Embed Size (px)
DESCRIPTION
up to date
Citation preview
journal.publications.chestnet.org 1013
[ Original Research Signs and Symptoms of Chest Diseases ]
Manuscript received January 15, 2014; revision accepted April 11, 2014; originally published Online First May 29, 2014.
ABBREVIATIONS: CXCL 5 C-X-C motif ligand; CXCR 5 C-X-C motif receptor; IL-1RA 5 IL-1 receptor antagonist; IRAK 5 IL-1 receptor-associated kinase; NF- k B 5 nuclear factor- k B; PBB 5 protracted bacte-rial bronchitis; PELI1 5 pellino-1; Q 5 quartile; TLR 5 Toll-like receptor; TNF 5 tumor necrosis factor
AFFILIATIONS: From the Priority Research Centre for Asthma and Respiratory Diseases (Drs Baines, Simpson, and Gibson), Th e University of Newcastle, Callaghan, NSW; Department of Respiratory and Sleep Medicine (Drs Baines, Simpson, and Gibson), Hunter Medical Research Institute, John Hunter Hospital, New Lambton Heights, NSW; School of Medicine (Drs Upham, Yerkovich, and Marchant and Ms Carroll), Th e University of Queensland, Brisbane, QLD; Qld Lung Transplant Service (Dr Yerkovich), Th e Prince Charles Hospital, Brisbane, QLD; Depart-ment of Respiratory Medicine (Drs Chang and Marchant), Queensland Children’s Medical Research Institute, Royal Children’s Hospital,
Brisbane, QLD; and Child Health Division (Dr Chang), Menzies School of Health Research, Darwin, NT, Australia.
FUNDING/SUPPORT: Drs Gibson , Upham, and Chang are supported by National Health and Medical Research Council (NHMRC; Common-wealth of Australia) fellowships [Grants 569240, 511019, and 545216, respectively]. Dr Baines is supported by a research fellowship from Th e University of Newcastle. Th e study was funded by the Financial Markets Foundation for Children [Grant 2010-005], NHMRC [Grant 1042601], and NHMRC Centre of Research Excellence (CRE) in Lung Health of Aboriginal and Torres Strait Islander Children [Grant 1040830].
CORRESPONDENCE TO: Katherine J. Baines, PhD, Level 2 West, HMRI Bldg, Lot 1 Kookaburra Circuit, New Lambton Heights, NSW 2305, Australia; e-mail: [email protected]
© 2014 AMERICAN COLLEGE OF CHEST PHYSICIANS. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details.
DOI: 10.1378/chest.14-0131
Mediators of Neutrophil Function in Children With Protracted Bacterial Bronchitis
Katherine J. Baines , PhD ; John W. Upham , PhD ; Stephanie T. Yerkovich , PhD ; Anne B. Chang , PhD ;
Julie M. Marchant , PhD ; Melanie Carroll , BSc ( Hons ); Jodie L. Simpson , PhD ; and Peter G. Gibson , MBBS
BACKGROUND: Protracted bacterial bronchitis (PBB) is a common and treatable cause of
chronic wet cough in children in which the mechanisms are not understood. Th is study inves-
tigates the IL-1 pathway and a neutrophil gene expression signature in PBB.
METHODS: BAL was collected from children in an experimental cohort (n 5 21, PBB; n 5 33,
control subjects), and a second validation cohort (n 5 36, PBB; n 5 11, control subjects). IL-1 b ,
IL-1 receptor antagonist (IL-1RA), and a -defensins 1-3 were assayed by enzyme-linked immu-
nosorbent assay, western blot, and quantitative real-time polymerase chain reaction, together
with selected IL-1 pathway members and neutrophil-related molecules.
RESULTS: In the experimental cohort, children with symptomatic PBB had signifi cantly higher
levels of IL-1 b and a -defensin gene and protein expression. Expression of the neutrophil che-
mokine receptor C-X-C motif receptor 2 was also higher in PBB. IL-1RA protein was higher,
however, the IL-1RA:IL-1 b ratio was lower in children with PBB than control subjects. In the
validation cohort, protein and gene expression of IL-1 b and a -defensins 1-3 were confi rmed
higher, as was gene expression of IL-1 pathway members and C-X-C motif receptor 2. IL-1 b
and a -defensin 1-3 levels lowered when PBB was treated and resolved. In children with recurrent
PBB, gene expression of the IL-1 b signaling molecules pellino-1 and IL-1 receptor-associated
kinase 2 was signifi cantly higher. IL-1 b protein levels correlated with BAL neutrophilia and
the duration and severity of cough symptoms. IL-1 b and a -defensin 1-3 levels were highly
correlated.
CONCLUSIONS: PBB is characterized by increased IL-1 b pathway activation. IL-1 b and related
mediators were associated with BAL neutrophils, cough symptoms, and disease recurrence,
providing insight into PBB pathogenesis. CHEST 2014; 146(4):1013- 1020
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014

1014 Original Research [ 1 4 6 # 4 C H E S T O C TO B E R 2 0 1 4 ]
Protracted bacterial bronchitis (PBB) is an important
and common cause of chronic wet cough in children. 1
Once correctly diagnosed, the child’s cough resolves
with prolonged antibiotic therapy. 2 PBB is now interna-
tionally accepted as a diagnostic entity 3 and has been
incorporated into national 4 and international 5 pediatric
guidelines for cough management. However, despite
this increased clinical recognition, the underlying mech-
anisms of PBB remain to be elucidated.
Prior studies have shown that bacterial colonization and
airway neutrophilia are present in children with PBB. 2,6
Th is was associated with upregulation of the Toll-like
receptors (TLRs) TLR2 and TLR4 in the BAL of chil-
dren with PBB. 6 Th is implicates persistent neutrophilic
infl ammation in the pathogenesis of PBB and suggests
that neutrophil pathway mediators such as IL-1 b may
play an important role in pathogenesis. In adults with
neutrophilic asthma, using gene expression profi ling we
have implicated the IL-1 and tumor necrosis factor
(TNF)- a /nuclear factor- k B (NF- k B) pathways in
sputum 7 and a blood gene expression signature
involving neutrophil defensins and proteases. 8 Since
neutrophils play a role in both PBB and neutrophilic
asthma, there may be common mechanisms involved.
Th erefore, this study evaluated these pathways and
mediators in two cohorts of PBB and control children.
We hypothesized that IL-1 b and the neutrophil gene
expression signature would be elevated in PBB and
related to symptoms and recurrence.
Materials and Methods Subject Recruitment and Sampling
Infl ammatory mediators were evaluated in two cohorts. Th e experi-
mental cohort (n 5 54) comprised subjects and BAL samples collected
in previous studies. 6,9 Th e validation cohort (n 5 47) was obtained
from a second cohort with purposive matching of control subjects. 2
Th e selection of samples for analysis was based on the availability of
specimens and clinical diagnosis; details of enrollment of children is
described previously. 2,6,9 A clinical history was obtained on the day of
the bronchoscopy, and parents were provided with a cough diary card 10
used to document response to antibiotics, defi ned as absence of cough
or . 75% reduction in score (for � 3 days) within 2 weeks of antibi-
otic use (amoxycillin-clauvanate 45 mg/kg/d in two doses for 14 days 2 )
postbronchoscopy. In the validation cohort, children with PBB were
contacted at monthly intervals to document recurrence.
PBB was defi ned as the presence of a history of chronic ( . 4 weeks)
wet cough and a response to antibiotic treatment with resolution of the
cough within 2 weeks in the absence of signs and symptoms of other
diseases. Symptomatic PBB was defi ned as children with PBB who
were coughing when bronchoscopy was undertaken. Resolved PBB
was defi ned as children who previously had a chronic wet cough that
responded to 2 weeks of antibiotics and who were cough-free at the
time when bronchoscopy was undertaken. Recurrent PBB was defi ned
prospectively as more than three episodes of wet cough responding to
antibiotic treatment within 12 months following the initial diagnosis,
and nonrecurrent PBB as those with fewer than three episodes in the
same timeframe.
Experimental cohort control was a convenient sample of children
undergoing gastroscopy, whereas in the validation cohort control sub-
jects were age-matched and obtained opportunistically from children
undergoing bronchoscopy for assessment of the airways (eg, stridor)
with no history of chronic cough and no respiratory infection in the pre-
ceding 2 weeks. Informed consent was obtained, and the studies were
approved by the Ethics Committees of the Royal Children’s Hospital
and University of Queensland (HREC/03/QRCH/17).
Target Selection and Gene Expression
Inflammatory gene expression was determined in RNA extracted
from BAL cell pellets using real-time quantitative polymerase chain
reaction and standardized TaqMan methods as described in detail
in e-Appendix 1 . Genes tested include those previously identifi ed as
increased in sputum in neutrophilic asthma and include IL-1 b ( IL1B ),
IL-1 receptor 2 ( IL1R2 ), IL-1 receptor antagonist ( IL1RN ), pellino-1
( PELI1 ), and IL-1 receptor-associated kinase 2 ( IRAK2 ); TNF- a /NF- k B
pathway members TNF receptor superfamily member 1B ( TNFRSF1B )
and NF- k light polypeptide gene enhancer in B cells 2 ( NFKB2 ); and
the chemoattractant receptor C-X-C motif receptor 2 ( CXCR2 ). 7 Also
tested was a blood neutrophil gene expression signature including the
a -defensins ( DEFA1-3 and DEFA4 ), protease elastase ( ELANE ), and
cathepsin G ( CTSG ). 8
Protein Measurements
IL-1 b (undiluted) and IL-1 receptor antagonist (IL-1RA) (one-fi ft h
dilution) protein levels were measured in BAL supernatant using the
DuoSet enzyme-linked immunosorbent assay as per the manufacturer’s
instructions (R&D Systems, Inc). a -Defensins 1-3 (also known as the
human neutrophil peptides 1-3) were measured in BAL supernatant
(undiluted) using the Human HNP1-3 enzyme-linked immunosorbent
assay kit as per the manufacturer’s instructions (HK317; Hycult Biotech).
Western blot was performed on undiluted BAL from a subset of subjects
in the experimental cohort as described in e-Appendix 1 .
Statistical Analysis
Data were analyzed using Stata 11 (StataCorp LP) and reported as
median (quartile [Q]1, Q3). Statistical comparisons were performed
using the two-sample Wilcoxon rank sum (Mann-Whitney) test for
nonparametric data with P , .05 considered signifi cant. Spearman rank
correlations were used to test relationships.
Results
Clinical Characteristics
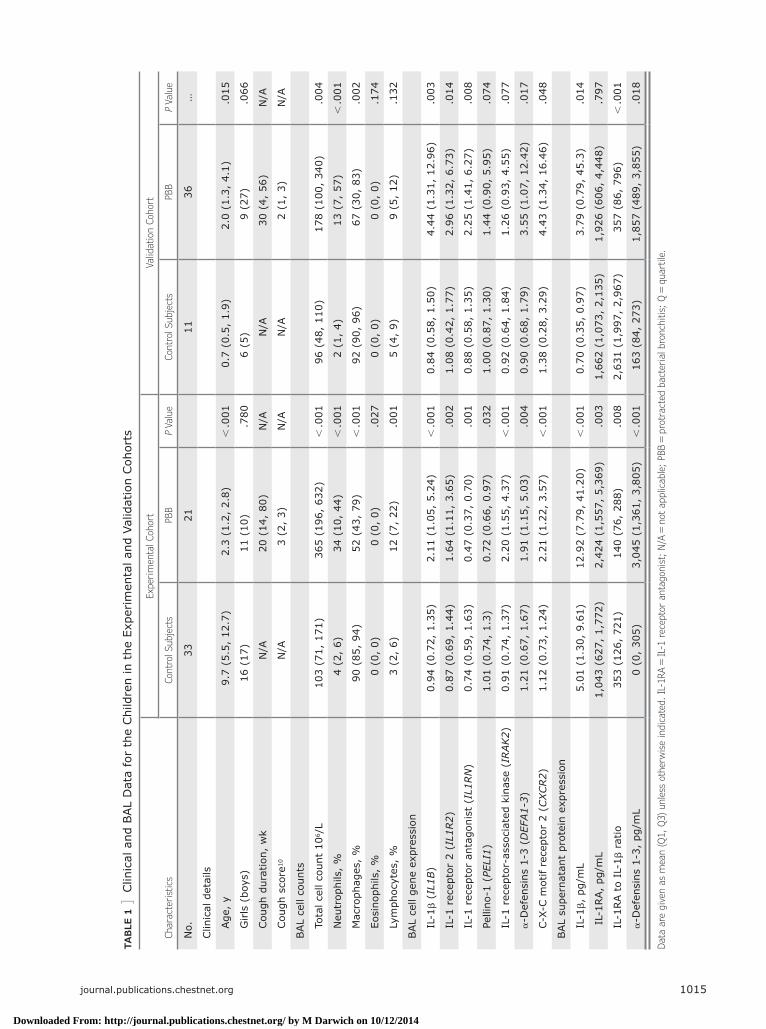
Th e children with PBB in both the experimental (n 5 21)
( Table 1 ) and validation (n 5 36) ( Table 1 ) cohorts com-
prised mainly infants and young children with similar
profi les of moderate cough severity and a mean symp-
tom duration of . 20 weeks. Lung infl amma tion was
present with increased BAL cellularity including neutro-
phils. Th e validation cohort tended to have more males
and less intense airway neutrophilia than the experi-
mental cohort. Th e control subjects were older in the
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014
journal.publications.chestnet.org 1015
TAB
LE 1
] C
linic
al a
nd B
AL
Dat
a fo
r th
e Chi
ldre
n in
the
Exp
erim
enta
l and
Val
idat
ion
Coh
orts
Cha
ract
eris
tics
Expe
rim
enta
l Coh
ort
Valid
atio
n Coh
ort
Con
trol
Sub
ject
sPB
B P
Valu
eCon
trol
Sub
ject
sPB
B P
Valu
e
No.
3321
1136
…
Clin
ical
det
ails
Age
, y
9.7
(5.5
, 12
.7)
2.3
(1.2
, 2.
8) ,
.001
0.7
(0.5
, 1.
9)2.
0 (1
.3,
4.1)
.015
G
irls
(bo
ys)
16 (
17)
11 (
10)
.780
6 (5
)9
(27)
.066
Cou
gh d
urat
ion,
wk
N/A
20 (
14,
80)
N/A
N/A
30 (
4, 5
6)N
/A
Cou
gh s
core
10
N/A
3 (2
, 3)
N/A
N/A
2 (1
, 3)
N/A
BAL
cell
coun
ts
To
tal c
ell c
ount
10 6
/L10
3 (7
1, 1
71)
365
(196
, 63
2) ,
.001
96 (
48,
110)
178
(100
, 34
0).0
04
N
eutr
ophi
ls,
%4
(2,
6)34
(10
, 44
) ,
.001
2 (1
, 4)
13 (
7, 5
7) ,
.001
M
acro
phag
es,
%90
(85
, 94
)52
(43
, 79
) ,
.001
92 (
90,
96)
67 (
30,
83)
.002
Eo
sino
phils
, %
0 (0
, 0)
0 (0
, 0)
.027
0 (0
, 0)
0 (0
, 0)
.174
Ly
mph
ocyt
es,
%3
(2,
6)12
(7,
22)
.001
5 (4
, 9)
9 (5
, 12
).1
32
BAL
cell
gene
exp
ress
ion
IL
-1 b
( IL1B )
0.94
(0.
72,
1.35
)2.
11 (
1.05
, 5.
24)
, .0
010.
84 (
0.58
, 1.
50)
4.44
(1.
31,
12.9
6).0
03
IL
-1 r
ecep
tor
2 ( IL1R2 )
0.87
(0.
69,
1.44
)1.
64 (
1.11
, 3.
65)
.002
1.08
(0.
42,
1.77
)2.
96 (
1.32
, 6.
73)
.014
IL
-1 r
ecep
tor
anta
goni
st (
IL1RN
)0.
74 (
0.59
, 1.
63)
0.47
(0.
37,
0.70
).0
010.
88 (
0.58
, 1.
35)
2.25
(1.
41,
6.27
).0
08
Pe
llino
-1 (
PELI1 )
1.01
(0.
74,
1.3)
0.72
(0.
66,
0.97
).0
321.
00 (
0.87
, 1.
30)
1.44
(0.
90,
5.95
).0
74
IL
-1 r
ecep
tor-
asso
ciat
ed k
inas
e ( IRAK2 )
0.91
(0.
74,
1.37
)2.
20 (
1.55
, 4.
37)
, .0
010.
92 (
0.64
, 1.
84)
1.26
(0.
93,
4.55
).0
77
a -
Def
ensi
ns 1
-3 (
DEFA1-3 )
1.21
(0.
67,
1.67
)1.
91 (
1.15
, 5.
03)
.004
0.90
(0.
68,
1.79
)3.
55 (
1.07
, 12
.42)
.017
C-
X-C m
otif
rece
ptor
2 (
CXCR2 )
1.12
(0.
73,
1.24
)2.
21 (
1.22
, 3.
57)
, .0
011.
38 (
0.28
, 3.
29)
4.43
(1.
34,
16.4
6).0
48
BAL
supe
rnat
ant
prot
ein
expr
essi
on
IL
-1 b ,
pg/
mL
5.01
(1.
30,
9.61
)12
.92
(7.7
9, 4
1.20
) ,
.001
0.70
(0.
35,
0.97
)3.
79 (
0.79
, 45
.3)
.014
I
L-1R
A,
pg/m
L1,
043
(627
, 1,
772)
2,42
4 (1
,557
, 5,
369)
.003
1,66
2 (1
,073
, 2,
135)
1,92
6 (6
06,
4,44
8).7
97
IL
-1RA t
o IL
-1 b
ratio
353
(126
, 72
1)14
0 (7
6, 2
88)
.008
2,63
1 (1
,997
, 2,
967)
357
(86,
796
) ,
.001
a -
Def
ensi
ns 1
-3,
pg/m
L0
(0,
305)
3,04
5 (1
,361
, 3,
805)
, .0
0116
3 (8
4, 2
73)
1,85
7 (4
89,
3,85
5).0
18
Dat
a ar
e gi
ven
as m
ean
(Q1,
Q3)
unl
ess
othe
rwis
e in
dica
ted.
IL-
1RA 5
IL-1
rec
epto
r an
tago
nist
; N/A
5 n
ot a
pplic
able
; PB
B 5
pro
trac
ted
bact
eria
l bro
nchi
tis;
Q 5
qua
rtile
.
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014
1016 Original Research [ 1 4 6 # 4 C H E S T O C TO B E R 2 0 1 4 ]
experimental cohort, but ages were similar in the valida-
tion cohort.
Gene expression was measured in the entire experimental
cohort, and protein was assessed in 30 control subjects
and 21 subjects with PBB. In the validation cohort,
IL-1 b and IL-1RA protein were measured in 10 control
subjects and 29 PBB subjects, a -defensin 1-3 protein
was measured in fi ve control subjects and 24 subjects
with PBB, and gene expression was assessed in 10 con-
trol subjects and 36 subjects with PBB, except for C-X-C
motif receptor (CXCR) 2 (eight control subjects and
25 subjects with PBB) due to insuffi cient remaining
samples.
Mediators in the Experimental Cohort
Th ere was altered expression of IL-1 pathway members
IL1B , IL1R2 , IL1RN , PELI1 , and IRAK2 and the neutro-
phil chemokine receptor CXCR2 in PBB ( Table 1 ) but
not TNF- a /NF- k B pathway members TNFRSF1B
[control subjects: 1.03 (0.77, 1.35); PBB: 1.09 (0.94, 1.49);
P 5 .183] and NFKB2 [control subjects: 1.06 (0.63, 1.53);
PBB: 1.16 (0.84, 1.48); P 5 .419]. Gene expression of
DEFA1-3 was higher in PBB, but ELANE [control sub-
jects: 1.21 (0.49, 2.04); PBB: 1.45 (0.92, 2.06); P 5 .370]
and CTSG [control subjects: 0.91 (0.72, 1.29); PBB: 0.84
(0.57, 1.35); P 5 .299] were not changed, and DEFA4
was not detected.
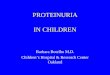
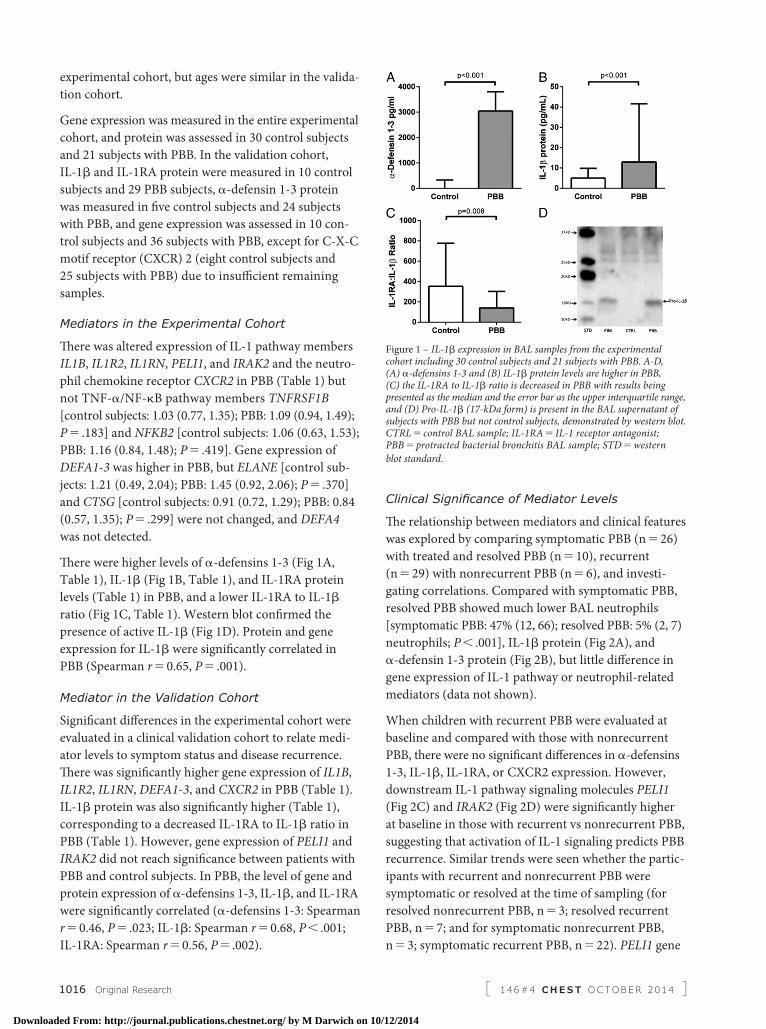
Th ere were higher levels of a -defensins 1-3 ( Fig 1A ,
Table 1 ), IL-1 b ( Fig 1B , Table 1 ), and IL-1RA protein
levels ( Table 1 ) in PBB, and a lower IL-1RA to IL-1 b
ratio ( Fig 1C , Table 1 ). Western blot confi rmed the
presence of active IL-1 b ( Fig 1D ). Protein and gene
expression for IL-1 b were signifi cantly correlated in
PBB (Spearman r 5 0.65, P 5 .001).
Mediator in the Validation Cohort
Signifi cant diff erences in the experimental cohort were
evaluated in a clinical validation cohort to relate medi-
ator levels to symptom status and disease recurrence.
Th ere was signifi cantly higher gene expression of IL1B ,
IL1R2 , IL1RN , DEFA1-3 , and CXCR2 in PBB ( Table 1 ).
IL-1 b protein was also signifi cantly higher ( Table 1 ),
corresponding to a decreased IL-1RA to IL-1 b ratio in
PBB ( Table 1 ). However, gene expression of PELI1 and
IRAK2 did not reach signifi cance between patients with
PBB and control subjects. In PBB, the level of gene and
protein expression of a -defensins 1-3, IL-1 b , and IL-1RA
were signifi cantly correlated ( a -defensins 1-3: Spearman
r 5 0.46, P 5 .023; IL-1 b : Spearman r 5 0.68, P , .001;
IL-1RA: Spearman r 5 0.56, P 5 .002).
Clinical Signifi cance of Mediator Levels
Th e relationship between mediators and clinical features
was explored by comparing symptomatic PBB (n 5 26)
with treated and resolved PBB (n 5 10), recurrent
(n 5 29) with nonrecurrent PBB (n 5 6), and investi-
gating correlations. Compared with symptomatic PBB,
resolved PBB showed much lower BAL neutrophils
[symptomatic PBB: 47% (12, 66); resolved PBB: 5% (2, 7)
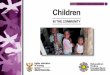
neutrophils; P , .001], IL-1 b protein ( Fig 2A ), and
a -defensin 1-3 protein ( Fig 2B ), but little diff erence in
gene expression of IL-1 pathway or neutrophil-related
mediators (data not shown).
When children with recurrent PBB were evaluated at
baseline and compared with those with nonrecurrent
PBB, there were no signifi cant diff erences in a -defensins
1-3, IL-1 b , IL-1RA, or CXCR2 expression. However,
downstream IL-1 pathway signaling molecules PELI1
( Fig 2C ) and IRAK2 ( Fig 2D ) were signifi cantly higher
at baseline in those with recurrent vs nonrecurrent PBB,
suggesting that activation of IL-1 signaling predicts PBB
recurrence. Similar trends were seen whether the partic-
ipants with recurrent and nonrecurrent PBB were
symptomatic or resolved at the time of sampling (for
resolved nonrecurrent PBB, n 5 3; resolved recurrent
PBB, n 5 7; and for symptomatic nonrecurrent PBB,
n 5 3; symptomatic recurrent PBB, n 5 22). PELI1 gene
Figure 1 – IL-1 b expression in BAL samples from the experimental cohort including 30 control subjects and 21 subjects with PBB. A-D, (A) a -defensins 1-3 and (B) IL-1 b protein levels are higher in PBB, (C) the IL-1RA to IL-1 b ratio is decreased in PBB with results being presented as the median and the error bar as the upper interquartile range, and (D) Pro-IL-1 b (17-kDa form) is present in the BAL supernatant of subjects with PBB but not control subjects, demonstrated by western blot. CTRL 5 control BAL sample; IL-1RA 5 IL-1 receptor antagonist; PBB 5 protracted bacterial bronchitis BAL sample; STD 5 western
blot standard.
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014
journal.publications.chestnet.org 1017
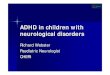
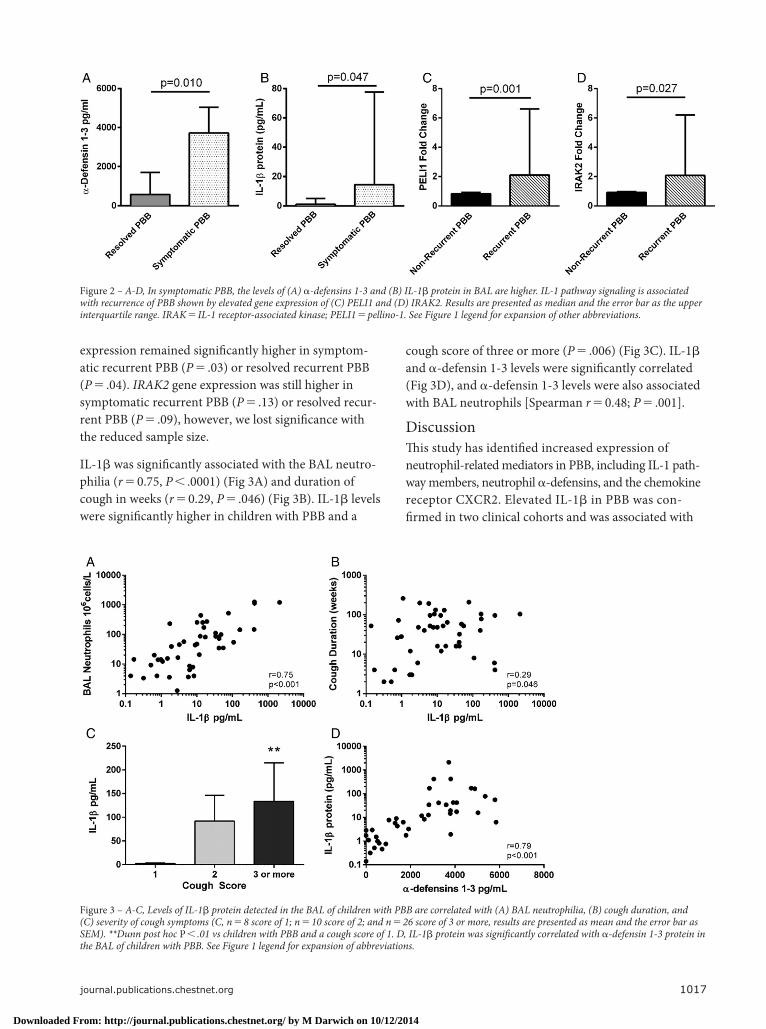
Figure 3 – A-C, Levels of IL-1 b protein detected in the BAL of children with PBB are correlated with (A) BAL neutrophilia, (B) cough duration, and (C) severity of cough symptoms (C, n 5 8 score of 1; n 5 10 score of 2; and n 5 26 score of 3 or more, results are presented as mean and the error bar as SEM). **Dunn post hoc P , .01 vs children with PBB and a cough score of 1. D, IL-1 b protein was signifi cantly correlated with a -defensin 1-3 protein in the BAL of children with PBB. See Figure 1 legend for expansion of abbreviations.
expression remained signifi cantly higher in symptom-
atic recurrent PBB ( P 5 .03) or resolved recurrent PBB
( P 5 .04). IRAK2 gene expression was still higher in
symptomatic recurrent PBB ( P 5 .13) or resolved recur-
rent PBB ( P 5 .09), however, we lost signifi cance with
the reduced sample size.
IL-1 b was signifi cantly associated with the BAL neutro-
philia ( r 5 0.75, P , .0001) (Fig 3A) and duration of
cough in weeks ( r 5 0.29, P 5 .046) (Fig 3B). IL-1 b levels
were signifi cantly higher in children with PBB and a
cough score of three or more ( P 5 .006) (Fig 3C). IL-1 b
and a -defensin 1-3 levels were signifi cantly correlated
( Fig 3D ), and a -defensin 1-3 levels were also associated
with BAL neutrophils [Spearman r 5 0.48; P 5 .001].
Discussion
Th is study has identifi ed increased expression of
neutrophil-related mediators in PBB, including IL-1 path-
way members, neutrophil a -defensins, and the chemokine
receptor CXCR2. Elevated IL-1 b in PBB was con-
fi rmed in two clinical cohorts and was associated with
Figure 2 – A-D, In symptomatic PBB, the levels of (A) a -defensins 1-3 and (B) IL-1 b protein in BAL are higher. IL-1 pathway signaling is associated with recurrence of PBB shown by elevated gene expression of (C) PELI1 and (D) IRAK2. Results are presented as median and the error bar as the upper interquartile range. IRAK 5 IL-1 receptor-associated kinase; PELI1 5 pellino-1. See Figure 1 legend for expansion of other abbreviations.
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014

1018 Original Research [ 1 4 6 # 4 C H E S T O C TO B E R 2 0 1 4 ]
symptomatic PBB. Importantly, IL-1 b protein levels
were correlated with BAL neutrophilia, as well as the
duration and severity of cough symptoms. Additionally,
baseline expression (time of bronchoscopy) of IL-1
pathway signaling members IL-1 receptor associated
kinase (IRAK) 2 and pellino-1 (PELI1) was higher in
those children who were more likely to experience
disease recurrence (more than three episodes of wet
cough in the year following baseline bronchoscopy). Th e
expression of a -defensins 1-3 was increased in PBB and
was signifi cantly correlated with IL-1 b .
IL-1 b is an important mediator of the infl ammatory
response and host defense, however, dysregulated and
persistent IL-1 b release can harm the host and has been
linked to the pathogenesis of several diseases such as
rheumatoid arthritis, type 2 diabetes mellitus, and
atherosclerosis, as well as certain specifi c autophagocytic
conditions. 11 IL-1 b is secreted as the inactive pro mole-
cule, proIL-1 b , and is then processed enzymatically to
activated IL-1 b . Typically this occurs via caspase-1 and
infl ammasome activation. 12 However, activation of
IL-1 b when released from neutrophils is not exclusively
dependent on caspase-1, as enzymes including neutro-
phil elastase are able to cleave IL-1 b into its active
form. 13 Released and active IL-1 b binds to its receptor
IL-1R1 and initiates a signaling cascade through MyD88
and IRAK1/IRAK4, assisted by IRAK2 and PELI1.
Eff ects of IL-1 b are blocked through its decoy receptor
IL-1 receptor 2 and receptor antagonist IL-1RA. 14 Th is
study shows that IL-1 b is associated with increased BAL
neutrophilia, suggesting that either neutrophils are the
source of this cytokine production, or alternatively that
IL-1 b induces neutrophil infi ltration into the lung. Either
way, our previous reports 6 detail increases in neutrophil
proteases including matrix metalloproteinase-9, which
may lead to activation of IL-1 b -mediated neutrophil infl ux.
IL-1 b has been observed to be elevated in other airway
diseases characterized by airway neutrophilia and/or
infection, such as neutrophilic asthma, 7 COPD, 15 cystic
fi brosis, 16 and non-cystic fi brosis bronchiectasis. 17 IL-1 b
is increased in stable COPD as well as acute exacerba-
tions, where it is associated with bacterial infection. 18
Bacterial infection is frequently detected in PBB and the
relationship between bacteria and IL-1 b activation in
PBB needs further research. In a number of models of
Pseudomonas pulmonary infection, IL-1 b production
occurs in response to bacterial infection 19 and is a deter-
minant of neutrophil infl ux likely through C-X-C motif
ligand (CXCL) 8. IL-1 plays a key role in coordinating
chemokine responses that lead to neutrophil infi ltration
in the lung. 20 Elevated IL-1 b in PBB is, therefore, consis-
tent with known host responses in neutrophilic airway
diseases, and suggests bacterial infection and neutrophil
infl ux are key features leading to ongoing IL-1 b release
and PBB symptoms.
Although PBB responds well to prolonged antibiotic
therapy, it can recur. In another infective disease, viral
encephalitis, levels of IL-1 b and IL-1RA were related to
prognosis. 21 We found that IL-1 b levels were highest in
symptomatic PBB and subjects with PBB who had
higher cough scores. IL-1 signaling molecules IRAK2
and PELI1 had signifi cantly increased gene expression
at baseline in children who went on to develop recur-
rent PBB. Th is suggests that IL-1 b pathway activation
may determine PBB recurrence. PELI1 is important in
regulating the innate immune response of the epithe-
lium to rhinovirus infection, including CXCL8 produc-
tion and neutrophil recruitment. 22 IRAK2 is critical in
sustaining late-phase infl ammatory responses aft er TLR
stimulation, which leads to increased cytokine produc-
tion. 23 We have previously reported the upregulation of
PELI1 and IRAK2 in response to rhinovirus infection of
human primary bronchial epithelial cells in COPD. 24
Th is evidence collectively suggests that IRAK2 and
PELI1 promote neutrophilic airway infl ammation trig-
gered by infection and IL-1 b and that this response is
dysregulated in PBB and contributes to disease
recurrence.
Th is study also reports increased expression of the CXCL8
high-affi nity G-protein-coupled receptor CXCR2 and
the neutrophil a -defensins 1-3 in PBB. CXCR2 is
thought to be involved in uncontrolled neutrophil infl ux
into the airways in acute lung injury. 25 Defensins are
small arginine-rich cationic peptides that have antimi-
crobial activity against a broad range of pathogens and
exert their antimicrobial eff ect through membrane per-
meabilization. Th e level of neutrophil a -defensins 1-3
was higher in symptomatic PBB and was signifi cantly
correlated with IL-1 b , indicating that these molecules
may interact and infl uence PBB pathogenesis. Indeed,
recent evidence implicates a -defensins in the release of
IL-1 b from lipopolysaccharide-primed macrophages
through the P2X7 receptor. 26 Intratracheal instillation of
a -defensins in mice leads to acute lung infl ammation
and dysfunction involving neutrophil infl ux and elas-
tase release. 27 a -defensins have a cytotoxic eff ect,
induce IL-8 and IL-1 b gene expression, IL-8 protein
production, and NF- k B binding activity in human
bronchial epithelial cells. 28 Expression of TNF/NF- k B
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014

journal.publications.chestnet.org 1019
Acknowledgments Author contributions: K. J. B., J. W. U., A. B. C., and P. G. G. are guarantors of this paper and take responsibility for the integrity of the work as a whole, from inception to published article, and conceived and designed the study. K. J. B., A. B. C., J. M. M., and P. G. G. contributed to data collection and interpreta-tion; K. J. B. wrote the fi rst draft of the manu-script and performed data analysis; K. J. B. and P. G. G. contributed to the writing of the manuscript; and K. J. B., J. W. U., S. T. Y., A. B. C., J. M. M., M. C., J. L. S., and P. G. G. contributed to the editing, revising, and reviewing of the manuscript.
Financial/nonfi nancial disclosures: Th e authors have reported to CHEST the following confl icts: Dr Upham has been the recipient of peer-reviewed research fund-ing from the National Health and Medical Research Council (Commonwealth of Australia), received speaking fees from AstraZeneca, Boehringer Ingelheim GmbH, and Novartis Corp, and sits on the medical advisory boards for Boehringer Ingelheim GmbH, Th e Menarini Group, and Novartis Corp. Drs Baines, Yerkovich, Chang, Marchant, Simpson, and Gibson and Ms Carroll have reported that no potential confl icts of interest exist with any companies/organizations whose products or services may be discussed in this article.
Role of sponsors: Th e study sponsors had no role in study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the paper for publication. No form of payment was given to anyone to produce the manuscript.
Other contributions: We are grateful to all of the parents and children who participated in this study. We also thank Brent Masters, Helen Buntain, Paul Francis, Nigel Dore, and Alan Isles for allowing us to recruit their patients
into the study; Carol Willis for maintaining the database; and Sophie Anderson-James and Helen Petsky for collecting the specimens and clinical data. We also thank Naomi Fibbens, Melinda Tooze, and Kellie Fakes for their tech-nical assistance with laboratory measurements.
Additional information: Th e e-Appendix can be found in the Supplemental Materials section of the online article.
References 1 . Chang AB , Landau LI , Van Asperen PP ,
et al ; Th oracic Society of Australia and New Zealand . Cough in children: defi ni-tions and clinical evaluation . Med J Aust . 2006 ; 184 ( 8 ): 398 - 403 .
2 . Marchant J , Masters IB , Champion A , Petsky H , Chang AB . Randomised con-trolled trial of amoxycillin clavulanate in children with chronic wet cough . Th orax . 2012 ; 67 ( 8 ): 689 - 693 .
3 . Donnelly D , Critchlow A , Everard ML . Outcomes in children treated for persistent bacterial bronchitis . Th orax . 2007 ; 62 ( 1 ): 80 - 84 .
4 . Gibson PG , Chang AB , Glasgow NJ , et al ; CICADA . CICADA: Cough in children and adults: diagnosis and assessment. Australian cough guide-lines summary statement . Med J Aust . 2010 ; 192 ( 5 ): 265 - 271 .
5 . Shields MD , Bush A , Everard ML , McKenzie S , Primhak R ; British Th oracic Society Cough Guideline Group . BTS guidelines: recommendations for the assessment and management of cough in children . Th orax . 2008 ; 63 ( suppl 3 ): iii1 - iii15 .
6 . Marchant JM , Gibson PG , Grissell TV , Timmins NL , Masters IB , Chang AB . Prospective assessment of protracted bacterial bronchitis: airway infl ammation and innate immune activation . Pediatr Pulmonol . 2008 ; 43 ( 11 ): 1092 - 1099 .
7 . Baines KJ , Simpson JL , Wood LG , Scott RJ , Gibson PG . Transcriptional phenotypes of asthma defi ned by gene expression profi ling of induced spu-tum samples . J Allergy Clin Immunol . 2011 ; 127 ( 1 ): 153 - 160 .
8 . Baines KJ , Simpson JL , Wood LG , Scott RJ , Gibson PG . Systemic upregulation of neutrophil a -defensins and serine proteases in neutrophilic asthma . Th orax . 2011 ; 66 ( 11 ): 942 - 947 .
9 . Chang AB , Cox NC , Faoagali J , et al . Cough and refl ux esophagitis in children: their co-existence and airway cellularity . BMC Pediatrics . 2006 ; 6 : 4 .
10 . Chang AB , Newman RG , Carlin JB , Phelan PD , Robertson CF . Subjective scoring of cough in children: parent-completed vs child-completed diary cards vs an objective method . Eur Respir J . 1998 ; 11 ( 2 ): 462 - 466 .
11 . Dinarello CA , Simon A , van der Meer JW . Treating infl ammation by block-ing interleukin-1 in a broad spectrum of diseases . Nat Rev Drug Discov . 2012 ; 11 ( 8 ): 633 - 652 .
12 . Martinon F , Mayor A , Tschopp J . The inflammasomes: guardians of the body . Annu Rev Immunol . 2009 ; 27 : 229 - 265 .
13 . Guma M , Ronacher L , Liu-Bryan R , Takai S , Karin M , Corr M . Caspase 1-independent activation of interleukin-1 b in neutrophil-predominant infl ammation . Arthritis Rheum . 2009 ; 60 ( 12 ): 3642 - 3650 .
14 . Weber A , Wasiliew P , Kracht M . Interleukin-1 (IL-1) pathway . Sci Signal . 2010 ; 3 ( 105 ): cm1 .
15 . Pauwels NS , Bracke KR , Dupont LL , et al . Role of IL-1 a and the Nlrp3/caspase-1/IL-1 b axis in cigarette smoke-induced pulmonary infl ammation and COPD . Eur Respir J . 2011 ; 38 ( 5 ): 1019 - 1028 .
16 . Eickmeier O , Huebner M , Herrmann E , et al . Sputum biomarker profi les in cystic
pathway members remained unchanged in PBB. Th is
suggests that while there are similarities between
neutrophil-related airway diseases in children and
adults, there are diff erences that indicate diff erent trig-
gers and underlying mechanisms.
While the sample size in this study was suffi cient to
establish a role for IL-1 b in PBB, it was nonetheless
insuffi cient to evaluate whether IL-1 b levels have prog-
nostic value or are related to specifi c subsets of PBB.
Further studies of IL-1 b in larger numbers of patients
with PBB are indicated. Th e role of IL-1 b in PBB could
be strengthened by showing changes in IL-1 b aft er
treatment, however, we could not justify a second
bronchoscopy for the children aft er PBB resolution.
Th e control groups in the two studies were dissimilar,
however, age diff erences were addressed in the valida-
tion cohort where purposive sampling led to matching
of age groups in the children with PBB and control
subjects.
In summary, we have identifi ed elevated IL-1 b and
implicated the IL-1 pathway in PBB. IL-1 b gene and
protein expression was increased, and the ratio of IL-1 b
to its antagonist was decreased in PBB. IL-1 b was asso-
ciated with symptomatic PBB compared with resolved
PBB, correlated with BAL neutrophilia, as well as dura-
tion and severity of cough symptoms. IL-1 pathway
signaling was associated with PBB disease recurrence.
Expression of CXCR2 and a -defensins 1-3 was higher in
PBB, a -defensins 1-3 were associated with PBB symp-
toms, and IL-1 b and a -defensin 1-3 protein levels were
signifi cantly correlated. Further research into the role
of the IL-1 pathway and its relationship to a -defensins
1-3 in PBB is warranted. Future studies should also
examine a blood gene expression signature for PBB.
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014
1020 Original Research [ 1 4 6 # 4 C H E S T O C TO B E R 2 0 1 4 ]
fi brosis (CF) and chronic obstructive pul-monary disease (COPD) and association between pulmonary function . Cytokine . 2010 ; 50 ( 2 ): 152 - 157 .
17 . Chalmers JD , Hill AT . Mechanisms of immune dysfunction and bacterial persistence in non-cystic fi brosis bron-chiectasis . Mol Immunol . 2013 ; 55 ( 1 ): 27 - 34 .
18 . Bafadhel M , McKenna S , Terry S , et al . Acute exacerbations of chronic obstructive pulmonary disease: iden-tifi cation of biologic clusters and their biomarkers . Am J Respir Crit Care Med . 2011 ; 184 ( 6 ): 662 - 671 .
19 . Cai S , Batra S , Wakamatsu N , Pacher P , Jeyaseelan S . NLRC4 infl ammasome-mediated production of IL-1 b modulates mucosal immunity in the lung against gram-negative bacterial infection . J Immunol . 2012 ; 188 ( 11 ): 5623 - 5635 .
20 . Marriott HM , Gascoyne KA , Gowda R , et al . Interleukin-1 b regulates CXCL8 release and infl uences disease outcome
in response to Streptococcus pneu-moniae, defi ning intercellular coop-eration between pulmonary epithelial cells and macrophages . Infect Immun . 2012 ; 80 ( 3 ): 1140 - 1149 .
21 . Griffi ths MJ , Ooi MH , Wong SC , et al . In enterovirus 71 encephalitis with cardio-respiratory compromise, elevated interleukin 1 b , interleukin 1 receptor antagonist, and granulocyte colony-stimulating factor levels are markers of poor prognosis . J Infect Dis . 2012 ; 206 ( 6 ): 881 - 892 .
22 . Bennett JA , Prince LR , Parker LC , et al . Pellino-1 selectively regulates epithelial cell responses to rhinovirus . J Virol . 2012 ; 86 ( 12 ): 6595 - 6604 .
23 . Kawagoe T , Sato S , Matsushita K , et al . Sequential control of Toll-like receptor-dependent responses by IRAK1 and IRAK2 . Nat Immunol . 2008 ; 9 ( 6 ): 684 - 691 .
24 . Baines KJ , Hsu AC , Tooze M , Gunawardhana LP , Gibson PG , Wark PA . Novel immune genes associated with
excessive infl ammatory and antiviral responses to rhinovirus in COPD . Respir Res . 2013 ; 14 : 15 .
25 . Konrad FM , Reutershan J . CXCR2 in acute lung injury . Mediators Infl amm . 2012 ; 2012 : 740987 .
26 . Chen Q , Jin Y , Zhang K , et al . Alarmin HNP-1 promotes pyroptosis and IL-1 b release through diff erent roles of NLRP3 infl ammasome via P2X7 in LPS-primed macrophages . Innate Immun . 2014 ; 20 ( 3 ): 290 - 300 .
27 . Zhang H , Porro G , Orzech N , Mullen B , Liu M , Slutsky AS . Neutrophil defensins mediate acute infl ammatory response and lung dysfunction in dose-related fashion . Am J Physiol Lung Cell Mol Physiol . 2001 ; 280 ( 5 ): L947 - L954 .
28 . Sakamoto N , Mukae H , Fujii T , et al . Diff erential eff ects of alpha- and beta-defensin on cytokine production by cultured human bronchial epithelial cells . Am J Physiol Lung Cell Mol Physiol . 2005 ; 288 ( 3 ): L508 - L513 .
Downloaded From: http://journal.publications.chestnet.org/ by M Darwich on 10/12/2014