Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
Worldviews on Evidence-Based Nursing
Volume 14, Issue 6, Virtual Issue
Published December 2017
Barriers to and Best Practices in Advancing Evidence-based Care
Edited By: Bernadette Melnyk
Impact Factor: 2.103
ISI Journal Citation Reports © Ranking: 2016: 11/116 (Nursing)
Online ISSN: 1741-6787
Associated Titles: Journal of Nursing Scholarship
© Sigma Theta Tau International
From the Editor
An abundance of studies have been published that demonstrate when patients receive
evidence-based care, their outcomes substantially improve. Further, consistent implementation
of evidence-based practice by all healthcare providers would result in achieving the quadruple
aim in healthcare, including improving the patient experience through high quality care,
enhancing population health, reducing costs, and empowering clinicians to be more engaged
and satisfied in their roles. This virtual edition of Worldviews contains a landmark series of
studies that further describe some of the existent barriers in healthcare systems that prevent the
advancement of evidence-based practice along with studies that highlight interventions and
factors that propel its implementation and sustainability. As always, Worldviews links the
research presented in its publications with recommended action tactics so readers can put the
evidence in active practice to improve outcomes. Enjoy reading and make use of this virtual
edition.
Bernadette Mazurek Melnyk
PhD, RN, CPNP/PMHNP, FAANP, FNAP, FAAN
Original Article
A Study of Chief Nurse Executives IndicatesLow Prioritization of Evidence-Based Practiceand Shortcomings in Hospital PerformanceMetrics Across the United StatesBernadette Mazurek Melnyk, RN, PhD, FNAP, FAANP, FAAN •Lynn Gallagher-Ford, RN, PhD, DPFNAP, NE-BC • Bindu Koshy Thomas, MEd, MS •Michelle Troseth, RN, MSN, DPNAP, FAAN • Kathy Wyngarden, RN, MSN, FNP •Laura Szalacha, EdD
Keywords
evidence-basedpractice,
chief nurse,nurse executive,
performancemetrics,
health care
ABSTRACTBackground: Although findings from studies indicate that evidence-based practice (EBP) results inhigh-quality care, improved patient outcomes, and lower costs, it is not consistently implementedby healthcare systems across the United States and globe.
Aims: The purpose of this study was to describe: (a) the EBP beliefs and level of EBP implementa-tion by chief nurse executives (CNEs), (b) CNEs’ perception of their hospitals’ EBP organizationalculture, (c) CNEs’ top priorities, (d) amount of budget invested in EBP, and (e) hospital perfor-mance metrics.
Methods: A descriptive survey was conducted. Two-hundred-seventy-six CNEs across the UnitedStates participated in the survey. Valid and reliable measures included the EBP Beliefs scale,the EBP Implementation scale, and the Organizational Culture and Readiness scale for EBP.The Centers for Medicare and Medicaid Services Core Measures and the National Database ofNursing Quality Indicators (NDNQI) were also collected.
Results: Data from this survey revealed that implementation of EBP in the practices of CNEs andtheir hospitals is relatively low. More than one-third of the hospitals are not meeting NDNQIperformance metrics and almost one-third of the hospitals are above national core measuresbenchmarks, such as falls and pressure ulcers.
Linking Evidence to Action: Although CNEs believe that EBP results in high-quality care, it isranked as a low priority with little budget allocation. These findings provide a plausible explana-tion for shortcomings in key hospital performance metrics. To achieve higher healthcare qualityand safety along with decreased costs, CNEs and hospital administrators need to invest in pro-viding resources and an evidence-based culture so that clinicians can routinely implement EBPas the foundation of care.
INTRODUCTIONThe evidence is irrefutable: findings from multiple studies indi-cate that evidence-based practice (EBP), compared to care that issteeped in tradition, leads to: (a) a higher quality and reliabilityof health care, (b) improved population health and patient out-comes, including the patient care experience, and (c) reducedcosts, now referred to as the Triple Aim in health care in theUnited States (Fielding & Briss, 2006; McGinty & Anderson,2008; Melnyk, Fineout-Overholt, Gallagher-Ford, & Kaplan,2012). Despite findings from research supporting the benefitsof evidence-based care and its emphasis in the Affordable CareAct, it is not the standard of practice implemented by manyclinicians and healthcare systems across the United States and
the globe due to multiple barriers that continue to be a deterrentto the translation of research findings into real-world practicesettings (Fink, Thompson, & Bonnes, 2005; Harding, Porter,Horne-Thompson, Donley, & Taylor, 2014; Melnyk, Fineout-Overholt et al., 2012). Among these barriers are: (a) inadequateknowledge and skills in EBP by clinicians, (b) lack of EBPmentors and practice facilitators, (c) misconceptions that EBPtakes too much time, (d) cultures and environments that do notsupport EBP, (e) inadequate resources, and (f) lack of expec-tations and organizational mandates to implement evidence-based care (Harding et al., 2014; Melnyk, Fineout-Overholtet al., 2012; Melnyk et al., 2012; Nagykaldi, Mold, Robinson,Niebauer, & Ford, 2006). Therefore, it is doubtful that the goal
6 Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14.C© 2016 Sigma Theta Tau International
Original Articleset by the Institute of Medicine (IOM) that 90% of health-care decisions will be evidence-based by 2020 will be achievedunless urgent action is taken to transform current healthcaresystems across the United States (2008).
EBP is a problem-solving approach to clinical decision-making in health care that integrates the best evidence fromwell-designed studies with a clinician’s expertise, which in-cludes internal evidence from patient assessments and practicedata, and a patient’s preferences and values (Melnyk & Fineout-Overholt, 2015). In the landmark summit sponsored by theIOM on health professions education, it was recommendedthat all health professional educational programs should in-clude five competencies, including: (a) providing patient cen-tered care, (b) applying quality improvement principles, (c)working in interprofessional teams, (d) using EBPs, and (e)using health information technologies (IOM, 2003). However,challenges remain in the teaching of EBP in academic pro-grams throughout the United States as many faculty continueto teach health sciences students the rigorous process of howto conduct research instead of how to use research and consis-tently implement evidence-based care (Melnyk, 2013).
In a national survey by Melnyk et al. (2012) with a randomsample of over 1,000 nurses who were members of the Ameri-can Nurses Association, 74% of the respondents indicated theneed for additional education in EBP. Nurses in this surveyalso indicated the persistence of many of the same EBP bar-riers that have been reported for decades (e.g., lack of time,organizational culture, inadequate EBP knowledge and skills).However, one new barrier was identified that had not beenpreviously reported in the literature: manager and leader resis-tance to EBP. Respondents to the national survey expressed aneed for support from their leaders, managers, and interdisci-plinary colleagues in order to be able to implement EBP.
The literature has revealed that leaders who create a visionfor EBP in their organization provide resources to support itand incorporate evidence into their own leadership practices,thus having a key influence on the implementation of evidence-based care (Melnyk & Fineout-Overholt, 2015; Rycroft-Malone,2008). Although findings from a prior study indicated thatChief Nursing Officers (CNOs) and Chief Nursing Executives(CNEs) often believe in the value of evidence-based care, theirown implementation of EBP is low (Sredl et al., 2011). In addi-tion to these known challenges related to leadership and EBP,there are major gaps in the literature regarding how nursingleaders prioritize EBP and the extent to which they invest init. Therefore, a national (US) survey was conducted with CNEsand CNOs throughout the nation to: (a) fill this knowledge gap,(b) assess their EBP beliefs and level of EBP implementation,(c) evaluate their perceptions of organizational culture and en-vironment for EBP, and (d) describe performance metrics intheir healthcare systems. Data from this survey were also in-tended to inform appropriate next steps in working with CNEsand CNOs across the United States to advance and sustain EBPin their healthcare systems to ultimately improve patient careand outcomes.
METHODSThe study was an anonymous online survey of CNEs and CNOsthroughout the United States granted exempt status by the firstauthor’s institutional review board. Elsevier provided an e-maillist of 5,100 CNOs and CNEs, and an e-mail was sent to allof them with an invitation to complete the anonymous survey.Participants were provided a cover letter with a description ofthe study. The e-mail provided a link to the survey. A remindere-mail was sent 1 week following the first contact and anotherreminder was sent 1 day before the survey closed.
The survey participants were offered an incentive to partic-ipate in the study; an opportunity to enter a drawing for 1 of 10$100 gift cards. The gift card recipients were determined us-ing a computer-generated random number list. The recipientsreceived their gift card after the survey closed.
MeasuresData collected on the survey included: (a) demographic ques-tions; (b) three valid and reliable instruments that measuredbeliefs about EBP, EBP implementation, and perceived organi-zational culture of EBP; (c) CNE and CNO priorities and budgetinvestment in EBP, and (d) CMS Core Measures and NationalDatabase of Nursing Quality Indicators (NDNQI) measures.
EBP beliefs were measured with the EBP Beliefs (EBPB)scale, which taps beliefs about the value of EBP and the abilityto implement it (Melnyk, Fineout-Overholt, & Mays, 2008).This is a 16-item Likert-type scale ranging from 1 (strongly dis-agree) to 5 (strongly agree). Sample items include: “I am clearabout the steps in EBP,” “I am sure that I can implementEBP,” and “I am sure that evidence-based guidelines can im-prove care.” The summed total EBP score with higher scoresindicate stronger EBP beliefs. The EBPB scale has establishedface, content, and construct validity, with internal consistencyreliabilities typically above 0.85 (Melnyk et al., 2008).
Implementation of EBP was measured with the EBP Imple-mentation (EBPI) scale (Melnyk et al., 2008), which assessedthe extent to which the CNEs and CNOs implemented EBP.Participants respond to 18-item Likert-type scale items by an-swering how often in the last 8 weeks they have performed cer-tain EBP tasks, including: (a) generated a PICO question aboutmy practice, (b) used evidence to change my clinical practice,and (c) shared outcome data collected with colleagues. Itemscores are summed for a total score range from 0 to 72, withhigher scores indicating greater implementation of EBP. TheEBPI has established face, content, and construct validity withinternal consistency reliabilities reported at above 0.85 (Melnyket al., 2008).
Organizational culture was measured with the Organiza-tional Culture and Readiness for System-Wide Integration ofEBP (OCRSIEP) scale, which taps organizational culture andreadiness for EBP (Fineout-Overholt & Melnyk, 2003). Thisinstrument measures the extent to which cultural factors thatinfluence system-wide implementation of EBP exist in the en-vironment and the overall perceived readiness for integration
Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14. 7C© 2016 Sigma Theta Tau International
CNE Study: EBP & Performance Metrics
of EBP and how it compares to 6 months ago. Respondents areasked to indicate their agreement with each item on a 5-pointLikert-type scale, with 1 meaning none at all and 5 meaningvery much. Examples of items on the 26-item scale include:(a) To what extent is EBP clearly described as central to themission and philosophy of your institution? and (b) To whatextent do you believe that EBP is practiced in your institution?Items are summed to create a total score, ranging from 25 to125, with higher scores reflecting greater organizational readi-ness for and movement toward a culture of EBP. The scale hasestablished face and content validity, with internal consistencyreliabilities reported at above 0.85 (Melnyk, Fineout-Overholt,Giggleman, & Cruz, 2010).
CNE priorities and budget investment in EBP were assessedwith the following questions: (a) As a CNE, what are the topthree priorities that you are currently focused on in your role?and (b) What percent of your annual operating budget do youspend on building and sustaining EBP in your organization?
Data on core performance measures were gathered withthe following question: In your most recent core measuresreport, at which level did your nursing unit perform in the fol-lowing nurse-related measurements (e.g., catheter-associatedurinary tract infections, pressure ulcer stage III and IV, vascu-lar catheter-associated infections)? Response choices included“below national rate,” “same as national rate,” and “above na-tional rate.” Data on NDNQI measures were assessed withthe following question: In your most recent NDNQI report, atwhich level did your nursing department perform on the fol-lowing nurse sensitive indicators (e.g., falls, falls with injury,hospital-acquired pressure ulcers). Response choices included“below benchmark,” “at benchmark,” and “exceeding bench-mark.”
DATA ANALYSISBecause this was a descriptive national survey, descriptivestatistics (e.g., means, standard deviations, and percentages)were conducted on the study’s variables. Cronbach alphas werecomputed on the EBP scales used. Prior to beginning the study,a decision was made to only include data on fully completedsurveys in the analysis.
RESULTSA convenience sample of 5,100 e-mails from a data base ofCNEs and CNOs from Elsevier were disseminated, and 1,199(24%) were returned as undeliverable. Therefore, the actualsample comprised 3,901 CNEs and CNOs. Although 327 CNEsand CNOs started the survey (8%), it was fully completed by276 (a 7% response rate) who were from 45 states in the UnitedStates and the District of Columbia. Ninety-three percent ofthe respondents were currently in the chief nurse role andwere an average of 55 years of age. The majority were whiteand female, with over two-thirds having a master’s degree astheir highest level of education (Table 1). Sixty-eight percentof the hospitals had less than 301 beds and 18% had Mag-
Table 1. CNO and CNE & Organizational Demo-graphics
CNO/CNE Demographic Data Frequency Percent
Gender
Male 21 8%
Female 255 92%
Ethnicity
American Indian 2 1%
Asian 4 1%
African American 10 4%
White 260 94%
Education
Diploma 4 1%
Associate’s degree 5 2%
Bachelor’s degree 17 6%
Master’s degree 189 69%
PhD 22 8%
DNP 29 10%
Other 10 4%
Currently CNO/CNE
Yes 255 93%
No 21 7%
Age Minimum Maximum Average
32 68 55
Organizational data Percent
Size
Fewer than 100 beds 37%
100-300 beds 31%
301-500 beds 14%
501-800 beds 9%
801-1,000 beds 4%
Greater than 1,000 beds 4%
Other 1%
Magnet designated
Yes 18%
No 82%
BSN preparation
Less than 25% 26%
(Continued)
8 Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14.C© 2016 Sigma Theta Tau International
Original ArticleTable 1. Continued
CNO/CNE Demographic Data Frequency Percent
26-50% 42%
51-75% 26%
76-100% 6%
Nursing satisfaction
Very dissatisfied 1%
Somewhat dissatisfied 11%
Somewhat satisfied 62%
Satisfied 26%
net status designation, which is a credential awarded by theAmerican Nurses Credentialing Center to healthcare organiza-tions for quality patient care, nursing excellence, and innova-tions in nursing practice. More than two-thirds of the hospitals(n = 188) had less than 51% baccalaureate prepared nurses.Sixty-two percent (n = 172) of the CNEs and CNOs reportedthat their nurses were “somewhat satisfied” with only 73 CNEsand CNOs (26%) reporting that their nurses were “satisfied”on their nurse satisfaction surveys (Table 1).
Although the CNOs and CNEs’ beliefs about the value ofEBP were high (Table 2), approximately 25% were not clearabout the steps of EBP and nearly 44% reported that they werenot sure they could implement EBP in a time efficient man-ner. More than 50% of CNEs and CNOs believed that EBP ispracticed in their organization from “not at all” to “somewhat.”Furthermore, 48% of the chief nurses reported that they wereunsure of how to measure the outcomes of services deliveredto patients.
The CNEs and CNOs’ own implementation of EBP was low(Table 2). Specifically, over half of the CNEs and CNOs reportedthat they had not accessed important databases for evidence-based guidelines or systematic reviews of evidence during thepast 8 weeks. Organizational culture and readiness for EBPacross the hospitals was low to moderate (Table 2). Specifi-cally, nearly 60% of the chief nurses reported they believedEBP is practiced in their organizations “not at all” to “some-what.” In response to the question, “compared to 6 monthsago, how much movement in your organization has there beentoward EBP culture?” 52% of the chief nurses said “not at all”to “somewhat.” In response to the question on the EBP cul-ture scale regarding to what extent fiscal resources were usedto support EBP, 72% of the respondents said “not at all” to“somewhat.”
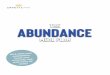
Regarding performance metrics, the chief nurses reportedthat more than one-third of their hospitals are not meetingbenchmarks for NDNQI measures (Figure 1), and almost one-
third of the hospitals are above national benchmarks for coremeasures (e.g., falls, pressure ulcers; Figure 2).
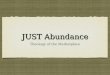
The top priorities as stated by the chief nurses were qualityand safety, yet EBP was cited as a top priority for only 3% of thechief nurses (Figure 3). Regarding budget, 74% of the CNOsand CNEs invested only 0% to 10% of their annual operatingbudgets on building and sustaining EBP in their organizations.
DISCUSSIONThe results of this survey indicate that, although the CNEsand CNOs reported that they believe in the value of EBP, theirown implementation of EBP is relatively low. More than halfof the CNEs and CNOs also reported that there is a low level ofevidence-based care practiced in their organizations. This lowlevel of EBP can be partially explained because the majority ofhospitals had less than a 51% baccalaureate prepared workforceand only 18% of the hospitals had achieved Magnet status. Inthe United States, research has supported that hospital out-comes (e.g., lower mortality and failure to rescue rates) are bet-ter with baccalaureate prepared nurses and they exhibit higherlevels of EBP than nonbaccalaureate prepared nurses (Aiken,Clarke, & Cheung, Sloane, & Silber, 2003; Wilson et al., 2015),which is the impetus for the IOM recommendation that 80%of nurses in the United States are baccalaureate prepared by2020 (IOM, 2011). Furthermore, a recent study of 136 Penn-sylvania hospitals (11 emerging Magnets and 125 non-Magnets)indicated that Magnet recognition is associated with significantimprovements over time in quality of the organization’s workenvironment as well as patient and nursing outcomes that ex-ceed those of non-Magnet hospitals, including fewer deathsper 1,000 patients (Kutney-Lee et al., 2015).
Although the CNEs and CNOs stated that their highest pri-orities were quality and safety, EBP was not listed as a toppriority and very little of their budgets were allocated to imple-menting and sustaining evidence-based care. These findingsprovide another explanation for the shortcomings revealed incore performance and NDNQI metrics in a substantial portionof the hospitals. The findings also indicate a disconnection orlack of understanding by chief nurses that EBP is a key driver toachieving quality and safety in health care. Without a prioritiza-tion on EBP and necessary investment in an infrastructure tosustain it by CNEs and CNOs and chief executive officers, keyquality and safety outcomes in healthcare systems are unlikelyto be achieved.
In order for the Triple Aim to be reached in the US health-care system, EBP needs to be the foundation of care deliveredby all healthcare professionals across disciplines, using an in-terprofessional team-based model of care. However, the litera-ture abounds with studies that indicate this type of practice isfar from reality. Findings from research have indicated that, al-though health professionals from a variety of disciplines believein the benefits of EBP, only a small percentage consistently usethis approach in caring for their patients (Harding et al., 2014;Melnyk, Fineout-Overholt et al., 2012; Melnyk et al., 2012). In
Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14. 9C© 2016 Sigma Theta Tau International
CNE Study: EBP & Performance Metrics
Table 2. CNO/CNE Scores on EBP Scales
Minimum Maximum
Possible Possible Standard
Score Score Mean Deviation
EBPB scale 16 80 60.17 11.22
EBPI scale 0 72 27.8 14.97
Organizational culture & readiness scale 14 70 41.9 11.80
0%
10%
20%
30%
40%
50%
60%
Falls Falls withinjury
Pressureulcers
Pressureulcers (Stage2 and above)
Restraints Nursing carehours
RN education RNcertification
Below benchmark
At benchmark
Exceeding benchmark
Figure 1. NDNQI Metrics.
a recent study, Harding and colleagues (2014) found that bothclinicians and managers did not view EBP as a core componentof clinical care because higher priorities took precedent (e.g.,maintaining patient flow).
Although nurse executive leadership competencies includethe implementation and sustainability of evidence-based im-provements in quality and costs, including creating structuresto ensure access to information, resources, and support (Amer-ican Organization of Nurse Executives, 2004; Everett & Sitter-ding, 2011), this study reflects that these executive activitiesare not routinely occurring in real-world clinical organizations.Nurse executives must be provided with the knowledge thatEBP should be the consistent foundation of care delivery be-cause it is linked to improved outcomes, which are measurableand meaningful returns on the investment in EBP. This knowl-edge would assist chief nurses in understanding the value ofallocating more of their budgets to creating an infrastructure
to support and sustain EBP. Nurse executives also must beactively engaged in EBP in their own decision making androle model it for their directors, managers, and point of carestaff as prior research has indicated that role modeling andvaluing of research by nursing management increases the useof evidence in practice (Gifford, Davies, Edwards, Griffin, &Lybanon, 2007).
It is critical for nursing and other interprofessional health-care executives to build a culture and environment that sup-ports the implementation and sustainability of evidence-basedcare in order to achieve best outcomes, which includes the pro-vision of necessary EBP resources and tools (Melnyk, 2014a;Rycroft-Malone et al., 2013). Organizations need to provideevidence that their policies and procedures are based uponthe best evidence and that clinicians are provided with rig-orous evidence-based guidelines and mechanisms to supporttheir implementation. Evidence-based councils comprised of
10 Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14.C© 2016 Sigma Theta Tau International
Original Article
0%
10%
20%
30%
40%
50%
60%
Catheter associatedurinary tractinfections
Pressure ulcers(Stage 3 and 4)
Vascular catheterassociated infections
Falls and trauma Manifestations ofpoor glycemic
control
Below national rate
Same as national rate
Above national rate
Figure 2. Core Measures.
0%
5%
10%
15%
20%
25%
Quality Patient safety Benchmarks Finance Recruitmentand retention
Staffing Patientsatisfaction
Vision/culture Evidence-basedpractice
Summarized from the survey question: “As a CNO/CNE, what are the top 3 priorities that you are currently focused on in your role?”
Figure 3. CNO/CNE Top Priorities.
transdisciplinary clinicians also can be instrumental for en-hancing EBP throughout the organization through an inter-professional team-based approach, which has been supportedto lead to a higher quality of care. Research supports that trans-disciplinary teamwork leads to a higher quality of care and bet-ter patient outcomes (Raab, Will, Richards, & O’Mara, 2013).Furthermore, time must be allocated for clinicians to engagein the EBP process. The time invested in EBP should be pro-
moted as essential and valuable as opposed to being labeled as“nonproductive” time as is the case in many hospitals acrossthe United States (Melnyk, 2014a).
It is not enough to disseminate evidence-based guidelinesand expect clinicians to readily implement them. For manyclinicians, EBP requires behavior change from practice steepedin tradition and organizational cultures of “this is the way wedo it here” to practice that is supported by science. Behavior
Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14. 11C© 2016 Sigma Theta Tau International
CNE Study: EBP & Performance Metrics
change in clinicians cannot be achieved by the provision ofinformation alone; often it is precipitated by an emotional rea-son to change (e.g., a compelling story) along with educationaland skill-building workshops to learn the EBP process (Mel-nyk, 2014a). Transformation to an EBP culture also requiresan exciting team vision and clear expectations from healthcareleaders that EBP is the foundation of all care delivered withinthe healthcare system. This expectation should be integratedinto the vision, mission, and strategic plan of the institutionand incorporated into the onboarding of all new clinicians.Furthermore, nurses should be expected to achieve the newEBP competencies for practicing nurses and advanced prac-tice nurses within their organizations (Melnyk, Gallagher-Ford,Long, & Fineout-Overholt, 2014), which means that baccalau-reate and associate degree academic programs must teach theirstudents EBP, not the complex process of how to conduct rig-orous research. For those clinicians who fall short on some ofthe competencies at the start of their employment, continuingeducation workshops with skill-building activities should beprovided until full competence is achieved. Integration of theseEBP competencies into job descriptions and clinical ladder pro-motion systems can also establish clarity of performance expec-tations and serve as an incentive for clinicians to attain them.A critical mass of EBP mentors also should be made availableto point of care clinicians throughout healthcare systems asresearch has indicated that they facilitate evidence-based careand improve patient outcomes (Levin, Fineout-Overholt, Mel-nyk, Barnes, & Vetter, 2011; Melnyk, 2007; Wallen et al., 2010).These mentors should document the “so what” outcomes (i.e.,outcomes that the current healthcare system is most focusedon, including cost, complications, length of stay, and rehos-pitalizations) to support the benefits of their work (Melnyk,2014b).
As a follow-up to our national survey of nurse executives,a national forum with over 150 CNEs and CNOs throughoutthe country was held at the 2014 national conference of theAmerican Organization of Nurse Executives. The purpose ofthis national forum was to share the findings from the recentsurvey and generate solutions to assist nurse executives withimproving their own EBP skills along with determining the bestresources and tools to help them to build strong EBP culturesand environments within their own hospitals and healthcaresystems.
The nurse executives at the national forum called for a bridg-ing of the knowledge gap between EBP and healthcare qualityand patient safety as well as the need for educational offer-ings, specifically for them, to enhance their own knowledgeand skills in EBP and assist them in creating stronger culturesand environments for EBP. They emphasized that it is criticalfor nurse executives and other healthcare administrators to behelped to understand the gap between EBP and its impact onclinical outcomes and return on investment (ROI).
Limitations to this study include a convenience sample andlow response rate, which decreases generalizability of the find-ings. In addition, the survey was a single snapshot of the state of
care and outcomes in hospitals across the United States alongwith self-reported data by the CNEs and CNOs. Future researchis needed that gathers objective data over time along with self-reported data and measures that tap EBP and investments inevidence-based care.
Although there has been progress in EBP over the pastdecade, there is much to be accomplished yet. In efforts to speedthe translation of research into real-world clinical settings, it iscritical to focus on nurse executives as they have important in-fluence over the clinical enterprise and budgetary responsibil-ity for nurses within their healthcare systems. Chief executiveofficers and other healthcare administrators also must under-stand the link between EBP and improved healthcare systemoutcomes. They must be assisted in understanding and valuingthe importance of EBP in reaching their high-priority goals ofhealthcare quality and safety. Only through accelerated effortsin working with executives to build cultures and environmentsthat support EBP and intensive skill building with point of caretransdisciplinary clinicians will EBP become the foundationfor high-quality, safe, and cost-effective care throughout theUnited States healthcare system and the globe. WVN
LINKING EVIDENCE TO ACTION
� Findings from this national survey indicate thatCNEs and CNOs need education and skill buildingin EBP and outcomes management so that theythemselves implement and role model EBP.
� Evidence regarding ROI with EBP is necessary sothat chief nurses and hospital administrators re-alize that healthcare outcomes are improved andcost savings are generated with EBP, and that it iskey to quality and safety.
� CNEs and CNOs and healthcare administratorsneed to build cultures and environments that pro-mote and sustain EBP, which requires financialinvestment.
� Healthcare systems need to provide support fortheir nurses to obtain baccalaureate degrees andbe encouraged to embark on the Magnet journey.
� The new EBP competencies for practicing nursesand advanced practice nurses need to be integratedinto job descriptions and organizational expecta-tions.
� All associate degree and baccalaureate nursingprograms need to prepare their students to meetthe new EBP competencies for practicing nursesand graduate nursing programs should preparetheir students to meet the EBP competencies foradvanced practice nurses.
12 Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14.C© 2016 Sigma Theta Tau International
Original ArticleAuthor information
Bernadette Mazurek Melnyk, Associate Vice President forHealth Promotion, University Chief Wellness Officer, Deanand Professor, College of Nursing, Professor of Pediatrics andPsychiatry, College of Medicine, The Ohio State University,Columbus, OH, USA; Lynn Gallagher-Ford, Director, Centerfor Transdisciplinary Evidence-Based Practice, Clinical Asso-ciate Professor, The Ohio State University, College of Nursing,Columbus, OH, USA; Bindu Koshy Thomas, Technology Coor-dinator, Center for Transdisciplinary Evidence-Based Practice,The Ohio State University, College of Nursing, Columbus, OH,USA; Michelle Troseth, Chief Professional Practice Officer, El-sevier Clinical Solutions, Grand Rapids, MI, USA; Kathy Wyn-garden, Manager, Elsevier CPM Consortium, Elsevier ClinicalSolutions, Grand Rapids, MI, USA; Laura Szalacha, Director ofResearch Methods and Statistics, University of Arizona Collegeof Nursing, Tucson, AZ, USAFunding for this project was provided by Elsevier Clinical So-lutions
Address correspondence to Dr. Bernadette Mazurek Melnyk,The Ohio State University, 1585 Neil Avenue, Columbus, OH43210; [email protected]
Accepted 4 August 2015Copyright C© 2016, Sigma Theta Tau International
ReferencesAiken, L. H., Clarke, S. P., Cheung, R. B., Sloane, D. M.,
& Silber, J. H. (2003). Educational levels of hospital nursesand surgical patient mortality. JAMA, 290(12), 1617–1623. doi:10.1001/jama.290.12.1617
American Organization of Nurse Executives. (2004). Guid-ing principles for future patient care delivery. Retrievedfrom http://www.aone.org/resources/PDFs/AONE_GP_Future_Patient_Care_Delivery_2010.pdf
Everett, L. Q., & Sitterding, M. C. (2011). Transformational lead-ership required to design and sustain evidence-based practice:A system exemplar. Western Journal of Nursing Research, 33(3),398–426. doi: 10.1177/0193945910383056
Fielding, J. E., & Briss, P. A. (2006). Promoting evidence-basedpublic health policy: Can we have better evidence and moreaction? Health Affairs (Project Hope), 25(4), 969–978.
Fineout-Overholt, E., & Melnyk, B. M. (2003). Organizational cul-ture & readiness for system-wide integration of EBP. Gilbert, AZ:ARCC.
Fink, R., Thompson, C. J., & Bonnes, D. (2005). Overcoming bar-riers and promoting the use of research in practice. Journal ofNursing Administration, 35(3), 121–129.
Gifford, W., Davies, B., Edwards, N., Griffin, P., & Lybanon, V.(2007). Managerial leadership for nurses’ use of research ev-idence: An integrative review of the literature. Worldviews onEvidence-Based Nursing, 4(3), 126–145.
Harding, K. E., Porter, J., Horne-Thompson, A., Donley, E., &Taylor, N. F. (2014). Not enough time or a low priority? Barriersto evidence-based practice for allied health clinicians. Journal ofContinuing Education in the Health Professions, 34(4), 224–231.doi: 10.1002/chp.21255
Institute of Medicine. (2003). Health professions education: A bridgeto quality. Washington, DC: The National Academies Press.
Institute of Medicine. (2011). The future of nursing: Leadingchange, advancing health. Washington, DC: National AcademiesPress.
Kutney-Lee, A., Stimpfel, A. W., Sloane, D. M., Cimiotti, J.P., Quinn, L. W., & Aiken, L. H. (2015). Changes in pa-tient and nurse outcomes associated with magnet hospi-tal recognition. Medical Care, 53(6), 550–557. doi: 10.1097/MLR.0000000000000355
Levin, R. F., Fineout-Overholt, E., Melnyk, B. M., Barnes, M., &Vetter, M. J. (2011). Fostering evidence-based practice to improvenurse and cost outcomes in a community health setting: A pilottest of the advancing research and clinical practice through closecollaboration model. Nursing Administration Quarterly, 35(1),21–33. doi: 10.1097/NAQ.0b013e31820320ff
McGinty, J., & Anderson, G. (2008). Predictors of physician com-pliance with American Heart Association guidelines for acutemyocardial infarction. Critical Care Nursing Quarterly, 31(2),161–172. doi: 10.1097/01.CNQ.0000314476.64377.12
Melnyk, B. M. (2007). The evidence-based practice mentor: Apromising strategy for implementing and sustaining EBP inhealthcare systems. Worldviews on Evidence-Based Nursing, 4(3),123–125.
Melnyk, B. M. (2013). Distinguishing the preparation and rolesof Doctor of Philosophy and Doctor of Nursing Practice grad-uates: National implications for academic curricula and healthcare systems. Journal of Nursing Education, 52(8), 442–448. doi:10.3928/01484834-20130719-01
Melnyk, B. M. (2014a). Building cultures and environmentsthat facilitate clinician behavior change to evidence-based prac-tice: What works? Worldviews on Evidence-Based Nursing, 11(2),79–80. doi: 10.1111/wvn.12032
Melnyk, B. M. (2014b). Speeding the translation of research intoevidence-based practice and conducting projects that impacthealthcare quality, patient outcomes and costs: The "so what"outcome factors. Worldviews on Evidence-Based Nursing, 11(1),1–4. doi: 10.1111/wvn.12025
Melnyk, B. M., & Fineout-Overholt, E. (2015). Evidence-based prac-tice in nursing & healthcare. (3rd ed.). Philadelphia, PA: WoltersKluwer/Lippincott Williams & Wilkins.
Melnyk, B. M., Fineout-Overholt, E., & Mays, M. Z. (2008).The evidence-based practice beliefs and implementation scales:Psychometric properties of two new instruments. World-views on Evidence-Based Nursing, 5(4), 208–216. doi: 10.1111/j.1741-6787.2008.00126.x
Melnyk, B. M., Fineout-Overholt, E., Giggleman, M., &Cruz, R. (2010). Correlates among cognitive beliefs, EBPimplementation, organizational culture, cohesion and jobsatisfaction in evidence-based practice mentors from a com-munity hospital system. Nursing Outlook, 58(6), 301–308. doi:10.1016/j.outlook.2010.06.002
Melnyk, B. M., Fineout-Overholt, E., Gallagher-Ford, L., &Kaplan, L. (2012). The state of evidence-based practice inUnited States nurses: Critical implications for nurse leadersand educators. Journal of Nursing Administration, 42(9), 410–417.
Melnyk, B. M., Grossman, D. C., Chou, R., Mabry-Hernandez, I.,Nicholson, W., DeWitt, T. G., . . . Flores, G. (2012). USPSTFperspective on evidence-based preventive recommendations
Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14. 13C© 2016 Sigma Theta Tau International
CNE Study: EBP & Performance Metrics
for children. Pediatrics, 130(2), e399–e407. Retrieved from:http://pediatrics.aappublications.org/content/130/2/e399.long
Melnyk, B. M., Gallagher-Ford, L., Long, L. E., & Fineout-Overholt, E. (2014). The establishment of evidence-based prac-tice competencies for practicing registered nurses and advancedpractice nurses in real-world clinical settings: Proficiencies toimprove healthcare quality, reliability, patient outcomes, andcosts. Worldviews on Evidence-Based Nursing, 11(1), 5–15. doi:10.1111/wvn.12021
Nagykaldi, Z., Mold, J. W., Robinson, A., Niebauer, L., & Ford,A. (2006). Practice facilitators and practice-based research net-works. Journal of the American Board of Family Medicine, 19(5),506–510.
Raab, C. A., Will, S. E., Richards, S. L., & O’Mara, E. (2013). The ef-fect of collaboration on obstetric patient safety in three academicfacilities. Journal of Obstetric, Gynecologic, and Neonatal Nursing,42(5), 606–616. doi: 10.1111/1552-6909.12234
Rycroft-Malone, J. (2008). Evidence-informed practice: From in-dividual to context. Journal of Nursing Management, 16(4),404–408. doi: 10.1111/j.1365-2834.2008.00859.x
Rycroft-Malone, J., Seers, K., Chandler, J., Hawkes, C. A., Crichton,N., Allen, C., . . . Strunin, L. (2013). The role of evidence, context,
and facilitation in an implementation trial: Implications for thedevelopment of the PARIHS framework. Implementation Science,8, 8–28. doi: 10.1186/1748-5908-8-28
Sredl, D., Melnyk, B. M., Hsueh, K -H., Jenkins, R., Ding, C., &Durham, J. (2011). Health care in crisis! Can nurse executives’beliefs about and implementation of evidence-based practice bekey solutions in health care reform? Teaching and Learning inNursing, 6(2), 73–79. doi: 10.1016/j.teln.2010.06.001
Wallen, G. R., Mitchell, S. A., Melnyk, B., Fineout-Overholt, E.,Miller-Davis, C., Yates, J., & Hastings, C. (2010). Implement-ing evidence-based practice: Effectiveness of a structured mul-tifaceted mentorship programme. Journal of Advanced Nursing,66(12), 2761–2771. doi: 10.1111/j.1365-2648.2010.05442.x
Wilson, M., Sleutel, M., Newcomb, P., Walsh, J., Wells, J. N.,& Baldwin, K. M. (2015). Empowering nurses with evidence-based practice environments: Surveying Magnet, Pathway to Ex-cellence, and non-magnet facilities in one healthcare system.Worldviews on Evidence-Based Nursing, 12(1), 12–21.
doi 10.1111/wvn.12133WVN 2016;13:6–14
14 Worldviews on Evidence-Based Nursing, 2016; 13:1, 6–14.C© 2016 Sigma Theta Tau International
Original Article
Empowering Nurses With Evidence-BasedPractice Environments: Surveying Magnet R©,Pathway to Excellence R©, and Non-MagnetFacilities in One Healthcare SystemMarian Wilson, RN-BC, PhD, MPH • Martha Sleutel, RN, PhD, CNS •Patricia Newcomb, RN, PhD, PNP • Deborah Behan, RN-BC, PhD • Judith Walsh, RN,PhD • Jo Nell Wells, RN-BC, PhD, OCN • Kathleen M. Baldwin, RN, PhD, FAAN,ACNS-BC, ANP-BC, GNP-BC, FAACM
Keywords
evidence-basedpractice,
nurses,readiness,
survey
ABSTRACTBackground: Nurses have an essential role in implementing evidence-based practices (EBP) thatcontribute to high-quality outcomes. It remains unknown how healthcare facilities can increasenurse engagement in EBP.
Purpose: To determine whether individual or organizational qualities could be identified thatwere related to registered nurses’ (RNs’) readiness for EBP as measured by their reported EBPbarriers, ability, desire, and frequency of behaviors.
Methods: A descriptive cross-sectional survey was used in which a convenience sample of 2,441nurses within one United States healthcare system completed a modified version of the Infor-mation Literacy for Evidence-Based Nursing questionnaire. Descriptive statistics, t tests, one-wayANOVA, and regression modeling were used to analyze the data.
Results: RNs employed by facilities designated by the American Nurses Credentialing Center(ANCC) as Magnet R© or Pathway to Excellence R© reported significantly fewer barriers to EBPthan those RNs employed by non designated facilities. RNs in Magnet organizations had higherdesire for EBP than Pathway to Excellence or non designated facilities. RNs educated at thebaccalaureate level or higher reported significantly fewer barriers to EBP than nurses with lesseducation; they also had higher EBP ability, desire, and frequency of behaviors. A predictivemodel found higher EBP readiness scores among RNs who participated in research, had specialtycertifications, and engaged in a clinical career development program.
Linking Evidence to Action: Education, research, and certification standards promoted by theMagnet program may provide a nursing workforce that is better prepared for EBP. Organiza-tions should continue structural supports that increase professional development and researchopportunities so nurses are empowered to practice at their full capacity.
BACKGROUNDHealthcare leaders and institutions have increased expectationsfor evidence-based practice (EBP) in the quest to improve out-comes, boost quality, and lower costs. An Institute of Medicine(IOM) aim is that 90% of clinical decisions will be evidence-based by 2020 (IOM, 2010). As the largest group of healthcareproviders, nurses have a pivotal role in meeting this goal. Cul-tivating a “spirit of inquiry” to support an EBP culture has beenrecognized as the first step for EBP (Melnyk, Gallagher- Ford,Long, & Fineout-Overholt, 2014). Identifying individual andorganizational qualities facilitating EBP is imperative to focuspatient care improvement efforts and spend resources wisely.
Frameworks developed by the American Nurses Creden-tialing Center (ANCC) for the Magnet Recognition Program R©
and Pathway to Excellence R© designations require nurses toengage in the process of incorporating new evidence intopractice (ANCC, 2014). While research has linked thesedesignations to quality and safety outcomes (Drenkard,2010; Messmer & Turkel, 2011), less is known about howANCC-designated organizations’ characteristics are linked togreater EBP implementation. To increase understanding, wesurveyed nurses employed by Magnet-designated, Pathway toExcellence-designated, and non designated facilities withinone large healthcare system in the southwest United States
12 Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21.C© 2015 Sigma Theta Tau International
Original Articleon barriers to EBP, EBP ability, desire, and frequency ofbehaviors. By exploring both individual and organizationalqualities, we were able to identify conditions facilitating EBP.This knowledge can guide efforts to reinforce or build a strongEBP culture at healthcare facilities.
Factors influencing EBP have been extensively reported.Individual nurse qualities include EBP beliefs, confidence,time, knowledge, and skills (Melnyk, 2013). Clinical nurses’varying backgrounds, education, and attitudes can influencetheir motivation and ability to integrate evidence into practice(Swenson-Britt & Berndt, 2013). Organizational qualities thatimpact EBP include administrative support and access toresources (Melnyk, 2013). Two categories of organizationalfactors are infrastructure aspects such as library resources,and unit or facility climate such as authority to make changes,resistance or support by colleagues and leaders (Kelly, Turner,& Speroni, 2012; Melnyk, Fineout-Overholt, Gallagher-Ford,& Kaplan, 2012; Swenson-Britt & Berndt, 2013). Consistentlycited barriers to research utilization are organizational factorsand difficulty understanding research findings (Kajermo et al.,2010).
Much work has been done to identify characteristics oforganizations that are both highly reliable (i.e., safe) andsupport a culture of EBP. As presented by Melnyk (2012),those characteristics are multifactorial and complex. Theyinclude: commitment to delivering high-quality care andpatient safety, trans disciplinary teamwork, standardizationof best practices and policies, and an environment thatpromotes a spirit of inquiry and continuous learning. Studiessuggest that organizational leadership, opinion leaders,and role models may increase the use of EBP (Flödgrenet al., 2011; Thorsteinsson, 2013). The challenge lies indetermining specific actions to build and strengthen an EBPculture.
The Promoting Action on Research Implementation inHealth Services (PARIHS) conceptual framework (Kitson et al.,1998; Rycroft-Malone, 2004) guided the present study andconsiders both the context and facilitation required for change.Context includes culture, leadership, and evaluation (De Pedro-Gómez et al., 2012). Facilitation can occur through specificindividuals or processes that empower healthcare providersto incorporate new evidence into practice. Once differences incontext or facilitation among settings are identified, it may thenbe possible to detect and manipulate variables associated withcultures most supportive of EBP.
Our healthcare system recently instituted hospital-basedpositions for nurse scientists (doctorally prepared nurse re-searchers) in each hospital to improve nurses’ use of EBP andresearch. With a long-term goal of seeking system-wide Mag-net status, greater understanding of nurses’ perceptions of EBPwas needed to guide strategies to increase use of research evi-dence. The majority (n = 11; 78.6%) of the 14 hospitals withinthe system had received ANCC designation as Magnet (n = 3;21.4%) or Pathway to Excellence (n = 8; 57.1%) at the time ofdata collection.
PURPOSEThe purpose of this study was to describe the current climate ofEBP as reported by registered nurses (RNs) employed across allacute care settings within one of the largest hospital networksin the southwest United States. The specific aims of this studywere fourfold:
� Describe self-reported EBP behaviors, abilities, de-sires, and barriers among RNs employed in the tar-geted hospital system;
� Determine if significant differences exist in scoresamong hospitals with various ANCC designation sta-tuses;
� Determine if significant differences exist in scoresamong RNs with various individual qualities (educa-tional level, certification status); and
� Determine whether individual and organizationalvariables can be identified that predict positive EBPscores (including job role, length of time as a nurse,and research experience).
We obtained permission to use and adapt the InformationLiteracy for Evidence-Based Nursing Practice (ILNP) question-naire (Pravikoff, Tanner, & Pierce, 2005). Nurse scientists fromeach hospital were involved in this minimal risk study andensured equitable access for RNs. An introductory e-mail ex-plained the voluntary nature of the online survey and stepstaken to ensure respondents’ anonymity and privacy. All datawere collected and reported in aggregate form to preserve con-fidentiality. The healthcare system Institutional Review Boardapproved the study and determined that completion of the sur-vey implied informed consent.
METHODSThe study was an exploratory cross-sectional descriptive survey.Participants were asked to complete a revised version of theILNP. Data were collected over a 3-month period in 2013. RNsworking at the 14 hospitals within the healthcare system (N =6,873) comprised the targeted population.
The ILNPThe ILNP was originally developed as a 71-item measurementto assess U.S. nurses’ readiness for EBP, use of EBP, andperceived barriers to EBP. The ILNP content validity was estab-lished by a panel of experts and the development and validationare described elsewhere (Pravikoff et al., 2005). While the toolhas been widely used, construct validity and reliability have notbeen previously reported (Pravikoff et al., 2005; Thorsteins-son, 2013). After receiving permission to use and modify thetool, we removed sections related to computer and library re-sources because those are standard throughout our system.We also modified demographic items to reduce potential for
Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21. 13C© 2015 Sigma Theta Tau International
Empowering Nurses With EBP Environments
respondent identification, and updated some items to alignwith current literature, such as barriers and EBP activities.
ProcedureThe nurse scientist at each hospital sent a weekly e-mail for4 weeks to all RNs listed on the hospital e-mail distributionlists. A web link imbedded within the e-mail allowed nurses tocomplete the survey from their home or work computers. Asan incentive, participants were given the option to click on aseparate link if they wished to enter a drawing to win one ofeight e-book readers.
Data AnalysisWe analyzed the data using SPSS, version 18 (2009; SPSSInc. Chicago, IL, USA). Descriptive statistics provided responsefrequencies and distributions. Survey items were categorizedinto subscales that represented four constructs of interest. Re-sponse formats for the subscales included:
� Frequency of behaviors (“In the past year, how fre-quently have you participated in the following activ-ities?” e.g., “Identified a researchable problem”). Re-sponse choices for five items include 1 (not at all) to 4(more than three times).
� Abilities (“How would you rate your ability to dothe following?” e.g., “Critique or evaluate a researchstudy”). Response choices for 5 items include 1 (notable) to 5 (highly able).
� Desire (“How would you rate your desire to be ableto do the following?” e.g., “Use research findings inpractice”). Response choices for 5 items include 1 (nodesire) to 5 (high desire).
� Barriers (“Rate how much these factors are barriersto your participating more in research or evidence-based nursing practice.” e.g., “I don’t understand theresearch process”). Response choices for 8 items in-clude 1 (not at all true) to 5 (highly true).
We calculated an EBP readiness score from the mean ofthe combined 15 subscale items for frequency, ability, and de-sire. To examine differences between groups of nurses withvarious certification statuses, t tests were used. We determinedeffect sizes between groups using Cohen’s d with values inter-preted as small = .20, medium = .50, and large = .80 (Cohen,1988). ANOVA tests examined differences between hospitalsand nurses’ varying educational levels using eta squared (η2) tocalculate effect sizes using small = .01, medium = .06, and large= .14 (Cohen, 1988). A regression model was constructed topredict the effects of selected variables on EBP readiness scores.Listwise deletion was used for missing data and it was deter-mined that missing data were random. Due to the exploratorynature of the study with no a priori hypotheses, multiple com-parisons adjustments were not required (Saville, 1990).
RESULTSRespondentsA convenience sample of 2,441 RNs comprised the final sam-ple, a response rate of 35.5%. The majority of respondents(81.0% or n = 1,977) identified themselves as clinical bed-side nurses. About 24% (n = 597) of the sample had been anurse for five years or less, while 45% (n = 1,105) had beena nurse for 5–20 years and 28% (n = 684) for more than20 years (missing data 2% [n = 55]). The majority (59.8%; n =1,459) reported holding at least one national nursing certifica-tion and were prepared at the baccalaureate level (44.9%; n =1,095). Respondents from rural hospitals were 17.9% (n = 412)of our sample, while participants from large urban centers andmedium suburban centers represented 43.2% (n = 995) and38.9% (n = 895), respectively. Table 1 compares respondentdata with available state RN data and shows similar propor-tions in education levels and roles.
INLP ResultsApproximately 80% (n = 1,961) of respondents stated theyhad a moderate or high understanding of the term “evidence-based nursing practice,” whereas .9% (n = 21) said they hadno understanding of it. Cronbach’s alpha for the revised 34item INLP was .85 (n = 2,276) indicating an acceptable levelof internal consistency reliability. Full sample mean scoreswith reliability values for the four EBP subscales (behaviorfrequency, ability, desire, and barriers) are presented in Table 2.
Comparisons of HospitalsSignificant differences were detected on INLP subscales whencomparing RNs in Magnet or Pathways designated hospitalsto those working in non designated hospitals (see Table 2).Post hoc comparisons using Tukey’s HSD test indicated highermean EBP barrier scores for non designated hospitals com-pared to both Pathways and Magnet hospitals at the .05 level ofsignificance. Magnet hospitals also scored significantly higherthan Pathway and non designated hospitals on EBP desirescores. The largest EBP desire differences when comparingdesignated and non designated hospitals were for the items“use research findings in practice,” and “participate in a re-search project.” Scores on EBP ability, frequencies, and overallreadiness did not differ significantly based on Magnet status.
Comparisons of Groups of NursesNursing education. Significant differences were detected onINLP subscales when comparing RNs of varying educationalpreparation. Mean scores for EBP barriers, frequency, abilities,readiness, and desire improved as educational level increasedas presented in Table 3. Post hoc comparisons using Tukey’sHSD test indicated that RNs with a bachelor’s degree or higherreported significantly fewer barriers to participating in researchor EBP compared to RNs with less educational preparation atthe .05 level of significance. Nurses with a bachelor’s degree orhigher degrees also scored significantly higher on EBP desire,
14 Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21.C© 2015 Sigma Theta Tau International
Original ArticleTable 1. Participant Demographics (N = 2,441) with State and Survey Comparisons
Survey respondents State data*
Education and employment % (n) % (n)
Highest level of education
Bachelor’s degree 44.9 (1,095) 43.3 (114,345)
Associate degree 32.9 (803) 40.02(106,143)
Diploma 6.5 (158) 6.9 (18,204)
Master’s degree 8.8 (215) 9 (23,802)
Doctoral degree .7 (18) .1 (1,470)
Not reported 6.2 (152) < 0 (20)
Nurse unit or role
Direct care, bedside RNs 81.0 (1,977) 82.9 (131,343)
Administration/management RNs 8.6 (211) 16.4 (31, 403)
Staff education RNs 2.5 (60) .7 (6,846)
Medical surgical/telemetry 25.0 (610)
Administration 8.6 (211)
Educator 2.5 (60)
Other Roles 6.2 (169)
Women/infant/children 20.3 (496)
Critical care 14.2 (346)
Perioperative/post-anesthesia/day surgery 11.7 (285)
Emergency 10.3 (252)
Mental health 2.0 (48)
Nurse certification 59.8 (1,459)
*Texas State Board of Nursing (2014)
ability, and frequency. At levels above the bachelor’s degree,significant increases were noted on EBP frequency and desirefor RNs with doctorate degrees compared to those with mas-ter’s degrees. EBP ability, readiness, and barriers scores didnot differ significantly between those two groups of RNs withadvanced education.
Nursing certification. Registered nurses who held a nursingcertification reported: (a) Higher frequency of EBP behaviors(M = 2.79, SD = .58) than non certified RNs (M = 2.58, SD =.53, t(1509) = –8.17, p � .001, d = .38); (b) higher desire forEBP (M = 3.35, SD = 1.07) compared to non certified RNs(M = 3.20, SD = 1.06, t(2165) = –3.19, p = .001, d = .14);and (c) higher EBP ability (M = 3.62, SD = .90) compared tonon certified RNs (M = 3.53, SD = .89, t(2152) = –2.39, p =.017, d = .10). In contrast, specialty-certified RNs identified
stronger barriers to participating in research or EBP (M = 2.11,SD = .71) compared to non certified RNs (M = 2.00, SD = .71,t(2119) = –3.173, p = .002, d = .15).
Predicting EBP ReadinessResults of regression modeling showed that a set of 12 variablespredicted 38% (adjusted R2 = .375) of the variance in the EBPreadiness score. Table 4 provides the coefficients, error, t-testvalues, and significance values for each variable. A history ofparticipation in a research project was the strongest positivepredictor of EBP readiness scores. Other positive predictorsincluded a perceived frequent need for information to supportclinical practice, specialty certification, and participation in thesystem career development (clinical ladder) program. Negativepredictors included difficulty understanding research articles,
Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21. 15C© 2015 Sigma Theta Tau International
Empowering Nurses With EBP Environments
Table 2. One-way ANOVA Exploring Differences in EBP Barriers, Desire, Ability, and Frequency among Magnet,Pathway to Excellence and Non-Magnet Hospitals
Number of EBP barriers EBP desire EBP ability EBP frequency EBP readinessDesignation status hospitals mean (SD) mean (SD) mean (SD) mean (SD) mean (SD)
Magnet 3 2.04 (.73) 3.38 (1.09) 3.57 (.92) 2.12 (.76) 3.02 (.76)
Pathway to Excellence 8 2.09 (.67) 3.14 (1.03) 3.63 (.87) 2.07 (.77) 2.94 (.74)
Non-Magnet/Non-Pathway 3 2.23 (.75) 3.22 (1.03) 3.56 (.89) 2.07 (.73) 2.95 (.74)
Full sample 14 2.07 (.72) 3.28 (1.07) 3.57 (.91) 2.71 (.57) 3.02 (.62)
Cronbach’s alpha .81 .91 .89 .82 .92
df 2, 2409 2, 2383 2, 2364 2, 2339 2, 2262
F statistic 15.424 9.836 .762 .871 3.158
p value
Original Article
Table 4. Association Between Variables and Personal Readiness Scores. Model Adjusted R2 = .38
Variable Unstandardized beta regression coefficient Standard error t-test value p value
Role: Bedside RN −2.73 .540 −5.055 .0001History of participation in a research project 7.633 .426 17.904 .0001
Frequency of need for information to support practice 2.98 .249 11.950 .0001
Barrier: Lack of understanding of research process −1.486 .269 −5.516 .0001Barrier: Difficulty understanding research articles −1.839 .278 −6.610 .0001Barrier: Perception that nurses do not want to change practice .644 .189 3.417 .001
Barrier: Difficulty finding research or library services −.684 .240 −2.847 .004RN Certification 1.068 .440 2.427 .02
Career Advancement Program level (clinical ladder) .751 .280 2.682 .007
Number of years since most recent nursing degree −.191 .031 −6.085 .0001Number of years nursing experience .122 .031 3.902 .0001
certification (ANCC, 2008). These expectations have addedto a growing emphasis on nurses obtaining the BSN, withmore organizations preferring to hire BSN-prepared graduates(O’Connor, 2012). Nurses are often skeptical that increasededucation and the time and money investment will have valuefor them, yet many change views during or after completingthe BSN (Hawkins & Shell, 2012). While research has shownlinks between higher nurse education and quality outcomes,less is understood about how those shifts occur and EBP isinfluenced. When scrutinizing budget practices related tonurse tuition and certification reimbursement, healthcaresystem leaders need evidence to understand how highereducation and certification can contribute to improved patientoutcomes and the work environment.
Magnet and Pathways Designation Relate to EBPIn our sample, nurses from hospitals with either Magnetor Pathways designation reported fewer barriers to EBP andMagnet hospitals had the highest desire for EBP. Similarfindings were reported by Melnyk et al. (2012) regardingbarriers, suggesting that Magnet facilities have a culturesupportive of EBP. The largest differences between nursesin designated and non designated hospitals in our samplewere in response to the barrier items “I don’t understand theresearch process,” along with “I don’t see the value of researchin practice,” and “physicians do not want to change practice.”The final two of these items may reflect organizational culture,while the first one indicates individual EBP education. TheANCC requires designated organizations to provide evidencethat nurses incorporate new evidence into practice (ANCC,2014). Therefore, these organizations can be considered as (a)
context that supports an EBP culture, and (b) supportive offacilitators or change agents who can engage clinicians in EBP.Striving for Magnet designation may serve to operationalizethe PARIHS framework by development of both context andfacilitation necessary for successful implementation of EBP.
Nurses’ subordinate role in many healthcare organizationscan be a hindrance to implementing EBP (Atkinson, Turkel,& Cashy, 2008; Brown, Wickline, Ecoff, & Glaser, 2009; DePedro-Gómez et al., 2012). Without empowerment to takeaction, nurses cannot practice professionally and respond tochallenges using their professional skill and knowledge (Rao,2012). Lacking power to change practice, nurses may rely oninflexible bureaucratic structures to guide practice (Rao, 2012).Therefore, it is reasonable to propose that strategies aimed to-ward building nurse autonomy and engaging nurses to thefullest extent of their capabilities may lead to improvementsin quality outcomes. In our sample, RNs who took advan-tage of clinical ladder and research opportunities and increasedknowledge-based skills through certification and advanced de-grees were more likely to feel prepared to engage in EBP. Thesefindings align with others across the globe that show increasedEBP self-efficacy and workplace research support are linkedto greater EBP behaviors (Boström, Rudman, Ehrenberg,Gustavsson, & Wallin, 2013; Eizenberg, 2011; Thorsteinsson,2013).
Numerous articles relate the impact of positive work envi-ronment on nursing empowerment and improved patient out-comes (Aiken, Clarke, Sloane, Lake, & Cheney, 2008; SpenceLaschinger & Leiter, 2006; Stimpfel, Rosen, & McHugh, 2014).The Magnet Model component of Structural Empowermentrequires leadership to provide systems, policies, and pro-grams to empower autonomous professionals who engage in
Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21. 17C© 2015 Sigma Theta Tau International
Empowering Nurses With EBP Environments
Figure 1. Influence of Structural Empowerment on Individual Nurse Factors.
continuous learning. Structural Empowerment further sup-ports the Magnet Model component of New Knowledge, Inno-vation, & Improvements that requires applying new evidenceand contributing to the science of nursing (ANCC, 2014). Thus,it is not surprising that mounting evidence links Magnet des-ignation to improved outcomes (McHugh et al., 2013; Stimpfelet al., 2014.) Figure 1 depicts how components of the Mag-net Model and its supporting standards impact nurses’ EBPbehaviors, ability, desire, and barriers through culture change.
Implications for PracticeMany influential professional organizations are in agreementwith Magnet standards that promote increased educationalpreparation of nurses. The IOM, the Tri-Council for Nursing,and the Carnegie Foundation for the Advancement of Teach-ing issued statements stressing the importance of highereducation to promote quality patient care and safety (AmericanAssociation of Colleges of Nursing [AACN], 2014). Autonomyand opportunities for professional development are identifiedas key ingredients for positive practice environments by theInternational Council of Nurses (ICN, 2008). Further argu-ments are strengthened by evidence that higher percentages ofBSN staff nurses are linked to reduced mortality and improvedpatient outcomes in diverse settings (Aiken, Clarke, Cheung,Sloane, & Silber, 2003; Aiken et al., 2008; Estabrooks, Midodzi,
Cummings, Ricker, & Giovanetti, 2005; Tourangeau et al.,2007; You et al., 2013). Globally, healthcare system leadersremain challenged by nurses’ job dissatisfaction and burnout,with one quarter of all U.S. nurses reporting intentions to leavetheir job (ICN, 2008; Neff, Cimiotti, Heusinger, & Aiken,2011; You et al., 2013). Hospital administrators must attend tothese critical issues to retain the nurse workforce (Neff et al.,2011). Future efforts to increase educational requirements fornurses may be overshadowed by priorities to keep positionsfilled, while budgetary constraints may curb efforts to providetuition and certification reimbursements. Our predictivemodel suggests that EBP readiness is advanced throughopportunities for nurses to engage in research projects;however, research activities are resource-intensive as well.
Certified RNs had higher mean EBP behavior, ability, anddesire scores, yet also had higher EBP barrier scores in our sam-ple. This finding may seem contradictory, but could indicategreater nurse awareness of EBP opportunities following certi-fication and an increased perception of barriers. By contrast,RNs with a BSN or higher education did not follow this patternand reported lower barrier scores. Specialty certification hasbeen associated with lower mortality and failure to rescue inprior research (defined as preventing a clinically important de-terioration, death, or disability; AHRQ, n.d.); however, this onlyheld true for nurses with a BSN or higher (Kendall-Gallagher,
18 Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21.C© 2015 Sigma Theta Tau International
Original ArticleAiken, Sloane, & Cimiotti, 2011). Future studies could examinewhether the achievement of the BSN gives nurses tools to over-come barriers, and how the addition of specialty certificationcontributes to desired behaviors.
LimitationsAlthough our sample closely matched state RN demograph-ics, convenience sampling methods may introduce bias. It isunknown how responses from those who did not participatewould alter findings. Self-report survey methods may be less ac-curate than other forms of measurement. Of note, most scoresfell into moderate ranges on average (e.g., 3 = some desire,somewhat able) indicating opportunities for improvements inall groups of nurses. Differences between groups were modest.It is unknown how they translate into meaningful clinical vari-ations. Sampling from one institution limits generalizability,however, our large healthcare system includes diverse culturesand a wide geographic range. Finally, our design limits causeand effect conclusions so further experimentation is needed tobuild confidence in findings.
CONCLUSIONSUsing current research in clinical care is an essential skill forhealthcare professionals. Organizations are challenged by howto increase EBP to meet quality outcomes goals. Our findingsadd support for continued efforts to increase nurse educationand certifications, and create opportunities for nurses to partic-ipate in career advancement opportunities and research. Thefindings also provide validation of Structural Empowermentstandards required for organizations designated with Magnetand Pathway to Excellence. Higher levels of education and certi-fication may empower nurses to act as autonomous practition-ers who advocate for evidence-based innovations, and allow aspirit of inquiry to flourish. WVN
LINKING EVIDENCE TO ACTION
� RNs with higher education and specialty certifica-tion feel more prepared for EBP.
� RNs with research experiences have increasedreadiness for EBP activities.
� Organizations should align with Magnet standardsfor increased professional development strategiesto achieve high-quality, evidence-based care.
Author information
Marian Wilson, Pain Management Board Certified Nurse,Nurse Scientist, Texas Health Presbyterian Hospital, Allen,Dallas, and Kaufman, TX, USA; Assistant Professor, Wash-ington State University, College of Nursing, Spokane, WA,USA; Martha Sleutel, Perinatal Clinical Nurse Specialist,
Nurse Scientist, Texas Health Arlington Memorial and TexasHealth Denton, TX, USA; Patricia Newcomb, Pediatric NursePractitioner–Board Certified, Nurse Scientist, Texas HealthHarris Fort Worth, Texas Health Azle, and Texas HealthSpecialty Hospitals, Fort Worth, TX, USA; Deborah Be-han, Medical-Surgical Board Certified Nurse, Nurse Scien-tist, Texas Health Hurst-Euless-Bedford, Bedford, TX, USA;Judith Walsh, Nurse Scientist, Texas Health Resources Plano,Plano, TX, USA; Jo Nell Wells, Oncology Certified Nurse(OCN), Medical-Surgical Board Certified Nurse, Nurse Scien-tist, Texas Health Resources, Alliance Hospital Argyle, TX,USA; Kathleen M. Baldwin, Adult Clinical Nurse Specialist–Board Certified, Adult Nurse Practitioner–Board Certified;Gerontologic Nurse Practitioner–Board Certified, Nurse Sci-entist, Texas Health Harris Hospital Southwest, Fort Worthand Texas Health Harris Hospital, Cleburne, TX, USA.The authors acknowledge the Texas Health Resources Foun-dation for grant funding to support our participant incentivesand the Texas Health Resources medical library services forassistance with literature retrieval.
Address correspondence to Dr. Marian Wilson, WashingtonState University, College of Nursing, P.O. Box 1495, Spokane,WA 99210; [email protected]
Accepted 26 October 2014Copyright C© 2015, Sigma Theta Tau International
ReferencesAgency for Healthcare Research and Quality (AHRQ). (n.d.)
Patient Safety Network glossary. Retrieved from http://www.psnet.ahrq.gov/popup_glossary.aspx?name=failuretorescue
Aiken, L. H., Clarke, S. P., Cheung, R. B., Sloane, D. M., & Silber,J. H. (2003). Educational levels of hospital nurses and surgicalpatient mortality. Journal of the American Medical Association,290, 1617–1623.
Aiken, L. H., Clarke, S. P., Sloane, D. M., Lake, E. T., & Cheney, T.(2008). Effects of hospital care environment on patient mortalityand nurse outcomes. Journal of Nursing Administration, 38(5),223–229.
American Association of Colleges of Nursing (AACN). (2014).The impact of education on nursing practice. Fact sheet:About nursing education. Retrieved from http://www.aacn.nche.edu/media-relations/fact-sheets/impact-of-education
American Nurses Credentialing Center. (2008). Magnet Recog-nition Program R© manual—Recognizing nursing excellence. SilverSpring, MD: The American Nurses Association, Inc.
American Nurses Credentialing Center. (2014). Magnet RecognitionProgram R© overview: Data and expected outcomes. Retrieved fromhttp://www.nursecredentialing.org/magnet/programoverview
Atkinson, M., Turkel, M., & Cashy, J. (2008). Overcomingbarriers to research in a Magnet community hospital. Jour-nal of Nursing Care Quality, 23(4), 362–368. doi: 10.1097/01.NCQ.0000336675.48466.37
Boström, A. M., Rudman, A., Ehrenberg, A., Gustavsson, J. P., &Wallin, L. (2013). Factors associated with evidence-based practiceamong registered nurses in Sweden: A national cross-sectionalstudy. BMC Health Services Research, 13, 165. doi: 10.1186/1472-6963-13-165
Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21. 19C© 2015 Sigma Theta Tau International
Empowering Nurses With EBP Environments
Brown, C. E., Wickline, M. A., Ecoff, L., & Glaser, D. (2009).Nursing practice, knowledge, attitudes and perceived barriersto evidence-based practice at an academic medical center. Jour-nal of Advanced Nursing, 65(2), 371–381. doi: 10.1111/j.1365-2648.2008.04878
Cohen, J. (1988). Statistical power analysis for the behavioral sciences(2nd ed.). Hilldale, NJ: Lawrence Erlbaum.
De Pedro-Gómez, J., Morales-Asencio, J. M., Bennasar-Veny,M., Artigues-Vives, G., Perelló-Campaner, C., & Gómez-Picard, P. (2012). Determining factors in evidence-based clin-ical practice among hospital and primary care nursing staff.Journal of Advanced Nursing, 68(2), 452–459. doi:10.1111/j.1365-2648.2011.05733.x
Drenkard, K. (2010). Going for the gold: The value of attainingmagnet recognition. American Nurse Today, 5(3), 50–52.
Eizenberg, M. M. (2011). Implementation of evidence-basednursing practice: Nurses’ personal and professional factors?Journal of Advanced Nursing, 67(1), 33–42. doi: 10.1111/j.1365-2648.2010.05488.x. Epub 2010 Oct 25.
Estabrooks, C. A., Midodzi, W. K., Cummings, G. C., Ricker, K. L.,& Giovanetti, P. (2005). The impact of hospital nursing charac-teristics on 30-day mortality. Nursing Research 54(2), 72–84.
Flödgren, G., Parmelli, E., Doumit, G., Gattellari, M., O’Brien,M. A., Grimshaw, J., & Eccles, M. P. (2011). Local opinionleaders: Effects on professional practice and health care out-comes. Cochrane Database Systematic Review, 8, CD000125.doi:10.1002/14651858.CD000125.pub4
Hawkins, J., & Shell, A. (2012). Magnet hospitals are attracted tothe BSN, but what’s in it for nurses? Nursing 2012, 42(3), 50–52.doi: 10.1097/01.NURSE.0000411434.84430.92
Institute of Medicine. (2010). The future of nursing: Leading change,advancing health. Washington, DC: The National AcademiesPress.
International Council of Nurses. (2008). Positive practice envi-ronments for health care professionals: Fact sheet. Retrieved fromhttp://www.icn.ch/images/stories/documents/publications/fact_sheets/17d_FS-Positive_Practice_Environments_HC_Professionals.pdf.
Kajermo, K. N., Boström, A. M., Thompson, D. S., Hutchinson,A. M., Estabrooks, C. A., & Wallin, L. (2010). The BARRIERSscale—The barriers to research utilization scale: A systematicreview. Implementation Science, 5, 32. doi: 10.1186/1748-5908-5-32
Kelly, K. P, Turner, A., & Speroni, K. G. (2012). National survey ofhospital nursing research, Part 2: Facilitators and hindrances.The Journal of Nursing Administration, 43(1), 18–23.
Kendall-Gallagher, D., Aiken, L. H., Sloane, D. M., & Cimiotti, J.P. (2011). Nurse specialty certification, inpatient mortality, andfailure to rescue. Journal of Nursing Scholarship, 43(2), 188–194.doi: 10.1111/j.1547-5069.2011.01391.x
Kitson, A., Harvey, G., & McCormack, B. (1998). Enabling theimplementation of evidence based practice: A conceptual frame-work. Quality Health Care, 7, 149–158. doi:10.1136/qshc.7.3.149
McHugh, M. D., Kelly, L. A., Smith, H. L., Wu, E. S., Vanak, J. M., &Aiken, L. H. (2013). Lower mortality in magnet hospitals. MedicalCare, 51(5), 382–388. doi: 10.1097/MLR.0b013e3182726cc5
Melnyk, B. M. (2012). Achieving a high-reliability organizationthrough implementation of the ARCC model for system widesustainability of evidence-based practice. Nursing AdministrationQuarterly, 36(2), 127–135. doi: 10.1097/NAQ.0b013e318249fb6a
Melnyk, B. M. (2013). Educational programming in undergraduateand graduate academic curricula: Friend or foe to acceleratingevidence-based practice? Worldviews on Evidence-Based Nursing,10(4), 185–186. doi: 10.1111/wvn.12020
Melnyk, B. M., Fineout-Overholt, E., Gallagher-Ford, L., & Ka-plan, L. (2012). The state of evidence-based practice in USNurses: Critical implications for nurse leaders and educators.The Journal of Nursing Administration, 42(9), 410–417. doi:10.1097/NNA.0b013e3182664e0a
Melnyk, B. M., Gallagher-Ford, L., Long, L. E., & Fineout-Overholt, E. (2014). The establishment of evidence-based prac-tice competencies for practicing registered nurses and advancedpractice nurses in real-world clinical settings: Proficiencies toimprove healthcare quality, reliability, patient outcomes, andcosts. Worldviews on Evidence-Based Nursing, 11(1), 5–15. doi:10.1111/wvn.12021
Messmer, P. R., & Turkel, M. C. (2011). Magnetism and the nurs-ing workforce. In A.T. Debisette & J.A. Vessey (Eds.), Annual re-view of nursing research (pp. 233–252). Philadelphia, PA: SpringerPublishing.
Neff, D. F., Cimiotti, J. P., Heusinger, A. S., & Aiken, L. H.(2011). Nurse reports from the frontlines: Analysis of a statewidenurse survey. Nursing Forum, 46(1), 4–10. doi: 10.1111/j.1744-6198.2010.00201.x
O’Connor, B. (2012). New American Association of Colleges ofNursing data show significant enrollment increases in baccalau-reate, master’s, and doctoral nursing degree programs. Journalof Professional Nursing, 28(1), 3–4.
Pravikoff, D. S., Tanner, A. B., & Pierce, S. T. (2005). Readinessof U.S. nurses for evidence-based practice. American Journal ofNursing, 105(9), 40–52.
Rao, A. (2012). The contemporary construction of nurse em-powerment. Journal of Nursing Scholarship, 44, 396–402. doi:10.1111/j.1547-5069.2012.01473.x
Rycroft-Malone, J. (2004). The PARIHS framework—A frame-work for guiding the implementation of evidence-based practice.Journal of Nursing Care Quality, 19(4), 297–304.
Saville, D. J. (1990). Multiple comparison procedures: The practicalsolution. The American Statistician, 44(2), 174–180.
Spence Laschinger, H. K., & Leiter, M. P. (2006). The impact ofnursing work environments on patient safety outcomes: Themediating role of burnout engagement. Journal of Nursing Ad-ministration, 36(5), 259–267.
Stimpfel, A. W., Rosen, J. E., & McHugh, M. D. (2014). Un-derstanding the role of the professional practice environ-ment on quality of care in Magnet R© and non-Magnet hos-pitals. Journal of Nursing Administration, 44(1), 10–16. doi:10.1097/NNA.0000000000000015
Swenson-Britt, E., & Berndt, A. (2013). Development and psy-chometric testing of the nursing research self-efficacy scale(NURSES). The Journal of Nursing Measurement, 21(1), 4–22.
Texas State Board of Nursing. (2014). Texas nursing statistics.Retrieved from: http://www.bne.state.tx.us/reports_and_data_nursing_statistics.asp
Thorsteinsson, H. S. (2013). Icelandic nurses’ beliefs, skills, andresources associated with evidence-based practice and relatedfactors: A national survey. Worldviews on Evidence-Based Nursing,10(2), 116–126.
Tourangeau, A. E, Doran, D. M., McGillis Hall, L., O’Brien Pal-las, L., Pringle, D., Tu, J. V., & Cranley, L. A. (2007). Impact of
20 Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21.C© 2015 Sigma Theta Tau International
Original Articlehospital nursing care on 30-day mortality for acute medical pa-tients. Journal of Advanced Nursing, 57(1), 32–41.
You, L. M., Aiken, L. H., Sloane, D. M., Liu, K., He, G. P., Hu, Y., &Sermeus, W. (2013). Hospital nursing, care quality, and patientsatisfaction: Cross-sectional surveys of nurses and patients in
hospitals in China and Europe. International Journal of NursingStudies, 50(2), 154–161. doi: 10.1016/j.ijnurstu.2012.05.003
doi 10.1111/wvn.12077WVN 2015;12:12–21
Worldviews on Evidence-Based Nursing, 2015; 12:1, 12–21. 21C© 2015 Sigma Theta Tau International
Original Article
Effectiveness of a Brief, Basic Evidence-BasedPractice Course for Clinical NursesAntonio J. Ramos-Morcillo, RN, MSc, PhD • Serafı́n Fernández-Salazar, RN, MSc •Marı́a Ruzafa-Martı́nez, RN, MSc, PhD • Rafael Del-Pino-Casado, RN, MSc, PhD
Keywords
evidence-basedpractice,nursing,
effectiveness,education,
intervention
ABSTRACTBackground: Barriers to the implementation of evidence-based practice (EBP) by nursing profes-sionals include a lack of knowledge, inadequate skills in searching for and appraising evidence,and consulting research articles. However, few studies have addressed the effectiveness of edu-cational interventions to improve their competence.
Aims: To evaluate the effectiveness of a brief basic online and face-to-face educational interven-tion to promote EBP attitudes, knowledge and skills, and practice in clinical care nurses.
Methods: This study was quasi-experimental, pretest-posttest design with a comparison group.The sample included registered nurses enrolled in the free continuing education courses offeredin 2013 by the Nursing Council of Jaén (Spain). The study included 109 participants (54 in theintervention group and 55 in the comparison group). The intervention was a brief, basic EBPcourse with online and face-to-face learning. The comparison group received an educationalintervention with different content. The evidence-based practice questionnaire (EBPQ) was usedto evaluate EBP attitude, knowledge and skills, and practice before the intervention, and at 21and 60 days following the intervention. Two-way mixed analysis of variance was conducted.
Results: There was a significant difference between intervention and comparison groups in theknowledge and skills dimension. The difference between groups was not significant in the EBPpractice dimension. Both groups had high scores in the attitude dimension that did not changeafter the intervention.
Linking Evidence to Action: A brief basic educational intervention on EBP with online andface-to-face learning can produce improvements in the knowledge and skills of clinical nurses.
INTRODUCTIONEvidence-based practice (EBP) is an essential element in thedelivery of optimal care quality. In EBP, healthcare profession-als make clinical decisions based on the best available researchresults while considering the preferences and clinical circum-stances of their patients. EBP implementation has been relatedto improved health outcomes (Meijers et al., 2006) and reducedhealth costs (McGinty & Anderson, 2008). It is also reported toincrease the satisfaction of nursing professionals (Maljanian,Caramanica, Taylor, MacRae, & Beland, 2002), who must meetincreasingly high expectations of care quality on the part of pa-tients and healthcare organizations.
Experts (Frenk et al., 2010) and international organiza-tions have emphasized the need for healthcare professionalsto possess adequate knowledge, skills, and attitudes for EBPimplementation. The Institute of Medicine of the United Statesconsiders EBP to be a central competency for all healthcare pro-fessionals and aims for 90% of health decisions to be basedon optimal evidence by 2020 (McClellan, McGinnis, Nabel,& Olsen, 2007). The International Council of Nurses (2007)
considers EBP a professional responsibility and a central char-acteristic of the work of nurses.
Incorporation of EBP into the clinical practice of nursesinvolves a highly complex behavioral change influenced by var-ious factors, and it has proceeded at a slower pace than desirablesince its inception 20 years ago (Melnyk, 2006). The adoptionand implementation of EBP by nurses has been described asinadequate (Sandström, Borglin, Nilsson, & Willman, 2011).A recent study showed that 34.5% of nursing professionals re-ported that their colleagues implemented EBP in their care,46.4% believed that EBP was routinely applied in their insti-tution, 76.2% reported a need for more knowledge and skillsin EBP, and 72.9% wanted online training on EBP (Melnyk,Fineout-Overholt, Gallagher-Ford, & Kaplan, 2012).
BACKGROUNDThere have been numerous studies on attitudes, knowledge,and skills in relation to EBP, including the practice and uti-lization of EBP (Melnyk et al., 2012; Pravikoff, Pierce, &Tanner, 2005) and the barriers against and opportunities for
Worldviews on Evidence-Based Nursing, 2015; 12:4, 199–207. 199C© 2015 The Authors. Worldviews on Evidence-Based Nursing published by Wiley Periodicals, Inc. on behalf of Sigma Theta Tau International The Honor Society of Nursing.This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs License, which permits use and distribution in any medium, provided theoriginal work is properly cited, the use is non-commercial and no modifications or adaptations are made.
Effectiveness of an EBP Course on Clinical Nurses
its implementation, which were generally classified in relationto the professionals themselves, organizations, and institutionpolicies (Sadeghi-Bazargani, Tabrizi, & Azami-Aghdash, 2014).The main barriers to EBP faced by healthcare professionalsinclude lack of time, inadequate authority to implement thechanges, inadequate numbers of EBP mentors along with aculture and environment that does not support EBP (Melnyk,2014), and a lack of knowledge and skills in searching for andappraising research articles (Sadeghi-Bazargani et al., 2014).Related to the knowledge and skills in EBP, disparities also ex-ist among nurses´ perceptions. In our context, higher scores inknowledge and skills were obtained among nurses with shorterprofessional experience (González-Torrente et al., 2012). Withrespect to attitudes toward EBP, several studies show moder-ate to high scores (Koehn & Lehman, 2008), and highlightthat nurses with positive attitudes are more likely to use EBP(Estabrooks, Floyd, Scott-Findlay, O’Leary, & Gushta, 2003;Melnyk et al., 2004).
FrameworkThe Theory of Planned Behavior (TPB; Ajzen, 1991) is consid-ered appropriate to explain the behavioral intentions of health-care professionals (Eccles et al., 2006; Godin, Bélanger-Gravel,Eccles, & Grimshaw, 2008). According to this theory, behav-ioral intention is explained by attitude, subjective norms, andperceived behavioral control. Attitudes refer to the general eval-uation of behavior and are determined by beliefs about it and byperceptions of its consequences. Subjective norms refer to theperceived social approval of the behavior and are determinedby expectations of approval or disapproval by key referencegroups. Perceived behavioral control refers to the confidenceof individuals in their capacity (knowledge and skills) to carryout a specific behavior and is determined by their perceptionof the opportunities, barriers, and resources involved.
Review of LiteratureVarious educational programs for clinical nurses have beendesigned to reduce the barriers and promote their acquisitionof EBP knowledge and skills (Schulman, 2008; Soukup & Mc-Cleish, 2008). The duration and content of these courses vary,but they all impart basic information on the EBP paradigmand its implementation, and discuss the behavioral changesinvolved. The teaching methodology also differs among pro-grams and includes face-to-face classes, discussion groups, on-line learning, and journal clubs, among others.
Despite the major potential benefits of education and skillsbuilding in EBP and the large number of instruments for itsevaluation (Leung, Trevena, & Waters, 2014), there has beenlittle