Embed Size (px)
Citation preview

Priority Medicines for Europe and the World
"A Public Health Approach to Innovation"
Update on 2004 Background Paper
Written by Bruce Neal
Background Paper 6.3
Ischaemic heart disease
By Dr Ruth Webster and Professor Anthony Rodgers
The George Institute for Global Health
Level 13, 321 Kent St
Sydney, NSW 2000, Australia
Tel +61 2 9993 4557

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-2
Table of Contents
1. Introduction ............................................................................................................................................. 4
2. What is the size and nature of the disease burden? ................................................................................. 4
3. What is the control strategy? ................................................................................................................. 11
3.1 Lifestyle intervention ........................................................................................................................... 11
3.2 Lipid-lowering therapy ......................................................................................................................... 13
3.3 Blood pressure lowering therapy ......................................................................................................... 14 3.3.1 Evidence on potential benefits of regimen simplification and use of two-drug combination pills. 15 3.3.2 Evidence on hypertension combination pills containing more than two medications ................... 16
3.4 Anti-platelet therapy ........................................................................................................................... 16
4. Why does the disease burden persist? ................................................................................................... 17
4.1 Non-optimal use of existing effective medications .............................................................................. 17
4.2 New innovative therapies .................................................................................................................... 19
5. What can be learnt from past/current research into pharmaceutical interventions for this condition? . 20
5.1 Previous trials – polypill versus placebo or no treatment .................................................................... 22 5.1.1 Summary of TIPS 1 and 2 ................................................................................................................. 22 5.1.2 Summary of Wald and Law trial ...................................................................................................... 23 5.1.3 PILL Collaborative Group ................................................................................................................. 24 5.1.4 Other trials ...................................................................................................................................... 25 5.1.5 Conclusions from previous trials of polypill versus placebo or no treatment ................................. 26
5.2 Ongoing trials – polypill versus placebo .............................................................................................. 26
5.3 Previous trials – polypill versus usual care ........................................................................................... 26 5.3.1 FP7-funded UMPIRE trial ................................................................................................................. 26
5.4 Ongoing trials versus usual care (Annexes 6.3.7) ................................................................................ 30 5.4.1 FP7 funded FOCUS trial ................................................................................................................... 30 5.4.2 Kanyini-GAP ..................................................................................................................................... 30 5.4.3 IMPACT ............................................................................................................................................ 30 5.4.4 SPACE Collaboration meta-analysis................................................................................................. 30
6. What is the current “pipeline” of products that are to be used for this particular condition? .................... 31
7. What are the opportunities for research into new pharmaceutical interventions? .................................... 31
8. What are the gaps between current research and potential research issues which could make a difference are affordable and could be carried out in a) five years or b) in the longer term? .......................................... 32
8.1 Need for large-scale trials among people with established cardiovascular disease and other indications for treatment .................................................................................................................................. 32
8.2 What are the effects of implementing a polypill strategy on cardiovascular outcomes? ................... 33
8.3 Potential benefits of next generation polypills .................................................................................... 33 8.3.1 Additional benefits from use of newer agents ................................................................................ 33 8.3.2 How many dose versions for each polypill? .................................................................................... 34 8.3.3 Low dose or high dose polypill components? ................................................................................. 34
8.4 Polypill approach in specific patient populations ................................................................................ 35
8.5 Expanding the polypill concept to acute care ...................................................................................... 35

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-3
9. For which of these gaps are there opportunities for pharmaceutical research? ..................................... 36
10. Conclusion ......................................................................................................................................... 36
11. Declarations ...................................................................................................................................... 38
References ..................................................................................................................................................... 38
Annexes ......................................................................................................................................................... 46
Annex 6.3.1: Mortality and burden of disease from IHD per age group and per region .................................. 47
Annex 6.3.2: Baseline characteristics of previous randomised controlled trials – versus placebo or no treatment .......................................................................................................................................................... 51
Annex 6.3.3: Actual versus expected reductions in systolic blood pressure and LDL-cholesterol in trials of ‘polypills’ versus placebo or no treatment ........................................................................................................ 53
Annex 6.3.4: Baseline characteristics of UMPIRE Trial ..................................................................................... 54
Annex 6.3.5: Ongoing randomised controlled trials – polypill versus usual care .............................................. 55
Annex 6.3.6: Ongoing trials of “hypertension polypills” ................................................................................... 56
Annex 6.3.7: Ongoing trials – polypill versus placebo or no treatment ............................................................ 57
Annex 6.3.8: Pipeline of polypills ...................................................................................................................... 58

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-4
1. Introduction
In 2004 Warren Kaplan and Richard Laing wrote the “Priority Medicines for Europe and the
World Report”.1 In this report they placed great emphasis on the background paper written
by Bruce Neal titled “Secondary Prevention of Cardiovascular Disease: Fixed Dose
Combinations.” (http://archives.who.int/prioritymeds/report/background/cardiovascular.
doc). In the 2004 report Kaplan and Laing stated “The simple solution to this deficiency (in the
effective treatment of patients with proven cardiovascular disease) is to develop and test a fixed-dose
combination (FDC) product of these proven effective medicines. The research agenda proposed in this
section is different to that of the other sections because this approach offers the greatest potential short-
to-medium term impact of all of the possible research activities in this Report.”(Page 58). This
background paper to the 2013 update of the Priority Medicines for Europe and the World
reports on the work that has been done since 2004 making the case that what was proposed
in 2004 has now been undertaken and that the next stage is to undertake large scale pan
European and global clinical trials to understand the place of “polypills” in the treatment of
individuals who have suffered from cardiovascular and/or cerebrovascular events. There
have been two large scale clinical trials funded in this area. One of these studies (the
UMPIRE trial) has since reported positive results as outlined in detail in this background
paper. This report updates the information on this topic.
This report updates the potential information on this topic and therefore continues to focus
on secondary prevention among patients who have already suffered a cardiovascular event.
The majority of such patients have IHD, but a significant minority have cerebrovascular
disease or peripheral vascular disease.
In addition to secondary prevention with the polypill, a number of other pharmacological
approaches to prevention and treatment of IHD will need to be researched in order to
provide more effective, safer and individualized intervention strategies. These include the
development of new lipid-lowering drugs; pharmacological means to address novel
mechanistic concepts of vessel wall damage and protect against conditions such as chronic
inflammation and local angiogenesis; and regenerative medicine/cell therapy approaches.
Similarly, new pharmacological treatment strategies need to be developed for heart failure
and arrhythmias, frequent consequences of IHD.
2. What is the size and nature of the disease burden?
Detailed analysis of overall global trends in burden of disease is available in Chapter 5,
however a summary of disease burden attributable to cardiovascular disease is included
here. Each year about 15.6 million deaths (30% of global mortality) occur from cardiovascular
disease (CVD) making it the leading cause of death.2 Worldwide, ischaemic heart disease
(IHD) is ranked as the leading specific cause of death, with 13.3 % of total deaths, followed
by cerebrovascular disease (11.1%) (Table 6.3.1).Together IHD and all forms of stroke
worldwide killed an estimated 12.9 million people in 2010, a quarter of the global total, an
increase from one in five deaths worldwide 20 years earlier.2

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-5
Following global trends, the largest single cause of death in the 2010 Global Burden of
Disease study in the combined region of Central, Eastern and Western Europe was ischaemic
heart disease (26.6% of all deaths), closely followed by cerebrovascular diseases (ischaemic
and haemorrhagic and other non-ischaemic stroke) with 11.0% of the total number of deaths
(Table 6.3.1).
The most common specific cause of cardiovascular death is IHD which accounts for 45% of
global cardiovascular deaths and 54.6% of European cardiovascular death. Cerebrovascular
diseases account for 37.6% of cardiovascular diseases globally and 31.4% in Europe.
Hypertensive heart disease is the third biggest contributor to this group of diseases with
5.6% of global cardiovascular mortality and 3.7% of the total cardiovascular mortality in
Europe.
Table 6.3.1: DALY and mortality data for the most common cardiovascular diseases, for
the European regions and the world.
Eastern, Western
and Central
Europeb
World Eastern, Western
and Central Europe
World
DALYs % of
total
DALYs % of
total
Mortality
(total
deaths)
% of
total
Mortality
(total
deaths)
% of
total
Ischemic heart
disease 32 928 727 13.8 129 819 898 5.2 2 204 942 26.6 7 029 270 13.3
Cerebrovascular
disease 16 913 463 7.1 102 232 304 4.1 1 269 233 11.0 5 874 182 11.1
Hypertensive heart
disease 1 857 167 0.8 15 324 193 0.6 150 413 1.8 873 152 1.7
Source: Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010
(GBD 2010) Results by Cause 1990-20103 b Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Hungary, Macedonia, the Former Yugoslav Republic of Montenegro, Poland,
Romania, Serbia, Slovakia, Slovenia, Belarus, Estonia, Latvia, Lithuania, Moldova, Russian Federation, Ukraine, Andorra , Austria,
Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Netherlands, Norway,
Portugal, Spain, Sweden, Switzerland, United Kingdom.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-6
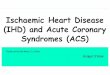
Figure 6.3.1: Distribution of global and European mortality for cardiovascular and
circulatory diseases.
Source: Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010
(GBD 2010) Results by Cause 1990-2010 3 a Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Hungary, Macedonia, the Former Yugoslav Republic of
Montenegro, Poland, Romania, Serbia, Slovakia, Slovenia, Belarus, Estonia, Latvia, Lithuania, Moldova, Russian Federation,
Ukraine, Andorra , Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy,
Luxembourg, Malta, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, United Kingdom.
In addition, cardiovascular disease causes a large non-fatal global disease burden as a
consequence of prevalent disease states such as angina. When the non-fatal disease burden is
taken in conjunction with the healthy life years lost due to premature death the total overall
disease burden attributable to cardiovascular and circulatory diseases accounted for 11.8% of
global DALYs (Disability Adjusted Life Years) in 2010.4 The major diseases within this group
worldwide are, just as with mortality data, ischaemic heart disease (5.2%), cerebrovascular
diseases (4.1%), and hypertensive heart disease (0.6%). In Central, Eastern and Western
Europe, 13.8% of the total DALY burden can be attributed to IHD, 7.1% to cerebrovascular
disease and 0.8% to hypertensive heart disease (Table 6.3.1).
Not only is CVD currently the greatest cause of death and disability worldwide, CVD
mortality is predicted to rise to approximately 23.4 million by 2030 with CVD predicted to
remain the leading cause of death.5 Recent data from the Global Burden of Disease study
2010 confirms the likelihood of reaching these predictions. Cardiovascular diseases and more
specifically ischaemic heart disease increased by 31.2% and 34.9%, respectively, in terms of
absolute deaths in the past two decades. In terms of years of life lost (YLLs), ischaemic heart
disease increased in rank from fourth in 1990 to first in 2010, reflecting an increase of 28%.
Cerebrovascular disease is currently ranked third globally for YLLs, but in some Asian
regions is ranked first. Ischaemic heart disease is ranked first in almost all regions other than
Asia. In addition, from 1990 to 2010, both ischaemic heart disease (IHD) and cerebrovascular
disease have risen in their position amongst the top 10 causes of DALYs – IHD from position
number four to number one and stroke from position number five to number three,
reflecting increases of 29% and 19% respectively.4 In Europe, ischaemic heart disease and
54.6%
31.4%
3.7% 6.9% 2.3% 1.1%
Central, Eastern and Western Europea
45.0%
37.6%
5.6%
7.0%
2.6% 2.2%
World
Ischemic heart disease
cerebrovascular disease(stroke)Hypertensive heartdiseaseOther cardiovascularand circulatory diseasesCardiomyopathy andmyocarditisRheumatic heartdisease

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-7
stroke have maintained their ranking as the leading and second most common causes of
death and YLLs over the past 20 years. In central and eastern Europe they have maintained
their respective highest and second highest rankings for DALYs also, however in western
Europe, low back pain has now emerged as the foremost cause for DALYs in that region.
IHD and stroke come in at numbers two and three.3
Figure 6.3.2 shows the amount of absolute disability-adjusted life years (DALYs) caused by
ischaemic heart disease (IHD) by age group for the world, Central, Eastern and Western
Europe. The highest burden of disease from ischaemic heart disease, amongst the three
European regions, is present in Eastern Europe in all age groups, followed by Western
Europe. The amount of DALYs caused by ischaemic heart disease peaks at 80 years and
above in all four regions.
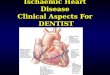
Figure 6.3.3: Absolute deaths caused by ischaemic heart disease by age group and region
demonstrates the mortality rates for ischaemic heart disease, in absolute death numbers, by
age group and region.3 As with the DALYs, Eastern Europe has the highest number of deaths
from ischaemic heart disease amongst the European regions in all age groups, except for in
the over 80 years age group, where Western Europe has slightly higher numbers of deaths
due to IHD. This is remarkable since Western Europe has approximately half the number of
deaths in the other age groups, compared to Eastern Europe. Furthermore, it’s striking that
Central Europe has less than half the number of deaths due to IHD than Eastern Europe or
Western Europe.
More figures for mortality and burden of disease from IHD per region and age group can be
found in the annexes of this background paper.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-8
Figure 6.3.2: Absolute DALYs caused by ischaemic heart disease by age group and region.3
Source: Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010 (GBD
2010) Results by Cause 1990-2010
Figure 6.3.3: Absolute deaths caused by ischaemic heart disease by age group and region.3
Source: Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010
(GBD 2010) Results by Cause 1990-2010

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-9
Common interests between Europe and the world
Despite the common misperception that CVD is a ‘rich man’s disease’, 80% of CVD deaths
occur in low- or middle-income countries (LMIC).6 These deaths in LMICs are not only
occurring more frequently than in high income countries but are also occurring earlier in life
causing a greater social and economic impact in these countries. Many of these countries
typically are least equipped to deal with this epidemic of CVD due to inadequate health care
systems and significant levels of poverty.
The commonality between high income countries and low income countries of risk factors
responsible for the identical leading causes of death ensures that any solutions that are found
have the potential (within the bounds of adaptation to local conditions) to advantage a broad
range of countries across the economic spectrum. Any intervention that has the capacity to
affect significant public good in Europe can be applied globally in many different settings.
This well documented epidemic of CVD is due to two main factors – ageing of the world’s
population, and epidemiological transition in LMIC leading to global exposure to the key
risk factors for CVD.7
Population Ageing
Chapter 5 provides significant detail on global ageing and will not be repeated here. Figures
5.1 and 5.2 in particular show the predicted ageing of the population globally and
particularly in the European Region. Such increases in life expectancy, although showing
global ‘successes’ in modernization and improvements in standards of living and health care,
mean that more people are living to an age where they are more likely to have a
cardiovascular event and if they survive that event, live longer with the disability associated
with that event.
Risk Factors
Risk factors associated with CVD are well established through multiple large
epidemiological studies which show that CVD is overwhelming preventable.8,9 Fifty-seven
per cent of CVD deaths (19% of global deaths) can be attributed to just eight risk factors
associated with poor diet and low rates of physical activity: high blood pressure, high blood
glucose, physical inactivity, being overweight or obese, high cholesterol and low fruit and
vegetable intake.10 The other key risk factor is tobacco use which accounts for nearly 10% of
CVD.10 The 2010 Global Burden of Disease study reported that the two leading risk factors
for global disease burden overall were high blood pressure (9.4 million deaths and 7% of
global DALYs) and tobacco smoking including second-hand smoke (6.3 million deaths and
6.3% DALYs) both of which are key factors in increasing risk of CVD. The leading risk factor
for Europe was also high blood pressure with smoking ranked either second or third
(depending on the region of Europe). Detailed proportions of global IHD DALYs attributable
to individual risk factors are presented in Table 6.3.2: Proportion of ischaemic heart disease
DALYs attributable to individual risk factors, worldwide, 201011 These risk factors are all
similarly implicated in other atherosclerotic disease such as stroke.
Of note is the high proportion of IHD DALYs attributable to excessive alcohol use. Although
significant, excessive alcohol use and the consequent disease states, treatment options and
recommendations for further research are covered in detail in Chapter 6.14: Alcohol use

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-10
disorders and alcoholic liver disease and the accompanying background paper. Hence, this
will not be addressed in this background paper.
Table 6.3.2: Proportion of ischaemic heart disease DALYs attributable to individual risk
factors, worldwide, 2010.
Disability adjusted life-years (%)
Physiological risk factors
High blood pressure 53%
High total cholesterol 29%
High body-mass index 23%
High fasting plasma glucose 16%
Alcohol use 33%
Tobacco smoking including second-hand
smoke
31%
Dietary risk factors and physical inactivity
Diet low in nuts and seeds 40%
Physical inactivity and low physical
activity
31%
Diet low in fruits 30%
Diet low in seafood omega-3 fatty acids 22%
Diet low in whole grains 17%
Diet high in sodium 17%
Diet high in processed meat 13%
Diet low in vegetables 12%
Diet low in fibre 11%
Diet low in polyunsaturated fatty acids 9%
Diet high in trans fatty acids 9%
Diet high in sugar-sweetened beverages 2%
Air pollution
Ambient particulate matter pollution 22%
Household air pollution from solid fuels 18%
Other environmental risks
Lead exposure 4%
Source: Lim SS et al. Lancet, 201211
Summary:
From the previously presented data, it is immediately apparent that CVD must be a priority
for any attempt to reduce burden of disease at a global level and within Europe. The
potential for public health benefit from the development of new or improved medical
interventions to address the pandemic of CVD is incontrovertible. Not only would this have
a major impact on Europe but would also potentially improve the lives of millions of patients
in LMIC as well. The most significant contributors to IHD (and via extrapolation of other
CVD) DALYs are amenable to pharmacological intervention i.e. the physiological risk factors
and tobacco smoking. Despite much progress in the development of pharmaceutical

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-11
interventions to prevent CVD, there is significant opportunity to further invest in this area,
as will be described in the remainder of this background paper.
3. What is the control strategy?
Recommended strategies for prevention of CVD (both primary and secondary) can be
categorized into lifestyle versus pharmacological interventions. Most attention in this
chapter will focus on pharmaceutical interventions.
3.1 Lifestyle intervention
Since most of the major risk factors for CVD are related to lifestyle; advocacy and promotion
at the population and patient level to modify poor lifestyle choices will always be an
important and critical method to reduce the burden of CVD. When adhered to by patients
not only is it cost-effective but will always be more effective that simply directly
recommending pharmaceutical therapy. Smoking cessation has been shown to significantly
decrease the smoking-attributable risk of disease and CVD risk return to that of a non-
smoker within about five years.12,13 Intuitively, modification of diet and activity levels will
positively benefit an individual’s cardiovascular risk factor profile. Physical activity and
dietary modification have not only been shown to have a significant favourable effect on
other major risk factors (including lipids, blood pressure and insulin resistance) but also to
have an independent role in prevention of cardiovascular disease.14,15,16,17,18 Taken in
conjunction, data has shown that adherence to lifestyles guidelines advocating moderate
physical activity, cardio-protective diet and abstinence from smoking can reduce the
incidence of cardiovascular disease by more than 80% compared to the rest of the
population. However, studies have shown that the general population nor (more
surprisingly) people with established CVD typically adhere to these recommended
guidelines. Recent data from the United States NHANES 2005 to 2010 study 19 showed that
22.6% of respondents were current smokers and 24.1% were former smokers. Thirty-two per
cent did not engage in any physical activity with a further 23% only engaging in
intermediate activity (better but still not reaching the ideal level of activity). A total of 77.7%
of people surveyed scored less than two out of out on a healthy diet score that included
consumption of fruit and vegetables, wholegrains, and fish, and limiting sugar and salt
intake. These figures have not changed significantly since previous NHANES surveys.19
It is not only the general population who are failing to follow lifestyle advice. The European
Action on Secondary and Primary Prevention by Intervention to Reduce Events
(EUROASPIRE) studies have completed three surveys on lifestyle and risk factor
management in patients with coronary heart disease (CHD).20,21,22 Each study recruited
consecutive patients with first or recurrent diagnosis or treatment for CHD across multiple
hospitals in nine to 22 countries and interviewed between six months and three years later to
see how many were adhering to recommended lifestyle and treatment measures. Arguably
this population should be the most motivated to apply and adhere to lifestyle guidelines,
having already experienced CVD and being at high risk of a recurrent event. In the latest
round of surveys in 2006 to 2007, the investigators found that 51.9% of smoking patients
persisted after their event and only 51.8% of obese patients had followed dietary

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-12
recommendations to lose weight, with only 38.2% of obese patients increasing their regular
physical activity.22 Of the overall cohort, only 48% increased their overall physical activity.
An impressive 92% of the cohort attempted to change their diet however this subjective
reporting is undermined by the objective measures of obesity (35.3%) and central obesity
(52.7%). Many of these high risk patients were not taking medicines that have been proven to
prevent reoccurrence of cardiac events.
The EUROASPIRE investigators also compared the results of the three different surveys to
see if any improvements had been made over time.23 Disappointingly, between the first and
third surveys rates of smoking in younger female patients increased (despite an overall
decrease in smoking) and prevalence of obesity increased by 13%. Raised blood pressure
increased by 3.4% and reporting of diabetes mellitus increased by 9.3%. Full prevalence data
for coronary heart disease risk factors in EUROASPIRE III are shown in Table 6.3.3:
Prevalence (%) of coronary heart disease risk factors in EUROASPIRE III, by country, age
and diagnostic category22
Table 6.3.3: Prevalence (%) of coronary heart disease risk factors in EUROASPIRE III, by
country, age and diagnostic category.
Source: Kotseva K et al. Eur J Cardiovasc Prev Rehabil, 200922

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-13
These data indicate that, despite public awareness campaigns and educational efforts,
population based lifestyle change is not happening. Into this evidence-practice gap fits the
opportunity for modification of CVD risk with pharmacological management. The role of
cholesterol lowering therapy, blood pressure lowering therapy and anti-platelet therapy is
now incontrovertible having been proven effective in large meta-analyses in all three
medication categories.
3.2 Lipid-lowering therapy
The role of lipids as a major risk factor for cardiovascular disease has been well established
and has been estimated to cause approximately a third of global ischaemic heart disease.24
Furthermore, the relationship between serum cholesterol and the risk of cardiovascular
disease has been shown to be continuous 25,26 with no defined level below which a person can
be considered to be at ‘low risk’. The discovery of the 3-hydroxy-3-methylglutaryl coenzyme
A (HMG-CoA) reductase inhibitors (statins) has dramatically impacted the treatment of
cardiovascular risk. Ongoing individual patient data meta-analyses by the Cholesterol
Treatment Trialists (CTT) Collaboration of large scale clinical trials of statins have shown
with standard statin regimes a consistent reduction in major vascular events over five years
of around 20% per 1 mmol/L decrease in LDL regardless of baseline lipid levels or other
patient characteristics.27 This benefit is seen even in those at lowest baseline risk with
demonstrated reduction in events greatly exceeding any known hazard of statin therapy.28
This raises the possibility that indications for treatment, which are currently aimed at
patients at high risk should possibly be widened to include those at 5 to 10% absolute
cardiovascular risk over five years.28 No level has been demonstrated below which reduction
in LDL produces an increase in adverse events, demonstrating an acceptable safety profile
for intensive treatment regimes capable of further LDL reductions.29
The observed benefit from statins improves with the length of time taken with only a 10%
decrease in events seen in the first year but up to 28% reduction in events by the third or
fourth year. These estimates of benefit are in fact likely to be an underestimate of the true
effect of long term benefit from statin therapy due to the problem of long term non-
adherence by patients. Full compliance would achieve larger overall reductions in LDL, up
to 1.5 – 1.8 mmol/L predicted in some cases 30,31 which would result in closer to a one third
reduction in vascular events overall.27
In addition to statins’ role in reducing LDL cholesterol, fibrates (agonists of the peroxisome
proliferator receptors selective for the α receptors - PPAR) have a clear role in raising HDL
cholesterol and reducing triglyceride concentrations 32 and consequently have recently been
shown in meta-analysis to be effective in reducing cardiovascular events in their own right
primarily by preventing coronary events.33 The relative risk reductions shown for fibrates
(10% for major cardiovascular events, 13% for coronary events, no effect on stroke) are much
less than for statins, however offer the potential for additive effects in risk reduction due to
targeting of different cholesterol sub fractions and hence addressing the ‘residual risk’
remaining after treatment with statins particularly those patients with combined
dyslipidemia. Despite this, the potential for increased risk of side effects, in particular muscle
damage (myopathy) when taken together with statins has somewhat limited concurrent use
of these drugs together, in particular gemfibrozil.34

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-14
Ezetimibe is a newer lipid-lowering agent which inhibits cholesterol absorption from the gut
available as monotherapy as well as combination therapy with simvastatin. Although shown
to be effective in significantly lowering LDL cholesterol (including an extra 12 to 19% when
coadministered with a statin35,36), there is still controversy about its use with three separate
trials showing paradoxical results in effect on carotid-artery intima-media thickness and also
superficial femoral artery atherosclerosis.37,38,39 Results from the ongoing IMPROVE-IT trial
(http://clinicaltrials.gov/show/NCT00202878) are required to determine the true value of
ezetimibe in CVD prevention.
Two other products of note are niacin and omega-3 fatty acids. Despite marketing approval
for nicotinic acid/laropiprant (niacin) being granted in 2008 by the European Medicines
Agency to treat adults with dyslipidemia, this approval was suspended in January, 2013 40
following the preliminary reporting of the HPS2-THRIVE study’s
(http://www.thrivestudy.org/) primary outcome and safety data which showed no
advantage of niacin in addition to statins on the outcome of CVD events and an increase in
non-fatal but serious side effects. Omega-3 fatty acids have received widespread publicity
and now represent a multi-million dollar industry due to positive findings in prevention of
CVD in early trials. Later trials however produced conflicting results. A recent systematic
review and meta-analysis 41 did find a significant effect of omega-3 fatty acids on vascular
death (RR 0.86, 0.75-0.99) however no significant effect on all other outcomes studied (it was
noted that there was significant heterogeneity between the trials which may have impacted
the overall results). The authors concluded that although there does seem to be a positive
effect on some cardiovascular outcomes, perhaps the public and physician’s expectations of
the true benefit should be lowered somewhat.
3.3 Blood pressure lowering therapy
Suboptimal blood pressure (systolic >115 mmHg) has been estimated to account for about
62% of global cerebrovascular disease and 49% of ischaemic heart disease globally.42 The
majority of adult blood pressures are this category, and only about half of the attributable
burden occurs among those with ‘hypertension’. This is true for both developing and
developed countries although in developed regions blood pressure levels are particularly
high.11 Major prospective observational studies have shown conclusively that blood pressure
(both diastolic and systolic) has a continuous, independent relationship with the risk of
cardiovascular disease.43,44,45
Evidence for the effectiveness of blood pressure lowering therapies 43,46,47 has led to a plethora
of such drugs in multiple classes. All commonly used regimens (including ACE inhibitors,
calcium channel antagonists, diuretics and beta blockers) have been shown to reduce
cardiovascular risk similarly with larger reductions in blood pressure producing larger
reductions in risk.46 As is the case for cholesterol lowering, an approximately consistent
proportional difference in CV risk (35 to 40% for stroke and 20 to 25% coronary heart
disease) is associated with each given absolute reduction in blood pressure (5-6 mmHg of
diastolic blood pressure) regardless of the BP at baseline.43 It follows then that if the size of
the absolute risk reduction is related to baseline untreated risk, then the greatest risk
reductions occur in those whose baseline risk is highest.47 In Europe, although no particular
medication class is recommended for treatment of uncomplicated high blood pressure,
certain classes have been recommended in certain clinical conditions (Table 6.3.4) 48 and new
guidelines are in development.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-15
Table 6.3.4: Position statement: Antihypertensive treatment: Preferred drugs. European
Society of Hypertension and European Society of Cardiology.
Subclinical organ damage Preferred drugs
LVH ACEI, CA, ARB
Asymptomatic atherosclerosis CA, ACEI
Microalbuminuria ACEI, ARB
Renal dysfunction ACEI, ARB
Clinical event
Previous stroke any BP lowering agent
Previous MI BB, ACEI, ARB
Angina pectoris BB, CA
Heart failure diuretics, BB, ACEI, ARB, anti-
aldosterone agents
Atrial fibrillation
Recurrent ARB, ACEI
Permanent BB, non-dihydropiridine CA
ESRD/proteinuria ACEI, ARB, loop diuretics
Peripheral artery disease CA
Condition
ISH (elderly) diuretics, CA
Metabolic syndrome ACEI, ARB, CA
Diabetes mellitus ACEI, ARB
Pregnancy CA, methyldopa, BB
Blacks diuretics, CA Abbreviations: LVH: left ventricular hypertrophy; ISH: isolated systolic hypertension; ESRD: renal failure;
ACEI: ACE inhibitors; ARB: angiotensin receptor antagonists; CA: calcium antagonists; BB: β-blockers
Source: Mancia G, et al. J Hypertens, 2009 49
Combination therapy for lowering blood pressure
Hypertension management strategies, such as those endorsed by most practice guidelines
including the European Society of Hypertension 49 have traditionally focussed on “tailored
therapy” and “stepped-care” approaches. These tend to be time consuming for doctor and
patient, only cautiously recognise that contemporary BP targets almost always necessitate
additional medication and ignore the auto-regulatory mechanisms that limit responsiveness
to a single drug administered alone.
3.3.1 Evidence on potential benefits of regimen simplification and use of two-
drug combination pills
Most patients with hypertension require BP lowering medication from two or more classes to
achieve adequate control.50 The need for titration of medication and addition of multiple
classes of drug requires multiple physician visits and this in itself triggers poor adherence to
prescribed medication and poor attendance at scheduled visits.51 The requirement to take
multiple medications in complex regimes also results in poor adherence.52 For physicians, the
need for repeated up-titrating or adding extra medications can lead to inertia and complicit

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-16
acceptance of inadequate BP control.53,54 Dual combination BP lowering medication has been
shown to improve achieved BP reductions as well as cardiovascular event rates.55 Initiating
anti-hypertensive treatment with dual combination therapy not only accelerates the time
taken to achieve control but also attains a lower final target.56,57 For the patient, improved
adherence has also been demonstrated without adversely affecting the side effect profile.58 59
Further benefits in BP control are also available via simplifying up-titration regimes.57
3.3.2 Evidence on hypertension combination pills containing more than two
medications
There are sound pharmacological principles to expect the maximum benefit to side effect
ratio from low-dose triple combinations.59,60,61 In short, benefits of each component are
additive, and low doses typically avoid most side effects while achieving most blood
pressure reduction. Thus for example, three half-dose medications would typically lower
blood pressure about as much as two full-dose medications, but with fewer side effects.59
A number of important questions however remain to be answered. The triple BP lowering
pills that have recently become available in western countries, have focussed exclusively on
severe hypertension that remains uncontrolled with full dose dual combination therapy.
Furthermore, previous trials have been within the mode of traditional stepped care, and
have not tested the integration of a low-dose triple combination within a simplified regimen.
For example, the recent trial of Exforge® 62 involved patients with baseline BP of 170⁄107
mmHg, randomised to receive five weeks of treatment with amlodipine ⁄valsartan ⁄HCTZ 10
⁄320 ⁄25 mg or one of the three dual therapies indicated previously herein. Perhaps
unsurprisingly, this trial showed that patients on triple therapy achieved better BP
reductions than patients on dual combination therapy.
To date no clinical trial has tested the benefits or cost-effectiveness of combination therapy
with three, low dose BP lowering drugs in hypertension. One such trial, the TRIUMPH
(TRIple Pill versus Usual care Management for Patients with mild-to-moderate
Hypertension) study
(https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=363169), a 700 patient
randomised controlled trial of a triple low dose blood pressure lowering pill versus usual
care is currently starting up in India with the aim of answering these questions.
3.4 Anti-platelet therapy
A meta-analysis by the Antithrombotic Trialists’ Collaboration in 2002 63 showed that use of
antiplatelet agents (primarily aspirin) in patients at high risk due to a pre-existing occlusion
or predisposing condition, decreased the occurrence of serious vascular events by one
quarter, with a third reduction in non-fatal myocardial infarction (MI) and a quarter
reduction in non-fatal stroke. Vascular mortality overall was decreased by one sixth. They
concluded that the absolute benefits of antiplatelet therapy substantially outweighed the
absolute risks of major extra-cranial bleeding in patients with vascular disease. The balance
of benefits and risks is less clear in lower risk populations, and conclusions have been
hampered by not recognising the heterogeneity of this “primary prevention” population. A
more detailed meta-analysis by the Antithrombotic Trialists’ Collaboration stratified results
by estimated cardiovascular risk, and showed that even in medium risk population the
number of excess haemorrhagic events (mostly gastrointestinal) was broadly similar to the

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-17
number of major vascular events prevented.64 However, further modelling and research is
required to determine appropriate patient populations, given the emerging evidence
showing that aspirin reduces the risk of several major cancers,65 and the changing
background rates of gastrointestinal haemorrhage and vascular events.
Clopidogrel is the next most commonly used anti-platelet agent, and has similar efficacy to
aspirin.63 Clopidogrel confers additional benefit when added to aspirin treatment in ST
elevation myocardial infarction (RRR 9%, 3-14) 66, non-ST elevation myocardial infarction
(RRR 20%, 10 – 28) 67 and long-term following percutaneous coronary intervention (RRR
26.9%, 3.9-44.4).68 Prior to coming off patent in May 2012, opinions varied as to the cost-
effectiveness of clopidogrel compared to aspirin,69,70 and LMIC cost almost certainly would
have limited its use significantly. However, now that generic clopidogrel is becoming
available, its use in prevention of CVD is likely to increase.
4. Why does the disease burden persist?
4.1 Non-optimal use of existing effective medications
Despite large-scale clinical trial/meta-analyses having demonstrated substantial reductions
in the risks of cardiovascular events with antiplatelet,63 blood pressure lowering 46 and
cholesterol lowering therapy 71 in patients with established CVD and those at high calculated
risk of CVD current treatment gaps among this patient group are very large. Despite the
majority of people with established CVD in high income countries being started on
recommended medications, significant numbers of people in high income countries 23,72,73
and even larger numbers in low and lower middle income countries do not either receive or
remain adherent to these treatments long-term.74,75,76 (Figure 6.3.4)
Within Europe, the EUROASPIRE III study22 showed that the majority of coronary patients
that required BP lowering and lipid lowering medications were not receiving them on a
long-term basis and if patients were receiving them, they were not reaching their BP and
lipid targets (Table 6.3.5) suggesting either poor adherence by the patient or insufficient
titration by physicians.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-18
Figure 6.3.4: PURE study: Number of drugs taken by individuals with established
cardiovascular or cerebrovascular disease by country economic status.
Source: Yusuf S, et al. Lancet. 2011 For coronary heart disease (A), drugs counted were aspirin, β blockers, ACE inhibitors or ARBs, or
statins. For stroke (B), drugs counted were aspirin, statins, ACE inhibitors or ARBs, or other blood-
pressure-lowering drugs (e.g., β blockers, diuretics, and calcium-channel blockers). ACE=angiotensin-
converting enzyme. ARB=angiotensin-receptor blocker.76
Table 6.3.5: Percentage of patients reaching BP and lipid targets in EUROASPIRE III
Reaching Target (%)
On BP lowering medication 43.9
Not on BP lowering medication 48.3
On lipid lowering medication 55.0
Not on lipid lowering medication 25.4
Source: Kotseva K et al. Eur J Cardiovasc Prev Rehabil, 200922
Various factors may underlie the suboptimal treatment of high risk patients, such as the need
to navigate complex guidelines by doctors, low continuation rates by patients, inequities in
health care and resistance to costs by both doctors and patients.
Non-adherence to therapy is one of the main obstacles for the unsatisfactory reduction of risk
factors, particularly in developed countries. It is characterized by the premature cessation of
treatment together with suboptimal use of medication, and is correlated with an increased
risk of mortality.77 Non-adherence is especially relevant in chronic, asymptomatic diseases as
cessation of treatment does not lead to symptoms in patients but they remain at high risk of
serious micro- and macrovascular complications in the case of atherosclerotic cardiovascular
diseases. Patients often do not understand the importance of taking long-term medication for
chronic diseases, particularly those that are generally symptom-free. Reported long-term
adherence is low with only 70% adherence to aspirin therapy and only 45% to lipid- and BP-

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-19
lowering therapy after 12 months.78 The main determinants of non-adherence are multiple
medications with complex dosing regimens, inadequate knowledge about the medications
and cost.79,80,81,82,83 Increasing age, established cardiovascular disease and/or type 2 diabetes
usually indicate the usage of more than five drugs per day (polypharmacy).84 Treating high
risk patients often requires polypharmacy even though this is known to be associated with
patients’ non-adherence, inadequate prescription of medication by doctors and drug
interactions. Therefore the complexity of the prevention of cardiovascular diseases requires
simplicity.
The lack of affordability of therapy largely affects treatment gaps in developing countries
since in developing countries most healthcare services are paid for out-of-pocket with little
or no subsidy through health insurance or the government. The economic burden of
secondary prevention of cardiovascular diseases is enormous, especially among the rural
and urban citizens. As a month’s treatment costs ranges from 1 to 18 days’ wages of
government workers, preventive drugs are unaffordable for the majority of individuals in
developing countries.85,86 Patients can delay or omit drug doses and not fill prescriptions as
strategies for cost reduction. Though the efficacy of preventive strategies may be proven and
recognized at a high level, supply and access at the population level remains the major
challenge.
Practical and affordable approaches to closing these treatment gaps are required.
Combination pills or ‘polypills’ may play a role in closing these treatment gaps in ischaemic
and cerebrovascular disease, and their use has been advocated for almost a decade.87,88,89
Reducing the complexity, number and costs of medication regimens with a ‘polypill’
containing off patent generic medicines will potentially improve adherence and hence
reduce cardiovascular events.
4.2 New innovative therapies
Further research into new, innovative therapies for the prevention and treatment of CVD is
ongoing particularly amongst the larger pharmaceutical companies. Advancements in the
knowledge of the pathophysiology and underlying determinants of the various types of
CVD (including advances in genomics and targeted population groups) are constantly
opening up new lines of enquiry into the possibility for a newer drug that may perhaps
target a more specific mechanism or a targeted clinical population which, when added to the
currently available medication options, may offer increased prevention or treatment for
CVD. There is clearly a need for development of new medication types as even if all of the
previously mentioned available therapies are utilized maximally, patients still have a
residual risk of CVD. The reality though is that development of a new drug costs well over a
billion US dollars. This scope of research is well outside any publically funded research
scheme and therefore will not be addressed in this background paper. Although new
innovative therapies are potentially worthwhile, the most cost-effective measure for
preventing CVD currently is improving access and adherence to currently available, generic
medications.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-20
5. What can be learnt from past/current research into
pharmaceutical interventions for this condition?
Research over the last half century involving hundreds of thousands of patients in clinical
trials has provided an enormous body of evidence on the efficacy and safety of different
blood pressure lowering, statin and antiplatelet agents in the control of cardiovascular
disease.88,89 The large majority of these trials were designed to assess the effects of individual
medicines given the understandable clinical, regulatory and commercial requirements to
assess the benefits and risks of specific drugs before access and uptake in the market. Hence
trials typically involved randomization of a single agent versus placebo, on top of a
background of usual care treatments at that time. Systematic reviews of these trials reveal an
overall finding of broad relevance to clinical and public health practice, and to development
of polypills: an approximate constancy of relative risk reduction (i.e. lack of interaction or
effect modification) of each modality (BP lowering, cholesterol lowering and anti-platelet
effect), irrespective of whether the other modality is present or absent.31,90,91 More specifically,
these systematic reviews of clinical trials have shown that proportional reductions in cause-
specific outcomes (such as CVD mortality) are closely similar across a wide range of patient
populations, with no major differences between agents (after accounting for the extent of risk
factor reduction for SBP and LDL) and even when event rates vary tenfold or more.For
example, aspirin produces a one-fifth reduction in CHD and ischaemic stroke risk in
‘primary’ and ‘secondary’ prevention, even though event rates differ by an order of
magnitude. There is clear evidence that the proportional reductions in major outcomes
achieved with each treatment modality are approximately the same in the presence or
absence of other interventions and across a range of risk factor levels which is expected given
the lack of interaction between treatments in terms of risk factor reduction and the
epidemiology of blood pressure and cholesterol joint effects– this is outlined in Figures 6.3.5
and 6.3.6.
Given this consistency in proportional reductions, it is an expectation that combination
therapy will have beneficial effects. More specifically, the combined effects are best estimated
by multiplying relative risks together, after adjusting for the size of SBP and LDL-cholesterol
reductions.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-21
Figure 6.3.5: Reduction in vascular events with a statin in the Heart Protection Study92 and
reduction in stroke events with blood pressure lowering in the PROGRESS study93 by
concomitant treatments and other factors
Source: Heart Protection Study Collaborative Group. Lancet, 2002
Progress Collaborative Group. Lancet, 2001
Figure 6.3.6: Reduction of serious vascular events with aspirin, by blood pressure and
cholesterol levels
Source: Baigent C et al. Lancet, 2009 90

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-22
The concept of combining multiple classes of cardiovascular medications into a single pill
also has a long history – for example, the term “asp-olol” was coined for an aspirin and
atenolol combination in the 1970’s. Patents claiming rights over combinations of various
cardiovascular medications had been filed since the late 1990s (for example 94,95,96). The first
major scientific meeting on the concept of a fixed dose combination pill for CVD prevention
was held in 2001, when the World Health Organization and the Wellcome Trust convened a
meeting of experts to discuss evidence-based and affordable interventions for non-
communicable diseases.87 A major impetus for the meeting was the potential for fixed-dose
combination pills containing aspirin, statin, and BP-lowering agents, noting ‘the use of a single
pill could well encourage patients to adhere to treatment as well as seriously reduce the cost of the
drugs’. In the medical literature, the concept of a fixed-dosed combination pill was discussed
by Yusuf in a Lancet editorial in 2002 88 and effectiveness and cost-effectiveness analyses
were conducted in the 2002 World Health Report.97 The term ‘polypill’ itself was introduced
with the publication of the Wald and Law’s seminal paper in 2003.89 Wald and Law
estimated that the use of a single pill (containing aspirin, a statin, three BP-lowering drugs,
and folic acid) in all people aged over 55 years would reduce cardiovascular disease by more
than 80%.
Over the ensuing decade several clinical trials in the area of fixed dose combination pills
have been conducted. These trials can be broadly grouped into two main areas:
- Comparisons of polypill versus usual care - in patient populations with established
indications for all the component medications e.g. previous coronary disease
- Comparisons of polypill versus placebo/no treatment - in patient populations with
established indications for none of the component medications e.g. those without
hypertension, dyslipidaemia or vascular disease but who are nonetheless at raised
cardiovascular risk
The 2004 Priority Medicines for Europe and the World Report1 and its recommendation to
prioritize research into fixed dose combinations for the secondary prevention of CVD led to
the European Commission funding of the largest Request for Proposal in this area, and hence
two of the largest polypill trials: the Use of a Multidrug Pill In Reducing cardiovascular
Events (UMPIRE) trial 98 and the Fixed Dose Combination Drug for secondary
Cardiovascular prevention (FOCUS) trial 99 and these will be discussed following a review of
other trials. While many of the patients involved in these trials suffered from IHD, some of
the patients included were suffering from cerebrovascular disease.
5.1 Previous trials – polypill versus placebo or no treatment
These trials are summarized in Annex 6.3.2 and main outcomes in Annex 6.3.3.
5.1.1 Summary of TIPS 1 and 2
The Indian Polycap Study (TIPS)100 was a randomised, partial factorial design trial of
Polycap® versus eight other medication combinations including aspirin alone, simvastatin
alone and different combinations of hydrochlorothiazide, ramipril, and atenolol (see
reference 100) for details of various combinations). Over two-thousand participants with at
least one risk factor for CVD (such as hypertension, diabetes, current smoker, raised lipids or
raised waist: hip ratio) were randomly allocated to one of the nine groups and followed up
for 12 weeks. Outcomes included effect on blood pressure, heart rate, lipids and urine

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-23
thromboxane B2 as well as safety and tolerability. The study showed that the BP lowering
effect of the Polycap® was comparable to the additive effects of each of the three component
BP lowering drugs. A lesser effect on LDL cholesterol than simvastatin alone was noted (0.13
mmol/L) which was significant. Mean changes in blood pressure and LDL are shown in
Figure 6.3.7 below.
Figure 6.3.7: Mean changes in blood pressure and LDL in the TIPS study
Source: The Indian Polycap Study (TIPS). Lancet, 2009
Error bars indicate 95% CI. Mean changes from baseline in the nine groups in the TIPS trial, and the
effects of no blood-pressure-lowering drugs (As, S), one blood-pressure-lowering drug (T), two blood-
pressure-lowering drugs (T+R, T+At, or R+At), or three blood-pressure-lowering drugs (T+R+At,
T+R+At+S), or the Polycap (P)
5.1.2 Summary of Wald and Law trial
Wald and Law 101 conducted a randomised, double-blind, cross-over trial of the polypill
studied containing three half-dose BP lowering medications and a statin in 86 participants
over the age of 50 with no history of CVD. Each participant took placebo or polypill for 12
weeks sequentially. Mean systolic blood pressure was reduced by 17.9 mmHg (95% CI, 15.7–
20.1) on a polypill, diastolic blood pressure by 9.8 mmHg (8.1–11.5), and LDL cholesterol by
1.4 mmol/L (1.2–1.6), reductions of 12%, 11%, and 39% respectively (Figure 6.3.8). These
results were almost identical to those predicted from previous trials of individual
components. This trial is in effect a large Phase 1 study of the polypills efficacy in patients
without cardiovascular disease.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-24
Figure 6.3.8: Observed and expected reduction of blood pressure and LDL-cholesterol in a
2x12 week crossover trial. 101
Source: Wald DS, et al. PLoS ONE, 2012
5.1.3 PILL Collaborative Group
The Pill Pilot study 102 was a randomised, double-blind placebo-controlled trial of a polypill
(containing aspirin 75 mg, lisinopril 10 mg, hydrochlorothiazide 12.5 mg and simvastatin 20
mg) in 378 individuals without an indication for any component of the polypill, but who had
an estimated five year cardiovascular disease risk over 7.5%. Over 12 weeks, polypill
treatment reduced SBP by 9.9 (95% CI: 7.7 to 12.1) mmHg and LDL-cholesterol by 0.8 (95%
CI 0.6 to 0.9) mmol/L.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-25
Figure 6.3.9: Change in BP and LDL cholesterol at 12 weeks in the Pill Pilot study.
Source: Pill Collaborative Group, Rodgers A, et al. PloS one, 2011.
5.1.4 Other trials
Two other trials have been conducted however have significant issues associated with them
meaning that their results must be interpreted very cautiously.
Malekzadeh et al 103 conducted a double-blind randomized, placebo controlled trial in Iran in
475 participants over 50 years without CVD. They found a small but significant different in
SBP at 12 months (4.5/1.6 mmHg) as well as LDL cholesterol (0.46 mol/L) however a
significant difference of 6 mmHg of SBP at baseline between the two groups infers failure of
the randomization process. Furthermore, the less than expected effects of the polypill on
their outcomes raises concern about the reliability of reported compliance with medication.
Soliman et al 104 reported on an open-label, randomized controlled trial of a polypill versus
usual care in 216 patients without CVD. No significant difference was found in SBP or total
cholesterol after three months which was presumed by the authors to be due to the usual
care arm receiving a higher than usual standard of care during the trial than would occur in
usual practice. Further, larger than expected reductions in risk factors (e.g. for SBP a decrease
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
0 2 4 6 8 10 12
LDL
(mm
ol/
L)
Follow-up (weeks)
0
20
40
60
80
100
120
140
160
0 2 4 6 8 10 12
Bloo
d pr
essu
re (m
mH
g)
Follow-up (weeks)
ΔLDL-cholesterol 0.8 mmol/L (0.6-0.9)
ΔSBP 9.9 mmHg (7.1-12.1)
ΔDBP 5.3 mmHg (3.3-6.7)

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-26
of 28.8 mmHg versus 26.9 mmHg in usual care) also raised concerns about standardization
of measurement of risk factors.
For the above mentioned reasons, these two studies are not generally considered to be
reliable representations of the true effect of polypill care.
5.1.5 Conclusions from previous trials of polypill versus placebo or no treatment
The key conclusions from the previous trials of polypill versus placebo/no treatment are that
short term risk factor reductions are of approximately the size expected from individual
agents, after taking into account loss to follow-up and non-adherence. The size of the
underestimation due to loss to follow-up and non-adherence was very small in some trials
(Wald et al, Pill Collaborative Group) and very large in others (Iranian Trial, Sri Lanka trial),
with consequent differences in the observed to expected risk factor reductions. The trials
provided relatively few data on side effects and tolerability but overall these were consistent
with effects known from the separate medications. There were no reliable data on long-term
risk factor reductions or cardiovascular outcomes though these would not be expected in
such short term small studies.
5.2 Ongoing trials – polypill versus placebo
Several large scale randomized trials have commenced (Annex 6.3.7) which aim to address
the question of the effect of a polypill on CVD outcomes (in particular CVD events) in
primary prevention. This is a patient population in which perhaps use of a polypill may be
considered more controversial as some may argue that the benefits of treatment may not
outweigh the risks of treating such patients (particularly in relation to the use of aspirin).
Three trials are recruiting/following-up patients who are at moderate risk of CVD in large
scale, long-term trials which are powered to assess the risk-benefit ratio of polypills in
primary prevention and particularly the effect on CVD events. The results of these trials will
also give an indication of the effect of a polypill on adherence over time in a group of
patients who, being asymptomatic without a diagnosis of CVD, may well be less inclined to
be adherent to preventive medication.
5.3 Previous trials – polypill versus usual care
5.3.1 FP7-funded UMPIRE trial
The “Use of a Multidrug Pill In Reducing cardiovascular Events” (UMPIRE) trial aimed to
assess whether a polypill-based strategy for delivery of medications (aspirin, statin and two
blood pressure lowering agents) compared to usual care would improve long-term
adherence to guideline-indicated therapy, systolic blood pressure (SBP) and low density
lipoprotein (LDL)-cholesterol in people with CVD or at similarly high risk. The trial was a
prospective, randomized, open-label, blinded-endpoint (PROBE) clinical trial among 2004
participants from India and Europe. The main eligibility criteria were established CVD or an
estimated five-year CVD risk of ≥15%. Participants were randomly assigned (1:1) to a fixed-
dose combination POLYPILL-based strategy or usual care. In the POLYPILL group,
physicians could use a POLYPILL that contained aspirin 75 mg, simvastatin 40 mg, lisinopril
10 mg and atenolol 50 mg or one containing aspirin 75 mg, simvastatin 40 mg, lisinopril 10
mg and hydrochlorothiazide 12.5 mg. In the usual care group, treatment continued

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-27
according to physician discretion. Adherence to medication (defined as self-reported use of
antiplatelet, statin and ≥2 BP-lowering medications) and changes in SBP and LDL-cholesterol
from baseline were the main outcomes. At baseline, mean blood pressure was 137/78 mmHg,
LDL-cholesterol was 91.5 mg/dl and 1233/2004 (61.5%) participants reported use of
antiplatelet, statin and ≥2 BP lowering medications. Full baseline characteristics are provided
in Annex 6.3.4.
Median follow-up was 15 months. Allocation to the POLYPILL group improved adherence
by one-third (RR 1.33, [95% CI 1.26, 1.41] p<0.0001), with reductions in SBP (-2.6 mmHg [95%
CI -4.0, -1.1] p=0.0005) and LDL-cholesterol (-0.11 mmol/l [95% CI -0.17, -0.05] p=0.0005) that
which corresponds to 4.6 patients needing to be treated with the polypill in order to gain one
additional adherent patient. These results are shown in Figure 6.3.10.
Figure 6.3.9: Adherence to indicated medications by treatment group over follow-up in the
FP7-funded UMPIRE trial
Source: personal communication, S Thom
Legend: Figure shows overall adherence (panel A), statin (panel B), antiplatelet drug (panel C), and ≥2
BP lowering drugs (panel D) by follow-up time in the POLYPILL and usual care groups. M6-M24 are
visits at months six to 24
In
dic
ate
d m
ed
ic
atio
ns
(
%)
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
B a s e l in e M 6 M 1 2 M 1 8 M 2 4
U s u a l c a re
F D C
1 .3 6 (9 5 % C I 1 .3 0 ; 1 .4 3 ) , p < 0 .0 0 0 1
6 3 .45 9 .7
6 3 5 /1 0 0 25 9 8 /1 0 0 2
6 8 .3
9 7 .3
6 7 .2
9 2 .0
6 5 7 /9 7 88 9 9 /9 7 7
6 5 .1
8 8 .4
6 0 2 /9 2 58 2 7 /9 3 5
6 4 .0
8 6 .3
3 3 4 /5 2 24 5 2 /5 2 4
5 0 .0
7 6 .5
1 8 /3 62 6 /3 4
Sta
tin
(
%)
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
B a s e l in e M 6 M 1 2 M 1 8 M 2 4
U s u a l c a re
F D C
8 7 .68 8 .0
8 7 8 /1 0 0 28 8 2 /1 0 0 2
9 3 .9
9 8 .9
9 3 .1
9 6 .7
9 1 1 /9 7 89 4 5 /9 7 7
9 1 .0
9 4 .5
8 4 2 /9 2 58 8 4 /9 3 5
8 9 .8
9 2 .4
4 6 9 /5 2 24 8 4 /5 2 4
8 3 .3
9 1 .2
3 0 /3 63 1 /3 4
An
tip
la
te
le
t d
ru
g (
%)
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
B a s e l in e M 6 M 1 2 M 1 8 M 2 4
U s u a l c a re
F D C
9 1 .09 1 .8
9 1 2 /1 0 0 29 2 0 /1 0 0 2
9 4 .8
9 9 .4
9 4 .7
9 7 .5
9 2 6 /9 7 89 5 3 /9 7 7
9 3 .4
9 5 .9
8 6 4 /9 2 58 9 7 /9 3 5
9 1 .0
9 2 .7
4 7 5 /5 2 24 8 6 /5 2 4
7 2 .2
8 8 .2
2 6 /3 63 0 /3 4
2 o
r m
or
e B
P-
lo
we
rin
g d
ru
gs
(
%)
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
B a s e l in e M 6 M 1 2 M 1 8 M 2 4
U s u a l c a re
F D C
7 1 .06 5 .9
7 1 1 /1 0 0 26 6 0 /1 0 0 2
7 4 .3
9 7 .9
7 3 .6
9 3 .0
7 2 0 /9 7 89 0 9 /9 7 7
7 3 .3
9 0 .8
6 7 8 /9 2 58 4 9 /9 3 5
7 3 .8
8 9 .3
3 8 5 /5 2 24 6 8 /5 2 4
7 2 .2
8 5 .3
2 6 /3 62 9 /3 4

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-28
Figure 6.3.10: Systolic blood pressure and LDL-cholesterol by treatment group over
follow-up in the FP7-funded UMPIRE trial
Source: personal communication, S Thom
Legend: Systolic blood pressure (panel A) and LDL-cholesterol (panel B) values shown at baseline,
during follow-up and at end of study (EOS) in the polypill and usual care groups.
There was broad consistency of effects across pre-defined subgroups including
cardiovascular history, gender, smoking status, diabetic status, region (Western Europe
versus India) and choice of POLYPILL. In addition, there was consistent evidence of larger
benefits among patients with lower adherence at baseline i.e. those who were not already
receiving antiplatelet, statin and two blood pressure drugs at baseline (Table 6.3.6). It should
be noted that the adherence rates of the non POLYPILL control patients was high as
compared to the results of normal care as reported in the EUROASPIRE studies described
above.
Table 6.3.6: Primary outcomes in UMPIRE trial, according to baseline adherence
Outcome Mean difference and 95% CI,
polypill versus usual care p-value for
heterogeneity Adherent* at
baseline
Not adherent* at
baseline
Adherence* (relative risk) 1.04 (1.01,1.08) 3.35 (2.74, 4.09) <0.001
Systolic BP (mmHg) -1.0 (-2.9, 0.8) -4.9 (-7.3,-2.6) 0.01
LDL cholesterol (mmol/l) -0.07 (-0.15, 0.01) -0.17 (-0.27, -0.07) 0.1
Source: personal communication, S Thom
* defined as taking statin, antiplatelet and two or more blood pressure lowering agents

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-29
In absolute terms, the improvement in adherence was particularly large in the group who
were under-treated at baseline (73.4% versus 23.1%) compared to those who were taking
medications from all recommended classes at baseline (92.1% versus 88.1%). There were no
significant differences in serious adverse events between the groups.
The trial had several strengths, in terms of sample size, duration of follow-up and
completeness of data collection. However, there are several issues to be considered when
interpreting results from adherence trials in general and this study in particular. Most
importantly, the trial likely under-estimated benefits in a general population setting with
typical adherence levels, since volunteers for clinical trials tend to be relatively motivated
and clinical management in a trial setting tends to be more intensive than usual care.105 The
size of this under-estimation is suggested in the minority of individuals who were not taking
indicated medications at baseline, in whom randomization to POLYPILL resulted in a three-
fold increase in adherence levels and larger reductions in SBP and LDL-cholesterol. Effects
were nonetheless observed in a trial population of whom 82% initially reported use of statin,
antiplatelet and blood pressure lowering drug(s), whereas comparable combination
treatment rates are around 50% in high income countries and 5 to 20% in low and middle
income countries.76 Furthermore, improvements were observed compared to a usual care
group in whom treatment rates rose initially and remained higher than baseline throughout
the study, whereas adherence typically reduces over time 78,106 and in the usual care group,
approximately three-quarters of all statin prescriptions were for atorvastatin or rosuvastatin
which are newer and somewhat more efficacious statins at the doses used.
Ethics Committees required the researchers to provide the polypill free of charge, whereas
the usual care group continued to receive their medications with attendant costs or subsidies.
In one sense, this reflects the real impact if the polypill were to be made available at low or
zero cost to the patient, for example as part of a universal health care program. Among this
trial population, the economic advantage for the polypill group would likely have been
modest, both in India given the generally low cost of medicines and relative affluence of
participants from tertiary care settings, and in Europe given the prevalence of medication
and prescription subsidies. A large United States trial recently showed that elimination of
copayments for core cardiovascular medicines improved adherence by about 5% in absolute
terms, which is smaller than the treatment effect seen here.107
The trial did not identify an effect on cardiovascular events, but with only 85 events it
provided little power to detect meaningful differences between groups. Based on observed
differences in SBP, LDL cholesterol and aspirin use, relative risk reductions of around 15% in
coronary disease and stroke are anticipated after a few years.102 However, a clinical trial
would need to observe over 1 000 events to reliably detect a relative risk reduction of 15%.108
Among patients who were under-treated at baseline, the observed risk factor reductions
would be expected to lead to about a 30% reduction in cardiovascular events.
The main conclusion overall from UMPIRE was that among a well-treated population with
CVD or at similarly high risk, long-term provision of indicated cardiovascular preventive
medication as a polypill led to improvements in adherence, SBP and LDL-cholesterol.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-30
5.4 Ongoing trials versus usual care (Annexes 6.3.7)
5.4.1 FP7 funded FOCUS trial
The second trial funded by the FP7 program is the Fixed Dose Combination Drug
for Secondary cardiovascular Prevention (FOCUS) trial (www.focus-fp7.eu), which includes
a multi-country 4 000 patient descriptive non-interventional study aiming to provide a
comprehensive analysis of potential factors precluding adequate secondary prevention,
including health system characteristics, drug affordability and availability, as well as patient
characteristics. The second component will be a 1 340 patient randomised trial of the effect of
a polypill on adherence, BP and lipid levels at six to 9 months in participants with
established CVD. Phase 2 will also include a prospective economic evaluation. Patient
recruitment has commenced in this trial however results are not expected for some time yet.
5.4.2 Kanyini-GAP
The Kanyini guidelines adherence with the polypill (Kanyini-GAP) study 109 is an Australian
623 patient randomised controlled trial of the effect of a polypill on adherence, SBP and total
cholesterol in indigenous and non-indigenous populations with established CVD or five year
CVD risk of at least 15%. This study was completed in September 2012 and is undergoing
analysis of results. Of note, the Kanyini-GAP trial aimed to recruit patients and conduct the
trial in as ‘real-life’ a setting as possible. This included:
• Recruitment and follow-up conducted through patient's usual primary care provider
to reflect actual practice once a ‘polypill’ enters the market
• Recruitment in urban, rural and remote settings to accurately reflect the challenges
inherent in following up patients in a range of clinical settings
• Patients pay the relevant co-payment amount for their Red Heart Pill (polypill)
prescription to reflect actual required payment once the Red Heart Pill is available in
the Australian market.
5.4.3 IMPACT
The IMProving Adherence using Combination Therapy (IMPACT) trial 110 is a New Zealand
513 patient randomised controlled trial investigating the impact of a polypill on adherence,
SBP and LDL cholesterol in both Maori and non-Maori populations with established CVD or
five year CVD risk of at least 15%. The study has completed recruitment and is currently
conducting final patient visits with results expected in late 2013. As for the Kanyini-GAP
trial, patients were recruited and followed up in as ‘real-life’ a setting as possible including
recruitment through general practitioners, in a variety of urban and rural settings and
including the relevant medication co-payment that would be required from a patient once a
polypill is available on the market.
5.4.4 SPACE Collaboration meta-analysis
The UMPIRE, Kanyini-GAP and IMPACT trials are all part of the Single Pill to Avert
Cardiovascular Events collaboration (www.spacecollaboration.org), an international group
of investigators who aim:

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-31
1. To facilitate the conduct of independent clinical trials of a fixed dose combination pill
containing aspirin, a statin and blood pressure lowering drugs in individuals at high
cardiovascular risk
2. To promote the opportunities for such trials in low and lower middle income countries
and in marginalized populations in high income countries
3. To ensure as much uniformity between trials as possible to enable subsequent data
pooling
4. To undertake IPD meta-analysis at the conclusion of all the trials.
Having individual patient data (IPD) available for meta-analysis will provide the ability to
perform more complex analyses (survival and multivariate analyses), investigate the
influence of covariates on heterogeneity of treatment effects, both within and between trials,
facilitate greater flexibility in the categorization of subgroups and reduce potential biases by
allowing consistency checks with individual study results.
Results from this IPD meta-analysis are expected in early 2014.
6. What is the current “pipeline” of products that are to be used for this
particular condition?
An exhaustive review of the pipeline of all products relevant to cardiovascular disease
control is beyond the scope of this Background Paper. A summary of the polypills that are in
development is given in Annex 6.3.8. As can be seen, there are several products in the
research pipeline that have aspirin, statin and one or more blood pressure lowering agents.
There are also a number of ‘semi-polypills’ in development, combining across two
therapeutic classes e.g. a statin and an anti-diabetic agent.
7. What are the opportunities for research into new pharmaceutical
interventions?
The use of fixed dose combinations in cardiovascular disease has stimulated much
discussion and debate in the medical literature. Criticism of the polypill strategy was based
on the view that it would largely be applied in the primary prevention of a population at a
relatively low absolute risk of cardiovascular disease. It was argued that a large proportion
of the population would be medicated unnecessarily. Furthermore, there was concern that
the polypill might induce a sense of protection and deflect attention from healthy lifestyle
behaviours like low fat diet and physical activity. The counter-arguments however are
strong. Although Professors Wald and Law still promote the concept of generic prescription
of a ‘polypill’ to all patients in a certain age group, it is worth clarifying that the majority of
clinical researchers working in the area of fixed dose combination pills for CVD prevention
do not agree with this proposal. Instead, the majority of work conducted so far in this area
has focused on proof of concept, placebo-controlled, pharmacodynamics trials, primary
prevention for patients with moderate CVD risk versus placebo trials, and polypill versus
usual care in secondary prevention and high risk primary prevention population trials.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-32
Several paradigm changes have been proposed in the area of fixed dose combinations, both
as and by the Wald and Law papers published in 2003 are involved in the “polypill” concept,
as broadly defined in Table 6.3.7.
Table 6.3.7: Paradigm changes in the field of polypill research.
Paradigm change / research question Relevant trials
ongoing
Gaps
Use in established indications: do any
benefits of fixed combinations of
indicated medicines (access,
adherence, treatment inertia)
outweigh any problems (lack of
tailoring, dose titration etc.)
UMPIRE, Kanyini-
GAP, IMPACT
None in specific disease
areas e.g. diabetes
No CV events (but see
discussion of limited trial
size and infrequent
events)
Prevention: new approach to
preventing CVD (indication not
available for separate components)
TIPS-3 High dose – side effects
may be too high
Sample size may be too
small
Use of low doses of three BP drugs TRIUMPH
TIPS-4
No event trials
Treatment initiation – based on CV
risk not risk factor level. In most
extreme form age is only risk
indicator needed
All trials have entry
based on CV risk
except Wald (age only)
Not amenable to trials -
more analysis and policy
Treatment monitoring – based only
on adherence, not based on risk factor
levels, or e.g. hypertension control
None Trial needed
8. What are the gaps between current research and potential research
issues which could make a difference are affordable and could be
carried out in a) five years or b) in the longer term?
8.1 Need for large-scale trials among people with established
cardiovascular disease and other indications for treatment
There are numerous reasons to focus on people with established cardiovascular disease and
other clear indications for future polypill research. From a public health viewpoint, this is a
large, easily identified, high-risk patient population among whom almost half of all
cardiovascular events occur.111 There are well-established large reductions in cardiovascular
events and mortality that can be achieved when patients are prescribed and adhere to
recommended preventive medications such as cholesterol lowering,27 blood pressure
lowering 112 and anti-platelet drugs,90 yet large treatment gaps still persist. Following an
acute myocardial infarction, if left untreated, patients with CVD have a persistent 5% risk of

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-33
mortality each year.113 In this context, the ‘low hanging fruit’ of CVD prevention is to make
available, prescribe and promote adherence to essential medications in those at highest risk
i.e. those who have established CVD. The FP7-funded UMPIRE trial showed that promising
improvement in adherence and clinical indicators could be achievement with provision of a
polypill in this patient group in different environments. However, a number of research
questions remain outstanding, and these include the following questions.
8.2 What are the effects of implementing a polypill strategy on
cardiovascular outcomes?
In circumstances in which individual medicines are already proven to be efficacious, there
should be no need to doubt or require repeat evidence of the benefit of combined therapy,
unless some new interaction or some new issue related to concomitant starting or stopping;
or that there perhaps exists benefits for some components and hazards for others. Thus
generally improvement in adherence can (and should) be taken as improvement in CV
outcomes. However there are legitimate reasons to assess the size of benefits, and risks, of
implementing a polypill strategy on a large scale. Many of the factors involved in scale-up
are system-level e.g. training, education, task shifting, electronic decision support, and many
of the patients, clinicians and environments most in need of adherence-improving strategies
are those least likely to join a standard clinical trial. Therefore the area would be well served
with a very large implementation trial, or a series of sister trials, with the following features
• cluster or step wedge implementation114
• unit of randomisation: primary healthcare facility
• denominator/patient population: individuals with established CVD stratified into
different population groups
• numerator/outcome: CV outcomes, and also to assess generalizability in subgroups
the percentage taking guideline-recommended medicines, and LDL and SBP levels
The UMPIRE trial showed improvements in risk factor reductions that would be expected to
result in a 10 to 15% reduction in CV events in that trial population, but that benefit might be
at least twice as great among a group not taking all indicated medications. One would
therefore require trials involving several tens of thousands of participants in order to reliably
assess CV outcomes, and assess consistency in different patient groups and in different
health systems. However if such a trial was successful it would result in the transformation
of the standard of care for patients with proven cardiovascular disease and save hundreds of
thousands of lives.
Several other pressing research questions exist, which could be addressed as part of the
above trial(s), or as separate trials.
8.3 Potential benefits of next generation polypills
8.3.1 Additional benefits from use of newer agents
Several agents have recently come off patent (e.g. atorvastatin, clopidogrel) and could
conceivably be included in the next generation of polypills, and other agents will be coming
off patent within five years (e.g. rosuvastatin). Research could usefully be directed to
assessment of the additional benefits of including these agents for specific patient
populations or having them replace agents in the existing polypills.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-34
8.3.2 How many dose versions for each polypill?
The ‘default’ option from a regulatory point of view is to make available all conceivable dose
versions, excluding perhaps those that are rarely or never used, whereas the original concept
of the polypill was based on a single dose version. An important research question is
whether the advantages of therapeutic flexibility outweigh the advantages of regimen
simplicity and avoidance of resistance to treatment.
8.3.3 Low dose or high dose polypill components?
The ideal dose(s) of component medications is a topic of intense debate in the area. In the
simplest case, there is little doubt that low doses of aspirin are ideal, given that higher doses
are associated with more side effects but not greater benefits.63 Statins have a shallow dose
response curve in terms of benefits, with each doubling of dose only leading to about a 7%
increase in LDL reduction.31 However, side effects are low at all doses except maximal ones.
In the context of combination therapy, there are surprisingly modest marginal benefits in
cardiovascular risk reduction of increased dosages of the blood pressure lowering drugs, at
the cost of an increase in side effects. Evidence from a very large number of clinical trials has
shown that doubling the dose of a blood pressure agent typically leads to much less than a
doubling in blood pressure reduction, but a moderate increase in side effects.115,116 The small
expected difference in overall cardiovascular event reduction for polypill formulations
differing in their extent of BP reduction is shown in Figure 6.3.8.
The recently completed TIPS 2 trial 117 suggests that maximal dose polypill versions will
achieve only a few mmHg additional SBP difference at most in the long-term. This trial
observed an increased SBP reduction of only 2.8 mmHg after doubling the dose of three
blood pressure lowering agents (i.e. one arm taking a single polycap containing ramipril 5
mg, atenolol 50 mg, hydrochlorothiazide 12.5 mg was compared to an arm taking two
polycaps). Furthermore, there was attenuation of the already small treatment differences at
week 12 compared to weeks two to eight. However increasing blood pressure lowering
drugs to maximal doses results in appreciable increases in side effects, which can reasonably
be expected to reduce long-term adherence.116

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-35
Table 6.3.8: Expected reduction in coronary heart disease risk with polypill versions
containing different doses of blood pressure lowering agents
Expected reduction in CHD risk
Modality
Polypill
– base
case
Polypill versions that achieve incremental
additional SBP reductions of:
1 mmHg 2 mmHg 3 mmHg 4 mmHg
BP reduction 26% 28% 29% 31% 33%
LDL reduction 42% 42% 42% 42% 42%
Aspirin 20% 20% 20% 20% 20%
Combination 66% 66% 67% 68% 69%
Data sources and assumptions:
Polypill “base case” version reduces SBP by 12 mmHg and LDL by 1 mmol/l (39 mg/dL)
Relative risks provided by systematic reviews of trials of aspirin,64 blood pressure lowering 115 and
cholesterol lowering.118,119 Since 1 mmol/L LDL-cholesterol reduction, 10 mmHg SBP reduction
and aspirin each individually lower CHD risk by 42% 118, 22% 120 and 20% 64 respectively (i.e. RRs
are 0.58, 0.78 and 0.80 respectively), the expected joint effects of a 1 mmol/L LDL-cholesterol
reduction, 16 mmHg SBP reduction and aspirin would be approximately a 69% lower CHD risk
(since 0.581.0/1.0 x 0.7816/10 x 0.80 = 0.41, and (1-0.41) x 100% = 69%).
8.4 Polypill approach in specific patient populations
The polypill approach can be adapted and adopted for other disease conditions, particularly
those with a large disease burden, for which adherence is a major factor. Polypills could be
developed in several of these areas, for example:
• a ‘diabetes polypill’, incorporating one or two hypoglycaemic agents as well as a
statin and an ACE-inhibitor
• A ‘hypertension polypill’ – incorporating three or even four very low dose
medications (see Annex 6.3.6 for current trials assessing this concept).
However, use in these conditions will likely require direct evidence of efficacy to convince
regulators and key opinion leaders, requiring trials similar to UMPIRE and FOCUS.
8.5 Expanding the polypill concept to acute care
To date, polypill trials have been conducted among a population with long-established
cardiovascular disease. However key issues arise concerning whether treatment should be
started sooner after an acute event:
• Are there greater benefits if people are started in hospital soon after an acute event?
• Can benefits accrue in the first year after acute coronary syndrome, when the greatest
risk for drop-off in adherence and for another major event are highest?
Therefore, trials of next generation polypills started in acute or semi-acute disease are
required.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-36
9. For which of these gaps are there opportunities for
pharmaceutical research?
There are considerable formulation challenges in simultaneously achieving bioequivalence,
long-term stability and maintaining a size for the polypill that is acceptable to patients.
Pharmaceutical research could be usefully directed to developing and testing new ways to
develop and manufacture polypills, including with some of the newer ingredients outlined
above.
An example of such research is the TI Pharma project “Design quality into products”
(http://www.tipharma.com/pharmaceutical-research-projects/production-technologies/
dosage.html, Accessed February 22nd, 2013) in which researchers successfully created a
production process that achieves homogeneity in drug mixtures, a process which is essential
in the creation of polypills as each pill must contain exactly the same dose of each of the
component drugs.
10. Conclusion
In the eight years since the last ‘Priority Medicines for Europe and World’ report, much work
has been done in the area of medication use for prevention of CVD. However the biggest
opportunity to have maximal impact on CVD prevention still remains further research into
ensuring widespread availability of fixed dose combination therapy (or polypills) that
include medications that have been demonstrated to be highly effective in CVD prevention,
are available in cheap generic formulations but are underutilized in almost every clinical
setting globally. Development of new medications for CVD prevention still has a role to play
but despite ongoing research costing billions of dollars, no new ‘blockbuster’ medication has
come to light recently that has the potential for greater effect than ensuring what already
exists is available and prescribed globally to patients with established CVD.
The FP7 funded UMPIRE trial has shown that even in a clinical trial population who were
already highly adherent at baseline, opportunity exists to improve BP and cholesterol control
via improved adherence with a polypill. In patients who were not adherent to all medication
classes at baseline, a massive 300% increase in adherence to all recommended classes of
medication was seen. If such a polypill were applied across non-adherent patients across
Europe the scale of potential prevention of CVD events would be counted in the hundreds of
thousands. Extension of this potential to LMIC where the bulk of the disease burden lies
extends this to millions of people. Funding from FP7 has contributed significantly to the
progress so far in understanding the potential benefit of polypills in CVD prevention
however further funding is required to build upon the available evidence.
The scale of funding required to further develop the evidence base that has already been
achieved in the area of polypill research is unlikely to be committed to by major
pharmaceutical companies as their focus lies in the development of newer patent-protected
products which are likely to have higher profit margins. Meanwhile, generic pharmaceutical
companies do not have the research budgets that would enable them to invest in such large-

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-37
scale clinical trials. Major public funding commitment is therefore needed to ensure that
what has been achieved so far is built upon and to provide the evidence necessary for
regulatory approval in both Europe and worldwide. The potential benefits of the widespread
use of polypills are enormous.
Other issues in this area that require further research include:
Potential additional benefits from newer agents now off-patent
Number of dose versions
Low-dose versus high-dose polypills
Specific populations (e.g. diabetes polypill, hypertension polypill)
Use in acute care (e.g. immediately after a heart attack versus use in chronic care).
Other cardiovascular research areas
As mentioned in the introduction, there are many other areas of research into
pharmacological approaches to IHD that may need to be supported. These include the
development of new lipid-lowering drugs; pharmacological means to address novel
mechanistic concepts of vessel wall damage and protect against conditions such as chronic
inflammation and local angiogenesis; as well as regenerative medicine/cell therapy
approaches. Similarly, new pharmacological treatment strategies need to be developed for
heart failure and arrhythmias, frequent consequences of IHD. While these areas have not
been investigated in this background paper or the chapter, opportunities for research may
exist that are not being addressed by the pharmaceutical industry.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-38
11. Declarations
The authors have received grants from several research charities and national funding
agencies for research on cardiovascular fixed dose combination medications, and from Dr
Reddys Ltd for co-ordination of the SPACE program (www.spacecollaboration.org). The
George Institute for Global Health obtained an exclusive global license in December 2012 for
the fixed dose combinations used in the SPACE trials following a decision by Dr Reddy’s Ltd
not to proceed with taking the products to market because of uncertainty in regulatory
requirements.
References
1 Kaplan W, Laing R. Priority Medicines for Europe and the World. Geneva: World Health
Organization; 2004.
2 Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality
from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global
Burden of Disease Study 2010. Lancet. 2013; 380(9859): 2095-128.
3 Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010 (GBD
2010) Results by Cause 1990-2010. 2013 [cited 17th January, 2013]; Available from:
http://www.healthmetricsandevaluation.org/ghdx
4 Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life
years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the
Global Burden of Disease Study 2010. Lancet. 2013; 380(9859): 2197-223.
5 World Health Organization. The Global Burden of Disease: 2004 update. Geneva: World Health
Organization; 2008.
6 World Health Organization. Global status report on noncommunicable diseases 2010. Geneva,
Switzerland: World Health Organization; 2011.
7 Beaglehole R, Bonita R, Horton R, Adams C, Alleyne G, Asaria P, et al. Priority actions for the non-
communicable disease crisis. Lancet. 2011; 377(9775): 1438-47.
8 Yusuf S, Hawken S, Ounpuu S, Daversus T, Avezum A, Lanas F, et al. Effect of potentially
modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART
study): case-control study. The Lancet. 2004; 364: 937 - 52.
9 O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic
and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control
study. Lancet. 2010; 376(9735): 112-23.
10 World Health Organization. Global health risks : mortality and burden of disease attributable to
selected major risks. Geneva, Switzerland: World Health Organization; 2009.
11 Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk
assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-39
21 regions, 1990?2010: a systematic analysis for the Global Burden of Disease Study 2010. The
Lancet. 2012; 380(9859): 2224-60.
12 Kawachi I, Colditz GA, Stampfer MJ, Willett WC, Manson JE, Rosner B, et al. Smoking cessation and
time course of decreased risks of coronary heart disease in middle-aged women. Archives of
Internal Medicine. 1994; 154(2): 169-75.
13 Bakhru A, Erlinger TP. Smoking cessation and cardiovascular disease risk factors: results from the
Third National Health and Nutrition Examination Survey. PLoS Med. 2005; 2(6): e160.
14 Hooper L, Summerbell C, Higgins J, Thompson R, Clements G, Capps N, et al. Reduced or modified
dietary fat for preventing cardiovascular disease [Systematic Review]. Cochrane Database of
Systematic Reviews. 2006; 3.
15 Ness AR, Powles JW. Fruit and vegetables, and cardiovascular disease: a review. International
Journal of Epidemiology. 1997; 26(1): 1-13.
16 Parikh P, McDaniel MC, Ashen MD, Miller JI, Sorrentino M, Chan V, et al. Diets and cardiovascular
disease: an evidence-based assessment. Journal of the American College of Cardiology. 2005; 45(9):
1379-87.
17 Thompson PD, Buchner D, Pina IL, Balady GJ, Williams MA, Marcus BH, et al. Exercise and
Physical Activity in the Prevention and Treatment of Atherosclerotic Cardiovascular Disease: A
Statement From the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and
Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on
Physical Activity). Circulation. 2003; 107(24): 3109-16.
18 de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean diet, traditional
risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of
the Lyon Diet Heart Study.[see comment]. Circulation. 1999; 99(6): 779-85.
19 Yang Q, Cogswell ME, Flanders WD, Hong Y, Zhang Z, Loustalot F, et al. Trends in cardiovascular
health metrics and associations with all-cause and CVD mortality among US adults. JAMA. 2012;
307(12): 1273-83.
20 EUROASPIRE I and II Group. Clinical reality of coronary prevention guidelines: a comparison of
EUROASPIRE I and II in nine countries. The Lancet. 2001; 357(March 31): 995-1001.
21 EUROASPIRE II Group. Lifestyle and risk factor management and use of drug therapies in coronary
patients from 15 countries; prinicipal results from EUROASPIRE II Euro Heart Survey Programme.
European Heart Journal. 2001; 22(7): 526-8.
22 Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U, et al. EUROASPIRE III: a survey
on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22
European countries. European Journal of Cardiovascular Prevention & Rehabilitation. 2009; 16(2):
121-37.
23 Kotseva K, Wood D, De Backer G, De Bacquer D, Pyörälä K, Keil U. Cardiovascular prevention
guidelines in daily practice: a comparison of EUROASPIRE I, II, and III surveys in eight European
countries. The Lancet. 2009; 373(9667): 929-40.
24 Global Atlas on cardiovascular disease prevention and control. Geneva; 2011.
25 Chen Z, Peto R, Collins R, MacMahon S, Lu J, Li W. Serum cholesterol concentration and coronary
heart disease in population with low cholesterol concentrations.[see comment]. BMJ. 1991; 303(6797):
276-82.
26 Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature
death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of
the Multiple Risk Factor Intervention Trial (MRFIT). JAMA. 1986; 256(20): 2823-8.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-40
27 Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of
cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14
randomised trials of statins. Lancet. 2005; 366(9493): 1267-78.
28 Cholesterol Treatment Trialists C. The effects of lowering LDL cholesterol with statin therapy in
people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials.
The Lancet. 2012; 380(9841): 581-90.
29 Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more
intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26
randomised trials. Lancet. 2010; 376(9753): 1670-81.
30 Tobert JA. Lovastatin and beyond: The history of the HMG-CoA reductase inhibitors. Nature
Reviews Drug Discovery. 2003; 2(7): 517-26.
31 Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein
cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ. 2003;
326(7404): 1423-.
32 Birjmohun RS, Hutten BA, Kastelein JJ, Stroes ES. Efficacy and safety of high-density lipoprotein
cholesterol-increasing compounds: a meta-analysis of randomized controlled trials. J Am Coll
Cardiol. 2005; 45(2): 185-97.
33 Jun M, Foote C, Lv J, Neal B, Patel A, Nicholls SJ, et al. Effects of fibrates on cardiovascular
outcomes: a systematic review and meta-analysis. Lancet. 2010; 375(9729): 1875-84.
34 Xydakis AM, Ballantyne CM. Combination therapy for combined dyslipidemia. Am J Cardiol. 2002;
90(10B): 21K-9K.
35 Ballantyne CM, Houri J, Notarbartolo A, Melani L, Lipka LJ, Suresh R, et al. Effect of ezetimibe
coadministered with atorvastatin in 628 patients with primary hypercholesterolemia: a prospective,
randomized, double-blind trial. Circulation. 2003; 107(19): 2409-15.
36 Davidson MH, McGarry T, Bettis R, Melani L, Lipka LJ, LeBeaut AP, et al. Ezetimibe coadministered
with simvastatin in patients with primary hypercholesterolemia. J Am Coll Cardiol. 2002; 40(12):
2125-34.
37 Kastelein JJ, Akdim F, Stroes ES, Zwinderman AH, Bots ML, Stalenhoef AF, et al. Simvastatin with
or without ezetimibe in familial hypercholesterolemia. N Engl J Med. 2008; 358(14): 1431-43.
38 Taylor AJ, Villines TC, Stanek EJ, Devine PJ, Griffen L, Miller M, et al. Extended-release niacin or
ezetimibe and carotid intima-media thickness. N Engl J Med. 2009; 361(22): 2113-22.
39 West AM, Anderson JD, Meyer CH, Epstein FH, Wang H, Hagspiel KD, et al. The effect of ezetimibe
on peripheral arterial atherosclerosis depends upon statin use at baseline. Atherosclerosis. 2011;
218(1): 156-62.
40 European Medicines Agency. Tredaptive, Pelzont and Trevaclyn. 2013 [cited 2013 9th February];
Available from:
http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/referrals/Tredaptive,_Pelzo
nt_and_Trevaclyn/human_referral_prac_000014.jsp&mid=WC0b01ac05805c516f
41 Kotwal S, Jun M, Sullivan D, Perkovic V, Neal B. Omega 3 Fatty acids and cardiovascular outcomes:
systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2012; 5(6): 808-18.
42 World Health Organization. Adherence to long-term therapies: Evidence for action. Geneva: World
Health Organization; 2003.
43 Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al. Blood pressure, stroke,
and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-41
randomised drug trials in their epidemiological context.[see comment]. Lancet. 1990; 335(8693): 827-
38.
44 Stamler J, Dyer AR, Shekelle RB, Neaton J, Stamler R. Relationship of baseline major risk factors to
coronary and all-cause mortality, and to longevity: findings from long-term follow-up of Chicago
cohorts. Cardiology. 1993; 82(2-3): 191-222.
45 Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. US
population data. Archives of Internal Medicine. 1993; 153(5): 598-615.
46 Blood Pressure Lowering Treatment Trialists Collaboration. Effects of different blood-pressure-
lowering regimens on major cardiovascular events: results of prospectively-designed overviews of
randomised trials. The Lancet. 2003; 362(9395): 1527-35.
47 Gueyffier F, Boutitie F, Boissel J-P, Pocock S, Coope J, Cutler J, et al. Effect of Antihypertensive Drug
Treatment on Cardiovascular Outcomes in Women and Men: A Meta-Analysis of Individual Patient
Data from Randomized, Controlled Trials. Ann Intern Med. 1997; 126(10): 761-7.
48 Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 Guidelines for
the management of arterial hypertension: The Task Force for the Management of Arterial
Hypertension of the European Society of Hypertension (ESH) and of the European Society of
Cardiology (ESC). Eur Heart J. 2007; 28(12): 1462-536.
49 Mancia G, Laurent S, Agabiti-Rosei E, Ambrosioni E, Burnier M, Caulfield MJ, et al. Reappraisal of
European guidelines on hypertension management: a European Society of Hypertension Task Force
document. J Hypertens. 2009; 27(11): 2121-58.
50 Cushman WC, Ford CE, Einhorn PT, Wright JT, Jr., Preston RA, Davis BR, et al. Blood pressure
control by drug group in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart
Attack Trial (ALLHAT). J Clin Hypertens (Greenwich). 2008; 10(10): 751-60.
51 Johnston A, Stafylas P, Stergiou GS. Effectiveness, safety and cost of drug substitution in
hypertension. Br J Clin Pharmacol. 2010; 70(3): 320-34.
52 Shaw E, Anderson JG, Maloney M, Jay SJ, Fagan D. Factors associated with noncompliance of
patients taking antihypertensive medications. Hosp Pharm. 1995; 30(3): 201-3, 6-7.
53 Faria C, Wenzel M, Lee KW, Coderre K, Nichols J, Belletti DA. A narrative review of clinical inertia:
focus on hypertension. J Am Soc Hypertens. 2009; 3(4): 267-76.
54 Okonofua EC, Simpson KN, Jesri A, Rehman SU, Durkalski VL, Egan BM. Therapeutic inertia is an
impediment to achieving the Healthy People 2010 blood pressure control goals. Hypertension. 2006;
47(3): 345-51.
55 Thijs L, Richart T, de Leeuw PW, Kuznetsova T, Grodzicki T, Kawecka-Jaszcz K, et al. Morbidity and
mortality on combination versus monotherapy: a posthoc analysis of the Systolic Hypertension in
Europe trial. J Hypertens. 2010; 28(4): 865-74.
56 Brown MJ, McInnes GT, Papst CC, Zhang J, MacDonald TM. Aliskiren and the calcium channel
blocker amlodipine combination as an initial treatment strategy for hypertension control
(ACCELERATE): a randomised, parallel-group trial. Lancet. 2011; 377(9762): 312-20.
57 Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SA, Feagan BG. A simplified approach to
the treatment of uncomplicated hypertension: a cluster randomized, controlled trial. Hypertension.
2009; 53(4): 646-53.
58 Gupta AK, Arshad S, Poulter NR. Compliance, safety, and effectiveness of fixed-dose combinations
of antihypertensive agents: a meta-analysis. Hypertension. 2010; 55(2): 399-407.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-42
59 Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood
pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003; 326(7404): 1427.
60 Dolley CT. Pharmacological basis for combination therapy of hypertension. Annu Rev Pharmacol
Toxicol. 1977; 17: 311-23.
61 Gradman AH. Rationale for triple-combination therapy for management of high blood pressure. J
Clin Hypertens (Greenwich). 2010; 12(11): 869-78.
62 Calhoun DA, Lacourciere Y, Chiang YT, Glazer RD. Triple antihypertensive therapy with
amlodipine, valsartan, and hydrochlorothiazide: a randomized clinical trial. Hypertension. 2009;
54(1): 32-9.
63 Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of
antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients.
British Medical Journal 2002; 324: 71-86.
64 Antithrombotic Trialists Collaboration. Aspirin in the primary and secondary prevention of vascular
disease: collaborative meta-analysis of individual participant data from randomised trials. The
Lancet. 2009; 373(9678): 1849-60.
65 Rothwell PM, Fowkes FGR, Belch JFF, Ogawa H, Warlow CP, Meade TW. Effect of daily aspirin on
long-term risk of death due to cancer: analysis of individual patient data from randomised trials.
The Lancet. 2011; 377(9759): 31-41.
66 Sabatine MS, Cannon CP, Gibson CM, Lopez-Sendon JL, Montalescot G, Theroux P, et al. Addition
of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment
elevation. N Engl J Med. 2005; 352(12): 1179-89.
67 Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Effects of clopidogrel in addition to
aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med.
2001; 345(7): 494-502.
68 Steinhubl SR, Berger PB, Mann JT, 3rd, Fry ET, DeLago A, Wilmer C, et al. Early and sustained dual
oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled
trial. JAMA. 2002; 288(19): 2411-20.
69 Gaspoz JM, Coxson PG, Goldman PA, Williams LW, Kuntz KM, Hunink MG, et al. Cost
effectiveness of aspirin, clopidogrel, or both for secondary prevention of coronary heart disease. N
Engl J Med. 2002; 346(23): 1800-6.
70 Karnon J, Brennan A, Pandor A, Fowkes G, Lee A, Gray D, et al. Modelling the long term cost
effectiveness of clopidogrel for the secondary prevention of occlusive vascular events in the UK.
Curr Med Res Opin. 2005; 21(1): 101-12.
71 Cholesterol Treatment Trialists Collaboration, Baigent C, Keech A, Kearney PM, Blackwell L, Buck
G, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data
from 90,056 participants in 14 randomised trials of statins. Lancet. 2005; 366(9493): 1267-78.
72 Kumar A, Fonarow GC, Eagle KA, Hirsch AT, Califf RM, Alberts MJ, et al. Regional and Practice
Variation in Adherence to Guideline Recommendations for Secondary and Primary Prevention
Among Outpatients With Atherothrombosis or Risk Factors in the United States: A Report From the
REACH Registry. Critical Pathways in Cardiology. 2009; 8(3): 104-11
10.1097/HPC.0b013e3181b8395d.
73 Webster RJ, Heeley EL, Peiris DP, Bayram C, Cass A, Patel AA. Gaps in cardiovascular disease risk
management in Australian general practice. Medical Journal Of Australia. 2009; 191(6): 324-9.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-43
74 Mendis S, Abegunde D, Yusuf S, Ebrahim S, Shaper G, Ghannem H, et al. WHO study on
Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE). Bulletin of the
World Health Organization. 2005; 83(11): 820-9.
75 Sharma KK, Gupta R, Agrawal A, Roy S, Kasliwal A, Bana A, et al. Low use of statins and other
coronary secondary prevention therapies in primary and secondary care in India. Vascular Health &
Risk Management. 2009; 5: 1007-14.
76 Yusuf S, Islam S, Chow CK, Rangarajan S, Dagenais G, Diaz R, et al. Use of secondary prevention
drugs for cardiovascular disease in the community in high-income, middle-income, and low-income
countries (the PURE Study): a prospective epidemiological survey. Lancet. 2011; 378(9798): 1231-43.
77 Gehi AK, Ali S, Na B, Whooley MA. Self-reported medication adherence and cardiovascular events
in patients with stable coronary heart disease: the heart and soul study. Arch Intern Med. 2007;
167(16): 1798-803.
78 Newby LK, LaPointe NM, Chen AY, Kramer JM, Hammill BG, DeLong ER, et al. Long-term
adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation.
2006; 113(2): 203-12.
79 Bailey JE, Lee MD, Somes GW, Graham RL. Risk factors for antihypertensive medication refill
failure by patients under Medicaid managed care. Clinical Therapeutics. 1996; 18(6): 1252-62.
80 Barat I, Andreasen F, Damsgaard EMS. Drug therapy in the elderly: what doctors believe and
patients actually do. British Journal of Clinical Pharmacology. 2001; 51(6): 615-22.
81 Miller NH, Hill M, Kottke T, Ockene IS. The Multilevel Compliance Challenge: Recommendations
for a Call to Action: A Statement for Healthcare Professionals. Circulation. 1997; 95(4): 1085-90.
82 Paes AH, Bakker A, Soe-Agnie CJ. Impact of dosage frequency on patient compliance. Diabetes
Care. 1997; 20(10): 1512-7.
83 Shaw E, Anderson JG, Maloney M, Jay SJ, Fagan D. Factors associated with noncompliance of
patients taking antihypertensive medications. Hospital Pharmacy. 1995; 30(3): 201-3.
84 Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and
medication compliance. Clin Ther. 2001; 23(8): 1296-310.
85 Mendis S, Fukino K, Cameron A, Laing R, Filipe A, Jr., Khatib O, et al. The availability and
affordability of selected essential medicines for chronic diseases in six low- and middle-income
countries. Bull World Health Organ. 2007; 85(4): 279-88.
86 van Mourik MS, Cameron A, Ewen M, Laing RO. Availability, price and affordability of
cardiovascular medicines: a comparison across 36 countries using WHO/HAI data. BMC Cardiovasc
Disord. 2010; 10: 25.
87 World Health Organization. Secondary prevention of non-communicable disease in low and middle
income countries through community-based and health service interventions. . Geneva; 2002 1 - 3
August.
88 Yusuf S. Two decades of progress in preventing vascular disease. Lancet. 2002; 360(9326): 2-3.
89 Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. British Medical
Journal 2003; 326(7404): 1419.
90 Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, et al. Aspirin in the primary and
secondary prevention of vascular disease: collaborative meta-analysis of individual participant data
from randomised trials. Lancet. 2009; 373(9678): 1849-60.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-44
91 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of
cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from
prospective epidemiological studies. BMJ. 2009; 338: b1665.
92 Heart Protection Study Collaborative G. MRC/BHF Heart Protection Study of cholesterol lowering
with simvastatin in 20,536 high-risk individuals: a randomized placebo-controlled trial. Lancet. 2002;
360: 7 - 22.
93 Progress Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering
regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;
358(9287): 1033-41.
94 Liang MH, Manson JE, inventors; Treatment of patients at elevated cardiovascular risk with a
combination of a cholesterol-lowering agent, an inhibitor of the renin-angiotensin system, and
aspirin. USA patent US patent: 6,576,256. 2001.
95 Tobert JA, Merck & Co Inc, inventors; Combination therapy for reducing the risks associated with
cardiovascular disease 1997.
96 Wald NJ, Law MR, inventors; Pharmaceutical formulation for the prevention of cardiovascular
disease patent GB 2361 185 A.
97 World Health Organization. The World Health Report 2002: Reducing risks, promoting healthy life.
Geneva; 2002.
98 Thom S, Field J, Poulter N, Patel A, Prabhakaran D, Stanton A, et al. Use of a Multidrug Pill in
Reducing cardiovascular Events (UMPIRE): rationale and design of a randomised controlled trial of
a cardiovascular preventive polypill-based strategy in India and Europe. European Journal of
Preventive Cardiology. 2012.
99 Sanz G, Fuster V, Guzman L, Guglietta A, Arnaiz JA, Martinez F, et al. The fixed-dose combination
drug for secondary cardiovascular prevention project: improving equitable access and adherence to
secondary cardiovascular prevention with a fixed-dose combination drug. Study design and
objectives. American Heart Journal. 2011; 162(5): 811-7.e1.
100 The Indian Polycap Study (TIPS). Effects of a polypill (Polycap) on risk factors in middle-aged
individuals wihtout cardiovascular disease (TIPS): a phase II, double-blind, randomised trial Lancet.
2009; 373: 1341-51.
101 Wald DS, Morris JK, Wald NJ. Randomized polypill crossover trial in people aged 50 and over.
PLoS ONE. 2012; 7(7): e41297.
102 Pill Collaborative Group, Rodgers A, Patel A, Berwanger O, Bots M, Grimm R, et al. An
international randomised placebo-controlled trial of a four-component combination pill ("polypill")
in people with raised cardiovascular risk. PloS one. 2011; 6(5): e19857.
103 Malekzadeh F, Marshall T, Pourshams A, Gharravi M, Aslani A, Nateghi A, et al. A pilot double-
blind randomised placebo-controlled trial of the effects of fixed-dose combination therapy
('polypill') on cardiovascular risk factors. International Journal of Clinical Practice. 2010; 64(9): 1220-
7.
104 Soliman E, Mendis S, Dissanayake W, Somasundaram N, Gunaratne P, Jayasingne IK, et al. A
Polypill for primary prevention of cardiovascular disease: A feasibility study of the World Health
Organization. Trials. 2011; 12(1): 3.
105 Hulley SB. Designing clinical research. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins;
2007.
106 Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J. Long-term persistence in use
of statin therapy in elderly patients. JAMA. 2002; 288: 455-61.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-45
107 Choudhry NK, Avorn J, Glynn RJ, Antman EM, Schneeweiss S, Toscano M, et al. Full coverage for
preventive medications after myocardial infarction. New England Journal of Medicine. 2011;
365(22): 2088-97.
108 Collins R, MacMahon S. Reliable assessment of the effects of treatment on mortality and major
morbidity, I: clinical trials. Lancet. 2001; 357: 373-80.
109 Liu HM, Patel A, Brown A, Eades S, Hayman N, Jan S, et al. Rationale and design of the Kanyini
guidelines adherence with the polypill (Kanyini-GAP) study: a randomised controlled trial of a
polypill-based strategy amongst Indigenous and non Indigenous people at high cardiovascular risk.
BMC public health. 2010; 10: 458.
110 Selak V, Elley CR, Crengle S, Harwood M, Doughty R, Arroll B, et al. Improving adherence using
combination therapy (IMPACT): Design and protocol of a randomised controlled trial in primary
care. Contemporary Clinical Trials. 2011; 32(6): 909-15.
111 Kerr AJ, Broad J, Wells S, Riddell T, Jackson R. Should the first priority in cardiovascular risk
management be those with prior cardiovascular disease? Heart. 2009; 95(2): 125-9.
112 Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events:
results of prospectively-designed overviews of randomised trials. Lancet. 2003; 362(9395): 1527-35.
113 Law MR, Watt HC, Wald NJ. The underlying risk of death after myocardial infarction in the
absence of treatment. Archives of Internal Medicine. 2002; 162(21): 2405-10.
114 Brown CA, Lilford RJ. The stepped wedge trial design: a systematic review BMC Med Res
Methodol. 2006 Nov 8;6:54.
115 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of
cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from
prospective epidemiological studies. British Medical Journal. 2009; 338: b1665-.
116 Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood
pressure lowering drugs: analysis of 354 randomised trials. British Medical Journal. 2003; 326(7404):
1427-31.
117 Yusuf S, Pais P, Sigamani A, Xavier D, Afzal R, Gao P, et al. Comparison of Risk Factor Reduction
and Tolerability of a Full-Dose Polypill (With Potassium) Versus Low-Dose Polypill (Polycap) in
Individuals at High Risk of Cardiovascular Diseases: The Second Indian Polycap Study (TIPS-2)
Investigators. Circulation Cardiovascular quality and outcomes. 2012; 5: 463-71.
118 Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein
cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. British
Medical Journal. 2003; 326: 1423-30.
119 Cholesterol Treatment Trialists' (CTT) Collaboration. Efficacy and safety of cholesterol-lowering
treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of
statins. Lancet. 2005; 366: 1267-78.
120 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of
cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from
prospective epidemiological studies. British Medical Journal. 2009; 338(may19_1): b1665-.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-46
Annexes
Annex 6.3.1: Mortality and burden of disease from IHD per age group and per region
Annex 6.3.2: Baseline characteristics of previous randomized controlled trials – versus
placebo or no treatment
Annex 6.3.3: Actual versus expected reductions in systolic blood pressure and LDL-
cholesterol in trials of ‘polypills’ versus placebo or no treatment
Annex 6.3.4: Baseline characteristics of UMPIRE trial
Annex 6.3.5: Ongoing randomized controlled trials – polypill versus usual care
Annex 6.3.6: Ongoing trials of “hypertension polypills”
Annex 6.3.7: Ongoing trials – polypill versus placebo or no treatment
Annex 6.3.8: Pipeline of polypills

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-47
Annex 6.3.1: Mortality and burden of disease from IHD per age group and
per region
Source: Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2010
(GBD 2010) Results by Cause 1990-2010
0
4,000,000
8,000,000
12,000,000
16,000,000
20,000,000
Ab
solu
te D
ALY
s
Age groups
Absolute DALYs due to IHD by age group in the world
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
Ab
solu
te D
ALY
s
Age groups
Absolute DALYs due to IHD by age group in Central Europe

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-48
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000A
bso
lute
DA
LYs
Age groups
Absolute DALYs due to IHD by age group in Eastern Europe
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
Ab
solu
te D
ALY
s
Age groups
Absolute DALYs due to IHD by age group in Western Europe

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-49
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000A
bso
lute
de
ath
s
Age groups
Global mortality for IHD by age group
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
Ab
solu
te d
eat
hs
Age groups
Mortality for IHD by age group in Central Europe

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-50
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
500,000A
bso
lute
de
ath
s
Age groups
Mortality for IHD by age group in Eastern Europe
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
500,000
Ab
solu
te d
eat
hs
Age groups
Mortality for IHD by age group in Western Europe

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-51
Annex 6.3.2: Baseline characteristics of previous randomised controlled trials – versus placebo or no treatment
Included Study Study population
characteristics
Mean age
(SD); female
gender (%)
Mean
SBP(SD)/D
BP (SD)
mmHg
Mean total
cholesterol
(SD); LDL
(SD)
mmol/L
‘Polypill’ contents
(dose); n
Comparison; n Duration of
follow-up;
Outcomes
assessed;
Notes
Malekzadeh
et al 2010 103*
Primary prevention (no
previous CVD)
Inclusion criteria: >50/55
years, no previous CVD; not
on active BP or lipid
lowering medications. No
exclusion for diabetes
59.1 (6.9);
33%
127.5 (17.3)
/ 79.8 (10.1)
5.26 (1.01);
2.99 (0.68)
Aspirin (81 mg),
Enalapril (2.5 mg),
Atorvastatin (20
mg) and
Hydrochloro-
thiazide (12.5 mg);
n=241
Placebo; n=234 12 months SBP, DBP,
Total
cholesterol,
LDL, AEs;
Imbalance in
baseline checks
suggests
inadequacy of
randomization;
Low follow-up
rate: 68% in
intervention,
78% in control
Pill
Collaborative
2011 121
Primary prevention (no
previous CVD)
Inclusion criteria: five-year
CVD risk >7.5% (based on
Framingham risk score) or
5% to 7.5% and 2 CVD risk
factors. No exclusion for
diabetes
61.4 (7.2);
19%
134.0 (13.5)
/ 80.5 (9.0)
5.50 (1.05);
3.65 (0.90)
Aspirin (75 mg),
Lisinopril (10 mg)
Hydrochlorothiazid
e (12.5 mg) and
Simvastatin (20
mg); n=189
Placebo; n=189 12 weeks SBP, DBP,
Total
cholesterol,
LDL, AEs;
99% follow-up
Wald 2012 122 Primary prevention (no
previous CVD)
Inclusion criteria: over 50
years of age
59 (range 51-
77);
26%
143.0 (16) /
86.0 (10)**
5.9 (1.0); 3.7
(0.9)**
Amlodipine (2.5
mg) Losartan (25
mg),
Hydrochlorothiazid
e (12.5 mg) and
Simvastatin (40
mg); n=86
Placebo; n=86 12 weeks
(cross-over
RCT)
SBP, DBP,
Total
cholesterol,
LDL, AEs
98% follow-up
The Indian
Polycap
Study ‘TIPS’
2009 100 #
Primary prevention (no
previous CVD)
Inclusion criteria: at least
one CV risk factor (including
diabetes)
53.6 (7.7);
44%
134.3 (12.3)
/ 85.2 (8.1)
4.7 (0.9); 3.0
(0.8)
Hydrochlorothiazid
e (12·5 mg),
Atenolol (50 mg),
Ramipril (5 mg),
Simvastatin (20
mg), Aspirin (100
mg); n=412
Aspirin (100
mg); n=205
(Simvastatin
20 mg group
added for BP
comparison
n=202)
12 weeks
(some 8-12
weeks);
SBP, DBP,
Total
cholesterol,
LDL, AEs;
85% follow-up
in these three
arms

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-52
* BP not assessed in meta-analysis as both arms contained an anti-hypertensive; ** Following placebo 12 weeks of cross-over RCT; # Double-blind nine-arm
with varying medication components and number of components. Only three arms were used in this meta-analysis: the polycap, aspirin and simvastatin
arms;
BP = blood pressure and measured in mmHg; SBP = systolic blood pressure; DBP = Diastolic blood pressure; Total chol. = total cholesterol in mmol/L; LDL =
LDL cholesterol in mmol/L; AE = adverse events; TLC = therapeutic lifestyle changes; SD = standard deviation; CVD = cardiovascular disease
121 Pill Collaborative Group, Rodgers A, Patel A, Berwanger O, Bots M, Grimm R, et al. An international randomised placebo-controlled trial of a four-
component combination pill ("polypill") in people with raised cardiovascular risk. PLoS ONE. 2011; 6(5): e19857. 122 Wald DS, Morris JK, Wald NJ. Randomized polypill crossover trial in people aged 50 and over. PLoS ONE. 2012; 7(7): e41297.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-53
Annex 6.3.3: Actual versus expected reductions in systolic blood pressure and LDL-cholesterol in trials of ‘polypills’
versus placebo or no treatment
Trial
Actual versus Expected Reductions in Systolic Blood Pressure (SBP) Actual versus Expected Reductions in LDL-Cholesterol
Antihyper-
tensive(s)
Standard
dose
equivalent 123
Mean
baseline
SBP mm
Hg*
Expected
reduction
in SBP
mmHg**
Observed
mean
difference in
SBP mmHg
Observed
/expected
Statin Mean
baseline
LDL in
mmol/l
Expected
reduction in
LDL mmol/l
^
Observed
control-
adjusted
reduction in
LDL mmol/l
Observed
/expected
Malekzadeh,
2010
Enalapril 2.5 mg 0.25 130 10.2 # 2.4 24% Atorvastatin
20 mg
2.99 1.29 0.45 35%
Hydrochlorothia
zide 12.5 mg
0.5
PILL
collaboration,
2011
Lisinopril 10 mg 1 130 10.2 # # 9.9 97% Simvastatin 20
mg
3.65 1.17 0.75 64%
Hydrochlorothia
zide 12.5 mg
0.5
Wald, 2012 Hydrochlorothia
zide 12.5 mg
0.5 140 17.6 17.9 100% Simvastatin 40
mg
3.70 1.37 1.4 102%
Losartan 25 mg 0.5
Amlodipine 2.5
mg
0.5
The Indian
Polycap Study,
2009
Hydrochlorothia
zide 12.5 mg
0.5 130 18.2 β 7.4 41% Simvastatin 20
mg
3.00 0.96 0.72 75%
Atenolol 50 mg 1
Ramipril 5 mg 2
* rounded to nearest 10 mm Hg; ** based on mean baseline SBP & standard dose equivalence (from Law 2009)124; ^mean baseline LDL x percentage reduction in LDL cholesterol
for the statin at that dose (from Law 2003) 125# estimate: two drugs at half dose therefore an overestimate of likely effect; # # estimate: two drugs at half dose therefore an
underestimate of likely effect; 12.7 mmHg for two drugs at standard dose; β estimate: three drugs at standard dose; 15.2 mmHg for three drugs at half standard dose.
123 Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials.
BMJ. 2003; 326(7404): 1427. 124 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in
the context of expectations from prospective epidemiological studies. BMJ. 2009; 338: b1665. 125 Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic
review and meta-analysis. BMJ. 2003; 326(7404): 1423.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-54
Annex 6.3.4: Baseline characteristics of UMPIRE Trial
FDC (N = 1002)
Usual care (N = 1002)
Age 62.1 (10.4) 61.6 (10.8)
Male 817 (81.5%) 825 (82.3%)
SBP (mmHg) 137.0 (21.3) 137.7 (21.1)
DBP (mmHg) 77.4 (12.0) 78.1 (11.5)
Heart rate (beats/ min) 71.0 (15.1) 70.8 (14.6)
Total cholesterol (mmol/L) 4.2 (1.0) 4.2 (1.1)
HDL cholesterol (mmol/L) 1.1 (0.3) 1.1 (0.3)
LDL cholesterol (mmol/L) 2.3 (0.8) 2.4 (0.9)
Triglycerides (mmol/L) 1.5 (0.9) 1.5 (0.9)
Glucose (mmol/L) 6.3 (2.4) 6.3 (2.3)
Creatinine (umol/L) 89.0 (22.10 89.7 (22.2)
Current smokers 131 (13.1%) 144 (14.4%)
Ever smoked cigarettes 541 (54.0%) 504 (50.3%)
Medical history
Coronary heart disease 769 (76.7%) 759 (75.7%)
Cerebrovascular disease 154 (15.4%) 157 (15.7%)
Peripheral vascular disease 56 (5.6%) 43 (4.3%)
Diabetes mellitus 283 (28.2%) 281 (28.0%)
Current drug treatment
Antihypertensive treatment
None 76 (7.6%) 66 (6.6%)
1 BP drug 266 (26.5%) 225 (22.5%)
≥2 BP drugs 660 (65.9%) 711 (71.0%)
Statin 882 (88.0%) 878 (87.6%)
Anti-platelet drug 920 (91.8%) 912 (91.0%)
Indicated medications1 598 (59.7%) 635 (63.4%)
Data not shown as n (%) are mean (SD).
1 Indicated medications = statin + anti-platelet + ≥2 anti-hypertensive drugs.
FDC = fixed dose combination.

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-55
Annex 6.3.5: Ongoing randomised controlled trials – polypill versus usual care
Study Study population
characteristics
N Regions ‘Polypill’ contents (dose); Comparison; Duration of
follow-up
Expected results Outcomes
Kanyini-GAP Established CVD or
CVD risk of >15%
over five years
623 Australia RHP version 1c:
aspirin 75 mg
lisinopril 10 mg
simvastatin 40 mg
atenolol 50 mg
RHP version 2c:
aspirin 75 mg
lisinopril 10 mg
simvastatin 40 mg
hydrochlorothiazide 12.5
mg
Usual care Minimum 12
months
Q2 2013 Adherence,
SBP, total
cholesterol
IMPACT Established CVD or
CVD risk of >15%
over five years
513 New Zealand RHP version 1c:
aspirin 75 mg
lisinopril 10 mg
simvastatin 40 mg
atenolol 50 mg
RHP version 2c:
aspirin 75 mg
lisinopril 10 mg
simvastatin 40 mg
hydrochlorothiazide 12.5
mg
Usual care Minimum 12
months
Q4 2013 Adherence,
SBP, LDL
cholesterol
FOCUS Post-myocardial
infarction
Phase 1
– 4 000
Phase 2
– 1 340
Argentina,
France, Italy,
Spain,
Switzerland
Aspirin 100 mg
Simvastatin 40 mg
Ramipril (2.5, 5, 10 mg)
Usual care 9 months ? Adherence, BP,
LDL
cholesterol,
safety, cost
effectiveness

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-56
Annex 6.3.6: Ongoing trials of “hypertension polypills”
Trial Aims Patient population Comparisons Follow-up Outcomes
TRIUMPH To assess role of a low-dose
triple antihypertensive
compared to usual care
Newly diagnosed patients
with persistent hypertension
despite adequate lifestyle
advice and/or changes;
and/or single drug therapy
for BP lowering
India
Triple pill versus usual care.
Triple pill is Telmisartan 20 mg, Amlodipine 2.5 mg,
Hydrochlorothiazide 6.25 mg or option with double
doses
Usual care: separate BP lowering medication
prescribed completely at the discretion of the
treating doctor
Six months Primary outcome: %
achieving target BP at
six months;
Secondary outcomes:
% with BP control at
six and 12 weeks;
change in BP;
tolerance to
treatment; use of
health care services;
self-reported BP
lowering medication
use; quality of life.
TIPS 4 To assess the incremental BP
lowering by full doses of
- two 3-BP lowering drugs
compared to
- three 2-BP lowering drugs
combinations.
• To assess the impact of
adding a statin on lipids to
the BP lowering drug
combinations
Men or women aged 30
years or older,
With SBP 150 to 180 mmHg
N= 825
India, Canada, Italy
1. HCTZ (25 mg) + Amlodipine (10 mg)
2. HCTZ (25 mg) + Atenolol (100 mg)
3. HCTZ (25 mg) + Ramipril (10 mg)
4. Low doses: – HCTZ 12.5 mg + rami 5 mg +
aten 50 mg or Amlodipine 5mg
5. Full doses: – HCTZ 25 mg + ramipril 10 mg +
atenolol 100 mg or Amlodipine 10mg
6 Simvastatin 40 mg
7. Atorvastatin 20 mg
Two weeks
run-in, eight
weeks
follow-up

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-57
Annex 6.3.7: Ongoing trials – polypill versus placebo or no treatment
Trial N Population Intervention Countries and Sponsors Outcomes Status
Indian Polycap Trial –
TIPS3
5 000 – 2x2x2
factorial
Men ≥55 and women
≥60 years with:
– an INTERHEART risk
score of ≥10,
– no known vascular
disease and
– no clear clinical
indication or
contraindication
for treatments
Polycap DS (thiazide
25 mg, atenolol 100
mg, ramipril 10 mg,
simvastatin 40 mg) -
daily +/- aspirin EC
75 g +/- vit D 60 000
IU monthly versus
control
China and India
Cadila Pharmaceuticals
Wellcome Trust
Canadian Institutes of Health
Research (CIHR)
Heart and Stroke Foundation
of Ontario
Major CVD events,
neurocognitive function
Enrolment started
Heart Outcomes
Protection (HOPE) 3
12 500- 2x2
factorial
Primary prevention in
men >55 years and
women >65 years with
at least one risk factor
and women aged >60
years with at least two
risk factors
Rosuvastatin 10 mg,
candesartan 16
mg/HCTZ 12.5 mg
factorial
22 countries
CIHR and Astra Zeneca
Major CVD events,
neurocognitive function,
renal function
Follow-up
complete 2015
Poly-Iran 7 000 Men and women
between 50 and 79
years old
Aspirin 81 mg,
enalapril 5 mg (or
valsartan 40 mg),
atorvastatin 20 mg
and
hydrochlorothiazide
12.5 mg
Iran
Tehran University of Medical
Sciences
CVD events, blood
sugar, cholesterol, BP,
compliance, tolerability
Enrolment started

Update on 2004 Background Paper, BP 6.3 Cardiovascular Disease
6.3-58
Annex 6.3.8: Pipeline of polypills
Company Name Active Components Clinical trial status
In development
Alborz Darou (Iran) Polyiran 1 Aspirin 81 mg, Atorvastatin 20 mg, Enalapril 5 mg,
hydrochlorothiazide 25 mg
Pilot studies conducted and published
Polyiran 2 Aspirin 81 mg, Atorvastatin 20 mg, Valsartan 40 mg,
hydrochlorothiazide 25 mg
Pilot studies conducted and published
Cadila (India) Ramitorva Aspirin 100 mg, simvastatin 20 mg, ramipril 5 mg, atenolol
50 mg, hydrochlorothiazide 12.5 mg
TIPS program published; FDA application in process
Cardio-Pharm (USA) CardiaPill BP lowering, statin and aspirin 3 components – specifics
undisclosed
Uncertain
CNIC-Ferrer (Spain) Trinomia Secondary prevention Aspirin 100 mg, simvastatin 40 mg, ramipril 2.5/5/10 mg 100 patients in trial in Spain; PD studies done in USA
and Spain
Large FOCUS trial underway in Italy, Spain, South
America; First patient randomized Nov 2011
Already available in Guatemala, and in registration
process in Latam
Dr Reddy’s (India)* Red Heart Pill (RHP) 1 Aspirin 75 mg, Lisinopril 10 mg, Simvastatin 20 mg (40 mg),
Atenolol 50 mg
SPACE trials underway, UMPIRE completed
Red Heart Pill (RHP) 2 Aspirin 75 mg, Lisinopril 10 mg, Simvastatin 20 mg (40 mg),
hydrochlorothiazide 12.5 mg
PILL trial published; SPACE trials underway, UMPIRE
completed
Polypill Company (United
Kingdom)
Polypill Simvastatin 20 mg; bendroflumethiazide 1.25 mg; losartan 25
mg ; amlodipine 2.5 mg
Uncertain
PolypillRx.com (USA) Customized production of different drugs into a single
capsule through registered pharmacies. Not actually a new
pill
None
On the market**
TajPharma (India) Multiple pill combinations Atorvastatin 10 mg, aspirin 75 mg, ramipril 5 mg
Atorvastatin 10 mg, aspirin 75 mg, ramipril 5 mg; metoprolol
50 mg (co-packaged),
Atorvastatin 10 mg, aspirin 150 mg, clopidogrel 75 mg
Torrent (India) CVPill Polytorva®. plus co-packaged metoprolol
Surien (India) Polytorva®. Atorvastatin 10 mg, Ramipril 5 mg, and enteric-coated
Aspirin 75 mg
Marketed by USV Ltd. In India only
Zyduscadila (India) Zycad – secondary prevention Atorvastatin 10 mg, ramipril 5 mg, Aspirin 75 mg
metoprolol 50 mg
*TGIGH has license –see Declarations ** Not developed to GMP standards, registered only on home country and not able to be exported. Only a selection of products shown here