Embed Size (px)
Citation preview

Implementation of a Remote Temperature Monitor for the Prevention of Diabetic Foot UlcersA Case Series of Two Patients
Jaminelli Banks, DPM; Aldijan Sabic, DPM; Robert G. Frykberg, DPM; Edward Tierney, DPM; Jaclyn Marino, DPM; Arthur J. Tallis, DPM
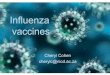
Figure 1 (a) thermogram from Patient 1 on day 12 showing elevated right medial forefoot temperature extending through hallux (b) thermogram on day 22 after patient was asked to reduce step count (c) image of hallux DFU post debridement on day 24 (d) time progression of temperature asymmetry at hallux
Introduction
Diabetic Foot Ulcers (DFU) are known to be associated with increased morbidity, mortality, and healthcare resource utilization. Monitoring plantar foot temperature has previously been demonstrated effective for preventing DFU when used to prompt timely, non-invasive interventions. An in-home, telemedicine, thermometric mat (the Podimetrics system) has recently been studied as part of a multi-center cohort trial to assess its usability and accuracy in predicting plantar DFU [15]. We are implementing this system in a veteran population as a tool for primary and secondary DFU prevention.
Methods
Through October 1, 2016, we have issued the Podimetrics system to 98 veterans at our clinic and have collected nearly 10 patient-years of thermometric data. Veterans were instructed to use the device daily, which requires that the patient stand on it for approximately 20 seconds while it completes a non-invasive thermometric scan of the feet.
Consistent with previous research [12-14], we considered temperature differences between six contralaterally-matched locations on the left and right plantar foot surfaces: the hallux, first, third, and fifth metatarsal heads, arch, and heel. If the temperature difference at one or more location exceeds 2.2 degrees Celsius (4 degrees Fahrenheit) over two or more consecutive scans, the veteran is deemed to have a “hotspot” and is instructed to reduce step-count by 50% for a week. In response to a hotspot and at the discretion of the clinician, a patient may also be referred to schedule an appointment for foot examination.
We present a case series consisting of the two patients who as of October 1, 2016 have most recently presented with hotspots. Each has history of diabetes mellitus, neuropathy, and recently-healed DFU.
Case 1Patient 1 is a 64 year old male with history of diabetes mellitus and elevated HbA1c (8.6% at last reading). The patient has absent protective sensation diagnosed via Semmes Weinstein monofilament exam (0/10 bilaterally). The patient has history of left foot Charcot arthropathy involving the mid and distal tarsal bones as well as the area of tarsometatarsal joints for which he has been prescribed custom Charcot shoes.
The patient presented approximately 5 weeks prior to receiving the Podimetrics system with bilaterally xerotic skin and severe, diffuse hyperkertosis with hemosiderin deposits bilaterally at the sub-hallux and at the left 3rd distal tip. Upon debridement of the right sub-hallux, a DFU measuring 0.3 x 0.3 x 0.1 cm was discovered. The wound was absent of drainage and malodor.
The patient was examined again on 4 days before receiving the Podimetrics system and was noted to have hyperkaratosis at the left medial plantar hallux, right medial plantar hallux, and left sub 3rd metatarsal head. The patient’s wound was found to be epithelized and he was issued the Podimetrics system. The patient has exhibited excellent adherence in the daily use of the mat, averaging 6.4 uses/week over three weeks.
ConclusionsTwo patients with hotspots have been described. Use of the Podimetrics system enabled timely and inexpensive treatment of DFU that otherwise would not have been identified as early under standard preventative care. Early detection may have the potential to limit further tissue damage as well as minimize the risk of infection. Continued implementation of the system may have a significant impact on DFU-related morbidity, mortality, and resource utilization.
These innovations in remote plantar temperature monitoring illustrate an important transfer in diabetic foot care from subjective to objective evaluation of the high-risk patient. They demonstrate clinical value and a large potential in helping to reduce the patient and economic burden of diabetic foot ulcerations.
References1. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;366(9498):1719–1724.2. Bakker K, Apelqvist J, Schaper NC. International Working Group on Diabetic Foot Editorial Board. Practical guidelines on the management and prevention of the diabetic foot 2011.
Diabetes Metab Res Rev. 2012;28(Suppl 1):225–231. 3. Lepäntalo M, Apelqvist J, Setacci C, Ricco JB, de Donato G, Becker F, Robert-Ebadi H, Cao P, Eckstein HH, De Rango P, Diehm N, Schmidli J, Teraa M, Moll FL, Dick F, Davies
AH. Chapter V: diabetic foot. Eur J Vasc Endovasc Surg. 2011;42(Suppl 2):S60–S74. 4. Murf RT, Armstrong DG, Lanctot D, Lavery LA, Athanasiou KA. How effective is manual palpation in detecting subtle temperature differences? Clin Podiatr Med Surg.
1998;15(1):151–154.5. Bharara M, Cobb JE, Claremont DJ. Thermography and thermometry in the assessment of diabetic neuropathic foot: a case for furthering the role of thermal techniques. Int J Low
Extrem Wounds. 2006;5(4):250–2606. Bharara M, Schoess J, Armstrong DG. Coming events cast their shadows before: detecting inflammation in the acute diabetic foot and the foot in remission. Diabetes Metab Res Rev.
2012;28(Suppl 1):15–207. Armstrong DG, Lavery LA, Liswood PJ, Todd WF, Tredwell JA. Infrared dermal thermometry for the high-risk diabetic foot. Phys Ther. 1997;77(2)8. Armstrong DG, Lavery LA. Monitoring neuropathic ulcer healing with infrared dermal thermometry. J Foot Ankle Surg. 1996;35(4):335–3739. Harding JR, Wertheim DF, Williams RJ, Melhuish JM, Banerjee D, Harding KG. Infrared imaging in diabetic foot ulceration. Proc 20th Annual Int Conf IEEE Engineering Med Biol
Soc. 1998;20:916–918.10. Oe M, Yotsu RR, Sanada H, Nagase T, Tamaki T. Thermographic findings in a case of type 2 diabetes with foot ulcer and osteomyelitis. J Wound Care. 2012;21(6):274, 276–27811. Armstrong DG, Lavery LA. Monitoring healing of acute Charcot’s arthropathy with infrared dermal thermometry. J Rehabil Res Dev. 1997;34(3):317–32112. Lavery LA, Higgins KR, Lanctot DR, Constantinides GP, Zamorano RG, Armstrong DG, Athanasiou KA, Agrawal CM. Home monitoring of foot skin temperatures to prevent
ulceration. Diabetes care. 2004 Nov 1;27(11):2642-7.13. Lavery LA, Higgins KR, Lanctot DR, Constantinides GP, Zamorano RG, Athanasiou KA, Armstrong DG, Agrawal CM. Preventing Diabetic Foot Ulcer Recurrence in High-Risk
Patients Use of temperature monitoring as a self-assessment tool. Diabetes care. 2007 Jan 1;30(1):14-20.14. Armstrong DG, Holtz-Neiderer K, Wendel C, Mohler MJ, Kimbriel HR, Lavery LA. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. The
American journal of medicine. 2007 Dec 31;120(12):1042-6.15. Frykberg RG, Rothenberg GM, Fitzgerald RH, et al. Abstract 141-OR/141. An automated home monitor for the early detection of diabetic foot ulcers. Presented at: ADA 76th
Scientific Sessions; June 10-14, 2016; New Orleans, LA.
Case 1 (continued)Almost two weeks after receiving the mat, the patient was found to have a hotspot at the hallux. The patient’s peak temperature difference was 2.8 degrees C. The veteran was notified and instructed to reduce step count, to continue using the mat daily, and to make an appointment for a foot exam. He reported he was unaware of any emergent changes in his feet. The patient’s next scheduled appointment was more than two months later, but the hotspot prompted an interim clinical visit 12 days later. Diffuse hyperkertosis was noted during examination. Upon debridement, a superficial wound with thick hyperkeratotic covering measuring 0.2cm x 0.3cm was identified; it was absent of malodor and drainage. The wound was dressed with Betadine.
Case 2Patient 2 is a 71 year old diabetic male with elevated HbA1c (7.1% at last reading) and extensive history of diabetic foot-related complications requiring previous surgical intervention on both lower extremities. The patient suffered a 4th and 5th ray resection of his left foot and a hallux amputation on his right foot more than 10 years prior to receiving the Podimetrics system. More than a year before issuance, the patient presented with a DFU at the sub 5th metatarsophalangeal joint which subsequently closed a month later. This wound recurred two months prior to receiving the Podimetrics system, and again one month prior, most recently healing a day prior.
Case 2 (continued)The patient was issued the Podimetrics mat to monitor his closed wound for signs of inflammation. Over the three months the patient has had the mat, he has averaged 4.0 uses/week.
Five weeks later, the patient was found to have a hotspot with a peak temperature difference of 3.4 degrees Celsius. Serendipitously, the patient was in the clinic for a routine foot exam on that day. The clinician debrided hyperkeratosis at the right sub 5th metatarsal head and sub 1st metatarsal head.
A month later, the patient again developed a hotspot with a peak temperature difference of 3.8 degrees Celsius. The patient was seen in clinic eight days later for an interim visit due to the hotspot. The clinician again noted a hyperkeratosicright forefoot, and upon debridement, a superficial recurrent DFU at the 5th sub metatarsal head was discovered. The wound was measured to be approximate 0.4 cm in diameter with no sign of infection or drainage. Notably, the clinician reported no increased temperature upon manual palpitation despite the large asymmetries measured by the Podimetrics system. This observation is consistent with previous research [4].
The wound was dressed with Betadine and TELFA. The patient’s right insert was customized to offload pressure to the 5th and 1st metatarsophalangeal joint. The patient was reminded to use the diabetic shoes and custom inserts at all times when ambulating. In a recent followup visit, the clinician noted reduced callousing. The DFU was found to be smaller in diameter (0.2 cm) and absent of malodor and drainage.
(b)(a) (c)
(d)