of administration was preferred in the facility? The presence
of guidelines/ protocols in the facility was also observed.
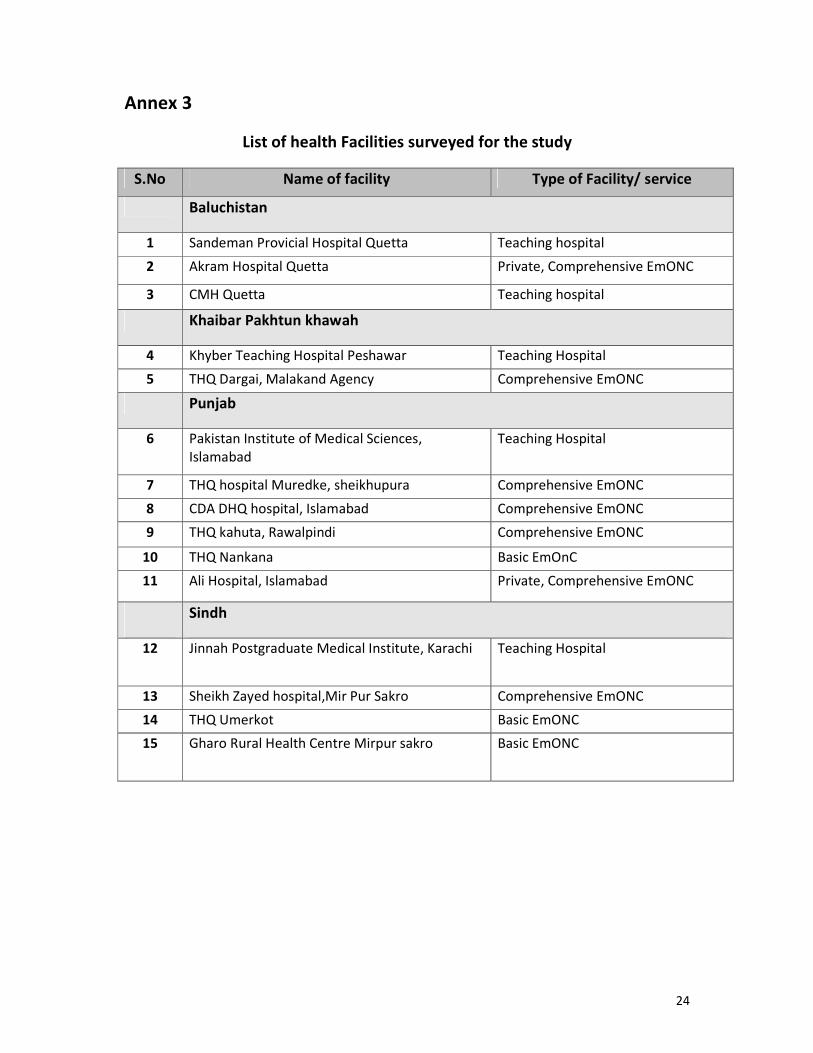
Sample selection of health facilities
A total of fifteen health facilities including teaching hospitals, District Head Quarter (DHQ),
tehsil head quarter (THQ), Rural health centers (RHC) and private hospitals were surveyed
[Annex3]. The pharmacy and the Obstetric departments were visited for data collection.
2.2 Data analysis
All interviews were audio recorded and transcribed. Categories emerging from the data
were identified and a coding frame developed. Quantitative data was analyzed using SPSS
version 15.

6
3. Findings
The barriers to the use of magnesium sulfate were assessed at various levels and the
findings are summarized below.
3.1 Policy, Guidelines and Registration
Magnesium sulphate injection is Registered for use in Pakistan and is listed as the first line
treatment for eclampsia in the key policy documents - the national Essential Medicines List
NEML (2007), Pakistan National Formulary (2005) and the MNCH EmONC training manual
(2005). In Pakistan Mg SO4 is registered for the treatment of both severe pre-eclampsia and
eclampsia and not for other convulsions. However, no national guidelines are available for
its use. Mg SO4 is not a part of the Pakistan Best Practices Policy (Karachi seminar
declaration, 2008). Only one Pakistan based multinational pharmaceutical company (Zafa) is
manufacturing the medicine. The dosage regimens recommended in the EmNOC are
different from the regimen recommended by the Oxford Group. There is no mention of the
intramuscular only regimen in any of the policy documents.
3.2 Procurement and Distribution
National procurement of medicines is carried out by the Ministry of Health and is based on
the national Essential Medicines List. There is no separate budget allocated for medicines to
the provinces and procurement of medicines is directly through provinces with whom the
NEML is shared. The Provincial Medical Store Depot (MSD) manages the acquisition, storage
and distribution of medicines for the province and is the main supplier of medicines to
public sector hospital pharmacies and district health offices (DHO). Private hospitals acquire
medicines from the open market. Central and specialized hospitals, such as the Pakistan
Institute of medical sciences (Teaching Hospital), are also given a grant by the ministry of
health for the independent procurement of emergency medicines and medical supplies. The
procurement of MgSO4 was mostly depended upon the demand by the health departments.
Indicating an independent procurement of emergency medicines and is therefore
dependent on facility policies rather than national procurement policies.
7
3.3 Cost and Production
Magnesium sulfate is a low cost drug and too inexpensive for being an incentive for the
pharmaceutical companies. Low price may also be a counter-incentive for facilities
especially when facilities have some freedom in independent procurement of drugs. The
market for the drug is small and the drug is not widely used for other conditions thereby
lacking the economy of scope. The average price is Rs 3.5 per ampoule. However in Quetta,
Baluchistan the all year availability is an issue and MgSO4 is being sold at a price of Rs 75 in
the open market implying out-of-pocket expenditure that may not be affordable by some
patients.
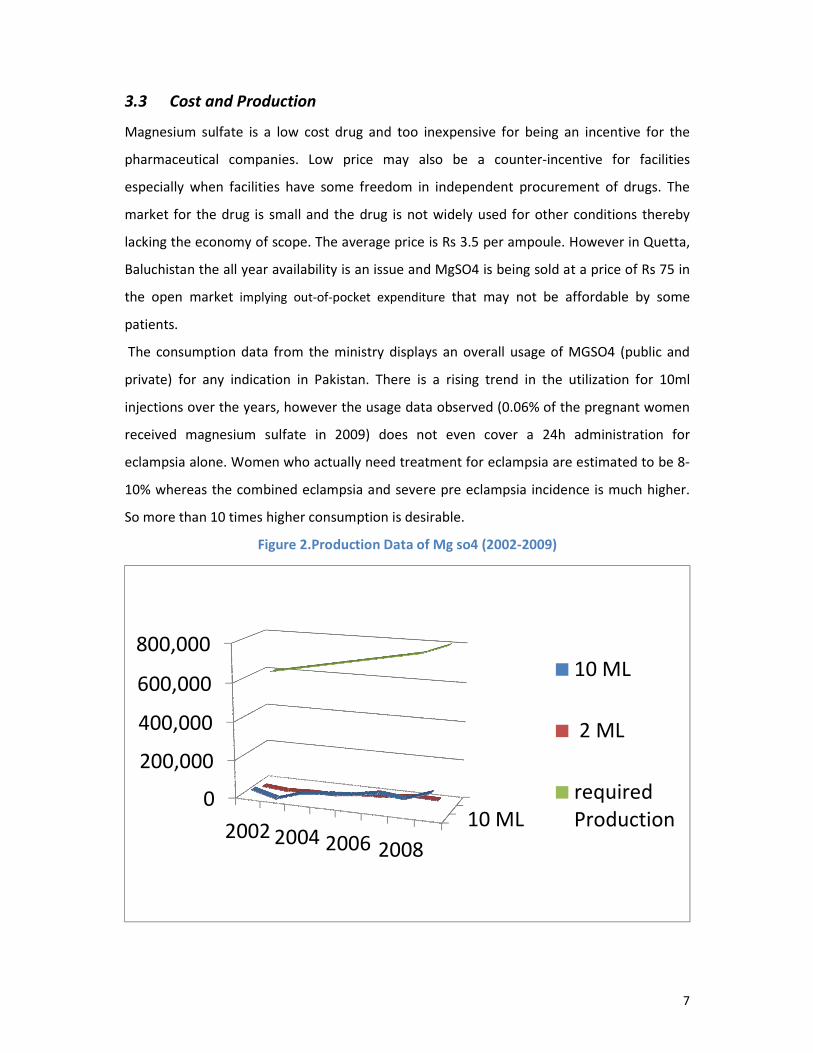
The consumption data from the ministry displays an overall usage of MGSO4 (public and
private) for any indication in Pakistan. There is a rising trend in the utilization for 10ml
injections over the years, however the usage data observed (0.06% of the pregnant women
received magnesium sulfate in 2009) does not even cover a 24h administration for
eclampsia alone. Women who actually need treatment for eclampsia are estimated to be 8-
10% whereas the combined eclampsia and severe pre eclampsia incidence is much higher.
So more than 10 times higher consumption is desirable.
Figure 2.Production Data of Mg so4 (2002-2009)
10 ML0
200,000
400,000
600,000
800,000
2002 2004 2006 2008
10 ML
2 ML
required
Production
8
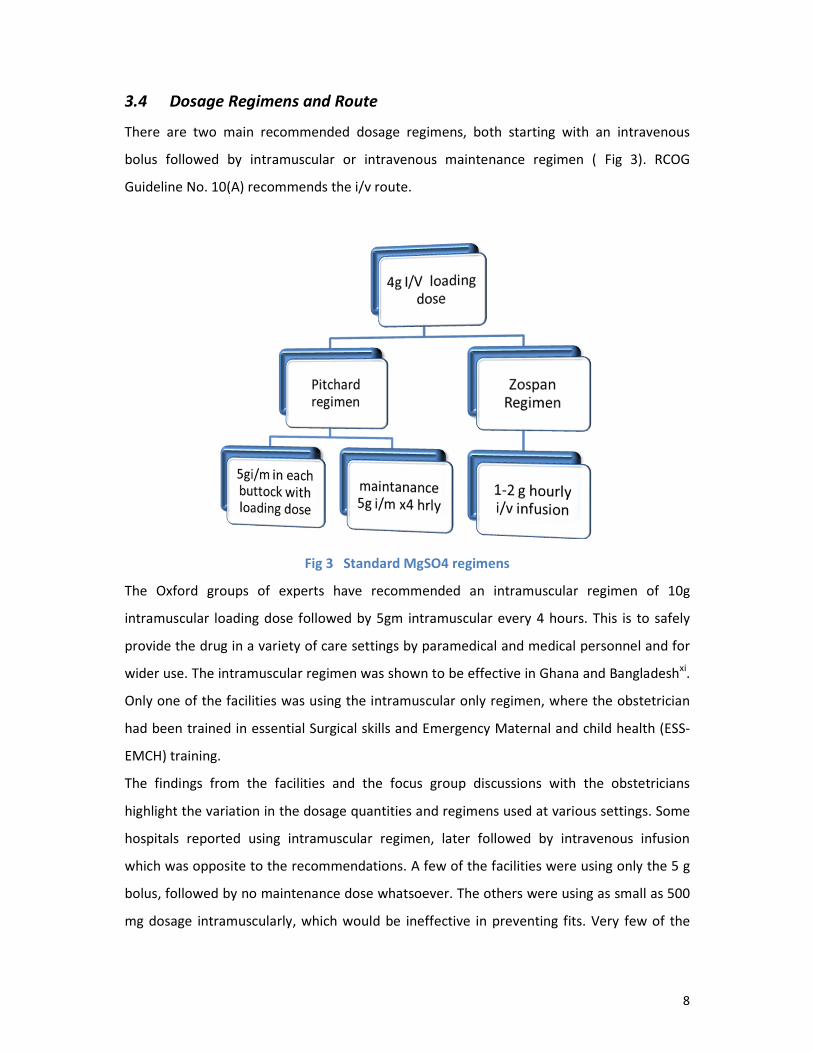
3.4 Dosage Regimens and Route
There are two main recommended dosage regimens, both starting with an intravenous
bolus followed by intramuscular or intravenous maintenance regimen ( Fig 3). RCOG
Guideline No. 10(A) recommends the i/v route.
Fig 3 Standard MgSO4 regimens
The Oxford groups of experts have recommended an intramuscular regimen of 10g
intramuscular loading dose followed by 5gm intramuscular every 4 hours. This is to safely
provide the drug in a variety of care settings by paramedical and medical personnel and for
wider use. The intramuscular regimen was shown to be effective in Ghana and Bangladeshxi.
Only one of the facilities was using the intramuscular only regimen, where the obstetrician
had been trained in essential Surgical skills and Emergency Maternal and child health (ESS-
EMCH) training.
The findings from the facilities and the focus group discussions with the obstetricians
highlight the variation in the dosage quantities and regimens used at various settings. Some
hospitals reported using intramuscular regimen, later followed by intravenous infusion
which was opposite to the recommendations. A few of the facilities were using only the 5 g
bolus, followed by no maintenance dose whatsoever. The others were using as small as 500
mg dosage intramuscularly, which would be ineffective in preventing fits. Very few of the

9
facility were using the i/v regimen because of lack of staff and equipment as reported in the
interviews as well as observed by the researchers.
3.5 Availability
The availability of Mg SO4 in the private and public pharmacies was assessed in all the four
provinces. The medicine was available in the pharmacies of larger cities, and the teaching
hospitals whereas it was not attainable in majority of other settings.
The pharmacies at the Teaching Hospitals had MgSO4 in stock, procured from a local
wholesaler/ vender using the grant provided by the MoH. The procurement was a result of
demand from the obstetricians working at the hospitals. The teaching hospital pharmacies
had the NEML with them at the time of survey. During focus group discussions, some of the
teaching staff raised the concern about continuous and persistent availability of MgSO4.
Since most of the eclampsia patients were referred to tertiary care, most of the non-
teaching hospitals lacked the demand, hence the availability. At some places patient’s
relatives were asked to bring the medicine from private pharmacies. The medicine is neither
easily available nor is availability throughout the year guaranteed in the Baluchistan and
Sindh province. However as it is acquired for teaching/ army hospitals through the MSD,
they had the stocks available at the time of visit. There was a shortage of the medicine in
the open market at some places and was being sold at a higher price compromising the
availability of the drug to the poor.
The private hospital pharmacies surveyed did not have the medicine as they only procured if
there was a demand and the demand was not great in private sector.
The availability of the 24 hour dosage in the labour wards was also assessed. All the teaching
hospitals had the medicine available in sufficient quantities but in THQ and some DHQs it
was either not available or was not in sufficient quantity (fig. 3). The availability of necessary
adjunct treatment and supplies was deficient even in some teaching hospitals. The antidote
calcium gluconate and local anesthetic 2% xylocain for i/m regimen was not available in
many settings. The infusion pumps for i/v infusions were not available in any setting. There
were no written protocols for use in majority of the facilities. In contrast to guidelines,
diazepam ampoules were on the emergency trays at some sites indicating that diazepam is
still used in an emergency.
10
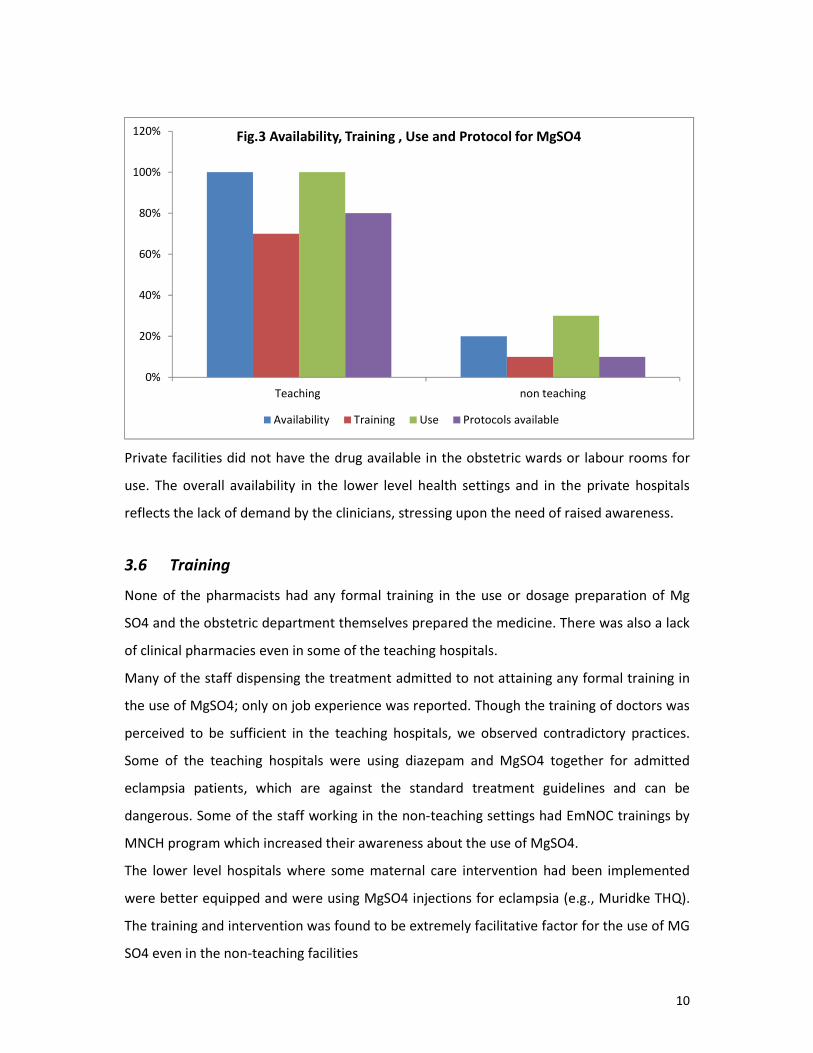
Private facilities did not have the drug available in the obstetric wards or labour rooms for
use. The overall availability in the lower level health settings and in the private hospitals
reflects the lack of demand by the clinicians, stressing upon the need of raised awareness.
3.6 Training
None of the pharmacists had any formal training in the use or dosage preparation of Mg
SO4 and the obstetric department themselves prepared the medicine. There was also a lack
of clinical pharmacies even in some of the teaching hospitals.
Many of the staff dispensing the treatment admitted to not attaining any formal training in
the use of MgSO4; only on job experience was reported. Though the training of doctors was
perceived to be sufficient in the teaching hospitals, we observed contradictory practices.
Some of the teaching hospitals were using diazepam and MgSO4 together for admitted
eclampsia patients, which are against the standard treatment guidelines and can be
dangerous. Some of the staff working in the non-teaching settings had EmNOC trainings by
MNCH program which increased their awareness about the use of MgSO4.
The lower level hospitals where some maternal care intervention had been implemented
were better equipped and were using MgSO4 injections for eclampsia (e.g., Muridke THQ).
The training and intervention was found to be extremely facilitative factor for the use of MG
SO4 even in the non-teaching facilities
0%
20%
40%
60%
80%
100%
120%
Teaching non teaching
Fig.3 Availability, Training , Use and Protocol for MgSO4
Availability Training Use Protocols available

11
Most of the doctors found the dosage preparation to be the biggest barrier to the use of the
medicine as they have to recall, calculate and prepare the dosage themselves.
3.7 Awareness and Practices of Health Professionals
There are certain clinical requirements for the use of magnesium sulfate, which include the
availability of infusion pumps for I/v use, dosage preparation, availability of the antidote
calcium gluconate and understanding the contra-indication to use especially alongside
diazepam. Magnesium levels are not required routinely for its use. This clearly demonstrates
that NEML and clinical guidelines only cannot solve the problem but that procedures need
to be in place at facility level, staff trained and equipment available.
Against the backdrop that most of the doctors and midwives were trained in the use of
diazepam, or 'lytic' cocktail as anticonvulsants for pre-eclampsia and eclampsia, majority of
the health professionals were aware of the usefulness of Mg SO4 as the first line treatment
for eclampsia, many had no knowledge of its use in severe pre eclampsia. One of the tertiary
care hospitals where MgSO4 was being used for severe pre-eclampsia, had been part of the
international MAGPIE trial. In addition to the reduced morbidity and mortality in severe pre-
eclampsia, obstetrician expressed that it also helped in prolonging the pregnancy duration,
leading to better fetal outcome. Most of the facilities using MgSO4 were not doing
magnesium levels.
Due to less numbers of the eclampsia patients entertained in some of the smaller level of
facilities, there is lack of recent knowledge and experience which is another potential barrier
to effective administration of MgSO4 and would highlight the need for frequent refresher
courses and other educational reminders, to ensure appropriate diagnosis and treatment.
There was a” Fear” of using Mg SO4 among the health professionals. The staff in many of
the THQs and BHUs immediately referred the convulsing patients without any emergency
management as they felt inadequate. There were no referral guidelines available for
use.The relatives would sometimes take the woman directly to a tertiary care even if was far
off, leading to repeated convulsions and higher morbidity and mortality when they do reach
the tertiary care setting.

12
The obstetricians felt that trained staff for dosage
preparation and monitoring of the toxicity is a
necessary pre- requisite for Mg SO4 use and hence
none of the obstetricians were using it in private
settings. The injection was mostly prepared by the
doctors and in some cases by the nurses in the
institutions. There was a misconception that this
drug can only be used in advanced settings with
intensive care availability. When asked whether primary health care should be using Mg
SO4, majority agreed to the benefit to women but stressed the need for proper training and
availability of pre- dosage calculated packs. There are concerns of magnesium sulfate
toxicity especially among the older generation of physicians.
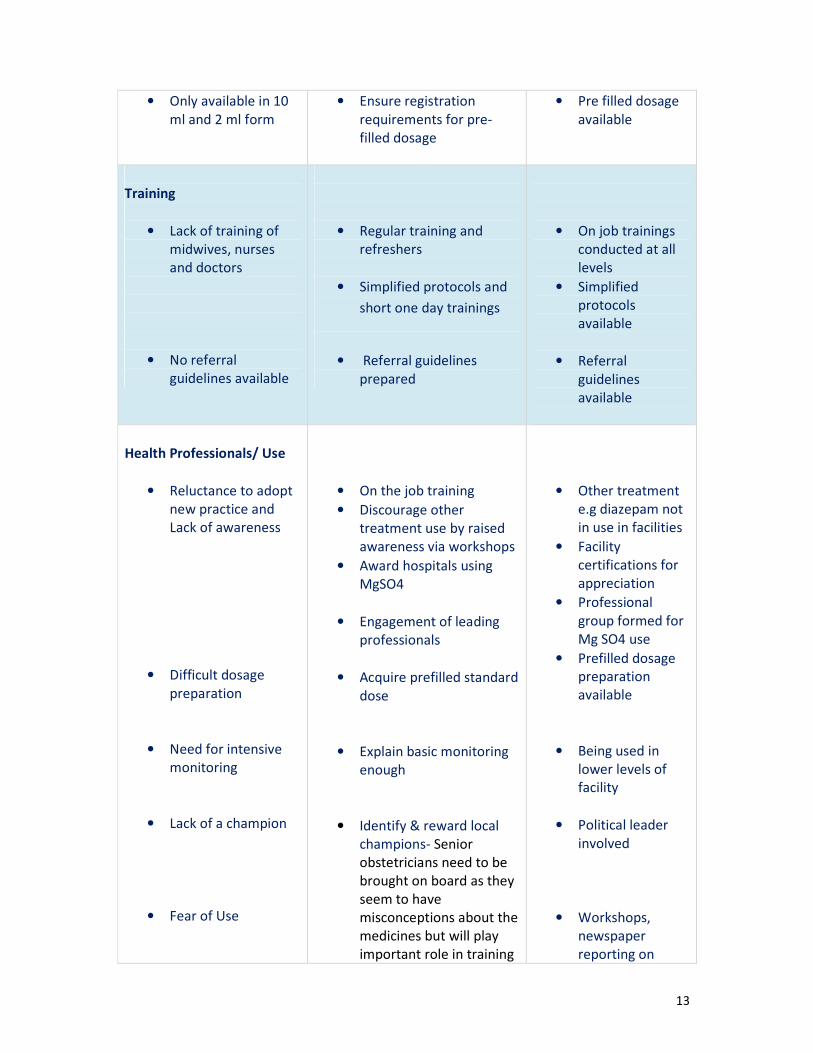
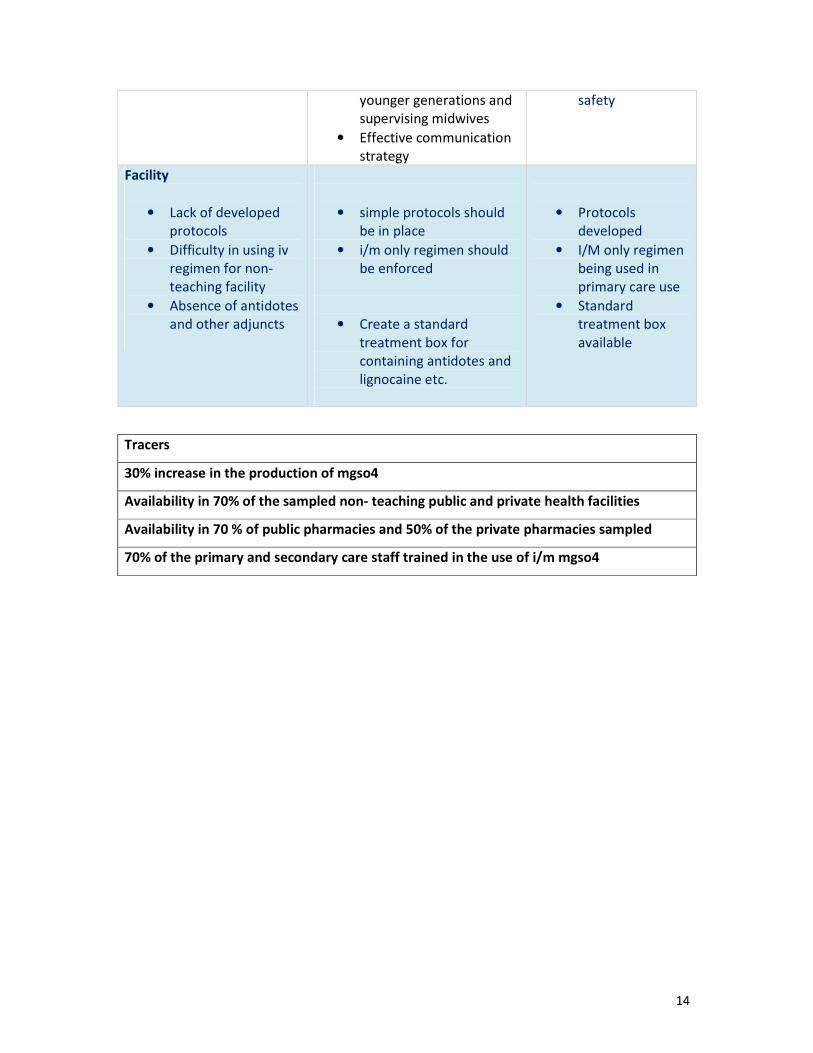
Table I. Summarizes the barriers and identifies actions needed
Table1. Barriers to the use of MgSO4, Recommendations and follow-up in Pakistan
Barriers Identified Recommendations Follow up Indicators
Policy
• No clear national
treatment guidelines
for MgSO4 use in
eclampsia / severe
pre-eclampsia
• Not included in the
Best Practices
• Pre/eclampsia
specifically, not a
priority on public
health agendas
• Preparation of Standard
national treatment
guidelines for MgSO4 use
• Develop Pakistan specific
standards of care based
on WHO guidelines &
area best practices for
MgSO4.
• Raise awareness of the
disease,
Show the “burden of the
disease
• Available
Standard national
treatment
guidelines for
MgSO4 use
• Included in the
Best practices
• Meetigs and
seminars
conducted
Supply, procurement and
distribution
• Interrupted supply in
some provinces
• Ensure uninterrupted
supplies
• Availability in the
facilities all year
“ I lost one patient because the i/v
infusion was turned fast by a
relative, So I will never use it as it
is not safe without monitoring”
( An obstetrician at a DHQ)
13
• Only available in 10
ml and 2 ml form
• Ensure registration
requirements for pre-
filled dosage
• Pre filled dosage
available
Training
• Lack of training of
midwives, nurses
and doctors
• No referral
guidelines available
• Regular training and
refreshers
• Simplified protocols and
short one day trainings
• Referral guidelines
prepared
• On job trainings
conducted at all
levels
• Simplified
protocols
available
• Referral
guidelines
available
Health Professionals/ Use
• Reluctance to adopt
new practice and
Lack of awareness
• Difficult dosage
preparation
• Need for intensive
monitoring
• Lack of a champion
• Fear of Use
• On the job training
• Discourage other
treatment use by raised
awareness via workshops
• Award hospitals using
MgSO4
• Engagement of leading
professionals
• Acquire prefilled standard
dose
• Explain basic monitoring
enough
• Identify & reward local
champions- Senior
obstetricians need to be
brought on board as they
seem to have
misconceptions about the
medicines but will play
important role in training
• Other treatment
e.g diazepam not
in use in facilities
• Facility
certifications for
appreciation
• Professional
group formed for
Mg SO4 use
• Prefilled dosage
preparation
available
• Being used in
lower levels of
facility
• Political leader
involved
• Workshops,
newspaper
reporting on
14
younger generations and
supervising midwives
• Effective communication
strategy
safety
Facility
• Lack of developed
protocols
• Difficulty in using iv
regimen for non-
teaching facility
• Absence of antidotes
and other adjuncts
• simple protocols should
be in place
• i/m only regimen should
be enforced
• Create a standard
treatment box for
containing antidotes and
lignocaine etc.
• Protocols
developed
• I/M only regimen
being used in
primary care use
• Standard
treatment box
available
Tracers
30% increase in the production of mgso4
Availability in 70% of the sampled non- teaching public and private health facilities
Availability in 70 % of public pharmacies and 50% of the private pharmacies sampled
70% of the primary and secondary care staff trained in the use of i/m mgso4

15
4. Discussion
Before undertaking any intervention to improve the management of eclampsia and severe
eclampsia a thorough understanding of the local situation is needed .Our study is the first of
its kind where we tried to assess the barriers to the use of MgSO4 both in public and private
settings of Pakistan using a mixed method approach. The qualitative discussions with the
health professionals have added depth to the understanding of the barriers. The sample
includes data from rural, urban, public and private sector hospitals in each province which
adds generalizability to the results. The barriers identified included the lack of clinical
guidelines from the Ministry of Health on the use of magnesium sulphate, lack of a clinical
champion, clinicians' ease with previous use of other drugs to manage eclampsia, difficult
dosage calculation and constraints on equipment, human resources and their training.
The teaching hospitals were getting the maximum load of eclampsia and severe pre
eclampsia patients, some getting as many as 2-3 per week. The tertiary care facility staff
feels that the patients referred to them are not given any emergency treatment at the first
level of care, hence the need to include referral guidelines as an important component of
national guidelines. The data from the clinical records and the anecdotes from staff
suggested that cases of pre-eclampsia and eclampsia were infrequent at small hospitals and
most of them were either referred or given alternative treatment for convulsions e.g.,
Diazepam as they were used to this treatment. Discrepancy between private and public
facilities, in the availability of treatment with magnesium sulfate is another issue to be
resolved.
This study highlights the importance of translating evidence base into policy and action for
meaningful outcome. There is a need to proliferate the use of this life saving medicine
outside the tertiary care settings to reduce mortality, as a very significant portion of the
maternal deaths from eclampsia reported from many developing countries are among
women who had multiple seizures outside the hospital and those without prenatal carexii
*.
In Pakistan majority of women do not have access to services where preeclampsia could
likely be diagnosed or have contact with professionals who could administer magnesium
sulfate. There is a shortage of human resource for health, an insufficient number of qualified
clinicians to monitor the use of magnesium sulfate or even to prescribe the drug in
peripheral hospitals but training the available resource can reduce adverse maternal
16
outcomes. The misconception that intensive hospital care is involved with providing Mg SO4
was a barrier and should be dispelled.
The small sample size may be a limitation of the study, but gives us a quick review of the
situation in different provinces. A large portion of the sample was the teaching hospitals
which give an optimistic view and does not reflect the current situation in smaller settings.
The diagnostic criteria for severe preeclampsia and eclampsia as well as the available
equipment for the diagnosis were not assessed.
The implication from the study is that MgSO4 is still not in widespread use. The public and
private sector hospitals and stake holders like the general practitioners and midwives need
the information, training and encouragement. It is important to disseminate these findings
to policy makers, program managers, obstetricians, and even journalists.
The cost effectiveness of the medicine should be assessed in light of its low cost, expenses
on the diagnosis of severe pre-eclampsia and eclampsia, monitoring costs, hospital stay
costs and death and long term morbidity prevention costs. Scaling up its use in Pakistan, by
addressing the barriers will significantly advance the safe motherhood agenda and thereby
add to our accomplishing the millennium development goals.

17
5. Recommendations
The desired use of magnesium sulfate in Pakistan would need ownership, commitment and
a dedicated group of professionals. This has to be a priority in the policy recommendations
and in public health arena. Awareness raising, guidelines preparation for easy use, trainings,
inclusion in the best practices, introduction of the I/M only regimen for lower level of health
facilities, uninterrupted supply and availability of pre filled dosage preparation will be a few
steps towards achieving the goal. Separate MgSO4 guidelines should be developed and
Ministry of Health should take a lead in implementation. Guidelines should be displayed at
the health facilities. Orientation sessions should be organized. Dissemination workshops
should be organized at district level. There should be multiple suppliers from
pharmaceutical industry. MgSO4 Kits should be locally prepared with instructions in local
language. Moreover injections should be ready to use with no preparation required. Those
who are practicing should be the role models and the facilities using the medicines should
be offered some kind of certification and reward. Clear guidelines should exit for safe
referral of patients after receiving emergency treatment.
There is a need for advocacy for the use of magnesium sulfate. Involvement of professional
and civil society, identifying a champion, political participation and policy briefs are the way
forward in this direction.
18
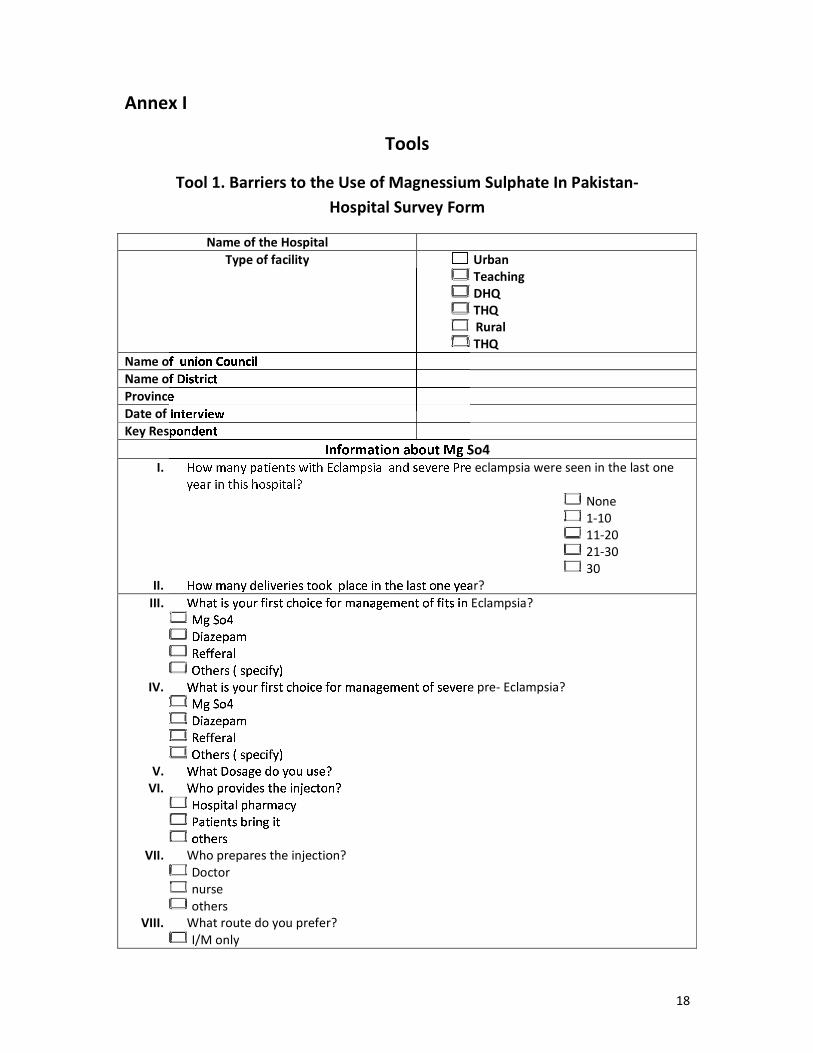
Annex I
Tools
Tool 1. Barriers to the Use of Magnessium Sulphate In Pakistan-
Hospital Survey Form
Name of the Hospital
Type of facility Urban
Teaching
DHQ
THQ
Rural
THQ
Name of union Council
Name of District
Province
Date of Interview
Key Respondent
Information about Mg So4
I. How many patients with Eclampsia and severe Pre eclampsia were seen in the last one
year in this hospital?
None
1-10
11-20
21-30
30
II. How many deliveries took place in the last one year?
III. What is your first choice for management of fits in Eclampsia?
Mg So4
Diazepam
Refferal
Others ( specify)
IV. What is your first choice for management of severe pre- Eclampsia?
Mg So4
Diazepam
Refferal
Others ( specify)
V. What Dosage do you use?
VI. Who provides the injecton?
Hospital pharmacy
Patients bring it
others
VII. Who prepares the injection?
Doctor
nurse
others
VIII. What route do you prefer?
I/M only
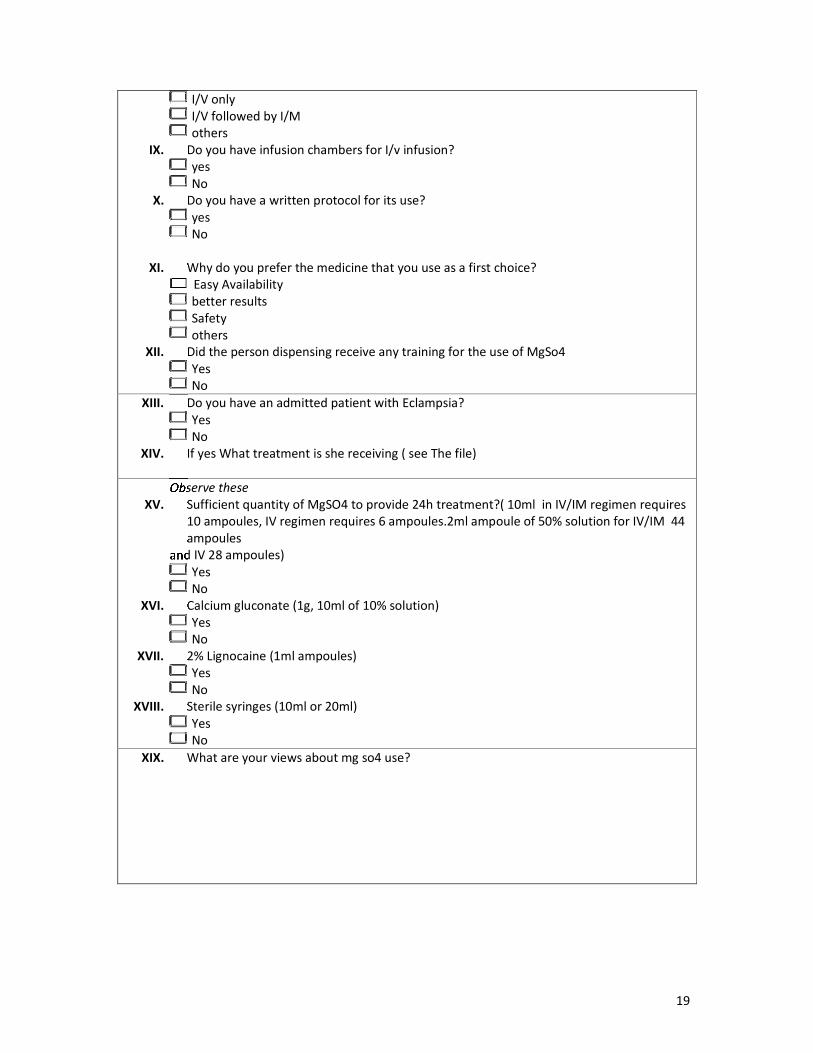
19
I/V only
I/V followed by I/M
others
IX. Do you have infusion chambers for I/v infusion?
yes
No
X. Do you have a written protocol for its use?
yes
No
XI. Why do you prefer the medicine that you use as a first choice?
Easy Availability
better results
Safety
others
XII. Did the person dispensing receive any training for the use of MgSo4
Yes
No
XIII. Do you have an admitted patient with Eclampsia?
Yes
No
XIV. If yes What treatment is she receiving ( see The file)
Observe these
XV. Sufficient quantity of MgSO4 to provide 24h treatment?( 10ml in IV/IM regimen requires
10 ampoules, IV regimen requires 6 ampoules.2ml ampoule of 50% solution for IV/IM 44
ampoules
and IV 28 ampoules)
Yes
No
XVI. Calcium gluconate (1g, 10ml of 10% solution)
Yes
No
XVII. 2% Lignocaine (1ml ampoules)
Yes
No
XVIII. Sterile syringes (10ml or 20ml)
Yes
No
XIX. What are your views about mg so4 use?
20
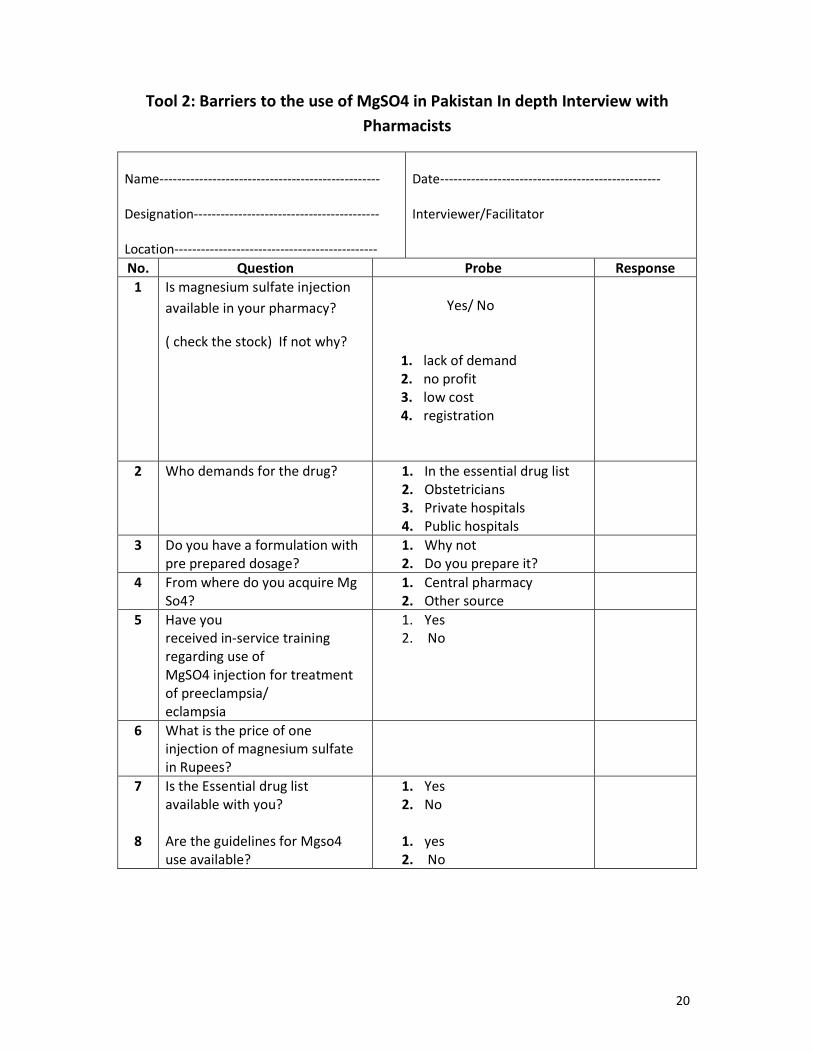
Tool 2: Barriers to the use of MgSO4 in Pakistan In depth Interview with
Pharmacists
Name--------------------------------------------------
Designation------------------------------------------
Location----------------------------------------------
Date--------------------------------------------------
Interviewer/Facilitator
No. Question Probe Response
1 Is magnesium sulfate injection
available in your pharmacy?
( check the stock) If not why?
Yes/ No
1. lack of demand
2. no profit
3. low cost
4. registration
2 Who demands for the drug? 1. In the essential drug list
2. Obstetricians
3. Private hospitals
4. Public hospitals
3 Do you have a formulation with
pre prepared dosage?
1. Why not
2. Do you prepare it?
4 From where do you acquire Mg
So4?
1. Central pharmacy
2. Other source
5 Have you
received in-service training
regarding use of
MgSO4 injection for treatment
of preeclampsia/
eclampsia
1. Yes
2. No
6 What is the price of one
injection of magnesium sulfate
in Rupees?
7
8
Is the Essential drug list
available with you?
Are the guidelines for Mgso4
use available?
1. Yes
2. No
1. yes
2. No
21
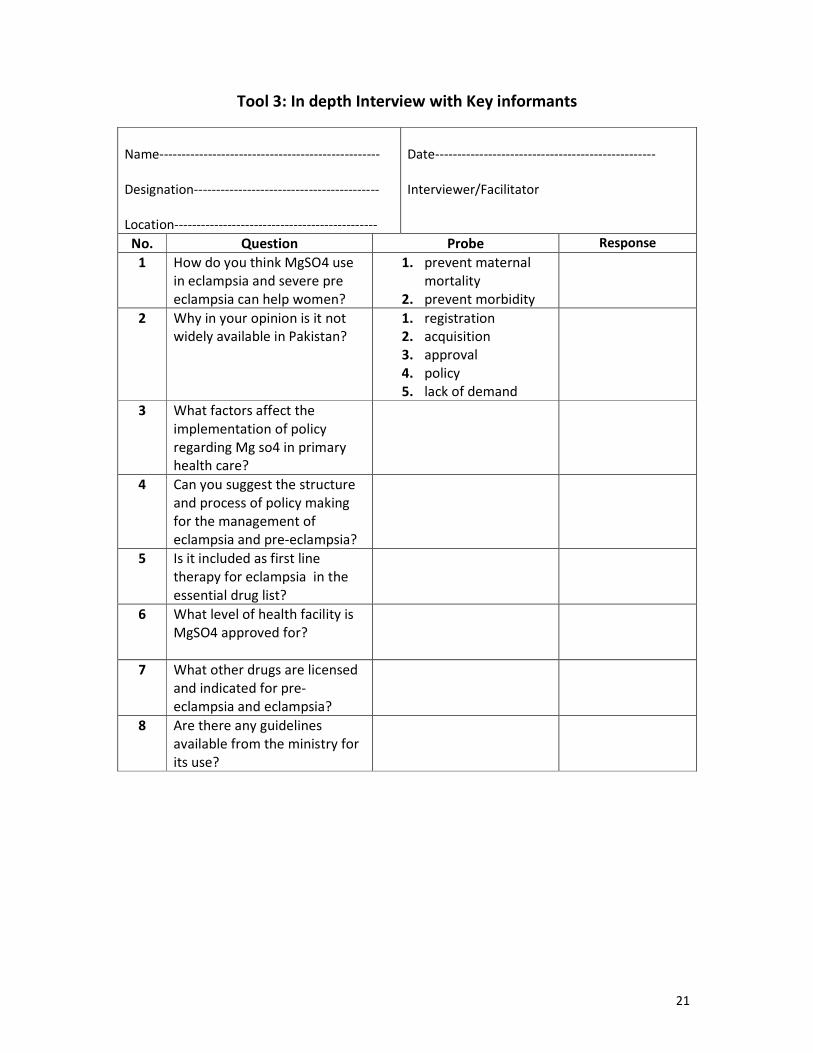
Tool 3: In depth Interview with Key informants
Name--------------------------------------------------
Designation------------------------------------------
Location----------------------------------------------
Date--------------------------------------------------
Interviewer/Facilitator
No. Question Probe Response
1 How do you think MgSO4 use
in eclampsia and severe pre
eclampsia can help women?
1. prevent maternal
mortality
2. prevent morbidity
2 Why in your opinion is it not
widely available in Pakistan?
1. registration
2. acquisition
3. approval
4. policy
5. lack of demand
3 What factors affect the
implementation of policy
regarding Mg so4 in primary
health care?
4 Can you suggest the structure
and process of policy making
for the management of
eclampsia and pre-eclampsia?
5 Is it included as first line
therapy for eclampsia in the
essential drug list?
6 What level of health facility is
MgSO4 approved for?
7 What other drugs are licensed
and indicated for pre-
eclampsia and eclampsia?
8 Are there any guidelines
available from the ministry for
its use?
22
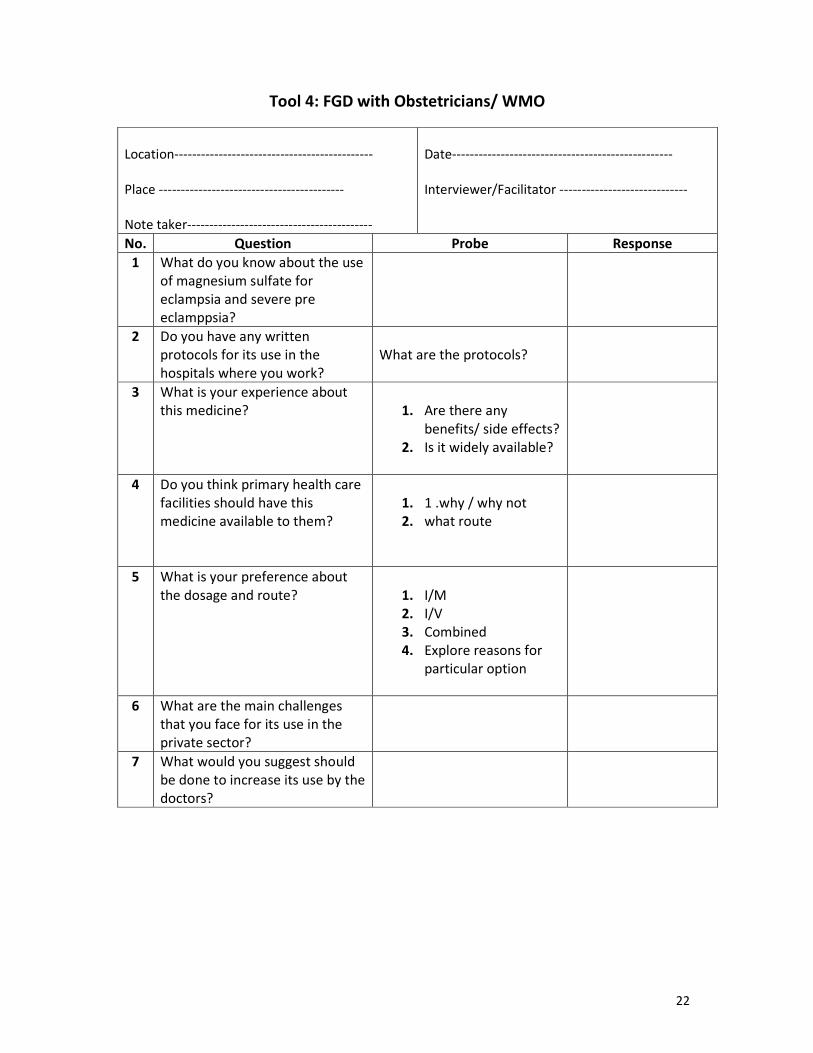
Tool 4: FGD with Obstetricians/ WMO
Location---------------------------------------------
Place ------------------------------------------
Note taker------------------------------------------
Date--------------------------------------------------
Interviewer/Facilitator -----------------------------
No. Question Probe Response
1 What do you know about the use
of magnesium sulfate for
eclampsia and severe pre
eclamppsia?
2 Do you have any written
protocols for its use in the
hospitals where you work?
What are the protocols?
3 What is your experience about
this medicine?
1. Are there any
benefits/ side effects?
2. Is it widely available?
4 Do you think primary health care
facilities should have this
medicine available to them?
1. 1 .why / why not
2. what route
5 What is your preference about
the dosage and route?
1. I/M
2. I/V
3. Combined
4. Explore reasons for
particular option
6 What are the main challenges
that you face for its use in the
private sector?
7 What would you suggest should
be done to increase its use by the
doctors?
23
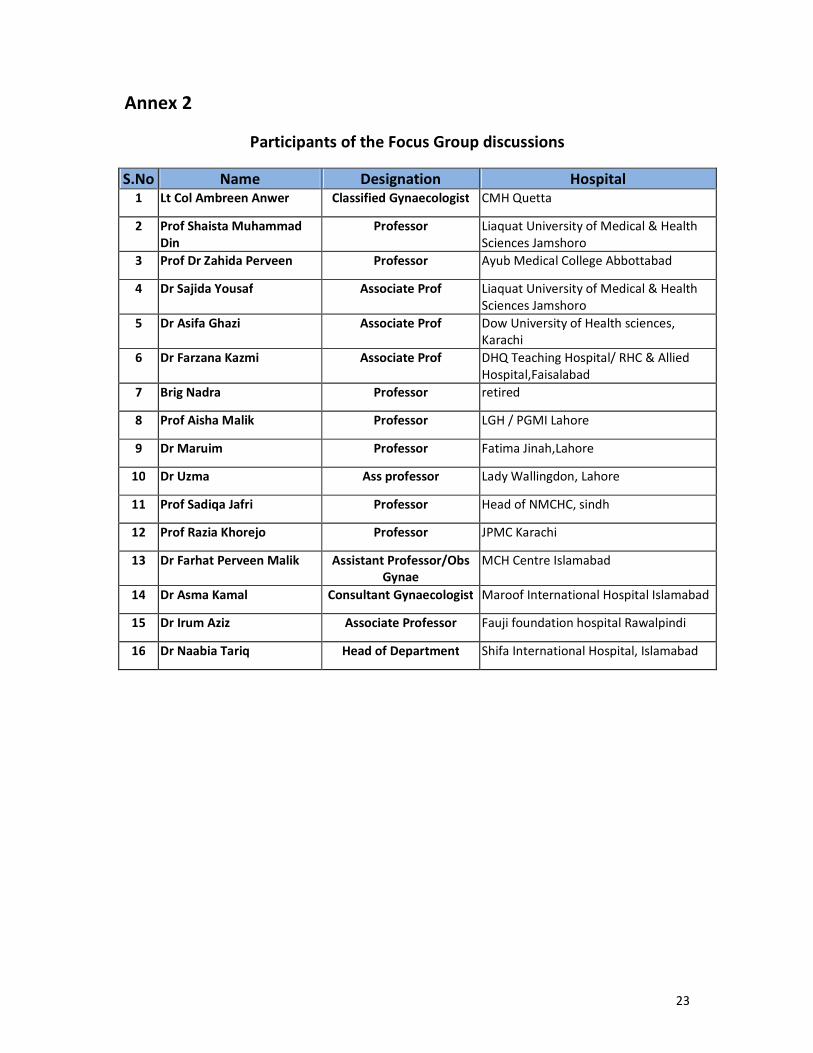
Annex 2
Participants of the Focus Group discussions
S.No Name Designation Hospital 1 Lt Col Ambreen Anwer Classified Gynaecologist CMH Quetta
2 Prof Shaista Muhammad
Din
Professor Liaquat University of Medical & Health
Sciences Jamshoro
3 Prof Dr Zahida Perveen Professor Ayub Medical College Abbottabad
4 Dr Sajida Yousaf Associate Prof Liaquat University of Medical & Health
Sciences Jamshoro
5 Dr Asifa Ghazi Associate Prof Dow University of Health sciences,
Karachi
6 Dr Farzana Kazmi Associate Prof DHQ Teaching Hospital/ RHC & Allied
Hospital,Faisalabad
7 Brig Nadra Professor retired
8 Prof Aisha Malik Professor LGH / PGMI Lahore
9 Dr Maruim Professor Fatima Jinah,Lahore
10 Dr Uzma Ass professor Lady Wallingdon, Lahore
11 Prof Sadiqa Jafri Professor Head of NMCHC, sindh
12 Prof Razia Khorejo Professor JPMC Karachi
13 Dr Farhat Perveen Malik Assistant Professor/Obs
Gynae
MCH Centre Islamabad
14 Dr Asma Kamal Consultant Gynaecologist Maroof International Hospital Islamabad
15 Dr Irum Aziz Associate Professor Fauji foundation hospital Rawalpindi
16 Dr Naabia Tariq Head of Department Shifa International Hospital, Islamabad
24
Annex 3
List of health Facilities surveyed for the study
S.No Name of facility Type of Facility/ service
Baluchistan
1 Sandeman Provicial Hospital Quetta Teaching hospital
2 Akram Hospital Quetta Private, Comprehensive EmONC
3 CMH Quetta Teaching hospital
Khaibar Pakhtun khawah
4 Khyber Teaching Hospital Peshawar Teaching Hospital
5 THQ Dargai, Malakand Agency Comprehensive EmONC
Punjab
6 Pakistan Institute of Medical Sciences,
Islamabad
Teaching Hospital
7 THQ hospital Muredke, sheikhupura Comprehensive EmONC
8 CDA DHQ hospital, Islamabad Comprehensive EmONC
9 THQ kahuta, Rawalpindi Comprehensive EmONC
10 THQ Nankana Basic EmOnC
11 Ali Hospital, Islamabad Private, Comprehensive EmONC
Sindh
12 Jinnah Postgraduate Medical Institute, Karachi Teaching Hospital
13 Sheikh Zayed hospital,Mir Pur Sakro Comprehensive EmONC
14 THQ Umerkot Basic EmONC
15 Gharo Rural Health Centre Mirpur sakro Basic EmONC
25
References:
i Dolea C, AbouZahr C: Global burden of hypertensive disorders of pregnancy in the year 2000. Global
Burden of Diseases 2000 Working Paper. Geneva: World Health Organization; 2003.
ii Duley L,Gülmezoglu A, Henderson-Smart D. Magnesium sulphate and other anticonvulsants for
women with pre-eclampsia. Cochrane Database Syst Rev 2003(2): CD000025.
iii
Magpie Trial Collaborative Group. Do women with pre-eclampsia, and their babies, benefit from
magnesium sulphate? The magpie trial: a randomised placebo-controlled trial. Lancet 2002; 359:
187790
iv Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence
from the collaborative eclampsia trial. Lancet 1995; 345: 145563.
v WHO Model List of Essential Medicines
[http://www.who.int/medicines/services/essmedicines_def/en/index.html]
vi Simon, J., Gray, A., Duley, L. and Magpie Trial Collaborative Group (2006), Cost-effectiveness of
prophylactic magnesium sulphate for 9996 women with pre-eclampsia from 33 countries: economic
evaluation of the Magpie Trial. BJOG: An International Journal of Obstetrics & Gynaecology, 113:
144–151.
vii
Sevene, E; Lewin, S; Mariano, A; Woelk, G; Oxman, AD; Matinhure, S; Cliff, J; Fernandes, B; Daniels,
K: System and market failures: the unavailability of magnesium sulphate for the treatment of
eclampsia and pre-eclampsia in Mozambique and Zimbabwe. BMJ 2005, 331:765-769.
viii
Aaserud M, Lewin S, Innvar S, Paulsen EJ, Dahlgren AT, Trommald M, Duley L, Zwarenstein M,
Oxman A: Translating research into policy in developing countries: a case study of magnesium
sulphate for pre-eclampsia. BMC Health Services Research 2005, 5: 68.
ix Flottorp S, Oxman A: Identifying barriers and tailoring interventions to improve the management of
urinary tract infections and sore throat: a pragmatic study using qualitative methods. BMC Health
Services Research 2003, 3: 3. x Sibai BM. Diagnosis, Prevention, and Management of Eclampsia. Am J Obstet Gynecol
2005;105(2):402-410 xi Bissallah A Ekele, Danjuma Muhammed, Lawal N Bello, and Ibrahim M Namadina .Magnesium
sulphate therapy in eclampsia: the Sokoto (ultra short) regimen BMC Res Notes. 2009; 2: 165 xii
Sibai BM. Diagnosis, Prevention, and Management of Eclampsia. Am J Obstet Gynecol
2005;105(2):402-410 and Katz VL, et al. Preeclampsia into eclampsia: toward a new paradigm. Am
J Obstet Gynecol 2000; 182:1389-96


















![Aluminium Sulphate[1]](https://img.pdfslide.us/doc/110x75/563db7b2550346aa9a8d1fe5/aluminium-sulphate1.jpg)










