Embed Size (px)
Citation preview
Bacterial Diseases of the Respiratory system
Dr. Shler Ghafour Raheem
BSc., MSc., PhD Medical Microbiology
LEARNING OUTCOMES
Structures of the Respiratory System.
Bacterial Diseases of the Upper Respiratory System
1- Streptococcal Respiratory Diseases
2- Diphtheria by Corynebacterium diphtheria
3- Rhinosinusitis and otitis media
Bacterial Diseases of the Lower Respiratory System
• Pneumonia
• Tuberculosis
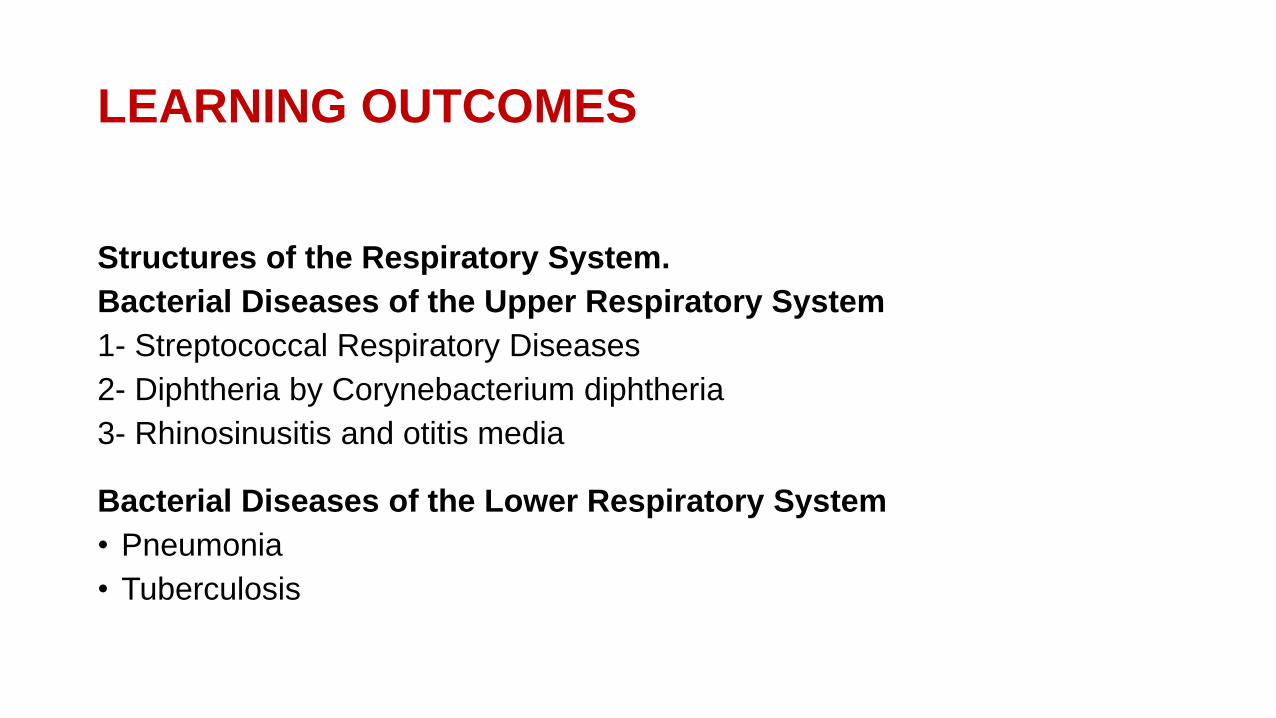
Structures of the Respiratory System
The respiratory system serves the vital function of exchanging gases between the atmosphere
and the blood.
Anatomists commonly divide its structures into two divisions:
Upper respiratory system
Lower respiratory system
https://adrenalfatiguesolution.com/anatomy-of-the-respiratory-system/
Upper respiratory system: nose, nasal cavity, pharynx.
• Collects air; filters dust, pollen, microorganisms
• Delivers it to the lower respiratory organs.
Lower respiratory system: larynx, trachea, bronchi, bronchioles, andalveoli. A ciliated mucous membrane lines the trachea, bronchi, and bronchioles.
The cilia beat synchronously about 1000 times per minute to carrymucus and trapped contaminants up to the pharynx. The mucus and itscontents pass into the digestive system, where digestive juices destroy them.
Alveolar macrophages, which enter the alveoli from blood capillariesand devour microorganisms.
Secretory antibodies (IgA), also provide protection from manypathogens.
Bacterial Diseases of the Upper Respiratory System
1- Streptococcal Respiratory Diseases
“Strep throat,” or streptococcal pharyngitis, is an inflammation of thepharynx caused by streptococci.
Signs and Symptoms
• The back of the pharynx appears red, with swollen lymph nodes,abscesses covering the tonsils. Pain during swallowing, bad breath, fever,malaise, and headache
• Bacteria spread into the lower respiratory tract, they may causeinflammation of the larynx or bronchi.
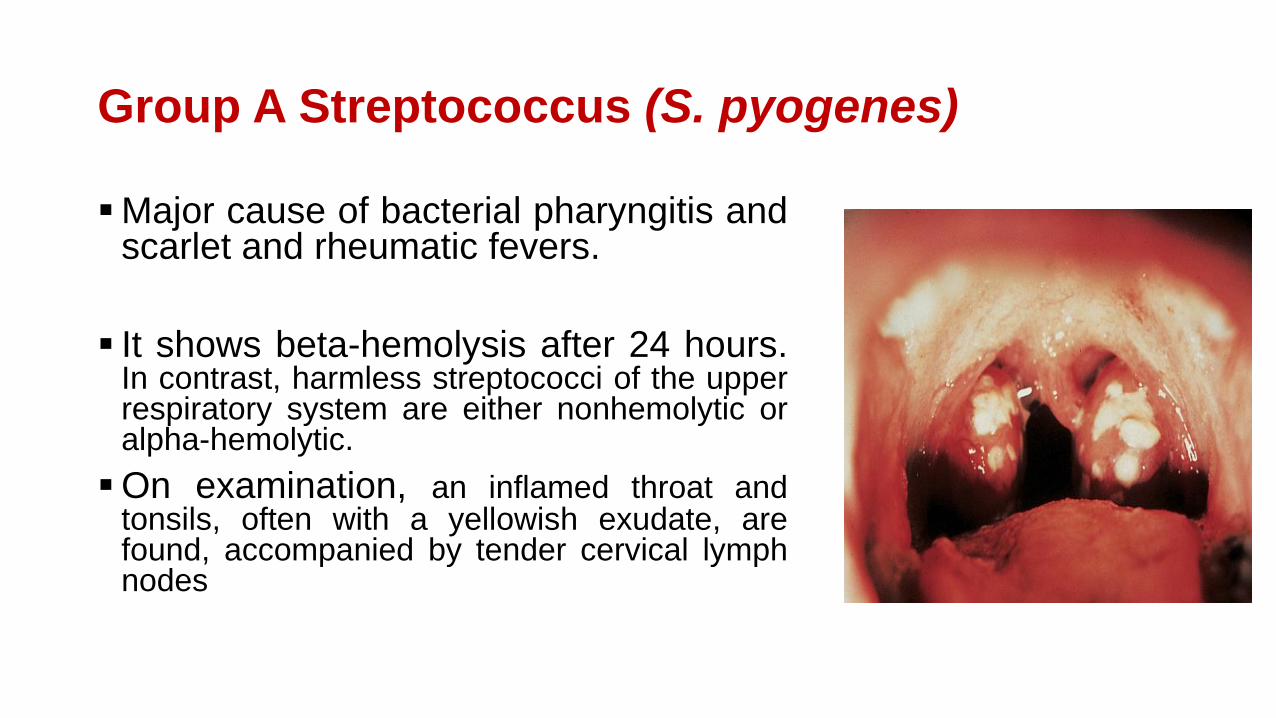
Group A Streptococcus (S. pyogenes)
Major cause of bacterial pharyngitis andscarlet and rheumatic fevers.
It shows beta-hemolysis after 24 hours.In contrast, harmless streptococci of the upperrespiratory system are either nonhemolytic oralpha-hemolytic.
On examination, an inflamed throat andtonsils, often with a yellowish exudate, arefound, accompanied by tender cervical lymphnodes
Home work
• Scarlet and rheumatic fevers.
Virulence Factors
M protein causes inhibition of complement component
The hyaluronic acid capsule
Streptokinases: break down blood clots, presumably enabling group Astreptococci to spread rapidly through damaged tissues.
Pyrogenic toxins (erythrogenic toxins) stimulate leukocytes to releasecytokines that in turn stimulate fever, rash, and shock.
Streptolysins lyse erythrocytes, leukocytes, and platelets
Diagnosis, Treatment, and Prevention
• 50% of patients diagnosed with strep throat actuallyhave it; the rest have viral pharyngitis. bacterial and viralpharyngitis are nearly identical, a sure diagnosis requiresserological testing.
• The most common bacterial infection is Group A beta-hemolytic streptococci, which causes around 36% ofcases of acute pharyngitis. Other bacterialetiologies include Group B streptococci, Chlamydiapneumoniae, Mycoplasma pneumoniae, Haemophilusinfluenzae, Candida, Neisseria meningitidis
https://www.google.com/search?q=Pharyngitis&source=lnms&tbm=isch&sa=X&ved=2ahUKEwjWvcGAtbbtAhWGDuwKHdg1DxcQ_AUoAXoECBEQAw&biw=1366&bih=657#imgrc=Mh30a3Bdv7AImM
• Penicillins, or amoxicillin, are very effective against both S.pyogenes and group C streptococci (S. equisimilis).
• Erythromycin or another macrolide to treat penicillin-sensitive
patients.
• Antibodies against M protein provide long-termprotection against S. pyogenes; however, antibodies directedagainst the M protein of one strain provide no protection against otherstrains. For this reason, a person can have strep throat more than once.
2- Diphtheria
• Physicians have brought the deadly childhood disease diphtheriaunder control in industrialized countries using effectiveimmunization. The disease is still a major threat to children living in less-developed regions of the world.
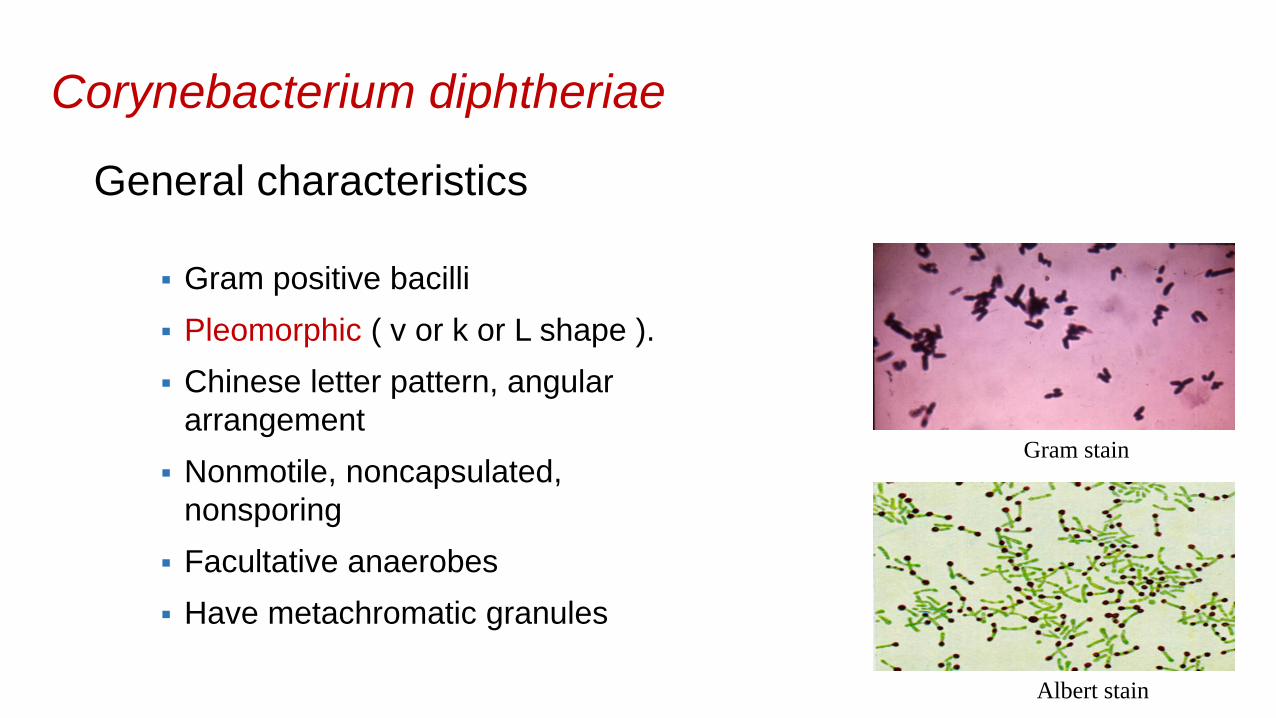
Corynebacterium diphtheriae
General characteristics
Gram positive bacilli
Pleomorphic ( v or k or L shape ).
Chinese letter pattern, angular
arrangement
Nonmotile, noncapsulated,
nonsporing
Facultative anaerobes
Have metachromatic granules
Gram stain
Albert stain
Reservoir
throat and nasopharynx
Transmission
Humans are the only natural host of C. diphtheriae. Both toxigenic and nontoxigenic organisms reside in the upper
respiratory tract and are transmitted by airborne droplets.
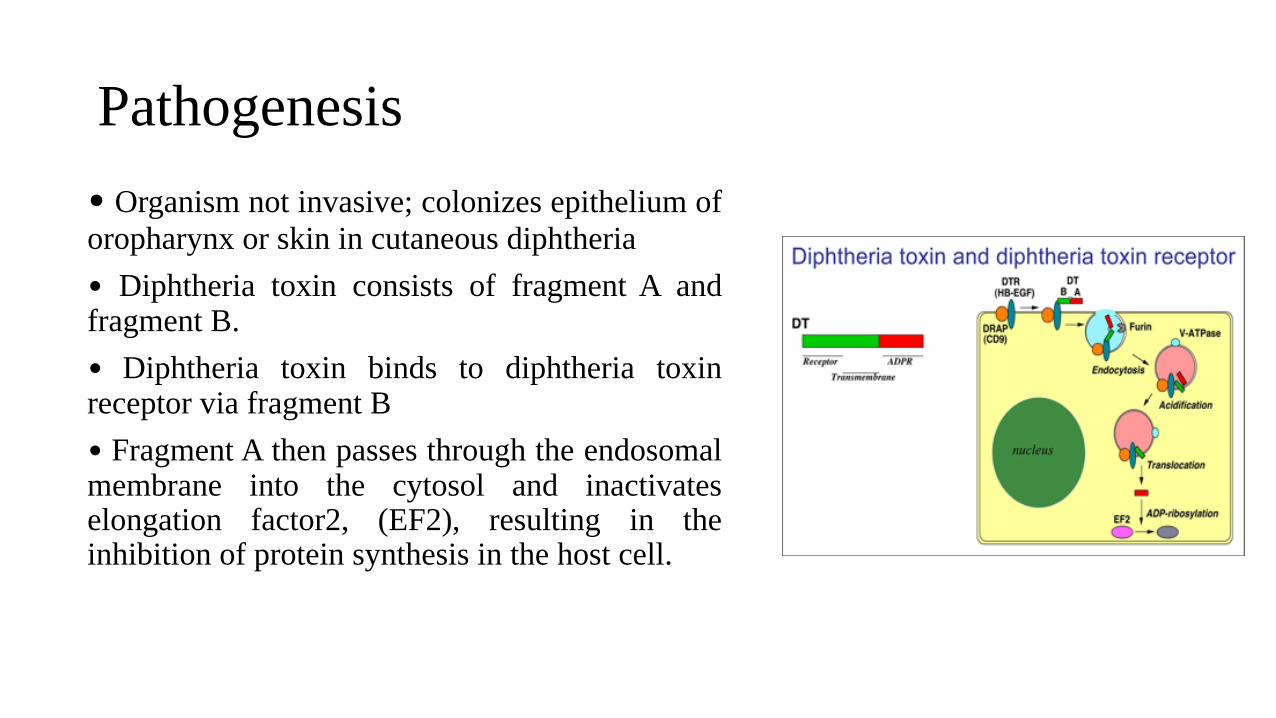
Pathogenesis
• Organism not invasive; colonizes epithelium of
oropharynx or skin in cutaneous diphtheria
• Diphtheria toxin consists of fragment A and fragment B.
• Diphtheria toxin binds to diphtheria toxin receptor via fragment B
• Fragment A then passes through the endosomalmembrane into the cytosol and inactivates elongation factor2, (EF2), resulting in the inhibition of protein synthesis in the host cell.
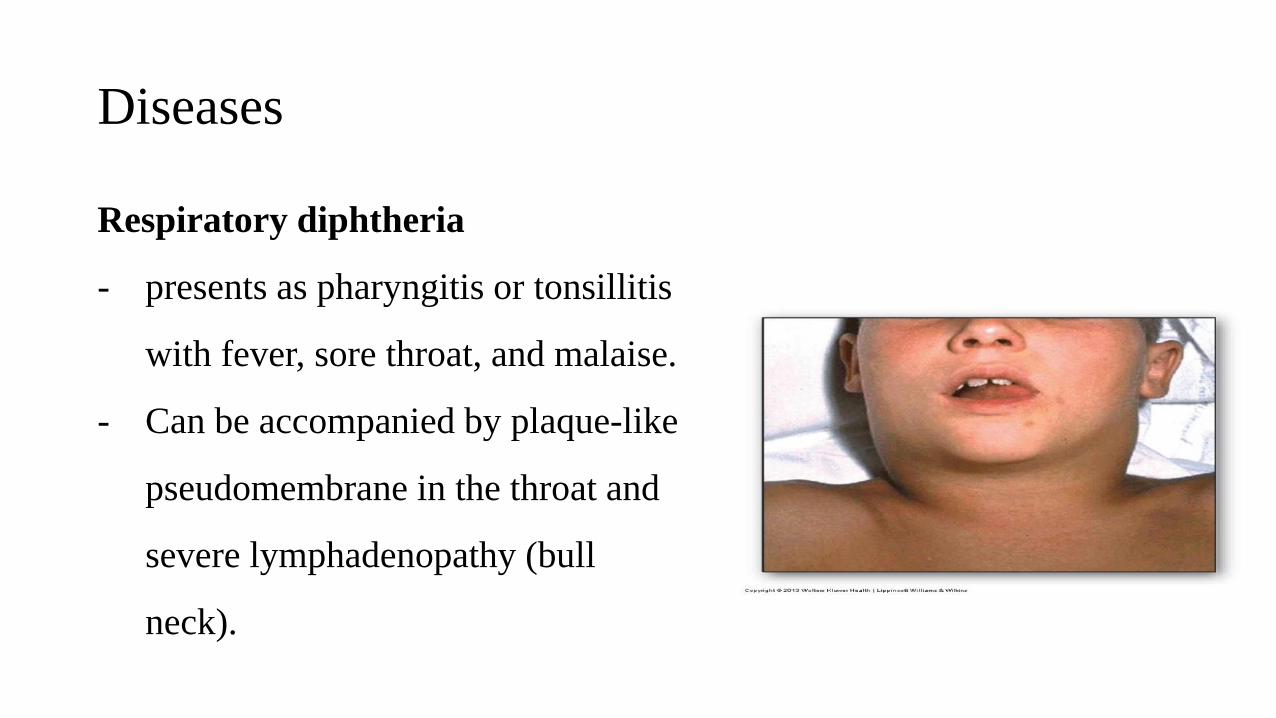
Diseases
Respiratory diphtheria
- presents as pharyngitis or tonsillitis
with fever, sore throat, and malaise.
- Can be accompanied by plaque-like
pseudomembrane in the throat and
severe lymphadenopathy (bull
neck).
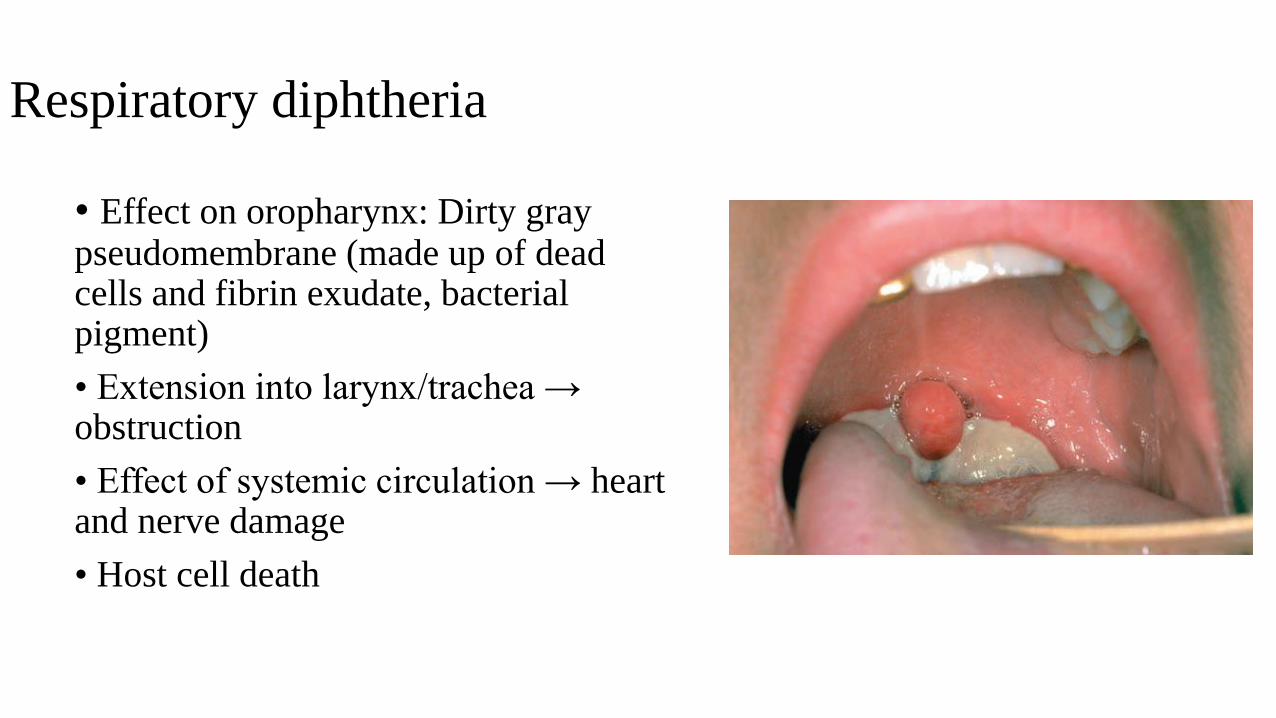
Respiratory diphtheria
• Effect on oropharynx: Dirty gray pseudomembrane (made up of dead cells and fibrin exudate, bacterial pigment)
• Extension into larynx/trachea → obstruction
• Effect of systemic circulation → heart and nerve damage
• Host cell death
Laboratory diagnosis
• Involves both isolating the organism and demonstrating toxin production.
• Decision to treat with antitoxin is a clinical one and cannot wait for the laboratory results
• Sample collection: Throat swab or swab from membrane
• Microscopy: Gram stain and Alberts stain
• Culture: Tellurite blood agar (selective medium)
Laboratory diagnosis
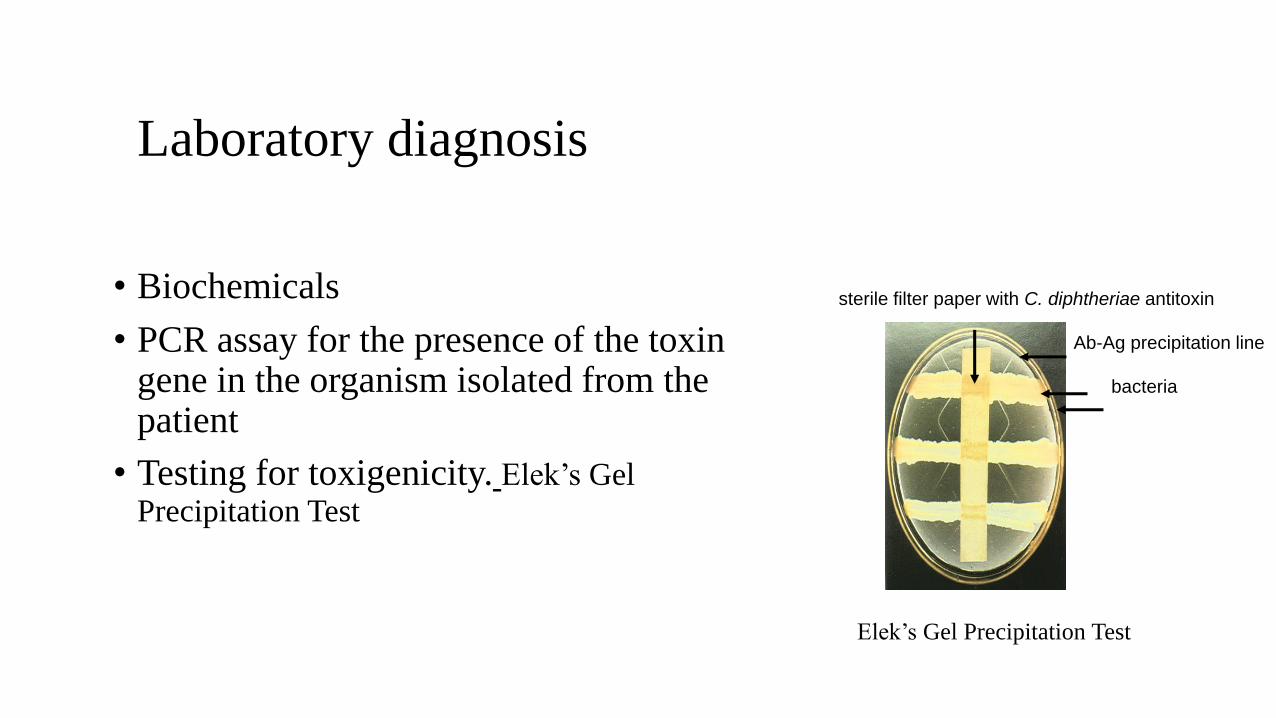
• Biochemicals
• PCR assay for the presence of the toxin gene in the organism isolated from the patient
• Testing for toxigenicity. Elek’s Gel
Precipitation Test
sterile filter paper with C. diphtheriae antitoxin
bacteria
Ab-Ag precipitation line
Elek’s Gel Precipitation Test
Treatment
Diphtheria antitoxin
Penicillin or erythromycin
preventionImmunization with diphtheria toxoid
Case Study
• A 4-year-old Russian immigrant was taken to a U.S. hospital due tomarked swelling of the throat and lymph nodes and the presence of athick, gray membrane over the throat and tonsils. Material recoveredfrom the throat was plated on tellurite blood agar, and black coloniesappeared after incubation, a Gram stain of the colony material revealsGram positive bacilli with a Chinese letter pattern and angulararrangement. What is the most likely etiology?
A. Haemophilus influenzae
B. Staphylococcus aureu
C. Group A streptococcus
D. Neisseria meningitidis
E. Corynebacterium diphteriae
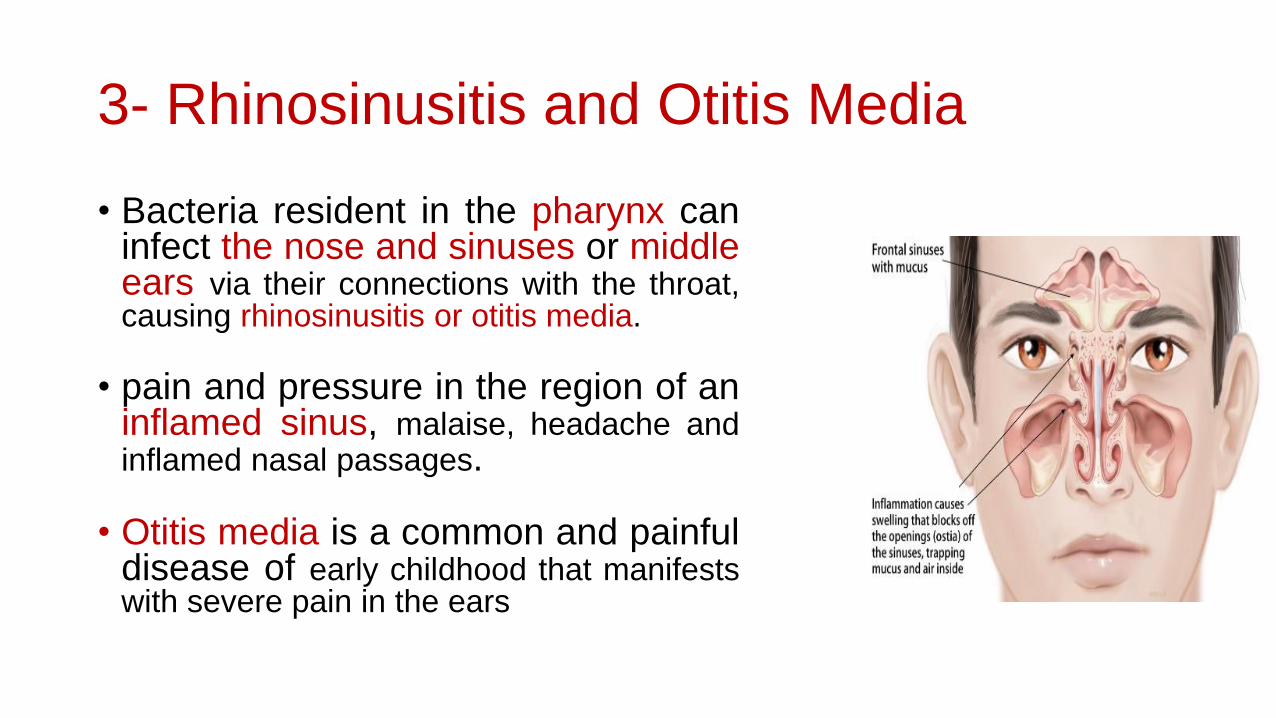
3- Rhinosinusitis and Otitis Media
• Bacteria resident in the pharynx caninfect the nose and sinuses or middleears via their connections with the throat,causing rhinosinusitis or otitis media.
• pain and pressure in the region of aninflamed sinus, malaise, headache andinflamed nasal passages.
• Otitis media is a common and painfuldisease of early childhood that manifestswith severe pain in the ears
Pathogens and Virulence Factors
• A number of bacteria that are normally part of the respiratorymicrobiota cause otitis media. These include:
• Streptococcus pneumoniae (about 35% of cases)
• Staphylococcus aureus (1–2%)
•Haemophilus influenzae (20–30%)
• Moraxella catarrhalis (10–15%).
These bacteria also cause most cases of rhinosinusitis.
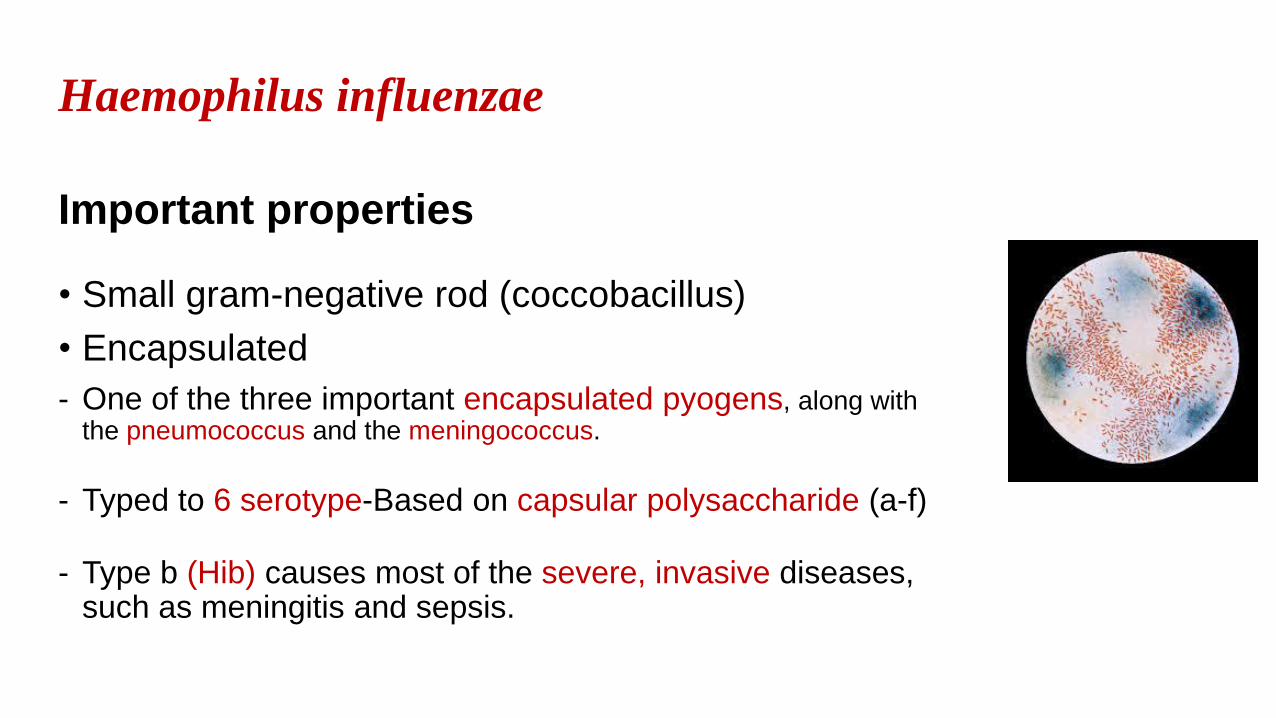
Haemophilus influenzae
Important properties
• Small gram-negative rod (coccobacillus)
• Encapsulated
- One of the three important encapsulated pyogens, along with the pneumococcus and the meningococcus.
- Typed to 6 serotype-Based on capsular polysaccharide (a-f)
- Type b (Hib) causes most of the severe, invasive diseases, such as meningitis and sepsis.
• Unencapsulated strains (termed nontypable (NTHi) because
they lack capsular serotypes), can also cause disease, such as sinusitis and otitis media, but are usually noninvasive.
• Fastidious: Requires growth factors X and V (NAD)
- X (haemin in blood)
- V (NAD inside RBC), NAD= nicotinamide-adenine dinucleotide
- Chocolate agar provides both X and V factors.
• Grows near S. aureus on BA = “satellite” phenomenon
Reservoir: Human nasopharynx. Infects only humans; there is no animal reservoir.
Transmission:
Respiratory droplets, shared toys
Virulence factors
Polysaccharide capsule
IgA protease is a mucosal colonizing factor
Endotoxin: LOS (Lipo-oligosaccharide)
Fimbriae
Pathogenesis
Antiphagocytic capsule and endotoxin; no exotoxin isproduced.
Most infections occur in children between the ages of 6months and 6 years, with a peak in the age group from 6months to 1 year ? (This age distribution is attributed to a decline inmaternal IgG in the child coupled with the inability of the child to generatesufficient antibody against the polysaccharide capsular antigen until the age ofapproximately 2 years).
Diseases
Diseases caused by H. influenzae , fall into two categories:
1- Disorders result from contiguous spread of the organism from itssite of colonization in the respiratory tract.
• Otitis media: Usually non-typeable strains
• Bronchitis: Exacerbations of acute bronchitis in smokers with COPD (Chronic
Obstructive Pulmonary Disease).
• Pneumonia: 1–24 months; rare in vaccinated children; smokers
• Epiglottitis: Rare in vaccinated children; seen in unvaccinated toddlers; H.influenzae was the major causal agent.
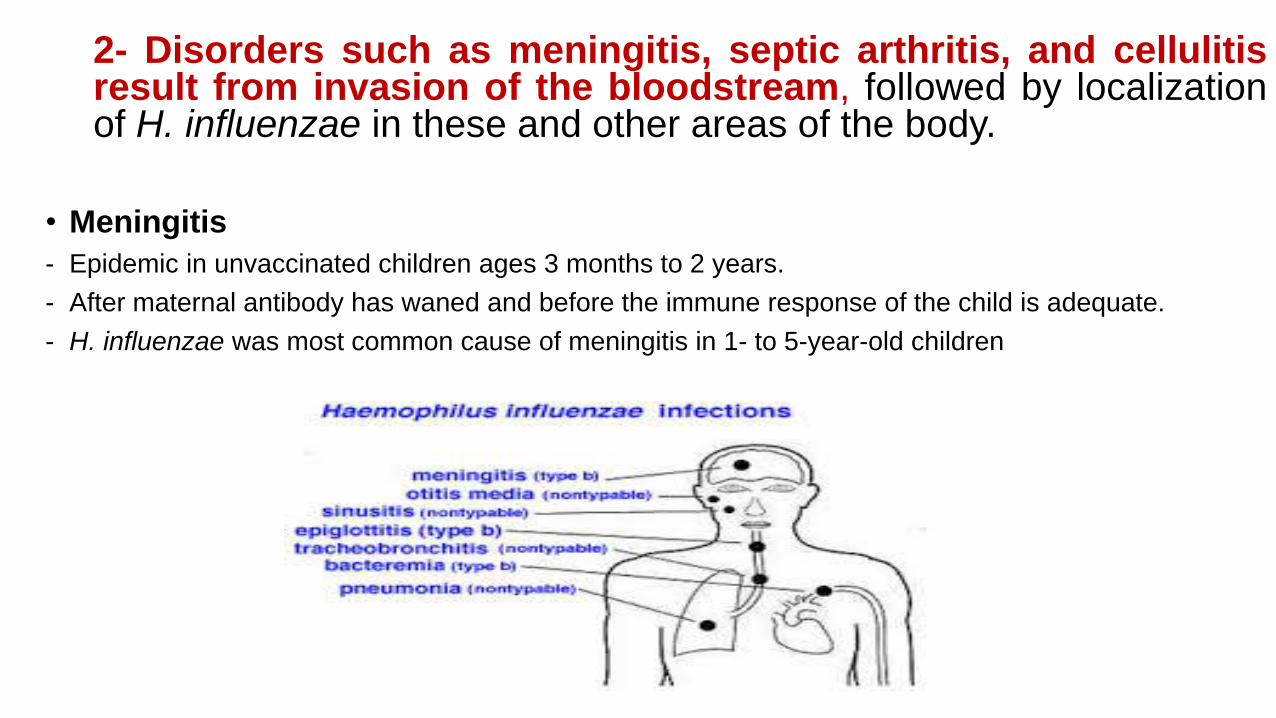
2- Disorders such as meningitis, septic arthritis, and cellulitisresult from invasion of the bloodstream, followed by localizationof H. influenzae in these and other areas of the body.
• Meningitis
- Epidemic in unvaccinated children ages 3 months to 2 years.
- After maternal antibody has waned and before the immune response of the child is adequate.
- H. influenzae was most common cause of meningitis in 1- to 5-year-old children
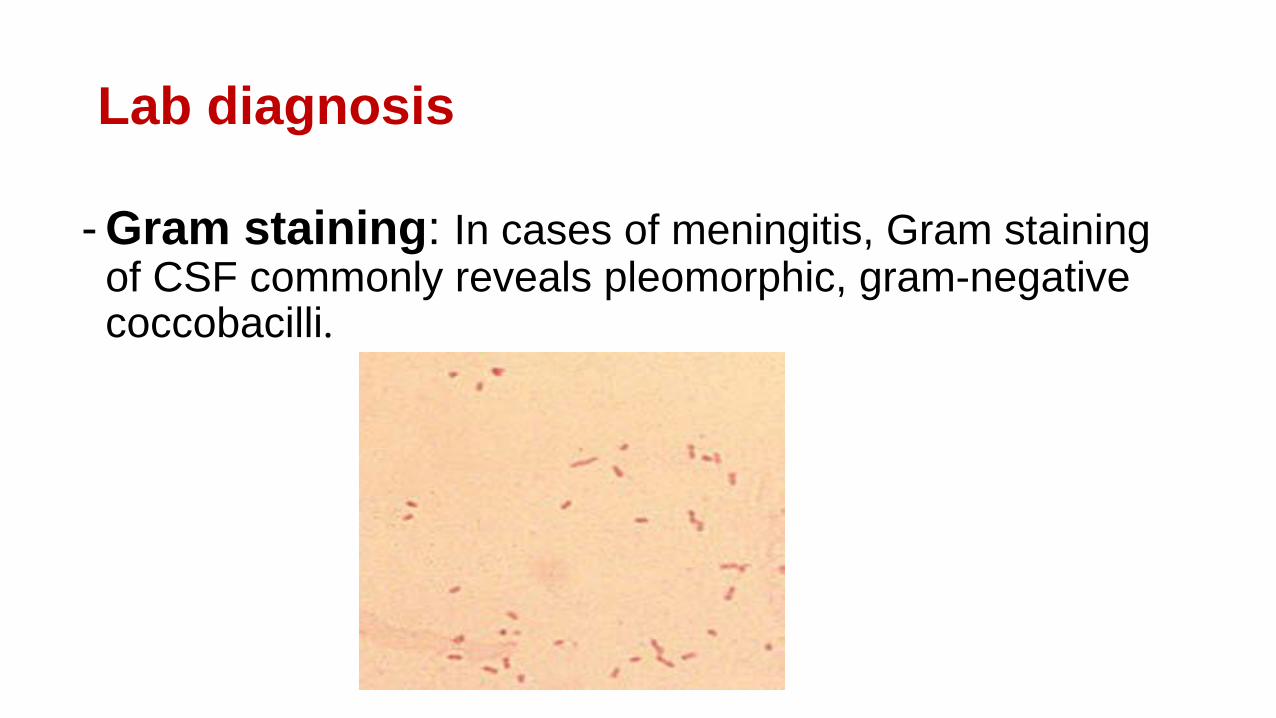
Lab diagnosis
- Gram staining: In cases of meningitis, Gram staining of CSF commonly reveals pleomorphic, gram-negative coccobacilli.
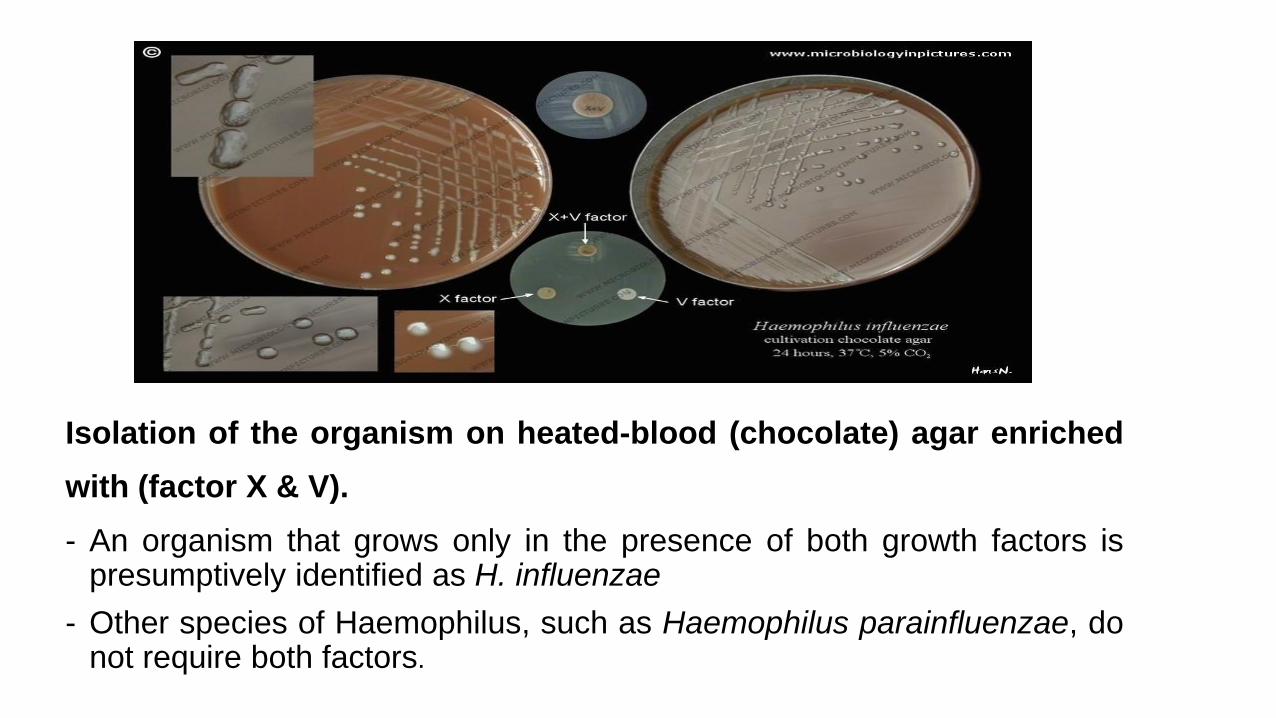
Isolation of the organism on heated-blood (chocolate) agar enriched
with (factor X & V).
- An organism that grows only in the presence of both growth factors ispresumptively identified as H. influenzae
- Other species of Haemophilus, such as Haemophilus parainfluenzae, donot require both factors.
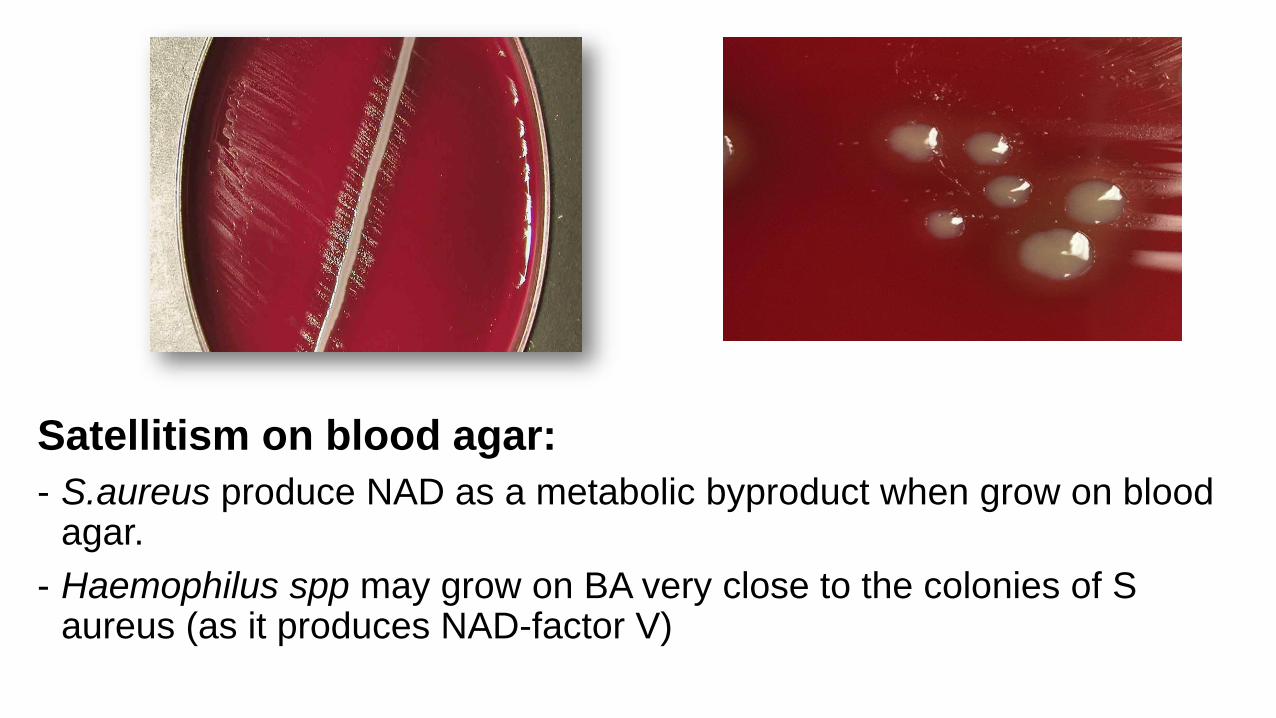
Satellitism on blood agar:
- S.aureus produce NAD as a metabolic byproduct when grow on blood agar.
- Haemophilus spp may grow on BA very close to the colonies of S aureus (as it produces NAD-factor V)
- Biochemical tests: oxidase +ve, catalase +ve
- Capsular swelling (quellung) reaction.
- Antigen detection of capsule (latex particle agglutination)
- ELISA
- Polymerase chain reaction (PCR)
Treatment
Cefotaxime or ceftriaxone for empirical therapy of meningitis; check nasal carriage before releasing; use rifampin if still colonized.
Prevention • Conjugate capsular polysaccharide-protein vaccine. Vaccination
effective to prevent type b disease.
• Rifampin reduces oropharynx colonization and prevents meningitis in unvaccinated, close contacts <2 years of age.
References
• Robert W. Bauman, Todd P. Primm. 2018. Microbiology with Diseases by Body
System. Fifth edition, Pearson.
• Stefan Riedel, Thomas G. Mitchell, Jeffery A. Hobden, Judy A. Sakanari. Steve Miller, Peter Hotez, Stephen A. Morse, Rojelio Mejia, Timothy A. Mietzner. 2019. Jawetz, Melnick, & Adelberg’s Medical Microbiology. 28th edition. McGraw-Hill Education.
• Patrick R. Murray, Ken S. Rosenthal, Michael A. Pfaller. 2020. Medical Microbiology. Elsevier.
• Gottlieb M, Long B, Koyfman A. Clinical Mimics: An Emergency Medicine-Focused Review of Streptococcal Pharyngitis Mimics. J Emerg Med. 2018 May;54(5):619-629.
• https://www.youtube.com/watch?v=b0J60sh-Vdo.
• https://www.youtube.com/watch?app=desktop&v=jE-AItLyYf0























![[S3Lab1] Respiratory Diseases](https://img.pdfslide.us/doc/110x75/577d349a1a28ab3a6b8e6d89/s3lab1-respiratory-diseases.jpg)