Embed Size (px)
Citation preview

Balloon Aortic Valvuloplasty
A n d r e w W a n g , J . K e v i n H a r r i s o n , a n d T h o m a s M. B a s h o r e
Balloon aortic valvuloplasty is a percutaneous, thera- peutic option for patients with severe aortic stenosis, yet the effectiveness of this procedure is dependent on the morphology of the stenotic aortic valve and the respective mechanism of dilation. In younger patients with congenital aortic stenosis, acute and intermediate-term results are good. However, in adult patients, in whom degenerative aortic stenosis is the most common cause, the acute clinical and hemodynamic benefits of balloon aortic valvulo- plasty are not lasting, as restenosis occurs in most patients within 6 months. Sympatomatic relief for adults undergoing balloon aortic valvuloplasty is only apparent in patients with normal left ventricular function, who generally are also candidates for aortic valve replacement. Furthermore, the long- term survival for adults after balloon aortic valvulo- plasty is similar to the natural history of untreated severe aortic stenosis. In this article, the mechanism of balloon aortic vaIvuloplasty, as well as its clinical and hemodynamic effects, are reviewed in the context of the different morphological types of aortic stenosis. In addition, two large registries of adult patients treated with balloon aortic valvuloplasty provide important information regarding the acute and long-term results of this procedure and are reviewed. Copyright © 1997 by W.B. Saunders Company
l 'n 1984, Lababidi et al first described the use of .balloon valvuloplasty in a pediatric population
with congenital aortic stenosis. 1 Two years later, Cribier et al reported the use of this procedure in three elderly patients with calcific aortic steno- s i s . 2 Studies which reported the acute clinical and hemodynamic effects of balloon aortic valvulo- plasty soon led to widespread interest in this percutaneous intervention as an alternative to aortic valve replacement, particularly for elderly patients with a high operative risk. However, since these initial reports, knowledge of the anatomic, hemodynamic, and clinical effects of balloon aortic valvuloplasty has not only grown considerably in a short time, but has limited the
role of this procedure for the treatment of aortic stenosis in the adult population. Specifically, two large registries with a combined enrollment of more than 1,100 adult patients have reported acute 3,4 and long-term 5.6 results of balloon aortic valvuloplasty and form the basis for understand- ing the current role of this procedure.
Etiologies of Aortic Stenosis
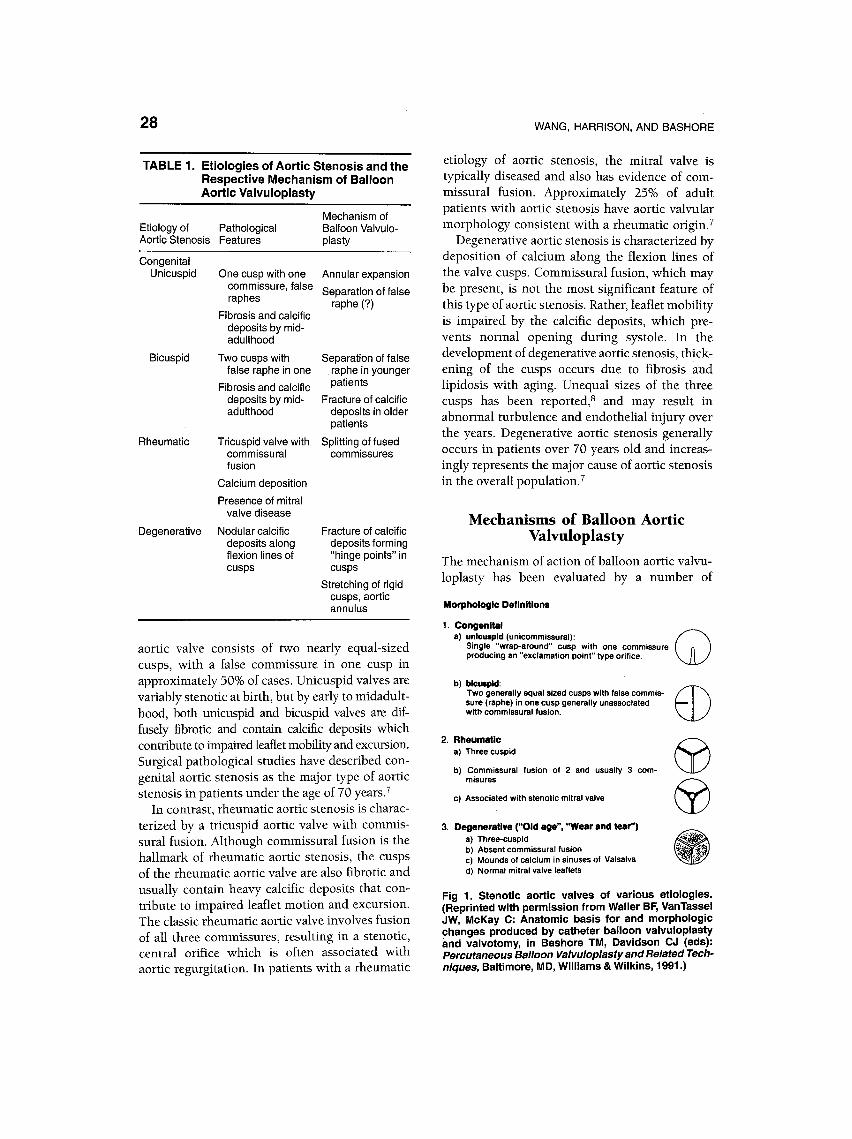
An understanding of the different etiologies or pathological types of aortic stenosis is essential for understanding the mechanism of balloon aortic valvuloplasty (Table 1). Aortic stenosis can be broadly grouped into three types which to- gether account for more than 95% of cases of aortic stenosis: congenital, rheumatic, and degen- erative disease (Fig 1). The determination of the etiology of aortic stenosis had largely been based on surgical or pathological examinations of ste- notic valves, r,s but two-dimensional echocardiog- raphy, particularly the parasternal short-axis view at the level of the aortic valve, offers an excellent noninvasive assessment of the morphology of aortic stenosis. In addition to the morphological appearance of the aortic valve, the age of the patient and the presence or absence of other valvular disease are helpful in determining the etiology of aortic stenosis in an individual patient.
Congenital aortic stenosis is primarily due to a unicuspid or bicuspid aortic valve. The unicuspid aortic valve usually consists of a single circumfer- ential cusp with one commissure, and potentially two false commissures, or raphes, at the expected sites of the other two commissures. The bicuspid
From the Division of Cardiology, Duke University Medi- cal Center, Durham, NC.
Address reprint requests to Thomas M. Bashore, MD, Box 3012, Duke University Medical Center, Durham, NC 27710.
Copyright © 1997 by W.B. Saunders Company 0033 -0620/97/4001-000355.00/0
Progress in Cardiovascular Diseases, Vol. 40, No. 1 (July/August), 1997: pp 27-36 27
28
T A B L E 1. Et io logies of Aort ic S tenos is and the Respect ive M e c h a n i s m of Bal loon Aort ic Va lvuloplasty
Etiology of Pathological Aortic Stenosis Features
Mechanism of Balloon Valvulo- plasty
Congenital Unicuspid
Bicuspid
One cusp with one Annular expansion commissure, false Separation of false raphes raphe (?)
Fibrosis and calcific deposits by mid- adulthood
Two cusps with false raphe in one
Fibrosis and calcific deposits by mid- adulthood
Rheumatic Tricuspid valve with commissural fusion
Calcium deposition
Presence of mitral valve disease
Degenerative Nodular calcific deposits along flexion lines of cusps
Separation of false raphe in younger patients
Fracture of calcific deposits in older patients
Splitting of fused commissures
Fracture of calcific deposits forming "hinge points" in cusps
Stretching of rigid cusps, aortic annulus
aortic valve consists of two nearly equal-sized cusps, with a false commissure in one cusp in approximately 50% of cases. Unicuspid valves are variably stenotic at birth, but by early to midaduh- hood, both unicuspid and bicuspid valves are dif- fusely fibrotic and contain calcific deposits which contribute to impaired leaflet mobility and excursion. Surgical pathological studies have described con- genital aortic stenosis as the major type of aortic stenosis in patients under the age of 70 years. 7
In contrast, rheumatic aortic stenosis is charac- terized by a tricuspid aortic valve with commis- sural fusion. Although commissural fusion is the hallmark of rheumatic aortic stenosis, the cusps of the rheumatic aortic valve are also fibrotic and usually contain heavy calcific deposits that con- tribute to impaired leaflet motion and excursion. The classic rheumatic aortic valve involves fusion of all three commissures, resulting in a stenotic, central orifice which is often associated with aortic regurgitation. In patients with a rheumatic
WANG, HARRISON, AND BASHORE
etiology of aortic stenosis, the mitral valve is typically diseased and also has evidence of com- missural fusion. Approximately 25% of adult patients with aortic stenosis have aortic valvular morphology consistent with a rheumatic origin. 7
Degenerative aortic stenosis is characterized by deposition of calcium along the flexion lines of the valve cusps. Commissural fusion, which may be present, is not the most significant feature of this type of aortic stenosis. Rather, leaflet mobility is impaired by the calcific deposits, which pre- vents normal opening during systole. In the development of degenerative aortic stenosis, thick- ening of the cusps occurs due to fibrosis and lipidosis with aging. Unequal sizes of the three cusps has been reported? and may result in abnormal turbulence and endothelial injury over the years. Degenerative aortic stenosis generally occurs in patients over 70 years old and increas- ingly represents the major cause of aortic stenosis in the overall population. 7
Mechanisms of Balloon Aortic Valvuloplasty
The mechanism of action of balloon aortic valvu- loplasty has been evaluated by a number of
Morphologlc Definitions
1. Congenital a) unicuspld (unicommissural):
Single "wrap-around" cusp with one commissure producing an "exclamation point" type orifice.
b) bicuspid: Two generally equal sized cusps with false commis- sure (raphe) in one cusp generally unassociated with commissural fusion.
2. Rheumatic a) Three cuspid
b) Commissural fusion of 2 and usually 3 com- misures
c) Associated with stenotic mitral valve
3. DegeneratlYe ("Old age", "Wear and tear") a) Three-cuspid b) Absent commissural fusion c) Mounds of calcium in sinuses of Valsalva d) Normal mitral valve leaflets
©
@ @
Fig 1. Stenotic aortic valves of various etiologies. (Reprinted with permission from Waller BF, VanTassel JW, McKay C: Anatomic basis for and morphologic changes produced by catheter balloon valvuloplasty and valvotomy, in Bashore TM, Davidson CJ (eds): Percutaneous Balloon Valvuloplasty and Related Tech- niques, Baltimore, MD, Williams & Wilkins, 1991.)

BALLOON AORTIC VALVULOPLASTY 29
methods: postmortem studies of dilated valves, examination of surgically excised valves, direct intraoperative inspection at the time of valve replacement, and noninvasively by two-dimen- sional echocardiography. 9-16 Balloon aortic valvu- loplasty may alter the stenotic aortic valve in various ways, including fracture of calcific nod- ules (resulting in increased cusp flexibility), annu- lar stretching, cusp tearing and splitting of valve commissures. 9-16 Importantly. the mechanism of balloon aortic valvuloplasty is largely determined by the etiology and pathological features of the stenotic aortic valve.
Within the group of patients with congenital aortic stenosis, factors such as the age of the patient and the number of valve commissures strongly influence the mechanism of balloon dilatation. In a group of young patients with congenital aortic stenosis (mean age = 9 -+ 9 years) examined by two-dimensional echocardiog- raphy after balloon aortic valvuloplasty. Sholler et al a5 described separation of a fused commissure by division of either the site of major or minor fusion in 24 patients with bicuspid aortic valves. On the other hand, in a population of older patients with congenital aortic stenosis (mean age = 54 years), Waller 9,1° reported that patients with bicuspid valves had evidence of cracking of calcific nodules and aortic wall expansion at nonfused commissure sites. Thus, the presence of aortic valve calcification in older patients with congenital aortic stenosis seems to alter the mechanism by which balloon aortic valvuloplasty may be efficacious. Of note, the mechanism of balloon aortic valvuloplasty in eight patients with unicuspid aortic valves was not reported by Sholler. is In the Waller series, 9,1° only one unicom- missural aortic valve was dilated and examined, with evidence of aortic valve expansion at the single nonfused commissure but without evi- dence of cuspal tearing or cracking of calcific nodules. Thus, within the group of patients with congenital aortic stenosis, the mechanism of action of balloon aortic valvuloplasty has been dependent on the age of the patient (which is associated with calcific deposits on the valve) as well as whether the aortic valve is unicuspid or bicuspid.
Balloon aortic valvuloplasty of rheumatic aortic stenosis has been found to result in splitting of fused commissures with minimal cuspal injury
and aortic wall expansion, and this type of aortic stenosis may be optimal for intervention with this procedure.9,1°, 14 However, the decreasing preva- lence of rheumatic heart disease in Western countries and the high incidence of associated aortic regurgitation are limiting factors to its applicability, and no studies have directly ad- dressed the clinical results of balloon aortic valvuloplasty in this patient population.
Finally, balloon aortic valvuloplasty performed in patients with degenerative aortic stenosis has been found to cause gross fracture of calcific nodules in the cusps of the valve. 9-1s The fracture sites form "hinge points" which allow increased leaflet mobility and excursion. 915 Although stretching of rigid valve cusps with or without fracture of calcific nodules has also been noted after balloon valvuloplasty and may result in an acute increase in aortic valve area, recoil of the leaflets has been noted soon after the procedure and may contribute to early restenosis. 9,z°,14
Procedure
Balloon aortic valvuloplasty is usually performed via a retrograde femoral approach, but may also be accomplished via a retrograde brachial ap- proach (in patients with significant peripheral vascular disease) or an antegrade transseptal approach. The retrograde femoral approach is simpler and can be performed in the vast majority (99%) of patients. There are multiple types of balloons which may be used for balloon aortic valvuloplasty: one balloon (single shaft), multiple balloons (with multiple shafts), or complex bal- loon configurations (bifoil or trefoil balloons on a single shaft) (Fig 2). In a majority of cases in which multiple balloons are eventually employed, dilatation with a single balloon is initially at- tempted. Use of double ballloons results in an obvious greater expansion of the aortic orifice. The complex configurations are thought to allow blood flow across the aortic valve during balloon inflation, perhaps reducing the hemodynamic disturbance of balloon inflation in patients with poor left ventricular function, severe coronary artery disease, or cerebrovascular disease. How- ever, there are no data to support a distinct clinical advantage with the use of these designs.
The choice of balloon size(s) is made on the basis of either aortic annulus diameter or area. In

30 WANG, HARRISON, AND BASHORE
Fig 2. Various balloon con- figurations used for balloon aortic valvuloplasty. (A) Low- profile polyethylene balloons, in inflated diameters of 15 and 20 mm (Courtesy of SClMED, Boston Scientific Corp). (B) Pigtail balloon catheters, in inflated diameters of 15 and 20 mm (Courtesy of SCIMED, Boston Scientific Corp). (C) Complextrifoil ballon (3 x 10 mm) design (Reprinted with permission from Bashore and Davidson (eds): Percutaneous Balloon Valvuloplasty and Re- lated Techniques. Williams & Wilkins, 1991). (D) Complex bifoil balloon (2 x 15 mm) design (Reprinted with per- mission from Bashore and Davidson (eds): Percutaneous Balloon Valvuloplasty and Re- lated Techniques. Williams & Wilkins, 1991).
children, fo,r balloon size based on aortic annulus diameter, the sum of the inflated balloon diameter should equal 1.2 to 1.3 times the diameter of the aortic annulus when two balloons are employed or equal to the diameter of the annulus when a single balloon is used. Similarly, in adults, the ratio of balloon area to aortic annulus area should be limited to -<1.2 as the risk of leaflet avulsion is increased above this size ratio. The most com- monly used single balloon sizes in the NHLBI Balloon Valvuloplasty Registry was 20 mm (56%) or 23 mm (37%). 4 With the use of multiple balloons, the average diameter pair was 35 mm (range 30 to 46 mm), with the most common pairing being of 15 and 20-mm balloons. 4
Patient Selection
Absolute contraindications to balloon aortic val- vuloplasty include the presence of left ventricular thrombus and moderate to severe aortic regurgita- tion. Because myocardial ischemia frequently oc- curs during balloon inflation, significant left main coronary artery disease is also an absolute contra- indication. The presence of left atrial thrombus is a contraindication to balloon aortic valvuloplasty via the transseptal approach.
In the adult patient population, the indications for balloon aortic valvuloplasty have primarily been the advanced age of the patient and the
presence of comorbid illness, factors which are associated with a higher operative risk. The mean age of the patients in studies of adults treated with balloon aortic valvuloplasty has been greater than 75 years, and thus, the vast majority of these patients had degenerative, calcific aortic stenosis.
Complications
The major complications of balloon aortic valvu- loplasty are listed in Table 2. Procedural mortality has been reported in 3% to 5% of cases, 3,4 with the
TABLE 2. Acute Complications of Balloon Aortic Valvuloplasty in the NHLBI Balloon Valvuloplasty Registry 4 and Mansfield Scientific Aortic Valvuloplasty Registry 3
NHLBI Mansfield Complication Registry, % Registry, %
Total acute complications 25 21 Procedural mortality 3 5 Vascular trauma 11
Blood transfusion 20 Surgery 5 6
Severe aortic regurgitation 1 1 Embolic events 4 2 Ventricular perforation 1 2 Myocardial infarction 1
NOTE. NHLBI Registry = 674 patients, Mansfield Regis- try = 492 patients.

BALLOON AORTIC VALVULOPLASTY 31
majority of deaths due to cardiac causes. Overall in-hospital mortality occurs in 8% to 10% of patients who undergo balloon aortic valvulo- plasty, Cardiovascular mortality in these patients is usually due to cardiogenic shock, sudden cardiac death, or cardiac tamponade due to left ventricular perforation. After discharge within the 30 days after the procedure, death occurs in a small percentage of patients. In the NHLBI Bal- loon Valvuloplasty Registry, 30-day mortality was related to evidence of cardiogenic shock (class IV congestive heart failure and systolic blood pres- sure <100 mm Hg), low cardiac output (---3.0 L/min), renal dysfunction, and use of antiarrhyth- mic agents. 4
Based on two large registries of patients who underwent balloon aortic valvuloplasty, 3,4 proce- dural and acute nonfatal complications occur in 21% to 25% of patients. Local vascular injury was the most common complication, occurring in approximately 10% of cases, and often necessi- tated blood transfusion. 3,4 Of patients with periph- eral arterial injury following balloon aortic valvu- loplasty, surgical intervention was required in as many as 50%. 3,4 Damage to the arterial access site was primarily due to trauma from the large, deflated valvuloplasty balloon, and use of larger balloons and multiple balloons may increase the risk of this complication. It has been reported that the use of lower-profile balloon catheters, which may be inserted and removed through percutane- ous arterial sheaths, reduces the risk of local arterial complications. 18
Aortic regurgitation may increase in patients following balloon aortic valvuloplasty, but signifi- cant increases have been observed in only 1% to 2% of patients. 3,4 Letac et al observed significant aortic regurgitation in only 3% of patients after balloon aortic valvuloplasty if aortic regurgitation was present before the procedure. 19 Among 492 patients in the Mansfield Scientific Aortic Valvulo- plasty Registry, acute severe aortic regurgitation developed in only four patients (0.8%), none of whom had significant aortic regurgitation before balloon aortic valvuloplasty,* Mechanisms of acute, severe aortic regurgitation have included annular dehiscence and intraleaflet tearing between cal- cific deposits or due to partial fusion of one leaflet. 2°,2I Possible risk factors for developing severe aortic regurgitation following balloon aor- tic valvuloplasty are an increased balloon to aortic
annulus ratio (use of oversized balloons) 21 and dilation of unicommissural valves.J6 In a minority of patients, the severity of aortic regurgitation may be decreased following balloon aortic valvu- loplasty, presumably as a result of improved leaflet coaptation.
Clinical embolic events occur in approximately 2% to 4% of cases, 3,4 and may manifest as either acute focal neurological deficits or evidence of systemic embolization. It is possible that embolic events occur more frequently but remain asymp- tomatic. 37 These events may result from small calcific or thrombotic emboli from the aortic valve or the left ventricular chamber. The rela- tively low incidence of this complication, even in studies primarily involving patients with calcific aortic stenosis, may be related to endothelializa- tion of the calcium, 12 which theoretically would prevent embolization of debris during fracturing of calcific nodules.
Ventricular perforation is an uncommon but often fatal complication (approximate incidence of 2% but with a mortality rate ~50%). 3,4,20 The mechanism of ventricular perforation may in- volve perforation by the wire alone, diagnostic catheter alone, the balloon catheter alone, or a combination of wire and balloon catheter. How- ever, Cribier et al, using balloon catheters with a pigtail curve on their distal ends, reported a decrease in the incidence of pericardial tampon- ade following balloon aortic valvuloplasty from 2% to 0.7%. 18
Arrhythmia during the procedure is an infre- quent complication but may manifest in a variety of forms including ventricular ectopy (from mo- tion of the guidewire and balloon catheter within the left ventricular chamber), atrial arrhythmia (from rapid changes in left ventricular filling pressure associated with balloon inflation), and atrioventricular and intraventricular conduction defects.
Despite the presence of significant coronary artery disease in many patients, the reported incidence of myocardial infarction following the procedure is low (< 1%). However, transient myo- cardial ischemia has been documented by studies of coronary flow and metabolism, including evi- dence of ischemia seen in the absence of coronary artery disease. 22,23 Transient ischemia may occur as a result of a number of different mechanisms during balloon inflation, including transient hypo-

32 WANG, HARRISON, AND BASHORE
tension from obstruction of left ventricular out- flow, transient interruption of coronary artery perfusion, and increased left ventricular wall stress with increased myocardial oxygen demand.
Acute Results
The majority of patients who undergo balloon aortic valvuloplasty experience short-term symp- tomatic improvement, with improvement in all of the cardinal symptoms of aortic stenosis (conges- tive heart failure, angina, and syncope). In studies of balloon aortic valvuloplasty, congestive heart failure has been the most common indication for performing the procedure, with approximately 75% of patients in NYHA class III or IV at baseline. 3,4,24-26 In the NHLBI Balloon Valvulo- plasty Registry of 484 survivors at 30-day follow- up, 75% experienced at least one NYHA class improvement in symptoms of heart failure (or were unchanged if they were functional class I at baseline) and only 30% remained in class III or IV. 4 However, short-term symptomatic benefit has been found to be dependent on left ventricular systolic function at baseline, as patients with depressed ejection fractions (<45%) had a much higher likelihood of recurrent symptoms at 3 months compared with patients with preserved systolic function (recurrent symptoms in 60% v 16%, respectively) 37 (Fig 3). Short-term improve- ments in the severity of angina and occurrence of syncope have similarly been reported. 24-26
For balloon aortic valvuloplasty, an unsuccess- ful procedure has been defined as procedural or in-hospital death, aortic valve replacement within
6O
,,o ,.0
o 20 0_
(n=25)
(n=44)
_>45 <45 <35 <25 Baseline LVEF (%)
Fig 3. Probability of recurrent symptoms at 3 months after balloon aortic valvuloplasty based on baseline left ventricular ejection fraction (LVEF). (Reprinted by permission of the publisher from Davidson CJ et al, American Journal of Cardiology, 60:72-77. Copyright 1990 by Excerpta Medica, Inc.)
the first 7 days after the procedure, or minimal change in aortic valve area or mean aortic valve gradient. In all reported series, balloon aortic valvuloplasty has been performed with success in the vast majority of patients (>80%).3.4.24-26 Most series have reported an acute decrease in the mean aortic valve gradient of approximately 50%. In the two largest registries, the mean aortic valve gradient fell from 55 -+ 21 mm Hg to 29 _+ 13 mm Hg (NHLBI Registry) 4 and 60 -+ 23 mm Hg to 30 -- 13 mm Hg (Mansfield Registry). 3 Both registries reported an increase in aortic valve area from 0.5 + 0.2 cm 2 to 0.8 -+ 0.3 cm 2 with similar results reported in other series. 24-3°
In both registries, 3,4 use of two balloons during the procedure was associated with a greater decrease in mean aortic valve gradient but this effect likely reflects the use of two balloons when dilation with one balloon was initially unsuccess- ful. Factors associated with a greater increase in valve area have been less consistent among differ- ent studies. Finally, despite the different morpho- logical types of aortic stenosis and the associated mechanisms of balloon aortic valvuloplasty, stud- ies of congenital aortic stenosis have reported similar decreases in the aortic valve gradient following the procedure as compared with studies of calcific, or degenerative, aortic stenosis. 16,31
Other acute hemodynamic effects following balloon aortic valvuloplasty reflect acute reduc- tions in afterload and preload. Immediately after the procedure, left ventricular systolic pressure, left ventricular end-diastolic pressure, and mean pulmonary artery pressure fall significantly and arterial systolic pressure increases. 27,2s,3° Cardiac output increases minimally or may remain un- changed. 27-3° Left ventricular ejection fraction increases slightly immediately after balloon aortic valvuloplasty. Although the increase in ejection fraction (EF) is minimal in patients with pre- served left ventricular systolic function, a greater increase has been seen in patients with impaired left ventricular systolic function (EF < 50%) at baseline 27-29 and this improvement has been found to continue in the months after the procedure. 2s,3° Thus, the hemodynamic changes following bal- loon aortic valvuloplasty result in improved left ventricular systolic performance acutely, espe- cially in patients with a decreased EF at baseline, consistent with the "afterload mismatch" effect of aortic stenosis. The continued improvement in

BALLOON AORTIC VALVULOPLASTY 33
EF in the months after the procedure suggests that left ventricular remodeling may occur, a hypothesis supported by a decrease in left ven- tricular end-diastolic volume seen months, but not acutely, after balloon aortic valvuloplasty in patients with left ventricular dilatation. 3°
Intermediate and Long-term Results
The symptomatic benefit of balloon aortic valvu- loplasty which is seen immediately after the procedure persists, but occurs in the setting of restenosis of the aortic valve and decreasing overall survival. In the NHLBI Balloon Valvulo- plasty Registry, the functional status score at 3-year follow-up remained similar to the func- tional status at 5 weeks and was greater than the baseline functional status. 6 However, of the 674 patients in the registry, only 78 (11%) were alive and in NYHA class I or II at 2-year follow-up. 6 Similarly, in the Mansfield Scientific Balloon Aor- tic Valvuloplasty Registry of 492 elderly patients, 66% were in NYHA class I or II at 1 year as compared with only 18% at baseline. 5 However, the one year survival rate was only 64% and the event-free survival rate (absence of death, repeat valvuloplasty, or valve replacement) was 43%. 5
In contrast with the overall symptomatic ben- efit, the effects of balloon aortic valvuloplasty on the aortic valve gradient and area in adult patients have been discouraging. Restenosis following ini- tially successful balloon aortic valvuloplasty has been defined as a 50% decrease in the initial improvement in the aortic valve area. The pathol- ogy of restenosis has not been well described, but thrombosis with ingrowth of fibroblasts and capil- laries have been seen in postmortem examina- tions of aortic valves after balloon valvuloplasty, 12 suggesting that restenosis is a response to injury It is likely that annular recoil also contributes greatly to restenosis in calcific valves without commissural fusion.
Few studies have evaluated patients systemati- cally after balloon aortic valvuloplasty. In studies that evaluated both asymptomatic and symptom- atic patients, restenosis was found in 24% to 76% of patients at approximately 6 months after the procedure. 25'26,29,3° Yet patients often remained asymptomatic despite evidence of restenosis. Whereas the majority of adult patients with recurrent symptoms had evidence of restenosis,
24% to 57% of asymptomatic patients also showed restenosis. 25,26,29 There is evidence that the contin- ued symptomatic benefit from balloon aortic valvuloplasty is dependent on left ventricular systolic function at baseline and improved dia- stolic function after valvuloplasty. 38,39 In patients with impaired systolic function (EF < 45%) at baseline, the likelihood of recurrent symptoms is high. 38 Furthermore, in patients with continued symptomatic benefit at 6 months, diastolic perfor- mance measures were consistently improved com- pared to those in whom symptoms had re- curred. 39 Recurrence of symptoms at 6 months appeared independent of restenosis (which was apparent in the majority of patients) but rather, were dependent on diastolic abnormalities (Fig 4))9
In studies of patients with congenital aortic stenosis, however, the intermediate hemody- namic results have been significantly better. In two studies of children with mean follow-up of 20 to 42 months after balloon aortic valvuloplasty, the peak aortic valve gradient as assessed by catheterization or Doppler echocardiography was significantly lower than baseline values and un- changed from postballoon valvuloplasty val- ues. 32'33 This difference in restenosis rates be- tween adult and pediatric patients emphasizes the
+60
+50
+40
Change from +30 Pre-R3AV to *20
Follow=up (%} *10
0
-10
-20
-30
-40
p value
[ ] Group I (n.16) • Group 2 (n-R)
AVA CO EF EDP EDV PFR TAU Kp PWT LVMI .80 30 ;30 ,04 .04 .0001 ,008 .001 .29 .004
Fig 4. Changes in hemodynamic and echocardio- graphic variables from before valvuloplasty to repeat catheterization at 6 months, depicting improvement in diastolic function variables in patients with symptom- atic improvement (group 1) compared with patients with recurrent symptoms (group 2). Bars represent median % change from before valvuloplasty (pre- PBAV) to repeat catheterization. AVA = aortic valve area; CO = cardiac output; EDP = end-diastolic pres- sure; EDV = end-diastolic volume; EF = ejection fraction; Kp = modulus of chamber stiffness; LVMI = left ventricular mass index; PFR = peak filling rate; PW=I" = posterior wall thickness; TAU = time constant of isovolumetric relaxation. (Reprinted with permis- sion of the publisher, from Sheikh et al, Journal of the American College of Cardiology, 16:795-803, 1990.)

34 WANG, HARRISON, AND BASHORE
importance of the morphological type of aortic' stenosis and the respective mechanism of balloon valvuloplasty on restenosis.
The evidence of restenosis soon after balloon aortic valvuloplasty is consistent with the poor long-term results in adult patients with aortic stenosis who undergo the procedure. The Mans- field Registry reported a 1-year survival rate of 66% and an event-free survival rate, defined as the absence of death, repeat valvuloplasty or aortic valve replacement, of 43%. 5 The NHLBI Registry reported a similar 1-year survival rate of 55%, and a 3-year survival rate of only 23%. 6 Although these registries lacked control groups of patients with severe, symptomatic aortic stenosis, O'Keefe et al described similar actuarial survival rates in 50 elderly patients with severe aortic stenosis in whom balloon aortic valvuloplasty or aortic valve replacement was not performed (1-, 2-, and 3-year survival rates of 57%, 37%, and 25%, respectively).34 Thus, balloon aortic valvuloplasty does not appear to alter the natural history of severe aortic stenosis.
Among patients undergoing balloon aortic val- vuloplasty, certain factors have been found to predict long-term survival. The Mansfield and NHLBI registries, as well as results from the authors' institution of 165 patients with median follow-up of 3.9 years, have consistently found that left ventricular systolic function is the most important determinant of long-term survival after balloon aortic valvuloplasty. 5'6'35 Other important independent variables included younger age, base- line functional status and factors reflecting comor- bid illness (such as the presence of significant coronary artery disease, renal insufficiency, or cachexia).5,6,35 In the NHLBI Registry, a 'low risk' subgroup of patients with minimal functional limitation and preserved left ventricular systolic function was found to have a 2-year survival of 53% compared with 'high risk' patients with more functional limitation, decreased left ventricular systolic function, or both, who had a survival rate of 28%. 6 Interestingly, variables associated with a procedural success, such as greater aortic valve area or lower aortic valve gradient after valvulo- plasty, have not been found to be important predictors of long-term survival, which is consis- tent with the lack of effect of balloon aortic valvuloplasty on the natural history of degenera- tive aortic stenosis.
Role of Aortic Valve Replacement After Balloon Valvuloplasty
In assessing long-term survival, it is important to discuss the role of aortic valve replacement in patients who have undergone balloon aortic valvu- loplasty. It is well known that the age of the patient is an important factor in the operative mortality of aortic valve replacement, with an operative mortality as high as 30% in patients older than 80 years. 36 However, compared with the survival of patients who undergo balloon aortic valvuloplasty alone, those patients who underwent subsequent aortic valve replacement had a better survival. Among patients at the authors' institution, the 1-year survival in pa- tients treated by balloon valvuloplasty and subse- quent aortic valve replacement was 95%, com- pared with 52% in patients treated by balloon valvuloplasty alone 35 (Fig 5). In the NHLBI Regis- try, 20% of patients underwent aortic valve replace- ment at 10 +- 10 days after balloon valvuloplasty and had a 2-year survival rate of 71% compared with 35% for all patients in the registry. 6 However, it should be recognized that these patients who have undergone subsequent aortic valve replace- ment constitute a lower risk group, with slightly lower age and better functional status. 6,35
Conclusion
Although balloon aortic valvuloplasty can be performed safely and successfully in the majority of patients with severe aortic stenosis, the effective- ness of the procedure is largely dependent on the morphological type of aortic stenosis and the respective mechanism of dilatation of the stenotic valve. Acute and intermediate-term results in younger patients with congenital aortic stenosis are good, with little evidence of restenosis within this interval. In adult patients, in whom degenera- tive aortic stenosis is the most common cause, symptomatic and hemodynamic benefits are acutely apparent, but restenosis is evident in approximately 50% by 6 months and universal in longer-term studies. Furthermore, long-term sur- vival after balloon aortic valvuloplasty is poor and does not appear to differ from the natural history of untreated severe aortic stenosis. Because symp- tomatic benefit may persist despite evidence of restenosis, balloon aortic valvuloplasty can be

BALLOON AORTIC VALVULOPLASTY 35
Fig 5. Actuarial survival from the time of balloon aortic val- vuloplasty in patients treated by valvuloplasty alone (BAV only) and those who subse- quently underwent aortic valve replacement (BAV + AVR). (Reprinted by permission of the publisher from Lieberman et al, Journal of the Ameri- can College of Cardiology, 26:1522-1528, 1995.)
100 . - I
~m'~4<o 050- 0 . 2 5 - ~
:z.--..- BAV ONLY o ~ - BAV+ AVR
0.00 0 i 3
YEARS n = 123 60 31 14 E~AV Or l l y
n = 4 2 35 3 0 18 B A Y + A V R
employed as a palliative procedure in symptom- atic patients who are not candidates for aortic valve replacement due to comorbid illness or advanced age. However, palliative benefit is likely only in patients with preserved left ventricular function. Finally, in the authors ' experience, the use of balloon aortic valvuloplasty as a means to reduce the risk of noncardiac surgery or as a bridge to future aortic valve replacement in pa- tients with severe heart failure or transient comor- bid illness has not been beneficial.
References
1. Lababidi Z, Jiunn-Ren W, Wails JT: Percutaneous balloon aortic valvuloplasty. Am J Cardio153:194-197, 1984
2. Cribier A, Saoudi N, Berland J, et al: Percutaneous transluminal valvuloplasty of acquired aortic stenosis in elderly patients: An alternative to valve replace- ment? Lancet 1:63-67, 1986
3. McKay RG: The Mansfield Scientific Aortic Registry. The Mansfield Scientific Aortic Valvuloplasty Registry: Overview of acute hemodynamic results and proce- dural complications. J Am Coil Cardiol 17:485-491, 1991
4. NHLBI Balloon Valvuloplasty Participants. Percutane- ous balloon aortic valvuloplasty Acute and 30-day follow-up results in 674 patients from the NHLBI Balloon Valvuloplasty Registry. Circulation 84:2383- 2397, 1991
5. O'Neill WW: The Mansfield Scientific Aortic Valvulo- plasty Registry. Predictors of long-term survival after percutaneous aortic valvuloplasty: Report of the Mans- field Scientific Balloon Aortic Valvuloplasty Registry. J Am Coil Cardio117:193-198, 1991
6. Otto CM, Mickel MC, Kennedy JW, et al: Three-year outcome after balloon aortic valvuloplasty Insights into
prognosis of valvular aortic stenosis. Circulation 89: 642-650, 1994
7. Passik CS, Ackermann DM, Pluth JR, et al: Temporal changes in the causes of aortic stenosis: A surgical pathologic study of 646 cases. Mayo Clin Proc 62:119- 123, 1987
8. Subramanian R, Olson L J, Edwards WD: Surgical pathology of pure aortic stenosis: A study of 374 cases. Mayo Clin Proc 59:683-690, 1984
9. Waller BF, McKay C, VanTassel JW, et al: Catheter balloon valvuloplasty of stenotic aortic valves Part I: Anatomic basis and mechanisms of balloon dilation. Clin Cardio114:836-846, 1991
10. Waller BF, Dorros G, Lewin RF, et al: Catheter balloon valvuloplasty of stenotic aortic valves--Part I1: Balloon valvuloplasty during life subsequent tissue examina- tion. Clin Cardio114:924-930, 1991
11. Isner JM, Sameuls DA, Siovenkai GA, et al: Mecha- nism of aortic balloon valvuloplasty: Fracture of valvu- lar calcific deposits. Ann Int Med 108:377-380, 1988
12. Berdoff RL, Strain J, Crandall C, et al: Pathology of aortic valvuloplasty: Findings after postmortem suc- cessful and failed dilatations. Am Heart J 117:688-690, 1989
13. Kennedy KD, Hauck A J, Edwards WD, et al: Mecha- nism of reduction of aortic valvular stenosis by percu- taneous transluminal balloon valvuloplasty: Report of five cases and review of literature. Mayo Clin Proc 63:769-776, 1988
14. McKay RG, Safian RD, Lock JE, et al: Balloon dilata- tion of calcific aortic stenosis in elderly patients: Postmortem, intraoperative, and percutaneous valvu- Ioplasty studies. Circulation 74:119-125, 1986
15. Safian RD, Mandell VS, Thurer RE, et al: Postmortem and intraoperative balloon valvuloplasty of calcific aortic stenosis in elderly patients: Mechanisms of successful dilation. J Am Coil Cardiol 9:655-660, 1987
16. Sholler GF, Kean JF, Perry SB, et al: Balloon dilation of congenital aortic stenosis Results and influence of
36
technical and morphological features on outcome. Circulation 78:351-360, 1988
17. Robicsek F, Harbold NB: Limited value of balloon dilatation in calcified aortic stenosis in adults: Direct observations during open heart surgery. Am J Cardiol 60:857-864, 1987
18. Cribier A, Gigera F, Eltchaninoff H, et al: New develop- ments in aortic balloon valvuloplasty. J Am Coil Cardiol 13:17A, 1989 (abstr)
19. Letac B, Gerber LI, Koning R: Insights on the mecha- nism of balloon valvuloplasty in aortic stenosis. Am J Cardio162:1241-1247, 1988
20. Isner JM and the Mansfield Scientific Aortic Valvulo- plasty Investigators: Acute catastrophic complications of balloon aortic valvuloplasty. J Am Coil Cardiol 17:1436-1444, 1991
21. Lewin RF, Dorros G, King JF, et al: Aortic annular tear after valvuloplasty: The role of aortic annulus echocar- diographic measurement. Cath Cardiovasc Diag 16: 123-129, 1989
22. Rousseau MF, Wyns W, Hammer F, et al: Changes in coronary blood flow and myocardial metabolism dur- ing aortic balloon valvuloplasty. Am J Cardio161:1080- 1084, 1988
23. Moore JW, Slack MC, Kirby WC, et al: Hemodynamics and coronary blood flow during experimental aortic valvuloplasty: Comparison of the dual versus the single catheter methods. Am Heart J 136-142, 1990
24. Cribier A, Savin T, Berland J, et al: Percutaneous transluminal balloon valvuloplasty of dult aortic steno- sis: Report of 92 cases. J Am Coil Cardiol 9:381-386, 1987
25. Desnoyers MR, Isner JM, Pandian NG, et al: Clinical and noninvasive hemodynamic Results after aortic balloon valvuloplasty for aortic stenosis. Am J Cardiol 62:1078-1084, 1988
26. Letac B, Cribier A, Koning R, et al: Results of percuta- neous transluminal valvuloplasty in 218 adults with valvular aortic stenosis. Am J Cardiol 62:598-605, 1988
27. McKay RG, Safian RD, Lock JE, et al: Assessment of left ventricular and aortic valve function after aortic balloon valvuloplasty in adult patients with critical aortic stenosis. Circulation 75:192-203, 1987
28. Safian RD, Warren SE, Berman AD, et al: Improve- ment in symptoms and left ventricular performance
WANG, HARRISON, AND BASHORE
after balloon aortic valvuloplasty in patients with aortic stenosis and depressed left ventricular ejection frac- tion. Circulation 78:1181 -1191, 1988
29. Safian RD, Berman AD, Diver D J, et al: Balloon aortic valvuloplasty in 170 consecutive patients. N Engl J Med 319:125-130, 1988
39. Harrison JK, Davidson C J, Leithe ME, et al: Serial left ventricular performance evaluated by cardiac catheter- ization before, immediately after and at 6 months after balloon aortic valvuloplasty. J Am Coil Cardiol 16:1351 - 1358, 1990
31. McCrindle BW: The Valvuloplasty and Angioplasty of Congenital Anomalies (VACA) Registry Investigators. Independent predictors of immediate results of percu- taneous balloon aortic valvotomy in children. Am J Cardio177:286-293, 1996
32. O'Connor BK, Beekman RH, Rocchini AP, et al: Intermediate-term effectiveness of balloon valvulo- plasty for congenital aortic stenosis A prospective follow-up study. Circulation 84:732-738, 1991
33. Moore P, Egito E, Mowrey H, et al: Midterm results of balloon dilation of congenital aortic stenosis: Predic- tors of success. JAm Coil Cardio127:1257-1263, 1996
34. O'Keefe JH, Vlietstra RE, Bailey KR, et al: Natural history of candidates for balloon aortic valvuloplasty. Mayo Clin Proc 62:986-991,1987
35. Lieberman EB, Bashore TM, Hermiller JB, et al: Balloon aortic valvuloplasty in adults: Failure of proce- dure to improve long-term survival. J Am Coil Cardiol 26:1522-1528, 1995
36. Edmunds LH, Stephenson LW, Edie RN, et al: Open- heart surgery in octogenarians. N Engl J Med 319:131- 136, 1988
37. Davidson C J, Skelton TN, Kisslo KB, et al: The risk for systemic embolization with percutaneous balllon valvu- Ioplasty in adults. Ann Int Med 108:557-560, 1988
38. Davidson C J, Harrison JK, Leithe ME, et al: Failure of balloon aortic valvuloplasty to result in clinical improve- ment in patients with depressed left ventricular func- tion. Am J Cardio165:72-77, 1990
39. Sheikh KH, Davidson C J, Honan MB, et al: Changes in left ventricular diastolic performance after aortic balloon valvuloplasty: Acute and late effects. J Am Coil Cardiol 16:795-803, 1990



![Intra-aortic balloon pump counterpulsation [IABP] for ...Intervention Review] Intra-aortic balloon pump counterpulsation (IABP) for myocardial infarction complicated by cardiogenic](https://img.pdfslide.us/doc/110x75/5b0c16167f8b9a8b038b916c/intra-aortic-balloon-pump-counterpulsation-iabp-for-intervention-review-intra-aortic.jpg)








![Research Balloon aortic valvuloplasty as a palliative …...After its introduction, more than 30 years ago 1], as a [possible treatment for severe aortic stenosis (AS), balloon aortic](https://img.pdfslide.us/doc/110x75/60f83045b1c55b2e1b1cd0e4/research-balloon-aortic-valvuloplasty-as-a-palliative-after-its-introduction.jpg)














