Embed Size (px)
Citation preview
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 1/13
Background
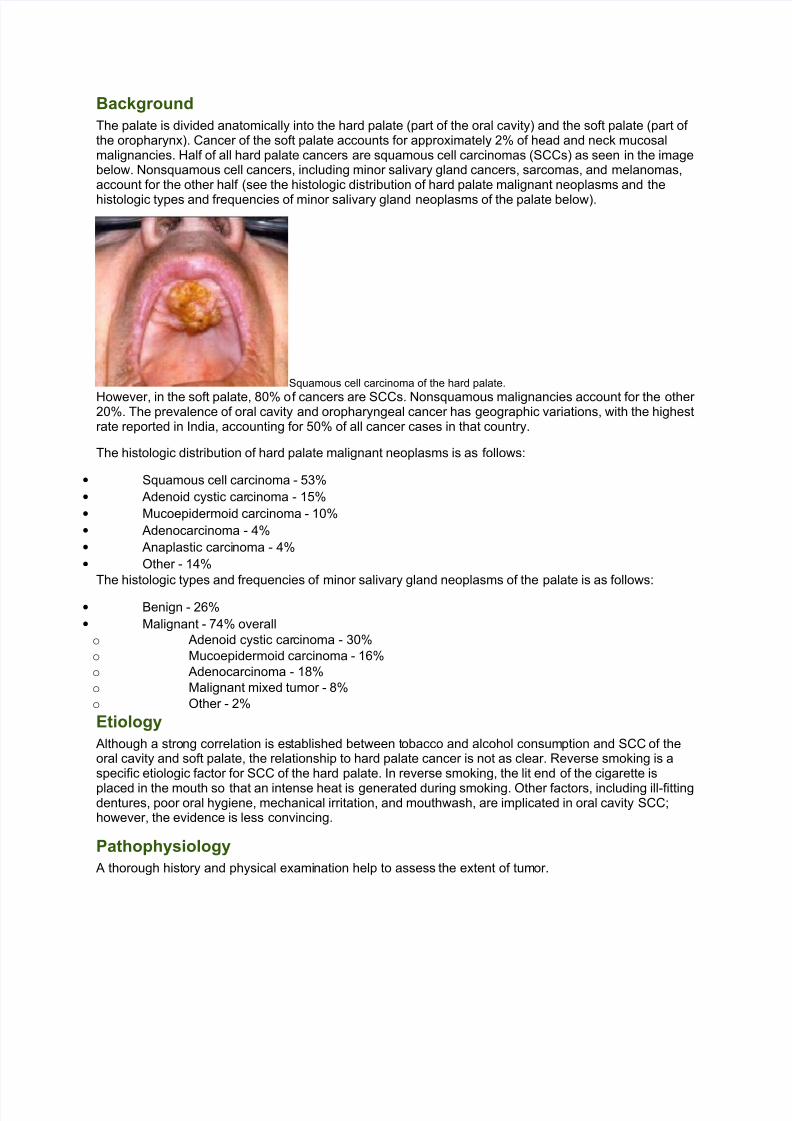
The palate is divided anatomically into the hard palate (part of the oral cavity) and the soft palate (part of the oropharynx). Cancer of the soft palate accounts for approximately 2% of head and neck mucosalmalignancies. Half of all hard palate cancers are squamous cell carcinomas (SCCs) as seen in the imagebelow. Nonsquamous cell cancers, including minor salivary gland cancers, sarcomas, and melanomas,account for the other half (see the histologic distribution of hard palate malignant neoplasms and the
histologic types and frequencies of minor salivary gland neoplasms of the palate below).
Squamous cell carcinoma of the hard palate.
However, in the soft palate, 80% of cancers are SCCs. Nonsquamous malignancies account for the other 20%. The prevalence of oral cavity and oropharyngeal cancer has geographic variations, with the highestrate reported in India, accounting for 50% of all cancer cases in that country.
The histologic distribution of hard palate malignant neoplasms is as follows:
• Squamous cell carcinoma - 53%
• Adenoid cystic carcinoma - 15%
• Mucoepidermoid carcinoma - 10%
• Adenocarcinoma - 4%
• Anaplastic carcinoma - 4%
• Other - 14%
The histologic types and frequencies of minor salivary gland neoplasms of the palate is as follows:
• Benign - 26%
• Malignant - 74% overall
o Adenoid cystic carcinoma - 30%
o Mucoepidermoid carcinoma - 16%
o Adenocarcinoma - 18%
o Malignant mixed tumor - 8%
o Other - 2%
Etiology
Although a strong correlation is established between tobacco and alcohol consumption and SCC of theoral cavity and soft palate, the relationship to hard palate cancer is not as clear. Reverse smoking is aspecific etiologic factor for SCC of the hard palate. In reverse smoking, the lit end of the cigarette is
placed in the mouth so that an intense heat is generated during smoking. Other factors, including ill-fittingdentures, poor oral hygiene, mechanical irritation, and mouthwash, are implicated in oral cavity SCC;however, the evidence is less convincing.
Pathophysiology
A thorough history and physical examination help to assess the extent of tumor.

7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 2/13
SCC extension beyond the hard palate occurs in up to 70% of lesions. Posterior extension involves thesoft palate, with possible velopharyngeal insufficiency and hypernasal speech. Palatal hypesthesiaindicates trigeminal nerve involvement in the sphenopalatine foramen or pterygopalatine fossa extension.
An absent corneal reflex is indicative of skull-base extension through the foramen rotundum, foramenovale, or inferior orbital fissure.
Dental numbness may indicate perineural invasion. Middle ear effusion is suggestive of nasopharyngealextension or invasion of the tensor veli palatini muscle.
Involvement of the mandibular division of the trigeminal nerve may manifest as hypesthesia along themandible or wasting of the temporalis or masseter muscles. This is indicative of infratemporal fossainvolvement. Trismus, malocclusion, and pain are symptoms of invasion of the pterygoid muscles.Extension to the gingiva requires assessment. Dental sockets provide a pathway of invasion to thealveolar process of the maxillary bone and into the maxillary sinus. Nasal floor involvement may occur bydirect extension through the palate.
Lymph node involvement is of special concern in SCC and high-grade mucoepidermoid cancer. It is rarein other salivary gland carcinomas. Approximately 30% of patients have cervical node metastasis at thetime of presentation.[1] The submandibular nodes (level I) and upper deep jugular lymph nodes (level II)are the first echelon of nodal drainage. However, in tumors with posterior soft palate extension,retropharyngeal nodes may be involved. Soft palate carcinomas are staged as oropharyngeal cancersaccording to the American Joint Committee on Cancer (see Staging).
Almost half of patients present with extension of the tumor beyond the soft palate. Common sites of extension include the tonsils, retromolar trigone, inferior or superior alveolar process, hard palate, andbase of tongue. Extension into the sphenopalatine foramen may result in palatal hypostasis. In extensivelesions extending into the nasopharynx, middle ear effusion is common. The tumor may extendanterosuperiorly into the pterygomaxillary and infratemporal fossa.
Presentation
SCCs of the palate manifest as ulcerative surface lesions. Often, patients are asymptomatic in the earlystages, but they may experience pain in advanced stages. A palate mass, bleeding, a foul odor, ill-fittingdentures in edentulous patients, or loose teeth may be the presenting symptoms for patients with hard
palate cancer. In persons with advanced-stage soft palate cancers, velopharyngeal insufficiency, alteredspeech, difficulty swallowing, referred otalgia, trismus, or a neck mass may be present. Because the areais easily visualized, tumors are often found at early stages incidentally by the patient or the physician.
On the other hand, minor salivary gland tumors manifest as submucosal lesions, as depicted in the imagebelow, with a smooth, normal mucosal covering. Melanomas are smooth, black lesions but may be brownor brownish gray. Kaposi sarcomas are bluish lesions that are commonly seen in patients with HIVinfection.
Thirty-two-year-old man with a submucosal lesion at the junction of the hard and softpalate.

7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 3/13
Pseudoepitheliomatous hyperplasia and necrotizing sialometaplasia are benign self-limited lesions thatcan mimic SCC and need to be distinguished histologically. Torus palatina (ie, bony hyperplasia of thepalate) are hard midline masses that produce no symptoms and should not be confused with tumors.
Relevant Anatomy
The palate separates the oral cavity from the nasal cavity and the maxillary sinuses. The mucosa of the
palate is a keratinizing pseudostratified squamous epithelium. However, the submucosa has numerousminor salivary glands, especially in the hard palate. The periosteal covering of the hard palate becomes arelative barrier to the spread of cancer into the palatine bone.
The neurovascular supply to the palate comes from the palatine foramina, located medial to the thirdmolar teeth. These foramina provide a pathway for the tumor to spread. Descending palatine arteries fromthe internal maxillary artery provide the blood supply. Vessels pass anteriorly through the nasopalatineforamen to the nose. Sensory and secretomotor fibers from the maxillary (V-II) branch of the trigeminalnerve and pterygopalatine ganglion traverse to the hard palate via the greater and lesser palatine nerves.
Anatomically, the soft palate is part of the oropharynx. It consists of mucosa on both surfaces. Interveningbetween the 2 mucosal surfaces are the connective tissue, muscle fibers, aponeurosis, numerous bloodvessels, lymphatics, and minor salivary glands. Functionally, the soft palate serves to separate theoropharynx from the nasopharynx during swallowing and speech. The soft palate approximates with the
posterior pharyngeal wall during swallowing to prevent nasopharyngeal regurgitation and approximatesduring speech to prevent air escape into the nose.
Contraindications
Contraindications to surgical correction of malignant palate tumors are based on the patient'scomorbidities and his or her ability to tolerate surgery. Coexisting medical conditions may put the patientat risk during anesthesia. Additionally, tumors may be deemed inoperable because of their size or extentof involvement. Tumors that have intracranial extension are considered inoperable if they involve thebrain parenchyma. Radiation therapy is a treatment option in these rare cases. See the Treatment sectionfor recommended treatments for various types and stages of palate cancer.
maging Studies
• Radiologic evaluation helps to increase the accuracy of staging. Computed tomography (CT)scanning and magnetic resonance imaging (MRI) are the imaging modalities of choice.
• Perform CT scanning in axial and coronal planes. Coronal images, as seen in the image below,
are best for assessing bony invasion of the palate and extension into the nasal fossa or maxillary sinus.
Coronal CT scan revealing intranasal extension of the tumor.
•CT scanning aids in assessing skull-base extension. Enlargement of skull-base foramina
is indicative of tumor invasion. Axial images aid in assessing extension in the horizontal plane along thesoft palate, pterygoid plates and muscles, infratemporal fossa, and masticator space.
• CT scanning with intravenous contrast infusion should include the neck to assess for
cervical node involvement. This is especially important for SCC and high-grade mucoepidermoidcarcinoma.
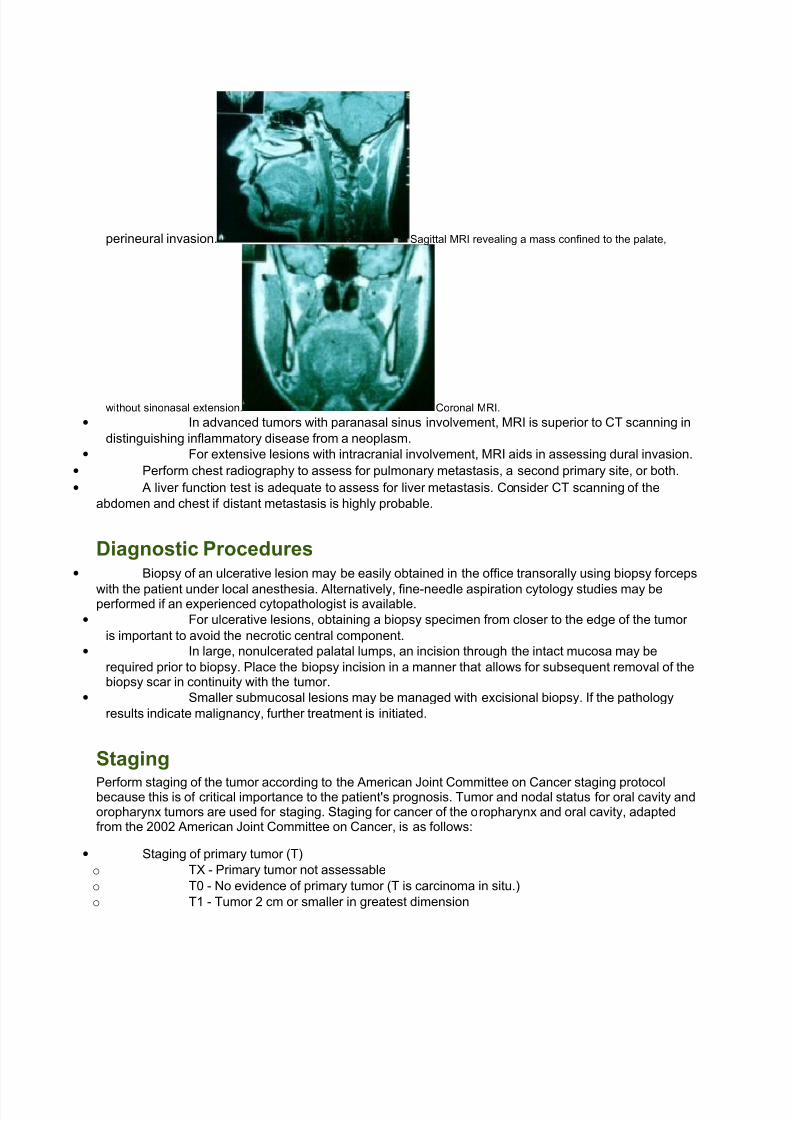
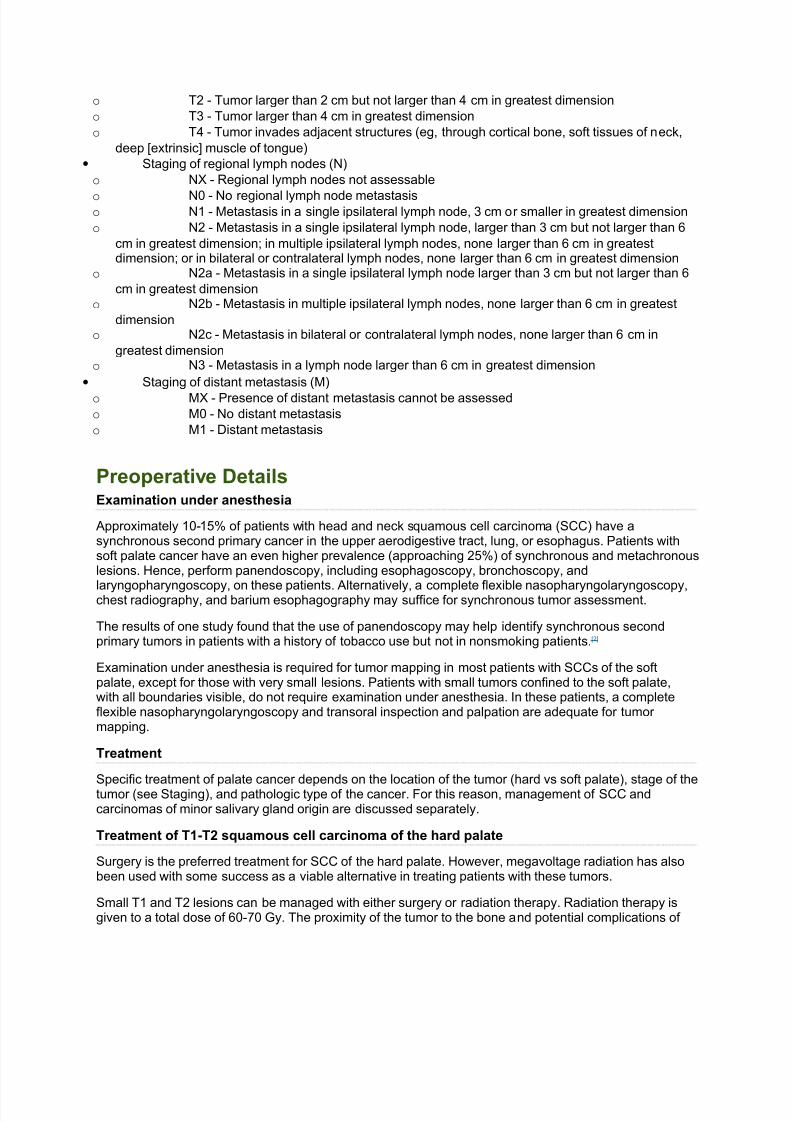
• MRI, as seen in the images below, is more accurate for assessing perineural extension
along the foramina. This is especially important in adenoid cystic carcinoma with the propensity for
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 4/13
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 5/13
o T2 - Tumor larger than 2 cm but not larger than 4 cm in greatest dimension
o T3 - Tumor larger than 4 cm in greatest dimension
o T4 - Tumor invades adjacent structures (eg, through cortical bone, soft tissues of neck,
deep [extrinsic] muscle of tongue)
• Staging of regional lymph nodes (N)
o NX - Regional lymph nodes not assessable
o N0 - No regional lymph node metastasiso N1 - Metastasis in a single ipsilateral lymph node, 3 cm or smaller in greatest dimension
o N2 - Metastasis in a single ipsilateral lymph node, larger than 3 cm but not larger than 6
cm in greatest dimension; in multiple ipsilateral lymph nodes, none larger than 6 cm in greatestdimension; or in bilateral or contralateral lymph nodes, none larger than 6 cm in greatest dimension
o N2a - Metastasis in a single ipsilateral lymph node larger than 3 cm but not larger than 6
cm in greatest dimensiono N2b - Metastasis in multiple ipsilateral lymph nodes, none larger than 6 cm in greatest
dimensiono N2c - Metastasis in bilateral or contralateral lymph nodes, none larger than 6 cm in
greatest dimensiono N3 - Metastasis in a lymph node larger than 6 cm in greatest dimension
• Staging of distant metastasis (M)
o MX - Presence of distant metastasis cannot be assessed
o M0 - No distant metastasis
o M1 - Distant metastasis
Preoperative DetailsExamination under anesthesia
Approximately 10-15% of patients with head and neck squamous cell carcinoma (SCC) have asynchronous second primary cancer in the upper aerodigestive tract, lung, or esophagus. Patients withsoft palate cancer have an even higher prevalence (approaching 25%) of synchronous and metachronouslesions. Hence, perform panendoscopy, including esophagoscopy, bronchoscopy, and
laryngopharyngoscopy, on these patients. Alternatively, a complete flexible nasopharyngolaryngoscopy,chest radiography, and barium esophagography may suffice for synchronous tumor assessment.
The results of one study found that the use of panendoscopy may help identify synchronous secondprimary tumors in patients with a history of tobacco use but not in nonsmoking patients. [2]
Examination under anesthesia is required for tumor mapping in most patients with SCCs of the softpalate, except for those with very small lesions. Patients with small tumors confined to the soft palate,with all boundaries visible, do not require examination under anesthesia. In these patients, a completeflexible nasopharyngolaryngoscopy and transoral inspection and palpation are adequate for tumor mapping.
Treatment
Specific treatment of palate cancer depends on the location of the tumor (hard vs soft palate), stage of thetumor (see Staging), and pathologic type of the cancer. For this reason, management of SCC andcarcinomas of minor salivary gland origin are discussed separately.
Treatment of T1-T2 squamous cell carcinoma of the hard palate
Surgery is the preferred treatment for SCC of the hard palate. However, megavoltage radiation has alsobeen used with some success as a viable alternative in treating patients with these tumors.
Small T1 and T2 lesions can be managed with either surgery or radiation therapy. Radiation therapy isgiven to a total dose of 60-70 Gy. The proximity of the tumor to the bone and potential complications of
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 6/13
osteoradionecrosis make radiation therapy less desirable for managing these lesions. On the other hand,surgery for these lesions is simple, with low morbidity and no loss of function.
For tumors that do not involve the periosteum or bone, through-and-through excision of the palate,opening the sinonasal fossa, is not necessary. For these lesions, a simple transoral excision into andincluding the periosteum is sufficient. A 1-cm margin is taken with the tumor. The periosteum serves asthe superior margin. The periosteum may be spared only in very superficial tumors that are not close to
the periosteum. This is an intraoperative decision. With surgical management, the 5-year survival ratesare 75% for stage I and 50% for stage II tumors.
In most cases, the defect from such lesions may be left open to heal by secondary intention andgranulation. Skin grafting is discouraged. Consider placing a palatal acrylic prosthesis (healing plate),which can be fabricated by a dentist or prosthodontist prior to resection. This helps protect the palatewound during the healing process. In some cases, palatal and/or buccal mucosal flaps are necessary torestore tissue deficiency, especially when dealing with patients’ postradiation therapy and/or those withlarger soft palate defects.[3]
Treatment of the neck in T1-T2 squamous cell carcinoma of the hard palate
Clinical and radiological N0 necks in these patients do not require elective treatment. When occult neckmetastasis is suggested, staging functional neck dissection (including levels 1, 2, and 3) is performed.Recently, a 27% rate of occult cervical metastasis was reported in a series of 26 patients with maxillaryalveolar ridge and hard palate squamous cell carcinoma. The authors thus suggest an elective neckdissection for such cancers with clinically N0 neck. [4] Other authors have suggested the use of sentinellymph node biopsy in such situations.[5]
Treatment of an N1 neck is controversial. A pathological N1 node is considered adequately treated withneck dissection alone when no extracapsular extension is present. However, in many centers, anypathological N1 node is treated with postoperative radiotherapy; this is recommended. Definitely initiatepostoperative radiation therapy for patients with extracapsular extension.
If the pathological stage of the neck is N2 or higher, initiate postoperative radiotherapy.
Treatment of T3-T4 squamous cell carcinoma of the hard palate
T3 and T4 lesions frequently require combined oncologic treatment, including surgery and radiationtherapy to both the primary site and the neck. N1 necks may be treated with radiotherapy or neckdissection. Necks that are N2 or higher are treated with planned combined surgery and radiotherapy.Larger palatal cancers have a poor prognosis and require multimodality oncologic therapy. Radiation isgiven using high-voltage equipment to a total of 60-70 Gy.
Importantly, when planning surgery for lesions that extend beyond the hard palate, determine the deficitthat will result from resection. Resection of the soft palate can cause significant velopharyngealinsufficiency. Because the soft palate is a dynamic structure, it is difficult to reconstruct. Lesions thatinvade the palatine bone require partial palatectomy, with resulting oroantral and oronasal fistula. Invasioninto the nasal cavity or the maxillary sinus requires inferior maxillectomy, partial maxillectomy, or totalmaxillectomy, depending on the extent of the lesion. Prosthetic rehabilitation is highly effective in thesepatients. However, use of vascularized free flaps, such as the scapular osteocutaneous flap or free fibula
osteocutaneous flap, are highly effective in functional as well as aestheticreconstruction and restoration of maxillary buttresses.[6, 7, 8]
Extension into the pterygopalatine and infratemporal fossa requires skull-base approaches to effectivelyextirpate the tumor.
Treatment of squamous cell carcinoma of the soft palate
Size, location, and contiguous spread of the primary tumor are important factors in the prognosis.Extension outside the palatine arch, especially to the base of the tongue, adversely affects patient
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 7/13
survival. Patients with midline tumors and tumors that extend across the palatine arch have poorer survival rates. This is because of a higher incidence of regional metastasis. Absence of the soft palateresults in velopharyngeal insufficiency, affecting both speech and swallowing.
Because of difficulties in adequate reconstruction, radiation therapy has been the recommendedtreatment for soft palate cancers in the past. Although advances in reconstructive techniques andprosthetic reconstruction have allowed for more effective surgical resection and rehabilitation for patients
with soft palate cancers, radiation therapy remains the primary treatment modality in many centers for T1,T2, and T3 lesions, with results comparable with those of surgery.
Using radiotherapy as the primary treatment, control of the primary lesion is achieved in 80-90% of T1lesions, 60-70% of T2 lesions, and 55-65% of T3 lesions. This rate drops to less than 50% for T4 lesions.Effective treatment for the primary lesion requires a dose of approximately 70 Gy.
Potential complications of radiotherapy include severe xerostomia, muscular fibrosis and resultanttrismus, osteoradionecrosis of the mandible, and soft tissue ulceration. Complications of radiotherapy arevolume dependent and dose dependent.
More recently, some centers prefer interstitial brachytherapy using iridium Ir 192 to boost the initialexternal beam of radiotherapy. The primary tumor is given 40-60 Gy of external beam radiation, followedby 20-40 Gy of brachytherapy. Boosting the primary tumor site to high doses allows improvedlocoregional control of the tumor, while reducing complications by avoiding wide-field, high-dose radiation.
Both radiotherapy and surgery are adequate for controlling early lesions. For advanced T3 and T4lesions, traditional external beam radiotherapy alone is associated with poor survival rates. As a result, for advanced stage III and IV tumors, a planned combined treatment, including surgical resection followed byradiation therapy to the primary tumor and the neck, is the recommended treatment.
An alternative is the use of chemotherapy combined with radiotherapy, followed by surgical resection.Cisplatin and 5-fluorouracil are the chemotherapeutic agents used. Chemotherapy may be given in 2-3cycles to assess the patient's response and to reevaluate. If the patient responds to chemotherapy,radiation is given for a full course of 70 Gy; surgery is reserved for salvage. Surgery is considered if thepatient responds poorly to the chemotherapy.
Chemotherapy may be given concomitantly with radiotherapy, reserving surgery for salvage. Administration of 5-fluorouracil can be performed as an intravenous bolus or continuous infusion over 72-120 hours. Doses range from 800-1200 mg/m2. For cisplatin, the usual dose is 60-100 mg/m2 every 3weeks. Accelerated fractionation radiotherapy has provided comparable disease-specific survival whencompared with concomitant chemoradiation (cisplatin) for locally advanced oropharyngeal stage III andIVA/B cancers, while yielding a lower rate of long-term dependency on gastric-tube feeding. Standardfractionation (hypofractionation) radiation is inferior to both accelerated fractionation and tochemoradiation in this group.[9]
Combined external beam radiation followed by brachytherapy is an alternative to surgery for themanagement of advanced lesions, reserving surgery for salvage.
Brachytherapy for tumors with bony invasion or in proximity of the mandible results in a high rate of osteoradionecrosis. These patients are best treated with planned surgical excision followed by external
beam radiotherapy, as are patients with tumor extension beyond the palatine arch into the base of thetongue.
Treatment of neck metastasis in soft palate squamous cell carcinoma
SCCs of the soft palate and uvula have a high rate of occult regional metastasis, as high as 20-30% atpresentation, even in early primary tumors. Therefore, definitive treatment must encompass regionallymphatics in all SCCs of the soft palate. In midline lesions or in those that cross the midline, the rate of bilateral metastasis is high, requiring treatment of both necks.
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 8/13
Tumor thickness is an excellent predictor of nodal metastasis in soft palate cancers. In one study, allpatients with tumors thicker than 3.12 mm had cervical metastasis, with tumor thickness correlating moredirectly with nodal metastasis than with T stage.
Clinical regional metastasis at presentation reduces the 5-year survival rate by half, from 80% in N0necks to 40% in necks with clinically evident metastasis. For small tumors treated primarily withradiotherapy, N0 and N1 necks can be controlled adequately with radiotherapy alone. For N2 and greater
neck metastasis, 74% of patients still have residual SCC following radiotherapy. Hence, treat N2 andgreater regional metastasis with planned combined therapy, including neck dissection followed byradiotherapy.
Treatment of minor salivary gland cancers of the palate
Seventy-four percent of minor salivary gland tumors are malignant (see the histologic types andfrequencies of minor salivary gland neoplasms of the palate in the Introduction section). The palate is themost common site for minor salivary gland carcinomas. Most of these occur in the hard palate. Minor salivary gland malignancies are divided into high- and low-grade tumors. High-grade tumors includeadenoid cystic carcinoma, high-grade mucoepidermoid carcinoma, high-grade adenocarcinoma,malignant mixed tumor, and carcinoma expleomorphic adenoma. Low-grade malignancies include low-grade mucoepidermoid carcinoma, polymorphous low-grade adenocarcinoma (with its propensity to occur
in the hard palate), acinic cell carcinoma, and other rare tumors.The most important poor prognostic factors for malignant minor salivary gland tumors of the palate aregrade 3 histology, tumor size larger than 3 cm, and positive margins.
Surgery is the mainstay of treatment for minor salivary gland tumors of the palate. For minor salivarygland tumors of the palate in which perineural invasion is suggested, identify and evaluate the greater palatine nerve by frozen section. If the nerve is involved, follow it with proximal resection until negativemargins are attained. If negative margins cannot be attained at the foramen rotundum, postoperativeradiation therapy must include the trigeminal ganglion.
Postoperative radiotherapy with or without chemotherapy is indicated for high-grade tumors, large T3 or T4 lesions, positive margins, tumors showing perineural invasion, and cervical lymph node metastasis.
Radiotherapy, possibly combined with chemotherapy, is used as the primary treatment if the patientrefuses surgery or is not a candidate for surgery because of extensive unresectable disease.
Cervical node metastasis is a rare event for salivary gland tumors of the palate, occurring inapproximately 3% of cases. Therefore, elective neck dissection is not indicated in these tumors in theabsence of clinical or radiological signs of nodal metastasis.
For adenoid cystic carcinoma, surgery followed by radiation therapy is the treatment of choice. Widesurgical margins are taken because this tumor is known for microscopic extension beyond the grosstumor margins. The propensity for perineural extension requires resection along the greater palatinenerves with frozen section control to achieve negative margins. Postoperative radiation is preferredbecause preoperative radiation therapy increases surgical complications.
Intraoperative DetailsTransoral approach
The transoral approach, as seen in the image below, provides adequate exposure for superficial tumorsof the hard palate that do not invade the bone. General anesthesia aids exposure and provides comfortfor the patient. The patient is placed in a supine position with the head extended.

7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 9/13
Transoral resection of a mucoepidermoid carcinoma of the palate.
A Dingman or Crockard mouth gag provides attachable cheek retractors to facilitate exposure as depictedin the image below.
Schematic per-oral approach to the palate using a Dingman mouth retractor.
Alternatively, a hard rubber bite block or a Denhardt gag may be used to retract the mouth open for exposure. The lesion is mapped with an adequate margin of 1 cm. A soft tissue incision is made with aknife or electrocautery device. Electrocautery reduces blood loss. Alternatively, the carbon dioxide laser provides adequate hemostasis and causes less tissue damage. The incision includes the periosteum if itis to be taken as the superior margin. Using a periosteal elevator, the periosteum is elevated under directvision, and the tumor is removed.
In cases in which the tumor involves the periosteum or the bone, the bone must be taken as the margin.This can be achieved using a cutting burr. If possible, preserve the superior mucoperiosteal coverage toprevent oronasal fistula, although this may be difficult. A prosthetic device is highly effective for swallowing and speech rehabilitation.
In cases in which the tumor is lateral and involves the alveolar ridge, a partial alveolectomy is includedwith palate resection. To improve exposure, a buccogingival sulcus incision is made to the level of theanterior maxillary wall. A facial degloving approach is used to improve exposure. The infraorbital nerve ispreserved. An opening is made into the maxillary antrum to expose the superior surface of the palate.Following soft tissue incisions, bony cuts are made as needed using a Stryker saw, and the tumor isremoved. Exposed soft tissue surfaces are covered with a split-thickness skin graft, except for closedcavities. Immediate prosthetic rehabilitation is performed with the aid of the prosthodontist whopreoperatively prepared the temporary prosthetic device.
For extensive tumors of the hard palate involving the hard palate bilaterally, a total palatectomy andinferior bilateral maxillectomy is required. These resections leave the patient with extensive midfacial
defects involving the palate, upper jaw, and sinuses. Flap and graft reconstruction of these defects isfraught with difficulty, often resulting in breakdown, which leads to oroantral or oronasal fistula. A totalmidfacial prosthetic rehabilitation is highly effective for restoring deglutition, speech, and facial contour and for making the postoperative surgical bed easier to monitor.
In cases of soft palate cancer, very small mucosal lesions may be resected transorally with preservationof the superior mucosa. If the defect is close to the hard palate, an advancement rotation flap from thehard palate may be used to close the defect. Small defects at the posterior margin of the soft palate maybe closed by approximating the superior and inferior mucosa. The resulting velopharyngeal insufficiencycorrects over time. A superiorly based pharyngeal flap may be used to close the defect.
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 10/13
Mandibulotomy
A mandibular approach provides wide exposure for resection of T4 soft palate cancers extending to thehard palate, lateral pharynx, tonsil, base of tongue, and/or mandible. A visor flap or lip-splitting neckincision may be used. A horizontal incision is made from the mastoid tip to the submentum. The lip is splitwith a stair-step cut along the vermilion to prevent lip notching, and a Z incision is carried over thementum to join the submental incision. The periosteum is raised on either side of the incision. A
parasymphysial stair-step osteotomy is made in a way that preserves the anterior muscular attachmentsof the mandible in the opposite side.
Once the position of the osteotomy is determined, mandibular miniplates are bent to adapt to the contour of the mandible for mandibular plating at the end. An incision is made in the floor of the mouth from thelabiogingival sulcus to the anterior resection margin. The mylohyoid muscle is cut. This allows themandible to swing open. Excellent exposure is provided to the entire soft palate and oropharynx.
If no mandibular bony invasion is noted based on preoperative imaging studies, the periosteum is raisedas the margin. Relevant soft tissue cuts are made around the tumor, and it is removed. If invasion of thehard palate or the upper alveolus is noted, osteotomies are made using a Stryker saw following adequatesoft tissue cuts. This exposure allows for an inferior maxillectomy. Give attention to assessing invasion of the medial pterygoid muscle, and, if invaded, take adequate deep margins. In irradiated patients or when
a chance for composite resection of the mandible exists, a lateral mandibulotomy is preferred. The site of the cut varies depending on the exact extent of the tumor. A visor flap can be used, obviating the need for lip splitting.
Reconstruction of the soft palate
A basic hard palate prosthesis can be designed with extension into the oropharynx. When a posterior functioning band of soft palate is preserved, the obturator extension sits in the defect. During swallowing,the posterior band raises against the obturator. For total soft palate defects, the posterior extension of theobturator sits in the oropharynx anterior to the pharyngeal constrictor. During swallowing, the superior constrictor is raised against this static prosthesis to achieve velopharyngeal closure.
For extensive defects of the soft palate and lateral pharyngeal wall with an exposed mandible,vascularized soft tissue reconstruction is mandatory. This is especially important for patients who are
irradiated. The temporalis muscle or musculofascial flap is reliable and readily available for reconstruction. It allows complete reconstruction of the soft palate and provides coverage for the lateralpharyngeal defect and exposed mandible. It may be combined with a superiorly based pharyngeal flap for a double-layer closure of the palate. A dermal graft is used to cover the muscle if it is not covered byfascia.
Microvascular radial forearm fasciocutaneous free-flap reconstruction is another alternative for total softpalate reconstruction.
Follow-upFor excellent patient education resources, visit eMedicineHealth's Cancer Center . Also, seeeMedicineHealth's patient education article Cancer of the Mouth and Throat.
ComplicationsComplications of surgical resection of the soft palate may include (1) velopharyngeal insufficiency (mostcommon), (2) hypernasal speech, (3) dysphagia, and (4) middle ear effusion from scarring at theeustachian tube opening or loss of function of tensor and/or levator palatini muscles.
Obviously, the extent of and potential for these complications depend on the extent of resection, the sizeof the defect, and the method of reconstruction. The larger the resection and the defect, the greater thechance for these complications. The soft palate is a dynamic structure; optimal functioning requiresmuscular action to elevate and tense it during deglutition and relax it during nasal respiration. Therefore,
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 11/13
any reconstruction of the soft palate with flaps and prosthetics does not reproduce its function; it will belimited in function in the best of circumstances.
Complications from hard palate resection depend on the extent of resection. For soft tissue resection withpreservation of the bony palate and soft palate only, the resulting defect heals with granulation andepithelialization, and no complications are expected. If patients had previous radiation therapy to the area,healing may be delayed.
For more extensive resection that results in oroantral or oronasal defects, oronasal and oroantral fistulasmay develop. Small defects may be closed with local flaps from the rest of the hard palate or from thebuccal mucosa. Larger defects are managed adequately and effectively with obturators. Because theorgan is not dynamic, obturators are very effective and well tolerated.
Outcome and PrognosisIn the last 5 years, inclusion of quality of life (QOL) measures in the treatment decisions for head andneck cancer have become important. Oropharyngeal cancers that include the soft palate are an area of active clinical research, using QOL as an outcome measurement. With combined modalities of treatmentincluding surgery and radiotherapy or chemoradiation, both being comparable in cure rates for advancedcancers, predicted QOL becomes an important consideration to help make treatment decisions.[10]
Future and ControversiesElective treatment of the clinically negative neck in head and neck cancer versus observation andsubsequent treatment of those who develop neck metastasis remains a subject of controversy. Recentretrospective data suggest that the rate of occult neck disease (pN1) in N0 patients receiving meticulousworkup is low. Close observation with later treatment reserved for subsequent neck disease producesstatistically similar survival rates to the elective prophylactic treatments and may be a valid form of treatment. Current literature, however, lacks clinical evidence to answer this question.
1. Yang Z, Deng R, Sun G, Huang X, Tang E. Cervical metastases from squamous cell carcinoma
of hard palate and maxillary alveolus: A retrospective study of 10 years. Head Neck . Jun 4 2013;[Medline].
2. Rodriguez-Bruno K, Ali MJ, Wang SJ. Role of panendoscopy to identify synchronous second
primary malignancies in patients with oral cavity and oropharyngeal squamous cellcarcinoma. Head Neck . Jul 2011;33(7):949-53. [Medline].
3. Stassen L, Khosa AD, Israr M. The value of the 'buccal pad of fat' in the reconstruction of oral
defects following removal of intraoral tumours--a clinical assessment. Ir Med J . Jan2013;106(1):13-5. [Medline].
4. Simental AA Jr, Johnson JT, Myers EN. Cervical metastasis from squamous cell carcinoma of the
maxillary alveolus and hard palate. Laryngoscope. Sep 2006;116(9):1682-4. [Medline].
5. Sanchez-Fernandez JM, Santaolalla-Montoya F, Sanchez-del Rey A, et al. In reference to:
"Cervical metastasis from squamous cell carcinoma of the maxillary alveolus and hardpalate.". Laryngoscope. Mar 2007;117(3):565-6; author reply 566. [Medline].
6. Germain MA, Hartl DM, Marandas P, et al. Free flap reconstruction in the treatment of tumors
involving the hard palate. Eur J Surg Oncol . Apr 2006;32(3):335-9. [Medline].
7. Genden EM, Wallace DI, Okay D, et al. Reconstruction of the hard palate using the radial forearm
free flap: indications and outcomes. Head Neck . Sep 2004;26(9):808-14. [Medline].
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 12/13
8. Yamamoto Y, Kawashima K, Sugihara T, et al. Surgical management of maxillectomy defects
based on the concept of buttress reconstruction. Head Neck . Mar 2004;26(3):247-56. [Medline].
9. Kader HA, Mydin AR, Wilson M, et al. Treatment outcomes of locally advanced oropharyngeal
cancer: a comparison between combined modality radio-chemotherapy and two variants of singlemodality altered fractionation radiotherapy. Int J Radiat Oncol Biol Phys. Jul 15 2011;80(4):1030-
6. [Medline].
10. Eskander A, Givi B, Gullane PJ, Irish J, Brown D, Gilbert RW, et al. Outcome predictors in
squamous cell carcinoma of the maxillary alveolus and hard palate. Laryngoscope. Apr 1 2013;[Medline].
11. Blot WJ, Winn DM, Fraumeni JF Jr. Oral cancer and mouthwash. J Natl Cancer Inst . Feb
1983;70(2):251-3. [Medline].
12. Chung CK, Constable WC. Squamous cell carcinoma of the soft palate and uvula. Int J Radiat
Oncol Biol Phys. Jun 1979;5(6):845-50. [Medline].
13. Chung CK, Johns ME, Cantrell RW, et al. Radiotherapy in the management of primary
malignancies of the hard palate. Laryngoscope. Apr 1980;90(4):576-84. [Medline].
14. Chung CK, Rahman SM, Lim ML, et al. Squamous cell carcinoma of the hard palate. Int J Radiat
Oncol Biol Phys. Feb 1979;5(2):191-6. [Medline].
15. Duvvuri U, Simental AA Jr, D'Angelo G, et al. Elective neck dissection and survival in patients
with squamous cell carcinoma of the oral cavity and oropharynx. Laryngoscope. Dec2004;114(12):2228-34.[Medline].
16. Evans JF, Shah JP. Epidermoid carcinoma of the palate. Am J Surg . Oct 1981;142(4):451-
5. [Medline].
17. Gillespie MB, Brodsky MB, Day TA, et al. Swallowing-related quality of life after head and neck
cancer treatment. Laryngoscope. Aug 2004;114(8):1362-7. [Medline].
18. Gluckman JL. Synchronous multiple primary lesions of the upper aerodigestive system. Arch
Otolaryngol . Oct 1979;105(10):597-8. [Medline].
19. Graham S, Dayal H, Rohrer T, et al. Dentition, diet, tobacco, and alcohol in the epidemiology of
oral cancer. J Natl Cancer Inst . Dec 1977;59(6):1611-8. [Medline].
20. Hollinshead WH. Anatomy for Surgeons. In: The Head and Neck . 3rd ed. Philadelphia, Pa:
Lippincott Williams & Wilkins; 1982:331-45.
21. Jaques DA. Epidermoid carcinoma of the palate. Otolaryngol Clin North Am. Feb 1979;12(1):125-
8.[Medline].
22.Keus RB, Pontvert D, Brunin F, et al. Results of irradiation in squamous cell carcinoma of the softpalate and uvula. Radiother Oncol . Apr 1988;11(4):311-7. [Medline].
23. Layland MK, Sessions DG, Lenox J. The influence of lymph node metastasis in the treatment of
squamous cell carcinoma of the oral cavity, oropharynx, larynx, and hypopharynx: N0 versusN+. Laryngoscope. Apr 2005;115(4):629-39. [Medline].
24. Leemans CR, Engelbrecht WJ, Tiwari R, et al. Carcinoma of the soft palate and anterior tonsillar
pillar.Laryngoscope. Dec 1994;104(12):1477-81. [Medline].
7/27/2019 Background MED SCAPE
http://slidepdf.com/reader/full/background-med-scape 13/13
25. Leipzig B, Zellmer JE, Klug D. The role of endoscopy in evaluating patients with head and neck
cancer. A multi-institutional prospective study. Arch Otolaryngol . Sep 1985;111(9):589-94. [Medline].
26. Mahboubi E. The epidemiology of oral cavity, pharyngeal and esophageal cancer outside of North
America and Western Europe. Cancer . Oct 1977;40(4 Suppl):1879-86. [Medline].
27. Martin JW, Chambers MS, Fleming TJ. Prosthetic rehabilitation of the nasal and paranasal sinus
area. In: Thawly SE, Panje WR, Batsakis JG, Lindberg RD, eds. Comprehensive Management .Vol 1. Philadelphia, Pa: WB Saunders; 1999:608-23.
28. Panje WR, Morris MR. Surgery of oral cavity, tongue, and oropharynx. In: Naumann HH, Helms J,
Herberhold C, Jahrsdoerfer RA, Kastenbauer ER, Panje WR, Tardy Jr ME, eds. Head and Neck Surgery . Pt 2. Vol 1. New York, NY: Thieme; 1995:739-53.
29. Pernot M, Malissard L, Hoffstetter S, et al. Influence of tumoral, radiobiological, and general
factors on local control and survival of a series of 361 tumors of the velotonsillar area treated byexclusive irradiation (external beam irradiation+brachytherapy or brachytherapy alone). Int J Radiat Oncol Biol Phys. Dec 1 1994;30(5):1051-7. [Medline].
30. Petruzzelli GJ, Myers EN. Malignant neoplasms of the hard palate and upper alveolar ridge. Oncology (Huntingt). Apr 1994;8(4):43-8; discussion 50, 53. [Medline].
31. Russ JE, Applebaum EL, Sisson GA. Squamous cell carcinoma of the soft palate. Laryngoscope.
Jul 1977;87(7):1151-6. [Medline].
32. Tschudi D, Stoeckli S, Schmid S. Quality of life after different treatment modalities for carcinoma
of the oropharynx. Laryngoscope. Nov 2003;113(11):1949-54. [Medline].
33. Weber RS, Peters LJ, Wolf P, et al. Squamous cell carcinoma of the soft palate, uvula, and
anterior faucial pillar. Otolaryngol Head Neck Surg . Jul 1988;99(1):16-23. [Medline].
34. Wynder EL, Kabat G, Rosenberg S, et al. Oral cancer and mouthwash use. J Natl Cancer Inst .
Feb 1983;70(2):255-60. [Medline].





























