Embed Size (px)
Citation preview

19
Building Trustworthy RelationshipsWith Critically Ill Patients and Families
AACN Advanced Critical CareVolume 18, Number 1, pp.19–30
© 2007, AACN
Cynda Hylton Rushton, PhD, RN, FAAN
Michelle L. Reina, PhD
Dennis S. Reina, PhD
The Case*
Mr Nelson is a 59-year-old man who has had acoronary artery bypass surgery and mitralvalve replacement. His medical history is sig-nificant for diabetes and peripheral vasculardisease. Preoperatively, Mr Nelson was alertand cared for himself. He had written a med-ical directive that designated his wife of 30years as his healthcare agent and stated that hedid not want to live “hooked up to machines.”Mr Nelson has 3 adult children, 2 daughterswho live locally on the East Coast and a sonwho lives on the West Coast.
Mr Nelson’s postoperative course was com-plicated by failure to wean from the ventilator,which required a tracheostomy for long-termmanagement. He has had 3 episodes of sepsis
and has developed methicillin-resistantStaphylococcus aureus sepsis. He is fed viacontinuous-infusion jejunal feedings.
Mr Nelson has now been in the intensivecare unit (ICU) for more than 5 months; multi-ple physicians have led the team, each with dif-ferent decision-making and communicationstyles. In team discussions, the primary criticalcare team members and consultants agree thatMr Nelson’s prognosis is poor and that his res-piratory and cardiac failure is irreversible. A
A difficult case study involving repeatedhealth crises and irreversible organ dys-function illustrates the challenges criticalcare professionals face in caring for patientsand their families. In such cases, trust is es-pecially fragile, and coexists with its coun-terpart, betrayal. The Reina Trust & BetrayalModel defines 3 types of TransactionalTrust. The first, Competence Trust, or theTrust of Capability, requires that clinicianspractice humility, engage in inquiry, honorthe patient’s choices, and express compas-sion. The second, Contractual Trust, or theTrust of Character, demands that clinicians
keep agreements, manage expectations,establish boundaries, and encouragemutually serving expectations. The third,Communication Trust, or the Trust of Disclo-sure, must be rooted in respect and basedon truth-telling. Particularly in life-and-death situations, communication requireshonesty and clarity. Each type of trustinvolves specific behaviors that build trustand can guide critical care professionals as they interact with patients and theirfamilies.Keywords: building trust, critical care,provider-patient relationships, trust models
A B S T R A C T
Cynda Hylton Rushton is from the School of Nursing and theChildren’s Center, Johns Hopkins University, 525 N Wolfe St,Box 420, Baltimore, MD 21205 (e-mail: [email protected]).
Michelle L. Reina is from the Reina Trust Building Institute,Stowe, Vt.
Dennis S. Reina is from the Reina Trust Building Institute,Stowe, Vt.
*This case is hypothetical and based on clinical experience.Any relationship of this case to actual cases is coincidental.

RUSHTON ET AL AACN Advanced Cri t ical Care
20
few physicians regularly inform the family ofthe treatment plans while others negotiate vari-ous aspects of the plan with the family. More-over, although some physicians skillfully com-municate about prognosis and goal setting,others are indirect and evasive and inadver-tently create expectations for unlikely out-comes. As a result, the family questions thegoals of care and the healthcare team’s commit-ment to aggressively treat Mr Nelson.
In the ICU, Mr Nelson has been intermit-tently confused and lucid. While confused, hetries to remove his tubes and disconnect him-self from the ventilator. While lucid, he writeson a message board that he wants to be takenoff the ventilator and be allowed to die. Eachtime he has expressed these wishes, his wifeand children insist that they want all support tocontinue and “everything” done. Mrs Nelsonhas said repeatedly that he “does not knowwhat he is saying” and that she cannot believethat he does not want to live. When remindedof his medical directive, she becomes angrystating that she is responsible for treatment de-cisions and that she cannot allow him to die.
Mr Nelson has experienced 3 acute deterio-rations in his health. Each time, the healthcareteam called the family together because theythought that Mr Nelson was dying; each timehe did not. The healthcare team has made mul-tiple attempts to communicate his poor prog-nosis to his family. Although Mr Nelson’s wifeand daughters admit that he would not wantto live in this condition, his son actively resistsany suggestions about limiting aggressive care.Mr Nelson’s wife is vigilant at his bedside, of-ten questioning the reasons for medicationsand procedures. Although pleasant, she ap-pears agitated and distrustful at times, repeat-edly stating that the team has “given up” onher husband. Over the course of her husband’sstay in the ICU, Mrs Nelson has withdrawnfrom her interactions with the healthcare teamand now refuses to discuss her husband’s carewith anyone who suggests limiting treatment.
IntroductionThe purpose of this article is to examine howtrust models can help clinicians better meet MrNelson’s needs and the needs of his family. Themodel for Transactional Trust is introducedand 3 types of trust are described. Ways to as-sess and rebuild trust with Mr Nelson’s wifeand son, who have grown to distrust the careteam, are examined.
TrustBroadly speaking, trust is “confidence in andreliance upon others, whether individuals,professionals, or organizations, to act in ac-cord with accepted social, ethical, and legalnorms.”1 In the critical care setting, trust mustbe present in each encounter with patients andfamilies, among interdisciplinary healthcareprofessionals, and across all levels of thehealthcare organization to achieve optimal pa-tient outcomes2 and create a healthy work en-vironment.3 Under conditions of great vulner-ability such as Mr Nelson’s critical illness,trust becomes especially fragile.
Trust and betrayal are 2 dichotomous forcesthat affect the quality of relationships at the in-terpersonal and intrapersonal, team, and orga-nizational levels.4 These 2 forces coexist inhuman interactions and are considered fun-damental to developing and maintaining rela-tionships, achieving outcomes and goals, andensuring the integrity of individuals, processes,and structures. Healthcare organizations, forexample, demonstrate their trustworthiness byputting into place integrated systems with aclinical, educational, and administrative infra-structure that can enable healthcare profession-als to practice in accord with professionalcompetencies to achieve the desired patientoutcomes.
Trust is built incrementally and earned be-haviorally.4–6 While individuals may claim thatthey value trust, it is only their behavior that actually builds it. A person’s capacity for trust refers to a readiness and willingnessto trust oneself and others; thus, trust is influ-enced by perceptions, beliefs, and expectationsof oneself and others.4,7 A person’s capacityfor trust expands or contracts, depending onpositive or negative experiences and percep-tions of reality in a particular situation.4 Fortrust to expand, participants in a relationshipinteract with each other with unguarded hon-esty, openness, and authenticity. An expressionof their capacity for trust, trustworthy behav-iors are an outgrowth of conscious or uncon-scious choices and depend on a person’s levelof awareness, readiness, and willingness.4
Betrayal often coexists with fear, anger, dis-engagement, disrespectfulness, or untrustwor-thy behavior. Betrayal is defined as an actualor perceived breach of trust and can be inten-tional or unintentional.4 Actual or perceivedbetrayal diminishes the capacity for trust.How individuals respond to perceived betrayal

21
VOLUME 18 • NUMBER 1 • JANUARY–MARCH 2007 BUILDING TRUST
is, in part, determined by their past experi-ences and their capacity for trust.
Mr Nelson’s family, for example, may per-ceive that the healthcare team no longer acts inhis interests because suggested interventionsare incongruent with the family’s understand-ing of what is best for him. The family’s capac-ity to trust may also be diminished in the cur-rent situation as a result of past experiences,such as when a diagnosis was missed or con-cerns were dismissed. Similarly, some cliniciansmay perceive that their expectations as to howthey will interact and make decisions with thefamily have been violated, or they may feel thattheir competence is being challenged when pa-tients or families do not follow prescribed care.When family members disregard the prefer-ences documented in a medical directive, clini-cians may feel that they are being asked to be-tray deeply held professional values and anexplicit promise to act on the patient’s behalf.Both parties may be responding to each otherfrom a diminished capacity for trust that re-sults from experiencing each other’s behaviors,consciously or unconsciously, as betrayal.
Trust is complex, emotionally provocative,and multidimensional and essential to the ho-listic care of critically ill patients. When partieswithin a relationship have a diminished capac-ity for trust, misunderstandings, diminishedcooperation, and conflict often result.
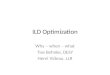
A Model for Transactional TrustThe Transactional Trust component of theReina Trust & Betrayal Model offers guidancein creating a trustworthy environment for care(Figure 1). Trust is transactional in that it existsin relationships between at least 2 parties, in-volves a mutual exchange, and is created incre-mentally over time.4 Transactional trust con-tains key elements found in analyses of theconcept of trust in the literature.5,8–13 Its ele-ments are congruent with the standards for ahealthy workplace environment,3 especiallyskilled communication, true collaboration,effective decision making, and authentic lead-ership.3 Each element relates to and integrateswith the others to create trustworthiness.
The Reina Trust & Betrayal Model defines3 types of Transactional Trust: (1) Competence
Figure 1: The Transactional Trust diagram from the Reina Trust & Betrayal Model. Reprintedwith permission from Reina DS, Reina ML. Trust and Betrayal in the Workplace: BuildingEffective Relationships in Your Organization. 2nd ed. San Francisco: Berrett-Kohler; 2006.

RUSHTON ET AL AACN Advanced Cri t ical Care
22
Trust, or trust of capability; (2) ContractualTrust, or trust of character; and (3) Communi-cation Trust, or trust of disclosure.4 For eachtype of trust, the model specifies behaviors thatare essential for building that trust and suggestsways to interact with patients and families.
Competence Trust: The Trust of CapabilityCompetence trust involves honoring the inher-ent wisdom that resides within each person toknow oneself and what is right for them and tohonor the knowledge and skills that they pos-sess. Applied to critical care, the competenceof the critical care professional, patient, andfamily must be considered within their respec-tive roles to build trustworthy relationships.When competence trust is present, patientsand families feel respected and are able to uti-lize their abilities to make decisions; cope withdisease, disability, and death; and carry outtreatment plans. Likewise, critical care clini-cians are able to practice congruently withpractice standards, ethical norms, and profes-sional guidelines.
From a professional perspective, compe-tence is a foundation for critical care prac-tice. It involves more than technical care-giving skills. Competence requires matchingknowledge, skills, and behaviors with theneeds of patients, families, colleagues, and in-stitutions to create trustworthy relationshipsand service. This is consistent with theAACN’s Synergy Model for Patient Care,14
which considers the patient’s needs andunique personal characteristics in the contextof family and community, and of nurses andwhere they practice.15 Competence also en-compasses skills in communication, ethicaldeliberation, professionalism, and clinicaljudgment.
In critical care settings, where events are of-ten unpredictable and stakes are high, criticalcare professionals must understand the pa-tient’s disease trajectory and prognosis, thecontours of possible treatments, and the bene-fits, burdens, and boundaries of ethically per-missible actions. Clinicians must work witheach other and with the patient and family todevelop patient-centric goals and treatmentplans. Ongoing communication is critical.Although families unable to accept a poorprognosis may appear to question the careteam’s competence, their concern often re-flects a fear of an uncertain or unwelcomeoutcome. In Mr Nelson’s case, the care team
repeatedly declares that he is dying; yet, eachtime he survives. As a result, the healthcareteam’s credibility is compromised and trust isundermined.
Critical care professionals can build compe-tence trust by trusting in the capabilities of oth-ers, including patients, families, and colleagues,supporting each person’s talents, and seekinginput into decisions and plans. It requires thatclinicians practice humility, engage in inquiry,honor the patient’s choices, and express com-passion. Table 1 includes questions that can beused to assess competence trust.
Acknowledge People’s Skills and AbilitiesCritical care professionals demonstrate com-petence trust when they work closely withpatients and families to clarify their inten-tions and assess their preferences. The act ofengaging the patient and family in exploringand understanding the implications of certaindecisions on the whole person and the family
Table 1: Competence Trust InquiryQuestions: Patient/Family/Professional4
Are power imbalances and vulnerabilitiesacknowledged?
How is respect for the patients’ and families’ skillsand abilities demonstrated?
Do HCPs appreciate and invite the patients’ andfamilies’ unique knowledge of themselves ortheir family member?
Are patients and families given the freedom,flexibility, and support to make decisions?
What behaviors communicate the healthcareteam’s competence in managing clinical care?
Do HCPs understand patients’ and families’preferences for making decisions?
How do HCPs involve patients and family membersin care and decision making in ways that aremeaningful to them?
Is it safe for patients and families to raiseobjections or question information?
Are patients and families offered the opportunity and support to learn new skills?
HCPs indicates healthcare professionals.
Adapted with permission from Reina DS, Reina ML. Trust andBetrayal in the Workplace: Building Effective Relationships in YourOrganization. 2nd ed. San Francisco: Berrett-Kohler; 2006.

23
system acknowledges their knowledge, skills,and abilities and demonstrates respect.
Critical care professionals can build or,when necessary, rebuild competence trust byengaging in an ongoing process of inquiry andreflection. End-of-life discussions representedin Mr Nelson’s case can be framed to honorboth the hopes of the patient or family and thereality of the situation and to simultaneouslyprepare for the possibility of death. Encourag-ing but not imposing such a framework cansupport the evolution of both hope and prepa-ration for death as the patient’s condition dete-riorates. In Mr Nelson’s case, talking with thefamily members about how he lived his lifeand listening to their stories about him canhelp them feel understood and heard. Clini-cians can engage the family in guided reflec-tion, ask them what Mr Nelson would want inthis circumstance, explore their fears, andwork with them in the synergistic process of“hoping for the best and planning for theworst.”16 A supportive approach does not de-mand that the family abandon its hope for MrNelson’s continued survival but allows ongo-ing dialogue about the possibility of death.
Allow People to Make Decisions and Seek Their InputCompetence trust supports patients and fami-lies in their own decision-making process andinvolves others who can support and facilitatepatients’ or families’ own internal resources.Inquiring about how they can be helped andsupported, the strengths that serve them asthey navigate through difficult times, andpractices that support their well-being ac-knowledges the inner capabilities of patientsand families.17
Trustworthiness in Mr Nelson’s situation re-quires that the healthcare team truly honor andrespect patient and family choices that may dif-fer from what the healthcare team propose.Clinicians must not be judgmental lest the fam-ily’s trust get contracted, leading them to feel-ings of betrayal. Feelings of betrayal can be ex-acerbated by the Nelson family’s past orcurrent experiences. The Nelsons’ faith may beweakened because prayers for a full recoveryhave not been realized, thereby diminishingtheir capacity for trust.18 Conceivably, MrsNelson may feel betrayed by her husband’s de-sire to discontinue treatment. Whatever has di-minished capacity for trust, the Nelsons are un-able to engage openly with the healthcare team.
These breaches of trust can be magnified whensystem issues create discontinuity among careproviders, ineffective communication and deci-sion making, or inadequate support systems.
The healthcare team feels challenged in re-sponding to Mr Nelson’s wife and children intrustworthy ways. Rather than withdraw andthreaten abandonment, they must engage, askquestions, and seek to understand. Cliniciansneed to resist inclinations to distance them-selves but, instead, remain fully present to thefamily.19 Trustworthiness is cultivated on thebasis of the healthcare professionals’ capacityfor presence and their ability to bear witness tothe struggle of others as well as their own.19
Help Patients and Families Learn New SkillsAt this point in Mr Nelson’s disease trajectory,the care team can also build trust by turning tocaring practices to lessen his pain and sufferingand to offer his family coping skills and alter-native ways to be with him in his current con-dition. Deliberate use of systems thinking canhelp the critical care team focus on holistic in-terrelationships and the broader needs of thepatient and family. For example, the teammembers can focus on the Nelson family’sneed to provide physical care and offer themopportunities to create his legacy through alife review, memory making, and other closureactivities.17 These activities increase compe-tence trust by the family by recognizing andsupporting their own inherent strengths, skills,and knowledge.
In cases like Mr Nelson’s, competence trustincludes accepting the perspectives of the pa-tient and his family as legitimate and meaning-ful, and working to bridge the gap betweenthem and the perspectives held by healthcareprofessionals. This means evaluating the goalsof the patient-professional relationship, theoutcomes of the process, and the process itselfas time moves forward.
Contractual Trust: The Trust of CharacterContractual trust, another dimension of trans-actional trust, is based on the confidence thatpromises that are made will be kept. Promisesmay concern the expectations patients or theirfamilies have about outcomes, treatmentprocesses, or potential complications to theboundaries and tenor of their relationshipswith healthcare professionals.
Contractual trust is evident in the AACNstandards related to collaboration, effective
VOLUME 18 • NUMBER 1 • JANUARY–MARCH 2007 BUILDING TRUST

RUSHTON ET AL AACN Advanced Cri t ical Care
24
decision making, and appropriate staffing3;it is also consistent with several precepts ofthe American Nurses Association Code ofEthics for Nurses.20 The behaviors that buildcontractual trust include managing expecta-tions, establishing boundaries, delegating ap-propriately, encouraging mutually servingintentions, keeping agreements and consis-tency. Table 2 sets forth questions that assesscontractual trust.
Manage ExpectationsDespite attempts of the critical care team tomake full disclosure of the likelihood of out-comes and complications, patients and theirfamilies may perceive that certain promiseshave been made. During the informed consentprocess before a course of treatment, for ex-ample, the patient and family may interpretpossibilities for treatment as promises for cer-tain outcomes. In the Nelsons’ case, the pa-tient and the family may have expected thathis heart function would be corrected withsurgery. When complications arose and theoutcomes they hoped for did not occur, theymay have felt betrayed. Unless expectationsare clarified and managed, the risk of notmeeting them is high. Trust erodes when ex-pectations remain unmet.
One role of critical care clinicians is tomake expectations explicit and to clarify thelimits and boundaries of what can be done totreat the patient’s condition. Clinicians mustresist inclinations to offer solutions that areunfeasible or are unlikely to change the out-come, in the attempt to lessen patient and fam-ily discomfort. Difficult cases involving longstays in the ICU, where outcomes cannot bepredicted with certainty, involve repeated at-tempts to reassure and inform the patient andfamily of progress and prognosis. Often well-meaning reassurance inadvertently results inallowing hoped-for expectations to remain im-plicit.21 Families who hold on to or form unre-alistic expectations will likely feel betrayedwhen those expectations are not met. In life-threatening situations where patients, families,and healthcare professionals may be over-whelmed by emotion, it is critical that expecta-tions are explicit and realistic.
Mr Nelson and his family came to the ICUwith the clear expectation that the interven-tions offered would cure him, giving the out-come they sought. Mrs Nelson and her chil-dren, especially her son, appear to be unclear
about how to relate to the healthcare team,what roles to play, or how to participate in MrNelson’s care. The healthcare team needs toengage with the family to clarify expectationsat this course in his illness and clarify how theywould like to participate in his decision mak-ing and care. In the highly unlikely event thatMr Nelson recovers well enough to leave theICU, his family must be prepared for whatoutcomes they can expect.
It is also the clinician’s role to make explicitwhat patients or families can expect in terms offrequency of communication, sharing of badnews, and discussing goals and other aspects ofcare. Unspoken expectations about the fre-quency and quality of communication withhealthcare professionals can create opportuni-ties for trust to be broken. The Nelsons,for example, may have been told that theywould receive information at a certain time,but if this does not occur as expected, it can in-tensify their withdrawal because trust has beenbroken.
Establish BoundariesOne key behavior to foster contractual trust isto work with patients, families, and colleaguesto clarify the meaning and conditions of the re-lationship. Establishing therapeutic and pro-fessional boundaries, and identifying sharedintentions about the relationship, helps avoidunintentional betrayals and creates a sharedunderstanding of expectations and of respon-sibility that are essential to building trust.
Clear boundaries, the limits of the profes-sional relationship that allow for a safe, thera-peutic connection between the professional andthe patient, are essential for trustworthy rela-tionships. The beginning of a therapeutic rela-tionship is the best time to establish respectfulboundaries with patients and families. Later,circumstances marked by increasing vulnera-bility may make maintaining a balance of en-gagement and separateness more difficult, es-pecially if either party has a diminishedcapacity for trust.4 Boundary violations, eitherconstricted or diffuse, can undermine trustwor-thiness.4 Critical care professionals, patients,and families may employ constrictive or con-trolling behaviors to create a sense of safetyfrom the uncertain and unpredictable eventsthat are inherent to critically ill patients.
Constrictive or controlling behaviors aremanifest in multiple ways: as rigidity in the in-dividual’s actions and thought, or as criticism of

25
VOLUME 18 • NUMBER 1 • JANUARY–MARCH 2007 BUILDING TRUST
Table 2: Contractual Trust Inquiry Questions: Patient/Family/Professional4
Manage expectations
How do HCPs clarify their understanding of the patients’ and families’ expectations of treatment and relationships?
Are the patients’ and families’ expectations attainable?
What implicit (unspoken) expectations of patients and families or the healthcare team should be made explicit?
What patient and family expectations are being met and not being met?
What might interfere with meeting patient and family expectations?
How do HCPs respond when patient and family expectations are not being met?
Establish boundaries
Does the patient and family understand the roles and responsibilities of the healthcare team?
Do HCPs understand the roles and responsibilities of the patient and family?
How do HCPs help the patient and family see their roles and responsibilities in the healing relationship?
Are there interpersonal boundaries that need to be established or clarified? If so, how might this be done?
Delegate appropriately
How do HCPs invite patients and families to participate in care?
What can be delegated to patients and families to assist in the care of the patients?
What concerns do HCPs have about delegating to patients and families or their participating in care?
How do HCPs know that patients and families clearly understand the activities delegated to them?
How do HCPs ensure that patients and families have the resources to carry out the treatment plan?
Encourage mutually serving intentions
What intentions (eg telling, asking, understanding) do HCPs have in their interactions with patients andfamilies?
Are patients and families aware of each HCP’s intentions toward them?
How do the intentions of HCPs serve them and others?
What assumptions do HCPs make about the intentions of patients and families?
What clarification is needed to verify the intentions of patients and families?
Keep agreements
Are agreements or promises clear and understood by patients and families and the healthcare team?
To what extent are agreements and promises honored?
How do HCPs respond when they are unable to meet an agreement and promise?
Are agreements and promises renegotiated when not met?
Be consistent
To what extent do HCPs consistently communicate, provide care, and make decisions regarding the patient’s care?
To what extent do different teams or team members respond to issues and concerns similarly?
Are policies and practices applied in a reliable way?
Are policies, norms, and practices applied fairly?
Do some patients and families receive “special” treatment?
Does the patient and family have equal access to healthcare team members, treatments, and services?
HCPs indicates healthcare professionals.
Adapted with permission from Reina DS, Reina ML. Trust and Betrayal in the Workplace: Building Effective Relationships in Your Organization.2nd ed. San Francisco: Berrett-Kohler; 2006.

RUSHTON ET AL AACN Advanced Cri t ical Care
26
others not sharing the same values. It can alsobe manifest as distancing behaviors, rangingfrom emotional withdrawal, physical isola-tion, and superficial interactions to raging,hostility, or distraction in a flurry of activity(ie, keeping busy to avoid feeling the feel-ings).22 Healthcare professionals who believethat death represents failure may distancethemselves as they attempt to avoid situationsthat arouse feelings of guilt, sorrow, or grief.23
Nurses’ intimate contact with patients andfamilies puts them at added risk. Patterns of“overinvolvement” may be the clinician’s at-tempt to relieve feelings of loneliness by estab-lishing connections; inappropriate disclosuresand interactions, including breaches of confi-dentiality, may be much the same. Whateverform they take, boundary violations can un-dermine relationships and break trust in everysphere—personal, professional, and community.
Boundary violations are at risk in theNelsons’ case, given Mrs Nelson’s contractedtrust, as evidenced by her withdrawal, and herson’s anger. Although the critical care teammembers believe that Mr Nelson is dying and hiscondition is irreversible, they cannot engage thefamily in considering limitations of aggressivetreatment. Members of the critical care teamneed to guard against trying more aggressive ac-tions to coerce the Nelsons to agree with them.Their role as professionals is to accept the Nelsonfamily’s differences in position as authentic andto engage with the family to work in the bestinterests of the patient.
Delegate AppropriatelyContractual trust also involves matching theneeds of patients and families to participate incare with appropriate opportunities, re-sources, and support. Critical care cliniciansmust be mindful to consider ways to engagepatients and families in meaningful participa-tion in treatment and caregiving. Understand-ing how patients and families wish to partici-pate and their own assessment of theircapacities to do so is the foundation for dele-gating appropriately. Mr Nelson’s wife hasbeen a constant presence at his side. She mayhave preferences about how she would like tocare for him but have insecurities about herability to do so. Without intentional discus-sions with her, the critical care team couldmake unfounded judgments about her inter-ests and skills. Therefore, ongoing dialogue onthe changing needs of the patient and family
should be encouraged to avoid situations thatmay inadvertently break trust.
Encourage Mutually Serving IntentionsEncouraging mutually serving intentions is an-other element of contractual trust. Contrac-tual trust is facilitated when the care teamworks with patients and families in mutuallyenhancing ways toward a common goal. Theresulting interdependence and equity createssynergy that helps healthcare professionalsavoid a paternalistic stance and instead respectthe ability of the patient and family to act ontheir own behalf. Critical care professionalsare more likely to succeed if they are as inter-ested in the patient’s needs as in their own ac-tions. Medical and nursing codes of ethics de-fine service as the intent to promote theinterests of patients and families.20,24
Mutually serving intentions can be under-mined, as evidenced in Mr Nelson’s case. Al-though the critical care team may believe thatthey are being supportive, their words and be-haviors may convey the opposite. The case iscomplicated by Mr Nelson’s own wishes, con-veyed earlier in his treatment. By failing to fol-low through on Mr Nelson’s wishes and refus-ing to discuss treatment options, Mrs Nelsonand her son are communicating their lack oftrust in the healthcare team, or perhaps in theirown ability to make decisions on his behalf.They may not perceive the critical care team tobe listening and responding tothe family’s con-cerns and exploring what could be mutuallyserving. The Nelsons may experience their ownvoice and views as disappearing, and their trustin the healthcare team as well.
Similarly, the critical care team may feelthat they are at odds with the family’s goals forMr Nelson’s treatment. They may perceivethat the family is asking them to do things thatundermine their sense of professional integrity,leading to moral distress.25 Restoring this typeof contractual trust requires attention to build-ing a common purpose and goals among thepatient, family, and critical care team.
Be ConsistentThe consistency and reliability of individuals inhonoring commitments makes or breaks con-tractual trust.4 Disruptions in the continuity ofthe care team often undermine trust, especiallywhen there are frequent changes in approach,information sharing, decision making, or lead-ership. With each transition, the continuity of

27
relationship between the critical care team andfamily is disrupted. Trust can be built by creat-ing systems of care that support continuity andconsistency in approach, decision making,communication, and staffing. The rapidlychanging condition of critically ill patients ne-cessitates an ongoing process of care planningand decision making, and keeping agreementsto preserve trust. In Mr Nelson’s 5-month ICUstay, for example, the care team and its ap-proach have changed frequently. With eachtransition, the continuity of relationship be-tween the critical care team and family was dis-rupted. Strategies that enhance continuity ofthe treatment plan, care providers, resources,and support systems can help rebuild compe-tence trust.
Communication Trust: The Trust of DisclosureCommunication trust is essential to a safe,healing environment, one where critical careprofessionals can develop and sustain relation-ships with patients and families, function incohesive and productive teams, and preservetheir professional and personal integrity andthat of their colleagues and organization.2 Thefirst standard for a healthy workplace isskilled communication; closely related is theability to address and manage conflict.3
Healthcare professionals foster communi-cation trust when they share information, tellthe truth, admit mistakes, maintain confiden-tiality, give and receive constructive feedback,and speak with good purpose.4 These behav-iors demonstrate the willingness to discloseand the quality of that disclosure. Table 3 out-lines key areas to assess communication trust.
Share InformationWhen rooted in respect, communication trustprovides the basis for shared decision makingand informed consent. This type of trust is fos-tered when the healthcare professional sharesinformation that the patient or surrogate iden-tifies as relevant and meaningful. For Mr.Nelson and his family, exploring their prefer-ences for information disclosure and decisionmaking is essential. Moreover, disclosure of in-formation must focus on the patient’s and thefamily’s understanding of the meaning of theinformation and its relevance to outcomes andcomplications. Inherent in information shar-ing are opportunities for misunderstanding ormisinterpretation. Clinicians must be inten-
tional about creating opportunities for ongo-ing discussion.
Tell the TruthTruth-telling involves neutral disclosure ofvarious options, the likelihood of their occur-rence and their consequences, and the degreeof uncertainty surrounding the treatment.Truth-telling also includes professional recom-mendations about the most desirable optionon the basis of their understanding of the per-son, diagnosis, prognosis, and expertise. Opencommunication about these issues decreasesthe likelihood of making decisions without ad-equate notification and involvement.
Communication in life-and-death situa-tions, such as Mr Nelson’s, requires particularhonesty and clarity. Especially under condi-tions of uncertainty and ambiguity, patientsand their families need to be alerted to the factthat the goals of care may change over time.Although Mr Nelson and his family begantreatment with the goal of significant improve-ment in his cardiac function, over time thatgoal was no longer attainable. Other goalssuch as comfort, breathing without ventilatorassistance, increasing periods of alertness, andso on may become priorities. Patients and fam-ilies should be encouraged to communicateopenly with the care team; the informationthey share may improve the ability of the teamto respond promptly and follow through oncare issues.
In Mr Nelson’s case, open communicationcan help minimize the risk of further marginal-izing the family’s involvement in his care.Truth-telling requires that the team membersshare what they do not know along with whatthey do know. Complete disclosure includessharing the possibility of death with Mr Nelsonif he has another period of lucidity and with hiswife and children, explaining its likelihood,and the nature of choices that will be availableto them. Without this exchange, there can beno informed consent.
Admit MistakesAdmitting mistakes is essential for communi-cation trust to exist between a clinician andthe patient and his or her family. If a cliniciandid make a mistake in Mr Nelson’s care, forexample a medication error, his family defi-nitely would want to know about it. For com-munication trust to exist, it is important thatteam members feel safe enough to admit and
VOLUME 18 • NUMBER 1 • JANUARY–MARCH 2007 BUILDING TRUST

RUSHTON ET AL AACN Advanced Cri t ical Care
28
Table 3: Communication Trust Inquiry Questions: Patient/Family/Professional4
Share information
Is information provided willingly, completely, or are patients and families told “what they need to know”?
How do patients and families access information from the healthcare team?
Do patients and families have what they need from HCPs and/or the healthcare system?
Tell the truth
Is information shared with patients and families honestly and accurately?
Are there safe forums for patients and families to express views and concerns?
How are tendencies to assume, prejudge, or overreact managed?
Is the truth told or exaggerated, “spun,” or selectively disclosed?
How are different opinions about the “truth” heard and mediated?
What is the whole truth that needs to be heard?
What gets in the way of truth telling?
What situations cause concern about truth telling?
What support do you need to be able to fully tell the truth?
Admit mistakes
Do healthcare team members readily admit any mistakes that occur?
How do HCPs take responsibility for mistakes?
What happens when people admit mistakes?
Is there a respectful process for disclosing, systematically analyzing the root causes, and providingsupport when an error occurs?
Give and receive constructive feedback
Are patients and families and HCPs able to give feedback in a respectful and growth-producing way?
Are patients and families and healthcare team members receptive to feedback?
How do HCPs respond to negative feedback, disagreements, or different views?
Do HCPs provide higher purpose feedback focused on the patient’s and family’s expectations and needs,or do they provide feedback with the intent of proving another person wrong?
Maintain confidentiality
Are preferences for privacy discussed with the patient and family?
Are competent patients asked who should have access to information about their treatment and condition?
Are the norms for disclosure of information about the patient with other members of the healthcareteam discussed?
Are institutional mechanisms to protect the patient’s privacy discussed?
How are boundaries of confidentiality honored and respected?
Speak with good purpose
Do HCPs explore what the patient or family thinks, or how the conversation makes them feel aboutthemselves as people?
Do HCPs engage in honest, clear, and respectful communication with patients and their families?
Do HCPs focus on what is said and what is not, and what is understood and what misunderstood, duringinteractions with patients and family members?
Do HCPs speak directly to patients and their families regarding their issues and concerns?
Do HCPs talk about issues and concerns they have with patients or families behind their backs, during shift report, or in other forums?
HCPs indicates healthcare professionals.
Adapted with permission from Reina DS, Reina ML. Trust and Betrayal in the Workplace: Building Effective Relationships in Your Organization.2nd ed. San Francisco: Berrett-Kohler; 2006.

29
VOLUME 18 • NUMBER 1 • JANUARY–MARCH 2007 BUILDING TRUST
take responsibility for their mistakes versusliving in fear of major repercussions. Establish-ing a respectful process for disclosing, system-atically analyzing the root causes, and provid-ing support when an error occurs is necessaryfor effective patient care and communicationtrust among the healthcare team members.
Give/Receive Constructive FeedbackIn a life-and-death situation such as MrNelson’s, giving and receiving constructive feed-back between clinicians and patients/families isvital. The message is important, but how themessage is delivered affects the receptivity of thefeedback. If the feedback is given in a respectfulmanner and the intention being a higher pur-pose focused on the patient’s and family’s ex-pectations and needs, then the relationship hasthe opportunity to grow. Providing feedbackwith the intent of making the person wrong iscounterproductive. In addition, how the health-care team member responds to negative feed-back, disagreements, or different views signifi-cantly affects the trusting relationship betweenclinicians and their patients and families.
Maintain ConfidentialityParamount to the trusting relationship is thedegree of confidentiality that is maintained be-tween the clinician and the patient and family.Norms for disclosure of information about thepatient with other members of the healthcareteam need to be discussed and clarified. Insti-tutional mechanisms to protect the patient’sprivacy and boundaries of confidentiality needto be honored and respected. Questions to as-sess this area of communication trust are pre-sented in Table 3.
Speak With Good PurposeSpeaking with good purpose is essential to pro-mote communication trust. When patients,families, and clinicians speak with good pur-pose, they speak directly to one another regard-ing their issues and concerns. When they fail tospeak with good purpose, issues and concernsare talked about behind people’s backs, fuelinggossip and backbiting. During each interactionwith patients and families, team membersshould focus on what is said and what is not,and what is understood and what misunder-stood. They should explore what the patient orfamily thinks, how the conversation makesthem feel about themselves as related to theirrole, and how their values influence their
responses.26 Honest, clear, and respectful com-munication contributes to building the founda-tion of trust essential to compassionate andholistic patient care.
Critical care professionals may inadver-tently create an opportunity for betrayal bycreating an illusion of choice or control whennone exists. According to the critical careteam, Mr Nelson’s condition is irreversibleand it believes that he is dying. Offering MrNelson’s wife and son the option to pursue ag-gressive life-sustaining treatments may inad-vertently give them the impression that theyhave the option to choose recovery and en-hanced quality of life. In reality, the onlychoice they have is how he lives until he dies; itis not a matter of whether he will die but whenand how. This degree of clarity and honestycan facilitate the family’s understanding of MrNelson’s condition and their grieving.
Building Trust: An Ongoing CommitmentThe goal of critical care clinicians is to deliverthe best care possible to critically ill patientsand families in a reliable, consistent, and trust-worthy manner, no matter the diagnosis orprognosis. This article provides insight intohow to create a trustworthy path of care forcritically ill patients and families. The Transac-tional Trust component of the Reina Trust& Betrayal Model identifies behaviors thatbuild trust. When critical care professionalsbecome aware of the myriad ways that trustcan be built, they are able to alter their com-munication, decision making, and behaviors intrustworthy ways. This awareness can lead tothe development of intentional strategies thatcan be integrated into each critical care en-counter, thereby allowing critical care clini-cians to fulfill their promises to patients, fami-lies, and themselves.
References1. Institute of Medicine. Organ Donation: Opportunities for
Action. Washington: National Academies Press; 2006.2. Maxfield D, Grenny J, McMillan R, Patterson K, Switzler A.
Silence kills: the seven crucial conversations for health-care. Available at: http://www.silencekills.com/Download.aspx. Accessed December 19, 2006.
3. American Association of Critical-Care Nurses. AACNStandards for Establishing and Maintaining HealthyWork Environments: A Journey to Excellence. AlisoViejo, Calif: American Association of Critical-CareNurses; 2005.
4. Reina DS, Reina ML. Trust and Betrayal in the Work-place: Building Effective Relationships in Your Organiza-tion. 2nd ed. San Francisco: Berrett-Kohler; 2006.

RUSHTON ET AL AACN Advanced Cri t ical Care
30
5. Thorne SE, Robinson CA. Reciprocal trust in health carerelationships. J Adv Nurs. 1988;13:782–789.
6. Thorne SE, Robinson CA. Guarded alliance: health carerelationships in chronic illness. Image J Nurs Sch. 1989;21:153–157.
7. Butler J. Toward understanding and measuring condi-tions of trust: evolution of a conditions of trust inven-tory. J Manage. 1991;17:643–663.
8. Blakeney RN. A transactional view of the role of trust inorganizational communication. Trans Anal J. 1986;16:95–98.
9. Gibson D. What makes clients trust nurses? SCI Nurs.1990;7:81–85.
10. Pask EJ. Trust: an essential component of nursingpractice—implications for nurse education. Nurse EducToday. 1995;15:190–195.
11. Robinson CA, Thorne S. Strengthening family “interfer-ence.” J Adv Nurs. 1984;9:597–602.
12. Meize-Grochowski R. An analysis of the concept of trust.J Adv Nurs. 1984;9:563–572.
13. Lynn-McHale DJ, Deatrick JA. Trust between family andhealth care provider. J Fam Nurs. 2000;6:230.
14. Hardin SR, Kaplow R. Synergy for Clinical Excellence:The AACN Synergy Model for Patient Care. Boston:Jones & Bartlett; 2004.
15. Curley MA. Patient-nurse synergy: optimizing patients’outcomes. Am J Crit Care. 1998;7:64–72.
16. Back AL, Arnold RM, Quill TE. Hope for the best, andprepare for the worst. Ann Intern Med. 2003;138:439–443.
17. Halifax J, Dossey B, Rushton C. Compassionate Care ofthe Dying: An Integral Approach. Sante Fe: PrajnaMountain Publishers; 2006.
18. Rushton CH, Russell K. The language of miracles: ethicalchallenges. Pediatr Nurse. 1996;22:64–67.
19. Rushton CH. Respect in critical care: a foundationalethical principle. Crit Care Nurse. In press.
20. American Nurses Association. Code of Ethics for NursesWith Interpretive Statements. Washington: AmericanNurses Association; 2001.
21. Steensma DP. Reassurance. J Clin Oncol. 2004;22:3196–3198.
22. Katherine A. Boundaries. Where You End and I Begin.New York: Parkside Publishing Corporation; 1991.
23. Meier DE, Back AL, Morrison RS. The inner life of physi-cians and care of the seriously ill. JAMA. 2001;286:3007–3014.
24. American Medical Association. Code of Medical Ethics.Chicago: American Medical Association; 2001.
25. Rushton CH. Defining and addressing moral distress.AACN Adv Crit Care. 2006;17:161–168.
26. Stone D, Patton B, Heen S, Fisher R. Difficult Conversa-tions: How to Discuss What Matters Most. New York:Penguin Books; 2000.