Embed Size (px)
DESCRIPTION
Bacterial and Viral Skin Diseases
Citation preview
Bacterial skin diseases
Department of Dermatology
University of Medical Sciences in Poznan
Bacterial flora of the skin
Resident flora numerous in moist, hairy areas rich in sebaceous glands
organisms are found in clusters in stratum corneum and hair follicles
a mixture of micrococcai and diphtheroids
Staphylococcus epidermidis predominates on the surface and anaerobic diphteroids (Propionibacterium acne) deep in the hair follicle
Transient and temporary flora

Resident flora
Aerobic organisms in general
Cocci (ball-shaped bacteria)
Bacilli (rod-shaped bacteria)
S. epidermidis
Corynebacterium
TRANSIENT AND TEMPORARY FLORA
STAPHYLOCOCCUS AUREUS
- nose and perianal region of some
individuals can be spread to the skin
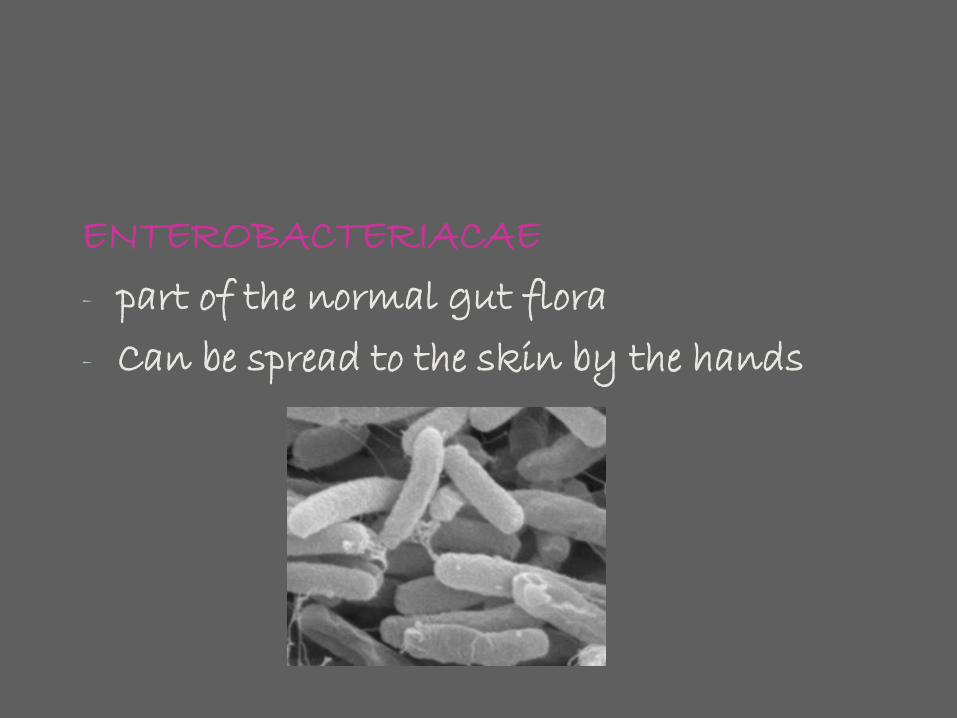
ENTEROBACTERIACAE
- part of the normal gut flora
- Can be spread to the skin by the hands

PSEUDOMONACAE
- present in the environment
- moist places
INTACT EPIDERMAL BARRIER
pH (5,4-5,9 on the free skin, like forehead, higher in the axillae and groin)
WATER AND FAT CONTENT OF THE STRATUM CORNEUM
SKIN TEMPERATURE
INTEGRITY OF NORMAL FLORA
Erysipelas
Acute erythematous, rapidly spreading skin infection, usually associated with systemic symptoms
Cause: Streptococus pyogenes (occasionally other streptococci)
Formerly: common, feared and fatal disease!
(„St. Anthony’s fire”)
Etiology
Presence of a defect in skin barrier function
Associated with HSV infection, interdigital tinea pedis, leg ulcer
Other even minor injury
30% of patients have Streptococcus pyogenes in their nares
Lymphatic obstruction as a second cofactor
STREPTOCOCCI THEMSELVES CAUSE FURTHER
LYMPHATIC DAMAGE, CREATING A VICIOUS CIRCLE, FACILITATING RECURRENCE!
CLINICAL FINDINGS
Warm, painful erythema
Rapidly spreads peripherally
Always sharp border to the adjacent normal skin
„tongue like” irregular extentions are common





Common sites
Cheeks
Legs
Edematous arm following mastectomy and lymph node dissection
Most patients are febrile and may have chills.
Erysipelas variants
Blisters
Hemorrhagic blisters (legs)= erysipelas vesiculosum et bullosum
Necrosis= erysipelas gangraenosum






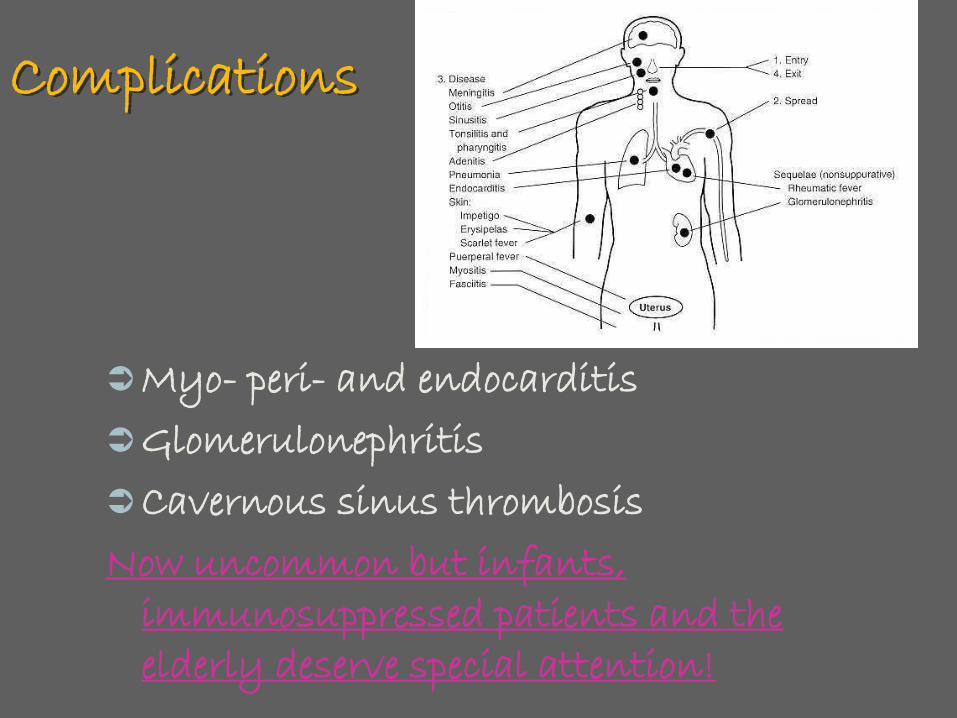
Complications
Myo- peri- and endocarditis
Glomerulonephritis
Cavernous sinus thrombosis
Now uncommon but infants, immunosuppressed patients and the elderly deserve special attention!
Therapy
Systemic: penicillin i.v. In case of allergy: oral erythromycin (2 weeks)
Topical: dressings with ichthyol or boric acid or aluminium acetotartrate (Altacet)
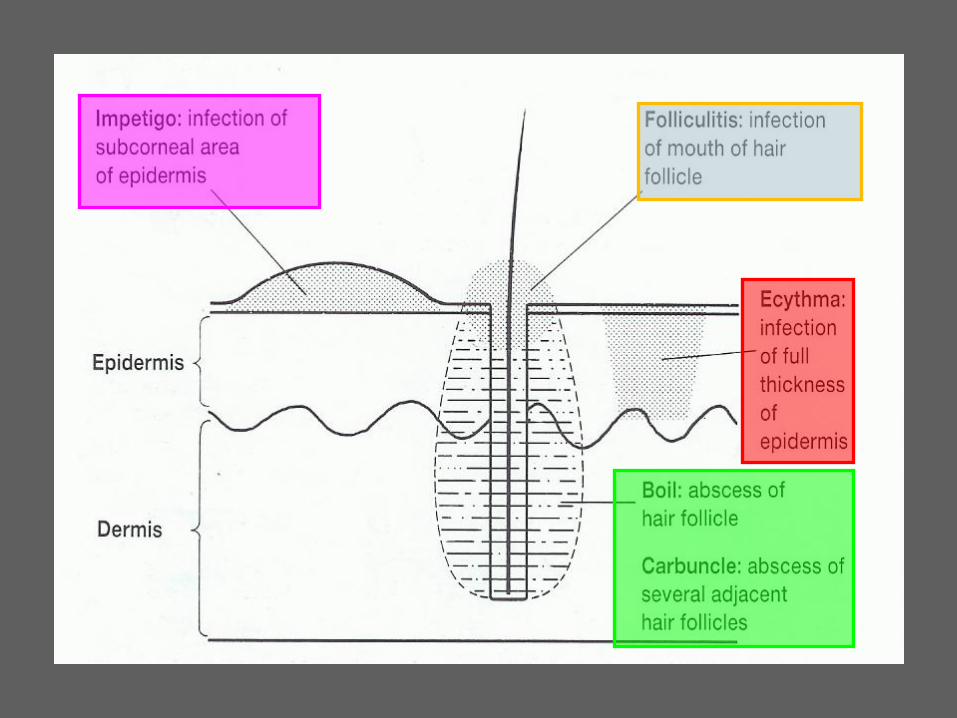
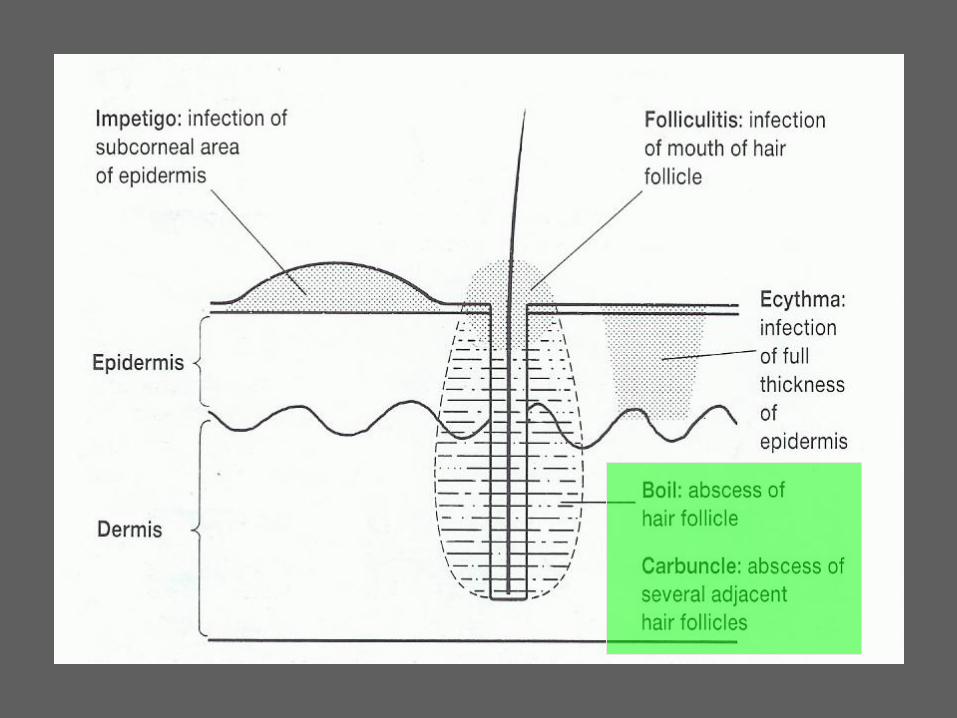
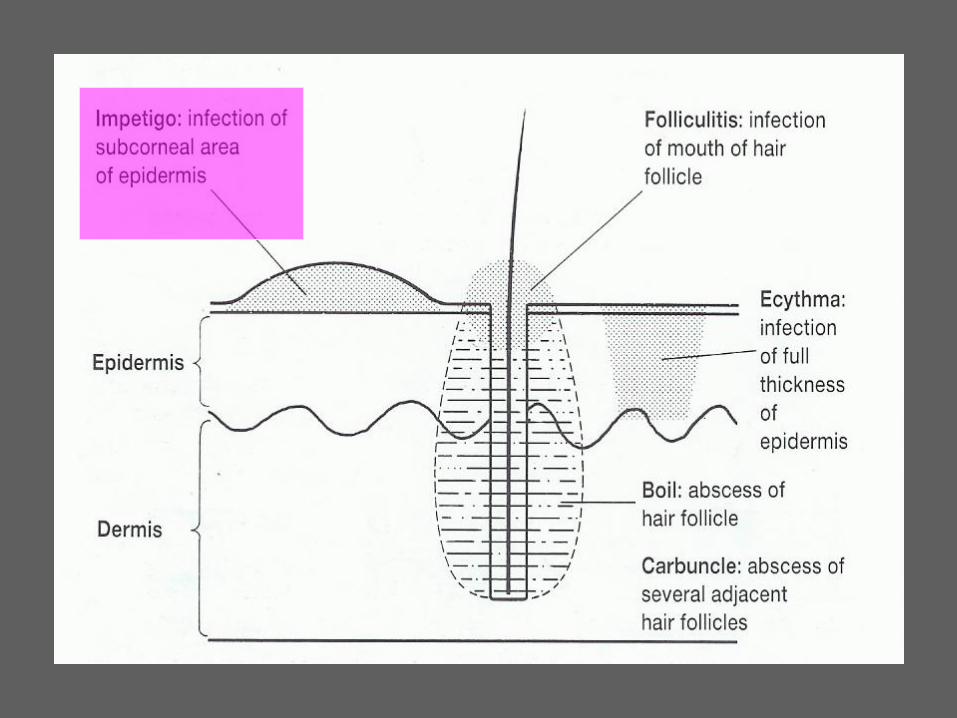
Folliculitis
Inflammation of the hair follicle usually clinically manifested as distinct papules and pustules
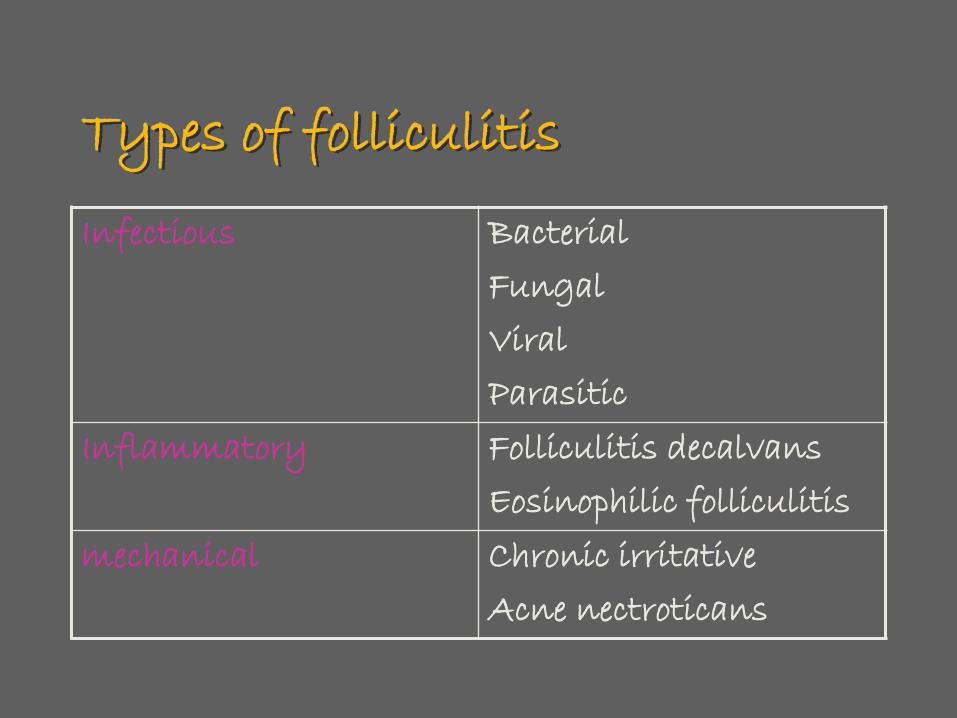
Types of folliculitis
Infectious Bacterial
Fungal
Viral
Parasitic
Inflammatory Folliculitis decalvans
Eosinophilic folliculitis
mechanical Chronic irritative
Acne nectroticans
Staphylococcal folliculitis
Infection of the terminal hair- almost exclusively a disease of men
Women: axilla, groins. Legs
Scalp folliculitis: men
Typical lesion: inflamed papule or pustule on the hair line („acne necrotica”), face, axillas, buttocks or pubic hairs; painful and pruritic with erythematous periphery.
Widespread infection: fever, lymphadenopathy
Therapy: antibiotics (temporary improvement, but relapses are common)
Topical: antibiotic drying solutions or lotions.





FURUNCLE (BOIL)
Deep inflammatory nodule with central pus, developing from a bacterial hair follicle infection.
Cause: Staphylococcus aureus.
May be associated with:
Poor hygiene
Immunosuppressive therapy
Risk factors (furuncle)
Corticosteroid therapy
Diabetes mellitus
HIV/AIDS
Wasting illnesses
Also: patients with atopic dermatitis who have a heavy skin carriage of S. aureus and minor defects in their skin are present.

Common location
Nape
Face
Axillae
Buttocks
Arms
Legs
Nasal vestibulum
External ear canal
Furuncle
Small yellow creamy pustulered nodule with a central yellow plug. Painful, tense and often associated with local
edema, lymphangitis, fever, lymphadenopathy
Especially dangerous furuncles: involving the mid-face (cavernous sinus thrombosis)


Therapy
Penicillinase-resistant penicillins or cephalosporins
In an immunocompromised patient: hospital and i.v. Therapy!
Topical: ointment based on ichthyol, povidone-iodine solutions.
Surgical: controversial
FURUNCULOSIS: multiple recurrent furuncles
CARBUNCLE: worst form of furuncle with coalescence of lesions and marked inflammation





Impetigo
Common superficial skin inflammation, chracterized by small blisters, that rapidly rupture and evolve into honey coloured crust.
Cause: Staphylococcus aureus
Streptococci gr A
Impetigo
Most common among children and quite contagious
Often several children (classmates) will present simultaneously
The infection may be transferred via wash clothes and towels
Impetigo
Face
Mouth
Nose
Neck
Hands
Outlook: good, with a prompt response to treatment
Impetigo
Feared complications: development of glomerulonephritis (4%)
Therapy: topical: mupirocin ointment, bacitracin ointment, clioquinol ointment, crust may be removed by wet compresses.
Systemic: penicillinase-resistant penicillins, cephalosporins, erythromycin
Erythrasma
Bacterial infection of intertriginous areas usually with asymptomatic, red-brownish macules.
Cause: Corynebacterium minutissimum
Erythrasma
20% of population infected
Most patients: older men
Intertriginous sites
Hyperhydrosis
Obesity
Diabetes mellitus
Most common sites-intertriginous
Groin
Axilla
Gluteal cleft
Inframammary folds
Umbillicus
Toe web spaces
Erythrasma
The best way to make the diagnosis
Woods lamp examination
Corynebacteria porphyrins
coral red fluorescencet
Course: erythrasma is both chronic and frequently recurrent, despite therapy.
Therapy: a short course of systemic erythromycin is the easiest method
Topical: imidazole creams ( for 1 week then weekly for prophylaxis), erythromycin (solution)
Eliminate predisposing factors
Obesity
Sweating and maceration
Frequent washing with antibacterial soaps
Monitoring of therapy with Wood light examination
Viral diseases
Dermatology Department
University of Medical Sciences in Poznań
Cutaneous lesions caused by viruses
Either reflect a direct skin infection by an
epidermotropic virus (verrucae, molluscum
contagiosum)
May be a reflection of a widespread viral
infection (measles, chicken pox)
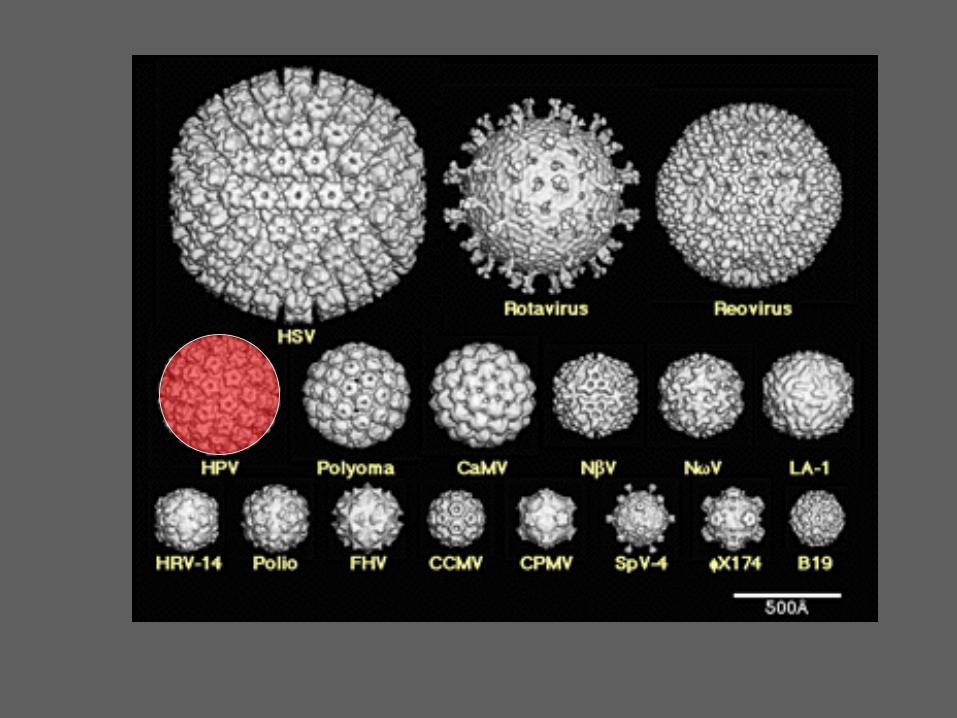
Warts (verrucae)
Cutaneous tumors caused by epidermotropic
viruses which tend to spontaneously regress, but
may rarely progress into cutaneous
malignancies
Cause: HUMAN PAPILLOMA VIRUS (HPV)
HPV transfer
HUMANS-HUMANS
ANIMALS-HUMANS
HUMANS-ANIMALS (?)
Incubation time: weeks to years
Autoinoculation is a rule:
inoculation with organisms already present in or on
the body
Detection of HPV
Direct immunofluorescence- comercially
available but not sensitive or specific
Serologic tests: research tool for a limited
number of HPV
PCR: able to identify very small amounts of virus
– sometimes too sensitive!
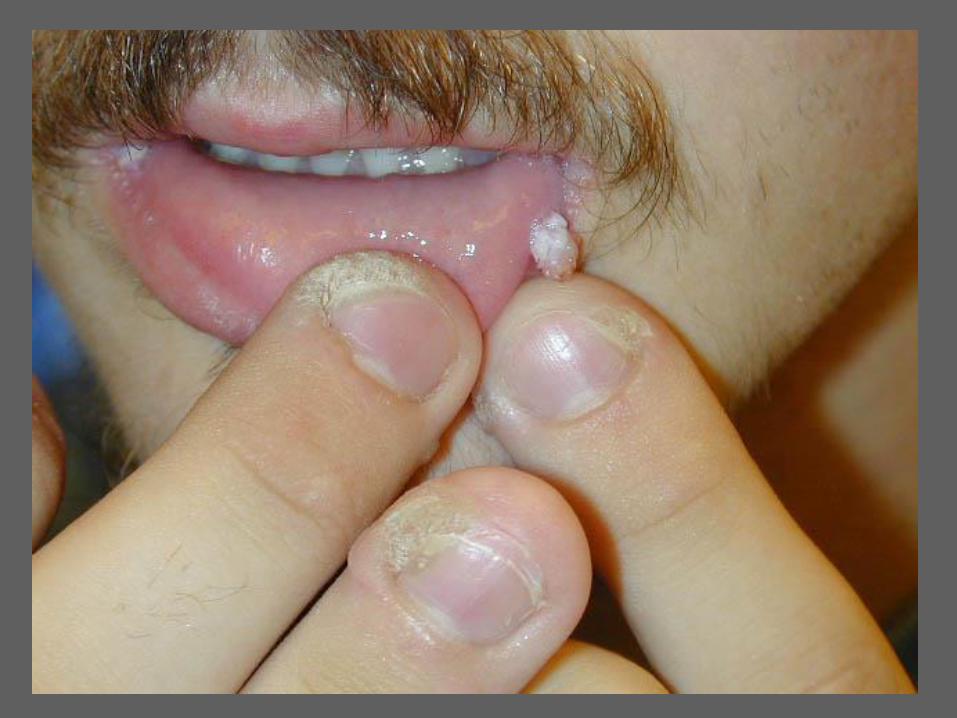
Common wart
(verruca vulgaris)





Nature of the warts
Fingers and back of the hands: papular warts
Eyelids: long, thin, filiform warts
Beard area: flat and filiform warts (often large
numbers spraed through shaving)
Scalp: large, exophytic
Palms: smooth and sharply bordered
Soles
Flat and often grow
into the skin like a thorn
spread like a tile
mosaic
Periungual region: very common, usually along
the lateral nail fold
Nail bed: very uncommon; present as painful
discoroured spots or nodules

Immunosuppressed patients:
Congenital immunodeficiences, HIV/AIDS,
chemotherapy
Warts are:
Widespread
Almost uncontrollable

Course and prognosis
Most tend to resolve spontaneously
Scarring as a result of therapy
Before dissapearance may become inflamed
(host immune response is active)
Plantar warts
Probably the most contagious of warts
Spread wherever large numbers of people go
barefoot (swimming pools, gymnasiums)
Plantar warts
Solitary: most typical location : over metacarpal
heads, may sometimes resemble a corn, or a
clavus
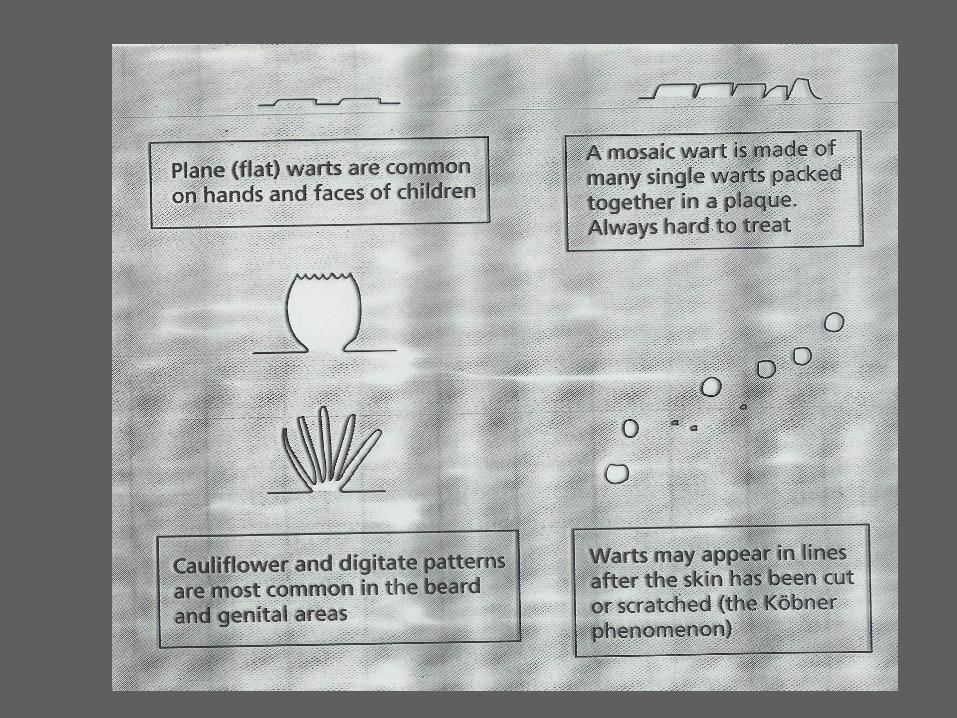
Mosaic warts: multiple warts that coalesce
together resembling a mosaic floor; tend to be
flat and asymptomatic but very difficult to treat



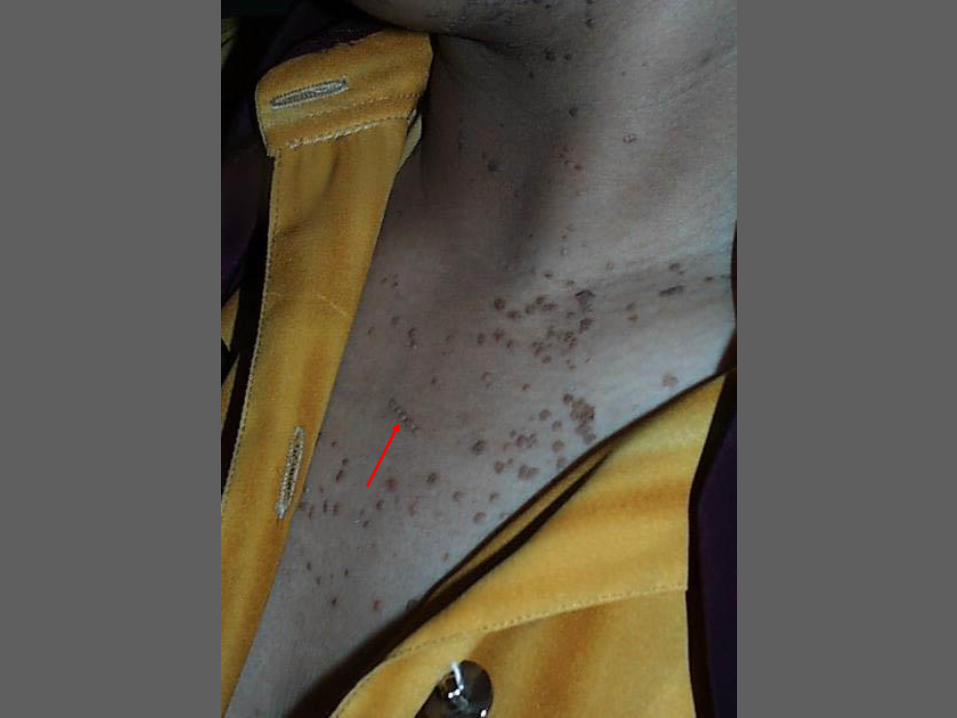
Plane warts
Small, flat papules, often slightly
hyperpigmented and most commonly found on
the face
Typically seen in children and young adults
Frequently dissapear spontaneously with diffuse
inflammation

Genital warts
Condylomata acuminata
Flat genital warts
Giant genital warts
Condylomata acuminata
Highly contagious
Major public health problem
SEVERAL TYPES OF HPV FOUND IN THE
GENITAL REGION (HPV-16, HPV-18) APPEAR
TO BE ONCOGENIC!
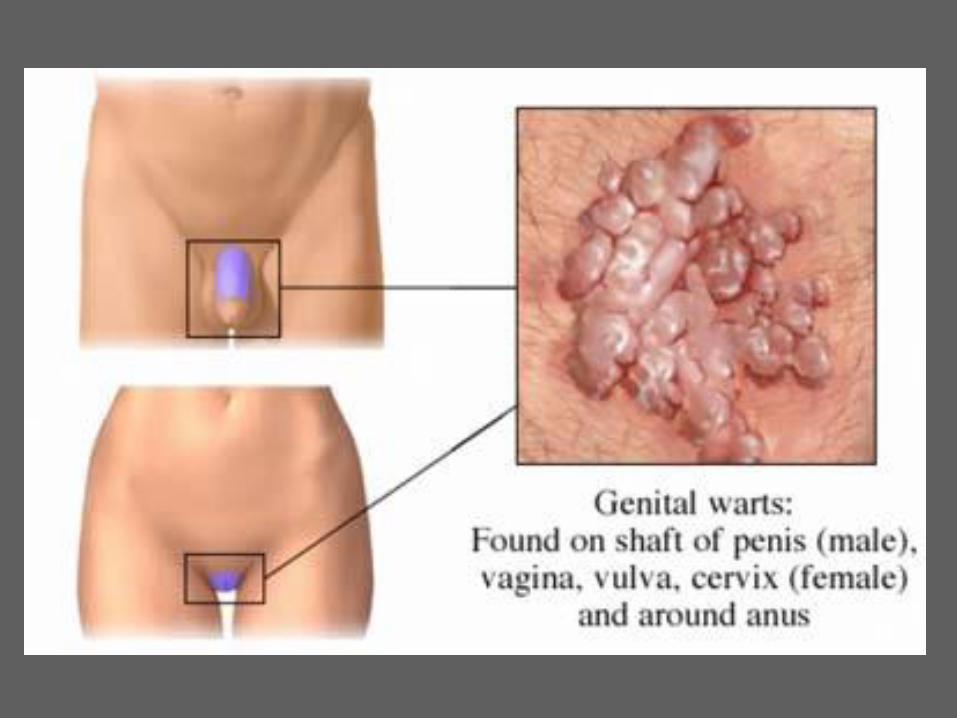
Tiny red papule coalesce together produce a
cauliflower-like picture
Typical locations:
Women: labia minora, vagina
Men: coronal sulcus, glans, urethral meatus
Perianal region


Pearly penile papules-normal!
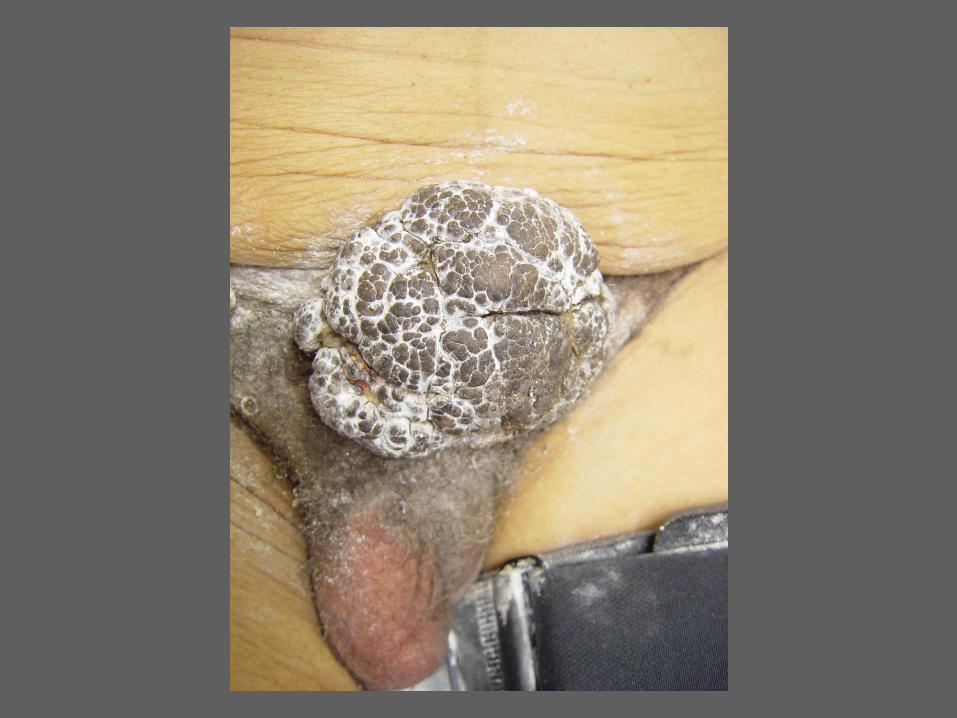
Giant genital warts (Buschke and
Löwenstein 1925)
Large destructive tumors
Perianal, under the foreskin
At some point they become squamous cell
carcinoma (verrucous type)
A large, persistent penile or perianal wart,
especially if appears clinically destructive
biopsied or excised!
Therapy of warts
Multiplicity of warts underscores the fact that no
one regimen is highly effective.
Treatment should be designed to avoid scarring
and should not be terribly aggressive or painful.
The method depends on the location, number, size,
as well as previous therapeutic attempts.
Cryotherapy
Liquid nitrogen: probably most widely used
method
Applied either with a spray applicator, cotton-
tipped swabs or metal sounds
Need to freeze hard enough to produce a blister-
HPV themselves are not damaged by the cold
temperature




Surgery
Curette, scalpel, electrosurgical device
Best suired for a small number of warts on
glabrous skin
Lasers
CO2 laser
HPV particles are potentailly infectious!
Well suited for periungual warts: less bleeding,
facilitate removal of part or all the nail
Keratolytic agents
Often in conjunction with cryotherapy
Salicylic acid: solutions, flexible collodion,
plasters, gel patches
Lactic acid
Trichloroacetic acid
Cytostatic agents
Podophyllin: inhibitor of the mitotic cytoskeleton
derived from the may apple (Podohyllum
peltatum); best suited for mucosal surfaces
1% podophyllotoxin: more standarized
podophyllin mixture: FDA approve for treatment
of genital warts
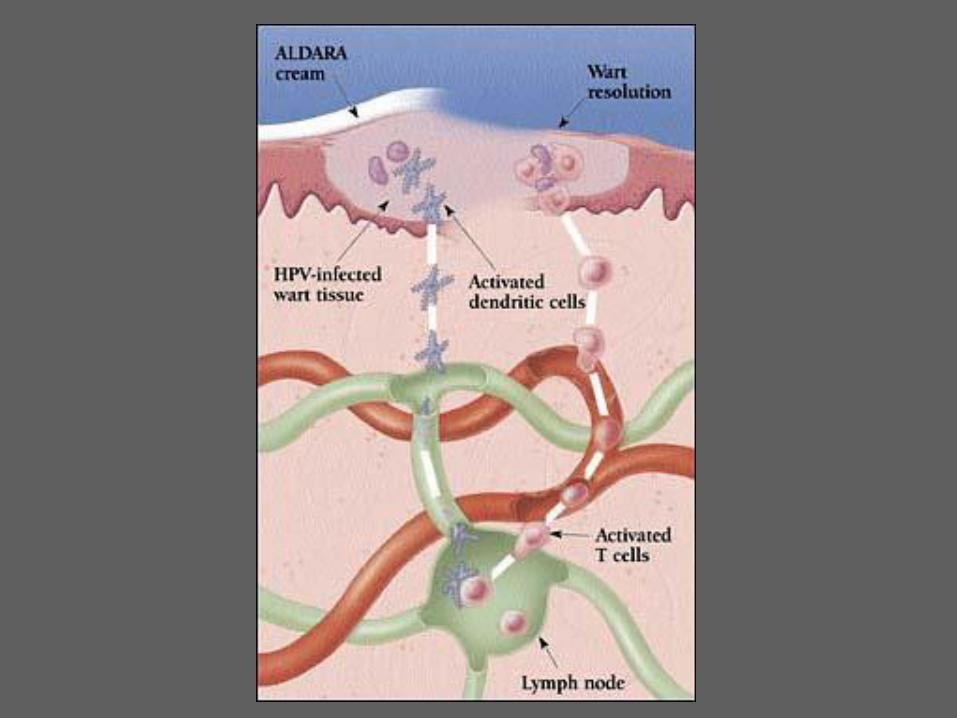
Immunologic therapy
Warts are sometimes cleared by cell mediated
immunity
Interferons: intralesional injection, often
combined with mechanical debulking, topical gel
also available
Imiquimod 5% cream: approved for external
anogenital warts

HPV VACCINES
Cervac (Glaxo): HPV 16 and 18
Gardasil (Merck): HPV 16, 18, 6,
Gardasil™, the investigational vaccine against HPV, significantly reduced the combined incidence of persistent HPV 6, 11, 16, or 18 infection and related diseases, including new cervical pre-cancers and genital warts compared to placebo in a Phase II study published for the first time in The Lancet Oncology.
"The level of protection in this study against infection with these four HPV types, including pre-cancerous lesions, was significant," said the study's lead investigator, Luisa Villa, PhD, head of the Virology Group at the Ludwig Institute for Cancer Research, São Paulo branch.
HERPES VIRUSES
HERPES SIMPLEX VIRUSES
VARICELLA ZOSTER VIRUS
Herpes viruses
Herpes simplex virus 1 (HSV1)
Herpes simplex virus 2 (HSV2)
Varicella zoster virus
Epstein-Barr virus
Human herpes virus 6
Human herpes virus 7
Human herpes virus 8
HSVs cause a wide range of
disorders
In newborns: sepsis, encephalitis
In young children: primary herpetic stomatitis
In older individuals: recurrent oral and genital
infections
In elderly and immunosuppressed patients:
disseminated infections

TRIGGERS
FEVER
TRAUMA
SUNLIGHT
STRESS
CLINICALLY
GROUPED BLISTERS OR EROSIONS
HERPETIFORM ARRANGEMENT

HSV
HSV1 HSV2
LIPSORAL MUCOSA
HEADNECK
GENITALIA
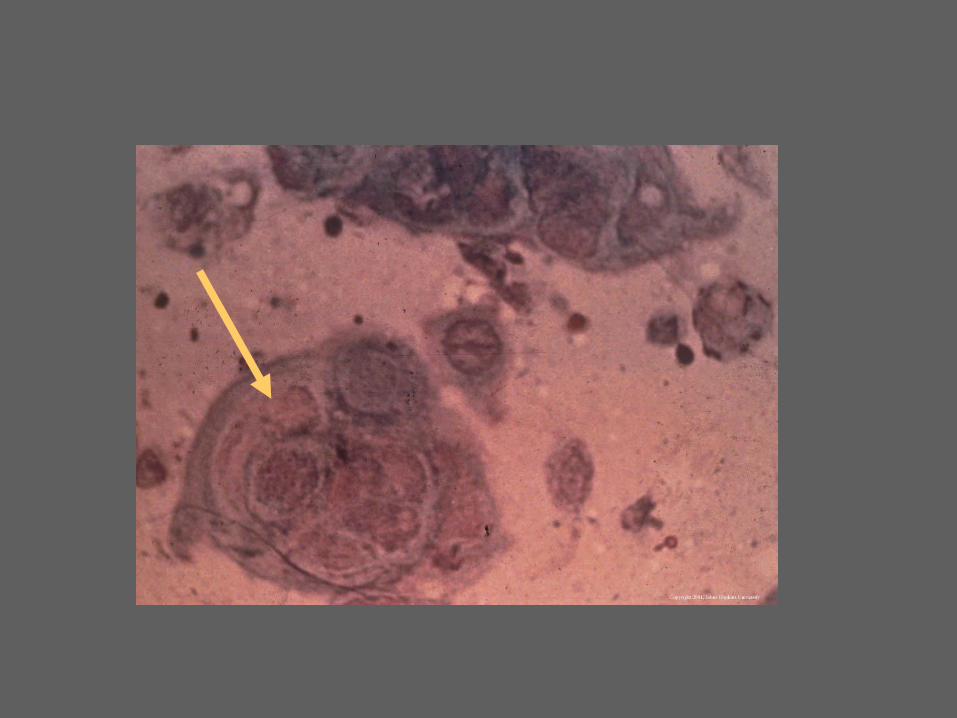
Laboratory findings
Tzanck smear:examined for the typical
multinucleated giant cells (HSV causes epithelial
cells to fuse together)- simple but gives definitive
diagnosis
Electron microscopy: identifies viral bodies
PCR: HSV can be identified from any tissue or
fluid
Immunofluorescent examination: tissue
examined with antibodies against HSV-1, HSV-2
Viral culture: takes up to 48h and may not yield
organisms if the source is not fresh
Serologic tests: epidemiological interest
Therapy
The mainstay: acyclovir: purine nucleoside
analogue, which interferes with viral DNA
synthesis
Cream, gel, tablets, intravenous form
Used to treat: initial infections, recurrences, may be
used for many months to supress infections
Safe drug


According to the U.S. Centers for Disease Control and Prevention,
45 million people in the United States ages 12 and older, or 1 out of
5 of the total adolescent and adult population, are infected with
HSV-2.
Eczema herpeticum
Generalized HSV infection in patients with atopic
dermatitis and other widespread skin diseases.
Result of an autoinoculation (labial HSV) or
heteroinoculation from an infected contact
Clinical findings
Fever
Malaise
Tight feeling skin





Treatment
Acyclovir and its relatives
Intravenous therapy preferred
Hospitalization needed
Antibiotics for secindary bacterial infections
Wet soaks zinc lotion
VARICELLA ZOSTER VIRUS
THE SAME VIRUS CAUSES VARICELLA IN
CHILDREN (PRIMARY INFECTION) AND
ZOSTER (SECONDARY INFECTION)
PATIENTS WITH ZOSTER CAN INFECT
NONEXPOSED CHILDREN AND
IMMUNOSUPPRESSED PATIENTS, CREATING
VARICELLA
Varicella is extremely common!
In most countries, 90-95% of the
population has had the infection by
15 years of age!
FIRST INFECTIONimmunity virus remains
behind in neural ganglia with age or
immunosuppression, unknown trigger factors
reactivate the virusinvolves a single sensory
nerve and its dermatome
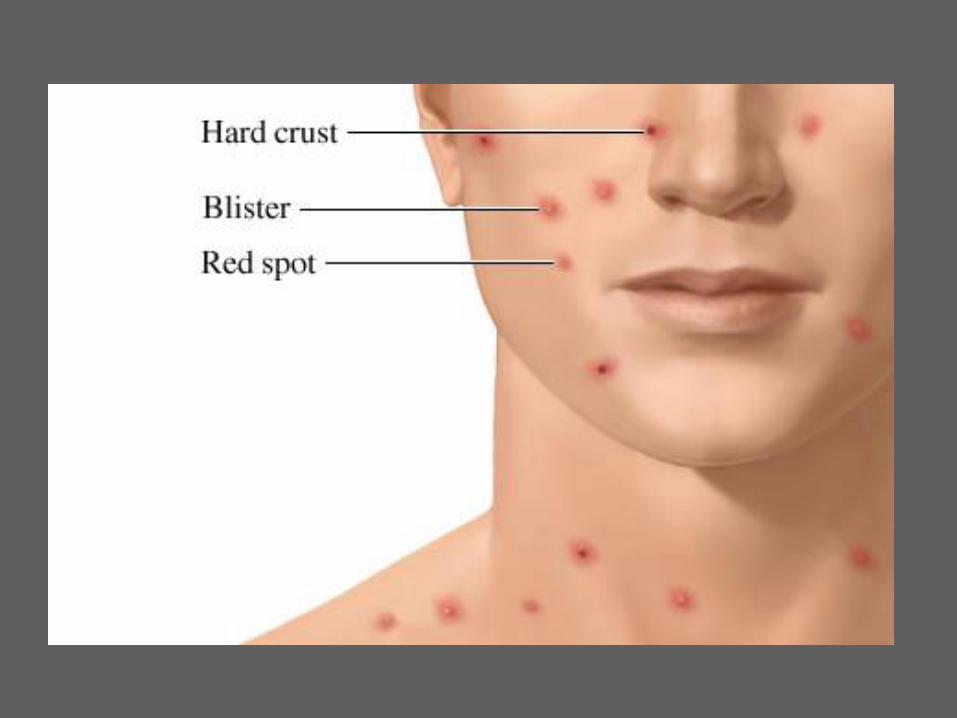
Varicella (chickenpox)
Initial infection with VZV in an unprotected host.
Spread by droplets („windpox”)
Reifection and a second clinical attack of varicella
is unheard of in normal individuals
Incubation period: 2 weeks
Fever, malaise
Widespread blisters typically on an
erythematous base
Scalp typically affected
Lesions in many stages: macules, blisters,
erosions, crust


Therapy
Oral acyclovir reduces the severity of varicella
Antibiotics
Zinc oxide lotion

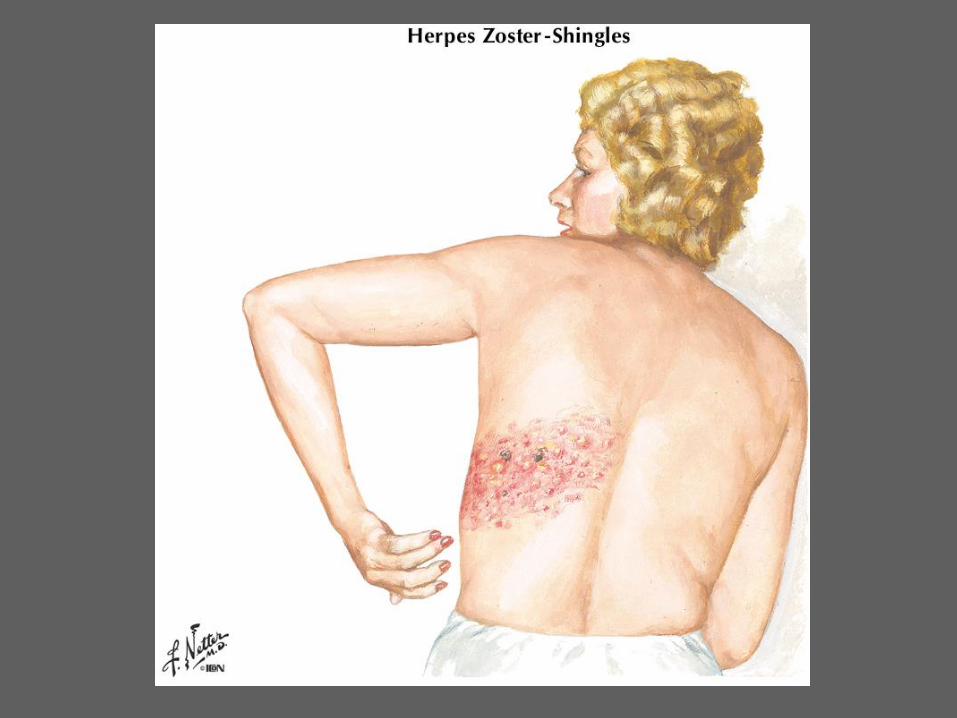
ZOSTER
SECOND INFECTION WITH vzv USUALLY IN
ADULTS AND LIMITED TO A DERMATOME
Primarily a disease of elderly and
immunosuppressed
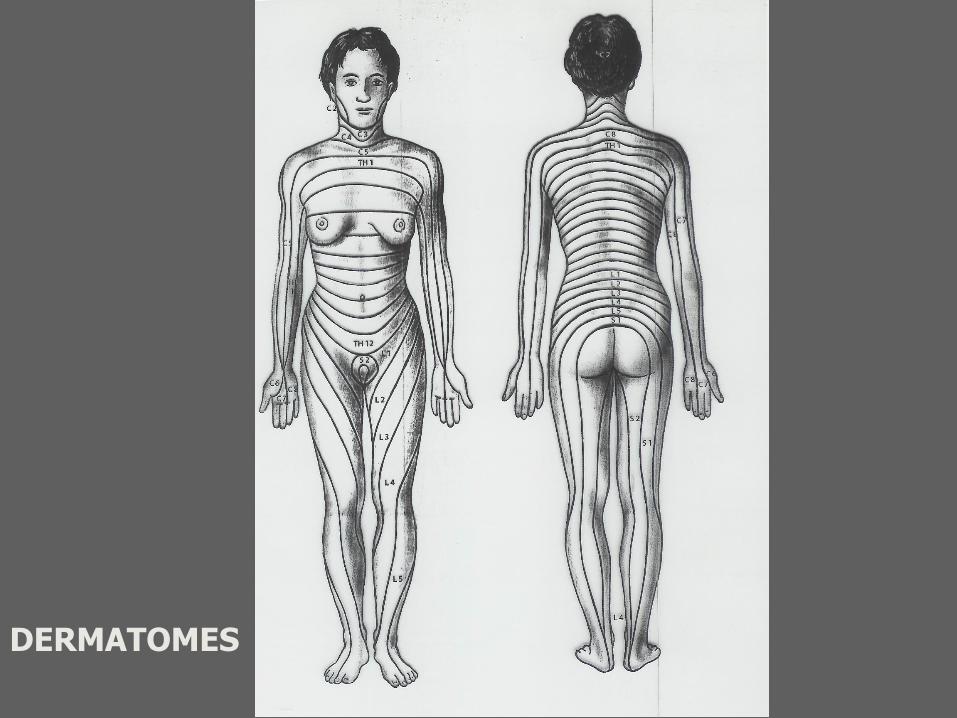
DERMATOMES
Varicella zoster virus remains in a neural ganglion while the patient has general immunity to the virus.
Factors triggering the outbreak of zoster:
Trauma
Radiation therapy
Sunburn
Other infections (syphilis)
Immunosupression (HIV, leukemia, lymphoma, chemotherapy)
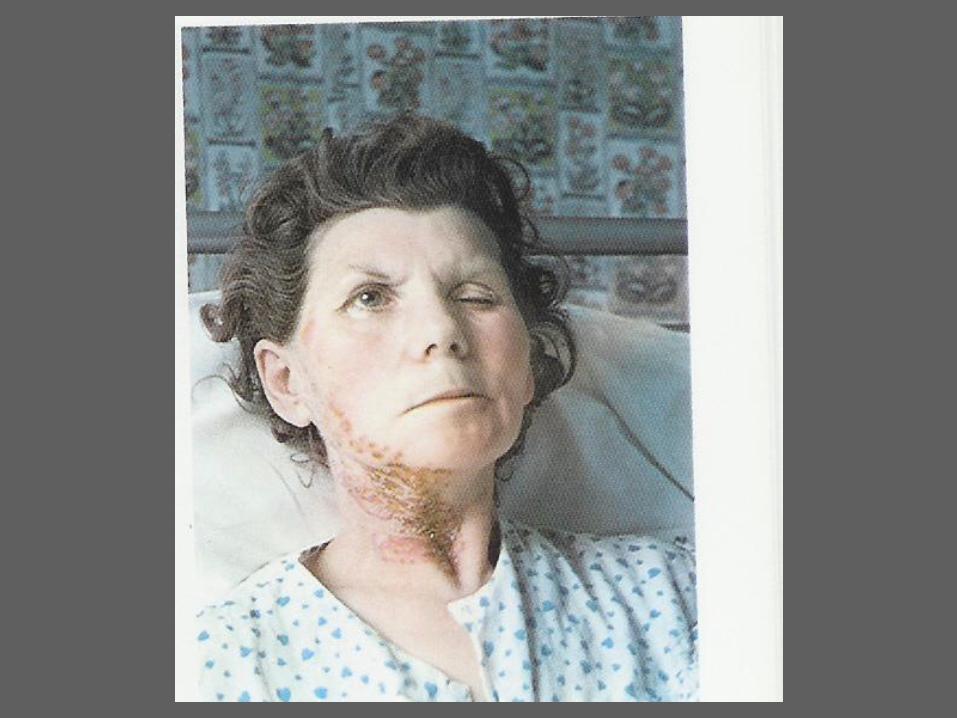
Clinical findings
- face: area of three branches of cranial nerve V
involved (forehead, mid-face and jaw line)
- Trunk
- Initially the patient experiences pain before skin
lesions appear


Postherpetic neuralgia
Persistent pain which may last for months to years
and which may be disabling.
Up to 30% of elderly patients develop some degree
of neuralgia.
Special variants of zoster
Oral zoster (hard palate, maxilla, tongue)
Otic zoster (tympanic membrane and ear canal)
Hemorrhagic and necrotic zoster
disseminated zoster



Therapy
Aciclovir
Topical drying agents (zinc oxide lotion or
clioquinol lotion)
Antibiotics (doxycycline)
Postherpetic neuralgia: antiviral agents,
psychotherapeutic agents: carbamazepine
POX VIRUSES
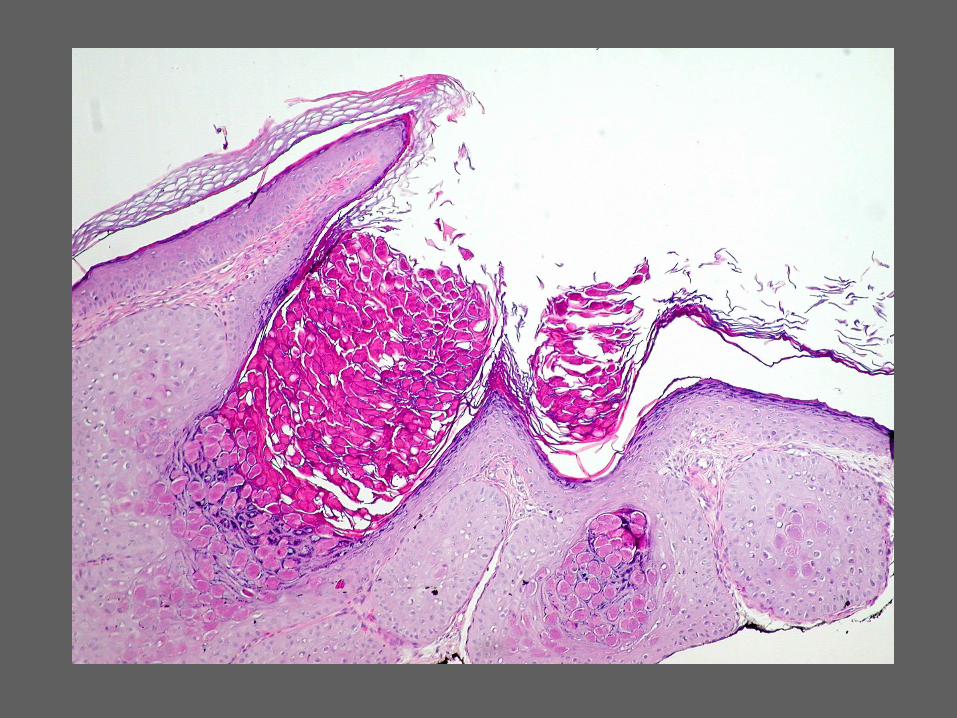
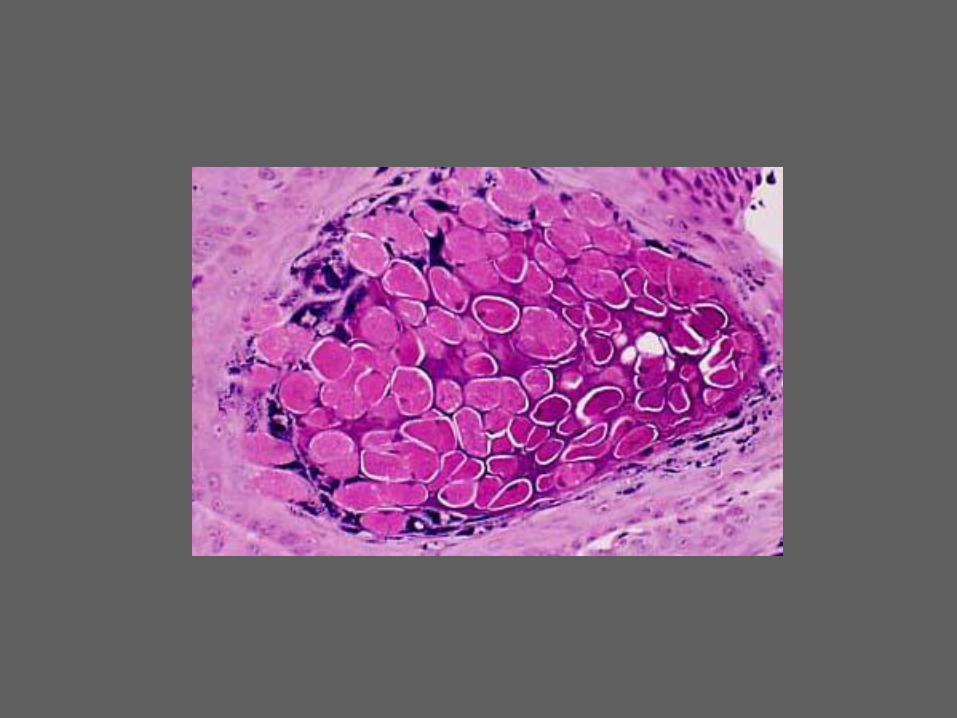
Moluscum contagiosum
Epidermotropic pox viruse infection producing
papular lesions with a central dell.
Common viral infection: in children spread by
casual contact; in adults: transmitted during
sexual intercourse.
Clinical findings
Small flesh-colored papules with a central
depresion (hollow, dell)
Lesions may be grouped together
Inguinal, axillary, neck region
Eyelids: troublesome site!
Adults: genital region





Therapy
Curettage after local anaesthesia (EMLA) or
general anaesthesia if lesions are multiple in a
small child
Lesions can be opened with a needle or forceps
Iodine paint