-
DEFINITIONDiabetes mellitus (DM) refers to a syndrome of
hyperglycemia resulting from many different causes. It can be
classi ed into type 1 (formerly insulin-dependent diabetes mellitus
[IDDM]) and type 2 (formerly noninsulin-dependent diabetes mellitus
[NIDDM]). Because insulin-dependent and noninsulin-dependent refer
to the stage at diagnosis, when a type 2 diabetic needs insulin, he
or she remains classi ed as type 2 and does not revert to type
1.
The American Diabetes Association (ADA) de nes DM as (1) a
fasting plasma glucose 126 mg/dL, (2) a nonfasting plasma glucose
200 mg/dL, or (3) glucose 200 mg/dL in the 2-hour sample in an oral
glucose tolerance test (OGTT). Fur-thermore, a value of 100 mg/dL
of fasting blood sugar is the upper limit of normal for glucose. A
fasting glucose between 100 and 126 mg/dL is classi ed as impaired
fasting glucose (IFG). CAUSEIdiopathic diabetes
TYPE 1 DIABETES MELLITUS Hereditary factors1. Islet cell
antibodies (found in 90% of patients within the rst year of
diagnosis)2. Higher incidence of HLA types DR3, DR43. 50%
concordance in identical twins Environmental factors: viral
infection (possibly coxsackie virus, mumps virus)TYPE 2 DIABETES
MELLITUS Hereditary factors: 90% concordance in identical twins
Environmental factor: obesity
Diabetes secondary to other factors Hormonal excess: Cushings
syndrome, acromegaly, glu-cagonoma, pheochromocytoma Drugs:
glucocorticoids, diuretics, oral contraceptives Insulin receptor
unavailability (with or without circulat-ing antibodies) Pancreatic
disease: pancreatitis, pancreatectomy, hemo-chromatosis Genetic
syndromes: hyperlipidemias, myotonic dystro-phy, lipoatrophy
Gestational diabetes
DIFFERENTIAL DIAGNOSIS Diabetes insipidus Stress hyperglycemia
Diabetes secondary to hormonal excess, drugs, pancreatic
disease
PHYSICAL FINDINGS AND CLINICAL PRESENTATION Physical examination
varies with the presence of complica-
tions and may be normal in early stages. Diabetic
retinopathy
Nonproliferative (background diabetic retinopathy)1. Initially:
microaneurysms (Fig. 2851), capillary dilation, waxy or hard
exudates, dot and ame hemorrhages (Fig. 2852), arteriovenous (AV)
shunts
2. Advanced stage: microinfarcts with cotton-wool exudates,
macular edema Proliferative retinopathy: characterized by formation
of new vessels (Fig. 2853), vitreal hemorrhages, brous scar-ring,
and retinal detachment
Cataracts and glaucoma occur with increased frequency in
diabetics.
Peripheral neuropathy: patients often complain of paresthe-sias
of extremities (feet more than hands); the symptoms are
symmetrical, bilateral, and associated with intense burn-ing pain
(particularly during the night). Mononeuropathies involving cranial
nerves III, IV, and VI, intercostal nerves, and femoral nerves are
also common. Physical examination may reveal the following:
916
285 Section 11: Endocrine and metabolic disorders
Chapter 285 Diabetes mellitus
A
B
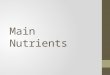
Fig 2851Nonproliferative diabetic retinopathy with
microaneurysms. A, Small dot hemorrhages, microaneurysms, hard
(lipid) exudates, circinate retinop-athy, an intraretinal
microvascular abnormality, and macular edema. B, Fluorescein
angiography of the eye shown in A. Microaneurysms are seen as
multiple dots of hyper uorescence, but the dot hemorrhages do not
uoresce. The foveal avascular zone is minimally enlarged.(From
Yanoff M, Duker JS: Ophthalmology, 2nd ed. St. Louis, Mosby,
2004.)
DISORDERS OF CARBOHYDRATE AND LIPID METABOLISM
Ch263-288_X4919_853-930.indd 916 10/10/08 12:26:37 PM
-
917
Chapter 285: Diabetes mellitus 285
Retinalhemorrhages
Cottonwool spots
Fig 2852Background diabetic retinopathy with cotton-wool spots
and retinal hemorrhages.(Courtesy of Dr. James Tiedeman.)
Fig 2853Neovascularization. A, Neovascularization of the disc
with some brous proliferation. B, Neovascularization
elsewhere.(From Yanoff M, Duker JS: Ophthalmology, 2nd ed. St.
Louis, Mosby, 2004.)
A
B
1. Decreased pinprick sensation, sensation to light touch, and
pain sensation2. Decreased vibration sense3. Loss of proprioception
(leading to ataxia)4. Motor disturbances (decreased DTR, weakness
and atro-phy of interossei muscles). When the hands are affected,
the patient has trouble picking up small objects, dressing, and
turning pages in a book.5. Diplopia, abnormalities of visual
elds
Autonomic neuropathy GI disturbances: esophageal motility
abnormalities, gas-troparesis, diarrhea (usually nocturnal) GU
disturbances: neurogenic bladder (hesitancy, weak stream, and
dribbling), impotence Orthostatic hypotension: postural syncope,
dizziness, light-headedness
Nephropathy: pedal edema, pallor, weakness, uremic ap-pearance.
Diabetic kidney changes are described in Figure 2854. Early
diabetic glomerulopathy is shown in Figure 2855.
Foot ulcers (Fig. 2856): occur in 15% of diabetics (an-nual
incidence, 2%) and are the leading causes of hospi-talization. They
are usually secondary to peripheral vascu-
lar insuf ciency, repeated trauma (unrecognized because of
sensory loss), and superimposed infections often lead-ing to
gangrene (Fig. 2857). If a diabetic foot ulcer has been present for
weeks and foot pulses are palpable, neu-ropathy should be
considered a major cause. Neuropathy can be detected with a simple
examination of the lower extremities using a 10-g mono lament to
test sensation. Prevention of foot ulcers in diabetics includes
strict glu-cose control, patient education, prescription foot wear,
intensive podiatric care, and evaluation for surgical
inter-ventions.
Neuropathic arthropathy (Charcots joints): bone or joint
deformities (Fig. 2858) from repeated trauma (secondary to
peripheral neuropathy).
Necrobiosis lipoidica diabeticorum: plaquelike reddened ar-eas
with a central area that fades to white-yellow found on the
anterior surfaces of the legs. In these areas, the skin be-comes
very thin and can ulcerate readily (Fig. 2859).
LABORATORY TESTS Diagnosis is made on the basis of the following
tests and
should be con rmed by repeated testing on a different day:1.
Fasting glucose 126 mg/dL (ADA criterion)2. Nonfasting plasma
glucose 200 mg/dL
Ch263-288_X4919_853-930.indd 917 10/10/08 12:26:39 PM
-
918
285 Section 11: Endocrine and metabolic disorders
Fig 2855Early diabetic glomerulopathy with slight
hypercellularity and a mild increase in the mesangial matrix
(H&E).(Courtesy of Dr. Benjamin Sturgill.)
Glomerulus
Increasedcellularityand mildincreasein matrix
Normal glomerulus Basement membrane thickening
Mesangial proliferation Nodular sclerosis
Diabetic changes in the kidney
Bowman'scapsule
Afferentarteriole Efferent
arteriole
Mesangium
Expandedmesangium
Fig 2854Diabetic changes in the kidney. Illustrated here are the
progressive changes in the renal glomerular architecture that occur
in the diabetic kidney.(From Besser CM, Thorner MO: Comprehensive
Clinical Endocrinology, 3rd ed. St. Louis, Mosby, 2002.)
Ch263-288_X4919_853-930.indd 918 10/10/08 12:26:45 PM
-
919
Chapter 285: Diabetes mellitus 285
Fig 2856Neuropathic plantar ulcer in diabetic
osteoarthropathy.(From Hochberg MC, Silman AJ, Smolen JS, et al
[eds]: Rheumatology, 3rd ed. St. Louis, Mosby, 2003.)
Fig 2857Diabetic gangrene.(From Swartz MH: Textbook of Physical
Diagnosis, 5th ed. Philadelphia, WB Saunders, 2006.)
A B
Fig 2858Diabetic osteoarthropathy. A, Fragmentation and severe
osteolysis on the articular surfaces of the rst metatarsophalangeal
joint. B, The pro-cess has healed, with moderate deformation of the
articular surfaces.(From Hochberg MC, Silman AJ, Smolen JS, et al
[eds]: Rheumatology, 3rd ed. St Louis, Mosby, 2003.)
Fig 2859Necrobiosis lipoidica. Shown is a chronic lesion with
ulceration and crusting.(Courtesy of the Institute of Dermatology,
London.)
Use of glycosylated hemoglobin (HbA1c) level is generally not
recommended for diagnosis because of lack of standard-ization of
HbAlc values and the imperfect correlation be-tween HbAlc and
fasting plasma glucose levels. However, some physicians use this
test to make the diagnosis of dia-betes mellitus if the random
plasma glucose is 200 mg/dL and the HbAlc level is 2 SDs (standard
deviations) above the laboratory mean.
Screening for diabetic nephropathy by measuring
microalbu-minuria is recommended in all patients with diabetes. It
can be accomplished by any of the following three methods:1.
Measurement of the albumin-to-creatinine ratio in ran-dom spot
urine collection. This is the easiest method to administer in the
of ce setting because it is an easy assay to perform in most
laboratories; the physician simply orders Urine for microalbumin
level.
2. Measurement of a 24-hour urine collection for albumin,
creatinine clearance3. Timed (4-hour or overnight) urine
collection
The diagnosis of microalbuminuria should be based on two or
three elevated levels within a 3- to 6-month period because there
is a marked variability in daily albumin excretion and possible
transient elevations in urine albumin from short-term
hyperglycemia, exercise, severe hypertension, and other illnesses,
such as sepsis and CHF. Patients with overt ne-phropathy do not
need screening for microalbuminuria
Ch263-288_X4919_853-930.indd 919 10/10/08 12:26:49 PM
-
920
285 Section 11: Endocrine and metabolic disordersbecause the
level of protein in the urine is high enough to be detected on
routine urinalysis.
A fasting serum lipid panel, serum creatinine, and electro-lytes
should be obtained annually on all adult diabetic patients.
TREATMENT Diet
Calories1. The diabetic patient can be started on 15 cal/lb of
ideal body weight; this can be increased to 20 cal/lb for an
ac-tive person and 25 cal/lb if the patient does heavy physical
labor.2. The calories should be distributed as 50% to 60%
carbo-hydrates, less than 30% fat, with saturated fat limited to
less than 10% of total calories, and 15% to 20% protein.3. The
emphasis should be on complex carbohydrates rather than simple and
re ned starches and on polyunsaturated instead of saturated fats in
a ratio of 2:1. Seven food groups1. The exchange diet of the ADA
includes protein, bread, fruit, milk, and low- and
intermediate-carbohydrate vegetables.2. The name of each exchange
is meant to be all-inclusive (e.g., cereal, muf ns, spaghetti,
potatoes, rice are in the bread group; meats, sh, eggs, cheese,
peanut butter are in the protein group).3. The glycemic index
compares the rise in blood sugar after the ingestion of simple
sugars and complex carbohydrates with the rise that occurs after
the absorption of glucose. Equal amounts of starches do not produce
the same in-crease in plasma glucose (pasta equal in calories to a
baked potato causes less of an increase than the potato). Thus, it
is helpful to know the glycemic index of a particular food
product.4. Fiber: insoluble ber (bran, celery) and soluble globular
ber (pectin in fruit) delay glucose absorption and attenu-ate the
postprandial serum glucose peak. They also appear to lower the
elevated triglyceride level often present in un-controlled
diabetics. A diet high in ber should be empha-sized (20 to 35 g/day
of soluble and insoluble ber). Other principles1. Modest sodium
restriction to 2400 to 3000 mg/day. If hypertension is present,
restrict to less than 2400 mg/day; if nephropathy and hypertension
are present, restrict to less than 2000 mg/day.2. Moderation of
alcohol intake (two drinks or less/day in men, one drink/day or
less in women)3. Non-nutritive arti cial sweeteners are acceptable
in mod-erate amounts.
Exercise increases the cellular glucose uptake by increasing the
number of cell receptors. The following points must be considered:
Exercise program must be individualized and built up slowly.
Insulin is more rapidly absorbed when injected into a limb that is
then exercised; this can result in hypoglycemia.
Weight loss: to ideal body weight if the patient is
over-weight
Screenings for nephropathy, neuropathy, and retinopathy When the
previous measures fail to normalize the serum
glucose, oral hypoglycemic agents (e.g., metformin, gli-tazones,
or a sulfonylurea) should be added to the regimen in type 2 DM. The
sulfonamides and the biguanide metfor-min are the oldest and most
commonly used classes of hy-poglycemic drugs. Metformins primary
mechanism is to decrease hepatic glucose output. Because metformin
does not produce hypo-glycemia when used as a monotherapy, it is
preferred for most patients. It is contraindicated for patients
with renal insuf ciency. Sulfonylureas and repaglinide work best
when given be-fore meals because they increase the postprandial
output of insulin from the pancreas. All sulfonylureas are
contraindi-cated for patients allergic to sulfa. Acarbose and
miglitol work by competitively inhibiting pancreatic amylase. Small
intestine glucosidases delay gas-trointestinal absorption of
carbohydrates, thereby reducing alimentary hyperglycemia. The major
side effects are atu-lence, diarrhea, and abdominal cramps.
Pioglitazone and rosiglitazone increase insulin sensitivity and are
useful in addition to other agents in type 2 diabetics whose
hyperglycemia is inadequately controlled. Serum transaminase levels
should be determined before starting therapy and monitored
periodically. Insulin is indicated for the treatment of all type 1
and type 2 DM patients who cannot be adequately controlled with
diet and oral agents. Pramlintide (Symlin), a synthetic analogue of
human amylin (a hormone synthesized by pancreatic beta cells and
cosecreted with insulin in response to food intake), can be used as
an adjunctive treatment for patients with type 1 or type 2 DM who
inject insulin at mealtime. Exenatide (Byetta), a synthetic peptide
that stimulates release of insulin from pancreatic beta cells, can
be used as adjunctive therapy for patients with type 2 DM. It is
not indicated in type 1 DM and is contraindicated in patients with
severe renal impairment. Combination therapy of various
hypoglycemic agents is commonly used when monotherapy results in
inadequate glycemic control. Continuous subcutaneous insulin
infusion (CSII, or in-sulin pump) provides better glycemic control
than conven-tional therapy and comparable with or slightly better
con-trol than multiple daily injections. It should be considered
for diabetes presenting in childhood or adolescence and during
pregnancy. Low-dose aminosalicylic acid (ASA) to decrease the risk
of cerebrovascular disease is bene cial for diabetics older than 30
years with other risk factors (hypertension, dyslip-idemia,
smoking, obesity). Strict lipid control (low-density lipoprotein
[LDL] 70 mg/dL) is indicated for all diabetics. Use of statins is
usually necessary to achieve therapeutic goals.
Ch263-288_X4919_853-930.indd 920 10/10/08 12:26:54 PM



![MAIN 24 Fi – 24 i SPARE PARTS CATALOGUEel]file.pdf · MAIN 24 Fi - i 1/10/04 BSB43624X650-MAIN 24 FIBSB43624X651-MAIN 24 FI BSB43224X650-MAIN 24 iBSB43224X651-MAIN 24 i X=1->LPG](https://img.pdfslide.us/doc/110x75/60839f3823da25701d2df967/main-24-fi-a-24-i-spare-parts-catalogue-elfilepdf-main-24-fi-i-11004-bsb43624x650-main.jpg)